Embed Size (px)
DESCRIPTION
TEKRARLAYAN GEBELİK KAYIPLARINDA AMPİRİK TEDAVİNİN SONUÇLARI. DOÇ. DR. A. GONCA İMİR YENİCESU CUMHURİYET ÜNİVERSİTESİ. Tanımlama. Tekrarlayan gebelik kayıpları (TGK) 20 hafta öncesinde, iki yada daha fazla gebelik kaybı olarak ifade edilmektedir. - PowerPoint PPT Presentation
Citation preview

TEKRARLAYAN GEBELİK TEKRARLAYAN GEBELİK KAYIPLARINDA AMPİRİK KAYIPLARINDA AMPİRİK TEDAVİNİN SONUÇLARITEDAVİNİN SONUÇLARI
DOÇ. DR. A. GONCA İMİR YENİCESUDOÇ. DR. A. GONCA İMİR YENİCESUCUMHURİYET ÜNİVERSİTESİCUMHURİYET ÜNİVERSİTESİ
24.04.2324.04.23

TanımlamaTanımlama• Tekrarlayan gebelik kayıpları (TGK) 20 Tekrarlayan gebelik kayıpları (TGK) 20
hafta öncesinde, iki yada daha fazla hafta öncesinde, iki yada daha fazla gebelik kaybı olarak ifade edilmektedir. gebelik kaybı olarak ifade edilmektedir.
The Practice Committee of the American Society for Reproductive Medicine. Definitions of infertility and recurrent pregnancy loss. Fertil Steril. 2008;89:1603
24.04.2324.04.23

PrevalansPrevalans
• Bir kez düşük % 15-40 Bir kez düşük % 15-40 • İki kez düşük %2-5 İki kez düşük %2-5 • Üç kez ardarda düşük %1 ‘den azdır.Üç kez ardarda düşük %1 ‘den azdır.
Christiansen OB. Evidence-based investigations and treatments of recurrent pregnancy loss.
Fertil Steril. 2005 Apr;83(4):821-39. 24.04.2324.04.23

24.04.2324.04.23
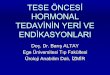
Kaplan-Meier plot showing percentage of women in the recurrentmiscarriage cohort who have had at least one live birth after firstconsultation by number of miscarriages before first consultation.(Lund et al. Recurrent miscarriage and prognosis for live birth.Obstet Gynecol 2012.) Practice Committee. Fertil Steril 2012.

EtiyolojiEtiyoloji• Genetik faktörlerGenetik faktörler• Endokrin faktörlerEndokrin faktörler• Otoimmun faktörlerOtoimmun faktörler• (Anti-Fosfolipid sdr,(Anti-Fosfolipid sdr,• Trombofili)Trombofili)• Anatomik faktörlerAnatomik faktörler• EnfeksiyonlarEnfeksiyonlar• İdiopatik İdiopatik
24.04.2324.04.23

EtiyolojiEtiyoloji• 1- 1- Genetik nedenler: Genetik nedenler: Parental yapısal ve Parental yapısal ve
gebelik ürününe ait kromozomal gebelik ürününe ait kromozomal bozukluklarbozukluklar
• 2- 2- Endokrin nedenler: Endokrin nedenler: Luteal faz defekti, Luteal faz defekti, Hipo/Hipertiroidi, D. Mellitus, PCOS, Hipo/Hipertiroidi, D. Mellitus, PCOS, HiperprolaktinemiHiperprolaktinemi
• 3- Enfeksiyona bağlı nedenler: 3- Enfeksiyona bağlı nedenler: CMV, CMV, M.Hominis, U.Urealyticum, T.Gondii, M.Hominis, U.Urealyticum, T.Gondii, Rubella, Coxackie, Herpetik viruslarRubella, Coxackie, Herpetik viruslar
24.04.2324.04.23

EtiyolojiEtiyoloji• 4- 4- Anatomik nedenler: Anatomik nedenler: Konjenital uterin Konjenital uterin
anomaliler, Asherman sendromu, anomaliler, Asherman sendromu, servikal yetmezlik, in utero DES servikal yetmezlik, in utero DES maruziyetimaruziyeti
• 5- 5- İmmunolojik nedenler: İmmunolojik nedenler: Otoimmun, Otoimmun, AlloimmunAlloimmun
• 6- 6- Trombofili: Trombofili: Kalıtsal, EdinselKalıtsal, Edinsel• 7- 7- Diğer: Diğer: Sigara, Alkol, Kimyasallar, Sigara, Alkol, Kimyasallar,
RadyasyonRadyasyon
24.04.2324.04.23

HeterojeniteHeterojenite• Gebeliğin farklı dönemlerinde etki Gebeliğin farklı dönemlerinde etki
eden etiyolojik faktörlerin farklı eden etiyolojik faktörlerin farklı olması nedeniyle gebelik kayıplarının olması nedeniyle gebelik kayıplarının preembryonik , embryonik ve fetal preembryonik , embryonik ve fetal dönem olarak ayrı ayrı sınıflanması ve dönem olarak ayrı ayrı sınıflanması ve çalışmaların bu şekilde planlanması çalışmaların bu şekilde planlanması önerilir. önerilir. Dawood FDawood F. . Recurrent miscarriage: anRecurrent miscarriage: an overview. Reviews in Gynaecological overview. Reviews in Gynaecological
Practice 2003;3:46-50.Practice 2003;3:46-50.
24.04.2324.04.23

• Günümüzde bilinen etiyolojik faktörler Günümüzde bilinen etiyolojik faktörler incelense bile TGK nedeniyle başvuran incelense bile TGK nedeniyle başvuran hastaların hastaların %50’sinde belirgin bir neden %50’sinde belirgin bir neden saptanamamaktadır. saptanamamaktadır.
• Ancak hiçbir tedavi uygulanmasa dahi Ancak hiçbir tedavi uygulanmasa dahi TGK hastalarının TGK hastalarının %50-70’inde canlı %50-70’inde canlı doğumla sonuçlanan başarılı gebelikler doğumla sonuçlanan başarılı gebelikler gerçekleşir. gerçekleşir.
24.04.2324.04.23

YÖNETİMYÖNETİM• Anamnez, obstetrik hikayeAnamnez, obstetrik hikaye• Antifosfolipid sendrom bulguları Antifosfolipid sendrom bulguları
araştırılmalıdır. araştırılmalıdır. • Tam bir FM ile uterus, serviks ve Tam bir FM ile uterus, serviks ve
vajen anomaliler için vajen anomaliler için değerlendirilmelidir.değerlendirilmelidir.
24.04.2324.04.23

24.04.2324.04.23

Tekrarlayıcı gebelik kayıplarında Tekrarlayıcı gebelik kayıplarında önerilen testlerönerilen testler
• *Açlık kan şekeri, TSH, prolaktin*Açlık kan şekeri, TSH, prolaktin• * HSG veya histeroskopi* HSG veya histeroskopi• * Parental karyotip incelemesi* Parental karyotip incelemesi• Trombofili taraması : Trombofili taraması : Aktive protein C rezistans oranı, Aktive protein C rezistans oranı,
Antitrombin III, Protein C ve S ölçümü?Antitrombin III, Protein C ve S ölçümü? Antifosfolilipid sendrom teşhisinde Antifosfolilipid sendrom teşhisinde
aCLA ve LAaCLA ve LA
24.04.2324.04.23

Genetik faktörler için, Genetik faktörler için, • Translokasyon taşıyıcılarıTranslokasyon taşıyıcıları• 35 yaş üzeri kadınlar35 yaş üzeri kadınlar• Daha önce aneuploid abort yaptığı Daha önce aneuploid abort yaptığı
bilinen çiftlerebilinen çiftlere PGD önerilebilir.PGD önerilebilir.
24.04.2324.04.23

TEDAVİTEDAVİ• Ampirik tedavi:Ampirik tedavi:• Kuramsal bir temele dayanmayan, Kuramsal bir temele dayanmayan,
deney ve tecrübe ile anlaşılmış deney ve tecrübe ile anlaşılmış olan (bilgi, bağıntı vb.)olan (bilgi, bağıntı vb.)
• Etki mekanizması bilinmeden, Etki mekanizması bilinmeden, sadece tecrübeyle belli bir sonucun sadece tecrübeyle belli bir sonucun elde edileceği bilinerek yapılan.elde edileceği bilinerek yapılan.
24.04.2324.04.23

TEDAVİTEDAVİ• Uterin ve servikal anomaliler Uterin ve servikal anomaliler
uygun cerrahi ile tedavi edilmelidir. uygun cerrahi ile tedavi edilmelidir. • Genetik testler teşvik edilmeli, Genetik testler teşvik edilmeli,
kromozomal bozukluk teşhiskromozomal bozukluk teşhis edilenlere genetik danışma edilenlere genetik danışma
verilmesi sağlanmalıdır.verilmesi sağlanmalıdır.
24.04.2324.04.23

Ampirik tedaviAmpirik tedavi• Antitrombotik tedaviAntitrombotik tedavi• *Heparin (DMAH), Aspirin*Heparin (DMAH), Aspirin• Levotiroxin tedavisiLevotiroxin tedavisi• Paternal lökosit Paternal lökosit • IVIGIVIG
24.04.2324.04.23

Ampirik tedaviAmpirik tedavi• Antitrombotik tedaviAntitrombotik tedavi• *Heparin (DMAH), Aspirin*Heparin (DMAH), Aspirin• Levotiroxin tedavisiLevotiroxin tedavisi• Paternal lökosit Paternal lökosit • IVIGIVIG
24.04.2324.04.23

Antithrombotic treatment for Antithrombotic treatment for recurrent pregnancy loss?recurrent pregnancy loss?
Greer IA. Antithrombotic treatment for recurrent pregnancy loss? Greer IA. Antithrombotic treatment for recurrent pregnancy loss? J Thromb Haemost 2011; 9: 302–305.J Thromb Haemost 2011; 9: 302–305.
• a prothrombotic phenotype, regardless a prothrombotic phenotype, regardless of specific heritableof specific heritable thrombophilia, thrombophilia, underlies RPL then it is logical to underlies RPL then it is logical to considerconsider a antithrombotic treatment for ntithrombotic treatment for unexplained RPL. unexplained RPL.
• AAss heparins have potentially beneficial heparins have potentially beneficial effects on trophoblast,effects on trophoblast, an effect an effect mediated through mechanisms other mediated through mechanisms other than anthan an anticoagulant effect is possible.anticoagulant effect is possible.
24.04.2324.04.23

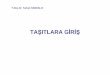
ALIFE TRIAL ALIFE TRIAL the Aspirin Combined withthe Aspirin Combined with
Low-Molecular-Weight Heparin and Aspirin Low-Molecular-Weight Heparin and Aspirin Alone in WomenAlone in Women with Recurrent with Recurrent
MiscarriageMiscarriageKaandorp SP, N Engl Jmed 2010; 362: 1586–96.Kaandorp SP, N Engl Jmed 2010; 362: 1586–96.
24.04.2324.04.23
Aspirin + nadroparin
Aspirin only
Placebo P value
No. ofwomen
97 99 103
Live birthno. (%)
67 (69.1) 61 (61.6) 69 (67.0) 0.52Relative risk(95% CI)
1.03 (0.85–1.25)
0.92 (0.75–1.13)
1.00

• Of the 364 women with recurrent miscarriage, who Of the 364 women with recurrent miscarriage, who werewere attempting to conceive, 299 became attempting to conceive, 299 became pregnant. The interventionpregnant. The intervention commenced at 6 commenced at 6 weeks gestation following the confirmation ofweeks gestation following the confirmation of a a viable pregnancy.viable pregnancy.
• The trial was halted prematurely when theThe trial was halted prematurely when the Data Data Safety Monitoring Board Safety Monitoring Board advised discontinuationadvised discontinuation because of futility.because of futility.
• Low dose aspirin combined with theLow dose aspirin combined with the LMWH LMWH nadroparin, and aspirin alone, did not improve livenadroparin, and aspirin alone, did not improve live birth rates compared to placebo in these women.birth rates compared to placebo in these women.
24.04.2324.04.23

SPIN Trial SPIN Trial (the Scottish (the Scottish Pregnancy Pregnancy
Intervention)Intervention)Clark P, Blood 2010; 115: 4162–7.Clark P, Blood 2010; 115: 4162–7.• This trial compared intensive pregnancy This trial compared intensive pregnancy
surveillance alone with an antithrombotic surveillance alone with an antithrombotic intervention, LMWH (enoxaparin), combined intervention, LMWH (enoxaparin), combined with low dose aspirin, in 294 women with a with low dose aspirin, in 294 women with a history of two or more RPL. history of two or more RPL.
• There was no reduction in pregnancy loss rate There was no reduction in pregnancy loss rate with antithrombotic intervention [odds ratio with antithrombotic intervention [odds ratio 0.91 (95%CI 0.52–1.59)] compared with 0.91 (95%CI 0.52–1.59)] compared with surveillance alone.surveillance alone.
24.04.2324.04.23

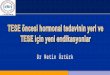
Table: Patients and outcome in the SPIN the Scottish Pregnancy Intervention Trial
24.04.2324.04.23
Characteristic
Anticoagulant group (n = 147)
Intensive surveillance group (n = 147)
Age (years)
31 (26–36) 32 (27–36)
N ‡ 1 previous live birth 67 (45.6%)
66 (44.9%)
No. of previous losses 2 (2–3)
2 (2–3)
No. with > 2 losses
66 (44.9%) 60 (40.8%)
BMI (Kg m 2 )
25.4 (21.8–29.0) 26.4 (23.1–32.4)
Current smoker
29 (19.7%) 25 (17.0%)
Gestation at randomization (weeks)
6 (6–7) 6 (6–6)
Multiple pregnancy
2 (1.4%) 3 (2.0%)
Pregnancy outcome
32 losses in 143 subjects (four subjects were lost to follow-up)
29 losses in 140 subjects (seven subjects were lost to follow-up)

• These data show that antithrombotic These data show that antithrombotic intervention should not be recommended for intervention should not be recommended for unexplained RPL in general. unexplained RPL in general.
• However, there may be specific groups such However, there may be specific groups such as those with an heritable thrombophilia, or as those with an heritable thrombophilia, or with three or more losses, or second with three or more losses, or second trimester losses that might benefit.trimester losses that might benefit.
Greer IA. Antithrombotic treatment for recurrent pregnancy loss? J Greer IA. Antithrombotic treatment for recurrent pregnancy loss? J Thromb Haemost 2011; 9 : 302–305.Thromb Haemost 2011; 9 : 302–305.
24.04.2324.04.23

• RPL and no identified thrombophilia.RPL and no identified thrombophilia. these these trials compared enoxaparin 20 mg day vs. trials compared enoxaparin 20 mg day vs. no treatmentno treatment or placeboor placebo in women idiopathicin women idiopathic recurrent miscarriages and reported recurrent miscarriages and reported higher rates of successfulhigher rates of successful pregnancy pregnancy outcome with LMWH. outcome with LMWH.
• However both had significantHowever both had significant methodologicalmethodological limitations such as lack of prospectivelimitations such as lack of prospective trial trial
registration and unclear blinding and thus registration and unclear blinding and thus may bemay be associated with significant bias. associated with significant bias.
Badawy AM, Badawy AM, J Obstet Gynaecol 2008; 28: 280–4.J Obstet Gynaecol 2008; 28: 280–4.• Fawzy M, Fawzy M, Arch Gynecol Obstet 2008; 278: 33–8Arch Gynecol Obstet 2008; 278: 33–8..
24.04.2324.04.23

Effectiveness of aspirin compare Effectiveness of aspirin compare with heparin pluswith heparin plus aspirin in aspirin in recurrent pregnancy loss recurrent pregnancy loss
treatment: A Quasitreatment: A Quasiexperimental studyexperimental study
N Ghasemi, Iran J Reprod Med Vol. 12. No. I. pp: 73-76, 2014N Ghasemi, Iran J Reprod Med Vol. 12. No. I. pp: 73-76, 2014• Background: Using aspirin, heparin, or both in women with Background: Using aspirin, heparin, or both in women with
unexplained recurrentunexplained recurrent miscarriage could be useful, because this miscarriage could be useful, because this problem might be initiated by thrombosisproblem might be initiated by thrombosis in decidual vessels. in decidual vessels.
• Materials and MethodsMaterials and Methods: : 520 women, who520 women, who had a history ofhad a history of unexplainedunexplained recurrent miscarriage. recurrent miscarriage. 250250 women were assigned to women were assigned to receive aspirin (80 mg daily) forreceive aspirin (80 mg daily) for two month before pregnancy and two month before pregnancy and after confirmation of a viable pregnancy until 36after confirmation of a viable pregnancy until 36 weeks of gestation weeks of gestation or receive aspirin plus heparin (5000 unit twice aor receive aspirin plus heparin (5000 unit twice a day) day) subcutaneously after confirmation of viable pregnancy until 4 weeks subcutaneously after confirmation of viable pregnancy until 4 weeks afterafter delivery. delivery.
• Conclusion: Live-birth rates did not different significantly Conclusion: Live-birth rates did not different significantly among the two studyamong the two study groups.groups.
24.04.2324.04.23

Efficacy of three different antithrombotic Efficacy of three different antithrombotic regimens on pregnancyregimens on pregnancy outcome in outcome in
pregnant women affected by recurrent pregnant women affected by recurrent pregnancy losspregnancy loss
A. Giancotti, A. Giancotti, The Journal of Maternal-Fetal and Neonatal Medicine, The Journal of Maternal-Fetal and Neonatal Medicine, 2012; 25(7): 1191–11942012; 25(7): 1191–1194
• Conclusion: Conclusion: For the For the congenital congenital thrombophilia thrombophilia we have studied we have studied physiologicalphysiological inhibitors of coagulation inhibitors of coagulation (antithrombin, protein C, protein S),(antithrombin, protein C, protein S), factor V factor V MutMut and factor II (G20210A) and factor II (G20210A) MutMut..
• For the For the acquired thrombophiliaacquired thrombophilia, we have , we have studied the presencestudied the presence of LA, ACA of LA, ACA and and plasma levels of Homocysteine.plasma levels of Homocysteine.
24.04.2324.04.23

• (a) group(a) group 1: A 1: ASASA 100 mg daily until third 100 mg daily until third month of pregnancy, month of pregnancy,
• (b) group(b) group 2: low molecular-weight 2: low molecular-weight heparin (LMWH) – enoxaparine 40 mgheparin (LMWH) – enoxaparine 40 mg
daily until third month of pregnancy, daily until third month of pregnancy, (c) group 3: ASA 100 mg(c) group 3: ASA 100 mg plus LMWH plus LMWH
40 mg daily until third month of 40 mg daily until third month of pregnancy.pregnancy.
24.04.2324.04.23

• In negative to thrombophilic screening In negative to thrombophilic screening pregnant women, thepregnant women, the comparison of comparison of efficacy of the three treatments shows efficacy of the three treatments shows that allthat all three treatment regimens were three treatment regimens were significantly effective comparingsignificantly effective comparing live live births against fetal losses.births against fetal losses.
• Comment:Comment: We suggest that We suggest that tthromboprophylaxishromboprophylaxis is indicated in is indicated in women with RPLwomen with RPL independently fromindependently from positiveness to thrombophilic markers.positiveness to thrombophilic markers.
24.04.2324.04.23

Ampirik tedaviAmpirik tedavi• Antitrombotik tedaviAntitrombotik tedavi• *Heparin (DMAH), Aspirin*Heparin (DMAH), Aspirin• Levotiroxin tedavisiLevotiroxin tedavisi• Paternal lökosit Paternal lökosit • IVIGIVIG
24.04.2324.04.23

Treatment of recurrent Treatment of recurrent pregnancy loss bypregnancy loss by
Levothyroxine in women with Levothyroxine in women with high Antl-TPO antibodyhigh Antl-TPO antibody
M H Mosaddegh, M H Mosaddegh, Iran J Reprod Med Vol. 10. No. 4. pp: 373-Iran J Reprod Med Vol. 10. No. 4. pp: 373-376, July 2012376, July 2012
Conclusion: Levothyroxine reduces Conclusion: Levothyroxine reduces the incidence ofthe incidence of spontaneous spontaneous abortions in women with high Anti-TPO abortions in women with high Anti-TPO antibody. It decreased anti-TPO antibody. It decreased anti-TPO antibody levels after 2-3 months antibody levels after 2-3 months treatment.treatment.
24.04.2324.04.23

• Thyroid peroxidase antibody Thyroid peroxidase antibody in women in women with unexplained recurrentwith unexplained recurrent miscarriage: miscarriage: revalence, prognostic revalence, prognostic value, and value, and response to empiricalresponse to empirical
• thyroxine therapythyroxine therapy• Junhao Yan, Fertil Steril 2012;98:378–82. Junhao Yan, Fertil Steril 2012;98:378–82.
Conclusion: Conclusion: EEmpirical thyroxine therapy in mpirical thyroxine therapy in those who tested positive did not seem those who tested positive did not seem toto
improve outcome. improve outcome.
24.04.2324.04.23

İmmunoterapiİmmunoterapi• Nedeni açıklanamayan TGK olan Nedeni açıklanamayan TGK olan
hastalarda normal plasentasyon ve hastalarda normal plasentasyon ve embryo gelişimini bozan henüz embryo gelişimini bozan henüz tanımlanamayan immunoloijk tanımlanamayan immunoloijk problemler bulunduğu düşünülerek problemler bulunduğu düşünülerek maternal immuno modulatuar tedaviler maternal immuno modulatuar tedaviler verilmektedir.verilmektedir.
Orgad, S. Orgad, S. Hum Reprod, 1999.,Hum Reprod, 1999., Ramhorst, R., Ramhorst, R., Am J Reprod Am J Reprod Immunol, 2000.Immunol, 2000.
24.04.2324.04.23

Ampirik tedaviAmpirik tedavi• Antitrombotik tedaviAntitrombotik tedavi• *Heparin (DMAH), Aspirin*Heparin (DMAH), Aspirin• Levotiroxin tedavisiLevotiroxin tedavisi• Paternal lökosit Paternal lökosit • IVIGIVIG
24.04.2324.04.23

İmmunoterapiİmmunoterapi• 1. 1. Paternal lökosit immunizasyonuPaternal lökosit immunizasyonu• a. Maternal immun cevap artar,a. Maternal immun cevap artar,• b. Antipaternal sitotoksik antikorların (APCA), anti- b. Antipaternal sitotoksik antikorların (APCA), anti-
idiotipik antikorların (Ab2) ve mikst lenfosit idiotipik antikorların (Ab2) ve mikst lenfosit reaksiyon bloke edici antikorların (MLR-Bf) reaksiyon bloke edici antikorların (MLR-Bf) oluşumunu sağlar.oluşumunu sağlar.
• c. Maternal T hücrelerinin paternal antijenleri c. Maternal T hücrelerinin paternal antijenleri algılayarak anti-T hücre reseptör idiotipik antikor algılayarak anti-T hücre reseptör idiotipik antikor (anti TCR) oluşumuna neden olarak fetusun (anti TCR) oluşumuna neden olarak fetusun matermal immunolojik ataktan kurtulmasını sağlar.matermal immunolojik ataktan kurtulmasını sağlar.
• d. Th1 sitokinlerini ve NK hücre aktivitesini de d. Th1 sitokinlerini ve NK hücre aktivitesini de azaltır.azaltır.
Ramhorst, R., Ramhorst, R., Am J Reprod Immunol, 2000.Am J Reprod Immunol, 2000.
24.04.2324.04.23

20062006• Immunotherapy for recurrent Immunotherapy for recurrent
miscarriage.miscarriage.
• TGK ile ilgili 12 randomize TGK ile ilgili 12 randomize kontrollü çalışmanın meta-kontrollü çalışmanın meta-analizinde bu tedavinin klinik etkisi analizinde bu tedavinin klinik etkisi olmadığı gösterilmiştir.olmadığı gösterilmiştir.
24.04.2324.04.23

Ampirik tedaviAmpirik tedavi• Antitrombotik tedaviAntitrombotik tedavi• *Heparin (DMAH), Aspirin*Heparin (DMAH), Aspirin• Levotiroxin tedavisiLevotiroxin tedavisi• Paternal lökosit Paternal lökosit • IVIGIVIG
24.04.2324.04.23

• 2. 2. İntravenöz immunglobulin (IVIG)İntravenöz immunglobulin (IVIG)• a. İn-vitro koşullarda proinflamatuar a. İn-vitro koşullarda proinflamatuar
sitokinlerin üretimini baskılar.sitokinlerin üretimini baskılar.• b. NK sayısı/aktivitesini azaltır. b. NK sayısı/aktivitesini azaltır. • c. Patolojik antikorları, Fc kısmı ile c. Patolojik antikorları, Fc kısmı ile
etkileşerek ya da pasif olarak anti-etkileşerek ya da pasif olarak anti-idiotipik antikorlar (Ab2) ile nötralize idiotipik antikorlar (Ab2) ile nötralize eder.eder.
Christiansen, O.B.,Christiansen, O.B., J Reprod Immunol, 2004.J Reprod Immunol, 2004.
24.04.2324.04.23

• Immunotherapy for recurrent Immunotherapy for recurrent miscarriage.miscarriage.
• TGK olgularında IVIG tedavisi üzerine 8 TGK olgularında IVIG tedavisi üzerine 8 randomize kontrollü çalışmanın meta-randomize kontrollü çalışmanın meta-analizinde canlı doğum oranlarında iyileşme analizinde canlı doğum oranlarında iyileşme saptanmamıştır.saptanmamıştır.
• Tekrarlayan gebelik kaybı yaşayan Tekrarlayan gebelik kaybı yaşayan hastaların yönetiminde immunoterapinin hastaların yönetiminde immunoterapinin deneysel tedavi dışında yeri yoktur.deneysel tedavi dışında yeri yoktur.
24.04.2324.04.23
2006

EVE GÖTÜRÜLECEK MESAJEVE GÖTÜRÜLECEK MESAJ• 1. TGK 20 hafta öncesinde, iki yada 1. TGK 20 hafta öncesinde, iki yada
daha fazla gebelik kaybı olup %2-5 daha fazla gebelik kaybı olup %2-5 oranında görülür. oranında görülür.
• 2. Etiyolojide heterojenite (genetik, 2. Etiyolojide heterojenite (genetik, endokrin, otoimmun, anatomik ve endokrin, otoimmun, anatomik ve trombofilik sebepler) mevcuttur. trombofilik sebepler) mevcuttur.
• 3. TGK hastaların %50’sinde belirgin bir 3. TGK hastaların %50’sinde belirgin bir neden saptanamamaktadır. neden saptanamamaktadır.
24.04.2324.04.23

EVE GÖTÜRÜLECEK MESAJEVE GÖTÜRÜLECEK MESAJ
4. Hiçbir tedavi uygulanmasa dahi TGK 4. Hiçbir tedavi uygulanmasa dahi TGK hastalarının %50-70’inde canlı doğumla hastalarının %50-70’inde canlı doğumla sonuçlanan başarılı gebelikler sonuçlanan başarılı gebelikler gerçekleşirgerçekleşir
5. Antitrombotikler ile tedavi meta 5. Antitrombotikler ile tedavi meta analizlerde etkin gibi görünmekle analizlerde etkin gibi görünmekle birlikte çalışmaların yetersizliklerinden birlikte çalışmaların yetersizliklerinden kaynaklanan önemli sorunları kaynaklanan önemli sorunları mevcuttur. mevcuttur.
24.04.2324.04.23

EVE GÖTÜRÜLECEK MESAJEVE GÖTÜRÜLECEK MESAJ
6. Levotiroxin ve immunoterapinin 6. Levotiroxin ve immunoterapinin ampirikampirik
tedavide yeri yoktur. tedavide yeri yoktur. 7. Uygulamada olan tüm tedavilerin iyi 7. Uygulamada olan tüm tedavilerin iyi
tasarlanmış çalışmalarda etkinliklerinin tasarlanmış çalışmalarda etkinliklerinin gösterilmesi gerekmektedir. gösterilmesi gerekmektedir.
24.04.2324.04.23

EVE GÖTÜRÜLECEK MESAJEVE GÖTÜRÜLECEK MESAJ
• Gelecekte tekrarlayıcı gebelik Gelecekte tekrarlayıcı gebelik kaybının etiyolojik nedenlerinin kaybının etiyolojik nedenlerinin daha net saptanması, tedavide fikir daha net saptanması, tedavide fikir birliğibirliği
oluoluşşabilmesi ve standart tedavi abilmesi ve standart tedavi protokollerinin önerilebilmesiprotokollerinin önerilebilmesi için için yeni çalışmalara ihtiyaç yeni çalışmalara ihtiyaç duyulmaktadır.duyulmaktadır.
24.04.2324.04.23

24.04.2324.04.23