Embed Size (px)
Citation preview
Indian J Pediat 47: 239-244, 1980
Spectrum of congenital malformations in the newborn
Meharban Singh, M.D., and N.K. Sharma, M.D., D.C.H.
Abstract
Of 6,274 consecut;ve live-births during 1975-78, 170 (2.7 percent) infants were diagnosed to have 241 major congenital malformations. The incidence of malforma- tions among preterm was almost twice (5.3 p~r cent), while two-thirds of infants with internal malformations weighed less than 50th centile for theirgestational age at birth. Musculoskeletaldefects accounted for one-third of all malformations. Out of systemic defect% central nervous system anomalies were most frequent (12.9 per cent) while other system defects (except respiratory system) had an identical frequency of about 10 p~'r ceat. The incidence of neural tube defects was found to be 7 per 1000 total births. Among individual anomalies, club foot, spina bifidal polydactyly, left-to-right cardiac shunt, cleft lip 4- cleft plate, hydrocele, Down syndrome and congenital dislocation of hips had a frequency greater than 1 per 1000 live-births.
In India, congenital malformations are overshadowed by numerically more important causes of neonatal mortality such as low birth weight, birth asphyxia and bacterial infections. Nevertheless, they account for 10-15 per cent of neo- natal deaths in our country. In countries where nutritional disorders and infections have been eradicated, genetic disorders constitute a major public health problem. A similar change in the pattern of diseases is anticipated in our country in due course of time.
The present study was undertaken to determine the frequency of significant or major structural malformations at birth among live-born infants. The still births have not been included because over one- third of these infants are macerated and it is difficult to diagnose internal ano- malies in still-born infants without the
From the Department of Pediatrics and Neonatal Section, All-India Institute of Medical Sciences, New Delhi
Reprint requests:Dr. M. Singh, Director, Institute of Child Health, Kabul, Afghanistan
aid of autopsy. For these reasons incidence of congenital malformations has been reported to vary widely between 7 to 38 per cent among still-born infants. 1-~ Moreover, anomalies among still-borns have no practical implication~ in terms of neonatal diagnosis, manage- ment and survival because they generally carry unsalvagable lethal defects.
Materials and Methods
The consecutive live-born infants delivered at the All-India Institute of Medical Sciences Hospital during the years 1975-78 were examined for major congenital malformations during their hospital stay. A detailed physical exami- nation was conducted at birth, 24 hours ' age and at the time of discharge accor- ding to a scheme previously described in detail) Major congenital malformations were defined to include all those defects causing serious structural, cosmetic and functional disability requiring surgical or medical management. The minor aberra-
240 TItE INDIAN JOURNAL OF PEDIATRICS
tions such as skin tags, capillary heman- giomata, preauricular sinuses, nevi, pilonidal dimples, accessory nipples, tongue-tie and congenital teeth etc. were ignored. Howcver, presence of minor abnormalities often alerted the physician to undertake a mole thorough clinical search to unearth associated major malformations. Because most infants with aner~cephaly are still born, all births
(live q- still births) during 1976-78 were analyzed to ascertain the true incidence of neural tube defects. The clinical diagnosis was complemented by autopsy and/or laparotomy findings as and when available. Detailed anthropometric measurements were taken in all infants.
Results
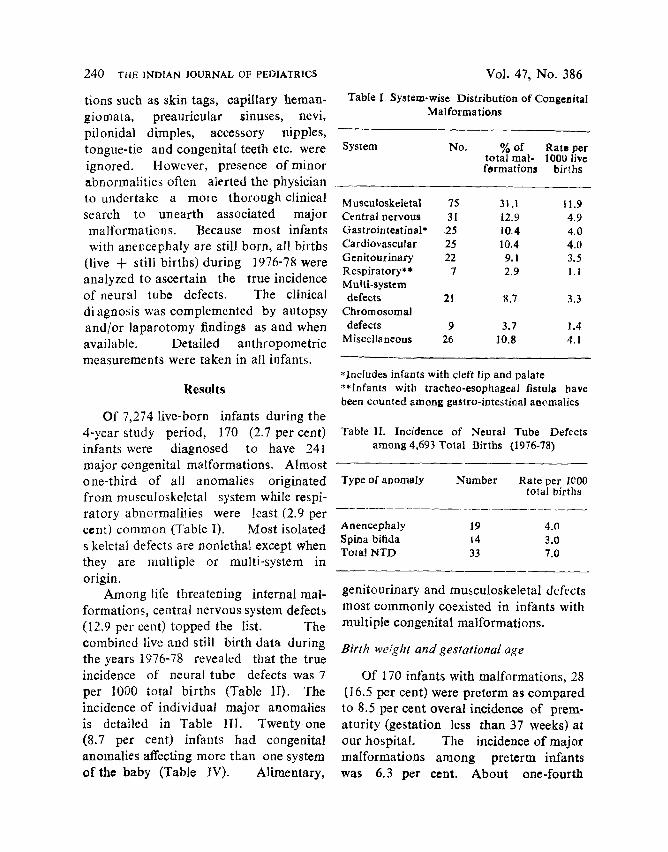
Of 7,274 live-born infants during the 4-year study period, 170 (2.7 per cent) infants were diagnosed to have 241 major congenital malformations. Almost one-third of all anomalies originated from musculoskeletal system while respi- ratory abnormalilies were least (2.9 per cent) common (Table I). Most isolated skeletal defects are nonlethal except when they are multiple or multi-system in origin.
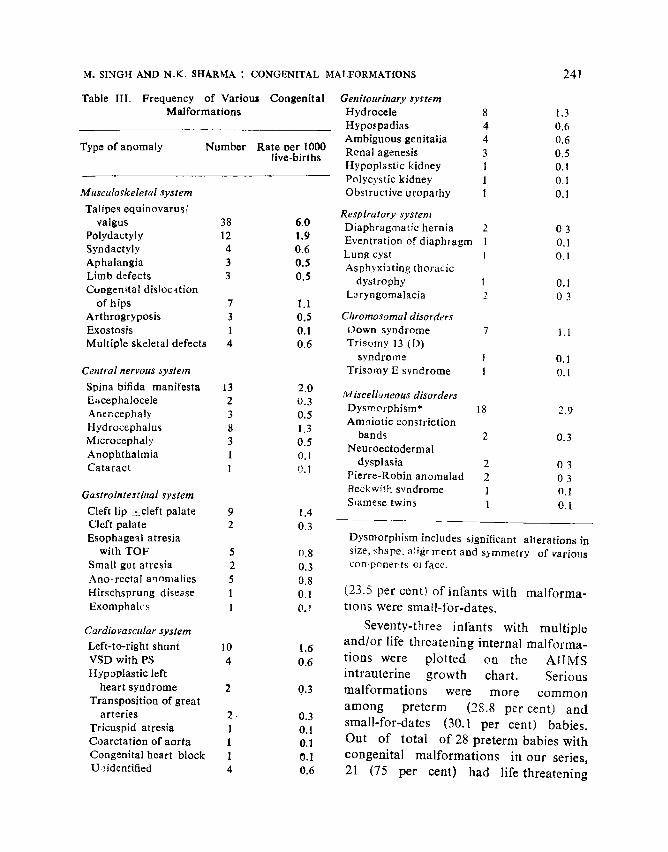
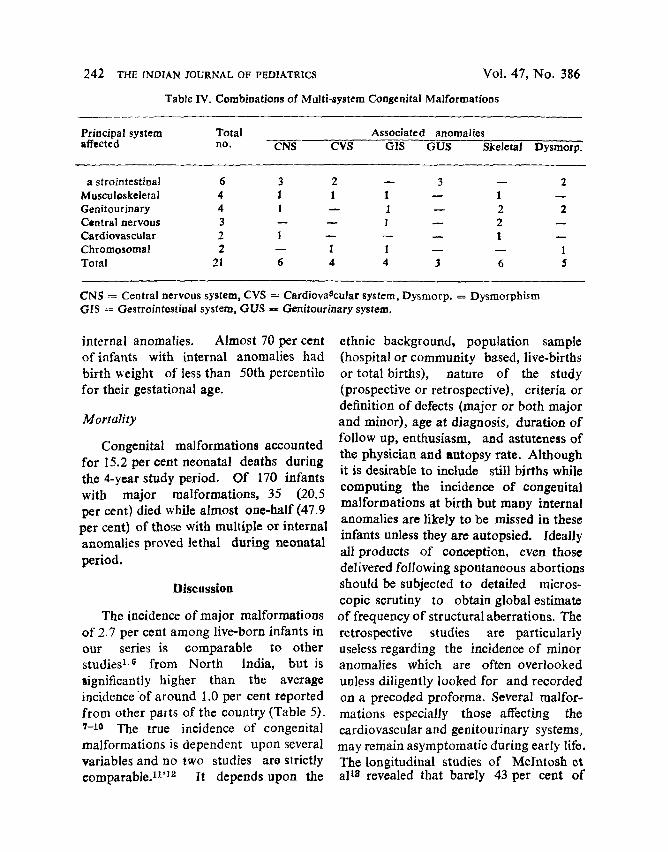
Among life threatening internal mal- formations, central nervous system defects (12.9 per cent) topped the list. The combined live and still birth data during the years 1976-78 revealed that the true incidence of neural tube defects was 7 per 1000 total births (Table 1I). The incidence of individual major anomalies is detailed in Table III. Twenty-one (8.7 per cent) infants had congenital anomalies affecting more than one system of the baby (Table IV). Alimentary,
Vol. 47, No. 386
Table I. System-wise Distribution of Congenital Malformations
System No. % of Rate per total real- 100o live formations births
M usculoskeletal 75 31.1 I 1.9 Central nervous 31 12.9 4.9 Gastrointestinal* .25 10.4 4.0 Cardiovascular 25 10.4 4.0 Genitourinary 22 9. I 3.5 Respiratory** 7 2.9 1. I Multi-system defects 21 8.7 3.3
Chromosomal defects 9 3.7 1.4
Miscellaneous 26 10.8 4.1
*Includes infants with cleft lip and palate **Infants with tracheo-esophageal fistula have been counted among gastro-intestinal anomalies
Table II. Incidence of Neural Tube Defects among 4,693 Total Births (19"/6-78)
Type of anomaly Number Rate per 1~00 total Oirths
Anencephaly 19 4.0 Spina bifida 14 3.0 Tota! N T D 33 7.0
genitourinary and musculoskeletal defects most commonly coexisted in infants with multiple congenital malformations.
Birth weight and gestational age
Of 170 infants with malformations, 28 (16.5 per cent) were preterm as compared to 8.5 per cent overal incidence of prem- aturity (gestation less than 37 weeks) at our hospital, The incidence of major malformations among preterm infants was 6.3 per cent. About one-fourth
M. SINGH AND N.K. SHARMA : CONGENITAL MALFORMATIONS 241
Table III. Frequency of Various Congenital Genitourinary system Malformations Hydrocele
Hypospadias Ambiguous genitalia
Type of anomaly Number Rate oer I000 Renal agenesis live-births
Hypoplastic kidney Polycystic kidney
Musculo~keletal system Obstructive uropathy
Talipes equinovarus/ Respiratory system valgus 38 6.0 Diaphragmatic hernia
Polydactyly 12 1.9 Eventration of diaphragm Syndactyly 4 0.6 Lung cyst Aphalangia 3 0.5 Asph:,xiating thoracic Limb defects 3 0.5 dystrophy Congenital dislocation La ryngomalacia
of hips 7 1.1 Arthrogryposis 3 0.5 Chromosomal disorders Exostosis 1 0.I Down syndrome Multiple skeletal defects 4 0.6 Trisomy 13 (D)
syndrome Central nervous system Trisomy E syndrome
Spina bifida manifesta 13 2.0 M iscelluneous disorders E~;cephalocele 2 0.3 Dysmorphism* Anencephaly 3 0.5 Amniotie constriction Hydrocephalus 8 1.3
bands Microcephaly 3 0.5 Neuroectodermal Anophthalmia 1 0.1
dysplasia Cataract 1 0.1 Pierre-Robin anomalad
Gastrointestbtal system Becktvith syndrome Smmese twins
Cleft lip -q-cleft palate 9 1.4 Cleft palate 2 0.3 Esophageal atresia Dysmorphism includes significant alterations in
with TOF 5 o.8 size, shape, aligr rrent and s)mmetry of various Small gut atresia 2 0.3 con.poner ts oJ fact. Ano-reetal annmalies 5 0.8 Hirschsprung disease i 0.1 (23.5 per cent) o f infants with ma l fo rma- Exomphalcs 1 0.T t ions were small-for-dates .
Cardiovascular system Seventy- three infants with mul t ip le
Left-to-right shunt 10 !.6 and /o r life threa ten ing internal rna l forma-
VSD with PS 4 0.6 t ions were p lo l t ed on the A I I M S Ilypoplastic left in t rauter ine g rowth chart . Serious
heart syndrome 2 0.3 ma l fo rma t ions were more c o m m o n Transposition of great a m o n g pre te rm (28.8 per cent) and
arteries 2. 0.3 smal l - for-dates (30.1 per cent) babies. Tricuspid atresia 1 0.1 Coarctation of aorta 1 0.1 Out o f total o f 28 pre te rm babies with Congenital heart block 1 0.1 congeni ta l ma l fo rma t ions in our series, U.~.identified 4 0.6 21 (75 per cent) had life threa tening
8 1.3 4 0.6 4 0.6 3 0.5 l 0.1 1 0 . l 1 0.1
I 0.1 2 03
7 1.1
I 0 . I I O . l
18 2.9
2 0.3
2 03 2 03 1 0.1 1 0 .1
2 03 1 0.I I 0 . I
242 THE tNOZAN JOURNAL OF PEDIATRICS Vol. 47, No. 386
Table IV. Combinations of Multi-system C o n g e n i t a l M a l f o r m a t i o n s
Principal system Total Associated anomalies affected no. CNS CVS GIS GUS Skeletal Dysmorp.
a s t r o i n t e s t i n a ! 6 3 2 ~ 3 - - 2
Musculoskeletal 4 1 1 1 - - 1 - - Genitourinary 4 1 - - 1 - - 2 2 Central n e r v o u s 3 - - - - 1 - - 2 m
Cardiovascular 2 1 - - -- - - 1 - - Chromosomal 2 - - I 1 - - - - 1
Total 21 6 4 4 :3 6 5
CN$ -= Central nervous system, CVS = CardiovaScular system, Dysmorp. = Dysmorphism GIS = G e s t r o i n t e s t i n a l system, GU$ -= Genitourinary system.
internal anomalies. Almost 70 per cent o f infants with internal anomalies had birth v, eight of less than 50th percentile for their gestational age.
M o r t a l i t y
Congenital malformations accounted for 15.2 per cent neonatal deaths during the 4-year study period. Of 170 infants with major malformations, 35 (20.5 per cent) died while almost one-half (47.9 per cent) of those with multiple or internal anomalies proved lethal during neonatal period.
D i s c u s s i o n
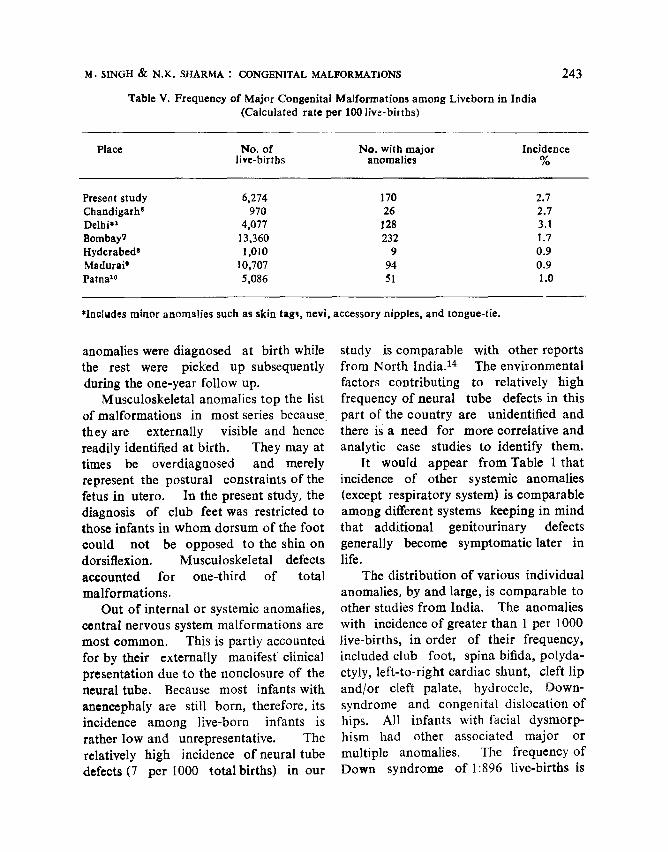
The incidence of major malformations of 2.7 per cent among live-born infants in our series is comparable to other studies 1-6 f rom North India, but is significantly higher than the average incidence o f around 1.0 per cent reported f rom other parts of the country (Table 5). 7-10 The true incidence of congenital malformations is dependent upon several variables and no two studies are strictly eomparab leY 'lz I t depends upon the
ethnic background, populat ion sample (hospital or communi ty based, live-births or total births), nature of the study (prospective or retrospective), criteria or definition of defects (major or both major and minor), age at diagnosis, durat ion o f follow up, enthusiasm, and astuteness of the physician and sutopsy rate. Although it is desirable to include still births while computing the incidence of congenital malformations at birth but many internal anomalies are likely to be missed in these infants unless they are autopsied. Ideally all products o f conception, even those delivered following spontaneous abortions should be subjected to detailed micros- topic scrutiny to obtain global estimate of frequency of structural aberrations. The retrospective studies are particularly useless regarding the incidence of minor anomalies which are often overlooked unless diligently looked for and recorded on a preceded proforma. Several malfor- mations especially those affecting the cardiovascular and genitourinary systems, may remain asymptomat ic during early life. The longitudinal studies of Mclntosh et alla revealed that barely 43 per cent of
M. SlNGH • N.K. SHARMA : CONGENITAL MALFORMATIONS
Table V. Frequency of Major Congenital Malformations among Liveborn in India (Calculated rate per 100 live-births)
243
Place No. of No. with major Incidence live-births anomalies %
Present study 6,274 170 2.7 Chandigarh 6 970 26 2.7 Delhi .1 4,077 128 3. I Bombay7 13,360 232 1.7 I-Iyderabed s 1,010 9 0.9 Madurai' 10,707 94 0.9 Patna x~ 5,086 51 1.0
*Includes minor anomalies such as skin tag% nevi, accessory nipples, and tongue-t ie .
anomalies were diagnosed at birth while the rest were picked up subsequently during the one-year follow up.
Musculoskeletal anomalies top the list of malformations in most series because they are externally visible and hence readily identified at birth. They may at times be overdiagnosed and merely represent the postural constraints of the fetus in utero. In the present study, the diagnosis of club feet was restricted to those infants in whom dorsum of the foot could not be opposed to the shin on dorsiflexion. Musculoskeletal defects accounted for one-third of total malformations.
Out of internal or systemic anomalies, central nervous system malformations are most common. This is partly accounted for by their externally manifest clinical presentation due to the nonclosure of the neural tube. Because most infants with an�9 are still born, therefore, its incidence among live-born infants is rather low and unrepresentative. The relatively high incidence of neural tube defects(7 per 1000 total births) in our
study is comparable with other reports from North India. 14 The environmental factors contributing to relatively high frequency of neural tube defects in this part of the country are unidentified and there is a need for more correlative and analytic case studies to identify them.
It would appear from Table 1 that incidence of other systemic anomalies (except respiratory system) is comparable among different systems keeping in mind that additional genitourinary defects generally become symptomatic later in life.
The distribution of various individual anomalies, by and large, is comparable to other studies f rom India. The anomalies with incidence of greater than 1 per 1000 live-births, in order of their frequency, included club foot, spina bifida, polyda- ctyly, left-to-right cardiac shunt, cleft lip and/or cleft palate, hydrocele, Down- syndrome and congenital dislocation of hips. All infants with facial dysmorp- hism had other associated major or multiple anomalies. The frequency of Down syndrome of 1:896 live-births is
244 THE INDIAN JOURNAL OF PEDIATRICS
comparable to other studies f rom India and abroad. 1'~'t~ Of seven infants
with Down syndrome in the present series two had associated cardiac and one had
imperforate anus with sacral ageneds . It
is desirable to under take karyotyping studies among infants with mu!tiple
defects and dysmorph i sm because
hetrogeneity and multiplici ty of defects is
suggestive of mult igenic or chromosomal
origin of the defect.
The incidence of m~jar matform at ions
among pre term infants was a lmost
twice (5.3 per cent) the overal incidence and abou t two-thi rds of infants with
in ternal m~Iformat ions weighed less t h a n
5')th percentile for their ges ta t ional age. This is comparab le to 3.8-8.8 p e r c e n t
incidence of congeni ta l ma l fo rma t ions among preterm infants reported by other workers, t'7,~0 t h e process of na tu ra l
selection con t inues th roughou t pregnancy and mal fo rmed babies are e l imina ted as
abor t ions , still births and early live bir ths
depend ing upon the site and severity of the defect. It is also unders tandab le that
systemic mal fo rmat ions would interfere with the growth potent ia l of the fetus
thus result ing in in t rau ter ine growth retardat ion. Most mal formed infants
were hypoplast ic rather than
malnour ished .
References
1. Ghosh S, Bali L : Congenital malformations in the newborn. Indian J Child Hlth 12 : 448, 1963
2. Sultana Z, Talib VH. Patil SD, Magar DN, Sharma KD : Congenital malformations- An autopsy study. J Obstet Gynecol (India) 25:329, 1975
3. Saxena HMK, Chandra M, Bhargava SK, Ghosh S: Congenital malformations in
Vol. 47, No. 386
perinatal deaths - an autopsy s~udy. Indian Pediatr 14:625, 1977
4. Puri RK, Verma IC, Madhavan M : Con- genital malformation~ in still births in Pondicherry - an autopsy s:udy. In Medical Gene,'ics in India. Vot 1 Ed. Verma IC, Auroma Enterprises, Pondicherry, 1978. p41
5. Singh M : Early diagnosis of congenital malformations. In Care of the Newborn. Sagar Publications, New Delhi, 2nd edn. 1979, I3 59
6. SaifuUah S Chandra RK, Pathak IC, Dhall G! : Congenital malformafions in newborn- A prospective longitudinal study. Indian Pediatr 4:251, 1967
7. Tibrewala NS. Pal PM : Congenital malfor- mations in the newborn period. Indian Pediatr 11 : 403, 1974
8. Mathur BC, Karan S, VijayaDeviKK: Congenital malformations in Ilae ne~vborn. Indian Pediatr 12:179, 1975
9. Kamala KG. Raghvendran VD. Krishna- murthy KA : Congenital malformations in the newborn in Madurai. In Medical Genetics in India, Vol. 1. Ed. Verma IC, Aurora Enterprises, Pondicherry 1978 p.53.
10. Khanna KK, Prasad LSN : Congenital malformations in the newborn. Indian J Pediatr '4:63, 1967
11. Leek I, Record RG : Sources of variations in the reporting of malformations. Develop Med Child Neurol 5:364, 1963
12. Master-Notani p,4, Kolah PG, Sanghvi LD: Congenital malforn~ations in the newborn in Bombay-part I and II. ActaGenet 18:97 and 193, 1968
13. Mc Into~h R, Merritt KK, Richards MR, Samufes MH, Bellows MT : The incidence of malformations. A study of 5,964 pre- gnancies. Pediatrics 14:505, 1954
14. Verma IC : Neural tube defects in India. In Medical Genetics in India Vel. I, Ed Verma IC. Auroras Enterprises, Pondicherry, 1978. p33
15. Aiyar RR, Agarwal JR : Observations on the new,corn - A study of 10,0f;6 consecutive live-births. Indian Pediatr 6:729, 1969