-
Annals ofthe Rheumatic Dtseases 1990; 49: 824-829
Surgery of the rheumatoid shoulder
I G Kelly
The patient with rheumatoid disease who has anaffected shoulder
joint complex will haverestriction of movements and will usually
com-plain of pain. Not infrequently the pain isattributed to a
flare in disease activity, the armis rested by the side with the
forearm across thetrunk, and the resolution of the pain is
associatedwith permanent restriction of motion. As aresult of this
many patients may not presentwith shoulder complaints until they
cannot copewith many of the activities of daily living andhave pain
even at rest. On occasion it is thedeterioration in lower limb
joint function andthe consequent need to use walking aids
thathighlights the state of the shoulder joint. As atleast two
thirds of adult rheumatoid patientshave shoulder pain,' 2 and the
shoulder isaffected in 90% of hospital patients with rheu-matoid
arthritis,' it is important to have an
understanding of the natural history of theproblems so that
rational treatment can beplanned.
Patterns of joint diseaseRheumatoid polyarthritis can, by
definition,affect any or all of the components of theshoulder joint
complex. Disease of the sterno-clavicular joint is not uncommon but
only rarelyrequires specific treatment. It is the
acromio-clavicular and the glenohumeral joints, togetherwith the
subacromial region, which requiremost attention. Dijkstra,
Dijkstra, and Klundertin a radiological study of the
rheumatoidshoulder emphasised that changes in the
acro-mioclavicular and the glenohumeral joints donot follow the
same course either in time or inthe severity of joint destruction.4
Radiological
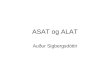
Figure I (A) Anteroposterior radiograph ofglenohumeraljoint
showing the periarticular erosions ofthe humeral headassociated
with active synovitis. These are always mostmarked near the
insertion ofthe rotator cufftendon to thegreater tuberosity. Note
the preserved glenohumeral jointspace. (B) The glenohumeral and
acromioclavicular jointswith osteophytes on the undersurface ofthe
acromion. Earlyerosions are visible in the subchondral bone ofthe
glenoid.(C) End stage rheumatoid disease ofthe shoulder with
erosionofboth the humeral head and glenoid. This will be manifestas
clinical medialisatin ofthe shoulder. Note the inferiorosteophyte,
which is more typical ofosteoarthritis.
Royal Infirmary,Glasgow G4 OSFI G Kelly
824
on June 16, 2021 by guest. Protected by copyright.
http://ard.bmj.com
/A
nn Rheum
Dis: first published as 10.1136/ard.49.S
uppl_2.824 on 1 October 1990. D
ownloaded from
http://ard.bmj.com/
-
Surgery ofthe rheumatoid shoulder
changes in the acromioclavicular joint com-monly predominate in
the early stages. My ownobservations suggest three patterns of
disease.Firstly, there is the least common group inwhich the
glenohumeral synovitis is active andproduces large erosions at the
margins of thehumeral head (fig IA). The glenoid bone stockis
usually preserved and there is a high incidenceof rotator cuff
rupture. In the second group,although there may be radiological
changes inthe glenohumeral joint, these are usually nomore than
joint space loss or narrowing, andradiological changes in the
acromioclavicularjoint and the underside of the acromion
pre-dominate (fig iB). These patients have rotatorcuff impingement
and may have small defects inthe supraspinatus tendon. The third
group isencountered about as often as the second andcomprises
severe erosion of the acromio-clavicular and glenohumeral joints
with signifi-cant loss of glenoid bone stock (fig IC) andclinical
medialisation of the shoulder. Therotator cuff may be thinned but
is intact in atleast 80% of these patients. Patients in the
firstgroup rarely seem to progress towards thechanges in the third
group, but progressionbetween the second and third groups is
notinfrequently seen.
RadiologyTo localise the changes occurring in the rheu-matoid
shoulder joint good radiographic viewsare required. The
glenohumeral joint lies at anangle of 300 to the coronal plane with
theglenoid cavity facing anteriorly. To assess thejoint space it is
therefore necessary to direct thex ray beam across the trunk. A
second view isdesirable to assess glenoid bone stock and thestate
of the humeral head. The axillary view (fig2) gives the best image
but may not be possiblein patients with very limited shoulder
move-ments. In these patients an apical projectionsuch as the
apical oblique projection of Garth,Slappey, and Ochs5 (fig 3) is of
great value. Theplane of the acromioclavicular joint is variablebut
is more nearly saggital. A 10-15' cephalictilt of the x ray beam
will avoid image overlap.
Figure 2 Axiliavy view ofthe shoulder showing loss ofthe
glenohumeral joint space and theamount ofremaining glenoid bone
stock. The acromiclaicular joint can be visualtsedthrough the
humeral head.
Figre 3 The apwal oblique view ofa rheumatoid shoulderindicating
reduced glenoid bone stock with a posteriorosteopSyte.
The radiographic changes in the rheumatoidshoulder have been
classified in several ways.For the glenohumeral joint the five
stageclassification of Larsen, Dale, and Eek6 (fig 4) isprobably
the bestknown among rheumatologists.As most patients coming to
surgery will be ingrades IV or V this system is of limited value
tosurgeons. Jonsson, Rydholm, and Lidgren haveintroduced a system
validated by operative andarthroscopic findings, which has three
stagescorresponding to loss of cartilage, humeral headerosions, and
severe destruction of the humeralhead.7 Petersson has clarified the
Larsen classi-fication of the changes which occur in
theacromioclavicular joint (fig 5), emphasising theloss of bone
which occurs,8 but to date very fewcommunications have made any
attempt todescribe the changes in this joint at all. Crossanand
Vallance considered the radiographicchanges in the
acromioclavicular and gleno-humeral joints together with the
subacromialregion and related them to the patient's func-tion.9
They found that loss of sphericity of thehumeral head and
decreasing width of thesubacromial space correlated with
deteriorationin function. Unfortunately, because of thevariable
effects of pain, function often does notmirror radiographic
changes, and this potentiallyuseful approach to classification has
not beenwidely adopted.When planning surgery the radiological
appearances are of value in so far as they showthe extent of the
bone destruction. Changes inthe soft tissues may be implied from
the bonychanges but are more usually deduced fromclinical
examination. My own study of 75consecutive rheumatoid shoulders has
shownthat the radiological staging of the glenohumeraland
acromioclavicular joints fails to correlatewell with the pattern of
the patient's pain or thepatient's functional status.
825
on June 16, 2021 by guest. Protected by copyright.
http://ard.bmj.com
/A
nn Rheum
Dis: first published as 10.1136/ard.49.S
uppl_2.824 on 1 October 1990. D
ownloaded from
http://ard.bmj.com/
-
Kelly
I
Figure 4 The Larsen, Dale, and Eek6 grading systemfor the
rheumatoid glenohumeraljoint.
Site of painThe aim of surgical treatment must be toprovide pain
relief and to restore function. Asseveral regions may be affected
the surgeonmust identify the site(s) of the pain. The site ofpain
indicated by the patient has been said to bethe best guide to its
origin. My own study,however, has shown that most
rheumatoidpatients complain of pain over the epauletteregion of the
shoulder radiating anteriorly andtowards the deltoid insertion (fig
6), irrespectiveof the degree of radiological change. Rest painwas
also common. Therefore, in these patientsthe pattern of the pain is
so non-specific that itis no guide to its origin.
Because the patient's history and the radio-graphs are poor
determinants of the site of painother methods must be used. Kessel
andWatson described the use of small injections (1ml) 1% lignocaine
into different parts of therotatorcuffto localise the site
ofimpingement. OIhave used the same technique to study the siteof
pain in 75 rheumatoid shoulders. In most
o
IV
v 0
Figure 5 The Larsen, Dale, and Eek6 systemfor
theacromioclavularjoint with diagrammatic
illustrationsfromPetersSon.8 Note the increasing erosion ofbone
withprogression ofthe disease. Reproduced withpermission ofJB
Lippincott Cofrom Clin Orthop1987; 223: 86-93.
65
6. .. .::: :
64 C AA
Fiue 6 The site ofpain indicated by thepatient in 75rheumatod
shole-r.
cases the pain emanated from the acromio-clavicular joint, the
subacromial region, or acombination of these two sites (fig 7).
Theglenohumeral joint was identified as a site ofpain infrequendy
and then only when the
826
t44
on June 16, 2021 by guest. Protected by copyright.
http://ard.bmj.com
/A
nn Rheum
Dis: first published as 10.1136/ard.49.S
uppl_2.824 on 1 October 1990. D
ownloaded from
http://ard.bmj.com/
-
Surgery ofthe rhewnatoid shoulder
24
14
sphericity of the humeral head had been lost.Thus, even with
advanced radiological changesin the glenohumeral joint, the source
of the painwas often elsewhere in the shoulder jointcomplex.Once
the site of the pain has been identified
by injection and the functional status has beenacquired from the
patient's history an informeddecision can be made about
treatment.
Operative treatmentACROMIOCLAVICULAR JOINT AND THESUBACROMIAL
REGIONIf the acromioclavicular joint is implicated byinjection
studies and fails to respond to localsteroid injection, excision of
the outer end of theclavicle can be a very effective procedure. If
thesubacromial region is also affected the excisionarthroplasty can
be combined with excision ofthe coracoacromial ligament and
anterioracromioplasty, thus decompressing the rotatorcuff tendons.
I have performed this procedurein 22 rheumatoid patients over the
past threeyears with very encouraging early results,though its
durability must remain in doubt.One patient who failed to regain
externalrotation and had lost the sphericity of thehumeral head did
not respond and subsequentlyunderwent total shoulder replacement.
Theresults of this procedure, commonly used inimpingement
syndromes,"1 12 have not pre-viously been reported in rheumatoid
arthritisand although Benjamin and Helal suggested
_r~~~~~~~~~~~~~~~~~~~.
that excision of the acromioclavicular joint wasonly rarely
indicated in this condition,'3Petersson reported good results for
this in 13patients when it was combined with bursectomyand
synovectomy of the glenohumeral joint.8
Occasionally, the disease is confined to thesubacromial bursa
and the patient presents withpain and a visible swelling (fig 8).
This conditionoften responds to subacromial intrabursal injec-tion
of steroid but, if refractory, excision of thebursa gives good
results.'4
GLENOHUMERAL JOINT'It is our concentration on this large joint
whichso often obscures the true pathology in a patientwith
rheumatoid arthritis."5 The truth of thisstatement can be attested
to by any surgeontreating the rheumatoid shoulder, but if
theglenohumeral joint can be clearly identified asthe source of
pain and limited function, severalwell evaluated surgical
procedures areavailable.
SynovectomyFor this seemingly logical procedure to besuccessful
synovium must be completelyremoved before there has been
significantdamage to the articular cartilage. Completesynovectomy
is difficult in the glenohumeraljoint and many patients have lost
their jointspace by the time of presentation. Pahle andKvarnes,
however, have reported good resultsin 54 patients followed up for
between one and16 years.2 Pain relief was gratifying and rangesof
motion were improved. No patient showedgreater than Larsen grade
III radiologicalchanges. They emphasised that the decision tocarry
out synovectomy rather than arthroplastydepended upon the joint
surfaces being smoothand congruous at arthrotomy. Myown
indicationfor this procedure is the unusual combination ofpain
located in the glenohumeral joint com-bined with the retention of
humeral headsphericity.
ArthrodesisArthrodesis of the glenohumeral joint in rheu-matoid
arthritis has been condemned by manyauthors on the grounds that the
prolongedimmobilisation necessary for fusion may pre-judice the
function of other diseased upper limbjoints. It is also felt that
the restriction ofrotation will impose a significant
functionalpenalty. Despite this Rybka and his colleaguesin Finland
have reported successful results in 39patients with rheumatoid
arthritis. 16 Afteroperation each patient was managed in a
lightthoracobrachial splint, which permitted earlymobilisation of
the ipsilateral elbow and wrist.Fusion was achieved in 900/o and
pain relief wasgood even in those with fibrous unions. Allpatients
could attend to their perineal care.
This last finding is in contrast with that of thestudy of
Cofield and Briggs,'7 in which only 44of 70 patients undergoing
arthrodesis for avariety of diagnoses could attend to theirpersonal
hygiene. The difference is almost
Figure 7 The sites atwhich injection of I ml 1%lignocaine
producedcomplete pain reliefin 75shoulders. In 21
shouldersinjections were required atboth the acromioclaviur(AC) and
subacromial sites.
Figure 8 Largesubacromial bursa.
827
on June 16, 2021 by guest. Protected by copyright.
http://ard.bmj.com
/A
nn Rheum
Dis: first published as 10.1136/ard.49.S
uppl_2.824 on 1 October 1990. D
ownloaded from
http://ard.bmj.com/
-
Kelly
certainly due to the position used for the fusion.Rybka used 200
each of abduction, flexion, andinternal rotation, which the studies
of Jonssonand his colleagues"8 have shown to be the mostdesirable
position. The more abduction presentin the fusion the less likely
is the patient to beable to reach the perineum.
Despite the success of Rybka the loss ofrotation associated with
arthrodesis makes itpotentially inferior to arthroplasty.
ArthroplastyGlenohumeral arthroplasty is now a well estab-lished
procedure, but care should be taken toseparate the results achieved
in rheumatoidarthritis from those in other diagnostic cate-gories.
Very few papers deal exclusively withrheumatoid arthritis,1922 and
even fewer giveany indication of the stage at which arthroplastyhas
been performed. Most surgeons now use anon-constrained type of
arthroplasty such asthat introduced by Neer23 (fig 9), and its
successis dependent upon the state of the deltoidmuscle and the
rotator cuff-both of which maybe impaired in rheumatoid
arthritis.
Relief of pain is a conspicuous feature ofarthroplasty, but
improvement in ranges ofmovement is usually much less dramatic.
Thisis especially true of movements against gravity,such as flexion
or abduction, where most authorsreport gains of between 14 and
240.20 21 24Internal and external rotation together withextension
show much greater improvementsand as these movements are of much
morefunctional significance (external rotation isneeded for the
hand to reach the side or theback of the head) most patients show
major
Figure 9 Radiograph ofNeer II total shoulderreplacement in a
rhewnutaoidshoulder. The glenoidcomponent is polyethyleneand has a
metal wiremarker. It isfixed withpolymethyl methacrylatebone
cement. In this patientthe humeral component hasbeen inserted
withoutcement.
Figure 10 Clinical picture ofadvanced rheumatoid diseaseofthe
glenohumeraljoint. It corresponds withfig IC.
functional gains after operation. These move-ments are only
obtained by intensive physio-therapy lasting for at least three
months, mostof which is carried out by the patient at
home.Improvement can be seen for up to two yearsafter operation.The
deltoid muscle is often thin but very
often the medialisation of the glenohumeraljoint which occurs
with erosion of the humeralhead or glenoid, or both, gives a false
impressionof the amount of wasting (fig 10). In mostpatients with
rheumatoid arthritis the rotatorcuff is intact despite advanced
joint destruc-tion.2' If the cuff is torn and irreparable a
non-constrained arthroplasty will not do well. Severalmethods of
tackling this problem have beentried but none has been very
successful. The useof a constrained arthroplasty is not a
solutionbecause loosening, especially of the scapularfixation, is
common and occurs early.25
Erosion of the glenoid bone may be verysevere in rheumatoid
arthritis (fig IC),26 andthis may prejudice the fixation of the
glenoidcomponent. In non-constrained arthroplastiesradiolucent
lines between the glenoid cementand bone (fig 11) have been
reported in 80% ofpatients,21 24 27 though revision of
glenoidcomponents is only infrequently reported. It ispossible to
manage these shoulders withoutresurfacing the glenoid-indeed on
occasion
Figure 11 Radiolucent lines between the bone and bonecement.
These changes were apparent within twoyears ofswgery, but the
patient remains asymptomatic sixyears later.
828
on June 16, 2021 by guest. Protected by copyright.
http://ard.bmj.com
/A
nn Rheum
Dis: first published as 10.1136/ard.49.S
uppl_2.824 on 1 October 1990. D
ownloaded from
http://ard.bmj.com/
-
Surgery ofthe rheumatoid shoulder
there may be insufficient bone stock for theglenoid component.
Marmor reported en-couraging results in 10 rheumatoid patientswith
only humeral head replacement,28 butClayton and his colleagues
reported inferiorresults of the hemiarthroplasty in comparisonwith
total joint replacement.'9 Gschwendreported that only 32% of
rheumatoid patientsfelt themselves to be 'much improved'
afterhemiarthroplasty as opposed to 82% after totaljoint
replacement.29
Resurfacing of the humeral head has beenused in rheumatoid
arthritis. In 1980 Varianreported the use of a silastic cup
covering thehumeral head in a series of 30 patients, 28 ofwhom had
rheumatoid arthritis.30 Pain reliefwas good initially, but recovery
of the motiondepended almost entirely upon the improvedrange of
scapulothoracic motion, and longerfollow up has highlighted the
problems ofsubluxation of the prosthesis and fragmentationof the
silastic cup with a consequent serioustissue reaction. Jonsson and
coworkers havereported the use of a cemented stainless steelcup to
cover the humeral head in 24 end stagerheumatoid shoulders with
very encouragingresults at two years.3' More recent studies
byJonsson32 suggest that the results are durable.This technique is
not suitable, however, wherethere has been extensive destruction of
thehumeral head.
Although failure of shoulder arthroplasty isuncommon it can be
managed by either revisionarthroplasty, excision arthroplasty, or
arthro-desis.2' 3
Other proceduresShoulder arthroplasty is contraindicated by
thepresence of infection or deltoid paralysis and, asalready
mentioned, absence of the rotator cuffor gross glenoid bone loss
can make arthroplastyinappropriate. In these situations useful
painrelief and functional improvement can beobtained by the use of
a double osteotomy.34This procedure entails incomplete osteotomy
ofthe surgical neck of the humerus and theglenoid neck. Pain relief
is often dramatic and itis apparently this which permits an
increase inthe range of movement of the shoulder girdle.The related
procedure of glenoidectomy,athough giving good results,35 36 can no
longerbe recommended for routine use as removal ofthe glenoid will
prevent the later performance ofan arthroplasty. It may still have
a role as asalvage procedure, however.
ConclusionCareful assessment of the rheumatoid patientwith
shoulder pain will permit the mostappropriate form of management to
be selected.With proper selection it is possible to achieve ahigh
degree of success with excellent pain reliefand restoration of
useful function.
1 Gschwend N. The rheumatoid shoulder. Surgical treatment
ofrhewnatoid arthritis. Stuttgart: Thieme, 1980: 35-44.
2 Pahle J A, Kvarnes L. Shoulder synovectomy. Ann ChirGynaecol
[Supplj 1985; 198: 37-9.
3 Petersson C J. Painful shoulders in patients with
rheumatoidarthritis. Prevalence, clinical and radiological
features.Scand J Rheunatol 1986; 15: 275-9.
4 Dijkstm J, Dijkstra M D, Klundert W V D. Rheumatoidarthritis
of the shoulder. Description and standard radio-graphs.
Forrschritte auf dem Gebiete der Rontgenstrahlen1985; 142:
179-85.
5 Garth W P Jr, Slappey C E, Ochs C W.
Roentgenographicdemonstration of instability of the shoulder: the
apicaloblique projection: a technical note. J Bone Joint Surg[Aml
1984; 66: 1450-3.
6 Larsen A, Dale K, Eek M. Radiographic evaluation ofrheumatoid
arthritis and related conditions by standardreference film. Acta
Radiol [Diagnl (Stockh) 1977; 18:481-91.
7 Jonsson E, Rydholm U, Lidgren L. A radiographic stagingsystem
for the glenohumeral joint in patients with rheuma-toid arthritis.
Quoted in: Jonsson E. Surgery of therheunatoid shoulder. Sweden:
University of Lund, 1988.(MD thesis.)
8 Petersson C J. The acromioclavicular joint in
rheumatoidarthritis. Clin Orthop 1987; 223: 86-93.
9 Crossan J F, Vallance R. The shoulder joint in
rheumatoidarthritis. In: Bayley I, Kessel L, eds. Shoulder
srgery.Berlin: Springer, 1982: 131-8.
10 Kessel L, Watson M. The painful arc syndrome.
Clinicalclassification as a guide to management. J Bone joint
Surg[Br] 1977; 59: 166-72.
11 Neer C S. Anterior acromioplasty for the chronic impinge-ment
syndrome of the shoulder. A preliminary report.J Bone joint Surg
[Am] 1972; 54: 41-50.
12 Watson M. The refractory painful arc syndrome.J BoneJointSurg
[Br] 1978; 60: 544-6.
13 Benjamin A, Hela B. Surgical repair and reconstrunction
inrheumatoid disease. London: Macmillan, 1980: 95-106.
14 Souter W A. The surgical treatment of the rheumatoidshoulder.
Ann Acad Med Singapore 1983; 12: 243-55.
15 Kessel L, Bayley I, eds. Clinical disorders of the shoulder.
2nded. Edinburgh: Churchill Livingstone, 1986.
16 Rybka V, Raunio P, Vainio K. Arthrodesis of the shoulder
inrheumatoid arthritis. A review of 41 cases. J Bone JointSurg [Br]
1979; 61: 155-8.
17 Cofield RH, BriggsB T. Glenohumeral arthrodesis. Operativeand
long term functional results. J Bone Joint Surg [Am]1979; 61:
668-77.
18 Jonsson E, Brattstrom M, Lidgren L. Evaluation of
therheumatoid shoulder after hemiarthroplasty and arthro-desis.
ScandJ Rheumatol 1988; 17: 17-26.
19 Clayton M L, Ferlic D C, Jeffers P D. Prosthetic
arthro-plasties of the shoulder. Clin Orthop 1982; 164: 184-91.
20 Pahle J A, Kvarnes L. Shoulder replacement arthroplasty.Ann
Chir Gynaecol [Suppl] 1985; 198: 85-9.
21 Kelly I G, Foster R S, Fisher W D. Neer total
shoulderreplacement in rheumatoid arthritisJ Bonejoint Surg
[Br]1987; 69: 723-6.
22 Sledge C B, Kozinn S C, Thornhill T S, Barrett W P.
Totalshoulder arthroplasty in rheumatoid arthritis. In: LettinA W
F, Petersson C J, eds. Rheumatoid arthritis surgery ofthe shoulder.
Basel, New York: Karger, 1989: 95-102.
23 Neer C S, Watson K C, Stanton F J. Recent experience
inshoulder replacement. J Bone joint Surg [Am] 1982; 64:319-37.
24 Cofield R H. Total shoulder arthroplasty with the
Neerprosthesis. J Bone Joint Surg [Aml 1984; 66: 899-906.
25 Lettin A. Shoulder replacement in rheumatoid
arthritis.Reconstr Surg Traumatol 1981; 18: 55-62.
26 Beddow F H. Surgical management of rheumatoid
arthritis.London: Butterworth, 1988.
27 Amstutz H C, Sew-Hoy A L, Clarke I C. UCLA anatomictotal
shoulder arthroplasty. Clin Orthop 1981; 155: 7-20.
28 Marmor L. Hemiarthroplasty for the rheumatoid shoulder.Clin
Orthop 1977; 122: 201-3.
29 Gschwend N. Is a glenoid component necessary for rheuma-toid
patients? Proceedings of 2nd congress of the EuropeanShoulder and
Elbow Society, Berne, Switzerland. 1988.
30 Varian J P W. Interposition silastic cup arthroplasty of
theshoulder. J Bone Joint Surg [Br] 1980; 62: 116-7.
31 Jonsson E, Kelly I G, Rydholm U, Lidgren L. Cuparthroplasty
of the rheumatoid shoulder. Acta OrthopScand 1986; 57: 542-6.
32 Jonsson E. Surgery of the rheumatoid shoulder.
Sweden:University of Lund. 1988. (MD thesis.)
33 Neer C S, Kirby R M. Revision of humeral head and
totalshoulder arthroplasties. Clin Orthop 1982; 170: 189-95.
34 Benjamin A, Hirschowitz D, Arden G P, Blackburn N.Double
osteotomy of the shoulder. In: Bayley I, Kessel L,eds. Shoulder
surgery. Berlin: Springer, 1982: 170-4.
35 Wainwright D. Glenoidectomy-a method of treating thepainful
shoulder in severe rheumatoid arthritis. AnnRhewn Dis 1974; 33:
110.
36 Gariepy R. Glenoidectomy in the repair of the
rheumatoidshoulder. J Bone Joint Surg [Br] 1977; 59: 122.
829
on June 16, 2021 by guest. Protected by copyright.
http://ard.bmj.com
/A
nn Rheum
Dis: first published as 10.1136/ard.49.S
uppl_2.824 on 1 October 1990. D
ownloaded from
http://ard.bmj.com/