Embed Size (px)
Citation preview

Takayasu arteritis – Takayasu arteritis – current issuescurrent issues
P.Nagaraj kumarP.Nagaraj kumar

DefinitionDefinition
An idiopathic inflammatory disease of An idiopathic inflammatory disease of
the large elastic arteries occurring in the large elastic arteries occurring in
the young and resulting in occlusive or the young and resulting in occlusive or
ectatic changes mainly in the aorta ectatic changes mainly in the aorta
and its immediate branches as well as and its immediate branches as well as
the pulmonary artery and its branches. the pulmonary artery and its branches.

SynonymsSynonyms• Takayasu’s ArteritisTakayasu’s Arteritis
• AortoarteritisAortoarteritis
• Pulseless DiseasePulseless Disease
• Young female ArteritisYoung female Arteritis
• Occlusive thromboaortopathyOcclusive thromboaortopathy
• Aortic arch syndromeAortic arch syndrome
• Reverse CoarctationReverse Coarctation
• Martorell’s syndromeMartorell’s syndrome
• Dhanraj’s diseaseDhanraj’s disease

HistoryHistory
• 1761- Morgagni- 1761- Morgagni- Reported first Case Reported first Case • 1856- Savory - reported a case 1856- Savory - reported a case • 1908- Takayasu, professor of ophthalmology - 1908- Takayasu, professor of ophthalmology -
21 yrs woman with characteristic fundal 21 yrs woman with characteristic fundal arterio- venous anastomoses and arterio- venous anastomoses and
absent absent radial pulse radial pulse• 1921- SHIKARE- first case report in india 1921- SHIKARE- first case report in india
• 1951- Shimizu and Sano- Pulseless Disease 1951- Shimizu and Sano- Pulseless Disease • 1962 & 1971 –1962 & 1971 –SenSen – Middle Aortic Syndrome – Middle Aortic Syndrome
and association with TB in 101cases.and association with TB in 101cases.• 1993- 1993- Chappel HillChappel Hill - Takayasu Arteritis as - Takayasu Arteritis as
granulomatous inflammations of Aorta granulomatous inflammations of Aorta and its major branches. and its major branches.

EPIDEMIOLOGYEPIDEMIOLOGY• Predominantly a disease of young females in their Predominantly a disease of young females in their
2 2ndnd or 3 or 3rdrd decades. decades. Less than 40 yrs – obligatory crtiteriaLess than 40 yrs – obligatory crtiteria
Childhood onset is not rare. Childhood onset is not rare. Mean age European study- 41yrs, Japan-29yrs Mean age European study- 41yrs, Japan-29yrs India –age of onset mean -24yrs, Age at India –age of onset mean -24yrs, Age at ΔΔ -28 -28
yrsyrs• Sex: Sex: FF>>MM• Geographical variation : Japan - 8:1, Israel - 1.2:1, Geographical variation : Japan - 8:1, Israel - 1.2:1,
Mexico - 5:1, India - 4 : 1 (recently,panja et al - Mexico - 5:1, India - 4 : 1 (recently,panja et al - 6.4:1) 6.4:1)
• Geographical variation :Japan-proximal AortaGeographical variation :Japan-proximal Aorta(Aortic Site) SE Asia-Middle Aortic (Aortic Site) SE Asia-Middle Aortic
syndromesyndrome North Europeans: North Europeans:
patchy .,assoc. patchy .,assoc. RArthritis,SLE RArthritis,SLE• Incidence & prevalence : most commonly seen in Incidence & prevalence : most commonly seen in
Japan, South East Asia, India, and Mexico.Japan, South East Asia, India, and Mexico. Hospital based studies- 0.8 -2.6per million.Hospital based studies- 0.8 -2.6per million.

EPIDEMIOLOGYEPIDEMIOLOGYGEOGRAPHICAL:GEOGRAPHICAL:

ETIOPATHOGENESISETIOPATHOGENESIS
GeneticGenetic::
India HLA B5, B21 (kumar et al) India HLA B5, B21 (kumar et al)
USA HLADR4, MB3USA HLADR4, MB3
Japan HLADR2, MB1, Bw52, DW2, DQW1 Japan HLADR2, MB1, Bw52, DW2, DQW1
HLA Bw52-IHD,AR,Pul involvement HLA Bw52-IHD,AR,Pul involvement
HLA B39-Renal artery stenosis HLA B39-Renal artery stenosis
AutoimmunityAutoimmunity: :
immune reaction against elastin immune reaction against elastin
circulating gammaglobulins (circulating gammaglobulins (alpha1& alpha1& globulins,IgG, globulins,IgG, IgA, IgM, IgA, IgM, CMI, ANA, Anti - CMI, ANA, Anti - Aorta Ab (AA), Anti - Aorta Ab (AA), Anti - endothelial cell Ab) endothelial cell Ab) , , raised ESR, leucocytosis, raised ESR, leucocytosis, arthralgia and high arthralgia and high titers of anti-aorta antibodies titers of anti-aorta antibodies
Cell mediated immunityCell mediated immunity

Rheumatic :Rheumatic :
(Upmark 1954) some pts had raised (Upmark 1954) some pts had raised ASO titreASO titre
Female predilectionFemale predilection : :
Urinary estrogens elevated. Estradiol and Urinary estrogens elevated. Estradiol and progesterone, but not testosterones, enhance progesterone, but not testosterones, enhance leucocyte adhesion to endothelial cells in the leucocyte adhesion to endothelial cells in the presence of TNF. presence of TNF.
?Infection?Infection: :
hypersensitivity to Mycobacterium tuberculosishypersensitivity to Mycobacterium tuberculosis

Tuberculosis and TATuberculosis and TA• Lupi-Herrera et al. Lupi-Herrera et al.
previous tuberculosis in 48% of Japanese patients previous tuberculosis in 48% of Japanese patients • Sen et al. Sen et al.
tuberculosis in 71% patients in India tuberculosis in 71% patients in India • Pantell and Goodman 1961 to 1981 Pantell and Goodman 1961 to 1981
tuberculin test positive in 73.3% – 100% of cases tuberculin test positive in 73.3% – 100% of cases active tuberculosis in 0.26% – 4.2% of the cases.active tuberculosis in 0.26% – 4.2% of the cases.
• Heightened response to tubercular antigens especially Heightened response to tubercular antigens especially the 65 kDa the 65 kDa
HSP HSP • Tubercular aortitis lesions- discrete, aneurysm Tubercular aortitis lesions- discrete, aneurysm
formation, formation, nonobstructive. nonobstructive.
• Granulomas -caseating in nature in TB. In TA -Granulomas -caseating in nature in TB. In TA -proliferative without caseation. proliferative without caseation.
• No evidence for causation No evidence for causation • ?Viral etiology?Viral etiology

Pathology - Lesions in the Pathology - Lesions in the AORTAAORTA
• LocalisedLocalised involvement of a segment involvement of a segment of Aorta varying in size 2-7 cms.of Aorta varying in size 2-7 cms.
• MultipleMultiple short segments with normal short segments with normal
“skipped areas”“skipped areas” in between. in between.
• DiffuseDiffuse involvement of large portion involvement of large portion
of aorta with a stretch of normal of aorta with a stretch of normal
aorta in between.aorta in between.• Proximally,lesion may start at aortic Proximally,lesion may start at aortic
valvevalve

• Variable amount of Variable amount of adventitial or adventitial or periadventitial fibrous thickeningperiadventitial fibrous thickening over over involved part of aorta.involved part of aorta.
• DilatationDilatation of Ascending Aorta seen in portion of Ascending Aorta seen in portion
proximal to obstructive lesion.proximal to obstructive lesion.• AneurysmAneurysm may occur without any obstructive may occur without any obstructive
lesion.lesion.
• FOUR Types of luminal changes:FOUR Types of luminal changes:1.1.Irregular lumenIrregular lumen2.2.EctasiaEctasia3.3.Obstructive lesion-Obstructive lesion-””stenosisstenosis”” (hallmark of (hallmark of
disease)disease)4.4.Aneurysms-saccular & fusiformAneurysms-saccular & fusiform

Distribution of lesion in the AortaDistribution of lesion in the Aorta
LocalizedLocalized: : 37.5% - Adults:- Abdominal Aorta 37.5% - Adults:- Abdominal Aorta
Children:-Thoracic+AbdominalChildren:-Thoracic+Abdominal
DiffuseDiffuse:: 62.5% -thoraco-abdominal62.5% -thoraco-abdominal
Descending thoracic Aorta is maximally affected area Descending thoracic Aorta is maximally affected area
Aortic Arch: Distal involvement more than proximal.Aortic Arch: Distal involvement more than proximal.
Relative involvement of branch arteries: (%)(Panja et al)Relative involvement of branch arteries: (%)(Panja et al)
Coronaries 16.75 Lt.CCA 7.5Coronaries 16.75 Lt.CCA 7.5
Innominate 7.5 Coeliac A Innominate 7.5 Coeliac A 3.753.75
Rt.SCA 13.75 Sup.Mesentric A Rt.SCA 13.75 Sup.Mesentric A 16.75 16.75
Lt.SCA 40 Renal A Lt.SCA 40 Renal A 63.7563.75
Rt.CCA 11.25Rt.CCA 11.25
Commenest lesion in branches is ostial stenosis.Commenest lesion in branches is ostial stenosis.
BL Renal A Stenosis > UL(2.5 times)BL Renal A Stenosis > UL(2.5 times)

VESSELS INVOLVEDVESSELS INVOLVED
Subclavian 93%Subclavian 93%Common carotid 58%Common carotid 58%Abdominal aorta 47%Abdominal aorta 47%Renal 38%Renal 38%Aorticarch&root 35%Aorticarch&root 35%Vertebral 35%Vertebral 35%Coeliac axis 18%Coeliac axis 18%Superior mesentric 18%Superior mesentric 18%Iliac 17%Iliac 17%Pulmonary 10%Pulmonary 10%Coronary <10% KERR ET Coronary <10% KERR ET
AL AL

DIAGNOSTIC CRITERIADIAGNOSTIC CRITERIA
• ISHIKAWA CRITERIA (1988)ISHIKAWA CRITERIA (1988)
• ACR CRITERIA (1990)ACR CRITERIA (1990)
• SURI & SHARMA et. al CRITERIA SURI & SHARMA et. al CRITERIA (1995)(1995)

Diagnostic Criteria Diagnostic Criteria ISHIKAWA’SISHIKAWA’S
• Obligatory: Obligatory: Age< 40yrs ; at the time of diagnosis, at Age< 40yrs ; at the time of diagnosis, at onset of characteristic symptoms & signs onset of characteristic symptoms & signs of 1 month durationof 1 month duration
• Major :Major :
• Left Mid Subclavian Artery LesionLeft Mid Subclavian Artery Lesion• Right Mid Subclavian Artery LesionRight Mid Subclavian Artery Lesion
*Most severe obstruction occurs in mid portion *Most severe obstruction occurs in mid portion 1cm 1cm proximal to lt vertebral to 3cm distalproximal to lt vertebral to 3cm distal

MINOR CRITERIAMINOR CRITERIA High ESRHigh ESR : :
unexplained high ESR > 20mm at diagnosis or unexplained high ESR > 20mm at diagnosis or presence of evidence in history.presence of evidence in history.
CAROTID ARETRY TENDERNESSCAROTID ARETRY TENDERNESS : :
unilateral or bilateral tenderness on carotid palpation.unilateral or bilateral tenderness on carotid palpation. HYPERTENSIONHYPERTENSION : :
persistent BP brachial > 140/90 or popliteal >160/90 persistent BP brachial > 140/90 or popliteal >160/90 at age < 40 yrs or history at age <40 yrs at age < 40 yrs or history at age <40 yrs
AR or annuloaortic ectasiaAR or annuloaortic ectasia : :
by auscultation or doppler echo or angiographyby auscultation or doppler echo or angiography Pulmonary artery lesionPulmonary artery lesion : :
lobar or segmental artery occlusion or equivalent (by lobar or segmental artery occlusion or equivalent (by angio or perfusion scintigraphy )or stenosis, aneurysm, angio or perfusion scintigraphy )or stenosis, aneurysm, luminal irregularity or any combination in pulmonary luminal irregularity or any combination in pulmonary trunk or in unilateral or bilateral pulmonary arteries.trunk or in unilateral or bilateral pulmonary arteries.

Left mid comon carotid lesionLeft mid comon carotid lesion : : presence of most severe occlusion in mid portion of presence of most severe occlusion in mid portion of 5cm in length from the point 2cm distal to its orifice 5cm in length from the point 2cm distal to its orifice determined by angiographydetermined by angiography
Distal brachiocephalic lesionDistal brachiocephalic lesion : : presence of severe stenosis or occlusion in distal presence of severe stenosis or occlusion in distal third in angiographythird in angiography
Descending thoracic aorta lesionDescending thoracic aorta lesion : : narrowing dilatation , aneurysm or luminal narrowing dilatation , aneurysm or luminal irruegularity or any combination determined by irruegularity or any combination determined by angiography . Tortuosity alone is unacceptable angiography . Tortuosity alone is unacceptable
Abdominal aorta lesion : : narrowing dilatation , aneurysm or luminal narrowing dilatation , aneurysm or luminal irruegularity or any combination and absence of irruegularity or any combination and absence of lesion in aortoiliac region consisting of 2cm of lesion in aortoiliac region consisting of 2cm of terminal aorta and bilateral common iliac arteries terminal aorta and bilateral common iliac arteries determined by angiography . Tortuosity alone is determined by angiography . Tortuosity alone is unacceptable unacceptable

Obligatory criteriaObligatory criteria
++ 2 Major criteria 2 Major criteria
oror
1 Major and ≥ 2 Minor criteria 1 Major and ≥ 2 Minor criteria
oror
≥≥4 Minor criteria4 Minor criteria
High probability of Takayasu’s High probability of Takayasu’s diseasedisease
( sensitivity:84%)( sensitivity:84%)

American College Of American College Of Rheumatology (ACR)criteriaRheumatology (ACR)criteria
• AgeAge at disease onset ≤ 40 yrs at disease onset ≤ 40 yrs
• ClaudicationClaudication of extremities. of extremities.
Brachial Artery Brachial Artery pulsepulse
• Systolic BPSystolic BP difference of > 10 mm Hg between difference of > 10 mm Hg between armsarms
• BruitBruit over Subclavian Artery or Aorta. over Subclavian Artery or Aorta.
• AortogramAortogram abnormality. abnormality. ≥ ≥ 3 criteria — TA3 criteria — TA ( sensitivity 90.5%, specificity 97.8%)( sensitivity 90.5%, specificity 97.8%)

Suri & Sharma et. al Criteria Suri & Sharma et. al Criteria (PGI)(PGI)
The proposed modifications include:The proposed modifications include: Removal of the obligatory criteria of age Removal of the obligatory criteria of age
less than 40 years.less than 40 years. Inclusion of characteristic signs and Inclusion of characteristic signs and
symptoms as a major criteria.symptoms as a major criteria. Removal of age in defining hypertension.Removal of age in defining hypertension. Deletion of the absence of aorto-iliac lesion, Deletion of the absence of aorto-iliac lesion,
in defining abdominal aortic lesion and.in defining abdominal aortic lesion and. An addition of coronary artery lesion in An addition of coronary artery lesion in
absence of risk factors. absence of risk factors.

The criteria proposed consists of The criteria proposed consists of three major three major criteria:criteria:
• left and right mid subclavian artery lesions andleft and right mid subclavian artery lesions and• characteristic signs and symptoms of at least characteristic signs and symptoms of at least
one month duration andone month duration and• Ten minorTen minor criteria:criteria:
• High ESRHigh ESR• HypertensionHypertension• Carotid artery tendernessCarotid artery tenderness• Aortic regurgitation or Annuloaortic ectasiaAortic regurgitation or Annuloaortic ectasia• Left mid common carotid lesionLeft mid common carotid lesion• Distal brachiocephalic trunk lesionDistal brachiocephalic trunk lesion• Descending thoracic aorta lesionDescending thoracic aorta lesion• Abdominal aorta lesion Abdominal aorta lesion • Coronary artery lesion.Coronary artery lesion.• Pulmonary artery lesionPulmonary artery lesionPresence of two major or one major and two minor Presence of two major or one major and two minor
criteria or four minor criteria suggests a high criteria or four minor criteria suggests a high probability of TA probability of TA

• Sensitivity of 92.5% and specificity of 95% Sensitivity of 92.5% and specificity of 95% that was that was higher higher than that of Ishikawa's than that of Ishikawa's criteria (sensitivity 60.4%, specificity 95%) criteria (sensitivity 60.4%, specificity 95%) and American college of Rheumatology and American college of Rheumatology criteria (sensitivity 77.4%, specificity 95%).criteria (sensitivity 77.4%, specificity 95%).
• Similarly, this criteria had a 96% sensitivity Similarly, this criteria had a 96% sensitivity and specificity when applied to 79 Japanese and specificity when applied to 79 Japanese patients of TA and 79 control subjects. patients of TA and 79 control subjects.
• Adoption of these criteria is expected to Adoption of these criteria is expected to prevent the possibility of an under prevent the possibility of an under diagnosis of TA. diagnosis of TA.

Classification Proposed by Classification Proposed by Ueno et al, modified by Ueno et al, modified by
Lupi Herrera Lupi Herrera • Type I - involvement of aortic arch and Type I - involvement of aortic arch and
its branches (16%)its branches (16%)
• Type II -Thoraco abdominal aorta,but Type II -Thoraco abdominal aorta,but
spares arch (8%)spares arch (8%)
• Type III-Features of I &II (76%)Type III-Features of I &II (76%)
• Type IV-Pulmonary artery involvement Type IV-Pulmonary artery involvement
(Lupi herrera et al) (36%)(Lupi herrera et al) (36%)
• Type V-Coronary artery involvement Type V-Coronary artery involvement
(Panja et al) (10%)(Panja et al) (10%)


Disease Basically evolves through Disease Basically evolves through
1.1. Early Pre-pulseless (50%): Active phaseEarly Pre-pulseless (50%): Active phaseNonspecific symptoms & signs: Fever, Wt Nonspecific symptoms & signs: Fever, Wt loss, Fatigue, Headache, Arthralgias, loss, Fatigue, Headache, Arthralgias,
Splenomegaly, LNpathy etc.Splenomegaly, LNpathy etc.
- - challenge in the early diagnosischallenge in the early diagnosis
2. Pulseless Phase (Ischemic): (sequel of 2. Pulseless Phase (Ischemic): (sequel of occlusion of arch of aorta) occlusion of arch of aorta)
HTN, HTN, / No Pulse, Bruit,, HF, Abnormal / No Pulse, Bruit,, HF, Abnormal Fundi.Fundi.
Clinical FeaturesClinical Features

Early phaseEarly phase
Non specific systemic symptoms : Non specific systemic symptoms :
fever, loss of weight, head ache, fatigue, fever, loss of weight, head ache, fatigue, gen weakness, night sweats, anoreia, gen weakness, night sweats, anoreia, arthralgia, skin rash, splenomegaly, cervical arthralgia, skin rash, splenomegaly, cervical lymphadenopathy, pleurisy, myocarditis, lymphadenopathy, pleurisy, myocarditis, pericarditis, CVA.pericarditis, CVA.
Lab abnormalities : Lab abnormalities :
↑↑ESR, mild leukocytosis, anemia, CRP, IGs, ESR, mild leukocytosis, anemia, CRP, IGs, RA factor, ANF, ANCA, mild proteinuria, RA factor, ANF, ANCA, mild proteinuria, albuminuria.albuminuria.

Kerr, G. S. et. al. Ann Intern Med 1994;120:919-929
Criteria for Active Disease in Patients with Takayasu Arteritis*

Late phaseLate phase
Diminished or absent pulsesDiminished or absent pulses 96%96%
BruitsBruits 94%94%
HTN HTN 72%72%
Heart failure Heart failure 28%28%

Hypertension Hypertension • 33–83% of patients, more among Indians 33–83% of patients, more among Indians • renal artery stenosis in 28–75%renal artery stenosis in 28–75%
Aortic regurgitation -20-24% Aortic regurgitation -20-24% • dilatation of the ascending aorta dilatation of the ascending aorta • separation of the valve leaflets separation of the valve leaflets • Valve thickening (Chhetri et al) Valve thickening (Chhetri et al)
Congestive cardiac failure Congestive cardiac failure • hypertension hypertension • aortic regurgitation aortic regurgitation • myocarditis. myocarditis.

Pulmonary involvement Pulmonary involvement • 70% angiographic studies (36% - Panja et al)70% angiographic studies (36% - Panja et al)• segmental and subsegmental branches, more segmental and subsegmental branches, more
in the upper lobes in the upper lobes • haemoptysis, chest pain, disproportionate haemoptysis, chest pain, disproportionate
PAH abnormal ventilation-perfusion scan PAH abnormal ventilation-perfusion scan
Coronary involvement Coronary involvement • in 10% in 10% • usually ostial and proximal usually ostial and proximal • diffuse lesions or arteritis and aneurysm diffuse lesions or arteritis and aneurysm
rarely occur.rarely occur.
Neurological Neurological • Secondary to hypertension or ischaemiaSecondary to hypertension or ischaemia..

OCULAR :OCULAR :• Amaurosis fugaxAmaurosis fugax• Hypertensive retinopathy [keith-wagner]Hypertensive retinopathy [keith-wagner] arteriolar narrowing, av crossing changesarteriolar narrowing, av crossing changes silver wiring, exudates, papilloedema.silver wiring, exudates, papilloedema.• Ischemic retinopathy [ Uyama and Asayama]Ischemic retinopathy [ Uyama and Asayama] Stage 1 : dilatation of small vessels Stage 1 : dilatation of small vessels stage 2 : micro aneurism formationstage 2 : micro aneurism formation stage 3 : wreath like AV anastamosisstage 3 : wreath like AV anastamosis formation surrounding optic formation surrounding optic papillae papillae stage 4 : cataract ,secondary stage 4 : cataract ,secondary
glacoma ,rubeosis,glacoma ,rubeosis, neo vascularisation, proliferative neo vascularisation, proliferative retinopathy, vitreous retinopathy, vitreous
hemorrhage.hemorrhage.

Kerr, G. S. et. al. Ann Intern Med 1994;120:919-929
Frequency of clinical features of Takayasu arteritis at presentation and during the course of disease

Takayasu’s Disease in Takayasu’s Disease in ChildrenChildren
• Not as frequent as in adultsNot as frequent as in adults• Clinical profile sameClinical profile same• Manifestations may be more severeManifestations may be more severe• Most common cause for renovascular Most common cause for renovascular
HTNHTN• Presenting features: HTN, CCFPresenting features: HTN, CCF• An association with TB has been An association with TB has been
hypothesized , never provenhypothesized , never proven

PREGNANCYPREGNANCY
• Pregnancy per se does not exacerbate the Pregnancy per se does not exacerbate the disease disease
• Management of hypertension is essential. Management of hypertension is essential. • Maternal complications: superimposed Maternal complications: superimposed
pre-eclampsia, congestive cardiac failure, pre-eclampsia, congestive cardiac failure, progressive renal impairment. progressive renal impairment.
• Abdominal aortic involvement and a delay Abdominal aortic involvement and a delay in seeking medical attention predicted a in seeking medical attention predicted a poor perinatal outcome.poor perinatal outcome.

Natural historyNatural history
• Subramanyam et al- cumulative survival Subramanyam et al- cumulative survival at 5 years-91%,10 yrs-84%. Event free at 5 years-91%,10 yrs-84%. Event free survival-75% survival-75%
• Ishikawa-Survival rate: 83.1 at 5 years Ishikawa-Survival rate: 83.1 at 5 years after diagnosis. after diagnosis.
• Cardiac failure - most common cause of Cardiac failure - most common cause of death. death.
• Spontaneous improvement can occur in Spontaneous improvement can occur in young patients. young patients.
• Childhood-onset particularly when Childhood-onset particularly when associated with a DCM like picture associated with a DCM like picture carries ominous prognosis. carries ominous prognosis.
• Failed angioplasty implicates high Failed angioplasty implicates high mortality.mortality.

Evaluation Of Takayasu’s Evaluation Of Takayasu’s ArteritisArteritis• HematologyHematology: :
Mild Anaemia Mild Anaemia Leucocytosis Leucocytosis
• Markers of disease activityMarkers of disease activity : : E S R >40mm E S R >40mm 50% cases progress with N ESR 50% cases progress with N ESR C R PC R P ASO titre – increased in 50% cases ASO titre – increased in 50% cases
but not correlated with activitybut not correlated with activity RA factor, ANA, fibrinogen , p-ANCARA factor, ANA, fibrinogen , p-ANCA
• CXRCXR:: Aortic knob wideningAortic knob widening Thoracic Aorta irregularityThoracic Aorta irregularity Pulm. VascularityPulm. Vascularity Aortic calcificationAortic calcification Cardiomegaly.Cardiomegaly. Notching of upper ribs Notching of upper ribs prox. Subclavian prox. Subclavian
blockblock lower ribs lower ribs Abd. Aortic stenosisAbd. Aortic stenosis• X-ray AbdomenX-ray Abdomen: Abd. Aorta calcification.: Abd. Aorta calcification.

In conclusion, the present results suggest that monitoring of circulating levels of MMP-2 as a helpful marker in diagnosing TA and those of MMP-3 and MMP-9 as disease activity markers might help provide adequate evaluation of treatment and guide therapeutic decision making for individual patients with TA. These measurements can be part of routine hospital laboratory examinations that are easy to perform at low cost. Furthermore, the noninvasive nature of such measurements is attractive, because patients can be spared from invasive angiographic examination.
Matrix Metalloproteinases as Novel Disease Markers in Takayasu Arteritis

Non –invasive imaging Non –invasive imaging modalitiesmodalities
• USGUSG: Duplex Scanning: Duplex Scanning • 2DECHO2DECHO: Assessment of LV Dysfunction,: Assessment of LV Dysfunction, Valvular involvement. Valvular involvement.
• CT AngiographyCT Angiography: Aorta & Pulmonary Artery : Aorta & Pulmonary Artery
• MRIMRI : Mural involvement ;dilatation of : Mural involvement ;dilatation of vasavasorum vasavasorum
• Flouroscein Angiogram of retinal vessels Flouroscein Angiogram of retinal vessels Ophthalmodynamometry . Ophthalmodynamometry .
• PET SCANPET SCAN

Ultrasound scan of the internal carotid artery demonstrating marked thickening of the arterial walls

Filling defect: A filling defect may
be present in either the retinal
or choroidal circulation which may be produced by emboli seen in
Takayasu's disease.
Fluorescein Angiogram

Intravascular Ultrasound
IVUS

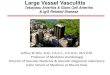
Magnetic resonance imaging of the aorta and its major proximal branches. There is thickening of the aortic arch that extends into both common carotid arteries
(A), with almost complete obliteration of the right carotid artery and both subclavian arteries (B).
A B

Catheterization and Catheterization and AngiographyAngiography
• Pan-aortographyPan-aortography,, preferably with intrarterial digital preferably with intrarterial digital
subtraction angiography subtraction angiography most important diagnostic investigation most important diagnostic investigation helps in planning management helps in planning management Visualisation of entire Aorta& its major Visualisation of entire Aorta& its major
branches branches special attention to special attention to innominate, subclavian&innominate, subclavian&
extracranial portions of carotid arteries.extracranial portions of carotid arteries.• Coronary AngiographyCoronary Angiography
• Pulmonary AngiographyPulmonary Angiography

Lt SCA

Rt SCA

CC A

Abd Aorta

Rt SCA Narrowing
Rt CCA Long Stenosis
Lt SCA Not Seen

Diagnosis of systemic arterial diseases with whole body 3D contrast-enhanced magnetic resonance
angiographyChin Med J 2006;
Fig. 1. A 45-year-old patient with polyarteritis nodosa. Whole-body MRA reveals multiple aneurysms of different size in bilateral lower extremity arteries (arrows).Fig. 2. A 70-year-old man with clinicallydocumented abdominal aorta aneurysm. A:Whole-body MRA demonstrates multiple aortic aneurysms and concomitant PAOD (arrows). B:Oblique sub-volume maximum-intensity-projection shows the aneurysm at the aortic arch (arrow). C:Sub-volume maximum-intensity-projection shows multiple aneurysms in the thoraco-abdominal,abdominal aorta and iliac arteries (arrows).

Management of TAManagement of TA• Depend on : Depend on : Clinical presentationClinical presentation Disease activityDisease activity
• One of the challenges in the management One of the challenges in the management of TA is determining of TA is determining disease activitydisease activity. .
Kerr et alKerr et al define active disease as define active disease as any any two or moretwo or more of the following of the following
1.1. New or worsening:Signs or symptoms of New or worsening:Signs or symptoms of vascular ischemia or inflammationvascular ischemia or inflammation
2.2. Increase in sedimentation rate Increase in sedimentation rate 3.3. Angiographic features Angiographic features 4.4. Systemic symptoms not attributable to Systemic symptoms not attributable to
another diseaseanother disease

Therapeutic StrategiesTherapeutic Strategies• Medical Therapy:Medical Therapy:
• Active or Early Lesions,Active or Early Lesions,• Not In Need of Interventions.Not In Need of Interventions.• Co-Morbid Conditions.Co-Morbid Conditions.• Refuse Interventions.Refuse Interventions. SteroidsSteroids AntihypertensivesAntihypertensives DecongestantsDecongestants Cytotoxic DrugsCytotoxic Drugs Oral AnticoagulantsOral Anticoagulants

MEDICAL MANAGEMENTMEDICAL MANAGEMENT
1. Immunosuppressive therapy1. Immunosuppressive therapy
2. decongestive therapy2. decongestive therapy
anti hypertensive therapyanti hypertensive therapy

Activity of diseaseActivity of disease
[clinical symptoms, ESR, angiography,biopsy][clinical symptoms, ESR, angiography,biopsy]
Active disease Inactive diseaseActive disease Inactive disease- Prednisolone 1 mg/kg ( 3 mon)Prednisolone 1 mg/kg ( 3 mon)
Remission ResistentRemission Resistent
cyclo phosphamide cyclo phosphamide 2mg/kg2mg/kg
Taper steroids methotrexate 20mg /wkTaper steroids methotrexate 20mg /wk
azathioprim 200mg/dayazathioprim 200mg/day
Persistent RelapsePersistent Relapse
remission remission

• Decongestive therapyDecongestive therapy
• Anti hypertensive therapyAnti hypertensive therapy
• Treatment of renal failureTreatment of renal failure
• Antiplatelet therapyAntiplatelet therapy
• Anti tuberculous therapyAnti tuberculous therapy
caution: ?????caution: ????? Steroids in aneurismal Steroids in aneurismal
dilation of vesselsdilation of vessels

Minocycline for the Treatment of Takayasu Arteritis
Annals of Internal Medicine
Actions of minocycline in these diseases are thought to be independent of antimicrobial activity and are related to pleiotropic effects, including inhibition of MMP activitiesMinocycline may be a valuable additive to steroids or an alternative to immunosuppressive agents for patients with Takayasu arteritis and should be tested in randomized, controlled trials.

Mycophenolate Mofetil for the
Treatment of Takayasu Arteritismycophenolate mofetil could
represent a valid alternative to conventional therapy in patients with Takayasu arteritis. Although the rareness of the disease is an obstacle to designing prospective, controlled clinical trials, this first description of mycophenolate mofetil therapy in patients with Takayasu arteritis is encouraging.

Infliximab is Effective for Takayasu Arteritis Refractory toGlucocorticoid and Methotrexate
The pathogenesis of TA includes vessel injury due to products from activated T cells, natural killer cells, γ/δ T cells and macrophages. One of the important humoral factors is TNF-α, the molecular target for human autoimmune diseases Glucocorticoid therapy is usually introduced for TA, but glucocorticoid alone is sometimes not efficient; Kerr et al reported that about half of active TA patients did not respond well to glucocorticoid alone (6). In addition to glucocorticoid, an immunosuppressive regime such as cyclophosphomide, methotrexate and azathioprine has been used to treat TA (6-8); however, some patients are refractory to both glucocorticoid and immunosuppressants. Hoffman et al have recently reported the efficacy of TNF blockers toward TA refractory to conventional glucocorticoid therapy and immunosuppressants Patient selection criteria described by Hoffman et al include:1] required toxic doses of glucocorticoids to maintain remission, and 2] either experienced multiple relapses while receiving conventional and experimental therapy or refused re-treatment with glucocorticoids following relapses

• Surgical Therapy: Surgical Therapy: (Definitive (Definitive Treatment for occlusive disease & Treatment for occlusive disease & Aneurysm)Aneurysm)• StenosisStenosis
• HypertensionHypertension• End organ DamageEnd organ Damage
• Bypass Grafting, Endarterectomy, Patch Bypass Grafting, Endarterectomy, Patch Aortoplasty, Resection of Narrow Aortoplasty, Resection of Narrow Segment, Excision of Saccular Segment, Excision of Saccular Aneurysms and AVRAneurysms and AVR
Therapeutic StrategiesTherapeutic Strategies (Cont)(Cont)

Surgical treatment Surgical treatment IndicationsIndications
• Hypertension with critical renal artery stenosis Hypertension with critical renal artery stenosis • Extremity claudication limiting activities of Extremity claudication limiting activities of
daily living, daily living, • Cerebrovascular ischaemia or critical stenoses Cerebrovascular ischaemia or critical stenoses
of three or more cerebral vessels of three or more cerebral vessels • Moderate or severe aortic regurgitation Moderate or severe aortic regurgitation • Cardiac ischaemia with confirmed coronary Cardiac ischaemia with confirmed coronary
artery involvement. artery involvement. • Thoracic aneurysms> 6 cm;abd aortic Thoracic aneurysms> 6 cm;abd aortic
aneurysms> 5 cm. aneurysms> 5 cm. • Surgery is recommended at a time of Surgery is recommended at a time of
quiescent disease to avoid complications like quiescent disease to avoid complications like restenosis, anastamotic failure, thrombosis, restenosis, anastamotic failure, thrombosis, haemorrhage, and infection. haemorrhage, and infection.

Fig.5. The onset segments of the celiac trunk, superior mesenteric artery and inferior mesenteric artery are occlusive completely but the vessel wall of the distal extremity has no hyperplasia lesion and the true lumen still exists.Fig.6. The infra-diaphragm aortic artery has no stenosis.Fig.7. The Aorto-SMA grafting by-pass.Fig.8. End to side anastomosis, 6-mm e-PTFE graft without outer rings, Gore.

AngioplastyAngioplastyBalloon Angioplasty ± Stenting of Balloon Angioplasty ± Stenting of the involved segment.the involved segment.• For discrete aortic lesions For discrete aortic lesions • low rates of restenosis (0%–19%) low rates of restenosis (0%–19%) • Renal angioplasty successful in 95% Renal angioplasty successful in 95% • Stent-supported angioplasty for Stent-supported angioplasty for
subclavian and carotid artery subclavian and carotid artery obstructions with good success rates obstructions with good success rates (86%) and moderate rates of (86%) and moderate rates of restenosisrestenosis


Sirolimus-Eluting Stent for In-Stent Restenosis of Left Main Coronary Artery in
Takayasu Arteritis
In conclusion, Takayasu arteritis with LMCA in-stent restenosis was successfully treated by a SES. Because of its immunosuppressive effects in the inflamed arterial walls, the SES shows promise for the treatment of stenotic lesions in patients with Takayasu arteritis.
Circ J 2005; 69: 752 –755

Coronary and pulmonary angiographic findings during the first hospitalization for angina. (A) Leftcoronary selective injection revealed 90% stenosis in the ostium of the left main coronary artery (LMCA).(B) Intact right coronary artery. (C) Totally occluded left pulmonary artery. (D) Left coronary angiographyafter percutaneous coronary stenting. The 90% stenosis of the LMCA was successfully dilated to 0%.

Multiple stenting in a Multiple stenting in a patientpatient
Fig. 2 - Preinterventional angiography: A and B: left and right coronary arteries, respectively, with no obstructive lesions; C: left common carotid artery with severe obstruction; D: right common carotid artery with mild obstruction; E: left subclavian artery with occlusion in the proximal third; F and G: right and left renal arteries with moderate and severe lesions, respectively; H: left iliac artery with occlusion in the proximal third; I: left ventricle with diffuse
hypokinesia; J: aortic valve regurgitation and ectasia of the ascending aorta.

Fig. 3 - Herculink stent implantation in renal artery lesion; pre and postintervention.

Smart stent implantation in carotid artery lesion; pre and postintervention.

Fig. 5 - Successful previous interventions remained unchanged. Lesion in the right common carotid artery.

Fig. 6 - Herculink stent implantation in carotid artery lesion; pre and postintervention.


AuthorAuthor No: No: of of pts.pts.
BallooBalloon n diamediameterter
Results : aorta at Results : aorta at stenosisstenosis
Major Major complicationscomplications
Follow upFollow up
BeforBeforee
AfterAfter Dilated Dilated %%
DuraDuration(tion(montmonths)hs)
resterestenosisnosis
Gu et Gu et al – al – 19911991
1616 10-2010-20 4.6m4.6mmm
10.210.2mmmm
14(87.514(87.5%)%)
Dissection-1Dissection-1 19.119.1 NilNil
Rao et Rao et al – al – 19931993
1616 All(100%All(100%))
Cerebral Cerebral infarct-1infarct-1
Axillary artery Axillary artery stenosis-1stenosis-1
Dissection-2Dissection-2
21.421.4 19%19%
SharmSharma - a - 1994 1994
1010 5-125-12 80.580.5%%
14%14% 8(80)8(80) Dissection-2Dissection-2 17.817.8 NilNil
Tyagi – Tyagi – 1992 & 1992 & 1999 1999
146146 7-207-20 4.2m4.2mmm
9.9m9.9mmm
120(82.2120(82.2))
141(96.5141(96.5) with ) with stentstent
Long Long dissection-4dissection-4
Retro Retro peritoneal peritoneal leak-1leak-1
54.454.4 8.2%8.2%
Balloon aortoplasty of aorta in TABalloon aortoplasty of aorta in TA

AuthorAuthor No: No: of of lesiolesionsns
Initial resultsInitial results ComplicComplicationsations
Follow upFollow up
DurationDuration resultsresults
Dong et Dong et al-1987al-1987
3232 D↑from 1.8 to D↑from 1.8 to 4.8mm4.8mm
16.7 %16.7 % 25.525.5 Htn ↓ 87%Htn ↓ 87%
Gu et al-Gu et al-19881988
66 No stenosis-1 No stenosis-1
Partial stenosis-5Partial stenosis-5-- -- Htn ↓Htn ↓
Park et al-Park et al-19891989
99 All dilatedAll dilated NilNil 44 Restenosis Restenosis 22%22%
Kumar et Kumar et al 1989al 1989
99 6/9 dilated6/9 dilated 33.3%33.3% --
Fava et Fava et al-1993al-1993
1212 83% success83% success -- -- 5 yr patency5 yr patency
Sharma Sharma et al-1998et al-1998
66 66 (96)(96)
Success Success 91/96(95%)91/96(95%)
6(9.1%)6(9.1%) 22±1722±17 Restenosis Restenosis 16%16%
Tyagi et Tyagi et al - 1999al - 1999
148 148 (205)(205)
Ptra success – Ptra success – 85.6%85.6%
Ptra + stenting –Ptra + stenting –95%95%
7(3.4%)7(3.4%)
Major-Major-2(1%)2(1%)
47±38.547±38.5 Restenosis -Restenosis -17%17%
Percutaneous transluminal renal angioplasty in TA

A follow-up study of balloon angioplasty and de-A follow-up study of balloon angioplasty and de-novo stenting in Takayasu arteritis.novo stenting in Takayasu arteritis.
Sharma BK, Jain S, Bali HK, Jain A, Kumari S Sharma BK, Jain S, Bali HK, Jain A, Kumari S (PGIMER)(PGIMER) Int J Cardiol. 2000 Aug 31;75 Int J Cardiol. 2000 Aug 31;75 Suppl 1:S147-52Suppl 1:S147-52
• Percutaneous balloon angioplasty(PTBA) was done in Percutaneous balloon angioplasty(PTBA) was done in 20 pts20 pts with TA. with TA. • All pts received steroids, aspirin and ticlodipine (for stenting) prior to All pts received steroids, aspirin and ticlodipine (for stenting) prior to
procedure. procedure. • Angioplasty was carried in pts with symptomatic stenotic vessel of Angioplasty was carried in pts with symptomatic stenotic vessel of
more than 70% of N. D or a peak systolic gradient of more than 50 mm more than 70% of N. D or a peak systolic gradient of more than 50 mm across stenotic aortic lesion. across stenotic aortic lesion.
• Stenting was performed for ostial lesion, long segment lesion or Stenting was performed for ostial lesion, long segment lesion or incomplete relief of stenosis and dissection following angioplasty. incomplete relief of stenosis and dissection following angioplasty.
• Carotid angioplasty and stenting was performed in 5 patients, Carotid angioplasty and stenting was performed in 5 patients, • aortic angioplasty in 9 pts, aortic angioplasty and stenting in 4 pts, aortic angioplasty in 9 pts, aortic angioplasty and stenting in 4 pts, • renal angioplasty in 3 pts, renal angioplasty and stenting in 2 pts and renal angioplasty in 3 pts, renal angioplasty and stenting in 2 pts and • subclavian angioplasty in 2pts,subclavian angioplasty & stenting in subclavian angioplasty in 2pts,subclavian angioplasty & stenting in
3pts & 3pts & • coronary angioplasty and stent placement in 1 patient. coronary angioplasty and stent placement in 1 patient. • The procedure was successful in all but 1 patient. The procedure was successful in all but 1 patient. • On following up, 2 patients with carotid stent placement had On following up, 2 patients with carotid stent placement had
restenosis. A saccular aneurysm developed at the lower end of stent in restenosis. A saccular aneurysm developed at the lower end of stent in 1 patient with aortic stenting. 1 patient with aortic stenting.
• The PTBA with or without stent placement is a safe and effective The PTBA with or without stent placement is a safe and effective method for relief of stenotic lesion in patients with TA.method for relief of stenotic lesion in patients with TA.