Embed Size (px)
DESCRIPTION
tetraparese.ppt
Citation preview
Case Presentation
Tetraparese Flaccid
By: Dian Isti Angraini, S.Ked.Supervisor: Dr. H. A. R. Toyo, Sp.S (K)
Department of Neurology – RSMH PalembangFaculty of Medicine University of Sriwijaya
IDENTIFICATION
Mr. T/42 years old/male/ Moslem/stay outside town in /Oct 2nd 2008.
ANAMNESIS The patient was hospitalized in neurology ward of RSMH Palembang because of the difficulty to walk that caused by the weakness of both lower and upper limb which happened slowly.
± 11 years before admitted, the upper and lower limb muscles was very well developed look like an athlete. No muscle weakness and disturbances of walking. Mixtie and defecation normal.
ANAMNESIS± 8 years before admitted, the
patient had fever, high, fluctuated, ±1 week until 1 month, no seizure, no decrease of consiousness. The fluctuated fever happened about 1 year. The patient already have weakness on the left lower limb, the patient can walk on the forward part of the foot with the heels off the ground . No sensibility disturbances and waddling. Mixtie and defecation normal.
ANAMNESIS
± 7 years before admitted, the patient had difficulty to stand up. The weakness on left lower limb become more seriously. He also felt weakness on right lower limb. When the patient want to stand up, he must hold his knee first after that hold his thigh, climb to hold his hip and stand up. He used to get fall down after take awalk few steps. It was difficult for him to have a balance gait when he stand up. The upper and lower limb’s muscles was going to be smaller. There were no disturbances of sensibility, mixtie and defecation.
ANAMNESIS± 5 years before admitted, the patient
couldn’t stand up again, he could seated and felt weakness on both of upper limb, he still could spoon of on behalf to his mouth with the elbow based on his thigh. Sometimes he felt twitch and become numb (paresthesi) on both of the lower limb and the upper limb. There were no disturbances of sensibility, mixtie and defecation.
ANAMNESIS
± 1,5 years before admitted, the patient couldn’t seated anymore, the backbone become curve if the patient in seated position. There were no disturbances of sensibility, mixtie and defecation.
ANAMNESIS
There were no history of febrile seizure, truncus injury, or truncus disease. There are family history in his old brother, young brother and 2 of his uncles.
This illness was the first time for him.
Physical Examination
General StatusSense : compos mentis (GCS=E4M6V5)
Nutritive : enoughTemperature : 36,8ºCPulse : 90 x/minuteRespiratory rate : 20 x/minuteBlood Pressure : 130/80 mmHg
Physical Examination
General StatusHeart : HR: 90 x/minute, murmur (-), gallop (-)Lung : vesiculer (+) normal, ronchi (-), wheezing(-)Liver : not palpableSpleen : not palpableExtremity : refer to neurological status

Physical Examination
Neurological Status Nn. Craniales:N. Accesorius : there is limitedness to raise the
shoulder.
Physical Examination
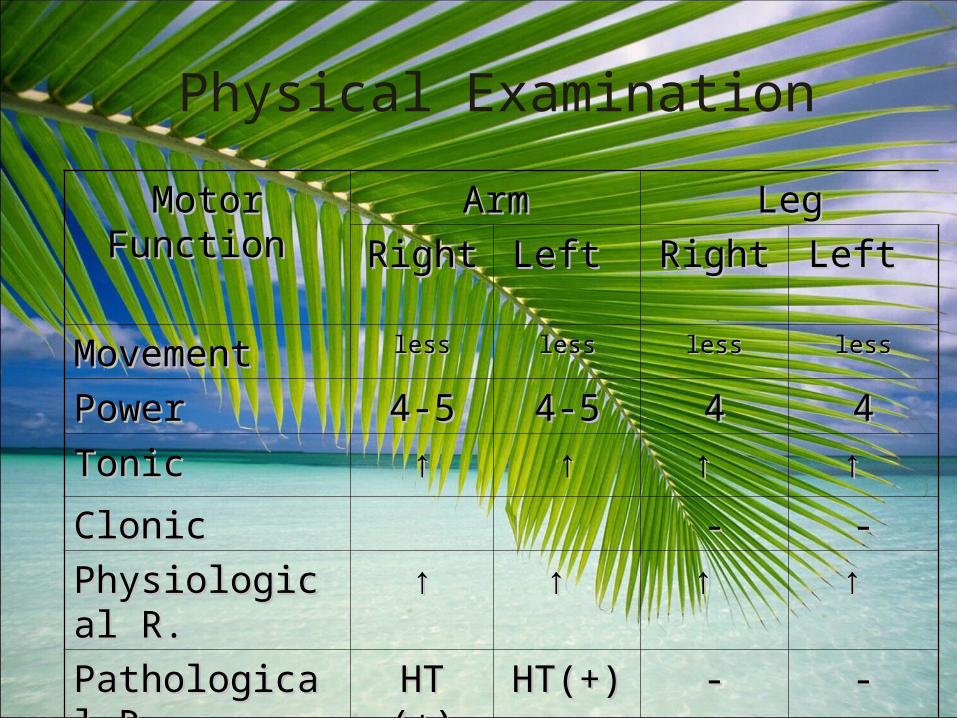
Motor Function Motor Function ArmArm LegLegRight Right Left Left Right Right Left Left
MovementMovement lessless lessless lessless lessless
PowerPower 4-54-5 4-54-5 44 44TonTonicic ↑↑ ↑↑ ↑ ↑ ↑ ↑
CloClonicnic -- --Physiological R.Physiological R. ↑↑ ↑ ↑ ↑ ↑ ↑ ↑ Pathological R.Pathological R. HT (+)HT (+) HT(+)HT(+) -- --
Physical Examination
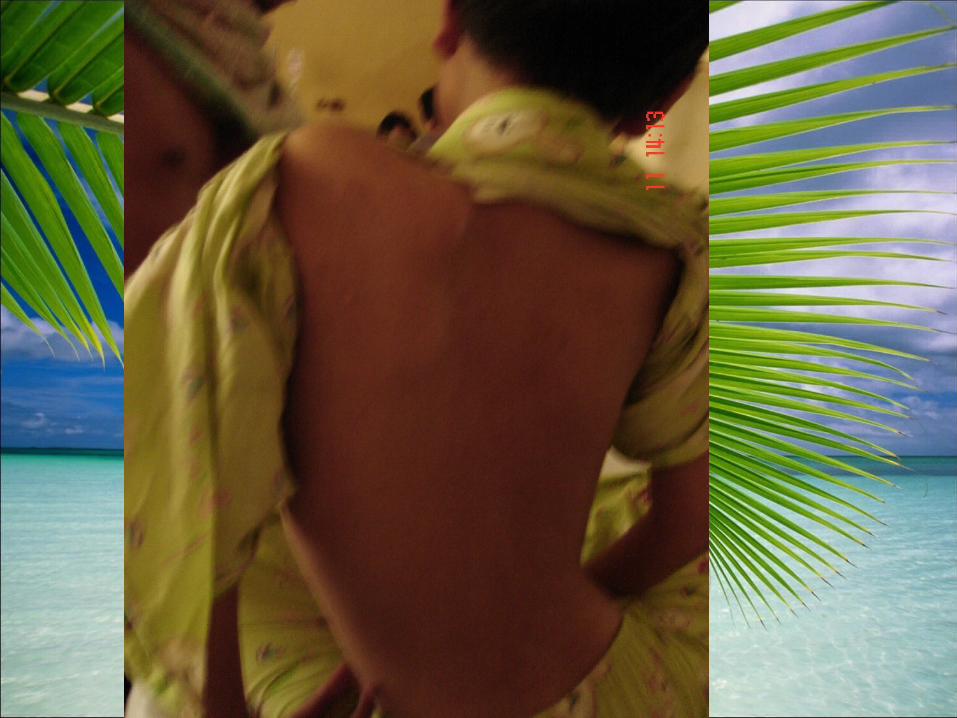
Tropic:There are atrophy on m. sternocleidomastoideus, m. trapezius, upper arm muscles, hand muscles, thoracalis muscles, hip muscles, upper leg muscles and foot muscles.
Contracture: on both of leg.
Columna Vertebralis : scoliosis (+)
Physical Examination
Sensory function : No abnormalityVegetative function : No abnormality
Higher nervous function : No abnormalityAbnormal Movement : No abnormality Gait, Balance &
Postural coordination : (-) Meningeal excitation : None
Laboratory
HAEMATOLOGY• Hemoglobin : 9,9 g/d• LED : 55 mm/jam• Leucocyt : 9.600/mm3• Diff Count : 0/6/2/72/17/3• Thrombocyt : 444.000/mm3• Haematocrit : 32 vol%
Laboratory
• BSS : 134 mg/dl • Total cholesterol : 247 mg/dl• HDL cholesterol : 60 mg/dl• LDL cholesterol : 116 mg/dl• Triglyceride : 125 mg/dl• Uric Acid : 8,4 mg/dl• Ureum : 30 mg/dl• Creatinin : 0,8 mg/dl
Laboratory• Total protein : 9,2 mg/dl• Albumin : 3,4 g /dl• Globulin : 5,8 g/dl• Sodium : 132 mmol/l• Potassium : 3,3 mmol/l• Calsium : 2,2 mmol/l• BTA I,II : negatif
Additional Examination
ECG:Ischemic anteroseptal + RBBB incomplete
Topical Diagnosis :
1. Cornu anterior1. Cornu anterior Symptoms on the patient Symptoms on the patient were:were:
Symptom: Symptom: Muscles weakness, first Muscles weakness, first weakness on hands then weakness on hands then shoulder muscles and upper shoulder muscles and upper arm.arm. Fasciculation (+) Fasciculation (+) Sensory disturbances (+)Sensory disturbances (+) Injury history (+)Injury history (+)
Weakness begin from leg muscles Fasciculation (-) Fasciculation (-) Sensory disturbances (-)Sensory disturbances (-) Injury history (-)Injury history (-)
The possibility on cornu anterior can be rejected.
Topical Diagnosis
2. 2. Motor End PlateMotor End Plate Symptoms on the patient were:Symptoms on the patient were:
Symptom:Symptom:
Weakness on both of arm and Weakness on both of arm and refer to hand muscles, ocular, refer to hand muscles, ocular, abdominal and thoracalis muscles abdominal and thoracalis muscles that happened after rest. that happened after rest. Diplopia (+) on the beginning, then Diplopia (+) on the beginning, then become bulbair paralysed and become bulbair paralysed and limb paralysed. limb paralysed.
Weakness on both of leg Weakness on both of leg and refer to arms that and refer to arms that happened slowly about 11. happened slowly about 11. Diplopia (-)Diplopia (-)
The possibility on motor end plate can be rejected.
Topical Diagnosis
3. Radiks Anterior3. Radiks Anterior Symptoms on the patient were:Symptoms on the patient were:
Symptom:Symptom:
Weakness on limb Weakness on limb muscles, developed little muscles, developed little by little. by little. Sensory disturbances (-)Sensory disturbances (-)Subacute and chronicSubacute and chronic
Weakness on limb muscles Weakness on limb muscles that happened slowlythat happened slowlySensory disturbances (-)Sensory disturbances (-)Weakness happened Weakness happened slowly about 11 yearsslowly about 11 years
The possibility on radiks anterior can be rejected.
4. Muscular4. Muscular Symptoms on the patient were:Symptoms on the patient were:
Symptom:Symptom:Pseudohypertrophy of Pseudohypertrophy of muscle muscle Flaccid paralyse on all of the Flaccid paralyse on all of the limblimbFamily history (+)Family history (+)High CPK value High CPK value
Pseudohypertrophy of Pseudohypertrophy of muscle (+)muscle (+)Flaccid paralyse on all of the Flaccid paralyse on all of the limblimbFamily history (+)Family history (+)High CPK value High CPK value
Topical Diagnosis
The possibility of muscular lession cannot be rejected.
Etiological Diagnosis
TThe possibility of myopathyhe possibility of myopathy can be can be rejectedrejected..
1. 1. MyopathyMyopathy Symptoms on the patient were:Symptoms on the patient were:
Symptom:Symptom:Periodic weakness or Periodic weakness or paralysed on all of the limbparalysed on all of the limbProgressive body weakness Progressive body weakness in short time, commonly in short time, commonly on rest or hyperactivityon rest or hyperactivityCorticosteroid history in Corticosteroid history in long timelong time
Weakness on all of the limb in stages and getting worse.Slowly weakness about 11 years.Corticosteroid history in Corticosteroid history in long time (-)long time (-)
Etiological Diagnosis
2. 2. MiocytisMiocytis Symptoms on the patient were:Symptoms on the patient were:
Symptom:Symptom:Fever history (+)Fever history (+)There are weakness and There are weakness and muscle pain.muscle pain.LMN paralyse on all of the LMN paralyse on all of the limb, motoric, one time and limb, motoric, one time and continously.continously.
Fever history (+)Muscle pain (-)Riwayat demam adaTidak ada nyeri ototSlowly LMN paralyse and getting worse
TThe possibility of myocytishe possibility of myocytis can be rejectedcan be rejected..
Etiological Diagnosis
3. 3. . Spinal Muscular Atrophy . Spinal Muscular Atrophy type IIItype III
Symptoms on the patient were:Symptoms on the patient were:
Symptom:Symptom:Onset : 2-17 years oldOnset : 2-17 years oldCan’t stand up without Can’t stand up without assisstassisstTremor (+)Tremor (+)
Onset of weakness: 7 years oldStill can stand up and walking in the first time of symptomTremor (-)
TThe possibility of SMA type IIIhe possibility of SMA type III can be rejectedcan be rejected..
Etiological Diagnosis
4. Becker Muscular Dystrophy4. Becker Muscular Dystrophy Symptoms on the patient Symptoms on the patient were:were:
Symptom:Symptom:Pseudohipertrofi (+)Pseudohipertrofi (+)Weakness started on proximal Weakness started on proximal muscles like hip muscles, muscles like hip muscles, upper leg muscles, shoulder upper leg muscles, shoulder and upper arm muscles. and upper arm muscles. Difficult and weakness on Difficult and weakness on walking, easy to fall and loss walking, easy to fall and loss of balance.of balance.
Pseudohipertrofi (+)Pseudohipertrofi (+)Weakness started on Weakness started on
proximal muscles like proximal muscles like hip muscles, upper leg hip muscles, upper leg muscles, shoulder and muscles, shoulder and upper arm musclesupper arm muscles
When stand up, he must hold his knee first after that hold his thigh,
Etiological Diagnosis4. Becker Muscular Dystrophy4. Becker Muscular Dystrophy Symptoms on the patient Symptoms on the patient
were:were:
Symptom:Symptom:
Contracture on joint (+)Contracture on joint (+)Onset: 11-21 years oldOnset: 11-21 years oldIncrease of CPK value 20-Increase of CPK value 20-100x100x
climb to hold his hip and stand up, difficult for him to have a balance gait.
Contracture (+) knee joint and ankle joint.
Onset : 7 years oldOnset : 7 years oldIncrease of CPK valueIncrease of CPK value ± ±
20 x20 x
TThe possibility of Becker Muscular he possibility of Becker Muscular DystrophyDystrophy can be rejectedcan be rejected..
Etiological Diagnosis5. Duchene Muscular Dystrophy5. Duchene Muscular Dystrophy Symptoms on the patient Symptoms on the patient
were:were:
Symptom:Symptom:Pseudohipertrofi (+)Pseudohipertrofi (+)Weakness started on Weakness started on proximal muscles like hip proximal muscles like hip muscles, upper leg muscles, muscles, upper leg muscles, shoulder and upper arm shoulder and upper arm muscles. muscles. Difficult and weakness on Difficult and weakness on walking, easy to fall and loss walking, easy to fall and loss of balance.of balance.
Pseudohipertrofi (+)Pseudohipertrofi (+)Weakness started on Weakness started on
proximal muscles like proximal muscles like hip muscles, upper leg hip muscles, upper leg muscles, shoulder and muscles, shoulder and upper arm musclesupper arm muscles
When stand up, he must hold his knee first after that hold his thigh,
Etiological Diagnosis5. Duchene Muscular Dystrophy5. Duchene Muscular Dystrophy Symptoms on the patient Symptoms on the patient
were:were:
Symptom:Symptom:
Contracture on joint (+)Contracture on joint (+)Onset: 3-7 years oldOnset: 3-7 years oldIncrease of CPK value 20-Increase of CPK value 20-100x100x
climb to hold his hip and stand up, difficult for him to have a balance gait.
Contracture (+) knee joint and ankle joint.
Onset : 3-4 years oldOnset : 3-4 years oldIncrease of CPK valueIncrease of CPK value ± ±
20 x20 x
TThe possibility of Duchene Muscular he possibility of Duchene Muscular DystrophyDystrophy cannot be rejectedcannot be rejected..
DIAGNOSIS
• Clinical Diagnosis :Tetraparese Spastik
• Topical Diagnosis :
• Etiological Diagnosis :

MANAGEMENT
• Diet NB TKTP• Vitamin B19 3x1 tablet / day• Neurobion 500 mg 3x1 tab
EXAMINATION PLANNING
• Rontgen thorax• EMG• Muscle biopsy• Ro columna vertebralis cervical-lumbosacral
AP-Lat
PROGNOSIS
Quo ad vitam : dubia ad malam
Quo ad functionam : malam