Embed Size (px)
Citation preview
Sleep and Chemical Dependency
The Problem and the Solution
Mark W. Mahowald, MDThe Retreat
Wayzata, MN7/11/2013
Disclosure of Potential Conflicts of Interest:
None
OverviewOverview of normal sleep
Function of sleepCircadian rhythms
Definition
Magnitude of the problem
Perspectives Why take the complaint seriously?Why the complaint is ignored
Etiology
Diagnosis and Treatment
Insomnia and Chemical Dependency
Management
Other Sleep DisordersRestless Legs SyndromeDelayed Sleep Phase Syndrome
Somnomythology
©MRSDC4
Somnomythology
Everybody needs 8 hours of sleep every night.
The best sleep occurs before midnight.
I know I'll be a wreck the next day if I don't get enough sleep.
Sleep is negotiable.
Exercise improves sleep.
REM sleep deprivation results in psychological or psychiatric problems.

©MRSDC5
Somnomythology - Dreams
Most dreams are in black and white.
Eating unusual foods results in more dreaming or nightmares.
Dreams occur in a flash.
External stimuli cause dreams.
The eye movements of REM sleep are following dream images.
Blind people don't dream.
Normal Sleep
Sleep requirement
Circadian factors
State dissociation
Function of sleep
Synaptic plasticity
Memory consolidation
Consequences of sleep deprivation
Determinants of Sleep
Homeostatic
Circadian
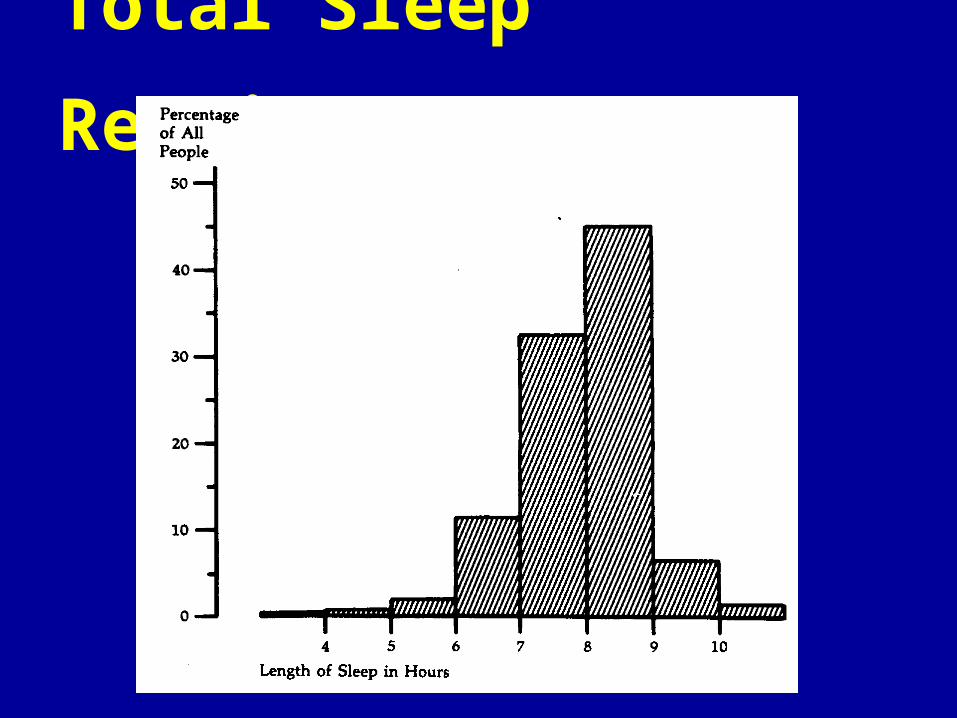
Total Sleep Requirement
©MRSDC9
Circadian Rhythms

©MRSDC10
Light Entrains the Human Biologic Clock
©MRSDC11
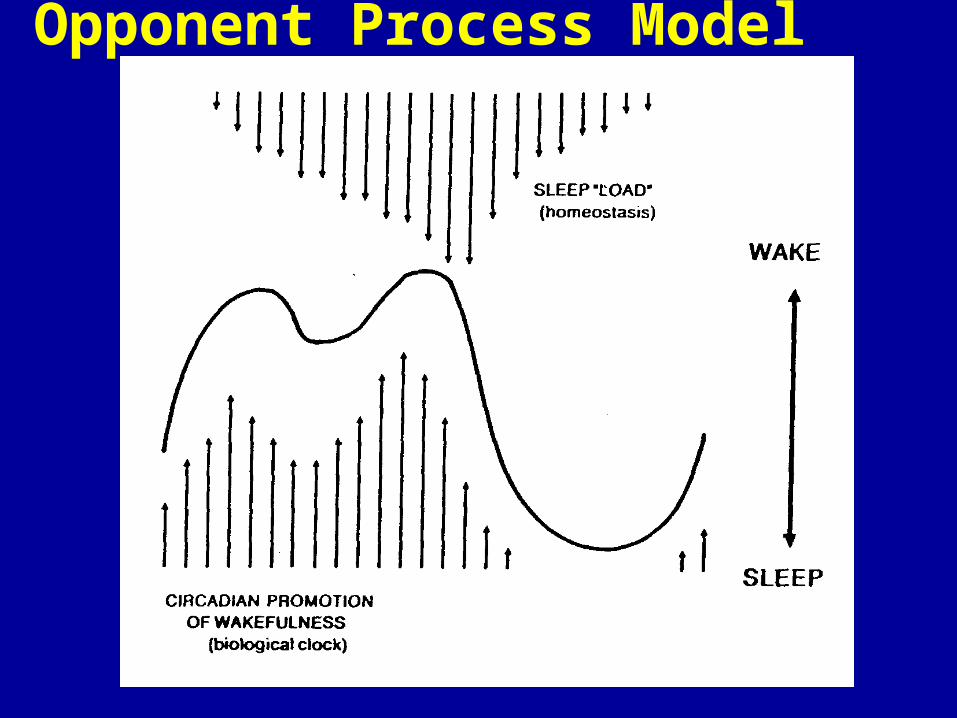
Opponent Process Model
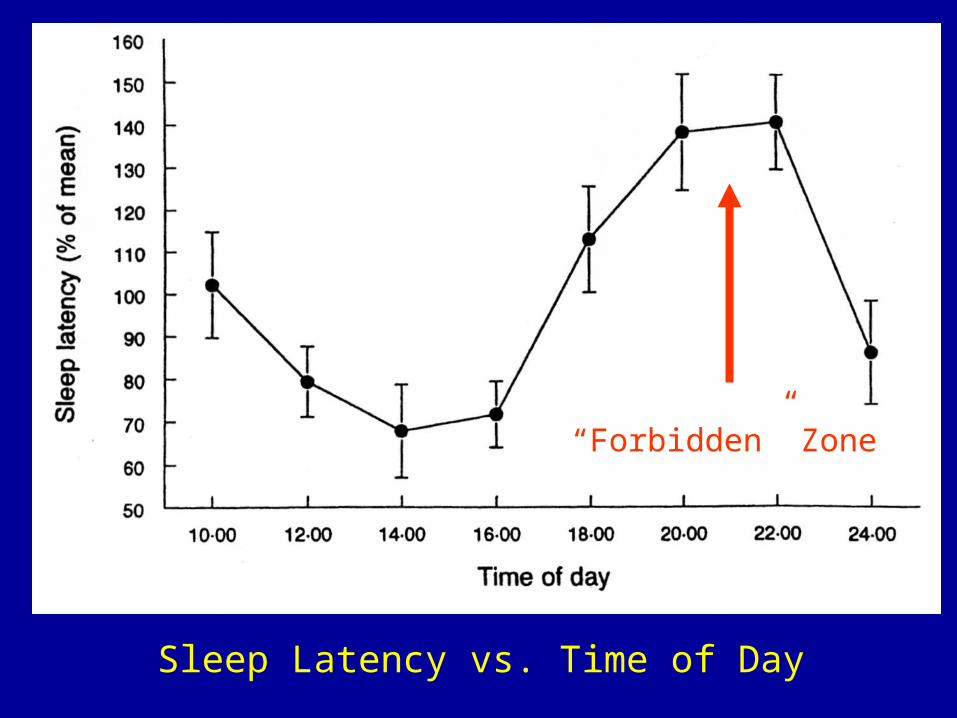
©MRSDCSleep Latency vs. Time of Day
“Forbidden” Zone
State Dissociation
Sleep is not a whole brain, global, phenomenon.
Parts of the brain can be awake while simultaneously, other parts can be asleep.
©MRSDC 13
Function of Sleep

©MRSDC15Almeida Junior: Descanco, (Circa-1882)
What Body Parts Benefit From Sleep ?
©MRSDC16
Function(s) of Sleep
Cognitive
Learning
Memory
Synaptic plasticity
Frank, Rev. Neurosci. 2006
©MRSDC17
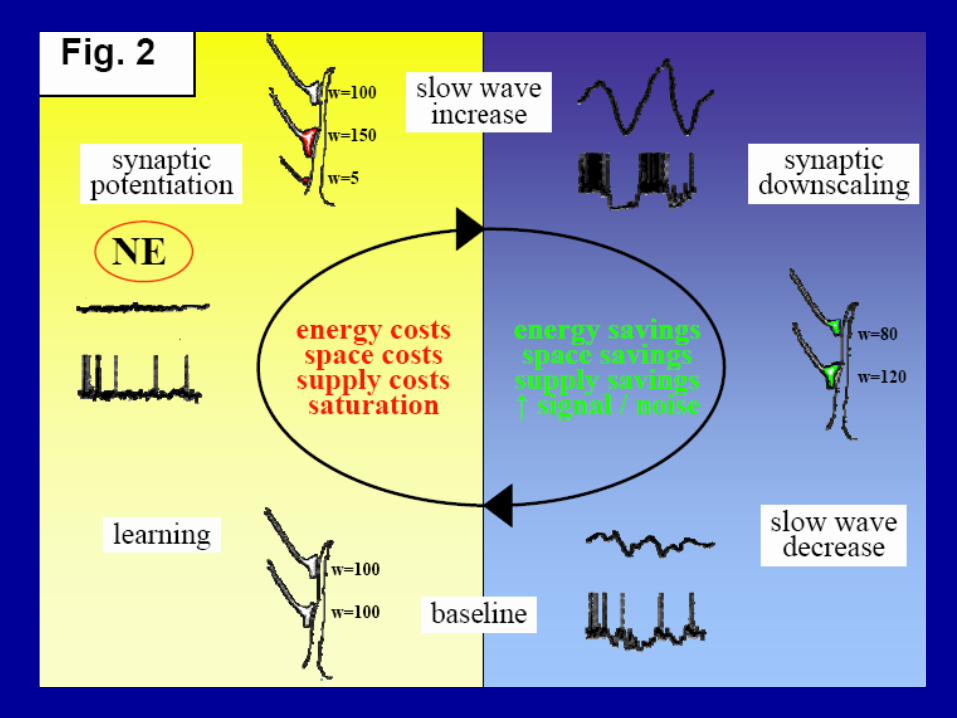
Function of Sleep
Sleep is the price we pay for plasticity, and its goal is the homeostatic regulation of the total synaptic weight impinging on neurons.
A full day of wakefulness is associated with a 20% global increase in cerebral blood flow.
And there is a net increase of synaptic strength (requiring increased energy and volume) during wakefulness.
Tononi, Sleep Med. Reviews, 2006
©MRSDC18
Function of Sleep
These changes presumably would not be sustainable indefinitely.
Sleep renormalizes total synaptic weight to an appropriate baseline level – enforcing synaptic homeostasis.
This results in energy and space saving effects.
Tononi, Sleep Med. Reviews, 2006
©MRSDC19
Sleep Deprivation
Impaired sustained attention
Impaired mood
Insomnia

Insomnia - DefinitionRepeated difficulty with:
Sleep initiation
Sleep consolidation or maintenance
Sleep duration
Sleep quality (non-restorative or poor quality)
Occurs despite adequate time and opportunity for sleep
Results in some form of daytime impairment
Magnitude of the Problem
Insomnia affects up to 30% of all Americans.
Insomnia is much more prevalent in the setting of chemical dependency and withdrawal.
Why so Little Information??
1. Assumption that co-morbid sleep problems will remit with treatment of the primary addiction
2. De-emphasized as less important in early treatment
3. Reluctance to address due to concerns about sleep medication addiction
4. Limited awareness of other treatment options
Arnedt,J of Addict Dis, 2007
Behavioral Consequences of Insomnia
Impairment of:
Working memory
Episodic memory
Executive functioning (verbal fluency, cognitive flexibility)
Fortier-Brochu, Sleep Med Rev, 2012

Insomnia in Alcoholics
Insomnia in previous 6 months
General population: 10%
Alcoholics: 18%
Insomnia in residential treatment centers: 36% - 72%.
Insomnia in Alcoholics
It has been estimated that 10% of alcohol-related expenses can be attributed to insomnia.
Insomnia is a “subacute” withdrawal symptom lasting about 5 weeks.
Sleep abnormalities (by formal sleep studies) may persist for 1-3 years after cessation of drinking.
Insomnia and Alcohol: Bidirectional
Alcohol is used by more than 1 in 10 individuals as a hypnotic agent to self-medicate sleep problems.
Insomnia is a risk factor for the development of alcohol problems.
Subjective and objective sleep continuity variables (insomnia) are robust predictors of relapse during recovery from alcohol dependence.
Arnedt,J of Addict Dis, 2007
Insomnia - Consequences
Medical treatment, drugs Reduced productivity Absenteeism Accidents Hospitalization Depression Increased alcohol consumption
©MRSDC 30
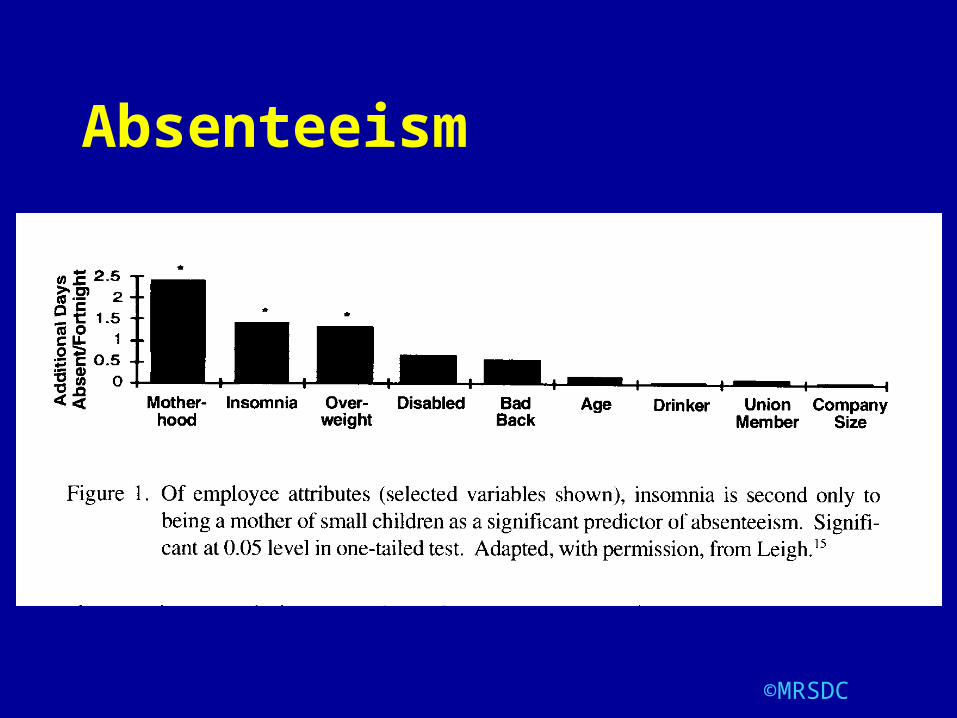
Absenteeism
©MRSDC 31
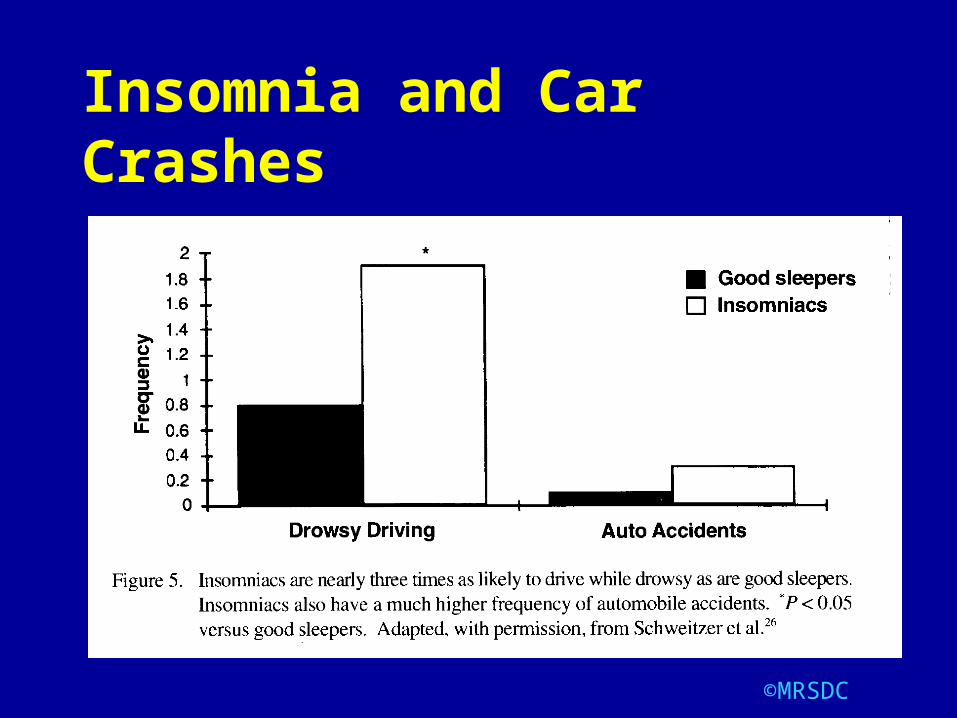
Insomnia and Car Crashes
©MRSDC 32
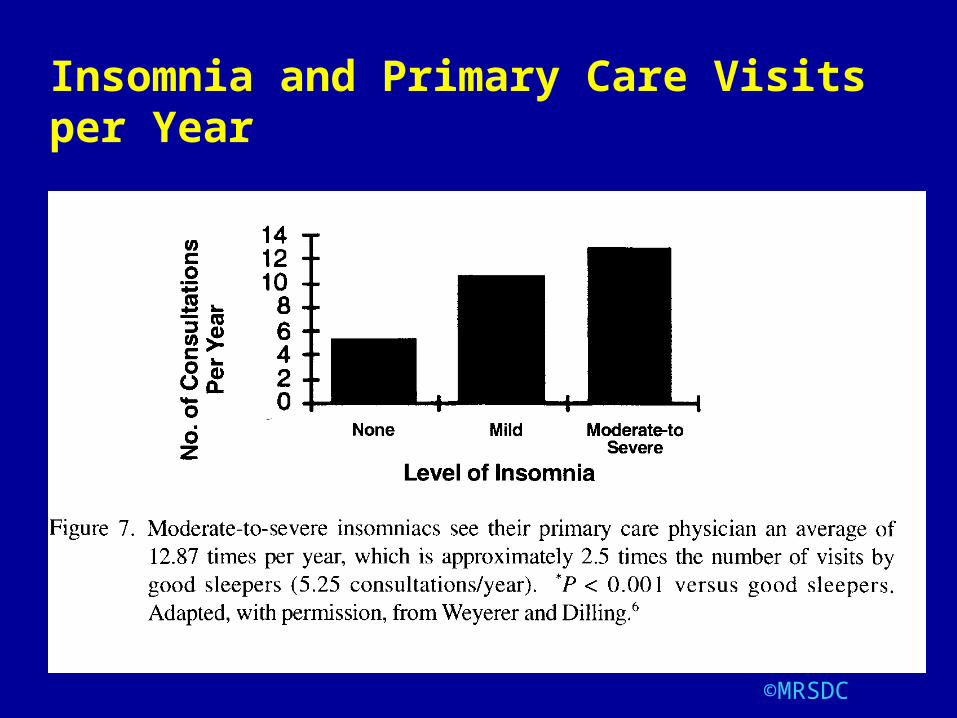
Insomnia and Primary Care Visits per Year
©MRSDC 33
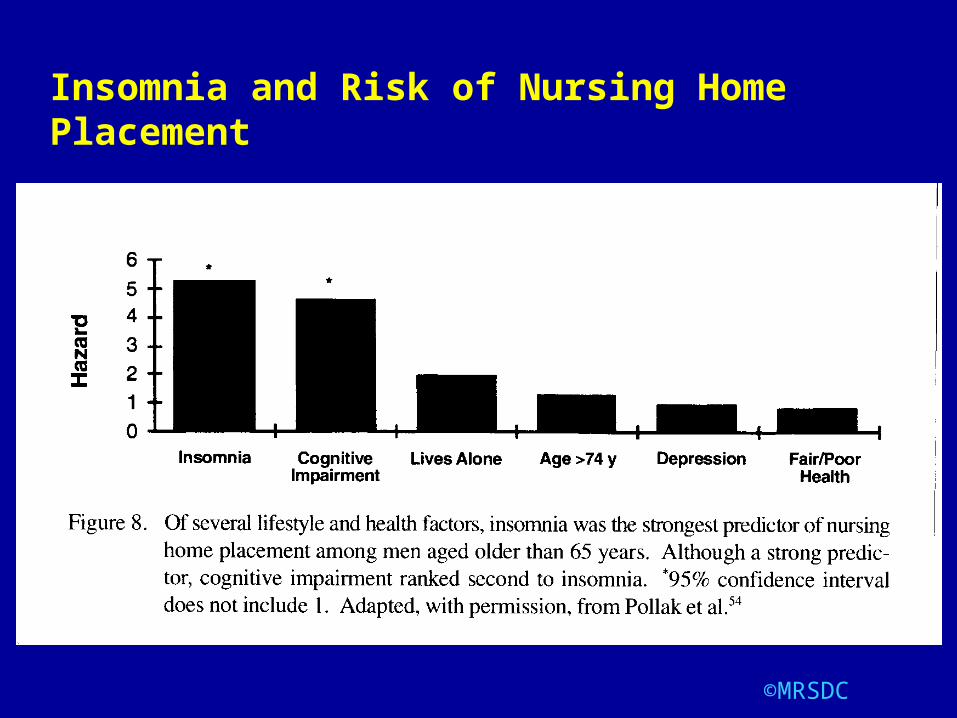
Insomnia and Risk of Nursing Home Placement

©MRSDC 34
Insomnia and Risk of Alcohol Abuse
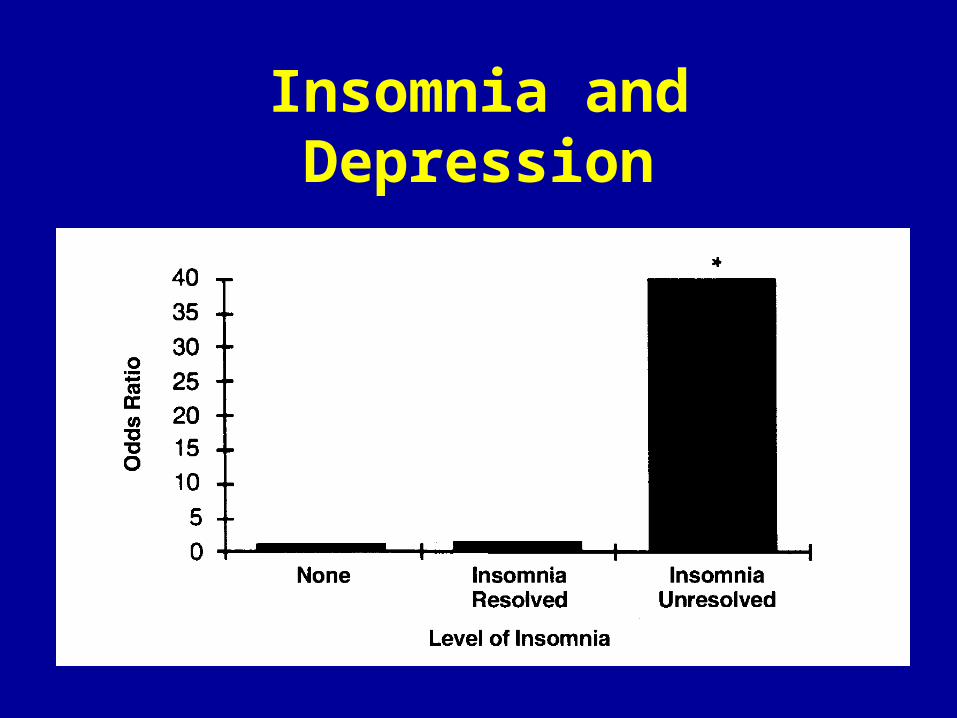
Insomnia and Depression
Insomnia and Depression
Non-depressed people with insomnia have a 2-fold risk to develop depression compared to people with no sleep difficulties.
Baglioni, J of Affective Dis, 2011

Association With Depression
In one study, the relative risk of suicide was 3.6 times greater for those with frequent insomnia compared to those without insomnia.
Paffenbarger et al (1994):
Suicide
Chemical dependency and insomnia are both risk factors for suicide.
Insomnia - Causes
Medical
Psychiatric
Psychological
*Other Sleep Disorders
Insomnia
Contrary to popular opinion, insomnia is often not due to psychiatric or psychological problems.
Insomnia likely results from neurophysiologic vulnerabilities
©MRSDC 41
Insomnia – Somnotypes
The basic level of sleepiness / alertness is genetically influenced and is stable over time.
Two "somnotypes" - "sleepy" and "alert"
The "alert" types may be prone to insomnia.
Some people are inherently more "brittle" sleepers than others.
Insomnia - Physiologic Profiles
Insomniacs are in a state of physiologic hyperarousal.
They are often less sleepy during the day than normals.
Insomnia - Hyperarousal
Activation of sympathetic nervous system and HPA axis.
Increased metabolic ratesElevated levels of circulating catecholaminesIncreased body temperatureAltered heart rate variabilityAltered pupillometry patternsIncreased fast activity on EEG
Seminars in Neurol. 2005
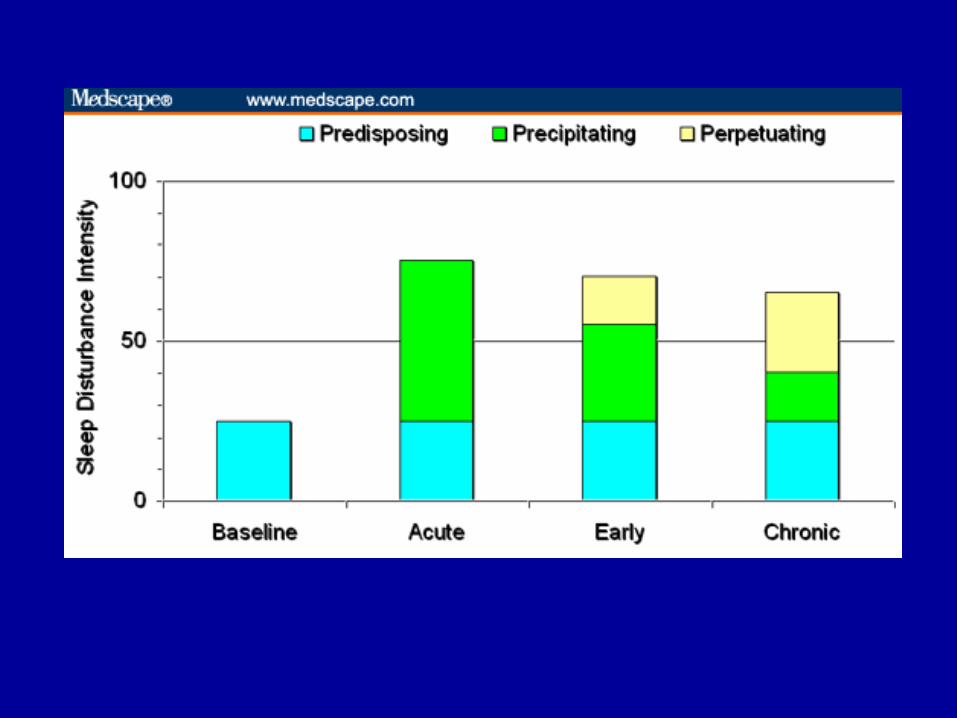
Models of Insomnia
Diathesis-stress model (predisposing, precipitating, and perpetuating factors)
Stimulus control model (classical conditioning)
Cognitive models (thoughts, feelings, and beliefs that may interfere with sleep)
Buysse, Drug Disc Today, 2011
Models of Insomnia
Psychobiological inhibition model (selective attention in the development and maintenance of insomnia)
Neurocognitive model (integrates diathesis stress with neurobiological and neurophysiological observations (increased EEG frequency during sleep) Buysse, Drug Disc Today, 2011
Neurobiological Model of Insomnia
Insomnia is one form of state dissociation – with simultaneous occurrence of activity in sleeping and waking neural activity
Buysse, Drug Disc Today, 2011
Proposed Neurobiological Model
Insomnia is a disorder of sleep-wake regulation characterized by persistent wake-like activity in neural structures during NREM sleep…
resulting in simultaneous and regionally specific waking and sleeping neuronal activity patterns.
Buysse, Drug Disc Today, 2011
Proposed Neurobiological Model
Common pharmacologic and behavioral interventions may reverse some of the regionally specific abnormalities in individuals with untreated insomnia.
Buysse, Drug Disc Today, 2011
Insomnia - Diagnosis
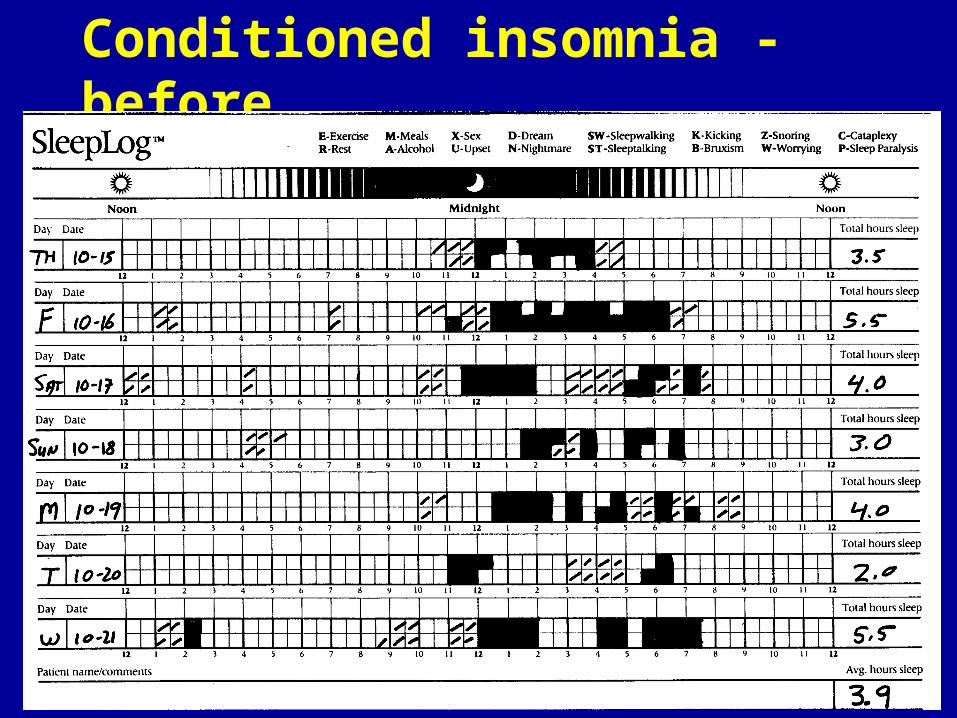
History and physicalSleep diaries
Actigraphy
Psychological tests
Formal sleep studies are usually not indicated
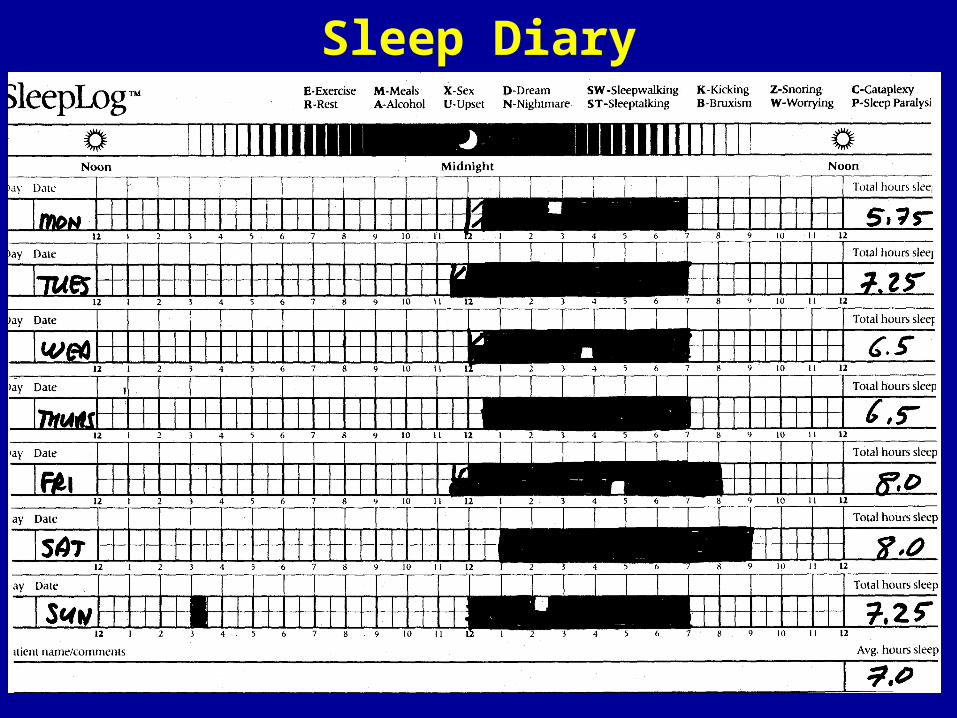
Sleep Diary
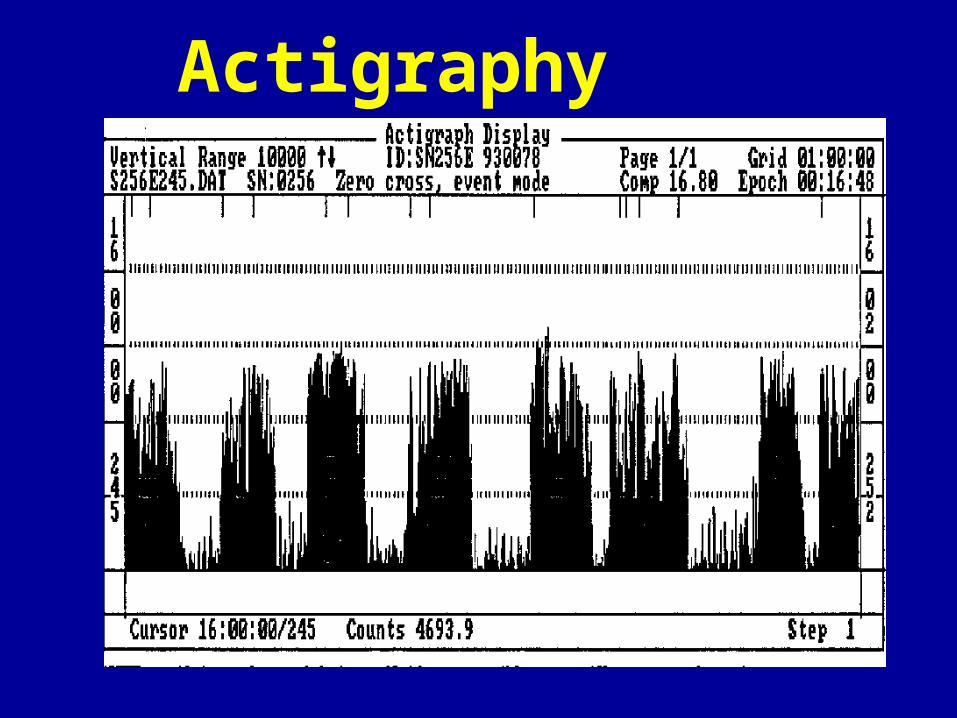
Actigraphy
The Utility of Actigraphy
Without actigraphy, it is virtually impossible to evaluate complaints of severe insomnia or circadian rhythm disorders.
Severe insomnia – case 1
32 y/o man with complaint of severe insomnia due to pain following spinal surgery.
Current medications: morphine (600 mg / day), fentanyl patch, benzodiazepines.
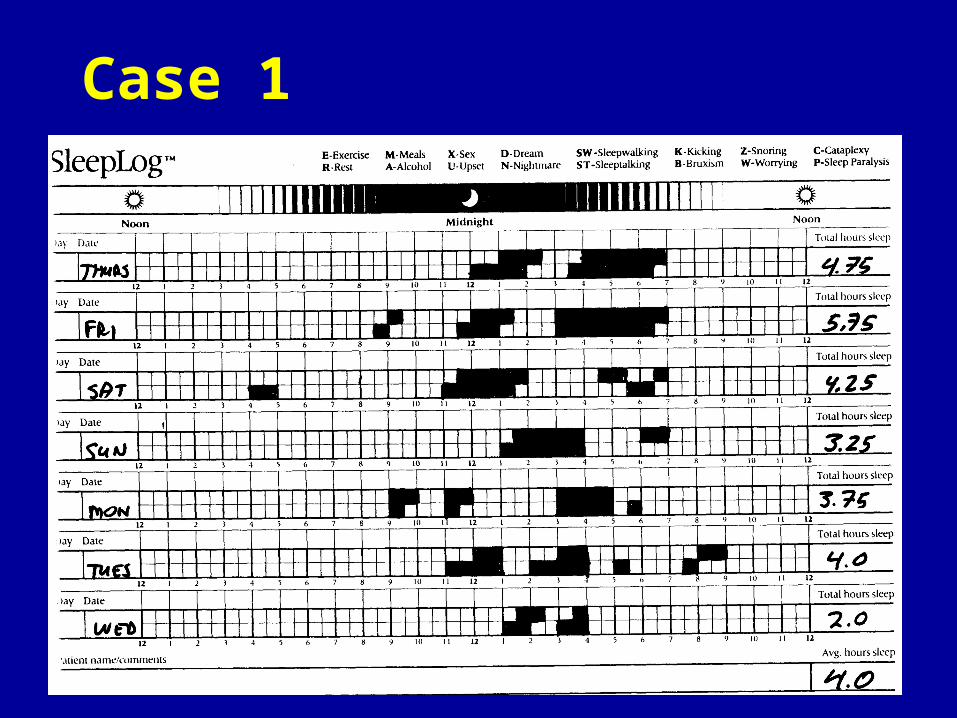
Case 1
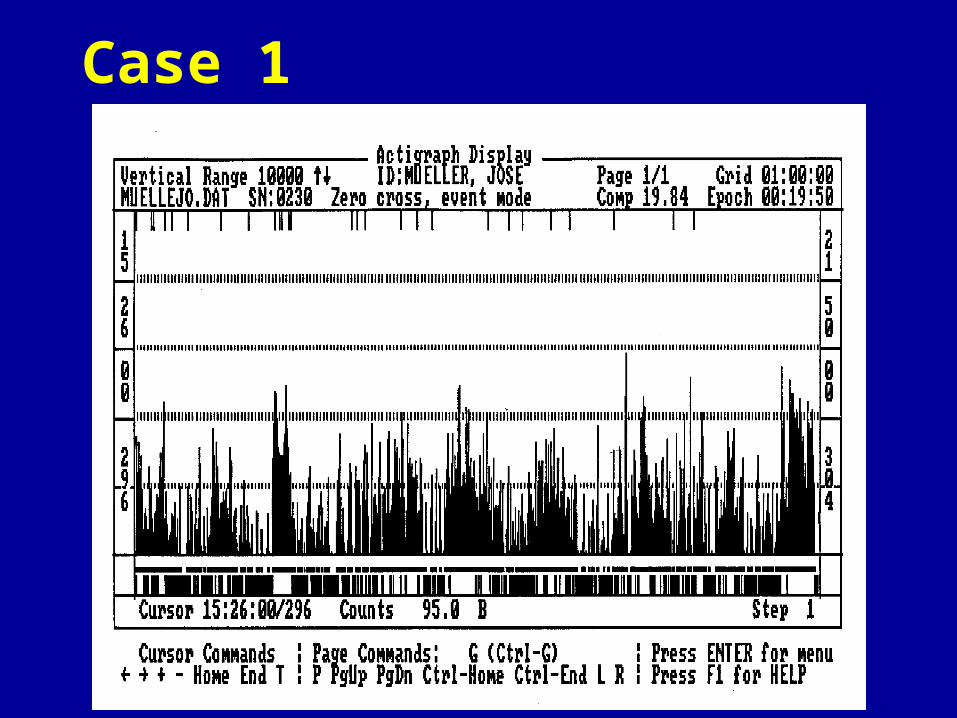
Case 1
©MRSDC 56
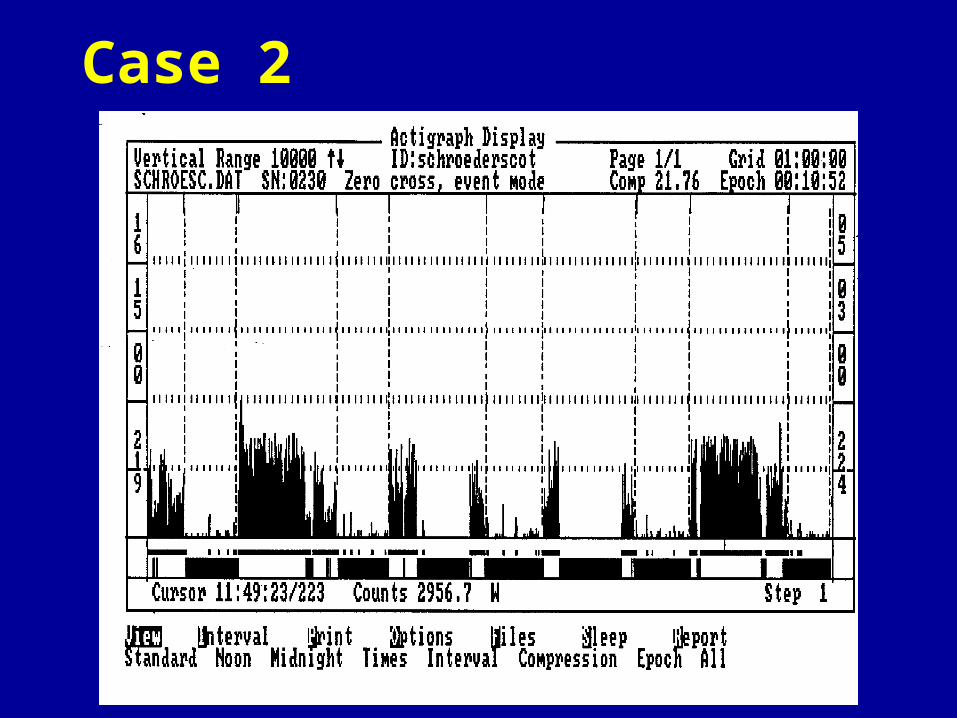
Severe insomnia – case 2
40 y/o businessman who reported sleeping only 2 hours per night, despite treatment with myriad sedative hypnotics.

Case 2
©MRSDC 58
Case 2
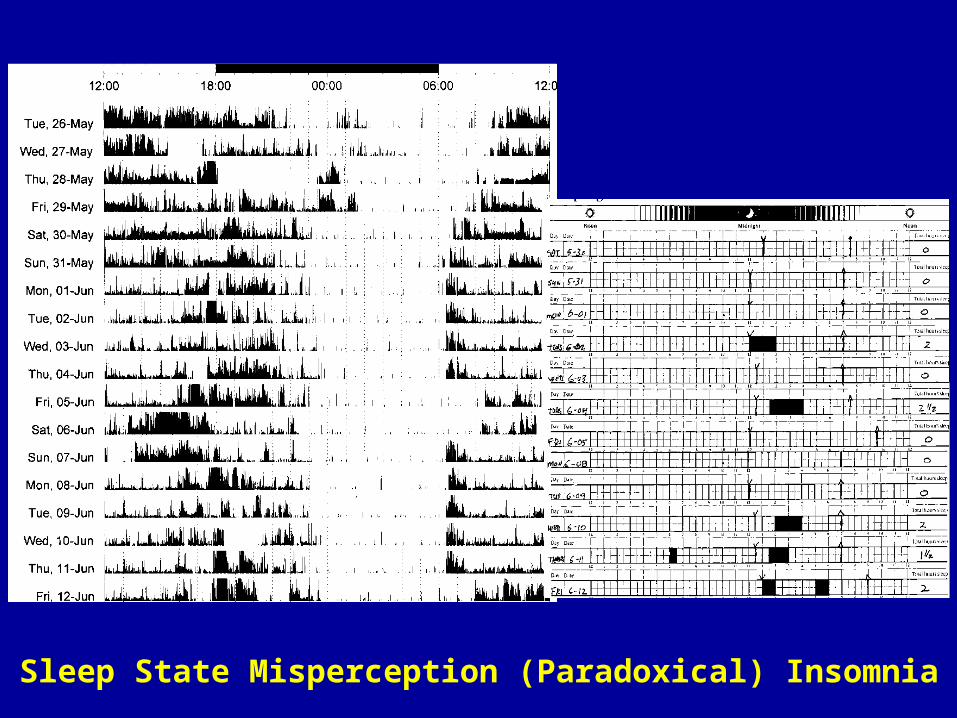
Sleep State Misperception (Paradoxical) Insomnia
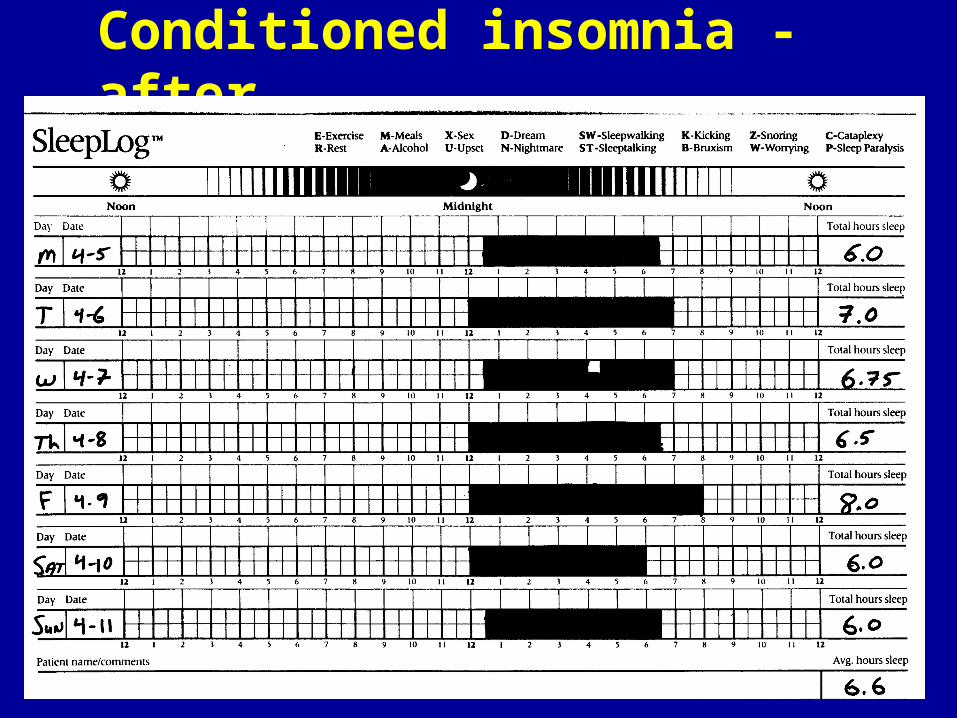
Conditioned Insomnia
©MRSDC 62
Conditioned insomnia - before
©MRSDC 63
Conditioned insomnia - after
Insomnia - Treatment
Pharmacologic
Behavioral
(Often used in combination)
Pharmacologic Treatment
“Natural” remedies
Over-the-counter preparations
Prescription sedative - hypnotics
“Natural” Remedies
Marijuana, cannabis extracts
There are no scientifically valid objective studies to support the often-stated idea that these agents improve sleep.
“Natural” Remedies
Valerian root
Kava
L-tryptophan (5-HT)
Chamomile tea
Passion flower
Coenzyme Q10
Hops
Lemon balm
Lavender
Skull cap
Acupuncture
There is no evidence that acupuncture is an effective treatment for insomnia (or any other medical condition for that matter).
©MRSDC 68
“Acupuncture is Theatrical Placebo”, Colquhoun, Anestheisia-Analgesia, June 2013
OTC Medications
More used than prescription sleep aids
Diphenhydramine (Benadryl, Nytol, Tylenol PM, Advil PM, etc)
Doxylamine (Unisom)
No documented efficacy
Rapid development of tolerance
Next-day sedation – particularly in the elderly
Non-FDA Approved Drugs
Antidepressants
Atypical antipsychotics
Gabapentin (Neurontin)
Carbamazepine (Tegretol)
Non-FDA Approved Drugs
Antidepressant Medications
Trazodone (Desyrel)
Mirtazepine (Remeron)
Amitriptyline (Elavil)
There is no good evidence that any antidepressant medication is effective in the treatment of insomnia in the absence of co-existing depression.
Wiegand, Curr Opinion, 2008
Non-FDA Approved Drugs
Atypical Antipsychotic AgentsQuetiapine (Seroquel)
Ziprasidone (Geodon)
Olanzaprine (Zyprexa)
Side effects: weight gain, metabolic syndrome, extrapyramidal symptoms, tardive dyskinesia.
There is no indication for the use of these drugs for insomnia in the absence of severe psychiatric disease.
Wilson,J Psychopharm, 2010
©MRSDC 73
Antipsychotic Agents for Sleep
“Among medications used for sleep, those with the greatest recent growth in use and risk of adverse effects are second-generation antipsychotic agents.” (particularly quetiapine [Seroquel])
Side effects include: weight gain, disturbances in glucose metabolism, hyperlipidemia
Very costly – up to $10 a day
©MRSDC 74
Hermes, Sleep, 2013
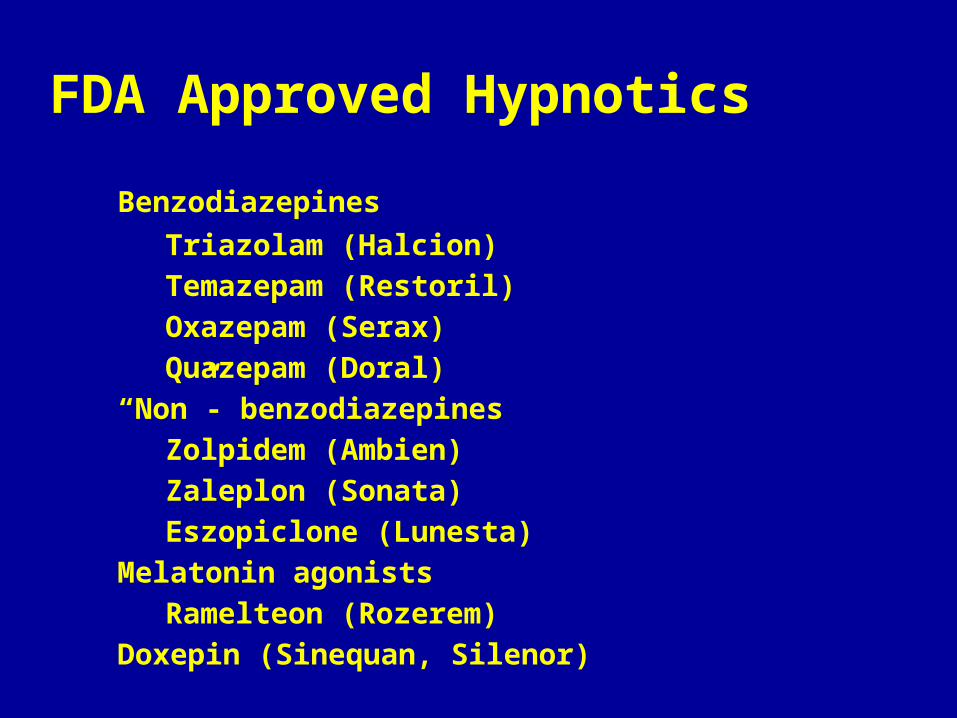
FDA Approved Hypnotics
Benzodiazepines
Triazolam (Halcion)
Temazepam (Restoril)
Oxazepam (Serax)
Quazepam (Doral)
“Non”- benzodiazepines
Zolpidem (Ambien)
Zaleplon (Sonata)
Eszopiclone (Lunesta)
Melatonin agonists
Ramelteon (Rozerem)
Doxepin (Sinequan, Silenor)
FDA Approved Sedatives
Doxepin (Sinequan, Silenor) is an old tricyclic antidepressant which in very low doses (3mg, 6mg) has recently been shown to be a very effective treatment for insomnia.
Virtually no side effects.
Absolutely no abuse/dependency potential.
Really cheap - $0.21/10 mg capsule
FDA Approved Sedatives
Melatonin (Ramelteon, Rozerem)
Of questionable value as a sedative
Used primarily in individuals with a delay in biologic clock
On the Horizon
Hypocretin antagonists
Serotonin antagonists and inverse agonists
Sodium oxybate (GHB)
Histaminergic antagonists

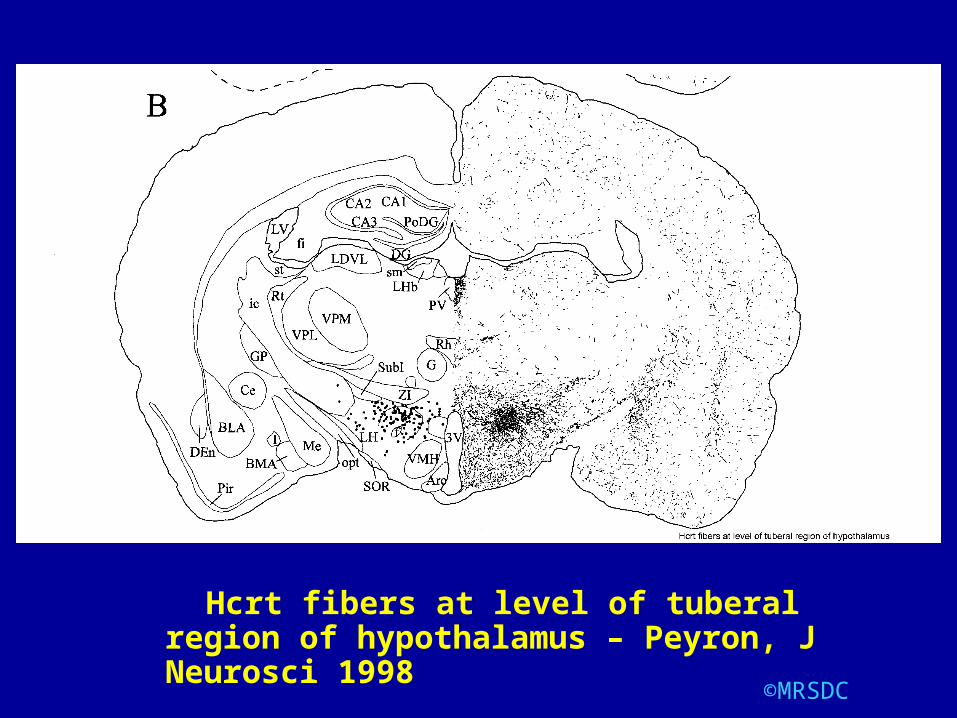
Hypocretin/Orexin System
Important role in both sleep and addiction.
Orexin is a hypothalamic neuropeptide that promotes wakefulness (it is absent in patient with narcolepsy)
Orexin receptor antagonists are effective sleep-inducing agents
©MRSDC 79
©MRSDC 80
Hcrt fibers at level of tuberal region of hypothalamus – Peyron, J Neurosci 1998
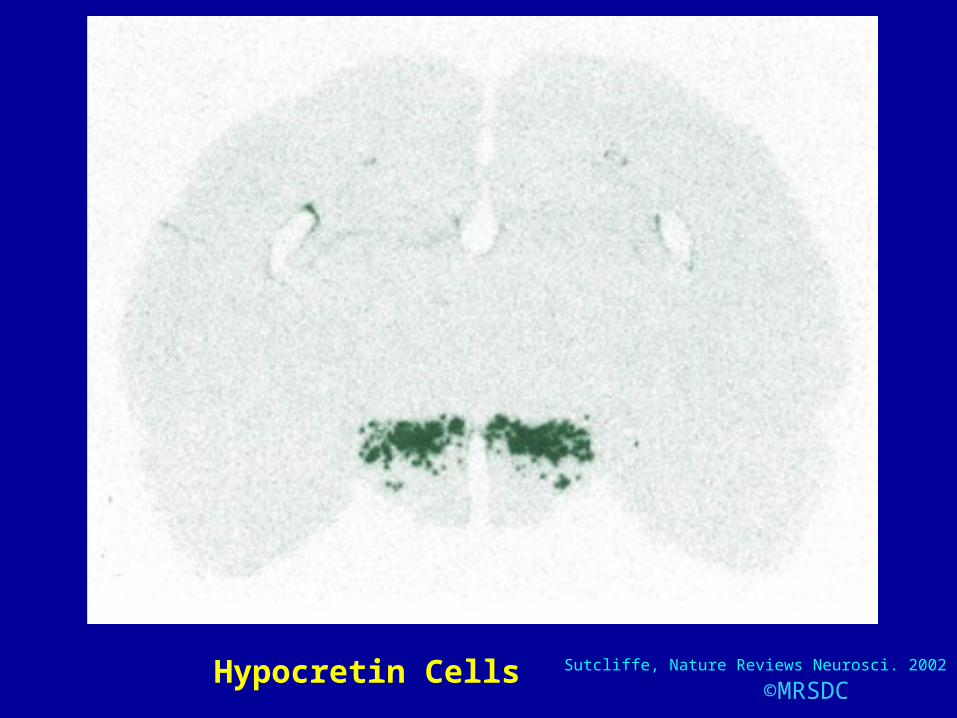
©MRSDC 81Hypocretin Cells Sutcliffe, Nature Reviews Neurosci. 2002

Hypocretin/Orexin Antagonists
Suvorexant
Effective sedative-hypnotic
No abuse potential
Well tolerated
©MRSDC 82
Hypocretin/Orexin System
Also play an important role in drug addiction and reward-related behaviors
Orexin plays a role in potentiating reward circuits and is necessary for the seeking of various classes of addictive drugs
©MRSDC 83
Mahler, Progr in Brain Res, 2012
©MRSDC 84
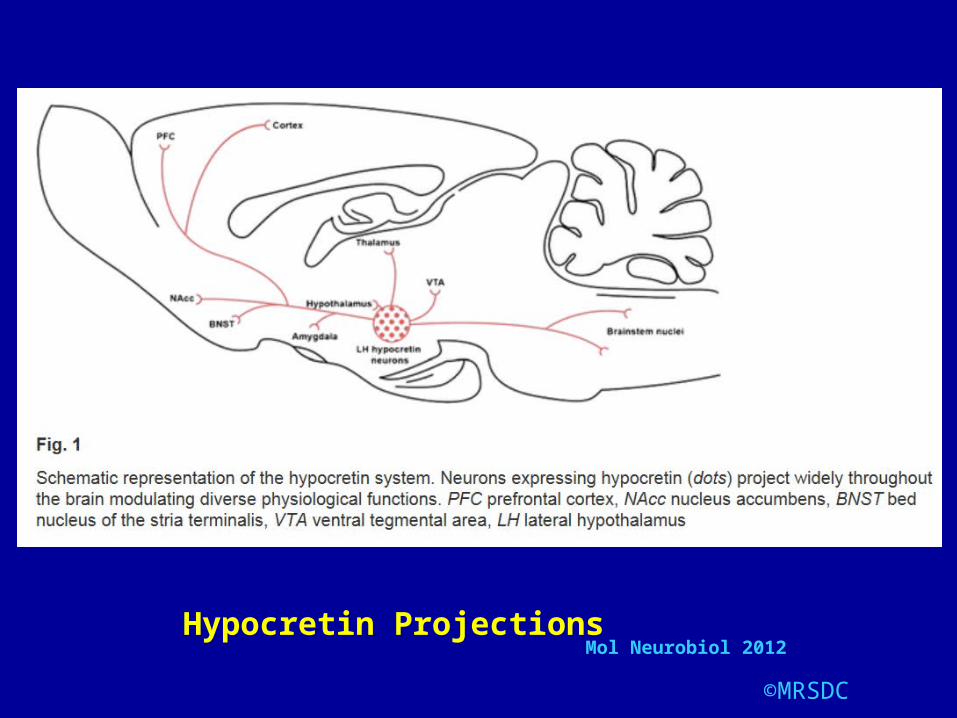
Hypocretin ProjectionsMol Neurobiol 2012
Hypocretin/Orexin Antagonists
Hypocretin/Orexin signaling likely plays a critical role in addiction.
It participates in the primary reinforcing and motivational properties of drugs of abuse
Also, involved in the processes that drive relapse to drug seeking
©MRSDC 85
Plaza-Zabala,Mol Neurobiol, 2012
Insomnia – Behavioral Treatments
Major Contributions:
Hyperarousal
Circadian dysregulation and sleep homeostatic abnormalities
Maladaptive behaviors
Dysfunctional thoughts and beliefs about sleep
Pigeon, J Clin Psychology, 2010
Behavioral Treatments
Sleep Hygiene & Education
Stimulus Control Therapy
Sleep Restriction Therapy
Relaxation Training
Cognitive Behavioral Therapy (CBT)
Sleep Hygiene
1. Regular schedule
2. Relaxing pre-sleep rituals
3. Comfortable environment
4. Bedroom for sleep and sex only
5. Avoid napping (if napping interferes with
sleep the next night)
6. Avoid caffeine within 6 hours of going to
bedPigeon, J Clin Psychology, 2010
Stimulus ControlLimits amount of time spent awake in bed and
develops a more consistent sleep schedule
1.Use alarm set for same time every morning
2.No napping
3.Bedroom only for sleep and sex
4.Go to bed only when sleepy
5.No more than 15 minutes in bed awake
6.Return to bed only when sleepy
Pigeon, J Clin Psychology, 2010
Sleep Restriction
Limits amount of time in bed that matches the ability to fill this with mostly sleep
1.Determine average total sleep time from sleep diaries or actigraphic study
2.Establish fixed wake-up time
3.Set “sleep window” to total sleep time plus 30 minutes
4.Adjust time in bed based upon sleep diaries
Pigeon, J Clin Psychology, 2010

Relaxation Training
Relaxation exercises, such as progressive muscle relaxation, may help you if you lie in bed with your mind racing. Examples include:
Breathing exercises
Guided imagery
Meditation
Progressive muscle relaxation
Cognitive Behavioral Therapy
Positive thinking, or healthy thinking, is a way to help you stay well or cope with a health problem by changing how you think.
Cognitive-behavioral therapy is a type of counseling that can help you understand why you have sleep problems and can show you how to deal with them.
CBT-I: Individual Components
Psycho-education
Behavioral strategies
Cognitive therapy
Relaxation training
Pigeon, J Clin Psychology, 2010

CBT-I
Standard delivery: weekly sessions over 6-8 weeks
Individual or group formats
Begins with sleep education and treatment rationale
Then stimulus control
Then sleep restriction
Then sleep hygiene, cognitive therapy, and relaxation training
Pigeon, J Clin Psychology, 2010
Cognitive Therapy
Focus on negative thoughts and maladaptive beliefs about sleep, insomnia, and its consequences
Challenge veracity and usefulness of those unhelpful thoughts and beliefs and then to change or modify them
CBT-I
Benefits 70-80% of non-alcoholic insomnia patients
More sustained benefit than medications
CBT-I Study in Adolescents
6-session group treatment:
Stimulus control
Bright light
Sleep hygiene
Cognitive therapy
Mindfulness-based stress reduction
Improved sleep and emotional distress and reduced substance use
Britton, Substance Abuse, 2010
Future CBT-I Directions
Brief behavioral treatments for insomnia (BBTI) appear to be effective (2 sessions followed by 2 phone calls)
Online CBT-I treatment programs for insomnia are being developed.
Integration of mindfulness meditation
Buysse, Arch Int Med, 2011
Vincent, Sleep, 2009
Ong, J Clin Psychology, 2010
CBTI
There are preliminary data supporting the efficacy of telephone-delivered CBTI in the treatment of chronic insomnia.
©MRSDC 99
Arnedt, Sleep, 2013
Insomnia - Treatment
Transient / short term(< 30 days)
The effective treatment of acute/short-term insomnia may prevent the development of persistent conditioned
insomnia.
Insomnia - Treatment
Chronic (> 30 days)
Psychological Behavioral Treatments
Pharmaceutical Intervention
Insomnia - Causes
Other Sleep Disorders
Restless Limb Syndrome
Conflict with Circadian Rhythms-i.e. Delayed Sleep Phase Syndrome
Insomnia - Neurologic
Restless Legs Syndrome (RLS)
Unpleasant, subjective sensation in the legs, appearing only at rest - producing an "irresistible need to keep the legs in motion"
RLS - Etiology
RLS is a neurologic movement disorder
Primary abnormality of iron metabolism in CNS
RLS - Treatment
Dopaminergic Agents
Pramipexole (Mirapex)
Ropinirole (Requip)
Opiates
(Benzodiazepines)
(Gabapentin)
Disorders of the
Wake/Sleep Cycle
CategoriesJet lag
Shiftwork
Delayed, advanced sleep phase
syndrome
Irregular or non-24 hour pattern
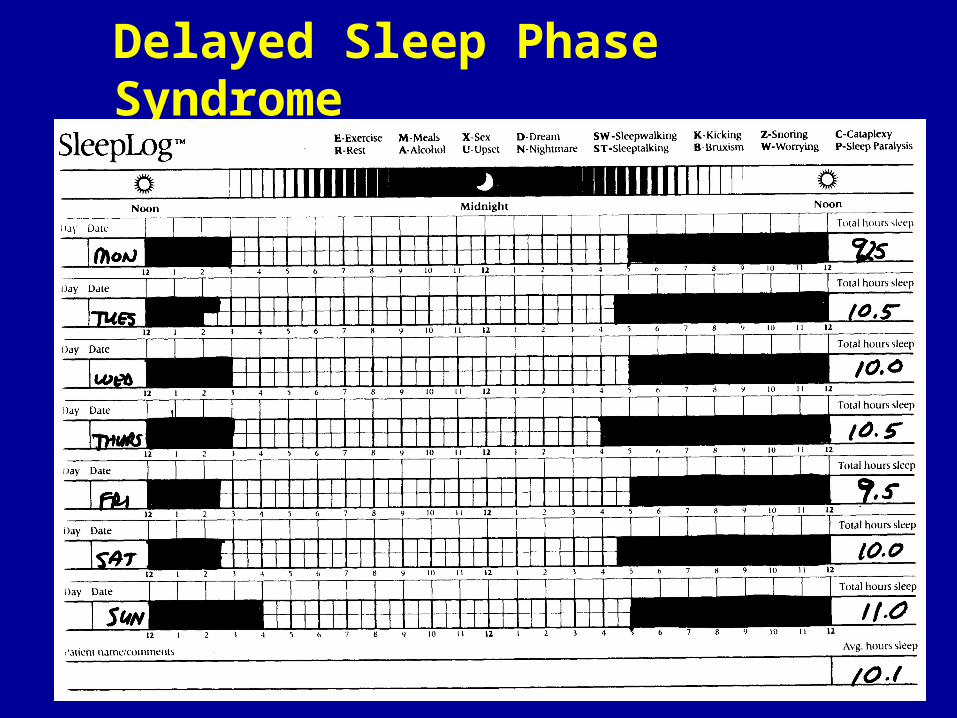
Delayed Sleep Phase Syndrome
Inability to fall asleep before 2-4am
Would prefer to sleep until 10am or noon
Presents as insomnia
©MRSDC 110
Delayed Sleep Phase Syndrome
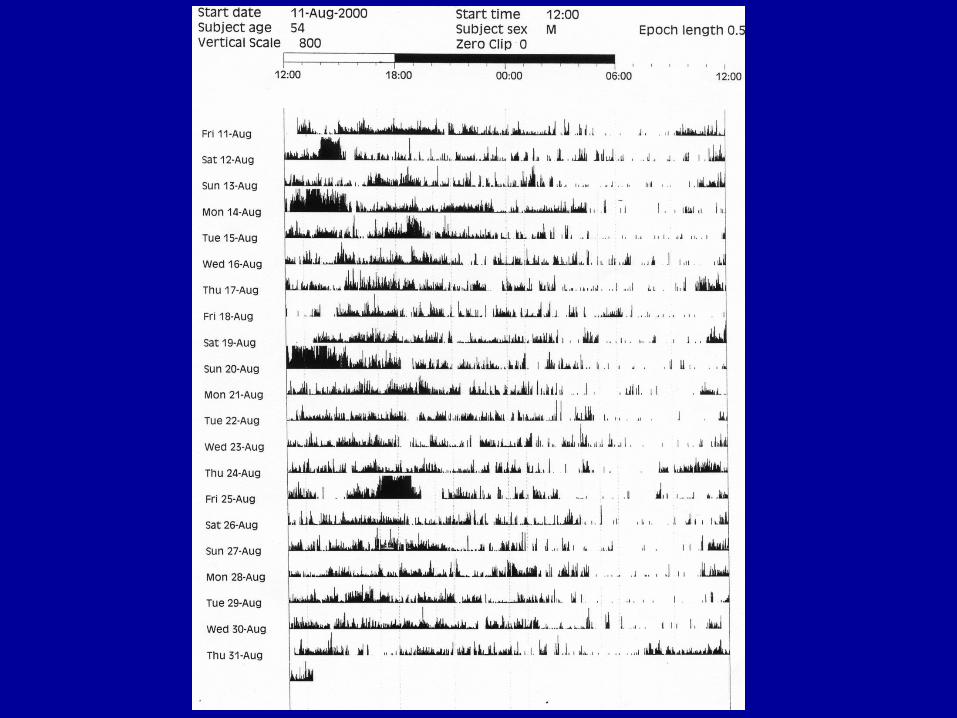
Circadian Factors
Melatonin secretion is disrupted during alcohol withdrawal.
Schmitz, Prog Neuro-Psychophar & Biol Psych, 1996
Circadian Factors
In animal studies, alcohol, opiates, and psychostimulants result in a change in circadian rhythm activity
Bergheim, Brain Res, 2012
Circadian Factors
The circadian clock not only regulates the wake/sleep cycle, but is also implicated in other behavioral and physiological processes relevant to substance abuse – such as mood and cognition.
Hasler, Sleep Med Rev, 2012
Delayed Sleep Phase - Rx
Melatonin 3 mg 5 hours before desired sleep onset.
Bright light exposure in the morning.
Other Interesting Sleep-Addiction Relationships
Drugs and Synaptic Plasticity
Addictive drugs cause changes in synaptic function within the striatal complex which can either mimic or interfere with the induction of synaptic plasticity.
These changes may help explain the long-lasting effect of addictive drugs.
Within the striatum, drugs of abuse modify dendritic morphology, glutamate receptors, and synaptic plasticity.
Grueter, Curr Opin in Neurobiol 2011
Neuroplasticity
Addiction may be a pathology of staged neuroplasticity.
Sleep may affect neuroplasticity.
©MRSDC 118
Kalivas, Neuropsychopharmacology, 2008
Learning and Memory
Memories of learned associations between rewarding properties of drugs of abuse and environmental cues contribute to craving and relapse in humans.
Disruption of reconsolidation dampens or even erases previous memories.
©MRSDC 119
Yan, Neuroscience, 2013
Learning and Memory
Addictive drugs may hijack the learning-and-memory machinery to produce persistent behavioral changes.
If so, this may lead to treatment opportunities.
©MRSDC 120
Robinson, Curr Opin in Neurobiol, 2013
Memory
The persistence of maladaptive drug-associated memories may obstruct the attainment of abstinence.
Addiction can be conceptualized as a disorder of aberrant learning.
Sleep may have an effect on memory.
©MRSDC 121
Milton, Neurosci and Biobehav Rev, 2012
Memory
Persistent, unwanted memories may contribute to drug addiction and chronic relapse.
Disruption of these memories by interfering with reconsolidation through amnestic agents during memory retrieval may be possible.
©MRSDC 122
Sorg, Neurosci and Biobehav. Rev, 2012Milton, Curr. Opin. In Neurobiol. 2012
Memory
Persistent maladaptive memories that maintain drug seeking and are resistant to extinction are a hallmark of addiction.
Therefore, disruption of memory consolidation after retrieval has received attention for its therapeutic potential.
If memories can be disrupted after retieval, then this may have potential for treatment of persistent or exaggerated memory in disorders such as PTSD and addiction.
©MRSDC 123
Tronson, Curr Opin in Neurol, 2012
Memory Consolidation
Persistent, unwanted memories may contribute to addiction and relapse.
One proposed function of sleep is memory consolidation.
Possible therapeutic implication:
Disruption of sleep-related memory reconsolidation through delivery of certain amnestic agents during memory retrieval.
Sorg, Neurosci Biobehav Rev, 2012

©MRSDC 125
Reward Activation
Model (RAM)Perogamvros, L and Schwartz, S. Neurosci Biobehav Rev 36: 1934-1951;2012
Mesolimbic Dopaminergic System (ML-DA)
Implicated in reward and emotional functions
Perturbed in schizophrenia, addiction, and depression
Is active during both wakefulness and sleep
Activation of the “Reward Activation Model” (RAM) for sleep and dreaming has implications for addiction
Sleep problems like insomnia may developmentally precede and predict early onset of alcohol, cigarette, and marijuana use in adolescents and young adults
©MRSDC 126
Perogamvros, Neurosci and Biobehav Rev, 2012
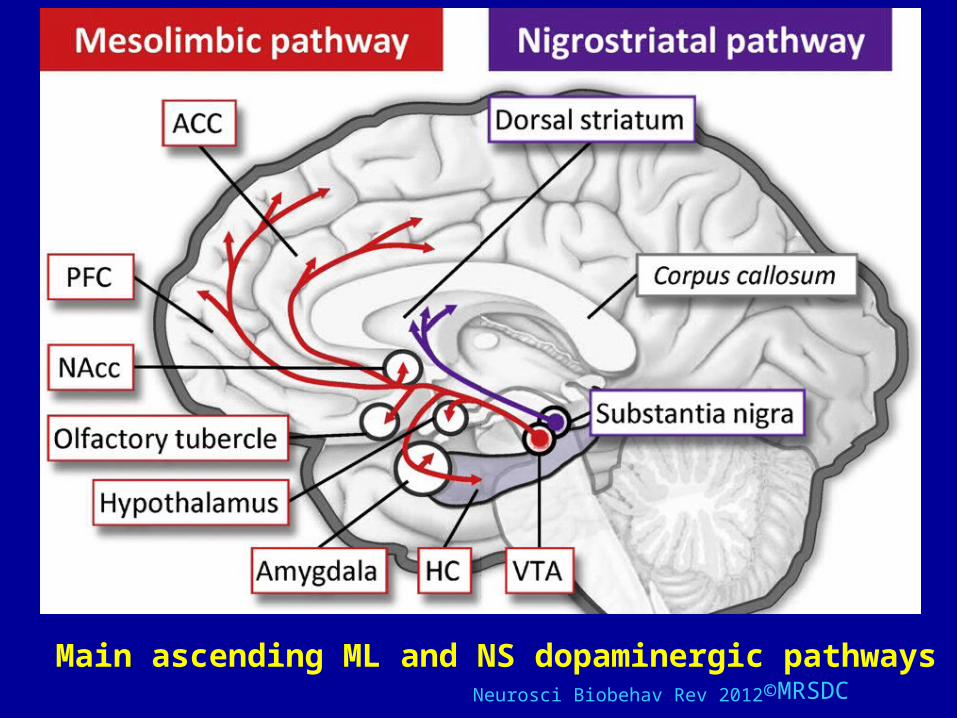
©MRSDC 127Neurosci Biobehav Rev 2012
Main ascending ML and NS dopaminergic pathways
Take-Home Message
Insomnia is very common in the setting of substance abuse and abstinence
Insomnia is a risk factor for relapse
Behavioral techniques are very effective in treating insomnia
Some medications with no abuse potential may be very effective in treating insomnia in this population
Other treatable sleep disorders may be masquerading as insomnia (restless legs syndrome, delayed sleep phase syndrome)
Sleep may be playing a role in maladaptive memory consolidation which may predispose to relapse
©MRSDC129
Somnomythology
©MRSDC130
SomnomythologyEverybody needs 8 hours of sleep every night.
The best sleep occurs before midnight.
I know I'll be a wreck the next day if I don't get enough sleep.
Sleep is negotiable.
Exercise improves sleep.
REM sleep deprivation results in psychological or psychiatric problems.
©MRSDC131
Somnomythology - Dreams
Most dreams are in black and white.
Eating unusual foods results in more dreaming or nightmares.
Dreams occur in a flash.
External stimuli cause dreams.
The eye movements of REM sleep are following dream images.
Blind people don't dream.
©MRSDC132
Somnomythology
Depression, laziness, boredom, slothfulness, or other defects of character cause sleepiness.
These conditions DO NOT cause physiologic sleepiness.
©MRSDC133
Somnomythology
"Incorporation"
Waking experiences and external stimulation determines dream content.
©MRSDC134
©MRSDC135
Dreaming - Incorporation
There is a relatively small overall
proportion of stimulus incorporation
(24%) and experimental modification
(12%) of dream content.
Therefore, ongoing sleep mentation is
relatively impervious to intrusions from
concomitant external sources.

©MRSDC136
Dreaming - Incorporation
Cognitive responses of some form may occur in both REM and NREM sleep as a result of external stimulation.
Pre-sleep films, both neutral and violent, resulted in incorporation in 8% - with no difference between the incorporation rate of neutral vs. violent.
©MRSDC137
Dreaming - Incorporation
Biological drive frustration (thirst, hunger, social isolation) is incorporated into dreams, but is certainly not universal.
There is no incorporation of the apnea stimulus into dreams of patients with obstructive sleep apnea.
Pain, even in patients with chronic pain conditions, is an infrequent dream sensation.
©MRSDC138
Somnomythology
Blind people don't dream.
Blind people don't have rapid eye movements during their REM sleep.

©MRSDC139
Dreaming and Blindness
Blind people do have rapid eye movements during REM sleep.
Congenitally blind people without any history of form vision are able to represent spatial relationships in dream experiences.
©MRSDC140
Dreaming and Blindness
People with acquired blindness report that
their dream visualization is as their waking
visual experience was before they became
blind.
Moreover, their visual imagery includes
well defined imaginal representations of
people and places known only since
becoming blind.
©MRSDC141
Dreaming and Blindness
Therefore, the dream is a constructive
cognitive process, rather than a
reproductive perceptual one.
Dreams are not simply simulations of
seeing: they are simulations of living –
not reflecting life as it is perceived,
but representing life as it is imagined.
©MRSDC142
Does Sleep Deprivation
Predispose to Infection ?
(Or, Were Our Mothers Right ? )
©MRSDC143
Sleep and Infection - Summary
There is no evidence in humans
that sleep deprivation
predisposes to infection, or that
sleep enhances recovery from
infection.
©MRSDC144
Does Exercise
Promote Sleep ?
©MRSDC145
Sleep and Exercise
Eight fit male endurance athletes:
Sleep studied after:
No exercise15-k run43.2-km runUltra-triathlon
©MRSDC146
Sleep and Exercise
Sleep patterns following the no exercise day and the 15-km and 43.2-km run days were similar.
Sleep patterns following the ultra-triathlon day showed increased wakefulness, delayed and decreased REM sleep, and no difference in SWS during 1st 6 hours of sleep.
©MRSDC147
Take-Home Message
Exercise has little, if any,
effect upon sleep.
©MRSDC148
Somnomythology
Coma and anesthesia are not on the wake/sleep continuum.
The state during hypnosis and other "altered states" is simply relaxed wakefulness.
OverviewOverview of normal sleep
Function of sleepCircadian rhythms
Definition
Magnitude of the problem
Perspectives Why take the complaint seriously?Why the complaint is ignored
Etiology
Diagnosis and Treatment
Insomnia and Chemical Dependency
Management
Other Sleep DisordersRestless Legs SyndromeDelayed Sleep Phase Syndrome
Somnomythology
Using Dreams
©MRSDC 150


©MRSDC 152