Embed Size (px)
Citation preview

Spinal Epidural Hematoma during Anticoagulant TherapyBy BERTRAM M. WINER, M.D., SIMON HORENSTEIN, M.D., AND
ALBERT M1. STARR, AI.D.
Spinal epidural hematoma complicated the course of anticoagulant therapy of cerebro-vascular disease in a patient in whom observations of multiple aspects of coagulationhad been obtained. Examination of this case and a review of the literature allowdelineation of a syndrome that should aid in early diagnosis of spinal epidural henmatoma.It is clear that coumarin derivatives induce multiple coagulation defects, which varyquantitatively and qualitatively with time. Contemporary evaluation of the benefitsand risks of long-term anticoagulants is beset by many problems that have not beenfully resolved.
SPINAL epidural hematoma in the absenceof trauma or malformation of spinal
vessels is an exceedingly rare disorder. How-ever, in recent years, at least 3, and possibly4, instances have been reported as complica-tions of anticoagulant therapy.1-4The purposes of this paper are 4-fold: (1)
to report an additional occurrence of spinalepidural hematoma in a patient on long-termanticoagulant therapy for cerebral vasculardisease; (2) to delineate a syndrome thatshould aid in the prompt recognition of spinalepidural hematoma when it is still amenableto therapy; (3) to consider the coagulationdefects induced by a coumarin derivative;and (4) to discuss the problem of evaluationof the benefits and risks of anticoagulants incerebral vascular disease.
CASE REPORTA 70-year-old woman was admitted to the Beth
Israel Hospital in May 1954 because of the suddenonset of nausea, vomiting, and vertigo. A rightlateral medullary tegmental syndrome evolved, asevidenced by crossed dissociated hypalgesia involv-ing the right face and the left side of the body.rhythmic ataxia of the right upper extremity, anda right Horner's syndrome. The vertigo graduallysubsided but the other neurologic abnormalitiespersisted. Additional findings included mild dia-betes mellitus and labile hypertension.
In September 1956, the patient experienced atransient episode of confusion, slurred speech,right facial weakness, and urinary incontinence.
From the Medical Research Department of theYamins Research Laboratory, Beth Israel Hospitaland the Departments of Medicine and Neurology,Harvard Medical School, Boston, Mass.
735
In the following week she developed lethargy,anorexia, defective memory, and blurred vision.Physical examination revealed the neurologic re-siduals of the previous illness but no new abnor-malities. The cerebral spinal fluid was normal.An electroencephalogram was diffusely abnormal.Routine hemogram, urinalysis, blood nonproteinnitrogen, and 1-hour postprandial blood sugar werenormal. Chest roentgenogram revealed a largeleft pulmonary artery; the left ventricle andthoracic aorta were dilated.
Three weeks later nausea, irritability, and visualhallucinosis appeared. Neurologic examination atthis time disclosed a relative left superior quad-rantanopia. The tendon reflexes had become in-creased on the right and a left extensor plantarresponse was present. Over the next week sherecovered from her confusion, ophthalmic palsy,and visual field defect.
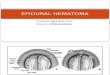
Dicumarol was thereupon administered by mouth(fig. 1). A rapid fall in prothrombic activitywas obtained as measured by a modified Quick1-stage prothrombin method. Beginning with thethird week determinations- of proconvertin activ-ityG and prothromnbin (Owren method)7 were ob-tained at intervals of 1 to 2 weeks for the follow-ing 7 months. In the last 6 months of this periodprothrombic activity by the Quick 1-stage methodranged from, 8 to 15 per cent of normal (20 to30 seconds). Proconvertin was reduced to approx-imiately the same percentage levels and correlatedwell with the prothrombic activity found by theQuick method. However, the prothrombin levelswere for months much less depressed, but gradual-ly fell to the 10 per cent level. In the last 4months of therapy only a Quick prothrombintime was obtained and this was done in a differentlaboratory. The patient received 25 mug. ofDieumarol daily during the last 8 months of ther-
*Kindly performed by Miss Angelina DiFrancesco,technician in the laboratory of Dr. Benjamin Alex-ander, Beth Israel Hospital.
Circulation, Volume XIX, May 1959
by guest on February 10, 2018http://circ.ahajournals.org/
Dow
nloaded from

IENR, HORlENSTEIN, STARR
E 300-,
150- L75
9 5o
QUICK PROTHROMBINA OWREN PROTHROMBINo OWREN PROCONVERTIN
EPIDURALHEMORRHAGE
R.l' ",' 14'
;i
*- 1 1 1* 1 1 1 1 1 1 1*I I I I I I I I I I IOCT NOV DEC JAN FEB MAR APR MAY JUN JUL AUG SEP
FIG. 1. The effect of Dicumarol on theprothrombin itself.
apy. Her clinical state remained stable throughthis interval.On September 28, 1957, she arose to void and
(Jetecate. While returning to bed she experiencedsudden severe pain between her shoulder blades.Six hours later she was unable to move her legsand was incontinent of urine. Thirty hours afterthie onset of the pain she was readmitted to theIhospital. Examination now revealed drowsiness,oderate ataxia of the right upper extremity, and
right Horner's syndrome, but no other neurologicabnormality above the costal margin. The thoracicspine was tender between the sixth and eleventhv'ertebrae, maximally at the eighth. There wasI1a(acid paralysis of both lower extremities. Thetenidon reflexes were absent. The plantar reflexeswseae bilaterally extensor with a crossed extensor(esponse. Position sense was lost in both lower
(exti emiities below the hip. Vib1ration sense was
absent below the iliac crest. Pinprick sensationwas completely, lost below the inguinal ligamentbilaterally including the lower saeral segnent.Fheier was a. sha1ding loss of pinprick below the
Quick prothrombic activity, proconvertin, and
costal maargin on each side. Thermal sensation.and touch were similarly affected.Lumbar puncture between the fourth and fifth
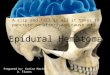
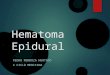
interspaces revealed clear, acellular, yellow-brownfluid with a pressure of 35 mm. of cerebrospinalfluid. Intentionally, only a few drops of cerebralspinal fluid were collected. There was a completedynamic block both to manual compression of thejugular veins and to jugular compression by meansof a blood pressure cuff inflated to 40 mm. Hg. Therewas prompt response upon abdominal compression.()One milliliter of pantopaque was then introducedinto the subarachnoid space. The mnyelog-rajdemonstrated a complete block between thoracicvertebrae 11 and 12 (figs. 2 and 3). At thistime prothrombic activity was 18 per cent of nor-
mal, as measured by the Quick 1-stage prothrombinmethod.
Fifty milligrams of vitamin K1 were admin-istered intravenously. Three hours later, 45 hoursafter the onset of symptoms, a laminectomy was
performed between the seventh and twelfththoracic vertebrae under local anesthesia with no
70-
60-
50-
F-
zWL 40-
0
W 30-
20-
10-
OM-a
736)
by guest on February 10, 2018http://circ.ahajournals.org/
Dow
nloaded from

EPIDURAL HEMATOMA
FIG. 2 Left. Anteroposterior view with the patient in head-down position. Myelographicdemonstration of complete spinal block.
FIG. 3 Right. Lateral view with the patient in head-down position. Myelographic blockand(l widening of the dorsal epidural space at T12 are evident.
unusual hleedini-. Tihe ligamelalieltuini flavumI wasbluish in color. Upon llsnOn a blood clot extend-ing from the sixth to eleventh thoracic spineswas found in the dorsal epidural space. It wasnot adherent to the dura. The original site ofbleeding was not identified. The spinal cord pul-satted upon remioval of the lieiiiaitoiiaa. The duramater was not opened.
Postoperatively there was no recovery of theneurologic defects. Cerebral spinal fluid dynamicswere norasal 1 week after the operation. Brownishpigmentation was still evident in the spinal fluid.In the ensuing 6 months, there was return ofpain sensation in the right lower extremity, butno other improvement in function. The paraplegiahas persisted.
DISCUSSION
The evolution of spinal epidural hematomiaas observed in our patient and in those re-viewed -4, 8-12 presents a pattern that can berecognized with ease. Acute back pain, rap-idly progressive spinal cord and nerve rootdeficit, usually with complete spinal block,accompanied by a brownish pigment in acel-lular cerebrospinal fluid are characteristic.Critical determinants are the location of thebleeding point, the volume of the vertebralcanal relative to that of the spinal cord inthe affected area, the proximity of interver-tebral foranina, the presence of coagulatioll
defects, and the final volume of the hema-tonma. These factors determine the degree ofemnbarrassmnelt of spinal cord circulation aswell as the amount of pressure necrosis. Thelong vertical extent of the lesion, particularlyif located in the luimbar or cervical enlarge-milent of spinal cord, may in addition producesevere atonic flaccidity segmentally and anyelographic block several segments belowthe upper edge of function disturbance. Illour case the mycelographic block was betweenT11 and T12 and the upper border of hypal-gesia w'as at Ts. The brown pigment observedin the cerebrospinal fluid in subdural, epi-dural, and intracerebral hematoma has beenidentified as niethemoglobin. In subarachnoidbleeding the golden-yellow pigment in theeerebrospinal fluid is bilirubin.13
In a review of 10 cases' of acute nontrau-iuatic spinal epidural hematoma straining ef-fort was found to be a common precipitatingevent. Back pain was the first symptom in6 of the patients. The interval from the onsetof the first symptoms to the development ofcomllplete paraplegia varied from 20 minutesto 10 days; however, 50 per cent of the pa-tients were completely paralyzed below thelevel of their lesion within 3 hours of the onset
737
by guest on February 10, 2018http://circ.ahajournals.org/
Dow
nloaded from

SWEINERY, IORENSTEIN, STARR
of comp)laillts. rThe shor test tine interval f oiii
1he developnmenit of p)talalegria to surgical iii-lervention was 4 (days. Three of thme 10 easc.were fatal b)(for e sur gical jutl erveuitioni. T
location of the heliiatoiina ini 2 of these cases
w-as in the upper cervical region. Recoveryafter surgery has varied from complete to
none. Epidural heinatomia in some cases doesnot cause complete spinal block and may not
pursue a rapid course; in 1 patient,̀ who hadback pain for mouths after an injury, thesyndromie of a r uiptunred intervertebral diskwas simulated.'4
Sponitanieous spinal epidural hematoma is a
rare disease. Of the 27 cases found in the
literature, 1 l)atielit had leukenmia, 1 henio-
philia, and including, our ease, 4 and possibly5 had coumiarin-induced coagurlation defects.Thus, approximately one fourth of patientswith this disease have had (coa(rgulationi dle-fects.
In the case presented, recurrent and pro-
gressive vertebral artery disease was the in-dication for anticoagulant therapy. Therew-ere no clhanlgres in dose (luring the last 8months of therapy. The Quick l)rothrombintime was steadily in the "therapeutic"' range
except for 1 determination. In this settinogaln epidlural heoliorrhage develop)ed in the ab-
se--ee of obvious traumia or localized disease.The only aevident aumteee(lent event was a pos-
sible Valsalva maneuver aeeompanying defe-cation. It is conceivable that as a result ofin(reased venious pressure during this effort,
one of the small valveless venules ini the epi-duiral space run)tnred and that in time pres-
e11(ce of her indmllced clotting defects Illelvlcedintr was not arrested.
Iii the last few years anticoagulant therapy
has been used on a loiou-term basis in the pro-
phylaxis of recurrent myocardial infare-tion15-1 and the syndromes of insufficiency ofthe internal carotid, basilar or vertebral ar-
teries..' '° In these states the -value of long-term anticoagulant therapy has been difficult
to establish. The disease processes demon-strate marked, spontaneous variability. New
clot formation, propagation. aimd dissemnina-tion p)lay a variable role iii the prodnetiomi of
symptoms. Brief hypot ension and transientlyreduced cardiac outpnit have beenl ieeogn ize(1als co'oiln riggesol' iselimnic lnl}tOmnswith and Nvitloiit ntewly adde(ld ascila pa-
thology.'-" '2 (liii(cal evaItiaoll of Illee eXtlltof vascular disease and chliiiical determinatiollof progression are difficult. Unconscious biasand nonspeeifie effects have not been easilyeliminated in studies of morbidity.23 Double-blind technies, which might indeed be helpful,are impraetieal.The hazards of counmiarii-iniduced coagula-
tion defects include b)lee liug imlto the skinamid subCUtaneous tissue, mucous membranes,kidney, gastroinitestinial and respiratorytracts, eye, pericardiimm, brain, and the cov-
crincrs of the nervous system. In patientstreated for weeks the incidence of majorbleedimng has been reported grenerally as 1 percent, the incidence of any bleeding as 9 percent.s4 The incidence of hlemorrhage in pa-tients maintained on anticoagulants formouthss to years is not as well established. Inonie series of more thtan 100 patieilts treatedfor 3 years the inci(lellce was 42.1 per cent.17In other large series tlme incidence of hemor-rliage has varied from 3 to 19 per eent.1'5 1`
The possibility clearly- exists that an increasedincidence of bleedi iog after lobu(g-term admin-istration may be due itot only to the quanti-tative factor of the increased time of reducedQuick prothromibie activity but to the quali-tative faclor of the development of newly(leveloping defects in coagulation after iimaniyweeks of administration.25 26
The degree of lhvpoprotlhroiiibinemia neces-
sarv for clinically significant and safe imiter-ference with coagulation has beei difficult to
define. In clinical practice the "therapeutic"level has been accepted as that represented bya Quick 1-stage prothrombin time of approxi-matelv 2 to 3 times normal in seconds, roughly-equivalent to 10 to 30 per cent of prothromibicactivity. The Quick 1-stage prothromibiimmethod reflects multiple factors influencingllthe rate of elaboration of thrombin and fi-
brin.27 Comnarin derivatives have beenshowni to induce multiple coagulatioln de-
feets.2-' 26, 28 Proconvertin, a factor stimnu-
-i 3s
by guest on February 10, 2018http://circ.ahajournals.org/
Dow
nloaded from

EPIDURAL HEMATOMA
latincg the conversion of prothrombin tothrombin, falls rapidly, as was observed illthis case. The induced decrease of procon-vertin is almost invariably greater ill degreeand earlier in time than that of prothrombinitself. A large fall in prothrombin may notbe obtained for weeks. Deficiencies in plasmathromboplastin component (PTC) and Stuartfactor are also induced. There is some evi-dence that there may be little antithromboticeffect from isolated proconvertin deficiencyunless the deficiency is extreme, that the anti-thrombotic effect of Dicumarol may correlatewith prothrombin deficiency, and that lowlevels of prothrombin and of PTC may favorhemorrhage.26 A clear-cut distinction hasbeen demonstrated between the coagulationdefect and the antithrombotic effect of Di-cumarol.29 Further studies of factors influ-encing antithrombotic and hemorrhagie effectsof anticoagulants are required. It is clearthat the commonly used Quick prothrombintime yields information of a general nature,which has been helpful but may not be ade-quate. At "therapeutic" levels, a defect illcoagulation is desired, which can interferewith gross intravascular thrombus formationand propagation and which nonetheless willnot produce excessive bleeding from normaltrauma.The qualitative risks of anticoagulant ther-
apy are clear. The occurrence of major bleed-ing appears unpredictable in an individual.Evaluation of the benefits and risks of long-term anticoagulanits requires further studiesonl both sides of the question.
SUMM1.31ARY
The occurrence of spinal epidural hema-toma ill a patient onl long-term anticoagulanttherapy of cerebral v7ascuilar disease has beenreported.
Tlle saliel fekltl'es of spinal epidutal hie-inatomia a ae beeln dese ribed.
Coiiiiuariii-i iideledt (lef eels ill coagulationhave been discussed.
Problems in the evaluation of long-term all-ticoaguilanit theralpy have been raised.
SUMMARIO IN INTERLINGUAEs reportate le occurrentia de hematoma
spino-epidural in un patiente sub tractamnentoanticoagulatori a longe vista pro morbo cere-bro-vascular.Es deseribite le saliente characteristicas de
hematoma spino-epidural.Es diseutite defectos coagulatori inducite
per coumarina.Es sublevate problemas in le evalutation de
therapia anticoagulatori a longe vista.
REFERENCES
1. ARIXIG, C. D.: Neurological clinical pathologi-cal conference of Cincinnati General Hos-pital. Dis. Nerv. System 13: 53, 1952.
ARIEFF, A. J., AND PYZIK, S. W.: Paraplegiafollowing or assoeiated with excessiveDicui narol therapy. QuLart. Bull. North-western Univ. AI. School 28: 221, 1954.
3. CLOWARD, R. B., AND YUHL, E. T.: Spontan-eous intraspinal hemnorrhage and paraplegiacomplicating Dicuinarol therapy. Neurology5: 600, 1955.
4. ALDERMAN, D. B.: Extradural spinal cordhemnatoma. Report of a case due toDicumarol and review of the literature. NevEng.land J. Med. 255: 839, 1956.
5. QUICK, A. J.: Clinical application of hippuricacid and prothrombin tests. Am. J. Clin.Path. 10: 222, 1940.
6. ALEXANDER, B.: Determination of SPCA. InThe Coagulation of Blood. Methods ofStudy. Edited by L. M. Tocantins. NewYork, Grune & Stratton, 1955, p. 141.
. OWrREN, P. A.: New Clotting Factors. ItTransactions of the Fifth Conference onBlood Clotting. and Allied Problems. Editedby J. E. Flynn. New York, Josiah Macy,Jr. Foundation, 1952, p. 98.
S. KAPLAN, L. I., AND DENKER, P. G.: Acutenon-traumiatic spinal epidural hemorrhage.Am. J. Surg.. 78: 356, 1949.
9. CARREA, R. AI. E., GIRADO, Al., AND EURNE-KIAN, A.: Chronic epidural and subduralspinal heiniatoimna, 3 cases. Analysis ofliterature. Medicina, Buenos Aires 14:379, 19.54.
10. ArMYs, E. W, VoGEL, P. J. AXN) RANEY, R.B.: Spinal (O01ild coimipre)ssiomi due to spon-tnieous el)illmlal heiohe ; 3 cases. Bull.Los Angreles Neurol. Soc. 20: 1, 1955.
11. SADKA, Mi.: Epidural spinal hemnorrhage, witha report on two cases. M. J. Australia 2:669, 1953.
739
by guest on February 10, 2018http://circ.ahajournals.org/
Dow
nloaded from

WINER, HORENSTEIN, STARR
12. SCHULTZ, E. C., JOHNSON, A. C., BROWN, C.A., AND MOSBERG, W. H., JR.: Paraplegiacaused by spontaneous spinal epidural hem-orrhage. J. Neurosurg. 10: 608, 1953.
13. BARROWS, L. J., HUNTER, F. T., AND BANKER,B. Q.: Nature and clinical significance ofpigments in cerebrospinal fluid. Brain 78:59, 1955.
14. SVIEN, H. J., ADSON, A. W., AND DODGE, H.W., JR.: Lumbar extradural hematoma:Report of case simulating protruded discsyndrome. J. Neurosurg. 7: 587, 1950.
15. TULLOCH, J., AND WRIGHT, I. S.: Long termanticoagulant therapy. Further experiences.Circulation 9: 823, 1954.
16. SUZMAN, M. N., RUSKIN, H. D., AND GOLD-BERG, B.: An evaluation of the effect ofcontinuous long term anticoagulant therapyon the prognosis of myocardial infarction.A report of 82 cases. Circulation 12: 338,1955.
17. KEYES, T. W., DRAKE, E. H., AND SMITH, F.J.: Survival rates after acute miyocardialinfarction with long term anticoagulanttherapy. Circulation 14: 254, 1956.
18. MANCHESTER, B.: The value of continuous(1-10 years) long-term anticoagulant ther-apy. Ann. Int. Med. 47: 1202, 1957.
19. MILLIKAN, C. H., SIEKERT, R. G., AND SHICK,R. N.: Studies in cerebrovascular disease.III. Use of anticoagulant drugs in treatmentof insufficiency or thrombosis within basilararterial system. Proc. Staff Meet., MayoClin. 30: 116, 1955.
20. -, -, AND -: Studies in cerebrovasculardisease. V. Use of anticoagulant drugs intreatment of intermittent insufficiency of in-
ternal carotid arterial system. Proc. StaffMeet., Mayo Clin. 30: 578, 1955.
21. DENNY-BROWN, D.: Treatment of recurrentcerebrovascular symptoms and question of"vasospasm." M. Clin. North America 35:1457, 1951.
22. CORDAY, E., AND ROTHENBERG, S. F.: Theclinical aspects of cerebral vascular insuffi-ciency. Ann. Int. Med. 47: 626, 1957.
23. FOLEY, J. M., AND HORENSTEIN, S.: Cerebralvascular disease. Disease a Month, March1958.
24. WRIGHT, I. S., MARPLE, C. D., AND BECK, D.F.: Myoeardial Infaretion. Its ClinicalManifestations and Treatment with Anti-coagulants. New York, Grune & Stratton,1954.
25. HUNTER, R. B., AND WALKER, W.: The controlof anticoagulant therapy in myocardial in-farction. Brit. M. J. 2: 197, 1954.
26. SISE, H. S., LAVELLE, S. M., ADAMIS, D., ANDBECKER, R.: Relation of hemorrhage andthrombosis to prothrombin during treatmentwith coumarin-type anticoagulants. NewEngland J. Med. 259: 266, 1958.
27. ALEXANDER, B.: Coagulation, hemorrhage andthrombosis. New England J. Med. 252:432, 484, 526, 1955.
28. -, DEVRIES, A., AND GOLDSTEIN, R.: Factorin serum which accelerates conversion ofprothrombin to thrombin. II. Its evolutionwith special reference to influence of condi-tions which affect blood coagulation. Blood4: 739, 1949.
29. WESSLER, S., BALLON, J. D., AND KATZ, J. H.:A distinction between the anticoagulant andantithrombotic effects of Dicumarol. NewEngland J. Med. 256: 1223, 1957.
9.
740
by guest on February 10, 2018http://circ.ahajournals.org/
Dow
nloaded from

BERTRAM M. WINER, SIMON HORENSTEIN and ALBERT M. STARRSpinal Epidural Hematoma during Anticoagulant Therapy
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1959 American Heart Association, Inc. All rights reserved.
75231is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TXCirculation
doi: 10.1161/01.CIR.19.5.7351959;19:735-740Circulation.
http://circ.ahajournals.org/content/19/5/735located on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer
of the Web page under Services. Further information about this process is available in thewhich permission is being requested is located, click Request Permissions in the middle columnClearance Center, not the Editorial Office. Once the online version of the published article for
can be obtained via RightsLink, a service of the CopyrightCirculationoriginally published in Requests for permissions to reproduce figures, tables, or portions of articlesPermissions:
by guest on February 10, 2018http://circ.ahajournals.org/
Dow
nloaded from