Embed Size (px)
Citation preview
The Electrocardiogram in Infarction of theLateral Wall of the Left Ventricle
A Clinicopathologic StudyBY WILLIAM J. DUNN, M.D., JESSE E. EDWARDS, M.D., AND RAYMOND D. PRUITT, M.D.
This reappraisal of the electrocardiographic manifestations of infarction of the lateral wall ofthe left ventricle is based on data acquired by simple and conventional technics. Categories ofcases have been determined by the age of the infarct and the distribution of the lesion with respectto the circumference of the left ventricular wall and its epicardial and endocardial boundaries.Significant data have been presented in the form of illustrative diagrams and reproductions. Theresults do not establish a simple pattern common to all cases of infarction of the lateral wall; theydo illustrate the varied yet limited electrocardiographic consequences of such lesions.
T WO notable facts justify reporting theresults of another study of infarction ofthe lateral wall of the left ventricle.
First, whereas the electrocardiographic ex-pressions of infarction of the anterior andposterior walls of the left ventricle have beenclearly defined and amply confirmed, thechanges that attend infarction of the lateralwall have evaded precise and conclusive treat-ment. Second, the justifiable suspicion persiststhat the lateral wall of the left ventricle is thesite of many infarcts that escape electrocardio-graphic detection, not only in their healed butalso in their acute phase. Both these circum-stances may be held to be reasonable conse-quences of those respects in which the lateralwall differs, so far as its contribution to thescalar electrocardiogram is concerned, from theanteroapical and posterobasal portions of theleft ventricle. The lateral portion of the freewall of the ventricle is so disposed as to precludeready exploration by semidirect leads; inmany instances, it appears to be relativelysilent so far as the extremity leads are con-cerned.
From the Mayo Foundation and the 1Iayo Clinic,Rochester, Minn. The Mayo Foundation, Rochester,Minnesota, is a part of the Graduate School of theUniversity of Minnesota.
Abridgment of thesis submitted by Dr. Dunn tothe Faculty of the Graduate School of the Universityof Minnesota in partial fulfillment of the require-ments for the degree of Master of Science in Medi-cine.
540
BACKGROUND
An appraisal of certain published accountsof the electrocardiographic expressions of in-farction of the lateral wall will serve to identifythe current state of knowledge concerning thisproblem.The study of Wood and associates,' iii 1938,
directed attention to the possibility of anelectrocardiographic pattern of infarction ofthe lateral wall. Their observations, based onlimited electrocardiographic exploration, in-cluded some points that have borne up underthe test of time and others that have ledperhaps to some confusion in past years.Significant were their suggestions that (1)some types of myocardial infarction produce apaucity of electrocardiographic evidence ascompared with other types, (2) the QRScomplex is usually unaffected by infarction ofthe lateral wall, and (3) the electrocardio-graphic signs of a lesion in the lateral wall maydisappear rapidly and completely. However,their pathologic data included only a singlecase with typical findings of infarction of thelateral wall at necropsy, a second case withsupportive but not definitive findings, and athird case in which they noted that the clinico-pathologic correlation was rendered uncertainby the 14-month interval between the clinicalsuggestion of infarction and the necropsy.From this evidence they proceeded to thegeneralization that electrocardiographic studyof infarction in other parts of the heart indicates
Circulation, Volume XIV, October, 1956
by guest on June 30, 2018http://circ.ahajournals.org/
Dow
nloaded from
DUNN, EI)WARDS, AND PRUITT
that myocardial ischemia in a certain locationtends to produce a characteristic electrocardio-graphic pattern: "Thus it is reasonableto suppose that the 17 cases without necropsywere instances of lateral infarction."
Depression of the RS-T segment in leads I,II, and, particularly, IVF was proposed byWood and co-workers as a characteristicfinding in infarction of the lateral wall of theleft ventricle. Currently accepted conceptswould suggest that depression of this segmentin the precordial electrocardiogram may occurin the presence of acute subendocardial injuryaffecting the anterior, apical, or lateral wall ofthe left ventricle. Existence of such a finding ina lead from the left portion of the precordiummay well be an expression of subendocardialinfarction of the lateral wall of the left ventriclebut is not a change specific to a lesion in thislocation only. Thomson and Feil2 reportedelectrocardiographic changes of this type in 4of their 9 cases of recent infarction of thelateral wall, and Myers and associates3 found4 such instances among their series of 28 casesof infarction of the lateral wall. However, theelectrocardiographic changes in 1 of these 4may have been produced by a combination ofleft ventricular hypertrophy and the effects ofdigitalis.Thomson and Feil,2 in 1944, recorded obser-
vations on a much larger collection of patho-logic material. Interpretation of their data isrendered difficult by the fact that in mostinstances recent infarction of the lateral wallwas attended by old infarction of the anterioror posterior wall or by infarction of the anterioror posterior wall continuous with infarction ofthe lateral wall.
Shaffer,4 in 1944, reported 5 cases of acuteinfarction of the lateral wall, giving conciselypresented evidence that can be interpretedreadily because of the homogeneity of thelesions involved. In all 5 cases, the infarctedregion apparently was transmural and wasreasonably well confined to the lateral wall ofthe left ventricle; the data, both electrocardio-graphic and pathologic, were secured duringthe acute or healing phase of the lesion. Whilethe electrocardiographic studies were incom-plete by present-day standards with respect to
the number of leads recorded, the observedchanges deserve summary. Two of the 5 caseswere characterized by the presence of electro-cardiographic changes ordinarily associatedwith injuries of both anterior and posteriordisposition, 1 showed predominantly posteriorfeatures (Q wave and elevated S-T segment inlead III, attended by depression of S-T segmentin lead I), 1 showed only inverted T waves inlead I, and 1 revealed only absence of the Rwave in lead IV. Shaffer concluded that notone of his cases showed the electrocardiographicfeatures typical of infarction of the lateral wallas defined by Wood's group, and that a singleconsistent pattern w-as absent.
In 1946, Rosenbaum and associates pre-sented the results of a purely clinicoelectro-cardiographic study on the precordial electro-cardiogram in "high" lateral myocardialinfarction. They contributed significantly toknowledge of the electrocardiographic conse-quences of infarction of the lateral wall withoutreporting the findings at necropsy in a singlecase. Pathologic correlation was confined to thestatement, "We have recently heard ofinstances of high lateral infarction demon-strated at autopsy in which the standardextremity and precordial electrocardiogramsresembled those described in this article."While they recognized the significant role thatrotation of the heart or some other change inthe relations of its surfaces to the usual leadsmust play in producing the electrocardiographicchanges, they considered infarction of thelateral wall to be the type that producescharacteristic findings in precordial leadsV5, V6, and V7, or in leads from the upper leftpart of the precordium or the left axilla. Aquestion remained, however, concerning theconsistency with which such changes appearedin infarction of the lateral wall.
In 1945, Hecht6 presented the results of astudy of 86 cases of infarction of the lateralwall. To our knowledge, his work appears inthe literature only in abstract form andappraisal of his data is rendered somewhatdifficult by the summarized character of thepresentation.Myers and associates,3 in 1949, reported their
findings in 27 cases of "primary" lateral in-
0-41
by guest on June 30, 2018http://circ.ahajournals.org/
Dow
nloaded from
ELECTROCARDIOGRAM IN INFARCTION OF LEFT VENTRICLE
Slice 1.(apex) Slice 4.
Slice
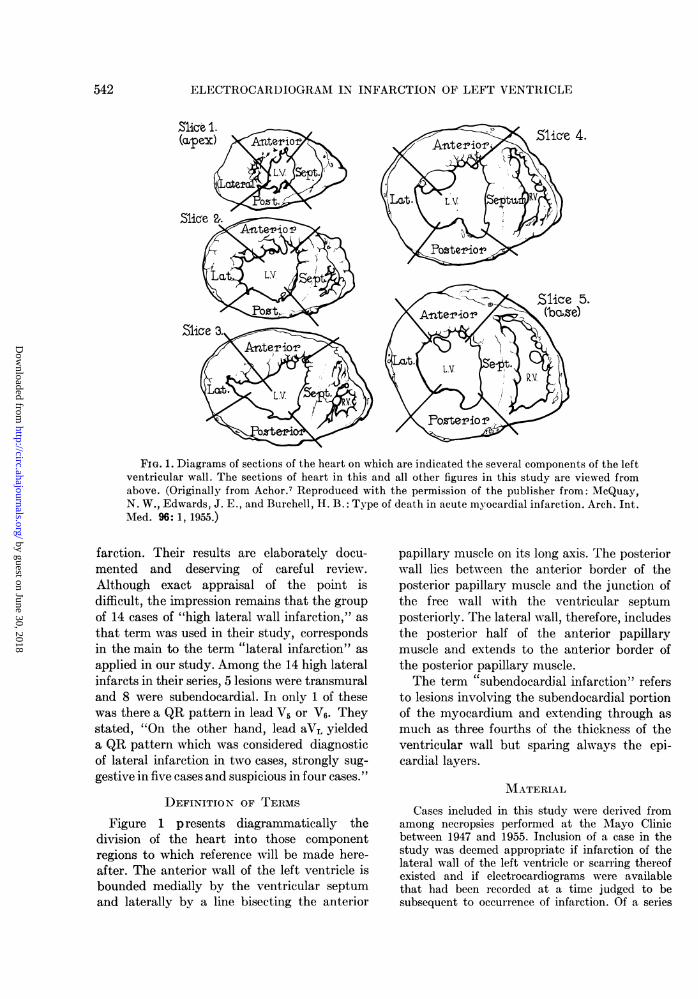
FIG. 1. Diagrams of sections of the heart on which are indicated the several components of the leftventricular wall. The sections of heart in this and all other figures in this study are viewed fromabove. (Originally from Achor.7 Reproduced with the permission of the publisher from: McQuay,N. W., Edwards, J. E., and Burchell, H. B.: Type of death in acute myocardial infarction. Arch. Int.Med. 96: 1, 1955.)
faretion. Their results are elaborately docu-mented and deserving of careful review.Although exact appraisal of the point isdifficult, the impression remains that the groupof 14 cases of "high lateral wall infarction," asthat term was used in their study, correspondsin the main to the term "lateral infarction" asapplied in our study. Among the 14 high lateralinfarcts in their series, 5 lesions were transmuraland 8 were subendocardial. In only 1 of thesewas there a QR pattern in lead V5 or V6. Theystated, "On the other hand, lead aVL yieldeda QR pattern which was considered diagnosticof lateral infarction in two cases, strongly sug-gestive in five cases and suspicious in four cases."
DEFINITION OF TERMS
Figure 1 p resents diagrammatically thedivision of the heart into those componentregions to which reference will be made here-after. The anterior wall of the left ventricle isbounded medially by the ventricular septumand laterally by a line bisecting the anterior
papillary muscle on its long axis. The posteriorwall lies between the anterior border of theposterior papillary muscle and the junction ofthe free wall with the ventricular septumposteriorly. The lateral wall, therefore, includesthe posterior half of the anterior papillarymuscle and extends to the anterior border ofthe posterior papillary muscle.The term "subendocardial infarction" refers
to lesions involving the subendocardial portionof the myocardium and extending through asmuch as three fourths of the thickness of theventricular wall but sparing always the epi-cardial layers.
MATERIAL
Cases included in this study were derived fromamong necropsies performed at the MIayo Clinicbetween 1947 and 1955. Inclusion of a case in thestudy was deemed appropriate if infarction of thelateral wall of the left ventricle or scarring thereofexisted and if electrocardiograms were availablethat had been recorded at a time judged to besubsequent to occurrence of infarction. Of a series
542
by guest on June 30, 2018http://circ.ahajournals.org/
Dow
nloaded from
DUNN, EDWARDS, AND PRUITT
of 47 cases fulfilling these criteria, 17 were dis-carded because existence of a separate infarct ofthe anterior wall rendered impossible the reliableascription of electrocardiographic changes to in-farction in the lateral wall. However, all cases in thefollowing categories were retained: (1) acutetransmural infarction confined to the lateral wall(6 cases); (2) acute transmural infarction of thelateroposterior wall (6 cases); (3) acute subendo-cardial infarction confined to the lateral wall (1 case);(4) healed subendocardial infarction confined to thelateral wall (13 cases); and (5) healed transmuralinfarction confined to the lateral wall (1 case). Inaddition to these 27 cases, 3 selected cases wereretained because the sequence of electrocardio-graphic changes permitted reasonably exact correla-tion between alterations in these records and themorphologic findings. These 3 included an instanceof healed transmural anteroseptal infarction com-plicated by acute subendocardial infarction of thelateral wall, 1 of healed transmural posterolateralinfarction complicated by acute anteroseptal in-farction, and 1 of old subendocardial posterolateralinfarction.
The 17 cases eliminated were instances of infarc-tion of the lateral wall of the left ventricle com-bined with separate anterior or anteroseptal infarcts(12 cases) and examples of subendocardial infarc-tion of the posterolateral wall of the left ventricle(5 cases). Interpretation of data was rendereddifficult in the majority of these rejected caseseither because infarction of the lateral wall wasassociated with infarction involving other regionsin such a way that a reliable correlation between theelectrocardiographic changes and pathologic findingscould not be formulated or because of uncertaintythat the electrocardiogram was recorded afterdevelopment of the infarction in the posterolateralwall of the ventricle.An attempt has been made in this selection to
strike a compromise between the dangerous dis-tortion of evidence that may result from injudiciouschoice and the confusion of detail that may obtainin the total absence of discriminating selection.
RESULTSThe results of this study can be compre-
hended most readily in the form of illustrations.Figures 2 through 8 present the essentialelectrocardiographic and morphologic data.The legends include certain clinical and patho-logic facts. Whenever possible, a single illustra-tion has been used to represent 2 or more casesconstituting a type as defined by the correlationof electrocardiographic and pathologic findings.
Acute Transmural Infarction Confined toLateral Wall of Left Ventricle. Cases 1 through
6 were of this type (figs. 2-4). Review of theillustrations discloses that 1 case (case 1)presented electrocardiographically as a "purelateral," 2 (cases 2 and 5) as "apicolaterals," 1(case 3) as a "postero-apical" and 1 (case 4) asa "posterolateral"; the electrocardiogram in 1(case 6) was essentially normal.QRS changes, when present at all, were of
limited extent. In cases 1 and 2, tiny Q de-flections were present in leads I and aVL, andthe R deflections in V, were increased in size inrelation to the S waves. In cases 3 and 4, Qwaves were present in leads II and III, butthese were small in case 3 and were precededinconstantly in case 4 by a small upwarddeflection. In case 5, the R waves in leads Iand V6 were notched on the descending limb.
Significant changes in S-T segments and Twaves were present in 5 of these 6 cases.Segmental elevation in leads from regionsfacing the epicardial surface of the infarctedzone was attended commonly by depression ofsegments in leads overlying uninvolved epi-cardial regions. This reciprocal relationshipobtained also for configuration of T waves andafforded evidence suggestive of an injury, suchas myocardial infarction, confined to a localregion of the ventricular wall, as opposed to amore widely distributed epicardial lesion, suchas acute pericarditis. In the presence of a moregeneralized epicardial lesion, a similar re-ciprocal relationship may be encountered butthe "bracketing leads" ordinarily face an epi-cardial surface on the one hand and an endo-cardial surface on the other. In the singleinstance (case 6) in which electrocardiogramsmade at the time of acute infarction disclosedno certain evidence of myocardial injury, theinfarct was small and confined to a single sliceof the sectioned heart.
In one instance (case 5) in which tracingswere obtained 6 years after acute infarction,definitive electrocardiographic evidence of ascar was absent. T waves in lead I were oflesser amplitude than in lead III. The factthat the major evidences of injury wereconfined to the S-T segments and T wavesallows reasonable prediction that similarlycomplete resolution of electrocardiographicchanges encountered in the acute stage in 4 of
543
by guest on June 30, 2018http://circ.ahajournals.org/
Dow
nloaded from
ELECTROCARDIOGRAM IN INFARCTION OF LEFT VENTRICLE
Case 1 Case 2
3rdInt ;le itrep
ce
4thInte
r
pace
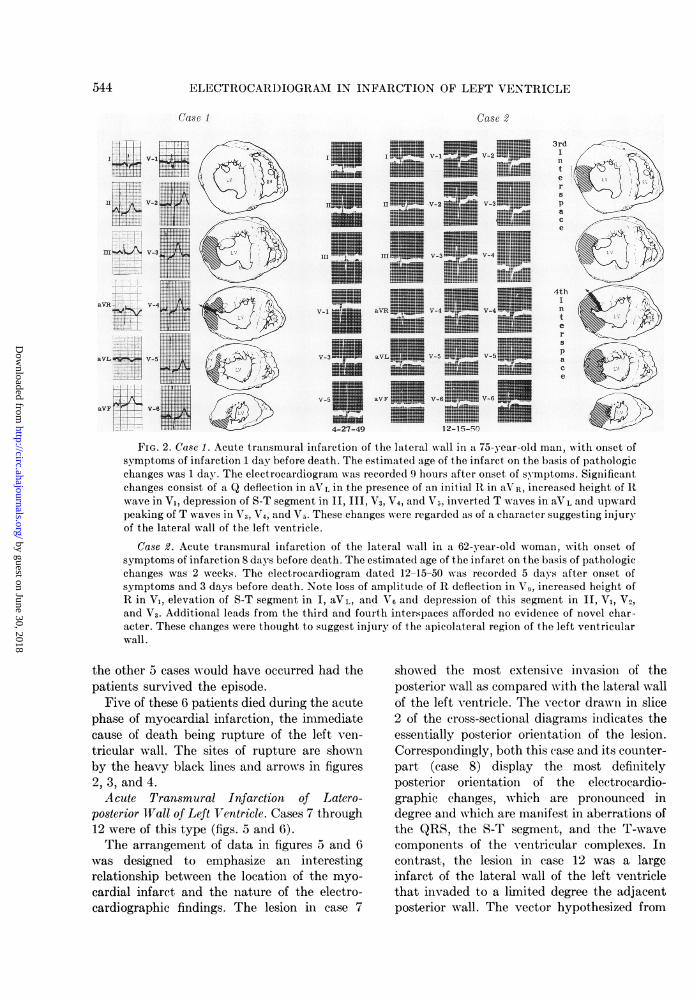
FIG. 2. Case 1. Acute transmural infarction of the lateral wall in a 75-year-old man, with onset ofsymptoms of infarction 1 day before death. The estimated age of the infarct on the basis of pathologicchanges was 1 day. The electrocardiogram was recorded 9 hours after onset of symptoms. Significantchanges consist of a Q deflection in aVL in the presence of an initial R in aVR, increased height of Rwave in V1, depression of S-T segment in II, III, V3, V4, and V5, inverted T waves in aVL and upwardpeaking of T waves in V3, V4, and V5. These changes were regarded as of a character suggesting injuryof the lateral wall of the left ventricle.
Case 2. Acute transmural infarction of the lateral wall in a 62-year-old woman, with onset ofsymptoms of infarction 8 days before death. The estimated age of the infarct on the basis of pathologicchanges was 2 weeks. The electrocardiogram dated 12-15-50 was recorded 5 days after onset ofsymptoms and 3 days before death. Note loss of amplitude of R deflection in V6, increased height ofR in V,, elevation of S-T segment in I, aVL, and V, and depression of this segment in II, V1, V2,and V3. Additional leads from the third and fourth interspaces afforded no evidence of novel char-acter. These changes were thought to suggest injury of the apicolateral region of the left ventricularwall.
the other 5 cases would have occurred had thepatients survived the episode.
Five of these 6 patients died during the acutephase of myocardial infarction, the immediatecause of death being rupture of the left ven-
tricular wall. The sites of rupture are shownby the heavy black lines and arrows in figures2, 3, and 4.Acute Transmural Infarction of Latero-
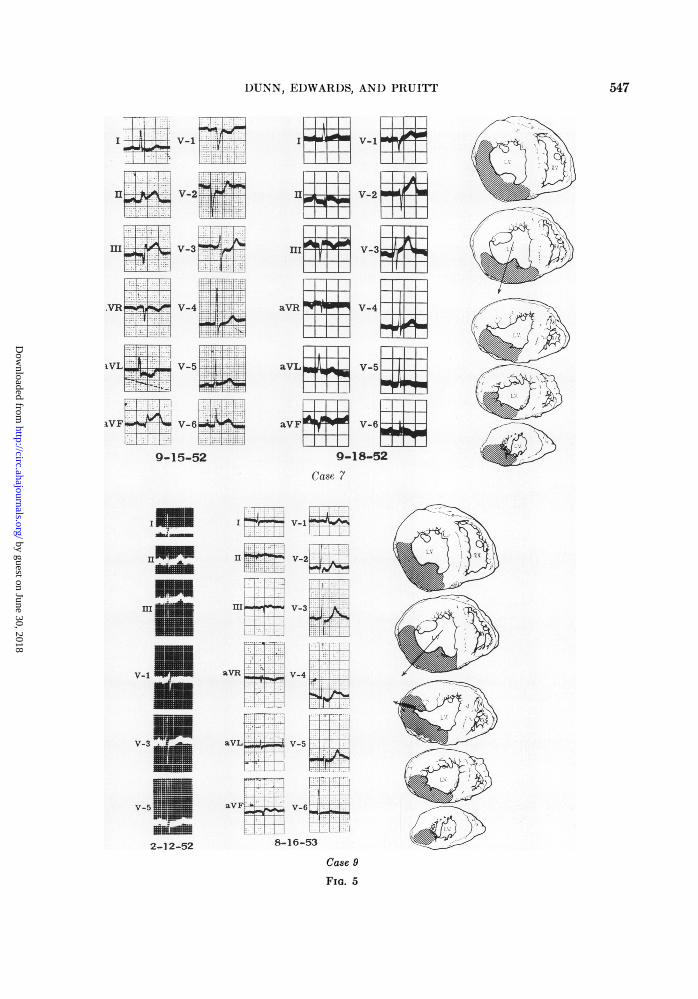
posterior Wall of Left Ventricle. Cases 7 through12 were of this type (figs. 5 and 6).The arrangement of data in figures 5 and 6
was designed to emphasize an interestingrelationship between the location of the myo-
cardial infarct and the nature of the electro-cardiographic findings. The lesion in case 7
showed the most extensive invasion of theposterior wall as compared with the lateral wallof the left ventricle. The vector drawn in slice2 of the cross-sectional diagrams indicates theessentially posterior orientation of the lesion.Correspondingly, both this case and its counter-part (case 8) display the most definitelyposterior orientation of the electrocardio-graphic changes, which are pronounced indegree and which are manifest in aberrations ofthe QRS, the S-T segment, and the T-wavecomponents of the ventricular complexes. Incontrast, the lesion in case 12 was a largeinfarct of the lateral wall of the left ventriclethat invaded to a limited degree the adjacentposterior wall. The vector hypothesized from
II- __V-23
T::1 E
aVR4-1, V-4
aVF SV-V-"
544
V-2
V-3
3 V-4
V-4
V-5
6 V-6
12-15-50
I I V-1
11 V-2
III ..AL.ni V-3
V-1 aVR V-4
v-3 aVL V-5
v-5 aVF V-6
by guest on June 30, 2018http://circ.ahajournals.org/
Dow
nloaded from
DUNN, EDWARDS, AND PRUITT
Case 3
I V- *
UUa V-2
III W V-3
aVRt V-4
aVL 4 V-5
aVF V-6
6-20-50
Case 4
Tl-m+Pl-l VT d. LI.-1 Gl
-r l 1'- 1.1- - l llaI11 rm V-2 I Lw1 1
- --- - I;I.1111 '1,11111u l 1,2amF Vl-3~ 1I Teal' _ i l {1
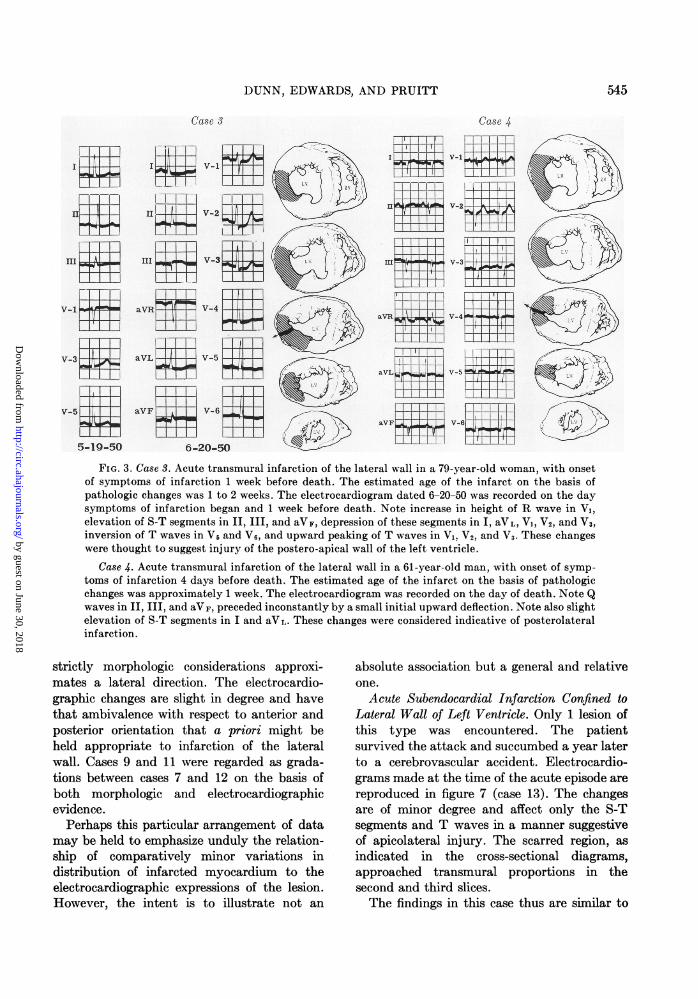
FIG. 3. Case 3. Acute transmural infarction of the lateral wall in a 79-year-old woman, with onsetof symptoms of infarction 1 week before death. The estimated age of the infarct on the basis ofpathologic changes was 1 to 2 weeks. The electrocardiogram dated 6-20-50 was recorded on the daysymptoms of infarction began and 1 week before death. Note increase in height of R wave in Vi,elevation of S-T segments in II, III, and aVF, depression of these segments in I, aVL, V1, V2, and V3,inversion of T waves in V5 and V6, and upward peaking of T waves in V,. V2, and V3. These changeswere thought to suggest injury of the postero-apical wall of the left ventricle.
Case 4. Acute transmural infarction of the lateral wall in a 61-year-old man, with onset of symp-
toms of infarction 4 days before death. The estimated age of the infarct on the basis of pathologicchanges was approximately 1 week. The electrocardiogram was recorded on the day of death. Note Qwaves in II, III, and aVF, preceded inconstantly by a small initial upward deflection. Note also slightelevation of S-T segments in I and aVL. These changes were considered indicative of posterolateralinfarction.
strictly morphologic considerations approxi-mates a lateral direction. The electrocardio-graphic changes are slight in degree and havethat ambivalence with respect to anterior andposterior orientation that a priori might beheld appropriate to infarction of the lateralwall. Cases 9 and 11 were regarded as grada-tions between cases 7 and 12 on the basis ofboth morphologic and electrocardiographicevidence.
Perhaps this particular arrangement of datamay be held to emphasize unduly the relation-ship of comparatively minor variations indistribution of infarcted myocardium to theelectrocardiographic expressions of the lesion.However, the intent is to illustrate not an
absolute association but a general and relativeone.
Acute Subendocardial Infarction Confined toLateral Wall of Left Ventricle. Only 1 lesion ofthis type was encountered. The patientsurvived the attack and succumbed a year laterto a cerebrovascular accident. Electrocardio-grams made at the time of the acute episode are
reproduced in figure 7 (case 13). The changesare of minor degree and affect only the S-Tsegments and T waves in a manner suggestiveof apicolateral injury. The scarred region, as
indicated in the cross-sectional diagrams,approached transmural proportions in thesecond and third slices.The findings in this case thus are similar to
I,
719lU . 1
5-1-50V-3XWF
T I 1
1 1 1v-5 _l
5-19-50
545
t.t,.
-TT-n-- FaVL V-5 j' %do Mm
_ii 11 M
aVII,IMMIWY00 V-6MP r--- r
1_. 1
by guest on June 30, 2018http://circ.ahajournals.org/
Dow
nloaded from
ELECTROCARDIOGRAM IN INFARCTION OF LEFT VENTRICLE
those encountered in acute transmural infarc-tion involving the same region.
Healed Subendocardial Infarction Confined toLateral Wall of Left Ventricle. Cases 14 through26 were of this type (fig. 7, cases 14, 16, and22).
Case
UU
m
CR2 V-1
IVR V-3E
V-5O2
10-18-44 12-12-51
Case 14 had a counterpart in 1 other case
with respect to distribution of the scar of themyocardial infarct and the nature of theelectrocardiographic findings. In these 2 cases,a subendocardial scar extending from apex tobase of the lateral wall of the left ventricle was
Case 6
0%1 1 IIE II _P V_1 r
111 1 [II0MIxw
m to me v3 _ K _
aVR% V4V4
aVLRV_ 11 117 [ I 1 1llBy
aVF V-6Err~WH
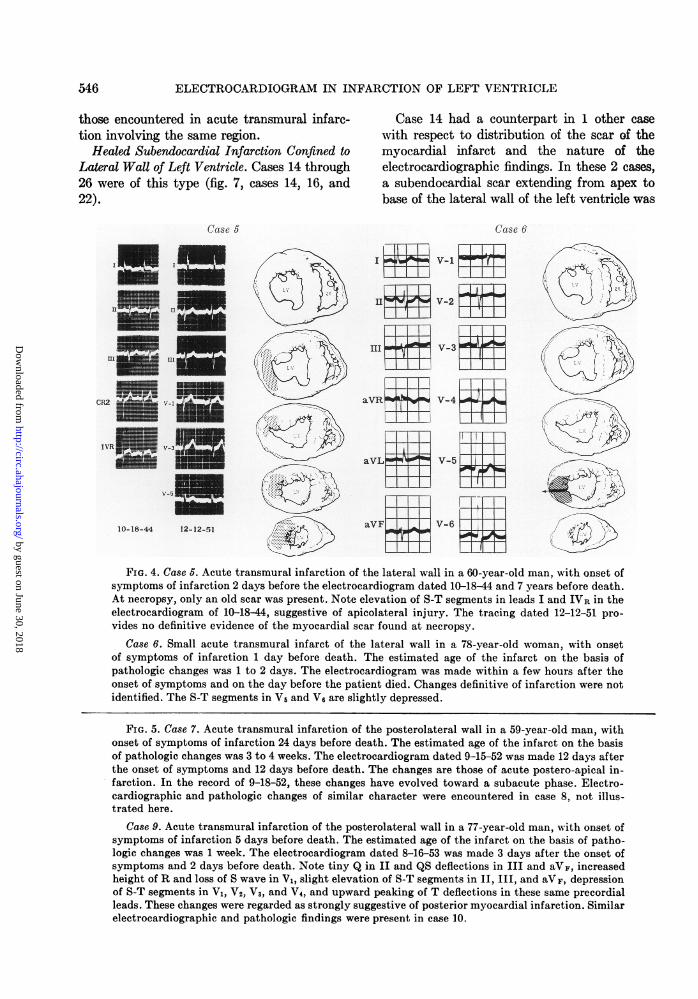
FIG. 4. Case 5. Acute transmural infarction of the lateral wall in a 60-year-old man, with onset ofsymptoms of infarction 2 days before the electrocardiogram dated 10-18-44 and 7 years before death.At necropsy, only an old scar was present. Note elevation of S-T segments in leads I and LVR in theelectrocardiogram of 10-18-44, suggestive of apicolateral injury. The tracing dated 12-12-51 pro-vides no definitive evidence of the myocardial scar found at necropsy.
Case 6. Small acute transmural infarct of the lateral wall in a 78-year-old woman, with onsetof symptoms of infarction 1 day before death. The estimated age of the infarct on the basis ofpathologic changes was 1 to 2 days. The electrocardiogram was made within a few hours after theonset of symptoms and on the day before the patient died. Changes definitive of infarction were notidentified. The S-T segments in Vs and V6 are slightly depressed.
FIG. 5. Case 7. Acute transmural infarction of the posterolateral wall in a 59-year-old man, withonset of symptoms of infarction 24 days before death. The estimated age of the infarct on the basisof pathologic changes was 3 to 4 weeks. The electrocardiogram dated 9-15-52 was made 12 days afterthe onset of symptoms and 12 days before death. The changes are those of acute postero-apical in-farction. In the record of 9-18-52, these changes have evolved toward a subacute phase. Electro-cardiographic and pathologic changes of similar character were encountered in case 8, not illus-trated here.
Case 9. Acute transmural infarction of the posterolateral wall in a 77-year-old man, with onset ofsymptoms of infarction 5 days before death. The estimated age of the infarct on the basis of patho-logic changes was 1 week. The electrocardiogram dated 8-16-53 was made 3 days after the onset ofsymptoms and 2 days before death. Note tiny Q in II and QS deflections in III and aVF, increasedheight of R and loss of S wave in V1, slight elevation of S-T segments in II, III, and aVF, depressionof S-T segments in V1, V2, V,, and V4, and upward peaking of T deflections in these same precordialleads. These changes were regarded as strongly suggestive of posterior myocardial infarction. Similarelectrocardiographic and pathologic findings were present in case 10.
546
1
12enp-.
'llb 1.
4 by guest on June 30, 2018http://circ.ahajournals.org/
Dow
nloaded from
1)UNN, EDWARDS, AND PRUITT
9-15-52
IIe 4-- - V-2 wi
IIII s- -3
.VR V-5 -slT-ttl~~~i'l~~~-7t ..-.-l .r.TT;
1.VF"QH~
H1i
V-1 MW
V-3
V-5
aVRla
aVL:
aV{
aF-
2-12-52
I9 e V-10
I111 AI+ V-2
V~ r 16
IOR I0' VI3L1 TH 111 1
aVR bC0 V-4 11
aVL0P v-5j
aVAF 9ON V-6
9-18-52
Case 7
HV-1+
e Vj-2
z :v-3Lj^
VV-4;
V-5<
84V-65
8-16-53
Case 9
FIG. 5
547
11
.Q
by guest on June 30, 2018http://circ.ahajournals.org/
Dow
nloaded from
ELECTROCARDIOGRAM IN INFARCTION OF LEFT VENTRICLE
attended by small Q deflections in leads II andIII in electrocardiograms recorded at a timeremote from occurrence of the infarct. Thesetracings were judged to afford evidence sug-gestive of old posterior myocardial infarction.
Case 16 had counterparts in 5 other cases. Ineach instance, a subendocardial scar in thelateral wall of the left ventricle was attendedby electrocardiographic evidence that in someway was suggestive but not definitive of oldapical or apicolateral infarction. In cases 16,17, and 18, Q deflections were present instandard leads I and II, and small Q deflections
Case 11
1J
m
aVR V-m+,. i.m
were present also in precordial lead V5 in cases16 and 17. Small Q deflections in V6 followedby R waves unusually small for this point onthe precordium were present in case 19. Aspossible evidence of an old scar, only a QRdeflection in extremity leads aV, and aVL wasnoted in case 20. In case 21, the final member ofthis group, increased height of the R de-flections in V1 was the only suggestion ofpossible loss of myocardial mass in the wall ofthat ventricle contralateral to the one overwhich the precordial electrode was placed.
Case 22 had counterparts in 4 other cases. In
Case 12
aVL $V-5 -711$XV54Va v
aVFt Xv V-6AtV V -6X-
11-27-51 12-19-51
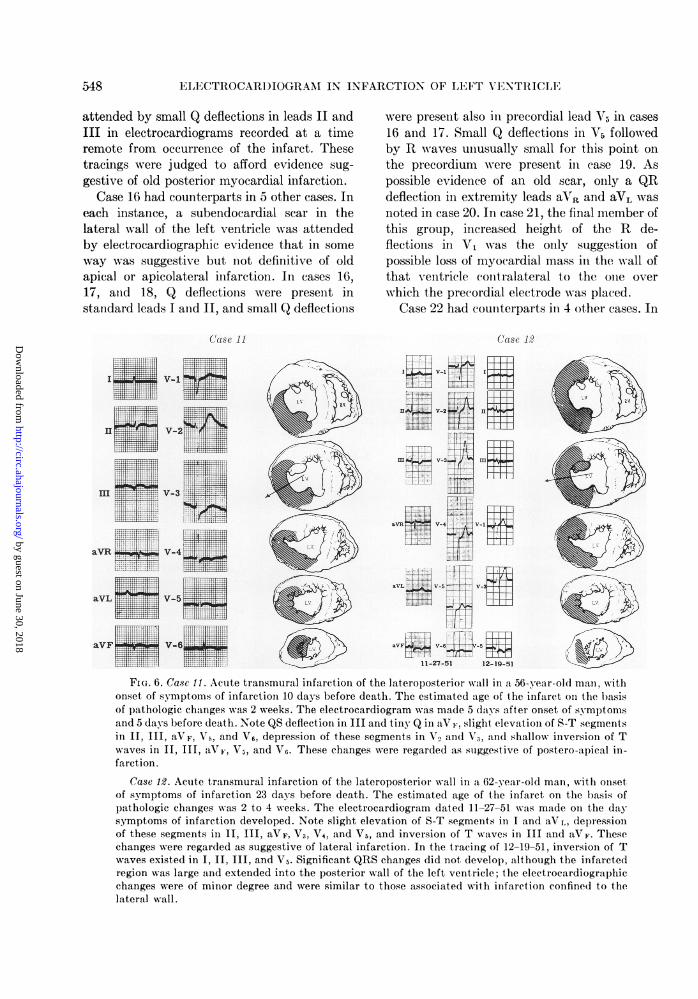
FIG. 6. Case 11. Acute transmural infarction of the lateroposterior wall in a 56-year-old man, withonset of symptoms of infarction 10 days before death. The estimated age of the infarct on the basisof pathologic changes was 2 weeks. The electrocardiogram was made 5 days after onset of symptomsand 5 days before death. Note QS deflection in III and tiny Q in aVF, slight elevation of S-T segmentsin II, III, aVF, V5, and V6, depression of these segments in V2 and V3, and shallow inversion of Twaves in II, III, aVF, V5, and V6. These changes were regarded as suggestive of postero-apical in-farction.
Case 12. Acute transmural infarction of the lateroposterior wall in a 62-year-old man, with onsetof symptoms of infarction 23 days before death. The estimated age of the infarct on the basis ofpathologic changes was 2 to 4 weeks. The electrocardiogram dated 11-27-51 was made on the daysymptoms of infarction developed. Note slight elevation of S-T segments in I and aVL, depressionof these segments in II, III, aVF, V3, V4, and V5, and inversion of T waves in III and aVF. Thesechanges were regarded as suggestive of lateral infarction. In the tracing of 12-19-51, inversion of Twaves existed in I, II, III, and V5. Significant QRS changes did not develop, although the infarctedregion was large and extended into the posterior wall of the left ventricle; the electrocardiographicchanges were of minor degree and were similar to those associated with infarction confined to thelateral wall.
548
W ..lfl,
V-1
V-2 T
X.m
........"_w Wfi
144
i V-3;!T:
7:
Itill, 1.51
by guest on June 30, 2018http://circ.ahajournals.org/
Dow
nloaded from
DUNN, EDWARDS, AND PRUITT
each instance, a subendocardial scar in thelateral wall of the left ventricle was associatedwith electrocardiographic findings judged to bewithin the range of normal.
Thus, electrocardiograms made at a timeremote from the period when the lesion wasacute in these 13 cases revealed evidence sug-gestive of posterior scarring in 2 cases, showedchanges classed as possible but far fromdefinitive evidence of apical or lateral scarringin 6 cases, and were normal in 5 cases.
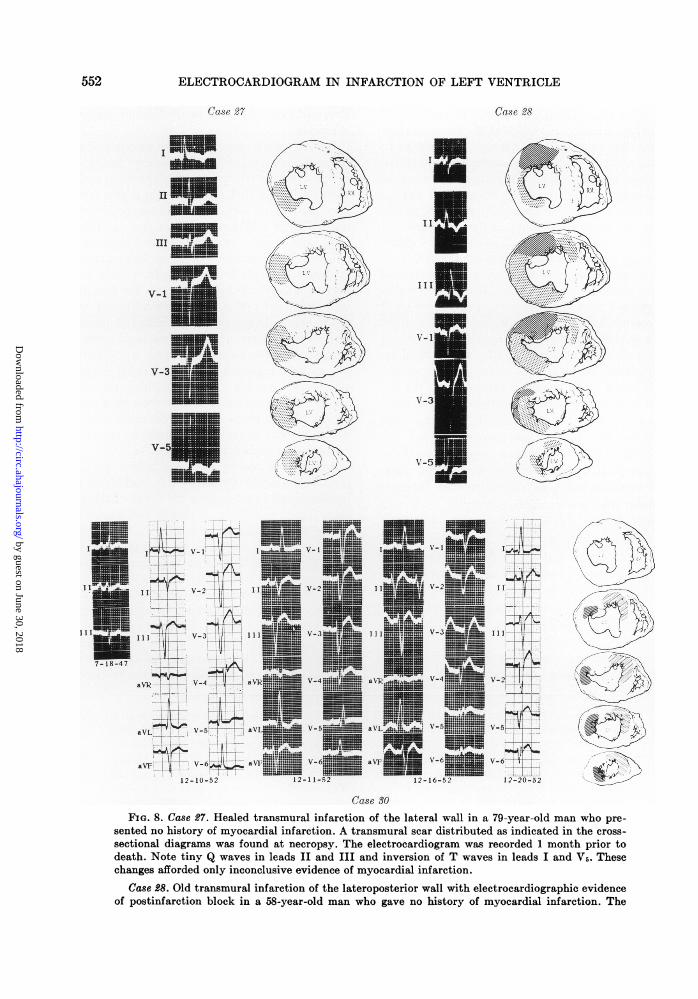
Healed Transmural Infarction Confined toLateral Wall of Left Ventricle. Only 1 instanceof this type was encountered (fig. 8, case 27).A tiny Q deflection 1 mm. in depth in leads IIand III constituted the only evidence sug-gestive of a myocardial scar, although pro-nounced scarring attended by thinning of theleft ventricular wall was present.
Selected Cases. As already noted, 3 cases wereretained from 2 categories otherwise deletedfrom the study.
Old Posterolateral Infarction with Post-infarction Block. In 2 of the 3 selected cases, theelectrocardiogram revealed changes held to becharacteristic of postinfarction block. Il-lustrated in case 28 of figure 8 are the electro-cardiograms and cross-sectional diagrams in 1of these 2. These tracings were recorded beforethe acute anterior infarction, and the Q wavesin leads II and III, together with the prolongedQRS interval, may be ascribed to the conse-quences of the old transmural posterolateralmyocardial infarct. The findings in case 29 werenearly identical as to both electrocardiographicchanges and the pertinent morphologic lesion;the latter consisted of an old posterolateralinfarct that was classed as subendocardial butthat approached transmural extent.
These 2 cases provide a small but perhapssubstantial basis on which to rest speculationregarding the nature of postinfarction block. Inleads II and III, and predictably aVF, the finalcomponent of the widened QRS complex is anR wave. Other studies, in which esophagealleads were used, support the view that this Rdeflection is an expression of delayed excitationof the ventricular myocardium in the postero-lateral region of the heart.8 A posterolateralinfarct of the type encountered in cases 28 and
29 must disturb the spread of the excitationprocess in such a manner that its arrival at theposterobasal fibers is delayed or its spread intothem is accomplished in an anomalous fashion.
Acute Subendocardial Infarction of LateralWall of Left Ventricle with Old TransmuralAnteroseptal Infarction and Left Bundle-BranchBlock. This complex of morphologic andfunctional phenomena is presented as anexcellent example of events occurring withinnature in an order that precisely and definitelytests existing concepts concerning bundle-branch block and the electrocardiographicconsequences of superimposed myocardial in-farction.
In case 30 of figure 8, the electrocardiogramof December 10, made in all probability beforethe acute lateral infarct, revealed left bundle-branch block unusual in the presence of a Qdeflection in leads I, aVL, V5, and V6. Thepresence of such a deflection suggests a loss ofseptal myocardium, a situation later confirmedin this case by the finding at necropsy of an oldanteroseptal myocardial infarct. The finalcomponent of the QRS complexes in leads V6and V6 in this same electrocardiogram is an Rwave, the origin of which is ascribed toexcitation of the apicolateral wall of the leftventricle. In the other 3 electrocardiogramsillustrated in this case, the R waves diminishprogressively in height at a time when clinicaland pathologic findings indicated the incidenceof infarction involving the myocardium of thatsame lateral wall.
DISCUSSIONThe principal objective of this article has
been to present as lucidly as possible a correla-tion of electrocardiographic and pathologic datain cases of infarction of the lateral wall of theleft ventricle with and without involvement ofadjacent regions. Certain comments alreadyhave been made. A condensation of results willbe undertaken in the section devoted tosummary and conclusions. Remaining forcomment are 3 points, 2 of which developnaturally from appraisal of the total body ofevidence; the other appears as a rather sur-prising and, in some measure, a chance de-velopment.
549
by guest on June 30, 2018http://circ.ahajournals.org/
Dow
nloaded from
ELECTROCARDIOGRAM IN INFARCTION OF LEFT VENTRICLE
Case 13
V-5~
7-8-52
ISki 15 Vx~~~3r83.. U
IIL V25f V-
I I I iV -3 =V-~75-52
OlR _ v- v-7
aVL iiiV-5 |V-8
aOF v-6 axt 1la s
7-15-52
1i 1v-1~
V_3+
v-5 I
Case 16
____
V-1.._SHas_
______
V-3.t=____H_____
__- - - - - | - - - - |-|-
- -
v-an:_-EP-_hF_-----
Case 22
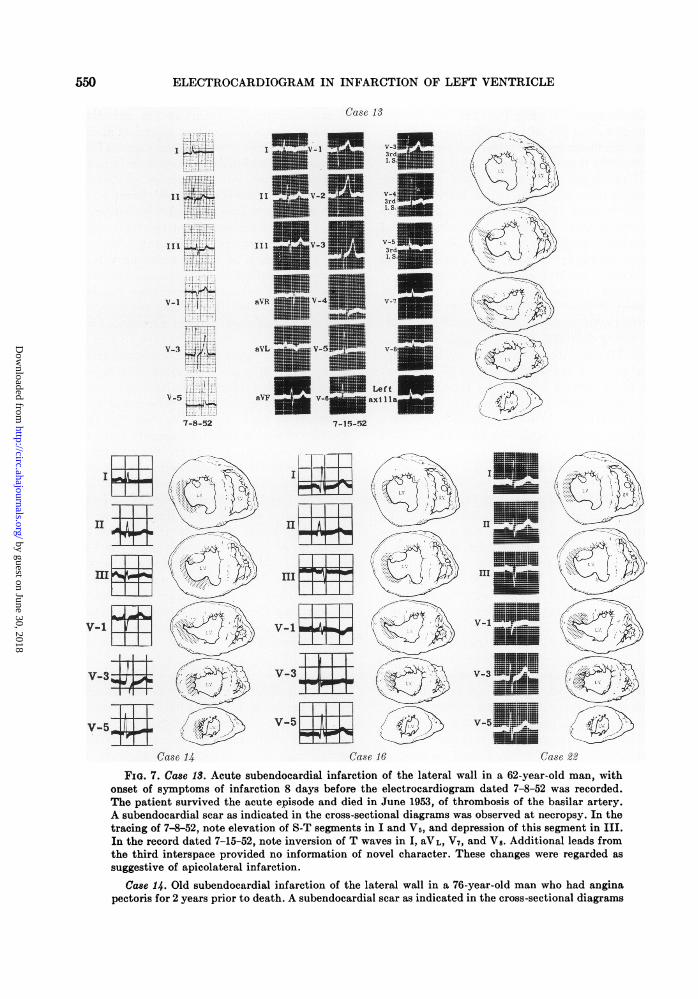
FIG. 7. Case 13. Acute subendocardial infarction of the lateral wall in a 62-year-old man, withonset of symptoms of infarction 8 days before the electrocardiogram dated 7-8-52 was recorded.The patient survived the acute episode and died in June 1953, of thrombosis of the basilar artery.A subendocardial scar as indicated in the cross-sectional diagrams was observed at necropsy. In thetracing of 7-8-52, note elevation of S-T segments in I and V5, and depression of this segment in III.In the record dated 7-15-52, note inversion of T waves in I, aVL, V7, and V8. Additional leads fromthe third interspace provided no information of novel character. These changes were regarded as
suggestive of apicolateral infarction.
Case 14. Old subendocardial infarction of the lateral wall in a 76-year-old man who had anginapectoris for 2 years prior to death. A subendocardial scar as indicated in the cross-sectional diagrams
IE&L1
%m
V41
V-3
v I I I.V mT
Case 14
550
by guest on June 30, 2018http://circ.ahajournals.org/
Dow
nloaded from

DUNN, EDWARDS, AND PRUITT
1. In the identification of the presence ofacute or healed infarction of the lateral wall ofthe left ventricle, the question is raised as tohow critical a factor is the adequacy of theelectrocardiographic exploration in terms ofnumber of leads recorded. Rosenbaum and co-
workers5 proposed that additional leads shouldbe recorded from points on the left portion ofthe precordium higher than the conventionalones when abnormal findings appear in the leftprecordial leads or in lead aVL. Myers andassociates3 observed that the electrocardio-grams frequently were normal in a series of 27cases of infarction of the lateral wall, except fora Q deflection regarded by these authors as
significantly abnormal in aVL. Our clinical ex-
perience would lead us to support the desira-bility of recording the potentials from the leftarm in any patient suspected of having myo-
cardial infarction. Additional leads from theupper left part of the precordium and leftaxilla have not proved especially helpfulinasmuch as the evidence supplied by themcommonly has been similar to that obtainedfrom the conventional precordial leads andaVL. If the latter were abnormal, the same kindof abnormality appeared in the added pre-
cordial leads, but these latter leads rarelyclarified appreciably the diagnostic problem. Ifthe conventionally derived leads were normal,so were the additional leads. Exceptions tothese generalizations exist, and a reasonablequestion is whether the frequency of theiroccurrence justifies encouraging physicians toobtain additional leads that must be in-
terpreted cautiously because of their unfamiliarcharacter.Review of our series of cases supports the
following observations. Acute transmural in-farction commonly produced segmental andT-wave changes that were minor in degree butwere distributed through several conventionalleads. Use of additional leads in cases of thistype offers scant prospect of clarifying sig-nificantly the diagnostic problem. In contrast,evidences of an electrocardiographic relic of anancient subendocardial infarct of the lateralwall either did not exist or were restricted toQRS changes of minor degree limited at timesto a single lead among the conventional series.Among this latter category of cases, use of leadaVL may be regarded as essential to adequateelectrocardiographic exploration, and the re-
cording of additional leads from the upper leftregion of the precordium is desirable whenminor changes in the QRS complexes are en-
countered in leads I, aVL, V5, and V6.2. Included among our illustrations are 2
instances in which the R wave in lead V, was
unusually tall in relation to the depth of the Swave (fig. 2, case 1; fig. 5, case 9) and 2 othersin which the R deflection in lead V1 was tallerin tracings made after infarction of the lateralwall had occurred than it was prior to in-farction (fig. 2, case 2; fig. 3, case 3).
Case 9 is a striking example of this electro-cardiographic finding and an excellent modelfor illustrating its origins. As seen in the cross-
sectional diagrams (fig. 5), the mass of infarctedmyocardium in the posterolateral wall was
located opposite to that portion of the anterior
was observed at necropsy. Note small Q waves in leads II and III of the electrocardiogram made 9days before death. These findings were considered suggestive of old posterior myocardial infarction.Electrocardiographic and pathologic changes of similar character were encountered in case 15.
Case 16. Old subendocardial infarction of the lateral wall in a 64-year-old man who gave a historysuggestive of myocardial infarction 12 years prior to death. At necropsy, a subendocardial scar of thedistribution indicated in the diagrams was observed. The electrocardiogram was recorded 6 monthsprior to death. Note Q waves in leads I, II, and V5. These findings were regarded as possibly relatedto old apicolateral infarction. Electrocardiographic and pathologic changes of similar character wereencountered in cases 17 through 21.
Case 22. Old subendocardial infarction of the lateral wall in a 74-year-old man who gave no historyof myocardial infarction. A subendocardial scar distributed as indicated in the cross-sectional dia-grams was noted at necropsy. The electrocardiogram was recorded 1 month prior to death. Changessuggestive of myocardial scarring were not defined. Electrocardiographic and pathologic changes ofsimilar character were encountered in cases 23 through 26.
551
by guest on June 30, 2018http://circ.ahajournals.org/
Dow
nloaded from
ELECTROCARDIOGRAM IN INFARCTION OF LEFT VENTRICLE
Case 27
_I__§_
!___IL_____
_______s___
T-;_-____
III |
___ __ _
_Aw
V-1
Case 28
II
II
V-1
V.
V -50
.1 i
7-8 -4
= VR
_ VL
1 _ V-1 ""-I_ V-1 _
11 V-2 ~|11 1 _ i -
il V-Ail 1s 3 V 2& 1i_ V-45X||11 I1VR V-
aVF
Case 30
FIG. 8. Case 27. Healed transmural infarction of the lateral wall in a 79-year-old man who pre-sented no history of myocardial infarction. A transmural scar distributed as indicated in the cross-
sectional diagrams was found at necropsy. The electrocardiogram was recorded 1 month prior todeath. Note tiny Q waves in leads II and III and inversion of T waves in leads I and V5. Thesechanges afforded only inconclusive evidence of myocardial infarction.
Case 28. Old transmural infarction of the lateroposterior wall with electrocardiographic evidenceof postinfarction block in a 58-year-old man who gave no history of myocardial infarction. The
552
1
V-2
V-5
v-6 2--
12-20-52
..............
-.............1....
k, 111.1.1.
aV 1 whathi.& V - 5 &VL----
avi., V-(
12-11-
_^-
,,\' ;
by guest on June 30, 2018http://circ.ahajournals.org/
Dow
nloaded from
DUNN, EDWARDS, AND PRUITT
wall of the heart over which the exploringelectrode in lead V1 commonly is placed. If theforces produced in electric systole by theposterolateral wall prior to infarction were
represented by the vector shown in the secondof these diagrams, then elimination of theseforces consequent to infarction of the myo-
cardium in that region would leave unopposedthe forces produced in that portion of theanterior wall of the heart underlying V1. Undersuch circumstances, the QRS complex in leadV1 might become a monophasic R wave.
Unfortunately, alteration in the height of a
normally occurring R wave may not beparticularly helpful in establishing the presence
of myocardial infarction. Perhaps vectorcardio-graphic study of this disturbance in the normalbalance of electric forces may afford a means ofusing the phenomenon to greater diagnosticadvantage.
3. A third point warrants comment, even
though it bears on a matter apart from thecorrelation of pathologic and electrocardio-graphic data that is the theme of this article. Asmentioned previously, death occurred in 5 ofthe 6 cases in which electrocardiograms were
made during acute transmural infarction of thelateral wall, and the cause of death in every
case was rupture of the left ventricular wall.Review of the cross-sectional diagrams of theheart in these cases discloses that the site ofrupture in cases 1, 3, and 4 was approximatelyin the center of the infarcted myocardium at a
point between the anterior and posteriorpapillary muscles where the ventricular wall isless thick. The rupture in case 6 was in thesame general location but disposed 1 slice
toward the apex; in case 2, it was at thejunction between infarcted and uninfarctedmyocardium along the anterior margin of theinfarct.
SUMMARY AND CONCLUSIONSPertinent electrocardiographic and patho-
logic findings have been correlated in 30 cases
of myocardial infarction involving the lateralwall of the left ventricle studied at the MayoClinic.
In acute transmural infarction confined tothe lateral wall of the left ventricle, electro-cardiograms made up of 6 leads (standard limbleads and precordial leads V1, V3, and V5) or
12 leads (the 6 just mentioned plus unipolarextremity leads and precordial leads V2, V4,and V6) recorded in the conventional manner
commonly disclosed evidence of acute myo-
cardial injury. QRS changes of magnitude andcharacter sufficient to be definitive of myo-
cardial infarction rarely developed. Segmentalelevation and subsequent inversion of T waves
commonly occurred in leads presumably so
oriented as to face the epicardial aspect of theinfarcted myocardium. However, the dispo-sition of these changes varied among the severalcases, suggesting in one or more instances apicalinjury (changes in leads V1 and V6), posteriorinjury (changes in leads II, III, and aVF) or
lateral injury (changes in leads I and aVL) or
some combination of 2 or more of thesevariants. No consistently recurring "pattern"could be derived.When acute transmural infarction involved
both the lateral and posterior portions of thewall of the left ventricle, the electrocardio-
electrocardiogram was recorded 8 days prior to death and before development of the acute myo-cardial infarct outlined in the cross-sectional diagrams. The significant correlation, therefore, in-volved the electrocardiogram and the old infarct of the lateroposterior wall. Note a QRS interval of0.12 sec., Q deflections in leads II and III, S deflections in leads I and V5, and absence of evidenceof right bundle-branch block in V,. Electrocardiographic and pathologic changes of similar characterwere encountered in case 29.
Case 30. Healed transmural anteroseptal infarction and acute subendocardial lateral infarctionin the presence of left bundle-branch block in a 61-year-old woman who had a history of anginapectoris for 6 months. The onset of symptoms of acute myocardial infarction was on December 13,1952, and death occurred on December 20. The age of the acute infarct as estimated at necropsywas 5 to 7 days. The electrocardiogram dated 12-10-52 reveals a QRS interval in excess of 0.12 sec.The Q waves in leads I, aVL, and V6 are related to the old anteroseptal infarct in the presence ofleft bundle-branch block. The progressive diminution in height of the final R deflection in V5 andVo in subsequent tracings resulted from and was pathognomonic of infarction of the lateral wall.
553
by guest on June 30, 2018http://circ.ahajournals.org/
Dow
nloaded from

ELECTROCARDIOGRAM IN INFARCTION OF LEFT VENTRICLE
graphic changes assumed a posterior characterto a degree roughly proportional to the extentof involvement of the posterior ventricular wall.As might be predicted from the character of
the electrocardiographic changes encounteredin the acute stage of transmural infarction ofthe lateral wall, the electrocardiographic relicsattending healed lesions of that wall were ofminor extent or were absent. Among electro-cardiograms made in 13 cases of healed sub-endocardial infarction of the lateral wall of theleft ventricle, 2 revealed evidence suggestive ofposterior scarring, 6 presented changes classedas affording possible evidence of apical orlateral scarring, and 5 were regarded as normal.According to the limited data in this study,only among cases in which routine electro-cardiograms are suggestive of apical or lateralscarring would there appear to be an indicationfor securing additional leads from the upper leftportion of the precordium or the left axilla.Two cases of healed lateroposterior infarction
attended by electrocardiographic evidence ofpostinfarction block were encountered.A single case of acute subendocardial in-
farction of the lateral wall of the left ventriclecombined with old transmural anteroseptal in-farction in the presence of left bundle-branchblock presented a basis for the evaluation ofcurrently accepted concepts concerning bundle-branch block and the electrocardiographicconsequences of superimposed myocardial in-farction.A change in QRS configuration peculiar to
lesions of the lateral wall as contrasted to myo-cardial infarcts of other localizations is anincrease in height of the R deflection in pre-cordial leads centered around position 1. Thediagnostic value of this finding is reduced bythe fact that it is a quantitative rather than aqualitative change
Infarcts of the lateral wall of the leftventricle, particularly in their acute phases, arenot electrocardiographically "silent"; theirvoice is, however, one of weak and mingledtones.
SUMMARIO IN INTERLINGUAPertinente constatationes electrocardio-
graphic e pathologic esseva correlationate in 30
casos de infarcimento myocardial involvente lepariete lateral del ventriculo sinsistre, studiateal Clinica Mayo.
In casos de acute infarcimento transmuralrestringite al pariete lateral del ventriculosinistre, electrocardiogrammas consistente de 6derivationes (le derivationes standard deextremitate e le derivationes precordial V,, V3,e V5) o de 12 derivationes (le 6 derivationesjusto mentionate, le derivationes unipolar deextremitate, e le derivationes precordial V2,V4, e V6), omnes registrate in le maniera con-ventional, revelava generalmente manifesta-tiones de acute lesion myocardial. Se disve-loppava rarmente alterationes de QRS demagnitude e de character sufficiente pro esserinterpretate como signos definitive de in-farcimento myocardial. Elevation segmental einversion subsequente del undas T occurrevacommunmente in derivationes que essevasupponitemente orientate de maniera a esserconfrontate con le aspecto epicardial delinfarcite myocardio. Tamen, le disposition deiste alterationes variava ab un caso al alteres,suggerente-pro un o plure patientes-lesionapical (alterationes in derivation V5 e V6),lesion posterior (alterationes in derivation II,III, e aVF), lesion lateral (alterationes inderivation I e aVL), o le un o le altere com-bination de 2 o plures de iste variantes. II nonesseva possibile derivar un specific "con-figuration" de recurrentia regular.
In casos in que le infarcimento transmuralinvolveva le portiones tanto lateral comoetiam posterior del pariete del ventriculosinistre, le alterationes electrocardiographicexhibiva un character posterior de gradosgrossiermente proportional al mesura de in-volvimento del pariete postero-ventricular.
Viste le character del alterationes electro-cardiographic incontrate in le stadio acute delinfarcimento transmural del pariete lateral, ilnon esseva un surprisa notar que le reliquiaselectrocardiographic associate con curate le-siones de ille pariete esseva pauco importantesi illos esseva presente del toto. Inter le electro-cardiogrammas obtenite in 13 casos de curateinfarcimento subendocardial del pariete lateraldel ventriculo sinistre, 2 exhibiva aspectossuggestive de cicatrisation posterior, 6 mons-
554
by guest on June 30, 2018http://circ.ahajournals.org/
Dow
nloaded from
DUNN, EDWARDS, AND PRUITT
trava alterationes que poteva esser interpre-tate como manifestationes de cicatrisationapical o lateral, e 5 esseva considerate comonormal. Super le base del restringite datos delpresente studio, il pare que le casos in que leelectrocardiogrammas de routine suggere lepresentia de cicatrisation apical o lateral es lesol casos in que il pote esser indicate obtenerderivationes additional ab le portion supero-sinistre del precordio o ab le axilla sinistre.Esseva incontrate 2 casos de curate in-
farcimento latero-posterior con signos electro-cardiographic de bloco postinfarcimental.Un sol caso de acute infarcimento sub-
endocardial del pariete lateral del ventriculosinistre in combination con ancian infarcimentotransmural anteroseptal e bloco de brancasinistre offereva un base pro le evalutation decurrentemente acceptate notiones in re blocode branca e le consequentias electrocardio-graphic de superimponite infarcimento myo-cardial.Un alteration del configuration de QRS que
es restringite a lesiones del pariete lateral (incontrasto con infarcimentos myocardial dealtere locationes) es un augmento de elevationdel deflexion R in derivationes precordialcentrate circa le position 1. Le valor diagnosticde iste constatation es reducite per le facto queil se tracta de un alteration quantitative plustosto que qualitative.
Infarcimentos del pariete lateral del ventri-culo sinistre, specialmente in lor phases acute,non es electrocardiographicamente "silente,"sed lor voce ha solmente sonos que es debile emiscite.
REFERENCES1 WOOD, F. C., WOLFERTH, C. C., AND BELLET, S.:
Infarction of the lateral wall of the left ven-tricle: Electrocardiographic characteristics. Am.Heart J. 16: 387, 1938.
2 THOMSON, H. W., AND FEIL, H.: Infarction of thelateral wall of the left ventricle: Pathologic andelectrocardiographic study. Am. J. M. SC. 207:588, 1944.
3 MYERS, G. B., KLEIN, H. A., AND STOFER, B. E.:Correlation of electrocardiographic and patho-logic findings in lateral infarction. Am. Heart J.37: 374, 1949.
4 SHAFFER, C. F.: Electrocardiographic study oflateral infarction, proved at autopsy. Am. HeartJ. 28: 39, 1944.
5ROSENBAUM, F. F., WILSON, F. N., AND JOHNSTON,F. P.: The precordial electrocardiogram in highlateral myocardial infarction. Am. Heart J.32: 135, 1946.
6HECHT, H. H.: The localization of myocardialinfarcts with particular reference to lateralinfarction and to the TI Q3 pattern. Proc. Am.Fed. Clin. Res. 2: 102, 1945.
7ACHOR, R. W. P.: The fate of patients who havesurvived acute myocardial infarction. Thesis,Graduate School, University of Minnesota, 1953.
8BURCHELL, H. B., AND PRUITr, R. D.: The valueof the esophageal electrocardiogram in theelucidation of postinfarction intraventricularblock. Am. Heart J. 42: 81, 1951.
e.The Foxglove is a plant sufficiently common in this island, and as we have but one species, and
that so generally known, I should have thought it superfluous either to figure or describe it; had Inot more than once seen the leaves of Mullein gathered for those of Foxglove. On the continent ofEurope too, other species are found, and I have been informed that our species is very rare in someparts of Germany, existing only by means of cultivation, in gardens.
Our plant is the Digitalis purpurea of Linnaeus. It belongs to the 2d order of the 14th class,or the Didynamnia Angiospermia. The essential characters of the genus are, Cup with 5 divisions.Blossom bell-shaped, bulging. Capsule egg-shaped, 2 celled.-WILLIAM WITHERING. An Accountof the Foxglove, and Some of Its Medical Uses. Brimingham, 1785.
555
by guest on June 30, 2018http://circ.ahajournals.org/
Dow
nloaded from
WILLIAM J. DUNN, JESSE E. EDWARDS and RAYMOND D. PRUITTA Clinicopathologic Study
The Electrocardiogram in Infarction of the Lateral Wall of the Left Ventricle:
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1956 American Heart Association, Inc. All rights reserved.
75231is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TXCirculation
doi: 10.1161/01.CIR.14.4.5401956;14:540-555Circulation.
http://circ.ahajournals.org/content/14/4/540located on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer
of the Web page under Services. Further information about this process is available in thewhich permission is being requested is located, click Request Permissions in the middle columnClearance Center, not the Editorial Office. Once the online version of the published article for
can be obtained via RightsLink, a service of the CopyrightCirculationoriginally published in Requests for permissions to reproduce figures, tables, or portions of articlesPermissions:
by guest on June 30, 2018http://circ.ahajournals.org/
Dow
nloaded from