Embed Size (px)
Citation preview

Subcutaneous mycoses (3) Lobomycosis
Mrs. Dalia Kamal Eldien
Msc in MicrobiologyLecture NO (8)

Objectives
• Introduction to lobomycosiso Causative agent o Mode of transmission o Clinical featureso Laboratory diagnosiso Treatment Introduction to Rhinosporidiosiso Causative agent o Mode of transmission o Clinical featureso Laboratory diagnosiso Treatment

Introduction
The main subcutaneous fungal infections include:MycetomaChromoblastomycosisSporotrichosisLobomycosisRhinosporidiosisSubcutaneous zygomycosis Subcutaneous phaeohyphomycosis.

Introduction
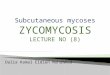
Lobomycosis also known as Lobo's disease or lacaziosis, is a rare chronic fungal infection of the subcutaneous tissue found in South America, mainly in Brazil.
Affects humans and members of the family Delphinidae Lobomycosis, a disease caused by the uncultivable
dimorphic fungi Lacazia loboi, formerly named Loboa loboi
Remains to date as an enigmatic illness, due to the impossibility of its aetiological agent to be cultured and grown in vitro, as well as because of its
unresponsiveness to specific antifungal treatments.

Clinical features
Infection most commonly develops after minor scratches or insect bites, but many patients cannot recall any skin trauma.
Human-to-human transmission does not occur, and the disease is only acquired from the environment.
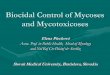
The appearances are of a chronic keloidal nodular lesions occur on the face, ears, or extremities.
The lesions are generally painless, that can resemble nodular leprosy or leishmaniasis, other subcutaneous mycoses (sporotrichosis, chromomycosis)

Different types of lesions may be seen at various stages of disease progression.
The disease generally does not affect the epidermis, and therefore skin lesions usually have a smooth and shiny appearance.
The disease is often misdiagnosed as Blastomyces dermatitidis or Paracoccidiodes brasiliensis due to its similar morphology.
Lesions can appear as isolated or aggregated, particularly in the exposed cooler areas of the body such as upper and lower limbs and ears.

Lobomycosis lesion

Lobomycosis lesion

Lobomycosis in dolphin

Laboratory diagnosis
Clinical material:
Tissue sample (a skin biopsy) obtained by curettage or surgical biopsy.
Direct Microscopy:
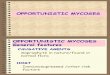
Tissue can be macerated and mounted in 10% KOH and Parker ink or calcofluor white mounts Lacazia loboi is characterized by long chains of spherical cells interconnected by tubules. The cells appear to be yeast-like with a diameter of 5 to 12 μm.
Culture:
L. loboi is an extremely slow growing fungus with a prolonged incubation period, which explains the chronic evolution of the disease. Attempts to culture L. loboi have so far been unsuccessful.

Histopathological examination H&E: the epidermis is usually atrophic and the dermis
is occupied by a fibrous, diffuse, inflammatory granuloma composed of histocytes, and giant cells containing the typical thick-walled cells.
Periodic acid-Schiff, GMS , Grocott's methenamine silver or Gram stains clearly distinguish the yeast-like cells
Serology: The serological tests are not available. Identification: Clinical features, geographic location
and microscopic morphology are important.

chained yeast cells consistent with Lacazia loboi a) H&E b) silver stain

yeast cells of Lacazia loboi

Treatment
For treatment, surgical removal of the lesions, followed by itraconazole and clofazimine for disseminated lesions, has been used with variable results.
Surgical removal of the lesion is often performed to prevent or correct cosmetic disfigurement.

Rhinosporidiosis
Rhinosporidiosis is a chronic granulomatous infection of the mucous membranes affecting the mucous membrane of nasopharynx, oropharynx, conjunctiva, rectum and external genitalia.
Though the floor of the nose and inferior turbinate are the most common sites, the lesions may appear elsewhere too.
The etiologic agent, Rhinosporidium seeberi, has never been successfully propagated in vitro.
This organism was previously considered to be a fungus, and Rhinosporidiosis is classified as a fungal disease under, It is now considered to be a parasite, classified under a new class Mesomycetozoea.

Ocular Rhinosporidiosis

Diagnosis
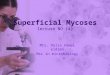
Microscopic demonstration of spherules (sporangia) of R seeberi in biopsy specimens confirms the diagnosis.
The spherules may be numerous, vary in size up to 300 μm, and contain spores that mature at different rates 4–19 μm in diameter, have thick walls that stain periodic acid-Schiff positive,
The organism has not been cultured.

Sporangia of Rhinosporidium
seeberi

Treatment
Surgical excision - wide excision with electro-coagulation of the lesion base
Medical treatment is not so effective but treatment with a year long course of dapsone has been reported