Embed Size (px)
Citation preview

The Bottleneck Problem Why provider organizations struggle to adopt digital health solutions (and how Redox can help).

© 2018 Redox, Inc. redoxengine.com | 2
TABLE OF CONTENTS
Technology Adoption Today ............................... 4
Making Sense of It All ......................................... 5Vendor SelectionSystems Integration
How This Problem Came to Be ........................... 6
The Integration Status Quo ............................... 7
Why This is So Detrimental ................................. 9Unscalable Reliance on Human ResourcesLinear Addition of Tech DebtDissatisfied Patients and Providers
The Good News: There’s an Alternative ............11
The Redox Approach .........................................12
Why This Approach Works .................................13
Where Redox is Used .........................................14The Redox Network
Where Do We Go from Here? ............................15
Redox exists to improve healthcare by uniting patients and providers through easily accessible technology. Technology can dramatically improve healthcare. It helps healthcare organizations become more efficient. It gives patients more control of their healthcare experience. And when done right, technology removes distractions so providers can focus on what’s important: their patients. redoxengine.com

© 2018 Redox, Inc. redoxengine.com | 3
INTRODUCTION
F irst things first… The last thing we want is for someone to spend their time reading this white paper only to find that the content was never intended for them. Our in-
tent is not to have more souls trudging through their morning commutes feeling as if we cheated them out of their time. So let’s get a few things out of the way.
► This document was written primarily for those entrusted with the technical strategies of healthcare organizations.
► If you’re another entrepreneur that looks at healthcare organizations as giant piggy banks waiting to be cracked open for the benefit of you and your investors—please look elsewhere.
► If you’re a generally curious individual who wonders about the influx of technology in healthcare and some of the unintended consequences of this quagmire, you might find this rather informative.
In examining how technology adoption in healthcare has gotten to be so convoluted, this document paints a fairly grim picture—but don’t fret! A path forward and viable solution is clearly presented. While the current state of things is worrisome, there is still hope if we act quickly.
Now that we are all on the same page, let’s get started.

© 2018 Redox, Inc. redoxengine.com | 4
Technology in healthcare can be a sticky subject—for many, it represents an intrusion on an age-old profession that was better off without it; for others, it promises advancements in diagnosis and care delivery that would otherwise be impossible. As with most things, the truth probably lies somewhere in the middle.
Regardless of one’s stance, the reality is that healthcare is experiencing very real pains when it comes to the adoption of technology. The dissat-isfaction with EHRs has been heard loud and clear across the country since their rapid implementation following the 2009 HITECH Act, which introduced financial incentives to promote the ‘meaningful use’ of health information technology generally and EHRs specifically. Providers feel as if they have been transformed into data entry clerks, and patients have become accustomed to watching their caregivers interact more with a computer screen than with them.
With 20% of GDP estimated to be spent on healthcare by 2025, this high level of user dissatisfaction represents one thing: an immense opportunity. The response of the market has been enormous—everyone from Fortune 500 companies to scrappy entrepreneurs have poured into healthcare to create replacements for systems providers hate working with, additional features current systems don’t offer, and, not to mention, develop a multitude of ways to make virtual patient care a reality.
With over 17.8 billion invested in “digital health” companies since 2011, one thing is clear—new ways of bringing technology into healthcare will continue to emerge.
Technology Adoption Today
AN ESTIMATED
20% of GDP will be spent
on healthcare by 2025
OVER
$17.8B Billion invested in Digital Health
since 2011

© 2018 Redox, Inc. redoxengine.com | 5
How is a healthcare administrator supposed to effectively vet and select a solution when there are so many alternatives prom-ising similar features and a better experience? She doesn’t have the luxury of simply downloading and experimenting with the few surgical scheduling solutions the way a consumer can simultaneously test half a dozen calendar applications on his phone and select the one that works best for him.
For a health system selecting a new solution, quickly switching or rebounding from an unexpectedly bad choice isn’t an option—the non-trivial purchasing decision requires extensive due diligence, multiple layers of approvals, and a lengthy contracting process, after which the chosen solution will be rolled out and used by a significant portion of providers and patients at a system level.
When health systems do select a new tool—probably at the behest of the head of oncology who can’t go another day without it—they must figure out how it will interact with the other systems in use, chief among them the EHR. Within this same problem is another even more complex issue: how to keep patient data consistent across all systems.
This is challenging because very rarely in healthcare do you see a full removal and replacement of a software solution; more often, a new tool is brought into the fold alongside existing systems. When this happens, these solutions must integrate seamlessly to ensure not only efficiency but patient safety as well—after all, even basic information like blood type and medication prescriptions can prove deadly when not recorded correctly across systems.
Though resolving the issues associated with solution selection is important, the focus of this paper is on the problem of systems integration, which is a problem so complex that it actually threatens the long-term viability of the organizations tasked with providing us care.
Making Sense Of It AllWhile the explosion of new solutions offering improvements on the status quo is exciting, it’s introduced two incredibly difficult problems for healthcare organizations: vendor selection and systems integration.
VENDOR SELECTION
SYSTEMS INTEGRATION

© 2018 Redox, Inc. redoxengine.com | 6
Let’s take a step back and discuss why this is happening.
The reality is that EHRs now represent the nervous system of clinical care in our country—from registration to discharge, every single event that happens within a clinic or hospital is recorded within one of these software systems.
While this cataloging is helpful, unfortunately, EHRs have very real limitations.
Most EHRs were initially designed as billing systems, and because of this, they are not well suited for patient-facing applications nor deliver an enjoyable user experience for providers. Beyond patient portals, (which were only prioritized because of government mandated regulation), there’s little functionality for patients as the user, if any at all.
Another common complaint of EHRs is how they facilitate care coordi-nation between various caregivers both within an institution and across institutions, as referrals through EHRs are inefficient (if not impossi-ble). Reporting and analytics functionalities, too, are weak points of EHRs, and the unique needs of specialists are not easily accommodated by software designed to serve a broader audience.
Long story short, today’s provider organizations recognize that their EHR cannot, in fact, do everything. Instead, they’re actively looking to extend and augment the EHR functionality with third-party solutions.
How This Problem Came To Be
Today’s provider organizations recognize that their EHR cannot, in fact, do everything. Instead, they’re actively looking to extend and augment the EHR functionality with third-party solutions.

© 2018 Redox, Inc. redoxengine.com | 7
The most common technical infrastructure at a healthcare organization is an EHR and an enterprise interface engine. This interface engine routes information from the electronic health record system to other systems that need it—this could be a lab for testing and results, a regis-try for pathology reporting, a PACs system for imaging, etc.
► These two systems require a significant amount of maintenance and configuration by specialized personnel
► There isn’t a huge market of experienced interface and EHR analysts
► The interface analyst market is so out of balance that instead of taking full-time positions at HCOs, most highly-skilled former em-ployees of EHRs choose to make their living as handsomely-paid consultants.
This market inefficiency makes it incredibly difficult for local hospitals and clinics to hire IT professionals to help with the adoption and integra-tion of new technologies, and even when they find the right people, they must pay premium salaries for a position they don’t entirely understand. This results in an organization that specializes in delivering patient care trying to negotiate and monitor the success of an ever-growing IT team. This puts both a financial and managerial strain on HCOs as they work to improve these teams.
When a new technology is to be adopted by an HCO, it’s generally added to a work queue. At any given time, there are dozens of projects that require the attention of EHR and interface analysts. Being human, these analysts can only work on so many projects at a time, so each one is scored based on priority and required resources. We’ve seen project wait times span anywhere from 6 to 24 months, and that’s just to get the right resources assigned. When the project does finally kick off, the normal implementation timeline averages six to eight months, “if every-thing goes as planned”.
The Integration Status Quo
With the way HCOs integrate today, even if that solution is selected and approved for implementation, the oncologists—and more importantly, the patients—won’t see that tool in use for at least 12-24 months.

© 2018 Redox, Inc. redoxengine.com | 8
To put this in perspective, let’s take a request from an oncologist who’s having trouble getting patients to attend required follow-up visits. They need to have consistent six-month checkups for at least two years to ensure the success of the treatment and prevent relapse. A technology vendor has developed a software platform that facilitates this commu-nication with patients and provides valuable survivorship information that not only leaves patients feeling confident and assured, but notifies providers if anything goes wrong between visits.
The head of oncology believes this technology will dramatically improve outcomes, drive revenue by increasing percentage of follow-up visits, and leave patients feeling as if the organization has gone above and beyond in their care. With the way HCOs integrate today, even if that solution is selected and approved for implementation, the oncologists—and more importantly, the patients—won’t see that tool in use for at least 12-24 months.
A normal project will require an incredible amount of coordination between the HCO IT team and that of the software solution. They will go back and forth on message specification, discuss what data is available, outline where they want information to live in the EHR, and finally, they’ll go through a security audit to ensure that compliance and safety requirements are met. After that, they may have to work directly with their EHR vendor to license an appropriate interface and manually configure the interface engine to interact with the third party. When the project is finally completed and the software solution is in use, the HCO IT team will be responsible for maintaining the connection and resolving issues as they arise.
And once all of that is done? The work that they did is not reusable, meaning it’s back to square one the next time they want to imple-ment another tool, and the connection they built to integrate the specialty solution with their EHR will need to be modified whenever there’s a change or update to either system.
In summary, the current approach to integration requires a heavy technical lift whose value can only be realized once. The cost to hire the right people to execute these projects diverts resources from where they should be focused, and ultimately, it hinders HCOs from adopting tools that would allow their providers to deliver better care.
This status quo is the Bottleneck Problem that holds healthcare back from adopting new technology that has the power to move the indus-try—and all of patient care—forward.
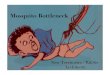
STATUS QUO INTEGRATION
Message Specification
Data Availability
Information Architecture
Security Audit
Interface Licensing via EHR Vendor
Manually Configure Interface Engine
Project Completion
Software Solution in Use
HCO IT Maintain Connection & Resolve issues
Back to square one to implement another tool
MONTH 1
MONTH 6
YEAR 2
YEAR 1

© 2018 Redox, Inc. redoxengine.com | 9
Why This Is So DetrimentalThe issues with this current model are numerous, but we’ll focus on the three most troublesome: unscalable reliance on specialized human resources, the linear addition of technical debt from each integration, and dissatisfied patients and providers.
First and foremost, this model—even with its current limitations—depends on the quality of the individuals developing and executing projects. The status quo provides an enormous number of scenarios where critical decisions are made that impact both the user experience of a product and the quality of the function performed—should data be filed as a note, or filed to a flowsheet row?
Well, in one scenario, you can analyze the discrete data and derive analytics, while in the other, you cannot. Are the people integrating this solution considering the implications of how they’re executing the proj-ect, or are they just trying to get it “up and running”?
Additionally, the lack of skilled professionals—and the premium salaries quality staff demand—add an incredible burden for HCOs who could better allocate resources elsewhere. It’s not uncommon for a group to face the very real dilemma of hiring more nurses or IT staff. Should this ever be a dilemma healthcare organizations face?
Finally, there is a very linear inputs-to-outputs equation for projects that can be executed using existing tools and staff: as demand increases for additional tools, so does the demand for additional staff to imple-ment them. The population of quality interface analysts is not increas-ing at a significant speed, but under the current status quo, the demand for more integration projects continues to rise and has shown no signs of slowing down.
Healthcare organizations are beginning to feel this pinch, and there are only two options: longer work queues—the “make do with what we have” approach—or invest more money in IT staff—the “brute force” approach. Unfortunately for everyone, both options hurt the long-term health of the organization.
This status quo is the Bottleneck Problem that holds healthcare back from adopting new technology that has the power to move the industry—and all of patient care—forward.
UNSCALABLE RELIANCE ON SPECIALIZED HUMAN
RESOURCES

© 2018 Redox, Inc. redoxengine.com | 10
Tech-debt is a phrase most commonly used in software development to describe the negative impact of crudely written code—it impacts performance, makes future changes more difficult, and is something high-functioning development teams seek to eradicate in general.
In our scenario, tech debt applies not to computer code but to inte-gration infrastructure. Each new connection that is built in this highly customized, non-reusable integration model is an additional piece of infrastructure that needs to be maintained and updated.
Over time, the more of these connections organizations establish, the more of their team’s man hours must transition to maintenance. This means they aren’t able to work on new projects because resources are devoted entirely to monitoring and maintaining existing connections. This becomes extremely troublesome when something new comes along that represents a drastic improvement on what’s in use today, because with traditional integrations, implementing one new tool means building a multitude of new connections.
We’re seeing this today with the adoption of FHIR—sure, some work-flows would be better served by leveraging newly available FHIR resources and protocols, but the initial integration is already in place and transitioning it is a non-vital task.
The result? No change is made even though benefits could be realized.
LINEAR ADDITION OF TECHNICAL DEBT

© 2018 Redox, Inc. redoxengine.com | 11
As HCOs continue to set up more and more integrations between their core EHR system and third parties, they’re looking at an infrastructure so riddled with tech debt that their ability to move or adopt improvements is greatly compromised. Add onto that the linear growth of maintenance requirements and we’re looking at a system that not only represents a growing portion of an organization’s operating budget, but is unable to realize the efficiencies that could be gained through the adoption of health tech.
Patients and providers should never come last, but with the very real challenges healthcare organizations are facing, the reality is that they often do—tools that would make providers happier and more effective in their jobs aren’t implemented due to technical and personnel limita-tions; tools that would delight patients and improve outcomes aren’t being used because of they can’t be prioritized.
The promise of technology in healthcare was to distribute the best information and tools to the largest number of patients and providers. We aren’t seeing this adoption of best practices because the status quo of how these solutions are adopted and incorporated into the modern healthcare system technical architecture is fundamentally flawed.
Oddly, healthcare has seen very few deviations from this unfortunate status quo. Most options on the market attempt to solve the highly-spe-cialized personnel problem by offering to do the work for you, but use the same technology and tools that result in linearly scaled tech debt and bloated systems.
Redox is fundamentally different in that our solution addresses both the personnel problem and the technical limitation problem facing HCOs today. We do this by providing centralized infrastructure and extensive managed services both during the project and beyond.
The Good News: There’s An Alternative
DISSATISFIED PATIENTS & PROVIDERS

© 2018 Redox, Inc. redoxengine.com | 12
We start with a technical platform that eliminates the need for individ-ualized connections and custom interfaces. Much like how interface engines are used to splice data to different systems, Redox acts as a centralized hub to facilitate the exchange of information within a health system’s ecosystem of software applications. The core difference from an existing interface engine is that it does not require additional configuration from health system IT teams—instead, Redox takes on the work of mapping existing interfaces from the EHR to our engine, so interface analysts don’t have to worry about meeting yet another new specification.
Redox delivers an out-of-the-box abstraction layer that effective-ly lays a modern API interface on top of existing legacy systems. Instead of going back and forth on what information is available or what workflow functionality is possible, any vendor simply has to build against that API—something any modern web developer is very familiar with. As part of our full-service approach, Redox can also map to the custom specifications of vendors who don’t want to use the API. Best yet, because hundreds of applications are already connected to Redox, once the platform is turned on at the health system, integrating those appli-cations become turn-key.
The result? Instead of a maze of point-to-point connections and redundant interfaces, HCOs have a set of core interfaces that run through Redox and are translated, spliced, and routed across all of their authorized data sharing partners. Redox maintains all connections and configurations to source systems, allowing HCOs to authorize the exchange of specific sets of data with authorized partners in a highly flexible manner.
For ongoing system maintenance, whenever EHRs or interface engines are updated, changes only need to be made once by the Redox team and all downstream system configurations will remain intact. Not only does this dramatically limit the ongoing maintenance burden for IT teams, but it also makes it very easy for organizations to shift infrastruc-ture to a new system should that become necessary.
The Redox Approach
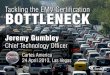
REDOX INTEGRATION
STATUS QUO
Kickoff & Connectivity
Configurations
Integration Test
Train
Go-Live
1 HOUR
6 HOURS
15 HOURS
11 HOURS
19 HOURS
YEAR 1
YEAR 2
Message Specification
Data Availability
Information Architecture
Security Audit
Manually Configure Interface Engine
Project Completion
Software Solution in Use
HCO IT Maintain Connection & Resolve issues
Back to square one to implement another tool
MONTH 6
MONTH 1

© 2018 Redox, Inc. redoxengine.com | 13
Why This Approach WorksInstead of hiring for a skill set outside of their specialty, HCOs can partner with the industry leaders in healthcare integration. Integra-tion is all we do, every day. Across hundreds of our HCO and technol-ogy vendor partners, we have integrated with 40+ EHRs and executed countless data exchange workflows. Instead of hiring a growing number of interface analysts, you work with us to get projects kicked off and executed quickly. Projects are expedited because there is no limit to the number we can work on—we have dedicated resources specifically for that function, and we have the advantage of knowing what needs to be accomplished during a project, when, and by whom.
Perhaps the biggest value in our approach lies in its reusability. Thanks to our centralized technical platform, 85% of work to integrate any given solution is completed as part of its initial implementation, allowing groups to go live with new tools in as quick as 48 hours instead of six months or more.
Every single HCO should have an efficient and scalable process for implementing new technology—it’s a mission-critical function of the modern healthcare organization. The groups that do this well will be able to dramatically differentiate from their competitors; they will drive more revenue, lower operating costs, improve provider satisfaction levels, and delight their patients with superior care. The groups that continue with the status quo will fall behind and likely succumb to the weight of inefficiency. If health systems don’t act quickly, they will very likely feel the effects when it is too late to make up the ground lost.
Thanks to our centralized technical platform, 85% of work to integrate any given solution is completed as part of its initial implementation, allowing groups to go live with new tools in as quick as 48 hours instead of 6 months or more.

© 2018 Redox, Inc. redoxengine.com | 14
Today, healthcare organizations like Brigham Health and Intermountain Healthcare are realizing the value the Redox Platform provides. New technologies are being adopted in days rather than months, innovative products are being piloted faster, and legacy interfaces are transitioning to more efficient and flexible connections. Over 400 healthcare orga-nizations are embracing this new paradigm for health data exchange, and our interoperable networks shares information more efficiently and freely than ever before.
Where Redox Is Used
The Redox NetworkEvery organization using the Redox platform is capable of exchanging data with any other node of our network through the same protocol and data standard. Building on Redox means joining the only truly interoperable network in healthcare.
Authenticate with API
NetworkRedox
Implementation
Build Configuration Record
EHR Interface Engine
Other Systems
Provider Organization
Vendor
Get to know the hundreds of
provider organizations and
vendors already sharing data
over the Redox Platform.
Explore the Redox Network >

© 2018 Redox, Inc. redoxengine.com | 15
Healthcare organizations are at a crossroads. Will they continue to become technology companies, diverting more and more resources to their technical infrastructure and teams? Or, will they say enough is enough and enlist a partner that will allow them to move quickly, stay flexible, and realize the financial efficiencies technology promises?
At Redox we are committed to helping healthcare organizations focus on what matters most: their patients. Together, we can redefine the way we deliver healthcare and ensure the adoption of technology only serves to move healthcare forward.
Reach out to your Redox point of contact and we’d be happy to dive deeper.
Where do we go from here?
Ready to Get Started?We’re passionate about maximizing technology investments, driving efficiency, and improving outcomes. We’d love to hear more about your integration challenges and share how we dramatically decrease integration timelines, transition legacy interfaces, and implement new solutions while finding new ways to delight patients and providers alike.
Contact Us
Get in Touch! redoxengine.com/contact-us