Embed Size (px)
Citation preview

Systemic Treatment Options for Untreated Patients WithMetastatic Clear Cell Renal Cancer
Ana M. Molina,a Robert J. Motzer,a and Daniel Y. Hengb
The introduction of therapy targeting vascular endothelial growth factor (VEGF) and the
mammalian target ofwith metastatic renal c
previously untreated ptherapeutic options ar
Semin Oncol 40:436-4
0270-9295/& 2013 Elshttp://dx.do
Conflicts o
aGenitourinDepartmNew Yor
bTom Bake
Address coKetteringUSA. E-
436
rapomycin (mTOR) has significantly improved the outcome of patients
ancer. In this article a comprehensive overview of treatment choices for
atients with metastatic disease is given. Both established and emerginge discussed, as are prognostic factors predicting outcome.
43 & 2013 Elsevier Inc. All rights reserved.
Renal cell carcinoma (RCC) is a malignancy of
the kidney that originates in the proximal
renal tubule and accounts for approximately3% of all cancers. In 2012, an estimated 64,770 new
cases of kidney and renal pelvis cancers are
expected to be diagnosed in the United States withan estimated 13,570 deaths within the same group.1
Surgical resection is the main treatment for tumors
that are confined to the kidney. Approximately 20%–40% of patients with localized disease will eventually
develop local recurrence or distant metastasis after
nephrectomy.2 In addition, about one third ofpatients with RCC have metastatic disease at diag-
nosis. The majority of these patients are candidates
for systemic therapy.Recently, an increased understanding of the
pathogenesis of RCC has led to the development of
novel drugs that target vascular endothelial growthfactor (VEGF) and the mammalian target of rapamy-
cin (mTOR). First-line treatment of metastatic renal
cell carcinoma (mRCC) relies heavily on the use ofsmall molecule targeted inhibitors. Phase III trials of
these agents have demonstrated substantially better
overall efficacy and fewer side effects than previ-ously used cytokines and have assumed a predom-
inant role in the standard management for mRCC.3–9
- see front matterevier Inc. All rights reserved.i.org/10.1053/j.seminoncol.2013.05.013
f interest: none.
ary Oncology Service, Division of Solid Tumor Oncology,ent of Medicine, Memorial Sloan-Kettering Cancer Center,k, NY.r Cancer Center, Calgary, AB, Canada.
rrespondence to Ana M. Molina, MD, Memorial Sloan-Cancer Center, 1275 York Ave, New York, NY 10021,
mail: [email protected]
Semin
Patients with advanced RCC present with a wide
spectrum of disease varying from asymptomatic or
indolent disease to symptomatic or rapidly progres-sive disease. Several prognostic factors identified
have led to the development of risk factor models
that have proven to be instrumental in the designand interpretation of clinical trials and risk-directed
therapy. Herein we review prognostic factors, clin-
ical data for established first-line therapies, andemerging first-line therapy for advanced RCC.
PROGNOSTIC FACTORS
Prognostic factors are important for the purposes
of clinical trial design, risk-directed therapy, and
patient counseling. They can be divided into patientfactors, tumor burden, inflammatory markers, and
treatment factors. Many of these factors have been
combined into multivariable models to assist theclinician in patient prognostication.10
Patient factors include symptoms such as night
sweats and weight loss, Karnofsky performance status(KPS), and Eastern Cooperative Oncology (ECOG)
performance status. A reflection of higher tumor
burden includes the presence of anemia, an elevatedlactate dehydrogenase (LDH) level, hypercalcemia,
elevated alkaline phosphatase, and the sites and num-
ber of sites of metastatic disease. Additionally, a shorterdisease-free interval or shorter time from diagnosis to
treatment indicates more aggressive disease while
longer ones depict more indolent disease. Inflamma-tory markers include and elevated erythrocyte sedi-
mentation rate (ESR), C-reactive protein (CRP),
neutrophilia, and thrombocytosis, which are all asso-ciated with poorer overall survival. Finally, treatment
factors, including a prior cytoreductive nephrectomy,
tend to be associated with a better prognosis.11
ars in Oncology, Vol 40, No 4, August 2013, pp 436-443
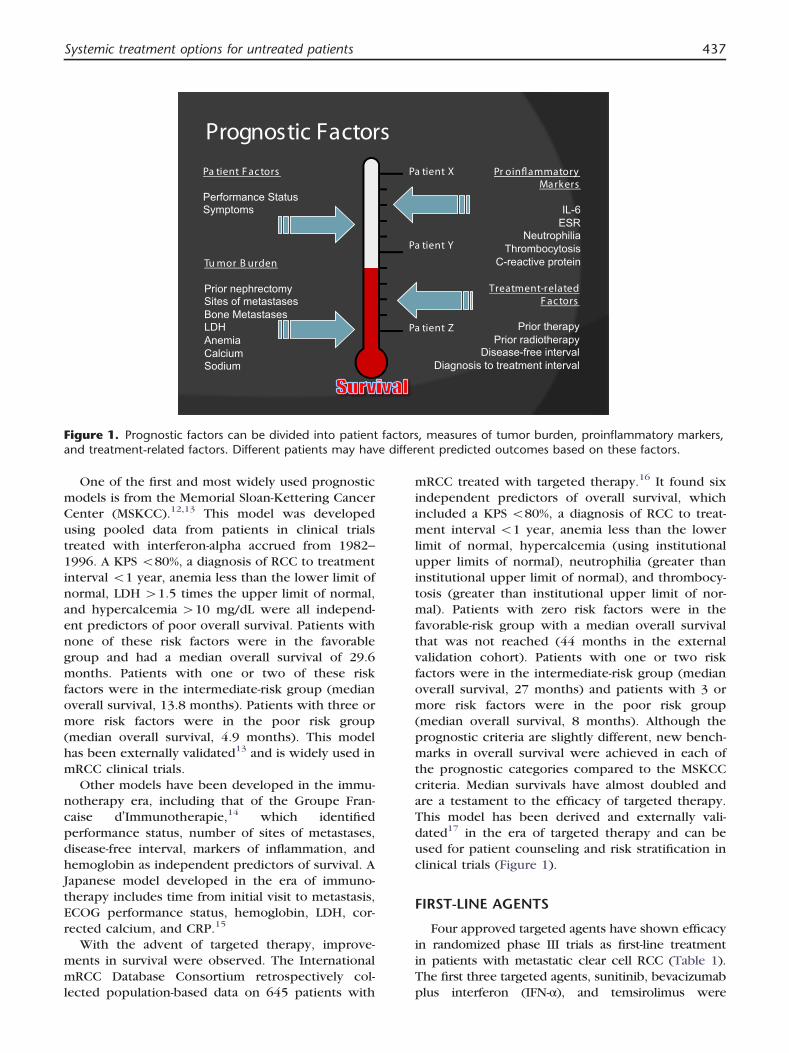
Figure 1. Prognostic factors can be divided into patient factors, measures of tumor burden, proinflammatory markers,and treatment-related factors. Different patients may have different predicted outcomes based on these factors.
Systemic treatment options for untreated patients 437
One of the first and most widely used prognostic
models is from the Memorial Sloan-Kettering CancerCenter (MSKCC).12,13 This model was developed
using pooled data from patients in clinical trials
treated with interferon-alpha accrued from 1982–1996. A KPS o80%, a diagnosis of RCC to treatment
interval o1 year, anemia less than the lower limit of
normal, LDH 41.5 times the upper limit of normal,and hypercalcemia 410 mg/dL were all independ-
ent predictors of poor overall survival. Patients with
none of these risk factors were in the favorablegroup and had a median overall survival of 29.6
months. Patients with one or two of these risk
factors were in the intermediate-risk group (medianoverall survival, 13.8 months). Patients with three or
more risk factors were in the poor risk group
(median overall survival, 4.9 months). This modelhas been externally validated13 and is widely used in
mRCC clinical trials.
Other models have been developed in the immu-notherapy era, including that of the Groupe Fran-
caise d’Immunotherapie,14 which identified
performance status, number of sites of metastases,disease-free interval, markers of inflammation, and
hemoglobin as independent predictors of survival. A
Japanese model developed in the era of immuno-therapy includes time from initial visit to metastasis,
ECOG performance status, hemoglobin, LDH, cor-
rected calcium, and CRP.15
With the advent of targeted therapy, improve-
ments in survival were observed. The International
mRCC Database Consortium retrospectively col-lected population-based data on 645 patients with
mRCC treated with targeted therapy.16 It found six
independent predictors of overall survival, whichincluded a KPS o80%, a diagnosis of RCC to treat-
ment interval o1 year, anemia less than the lower
limit of normal, hypercalcemia (using institutionalupper limits of normal), neutrophilia (greater than
institutional upper limit of normal), and thrombocy-
tosis (greater than institutional upper limit of nor-mal). Patients with zero risk factors were in the
favorable-risk group with a median overall survival
that was not reached (44 months in the externalvalidation cohort). Patients with one or two risk
factors were in the intermediate-risk group (median
overall survival, 27 months) and patients with 3 ormore risk factors were in the poor risk group
(median overall survival, 8 months). Although the
prognostic criteria are slightly different, new bench-marks in overall survival were achieved in each of
the prognostic categories compared to the MSKCC
criteria. Median survivals have almost doubled andare a testament to the efficacy of targeted therapy.
This model has been derived and externally vali-
dated17 in the era of targeted therapy and can beused for patient counseling and risk stratification in
clinical trials (Figure 1).
FIRST-LINE AGENTS
Four approved targeted agents have shown efficacyin randomized phase III trials as first-line treatment
in patients with metastatic clear cell RCC (Table 1).
The first three targeted agents, sunitinib, bevacizumabplus interferon (IFN-α), and temsirolimus were

A.M. Molina, R.J. Motzer, and D.Y. Heng438
compared as first-line therapy with IFN-α in separate
studies.6–8,11,12 Each of these agents was found to besuperior to IFN-α in prolonging progression-free sur-
vival (PFS), overall survival, or both. The fourth agent,
pazopanib was shown to have superior efficacy to thatof placebo in a phase III randomized controlled trial
that treated approximately one half treatment naı̈ve-
patients and one half cytokine-pretreated patients.9
In addition, the toxicity profile of these agents
varies with unique class drug effects (Table 2).
Sunitinib
Sunitinib is an oral multi-kinase inhibitor targetingseveral receptor tyrosine kinases (RTKs). In the
pivotal phase III trial of first-line treatment, 750
patients with clear cell mRCC were randomized tosunitinib (50 mg daily orally, 4 weeks on and 2 weeks
off) versus IFN-α (9 million units given subcutane-
ously three times weekly).3 The majority of thepatients treated with sunitinib (94%) and IFN-α(93%) had favorable or intermediate risk factors.3
The primary endpoint was PFS as assessed by inde-pendent, central review of radiographs. The secon-
dary endpoints were objective response rate, overall
survival, patient-reported outcomes, and safety. PFS asassessed by independent review was statistically
significant in favor of sunitinib (11 v 5 months,
≥.001).3 This benefit of sunitinib was observedacross all subgroups of patients; favorable (14.5 v7.9 months), intermediate (10.6 v 3.8 months), and
poor (3.7 v 1.2 months) risk groups. Treatment withsunitinib was also associated with a higher objective
response rate compared with the IFN-α group (31% v6%, respectively, P o.001). In the final analysis of thistrial, median overall survival was prolonged in the
sunitinib arm compared with the IFN-α arm (26.4 v21.8 months, P ¼ .051).4
Table 1. Randomized Phase III Trials of TargetedRenal Cell Carcinoma
Study n ORR %
Sunitinib v IFN-α3 750 47 v 12Bevacizumab þ IFN-α v IFN-α8 649 31 v 12Bevacizumab þ IFN-α v IFN-α7 732 25.5 v 13.1Pazopanib v placebo9 233 30 v 3* 11Temsirolimus v IFN-α6 626 8.6 v 4.8Pazopanib v sunitinib23 1110 31 v 25 8Tivozanib v sorafenib25 517 33 v 23t
Abbreviations: IFN-α, interferon-alfa; ORR, objective response rate; Pratio; NA, not available.
⁎ Treatment-naïve or cytokine-refractory mRCC.t Treatment-naïve or one prior systemic therapy for mRCC.
Hypertension, vomiting, hand-foot sydrome, and
diarrhea were observed with sunitinib treatment.Health-related quality of life as reported by patients
in post-baseline assessments was significantly better
in the sunitinib group.Furthermore, the activity and safety of sunitinib
was assessed in the expanded-access trial that pro-
vided sunitinib on a compassionate-use basis toclinical trial-ineligible patients with RCC from coun-
tries where regulatory approval had not been
granted.18 In this study, 4,564 previously treatedand untreated patients received open-label sunitinib
50 mg orally daily (4 weeks on treatment, 2 weeks
off). The patient population included 321 (7%)patients with brain metastases, 582 (13%) with
ECOG performance status of 2 or higher, 588
(13%) non-clear cell histology, and 1,418 (32%) aged65 years or greater. The objective response rate for
3,464 evaluable patients was 17% (n ¼ 603). Sub-
group overall response rates were as follows: brainmetastases (26 of 213 [12%]), ECOG performance
status 2 or higher (29 of 319 [9%]), non-clear cell
RCC (48 of 437 [11%]), and age 65 years or greater(176 of 1,056 [17%]). The median PFS was 10.9
months (95% confidence interval [CI], 10.3–11.2)and overall survival was 18.4 months (17.4–19.2).Median PFS by MSKCC risk group was 14.6 months
(95% CI, 13.8–15.6) in the favorable-risk group (n ¼1,928), 8.5 months (8.1–9.2) in the intermediate-riskgroup (n ¼ 1,928), and 4.1 months (3.1–5.0) in
the poor-risk group (n ¼ 373).18 Median overall
survival times in the favorable-, intermediate-, andpoor-risk groups were 24.7 months (23.5–NA), 14.4months (13.3–15.1), and 5.3 months (4.6–6.4),respectively.18
Sunitinib was found to be safe in this broad
population of patients and treatment-related adverse
events were manageable. Diarrhea (n ¼ 1,936 [44%])
Agents for First-Line Treatment of Metastatic
Median PFS (mo) Final Median OS (mo)
11 v 5 P o.001 26.4 v 21.8 P ¼ .05110.4 v 5.5 P o.0001 23.3 v 21.3 P ¼ .12918.4 v 4.9 P o.0001 18.3 v 17.4 P ¼ .069.1 v 2.8 P o.0000001 NA5.5 v 3.1 P o.001 10.9 v 7.3 P ¼ .0069.4 v 9.5 HR ¼ 1.0466 28.4 v 29.3 P ¼ .27511.9 v 9.1 P ¼ .042 NAFS, progression-free survival; OS, overall survival; HR, hazard

Table 2. Selected Serious Adverse Events (Grade 3/4) by Targeted Agent
Adverse Event (%) Sunitinib4 Bevacizumab þ IFN-α8 Temsirolimus6 Pazopanib9
Anorexia 2 3 3 2Asthenia 2 10 11 3Diarrhea 9 2 1 4Dyspnea 2 o1 9 –
Nausea 5 – 2 o1Vomiting 4 – 2 2Fatigue 11 12 – 2Hand-foot syndrome 9 – – –
Hyperglycemia – – 11 –
Hypertension 12 3 – 4Anemia 8 3 20 –
Neutropenia 18 4 3 1Thrombocytopenia 9 2 1 –
Leukopenia 8 – 1 –
Discontinuations due to adverse events 19 28 7 NRAbbreviation: AE, adverse event; NR, not reported.
Systemic treatment options for untreated patients 439
and fatigue (n ¼ 1,606 [37%]) were the most
common treatment-related adverse events. Fatigue(n ¼ 344 [8%]) and thrombocytopenia (n ¼ 338
[8%]) were the most common grade 3/4 adverse
events.Sunitinib was approved by the US Food and Drug
Administration (FDA) in 2006 and became a standard
first-line therapy for patients with advanced RCC,particularly those in the favorable- and intermediate-
risk groups. The expanded access trial has provided
further data to support the use of sunitinib in a broadpopulation of patients who generally have a poor
prognosis.
Bevacizumab
Bevacizumab is a recombinant humanized mono-clonal IgG1 antibody that selectively binds to and
inhibits the biologic activity of human VEGF. The
efficacy of bevacizumab in combination with IFN-αwas established by two pivotal phase III trials.7,8 The
AVOREN phase III study, randomized 649 patients
with untreated metastatic RCC to bevacizumab (10mg/kg administered intravenously every 2 weeks)
plus IFN-α (9 million units subcutaneously 3 times
per week) versus IFN-α plus placebo.8 Patients hadpredominantly (450%) clear cell RCC and the
majority (480%) had favorable or intermediate risk
factors. The primary endpoint was overall survival;secondary endpoints included PFS and safety. There
was a statistically significant difference in the median
PFS in favor of bevacizumab plus IFN-α (10.2 v5.4 months, P ¼ .0001). Subgroup analysis suggested
improved PFS in all MSKCC risk groups treated with
the combination of bevacizumab plus IFN-α.Improvements in PFS were seen in the favorable-
prognosis group (n ¼ 180; median PFS, 12.9 v7.6 months) and in the intermediate-prognosis group(n ¼ 363; median PFS, 10.2 v 4.5 months). A
significant improvement in PFS was not observed
in the poor-prognosis group (n ¼ 54; median PFS,2.2 v 2.1 months). The final analysis of overall
survival, although not statistically significant,
showed an improvement with the combination(23.3 v 21.3 months, P ¼ .3360, unstratified).19
The most commonly reported grade 3 or worse
adverse events in both the combination versus IFN-αgroups were established interferon-related toxicities
(fatigue, 12% v 8%; asthenia, 10% v 7%; and neu-
tropenia, 4 v 2%). The incidence of grade 3/4adverse events in patients treated with bevacizumab
was low, and included hypertension (3%), gastro-
intestinal perforations (1%; three grade 4) and arte-rial/venous thromboembolic events (3%, four
grade 4).
The second phase III trial, Cancer and LeukemiaGroup B (CALGB) 90206, randomized 732 previ-
ously untreated patients with metastatic clear cell
RCC to bevacizumab plus IFN-α versus IFN-α alone atthe same doses described for the AVOREN trial.7 The
majority of the patients (90%) had favorable- or
intermediate-risk factors. The primary endpoint wasoverall survival. The secondary endpoints included
PFS, objective response rate, and safety. There was a
statistically significant difference in median PFS infavor of the combination arm (8.5 v 5.2 months,

A.M. Molina, R.J. Motzer, and D.Y. Heng440
P o.0001). In an exploratory subset analysis by
MSKCC risk status, the PFS data was also confirmed.The median PFS in the favorable risk group was 11.1
versus 5.7 months and 8.4 versus 5.3 months in the
intermediate-risk group. Additionally, higher objec-tive response rates were seen in the combination
group (25.5% v 13.2%, P o.0001). Similarly to the
AVOREN study, overall survival favored the combi-nation arm but did not meet the predefined criteria
for significance.20
Bevacizumab plus IFN-α resulted in significantlymore grade 3 toxicities, including hypertension (9%
v 0%), anorexia (17% v 8%), fatigue (35% v 28%), and
proteinuria (13% v 0%). The incidence of grade4 toxicities was low in each arm.
Based on the results of these two phase III studies,
the combination of bevacizumab plus IFN-α wasapproved for the treatment of patients with
advanced or metastatic RCC by the European Med-
icines Agency in 2007 and the FDA in 2009.Furthermore, combinations of bevacizumab with
other targeted agents have been of great interest.
The phase III INTORACT trial recently reportedcompared the combination of bevacizumab plus
temsirolimus versus bevacizumab plus IFN-α as
first-line treatment in 791 patients with predomi-nantly clear cell mRCC.21 The majority of the
patients treated (490%) had favorable- or
intermediate-risk factors. The primary endpoint wasPFS and there was no advantage to the addition of
temsirolimus over IFN-α. The median PFS with the
temsirolimus combination was 9.1 months versus9.3 months with the IFN-α combination. Based on
these results, the combination of bevacizumab plus
IFN-α remains a recommended option for first-linetreatment of patients with advanced RCC with good-
or intermediate-risk factors.
Temsirolimus
Temsirolimus is a mTOR kinase inhibitor. Efficacywas established based on the Global Advanced Renal
Cell Carcinoma (ARCC) trial that randomized 626
previously untreated patients with mRCC to receive25 mg of intravenous temsirolimus weekly, 3 million
units of IFN-α (with an increase to 18 million units)
subcutaneously three times weekly, or combinationtherapy with 15 mg temsirolimus weekly plus 6 mil-
lion units of IFN-α three times weekly.6 Eighty
percent of patients had clear cell histology and themajority of patients (74%) had poor-risk factors.
Poor-risk eligibility for the trial, defined as exhibiting
three or more of six risk criteria predictive of shortsurvival, was based on expanded MSKCC criteria.22
The primary endpoint was overall survival and there
was a statistically significant difference in favor oftemsirolimus. The median overall survival for
patients who received temsirolimus alone was 10.9
months compared with 7.3 months in the IFN-αgroup, and 8.4 months in the combination group.
Overall survival did not differ significantly in the
combination group versus the IFN-α monotherapygroup. However, compared to treatment with IFN-αalone, temsirolimus monotherapy was associated
with a significant prolongation of survival (hazardratio, 0.73; 95% CI, 0.58–0.92; P ¼ .008). PFS was
significantly longer in patients receiving temsiroli-
mus, with median PFS times of 1.9, 3.8, and3.7 months for the IFN-α, temsirolimus, and the
combination group, respectively (P o.001). The
proportion of patients with stable disease for at least6 months or an objective response was significantly
greater in the temsirolimus group (32.1%) and in
the combination therapy group (28.1%) than in theIFN-α group (15.5%; P o.001 and P ¼ .002, re-
spectively).
Common adverse events in the temsirolimus andcombination therapy groups included hyperglyce-
mia, hypercholesterolemia, and hyperlipidemia,
reflecting inhibition of mTOR-regulated glucose andlipid metabolism. Additionally, mild to moderate
rash, peripheral edema, and stomatitis affected more
patients who received temsirolimus, either alone orin combination with IFN-α. Asthenia was most
common in the two groups receiving IFN-α mono-
therapy or in combination. Overall, fewer grade 3/4adverse events occurred in patients treated with
temsirolimus (67%), as compared with 78% of
patients in the IFN-α group (P ¼ .02) and 87% ofpatients in the combination group (P ¼ .02).
Based on these results, temsirolimus was
approved by the FDA in 2007 for the treatment ofadvanced RCC and is most commonly used to treat
patients with poor-risk disease.
Pazopanib
Pazopanib is an oral multi-kinase inhibitor targetingvascular endothelial growth factor receptor (VEGFR),
platelet-derived growth factor receptor (PDGFR), and
stem cell receptor factor (c-KIT) approved by the FDAfor the treatment of advanced RCC in 2009. A
placebo-controlled, randomized, double-blind, phase
III trial evaluated the efficacy and safety of pazopanibmonotherapy. Patients received pazopanib 800 mg
orally daily or a matching placebo in a 2:1 ratio.9 The
study enrolled 435 patients with advanced RCC, 233were treatment-naı̈ve (54%), and 202 had prior cyto-
kine treatment (46%). The majority of the patients
(490%) had favorable or intermediate MSKCC riskfactors. The primary endpoint was PFS and there was
a statistically significant difference in favor of pazopa-
nib in the overall population (9.2 v 4.2 months;P o.0001), the treatment naı̈ve-subpopulation (11.1

Systemic treatment options for untreated patients 441
v 2.8 months; P o.0001), and the cytokine-pretreated
subpopulation (7.4 v 4.2 months; P o.001). Theobjective response rate was 30% with pazopanib
compared with 3% with placebo (P o.001).
Pazopanib was well tolerated and the most com-mon adverse events included diarrhea (52%), hyper-
tension (40%), hair color changes (38%), nausea
(26%), anorexia (22%), and vomiting (21%). Themost common grade 3/4 adverse events in the
pazopanib arm were hypertension (4%) and diarrhea
(4%). ALT and AST elevations were the most com-mon clinical laboratory abnormalities observed in
the pazopanib arm. In general, most adverse events
and clinical abnormalities were grade 1/2.More recently, results of the COMPARZ study, a
randomized open-label phase III trial of pazopanib
versus sunitinib in first-line treatment of patientswith mRCC, were reported at the 2012 European
Society for Medical Oncology meeting.23 The study
enrolled 1,110 previously untreated patients withmRCC to receive pazopanib 800 mg orally daily (n ¼557) or sunitinib 50 mg orally daily, 4 weeks on and
2 weeks off (n ¼ 553).Patients had clear cell RCC and the majority of the
patients (≥85%) had favorable or intermediate
MSKCC risk factors. Pazopanib demonstrated non-inferiority compared to sunitinib for PFS (8.4 v9.5 months; hazard ratio, 1.04, independent review).
Objective response rates were similar in the pazopa-nib and sunitinib treatment groups (31% v 25%,
respectively). Overall survival at interim analysis was
also similar in the pazopanib and sunitinib treatmentgroups (28.4 v 29.3 months, respectively), further
supporting the efficacy of pazopanib.
Pazopanib was found to have a different safetyprofile with a lower incidence of hand-foot syn-
drome (29% v 50%), fatigue (55% v 63%), and
mucositis (11% v 26%). There was a higher inci-dence of liver function abnormalities in the pazopa-
nib treatment group. In addition, quality-of-life
assessments favored pazopanib over sunitinib.Another randomized, double-blind, placebo-
controlled crossover study evaluated patient prefer-
ence between pazopanib and sunitinib in untreatedpatients with mRCC (PISCES study).24 One hundred
sixty-eight patients were randomized 1:1 to receive
as first-line treatment pazopanib 800 mg orally dailyfor 10 weeks followed by a 2-week washout and
then sunitinib 50 mg orally daily (4/2 weeks sched-
ule) for 10 weeks or vice versa. The primaryendpoint of patient preference was assessed at 22
weeks and demonstrated better tolerability of pazo-
panib compared to sunitinib. The most commonreasons for pazopanib preference included better
quality of life and less fatigue. Health-related quality
of life statistically favored pazopanib for fatigue,foot/hand soreness, and mouth/throat soreness.
Both pazopanib and sunitinib are valid first-line
treatment options for patients with mRCC. How-ever, the studies cited above suggest that pazopanib
may have a better safety profile and may be associ-
ated with better quality of life.
EMERGING NEW FIRST-LINE AGENTS
Tivozanib is a potent and selective VEGFR antag-
onist. In the TIVO-1 trial, patients with clear cell
mRCC who had a prior nephrectomy were random-ized to tivozanib (1.5 mg daily, 3 weeks on and
1 week off) versus sorafenib (400 mg twice daily).25
Patients could have been treated with prior immu-notherapy but previous VEGF or mTOR inhibitors
were not allowed. The primary endpoint was PFS
and there was a statistically significant difference infavor of tivozanib (11.9 v 9.1 months, P ¼ .042).
Tivozanib was well tolerated with numerically less
hand-foot syndrome (all-grade toxicity, 13% v 54%)and diarrhea (22% v 32%), but there was a higher
incidence of hypertension (44% v 34%) and dyspho-
nia (21% v 5%). Tivozanib has not been compared tothe other anti-VEGF inhibitors that are commonly
used in the first-line setting, such as pazopanib and
sunitinib.Axitinib is a highly potent VEGFR antagonist that
has been FDA-approved and is usually reserved for
patients with mRCC who have progressed on theirfirst anti-VEGF therapy. In a randomized phase II trial
to assess the importance of dose escalation, patients
with treatment-naı̈ve mRCC were treated with axiti-nib at the dose of 5 mg twice daily. Those patients
that developed side effects were maintained on the
same dose and achieved an impressive median PFSof 16.4 months and an overall response rate of
59%. Those patients that did not develop side
effects were randomized to dose escalation versusno dose escalation. The results for the individual
randomized arms of the study have not yet been
reported; however, when the entire cohort ofrandomized patients that did not develop side
effects was examined, a median PFS of 14.5
months and an overall response rate of 43% wereobserved.
These outcomes may appear to be better than
historical controls using other targeted therapies;however, patient selection bias may account in part
for these excellent outcomes. Thus, the use of
axitinib in the first-line setting requires further studyperhaps in a randomized trial compared to existing
first-line standards of care.
The axitinib phase II trial results suggest thatpatients that develop toxicities such as hypertension
tend to be associated with improved outcomes. For
example, patients that had a diastolic blood pressure≥90 mm Hg versus those who had o90 mm Hg on

Table 3. First-Line Treatment Nomogram in Patients With mRCC
Treatment Options
Patient Group Level 1a ≥ Level 2*
Good or intermediate risk Sunitinib Bevacizumab þ IFN High-dose IL-2
Poor riskPazopanib SorafenibTemsirolimus Sunitinib
Abbreviations: mRCC, metastatic renal cell carcinoma; IFN, interferon; IL-2, interleukin-2.⁎ Levels described at: http://www.ncbi.nlm.nih.gov/books/bv.fcgi?rid=hstat3.section.17745#17746.a Adapted from AM Molina, 2008, with permission.26
A.M. Molina, R.J. Motzer, and D.Y. Heng442
cycle 1 day 15 of the study had a median PFS and
overall response rate of 22.5 months versus 13.7
months and 65% and 50%, respectively.
CONCLUSION
VEGF and mTOR-targeted therapies have im-
proved patient outcomes and are the mainstay of
treatment for mRCC. Risk-derived models have beenincorporated into clinical trial design and conduct,
assisting clinicians with patient prognostication and
risk-directed therapy. Treatment paradigms andclinical practice recommendations are classified by
line of therapy, risk score, and level of evidence
(Table 3).Emerging TKIs, tivozanib and axitinib, provide
increased target specificity and may have less off-
target adverse event effects. These newer agentshave the potential to improve our ability to treat
patients with mRCC by allowing long-term tolerance
to treatment and improving overall quality of life.
REFERENCES1. Siegel R, Naishadham D, Jemal A. Cancer statistics,
2012. CA Cancer J Clin. 2012;62(1):10–29.
2. Janzen NK, Kim HL, Figlin RA, Belldegrun AS. Surveil-
lance after radical or partial nephrectomy for localized
renal cell carcinoma and management of recurrent
disease. Urol Clin North Am. 2003;30(4):843–52.
3. Motzer RJ, Hutson TE, Tomczak P, et al. Sunitinib
versus interferon alfa in metastatic renal-cell carci-
noma. N Engl J Med. 2007;356(2):115–24.
4. Motzer RJ, Hutson TE, Tomczak P, et al. Overall
survival and updated results for sunitinib compared
with interferon alfa in patients with metastatic renal
cell carcinoma. J Clin Oncol. 2009;27(22):3584–90.
5. Motzer RJ, Escudier B, Oudard S, et al. Efficacy of
everolimus in advanced renal cell carcinoma: a double-
blind, randomised, placebo-controlled phase III trial.
Lancet. 2008;372(9637):449–56.
6. Hudes G, Carducci M, Tomczak P, et al. Temsirolimus,
interferon alfa, or both for advanced renal-cell carci-
noma. N Engl J Med. 2007;356(22):2271–81.
7. Rini BI, Halabi S, Rosenberg JE, et al. Bevacizumab plus
interferon alfa compared with interferon alfa mono-
therapy in patients with metastatic renal cell carci-
noma: CALGB 90206. J Clin Oncol. 2008;26:5422–8.
8. Escudier B, Pluzanska A, Koralewski P, et al. Bevaci-
zumab plus interferon alfa-2a for treatment of meta-
static renal-cell carcinoma: a randomised, double-blind
phase III trial. Lancet. 2007;370:2103–11.
9. Sternberg CN, Davis ID, Mardiak J, et al. Pazopanib in
locally advanced or metastatic renal cell carcinoma:
results of a randomized phase III trial. J Clin Oncol.
2010;28(6):1061–8.
10. Tang PA, Vickers MM, Heng DY. Clinical and molec-
ular prognostic factors in renal cell carcinoma: what
we know so far. Hematol Oncol Clin North Am.
2011;25(4):871–91.
11. Flanigan RC, Mickisch G, Sylvester R, Tangen C, Van
Poppel H, Crawford ED. Cytoreductive nephrectomy
in patients with metastatic renal cancer: a combined
analysis. J Urol. 2004;171(3):1071–6.
12. Motzer RJ, Bacik J, Murphy BA, Russo P, Mazumdar M.
Interferon-alfa as a comparative treatment for clinical
trials of new therapies against advanced renal cell
carcinoma. J Clin Oncol. 2002;20(1):289–96.
13. Mekhail TM, Abou-Jawde RM, Boumerhi G, et al.
Validation and extension of the Memorial Sloan-
Kettering prognostic factors model for survival in
patients with previously untreated metastatic renal
cell carcinoma. J Clin Oncol. 2005;23(4):832–41.
14. Negrier S, Escudier B, Gomez F, et al. Prognostic
facotrs of survival and rapid progression in 782
patients with metastatic renal carcinomas treated by
cytokines: a report from the Groupe Francais d'Immu-
notherapie. Ann Oncol. 2002;13:1460–8.
15. Naito S, Yamamoto N, Takayama T, et al. Prognosis of
Japanese metastatic renal cell carcinoma patients in
the cytokine era: a cooperative group report of 1463
patients. Eur Urol. 2010;57(2):317–25.
16. Heng DY, Xie W, Regan MM, et al. Prognostic factors
for overall survival in patients with metastatic renal
cell carcinoma treated with vascular endothelial
growth factor-targeted agents: results from a large,
multicenter study. J Clin Oncol. 2009;27(34):5794–9.
17. Heng DY, Xie W, Regan MM, et al. External validation
and comparison with other models of the International
Metastatic Renal-Cell Carcinoma Database Consortium
Systemic treatment options for untreated patients 443
prognostic model: a population-based study. Lancet
Oncol. Jan 8, 2013.
18. Gore ME, Szczylik C, Porta C, et al. Safety and efficacy
of sunitinib for metastatic renal-cell carcinoma:
an expanded-access trial. Lancet Oncol. 2009;10(8):
757–63.
19. Escudier B, Bellmunt J, Negrier S, et al. Phase III trial of
bevacizumab plus interferon alfa-2a in patients with
metastatic renal cell carcinoma (AVOREN): final anal-
ysis of overall survival. J Clin Oncol. 2010;28(13):
2144–2150.
20. Rini BI, Halabi S, Rosenberg JE, et al. Phase III trial of
bevacizumab plus interferon alfa versus interferon alfa
monotherapy in patients with metastatic renal cell
carcinoma: final results of CALGB 90206. J Clin Oncol.
2010;28(13):2137–43.
21. Rini BI, Bellmunt J, Clancy J, Wang K, Niethammer A,
Escudier B. Randomized phase IIIB trial of temsiroli-
mus and bevacizumab versus interferon and bevacizu-
mab in metastatic renal cell carcinoma: results
from INTORACT. 37th Congress of the European
Society for Medical Oncology. 2012. Ann Oncol.
2012;23(suppl 9).
22. Motzer RJ, Bacik J, Murphy BA, Russo P, Mazumdar M.
Interferon-alfa as a comparative treatment for clinical
trials of new therapies against advanced renal cell
carcinoma. J Clin Oncol. 2002:289–96.
23. Motzer RH, Hutson TE, Reeves J, et al. Randomized,
open label, phase III trial of pazopanib versus
sunitinib in first-line treatment of patients with meta-
static renal cell carcinoma (mRCC): results of the
COMPARZ trial. 37th Congress of the European
Society for Medical Oncology. 2012. Ann Oncol.
2012;23(suppl 9).
24. Escudier BJ, Porta C, Bono P, et al. Patient preference
between pazopanib (Paz) and sunitinib (Sun): Results
of a randomized double-blind, placebo-controlled,
cross-over study in paitents with metastatic renal cell
carcinoma (mRCC)—PISCES study. NCT 01064310.
J Clin Oncol. 2012;30(suppl abstr CRA4502).
25. Motzer RJ, Nosov D, Eisen T, et al. Tivozanib versus
sorefenib as initial targeted therapy for patients with
advanced renal cell carcinoma: Results from a phase III
randomized, open-label, multicenter trial. J Clin Oncol.
2012;30(suppl abstr 4501).
26. Molina AM, Motzer RJ. Current algorithms and prog-
nostic factors in the treatment of metastatic renal cell
carcinoma. Clin Genitourinary Cancer. Dec 2008;6
suppl 1:S7-13.