Embed Size (px)
Citation preview

Sumit Ray Senior Consultant & Vice-Chair
Critical Care & Emergency Medicine Sir Ganga Ram Hospital



ARDS pathophysiology B Taylor Thompson et al. NEJM 2017;377:562-72.

-
Outcome
Australian Epidemiologic study A 28-day mortality rate of 32% Bersten AD, et al. Incidence of mortality of ALI and ARDS in three Australian States. AJRCCM
2002; 165:443-448
European ALIVE Study Group ICU mortality and hospital mortality 46% and 55% respectively Brun-Buisson C, et al. Epidemiology and outcome of ALI in European intensive care units:
results from the ALIVE study. Intensive Care Med 2004; 30:51-61
LUNG SAFE Trial (5 continents,50 countries, 459 ICU’s) Hospital mortality of 35% (Mild),40%(Moderate) & 46% (Severe) Bellani et al. Epidemiology, patterns of care & mortality for patients of ARDS in ICU’s in 50
countries. JAMA 2016; 315(8) 788-800
Mortality

Baby Lung Concept Recognised in mid-1980’s
ARDS resulted in significant reduction in the amount of normally aerated lung tissue
But, with preserved areas of normal compliance “The ‘baby lung’ which was markedly over distended by high tidal volumes”
Gattinoni L, Preseti A. The concept of ‘baby lung’
Intensive Care Med 1996; 17:555-75

Spectrum of Regional Opening Pressures (Supine Position)
Superimposed
Pressure Inflated 0
Alveolar Collapse
(Reabsorption) 20-60 cmH2O
Small Airway Collapse
10-20 cmH2O
Consolidation
(from Gattinoni)
Lung Units at Risk for Tidal
Opening & Closure =
Opening
Pressure

ARDS– Problems & concerns
Strain (stretch) due to over distension of compliant alveoli
leading to volutrauma. (Lung strain is the ratio of TV/FRC)
Shear stress due to complete closure & re-opening of non-
compliant alveoli (atelectrauma).
(Stress is defined as transpulmonary pressure at the end of inspiration (PTPinsp)
High inspiratory pressures (Pplat) leading to barotrauma.
Release of inflammatory mediators from lung (biotrauma)
Leading to VILI(Ventilator induced lung injury)

VILI

10 university centers in the US N =861
Conventional (429) Low VT (432)
Vt = 12 mls/kg
Pplat =<50cms of H2O
Vt = 6 mls/kg
Pplat =<30cms of H2O
PEEP based on protocol – up to 20 to 24
Labelled as Respiratory Management in Acute Lung Injury/ARDS Trial (ARMA)

ARDSnet Tidal Volume Study
NEJM 2000;342:1301-8.
Mortality: Intervention group: 31% Control group: 39.8% p Value: 0.007
Other benefits: Lower duration of ventilation Lower incidence of non-lung organ failure days

Ventilator Strategies in ARDS
Objectives
Adequate ventilation of compliant alveoli without causing: Volutrauma
Avoid Barotrauma
Strategies
Small VT (4-6ml/kg)
High RR (30/min)
Allowing hypercapnia (?) (PaCO2 80mm Hg)
Limit PPlat 30 cms H2O
Pressure Control Ventilation (± IRV) or Dual modes PRVC/Autoflow(if needed)

From: Association Between Use of Lung-Protective Ventilation With Lower Tidal Volumes and Clinical
Outcomes Among Patients Without Acute Respiratory Distress Syndrome-A Meta-analysis
JAMA. 2012;308(16):1651-1659. doi:10.1001/jama.2012.13730
20 studies -1416 pts Low VT — 1406 pts Conventional vent

Ventilator Strategies in ARDS Recruitment Maneuver
Objectives Recruitment- opening up
closed, non-compliant alveoli
Recruitment potential is highest in early phase & in extra pulmonary ARDS
Strategies
Recruitment maneuvers
30-40cms CPAP for 30-40 secs
Series of PCV breaths-Phigh 40-50 cm H2O & PEEP of 20-35 cm H2O for 2 mins
Series of large VT=12-15 ml/kg for 2 mins
CT-Scan method

Recruitable lung

6 Trials = 1423 pts
Mortality

Oxygenation
Barotrauma
Rescue Therapies

2016

PCV at RR of 10/min
2 mins PEEP =45


Ventilator strategies in ARDS
Objectives
Stop De-recruitment of recruited alveoli(open lung), thus avoiding ‘shear stress’(atelectrauma)
Strategies Titrated PEEP
Incremental in PEEP
Decremental steps of PEEP
LIP method (Amato)
ARDS Net table
CT scan method
USG method

Open Lung Ventilation Strategy
Volume
Pressure
Zone of Overdistention
Safe
window
Zone of
Derecruitment
and
atelectasis
Goal is to avoid injury zones
and operate in the safe window
Froese, CCM, 1997

Adjusting PEEP ARDS Network study
Fixed combinations of FiO2 and PEEP Arterial Oxygenation Goal: PaO2=55-80
mmHg or SpO2=88-95% FiO2 PEEP FiO2 PEEP 0.3 5 0.7 12 0.4 5 0.7 14 0.4 8 0.8 14 0.5 8 0.9 14 0.5 10 0.9 16 0.6 10 0.9 18 0.7 10 1.0 20-24
Brower et.
ARDS Network
NEJM
2000;342:1301-
1308


Better survival
Less Rescue Therapies with High PEEP in moderate-severe ARDS
Moderate/Severe ARDS Mild

RCT =120 ICU’s= 1010 pts
INTERVENTIONS: Experimental group-- Lung recruitment maneuver and PEEP titration according to the Best CRS (n = 501;) or a Control strategy of low PEEP (n = 509). Recruitment maneuver of 45 cms H2O of PEEP → ↓ed to 35 cms later

“…an unfavorable balance between potential positive (reduction in ∆P) and negative (increase in overdistention, hemodynamic impairment) physiological consequences of lung recruitment and PEEP.”

“….we hypothesized that normalizing VT to CRS and using the ratio as an index
indicating the “functional” size of the lung would provide a better predictor of
outcomes in patients with ARDS than VT alone.
This ratio, termed the driving pressure (ΔP = VT/CRS).”
Derivation cohort=336 pts
Validation cohort =861 pts
Re-validation = 2365 pts

RESULTS
-Among ventilation variables, ΔP was most strongly associated with survival.
- A 1-SD increment in ΔP (≈ 7 cm of H2O) was associated with increased mortality
(RR = 1.41; 95% CI 1.31 to 1.51; P<0.001),
-Even in patients receiving ―protective‖ plateau pressures and VT (RR= 1.36; 95% CI,
1.17 to 1.58; P<0.001).
-Individual changes in VT or PEEP after randomization were not independently
associated with survival; they were associated only if they were among the changes that
led to reductions in ΔP
14


Prone Position

Shape Matching & Sponge Theory ↓ Strain

Methods: 24 ARDS pts on MV with 6ml/kg PBW underwent whole lung CT-Scans at breath-holding pressures of 5, 15 & 45 cms of H2O at PEEP of 5 & 15 cms in Supine & Prone positions →RM performed (45 cms of H2O) before each PEEP change
Lung recruitability was defined as the difference in % of non-aerated tissue between 5 and 45 cm H2O. Cyclic recruitment/de-recruitment was determined by tidal changes in % of non-aerated lung tissue Tidal hyperinflation was determined by % of hyper-inflated lung

Results:
Supine position →↑ing PEEP from 5 to 15 cmH2O,↓non-aerated
tissue(501 to 322 gms) (P<0.001) but, ↑ tidal-hyperinflation (0.41 to
0.57 %; P=0.004)
Prone positioning further ↓ non-aerated tissue (322 to 290 gms)
(P=0.028) & ↓ tidal hyperinflation observed at PEEP 15 in supine pts
Cyclic recruitment/de-recruitment ↓ only when high PEEP & prone
positioning were applied together (4.1 to 2.9%; P= 0.003)

Prone Position- Initial studies
Improves oxygenation Allows ventilation with lower VT, pressures, FiO2 Drainage of secretions Rise in PaO2 sustained after return to supine Problems
Pressure ulcers, facial edema Lines, tubes CPR
20% patients are non-responders Does not improve outcome in ARDS
Gattinoni et al
NEJM 2001;345:568-73.

Difference in Survival: Prone vs Supine

PROSEVA trial
Prone= 237 / Supine=229


Damned if you do & damned if
you don’t?!

Benefits of spontaneous breathing during invasive mechanical ventilation Diaphragm muscle tone:
Controlled MV → diaphragmatic muscle dysfunction & atrophy →
detectable within 18 hrs
Pulmonary Function:
- Spontaneous breathing ↑ aeration in dependent lung , as well as ↑
lung perfusion
- Intrapulmonary shunt is ↓, V/Q matching and oxygenation ↑
Cardiovascular Effects:
- CMV ↓ transvascular pressure & ventricular preload & afterload.
- Spontaneous breathing– does just the opposite → may ↑ or↓ CO
depending on ventricular contractility & volume status

Spontaneous Breathing Causes Injury during Mechanical Ventilation!
Experimental studies: mechanically ventilated rabbits with established lung injury → vigorous spontaneous effort did not
change Pplat but did worsen injury
“Strong spontaneous effort can injure not only the injured lung but also the diaphragm.”*
RCT’s support this concept in demonstrating that NM blockade (to prevent spontaneous effort) results in improved lung function, and increased survival in severe ARDS. **
*Goligher et al: Evolution of diaphragm thickness during mechanical ventilation: impact of
inspiratory effort. AJRCCM 2015;192:1080–1088
** Papazian et al, ACURASYS Study Investigators. Neuromuscular blockers in early ARDS N Engl J
Med 2010;363:1107–1116.

Mechanisms of Injury from Spontaneous Breathing
Increased Lung Perfusion
Distending Pressure & ↑Tidal Volumes
Patient–Ventilator Asynchrony

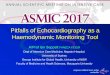
Increased Lung perfusion & distending pressures
Mechanical Breath Spontaneous effort
Transpulmonary pressure
(Paw-Ppl = PL)= 30-10 =20
Transvascular pressure
(Pcap-Ppl) is low (12- 10 = 2)
Transpulmonary pressure
(Paw-Ppl = PL)= 30+20 =50
Transvascular pressure
(Pcap-Ppl) = 8-(-20) = 28

Spontaneous effort and distribution of regional
ventilation and pleural pressure
The ―swing‖ in regional Ppl is 2-fold greater than the ―swing‖ in Pes
→indicating that diaphragm contraction results in greater distending
pressure applied to the regional lung near the diaphragm, compared with the
pressure transmitted to the remainder of the lung (i.e., Pes).
Insp Pl Pressure
End-expiration End-Inspiration-Spontaneous Breathing
Aerated Lung Aerated Lung Partially aerated

Mechanisms of Injury from Spontaneous Breathing
In the healthy lung, changes in local Ppl, are evenly transmitted across the lung surface; this phenomenon is called “fluid-like” behavior
In contrast, injured lungs exhibit “solid-like” behavior, where a non-aerated lung region impedes the rapid generalization of a local change in Ppl→ the lung expansion is heterogeneous

Mechanisms of Injury from Spontaneous Breathing Patient–Ventilator Asynchrony
“Double triggering”- occurrence of two consecutive inspirations after
a single respiratory effort→ leads to higher VT (> 150% of preset VT)
“Reverse triggering” (entrainment) - in which the diaphragm is
“triggered” by ventilator-driven inspiration
More severe the ARDS, more chances of further injury with
spontaneous breathing.
Mild ARDS possibility of better lung functions with spontaneous
breathing

Where RR is the respiratory rate, ΔV is the tidal volume, ELrs is the elastance of the respiratory system, I:E is the inspiratory-to-expiratory time ratio, and Raw is the airway resistance.
Concept of mechanical power & ergotrauma
The potential for mechanical power to inflict lung damage is conditional upon multiple factors: 1. Mechanical heterogeneity of the tissue/local amplification 2. Size (capacity) of the baby lung; 3. Elasticity of the chest wall; 4. Maximal tidal stress 5. Magnitude of dynamic strain per cycle; 6. Size-adjusted driving power (plateau-PEEP) x VE x (Cexpected/Cobserved) 7. Maximum transpulmonary pressure achieved per cycle 8. Respiratory rate (RR) 9. Flow rate and contour of the delivered breath 10.PEEP level

The idea is to use the extracorporeal gas-exchange to reduce VT
to ―supra-lung protective ventilation‖
Extracorporeal Membrane Oxygenation

Methods: UK-based multicenter trial; 180 pts, Randomized 1:1(July 2001-August 2006) Conventional ARDS management vs Referral to ECMO
123 ECMO pts → Propensity score matching of 52 pts
Mortality did not differ between the two matched cohorts (OR= 1.48;CI, 0.68–3.23
4 RCT’s (3 with low risk of bias) =389 pts→“No statistically
significant differences in all-cause mortality at six months…..

Randomly assigned patients with very severe ARDS, as indicated by one of 3 criteria — 1. PaO2/FiO2 ratio ≤ 50 mm Hg ≥ 3 hours; 2. PaO2/FiO2 < 80 mm Hg for >6 hours or 3. An ABG pH <7.25 with a PaCO2 ≥ 60 mm Hg for > 6 hours — to
receive immediate veno-venous ECMO (ECMO group) or continued conventional treatment (control group).
EOLIA Trial

Extracorporeal CO2 removal devices

Driving Pressures
Thank you!
???




Extracorporeal CO2 removal devices


Thank You!

DPA (Driving Pressure-Airway) = PPlat – PEEP
DPL (Driving Pressure-Lung) = PTPinp – PTPexp
Stress was defined as transpulmonary pressure at the end of inspiration (PTPinsp) Strain as the relation between TV/EELV Atelectrauma as the difference between non-aerated lung during inspiratory and expiratory pause in the CT scan.

459 ICUs from 50 countries across 5 continents.
RESULTS: 29 144 pts admitted, 3022 (10.4%) fulfilled ARDS criteria → 2377 pts
managed with invasive mechanical ventilation.
LUNG-SAFE Trial

Methods: In a proof-of-concept study. 10 patients with lung injury & a VT > 8
ml/kg under PSV & sedation. After baseline measurements, rocuronium titrated to a
target VT of 6 ml/kg during NAVA→ patients were ventilated in PSV and NAVA
under continuous rocuronium infusion for 2 hrs

Methods: Secondary analysis of data from 787 ARDS patients enrolled in two
independent RCT’s- PROSEVA & ACURASYS
Results: Colinearity between ΔP, Crs and Pplat, which was expected as these
variables are mathematically coupled, was statistically significant.
Hazard ratios from the Cox models for day-90 mortality were :
ΔP = 1.05 (1.02–1.08) (P = 0.005),
Pplat = 1.05 (1.01–1.08) (P = 0.008)
Crs = 0.985 (0.972–0.985) (P = 0.029)
PEEP and VT were not associated with death in any model.
Conclusions: When ventilating patients with low VT , ΔP is a risk factor
for death in ARDS patients, as is Pplat or Crs.

15 cms of H2O
26 cms of H2O 26 ml/cms of H2O
≤ 15 J /min
Driving Pressure Mechanical Power
Plateau Pressure CRS
Adjusted 90 day mortality Cut- off for survival

Secondary analysis of 3 prospective non-interventional cohort studies focusing
on ARDS patients from 927 intensive care units (ICUs) in 40 countries- 1899 pts
Permissive Hypercapnia?

Mortality was higher even after adjusting for age, SAPS II score, RR,
PEEP, PaO2/FiO2 ratio, ∆P, Protective lung strategy, corrected minute
ventilation, and presence of acidosis
Probable causes:
1.Hypercapnia impairs innate immunity
2.Hemodynamic consequences like ↑ PA pressures & worsening RV
function are associated with worse outcomes in patients with ARDS
“Overall, the data reported here may serve as a first step towards defining
possible limits for hypercapnia. In the absence of strong evidence, our
findings may provide some guidance for reasonable limits of PaCO2 for
ARDS patients in the ICU and also for potential reassessment of the
previous assumption that severe hypercapnia is safe.”