Embed Size (px)
Citation preview

2013
http://informahealthcare.com/adaISSN: 0095-2990 (print), 1097-9891 (electronic)
Am J Drug Alcohol Abuse, 2013; 39(6): 424–432DOI: 10.3109/00952990.2013.847446
ORIGINAL ARTICLE
Striatal-insula circuits in cocaine addiction: implications for impulsivityand relapse risk
Meredith J. McHugh, PhD1, Catherine H. Demers, BA
1, Jacquelyn Braud, PhD2, Richard Briggs, PhD
3,Bryon Adinoff, MD
2,4, and Elliot A. Stein, PhD1
1Neuroimaging Research Branch, National Institute on Drug Abuse-Intramural Research Program, Baltimore, MD, USA, 2Department of Psychiatry,
UT Southwestern Medical Center, Dallas, TX, USA, 3Department of Radiology, UT Southwestern Medical Center, Dallas, TX, USA, and 4VA North
Texas Health Care System, Dallas, TX, USA
Abstract
Background: Dysregulated striatal functioning coupled with executive control deficits arisingfrom abnormal frontal cortical function are considered key mechanisms in the developmentand maintenance of cocaine addiction. The same features are thought to underlie high traitimpulsivity observed in cocaine-addicted populations. Objectives: Employing resting statefunctional connectivity, the current study sought to identify cortico-striatal circuit alterationsin cocaine addiction and examine the degree to which circuit connectivity contributes torelapse risk and impulsivity among cocaine-addicted individuals. Methods: Whole-brain resting-state functional magnetic resonance imaging connectivity was assessed in 45 cocaine-addictedindividuals relative to 22 healthy controls using seed volumes in the left and right caudate,putamen and nucleus accumbens. Cocaine-addicted individuals completed scans in the finalweek of a 2–4 weeks residential treatment episode. Relapse by day 30 post-discharge servedto separate cocaine-addicted individuals into relapse and non-relapse groups. All participantscompleted the Barratt Impulsivity Scale (BIS-11a). Results: Cocaine-addicted individualsexhibited reduced positive connectivity between the bilateral putamen and posterior insulaand right postcentral gyrus. Group differences were primarily driven by reduced connectivityin relapse individuals relative to controls. No relapse versus non-relapse differences emerged.Impulsivity (BIS-11a) was higher in cocaine-addicted participants, an effect that was partiallymediated by reduced putamen-posterior insula connectivity in this group. Conclusion: Cocaineaddiction, relapse risk and impulsivity were associated with reduced connectivity in putamen-posterior insula/postcentral gyrus circuits implicated in temporal discounting and habitualresponding. Findings provide new insight into the neurobiological mechanisms underlyingimpulsivity and relapse in cocaine addiction.
Keywords
Addiction, cocaine, connectivity, impulsivity,insula, neuroimaging, relapse, striatum
History
Received 8 April 2013Revised 11 September 2013Accepted 16 September 2013Published online 4 November 2013
Introduction
Treatment outcomes for cocaine addiction are notoriously
poor, with high rates of early relapse and poor treatment
retention (1–3). Nationwide surveys of outpatient treatment
report cocaine treatment completion rates of just 25% (3), and
mean relapse rates approaching 70% (1). Efforts to charac-
terize relapse risk have primarily focused on clinical measures
such as cocaine use history or measures of neurocognitive
and affective processes known to be altered in cocaine
addiction (4–6). To date, such efforts have not produced a
robust predictor of treatment outcome, and yielded little
insight into the neurobiological mechanisms that drive high
rates of relapse among cocaine-addicted individuals.
In contrast, the past three decades have seen extensive
preclinical interrogation of the neural circuitry underlying the
development of cocaine-seeking behavior and reinstatement
to cocaine-seeking following forced abstinence and extinction
(7). Much of this work has centered on neuroadaptations
within the ventral and dorsal striatum accompanying the
escalation of cocaine self-administration and the progression
to habitual and compulsive cocaine-seeking (8).
Within the striatum a dissociation exists between ventral
(nucleus accumbens), dorsomedial (caudate) and dorsolateral
(putamen) striatal regions that maps onto early development
of cocaine-seeking and later habitual, compulsive use (8,9).
Dopaminergic input from midbrain regions to the ventral
and dorsomedial striatum are critical to the reinforcing effects
Address correspondence to Meredith J. McHugh, NeuroimagingResearch Branch, National Institute on Drug Abuse, NIH, 251 BayviewBoulevard, Baltimore, MD 21224, USA. Tel: +1 443 740 2617. Fax: +1443 740 2816. E-mail: [email protected] A. Stein, Neuroimaging Research Branch, National Institute onDrug Abuse, NIH, 251 Bayview Boulevard, Baltimore, MD 21224, USA.Tel: +1 443 740 2650. Fax: +1 443 740 2734. E-mail: [email protected]
Am
J D
rug
Alc
ohol
Abu
se D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y T
ulan
e U
nive
rsity
on
09/0
1/14
For
pers
onal
use
onl
y.

of cocaine (10) and early acquisition of cocaine-seeking
behavior (8,9,11). Following extended periods of cocaine
self-administration, cocaine-seeking becomes habitual and
ultimately compulsive as evidenced by insensitivity to
outcome devaluation (12) and persistence in the face of
punishment (13). This transition to habitual, compulsive
cocaine-seeking is accompanied by a progressive shift in
control over behavior from ventral/dorsomedial to dorsolat-
eral striatal regions (9,11–17).
Striatal mechanisms underlying goal-directed and compul-
sive aspects of cocaine-seeking are further mediated by
connections between the striatum and prefrontal cortex
(18,19). Prefrontal-striatal pathways have been implicated
in both driving and inhibiting cocaine-seeking behavior
(18,20,21). This is consistent with neuroimaging studies
in cocaine-addicted humans. Here, exposure to cocaine-
associated cues engages ventral and dorsal striatal regions as
well as a distributed network of cortical structures including
the dorsolateral prefrontal cortex (dlPFC), orbitofrontal cortex
(OFC), anterior and posterior cingulate cortex (ACC; PCC)
and insula (22–27). Chronic cocaine abuse in humans has also
been associated with a significant reduction in striatal
dopamine D2/D3 receptor availability and reduced striatal
dopamine release (28–30) coupled with a well-documented
hypofrontality thought to contribute to more general executive
control deficits (19,31–34).
The combination of altered striatal function and hypo-
frontality are considered key neurobiological mechanisms
maintaining compulsive cocaine-use behavior (19,31).
Altered cortico-striatal functioning are also implicated in
high trait impulsivity characteristic of cocaine-addicted
individuals (19,32,35). Impulsivity, in turn, looks to be a
key factor in the transition from goal-directed to habitual,
compulsive cocaine-seeking (36) and relapse (37) and
may present a critical phenotype driving high rates of relapse
in cocaine-addicted populations (19,37,38).
Despite the implication of cortico-striatal circuits in
neurobiological theories of cocaine addiction, surprisingly
few studies have directly interrogated ventral and dorsal
striatal circuitry in cocaine-addicted individuals (23,39,40).
Furthermore, the contribution of cortico-striatal circuitry to
relapse risk and impulsivity in cocaine-addicted populations
is yet to be addressed. In the present study, we employed
resting state functional connectivity analysis to interrogate
these circuits. Resting state functional connectivity reflects
covariation in spontaneous low frequency (0.01 to 0.1 Hz)
fluctuations of the blood-oxygen-level-dependent (BOLD)
functional magnetic resonance imaging (fMRI) signal across
different regions of the brain (41). Patterns of covariation in
this spontaneous signal exhibit a spatial-temporal corres-
pondence to known functional networks (41,42) and are
sensitive to psychiatric disease states such as addiction (43).
Here, striatal circuits including the caudate, putamen and
nucleus accumbens were measured in cocaine-addicted indi-
viduals during the final week of a 2–4 week cocaine addiction
treatment episode. Circuit connectivity strength was also
measured in a sample of healthy controls. It was hypothesized
that differences in cortico-striatal connectivity strength would
emerge as a function of cocaine addiction status. Further,
we expected alterations in cortico-striatal connectivity
strength to be most marked in cocaine-addicted individuals
at greater risk of early relapse following treatment and
contribute to higher trait impulsivity in this population.
Materials and methods
Subjects
Participants were 22 healthy controls and 45 individuals who
met criteria for cocaine dependence on the Structured Clinical
Interview for DSM-IV-TR Axis I disorders (SCID-I),
recruited from three inpatient treatment facilities. Subjects
were excluded if they had any history of major illness, were
left-handed, had an estimated IQ below 70 (per the Wechsler
Test of Adult Reading [WTAR]), or met criteria for any
neurological or active Axis I disorder (other than Substance
Use Disorders) or were on psychotropic medications. Other
drug use among cocaine-addicted subjects was not a condition
for exclusion as long as cocaine dependence was the primary
diagnosis.
All aspects of the research protocol were reviewed and
approved by the Institutional Review Boards of the University
of Texas Southwestern Medical Center at Dallas and the
Veterans Administration North Texas Health Care System.
Subjects provided informed consent prior to study
participation.
Impulsivity
Impulsivity was assessed using the Barrett Impulsivity
11a scale (BIS-11a) (44), a 24 item self-report instrument
adapted from the BIS-11 and comprised of three subscales:
Attentional Impulsiveness, Motor Impulsiveness and
Nonplanning (45). Attentional Impulsiveness reflects an
inability to focus on current tasks, Motor Impulsiveness
assesses the tendency to act quickly without thinking, while
Nonplanning reflects a lack of foresight for the future. Total
Impulsiveness reflects the sum of all three subscales.
Procedure
Cocaine-addicted participants were recruited from patients
admitted to a residential treatment program for cocaine
dependence at the Veteran’s Administration Medical Center,
Homeward Bound, Inc., or Nexus Recovery Center in
Dallas, Texas. Almost all participants used crack cocaine.
All programs utilized a Minnesota Model psychosocial
treatment approach. Cocaine-addicted participants were
hospitalized as soon as possible after their last reported use
of cocaine and remained in a structured, residential unit until
study completion. Abstinence was verified throughout resi-
dential treatment by urine drug screens. BIS-11a was
administered during the first or second week of treatment.
During the final week of treatment cocaine-addicted individ-
uals completed a 6-min resting scan during which they were
instructed to lie as still as possible with their eyes open.
Following discharge, follow-up sessions occurred twice
weekly (once by phone), and included a structured interview
assessing substance use since their previous visit and a urine
drug screen. Relapse was defined as any use of cocaine or
amphetamine since discharge and marked as the day of first
use, or the day of their first missed appointment if participants
DOI: 10.3109/00952990.2013.847446 Striatal-insula circuits in cocaine addiction 425
Am
J D
rug
Alc
ohol
Abu
se D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y T
ulan
e U
nive
rsity
on
09/0
1/14
For
pers
onal
use
onl
y.

missed two consecutive appointments. For analyses reported
here, users were categorized as relapsed and non-relapsed
based on their relapse status at day 30 following discharge
from treatment. Relapse by day 30 is the DSM-IV criteria
for early relapse. Control participants completed an identical
scan session and typically completed the BIS-11a within
1 week of this session.
MRI data acquisition
Functional MRI data were collected on a 3-T Phillips MR
scanner equipped with an eight channel RF coil. Thirty-six
3 mm thick functional slice locations were obtained in the
axial plane parallel to the AC-PC line allowing for whole
brain coverage. Functional BOLD signals were acquired using
a single-shot gradient echo planar imaging (EPI) sequence
with a matrix of 64� 64, echo time (TE) of 25 ms, repetition
time (TR) of 1.7 s, flip angle (FA) of 70�, field of view
(FOV) of 208� 208 mm yielding an in-plane resolution of
3.25� 3.25 mm. For spatial normalization and localization,
corresponding high resolution anatomical T1 images were
acquired using 3D magnetization prepared rapid gradient-
echo (MPRAGE) sequence with a TR/TE 8.2/3.8 ms, FA of
12�and voxel size of 1� 1� 1 mm.
Data processing
Data were preprocessed and analyzed using AFNI (46),
FreeSurfer (http://surfer.nmr.mgh.harvard.edu/) and SPSS
version 20.0 (Armonk, NY). Following image reconstruction,
resting data were submitted to slice-timing correction, motion
correction, and quadratic detrending of time series data. A
low band pass temporal filter was applied to restrict signal
variation to frequencies between 0.01 and 0.1 Hz (41). Images
from resting data were then registered to standard (Talairach)
space with a resampled resolution of 3.25� 3.25� 3 mm3 and
smoothed with an isotropic 6 mm full-width half-maximum
Gaussian kernel. To facilitate group analysis, an unbiased
groupwise non-linear registration method was used to gener-
ate an implicit group reference image (47). Six striatal seeds
were derived using FreeSurfer volumetric segmentation in
original space bilaterally for the nucleus accumbens, caudate
and putamen. Table 1 lists mean volume for each seed region.
No significant group differences were present for seed
volume (all ps40.05). Seed reference time courses, derived
by averaging all voxel time-courses within a given seed, were
regressed against all brain voxels to generate cross correlation
(CC) maps. Time-courses for six motion parameters and
fluctuations in BOLD signals from cerebrospinal fluid and
white matter were modeled as nuisance variables. Finally,
CC distributions were normalized by applying Fisher’s
z-transformation.
Data analysis
Group differences in demographics, drug use history, treat-
ment characteristics and impulsivity were examined with
one-way between-subjects ANOVAs, Chi-squared tests (for
differences in frequencies) and Bonferroni-corrected post-hoc
comparisons. The impact of cocaine-addiction and relapse-
risk on resting state connectivity was assessed for each seed
region using a general linear mixed model with gender and
group entered as fixed effects. For models assessing cocaine-
addiction, group had two levels (controls, cocaine-addicted)
and for those assessing relapse risk, three levels (controls,
relapse, non-relapse). For relapse-risk analyses, post-hoc
contrasts revealing differences between relapse and non-
relapse participants, or between controls and relapse partici-
pants only (i.e. no differences between controls and non-
relapse), were considered to reflect early relapse risk. Effects
were considered significant if they passed an uncorrected
voxel-wise threshold of p¼ 0.005 and corrected clusterwise
threshold of p¼ 0.05.
Where group effects emerged, bivariate correlations
(Bonferroni corrected for multiple comparisons) were con-
ducted between striatal connectivity strength within signifi-
cant clusters (controlling for gender) and BIS-11a Total
Impulsiveness, Nonplanning, Motor Impulsiveness and
Attentional Impulsiveness across the whole group. Where
the conditions for mediation were met the Joint Significance
Test (48,49) was employed to test striatal connectivity
strength as a mediator of the relationship between impulsivity
and cocaine addiction or relapse status. Here evidence for
mediation is based on a significant relationship between the
predictor and mediator (a) and the mediator and outcome
variable (b), controlling for the predictor (Figure S1). Due to
the use of dichotomous outcome variables (cocaine addiction/
relapse status) mediation analyses required an additional
processing step to derive comparable path coefficients (50)
(see Supplementary Materials for details). Significance of the
mediated effect (ab) was assessed with ProdClin (48), which
applies a bootstrap method to generate confidence intervals
for the mediated effect.
Finally, to determine whether striatal connectivity effects
reflected variability in demographic, cocaine-use, or treat-
ment characteristics, bivariate correlations or independent
sample t-tests were conducted assessing striatal connectivity
as a function of: cocaine use and spending in the past 90 d,
lifetime cocaine use, age at first use, days since last use, years
of education, IQ, cigarettes smoked per day, years of cigarette
smoking, alcoholic drinks per week and treatment duration
and treatment centre attended. We set a p50.01 threshold
to reduce the false positive rate associated with such a large
number of exploratory analyses.
Results
Participant characteristics
Of the 45 cocaine-addicted individuals in the study, 24 were
categorized as relapsed during the first 30 d post-treatment
(relapse), while 21 remained abstinent throughout this period
(non-relapse). As illustrated in Table 2, control participants
had a higher IQ, and greater years of education than relapse
Table 1. Mean and standard deviation for seed region volumes.
Seed region Mean (SD) volume (mm3)
Left putamen 5402.10 (620.33)Right putamen 5220.39 (703.49)Left caudate 3496.70 (517.45)Right caudate 3506.67 (541.42)Left nucleus accumbens 527.78 (144.55)Right nucleus accumbens 554.00 (94.93)
426 M. J. McHugh et al. Am J Drug Alcohol Abuse, 2013; 39(6): 424–432
Am
J D
rug
Alc
ohol
Abu
se D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y T
ulan
e U
nive
rsity
on
09/0
1/14
For
pers
onal
use
onl
y.

participants. Non-relapse participants also had greater years
of education than relapse participants. Control participants
were significantly less likely to be cigarette smokers and
reported fewer alcoholic drinks per week relative to both
relapse and non-relapse participants. Relapse participants
reported a greater number of years smoking cigarettes than
non-relapse participants. Both cocaine-addicted groups scored
higher than controls across all BIS-11a scales. No other
significant differences in demographic, personality, drug use
or treatment characteristics emerged.
Putamen connectivity
Cocaine-addiction status
Significant effects of cocaine-addiction status emerged for
both the left and right putamen seeds, with significantly
reduced connectivity between the bilateral putamen and a left
posterior insula cluster and right lateralized cluster focused
on the right putamen, extending into the postcentral gyrus
in cocaine-addicted individuals relative to healthy controls
(Table 3 and Figure S2).
Relapse risk
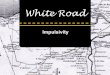
As illustrated in Figure 1(A) and Table 4 an effect of group
(controls, relapse, non-relapse) emerged for connectivity
between the right putamen and a right posterior insula/
postcentral gyrus cluster. Post-hoc contrasts revealed that
this effect was driven by significantly reduced connectivity
within this cluster in relapse versus control participants
(Figure 1C). Differences between control and non-relapse
participants and between relapse and non-relapse participants
illustrated in Figure 1(C) did not reach significance.
Group main effects were also present in connectivity
between the left putamen and a left posterior insula cluster
and right posterior insula/postcentral gyrus cluster (Figure 1B
Table 2. Demographic, drug use, treatment and behavioral characteristics.
Participant characteristic Control (n¼ 22)Non-relapsed atday 30 (n¼ 21)
Relapsed atday 30 (n¼ 24)
Age 42.05(8.40) 43.10(6.84) 43.75(7.53)Years of Education **,a,b 13.91(1.41) 13.29(2.05) 11.83(1.88)IQ*,a 96.86(10.26) 90.71(9.35) 88.61(8.63)Gender (no. males) 14 18 21Cigarette smokers**,a,b(no. smokers) 1 16 19Cigarettes/day – 12.94(2.63) 16.00(8.52)Years smoking cigarettes*,c – 17.88(9.07) 24.32(9.32)Alcohol/week (no. standard drinks)**,a,c 2.06 (2.09) 2.76(2.28) 2.50(2.30)Current opiate use (no. users) 0 1 2Current stimulant use (no. users) 0 0 1Current cannabis use (no. users) 0 3 3Current other drug use (no. users) 0 1 0Age of onset cocaine dependence NA 27.15(7.46) 26.48(9.59)Days cocaine used – last 90 d 0 71.43(21.51) 69.88(24.65)Years cocaine used – lifetime 0 7.72 (3.99) 8.88(6.48)Days since last cocaine use 0 22.81 (4.31) 22.58 (3.62)Amount spent on cocaine – last 90 d 0 $8075.05(6296.51) $5910.67(5484.34)Treatment centre (no. in A,B,C)d NA 3, 16, 2 7, 14, 3Treatment duration NA 24.74(8.08) 26.19(14.04)BIS-11a Nonplanning**,a,c 18.00(2.73) 19.90(2.62) 20.28(1.87)BIS-11a Motor Impulsiveness***,a,c 17.83(3.01) 25.32(5.48) 24.33(3.93)BIS-11a Attentional Impulsiveness***,a,c 12.95(2.92) 16.84(3.45) 16.63(3.54)BIS-11a Total Impulsiveness***,a,c 48.84(6.40) 61.69(9.05) 60.94(6.77)
A¼Veteran’s Administration Medial Center; B¼Homeward Bound Inc.; C¼Nexus Recovery Center. Cocaine-addictedparticipants had been abstinent from all drugs of abuse for a minimum of 17 d at the day of scanning.
*p50.05.**p50.01.***p50.001 for group main effects.aDifference between relapse and non-relapse.bDifference between relapse and controls.cDifference between non-relapse and controls.dTreatment centers based in Dallas, TX.
Table 3. Clusters showing significant resting connectivity differences between cocaine-addicted participants (n¼ 45) and controls (n¼ 22) for seedsplaced in the left and right putamen. For all clusters listed cocaine-addicted participants evidenced reduced connectivity relative to control participants.
Peak coordinates (Talairach)
Seed regionRegions of difference in
connectivity strengthCluster size
(Voxels)Peak difference
F Value L P I
Left putamen Left posterior insula 203 18.27 �31.5 �22.5 20.5Left putamen Right posterior insula/post-central gyrus 202 15.82 37.5 �25.5 14.5Right putamen Left posterior insula 85 12.70 52.5 �13.5 17.5Right putamen Right posterior insula/post-central gyrus 148 17.04 �40.5 �13.5 11.5
DOI: 10.3109/00952990.2013.847446 Striatal-insula circuits in cocaine addiction 427
Am
J D
rug
Alc
ohol
Abu
se D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y T
ulan
e U
nive
rsity
on
09/0
1/14
For
pers
onal
use
onl
y.

and Table 4). Post-hoc control versus relapse contrasts
revealed significant clusters (Figure S3A) which overlapped
the group main effects, reflecting significantly reduced
connectivity in relapse relative to control participants
(Figure 1D). Control versus non-relapse contrasts also
revealed two clusters which overlapped the group main
effects illustrated in Figure 1(B), but clusters were small
and did not survive clusterwise thresholding (Figure S3B).
Together the above findings suggest that the left putamen to
left posterior insula and right-posterior insula/postcentral
gyrus connectivity group main effects illustrated in
Figure 1(B) were primarily driven by differences between
control and relapse participants, but may also partially reflect
reduced connectivity in non-relapse relative to control
participants (Figure 1D). No differences in left putamen
connectivity emerged between non-relapse and relapse
participants.
Caudate and nucleus accumbens connectivity
No group effects emerged when whole-brain resting connect-
ivity was examined for left and right caudate or left and
right nucleus accumbens seeds.
Putamen connectivity and impulsivity
Because connectivity within the putamen-posterior insula
circuits illustrated in Figure 1 were highly correlated
(all rs40.789, p50.001), we averaged connectivity across
these circuits and conducted correlational analyses on aver-
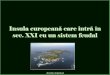
age putamen-posterior insula connectivity. Significant nega-
tive correlations emerged between putamen-posterior insula
connectivity and Motor Impulsiveness, r (65)¼�0.35,
p¼ 0.004 (see Figure 2) and Total Impulsiveness,
r (65)¼�0.34, p¼ 0.006. A negative association between
Nonplanning and putamen-posterior insula connectivity
Figure 1. Significant group main effects for resting connectivity when seeds were located in (A) right putamen (R.PUT), (B) left putamen (L.PUT).Mean resting connectivity strength within significant clusters for controls (n¼ 22), relapse (n¼ 24) and non-relapse (n¼ 21) cocaine-addictedparticipants between (C) right putamen and right posterior insula (L.PI), (D) right putamen and left/right posterior insula (R.PI). Error bars representstandard error of the mean. Uncorrected voxel-wise threshold at p¼ 0.005, corrected clusterwise threshold at p¼ 0.05.
Table 4. Significant main effects of group (control, relapse, non-relapse) for seeds located in the left and right putamen.
Peak coordinates (Talairach)
Seed region Regions of difference in connectivity strengthCluster size
(Voxels)Peak difference
F Value L P I
Left putamen Right posterior insula/post-central gyrus 80 8.0 46.5 �16.5 14.5Left putamen Left posterior insula 79 8.99 �31.5 �22.5 20.5Right putamen Right posterior insula/post-central gyrus 74 9.13 46.5 �13.5 20.5
428 M. J. McHugh et al. Am J Drug Alcohol Abuse, 2013; 39(6): 424–432
Am
J D
rug
Alc
ohol
Abu
se D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y T
ulan
e U
nive
rsity
on
09/0
1/14
For
pers
onal
use
onl
y.

approached our p50.01 statistical threshold, r (65)¼�0.29,
p¼ 0.017.
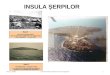
Putamen-posterior insula connectivity was then tested as
a mediator of the enhanced Motor Impulsiveness seen in
cocaine-addicted individuals relative to healthy controls. We
focused on the Motor Impulsiveness subscale because
effects were strongest here. As illustrated in Figure 3,
higher Motor Impulsiveness in cocaine-addicted individuals
was partially mediated by reduced putamen-posterior
insula connectivity in this group (unstandardized coeffi-
cient¼ 0.011, CI95: 0.001–0.024).
Putamen connectivity, demographics and druguse history
Putamen-posterior insula connectivity effects were unrelated
to years of education, years of cigarette smoking, cigarettes
per day, alcoholic drinks per week, days of cocaine use and
amount spent in the last 90 d, lifetime days of cocaine use,
days since last cocaine use, treatment duration or treatment
centre attended (all ps40.01).
Discussion
Based on evidence implicating the striatum and cortico-
striatal circuits in cocaine addiction and relapse, we
hypothesized that resting state functional connectivity
within dorsal and ventral striatal circuits would be altered
in cocaine-addicted individuals relative to healthy controls.
We expected the most marked differences to emerge between
healthy controls and cocaine-addicted individuals at greatest
risk of early relapse, and expected connectivity effects to
contribute to higher trait impulsivity in cocaine-addicted
individuals. Overall, cocaine-addicted individuals displayed
reduced connectivity between the bilateral putamen and
posterior insula, with right insula effects extending into the
postcentral gyrus. However, these effects were primarily
driven by reduced connectivity in those individuals who
relapsed by day 30 relative to controls. This pattern suggests
that reduced positive connectivity between the putamen and
posterior insula/postcentral gyrus may reflect a characteristic
of cocaine-addicted individuals in general that is most
marked in those individuals at greatest risk of early relapse.
No cocaine-addiction or relapse-related differences emerged
when examining connectivity in caudate and nucleus
accumbens circuits. Finally, consistent with previous reports
(51–54), cocaine-addicted individuals reported significantly
higher trait impulsivity than healthy controls, an effect that
was partially mediated by reduced putamen-posterior insula
connectivity in cocaine-addicted individuals.
While neurobiological models of addiction have largely
centered on the striatum (55–57), human neuroimaging and
lesion studies have also highlighted the insula as a key player
in the neurobiology of addiction (58,59). Given its role
in interoceptive awareness and subjective emotional states
(60–62), the insula, in particular the anterior portion, has
been charged with the generation of conscious urges, such as
cocaine craving (58). This accords with lesion and imaging
studies which implicate the anterior insula in subjective drug
craving (63). The current findings suggest that the posterior
insula may also play a role in the neurobiology of addiction;
contributing to impulsive decision-making and relapse in
cocaine-addicted populations.
High trait impulsivity in cocaine-addicted individuals is
thought to, in part, reflect steeper temporal discounting of
rewards (64,65). Temporal discounting tasks involve deci-
sions between an immediate reward and larger reward
delivered after a given delay. As delay to reward delivery
increases, the perceived value of the delayed reward declines
exponentially (66). Cocaine-addicted individuals show a
sharper discounting of perceived reward value as a function
of time to reward delivery (64,65). Critically, enhanced
engagement of the posterior insula and putamen has been
observed as a function of choosing the delayed over the
immediate reward (67,68) as well as performance that relies
upon the prediction of delayed rewards (69).
A putative mechanism of temporal discounting is that
time to reward delivery imposes a cost that discounts the
delayed reward value (70). Wittmann and Paulus (70) propose
that impulsive decision making is tightly coupled to time
perception, such that highly impulsive individuals overesti-
mate time intervals and thus experience greater cost when
delaying gratification (e.g. selecting the delayed over the
immediate reward). Interestingly, both the posterior insula
and the putamen have been implicated in time perception
(71,72). In sum, current findings suggest a potential neuro-
biological candidate for steeper temporal discounting in
cocaine-addicted populations, implicating a disrupted puta-
men-posterior insula circuit which drives impulsive decision-
making by altering the perceived cost of time to reward
delivery.
Figure 2. Negative bivariate correlation between BIS-11a MotorImpulsiveness and average putamen (PUT) – posterior insula (PI)connectivity were conducted across the whole sample (n¼ 66).
Figure 3. Model depicting average putamen-posterior insula connectiv-ity strength as a partial mediator of the degree to which MotorImpulsiveness distinguishes cocaine-addicted participants (n¼ 44) fromhealthy controls (n¼ 22). Path values reflect standardized beta andWald coefficients derived from linear and logistic regression modelsrespectively (the latter where path outcome is cocaine addiction status).*p50.05 **p50.01.
DOI: 10.3109/00952990.2013.847446 Striatal-insula circuits in cocaine addiction 429
Am
J D
rug
Alc
ohol
Abu
se D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y T
ulan
e U
nive
rsity
on
09/0
1/14
For
pers
onal
use
onl
y.

It is noteworthy that putamen connectivity effects
extended into the postcentral gyrus, the somatosensory
portion of the sensorimotor cortex. Putamen-sensorimotor
circuits are implicated as key circuitry underlying relapse to
drug use following abstinence or extinction (18). Putamen-
sensorimotor circuits are also central to the development
and execution of habitual responding generally (73). Recently,
the posterior insula, putamen and postcentral gyrus were
all implicated in a network of brain structures activated during
the execution of an extensively trained choice response
designed to model habitual responding (74). Together these
findings suggest that reduced putamen-posterior insula/
postcentral gyrus connectivity in cocaine-addicted individuals
at risk of early relapse may in part reflect altered habit
circuitry.
While putamen-posterior insula connectivity varied as a
function of both cocaine-addiction and relapse risk in the
current study, variability in this circuitry did not reflect
cocaine-use history, but instead trait impulsivity. Preclinical
studies suggest that enhanced trait impulsivity may both
precede the onset of cocaine-dependence and arise as a result
of chronic cocaine use (36,75). Recently, putamen and
posterior insula structural abnormalities have been reported
in stimulant-addicted individuals (76,77) and their biological
siblings (77). Together with the current findings, this suggests
that altered putamen-posterior insula circuitry may confer
vulnerability to the development of cocaine addiction and
enhance the risk of poor outcomes following treatment.
Several limitations to the current study should be noted.
Firstly, control and cocaine-addicted participants differed
across demographic characteristics. However, analyses were
conducted to rule out the contribution of demographic
characteristics to striatal connectivity group effects.
Secondly, it is possible that resting connectivity effects
observed during a period of cocaine abstinence reflect
withdrawal-related symptoms such as cocaine craving, anhe-
donia or anxiety (43). Unfortunately contemporaneous meas-
ures of craving and other withdrawal symptoms were not
taken on the day of the resting scan reported here. Finally,
resting state functional connectivity measures cannot be used
to determine directionality of circuits, nor do they imply a
direct anatomical path between two regions.
Despite these limitations, the current study provides new
insight into the neural circuitry underlying cocaine addiction
and relapse risk. It is the first study to examine dorsal striatal
circuitry in a cocaine-addicted population and the first to
examine striatal connectivity as a function of relapse risk and
impulsivity. Findings revealed reduced positive connectivity
between the putamen and the bilateral posterior insula and
right postcentral gyrus in cocaine-addicted individuals that
was primarily driven by reduced connectivity among indi-
viduals at greatest risk of early relapse. Reduced putamen-
posterior insula connectivity also partially mediated enhanced
trait impulsivity observed in cocaine-addicted individuals.
Circuits showing reduced connectivity in cocaine-addicted
individuals have been implicated in temporal discounting of
rewards and habitual responding, processes that are con-
sidered key mechanisms in the development and maintenance
of addictive behavior (78,79). Future studies are needed to
further explore the relationship between these mechanisms
and putamen-posterior insula circuits and their role in
addiction and relapse.
Acknowledgements
The authors gratefully acknowledge the assistance of the
Substance Abuse Team at the VA North Texas Health Care
System, Homeward Bound, Inc., and Nexus Recovery Center
for their support in the screening and recruitment of study
subjects.
Declaration of interest
This work is supported by the Intramural Research Program
of the National Institute on Drug Abuse and by NIDA grant
DA023203 (BA, JB, RB). The authors report no conflicts of
interest.
References
1. Dutra L, Stathopoulou G, Basden SL, Leyro TM, Powers MB,Otto MW. A meta-analytic review of psychosocial interventions forsubstance use disorders. Am J Psychiat 2008;165:179–187.
2. Simpson DD, Joe GW, Broome KM. A national 5-year follow-up oftreatment outcomes for cocaine dependence. Arch Gen Psychiat2002;59:538–544.
3. Substance Abuse and Mental Health Services Administration(SAMHSA), Office of Applied Studies. The TEDS Report:Treatment Outcomes among Clients Discharged from OutpatientSubstance Abuse Treatment. Rockville, MD: SAMHSA; 2009.
4. Ahmadi J, Kampman K, Dackis C. Outcome predictors in cocainedependence treatment trials. Am J Addiction 2009;15:434–439.
5. Poling J, Kosten TR, Sofuoglu M. Treatment outcome predictorsfor cocaine dependence. Am J Drug Alcohol Ab 2007;33:191–206.
6. Turner TH, LaRowe S, Horner MD, Herron J, Malcolm R.Measures of cognitive functioning as predictors of treatmentoutcome for cocaine dependence. J Subst Abuse Treat 2009;37:328–334.
7. Shaham Y, Hope BT. The role of neuroadaptations in relapse todrug seeking. Nat Neurosci 2005;8:1437–1439.
8. Everitt BJ, Wolf ME. Psychomotor stimulant addiction: a neuralsystems perspective. J Neurosci 2002;22:3312–3320.
9. Willuhn I, Burgeno LM, Everitt BJ, Phillips PEM. Hierarchicalrecruitment of phasic dopamine signaling in the striatum during theprogression of cocaine use. Proc Natl Acad Sci USA 2012;109:20703–20708.
10. Koob GF. Drugs of abuse: anatomy, pharmacology and functionof reward pathways. Trends Pharmacol Sci 1992;13:177–184.
11. Murray JE, Belin D, Everitt BJ. Double dissociation of thedorsomedial and dorsolateral striatal control over the acquisitionand performance of cocaine seeking. Neuropsychopharmacol 2012;37:2456–2466.
12. Zapata A, Minney VL, Shippenberg TS. Shift from goal-directedto habitual cocaine seeking after prolonged experience in rats.J Neurosci 2010;30:15457–15463.
13. Jonkman S, Pelloux Y, Everitt BJ. Differential roles of thedorsolateral and midlateral striatum in punished cocaine seeking.J Neurosci 2012;32:4645–4650.
14. Porrino LJ, Lyons D. Orbital and medial prefrontal cortex andpsychostimulant abuse: studies in animal models. Cereb Cortex2000;10:326–333.
15. Porrino LJ, Daunais JB, Smith HR, Nader MA. The expandingeffects of cocaine: studies in a nonhuman primate model of cocaineself-administration. Neurosci Biobehav R 2004;27:813–820.
16. Porrino LJ, Smith HR, Nader MA, Beveridge TJR. The effectsof cocaine: a shifting target over the course of addiction. ProgNeuro-Psychoph 2007;31:1593–1600.
17. Porrino LJ, Lyons D, Smith HR, Daunais JB, Nader MA. Cocaineself-administration produces a progressive involvement of limbic,association, and sensorimotor striatal domains. J Neurosci 2004;24:3554–3562.
430 M. J. McHugh et al. Am J Drug Alcohol Abuse, 2013; 39(6): 424–432
Am
J D
rug
Alc
ohol
Abu
se D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y T
ulan
e U
nive
rsity
on
09/0
1/14
For
pers
onal
use
onl
y.

18. Kalivas PW. Addiction as a pathology in prefrontal corticalregulation of corticostriatal habit circuitry. Neurotox Res 2008;14:185–189.
19. Jentsch JD, Taylor JR. Impulsivity resulting from frontostriataldysfunction in drug abuse: implications for the control of behaviorby reward-related stimuli. Psychopharmacology 1999;146:373–390.
20. McFarland K, Lapish CC, Kalivas PW. Prefrontal glutamate releaseinto the core of the nucleus accumbens mediates cocaine-inducedreinstatement of drug-seeking behavior. J Neurosci 2003;23:3531–3537.
21. McFarland K, Davidge SB, Lapish CC, Kalivas PW. Limbic andmotor circuitry underlying footshock-induced reinstatement ofcocaine-seeking behavior. J Neurosci 2004;24:1551–1560.
22. Wong DF, Kuwabara H, Schretlen DJ, Bonson KR, Zhou Y, NandiA, Brasic JR, et al. Increased occupancy of dopamine receptors inhuman striatum during cue-elicited cocaine craving.Neuropharmacology 2006;31:2716–2727.
23. Wilcox CE, Teshiba TM, Merideth F, Ling J, Mayer AR. Enhancedcue reactivity and fronto-striatal functional connectivity in cocaineuse disorders. Drug Alcohol Depen 2011;115:137–144.
24. Duncan E, Boshoven W, Harenski K, Fiallos A, Tracy H,Jovanovic T, Hu X, et al. An fMRI study of the interaction ofstress and cocaine cues on cocaine craving in cocaine-dependentmen. Am J Addiction 2007;16:174–182.
25. Bonson KR, Grant SJ, Contoreggi CS, Links JM, Metcalfe J,Weyl HL, Kurian V, et al. Neural systems and cue-induced cocainecraving. Neuropharmacology 2002;26:376–386.
26. Volkow ND, Wang G-J, Telang F, Fowler JS, Logan J, ChildressAR, Jayne M, et al. Cocaine cues and dopamine in dorsal striatum:mechanism of craving in cocaine addiction. J Neurosci 2006;26:6583–6588.
27. Koya E, Uejima JL, Wihbey KA, Bossert JM, Hope BT, Shaham Y.Role of ventral medial prefrontal cortex in incubation of cocainecraving. Neuropharmacology 2009;56:177–185.
28. Volkow ND, Fowler JS, Wang GJ, Baler R, Telang F. Imagingdopamine’s role in drug abuse and addiction. Neuropharmacology2009;56:3–8.
29. Volkow ND, Fowler JS, Wolf AP, Schlyer D, Shiue CY, Alpert R,Dewey SL, et al. Effects of chronic cocaine abuse on postsynapticdopamine receptors. Am J Psychiat 1990;147:719–724.
30. Asensio S, Romero MJ, Romero FJ, Wong C, Alia-Klein N,Tomasi D, Wang GJ, et al. Striatal dopamine D2 receptoravailability predicts the thalamic and medial prefrontal responsesto reward in cocaine abusers three years later. Synapse 2010;64:397–402.
31. Goldstein RZ, Volkow ND. Drug addiction and its underlyingneurobiological basis: neuroimaging evidence for the involvementof the frontal cortex. Am J Psychiat 2002;159:1642–1652.
32. Volkow ND, Fowler JS. Addiction, a disease of compulsion anddrive: involvement of the orbitofrontal cortex. Cereb Cortex 2000;10:318–325.
33. van der Plas EA, Crone EA, van den Wildenberg WP, Tranel D,Bechara A. Executive control deficits in substance-dependentindividuals: a comparison of alcohol, cocaine, and methampheta-mine and of men and women. J Clin Exp Neuropsyc 2009;31:706–719.
34. Adinoff B, Braud J, Devous MD, Harris TS. Caudolateralorbitofrontal regional cerebral blood flow is decreased in abstinentcocaine-addicted subjects in two separate cohorts. Addict Biol2012;17:1001–1012.
35. Dalley JW, Fryer TD, Brichard L, Robinson ES, Theobald DE,Laane K, Pena Y, et al. Nucleus accumbens D2/3 receptors predicttrait impulsivity and cocaine reinforcement. Int S Techn Pol Inn2007;315:1267–1270.
36. Belin D, Mar AC, Dalley JW, Robbins TW, Everitt BJ. Highimpulsivity predicts the switch to compulsive cocaine-taking. Int STechn Pol Inn 2008;320:1352–1355.
37. Economidou D, Pelloux Y, Robbins TW, Dalley JW, Everitt BJ.High impulsivity predicts relapse to cocaine-seeking after punish-ment-induced abstinence. Int Congr Ser 2009;65:851–856.
38. Moeller FG, Dougherty DM, Barratt ES, Schmitz JM, Swann AC,Grabowski J. The impact of impulsivity on cocaine use andretention in treatment. J Subst Abuse Treat 2001;21:193–198.
39. Hanlon CA, Wesley MJ, Stapleton JR, Laurienti PJ, Porrino LJ. Theassociation between frontal-striatal connectivity and sensorimotorcontrol in cocaine users. Drug Alcohol Depen 2011;115:240–243.
40. Gu H, Salmeron BJ, Ross TJ, Geng X, Zhan W, Stein EA, Yang Y.Mesocorticolimbic circuits are impaired in chronic cocaine users asdemonstrated by resting-state functional connectivity. NeuroImage2010;53:593–601.
41. Biswal B, Yetkin FZ, Haughton VM, Hyde JS. Functionalconnectivity in the motor cortex of resting. Magnet Reson Med1995;34:537–541.
42. Greicius MD, Krasnow B, Reiss AL, Menon V. Functionalconnectivity in the resting brain: a network analysis of the defaultmode hypothesis. Proc Natl Acad Sci USA 2003;100:253–258.
43. Sutherland MT, McHugh MJ, Pariyadath V, Stein EA. Resting statefunctional connectivity in addiction: Lessons learned and a roadahead. NeuroImage 2012;62:1–15.
44. Barratt ES. Impulsiveness and aggression. In: Monahan J,Steadman H, eds. Violence and mental disorder. Chicago, IL:Univeristy of Chicago Press; 1994:61–79.
45. Patton JH, Stanford MS, Barratt ES. Factor structure of the Barrattimpulsiveness scale. J Clin Psychol 1995;51:768–774.
46. Cox RW. AFNI: software for analysis and visualization offunctional magnetic resonance neuroimages. Comput Biomed Res1996;29:162–173.
47. Geng X, Christensen GE, Gu H, Ross TJ, Yang Y. Implicitreference-based group-wise image registration and its applica-tion to structural and functional MRI. NeuroImage 2009;47:1341–1351.
48. MacKinnon DP, Fairchild AJ, Fritz MS. Mediation analysis.Annu Rev Psychol 2007;58:593–614.
49. Mackinnon DP, Lockwood CM, Hoffman JM, West SG, Sheets V.A comparison of methods to test mediation and other interveningvariable effects. Psychol Methods 2002;7:83–104.
50. Mackinnon DP, Dwyer JH. Estimating mediated effects in preven-tion studies. Evaluation Rev 1993;17:144–158.
51. Moeller FG, Dougherty DM, Barratt ES, Oderinde V, Mathias CW,Harper RA, Swann AC. Increased impulsivity in cocaine dependentsubjects independent of antisocial personality disorder and aggres-sion. Drug Alcohol Depen 2002;68:105–111.
52. Moeller FG, Barratt ES, Fischer CJ, et al. P300 event-relatedpotential amplitude and impulsivity in cocaine-dependent subjects.Neuropsychobiology 2004;50:167–173.
53. Moreno-Lopez L, Catena A, Fernandez-Serrano MJ, Delgado-RicoE, Stamatakis EA, Perez-Garcıa M, Verdejo-Garcıa A.Trait impulsivity and prefrontal gray matter reductions incocaine dependent individuals. Drug Alcohol Depen 2012;125:208–214.
54. Verdejo-Garcıa AJ, Perales JC, Perez-Garcıa M. Cognitive impul-sivity in cocaine and heroin polysubstance abusers. Addict Behav2007;32:950–966.
55. Everitt BJ, Robbins TW. Neural systems of reinforcement for drugaddiction: from actions to habits to compulsion. Nat Neurosci 2005;8:1481–1489.
56. Koob GF, Volkow ND. Neurocircuitry of addiction.Neuropharmacology 2010;35:217–238.
57. Robinson TE, Berridge KC. The psychology and neurobiology ofaddiction: an incentive-sensitization view. Addiction (Abingdon,England) 2000;95:S91–S117.
58. Naqvi NH, Bechara A. The insula and drug addiction: aninteroceptive view of pleasure, urges, and decision-making. BrainStruct Funct 2010;214:435–450.
59. Naqvi NH, Rudrauf D, Damasio H, Bechara A. Damage to theinsula disrupts addiction to cigarette smoking. Int S Techn Pol Inn2007;315:531–534.
60. Ture U, Yas� argil DC, Al-Mefty O, Yas� argil MG. Topographicanatomy of the insular region. J Neurosurg 1999;90:720–733.
61. Augustine JR. Circuitry and functional aspects of the insular lobein primates including humans. Brain Res 1996;22:229–244.
62. Craig AD. How do you feel–now? The anterior insula and humanawareness. Nat Rev Neurosci 2009;10:59–70.
63. Naqvi NH, Bechara A. The hidden island of addiction: the insula.Trends Neurosci 2009;32:56–67.
64. Heil SH, Johnson MW, Higgins ST, Bickel WK. Delay discountingin currently using and currently abstinent cocaine-dependent
DOI: 10.3109/00952990.2013.847446 Striatal-insula circuits in cocaine addiction 431
Am
J D
rug
Alc
ohol
Abu
se D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y T
ulan
e U
nive
rsity
on
09/0
1/14
For
pers
onal
use
onl
y.

outpatients and non-drug-using matched controls. Addict Behav2006;31:1290–1294.
65. Coffey SF, Gudleski GD, Saladin ME, Brady KT. Impulsivityand rapid discounting of delayed hypothetical rewards incocaine-dependent individuals. Exp Clin Psychopharm 2003;11:18–25.
66. McClure SM, Laibson DI, Loewenstein G, Cohen JD. Separateneural systems value immediate and delayed monetary rewards. IntS Techn Pol Inn 2004;306:503–507.
67. Kayser AS, Allen DC, Navarro-Cebrian A, Mitchell JM, Fields HL.Dopamine, corticostriatal connectivity, and intertemporal choice.J Neurosci 2012;32:9402–9409.
68. Wittmann M, Leland DS, Paulus MP. Time and decision making:differential contribution of the posterior insular cortex and thestriatum during a delay discounting task. Exp Brain Res 2007;179:643–653.
69. Tanaka SC, Doya K, Okada G, Ueda K, Okamoto Y, Yamawaki S.Prediction of immediate and future rewards differentially recruitscortico-basal ganglia loops. Nat Neurosci 2004;7:887–893.
70. Wittmann M, Paulus MP. Decision making, impulsivity and timeperception. Trends Cogn Sci 2008;12:7–12.
71. Wittmann M, Simmons AN, Aron JL, Paulus MP. Accumulation ofneural activity in the posterior insula encodes the passage of time.Neuropsychologia 2010;48:3110–3120.
72. Livesey AC, Wall MB, Smith AT. Time perception: manipulationof task difficulty dissociates clock functions from other cognitivedemands. Neuropsychologia 2007;45:321–331.
73. Yin HH, Knowlton BJ. The role of the basal ganglia in habitformation. Nat Rev Neurosci 2006;7:464–476.
74. Wunderlich K, Dayan P, Dolan RJ. Mapping value based planningand extensively trained choice in the human brain. Nat Neurosci2012;15:786–791.
75. Setlow B, Mendez IA, Mitchell MR, Simon NW. Effects of chronicadministration of drugs of abuse on impulsive choice (delaydiscounting) in animal models. Behav Pharmacol 2009;20:380–389.
76. Gardini S, Venneri A. Reduced grey matter in the posterior insulaas a structural vulnerability or diathesis to addiction. Brain Res Bull2012;87:205–211.
77. Ersche KD, Barnes A, Simon Jones P, Morein-Zamir S, RobbinsTW, Bullmore ET. Abnormal structure of frontostriatal brainsystems is associated with aspects of impulsivity and compulsivityin cocaine dependence. Brain 2011;134:2013–2024.
78. Mackillop J, Amlung MT, Few LR, Ray LA, Sweet LH,Munafo MR. Delayed reward discounting and addictive behavior:a meta-analysis. Psychopharmacology 2011;216:305–321.
79. Redish AD. Addiction as a computational process gone awry.Int S Techn Pol Inn 2004;306:1944–1947.
Supplemental content
Supplementary Methods: Data Analysis
Supplementary Results: Putamen Connectivity
Supplemental content is available for download at informahealthcare.com/ada.
432 M. J. McHugh et al. Am J Drug Alcohol Abuse, 2013; 39(6): 424–432
Am
J D
rug
Alc
ohol
Abu
se D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y T
ulan
e U
nive
rsity
on
09/0
1/14
For
pers
onal
use
onl
y.