Embed Size (px)
Citation preview

Telling the Story in Catastrophic Injury and Wrongful Death Cases
Illinois State Bar Association February 24, 2017
Stephen I. Lane Lane & Lane, LLC
230 W. Monroe Street Suite 1900
Chicago, Illinois 60606 (312) 332-1400
(312) 899-8003- fax (847) 736-7769 - mobile [email protected]
www.lane-lane.com
1

Telling the Story- The Plaintiffs Side
There is at least one good story to every case. Obviously, there are at least 2 versions of that story ... yours and your opponent's. Your case began with people and events that, over time, have evolved into the case you've brought. In communicating the story of your case, you want to inspire feelings in the jurors or judge who will decide it that will allow them to find the path of least resistance to your position. How can you best do this? The answer is different in each case, but here are some concepts to keep in mind in figuring out the best way for you to tell your story.
To illustrate some of these tips, I have bmmwed liberally from a recent medical malpractice case which my pminer, Scott Lane and I tried last year involving a 42 year-old working single mother of 5, one of whom was disabled. Please note that I am giving you these abbreviated facts in chronologie order to give you context, which is decidedly not how I would tell the story to a JUly.
Turner v. Mercy
Several years before her admission, our client, "J", had undergone a heart valve replacement, and as a result, was required to be on anticoagulant medications for the rest of her life in order to avoid the risk of clotting because of the artificial valve. She had developed a dental abscess which progressed to a potentially deadly infection of the soft tissues of her neck. The infection had progressed to the point where her airway was beginning to be compromised. She was admitted to the defendant hospital, where an emergent tracheotomy was performed.
She was in the ICU for a few days and then transfened to a step-down unit. The infection of her neck responded to IV antibiotics, and the swelling and white blood counts had gone down. From the day after the tracheotomy was placed, and for several days, there were no signs of bleeding, and no signs of anxiety or choking.
On the evening of the fifth post-operative day, the evening nurse noted that J was coughing up blood through the trach, but she had no discussion of this with any physician.
In the early afternoon the next day, J was scheduled for a cine-fluoroscopy in the cardiac catheterization lab to see if there had been a spread of the infection to her heart. When she mTived there at around 2 pm, the staff noted that there was active bleeding from the trach site. The ENT service was called, and an ENT resident came to the cm·diac cath lab, cauterized the trach site with silver nitrate, and repacked the trach Vaseline gauze. He said the bleeding was "pmiially controlled" in his notes. At around 5 pm, the ENT attending physician saw J and said there was no active bleeding, and at 5:26pm, the cardiologist who was doing the cine-fluoroscopy confinned that there was no active bleeding.
J was returned to the step-down unit at about 5:30pm, and at that time, her sister, "A", was also present. A recalls that over the course of hours from the time that J was returned from the cath lab, she had complained of choking, and in particular, complained of "choking on blood clots". A said she tried to get someone, nurses and doctors, to do something, that J was bleeding from the trach site and choking, and that she knew this couldn't be "right". At 6 pm, the ENT resident placed an order for the STAT transfusion of FFP (fresh frozen plasma) and PRBC's (packed red blood cells), but at 7 pm, he wrote an order for just the FFP, although he did not rescind the previous directive to also administer PRBC's.
2

According to A, who was present throughout the afternoon and evening, she noted that the patient was choking and complaining of choking on blood clots, and complained to the nurse about it. The nurse had very little, almost no experience in managing trach patients. Eventually, at around II pm, the nurse paged the medical resident on call, who was a second year resident. There are notes in the chart for 11 pm that showed that J was complaining of pain, and "choking on these clots", that suggest that J was now able to vocalize through the trach, although she had not been able to do so before, as the trach was one which had an inflated cuff. The cuff was supposed to be inflated in order to protect against the aspiration of any fluids, including blood.
Although the nurse and resident both testified that the resident responded to the call within about I 0 minutes, there are no notes that suggest that the resident did actually come. An hour and a half later, after continued complaints from the sister about the bleeding and choking, the nurse paged the MROC again. The nurse, medical resident on call and ICU resident who came later claim that they saw no bleeding from the trach site ... just dried blood, although in a "late note", the MROC wrote that she saw blood on the sister's hands.
After the MROC was paged a second time, she then paged the senior resident, who came to the room. By then, the patient was anxious, pacing around the room, and complaining of choking. The senior resident charted in a late entry, and testified that, when he came to J's room, he saw J and her sister there "trying to stop bleeding with applying pressure near and around the trach site and adjusting the trach". The sister, a germaphobe, maintained that neither she, nor J ever touched the trach. She testified that throughout, there was blood oozing fi·om the trach site, that for at least a few hours, she had been dabbing up blood from the site and complaining to the staff that this couldn't be right, and was trying to get someone do something.
Shortly after the senior resident anived, J suddenly became unresponsive, and a Code Blue was called. The code sheet was extremely lacking in its detail, and notably, failed to identify most of the individuals who attended the Code. In patiicular, there was an unidentified anesthesiologist, who had repositioned the tracheostomy tube during the Code. Somehow, neither the hospital, nor any of the doctors or nurses who were involved were able to identify this individual. Another aspect of the Code sheet and the record, for that matter, was the recording of J' s 02 saturation levels. According to the notes written in the chart, J's saturations were never alarming. However, a lab slip recorded a very different, and alatming result during the time of the Code. When the ENT resident an·ived, about 19 minutes after the Code had been called, he repositioned the trach tube, and J's 02 saturations rose to normal levels. Unfotiunately, by then, J had suffered irreversible brain damage. As a result of the damage, J suffered tremors that impacted every volitional act she attempted ... Each intentional action elicited the tremors, and the harder she tried to perform the act, the more pronounced the tremors becatne. Cognitively, she was fairly highfunctioning, although her executive functioning and behavior characteristics were impacted. As a result of the tremors, she was confined to a bed or wheelchair, and required assistance for vitiually all of her activities of daily living. Her speech was almost always garbled, and others who didn't know her often found it hard to understand her, especially over the phone. People often hung up on her because they could not understand what she was saying, She was awme of all of it, and she knew what she had lost. Still, she maintained a positive and hopeful attitude.
1. Talk to the jurors, not just the jury. When you me telling a story, make sure the people you need to listen are. Before you begin delivering your opening or closing, pause. Malee eye contact and get a cue from each juror so that you are sure that he/she is listening. Throughout your story,
3

make sure you retum to make eye contact with each juror so that they !mow you're talking to them personally.
2. Be yourself. It's a mistake to take on the personality and persona of someone else. One of the most important factors in trial success is credibility. Your own credibility is no less impottant than the credibility of your clients, witnesses and evidence.
3. Develop a theme, and maintain the theme throughout your case. Your theme should be simple. Jury consultant, Joshua Karton and others have suggested that a theme should be able to be limited to a 10 word statement. In your materials, I've included the closing arguments in the case ofTumer v. Mercy, a medical malpractice case my brother/partner, Scott Lane and I tried last December. Our theme was that "our client's life was a book that had been written about her. .. some chapters having been written by her, some about her by others." Tlu·oughout the case, we maintained the theme that the defense, and its witnesses, had written the chapter of her life involving our client's hospitalization (the hospital record), but were now trying to re-write that chapter even though the defendant hospital's own doctors and nurses had written it in the first place. We revisited the theme in our closing, asking the jury to write the next chapter in our client's book.
"A point in any direction is the same as no point at all." -Harry Nilsson
"The law charges you to serve your client by discovering and delivering that client's cast story in the proper forum to the very best of your ability, consistent with the law. It's your professional and legal duty to do so-and failure can result in severe consequences. It's up to you to thoroughly and clearly communicate your client's message." Eric Oliver
Anyone that you tell your story to comes to that story with their own individual experience and history. How many times have you been to a court, and felt that the judge had a perception of the case that was different from yours ... This is just a fact based on research into and empirical observation of human decision making. People often jump the gun in presuming what any story is all about.
Your theme gives the court and jury the context within which they will interpret every fact and argument they are presented with. The court's and jurors preconceived presumptions will always color the legal decision-making process. You can meet and defeat these presumptions in the way you choose to deliver your story. For example, in the Tumer case, our client, a single working mother of 5, was being criticized by the defendants for her general failing to take care of her own health generally. During discovery, they developed evidence of what they considered her poor dental hygiene and uneven medication control... things that had occurred well before the hospitalization and care that was truly at issue in the case. The apparent thought seemed to be that our client was "damaged" by her own failures, when the defendants became involved ... that they actually saved her from herself. One of her own primary care physicians even said that that our client's failures actually led to the need for the defendant's services.
You should think about anchors and framing for your story. Anchors are the phrases and images which conjure an image of some kind. Frames are the labels or concepts that are built or set by the anchors. One powerful anchor we used in the case was the continuous reference to "The Story". We framed that part of the story to reflect the credibility of what had been written when
4

the record had been written as compared with what the defendants and their experts were saying during the trial. We'd found six notes in the chart, that had been written by five different physicians, contradicting the defendant's position that J's trach had been occluded because her sister had moved it out of position while trying to clean up the blood, recounting a history along the lines of J's tracheotomy having been occluded by blood clots. I've never counted the number of times we said the phrase "six different notes by five different doctors", but it was a lot!
The chapters of the book that our client had written showed her to have been an incredible, and utterly responsible, lady. In part to refute any notion that our client was even partly responsible for her injuries, we showed the extensive efforts made by our client to be a telTific mother and provider for her children, and even her children's friends, to be an MVP-type worker in her job, to show the great effort that she'd made to take care of everyone else, and to be responsible in ALL areas of her life before she'd been injured. We used these facts to develop the psychological notion and perception that our client WAS responsible and WAS reliable, and that it would be out of character for her to not take responsibility for what she could control. This approach will allow the jury to think less about penalizing the plaintiff, and more about finding a legitimate reason to excuse any such failure. At the same time, our client's lifetime of taking charge and taking responsibility in the different areas of her life provided a stark conh·ast for the defendants' failures to acknowledge and accept responsibility for what was in their control.
4. Rules of the Road- The concept of there being rules which govern everyone's conduct is not a new one. We are taught that we must follow rules for our behavior as young children. Those mles gave us stmchn·e, and in many circumstances, they assured us of safety. "Look both ways" is a universal guideline that applies in almost any settings, as does "Look before you leap" and "Measure twice, cut once". These simple concepts can be applied to many contexts. Your stmy should incorporate "rules" by which the defendant's standards should be measured. These rules, introduced in your story, will give the jurors a measuring stick to gauge the evidence they hear from both sides. One rule we used repeatedly throughout the Tumer case was that "The one thing that a tracheostomy patient can't have is a blocked trach tube". Another was, "If there's bleeding, you should call a doctor."
5. When you tell your story, and describe what happened, tell the story in present tense, as though it is happening now. Plan your story as if you were creating a film. Many jury consultants advocate the use of story boards to map out the course of your story. Each board reflects a scene or point of the story. You should understand the importance of sequencing of your story. People tend to remember beginnings and endings. In the story of your case, you will typically want the jury to be focusing on what the defendant did wrong, rather than your client's conduct, and so you might want to begin your story with the defendant, who he was and what his choice of conduct was that brought about the events which injured your client. Use psychodrama techniques to bring the court and jury into the scene. You are empowered to enable the court and jury to see your story any way you want them to, choosing the perspective you want them to see, the level of detail, and every fact you want them to know. Use objects in your courtroom to represent landmarks from the scene. Let the jury envision what you're talking about by bringing the scene into the courtroom. It's more inviting and draws them in to the story if they can experience the events themselves as you tell it. As you go through the story, pay attention to making each phrase advance the story. Your story will force the listener to envision what you're saying.
"When it comes to which of our three primary sensory systems are used to process and "make sense" of any case story: 1) words and phrases (auditory), 2) sights and
5

images (visual) and 3) sensations and emotions (feeling), it is the second one, visual imagery, that is the most influential when building the embodied nanatives that lead to a pmiicular leaning or eventual judgment. Of course, this makes complete sense. You really can't appreciate a human narrative without seeing the humans involved in the events. How many times have you thought "the movie wrecked the book," or maybe the opposite, how the movie predetetmined what you saw when you read the book." Eric Oliver, "Show Will Tell, Managing Mental Images with Legal Decision Makers", 2015.
6. Use of Phrasing: Use active phrasing, and think about what is envisioned by your words. In the "Show Will Tell" miicle, above, Eric Oliver gives examples of a variety of language choices in different case settings which can steer the listener in different directions:
Nursing Homes:
"Fall" v. "Drop." You only need to see one person, the injured plaintiff, to see a fall, but, it takes seeing two people for someone to get dropped. "Lift" v. "Lift and Transfer." In the first, a lift is a fi·iendly hand up; in the second, it is a serious matter of maintaining patient health and safety through the transfer.
Car Wrecks:
"Accident" v. "Wreck" or "Crash." One is like lightning striking, it's unexpected and through the fault of no one person; the other two are not.
Medical Practice:
"Care Given" v. ''Actions Taken" or ''Actions Withheld." The first invites imagery that overrides any claim of neglect itself; the second two reinforce imagery of neglect.
Claim Language:
"Failed to" v. "Did Not Do Properly." Which picture actually invites decision makers to envision "good intentions" on the part of the bad actors? Ironically it's, "okay, he failed, but he meant well and we should let him keep at it," instead of the more straightforward, "he did not do it right, although doing it right is his job."
Dmnage Atn·ibution:
"The Plaintiff Develops/Acquires More Consequences" v. "The Plaintiff Is Forced to Go Through These Consequences. " In the fmmer version, the plaintiff is seen as the only apparent party actively affecting his or her condition; in the latter, the plaintiffs condition is actively linked to the effects
6

of negligent actions. This particular kind of mismanagement of mental imagery is the bane of catastrophic injury work.
Tenns of Att:
"Minor Head Injury" v. "Injury to the Brain. "No permanent or serious images are allowed to be seen or imagined in version one; in version two there is no doubt as to what is there to see.
7. Understand the power of visuals. Jurors are far better at looking than at listening or reading. Each impmtant point of your case should have a visual exhibit that brings home the point. Think about what images you' d want the jury to be thinking about when they deliberate case. Use images to emphasize the truly pivotal points.
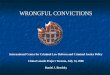
In the Turner case, our client's tracheotomy had been occluded by blood and blood clots. The defense disputed that there was any significant bleeding from our client's tracheostomy, while we contended there had been a great deal of bleeding, as evidenced by the testimony of a family member. The hospital chmting was sketchy, and didn't provide much description of bleeding. None of the hospital people ... nurses, residents and doctors, provided much suppmt to us beyond what had been written in the hospital record. However, the hemoglobin levels, which had been recorded every day since our client's admission, showed a drop from 10.1 to 6.6, representing a significant loss of blood, over a shmt time. We demonstrated that fact by the diagrmn below, which showed the comt and jury without a doubt, how much blood was actually lost over the relevant time period based on the hospital ' s own lab values. The defense argued that the lab results were either spmious or caused entirely by hemodilution as a result of the blood products, fresh frozen plasma and packed red cells that she had received dming that time. Our chart easily showed the jury what the hemoglobin levels should have been ifthere had been no bleeding.
2 Units IH Pockod Rod Blood Co lis I b. L Mercy Hospita e mog o In e ve s
1 :25-11120 ~~:!;:~~~ 400cc PAIC 16 -
~-
I
Hospital's Reference Range • 15.5 to 1 2 I
1< -
-."' I ' -j b pec1•d Hemog lobin
l eve l tf N o Blood los•
\ ' .,~ ,, '1> ~ '\
13
12
.... ~~
.,,. ~ ! 9~
:£..-- ~ t -- ~" ~ .,<>
\ -I>
2121105 ' 2/2210 5 ' 2123105 ' 2/24/0 5 ' 2125/05 ' 2/26/ 0S 2127/0S 2/28/0S 311/05 3/2105 3/3/ 05 21 :~3 4 :43& 11:0 5 5:27 •1:50 6 :1S. 5:26 4 .47 & 1&:'- 3 1;50 &6.32 2 .4!t
7

You can overdo visuals, though. Less is often more effective than oversaturating with visuals. The effectiveness can be diluted if too many are used ... Especially with PowerPoint. Noted jury consultants and educators, David Ball and Joshua Karton often joke, "Friends don't let friends overuse PowerPoint". Their reasoning is simple. When you are using PowerPoint, you necessarily are asking the jury to focus on the presentation, and away from you. Sometimes, you will have to even darken the room so that the screen is clearly seen. If you are telling a story, you want you and your surroundings to be the actors and the scene. You want the live human connection between you and the jury.
PowerPoint can be a valuable tool for the presenting lawyer, as long as it's the lawyer who is viewing it and not the jury! Put your PowerPoint presentation on a laptop that faces you as your talking, so that you can use it to keep your place in your story. Keep it simple ... give yourself cues instead offumbling with notes.
8. There is no "standard" man or woman who can be measured in arguing the extent of damages, and as one noted jury scholar, Hany Kalven, Jr. noted about the jury's ability to measure the worth of human injury and suffering for each individual plaintiff: "There is in brief no standard man, no reasonable man afoot in the law of damages .... And the jury is of necessity left free to price the hann on a case by case basis." Hany Kalven, Jr., The Jury, the Law, and the Personal Injury Damage A;vard, 19 Ohio St. L.J. 158, 160 (1958).
In a catastrophic injury or wrongful death case, there is a story to tell about both the harms and losses that have been sustained by the plaintiff. The harms are the actual, tangible, injuries, while the losses are all of those impacts that the injuries have caused. St. Louis attorney, David Damich, couched the argument for the value of every person' right to the life they had nicely:
"There is not a soul on this earth that lives that does not die. But there is not a soul on this earth that has the right to carelessly shorten one minute of another person's days.
If you could be on earth for just one day - one day to watch the sun rise, one day to smell the air, the perfume, the stink, one day to look in the eyes of your children and tell them you love them, goodbye, and that it will be all right- if you had that day, what is the value to you of that? That is the first day that defense counsel says is worthless."
We all live three "lives" ... our lives at home, at work and our lives everywhere else. Each of these arenas contains witnesses to and evidence of who and what we are as individuals. Each arena should be explored before and during discovery to identify the best proof of what your client, as well as the client's family, has had to deal with as a result of the injuries sustained. Jurors are always confronted with at least the innuendo that their verdict is something akin to a lottery award. They may feel that a plaintiffs verdict is a win or a gain for the plaintiff
In fact, the verdict is purely an attempt to make the plaintiff whole ... to put him back in the position he would have been in if he had not been injured. It is critically impmiant for the plaintiff's attorney to frame the matter of compensation in a way that clearly shows was taken away from the plaintiff as a result of the defendant's wrongful actions and choices. Economic losses are, no doubt, in many cases, important. In the world of catastrophic injury cases, though, they are often
8

the least significant losses that the plaintiff has suffered. The pmiion of the verdict that replaces economic losses is just that. From an economic standpoint, that part of a verdict simply puts the plaintiff back where he/she would have been economically if the injury had not occurred. That pmi of the verdict does nothing to compensate the plaintiff for their pain and suffering, loss of a normal life, disfigurement, etc. Each of those damage elements must be addressed in the verdict, and in order for that to happen, they must addressed in your evidence and in your story.
"Disability, by definition, involves the loss of some ability, some kind of normal physical functioning. It could be, and in fact has been, m·gued that such abilities, or capabilities, are important for welfare even if they have little or no impact on hedonics. This is the central insight of the capabilities approach to welfare proposed by Arnmiya Sen (1985, 1992) and elaborated on by Mmiha Nussbaum (2000). It was originally designed to deal with problems of social injustice, and specifically the idea that people may be content with poor social and physical conditions or injustice because they have adapted to them or have never experienced anything else. As Nussbaum (2000, p. 114) expresses it, aspirations for a better life can be squelched by habit, fear, low expectations, and unjust background conditions that deform people's choices and even their wishes for their own lives." Sen and Nussbaum delineate a series of central human capabilities, such as health, fi·eedom from assault, political voice, property rights, equal employment, and access to education, as well as others that involve self -actualization, such as expression of emotion, affiliation with others, and recreation, that they view as universal desiderata. Some of these capabilities, such as health and recreation, m·e very likely to be undermined by disability and hence, it could be argued, warrant compensation even if an individual is unaffected hedonically because of adaptation or for other reasons." Peter A. Ubel and George Lowenstein, "Pain and Suffering A wards: They Shouldn't be (Just) about Pain and Suffering", Journal of Legal Studies, vol. 37 (June, 2008), University of Chicago.
The Family.
It is important that family members in injury cases focus on what the injured person has lost, and not on the burden the family member has to bear because of the injury, UNLESS there is a claim by that person for lost consmiium or services. As an example, a plaintiff who had been independent, and a parent, but has been disabled by their injuries, may now require the support and attendant care of their fmnily. There is no doubt, regardless of the love and desire the fmnily has to help, that there is a burden placed upon and felt by the family members. The loss, however, is what the plaintiff has suffered. The injured parent may very well suffer enormous embmTassment and loss of dignity if his/her child's care to change diapers is needed. Safety and security measures may be needed for the parent, and they may feel the same loss of their own ability to protect themselves or their children. This loss is a keen one. The freedom to choose how to live each day, is supremely valuable. Liberty and independence are rights to which we are all entitled. Our criminal justice system is based upon the need to establish guilt beyond reasonable doubt in no small part because of the severity of punishment which is dealt for serious offenses. The punishment for criminal conduct is the taking away of libmiy, the loss of independence. The victim of a catastrophic injury has often been confined, against their will, to a jail cell whose walls are defined by the limitations of their physical and cognitive abilities.
9

Use of Visuals and Anecdotes
Visuals and anecdotes give the comi and jury context and real-life illustrations of what consequences occurred in the past and a basis to fmm some feelings about what might have been. Stories, always told by others whenever possible, about acts of kindness, work ethic, stories that paint a picture of the client's nature and character tell the jury what kind of person was lost because of the injuries or death.
In the Turner case, om client was a single working mother of 5, and as a result of the injuries that were the subject of the case, she lost her employment, and every aspect of her life that she'd enjoyed. She'd loved people, and her job, and she loved caring for her kids and her kids' friends. In voir dire, we used a very brief clip of our day-in-a-life video to show the jurors that a) they were there to decide a very serious and important case; and b) make sure that the jmors who heard the case would be able to tolerate the evidence we would be submitting without being upset; and c) to show the jmy why we were asking if they would be able to grant a verdict in the millions of dollars if it was justified by the evidence. We had a co-worker testify to how valued and reliable an employee Jeanette had been, how she had loved to deal with people, and how hard she worked each day to get to her job and take care of her family's needs too. Her children and others talked about how she took care oftheir friends, often providing them with food, clothing and housing for long stretches of time.
Day-in-a-Life videos can be extremely useful in communicating how the plaintiff's injuries translate to their daily life. You have a real oppmtunity to develop the story of your client's joumey by compiling pre- and intra-case documentation of who yom client was, what they' ve gone through, what they and their life has become and what it will be in the future. There is a "danger" in waiting until you' re preparing for trial to stmi the recording of that story. The jmy might get a good idea of how the plaintiff ended up, but miss the story of what it took for them to get there. Whenever possible, stmi collecting photos and videos of the plaintiff as early as possible. Go to family and friends and find whatever you can recover ofthe plaintiffs life before he or she had been injured, and especially if the case involves ongoing medical care or significant disability, have periodic day-in-a-life videos and photos done so that the court and jmy can be taken on the plaintiffs journey from the time of injmy to trial.
During the damages pmtion of our closing argument, we displayed one photo of om client, as she'd been before her injuries. The jury was reminded of the woman our client had been, and how catastrophically different she had become as a result of her injuries.
10

9. With your visual exhibits, be frugal with the use of text. Keep it to a minimum. You want the image of the exhibit in the jurors' minds to be the message.
10. Medical and technical drawings: Use as little labeling as possible. The drawing itself should be simple and make your point! It should be designed in a way that it can be easily seen, and quickly understood. A good rule to live by is to limit each exhibit to making one point.
11. Talk to your exhibits person about using colors for emphasis and contrasting. The eye notices the difference between just two or three colors more readily than the differences amongst four or more colors. If you know that you may be using colors that might be difficult for jurors who might be color blind, and you can't change your color scheme, make sure you address any visual difficulties in voir dire. Better yet, though, think again about your color choices!
12. Photos should have matte/flat finishes which don't reflect comtroom lighting or glare.
13. TEST! Your exhibits are intended to be used to make some of your most impmtant points. Make sure they do, and test them with people, even if it's just the people in your family or office. Show them for a few seconds and see what people think they portrayed. Ask them again the next day ... What did they take away from the exhibit? How did it make them feel?
Resources:
I. Show the Story, the Power of Visual Advocacy, by WilliamS. Bailey & Robert W. Bailey, published by Trial Guides, LLC 2011
2. Pennington and Hastie, A Cognitive Theory of Juror Decision Making: The Story Model, 13 Cardozo Law Review 519 (1991); Carlson and Russo, "Biased Interpretation of Evidence by Mock Jurors," Joumal of Experimental Psychology, Applied (2001), Vol. 7, No.2, 91-103.
3. Oliver, Eric, Facts Can't Speak For Themselves: Reveal The Stories That Give Facts Their Meaning, NITA, Louisville, CO, 2005
4. Zaltman, Gerald and Lindsay Marketing Metaphoria: What Deep Metaphors Reveal about the Minds of Consumers, Harvard Business Books, 2008
5. Peter A. Ubel and George Lowenstein, Pain and &iffering Awards: They Shouldn't be (Just) about Pain and Suffering, Joumal of Legal Studies, vol. 37 (June, 2008), University of Chicago.
6. Rick Friedman and Patrick Malone, Rules of the Road, Trial Guides
7. David Ball, David Ball on Damages 3, Trial Guides
8. Mark S. Mandell, Case Framing, Trial Guides
9. Carl Bettinger, Twelve Heroes, One Voice, Trial Guides 11

make an independent opinion on the cause of her in this case, I do have to apologize. This has 2 injury, and subsequently removed the comments 2 been bothering me for three weeks since I gave 3 because I did not form an opinion of what 3 the opening statement. 4 happened. 4 I used the "R" word during opening 5 THE COURT: All right. Thank you, Ms. 5 statement to describe the way in which Jeanette 6 Dzik. 6 felt that other people looked at her, that 7 And now, Mr. Lane, your closing 7 that's the way that people looked at her, and I 8 argument. 8 am sorry that Jeanette feels that way, and I'm 9 CLOSING ARGUMENT 9 sorry that I used that word. It wasn't a good
10 MR. SCOlT LANE: May it please the 10 reason, and I don't feel good about it. It was 11 Court, counsel, Ladies and Gentlemen of the 11 how she felt, and that is not a good excuse, and 12 Jury. Good morning. 12 I am sorry if I offended anybody. It was 13 You know, when I spoke to you about 13 offensive to me. 14 three weeks ago, I said that I am giving you an 14 I also want to apologize about my habit 15 opening statement, and I considered that opening 15 of sometimes beating a dead horse during an 16 statement to be a promise, a promise of what the 16 examination, and I did that, because frankly, I 17 evidence was going to show in this case, and I 17 was afraid, I was afraid that I was going to 18 told you during that opening statement, I said 18 miss something or that I wasn't going to make my 19 you're going to see the medical records, these 19 point perfectly clear, and I wanted to do my 20 medical records, and I told you, you were going 20 best for Jeanette, and if somehow, some way that 21 to see the medical records from Mercy Hospital, 21 bothered you, again, I apologize. 22 and I told you that those medical records really 22 Now, the last thing I want to do is I 23 were a chapter that was written about Jeanette's 23 really want to thank you on behalf of all of us 24 life, a very, very important chapter that was 24 for serving as a juror.
37 39
written about Jeanette's life, a chapter that 1 It sounds like you guys are enjoying 2 was written by the hospital through its agents, 2 yourselves with each other, which is nice, but 3 doctors, nurses, those physicians and nurses 3 we also know that it's not easy, it's not easy 4 that they agreed they're responsible for their 4 to spend this much time away from your family, 5 conduct, and I told you, you were going to 5 away from work, so we all really appreciate 6 actually see the pages of the record, see the 6 that. 7 pages of that chapter that they wrote, and that 7 Now, your Honor mentioned that I am 8 you were going to really get an opportunity to 8 going to be giving -- or that we are going to 9 understand that chapter, and I told you, I 9 give closing arguments, and counsel has an
10 promised you that after you had an opportunity 10 opportunity to speak, and we will also have an 11 to read that chapter, you were going to come to 11 opportunity to speak, but Steve Lane and I are 12 the conclusion that the hospital was responsible 12 dividing up this part ofthe closing argument, 13 for Jeanette's brain injuries, because the 13 liability and damages, meaning, I'm going to 14 hospital did not do what was reasonable under 14 discuss why the hospital is at fault here, and 15 the circumstances that they were presented with. 15 Steve is going to discuss with you what injuries 16 The hospital is responsible for 16 were caused by the hospital's negligent conduct. 17 Jeanette's brain injury. That was a promise, 17 There are several points frankly that 18 that was a promise, and I can say without 18 we agree on, the hospital and us. 19 hesitation that everything that I told you, that 19 No. 1, Rule No. 1, keep the trach open. 20 I promised you in opening statement came true. 20 It's the only way the patient is going to 21 I told you what the evidence was going 21 breath. You need to keep the trach open. 22 to be in this case, and I meant that as a 22 Coumadin, when a patient is on 23 promise, and I kept that promise. 23 Coumadin, we know, everybody agrees that the 24 Now, before we talk about what happened 24 patient is at an increased risk of bleeding, an
38 40
Pages 37 to 40 Mccorkle Litigation services, Inc. chicago, Illinois (312) 263-0052

1 increased risk of clotting as a result of 2 bleeding, and at an increased risk of occlusion 3 of the trach because of the bleeding and the 4 clots that form. 5 Occlusion, everybody agrees that when 6 there's occlusion, that there is a possibility 7 that the patient can suffer severe brain damage 8 as a result of that occlusion, and occlusion can 9 result in clots.
1 0 Inflated cuffs, everybody agrees that 11 when the cuff is inflated, that prevents blood 12 and clots from traveling down the trachea, and 13 prevents it from having an opportunity to clog 14 the distal, the bottom part, of the trachea and 15 cause an occlusion, and everyone agrees that 16 when the cuff is inflated, the patient cannot 17 talk. So, if the patient is talking, that means 18 the cuff is at least partially deflated, and if 19 partially deflated, that allows blood and clots 20 to travel down below the trachea and potentially 21 occlude the trachea. 22 Vital signs. Everyone agrees that if 23 there is a total occlusion, the vital signs are 24 not going to be stable. They are going to be
41
1 abnormal. 2 And everyone agrees -- and this is 3 important -- that when there is partial 4 occlusion of the trach, the vital signs can be 5 normal. 6 One last point that everybody agrees 7 on. Recordkeeping. Recordkeeping is important. 8 It's important that the record be accurate, 9 complete and timely. We all know that the
1 o physicians and nurses rely on the accuracy of 11 records in providing appropriate treatment to 12 patients, and also reliability of records. 13 When records are prepared, they are 14 prepared close in time to the event. They are a 15 whole lot more reliable than that person's 16 memory ten years later, especially after a 17 lawsuit has been filed. 18 You are going to be-- you are going to 19 receive several instructions from your Honor, 20 and one of the instructions is going to be the 21 burden of proof instruction. 22 The plaintiff has the burden of proof 23 to prove the elements in this case; meaning, 24 that we have to prove beyond -- by a
42
preponderance of the evidence; meaning, more 2 probably true than not true, that the fact took 3 place. 4 What does that mean? It means if you 5 have a scale, and you have a feather on this 6 side, and the scales are equal, and you have a 7 feather on this side, ever so slightly, that is 8 our burden. Just a little bit difference in 9 weight, a little bit lower, the weight of a
10 feather, preponderance of the evidence. 11 Now, we welcome that burden. We 12 welcome that burden. 13 Now, Jeanette had a trach, and she was 14 on Coumadin, and under those circumstances it's 15 like Mercy Hospital was like a lifeguard for 16 Jeanette. She relied on them. A lifeguard not 17 for, let's say, a college swimming team swimming 18 in three feet of water, but like a lifeguard for 19 toddlers in a swimming pool, because we all know 20 that if the lifeguard is not attentive even for 21 a split second, that can lead to absolute 22 tragedy. 23 Jeanette was helpless in the hospital 24 relying on the doctors just like a toddler
43
1 relies on the parents or the lifeguards at the 2 pool. 3 And that is what happened here, that 4 the hospital was not attentive. The hospital 5 did not provide the care that Jeanette needed in 6 that situation. The hospital failed to provide 7 the attention that she needed and that she 8 required during that hospitalization. 9 It all started February 27th, late into
10 the evening, into the early morning, and 11 continued on all the way through February 28th 12 until about 12:45, and we will hear about that, 13 but through that entire time off and on 14 bleeding, coughing, coughing up clots, coughing 15 up clots through the trach, you heard all about 16 the evidence of bleeding throughout that period 17 off and on, and now she relied -- Jeanette 18 relied on the hospital to do what was 19 appropriate under the circumstances to prevent 20 occlusion of that trach, to allow for finding 21 the bleed, to allow for treating the bleed, and 22 most importantly, prevent occlusion of the 23 trach, the No. 1 rule. 24 So, how was the hospital negligent?
44
Pages 41 to 44
McCorkle Litigation services, Inc. chicago, Illinois (312) 263-0052

And again, negligence means that they failed to the same day in the evening another bleed occurs 2 do what was reasonable under the circumstances. 2 in the cath lab. A good thing happens. A nurse 3 You heard from Dr. Cooke, and you heard 3 sees Jeanette bleeding. Lo and behold, good 4 from Dr. Graham. 4 thing, calls a doctor to have her checked out. 5 Dr. Cooke is a nursing specialist, and 5 She's bleeding. That was appropriate. 6 you know all about her credentials, Lieutenant 6 Dr. Cundiff came down, repaired the 7 Colonel in the Army and all the awards and years 7 bleed, very nicely done, has a plan, this 8 and years of experience, and you heard from Dr. 8 patient bleeds again, we're going to give fresh 9 Graham, super qualified physician, and you saw 9 frozen plasma. You heard all about that. That
10 his demeanor on the stand. Couldn't be a nicer, 10 is to stop bleeding. 11 more honest, more qualified physician. 11 So, he repairs the bleed, walks out of 12 You heard what they said. First of 12 the cath lab, and lo and behold, a half hour 13 all, Jeanette came in for an infection. We all 13 later Nurse Chibucos says, Dr. Cundiff, she's 14 know that. It was a life-threatening situation, 14 bleeding again. 15 but we also know unrebutted, meaning no evidence 15 And remember why Nurse Chibucos called 16 that contradicts this, we also know that she got 16 Dr. Cundiff, because Annette, Jeanette's sister 17 past that. That as of February 27th and 17 asked Ms. Chibucos to come see her sister, see 18 February 28th the infection was virtually gone, 18 Jeanette, and said she's bleeding, and Nurse 19 and they were talking about discharging her. 19 Chibucos saw the bleeding, and said I'm going to 20 So, this infection, yes, it's true, it 20 call Dr. Cundiff. 21 was serious, and that's why the trach was 21 So, then Dr. Cundiff comes. We don't 22 needed, but it's a non-issue, because the i 22 know exactly what he did. He doesn't have a 23 infection was done. She was on her way out. 23 note, but he does have orders, which is 24 So, what happened on February 28th? In 24 critical, because that shows he was there, and
45 47
the morning -- well, actually late at night on at that point in time he enters an order saying 2 the 27th and into the morning, bleeding started 2 let's give the fresh frozen plasma that he had a 3 after six days of not having any bleeding 3 plan for. That's all good. That's all good. 4 whatsoever, but was it just bleeding? No. It 4 The problem is after he orders the 5 was coughing up blood through the trach. 5 fresh frozen plasma, what does he do? He 6 Concerning? I think so. Dr. Cooke says it was 6 leaves. He leaves. 7 very concerning. Nurse Krooswyk, hospital 7 Now, why is that a problem? Well, he 8 nurse, not so concerned. 8 can leave as long as he at some point checks in 9 Now, Dr. Cooke said the standard of 9 on his patient that has now had three episodes
10 care under those circumstances because you're 10 of bleeding in the last 17 hours. That's a 11 worried about the bleed, you're worried about 11 problem. 12 blockage of the trach, is to call a doctor to 12 And the standard of care required Dr. 13 get the patient checked out. 13 Cundiff to follow up on this patient, to give 14 Nurse Krooswyk says no worries, you 14 instructions to the nurses that are watching 15 don't need to under those circumstances. Keep 15 this patient, and to follow up on this patient 16 your fingers crossed. Hopefully there won't be 16 that's been bleeding. 17 any blockage. 17 He didn't do that. That was a 18 Now, that time Jeanette was lucky, 18 violation of the standard of care. If he had 19 because she coughed up blood through the trach. 19 followed up, if he had made a call, if he had 20 It was a difficult situation obviously, but 20 come see the patient, at some point in the 21 luckily nothing clogged the trach. So, she went 21 evening he would have seen the patient, he would 22 on for a little while. 22 have found the cause of the bleeding, he would 23 Now, what's the next time that's 23 have treated the bleeding, and he would have 24 important? February 28th, 5:00 o'clock. So, 24 protected the airway, but he never followed up.
46 48
Pages 45 to 48
Mccorkle Litigation Chicago, Illinois
services, Inc. (312) 263-0052

So, that never happened. of them. Dr. Cundiff never followed up. 2 Now, another thing about that episode 2 Now, what happened after that? 3 of the bleeding after the cath lab is Nurse 3 Jeanette continued to bleed. She continued to 4 Chibucos. 4 cough out blood clots. She continued to talk. 5 Do you remember Nurse Chibucos? Do you 5 The cuff remained deflated or partially 6 remember when she was called to testify, and she 6 inflated, however you want to look at it. 7 was represented by the hospital at that point in 7 Should a doctor have been called? 8 time, and you remember how she talked about the 8 Absolutely. Would a doctor have identified the 9 fact that Jeanette was talking, and how 9 bleed? Absolutely. Treated the bleed? Sure.
10 difficult it was to admit that Jeanette was 10 Kept the airway open? Absolutely. That would 11 talking even though she gave a recorded 11 have been the goal. 12 statement that says she was talking, even though 12 Now, at-- I'm sorry -- at 8:50 p.m. 13 she gave a deposition where she said she was 13 Nurse David sees Jeanette. She reinforces the 14 talking, and she finally admitted, yeah, that's 14 padding. Now, Nurse David said, oh, I do that 15 what I said, and she remembered the fact that 15 sometimes. What did Nurse Krooswyk say, their 16 Jeanette was talking, and this is important, she 16 expert? That's because she was bleeding at that 17 said I remember that conversation, because 17 time. That's why she did it. That's 18 Jeanette said can you believe this all started 18 reinforcement. You can't hold the blood, so you 19 with a tooth problem? Very specific memory. 19 reinforce it. She's bleeding. 20 We know that Jeanette was talking at 20 The standard of care according to Dr. 21 that point in time. Why is that important? Why 21 Cooke at that point in time is again, call the 22 is that important? 22 doctor. Was that done? No. That was a 23 It's important because we know then the 23 violation of the standard of care. 24 cuff is deflated. So, now you have Jeanette 24 This continued on, as you know, from
49 51
with a cuff deflated, because she could talk, Annette's testimony, this continued on bleeding, 2 and she is bleeding. Not a good combination for 2 coughing up blood clots and then at 11:00 p.m. 3 keeping the trach clear. 3 Nurse David enters a note finally, another note, 4 What else did Nurse Chibucos do? She 4 and at 11:00 p.m. the note says that the patient 5 saw the bleeding, and she gave Annette gauze so 5 stated -- meaning talking -- we all know that's 6 that she, herself, could dab around the trach 6 what it means, it's not constantly writing, 7 area and help control the bleeding in that area 7 she's talking, the evidence supports that she's 8 and help keep Jeanette cleaner. 8 talking plain meaning of these records, she 9 Remember she said there was blood that 9 stated that these clots are choking me, and
10 was trickling around on to her gown, Annette was 10 Nurse David noted that the patient continues to 11 using gauze to help control that bleeding, and 11 cough up blood with clots. 12 that is important, as you know, later on. 12 What does continues means? It means it 13 Now, the reason Nurse Chibucos fought 13 was happening before, and we know that it was 14 me so hard on that talking, because somehow, 14 happening before. We know it from Annette, and 15 some way she knew the importance of the cuff 15 we know it from the record. 16 being deflated. 16 So, now she's continuing to cough out 17 Now, Dr. Cundiff left. We know that is 17 blood with clots. Again, reinforces the 18 below the standard of care to do that, and who 18 dressing. Why? She's bleeding. This is just 19 did he leave Jeanette with? This patient that 19 two hours later, she's reinforcing the dressing 20 has bled three times in the last 17 hours, who 20 again. There's a lot of bleeding going on, but 21 did he leave Jeanette with? He left Jeanette 21 this time Nurse David calls Dr. Noriega. 22 with Dr. Noriega and Nurse David. 22 Perfect. That's good. The only problem is Dr. 23 Between the two of them they had one or 23 Noriega did not come, and we know that because 24 two trach patient's experience between the two 24 the record clearly said she didn't come in the
50 52
Pages 49 to 52
Mccorkle Litigation services, Inc. chicago, Illinois (312) 263-0052

sense that there is absolutely nothing to 2 indicate that she did come, and I'm not going to 3 go through that. You have sat through that a 4 million times through every single witness, but 5 we all know that there is absolutely no order, 6 no note from either one of them that indicates 7 that Dr. Noriega was at the-- that Dr. Noriega 8 came to see this patient. 9 Now, this was not a hello, you know, in
10 other words, the doctor would be walking by the 11 patient's room and saying hi, how are you, this 12 was a page. This was a page to come see this 13 patient that was now continuing to cough out 14 blood clots and was talking about choking. 15 If a doctor goes to see a patient and 16 responds to a page like that, you would think 17 they enter an order, they write an order if it's 18 true everything is okay. At least do something 19 to indicate that you were there to check on this 20 patient. Absolutely nothing there. 21 You remember Dr. Derman testifying, 22 well, you know, if you wrote everything down, 23 that you wouldn't have time to even treat the 24 patients, you remember Dr. Derman saying that.
1 Come on. How long does it take to 2 write this patient is doing fine? That's 3 insulting. 4 Of course, Dr. Noriega did not see --5 and I'm not saying that Dr. Noriega is a liar. 6 I've never said that about anybody in my life, 7 quiet frankly, that they're a liar. 8 I think she's mistaken, just like Nurse 9 David, when she was testifying on the stand, she
53
1 o said, you know what, maybe I am mistaken between 11 11:00 and 12:30 as to whether Dr. Noriega had 12 come-- whether Dr. Noriega came. I think Dr. 13 Noriega is confused. I think she can't 14 remember, and that's not so weird. You know, 15 it's ten years ago, but she's confused. She's 16 confused, because there is absolutely no 17 indication that she came. 18 And you remember Annette saying, yeah, 19 Dr. Noriega had come, but I remember a period of 20 time where she just stopped coming, and that 21 period of time was between 10:30, and that's 22 what Annette said, and the time that Jeanette 23 arrested. 24 So, I think the evidence is very clear
54
that she just did not come at that time, and 2 everybody agrees that if Dr. Noriega did not 3 come in response to the page, that was below the 4 standard of care. 5 You've got to come. If you don't, for 6 whatever reason, that's below the standard of 7 care. 8 And also, Nurse David was also -- her 9 conduct was below the standard of care, too,
10 because she's got to make sure that a doctor 11 comes and sees this patient. 12 This is a patient who is coughing up 13 blood clots through the trach. There is a risk 14 of blockage here. You need a doctor to find out 15 what is going on with the bleed, treat the 16 bleed, identify the bleed, and most importantly, 17 make sure the airway is clear. 18 That didn't happen, and it didn't 19 happen at 11:15, 11:30, 11:45, 12:00, 12:15, 20 nothing done to get a doctor to see this 21 patient. 22 Now, at 12:30 Nurse David finally sees 23 the patient and says -- and she had seen the 24 patient and seen Jeanette during that time
55
1 period, there was a time, you know, where she's 2 checking vitals, her vitals are normal, but, of 3 course, there's partial occlusion, and we all 4 know, partial occlusion you can have normal 5 vitals, but as Nurse Krooswyk said, again the 6 defense expert, you can't just look at the vital 7 signs, you've got to look at the patient. Well, 8 look at the patient. She's coughing up blood 9 clots through the trach. She needs to see a
10 doctor, and no doctor is seeing her. 11 So, now Nurse David at 12:30, she notes 12 the patient is still choking, and she decides 13 I'm going to page Dr. Noriega again. Remember 14 that note, again. Doesn't say Dr. Noriega was 15 just there. She's paging her again, and that is 16 what nurses do when they're trying to cover 17 themselves, they put again to make sure that 18 everybody knows that they had tried to call this 19 doctor an hour and a half earlier. 20 So, Nurse David contacts Dr. Noriega, 21 and she notes in her note that Dr. Noriega came, 22 but it's too late. It's now 12:30, it's an hour 23 and a half later. She's been coughing up blood 24 and coughing up clots, and we know about the
56
Pages 53 to 56
Mccorkle Litigation services, Inc. Chicago, Illinois (312) 263-0052

fresh frozen plasma, that she's been given four know what, you're going to hear from -- you're 2 bags of fresh frozen plasma, and I know you 2 going to hear from Dr. Reddy, and you're going 3 heard this a million times, but it's just not a 3 to hear that Dr. Reddy is going to testify that 4 coincidence that the fourth bag of fresh frozen 4 he saw her hands, Annette's hands, around the 5 plasma is given at 12:05, and we know that that 5 trach, around the actual tube, itself. 6 creates-- promotes clotting, and at 12:45, lo 6 That's not what he testified to during 7 and behold, she's coughing up blood clots. It's 7 the course of this trial. 8 not a coincidence, and it's silly, frankly, when 8 What he said was I really couldn't see 9 somebody says blood clots are being coughed out 9 where her hands were. They were just in the
10 under the physical examination portion of the 10 vicinity. My view was blocked, and guess what 11 note, and it says that's what the sister was 11 she was doing? Probably the same thing she was 12 telling me. 12 doing for hours and hours and hours, trying to 13 I'm sorry, I'm sorry, that just doesn't 13 control the bleeding. 14 make any sense whatsoever. 14 Jeanette continued to cough up blood 15 Now, Dr. Noriega notes blood-- the 15 and blood clots. She continued to cough out 16 coughing out blood clots at 12:45, obviously the 16 blood and blood clots. 17 fresh frozen plasma is working, and Dr. Noriega 17 This was going on -- this has been 18 notes that there's bloody gauze, a basin half 18 going on the whole night, and now it's at a 19 full of bloody gauze, that didn't just happen in 19 climax. Now its peaking. 20 20 seconds or 5 minutes or an hour. The basin 20 And what happens? Lo and behold, no 21 is half full of bloody gauze, and she notes that 21 mystery. She was coughing up blood clots, all 22 the sister has blood on her gloves. 22 the sudden she didn't cough up the blood clots, 23 Well, of course, she has blood on her 23 and we know that one or more of those clots that 24 gloves. She's been cleaning up her sister for 24 she had been coughing out got lodged in her
57 59
hours and hours and hours and cleaning it up and trach, and then her vital signs became abnormal, 2 putting the bloody gauze in the basin. 2 because there is now total occlusion, and then 3 At that time, 12:45, Jeanette is known 3 she arrested, and that was at about 1:00 a.m., 4 to be hysterical, running around stating I'm 4 and after that point in time the sequence is 5 choking, I can't breath. Clearly in respiratory 5 very unclear. It's unclear based upon the 6 distress. And most importantly -- not most 6 records, unclear based upon the depositions. 7 importantly --very importantly, this is all 7 I mean, the hospital physicians and 8 before Dr. Reddy gets there. All before Dr. 8 nurses cannot tell us exactly what happened and 9 Reddy gets there. In fact, these problems are 9 what sequence.
10 the reason that Dr. Reddy was called. 10 I mean, there's just so much that we 11 So, this respiratory distress was going 11 can do to try to figure out what happened in 12 on before Dr. Reddy even entered into the 12 what sequence, but we do know that several 13 picture. 13 things occurred at that point in time. 14 So, Dr. Reddy is paged, and based on 14 We know that there was aggressive and 15 what Dr. Reddy sees, he calls the universe; he 15 continuous suctioning. We know that there was 16 calls ICU, a resident, anesthesia, and the ENT 16 bagging that Dr. Reddy-- remember, Dr. Reddy 17 all based upon when he walks in the room what he 17 tried to bag. He wasn't able to. We don't know 18 sees going on. 18 exactly what he did. Then we know that there is 19 Now, Dr. Reddy, you remember what he 19 the anesthesiologist. The mystery man that 20 said during his testimony. He said I honestly 20 nobody knows. The anesthesiologist came, and he 21 couldn't see where Annette's hands were. 21 bagged the patient, but before he bagged the 22 Now, if you recall, I'm sure taking 22 patient, what did he do? He repositioned the 23 notes, you recall that counsel for Mercy 23 trach. 24 Hospital at the beginning of the case said, you 24 So, from what we see in the notes, we
58 60
Pages 57 to 60
McCorkle Litigation services, Inc. chicago, Illinois (312) 263-0052

know that there is plenty of bleeding going on I a blood clot that was present to be gone by the 2 just from the note, itself, and we know from the 2 time Dr. Cundiff gets there. 3 deposition testimony of Annette that she 3 And, you know, I don't know about Dr. 4 observed the bleeding, but how else do we know 4 Cundiff. That's up to you to decide the 5 that there was bleeding, substantial bleeding? 5 credibility of Dr. Cundiff, but I can tell you 6 We know from Dr. Bitran, the defense 6 one thing, that his note -- and he agrees with 7 expert, who basically agreed with everything Dr. 7 this -- that it's a hundred percent consistent 8 Hirsh said, and why not? Dr. Hirsh is probably 8 with a blood clot being present. 9 the world's top hematologist expert, again, in 9 Remember, he said partial -- the trach
10 the world. I mean, that's not an exaggeration. 10 tube was partially occluded when he got there, 11 You heard his testimony. For an hour 11 and partially occluded could be occluded by some 12 he was talking about his qualifications, because 12 sort of dislodgement or it could be by a clot. 13 that was important for you to know who this 13 You can't tell by looking at that note, 14 hematologist is, and he told us about the lab 14 but regardless, it doesn't matter whether he 15 work that was done at the hospital, the lab 15 found the clot or whether it was somehow 16 work, the hospital's lab work. Is that made up 16 suctioned or Ambu bagged during the 20, 17 somehow, how there was pints of blood that were 17 30 minutes that was going on. We don't know, 18 lost based on the lab work that came from the 18 but we do know that a clot is what lodged in the 19 hospital? 19 trach. 20 And we also know that she received two 20 Now, you're going to get an issue 21 pints of blood, packed red blood cells, two 21 instruction it's called, and you're going to be 22 pints. It's not preventive, meaning, okay, if 22 asked to decide these issues, and I am going to 23 somehow she bleeds, let's give this. No. 23 run through them very quickly. 24 Everybody agrees that packed red blood cells are 24 Did the nurses fail to contact the
61 63
given to replace blood loss. physicians and inform them of the medical 2 So, you're given two because the 2 condition of Jeanette Turner and request her 3 patient has lost two. You're giving one because 3 examination? Absolutely. The nurses throughout 4 the patient lost one. It's to replace blood 4 the entire night failed to contact these 5 loss. 5 physicians except for the one time that Nurse 6 We know from every angle Jeanette was 6 David contacted Dr. Noriega, but then didn't 7 bleeding and plenty of blood to allow for clots 7 follow up at all. 8 and clotting of a size of a 6.4 millimeter to 8 Dr. Cundiff failed to follow up with 9 block the distal tip of the trach. 9 the hospital staff to assess Jeanette Turner's
10 Now, we also know that even though we 10 condition and determine the effectiveness of 11 don't know the exact sequence, we also know 11 this treatment. He didn't do that at all. He 12 that, boy, there was plenty of opportunity for 12 just left, never followed up. 13 the clots -- clot or clots with her bleeding 13 Dr. Cundiff failed to identify and 14 going on to get blown out through the Ambu bag, 14 correct the bleeding. Dr. Cundiff absolutely 15 to be suctioned out through the Ambu bag, to be 15 did not do anything to identify and correct the 16 suctioned out by the suctioning device, and once 16 bleeding, because he never followed up. So, 17 it gets in the Ambu bag, then you remember, you 17 that's why he never identified and corrected the 18 can't see in the Ambu bag, you can't see through 18 bleeding. 19 the suction. Once it's suctioned and once the 19 Dr. Cundiff failed to prevent the 20 Ambu bag gets it, it's gone, we don't know. 20 occlusion. Again, same reason. He never 21 There is repositioning going on. So, 21 followed up, so he didn't know anything about 22 you've got suctioning, repositioning and Ambu 22 all this stuff that was going on, so how can he 23 bag going on, who knows what in the world 23 prevent the occlusion? 24 happened, but there is plenty of opportunity for 24 And then Dr. Noriega failed to assess
62 64
Pages 61 to 64
Mccorkle Litigation services, Inc. Chicago, Illinois (312) 263-0052

2 3 4 5 6 7 8 9
10 11 12 13 14 15 16 17 18 19 20 21 22 23 24
2 3 4 5 6 7 8 9
10 11 12 13 14 15 16 17 18 19 20 21 22 23 24
Jeanette, and we know she did, because she didn't show up at 11:00 o'clock, and didn't have an opportunity to assess Jeanette, and didn't to it at any time after that, and she admits that as well.
And Dr. Reddy, he failed to identify the occlusion of Jeanette Turner's airway and failed to restore Jeanette Turner's airway in a timely manner.
Now, you remember his testimony, that he tried to bag the patient right after the arrest.
Well, the problem is he wasn't able to, and he said, well, I tried, and their doctor, Dr. Derman said, well, he tried.
Well, he was the code leader. He was responsible for this patient during the code. He was with the patient when she apparently arrested.
You remember what he said, he said the anesthesiologist turned her a little bit and then was able to bag the patient.
Dr. Reddy has to be able to do that involved in a code, the code leader, and you
65
remember Dr. Graham yesterday testified by deposition, and he said, absolutely, Dr. Reddy, the standard of care would have required him to be able to reposition the trach in a timely manner, and because he didn't, Jeanette suffered brain damage, because for those several minutes that Dr. Reddy tried to bag the patient, but couldn't, Jeanette suffered brain damage.
Again, all he had to do apparently by his own testimony was turn it just a little bit.
So, we have satisfied our burden on these issues by way more than a preponderance of the evidence.
The bottom line is that it really didn't need to get to that point where everything climaxed at 12:45.
All we needed -- all Jeanette needed was for Dr. Cundiff to follow up like the standard of care required.
If he had followed up, he would have found out what was going on address, the bleeding, and again, most importantly, protect the airway.
The nurses needed to contact the
66
2 3 4 5 6 7 8 9
10 11 12 13 14 15 16 17 18 19 20 21 22 23 24
2 3 4 5 6 7 8 9
10 11 12 13 14 15 16 17 18 19 20 21 22 23 24
doctors and follow up with the doctors, and make sure they come and assess the patient, and the doctors again needed to evaluate and identify the bleed to protect the airway.
If we prove any of these allegations; A, B -- A through G, any of them -- it's not like we have to prove all of them -- if we prove any of them, again by a preponderance of the evidence, then the verdict should be in favor of Jeanette.
Now, as a result of the hospital's negligent conduct, a clot lodged in Jeanette's trach and resulted in brain damage.
How do we know that a clot is what lodged in her trach?
First, as opposed to dislodging, let's address dislodgement quickly.
The bottom line is there is absolutely no evidence whatsoever that there was any dislodgement or any dislodgement that caused the brain damage.
Everybody agrees that there is no note in the chart that indicates dislodgement is what caused the brain damage.
67
We've already talked about the only person, Dr. Reddy, the only person that saw anything that Jeanette -- or Annette was doing, and he's already told us under oath I couldn't tell -- so, that is really a non-issue, and then nobody else testified about the position of the trach until Dr. Cundiff, but again, Dr. Cundiff, what's the relevance, why is it important how Dr. Cundiff finds the trach when we know that he found it after suctioning, after bagging, and most importantly, after the anesthesiologist had repositioned the trach.
So, how Dr. Cundiff found the trach, there is no question, there is no issue. That's how the anesthesiologist put it. That's how the anesthesiologist put it.
How did -- what position did the anesthesiologist find it? I don't know. I'd love to hear from that anesthesiologist that worked at Mercy Hospital.
Now, there really is just absolutely no evidence, and I know you know that there is no evidence of dislodgement at the time of the arrest, and no evidence that says dislodgement
68
Pages 65 to 68
McCorkle Litigation chicago, Illinois
Services, Inc. (312) 263-0052

is what caused the arrest. 2 So, how do we know there's a clot, 3 there was a clot lodged? Let's look at the 4 testimony first. 5 First, there is Annette, Jeanette's 6 sister. Annette, you saw her demeanor on the 7 stand. She's telling the truth here, and what 8 does she say? She said that an African-American 9 nurse after the arrest came to her, gave her her
10 purse and said -- because Annette wanted to know 11 what was going on, she told her -- and remember 12 Annette described her in detail, okay -- and the 13 nurse said the doctor found a clot. 14 Okay. That's Annette, and I understand 15 you may be saying, well, that's her sister, and, 16 you know, maybe -- I don't know, I don't know, 17 but the bottom line is who else said that they 18 heard about a clot? Nurse Chibucos. Even 19 though she hated to just say-- admit that 20 Jeanette was talking, she had to admit that when 21 she came back to work at Mercy Hospital, close 22 in time after this happened. She was told that 23 a clot is what caused the problem with Jeanette. 24 That's pretty darn reliable.
69
· 1 Now, who else? Dr. Vern, remember Dr. 2 Vern? Dr. Vern was Jeanette's treating 3 physician at the University of Illinois. 4 Treating physician. It wasn't like we went to 5 him to get expert testimony. He was already 6 involved in her care and treatment, and he 7 expressed an interest in Jeanette and wanted to 8 find out what was going on. 9 So, he reviewed the records, and what
10 did he find? He found it was his determination 11 that it was clots is what caused the occlusion 12 in Jeanette, clots, that was his opinion, and 13 that that's what resulted in her brain damage as 14 well. 15 Very credible. Treater, not a retained 16 expert. Yes, he was paid for his time after he 17 got involved, but how did he get involved? We 18 didn't go out and try to find him, and that's 19 important. 20 Then we heard from Dr. Graham, we heard 21 from Dr. Cooke, and then you heard from Dr. 22 Hirsh. 23 And Dr. Hirsh, you heard him testify by 24 video. Could there be a more credible person?
70
1 I have never seen a more credible witness. He 2 was not attacked in any way, because he can't 3 be. 4 He is literally the top expert in the 5 world, and it's fine to say that, because it's 6 true, and he is telling us about everything --7 you know, a lot about blood, but a lot about 8 clotting, and what he told us, without question, 9 that it was clotting that is what caused the
10 occlusion in this case, in this case. 11 I think you need to put a lot of weight 12 in Dr Hirsh's testimony in any event. 13 So, that's not where it ends. I mean, 14 that's the testimony, but let's look elsewhere, 15 and you've heard a lot about clots. You've 16 heard a lot about clot notes, and I'm not going 17 to show them all to you, because you've seen 18 them, but you remember that there are six notes 19 in the chart written by doctors at the hospital 20 saying that after surgery the patient was on the 21 floor and went into respiratory distress and 22 arrest when a blood clot lodged in her trachea 23 causing anoxic encephalopathy. During this 24 event patient maintained blood pressure and
71
pulse, she was transferred to ICU, ENT removed 2 the clot. 3 This was just one of the notes, and you 4 remember that there is five other notes. Some 5 of them talking about 20 minutes of anoxia, and 6 you remember them -- you remember that as well. 7 It's not like these notes are exact 8 duplicates like somebody just sat there with a 9 stencil and wrote the notes, just copied them
10 over word-for-word, these are six different 11 physicians -- I mean, five different physicians 12 writing six different notes, including the 13 discharge notes where the entire course of the 14 hospitalization is discussed, and it's funny 15 because nobody questioned anything else about 16 any of these notes except for the fact that it 17 says a clot is lodged, but that's something that 18 the hospital doesn't like to hear. 19 So, that's the part of each one of 20 these notes that they don't like. 21 Now, what's interesting, and I'm piling 22 these over here for a reason, and you will see 23 in a minute, but what's interesting is that two 24 of the notes are consultations from Dr.
72
Pages 69 to 72
McCorkle Litigation services, Inc. chicago, Illinois (312) 263-0052

Milenkovich where Dr. Milenkovich requested a the anoxic event of 20 minutes. 2 consultation by a physician, and those notes 2 Now, there is one other --3 with the consultation from Dr. Milenkovich 3 THE COURT: Mr. Lane, you're at 45 4 indicate that a blood clot was lodged in the 4 minutes just to let you know. 5 trach. 5 MR. SCOTT LANE: 45 minutes? 6 Why is that important? Because Dr. 6 THE COURT: You have gone for 45 7 Milenkovich was Jeanette's attending physician 7 minutes. You have 15 minutes left. 8 during this hospitalization. She's the 8 MR. SCOTT LANE: Okay. All right. Let 9 gatekeeper. Remember Dr. Derman talking about 9 me wrap it up.
10 that? She's the doctor that knows everything 10 There is one other person, Annette 11 about everything that's going on during the 11 Mitchell. Annette Mitchell also wrote a note in 12 hospitalization. 12 the chart -- I mean, not in the chart. Annette 13 Where do you think these doctors got 13 Mitchell was the expert life care planner, and 14 the information from? The attending physician, 14 that's what I just read a moment ago, and the 15 Dr. Milenkovich is requesting a consultation and 15 importance of that is she wrote a report that on 16 telling these doctors what's going on with this 16 August 4th said nothing about a blood clot being 17 patient and reviewing the records, it's a 17 lodged in Jeanette's trach, and then on 18 combination, but don't you think that if Dr. 18 August 11th, lo and behold, she writes a report 19 Milenkovich said there was a cause, anything 19 after reviewing the file and says this was 20 other than a blood clot, that would be noted in 20 related to a blood clot lodged in the trach, and 21 those consultation notes? Absolutely. 21 after that report, lo and behold, Nurse Vinett 22 You know, I've heard Mr. Patterson 22 is not called to testify by the defense in this 23 asking experts for their interpretation of why 23 case. 24 these notes don't make sense, but what I haven't 24 MR. PATTERSON: Your Honor, objection,
73 75
1 heard is anybody else, any doctor from the improper argument. 2 hospital explaining these notes, explaining why 2 THE COURT: Overruled. 3 they don't say -- why they don't mean exactly 3 MR. SCOTT LANE: Interesting. The 4 what they say. That's kind of interesting, I 4 evidence is overwhelming that a blood clot 5 think. 5 lodged in the trach, and as a result of that, 6 You know what, it's -- you can't stop 6 it's clear that Jeanette suffered brain damage. 7 -- you can't stop at Mercy Hospital as far as 7 There is one other instruction that I 8 clot notes, because Dr. Gittler -- do you 8 want to talk to you about very briefly. It's 9 remember Dr. Gittler? Dr. Gittler was the 9 called a 5.01 instruction. It's a missing
1 O attending physician at Schwab University -- I 10 witness instruction, and that instruction allows 11 mean, at Schwab Hospital, and Dr. Gittler wrote 11 an adverse inference to be made if certain 12 a note in her chart that said tracheostomy 12 elements are satisfied. 13 performed for airway protection, records report 13 No. 1, if the witness is under the 14 that post-op patient developed clot in 14 control of the side -- do you have the -- there 15 tracheostomy tube, was anoxic for 20 minutes. 15 is an instruction, and here it is, and the Judge 16 Now, you might be thinking, well, wait 16 is going to read it to you, basically what it 17 a minute, maybe she's just taking the note from 17 says is if a witness is under the control of 18 the hospital and just putting that in her chart. 18 another party, and the adverse party has no 19 The problem is she also spoke to Dr. 19 access to that witness -- and I'm 20 Milenkovich. Who is Dr. Milenkovich? The 20 paraphrasing -- that you can conclude, you can 21 attending physician from the hospital. 21 infer that if that witness is not called by that 22 Do you think Dr. Milenkovich spoke to 22 other party, then the testimony would have been 23 Dr. Gittler and told her what happened? 23 adverse to that party. 24 Absolutely. Absolutely. And there she notes 24 Now, I want you to think about the fact
74 76
Pages 73 to 76
Mccorkle Litigation Services, Inc. chicago, Illinois (312) 263-0052

1 that the anesthesiologist was never identified. asked you a couple of things, and I asked you do 2 There was a court order, and we talked 2 you want to sit on this case, is this the right 3 about that stipulation, there was a court order 3 case for you, and I asked you assuming we prove 4 entered by the Court telling them that they need 4 our case, assuming we show you the evidence that 5 to disclose everybody that was involved in 5 we are entitled to a verdict in favor of 6 managing the patient's airway, and lo and 6 Jeanette Turner, would you have any hesitancy at 7 behold, 24 people were disclosed, but not the 7 all, any hesitancy in awarding a verdict in 8 anesthesiologist. They claim that they don't 8 favor of Jeanette for the full measure of each 9 know who this anesthesiologist is, and all I can 9 element of damage that she is entitled to be
10 say is I'm going to let you decide whether 10 compensated for, and you all said yes, you would 11 that's reasonable, whether that's a reasonable 11 have no problem with that. 12 excuse for not calling the anesthesiologist. Is 12 I'd like to go through the verdict 13 it believable that they don't know who this 13 form, Verdict Form A that we ask that you enter, 14 anesthesiologist is, and remember, the petition 14 and you enter a judgment in favor of Jeanette 15 that we filed to get the name of this 15 Turner, and I would like to help you answer the 16 anesthesiologist, to get the name of anybody 16 elements that are listed on the verdict form to 17 involved in the management of her airway, we 17 fill out the damages that the evidence has 18 filed that petition while she was hospitalized 18 shown. 19 at the request of the family, and they still 19 Verdict Form A is the verdict form that 20 didn't disclose this anesthesiologist. Why? 20 is used for plaintiff's verdict, for your 21 And so, we're going to ask you to 21 verdict in favor of Jeanette Turner. 22 consider that jury instruction where you can 22 The first element of damage is the 23 have an adverse inference; in other words, if 23 reasonable expense of necessary medical care and 24 the anesthesiologist were called to testify, his 24 treatment and services to date.
77 79
1 testimony would be adverse to the hospital, We agree with the defendant. We've 2 otherwise, why wouldn't they identify him, and 2 stipulated to that amount. There is no issue 3 why wouldn't they call him to testify? So, I'd 3 about that. 4 ask you to keep that in mind. 4 The next item is the present cash value 5 Thank you very much. 5 of the reasonable expenses of medical care, 6 MR. STEPHEN lANE: Good morning. 6 treatment and services reasonably certain to be 7 You know, I've waited literally over 7 received in the future. 8 ten years to have this conversation with you. 8 Now, the past amount of necessary 9 I have a limited amount of time. 9 medical care, treatment and services received to
10 Chris, can you put up 428, please? 10 date total $663,860.09. 11 You all met Jeanette. You saw her the 11 And you remember Dr. Yarkony came in, 12 other day in court. You saw her at Schwab 12 and Dr. Yarkony told us about the plan of care 13 Hospital. You saw her before she went to Schwab 13 that would be needed in order to take care of 14 when she was at Mercy Hospital. 14 Jeanette to make sure that she's safe, to make 15 I don't have to go through all of the 15 sure that she has housing and transportation and 16 ways that she has been disastrously injured. I 16 the wheelchair that she needs, the housing that 17 don't have to tell you what you already know, 17 she needs, the van, transportation that she 18 but I believe your Honor will give you an 18 needs. 19 instruction based on the law and based on the 19 And do you remember Dr. Rushing came 20 evidence that you've heard in this case for the 20 in, the economist, and Dr. Rushing told you the 21 past three weeks, you were selected to sit in 21 amount of money reduced to present value which 22 this case, and you remember during voir dire 22 if it was properly invested, would take care of 23 jury selection I didn't ask you about what TV 23 Jeanette for the rest of her life, and that 24 shows or what books you watched or read. I 24 figure is $7,153,314.77.
78 80
Pages 77 to 80
McCorkle Litigation services, Inc. chicago, Illinois (312) 263-0052

Dr. Rushing also calculated the cost of 2 the reasonable expense of necessary help 3 received to date, and also the present cash 4 value of the reasonable expense of necessary 5 help reasonably certain to be required in the 6 future, and those figures are $114,562.43 for 7 past help, and $179,548.23 for future help. 8 And then Dr. Rushing also calculated 9 for you the amount of the value of the earnings
10 and benefits that Jeanette lost up to this time, 11 and that figure was $399,210.30. 12 He also calculated the amount of the 13 present cash value of the earnings and benefits 14 reasonably certain to be lost in the future, and 15 that amount was $425,102.68. 16 You might think that if you feel that 17 Jeanette's injuries were negligently caused by 18 the hospital-- and we believe they were-- that 19 reimbursing those expenses that she's lost is 20 full and complete compensation, but that only 21 brings Jeanette to the point where she is 22 restored financially for the things that she 23 would have had up to today and into the future. 24 It doesn't touch the most important damage that
81
Jeanette has had. 2 You saw Jeanette. You heard from her 3 daughter Jazmin. You heard from her sister. 4 You heard from her employer, Rosalind Jones. 5 You heard from her doctors, Dr. Vern who's taken 6 care of her for ten years. You've heard from 7 Dr. Jerry Morris, the neuropsychologist. 8 Jeanette was an incredible woman, an 9 incredible woman. Raised six kids. Was a great
1 o worker. Took care of her kids, took care of 11 other people's kids, was out, lived, loved life, 12 and you remember when she came in and testified 13 here, and I asked her if you could change 14 anything, what would you change? Nothing, 15 nothing. Only God can do that. I have to deal 16 with the hand that I'm dealt. 17 So, there are economic losses that she 18 has had, and will have, but let's talk about the 19 things that are so important. Her life. 20 Pain and suffering suffered over the 21 past ten years. Do you remember the tremor that 22 caused her to try to drink a cup of coffee and 23 got third degree burns on the insides of her 24 thighs, surgery, scars.
82
Do you remember when she was still in 2 the hospital at Mercy, and she fell from the 3 commode and cut open her head? 4 Do you remember in the videos, in the 5 day-in-the-life videos where you got a little 6 picture of what it's like to be Jeanette? 7 Do you remember at Schwab when she 8 stood up, tried to stand up, and the pain that 9 she was obviously in?
10 Respectfully we ask that you enter an 11 amount of one million dollars for the past ten 12 plus years for her pain and suffering, and 13 fortunately, fortunately, she doesn't have that 14 much pain wise, physical pain wise these days, 15 and so respectfully, we are asking that you 16 enter for pain and suffering reasonably certain 17 to be experienced in the future for the rest of 18 her life $500,000. 19 The next line item is disfigurement 20 resulted. And you remember how proud Jeanette 21 was. How she loved to dress up. The bubbly 22 personality that she had. 23 Remember how Rosalind Jones talked 24 about her at work how she would go the extra
83
mile. She would be the first one to help out 2 anybody else. 3 She used to go out with her friends, 4 socialize, and take her kids everywhere she 5 went. She'd take them to work, she'd take them 6 to the Buckingham Fountain, she'd take them 7 everywhere, and what she did with her kids, and 8 the crafts and the clothes that she made for 9 them, the birthday parties that she planned for
10 them. 11 And do you remember in the videos, and 12 do you remember when she was here with us, and 13 do you remember the tremors? And do you 14 remember what she sounds like? And do you 15 remember that she told you she has a slight 16 speech impediment? And she told us what it's 17 like when she talks to people on the phone and 18 when they hang up because they can't understand 19 her. 20 And this incredible woman felt like she 21 was nothing. And when she sees people and she 22 goes to try to do something, and we know from 23 the nature of this -- do you remember active 24 myoclonic tremors -- what happens when she tries
84
Pages 81 to 84
McCorkle Litigation Services, Inc. chicago, Illinois (312) 263-0052

to do anything? It gets worse. She's punished 1 she needs help with virtually every single thing 2 when she tries to do anything. If she tries to 2 she does every single day of her life. 3 talk, it becomes harder. If she tries to reach, 3 She could make decisions. She could 4 she shakes more. 4 make decisions for her kids. She could 5 And when she sees people in public, 5 discipline her grandchildren. She could 6 they see this. And when she sees her 6 baby-sit for them. 7 grandchildren, they've been frightened. 7 And do you remember Jazmin told us 8 We ask for an entry of five million 8 about the time that she came over with the kids, 9 dollars for the disfigurement that Jeanette has, 9 and Jeanette was going to watch them, but the
10 and disfigurement is -- it's how somebody is 10 caretaker hadn't shown up, and she couldn't 11 perceived, how people look at someone, what they 11 answer the door, and she couldn't get there, and 12 think when they're met with them, and that she 12 she couldn't watch them, and it ended up that 13 feels that she is disfigured, this beautiful 13 her grandchildren had to sit for her. 14 woman. 14 Do you remember her grandchild asking 15 The next item is emotional distress 15 her why she wears diapers? She's alone. No 16 experienced to date. 16 friends. No social life. No work. 17 I've never met anybody quite like 17 She loved that job, and the job loved 18 Jeanette. There's no doubt when people hang up 18 her. 19 on her, there's no doubt when her grandchildren 19 You heard -- you heard from Rosalind 20 are afraid, there's no doubt when she suffers 20 Jones how excellent an employee she was. What a 21 the indignity of her son having to see her 21 team player she was, and you heard about all the 22 naked, having to bathe her, having to change her 22 things that Jeanette did for her family, for her 23 underwear, having to help her at that time of 23 kids, for the neighbor's kids. 24 the month. 24 She lost virtually every part of every
85 87 --···········-------------·--·---··-·-··--··-------... ····----------- . . ···············-------
We ask that you enter on this line an moment of every day of her normal life because 2 amount of two million dollars for that emotional 2 of the injuries she suffered as a result of the 3 distress experienced to date. 3 hospital's negligence. 4 And is there any doubt, is there any 4 I asked if you had hesitancy, if you 5 doubt that the emotions that she has gone 5 would have any hesitancy if we proved our case, 6 through for the past ten years, is there any 6 if we gave you the evidence that establishes 7 doubt that's going in the future? And we ask 7 full and fair compensation for every element, 8 for the rest of her life that you enter an 8 every element, full, that means complete, that 9 amount of six million dollars for the emotional 9 means leaving no gaps, that means as much as you
1 o distress reasonably certain to be experienced in 10 can give for that, a full cup is a cup that's 11 the future. 11 just short of spilling over, and we ask for past 12 And now I want to talk to you about 12 loss of normal life you enter the amount of four 13 what I think is the most important thing. 13 million dollars for the past ten years, and 14 Jeanette had a right, she had a right 14 eight million dollars for the loss of a normal 15 to live a normal life, and that normal life for 15 life reasonably certain to be experienced in the 16 Jeanette was a productive work life, was an 16 future. 17 active hands-on mom, was an active hands-on 17 These are just suggestions, and the 18 grandmother who was financially independent, who 18 prison that is Jeanette Turner's body is about 19 could go anywhere she wanted any time she 19 the worst thing that could happen to anyone, and 20 wanted, now can go anywhere she wants as long as 20 our laws are very clear about what it takes to 21 somebody picks her up and puts her there. 21 put someone in jail. Imagine what it would be 22 She was a mother who took care of 22 like to be in that jail for something you didn't 23 everybody; kids from the neighborhood, people at 23 do.
24 work, and she can't take care of anybody, and 24 I know that Mr. Patterson is going to
86 88
Pages 85 to 88
Mccorkle Litigation Services, Inc. Chicago, Illinois (312) 263-0052

talk to you next, and he's probably going to THE COURT: Thank you. 2 tell you that he disagrees with me, and he 2 Welcome back everyone. And now we're 3 disagrees with what I've asked of you. 3 going to proceed with closing arguments on 4 He's probably going to tell you that 4 behalf of Mercy Hospital. 5 you should enter a verdict for the hospital, 5 Mr. Patterson, good morning. 6 because they still deny that they were 6 MR. PATTERSON: Thank you, your Honor. 7 responsible. 7 May it please the Court, counsel, 8 This hospital is not simply trying to 8 Ladies and Gentlemen of the Jury, hello again. 9 defend itself. Its trying to deny and escape 9 I finally get to talk to you straight on, and I
10 the responsibility it has under the law, under 10 hope you don't mind if I just launch right into 11 the law, and because of the evidence that you've 11 it, because I have a lot to talk about, and I 12 seen, and if you agree with me, I ask that you 12 might talk fast, and I only have an hour, so 13 enter a verdict in the amounts that I have 13 here we go. 14 written here, but as I said, it's a suggestion. 14 In opening, which seems like it was a 15 And if you think that I have been -- if 15 long time ago, I told you that the evidence 16 I have asked too much, if you think it's not 16 would show that Ms. Turner received proper trach 17 fair, it's a lot of money, there's no question, 17 care, that her acute brain injury was due to a 18 it's a lot of money for anybody. 18 sudden trach complication, that Ms. Turner was 19 You have to ask yourselves is it a lot 19 clinically stable right up to the moment of the 20 for what Jeanette Turner has gone through and is 20 arrest, and that the nurses and doctors did not 21 going through and is going to go through? Is 21 cause this complication. 22 that amount of money too much to pay someone to 22 Miss Turner's respiratory arrest and 23 go through what she has? 23 brain damage is a horrific tragedy, but Mercy 24 And if Mr. Patterson -- if by chance 24 nurses and doctors are not to blame, and I
89 91
I'm right, and you agree with me, I invite Mr. believe the evidence has supported that. 2 Patterson to explain to you why the numbers that 2 I'm going to go through everything. 3 I've given you are unreasonable. 3 February 21st, you know, it was really 4 Every one of the economic losses; the 4 uncontroverted that she had a life-threatening 5 cost of care, the expenses of medical care, Dr. 5 condition, you heard from Dr. Cundiff how 6 Yarkony's care plan, the earnings in all of this 6 seriously life-threatening it was. She required 7 were either -- I told you about the ones that 7 an emergency trach. It was such an emergency, 8 were stipulated, but there isn't one shred of 8 it had to be done in an awake procedure. 9 evidence that the defendant produced to 9 She had to take Coumadin, so she was at
10 contradict anything that I said in those. 10 increased risk of bleeding. Some criticism of 11 And if you feel any of these are 11 the care for the first five, six days, and then 12 unreasonable, please, please, talk among 12 we get to the fact there were recognized 13 yourselves. You decide. You have the 13 complications of the trach that everybody 14 opportunity. You decide what is fair and full 14 agrees, dislodging it and negligence, blockage 15 and complete compensation for Jeanette. 15 can occur in the absence of negligence, that's 16 Thank you. 16 what happened in this case, she had a 17 THE COURT: All right. Thank you, Mr. 17 complication, and nobody was negligent at Mercy 18 Lane. 18 Hospital. 19 Ladies and Gentlemen, we'll take our 19 So what happened? Again, as I said in 20 morning break. 20 opening, it's not the defendant's burden of 21 Please don't discuss the case at all 21 proof. It is the plaintiff's burden of proof, 22 during break. 22 but it's clear that whatever it was, it was 23 (Whereupon, a short recess was 23 sudden, and it was acute, and did the trach tube 24 taken.) 24 become dislodged, was a blood clot obstructing
90 92
Pages 89 to 92
McCorkle Litigation Services, Inc. Chicago, Illinois (312) 263-0052

it, well, that's for you to decide, but I 2 respectfully submit that the evidence supports a 3 defense verdict regardless of what the cause 4 was. 5 Again, it's the plaintiffs burden of 6 proof, and the real question is how could the 7 Mercy nurses and doctors have prevented this 8 awful tragedy? 9 I told you during opening that the
1 O evidence will show that the patient's, Ms. 11 Turner's vital signs were stable throughout the 12 entire timeframe. That really hasn't been 13 challenged. 14 If a trach is blocked by blood, there 15 is not going to be normal vital signs. If it's 16 dislodged, you will not see normal vital signs. 17 I'm going to put this up again. I know 18 you're probably sick of seeing it, but it's an 19 important graphic that I'm going to subject you 20 to yet again. 21 Vital signs are, you know, it's 22 uncontroverted that they were stable up until 23 the very end. 24 What is the plaintiffs explanation?
93
How do they get around the stable vital signs? 2 Well, one theory is that this was a 3 partial obstruction, okay? 4 Ladies and Gentlemen, what evidence is 5 it? This is a court of law. 6 What is the evidence of a partial 7 obstruction? When did it occur? Was it before 8 or after the nurse is suctioning? Why wasn't 9 the partial obstruction suctioned out? Were
1 o there any signs or symptoms of the partial 11 obstruction? How could Mercy diagnose it if 12 there is no signs or symptoms? And even if it 13 was diagnosed, hypothetically, if it existed 14 hypothetically, then what? What would an ENT 15 doctor do to intervene? 16 Another explanation is that there was 17 an intermittent blockage, and Dr. Graham 18 actually suggested to you that, well, perhaps in 19 between the normal vital signs there were 20 abnormal vital signs, that's just not worth 21 recording. 22 He described that as a hypothesis upon 23 a hypothesis. 24 When did this intermittent blockage
94
occur? Was it before or after suctioning? 2 Should Mercy have expected it, and more 3 importantly, even if it existed, hypothetically, 4 then what? What would an ENT doctor do about an 5 intermittent blockage? There is no evidence of 6 either. 7 I told you during opening, and as we go 8 through this, it's designated, and this is a 9 slide from my opening statement, and I indicate
10 it as such. I told you that there were several 11 issues that were undisputed. 12 Ms. Turner came with a life-threatening 13 emergency, excellent care was provided during 14 the first week, steps taken in the cardiac cath 15 lab were reasonable. No criticisms of the plan 16 that was formulated in the cath lab. Tracheal 17 bleeding is a recognized complication. No 18 criticism that the bleed occurred. No criticism 19 of Dr. Cundiff's assessment the morning of the 20 28th. Appropriate to order blood products. No 21 criticism of that. No criticism of the plan. 22 All of those issues have been supported 23 by the evidence. I told you the evidence would 24 support it, and it did.
1 I also told you that the evidence would 2 show when a balloon is inflated, it prevents
95
3 blood from going into the lungs, it prevents the 4 exact same complication that the plaintiff's 5 theory is what happened. 6 All vitals signs were normal. Everyone 7 agrees with that. No evidence of acute massive 8 bleed. Everyone agrees with that. No criticism 9 of the code team. That one you have to put a
1 o little asterisk next to it, because coming into 11 this trial there were no criticisms of the code, 12 but yesterday Dr. Graham phoned in a criticism 13 from Australia. 14 I told you that the evidence would say, 15 tell you that sometimes mistakes are made in the 16 hospital chart. 17 You get that at this point in time. 18 Clearly mistakes can be made in hospital charts. 19 So, that's what I told you the evidence 20 would show. 21 Now, I just want to go over some of the 22 points that Mr. Lane said in his opening 23 statement about what he believed the evidence 24 would show.
96
Pages 93 to 96
Mccorkle Litigation Services, Inc. Chicago, Illinois (312) 263-0052

He described it as promises during 2 opening. Did he deliver all those promises? 3 Well, he told you that the Mercy chart 4 is a chapter in Ms. Turner's biography, and that 5 Mercy was trying to rewrite the story. 6 Clearly that's a pretty sinister 7 suggestion that we're trying to rewrite the 8 story. 9 He told you the evidence would show
10 that it would be very concerning to have 11 complaints of choking so many days after a trach 12 is placed. 13 Well, you heard Dr. Cundiff say that 14 the balloon had not been infiated. It was when 15 the balloon was infiated, that that's when 16 complaints of choking would be expected, because 17 it's uncomfortable to the patient. 18 He told -- there was no mention of the 19 normal vital signs during Mr. Lane's opening. 20 He didn't mention that. He didn't mention that 21 the plaintiff had no criticism of the ENT plan, 22 and he didn't tell you that that ENT plan would 23 take about three hours to carry out which was 24 implemented.
97
He told you that the evidence would 2 show that Dr. Cundiff did not know what was 3 going on, and that Dr. Cundiff believed the 4 bleeding was completely stopped in the cardiac 5 cath lab. 6 Well, you heard from Dr. Cundiff that 7 there was an expectation that there would 8 probably be continued bleeding because of her 9 anticoagulation, because it would take the fresh
1 o frozen plasma awhile to work. 11 So, with all due respect to Mr. Lane, I 12 don't believe that he delivered on those 13 promises. 14 He also told you that doctors need to 15 come when they're told. He didn't tell you that 16 Dr. Noriega's testimony is that she did come. 17 He told you that there was overwhelming 18 evidence that Ms. Turner could vocalize. He 19 referred to Ms. Fernando's note where she said 20 talk, talk, talk. 21 He didn't tell you, he knew, because 22 Nurse Fernando has given deposition testimony, 23 that she wasn't talking with Ms. Turner, she was 24 communicating via writing.
98
He told you that the evidence would 2 show that the sister was continually calling for 3 help. Well, that's true. She was. What he 4 didn't mention is that Nurse Fernando constantly 5 came and was in the room throughout this period 6 of time that is the subject of this lawsuit. 7 He told you that did any doctors come? 8 No. Well, again, Dr. Noriega did. 9 And also, remember the timeline from
10 the plaintiff's opening where it went from 11 yellow to red, and, oh, this is danger, danger. 12 He didn't mention that during that timeframe; 13 11:30, 11:45, midnight, that the vital signs 14 were completely stable, and Ms. Turner was 15 watching television with her sister. 16 He also said that Dr. Noriega didn't 17 respond to the first page, and, boy, we spent so 18 much time and energy on that issue about Dr. 19 Noriega, did she come, didn't she come, and then 20 Ms. Annette Turner took the stand and said, oh, 21 yeah, I saw Dr. Noriega more than once. So, did 22 he deliver on that? 23 Six different notes by five different 24 doctors. We've heard that over and over again.
99
He did not mention it wasn't told to 2 you during opening that those notes were written 3 three weeks later by people who were not present 4 at the code, and he also told you that the 5 evidence would show that Dr. Cundiff found a 6 clot blocking the trach. That's what he told 7 you the evidence would show, and you heard 8 directly from Dr. Cundiff that he did not find a 9 clot blocking the trach.
1 o What exactly is the plaintiff's theory 11 of liability? 12 In the opening statement the only time 13 that Mr. Lane came close to telling you what is 14 the theory, this is a medical malpractice case, 15 professional negligence, catastrophic injuries, 16 what is the theory? 17 He told you that the Mercy doctors and 18 nurses did not do what they were supposed to do. 19 What's that mean? What is the specific 20 criticism? What is the deviation from the 21 standard of care? 22 He told you that the evidence would 23 show that they needed to do whatever they need 24 to do to prevent blockage.
100
Pages 97 to 1 00 McCorkle Litigation services, Inc. Chicago, Illinois (312) 263-0052

What does that mean? And what exactly that there were several undisputed issues 2 is the plaintiffs theory of causation? 2 concerning the fact that Ms. Turner works, she 3 All comes down to ENT should have been 3 has significant future care costs, she was a 4 called sooner. When you go through all of the 4 positive generous person. These are very 5 issues that are in the jury instructions, it 5 serious injuries. 6 always comes down to that, should have gotten 6 For the 35 million dollar damages 7 ENT there sooner. 7 request, damage awards must be fair and 8 What treatment, what intervention would 8 reasonable for both sides, and I have to -- I'm 9 have been provided to avoid this outcome? What 9 required to address it, and I'm only going to
10 exactly would an ENT have done? 10 touch on it very briefiy. 11 Well, you heard from Dr. Cundiff. He 11 Damages are not supposed to punish 12 said if I had been called and told that there 12 Mercy. Sympathy is not supposed to play any 13 was some continued bleeding and that the vital 13 role in your analysis. 14 signs were normal and that Ms. Turner was having 14 Stipulations, just because we have 15 the subjective sensation of choking, I would 15 stipulated to certain elements of damages 16 have said that's expected, everything is good, 16 doesn't mean that we agree we're responsible for 17 no need to do anything further. 17 them, and the question is what is fair and 18 The plaintiff has the burden of proof, 18 reasonable? 19 and basically, when you get all through those 19 And I would respectfully submit that 20 instructions, there's three sort of hurdles, if 20 under these circumstances 35 million is not fair 21 you will, that the plaintiff must overcome in 21 and reasonable. Something more around the area 22 order to get to Verdict Form A. 22 of 4 to 5 million would be, but if you decide 23 The first hurdle is a deviation from 23 for the defendants on the question of liability, 24 the standard of care. It's another way of 24 you do not even need to think about -- you don't
101 103
saying negligence, professional negligence. even need to discuss damages. That's one of the 2 You all are not doctors or ENT 2 instructions, and I respectfully believe that 3 specialists. In order to get past that first 3 the plaintiff can't even satisfy that first 4 hurdle, you must necessarily rely upon expert 4 hurdle of deviation, so there will be no 5 opinion testimony. 5 occasion for you to even consider damages. 6 Ladies and Gentlemen, I don't think 6 The plaintiffs case I respectfully 7 that the evidence supports even getting over 7 submit is premised largely on appeals for 8 that very first hurdle. 8 sympathy. 9 And even if some of you might think, 9 Okay. This emotionally charged video
10 oh, well, you know, maybe they do, the next 10 footage of Ms. Turner. Ms. Turner was helpless 11 hurdle is even more insurmountable for the 11 we just heard during opening -- or at closing 12 plaintiff, and that is causation. 12 that she's helpless, and then we have the parade 13 In other words, they have to show that 13 of damage experts. 14 there was a deviation, a failure to getting an 14 Dr. Meyer to tell us that she has a 15 ENT there sooner, and that somehow that 15 brain injury. The defense doesn't dispute that. 16 deviation was the cause of the injury. 16 Jerry Morris to tell us about her 17 Well, Dr. Cundiff is the ENT who would 17 limitations. We don't dispute that. 18 have been contacted, and he told you there would 18 It was a parade of damage experts that 19 have been no reason to do anything different. 19 Mercy Hospital really didn't challenge. We 20 And then the last element is an injury, 20 don't dispute that this is a very serious 21 and there is no question that the plaintiff 21 injury. 22 satisfies that element. We don't even dispute 22 And then it was Ms. Turner's testimony, 23 that. 23 itself. Very sympathetic, and then she says 24 I told you during the opening statement 24 Mercy Hospital has not beaten her like Mercy
102 104
Pages 101 to 104
Mccorkle Litigation services, Inc. chicago, Illinois (312) 263-0052

Hospital is some evil institution and that we 2 need to stop Mercy from doing this to others. 3 Folks, it's understandable that Ms. 4 Turner would be upset and angry about the 5 condition that she's in, but those types of 6 inflammatory remarks from a very sympathetic 7 person are very, very hard to deal with. It's 8 manipulation of our emotions. 9 Other than appeals for emotions, the
10 other thing that we have heard from the 11 plaintiff's side are the conspiracy theories 12 about recordkeeping. All right. The mystery 13 anesthesiologist. Records were held from 14 defense experts. 15 Well, Mr. Lane didn't tell you that he 16 has all the records that we gave to the defense 17 experts, he has them, and he knows that there is 18 nothing substantive missing from those records. 19 MR. SCOTT LANE: Objection, your Honor. 20 THE COURT: Overruled. 21 MR. PATTERSON: There is all these 22 suggestions of missing notes and that Dr. 23 Noriega is not providing truthful testimony. 24 Nurse Fernando is also not providing
105
truthful testimony, Reddy, Cundiff. 2 Apparently, they believe Dr. Cundiff 3 didn't find a blood clot, and that necessarily 4 means that he was lying to you when he testified 5 a couple days ago. 6 You are the judges of the credibility 7 of the witnesses. You are the judges of the 8 credibility of the attorneys. You are the 9 judges of the credibility of the plaintiff's
10 case, and I respectfully submit that in order to 11 conclude that the plaintiff has met the burden 12 of proving a deviation from the standard of 13 care, you must necessarily conclude that 14 Noriega, Fernando, Reddy and Cundiff are all 15 lying. 16 This notion of this adverse inference 17 and the jury instruction that Mr. Lane 18 referenced regarding the anesthesiologist, that 19 only occurs if there's no reasonable explanation 20 offered to explain, and you heard from Nurse 21 Fernando that, hey, in code situations people 22 come running, we don't have video surveillance, 23 people aren't wearing Go Pro cameras on their 24 heads. We don't know who the anesthesiologist
106
was, because it was a hectic code situation, and 2 they didn't have sign-in sheets. 3 So, the Mercy chart, is it reliable or 4 is it suspect? 5 Okay. In opening statement Mr. Lane 6 told you that the Mercy records were the 7 definitive biography of Ms. Turner, right, it 8 was a chapter from her biography, but Mr. Lane 9 tells his experts that the Mercy records are
10 suspect and contain suspicious entries. Which 11 is it? 12 He suggests that Dr. Reddy's note is 13 suspicious because it was written about nine 14 hours after the code, yet, then they will 15 suggest that you should embrace the six 16 different notes by five different doctors as 17 being reliable, the gospel truth, even though 18 they were written three weeks later by people 19 who did not have personal knowledge. 20 Mr. Lane embraces the notes that 21 support the blood clot theory, six notes from 22 five different doctors, and then rejects those 23 notes. 24 Embrace the notes of Nurse Fernando and
107
1 Dr. Noriega, but then reject their 2 interpretation and their explanation of what 3 those notes mean, because it's some dishonest, 4 sinister attempt to rewrite the Mercy chapter. 5 Burden of proof. Did Mr. Lane satisfy 6 his burden of proving a case of medical 7 negligence? 8 Appeals to sympathy and unfounded 9 conspiracy theories do not establish
10 professional negligence. 11 These are transparent attempts to 12 distract you from the real issues in this case. 13 I told you during opening that you 14 would hear from five of the critical witnesses, 15 and on this point I should point out that the 16 defense, because we do not have the burden of 17 proof, we did not have to call one single 18 witness, but you have a right to know what 19 happened. You deserve to hear the testimony of 20 the people who were there at the time. So, we 21 presented these witnesses. 22 This is again the same slide from 23 opening statement, I told you that this is what 24 the evidence would show regarding Nurse David
108
Pages 1 05 to 1 08
McCorkle Litigation services, Inc. Chicago, Illinois (312) 263-0052

Fernando, and it totally did. She was in the 2 room repeatedly. She observed bleeding, 3 absolutely. It was minimal amount of bleeding. 4 She told you that the sister would get kind of 5 panicky and was fussing around Ms. Turner, and 6 she observed the sister earlier before the code 7 touching near the area of the trach side, and 8 she told Ms. Annette Turner to stop, and she 9 told you that when we got closer to the code,
10 things got hectic and agitated, and that 11 everyone responded to the Code Blue timely. 12 Dr. Noriega, this is the same slide 13 from opening, and every single point on that has 14 been established during the course of this 15 trial. 16 Dr. Noriega took the stand and told you 17 under oath that she came in response to the 18 first page. 19 Nurse Fernando David said the same 20 thing. 21 Miss Annette Turner said basically the 22 same thing. She had seen Dr. Noriega prior to 23 the time. 24 Why did we spend so much time on that
109
issue? Because, well, because they don't have 2 much else to say other than appeal to sympathy 3 and conspiracy theories. 4 Dr. Noriega also observed blood on the 5 sister's hands or gloves I should say, and that 6 when you have complaints of choking, but you 7 have normal oxygen saturation, that you're not 8 choking. 9 She also told you how she contacted ENT
10 after paging Dr. Reddy, and she had a discussion 11 with Dr. Cundiff before the events of the code. 12 Then there's Dr. Reddy's testimony, and 13 it's interesting how we would hear from Mr. Lane 14 that we should always put more emphasis on the 15 notes that are written at or near the time of 16 the events described, right, and that we should 17 be somewhat suspect or don't give as much weight 18 to the testimony of that individual ten years 19 later or at a deposition. 20 That apparently doesn't apply to Dr. 21 Reddy, because Dr. Reddy's note that was written 22 shortly after the code described seeing the 23 sister adjust the trach tube, but Mr. Lane 24 doesn't like that note, and said he wants to
110
embrace the testimony ten years later that, you 2 know, I honestly can't remember exactly what I 3 saw, but I saw something, something so unusual 4 and so concerning that Dr. Reddy called 5 security. 6 Remember there was no mention in the 7 plaintiff's opening statement about the fact 8 that security was called. 9 Security had to come. The sister left
10 the room, and then moments later the respiratory 11 arrest occurred. 12 Dr. Cundiff's testimony, again, I've 13 got to speed things along, but that's what I 14 said in opening, and every single point on there 15 was established. 16 You know, counsel just said something 17 about how there's nothing in Dr. Cundiff's note 18 that supports the notion that -- there's nothing 19 in Dr. Cundiff's note that goes against a blood 20 clot being there. 21 What about the part where it says no 22 airway obstruction? That's in his note. He 23 likes to pick the parts of Cundiff's note that 24 support his theory, and then ignore those
111
portions of the note that don't. 2 And then there's Ms. Annette Turner's 3 testimony, and this is what I told you in 4 opening, and it's every single one of those 5 points came out. 6 After midnight is when things got 7 worse, when she recalled that her sister's blood 8 was not clotting after the last bag of fresh 9 frozen plasma, and then there were some other
1 o things that this is not in opening that I just 11 want to refresh all your memories about, Ms. 12 Annette Turner's testimony was that her sister, 13 Ms. Jeanette Turner, was constantly writing I 14 got too much Coumadin, I got too much Coumadin, 15 and that she recalled some doctor at some point 16 coming and saying, yeah, too much Coumadin, 17 that's not an issue in this case, and none of 18 the plaintiff's experts have said anything about 19 too much Coumadin. 20 She told you that two doctors explained 21 this plan regarding fresh frozen plasma, 22 remember, sort of the consent, because Ms. 23 Annette Turner signed the form, and everything 24 was explained to her. She told you that she was
112
Pages 109 to 112
McCorkle Litigation services, Inc. chicago, Illinois (312) 263-0052

begging for help, and nobody was doing anything, then there's that other note, which is a very 2 but then subsequently on Cross she agreed, oh, 2 important note, because this was one of the 3 yeah, Nurse Fernando was constantly in the room 3 notes that was closest in time to the event in 4 suctioning. 4 question contemporaneous that ICU respiratory 5 And also she testified that she was 5 therapy note at 3:45a.m. the trach was 6 trying to keep Ms. Turner calm, and yet they 6 dislodged. 7 were watching lV, and the other thing is that 7 Doctors are not journalists. That was 8 Ms. Annette Turner is very -- she's a 8 something from opening statement. 9 germaphobe. I didn't call her that. She called 9 Clearly, clearly, if you believe Dr.
10 herself that, and she doesn't like blood at all, 10 Cundiff, if you belief that Dr. Cundiff did not 11 and she was clearly very concerned about blood. 11 commit perjury when he came in here and looked 12 She also said that it was after the 12 you in the eyes and said I didn't remove a blood 13 last unit of fresh frozen plasma that Ms. Turner 13 clot from a trach, then that necessarily means 14 vocalized, which is entirely consistent with a 14 that sometimes inaccurate information is 15 tube being dislodged right around that 15 perpetuated through a medical chart, and where 16 timeframe. 16 did that information come from? You don't just 17 She told you that her sister, Ms. 17 make it up, right? We've heard that from the 18 Jeanette Turner, was upset, throwing her arms 18 plaintiff, right, you don't just make up stuff. 19 around, that Annette tried to calm her down, and 19 Well again, if you were a doctor trying to 20 mentioned the unidentified doctor who said too 20 summarize what happened, and you look back at 21 much Coumadin, and also this unidentified nurse 21 the notes from Nurse David and Dr. Noriega about 22 that said that Dr. Cundiff said that he found a 22 choking on blood clots, and then you see the 23 blood clot lodged in the trach. 23 note by Dr. Cundiff that uses the word occluded, 24 Well, you heard from Dr. Cundiff, and 24 it would be a reasonable interpretation if
113 115
in order to believe that, you must necessarily you're not there and you're not conducting 2 include that he was giving you false testimony. 2 interviews, and you're not a journalist, a 3 There is an abundance of circumstantial 3 trained journalist, that, hey, it looks like it 4 evidence of what happened, right? 4 was a blood clot, plaintiff's blood clot theory. 5 We don't have the burden of proof 5 What would be the intervention? If 6 again, but there is circumstantial evidence that 6 there was a blood clot, what would the 7 the sudden trach complication that occurred 7 intervention be? 8 right around 1:00 a.m. or thereabouts was the 8 Well, you heard from Dr. Lavertu, and 9 result tragically of dislodgement of the 9 you heard from Dr. Cundiff that-- and you heard
10 trachea, and no one is suggesting that the 10 from Dr. Graham that suctioning, oh, if you 11 sister was doing anything other than what she 11 think that there's blood in the trach, you think 12 thought was in the best interest of her sister, 12 there's a clot, the standard of care of 13 but the reality is that the most likely 13 intervention is to suction the patient, which is 14 explanation that is supported by significant 14 exactly what was done. Suctioning was being 15 circumstantial evidence is dislodgement by the 15 performed up until shortly before the code, 16 sister, Nurse Fernando's observation, Dr. 16 before Dr. Reddy arrived. 17 Reddy's note about adjusting the trach. Dr. 17 Counsel wants to say the suctioning was 18 Reddy called security. The temporal proximity 18 done after Dr. Reddy saw this incident with the 19 between what Dr. Reddy observed and the 19 sister, and we heard that over and over again, 20 respiratory arrest. Vital signs stable up until 20 but Dr. Reddy, himself, said that, you know, on 21 the very moment of arrest. The inability to 21 the timeline that was done before I arrived. 22 Ambu bag during the code. Evidence of blood on 22 Just now we heard Mr. Lane say that Dr. 23 the sister's gloves. Dr. Cundiff, trach 23 Cundiff's note is 100 percent consistent with a 24 dislodged. He did not find a blood clot, and 24 blood clot blocking the trach when we just noted
114 116
Pages 113 to 116
McCorkle Litigation services, Inc. chicago, Illinois (312) 263-0052

1 2 3 4 5 6 7 8 9
10 11 12 13 14 15 16 17 18 19 20 21 22 23 24
1 2 3 4 5 6 7 8 9
10 11 12 13 14 15 16 17 18 19 20 21 22 23 24
that he actually wrote in his note no airway 1 It also refers to Nurse Rhorwasser. obstruction. 2 You heard a lot about her alleged deviation that
So, hematology issues, I just want to 3 occurred way over here, and with every single address them very briefly. 4 one of these, first, you must conclude that it
We heard from Dr. Hirsh about 5 was professional negligence, but then you also approximately three pints over five days. 6 have to conclude that that was a cause of the
Well, that might sound like a lot, but 7 injury, and with respect to Nurse Rhorwasser, I you've got to remember that there were repeated 8 would respectfully submit that that is -- I blood draws during that time. 9 mean, the notion that any deviation that
Even Dr. Hirsh agreed that this was not 10 occurred 24 hours before the code, when in an acute bleed that occurred over a very small 11 between there were a multitude of doctors and period of time. Dr. Hirsh agreed that not all 12 nurses seeing the patient, that's not credible. the bleeding was from the trach. There was a I 13 And with respect to Nurse David, well, lot of stuff that went on. During the code she I 14 she was in the room constantly, and whenever the had central lines put. There was a lot of blood 15 sister requested, she would call the doctor. loss during the code. 16 There is some issues about Dr. Cundiff.
And then also a hemoglobin of 6.1. He 17 Again, you need to go through them, and you need said, you know, that's a red herring, that's not 18 to decide did plaintiff meet the burden of accurate. There's no way you can go from a 10 19 proving that Dr. Cundiff was professionally something down to a 6.1 and then back up to a 20 negligent? 10, that is a red herring. 21 If the answer is no, then you move on
And then Dr. Hirsh, the only basis for 22 to the next issue. If the answer is yes --the opinion that this was a blood clot lodged in 23 which I don't think it will be, because the the trach is the six notes by five different 24 evidence doesn't support it -- you then need to
117 119
doctors. 1 go the next step and conclude, well, how does The post-code chest x-ray showed no 2 that causally connect things? What would Dr.
aspirations, no evidence of blood or fluid in 3 Cundiff have done, what would the standard of the lungs. 4 care have required if he had been contacted
So, now we can get to the issue 5 sooner? And, folks, with the stable vital instruction, and, I think, Mr. Lane has it on 6 signs, normal oxygen saturations, there would the board, and I'm just kind of briefly 7 have been no reason to do anything. summarizing it, but when you get the jury 8 Dr. Noriega, the issue for Dr. Noriega instructions, first off, you're going to have to 9 is that she failed to assess Jeanette Turner's elect a foreperson, and then the first hurdle, 10 condition in a timely manner. That is the remember, the first element that is plaintiff 11 contention of the plaintiff, and that again is must prove is a deviation from the standard of 12 based entirely upon the notion that she didn't care, and that's when this issue instruction 13 come and respond to that first page. comes into play. 14 And if you conclude that the plaintiff
These are the alleged deviations from 15 has not met the burden of proving that Dr. the standard of care, and the first alleged 16 Noriega is lying to you and that she didn't deviation is that the nurses failed to contact 17 come, then you go on to the next issue. physicians, inform them of the medical condition 18 And, folks, I respectfully submit that of Jeanette Turner and request their examination 19 when you do this analysis, and when you go of Jeanette Turner in a timely manner, and that 20 through the issues, you will never even need to refers to Nurse David, and that is entirely 21 get to the question of causation or damages, premised on the notion that Dr. Noriega didn't 22 because the plaintiff has not met their burden come, and she needed to call and make sure 23 of proof. somebody did. 24 There is a lot of non-issues that
118 120
Pages 117 to 120
McCorkle Litigation services, Inc. chicago, Illinois (312) 263-0052

you've been hearing a lot during this trial, and 2 they're not in the jury instructions. 3 Delay in giving fresh frozen plasma, 4 that's not an issue. 5 Too much Coumadin, remember, that's 6 what the sister remembered, Jeanette, oh, too 7 much Coumadin, too much Coumadin, oh, the doctor 8 told me we had too much Coumadin, that's not an 9 issue in the jury instructions.
10 A sentinel bleed, we heard Dr. Graham 11 describe how ominous that is, where's the 12 bleeding, through the lungs, and you drown in 13 your own blood. I'm not saying that happened 14 here. 15 Failure to write a note. You know, Dr. 16 Cundiff didn't write a note at 7:00 o'clock. 17 Dr. Noriega didn't write a note around 11:00. 18 That's not one of the issues in the instruction. 19 Failure to chart, failure to write a 20 note cannot possibly cause catastrophic brain 21 damage. So, it's not even an issue. 22 Missing notes, that's not an issue. 23 The time that it took to carry out the 24 , ENT plan is not an issue, and that's an
1 important point because Dr. Graham and Dr. 2 Dorothy Cooke both agree that they have no 3 criticism of the assessment by the ENT, they 4 have no criticism of the plan by the ENT, and
121
5 they also agree that that plan would take a long 6 time to carry out. It takes awhile to infuse 7 four units of fresh frozen plasma, and that 8 plan, Ladies and Gentlemen, was not done until 9 moments before the code.
1 o Why would Dr. Cundiff be required under 11 the standard of care to call back at midnight or 12 12:30 to say, hey, how's it going? It's not 13 until the fresh frozen plasma was infused that 14 you have to then wait to see is the plan 15 working, is the bleeding stopping. 16 So, again, what is in dispute? When we 17 go through all of these issue instructions, and 18 we follow them through to their logical 19 conclusion, it all comes back to ENT should have 20 been contacted sooner. 21 Plaintiff's theory is that a possible 22 blood clot -- that was Dr. Graham's word, 23 possible -- if it's only possible, how does that 24 meet burden of proof, right? If your own
122
expert, the furthest he is willing to go is say, 2 oh, it's a possible blood clot, it doesn't 3 satisfy the burden of proof. 4 And on the issue of blood clot versus 5 dislodgement -- I should have mentioned that a 6 long time ago -- that really doesn't have 7 anything to do with the issues. That's not 8 anything to do with the negligence. That really 9 only goes to the question of what -- did the
10 negligence cause the injury, and in order to 11 conclude that, in order to answer that question, 12 that's when you have to consider was it a blood 13 clot or was it dislodging. 14 And then it all comes back to what 15 treatment would have been provided if the ENT 16 were contacted sooner, and you heard from Dr. 17 Cundiff himself, I wouldn't have done anything 18 different. You heard from them, and 19 collectively have over a hundred years of 20 experience. 21 I told you during opening that it's 22 going to be a little bit overwhelming for some 23 of you, most of you, you don't have training in 24 medicine or EMT, and we have very well qualified
123
experts on both sides, and how in the world are 2 you supposed to work this out. 3 Well, folks, you again are the only 4 judges of the credibility, and you can consider 5 which experts for the plaintiff or the defense 6 were more impartial, were objective, not 7 advocates, not partisans, but view the case in a 8 balanced manner, and I respectfully submit that 9 although the plaintiff's experts are very well
10 qualified, and they have very distinguished 11 awards, and one is an English Knight in Canada 12 and the Medical Hall of Fame and a bronze star, 13 it doesn't change anything that you-- you are 14 the judges of the credibility, and you decide 15 which experts made the most sense, which ones 16 seemed to be the most reasonable and made 17 reasonable confessions, and I respectfully 18 submit, I believe that that panel of experts, 19 there is a lot of reasons to conclude that the 20 plaintiff's experts were perhaps just a little 21 bit too partisan in their review of this case. 22 Dr. Graham, I've already talked a lot 23 about him, but it's important, he had no 24 criticism of the plan. He acknowledges the plan
124
Pages 121 to 124
McCorkle Litigation services, Inc. chicago, Illinois (312) 263-0052

1 2 3 4 5 6 7 8 9
10 11 12 13 14 15 16 17 18 19 20 21 22 23 24
1 2 3 4 5 6 7 8 9
10 11 12 13 14 15 16 17 18 19 20 21 22 23 24
would take a long time to carry out. 1 catastrophic injuries out of the courtroom with He never clearly articulated, despite 2 no money damages, and that's what you need to do
extensive testimony, four-hour Direct 3 if the evidence supports it, the plaintiff did Examination, never clearly articulated what an 4 not satisfy the burden of proving the first ENT would have done if called, and then he 5 hurdle, you don't even get to the second hurdle. offers new criticisms every time he testifies 6 The only thing that they really proved including the criticism of the code that was 7 was that Ms. Turner suffered a catastrophic phoned in for the first time on the last day of 8 brain injury. evidence. 9 I thank you, but before I sit down, I
Folks, is that credible? Is that 10 have one final parting comment. credible, that three sessions of deposition, no 11 Because the plaintiff has the burden of criticism of the code, no criticism of the code, 12 proof, okay, Mr. Lane gets to have the last oh, I have no criticism of anything that was 13 word, and that's only fair. That's called done during the code, codes are hectic, codes 14 Rebuttal. are stressful, codes are difficult, and then on 15 So, I'm going to have to sit down, and the last day of evidence he phones in, oh, no, 16 then he's going to get the last word, and I have I've got a criticism of the code. 17 to sit there and be quiet, I can't really ever
That is not credible. That is not 18 respond, I'm not going to be able to talk to you credible. 19 again during this trial, but I do have some
So, I am near the end, you'll be happy 20 questions that I would like to pose to Mr. Lane to hear that. 21 to address during Rebuttal.
This is again, my -- you know, what I 22 What is the evidence? This is a said from the beginning, that the evidence will 23 courtroom. This is a court of law. What is the
establish those points, and I believe that the 24 evidence of partial occlusion?
125 127
evidence overwhelmingly did, and that's why I 1 I know it's a good theory. I mean, believe the evidence supports Verdict Form B. 2 they have been subjecting me to constantly this
Now, folks, here in a little bit we're 3 diagram that sort of shows their theory about going to be done. Ms. Dzik and I are going to 4 how this happened and that -- the blood clot, pack up our stuff and we're going to clean up 5 you know, demonstrative, they have a theory. the room that's a mess back there, and we're 6 Where's the evidence? Where is the evidence of going to be done, and then you guys start work. 7 an intermittent blockage? And, folks, this is not going to be easy. It's 8 What treatment would ENT have provided not going to be easy. 9 if called?
It's not going to be easy, because 10 Which records are reliable, and which Jeanette Turner was a wonderful woman who 11 ones are suspicious? suffered a catastrophic brain injury, and all of 12 How can you be in respiratory distress us sympathize for her, all of us want to give 13 with an oxygen sat of 100 percent on room air? her something, a new house, give her money, but 14 Why wasn't Ms. Turner able to cough out this is a court of law, and your duty as jurors 15 this blood clot if that's what happened? is to not allow sympathy to influence your 16 Why did Dr. Reddy call security if he verdict, and signing Verdict Form B under these 17 didn't observe the sister doing something circumstance is going to be difficult, but our 18 regarding the trach that posed a danger to Ms. system of justice is premised on you doing your 19 Jeanette Turner? duty. 20 Why wasn't the clot expelled with
The jury system is the most radically 21 positive pressure during the Ambu bag, and where democratic feature of our Republic, but it only 22 did the blood clot go? works if you do your job, and sometimes doing 23 Ladies and Gentlemen, on behalf of your job means sending someone who has 24 Mercy Hospital and Medical Center, I thank you
126 128
Pages 125 to 128
Mccorkle Litigation services, Inc. Chicago, Illinois (312) 263-0052

for your time, and I thank you for your jury 2 service. Thank you. 3 THE COURT: Thank you Mr. Patterson. 4 Mr. Lane. 5 MR. SCOTT LANE: Your Honor, I thought 6 we were taking a break. 7 THE COURT: No. Are you ready to go? 8 No. Keep going. 9 Thank you.
10 REBUTTAL 11 MR. SCOTT LANE: Well, for starters, I 12 sure wish I had more time to answer all the 13 questions that Mr. Patterson just asked for me 14 to answer, because, you know what, there has 15 been an answer to every single one of those 16 questions, but thankfully, you all were paying 17 attention during the course of this trial, and 18 you were listening to each of the witnesses that 19 testified during the course of this trial. 20 Let's start off with a couple of real 21 quick points. 22 The respiratory therapist's note that 23 states that the trach was dislodged. Of course, 24 it was out of place. We all know it was out of
129
1 place. 2 Dr. Cundiff came to the code, and what 3 did he find? He found that the trach was in a 4 different position, but the question is, how did 5 it get there? And the answer is there was 6 suction, there was bagging, and most 7 importantly, there was an anesthesiologist who 8 put the trach in that position. 9 That has absolutely nothing, nothing at
10 all to do with the position of the trach at the 11 time Jeanette arrested. 12 Have you heard any testimony from 13 anybody that indicates that the trach was 14 dislodged at the time Jeanette arrested? The 15 answer is no. 16 Security? You're talking about 17 security? How come -- you know, Mr. Lane, why 18 was security called? You heard Annette testify. 19 She testified that security was called because 20 she was trying to stay with her sister after she 21 arrested, after she collapsed, and she thought 22 that she was dying. 23 What is more believable, that or that 24 the security came because Annette was blocking
130
Dr. Reddy from getting to this patient? Does 2 that make any sense? 3 According to their theory, because I 4 understand it, and I'm trying to get my hands 5 around it, apparently Annette grabbed the trach, 6 yanked it out of her throat, because remember 7 what their expert said, what Dr. Cundiff said is 8 that the only way to dislodge the trach because 9 of the way it's configured is to actually pull
10 it out of the trach. 11 Where is the testimony? Where is the 12 evidence from anybody that the trach was 13 actually pulled out of the trach and sticking 14 out of the patient's throat? Is there any 15 evidence of that whatsoever? Absolutely not. 16 So, as I understand it, the theory is 17 that she was blocking the patient from Dr. 18 Reddy, that she dislodged the trach and caused 19 the brain damage. That's what they're trying to 20 tell you. 21 A couple problems with that. No. 1, do 22 you think that maybe somewhere in some part of 23 the medical record, anywhere, that it would 24 mention that the trach was dislodged, and that
that's what caused the brain damage? Do you 2 think that maybe if that's what happened, that 3 security was called to get this patient -- I
131
4 mean, to get this woman away from this patient, 5 and it's that patient that dislodged the trach 6 and caused this brain damage, do you think that 7 that event, even the mention of security, might 8 be mentioned somewhere in the chart by somebody, 9 somebody? Somebody talk about it, somebody
1 o mention it. You know what, that would be on the 11 news. 12 Dr. Graham, remember what he said, that 13 would be big news. 14 Because, of course, don't you think the 15 hospital would protect themselves and put that 16 in the record if that's what happened? Of 17 course. 18 It's ridiculous, and we know that 19 Annette had tried to get doctors all night long. 20 You heard Nurse David say, yeah, the 21 sister was trying to get -- trying to get me to 22 get a doctor, and then you heard Chibucos say 23 that, yeah, Annette told me to go get Dr. 24 Cundiff.
132
Pages 129 to 132
Mccorkle Litigation services, Inc. Chicago, Illinois (312) 263-0052

2 3 4 5 6 7 8 9
10 11 12 13 14 15 16 17 18 19 20 21 22 23 24
2 3 4 5 6 7 8 9
10 11 12 13 14 15 16 17 18 19 20 21 22 23 24
Does it make any sense that she's trying desperately to get a doctor, and then when a doctor comes, she blocks them? Does it make any sense whatsoever?
You know, I wish I was as smooth as Mr. Patterson. I'm not as smooth, but you can't change the facts. You can't change the records.
I have prepared 20 different pages --I don't have the time to go through this, but it doesn't matter, because I know you were listening, I know you were watching. You remember all the different times we were talking about the medical records.
The reason I said rewriting the medical records is because they had ridiculous interpretations of what took place in the medical records.
You know, every one of these clot found notes, go ahead, just cross out the words that the trach was -- that there was a clot lodged in the trach, and cross out those words, and now it's sister dislodged the trach, that's what caused the brain damage, that's what they want to insert in each of these records, rewrite
133 "" -············ .... --..... ------·---·-----
those records, that's what they want to do. And then you remember Nurse David?
She's looking at the medical -- she's looking at her own record where it says -- you know what, I don't even want -- I don't need to show it to you, because we saw it 20 different times during the trial.
Do you remember she checked off under neurologic exam that she had clear speech, clear speech, she checked off clear speech, and one expert said, oh, no, that was -- she was writing, and I asked does that mean clear penmanship? I don't understand.
Taking very obvious -- taking various obvious -- very obvious words and just giving ridiculous interpretation. That's what I'm talking about as rewriting, and inserting things that were not events that apparently they're saying took place that aren't in the records.
You know, notes like Dr. Noriega's talking about an event that took place at 11:00.
You think just because she testified ten years later, that she testified, oh, I remember going to see this patient at
134
2 3 4 5 6 7 8 9
10 11 12 13 14 15 16 17 18 19 20 21 22 23 24
2 3 4 5 6 7 8 9
10 11 12 13 14 15 16 17 18 19 20 21 22 23 24
11:00 o'clock ten years ago, and everything was normal. I remember. I remember going and doing that.
Do you remember how she talked about hundreds and thousands of patients that she has seen since then, and now ten years later she remembers that she went? Come on. Come on. Come on. It's ridiculous. Ridiculous.
She was paged to see this patient because she was choking and coughing up blood clots, and she doesn't have the time to write in the chart everything is normal. Ridiculous. Smoke screen. Smooth, but ridiculous.
Now, the clot found notes. The clot found notes. You know what? They are super credible. They're very important.
Was there a clot lodged in this trach? Was that-- is that what happened here? Of course, it is.
You have five different doctors, five different doctors from the hospital. They're talking about a clot being lodged, and he -what Mr. Patterson said was, well, they looked at the records, and they interpreted the
135
records, and then they-- all of them, every one of them misunderstood the record in exactly the same way, they all misunderstood.
Again, ridiculous. You're not going to fall for that. I know that. I know that. That is ridiculous.
Now, those five doctors, what exactly did they do?
Those five doctors looked at the medical records, and they made an interpretation of what took place.
Does that sound familiar? Like maybe the defense experts, that's what they did? Maybe it's the plaintiff's experts, that's what they did, looked at the records? Okay. Except for one difference. These are five doctors from Mercy Hospital.
Before any litigation they conducted an unbiased evaluation of the records, but that's maybe not even true. Maybe they didn't just review the records. Maybe they were personally involved.
Of course, they were, they were involved in the treatment. Maybe they have
136
Pages 133 to 136
Mccorkle Litigation services, Inc. chicago, Illinois (312) 263-0052

1 personal knowledge that, in fact, there was a 2 clot that was lodged in the trach. They were 3 there. They were involved in the treatment, and 4 they reviewed the records. 5 But they're not credible? They don't 6 believe it? On what basis? Has any of those 7 doctors -- any doctor from Mercy Hospital come 8 in here and said, oh, that's not right, that's 9 not right? Do you think that that would be
1 o something --11 MR. PATTERSON: Objection, improper 12 argument. 13 THE COURT: Overruled. 14 MR. SCOTT lANE: You'd expect that, 15 some explanation for why those records -- those 16 entries are not correct. You didn't hear it. 17 You didn't hear it at all. 18 I want to mention something else about 19 those records. 20 Do you know why we know that those five 21 clot notes are a hundred percent accurate? 22 The reason is that's a blowup of this 23 note in the original chart. It's a little tiny 24 note, a little tiny record, and what it says is
-- and you remember this, I'm sure --2 77.2 percent. I just wanted to show you the 3 actual document, because guess what? This is 4 the key to the entire case. Isn't that amazing, 5 this little sheet of paper? You know why? The 6 reason is because it says -- and here's the 7 blowup -- it says --8 MR. PATTERSON: I haven't seen this. 9 MR. SCOTT lANE: Same one you've seen
10 20 times. 11 MR. PATTERSON: Okay. 12 MR. SCOTT lANE: Yes. So, this exhibit 13 on March 1st at 1:18. I would say that 1:18 is 14 approximately 20 minutes after 1:00 o'clock; 15 fair? 16 At 1:18 the blood gas was 77.2 percent,
137
17 and I'm sure you remember Dr. Derman, how hard I 18 had to work to get Dr. Derman to admit that 19 77.2 percent is a blood gas that is extremely 20 low, extremely low. 21 He said it's low. She can breath. 22 She's getting some oxygen. Doctor, is it super 23 low? It's low. Doctor, come on, isn't it 24 extremely low? Isn't that going to cause brain
138
1 damage? Yes, yes. Finally admits it. 2 Why is that so important? Because 3 there are four notes, and you've seen them. 4 There are four of those clot found notes, I like 5 to call them that to summarize it, four of those 6 clot found notes talk about approximately 7 20 minutes of anoxia, 20 minutes of severe 8 deprivation of oxygen. 9 Wow, what a coincidence. Isn't that
10 amazing coincidence that this is at 1:18 it 11 shows that she has deprivation of oxygen? 12 Severe deprivation of oxygen? 13 So, now we've got clot, we've got this, 14 and does it really take a rocket scientist to 15 think that, wait a minute, she's coughing up 16 blood clots through the trach? Fifteen minutes 17 right before the code is called she is coughing 18 up blood clots through the trach and stating 19 that she's choking, and lo and behold, oh, my 20 goodness, it's crazy, I can't believe what a 21 conclusion you can come to, one of those clots 22 got lodged in the trach when every single expert 23 talked about the fact that that's a major risk 24 of a trach tube when you have blood clots and
139
1 clotting and fresh frozen plasma that causes 2 clotting, that's a major risk, and lo and 3 behold, it happened, and, wow, it's crazy, I 4 can't believe it. You mean, during suctioning 5 and Ambu bag and repositioning, that somehow 6 these clots, 6.4 millimeter clot, that somehow 7 Dr. Cundiff didn't see it during resuscitation 8 of 20 minutes, somehow this clot disappears in 9 an Ambu bag that pushes it out or sucks it in,
10 and you can't ever see it again or the 11 suctioning device somehow -- wow, that's crazy, 12 I can't believe there's no clot there. 13 It's ridiculous. It is ridiculous to 14 call five notes by six -- six notes by five 15 different doctors as totally false with 16 absolutely no basis to say that and no 17 explanation as to why they're ridiculous other 18 than, oh, they're later, they're just later. 19 Well, Mr. Lane says don't-- you can't 20 make it up. That's right. These doctors do not 21 make this stuff up. They're not going to make 22 up that the patient had a blood clot lodged in 23 her trach and suffered brain damage. 24 All of them are wrong. All of them are
140
Pages 137 to 140
McCorkle Litigation Services, Inc. chicago, Illinois (312) 263-0052

wrong, and none of them knew about this blood different, no, the question is really what is a 2 gas. Just a super coincidence. Again, 2 reasonably well qualified physician going to do 3 ridiculous. 3 under similar circumstances, and this is what's 4 THE COURT: Mr. Lane, you're down to 4 interesting. 5 five minutes. 5 Dr. Lavertu, their expert, what did he 6 MR. SCOTI LANE: Okay. And it sure is 6 say when I asked if you got called, what would 7 funny how things change. 7 you have done? He said I would have gone there, 8 Mr. Patterson sure talked a lot about 8 I would have identified the bleed, I would have 9 me in opening statement, but you know what I 9 treated the bleed, and most importantly, what
10 remember Mr. Patterson saying in opening 10 did he say? I would have protected the area, 11 statement when his theory was about the 11 and I would have prevented occlusion by 12 dislodged trach by Annette? I remember him 12 protecting the airway. 13 saying you're going to hear Dr. Reddy say that 13 It's not rocket science. We're talking 14 he had his hands around her trach and actually 14 about clots lodging in the trach. You just 15 around the trach tube, and then, lo and behold, 15 protect the area, make sure you suction and make 16 during the course of the trial it became 16 sure you monitor very carefully, and don't let 17 abundantly clear that that's not going anywhere. 17 it happen, because that's Rule No. 1. 18 Why? Because Dr. Reddy, himself, said you know 18 Lastly, your Honor, you know, and I get 19 what, I didn't see it, and you say I don't 19 emotional, and I'm sorry, but this is important. 20 remember? He said I didn't see it. I didn't 20 This is important to everybody in this 21 see that happen. Big difference between that 21 courtroom. It's important to Jeanette Turner. 22 and, oh, I don't remember, and then he gets to 22 It's real important, and sympathy shouldn't play 23 say, well, look at the record. No. He said, 23 a role. It shouldn't. We're not asking for 24 you know what, I really didn't see it. That's 24 sympathy, nobody is, and Jeanette Turner is the
141 143 ·········-----,--.--- - --·-····-----~--
what he said. 1 last person to ask for sympathy, but don't bend 2 And also, do you remember Dr. Bitran 2 over backwards and ignore the facts. 3 getting on the stand, their expert hematologist, 3 It should be very difficult to walk out 4 and what did he say? That counsel told him when 4 of here and not award her money, not because of 5 he was off the stand, that Dr. Reddy had said he 5 sympathy, but because of the evidence that's 6 didn't see it happen. Do you remember Dr. 6 been presented in this case over three weeks and 7 Bitran saying that? 7 25 witnesses. 8 That's important, because he realized 8 Don't ignore the evidence. That's all 9 that that can't be the theory any longer. Now 9 we ask you is to seriously consider the evidence
10 its all the sudden, sudden, sudden change, 10 and think about what's more likely; the evidence 11 sudden change of the trach, somehow, some way. 11 of dislodgement, which is right here, nothing, 12 It used to be all about Annette. Not anymore. 12 zero, or all of this evidence over here that 13 Now it's a sudden change. 13 supports the fact that there was a clot lodged 14 Last thing about causation. You 14 in the trach? 15 remember-- you heard Dr. Graham testify. You 15 MR. PATIERSON: Your Honor, I object to 16 heard Dr. Cooke testify. You heard the 16 the length of this Rebuttal. 17 negligence. 17 THE COURT: You're wrapping up, right? 18 Causation, oh, it's really difficult 18 MR. SCOTI LANE: Yes. 19 causation. You get a doctor there to find out 19 THE COURT: One minute. 20 about the bleeding, to treat the bleed and 20 MR. SCOTI LANE: That is an awesome 21 protect the airway. 21 responsibility that you have, and we appreciate 22 Do you think that the doctor came -- 22 your time and dedication, and we appreciate the 23 just because Dr. Cundiff says in this trial, you 24 know, I don't think I would have done anything I
23 fact that you've obviously taken this very 24 seriously, and we know that you're going to take
142 I 144
Pages 141 to 144
McCorkle Litigation services, Inc. chicago, Illinois (312) 263-0052

your job seriously when you walk back into that You may use your common sense gained 2 room, but please think about the next chapter, 2 from your experiences in life in evaluating what 3 think about the next chapter for Jeanette. You 3 you see and hear during trial. 4 have the opportunity to write the chapter. 4 You're the only judges of the 5 Don't let Mercy Hospital write the next chapter 5 credibility of the witnesses. You will decide 6 for Jeanette Turner. You have the opportunity 6 the weight to be given to the testimony of each 7 to write the chapter, and make sure that her 7 of them. 8 life is as full as it can be. 8 In evaluating the credibility of a 9 And you heard Steve talk about the 9 witness, you may consider that witness' ability
10 elements of damages. All we ask is that you 10 and opportunity to observe memory, manner, 11 award an amount that is fair, that is fair and 11 interest, bias, qualifications, experience and 12 reasonable, and whatever you think is fair and 12 any previous inconsistent statement or act by 13 reasonable, that's fine, and we appreciate it 13 the witness concerning an issue important to the 14 very much, and Jeanette, if she were here, and 14 case. 15 she would love to be here, she would appreciate 15 Pay close attention to the testimony as 16 it as well. 16 it's given. At the end of the trial you must 17 Thank you very much for all your time 17 make your decision based on what you recall of 18 and attention. 18 the evidence. 19 THE COURT: Thank you, Mr. Lane. 19 You will not receive a written 20 All right. Ladies and Gentlemen, that 20 transcript of the testimony when you retire to 21 concludes the closing arguments by counsel. 21 the jury room. 22 These are your jury instructions. This 22 A closing argument is given at the 23 is the law in the case. I'm going to read these 23 conclusion of the case, and is a summary of what 24 to you at this time. You will be taking all of 24 the attorneys intend that the evidence has
145 147
1 this back with you when you go to deliberate. shown. 2 Now that the evidence is concluded, I 2 If any statement or argument of an 3 will instruct you as to the law and your duties. 3 attorney is not supported by the law or the 4 The Jaw regarding this case is contained in the 4 evidence, you should disregard that statement or 5 instructions I will give you. You must consider 5 argument. 6 the Court's instructions as a whole, not picking 6 The testimony of Jack Hirsh, M.D., 7 out some instructions and disregarding others. 7 Stephen Veluz, M.D., Herbert Tannowitz, M.D. and 8 It's your duty to resolve this case by 8 Rosalind Jones was presented by videotape. 9 determining the facts based on the evidence and 9 The rebuttal testimony of Dr. Graham,
1 o following the law given in the instructions. 10 M.D. was-- excuse me-- Scott Graham, M.D. was 11 Your verdict must not be based upon 11 presented by the reading of his testimony. You 12 speculation, prejudice or sympathy. 12 should give this testimony the same 13 Each party, whether a corporation or 13 consideration you would give it had this witness 14 individual, should receive your same fair 14 personally appeared in court. 15 consideration. 15 An attorney is allowed, if a witness 16 My rulings, remarks or instructions do 16 agrees, to talk to a witness to learn what 17 not indicate any opinion as to the facts. You 17 testimony will be given. Such an interview by 18 will decide what facts have been proven. Facts 18 itself does not effect the credibility of the 19 may be proven by evidence or reasonable 19 witness. 20 inferences drawn from the evidence. Evidence 20 Whether a party is insured or not 21 consists of the testimony of witnesses and of 21 insured has no bearing on any issue that you 22 exhibits admitted by the Court. You should 22 must decide. You must refrain from any 23 consider all the evidence without regard to 23 inference, speculation or discussion about 24 which party produced it. 24 insurance.
146 148
Pages 145 to 148
McCorkle Litigation services, Inc. chicago, Illinois (312) 263-0052