Embed Size (px)
Citation preview

Teach Evaluation & Management Codingto Your Doctor in One Hour
2012AAPC2480 South 3850 West, Suite BSalt Lake City, Utah 84120800-626-CODE (2633), Fax 801-236-2258www.aapc.com


Teach Evaluation & Management Coding to Your Doctor in One Hour
By: Stephanie L Cecchini, CPC, CEMC, CHISP

ii AAPC 1-800-626-CODE (2633) CPT® copyright 2011 American Medical Association. All rights reserved.
Introduction
Disclaimer This course was current at the time it was published. This course was prepared as a tool to assist the participant in educat-ing providers and is not intended to grant rights or impose obligations. Although every reasonable effort has been made to assure the accuracy of the information within these pages, the ultimate responsibility for the correct submission of claims and response to any remittance advice lies with the provider of services. AAPC employees, agents, and staff make no representation, warranty, or guarantee that this compilation of information is error-free and will bear no responsibility or liability for the results or consequences of the use of this course. This guide is a general summary that explains commonly accepted aspects of selecting Evaluation and Management (E/M) codes, but it is not a legal document. View points are discussed from the standpoint of the 1995 and 1997 Centers for Medicare and Medicaid Services (CMS) Evaluation and Management Documentation Guidelines with medical necessity and the nature of the presenting problem as the primary criterion of code selection (Medicare Claims Processing Manual Chapter 12—Physicians/Nonphysician Practitioners, 30.6.1—Selection of Level of Evaluation and Management Service, A. Use of CPT® Codes.) For the purpose of objective consistency, specific logics are primarily based on the same used by the E/M Documentation Auditors’ Worksheet, Marsh-field Clinic, available through the Medical Group Management Association (MGMA). Specific payers, including Medicare Carriers, may use different and sometimes varied audit tools logics to gain objective consistency around the 95 and 97 Documentation Guidelines. Official provisions are contained in the relevant laws, regulations, rulings and contractual agreements of providers.
Notices Current Procedural Terminology (CPT®) is copyright ©2011 American Medical Association. All Rights Reserved. CPT® is a registered trademark of the American Medical Association (AMA).
It is recommended that the participant of this course will be familiar with:
z 1995 Documentation Guidelines for Evaluation and Management Services z 1997 Documentation Guidelines for Evaluation and Management Services
These may be downloaded from the CMS website at: www.cms.hhs.gov/MLNEdWebGuide/25_EMDOC.asp
Notice Regarding Clinical Examples Used in this BookAAPC believes it is important in training and testing to reflect as accurate a coding setting as possible to students and examinees. All examples and case studies used in our study guides and exams are actual, redacted office visit and proce-dure notes donated by AAPC members.
To preserve the real world quality of these notes for educational purposes, we have not rewritten or edited the notes to the stringent grammatical or stylistic standards found in the text of our products. Some minor changes have been made for clarity or to correct spelling errors originally in the notes, but essentially they are as one would find them in a coding setting.
© 2012 AAPC2480 South 3850 West, Suite B, Salt Lake City, Utah 84120
800-626-CODE (2633), Fax 801-236-2258, www.aapc.com
All rights reserved.
CPC®, CPC-H®, CPC-P®, CIRCC®, CPCOTM, and CPMATM are trademarks of AAPC.

Teach Evaluation & Management Coding to Your Doctor in One Hour www.aapc.com iii
Introduction
Contents
Chapter 1: Effective Communication. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .1
Three Steps to Setting the Stage for Effective Communication . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1
Chapter 2: Medical Necessity, The First 0–10 Minutes of Coaching Time . . . . . . . . . . . . . . . . . . . . . . . . .2
Helpful Links on Medical Necessity: . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
Chapter 3: History Taking, The Next 11–20 Minutes of Coaching Time . . . . . . . . . . . . . . . . . . . . . . . . . . .4
Review of Systems . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5
Past, Family, and Social History . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6
History Coding . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .7
Chapter 4: Exam, The Next 21–30 Minutes of Coaching Time . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .7
The 1995 Documentation Guidelines . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8
The 1997 Documentation Guidelines . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
Chapter 5: Medical Decision Making, The Next 31–40 Minutes of Coaching Time . . . . . . . . . . . . . . . . . . . .12
The Number of Diagnoses and Management Options . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12
Amount and/or Complexity of Data to be Reviewed. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
Risk Significant Complications, Morbidity, and/or Mortality . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
Chapter 6: Putting It Together—The Last 41–50 Minutes of Coaching Time . . . . . . . . . . . . . . . . . . . . . . .15
Organizing Physician Communication. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16
Visual references and practical examples . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16
Chapter 7: Final Points . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .18
Practical Activity . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19


Teach E/M Coding to Your Doctor
Teach Evaluation & Management Coding to Your Doctor in One Hour www.aapc.com 1
Chapter 1: Effective CommunicationCommunicating effectively with physicians requires an understanding of their needs, wants and mindset. Typi-cally life-long learners, physicians are highly intelligent, with a deep appreciation for logic and reason. They are naturally intuitive; some even feeling spiritually drawn to practice the art of medicine and healing. Generally hungry for and appreciative of tips and techniques in learning new skills, physicians crave correctness. So holds true to billing, and it applies equally to coding correctly as well as being paid correctly. Accurate Evaluation and Management (E/M) coding can prove a frustrating dichotomy; it is both a zealous challenge to achieve cor-rectness, while also an intrusion.
Why? z Over-reacting: Defensive under-coding or emotional over-coding
z Payment: Unease about being paid properly for the value of the service
z Ambiguity: Concerns regarding subjective, hidden, or unknown aspects of proper coding
z Fear: Consequences effectively begin the process of communicating coding rules, these concerns should be addressed. The following three-step approach can be very helpful in setting the stage for positive outcomes.
Three Steps to Setting the Stage for Effective CommunicationPayment: The Price of the Ticket has Nothing to Do with the Rules of the Ball Game.
z Correct coding is static with literally nothing to do with flexible payments. Regardless of payment, the level of service coded is based on proper coding requirements and never on payment
z Payments are important to physicians. This must be acknowledged by an effective coach :
Those concerns will be addressed by other means, such as contract re-negoTiaTions, buT noT in This conver-saTional arena.
Ambiguity: It Is Okay to Yell at the Umpire—If You Can Prove to Him You’re Right.Part of the problem physicians have with coding rests with difficulties in the subjective aspects of correct code selection for E/M services. On the surface, code selection appears black and white with a clearly correct answer. However, interpretations of the rules for documentation requirements and determinations of medical necessity can be frustrating.
z From the aspect of medical necessity, the correct level of service is determined by how “sick” a patient is. The provider can usually tell by the nature of the presenting problem(s) what level of E/M should be billed. As a coding coach and resource, it is our job to help the provider understand the documentation required to support the services performed. Condi-tions posing an immediate threat to life or limb qualify for the highest level, whereas patients whose conditions reflect minor or well controlled problems are at the lowest. For many physicians, selecting a level of service to bill becomes hazy. On a scale of one to five, with five being the highest level of ser-vice, selecting between a Level 3 and a Level 4 or 2 is more difficult.
z Peers may see the same patient and, assuming the same diagnosis, may still argue how sick the patient really is. One may argue that managing three stable chronic illnesses in a patient without complaint is a Level 3 or a Level 4. The other may feel differently. Beyond medical necessity aspects, the rules governing documentation requirements are also in many ways subjective.
z Properly trained and certified auditors may agree on the actual code selection better than 90 percent of the time; however, the means and measurements of their conclusion can be different upwards of 50 percent.
{ Familiarities with clinical examples from credible sources are valuable in making determinations. Where no examples can be found, the written opinions of specialty associations are very power-ful and establish objective measures where there is subjectivity. A solid understanding of code require-ments and the backing of medically-accepted standards of practice allows a physician to shore up subjectivity to assure uncontestable coding and billing, ultimately achieving the most favorable and correct ongoing outcomes for all involved.

Teach E/M Coding to Your Doctor
2 AAPC 1-800-626-CODE (2633) CPT® copyright 2011 American Medical Association. All rights reserved.
Fear: What’s More Likely to be Hit: The Batter or the Ball?
z Code selection is usually predictable within the first few moments and during the history taking of the patient encounter. The nature of the presenting prob-lem and severity of illness drives documentation in the same way that it evokes the medically-indicated examination and clinical decision making. When physicians recognize the clinical relationship of code selection, documentation is an easier process with a key purpose of supporting the correct code and the service rendered.
z Coding software and paper templates are helpful but not necessary. When a physician is familiar with what is needed in documentation to support a given level of service, the process becomes rote.
{ With minimal instruction, a physician’s clinical training makes him or her an expert in correctly identifying a level of service. Following the easy techniques outlined in this course, a coach can teach physicians easy recall on the specific elements needed to document and support the correct level of service.
Overcoming ObjectionsIt is easier to teach E/M coding to a physician who is ready and eager for the information. Sometimes, physicians may be attending training as a requirement made by a practice manager, partner or compliance department and may not be as receptive. Overcoming objections may be necessary before effective training can begin.
More often than not when physicians object to training, it is because they have not been convinced your training will have a sufficient benefit for them. You can often over-come this by asking questions around what their current situation is (“I’m too busy!”), or what concerns they are facing…or not facing (“No one is going to audit me!”). By asking questions you are including physicians in the solu-tion from the very beginning. You are also qualifying their objections, which will help you overcome them.
Tip #1: Add information to the objection to boost interestExample Objection: I don’t have time for this!
Response: “With cuts in fees from Medicare and private insurers, many doctors must see more patients to main-tain their incomes, and that means that they have less time. I understand your problem and want to make this
painless. This training takes less than an hour and may ultimately save you time and money. You’ll learn how to avoid under-coding and under-documentation. Typically you’ll get the most out of it if we do it all at once in under one hour—but we can do it in 10 minute sessions if you prefer.”
With this response you build credibility by demonstrating that you understand and care about the value of the physi-cian’s time. You also imply that you have had the same objection from other physicians who still agreed to attend your training.
Tip # 2: Turn the objection into a question to get the right attentionObjection: No one is going to audit me!Response: “Can you afford to be wrong?” Traditionally, the relative high cost of auditing E/M records meant that only large groups or suspected fraud cases were audited. However, because of the Internet and new technology, auditing E/M records has never been easier and is no longer cost prohibitive. Government offi-cials, employers, and patient consumer stakeholders are demanding controls on health care costs. Inaccuracies in the coding of physician visits are estimated to account for up to 3 percent of the medical loss ratio in commer-cial plans and up to 1 percent in Medicaid plans. Fraud accounts for annual losses of more than $90 billion. All of this adds up to increased post-payment payer audits and a much greater risk of being selected for audit. Physicians must have a defensible medical record in order to avoid unfavorable audit results.
Further response: “I hope you are not audited. No one likes to be audited. But, this education is not about that. This education is to ensure that you are coding the highest correct level with confidence. It is an added bonus for me to know you’d pass an audit. Why not give me a few minutes so that you can easily avoid unfa-vorable outcomes?”
Chapter 2: Medical Necessity, The First 0–10 Minutes of Coaching TimeThe typical bell curve mindset should not be forefront to code selection. It is only helpful when making a determi-nation of how similar the billing pattern is among same specialty peers. A bell curve demonstrating that a physician is an outlier from the norm should only be an indication to

Teach E/M Coding to Your Doctor
Teach Evaluation & Management Coding to Your Doctor in One Hour www.aapc.com 3
look closer for a possible cause. Some trauma surgeons, for example, may only ever see Level 5 patients. Although the curve can be helpful in identifying coding patterns that are outside of the norm, code selection is always based solely on medical necessity as supported by documentation. The good news for physicians is there is no one better qualified to determine medical necessity than they are.
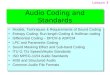
In its simplest terms, the five base levels of service can be visualized using the same logic in the Wong-Baker children’s pain chart.
Most physicians readily understand that Levels 3–5 are reserved for actively “sick” patients (Levels 1–3 in the hos-pital setting). The lower levels of service are reserved for patients with minor and/or well controlled conditions. It is tremendously helpful for physicians to have access to clini-cal examples in order to better define just how sick a patient needs to be (with conditions that the physician plans to treat) to support the specific use of a Level 3, 4, or 5.
What is confusing for some physicians is that a qualified coder, or a code optimizing electronic health record (EHR), may review a document and establish that a comprehensive high level service was rendered. However, it is important for physicians to remember that a medical review may find the same document lacking in demonstrable necessity. For example, a comprehensive history and physical may not be necessary to repeat on a two-week follow-up visit to recheck the patient’s normal blood pressure, even when doing so produces documentation that technically supports a higher level. The length of time before the next necessary follow-up visit is sometimes a very good indication of the level of medical necessity. For example, a level 5 may not be justifi-ably supported when the patient is healthy enough to not be asked to follow up sooner than six months.
Although a comprehensive service may be a physician’s personal art and style of practice it may not be consid-ered necessary and billable by a majority of peers. It is the necessity of the work versus the actual volume of work that should be coded and billed. In situations where a history and physical are not foremost, such as billing based on time, the criteria for documentation is quite different and limited only by the need for counseling and coordination of care. It is also limited in that 50 percent or more of the encounter required it. The American Medical Association’s (AMA) “CPT® Reference of Clinical Examples: Official
Scenarios for Correct Coding” can be a valuable resource. The AMA CPT® manual offers several clinical examples. The unbiased opinion of peers can be the most valuable with clinical examples available from a physician’s specialty organization being particularly ideal.
Helpful Links on Medical Necessity: Remember the rules that apply to the physician you are coaching are contained in the relevant laws, regulations, rulings, and contractual agreements of the physician. From a Medicare perspective the links below are helpful and are normally only superseded by state law if the state law is more stringent.
Medicare Claims Processing Manual, Chapter 12—Physicians/Nonphysician Practitioners, 30.6.1—Selec-tion of Level of Evaluation and Management Service A. Use of CPT® Codes
“Medical necessity of a service is the overarching criterion for payment in addition to the individual requirements of a CPT® code. It would not be medically necessary or appro-priate to bill a higher level of E/M service when a lower level of service is warranted. The volume of documentation
Medical Necessity “Faces” E/M Coding Scale
Preventive 1 2 3 4 5
**Adapted from Wong-Baker “Faces” Pain Rating Scale

Teach E/M Coding to Your Doctor
4 AAPC 1-800-626-CODE (2633) CPT® copyright 2011 American Medical Association. All rights reserved.
should not be the primary influence upon which a specific level of service is billed. Documentation should support the level of service reported. The service should be docu-mented during, or as soon as practicable after it is provided to maintain an accurate medical record…” www.cms.hhs.gov/manuals/downloads/clm104c12.pdf
1862 (a) (1) of the Social Security Act
“…Sec. 1862. [42 U.S.C. 1395y] (a) Notwithstanding any other provision of this title, no payment may be made under part A or part B for any expenses incurred for items or services—
(1)(A) which, except for items and services described in a succeeding subparagraph, are not reasonable and neces-sary for the diagnosis or treatment of illness or injury or to improve the functioning of a malformed body member,
(B) in the case of items and services described in section 1861(s)(10), which are not reasonable and necessary for the prevention of illness…”
www.ssa.gov/OP_Home/ssact/ssact.htm
Chapter 3: History Taking, The Next 11–20 Minutes of Coaching TimeYour goal is to have physicians feel confident that they will not under or over-code a visit after completing your train-ing. It is not always necessary in an initial one-hour train-ing to coach a physician on every “if/then” scenario. Doing so can sometimes become overwhelming and confusing. Ensuring you communicate key points is essential in order to maximize outcomes of the training. The entire focus of these next 10 minutes of coaching time is on history. The coach must be prepared to offer examples when asked.
Special circumstances to be watchful for in History include:
z If documentation shows that the provider is unable to obtain a history from the patient or other source (for example, “patient has Alzheimer’s and is a poor histo-rian and presents without a caregiver”, patient is “not conscious”, etc.). The overall level of medical necessity and the work of the provider are not penalized by the fact that the physician could not obtain a history from the patient. Note: If the provider summarizes addi-tional history supplied by a family member, or care giver, remember to credit this under MDM.
z ROS and PFSH taken from an earlier encounter can be reviewed and updated without complete re-docu-mentation. It is necessary for the provider to indicate the new status of the history and to leave an audit trail regarding where the original documentation is stored (indicate the date the original ROS and/or PFSH was documented). Physicians should be cautioned that, although a comprehensive service may be performed, a comprehensive service is not always medically neces-sary or billable. Unless the encounter is for a preven-tive medical history and physical, it is important to ensure physicians understand that the Chief Com-plaint (CC) must be readily identifiable. This is the first step in establishing medical necessity.
z The history (Hx) component is riddled with subjective terms. There are times when two separate audits of the same service may produce different results and neither party can be proven technically or medically wrong. Reviewer A may argue with Reviewer B that an ele-ment of (HPI) is a “timing” versus “duration”, or other element. Reviewer B may state that the documented “NKDA” constitutes an element of ROS or conversely an element of Past history.
{ Any free-form text is to some degree interpre-tive. This holds true with physicians’ notes. Since coding relies on counting subjective elements, the correct interpretation requires consistency, citable references, a logical argument and—ultimately—medical necessity.
The following is a guide to assist a physician in developing personal objectivity. With a known logic and solid argu-ment, the correct code for the medically necessary rendered services can prevail.
History of present illness: z Location: For example “chest” pain, sore “knee”, etc. Conversely, examples such as “COPD”, “Diabetes”, and “Hypertension” are not locations—these are “chronic conditions” Note: To credit chronic conditions use the 97 DG or one of the other elements of 95 HPI (such as Sever-ity: ie. CC = Return BP check, patient states it has been running 120/80 at Walgreen’s self service cuff.)
z Severity: A statement of degree or measurement regarding how bad it is… that it is improved, it is extreme pain, “BS is 200,” feeling “better,” pain is bad enough “that the patient can’t sleep,” etc.

Teach E/M Coding to Your Doctor
Teach Evaluation & Management Coding to Your Doctor in One Hour www.aapc.com 5
z Timing: A measurement of when or at what frequency; i.e. “intermittent,” “constant,” in the “morning,” lasted “5 minutes,” “occasional,” “on and off,” etc.
z Associated signs and symptoms: Any associated or secondary complaints.
z Modifying factors: Anything that makes the prob-lem better or worse, a factor that changes, improves, or alters the problem. For example, improved “with Tylenol,” worse “when standing,” better “when rest-ing,” “calms down when mother feeds her” Note: Medication may be a modifying factor when it changes, improves, or alters the problem. Otherwise, it is most often credited to PAST Hx. Some auditors will credit medications that were used in an unsuccessful attempt to modify the condition as a “modifying factor.”
z Context: What the patient was doing, the environ-mental factors/circumstances surrounding the com-plaint, for example, “while sleeping,” “MVA,” “slipped and fell,” after “eating peanuts,” “while dusting,” “when arguing with his wife,” etc.
z Duration: A measurement of time regarding when the complaint first occurred. For example, began “in childhood,” “since 1995,” first noticed “2 weeks ago”, “symptoms x 3 days,” etc.
z Quality: Any characteristic about the problem and/or expresses an attribute. For example: how it looks or feels; for example. “green” phlegm, “popping” knee, “dull” ache, “sharp” pain, “metallic” taste, etc.
Review of SystemsThe review of system (ROS) is an account of body systems obtained through a series of questions seeking to spot signs and/or symptoms that the patient may be experiencing or has experienced. This query is made by the physician and/or the staff (verbally or via patient intake forms) in order to best define the patient’s total problem. It includes defin-ing the need for expanded examination, testing, possible affected management options, etc. The review may be about the system(s) directly related to the problem(s) iden-tified in the HPI and/or additional body systems.
The ROS may be supplied in any format including but not limited to a separate patient intake or questionaire form. It is commonly interspersed within the HPI.
There is a fine line between the signs and symptoms that patient shares in the HPI and those obtained via the ROS. The ROS is a distinct review of the system. For example, If the documentation reads: “Patient states that her hip has
been painful” credit is not given to both the HPI “loca-tion” and to the musculoskeletal (MS) review of system. If, on the other hand, the documentation reads: “Patient states that her hip has been painful. She denies any other MS complaint,” there is a distinct component of both the HPI and also a separate MS review of system.
ROS elements typically reference signs and symptoms, of which both positive and negative comments are considered. Auditors commonly watch for indications of a question that has been asked by the physician and answered by the patient (for example, “pt denies fever,” “upon further ques-tioning the…”)
ROS should be medically necessary. It may be considered necessary to obtain a complete ROS when a patient pres-ents as an initial new patient. It may not be considered necessary to repeat a complete review on every follow up.
Please note the following are common examples only and do not constitute a complete list of all possible signs or symptoms.
z CONSTITUTIONAL: Patient answers about gen-eral constitutional signs or symptoms: Examples—fatigue, general appearance, exercise tolerance, fever, weakness, impaired ability to carry out functions of daily living, etc.
z RESPIRATORY: Patient answers about signs or symptoms of the respiratory system: Examples—cough, phlegm, wheeze, SOB, rapid or difficult breathing, chest pain on deep inhalation, etc.
z INTEGUMENTARY: Patient answers about signs or symptoms of the skin or breast: Examples—skin reac-tions to hot or cold, itching, rash, changes in scars, moles, sores, lesions, nail color or texture, changes in the color of the skin, bruising, breast pain, tenderness, swelling, lumps, nipple discharge or changes, etc.
z PSYCHIATRIC: Patient answers about signs or symptoms of the psychiatric condition: Examples—depression, stress, excessive worrying, suicidal thoughts, persistent sadness, anxiety, lost pleasure from usual activities, energy loss, physical problems not responding to treatment, restlessness, irritability, excessive mood swings, etc.
z EYES: Patient answers about signs or symptoms of the eye: Examples—use of glasses, discharge, itching, tear-ing or pain, spots or floaters, blurred or double vision, twitching, light sensitivity, visual disturbances, swell-ing around eyes or lids, etc.

Teach E/M Coding to Your Doctor
6 AAPC 1-800-626-CODE (2633) CPT® copyright 2011 American Medical Association. All rights reserved.
z GASTROINTESTINAL: Patient answers about signs or symptoms of the GI system: Examples—heart burn, indigestion or pain with eating, burning sensa-tion in the esophagus, frequent nausea and/or vomit-ing, changes in bowel habits or stool characteristics, abdominal swelling, diarrhea or constipation, use of digestive aids or laxatives, etc.
z NEUROLOGICAL: Patient answers about signs or symptoms of the neurologic system: Examples—numbness, tingling, dizziness, syncope or uncon-sciousness, seizures, convulsions, attention difficulties, memory gaps, hallucinations, disorientation, speech or language dysfunction, tremor or paralysis, inability to concentrate, sensory disturbances, motor disturbances including gait, balance, coordination, etc.
z ALLERGIC/IMMUNOLOGIC: Patient answers about signs or symptoms of the allergic/immunologic system: Examples—allergies to medicine, foods, envi-ronmental or other substances, frequent sneezing, hives and/or itching, chronic clear PND, conjunctivi-tis, chronic infections, etc.
z ENT: Patient answers about signs or symptoms of the ears, nose, and throat: Examples—Ears: sensitivity to noise, ear pain, vertigo, ringing in the ears, “full-ness” in the ears, ear wax abnormalities, etc. Nose: nosebleeds, post nasal drip, nasal drainage, impaired ability to smell, sinus pain, snoring, difficulty breath-ing, sinus infections, etc. Throat/Mouth: sore throat, mouth lesions, teeth sensitivity, bleeding gums, hoarseness, change in voice, difficulties swallowing, changed ability to taste, etc.
z GENITOURINARY: Patient answers about signs or symptoms of the GU system: Examples—painful urination, urine color, urinary patterns, hesitance, flank pain, decreased or increased output, dribbling, incontinence, frequency at night, genital sores, erectile dysfunction, irregular menses, toilet training or bed-wetting, etc.
z ENDOCRINE: Patient answers about signs or symp-toms of the endocrine system: Examples—BS readings at home, changes in height and/or weight, increased appetite or thirst, intolerance to heat or cold, etc.
z CARDIOVASCULAR: Patient answers about signs or symptoms of the cardiovascular system: Examples—heart rate, chest pain, tightness, numbness, palpita-tions, heart murmurs, irregular pulse, color changes in fingers or toes, edema, leg pain when walking, etc.
z MUSCULOSKELETAL: Patient answers about signs or symptoms of the MS system: Examples—cramps, twitching or pain, difficult walking, run-ning or participation in sports, joint swelling, redness or pain, joint deformities, stiffness, noise with joint movement, etc.
z HEMATOLOGIC/LYMPHATIC: Patient answers about signs or symptoms of the hemat/lymph systems: Examples—easy bruising, fevers which can come and go, swollen glands, night sweats, itching without rash, excessive bleeding, unusual bleeding, etc.
z “REST NEGATIVE”: For a complete systems review, most payers do not require individual documentation of each negative system reviewed. If there is distinct documentation of at least one or more ROS ele-ments and the physician indicates that “all others” or “remaining” systems are “negative,” credit should be given for all systems. For many auditors, documen-tation of the term “non-contributory” is equivalent to the term negative; however, physicians should be advised that this is interpretive. Some MACs will not allow credit for elements documented as “non-con-tributory”. Providers are encouraged not to use “non-contributory in their documentation. The following notation alone (without mention of at least one spe-cific ROS element) is not creditable for a full system review: ROS: negative.
Past, Family, and Social History z Past history: The patient’s past experiences with ill-nesses, operations, injuries and treatments, and medi-cations; If a patient presents for follow up on a chronic condition both HPI and Past History would be con-sidered. Positive findings of past diagnoses and current medication discovered on ROS would be considered.
z Family history: A review of medical events in the patient’s family, including age at death, diseases which may be hereditary or place the patient at risk.
z Social history: An age-appropriate review of past and current activities, for example occupation, smoking, alcohol use (ETOH), sexual activity, marital status, etc.
Some payers will not allow the use of “non-contributory” when used to describe elements of the history. A visual reference on the elements of history, and how they tie into a level of code can be very helpful when describing the his-tory component to physicians.

Teach E/M Coding to Your Doctor
Teach Evaluation & Management Coding to Your Doctor in One Hour www.aapc.com 7
History CodingNote: All three area of history must line up with a level of service, or default to the lowest of the three.
HPI:1.Location2. Quality3. Severity4. Timing5. Context6. Modifying Factors7. Duration8. Associated S&S
ROS:1. Constitutional2. Eyes3. ENMT4. Cardio5. Respiratory6. GI7. GU
8. MS 9. Skin10. Neuro11. Psych12. Endo13. Hemat/Lymp14. Allergic/Immuno
PFSH:1. Past2. Family3. Social Type
New PatientLEVEL
Est Patient LEVEL
Brief: 1–3 N/A N/A Problem Focused 1 2
Brief: 1–3 Problem Pertinent: 1 N/A Expanded Problem Focused
2 3
Extended: 4 or1997: status of 3 chronic conditions
Extended: 2–9 Pertinent: 1 Detailed 3 4
Extended: 4 or1997: status of 3 chronic conditions
Complete: 10Complete:3 or 2+ (Est.)
Comprehensive 4 or 5 5
*Please note: Rules discussed apply to New and Established outpatients visits.
Chapter 4: Exam, The Next 21–30 Minutes of Coaching TimeMost payers will allow the 1995 or 1997 Documentation Guidelines (DGs) to be used in code selection and a physi-cian should be familiar with both. Strictly from a coding perspective, the examination component is the least subjec-tive aspect of the documentation requirements with only two readily identifiable grey areas associated with the ’95 DGs. These two subjective areas are:
z The difference between an Expanded Problem Focused exam and a Detailed exam
{ The ‘95 DGs distinguish between the two levels only in that they both require at least 2 body areas and/or organ systems and that one is a “limited exam” and the other is “extended”.
z The definition of a Comprehensive single system exam { The ‘95 DGs distinguish only that the single system exam is “complete”.
To eliminate subjectivity, many practices choose to docu-ment according to the ‘97 DGs to ensure that coding is more easily defensible. Conversely, many insurers audit using the ‘95 DGs to ensure that audit findings are more easily defensible. This is because these two areas of the ‘95 documentation guidelines are subjective enough to often be interpretively more favorable, and only in some cases will the ‘97 DGs produce an allowable higher code.
A coach first must evaluate the nature of the specialty and the philosophy of the practice in order to determine which set of DGs to concentrate training. A coach should always focus training on the medical necessity of the exam. Never base training on getting to a higher code because of “just one more bullet”. Instead, ask a physician, “What would make you want to perform a more detailed exam for one patient versus another?” Also ask, “Would the majority of your peers agree with you that this was necessary?”
Prior to coaching, know the top five most commonly seen patient complaints. These are typically obtained by running or asking for billing reports, but because many specialists see the same types of complaints over and over again it is sometimes only necessary to ask the physician

Teach E/M Coding to Your Doctor
8 AAPC 1-800-626-CODE (2633) CPT® copyright 2011 American Medical Association. All rights reserved.
Body Areas: z Head/Face z Neck z Back, including spine z Abdomen z Genitalia, groin, buttocks z Chest/axillae/breast z Each extremity
Systems: z Constitutional z Eyes z Ears, nose, mouth and throat z Cardiovascular z Respiratory z Gastrointestinal z Genitourinary z Musculoskeletal z Skin z Neurologic z Psychiatric z Hematologic, lymphatic, immunologic
Number of Areas/Systems Examined Type
New Patient LEVEL Est. Patient LEVEL
1 PF 1 2
2 Limited EPF 2 3
2 Extended Detailed 3 4
8 (Systems only) Comprehensive 4 or 5 5
or the office manager. This is important so that you can be prepared during the coaching session to refer to clinical examples that help guide a physician in visualizing the dif-ference between levels of service for these complaints.
The 1995 Documentation GuidelinesA visual reference on the elements of 1995 exam, and how they tie into a level of code can be very helpful when describing the exam component to physicians.

Teach E/M Coding to Your Doctor
Teach Evaluation & Management Coding to Your Doctor in One Hour www.aapc.com 9
The 1997 Documentation GuidelinesUse the specialty specific pages of the 1997 Documentation Guidelines for Evaluation & Management Services (p. 14–45) as a visual example when coaching on these rules. It can be especially helpful to ask the physician to highlight the elements on the 97 DGs he or she would perform comparative to the physician’s five most common patient complaints.
System/Body Area Elements of Examination
Constitutional z Measurement of any three of the following seven vital signs: 1) sitting or standing blood pressure, 2) supine blood pressure, 3) pulse rate and regularity, 4) respiration, 5) temperature, 6) height, 7) weight (may be measured and recorded by ancillary staff)
z General appearance of patient (eg, development, nutrition, body habitus, deformities, attention to grooming)
Eyes z Inspection of conjunctivae and lids z Examination of pupils and irises (eg, reaction to light and accommodation, size, and symmetry)
z Ophthalmoscopic examination of optic discs (eg, size, C/D ratio, appearance) and posterior segments (eg, vessel changes, exudates, hemorrhages)
Ears, Nose, Mouth, and Throat
z External inspection of ears and nose (eg, overall appearance, scars, lesions, masses) z Otoscopic examination of external auditory canals and tympanic membranes z Assessment of hearing (eg, whispered voice, finger rub, tuning fork) z Inspection of nasal mucosa, septum, and turbinates z Inspection of lips, teeth, and gums z Examination of oropharynx: oral mucosa, salivary glands, hard and soft palates, tongue, tonsils, and posterior pharynx
Neck z Examination of neck (eg, masses, overall appearance, symmetry, tracheal position, crepitus)
z Examination of thyroid (eg, enlargement, tenderness, mass)
Respiratory z Assessment of respiratory effort (eg, intercostal retractions, use of accessory muscles, diaphragmatic movement)
z Percussion of chest (eg, dullness, flatness, hyperresonance) z Palpation of chest (eg, tactile fremitus) z Auscultation of lungs (eg, breath sounds, adventitious sounds, rubs)

Teach E/M Coding to Your Doctor
10 AAPC 1-800-626-CODE (2633) CPT® copyright 2011 American Medical Association. All rights reserved.
System/Body Area Elements of Examination
Cardiovascular z Palpation of heart (eg, location, size, thrills) z Auscultation of heart with notation of abnormal sounds and murmurs
Examination of: z carotid arteries (eg, pulse amplitude, bruits) z abdominal aorta (eg, size, bruits) z femoral arteries (eg, pulse amplitude, bruits) z pedal pulses (eg, pulse amplitude) z extremities for edema and/or varicosities
Chest (Breasts) z Inspection of breasts (eg, symmetry, nipple discharge) z Palpation of breasts and axillae (eg, masses or lumps, tenderness)
Gastrointestinal (Abdo-men)
z Examination of abdomen with notation of presence of masses or tenderness z Examination of liver and spleen z Examination for presence or absence of hernia z Examination (when indicated) of anus, perineum, and rectum, including sphincter tone, presence of hemorrhoids, rectal masses
z Obtain stool sample for occult blood test when indicated
Genitourinary MALE: z Examination of the scrotal contents (eg, hydrocele, spermatocele, tenderness of cord, testicular mass)
z Examination of the penis z Digital rectal examination of prostate gland (eg, size, symmetry, nodularity, tenderness)
FEMALE:Pelvic examination (with or without specimen collection for smears and cultures), including:
z Examination of external genitalia (eg, general appearance, hair distribution, lesions) and vagina (eg, general appearance, estrogen effect, discharge, lesions, pelvic support, cystocele, rectocele)
z Examination of urethra (eg, masses, tenderness, scarring) z Examination of bladder (eg, fullness, masses, tenderness) z Cervix (eg, general appearance, lesions, discharge) z Uterus (eg, size, contour, position, mobility, tenderness, consistency, descent or support) z Adnexa/parametria (eg, masses, tenderness, organomegaly, nodularity)

Teach E/M Coding to Your Doctor
Teach Evaluation & Management Coding to Your Doctor in One Hour www.aapc.com 11
System/Body Area Elements of Examination
Lymphatic Palpation of lymph nodes in two or more areas: z Neck z Axillae z Groin z Other
Musculoskeletal z Examination of gait and station z Inspection and/or palpation of digits and nails (eg, clubbing, cyanosis, inflammatory conditions, petechiae, ischemia, infections, nodes)
Examination of joints, bones, and muscles of one or more of the following six areas: 1) head and neck; 2) spine, ribs, and pelvis; 3) right upper extremity; 4) left upper extremity; 5) right lower extremity; and 6) left lower extremity. The examination of a given area includes:
z Inspection and/or palpation with notation of presence of any misalignment, asymmetry, crepitation, defects, tenderness, masses, effusions
z Assessment of range of motion with notation of any pain, crepitation, or contracture z Assessment of stability with notation of any dislocation (luxation), subluxation, or laxity z Assessment of muscle strength and tone (eg, flaccid, cog wheel, spastic) with notation of any atrophy or abnormal movements
Skin z Inspection of skin and subcutaneous tissue (eg, rashes, lesions, ulcers) z Palpation of skin and subcutaneous tissue (eg, induration, subcutaneous nodules, tightening)
Neurologic z Test cranial nerves with notation of any deficits z Examination of deep tendon reflexes with notation of pathological reflexes (eg, Babinski) z Examination of sensation (eg, by touch, pin, vibration, proprioception)
Psychiatric z Description of patient’s judgment and insightBrief assessment of mental status including:
z Orientation to time, place, and person z Recent and remote memory z Mood and affect (eg, depression, anxiety, agitation)
Content and Documentation Requirements
Level of Exam Perform and Document:
Problem Focused One to five elements identified by a bullet.
Expanded Problem Focused At least six elements identified by a bullet.
Detailed At least two elements identified by a bullet from each of six areas/systems
OR at least twelve elements identified by a bullet in two or more areas/systems.
Comprehensive Perform all elements identified by a bullet in at least nine organ systems or body areas and document at least two elements identified by a bullet from each of nine areas/systems.

Teach E/M Coding to Your Doctor
12 AAPC 1-800-626-CODE (2633) CPT® copyright 2011 American Medical Association. All rights reserved.
Chapter 5: Medical Decision Making, The Next 31–40 Minutes of Coaching TimeThe art of medical practice comparative to the subjective nature of the Medical Decision Making (MDM) compo-nent makes this aspect of code selection among the most frustrating for many physicians. This combined with the different and varied audit tools used by payers can be dif-ficult for some. The nature of the presenting problem and the medical necessity of the encounter is a physician’s best guide with regard to this component. Clinical examples are an important part of training. The most important aspect of coaching is to be prepared to discuss each of the sec-tions. Visual references are key with the physicians’ ques-tions driving the discussion.
The Number of Diagnoses and Management OptionsThe number of Diagnoses and Management options is based on the relative level of difficulty in making a diag-nosis and by the status of the problem (controlled versus worsening.). Usual indicators include the following:
z Problems that are new to the patient or that the physi-cian is seeing in this patient for the first time.
z Seeking additional work-up such as a consultant’s opinion.
z Ordering additional work-up such as diagnostic tests to confirm or to rule out the suspected diagnoses and/or differential diagnoses.
z Established problems for which the patient shows no improvement or have not responded as expected.
It is important to note that audit tools and coding references used by payers can be varied and different. For example, one audit tool may place a larger emphasis on the number of necessary differential diagnoses and list specific treatments and therapeutic options not mentioned in another. The majority of industry accepted audit tools are reported to pro-duce consistent findings greater than 95 percent of the time. However, as a precaution a coach should always contact the local MAC to request any and all available coding guides, specifically relative to E/M audit tools before conducting training with a billing physician. One area where MACs may have a different interpretation is what is considered “additional work-up”. Some MACs consider it tests per-formed during the same encounter and others consider it to be scheduled following the encounter. Check the guidance provided by the MAC in your region.
A visual reference and how it ties into a level of code can be very helpful when describing this aspect of code selec-tion. The chart below is one version. It is important to note that not all MACs use the same scoring system to determine MDM. For example, Trailblazer Health Enter-prises uses a different audit tool to determine MDM. You should use the guidance and audit tool (if available) from the MAC in your region when educating your providers.
Number of DX and Management Options
z Minor =1 each (max 2) z Est. stable/improved = 1 each z Est. worsening =2 each
z New problem, w/o workup =3 each (max 1) z New problem, w/workup=4 each
Example TypeNew or Established Outpatient LEVEL
Minimal: 1 point as totaled from above
Uncomplicated, non-infected insect bite Straightforward 1 & 2
Limited:2 points as totaled from above
Controlled HTN and tachycardia Low 3
Multiple:3 points as totaled from above
New patient with migraine headaches Moderate 4
Extensive:
4 + points as totaled from above
Patient seen today for f/u on OA knees and 1 year THR check. C/O knee pain. MRI ordered for possible meniscus tear. R/O symptom of osteoarthritis and sprain
High 5
Point system is from the Marshfield Clinic audit tool.

Teach E/M Coding to Your Doctor
Teach Evaluation & Management Coding to Your Doctor in One Hour www.aapc.com 13
Amount/Complexity of Data
One Point Each:Clinical Labs test ordered and/or reviewedCPT® Medicine Section Test—ordered and/or reviewedCPT® Radiology Section Test—ordered and/or reviewed Discuss patient results with performing or consulting physician Decision to obtain old records or additional history from other than patient
Two Points Each:Review and summarize data from old records or additional history gathered from other than patientIndependent interpretation of an image, tracing, specimen (not just review of the report)
TypeNew or Established Outpatient LEVEL
Minimal: 1 point as totaled from above Straightforward 1 & 2
Limited:2 points as totaled from above Low 3
Moderate:3 points as totaled from above Moderate 4
Extensive: 4 + points as totaled from above High 5
Point system is from the Marshfield Clinic audit tool.
Amount and/or Complexity of Data to be ReviewedThe amount and complexity of data to be reviewed is measured by the need to order and review tests and the need to gather information and data. Planning, scheduling, and performing clinical labs and tests from the CPT® Medicine and Radiology sections are indicators. The need to request old records or to obtain additional history from someone other than the patient (for example. family member, care giver, teacher, etc.) is credited in this section.
Also documented are discussions with the performing physician about unusual or unexpected patient results.
If a physician needs to make an independent visualization and interpretation (for example, MRI film, gram stain, etc.) and he or she is not billing separately for this service, it too is credited to this component of code selection.
A visual reference and how it ties into a level of code can be very helpful when describing this aspect of code selection. The chart below is one version:
Risk Significant Complications, Morbidity, and/or MortalityRisk is measured based on the physician’s determination of the patient’s probability of becoming ill or diseased, having complications, or dying between this encounter and the next planned encounter. The nature of the presenting problem and the urgency of the visit, comorbid conditions, as well as the need for diagnostic tests or surgery, are indicators of risk. Providers can usually relate to the
examples of presenting problems and the level of risk that applies to the encounter. A visual reference and how it ties into a level of code can be very helpful when describing this aspect of code selection. Refer to the CMS Table of Risk on page 14 of the ‘95 DGs.
Overall Risk (Table on next page)Any example listed from a row for any of the three columns will equal a level of risk.

1. P
rese
ntin
g P
robl
em(s
)2.
Dia
gnos
tic P
roce
dure
(s)
Ord
ered
3. M
anag
emen
t O
ptio
ns S
elec
ted
Type
New
or
Es
tabl
ishe
d
Out
patie
nt L
EVE
L
y
One
self-
limite
d or
min
or p
robl
em, e
g co
ld,
inse
ct b
ite, t
inea
cor
poris
y
Labo
rato
ry te
sts r
equi
ring
veni
punc
ture
y
Che
st x
-ray
s y
EKG
/EEG
y
Urin
alys
is y
Ultr
asou
nd, e
g, e
choc
ardi
ogra
phy
y
KO
H p
rep
y
Res
t y
Gar
gles
y
Elas
tic b
anda
ges
y
Supe
rfic
ial d
ress
ings
Stra
ight
- fo
rwar
d1
& 2
y
Two
or m
ore
self-
limite
d or
m
inor
pro
blem
s y
One
stab
le c
hron
ic il
lnes
s, eg
wel
l co
ntro
lled
hype
rten
sion
or n
on-in
sulin
de
pend
ent d
iabe
tes,
cata
ract
, BPH
y
Acu
te u
ncom
plic
ated
illn
ess o
r inj
ury,
eg,
cyst
itis,
alle
rgic
rhin
itis,
simpl
e sp
rain
y
Phys
iolo
gic
test
s not
und
er st
ress
, eg,
pul
mon
ary
func
tion
test
s y
Non
-car
diov
ascu
lar i
mag
ing
stud
ies w
ith
cont
rast
, eg,
bar
ium
ene
ma
y
Supe
rfic
ial n
eedl
e bi
opsie
s y
Clin
ical
labo
rato
ry te
sts
y
requ
iring
art
eria
l pun
ctur
e y
Skin
bio
psie
s
y
Ove
r-the
-cou
nter
dru
gs y
Min
or su
rger
y w
ith n
o id
entif
ied
risk
fact
ors
y
Phys
ical
ther
apy
y
Occ
upat
iona
l the
rapy
y
IV f
luid
s with
out a
dditi
ves
Low
3
y
One
or m
ore
chro
nic
illne
sses
with
mild
ex
acer
batio
n, p
rogr
essio
n, o
r sid
e ef
fect
s of
trea
tmen
t y
Two
or m
ore
stab
le c
hron
ic il
lnes
ses
y
Und
iagn
osed
new
pro
blem
with
unc
erta
in
prog
nosis
, eg,
lum
p in
bre
ast
y
Acu
te il
lnes
s with
syst
emic
sym
ptom
s, eg
, py
clon
ephr
itis,
pneu
mon
itis,
colit
is y
Acut
e co
mpl
icat
ed in
jury
, eg
head
inju
ry
with
brie
f los
s of c
onsc
ious
ness
y
Phys
iolo
gic
test
s und
er st
ress
, eg,
car
diac
stre
ss
test
, fet
al c
ontr
actio
n st
ress
test
y
Dia
gnos
tic e
ndos
copi
es w
ith n
o id
entif
ied
risk
fact
ors
y
Dee
p ne
edle
or i
ncisi
onal
bio
psy
y
Car
diov
ascu
lar i
mag
ing
stud
ies w
ith c
ontr
ast
and
no id
entif
ied
risk
fact
ors,
eg a
rter
iogr
am,
card
iac
cath
eter
izat
ion
y
Obt
ain
fluid
from
bod
y ca
vity
, eg
lum
bar
punc
ture
, tho
race
ntes
is, c
uldo
cent
esis
y
Min
or su
rger
y w
ith id
entif
ied
risk
fact
ors
y
Elec
tive
maj
or su
rger
y (o
pen,
per
cuta
neou
s or
endo
scop
ic) w
ith n
o id
entif
ied
risk
fact
ors
y
Pres
crip
tion
drug
man
agem
ent
y
The
rape
utic
nuc
lear
med
icin
e y
IV f
luid
s with
add
itive
s y
Clo
sed
trea
tmen
t of f
ract
ure
or d
isloc
atio
n w
ithou
t man
ipul
atio
n
Mod
erat
e4
y
One
or m
ore
chro
nic
illne
sses
with
seve
re
exac
erba
tion,
pro
gres
sion,
or s
ide
effe
cts o
f tr
eatm
ent
y
Acu
te o
r chr
onic
illn
esse
s or i
njur
ies t
hat
pose
a th
reat
to li
fe o
r bod
ily fu
nctio
n, e
g m
ultip
le tr
aum
a, a
cute
MI,
pulm
onar
y em
bolu
s, se
vere
resp
irato
ry d
istre
ss,
prog
ress
ive
seve
re rh
eum
atoi
d ar
thrit
is,
psyc
hiat
ric il
lnes
s with
pot
entia
l thr
eat t
o se
lf or
oth
ers,
perit
oniti
s, ac
ute
rena
l fai
lure
y
An
abru
pt c
hang
e in
y
neur
olog
ic st
atus
, eg
seiz
ure,
TIA
, w
eakn
ess,
or se
nsor
y lo
ss
y
Car
diov
ascu
lar i
mag
ing
stud
ies w
ith c
ontr
ast
with
iden
tifie
d ris
k fa
ctor
s y
Car
diac
ele
ctro
phys
iolo
gica
l tes
ts y
Dia
gnos
tic E
ndos
copi
es w
ith id
entif
ied ri
sk fa
ctor
s y
Disc
ogra
phy
y
Elec
tive
maj
or su
rger
y (o
pen,
per
cuta
neou
s or
endo
scop
ic) w
ith id
entif
ied
risk
fact
ors
y
Emer
genc
y m
ajor
surg
ery
(ope
n, p
ercu
tane
ous
or e
ndos
copi
c) y
Pare
nter
al c
ontr
olle
d su
bsta
nces
y
Dru
g th
erap
y re
quiri
ng in
tens
ive
mon
itorin
g fo
r tox
icity
y
Dec
ision
not
to re
susc
itate
or t
o de
-esc
alat
e ca
re b
ecau
se o
f poo
r pro
gnos
is
Hig
h5

Teach E/M Coding to Your Doctor
Teach Evaluation & Management Coding to Your Doctor in One Hour www.aapc.com 15
Determine Medical Decision MakingTwo of the three elements of MDM must be met or exceeded to determine the overall level of MDM.
Number of Dx and Management Options
Amount and/or Complexity of Data Risk Type of Decision Making
Minimal (1) Minimal or None (0–1) Minimal Straightforward
Limited (2) Limited (2) Low Low
Multiple (3) Moderate (3) Moderate Moderate
Extensive (4+) Extensive (4+) High High
Chapter 6: Putting It Together—The Last 41–50 Minutes of Coaching TimeTo help a physician learn the process of selecting a code, it is important to emphasize that the code is selected based on the nature of the presenting problem and the overall needs
of the patient. Based on this, the correct code is known to the physician prior to documentation. The second step is to document the encounter and the last step is to ensure that documentation supports the code the physician feels is most appropriate based on the patient’s needs. Providers must be trained that the volume of the documentation and the scoring of the E/M components alone do not justify the level of E/M. It is very easy, especially with EMRs, to
Pt Actively
“sick” or injured?
Pt w/ stable or inactive
Condition/s?
Pt w/ minor or self limited problem/s?
Start:A medically necessary, separately billable, evaluation and management service.
Dr. is treating (or Tx is impacted by all diagnoses counted )
No
No
Pt risk of life or limb between now &
next encounter?5Yes Yes
3 or 4
No
More than 1 problem?
2 or 3
Yes
No
Yes
1 or 2
More than 1problem?Yes
No
More than 2problems? 2 or 3
2 or 3
Yes Yes
No
Preventive Medicine
No
More than 3 problems? 4 or 5
3 or 4
Yes
No

Teach E/M Coding to Your Doctor
16 AAPC 1-800-626-CODE (2633) CPT® copyright 2011 American Medical Association. All rights reserved.
generate documentation to support higher levels of service. The question will be “was it medically necessary?” For example, a patient presents with otitis media. The patient will be given a prescription. The MDM for this patient is moderate according to the guidelines: new problem to the examiner-most likely without additional workup and moderate risk due to the prescription. Depending on the history and exam performed, the E/M level could be as high as a 99214. Most providers will agree that the nature of the presenting problem and services needed to treat otitis media would not support a 99214. The chart (on the previous page) is not all-inclusive and is not an endorsed coding tool. It should be used for discussion purposes only. However, a chart, like the one on the previous page, can be helpful to facilitate discussion during the coaching process (relevant to new outpatient codes).
Organizing Physician CommunicationSome physicians find it easier to learn coding when the coach cuts to the chase. Common questions by physicians may include the following:
z Can you just tell me what I need for a Level 3? z What makes it a Level 4? z When do I know it is a Level 5? z This patient has an ACL tear—what E/M level is that?
For this reason, many coaches start training from Chapter 6 earlier in the coaching session. Depending on the person-ality of the physician, getting right to it is a much better approach that often results in better questions during the duration of the training. You may find it helpful to perform this aspect of the training during the time frame discussed in Chapter 3 for the “next 11–21 minutes”, rather than to wait until the end.
Visual References and Practical ExamplesTake examples of correctly documented levels of service to illustrate what makes them correct. Level 3. Example Established Outpatient:
Incorrect: A patient on TOPROL-XL 50 mg qd comes in today for follow up on hypertension and tachycardia. BP 130/82, 80 BPM, S1 & S2 normal. Continue medication. Return x 3 months. (31 words)
Physician knows that documenting 1 HPI, 1 ROS, 2 Body Areas/Organ Systems will support this medically necessary level 3 visit
Correct: Patient on TOPROL-XL 50 mg qd in for follow up with controlled hypertension and tachycardia. Confirms palpitations have decreased. BP 130/82, 80 BPM, S1 & S2 normal. Continue medication. Return in 3 months. (33 words---Hint: Just 2 more words!)
The following page contains a quick reference code sheet that allows a coach to provide an easy visual reference on all three key components of documenting code selection.

How
to Effectively Teach Evaluation and Managem
ent in Under O
ne Hour, w
ritten by Stephanie Cecchini, CPC, CEMC, CH
ISP
© Copyright A
APC 2007-‐2012
26
Ex 95 DG Exam
MM
Body Areas:
head/face
neck
back
abdom
en
genitalia
chest/axillae/breast
each extrem
ity
Systems:
constitutional
eyes
EN
MT
cardiovascular
respiratory
gastrointestinal
genitourinary
musculoskeletal
skin
neurologic
psychiatric
hem
atologic, lymphatic im
munologic
Quick-‐Reference Code Sheet
New
PT: Default to the low
est LEVEL identified by the H
x, Ex, & M
DM
. Est PT: U
se the LEVEL identified by the best 2 of 3 on the H
x, Ex, & M
DM
(99211 not a Dr Code)
Hx H
istory ( 3 of 3) HPI:
location quality severity tim
ing
context m
od factor duration asso. S&
S
ROS:
constit eyes EN
MT
cardio respir
GI
GU
M
S skin
neuro psych endo hem
at/lymph
allerg/imm
uno
PFSH:
past fam
ily social
Type
New
O
ut Pt LEV
EL Est Pt LEV
EL
1 0
0 PF
1 2
1 1
0 EPF
2 3
4 or 1997:3 chronic 2-‐9
1 D
3 4
4 or 1997:3 chronic 10+
3 or2+ (Est.) C
4 & 5 5
MDM M
edical Decision M
aking ( 2 of 3)
Num
ber of Body Areas/System
s Examined
Type
New
Out Pt
LEVEL
Est. Out
Patient LEV
EL
1 PF
1 2
2-‐7 Limited
EPF 2
3
2-‐7 Extended D
3 4
8 (Systems only)
C 4 & 5
5
NUMBER O
F DX and
MANAGEM
ENT O
PTIONS
Minor =1 ea
. (max 2 points)
Est. stable/improved = 1 ea
.
Est. worsening =2 ea
.
New
problem(S), w
/o workup =3
New
problem, w
workup=4 ea.
AMOUNT/CO
MPLEXITY O
F DATA
: One Point Each:
Clinical Labs test ordered or reviewed
CPT® Medicine Section Test-‐ ordered/review
ed
CPT® Radiology Section Test-‐ ordered/review
ed
D
iscuss patient results w perform
ing / consulting Dr
Decision obtain old records or additional hx other than pt
Two Points Each:
Review/sum
marize data old records/add hx other than pt
Independent interpretation of an image, tracing, specim
en
OVERA
LL RISK: The quick reference guide below
shows excerpts from
the CMS Table of Risk.
*Remem
ber: Risk is based on the disease process anticipated between the present
encounter and the next one.
Type
New
or Est. O
ut Pt LEV
EL
1 1
Clinical testing/managem
ent examples: Venipuncture, X-‐ray, EKG
, U/A
, U/S, rest, superficial
dressings, elastic bandage, gargles, etc.
Presenting Problem Exam
ple: 1 minor / self lim
ited
SF 1 & 2
2 2
Clinical testing/managem
ent examples: Biopsy, pulm
onary function, barium enem
a, minor
surgery without risk factors, O
TC drugs, PT, OT, IV w
ithout additives, etc.
Presenting Problem Exam
ple: 1 –2 minor, 1 stable chronic / 1 acute uncom
plicated
L 3
3 3
Clinical testing/managem
ent examples: Stress tests, endoscopies, cardiovascular im
aging, centesis, closed Tx of Fx, Rx drug m
anagement, m
inor surgery with risk factors, m
ajor elective surgery w
ithout risk factors, therapeutic radiation tx, etc.
Presenting Problem Exam
ple: 1 chronic exacerbated / 2 stable chronic / New
Undiagnosed
with uncertain outcom
e / Acute w
ith systemic sym
ptoms / acute com
plicated injury
M
4
4
4
Clinical testing/managem
ent examples: Cardiovascular im
aging with risk factors,
endoscopies with risk factors, discography, m
edication toxicity managem
ent, major surgery
with risk factors, em
ergency surgery with risk factors, etc.
Presenting Problem Exam
ple: 1+ chronic severely exacerbated / Illness or injury that poses a threat to life / A
brupt change in neurological status
H
5
Reprinted w
ith Permission: Q
uick Reference Code Sheet © Copyright 2006-‐2012 Stephanie Cecchini, CPC, CEM
C, CHISP

Teach E/M Coding to Your Doctor
18 AAPC 1-800-626-CODE (2633) CPT® copyright 2011 American Medical Association. All rights reserved.
Chapter 7: Final PointsBe aware of different learning styles and customize your approach to best serve the physician you are coaching.
1. Learning TypesBe prepared to adjust for different learning styles:
z Audio: { Learn best from listening to your instruction. { Give lots of verbal details and ask the physician to add to them.
{ Review forms together aloud. z Visual learners:
{ Skim the reference tool prior to starting so that the physician has a general understanding.
{ Use visual reference forms continuously during coaching.
{ Use highlighter pens in different colors to make different points.
{ Eye contact is important. z Kinesthetic:
{ Compare one of the physician’s notes with a quick reference form.
As you review it together: Ask the physician to circle salient points on note and highlight them on the reference form.
2. It is okay to say, “I don’t know”. No matter what you prepare for, a question will almost always come up you have not considered before. To some people, being a teacher—or a leader—means appearing as though you have all the answers. Any sign of vulnerability or ignorance is seen as a sign of weakness. Those people can make the worst teachers. Sometimes the best answer a teacher can give is, “I don’t know.” Instead of losing credibility, she gains trust, and that trust is the basis of a productive relationship.
Parker Palmer, longtime instructor and author of “The Courage to Teach: Exploring the Inner Landscape of a Teacher’s Life” (Jossey-Bass, 1997).
3. Follow a Strategy for Effective Communication z Sympathize with the physician’s mindset. Coding and billing affects a physician’s livelihood.
z Be prepared to overcome objections. z Know how to best organize coaching based on the personality type of the physician.
z Be aware of the time allotted to make your salient
points but flexible with questions. z Be willing to rearrange delivery of the information in order to answer questions.
z Address the physician’s concerns openly, directly and with respect.
z A physician may be frustrated; a good coach recog-nizes that these emotions are not personal.
4. Ensure Awareness of Medical Necessity as the Driver of Code Selection
z Empower the physician with the understanding that the nature of the presenting problem and the severity of the patient’s illnesses are the most important factors of code selection.
z The physician’s medical training makes him or her an expert in determining medical necessity and in recog-nizing the most proper code. Clinical examples spe-cific to a specialty correlated to proper code selection are valuable to demonstrate this concept to physicians. Especially when they are customized to the types of patients/conditions the physician most often sees.
z Documentation is not the key to code selection—medical necessity is. The key lies with how “sick” a patient is, and what service was needed and rendered.
z If medical necessity is the key, documentation can be thought of as the lock. Documentation is the most powerful (and sometimes only) evidence of medical necessity. Nothing can be supported without it.
5. The Three Key Components of History, Exam, and Medical Decision Making and Selecting a Level of Service
z Proper documentation is not always clinically intui-tive, training focuses on what aspects of documenta-tion are important in order to support the needed and rendered service.
z It is not always necessary in an initial one-hour train-ing to coach a physician on every technical term (for example, a “detailed” exam). Many physicians find it easier instead to refer to the outcome documentation (for example, a “Level 4 established patient exam”). Anything that a coach can do to prevent a physician from becoming overwhelmed is valuable. Bypassing details like some technical terms can make recall on salient points easier.
z Quick reference forms and visual examples are highly valuable and should be used specific to the physician’s specialty and practice for the greatest impact.

Teach Evaluation & Management Coding to Your Doctor in One Hour www.aapc.com 19
Practical Activity
Practical ActivityFor the following cases, review the accuracy of the code selected by the provider and determine talking points you would review with the provider.
Case 1CHIEF COMPLAINT: Follow-up cutaneous lupus.
HISTORY OF PRESENT ILLNESS/SUBJECTIVE: 36-year-old female who we follow for a newly diagnosed rash on her breasts, which turned out to be cutaneous lupus. She is doing much better after having increased her steroids. She does notice a bit of a rash under the left breast.
In reviewing her recent blood work I see that her sed rate was slightly high at 39 and her AST and ALT were slightly elevated at 51 and 102 respectively. She does have a leukocytosis possibly from the steroids and she is anemic at 11.3. Her C3 complement was high at 165 and her double-stranded DNA is negative. She continues to take Plaquenil 200 mg twice a day in addition to the steroids, which are approximately 40 mg now.
REVIEW OF SYSTEMS: Otherwise well. No other skin complaints. Her pregnancy is going well.
PHYSICAL EXAM: No apparent distress. Alert and oriented x 3. Patient is a pregnant woman with hyperpigmented patches on both breasts. There is a slight bit of erythema underlying the hyperpigmentation. There is only a slight indura-tion to some areas of the bilateral breasts.
ASSESSMENT/PLAN: Cutaneous lupus in the setting of SLE.
• Discontinuetopicalsteroidsatthispointastheymayputheratriskforthecandidaintertrigo,whichshehasunderthe left breast. For this we recommend nystatin ointment twice daily.
• Follow-upin2months.Weexplainedthatifshenoticestherednessonherbreastsisincreasingwewilladdthetopical steroid back, but possibly use something milder.
Code selected by provider: 99214
Code documented: ____________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
Key points to review with the provider: _______________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________

20 AAPC 1-800-626-CODE (2633) CPT® copyright 2011 American Medical Association. All rights reserved.
Practical Activity
Case 2Subjective: Patient presents to clinic today for multiple complaints.
1. He is here for follow-up of his hypertension. He has been doing well on his labetalol, is not having any difficulties. However, over the last week he has had an upper respiratory infection and has been taking Sudafed-based cold products. He has not taken his blood pressure at home since he has been sick.
2. He is having some trouble with his knees. Anytime he gets up to move, his knees are stiff in particular when he starts walking or going down stairs his knees ache. The more steps he does, the better this becomes. It is more of an ache and stiffness than actual pain.
3. He was given a letter stating that his blood sugar was elevated. He should come in to discuss diabetes.
4. Next issue is he has a rash on his scalp that he has used special shampoo for in the past. This has helped somewhat but has never resolved completely. He would like this looked at also today.
PFSH: No changes since last visit
Objective: Today, respirations 18. Pulse is 92. Blood pressure is 150/88. This is on Sudafed. Temp is 99. Weight is 164. Height 68-1/2 inches. In general, this is a 60-year-old obese male, very pleasant, here with his wife, who has slight nasal congestion in the office today. Skin is warm and moist. General: Sclerae are white. Examination of the feet noted to have some thickening and scaling with some calluses noted. Sensation is intact with good vascular supply. There is no discol-oration noted. This is mainly between the toes and the dorsum of the foot distally. Heart was regular rate and rhythm. Lungs are clear to auscultation. No wheezes, rhonchi or rales. Knees noted to have X-rays that were done in the beginning of the year that shows arthritis in both knees. Examination of the scalp revealed multiple patches, scaliness and flaky skin that are in circular areas more prominent on the edge of the circle with some central clearing. A Wood’s lamp was used and noted that these areas fluoresced.
Assessment/Plan:
1. Hypertension slightly elevated today but patient has been taking Sudafed. Patient was instructed to avoid all pseudoephedrine and we will recheck this in a month.
2. Diabetes mellitus. This is a new diagnosis for him. We will send him for diabetic management and we will start him on Glucophage 500 mg twice a day. We will also get a hemoglobin A1c and microalbumin to creatinine ratio, basic metabolic and CBC today.
3. Bilateral osteoarthritis of his knees. We will send him to Dr. O (orthopaedic) for a further evaluation.
6. Tinea capitis. We will give him some Diflucan for 4 weeks to see if this clears it up. If this continues to be a problem, may need to do scraping or a biopsy.
Code selected by provider: 99212
Code documented: ____________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
Key points to review with the provider: _______________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________

Teach Evaluation & Management Coding to Your Doctor in One Hour www.aapc.com 21
Practical Activity
Case 3CHIEF COMPLAINT: Fever
PRESENT ILLNESS: The patient is a 2-year-3-month-old female with less than 1 day of a high fever with decreased appetite. There has been no vomiting or diarrhea. Parents are unaware of any cough.
CURRENT MEDICATIONS: Tylenol 160 mg q.4 h. per infant Tylenol drops.
ALLERGIES: NONE.
IMMUNIZATIONS: Up-to-date.
REVIEW OF SYSTEMS: As per HPI. Rest of review of systems reviewed and negative.
PAST, FAMILY, SOCIAL HISTORY: The patient is not exposed to second hand cigarette smokeor sick contacts.
PHYSICAL EXAMINATION: CONSTITUTIONAL: Vital Signs: Pulse: 160. Resp: 28. Temp: 104.7 at triage rectally. 02 sat: 99% on room air. GENERAL APPEARANCE: The child is well hydrated, well nourished and alert. Physical develop-ment and nutrition are normal for the patient’s stated age. HEENT: Normocephalic, atraumatic. Pupils equal, round reac-tive to light. Conjunctivae clear, ears somewhat injected to tympanic membranes. No overt otitis media is noted. Auditory canals are clear bilaterally. Nares wet with clear rhinorrhea. Throat reveals bi tonsillar enlargement with scant exudate noted. No viral vesicles are noted. Airway is patent. Palate symmetric. Tongue midline. Neck is supple without meningismus, mass, thyromegaly, lymphadenopathy. RESPIRATORY; Equal chest wall excursion. There are no intercostals retractions or the use of accessory muscles. Breath sounds are clear and symmetrical. There are no wheezes, rales or rhonchi. CARDIOVASCU-LAR: Regular rate and rhythm. No murmurs are heard on auscultation of the heart. GASTROINTESTINAL: Abdomen is nondistended. Positive normoactive bowel sounds, soft, nontender without mass, megaly or CVA tenderness, extremities. SKIN: Reveals no rash, petechia or purpura, neurologic. NEUROLOGIC; Movements are smooth and symmetrical. Gross sensation is intact, MUSCULOSKELETAL: There are no signs of trauma to the extremities. Strength and tone are normal. No cyanosis, clubbing or edema. LYMPHATIC; No significant adenopathy noted. There are no petechiae noted.
EMERGENCY ROOM COURSE: The patient is seen examined. Ultimately assessed for discharge. The patient did receive Motrin 100 mg p.o.
IMPRESSION: Fever, Pharyngitis.
MEDICAL DECISION MAKING: It is apparent that the patient can be discharged home given adequate antipyresis as well as antibiotic coverage. Fluids should be pushed. Discussion was held between myself and parents regarding avoiding tepid bath therapy and to using open air therapy by way of convection heat loss.
DISPOSITION: The patient is discharged home. Prescription of Zithromax suspension is provided for antibiotic coverage over the next 5 days. Parents are advised to use Tylenol and/or Motrin for fever. Fluids should be pushed. Follow-up should occur with primary pediatrician. The patient is welcome to be returned if worse.
CONDITION ON DISCHARGE: Stable.
Code selected by provider: 99284
Code documented: ____________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
Key points to review with the provider: _____________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________

22 AAPC 1-800-626-CODE (2633) CPT® copyright 2011 American Medical Association. All rights reserved.
Practical Activity
Case 4ADMISSION DATE: 1/16/12
CHIEF COMPLAINT: HISTORY OF PRESENT ILLNESS: This is a 78-year-old Caucasian woman with history of coronary artery disease, diabetes meliitus type II, hypertension, and dementia who presented to the emergency room late last night after experiencing some shortness of breath at home. According to the family, patient was not able to move out of bed but, otherwise, was alert and oriented. Daughter also noted some wheezing with shortness of breath at home. Patient denies any chest pain, nausea or vomiting that was associated with this shortness of breath. She denies any fevers or chills. No headaches or dizziness.
SOCIAL HISTORY: She does not drink or smoke. She is married, and her husband lives with her.
She has a family support with regards to her daughters who live close by.
FAMILY HISTORY: Mother had a stroke at 91, father at 66. Sister died of diabetes.
PHYSICAL EXAMINATION:
GENERAL: She is well developed and alert and oriented.
VITAL SIGNS: Temperature is 96.8. Blood pressure is 150/102, irregularly irregular pulse of 148. Respiratory rate is 20. Pulse ox is 97% on room air.
HEENT: Pupils equal, round and reactive to light. Extraocular movements are intact. Oral and nasopharynx clear.
NECK: No bruits. No JVD.
LUNGS: Clear to auscultation bilaterally.
CARDIAC: Irregularly irregular. No murmur was noted.
ABDOMEN: Soft, nontender and nondistended. Positive bowel sounds.
EXTREMITIES: No cyanosis, clubbing or edema. No calf tendemess.
NEURO: Cranial nerves II–XII are grossly intact with no focal deficits. Deep tendon reflexes are 2+/2+ in all four extremities.
HISTORY AND PHYSICAL EXAMINATION
LABS: Results are as follows: White count is 15.4. Hemoglobin is 13.2. Hematocrit is 40.1. Platelet count is 346. Neutro-phil percentage is 75%, lymphocytes 19%. Chemistry: Sodium 144, potassium 4.2, chloride 106, carbon dioxide 20, BUN 16, creatinine 1, glucose 272, calcium 8.9. Total creatinine kinase is 60. Troponin I is less than 0 03, Brain natriuretic pep-tide is 376. Her PT is 13.5, INR 1.3. Urine is yellow, clear, pH of 5.5, specific gravity less than or equal to 1.030, protein greater than or equal to 300, negative glucose, negative ketones, small occult blood, negative nitrates, bilirubin, negative leukocyte esterase, EKG shows atrial fibrillation with rapid ventricular response. She has what seems to be mild pulmonary edema on preliminary read of chest X-ray. I will await radiologist’s reading.

Teach Evaluation & Management Coding to Your Doctor in One Hour www.aapc.com 23
Practical Activity
IMPRESSION/PLAN:
1. Mild congestive heart failure. Admit patient. We will monitor for now. Patient did receive some Lasix in the emergency room.
2. New onset atrial fibrillation with rapid ventricular response. Patient was given Cardizem and Lopressor. We will wait to see the results. We will go ahead and re-consult Dr. for her atrial fibrillation and new onset congestive heart failure.
3. Diabetes. We will continue her Glucophage and place on sliding scale insulin.
4. Hypertension. We will continue her metoprolol, Cardizem and benazepril.
Long-term anticoagulation. Warfarin will be kept on hold until we get recommendations from the cardiologist.
Code selected by provider: 99223
Code documented: ____________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
Key points to review with the provider: _______________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________

24 AAPC 1-800-626-CODE (2633) CPT® copyright 2011 American Medical Association. All rights reserved.
Practical Activity
Case 57-year-old child presents for headaches. States has been going on 1 month to 6 weeks at least 1x weekly, bi-temporal. Last month has been complaining of headaches. Happens more at nights. No fever; no other symptoms; sleeps normal; appetite normal. + nausea sometimes; no emesis; no h/o motion sickness.
ROS: Constitutional; Neuro; all others negative
Wt: 50 lbs; BP 110/70
Exam:
General: Normal,
Eyes: PERRL, EOMI, fundi wnl
Nose: Normal
Moutht/throat: Normal
Neuro: nl speech, nl gait, CNII–XII grossly intact, nl finger to nose, negative rhomberg. can balance on 1 foot, nl head to toe, 3+ sm reflexes
Assessment: probably migraines, h/o HA triggers
Code selected by provider: 99204
Code documented: ____________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
Key points to review with the provider: _______________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________

Teach Evaluation & Management Coding to Your Doctor in One Hour www.aapc.com 25
Practical Activity
Case 6S: Patient returns for follow up of her rheumatoid arthritis.
O: Vital signs are recorded, lungs clear, cardiac exam regular rate and rhythm.
A: 1. Early aggressive form of rheumatoid arthritis, tolerating institution of ETANERCEPT. Disease is still quite active, however.
2. Risk for glucocorticoid-induced osteoporosis.
P: 1. Encouraged her to increase her dietary CALCIUM.
2. DXA is scheduled.
3. Hold off a few more weeks on tapering her PREDNISONE.
Code selected by provider: 99214
Code documented: ____________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
Key points to review with the provider: _______________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________

26 AAPC 1-800-626-CODE (2633) CPT® copyright 2011 American Medical Association. All rights reserved.
Practical Activity
Case 7S: R elbow has remained painful. Some difficulty sleeping.
O: Previous office notes, labs, problem list, Consults, medication sheet, PMH, FH, SH,
ROS reviewed.
CONS: 3VS X GEN X Marked swelling of elbow bursa.
1. Traumatic bursitis, not responding to conservative Rx.
Prepped with betadine and local anesthetic injected. 3 cc bloody transudate withdrawn and 1/2 cc Depomedrol with 1/2 cc Xylocaine injected. Local compression and follow prn.
Code selected by provider: 99213
Code documented: ____________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
Key points to review with the provider: _______________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________

Teach Evaluation & Management Coding to Your Doctor in One Hour www.aapc.com 27
Practical Activity
Case 8CHIEF COMPLAINT: Rash on back, Left big toe pain and swelling
HISTORY OF PRESENT ILLNESS:
This is a new 43-year-old female patient who is here complaining of a rash on her back. She states that this started on July 1, when she was camping up north. There has not been any change. She also had a rash on her left arm. She took some Medrol pak and the rash on the left arm is gone now, but the rash on her back did not change. It is itchy, and is now becoming dry. She had chickenpox in her childhood.
She is also complaining about left big toe pain and swelling. This has been going on for a year and a half. It is present all the time. She was seen by her primary care physician, who diagnosed her with gout. She was given medicine, which she took for one month, without any relief of her symptoms.
REVIEW OF SYSTEMS:
Ten systems were reviewed and were all negative, except as mentioned in the History of Present Illness.
PAST MEDICAL HISTORY: Noncontributory
PAST SURGICAL HISTORY: Noncontributory
ALLERGIES: To Sulfa
MEDICATIONS: None
SOCIAL HISTORY: The patient smokes one pack a day and drinks alcohol 2 to 4 times a week.
PHYSICAL EXAMINATION:
General: The patient is a 43-year-old female who is well-nourished and in no acute distress.
Vital Signs: Blood pressure is 110/69; pulse 67; temperature 98.1; pulse 72. Height is 5’ 5” and weight is 131.
Skin: The patient has a rash on the left lower back. The rash covers an area about 6 x 6 cm. There are some vesicles and also some erythema, as well as macules.
Lower Extremities: The left big toe has small to moderate edema of the metacarpophalangeal joint. There is also some inflammation going on. There is full range of motion, with some discomfort.
Neurovascular: Exam of the left foot is within normal limits.
ASSESSMENT: 1. Shingles
2. Arthritis of the left big toe
Code selected by provider: 99215
Code documented: ____________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
Key points to review with the provider: _______________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________

28 AAPC 1-800-626-CODE (2633) CPT® copyright 2011 American Medical Association. All rights reserved.
Practical Activity
Case 9Nurse Note: 43-year-old female presents today for productive cough and congestion, with sore throat, ear ache and head-aches. Very fatigued. Coughing up yellow phlegm. These symptoms have been resent for one week, OTC Tylenol Cold and Alka Seltzer with little effect.
SubjectiveCC: Patient presents with upper respiratory infection.
HPI: Congestion, cough, earache, ear fullness/pressure, fever, headache, nasal discharge, sore throat and swollen glands, denies sinus pain.Cough: Described as barking cough. Cough is productive of yellowish sputum.Fever: Temperature reported to be warm to touch, per parent/guardian, comes and goes.Sore throat: Described as scratchy, raw this am.
ROS:Const: Reports loss of appetite, body aches, chills, fatigue and fever. General health stated as good.
ENMT: Reports congestion/fullness of the ears bilaterally. Reports congestion, nasal discharge and sinus pain. Reports sore throat.
CV: Reports chest tightness, but denies palpitations.
Resp: Reports cough and congestion, but denies wheezing.
GI: Denies nausea and vomiting.
Current Meds:
Allergies: NKDA
PMH:Health Maintenance:Blood Test—(2/2006)Bone Density Test—noneColonoscopy—yearsDT—unknownDental—(11/2007)Eye Exam—(9/2007)Mammogram—nonePelvlc/Pap Exam—(9/2007)Physical Exam—(9/2007)Flu Vaccine—(11/2007)Pneumovax—noneChildhood Illnesses: Chickenpox, Measles, Tonsillitis, Strep Throat
Surgeries: Total hysterectomy—(1995) Appendectomy—(1990) Cholecystectomy—(2006) Knee Surgery—(1980) Assistive Devices: Wears glasses.
Reviewed and updated.

Teach Evaluation & Management Coding to Your Doctor in One Hour www.aapc.com 29
Practical Activity
FH: Father: Deceased due to MI—(1999); Prostate Cancer. Mother: Deceased due to Arthritis; Lung Disease—(age 57 Years). Reviewed and updated.
SH: Martial status: Married. Lives with spouse. The home is not smoke free. Household pets include a dog. The patient does not have an advance directive. No history of abuse.
Personal Habits: Cigarette Use: Current Cigarette Smoker 1/2 Pack Daily. Alcohol: Rare. Drug Use: Denies Drug Use. Daily Caffeine: Consumes on average 1 pot of coffee per day. Consumes on average 1 soda per day. Consumes on average 1 cup of tea per day. Reviewed and updated.
ObjectiveBP: 130/84 Pulse: 80 T: 97.7 Resp: 18 Ht: 62” 5’2” Wt: 1381b 2oz BMI: 26.3 LMP: hyster
Exam:Const: Appears appropriate for age, healthy and well developed.Head/Face: Palpation reveals no frontal or maxillary sinus tenderness.ENMT: Auditory canals normal. TM’s Intact and middle ear well aerated. Congestion of the nasal mucosae. Oral mucosa: pink, smooth and moist. Posterior pharynx shows redness, but no exudate or irritation.Neck: Supple and symmetric. Palpation reveals no swelling or tenderness.Resp: Chest expansion is adequate bilaterally and symmetrical. Respiration rate is normal. No use of accessory muscles noted. No intercostal retraction. No wheezing. Auscultate mildly decreased airflow. Lungs are clear bilaterally.
CV: Rate is regular. Rhythm Is regular.Lymph: No visible or palpable cervical lymphadenopathy.Skin: Skin is warm and dry.
Assessment #1: Bronchitis Acute
Plan for #1: Comments: Push fluids and rest.
Med Current: Doxycycline Hyclate 100 mg 1 po bid for 10 days Proventil HFA 108 mcg/act 2 puffs qidMed New: Doxycycline Hyclate 100 mg 1 po bid for 10 days Proventil HFA 108 mcg/act 2 puffs qid
Lab: Annual Labs For Females Age 40
Assessment #2: Tobacco Use DisorderPlan for #2:Comments: Advised to quit smoking. She will most likely need a PFT, discuss at follow up.Lab: Annual Labs For Females Age 40Followup: Slip for annual labs and mammogram. She will follow up to review labs and have a Physical exam.
Code selected by provider: 99204
Code documented: ___________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
Key points to review with the provider: _____________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________

30 AAPC 1-800-626-CODE (2633) CPT® copyright 2011 American Medical Association. All rights reserved.
Practical Activity
Case 10Nurse Note: Patient is here with mom c/o bilateral ear aches, R is worse, sore throat. hurts to swallow and a sty in R eye.
Subjective:
CC: Earache, stye
HPI: Recurrent AOM. URI, no injury, exposure of her eye
ROS:
Const: Reports fever. General health stated as good.
Eyes: Denies visual disturbance.
ENMT: Reports pain of the ears bilaterally. Reports congestion.
CV: Denies chest pain and palpitations.
Resp: Denies cough. dyspnea and wheezing.
GI: Denies gastrointestinal symptoms.
GU: Denies urinary symptoms.
Skin: Denies rashes.
Current Meds: Loratadine 10 mg. Multivitamins
Allergies: NKDA
Qbjective
BP: 90/58 Pulse: 100 T: 97.5 Reap: 20 Wt: 73 Wt Prior: 69 as of 11/01 /07 Wt Oif: +4 Wt”lo: 89th
Exam:
Const: Appears well. No signs of apparent distress present.
ENMT: Auditory canals normal. Tympanic membranes are intact. Nasal mucosa is pink and moist.
Dentition is in good repair. Posterior pharynx shows no exudates, irritation or redness.
Neck: Palpation reveals no node on the anterior neck, on the posterior neck, swelling or tenderness.
Resp; Respiration rate is normal. No Wheezing. Auscultate good airflow. Lungs are clear bilaterally.
CV: Rate is regular.
Skin: Skin is warm and dry. Small Stye right lower eyelid
Assessment #1: 381.4 Otitis Media Acute Or Chronic Nonsuppurative
Plan for #1:
Zithromax 200 mg/5 ml 2 tsp qdx 3 days
ENT for recurrent URI/AOM
FlU if symptoms persist
Leiter-excuse School
Assessment #2: 373.12 Hordeolum Intemum
Plan for #2:

Teach Evaluation & Management Coding to Your Doctor in One Hour www.aapc.com 31
Practical Activity
Erythromycin 5 mg/gm righteye bidfor 1 week
Code selected by provider: 99213
Code documented: ____________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
Key points to review with the provider: _______________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________


Teach Evaluation & Management Coding to Your Doctor in One Hour www.aapc.com 33
Presentation
Teach E/M Coding to Your Doctor in One Hour
Presenter name, credentials
Agenda
– Set the Stage for Coaching: • Physician Concerns, Overcoming Objections
– 0-10 Minutes: Medical Necessity: Determine Clinical Examples– 11-20 Minutes: History Taking: HPI, ROS, PFSH– 21-30 Minutes: Exam, ‘95 Subjectivity and Medical Necessity– 31-40 Minutes: MDM, Number of Dx, Data, Risk– 41-50 Minutes: Put it together:
• Learning Types
2
Learning Types• Physician Note Example, Physician Form Example• Teaching Tips
– Conclusion

34 AAPC 1-800-626-CODE (2633) CPT® copyright 2011 American Medical Association. All rights reserved.
Presentation

Teach Evaluation & Management Coding to Your Doctor in One Hour www.aapc.com 35
Presentation
Concerns
Payments are important to physicians.
• The level of service coded is based on how sick a patient is and meeting documentation requirements.
• Payment and coding must be unrelated.
5
y g– They just need to be addressed by other
means, such as contract re-negotiations.
Concerns
Ambiguity frustrates physicians.
• The level of service coded is based on how sick a patient is and meeting documentation requirements.
• It can be subjective – “Within the next hour you’ll have the tools you need to
enjoy successful outcomes ”
6
enjoy successful outcomes.”

36 AAPC 1-800-626-CODE (2633) CPT® copyright 2011 American Medical Association. All rights reserved.
Presentation

Teach Evaluation & Management Coding to Your Doctor in One Hour www.aapc.com 37
Presentation
Overcoming Objections
I don’t have time for this!
– Add information • With cuts in fees from Medicare and private
insurers, many doctors must see more patients to maintain their incomes.
– You have less time
9
• This training takes less than an hour and may ultimately save you time (and money).
Overcoming Objections• No one is going to audit me!
– Ask questions! • Can you afford to be wrong?• How can you be sure you are right?
The Way it WAS The Way it IS$ claims in quantity = cost prohibited review
Outsourcing and technology = Cost of review
Hospital and Surgery Claims Auditsproduce high ROI
Pressure to collect and correct$20B+ in abusive E/M claims
E/M Claims are cost prohibitive to E/M Claims audits now produce
10
• Would you like to never under-code? • Would you like to not have to ever worry about it?
E/M Claims are cost prohibitive toAudit
E/M Claims audits now produce ROI

38 AAPC 1-800-626-CODE (2633) CPT® copyright 2011 American Medical Association. All rights reserved.
Presentation

Teach Evaluation & Management Coding to Your Doctor in One Hour www.aapc.com 39
Presentation
Determine Examples:Clinical examples: • AMA vignettes• Opinions by peers• Opinions by peers• The CMS Table of Risk• The physician’s work
– “Describe to me the most common patient complaint(s) you see…”
• Tip: Many times this will represent a level 3Wh t ld k d?
13
– What would make you more concerned?– What makes you decide how soon a patient should
return for a follow up visit or see a specialist?– What would your peers say?
Determine Examples:Give examples the physician will personally relate to and can expand on:
– Example Level 1: Patient with simple abrasion, dressed. F/U PRN
– Example Level 2: Patient returns for 4 year follow up visit hip replacement, no complaints
– Example Level 3: 14 year old with first degree ankle sprain, Rx rest and OTC meds
Ask questions:
-- You’re the medical expert: What other examples of injuries or illness fall in this level?
– Example Level 4: Patient with painful total hip 1 year post replacement, worsening x 6 months
– Example Level 5: Femur and Hip Fracture in 80 year old diabetic brought in from the parking lot after hit and run while walking in
-- Clinically, what makes this problem a level 4 instead of a level 3?
Examples are made for the purpose of discussion only on new patients and may not always support the level cited above *

40 AAPC 1-800-626-CODE (2633) CPT® copyright 2011 American Medical Association. All rights reserved.
Presentation
11-20: History Taking• Now that the physician is comfortable identifying a level of service, he or
she needs to learn what elements of service are needed in the documentation in order to support it.
• The history component has subjective aspects in both sets of guidelines– The DGs are just guidelines.
• There are multiple audit forms used in the industry to conform to the DGs but can also produce different outcomes.
– Marshfield Clinic model– TrailBlazers model
• A coach must assist a physician in developing his or her personal objectivity
15
• A coach must assist a physician in developing his or her personal objectivityso that a logical and solid argument can be made for the documentation and the correct use of a code.– This is accomplished by pointing out areas of subjectivity and special
circumstance.
Special Circumstance• Patient is unable to give a history.• (ROS) and (PFSH) History taken from an earlier encounter
– May not be medically necessary
• A comprehensive service may be performed and documented but …– A comprehensive service is not always medically necessary or billable.
• Unless Preventive, a Chief Complaint (CC) must be identifiable – This is the first step in establishing medical necessity.
• Subjective aspects…– Reviewer A may argue with Reviewer B that an element of (HPI) is a “timing”
versus “duration” or other (HPI) element. R i B t t th t th d t d “NKDA” tit t l t f
16
– Reviewer B may state that the documented “NKDA” constitutes an element ofROS or conversely an element of Past history.
– Any free-form text is to some degree interpretive. This holds true with physicians’ notes. Since coding relies on counting subjective elements, the correct interpretation requires consistency, citable references, a logical argument and - ultimately - medical necessity.

Teach Evaluation & Management Coding to Your Doctor in One Hour www.aapc.com 41
Presentation
HPI
• Be prepared to discuss examples of HPI and to answer questions butHPI and to answer questions but avoid excessive instruction.
• Location: For example “chest” pain, sore “knee,” etc. Conversely, examples such as “COPD,” “Diabetes,” and “Hypertension” are not locations - these are “chronic conditions” Note: To credit chronic conditions use the ‘97 DG or one
17
chronic conditions use the 97 DG or oneof the other elements of ‘95 HPI (such as Severity: i.e., CC = Return BP check, patient states it has been running 120/80 at Walgreen’s self service cuff. )
HPI• Severity: A statement of degree or measurement regarding how bad it is…
that it is improved, it is extreme pain, “Blood Sugar is 200,” feeling “better,” pain is bad enough “pt can’t sleep,” etc.
• Timing: A measurement of when or at what frequency; i.e., “intermittent,”Timing: A measurement of when or at what frequency; i.e., intermittent,“constant,” in the “morning,” lasted “5 minutes,” “occasional,” “on and off,” etc.
• Associated signs and symptoms: Any associated or secondary complaints.
• Modifying factors: Anything that makes the problem better or worse, a factor that changes, improves, or alters the problem. For example, improved “with Tylenol,” worse “when standing,” better “when resting,” “calms down when mother feeds her.”
18
when mother feeds her. – Subjectivity Alert: Medication may be a modifying factor when it changes,
improves, or alters the problem. Otherwise, it is most often credited to PAST Hx. Some auditors will credit medications that were used in an unsuccessful attempt to modify the condition as a “modifying factor.”

42 AAPC 1-800-626-CODE (2633) CPT® copyright 2011 American Medical Association. All rights reserved.
Presentation
HPI
• Context: What the patient was doing, the environmental factors/circumstances surrounding the complaint, for example, “while sleeping,” “MVA,” “slipped and fell,” after “eating peanuts,” “while dusting,” “when arguing with his wife,” etc.
• Duration: A measurement of time regarding when the complaint first occurred. For example, began “in childhood,” “since 1995,” first noticed “two weeks” ago, “symptoms x 3d,” etc.
• Quality: Any characteristic about the problem and/or expresses an attribute. For example: how it looks or feels; for example. “green”
19
phlegm, “popping” knee, “dull” ache, “sharp” pain, “metallic” taste, etc.
ROS
• The ROS may be supplied in any format: separate patient intake or questionnaire form within the HPIpatient intake or questionnaire form within the HPI.
• ROS elements typically reference signs and symptoms, of which both positive and negative responses are considered. Auditors commonly watch for indications “pt denies fever,” “upon further questioning the…”).
• ROS should be medically necessary.
20
– It may be considered necessary to obtain a complete ROS when a patient presents as an initial new patient.
– It may not be considered necessary to repeat a complete review on every follow-up visit.

Teach Evaluation & Management Coding to Your Doctor in One Hour www.aapc.com 43
Presentation
ROS• There is a fine line between the signs and symptoms that
a patient shares in the HPI and those obtained via the ROS.
– If the documentation reads: • “Patient states her hip has been painful since her fall last week.”
Documentation is HPI. – If, on the other hand, the documentation reads:
• “Patient states that her hip has been painful since her fall last week
21
• Patient states that her hip has been painful since her fall last week.– She denies any other musculoskeletal complaint.” There is
distinct documentation that shows the HPI and also a separate musculoskeletal review of system.
PFSH
• Past history: The patient's past experiences with illnesses, operations, injuries and treatments, and medications; If a patient presents for follow up on a chronic condition both HPI and Past History would be considered. Positive findings of past diagnoses and current medication discovered on ROS would be considered.
• Family history: A review of medical events in the patient's family, including age at death, diseases which may be hereditary or place the
22
patient at risk.• Social history: An age-appropriate review of
past and current activities, for example occupation, smoking, alcohol use (EtOH), sexual activity, marital status, etc.

44 AAPC 1-800-626-CODE (2633) CPT® copyright 2011 American Medical Association. All rights reserved.
Presentation
HxHPI:1.Location2. Quality3. Severity4. Timing
ROS:1. Constitutional2. Eyes3. ENMT
8. MS9. Skin10. Neuro11. Psych
5. Context6. Modifying Factors7. Duration8. Associated S&S
4. Cardio5. Respiratory6. GI7. GU
12. Endo13. Hemat/Lymp14. Allergic/Immuno
PFSH:1. Past2. Family3. Social Type
NewPatientLEVEL
EstPatient LEVEL
Brief:1
N/A N/A Problem Focused 1 2
Brief:1
Problem Pertinent:1
N/A Expanded Problem Focused
2 3
4 Extended: Pertinent:4or1997:status of 3 chronic
Extended:2
Pertinent:1
Detailed 3 4
Extended:4or1997:status of 3 chronic
Complete:10
Complete:3 or 2+ (Est.) Comp 4 or 5 5
HPI:1.Location2. Quality3 S i
ROS:1. Constitutional2 E
8. MS9 Ski
CC: headachePt states “I fell off my chair an hour ago and hit my head against the desk. I have a throbbing headache.” The patient states the pain is 8 out of 10. Patient denies any visual disturbances. Patient takes Zoloft 25 mg QD.
3. Severity4. Timing5. Context6. Modifying Factors7. Duration8. Associated S&S
2. Eyes3. ENMT4. Cardio5. Respiratory6. GI7. GU
9. Skin10. Neuro11. Psych12. Endo13. Hemat/Lymp14. Allergic/Immuno
PFSH:1. Past2. Family3. Social Type
NewPatientLEVEL
EstPatient LEVEL
Brief:1
N/A N/A ProblemFocused 1 2
Brief:1
Problem Pertinent:1
N/A Expanded Problem Focused
2 3
24
Focused
4or1997:status of 3 chronic
Extended:2
Pertinent:1 Detailed 3 4
Extended:4or1997:status of 3 chronic
Complete:10
Complete:3 or 2+ (Est.) Comp 4 or 5 5

Teach Evaluation & Management Coding to Your Doctor in One Hour www.aapc.com 45
Presentation
21-30: Exam• Best results come when you focus on only one of the DGs .
– This avoids overwhelming the physician .• Know what documentation guidelines are best suited for your
physician.– Is there an internal policy mandating the use of one or the other?– Which set will this physician benefit the most from?
• Standards (and individual style) of practice often result in repeating patterns of exam for the same kind of complaints. – Take copies of the ’97 DG examination and ask the physician to
25
p p yhighlight the elements he or she would perform for his or her five most common complaints.
• Even if you are teaching the ’95 DGs, this gives the physician a visual idea of what’s required in documentation for a given level of service.
Subjectivity• The examination component is the least subjective aspect of the DGs.
• There are only two readily identifiable grey areas:– Expanded Problem Focused exam vs. Detailed exam
• Both require at least two body areas and/or systems with a “limited” or an “extended” exam. – Comprehensive single system exam
• A single system exam is “complete”.
• Ask questions to help a physician develop objectivity.– Was a more extended exam medically necessary?
26
y y– Would peers agree that more than a limited exam was documented?
• Be prepared to give an opinion. – You may want to refer to the ‘97 DGs for comparative value.

46 AAPC 1-800-626-CODE (2633) CPT® copyright 2011 American Medical Association. All rights reserved.
Presentation
Exam
NEVER base training on getting to a higher code because of “just one more bullet ”because of just one more bullet.
The level of service coded is based on how sick a patient is and meeting documentation requirements.
• Ask:– “What would make you want to perform a more detailed
exam for one patient versus another?”
27
p– “Would the majority of your peers agree with you that this
was necessary?”
95 DGsBody Areas: Head/Face Neck Back Abdomen Genitalia Chest/axillae/breast Each Extremity Systems: Constitutional
E Eyes Ears, nose, mouth and throat Cardiovascular Respiratory Gastrointestinal Genitourinary Musculoskeletal Skin Neurologic Psychiatric Hematologic, lymphatic immunologic
Number of Areas/Systems Examined Type New Patient LEVEL Est. Patient LEVELExamined Type New Patient LEVEL Est. Patient LEVEL
1 PF 1 2
2‐7 LimitedEPF 2 3
2‐7 ExtendedDetailed 3 4
8 (Systems only) Comprehensive 4 or 5 5

Teach Evaluation & Management Coding to Your Doctor in One Hour www.aapc.com 47
Presentation
95 DGsBody Areas: Head/Face Neck Back Abdomen Genitalia Chest/axillae/breastSystems: Constitutional Eyes
BP 120/80. The patient’s gait isnormal. Some swelling noted on
the lateral side of her head. Eyes: PERLA Neck: supple
Ears, nose, mouth and throat Cardiovascular Respiratory Gastrointestinal Genitourinary Musculoskeletal Skin Neurologic Psychiatric Hematologic, lymphatic immunologic
Number of Areas/Systems Examined Type New Patient LEVEL Est. Patient LEVEL
1 PF 1 2
2‐7 LimitedEPF 2 3
2‐7 ExtendedDetailed 3 4
8 (Systems only) Comprehensive 4 or 5 5
31-40: MDM
• Different audit forms vary dramatically in this component and may produce different codesand may produce different codes.– Before coaching, obtain the audit form used by the physician’s
local Medicare Administrative Contractor (MAC).
• Code selection is based on the relative level of difficulty in making a diagnosis and by the status of the problem (controlled versus worsening.).
30
• The amount of work involved in reviewing the necessary data and the immediate risk of the patient are very important aspects of documentation.

48 AAPC 1-800-626-CODE (2633) CPT® copyright 2011 American Medical Association. All rights reserved.
Presentation
Number of Dx and Tx Options
‐Minor =1 each (max 2)‐ Est. stable/improved = 1 eachE t i 2 h‐ Est. worsening =2 each
‐ New problem, w/o workup =3 each (max 1)
‐ New problem, w workup=4 each
Example TypeNew or Established Outpatient LEVEL
Minimal: 1 point as totaled from above
Uncomplicated, non-infected insect bite
Straight-forward 1 & 2
Limited: 2 points as totaled from above
Controlled HTN andtachycardia
Low 3Multiple: 3 points as totaled from above
New patient with migraineheadaches
Moderate 4Extensive: 4 + points as totaled from above
Patient seen today for f/uon OA knees and 1 yearTHR check. C/O knee pain.MRI ordered for possiblemeniscus tear. R/Osymptom of osteoarthritisand sprain
High 5
Amount and Complexity of DataOne Point Each: Clinical Labs test(s) ordered and/or reviewed CPT® Medicine Section Test(s)- ordered and/or reviewed CPT® Radiology Section Test(s)- ordered and/or
reviewed Discuss patient results with performing or consulting
ph sicianphysician Decision to obtain old records or additional history from
other than patient Two Points Each: Review and summarize data from old records or
additional history gathered from other than patient Independent (2nd) interpretation (from another
physician) of an image, tracing, specimen (not just review of the report)
TypeNew or Established Outpatient LEVEL
Mi i l St i ht f dMinimal: 1 point as totaled from above
Straight-forward 1 & 2
Limited: 2 points as totaled from above
Low 3
Moderate: 3 points as totaled from above
Moderate 4
Extensive: 4 + points as totaled from above
High 5

Teach Evaluation & Management Coding to Your Doctor in One Hour www.aapc.com 49
Presentation
CMS TABLE OF RISKOverall Risk between planned encounters
Any example listed from a row below for any of the three columns will equal a level of risk.
1. Presenting Problem(s) 2. Diagnostic Procedure(s) Ordered 3. Management Options Selected TypeNew or Established Outpatient LEVEL
• One self-limited or minor problem, eg cold, insect bite, tinea corporis
• Laboratory tests requiring venipuncture• Chest x-rays• EKG/EEG• Urinalysis• Ultrasound, eg, echocardiography• KOH prep
• Rest• Gargles• Elastic bandages• Superficial dressings
Minimal 1 & 2
• Two or more self-limited or minor • Physiologic tests not under stress, eg, pulmonary function tests • Over the counter drugsproblems
• One stable chronic illness, eg, well controlled hypertension or non-insulin dependent diabetes, cataract, BPH• Acute uncomplicated illness or injury, eg, cystitis, allergic rhinitis, simple sprain
pulmonary function tests• Non-cardiovascular imaging studies with contrast, eg, barium enema• Superficial needle biopsies• Clinical laboratory testsrequiring arterial puncture• Skin biopsies
• Over-the-counter drugs• Minor surgery with no identified risk factors• Physical therapy• Occupational therapy• IV fluids without additives
Low 3
• One or more chronic illnesses with mild exacerbation, progression, or side effects of treatment• Two or more stable chronic illnesses• Undiagnosed new problem with uncertain prognosis, eg, lump in breast• Acute illness with systemic symptoms, eg, pyclonephritis, pneumonitis, colitis• Acute complicated injury, eg, head injury with brief loss of consciousness
• Physiologic tests under stress, eg, cardiac stress test, fetal contraction stress test• Diagnostic endoscopies with no identified risk factors• Deep needle or incisional biopsy• Cardiovascular imaging studies with contrast and no identified risk factors, eg arteriogram, cardiac catheterization• Obtain fluid from body cavity, eg, lumbar puncture thoracentesis culdocentesis
• Minor surgery with identified risk factors• Elective major surgery (open, percutaneous or endoscopic) with no identified risk factors• Prescription drug management• Therapeutic nuclear medicine• IV fluids with additives• Closed treatment of fracture or dislocation without manipulation
Moderate 4
j y puncture, thoracentesis, culdocentesis p
• One or more chronic illnesses with severe exacerbation, progression, or side effects of treatment• Acute or chronic illnesses or injuries that pose a threat to life or bodily function, eg multiple trauma, acute MI, pulmonary embolus, severe respiratory distress, progressive severe rheumatoid arthritis, psychiatric illness with potential threat to self or others, peritonitis, acute renal failure• An abrupt change inneurologic status, eg, seizure, TIA, weakness, or sensory loss
• Cardiovascular imaging studies with contrast with identified risk factors• Cardiac electrophysiological tests• Diagnostic Endoscopies with identified risk factors• Discography
• Elective major surgery (open, percutaneous or endoscopic) with identified risk factors• Emergency major surgery (open, percutaneous or endoscopic)• Parenteral controlled substances• Drug therapy requiring intensive monitoring for toxicity• Decision not to resuscitate or to de-escalate care because of poor prognosis
High 5
41-50: Put it together• Answer questions even if they are “out of order” with emphasis on:
– 1st Medical Necessity• This helps bring clinical relevanceThis helps bring clinical relevance
– 2nd Documentation Requirements
• Be prepared to have many questions fired at once:
– Can you just tell me what I need for a Level 3?– What makes it a Level 4?– When do I know it is a Level 5?– This patient has chest pain - what E/M level is that?
34
• “It all depends on how ‘sick’ the patient is” – Let’s review clinical examples so you know how to define that– Then let’s review this quick reference form so you can easily see what
documentation is necessary

50 AAPC 1-800-626-CODE (2633) CPT® copyright 2011 American Medical Association. All rights reserved.
Presentation
Learning TypesBe prepared to adjust for different learning styles:• Audio:
– Learns best from listening to your instruction. Give lots of verbal details and ask the physician to add to them– Give lots of verbal details and ask the physician to add to them.
– Review forms together aloud.
• Visual learners:– Skim the reference tool prior to starting so that the physician has a general
understanding.– Use visual reference forms continuously during coaching.– Use highlighter pens in different colors to make different points.– Eye contact is important.
35
• Kinesthetic:– Compare one of the physician's notes with a quick reference form
• As you review it together: Ask the physician to circle salient points on note and highlight them on the reference form.
Note
Established patient presents complaining of a frontal headache. The patient has no know seasonal allergies.
/Exam: BP 138/72 Pulse 72 Temp 97.1ENT: normalHeart: RRRLungs: CTAAbdomen: Soft
Impression:1. Headache-possible migraine. Patient scheduled for CT of the head. Azert
36
eadac e poss b e g a e at e t sc edu ed o C o t e ead e tsample given with a written script. Return to the office in 4 weeks.
2. HTN-refill on Lopressor3. Nasal Polyps4. Hyperlipidemia

Teach Evaluation & Management Coding to Your Doctor in One Hour www.aapc.com 51
Presentation
Form
99213
Teaching Tip• Be aware of the time allotted to make your salient points but be
flexible with questions. If f l tti ff– If you feel you are getting off course:
• “I’ll be happy to discuss that in detail with you. Let me first give you the general points you need so that we can make the best use of your time today.”
• Be willing to rearrange delivery of the information in order to answer questions.
• Address the physician’s concerns openly, directly, and with respect.A physician may be frustrated; a good coach recognizes these
38
• A physician may be frustrated; a good coach recognizes theseemotions are not meant personally.

52 AAPC 1-800-626-CODE (2633) CPT® copyright 2011 American Medical Association. All rights reserved.
Presentation
Teaching Tip• It is okay to say, “I don’t know.” • No matter what you prepare for, a question willNo matter what you prepare for, a question will
almost always come up that you have not considered before.
– To some people, being a teacher -- or a leader -- means appearing as though you have all the answers. Any sign of vulnerability or ignorance is seen as a sign of weakness. Those people can make the worst teachers.
– Sometimes the best answer a teacher can give is, “I don't k " I t d f l i dibilit h i t t d th t
39
know." Instead of losing credibility, she gains trust, and thattrust is the basis of a productive relationship.
– Parker Palmer, longtime instructor and author of “The Courage to Teach: Exploring the Inner Landscape of a Teacher's Life” (Jossey-Bass, 1997).
Conclusion• Empower the physician with the understanding that the nature of the presenting
problem and the severity of the patient’s illnesses are the most important factors of code selection.
– The physician’s medical training makes him or her an expert. Documentation must support the services rendered and the code• Documentation must support the services rendered and the codeselection.
• Sympathize with the physician’s mindset: Coding and billing affects a physician’s livelihood.
• Be prepared to overcome objections.• Know how to best organize coaching based on the personality type of the
physician.• Be aware of the time allotted to make your salient points but flexible with
questions.
40
• Be willing to rearrange delivery of the information in order to answer questions.• Address the physician’s concerns openly, directly and with respect. • A physician may be frustrated; recognize that it is not personal.

Teach Evaluation & Management Coding to Your Doctor in One Hour www.aapc.com 53
Presentation
Case Exercises
R i h id d f• Review the ten cases provided for proper code selection and indicate any deficiencies you would discuss with the provider. Also make note of any positive feedback for the provider.
41
p