Embed Size (px)
Citation preview

2 0 0 8 - 2 0 0 9
Efficient | Effective | Creative | AdvocacyT E L E C A R E C O R P O R A T I O N A N N U A L R E P O R T F Y 0 8 - 0 9
T E L E C A R E C O R P O R A T I O N W E E X I S T T O H E L P P E O P L E W I T H S E R I O U S M E N T A L I M P A I R M E N T S R E A L I Z E T H E I R F U L L P O T E N T I A L

T E L E C A R E C O R P O R A T I O N E F F I C I E N T | E F F E C T I V E | C R E A T I V E | A D V O C A C Y2
Letter from the President & CEO
A N N E L . B A K A R
The economic upheavals of the past year have challenged all of us — as a nation, as mental health organizations, as individual providers, and as consumers. We have had to lean on each other for guidance and sup-port. We’ve had to examine our priorities and streamline our operations. We’ve had to make difficult decisions and uncomfortable sacrifices. Yet, despite these difficulties, we are rising to the challenges and discovering new strengths in the process.
T E L E C A R E I S W O R K I N G W I T H O U R C U S TO M E R S TO A D D R E S S C H A L L E N G E S T H R O U G H F O U R M A J O R PA R T N E R S H I P I N I T I AT I V E S
The first initiative involves a drive towards greater efficiency through program/system restructuring that is data-driven, as well as a careful examination of how third party funding steams can be maximized. In the “Efficient Solutions” section of this report, we are pleased to share stories of how we’ve done this work creatively in Los Angeles, Stanislaus, Santa Barbara, and Alameda Counties, as well as the state of Nebraska, so that money could be saved while access and/or quality could be enhanced. This work has been particularly well planned in our Full Service Partnership (FSP) programs where Telecare has the broadest presence of any provider in the state.
The second initiative focuses on a push for greater effectiveness both in the areas of cus-tomer service and clinical work supporting our clients. In the “Effective Solutions” section, we are eager to share our preliminary research studies around our recovery model and how our program culture appears to be influencing our results. We are also working hard to listen to the feedback from our recent customer survey and to use it in ways that will noticeably improve our operations.
The third initiative involves our drive to be creative in addressing system needs. A major focus this year was to create programs to serve clients with serious mental illness outside the traditional public mental health system. This includes older adults in medical centers, parolees exiting the criminal justice system, and individuals who are dually diag-nosed in Regional Centers. These services are filling important gaps in public mental health systems utilizing new funding sources. We share our progress in this area in the “Creative Solutions” section of this report.
Our final initiative involves advocating on behalf of systems and individual consumers on statewide and national levels. We have presented our efforts in the “Advocating for Solutions” section of this report.

E F F I C I E N T | E F F E C T I V E | C R E A T I V E | A D V O C A C Y T E L E C A R E C O R P O R A T I O N 3
LO O K I N G B AC K , LO O K I N G A H E A D
In FY 08-09, several of Telecare’s county customers were forced to address tremendous budget deficits. In some cases, the need to cut costs was so pronounced that counties were compelled to take drastic steps, such as closing large inpatient programs and increasing their reliance on skilled nursing facilities. Although we understand these decisions and the mount-ing financial pressures on counties, we are striving to partner with our customers in ways that save costs while also preserving the stabil-ity needed to promote long-term recovery.
In our 45 year history, Telecare has faced challenging times before. We are grateful for our partnership and the trust you have placed in our hands. We are confident that by continuing to pull together and focusing on shared values, we will successfully build upon our past accomplishments in the year ahead.
L E F T: T E L E C A R E F O U N D E R S , M O R TO N B A K A R A N D A R T G L A D M A N . R I G H T: T E L E C A R E ’S C U R R E N T E X E C U T I V E T E A M , I N C LU D I N G ( C LO C K W I S E F R O M TO P L E F T ) PAT R I C K D OY L E, C A R O L C A P U TO, S T E P H E N W I L S O N , R O S S P E T E R S O N , A N N E B A K A R , S TAC E Y C A L H O U N , A N D M A R S H A L L L A N G F E L D.

T E L E C A R E C O R P O R A T I O N E F F I C I E N T | E F F E C T I V E | C R E A T I V E | A D V O C A C Y4
Efficient SolutionsMaximizing Limited Resources
During FY08-09, Telecare worked directly with customers to address resource challenges in several ways: expanding and improving services in community-based Assertive Community Treatment (ACT) and Full Service Partnership (FSP) programs; bridging service gaps with crisis residential services; maximizing revenue with Medicaid funding; and leveraging third-party reimbursements.
Making ACT/FSP Programs More Effi cient through Data
Improving Results, Increasing Service, Controlling Costs
As one of the nation’s largest Assertive Community Treatment (ACT)/Full Service Partnership (FSP) providers — with programs in Oregon, Texas, North Carolina and California — Telecare has a large geographic footprint and numerous programs using an ACT-based model. These programs serve different target populations, using different approaches to address specific needs.
In California, while the state mandates col-lection of data for all Mental Health Services Act (MHSA) funded FSP programs, Telecare also voluntarily decided two years ago to have all non-MHSA programs begin collecting the same data as well. We wanted to demonstrate that our programs were helping clients to make strides in their lives, in a data-oriented manner.
During FY08-09, we led a coordinated effort to create an aggregated outcome/utilization report across all Telecare ACT and FSP pro-grams. This is significant because it will enable us to accrue the knowledge gained from one program to illuminate better practices and
procedures in others. We will be able to slice our data by a variety of means — size of program, geographical and services differ-ences, etc. — to help our customers serve more clients, with smaller budgets, while offering greater flexibility and options for persons served. We are currently testing our report, process, and data for integrity and will begin consistent use of this report in FY09-10.
Consistent with this goal, a Telecare ACT/FSP committee was formed during FY08-09 for the purpose of examining the operations of our programs and how individuals served can be “stepped down” or moved through ACT/FSP programs effectively. We have imple-mented levels of care within several ACT/FSP programs, which have enabled us to expand services, while maintaining or reducing costs.
Stanislaus County’s TRAC program and Los Angeles County’s ACT/FSP programs areexamples of the improved results and increased services achieved through this process.

E F F I C I E N T | E F F E C T I V E | C R E A T I V E | A D V O C A C Y T E L E C A R E C O R P O R A T I O N 5
T E L E C A R E ’S AC T / F S P DATA I S C A P T U R E D A N D R E P O R T E D U S I N G O U R B U S I N E S S I N T E L L I G E N C E S Y S T E M .
Stanislaus County, CA
Challenges: Stanislaus County wanted to create a system that could flex and adapt to the changing needs of clients. Specifically, they hoped to accommodate more clients without bouncing people between various programs and levels of care, disrupting support networks that are crucial to recovery.
Solutions: Telecare worked closely with thecounty to redesign the two original programsinto six distinct services (one funded by county monies, five by MHSA) now knownas Telecare Recovery Access Center (TRAC) and Telecare Modesto Recovery Services (TMRS). Collectively, the programs offer three levels of care (ACT, outpatient, and wellness center services). This approach pro-vides continuity of care with a primary focus on peer support and family involvement. Th e menu of treatment options ranges from high- to low-intensity:
Partnership TRAC:• High-intensity ACT services with a low member-to-staff ratio, group and individual support,
individualized recovery planning, and 24/7 crisis intervention services.
Fast TRAC: • Moderate-intensity outpatient services.
Wellness TRAC: • Low-intensity member-supported services.
Results: The variety of options supports indi-viduals at all levels of their recovery, allowing people to move fluidly between levels of care according to their intensity of need. The system is also self-regulating — as more people move toward wellness, there is space for new clients at other levels without the need to adjust staff-ing. TRAC uses multidisciplinary teams which include a psychiatrist, a nurse, and a Master’s- prepared clinician, as well as personal service coordinators/case managers with experience in substance abuse recovery, housing, employ-ment, and mental health support. Teams work in partnership with each other and with other agencies and service providers to assist mem-bers in linking to community resources.

T E L E C A R E C O R P O R A T I O N E F F I C I E N T | E F F E C T I V E | C R E A T I V E | A D V O C A C Y6
M E M B E R S O F T E L E C A R E ’S L A 4 P R O G R A M — A N AC T / F S P P R O G R A M I N L A CO U N T Y — C E L E B R AT E T H A N K S G I V I N G I N S YC A M O R E PA R K A N D R E C E I V E R E CO G N I T I O N F O R T H E I R M A N Y AC H I E V E M E N T S D U R I N G T H E P R E V I O U S Y E A R .
Challenges: Changes in the LA County tax base left the county’s General Fund with a $53 million budget shortfall. As a result, Los Angeles needed to trim county-operated programs as well as those operated by external providers. Concurrently, the county needed its providers to creatively restructure programs to maximize MHSA dollars to develop a true continuum of care for individuals in commu-nity settings. The county specifically requested that Telecare reduce its contracts by $974,000 across its own ACT/FSP programs, effective July 1, 2009.
Solutions: Telecare proposed a solution for redesign that used fewer MHSA dollars, while implementing a true continuum of care. We were able to maintain the current members and also increase our capacity by adding a low-er level of care: Field Capable Clinical Services
(FCCS). Using the Milestones of Recovery Scale and other outcome indicators, we were able to accurately identify individuals eligible for MHSA funding who could be successfully served in lower levels of care. Additionally, we were able to minimize layoffs and preserve consistency in long-term client-staff relation-ships by consolidating and reorganizing our leadership staff.
Results: Through this process, we adapted to LA County’s changing needs in a short period of time. We met our cost-saving objectives without service reductions or member dis-enrollments and with minimal staff layoffs. We were able to expand the services in our programs and add value to our members by becoming a true continuum of care.
Los Angeles County, CA

E F F I C I E N T | E F F E C T I V E | C R E A T I V E | A D V O C A C Y T E L E C A R E C O R P O R A T I O N 7
Challenges: Santa Barbara’s north county region was unable to effectively serve those ex-periencing a mental health crisis, offering lim-ited options between outpatient services (ACT) and acute psychiatric care. Those in need often attracted police attention or were relegated to homeless shelters if they didn’t qualify for ad-mission to an acute care facility. Additionally, acute services are distant — the nearest acute inpatient facility is 80 miles away, with others in Ventura (120 miles) or LA County (around 200 miles). Logistical challenges included locating an appropriate site for a new facility and gaining community acceptance.
Solutions: The county partnered with Telecare to open CARES Crisis Residential North (CCRN) — a 12-bed residential crisis facility in Santa Maria serving adults in crisis due to mental health issues and co-occurring sub-stance diagnoses. CCRN provides voluntary, unlocked, short-term services, typically lasting three to seven days.
Collaborating closely with the county, this pro-gram is co-located with another county facility which handles screening and referrals to the CCRN. The program takes after-hours
admissions referred by the County Mobile Crisis Team, County ACT programs, or by CARES Santa Barbara.
Results: It took four years of planning to bring this program to fruition. However, it has proven to be a much-needed addition to the system of care. CCRN provides a safe, unlocked environment for people in crisis until they’re ready to transition back home, or to less restrictive levels of care. Telecare’s recovery-model is fundamental to the CCRN program, working to expand choices, instill hope, and begin a recovery plan for each individual served. A strong multi-lingual and multi-cultural staff enables CCRN to serve cli-ents in variety of languages, including Spanish, Tagalog, Mandarin, and ASL. Due to changes in licensing requirements, the program can now serve people over age 59, which opens options for more people in the county.
A key difference in this program is that it invites external case managers to be active participants in their clients’ treatment process. This steps has helped to increase continuity of care for people served.
Closing the Gap between Acute and Outpatient Care
Santa Barbara County, CA
“... there are caring people in my life through Telecare... the team has been a positive
force in my life. ” — T E L E C A R E C L I E N T, S A N TA B A R B A R A CO U N T Y

T E L E C A R E C O R P O R A T I O N E F F I C I E N T | E F F E C T I V E | C R E A T I V E | A D V O C A C Y8
Challenge: Since 2004, Nebraska’s men-tal health system has been going through a transformation. In the Omaha area, Region Six Behavioral Healthcare (BHC) had been working to bring a more comprehensive array of services to the local community. However, after opening two short-term subacute programs with Telecare — the Region Six Recovery Center and the Recovery Center at Sarpy — abrupt changes in the system made those services redundant.
Solutions: Rather than simply closing the programs, BHC partnered with Telecare to adapt the programs to tackle other unmet needs. Telecare assisted BHC in several steps. First, we worked with local legislators to lobby for changes that would allow programs that are 16-beds or less (like these programs) to be partially funded by Medicaid. This helped to offset the local program costs by $1.1 million. Second, we worked with BHC and the state to rewrite service guidelines to include a new
level of care: secure residential services (long-term residential programs, like the proposed new programs would be after redesign). These guidelines established how programs at this level should operate and the services that should be provided. This enabled BHC to redesign their two Telecare-operated programs and provide services that were previously un-available in the Omaha area.
Results: The main objective of these efforts was to continue to bring people back to their home communities with appropriate services. The BHC was able to bring more people back from the distant and more restrictive state hospital setting, with a secure, long-term program that is deeply recovery-centered. It enables people to be closer to home while preparing for even-tual transition to lower levels of care. And, in addition to offsetting local program costs with federal funds, BHC was also able to sell beds to Region Four Behavioral Healthcare.
Maximizing Funding Streams
Region Six Behavioral Healthcare, Nebraska
S TA F F, C L I E N T S , A N D FA M I LY F R O M T H E R E CO V E R Y C E N T E R AT S A R P Y A N D T H E R E G I O N S I X R E CO V E R Y C E N T E R .

E F F I C I E N T | E F F E C T I V E | C R E A T I V E | A D V O C A C Y T E L E C A R E C O R P O R A T I O N 9
Challenge: In 2007, Alameda County opened the doors to Willow Rock Center (WRC), a 12-bed facility designed for adolescents with serious emotional disturbances, who were experiencing acute symptoms related to ill-ness and/or the emotional fall-out of intense victimization and other challenging situations. Offering both short-term crisis services as well as inpatient acute support, WRC was intended to fill a much needed gap in the system for indigent and Medical-funded kids. Unfortu-nately, Alameda County alone was not able to maintain a high enough daily census to cover the high cost of staffing required to address the acute needs of the kids served. This imbalance threatened the program’s long-term viability.
Solution: To make the program more finan-cially sustainable for Alameda County, the decision was made to open the doors to other payors. Telecare established a partnership with Kaiser for four dedicated beds each month. The arrangement allows Kaiser to have a “roll-ing census” which means that when their needs flex, Willow Rock can flex with them. While they tend to average four beds per month, however, their census can be higher or lower, depending on need. Additionally, the overall
program was redesigned to accommodate a longer average length of stay, so that the clini-cal staff could make greater headway in terms of identifying and addressing core issues verus simply stabilizing symptoms with medication and releasing kids to go home.
Results: By bringing in Kaiser, Telecare has been able to maintain a higher census level on a more consistent basis. The total census is about 60 admissions per month, which usu-ally equates to a daily average census of 11. The longer LOS has enabled the program to work with kids on skill development, which enables them to better handle stressors and trauma, and gain greater self-control to prevent recidivism. The program has also been actively working with families and kids in a more ho-listic way to address issues and prevent repeat cycling through the system. One surprising point is that there is no significant difference in the severity of symptoms and treatment needs between private pay clients and those receiving MediCal funding. This has meant that the pro-gram’s existing psychiatric and clinical staffing has been seamlessly able to accommodate both groups of kids.
Alameda County, CA
Adding Payors to Off set Costs of Adolescent Services
L E F T: DAV E K E A R S , F O R M E R D I R E C TO R O F A L A M E DA CO U N T Y D E PA R T M E N T O F P U B L I C H E A LT H , A N D A N N E B A K A R , T E L E C A R E P R E S I D E N T A N D C E O, AT H I S R E T I R E M E N T C E L E B R AT I O N . R I G H T: S TA F F AT W I L LO W R O C K C E N T E R .

T E L E C A R E C O R P O R A T I O N E F F I C I E N T | E F F E C T I V E | C R E A T I V E | A D V O C A C Y10
Effective SolutionsDemonstrating Measurable Results
Telecare partners with clients, staff, customers, and external agencies in our ongoing efforts to improve services, address challenges, and contribute to the overall health and vitality of the communities in which we work.
Customer SatisfactionIdentifying Opportunities for Continued Improvement
During FY08-09, Telecare enlisted an external research firm to conduct a satisfaction survey of our customers, our first in over six years. Telecare interviewed over 40 individuals in over nine county and state agencies. Several trends emerged:
Telecare’s customers want providers • to meet contract objectives and solve problems quickly and effectively. They want effective systems, communication, and collaboration in these processes.
They want providers to build competencies • in community-based care, to keep up with the shift from inpatient to outpatient care.
They want providers to be strong strategic • partners, leveraging their knowledge and expertise to support customers in staying ahead of the information curve, and beactive partners in the local system of care.
Cultural competency is a consistent area • of challenge, for both customers and providers. Day-to-day realities of staffing, language, etc., remain significant.
T E L E C A R E ’S R E S P O N S E
Telecare is responding to customer feedback in a variety of ways. Our initial steps included:
Immediate response to issues raised on a 1. customer-specific basis.
Established routine meetings between 2. Telecare’s customers and our local program, regional and executive leadership to review and manage issues, outcomes, and perfor-mance. Regional Telecare staff members have the deepest knowledge of local needs and are now taking a more consistent and active role in ensuring an open flow of communications.
Increased collaboration and connection 3. with our local communities. Some current community efforts include: NAMI Walks for the Minds of America; student intern-ships with Girls, Inc. and Achieve; the Jump Start Fellowship Program in Los Angeles; and Jewish Vocational Services. We are also working on strategic collabora-tion including some of the advocacy work discussed later in this report.
T E L E C A R E ’S CO R P O R AT E O F F I C E S TA F F, I N C LU D I N G R O S S P E T E R S O N , V I C E P R E S I D E N T O F D E V E LO P M E N T ( 2 N D F R O M L E F T ) , H E A D O U T TO G O L D E N G AT E PA R K I N S A N F R A N C I S CO TO PA R T I C I PAT E I N N A M I WA L K S F O R T H E M I N D S O F A M E R I C A .

E F F I C I E N T | E F F E C T I V E | C R E A T I V E | A D V O C A C Y T E L E C A R E C O R P O R A T I O N 11
Recovery-Centered Clinical System (RCCS)Measuring the Impact of Program Culture on Recovery
Telecare is committed to validating the ef-fectiveness of the RCCS and is undertaking this effort by conducting the research studies required of an evidence-based practice.
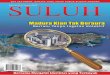
Our focus has been to evaluate the program culture and its role in the recovery process. During the past year, we began developing our first evaluation study of our Program Culture Assessment Tool. Our goal is to measure our ability to foster a program culture that enhanc-es the recovery of individuals. The graphics above show two of the facets of culture we are measuring, the motivation and judgmentalness
of our staff and the impact of these on client recovery. The Program Culture Assess-ment Tool was first piloted at the Recovery Center at Sarpy, located in Nebraska, where staff worries over the security of their program had impacted morale, as well as their ability to deliver optimum services to clients. After a baseline assessment of their culture was completed, staff worked with each other to im-prove their culture. When the assesment was repeated at 6 and 12 months, there was signifi-cant improvement in all areas. The Program Culture Assessment Tool will be tested at 12 locations during the coming year.
Clinical ServicesRedefi ning Seclusion and Restraint Standards, Exceeding Accreditation Standards
Seclusion and Restraint Standards (S&R): In FY08-09, Stacey Calhoun, Telecare’s Vice President of Operations, was invited to participate on a small international committee of the Commission on Accreditation of Reha-bilitation Facilities (CARF) to redefine S&R standards. The new S&R standards, released in 2009, focus on building a recovery culture and mandate the eventual elimination of S&R in favor of non-violent practices, while providing de-escalation training for staff.
Accreditation: As of FY08-09, 91% of Telecare programs are CARF or Joint Commission accredited. Telecare received a three-year CARF accreditation plus two com-mendations of excellence. Telecare’s own peer quality review process is at the foundation of our successful accreditation reviews. Each year, we conduct an internal survey of all programs to ensure that we are identifying opportunities for improvement. This process allows staff to proactively collaborate on program adjustments and enhancements.
Outstanding/Acceptable Needs Attention
Staff Judgmentalness
70%initial
30%initial
19%after
1 year
81%after 1 year
75%before
47%after
Outstanding/Acceptable Needs Attention
Staff Motivation
74%initial
26%initial
81%after 1 year
19%after
1 year
T W O M E A S U R E S F R O M T H E P R O G R A M C U LT U R E A S S E S S M E N T TO O L F R O M T H E R E CO V E R Y C E N T E R AT S A R P Y.

T E L E C A R E C O R P O R A T I O N E F F I C I E N T | E F F E C T I V E | C R E A T I V E | A D V O C A C Y12
Creative SolutionsCollaborating to Meet Evolving Client Needs
Since 1965, Telecare has consistently worked to marshal our collective knowledge, expertise, passion, and resources to provide excellent clinical services while advancing the study and field of recovery. This year, we made progress in bringing effective, efficient approaches to areas where the needs are pronounced and options are limited, including forensic, DD/SMI, and contract management services.
Closing Service Gaps
California Department of Corrections & Rehabilitation (CDCR)
Overview: California legislation mandates increased treatment services for the estimated 4,250 inmates and 3,000 parolees in the system who have serious mental illness (SMI). When these individuals are paroled, they frequently have limited resources to manage their mental health needs. The cost of their crisis and inpa-tient care often falls to local county behavioral health departments. More than 90% of parolees with serious mental illness return to prison within three years of release, which contributes to overcrowding.
Steps Taken: In FY08-09, Telecare began a partnership with CDCR to provide ACT- and FSP-type integrated services for parolees in San Diego, San Bernardino, and Los Angeles counties. Additional forensic/SMI programs are anticipated in the coming fiscal year.
System Benefits: The CDCR benefits by meeting legislative requirements with a robust, research-proven service model. Wrap-around ACT-like programs have been proven to help people remain stable and live successfully in the community.
Counties benefit by leveraging dollars from other systems to service targeted populations (versus relying on county general funds), while also alleviating strain on existing resources such as ERs, law enforcement, and crisis response.
Clients benefit from having intensive, recovery-centered, wrap-around services and supports, which can help to awaken hope and bolster the recovery process. Although it is too early to measure the coutcomes of this service, we are confident it will contribute to significantly reduced recidivism.

E F F I C I E N T | E F F E C T I V E | C R E A T I V E | A D V O C A C Y T E L E C A R E C O R P O R A T I O N 13
Overview: An estimated 32,000 individuals in the US have co-occurring SMI with developmental disabilities (DD). These individuals often have intense needs that are not adequately managed in either the DD or SMI systems alone.
Steps Taken: Telecare has partnered with Regional Centers since 2003 to fill the service gaps for this historically underserved popula-tion with recovery-centered inpatient services. In FY08-09, we also added a community-based ACT-like model for the DD/SMI population.
Telecare is also participating as one of only three or four DD/SMI providers on a statewide, government-funded DD/SMI collaborative. This group meets quarterly to share resources, discuss public policy, budgets, and trends, and to think broadly about strategies for serving this
underserved population.
System Benefits: One outgrowth of these efforts is that Telecare is now partnering with various Regional Centers agencies and is in progress on the development of two new Mental Health Rehabilitation Centers (MHRC) for the DD/SMI population. These include one in the Central Valley and one on the Fairmont Hospi-tal Campus in Alameda County. Both programs help bridge gaps for people who can benefit from a structured, sub-acute environment while they prepare for eventual transition to lower levels of care.
Regional Centers Organizations
T E L E C A R E ’S VA L L E N O R T E P R O G R A M P R O V I D E S AC T S E R V I C E S TO P E O P L E W I T H S M I A N D D E V E LO P M E N TA L D I S A B I L I T I E S .

T E L E C A R E C O R P O R A T I O N E F F I C I E N T | E F F E C T I V E | C R E A T I V E | A D V O C A C Y14
Overview: Currently in the United States, there is only one geriatric psychiatrist for 11,372 Americans age 75 and older. In 2020, that num-ber will be one for every 20,195.
Between now and 2030, another 75 million Americans will reach age 65. An estimated two million Americans over age 65 suffer from a diagnosed depressive illness, yet only 3% of older persons receive specialty mental health services. Hospitals are having to make plans to serve their aging patient populations effectively.
Steps Taken: Telecare began expanding its abil-ity to provide contract management services for hospitals that need assistance in establish-ing or operating more financially viable acute inpatient psychiatric servivces. While Telecare will provide both adult and older adult acute services, the geropsychiatric component pres-
ents a particularly pressing need for customers. Telecare will be opening its first geropsychiatric acute contract management program in Rancho Mirage, CA during 2010.
System Benefits: Acute care hospitals can treat their older adult patients’ mental health and concomitant physical illnesses, providing better care to patients in a more efficient manner. At the same time, geropsychiatric units tend to have less bad debt and a more uniform payor source. Hospitals have the opportunity of developing enhanced revenue through the creation of a distinct unit that is eligible for the recently updated Medicare inpatient psychiatric Prospective Payment System (PPS) per diem.
Contract Management: Acute Psychiatric Services in
Medical/Surgical Hospitals
I N F Y 08 - 09, T E L E C A R E S I G N E D I T S F I R S T CO N T R AC T M A N AG E M E N T AG R E E M E N T W I T H E I S E N H O W E R M E D I C A L C E N T E R . T H E N E W P R O G R A M I S E X P E C T E D TO O P E N I N J U LY 2010 A N D W I L L H AV E B E T W E E N 15 - 25 B E D S .

E F F I C I E N T | E F F E C T I V E | C R E A T I V E | A D V O C A C Y T E L E C A R E C O R P O R A T I O N 15
National Health Reform
Telecare is an active member of the National Council for Community Behavioral Health (NCCBH), which has emerged as a potent force in Washington under the leadership of its President and CEO, Linda Rosenberg. Throughout the long debate on health reform, Telecare has used its close relationships with key California Representatives to promote the agenda of the National Council, includ-ing advocating for the expansion of benefits to the uninsured that are more closely aligned with the comprehensive benefits now provided under Medicaid.
Licensing
Telecare was an early advocate for the MHRC license in California, which greatly enhanced the opportunity for recovery programming in sub-acute environments. Today, we are work-ing to introduce language to the state plan that would permit the licensing of 16-bed MHRCs. This development could have significant finan-cial and programmatic advantages for counties that are looking to reconfigure their current IMD service system.
Ancillary IMD Work Group
Telecare has worked closely with Pat Ryan, Executive Director of California Mental Health Directors Association (CMHDA) to develop and pursue strategies relating to the State’s decision to cost-shift IMD ancillary services. We have collaborated on legislative and legal strategies as well as worked to identify practi-cal and logistical barriers to making the State’s policy change work. This shift would be very onerous to counties at a time when the finan-cial pressures are already tremendous, and as a provider, Telecare is doing its part to preclude this action from being implemented.
Local Advocacy
As Telecare works with agencies across the state to make necessary changes to the public mental health system, we are partners in the process of developing the necessary political will and engaging key stakeholders including families, consumers, and local elected officials. A key example over the past year includes our work with the criminal justice system, county mental health agencies, and Boards of Supervisor representatives to get our forensic programs Short-Doyle certified.
Advocating for SolutionsLobbying to Protect and Expand Services
L E F T: T E L E C A R E ’S R O S S P E T E R S O N A N D C A L I F O R N I A’S S E N AT E P R E S I D E N T P R O T E M DA R R E L L S T E I N B E R G , AT A F U N D R A I S I N G LU N C H E O N . R I G H T: A S S E M B LY W O M A N M A R Y H AYA S H I , T I P P E R G O R E, A N D A N N E B A K A R O F T E L E C A R E S U P P O R T I N G T H E I R I S A L L I A N C E A N D I T S E F F O R T S TO E N D YO U T H S U I C I D E.

Telecare SnapshotAt-a-Glance in FY08-09
Telecare ServicesSince 1965, Telecare has evolved to address the changing needs of people with serious mental illness (SMI). Today, we provide and manage an array of services — from inpatient and community-based programs to crisis, residential, and administrative services.
We also provide specialized services to individuals who face other challenges in addition to their mental illness. These individuals may be homeless, incarcerated, be developmentally disabled, have medical issues associated with aging, or face addiction issues. Telecare serves adults and adolescents, particularly those who may require more intensive, recovery-centered mental health programs.
Facts & Figures17,500 persons served• 52 programs across 22 counties and 5 states• 3 new programs opened in FY08-09• 7 programs redesigned or expanded• 44 programs now using Telecare’s • Recovery-Centered Clinical System (RCCS)91% of programs now accredited by CARF • or Joint Commission2,241 employees•
AwardsIn FY08-09, Telecare was once again named one of the Top 100 Best Places to Work in the Greater Bay Area. Telecare has received this award for five out of the last six years. We are deeply proud of our staff and the work they do to support individuals in recovery.
T E L E C A R E C O R P O R AT I O N 1 0 8 0 M A R I N A V I L L A G E P K W Y, S U I T E 1 0 0 , A L A M E D A , C A 9 4 5 0 1 , 5 1 0 - 3 3 7 - 7 9 5 0 , W W W. T E L E C A R E C O R P. C O M
“At 39, I was working as an electrician when I had a seizure on the job.
I lost my job and found myself homeless, sleeping in a parking lot. Homelessness makes
you feel like garbage no one wants around. This week, I’ll be moving into an apartment. ”
— T E L E C A R E C L I E N T, O R A N G E CO U N T Y