Embed Size (px)
Citation preview
American Journal of Medical Genetics 49:270-273 (1994)
Spondyloepiphyseal Dysplasia With Nephrotic Syndrome (Schimke Immunoosseous Dysplasia)
Alena Santava, Jieina Zapletalova, Kamila Michalkova, Stanislava Hanakova, FrantiSek Kopi.iva, Jifi Santavy, Jaroslav DulSek, and DuSana Kleinova Department of Medical Genetics (A.S., J.S.) , Pediatric Clinic (J.Z., S.H., F.K.), Radiologic Clinic (K.M.), and Department of Pathology, University Olomouc (J.D., D.K.), Czech Republic
The fist symptoms of immunoosseous dys- plasia were growth retardation and myopia. Nephrotic syndrome was diagnosed at the age of 8 years. Skeletal roentgenograms showed spondyloepiphyseal dysplasia. In the renal biopsy there was nodular accumulations of PAS-positive hyaline material at the base of the granular stalks. There was lymphopenia with decreased CD4 and CD8 subpopulations. The condition of the patient gradually wors- ened until she died unexpectedly at 10 years with clinical symptoms of encephalitis. Au- topsy documented cytomegaloviral pneu- monia and advanced mesangioproliferative glomerulonephritis. In the spleen there was PAS-positive hyaline material massively infil- trating the walls of the central arterioles of the splenic follicles. There was marked depletion of lymphocytes in the spleen and in lymph- nodes. The differential diagnosis of immu- noosseous dysplasia in the framework of spondyloepiphyseal dysplasia is discussed. 0 1994 Wiley-Liss, Inc.
KEY WORDS: immunoosseous dysplasia, Schimke syndrome
INTRODUCTION Schimke et al. U9741 described an SED syndrome
with defective cellular immunity and glomerulonephri- tis with immune complexes and named it immu- noosseous dysplasia. We report on a girl with SED, ne- phrotic syndrome, and immune deficiency presenting at the age of 8 years.
Received for publication November 2, 1992; revision received March 17, 1993.
Address reprint requests to A. Santava, M.D., Department of Medical Genetics, University Olomouc, I.P. Pavlova 6, 775 00 Olomouc, Czech Republic.
0 1994 Wiley-Liss, Inc.
CLINICAL REPORT A 10-year-old girl had been followed from the age of 5
years for growth retardation. Both parents and her elder sister have normal stature. The proposita was born spontaneously after an uneventful pregnancy, in the 38th week, head presentation: birth weight was 1500 g and length was 49 cm. No resuscitation was needed.
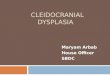
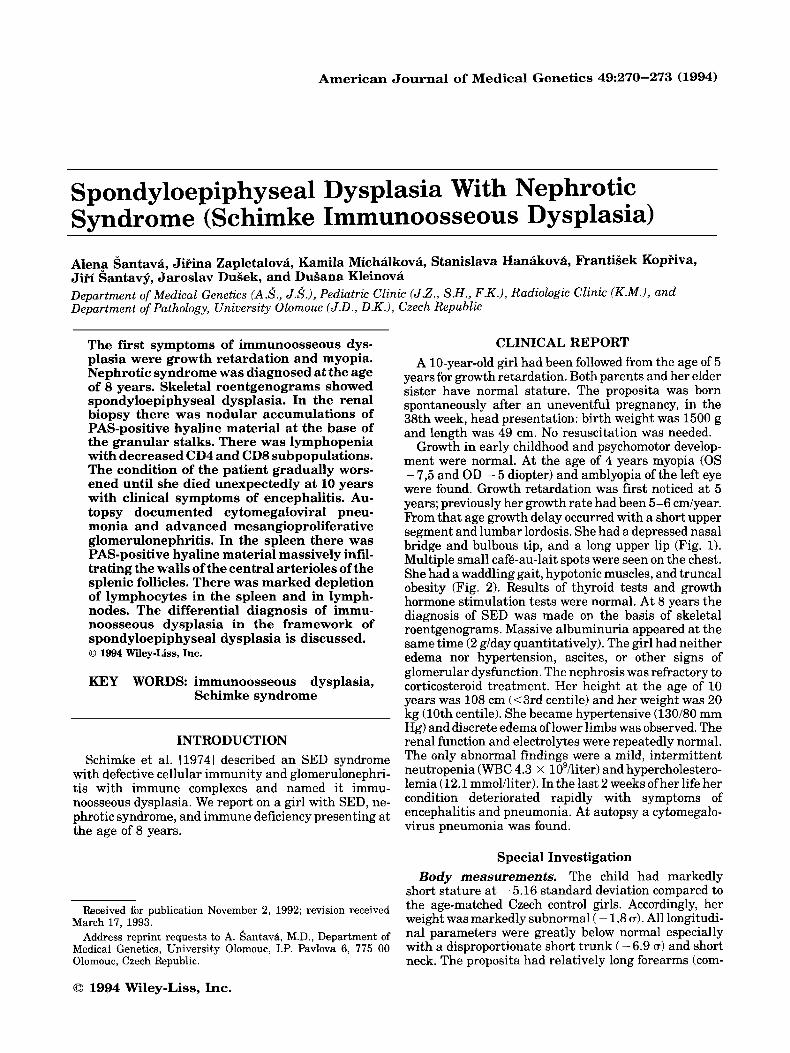
Growth in early childhood and psychomotor develop- ment were normal. At the age of 4 years myopia (0s - 7,5 and OD - 5 diopter) and amblyopia of the left eye were found. Growth retardation was first noticed at 5 years; previously her growth rate had been 5-6 cdyear. From that age growth delay occurred with a short upper segment and lumbar lordosis. She had a depressed nasal bridge and bulbous tip, and a long upper lip (Fig. 1). Multiple small caf6-au-lait spots were seen on the chest. She had a waddling gait, hypotonic muscles, and truncal obesity (Fig. 2). Results of thyroid tests and growth hormone stimulation tests were normal. At 8 years the diagnosis of SED was made on the basis of skeletal roentgenograms. Massive albuminuria appeared at the same time (2 g/day quantitatively). The girl had neither edema nor hypertension, ascites, or other signs of glomerular dysfunction. The nephrosis was refractory to corticosteroid treatment. Her height at the age of 10 years was 108 cm (<3rd centile) and her weight was 20 kg (10th centile). She became hypertensive (130/80 mm Hg) and discrete edema of lower limbs was observed. The renal function and electrolytes were repeatedly normal. The only abnormal findings were a mild, intermittent neutropenia (WBC 4.3 x 10’iliter) and hypercholestero- lemia (12.1 mmoliliter). In the last 2 weeks ofher life her condition deteriorated rapidly with symptoms of encephalitis and pneumonia. At autopsy a cytomegalo- virus pneumonia was found.
Special Investigation The child had markedly
short stature a t - 5.16 standard deviation compared to the age-matched Czech control girls. Accordingly, her weight was markedly subnormal ( - 1,s a). All longitudi- nal parameters were greatly below normal especially with a disproportionate short trunk ( - 6.9 a) and short neck. The proposita had relatively long forearms (com-
Body measurements.
Schimke Immunoosseous Dysplasia 271
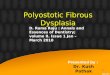
Fig. 3. Pelvic skeleton at 10years: dysplasia ofacetabula, the heads deformed, flattened in varus position, shortness and widening of ossis ilium.
Fig. 1. Face of proposita.
Fig. 2. Proposita at 10 years.
mensurate with the control population). Shoulder width, ankle width (>3 standard deviation), and the occipital-frontal head circumference (<0.2 a) were all below the control values.
Roentgenograms. Pelvic skeleton (at the age of 10 years): short and broad iliac bones, advanced dysplastic alterations of acetabula (flat acetabula with uneven con- tours), flattened heads (Fig. 3).
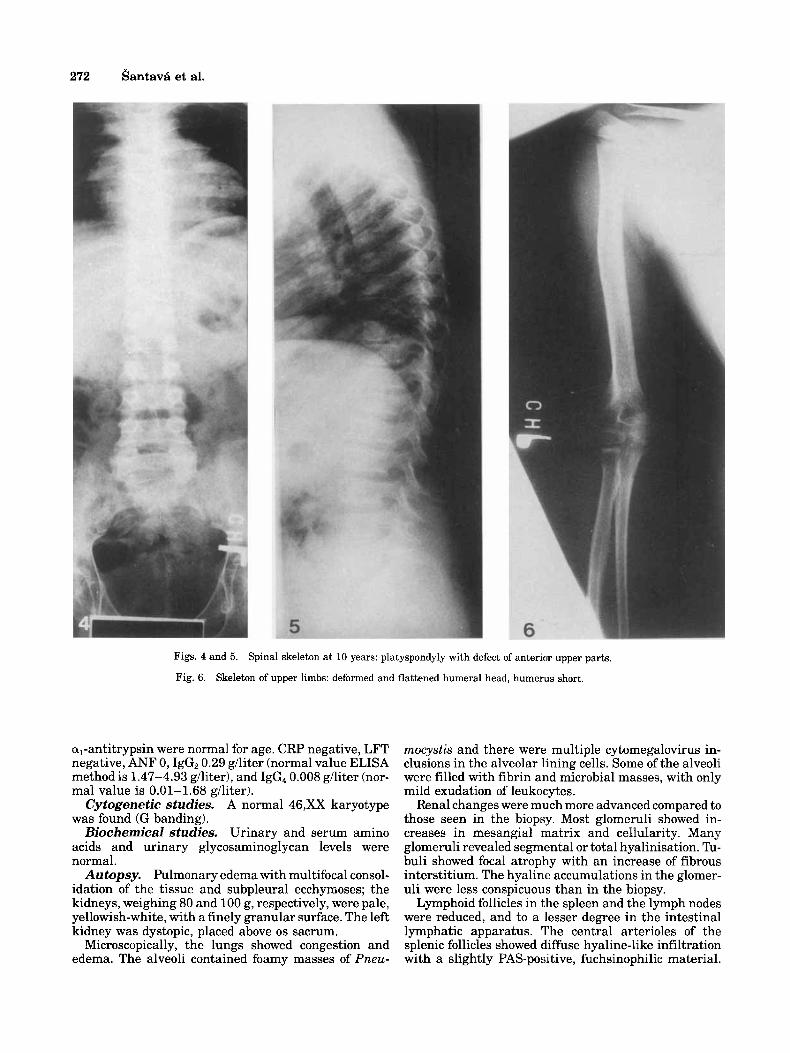
Spine (at the age of 10 years): axial position of ver- tebrae, vertebral bodies flattened, pearshaped, with de- fects on the anterior upper parts and concave lateral contours (Figs. 4, 5).
Upper limbs: humeri with deformed and flattened heads (Fig. 6).
All these changes were typical SED. Renal Studies. Intravenous pyelography. The
right kidney was in normal position. The left kidney was positioned over the sacrum, with a delicate and atypi- cally formed collecting system.
At 7 years renal biopsy disclosed only a minimal to mild increase of the mesangium in some of the glomeruli. An unusual finding was focal globular accumulation of an eosinophilic hyaline material in Bowman’s capsule close to the entrance of the glomeru- lar vascular stalk or in the entering vessels themselves. The tubules and the renal interstitium were otherwise unremarkable.
As studied 1 year after discontinuation of corticosteroid treatment, a marked decrease ofthe total number of lymphocytes (1.38 x lo9/ liter) was found. The CD4 lymphocyte subpopulation was only 12% (0.17 x 10’iliter) and the CD8 subpopula- tion decreased to 22% (0.30 x lOgiliter).
Phagocytic activity studied with 2-hydroxyethyl- methacrylate particles (HEMA) revealed 29% pha- gocytosing neutrophils and 2% eosinophils, and a test with Candida albicans 51% phagocytosing neutrophils and 2% eosinophils (both within the normal range of our laboratory). The levels of IgG, IgM, IgA, C3, C4, and
Renal biopsy.
Immunological studies.
272 Santava et al.
Figs. 4 and 5. Spinal skeleton at 10 years: platyspondyly with defect of anterior upper parts.
Fig. 6 . Skeleton of upper limbs: deformed and flattened humeral head, humerus short.
al-antitrypsin were normal for age. CRP negative, LFT negative, ANF 0, IgGz 0.29 giliter (normal value ELISA method is 1.47-4.93 g/liter), and IgG, 0.008 g/liter (nor- mal value is 0.01-1.68 giliter).
Cytogenetic studies. A normal 46,XX karyotype was found (G banding).
Biochemical studies. Urinary and serum amino acids and urinary glycosaminoglycan levels were normal.
Autopsy. Pulmonary edema with multifocal consol- idation of the tissue and subpleural ecchymoses; the kidneys, weighing 80 and 100 g, respectively, were pale, yellowish-white, with a finely granular surface. The left kidney was dystopic, placed above 0s sacrum.
Microscopically, the lungs showed congestion and edema. The alveoli contained foamy masses of Pneu-
mocystis and there were multiple cytomegalovirus in- clusions in the alveolar lining cells. Some of the alveoli were filled with fibrin and microbial masses, with only mild exudation of leukocytes.
Renal changes were much more advanced compared to those seen in the biopsy. Most glomeruli showed in- creases in mesangial matrix and cellularity. Many glomeruli revealed segmental or total hyalinisation. Tu- buli showed focal atrophy with an increase of fibrous interstitium. The hyaline accumulations in the glomer- uli were less conspicuous than in the biopsy.
Lymphoid follicles in the spleen and the lymph nodes were reduced, and to a lesser degree in the intestinal lymphatic apparatus. The central arterioles of the splenic follicles showed diffuse hyaline-like infiltration with a slightly PAS-positive, fuchsinophilic material.

Schimke Immunoosseous Dysplasia 273
were ascribed to a possible defect in intrathymic differ- entiation or selection of T cells. Urinary chondroitin 6-sulphate levels were normal. All cases but one broth- er-sister pair were sporadic and autosomal recessive inheritance was suggested. Spranger named this multi- system disorder Schimke immunoosseous dysplasia.
The skeletal, facial, skin, immunological, and renal findings (nephrotic syndrome) warrant a similar diag- nosis in our proposita. Her renal function loss was slowly progressive over 2 years. The defective T cell function or a dysgenesis of T cells might lead to an increased risk of autoimmune processes and, therefore, of the nephrotic syndrome. The generalised cytomegalovirus infection was fatal in our patient with defective cellular immunity.
Since Schimke immunoosseous dysplasia is a severe multisystem disorder, the defects should be found in chondrocytes, lymphocytes, and melanocytes for more precise explanation of this disease.
DISCUSSION The association of SED with nephrotic syndrome was
reported in 3 small-for dates boys by Ehrlich et al. [1988]. The first had disproportionate growth retarda- tion, a characteristic facial appearance, and multiple cafe-au-lait spots on the trunk at the age of 4 years. He had rapidly progressive nephrotic syndrome with seg- mental glomerulosclerosis at biopsy. Kidney transplan- tation was indicated because of renal failure. Recurrent episodes of lymphopenia were documented.
At 3 years the second boy had disproportionate growth retardation, a nephrotic syndrome, and a hypoplastic left kidney with reduced function. Renal failure neces- sitated dialysis at the age of 5 years. The third boy had only a mild growth retardation (3rd centile), mini- mal flatness of vertebrae, and mild pelvic dysplasia. The nephrotic syndrome became apparent at the age of 7 years. Renal biopsy showed focal and segmental glomerulosclerosis.
A similar clinical picture was reported earlier [Schimke et al., 19741 in a 6-year-old girl with SED, progressive glomerulopathy, lymphopenia, and a defective cellular immunity. The abnormal level of urinary chondroitin sulphate promoted classification as a probable new type of mucopolysaccharidosis. In 1991 Spranger et al. de- scribed another 5 patients with SEDs (a broad nasal bridge and a bulbous tip of the nose), multiple cafe-au- lait spots on the trunk, and nephrosis resistant to ste- roid and immunosuppressive therapy and with rapid loss of renal function. Disturbances of T cell function
REFERENCES Ehrlich JHH, Offner G, Schirg E, Helmchen U, Brodehl J (1988):
Minderwuchssyndrom mit Skelettdysplasien and fokal segmental sklerosierender Glomerulonephritis. Monatsschr Kinderheilk 1366.
Schimke RN, Horton WA, King CR, Martin NL (1974): Chondroitin-6- sulfate mucopolysaccharidosis in conjunction with lymphopenia, defective cellular immunity and the nephrotic syndrome. BD:OAS X(12):258-256.
Spranger J, Hinkel KG, Stoss H, Thoenes W, Wargowski D, Zepp F (1991): Schirnke immuno-osseous dysplasia: A newly recognized multisystem disease. J Pediatr 119:64-72.