Embed Size (px)
Citation preview
8/3/2019 Electrocardiogram Differentiation of Benign Early Re Polarization Versus Acute Myocardial Infarction by Emergency P…
http://slidepdf.com/reader/full/electrocardiogram-differentiation-of-benign-early-re-polarization-versus-acute 1/6
Electrocardiogram Differentiation of BenignEarly Repolarization Versus Acute MyocardialInfarction by Emergency Physicians and
CardiologistsSamuel D. Turnipseed, MD, Aaron E. Bair, MD, J. Douglas Kirk, MD, Deborah B. Diercks, MD,
Poroshat Tabar, DO, Ezra A. Amsterdam, MD
Abstract
Objectives: ST-segment elevation (STE) related to benign early repolarization (BER), a common normal
variant, can be difficult to distinguish from acute myocardial infarction (AMI). The authors compared the
electrocardiogram (ECG) interpretations of these two entities by emergency physicians (EPs) and cardiol-
ogists.
Methods: Twenty-five cases (13 BER, 12 AMI) of patients presenting to the emergency department with
chest pain were identified. Criteria for BER required four of the following: 1) widespread STE (precordialgreater than limb leads), 2) J-point elevation, 3) concavity of initial up-sloping portion of ST segment, 4)
notching or irregular contour of J point, and 5) prominent, concordant T waves. Additional BER criteria
were 1) stable ECG pattern, 2) negative cardiac injury markers, and 3) normal cardiac stress test or angi-
ography. AMI criteria were 1) regional STE, 2) positive cardiac injury markers, and 3) identification of cul-
prit coronary artery by angiography in less than eight hours of presentation. The 25 ECGs were distributed
to 12 EPs and 12 cardiologists (four in academic medicine, four in community practice, and four in commu-
nity academics [health maintenance organization] in each physician group). The physicians were informed
of the patients’ age, gender, and race, and they then interpreted the ECGs as BER or AMI. Undercalls (AMI
misdiagnosed as BER) and overcalls (BER misdiagnosed as AMI) were calculated for each physician group.
Results: Cardiologists correctly interpreted 90% of ECGs, and EPs correctly interpreted 81% of ECGs. The
proportion of undercalls (missed AMI/total AMI) was 2.8% for cardiologists (95% confidence interval [CI] =
0.09% to 5.5%) compared with 9.7% for EPs (95% CI = 4.8% to 14.6%) (p = 0.02). The proportion of overcalls
(missed BER/total BER) was 17.3% for cardiologists (95% CI = 11.4% to 23.3%) versus 27.6% for EPs (95%
CI = 20.6% to 34.6%) (p = 0.03). The mean number of years in practice was 19.8 for cardiologists (95% CI =19 to 20.5) and 11 years for EPs (95% CI = 10.5 to 12.0) (p < 0.001).
Conclusions: Although correct interpretation was high in both groups, cardiologists, who had significantly
more years of practice, had fewer misinterpretations than EPs in distinguishing BER from AMI electrocar-
diographically.
ACADEMIC EMERGENCY MEDICINE 2006; 13:961–967 ª 2006 by the Society for Academic Emergency
Medicine
Keywords: benign early repolarization, acute myocardial infarction, electrocardiogram
The proven benefit of urgent coronary reperfusion
for patients with acute myocardial infarction (AMI)
necessitates rapid recognition of ST-segment ele-
vation myocardial infarction (STEMI) by emergency phy-
sicians (EP). However, AMI is the etiology of ST-segment
elevation (STE) in a minority of patients presenting with
chest pain.1,2 Among the multiple causes of noninfarc-
tion electrocardiographic (ECG) patterns that may mimic
STEMI are benign early repolarization (BER), left bun-
dle branch block, left ventricular aneurysm, left ven-
tricular hypertrophy, paced ventricular rhythms, and
From the Department of Emergency Medicine (SDT, AEB, JDK,
DBD, PT) and Department of Internal Medicine, Division of Car-
diovascular Medicine (EAA), University of California, Davis,
Medical Center, Sacramento, CA.
Received November 3, 2005; revisions received January 24, 2006,
and March 4, 2006; accepted April 8, 2006.
Address for correspondence and reprints: Samuel D. Turnip-
seed, MD, Department of Emergency Medicine, University of
California, Davis, Medical Center, 4150 V Street, Suite 2100, Sac-
ramento, CA 95817. Fax: 916-734-7950; e-mail: sdturnipseed@
ucdavis.edu.
ª 2006 by the Society for Academic Emergency Medicine ISSN 1069-6563
doi: 10.1197/j.aem.2006.04.014 PII ISSN 1069-6563583 961
8/3/2019 Electrocardiogram Differentiation of Benign Early Re Polarization Versus Acute Myocardial Infarction by Emergency P…
http://slidepdf.com/reader/full/electrocardiogram-differentiation-of-benign-early-re-polarization-versus-acute 2/6
pericarditis. The potential for these conditions to be con-
fused with STEMI is reflected in the report of Sharkey
et al., in which 11% of patients receiving a thrombolytic
agent were subsequently found not to have AMI.3
Benign early repolarization, a normal variant, is a rela-
tively frequent ECG finding and can be particularly diffi-
cult to distinguish from AMI in patients presenting to the
emergency department (ED) with chest pain. It is foundin approximately 1% of the population; the majority of
these individuals are younger than 50 years of age and
are rarely older than 70 years.4 African American men
between the ages of 20 and 40 years comprise a large
proportion of this group.5,6 In patients presenting to
the ED with STE, Brady et al. found that BER was almost
as common as AMI (15% vs. 13%).1 In the report by Shar-
key et al. citing an 11% frequency of erroneous adminis-
tration of a thrombolytic agent, almost one third of
patients without AMI had BER.3
It is essential to recognize BER to avoid subjecting pa-
tients to unnecessary medications or procedures. The
risks of thrombolytic therapy include an 8% rate of major
bleeding, of which 1%–2% are intracerebral hemor-
rhages usually resulting in devastating stroke.7 Unneces-
sary emergency percutaneous coronary intervention is
also associated with an unfavorable risk/benefit profile.
On the other hand, misinterpretation of AMI as BER de-
prives patients of potential lifesaving therapy. Because of
the continuing challenge of distinguishing BER from
STEMI, we compared the ECG interpretations of these
two entities by EPs and cardiologists.
METHODS
Study Design
This was a retrospective study that compared ECG inter-
pretations by EPs and cardiologists in terms of AMI vs.
BER. The study was approved by our institutional review
board.
Study Setting and Population
The initial ECGs of each patient were distributed to 12
EPs and 12 cardiologists who were blinded to the final
diagnosis. To achieve diversity among the ECG readers,
we chose physicians from three unique practice environ-
ments. Of these 12 physicians in each of the two groups,
four in each group practiced at our academic training
center, four practiced at a large local health maintenance
organization (teaching) community hospital, and four
were in community practice. All cardiologists involved
in the study routinely evaluated and admitted patients
from the ED. The number of years practiced after com-
pletion of training was recorded for each physician.
Study Protocol
We selected 25 ECGs of patients who had presented to
the ED with the chief complaint of chest pain and who
had complete cardiac evaluations. The ECGs included
13 with BER and 12 with STEMI. BER ECGs were chosen
from our Chest Pain Evaluation Unit database under the
heading ‘‘ECG Interpretation: BER.’’ Criteria for BER
have been previously established8 and are listed in Table
1. In our study, the diagnosis of BER required four of the
five criteria (Figure 1). Additional criteria of BER used in
this study included the following: 1) ECGs demonstrated
a stable pattern, 2) patients had at least three consecutivenegative cardiac injury markers (creatine phosphoki-
nase-MB and/or troponin I), and 3) patients had a normal
noninvasive cardiac stress test or normal coronary angi-
ography. STEMI ECGs were chosen from a computer-
generated list using the International Classification of
Disease billing code for AMI. The criteria for AMI were
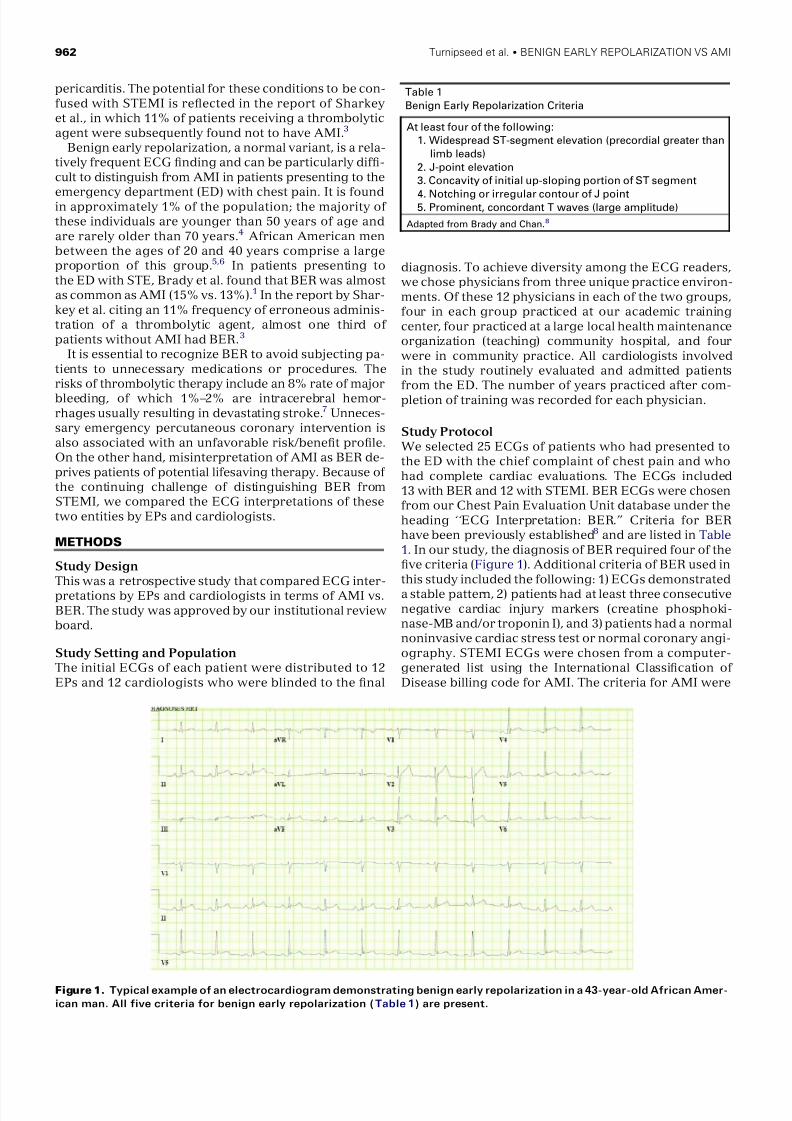
Table 1
Benign Early Repolarization Criteria
At least four of the following:
1. Widespread ST-segment elevation (precordial greater than
limb leads)
2. J-point elevation
3. Concavity of initial up-sloping portion of ST segment
4. Notching or irregular contour of J point5. Prominent, concordant T waves (large amplitude)
Adapted from Brady and Chan.8
Figure 1. Typical example of an electrocardiogram demonstrating benign early repolarization in a 43-year-old African Amer-
ican man. All five criteria for benign early repolarization (Table 1) are present.
962 Turnipseed et al. BENIGN EARLY REPOLARIZATION VS AMI
8/3/2019 Electrocardiogram Differentiation of Benign Early Re Polarization Versus Acute Myocardial Infarction by Emergency P…
http://slidepdf.com/reader/full/electrocardiogram-differentiation-of-benign-early-re-polarization-versus-acute 3/6
as follows: 1) regional STE, 2) positive serial cardiac in-
jury markers, and 3) coronary angiography within eight
hours of the patient’s arrival in the ED that identified
the culprit vessel.
Chest pain was the chief complaint in all 25 cases. ECG
readers were informed of the age, gender, and race of the
patient for each ECG. No other clinical data were pro-
vided.Readers were askedto interpret each ECG as eitherBER or AMI. It was also clearly stated that if STEMI was
selected, the reader should assume the patient would
receive thrombolytic therapy, not intervention in a cathe-
terization laboratory. ECG interpretations were then col-
lected by a single researcher. Physician interpretations
were classified as correct, undercall, and overcall. Under-
calls were defined as AMI misdiagnosed as BER, and
overcalls were defined as BER misdiagnosed as AMI.
Data Analysis
Physician groups’ continuous data were expressed us-
ing mean or median and then were compared using
Student’s t-test where appropriate. Proportion and
frequency data related to ECG interpretations were
compared using Fisher’s exact test. To account for clus-
tering of repeated measures, a generalized linear model
was used for linear regression analysis. When appropri-
ate, 95% confidence intervals (CIs) are presented. All
tests were based on two-tailed alternatives. We per-
formed the statistical analyses using Stata 7.0 (Stata
Corp., College Station, TX) for Windows (Microsoft
Corp., Redmond, WA).
RESULTS
The number of interpretations for each specialty group
was calculated by multiplying the number of physiciansin each group ( n = 12) by the number of ECGs ( n = 25),
yielding a total of 300 interpretations for each group.
The cardiologists correctly interpreted 90% (269/300;
95% CI = 86% to 93%) of the ECGs, and the EPs’ inter-
pretations were correct in 81% (243/300; 95% CI = 76%
to 85%) of cases (Table 2). The average number of correct
interpretations for the individual cardiologists was 22
(range, 20–24) and for each EP was 20 (range, 15–23).
The proportion of undercalls (AMI misdiagnosed as
BER) was different between specialty groups. Overall,
the proportion of undercalls (missed AMI/total AMI)
was 2.8% for cardiologists (95% CI = 0.09% to 5.5%)
compared with 9.7% for EPs (95% CI = 4.8% to 14.6%)
(p = 0.02). The proportion of overcalls (BER misdiag-
nosed as AMI) was also different between specialty
groups. The proportion of overcalls (missed BER/total
BER) was 17.3% for cardiologists (95% CI = 11.4% to
23.3%) versus 27.6% for EPs (95% CI = 20.6% to 34.6%)
(p = 0.03). The percentage of correct ECG interpretations
by specialty and type of ECG is shown in Table 3. A com-
monly missed BER ECG is shown in Figure 2, and a
commonly missed AMI ECG is shown in Figure 3.There was a disparity of years in practice between spe-
cialty groups. Among the cardiology group, the mean
number of years in practice was 19.8 (95% CI = 19 to
Table 2
Cardiologist and Emergency Physician Interpretations
Cardiologists
Emergency
Physicians
p-
value
Total correct ECGs 90% (269/300) 81% (243/300)
Average no. correct
ECGs per physician
22 20
Proportion undercalls 2.8% (4/144) 9.7% (14/144) 0.02Proportion overcalls 17.3% (27/156) 27.6% (43/156) 0.03
Average years
practiced
19.8 11.0 <0.001
Undercalls = acute myocardial infarction misdiagnosed as benign early
repolarization; overcalls = benign early repolarization misdiagnosed as
acute myocardial infarction.
Table 3
Percentage of Correct ECG Interpretations by Physician Specialty and Type of ECG
Condition ECG No.
Patient
Age (yr)
Patient
Gender
Patient
Race
% Emergency Physicians
Correct (n = 12)
% Cardiologists
Correct (n = 12)
BER 1 54 Male African American 58 92
BER 3 52 Male African American 83 50
BER 5 56 Female African American 66 75
BER 6 60 Male African American 75 58BER 12 41 Male White 75 50
BER 14 46 Male African American 58 58
BER 18 49 Male African American 75 100
BER 19 46 Male African American 75 100
BER 22 57 Male White 66 92
BER 23 36 Male African American 100 92
BER 25 43 Male African American 50 75
AMI 4 52 Male White 92 100
AMI 7 71 Male White 75 92
AMI 8 55 Male Hispanic 83 92
AMI 13 52 Male Hispanic 92 100
AMI 15 38 Male White 92 100
AMI 17 42 Male White 92 100
AMI 20 67 Male White 66 83
All ECGs that were correctly interpreted by all physicians of both groups were excluded from the table.
BER = benign early repolarization; AMI = acute myocardial infarction.
ACAD EMERG MED September 2006, Vol. 13, No. 9 www.aemj.org 963
8/3/2019 Electrocardiogram Differentiation of Benign Early Re Polarization Versus Acute Myocardial Infarction by Emergency P…
http://slidepdf.com/reader/full/electrocardiogram-differentiation-of-benign-early-re-polarization-versus-acute 4/6
20.5). The EPs, however, had only been in practice for a
mean of 11 years (95% CI = 10.5 to 12.0) (p < 0.001).
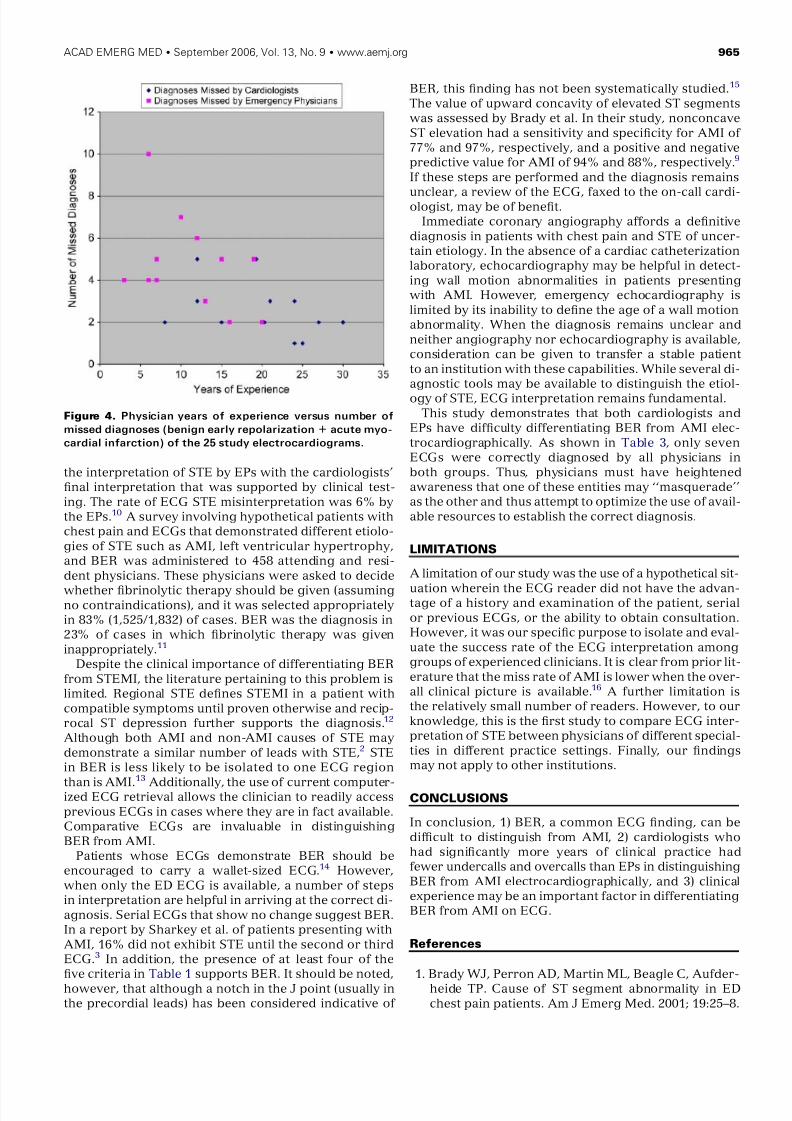
ECG misdiagnoses (both overcalls and undercalls) corre-
lated inversely with years in practice for all 24 physicians
considered as a single group (Figure 4). Among misdiag-
nosed ECGs (overcalls and undercalls in both physician
groups), the mean number of years in practice was 13
(95% CI = 12 to 15). In contrast, the mean number of years
of practice reported among those who correctly
diagnosed the ECGswas16 (95%CI = 15to 16.5) (p= 0.001).
After adjusting for covariates (specialty training, years
in practice, practice location, and diagnosis) and cluster-
ing of physician responses, the most significant variable
contributing to a correct diagnosis was the presence of AMI (b coefficient, 0.16; 95% CI = 0.08 to 0.24; p < 0.001).
DISCUSSION
Our study demonstrates the difficulty in differentiating
BER from STEMI. The range of correct answers for the
25 ECGs among the cardiologists and EPs was 15–24.
The cardiologists had fewer undercalls and overcalls
compared with the EPs. However, the cardiologists had
also practiced significantly longer than the EPs. It is note-
worthy that after adjusting for covariates (specialty train-
ing, years in practice, practice location, and diagnosis)
and clustering of physician responses, the most signifi-
cant variable associated with a correct diagnosis was
the presence of AMI. This finding suggests that BER
and STEMI can be distinguished electrocardiographi-
cally in a majority of patients by experienced clinicians
but that frequent errors of overcalls and undercalls will
still unavoidably exist.
Benign early repolarization is a ‘‘pseudoinfarction’’ECG pattern frequently encountered in the ED. Of 171
patients presenting to an ED with STE, Brady et al. found
that BER was the cause in 12%.9 This finding has been as-
sociated with inappropriate administration of fibrinolytic
therapy to patients with BER.3 In patients admitted to the
hospital with ECG findings of STE, Brady et al. compared
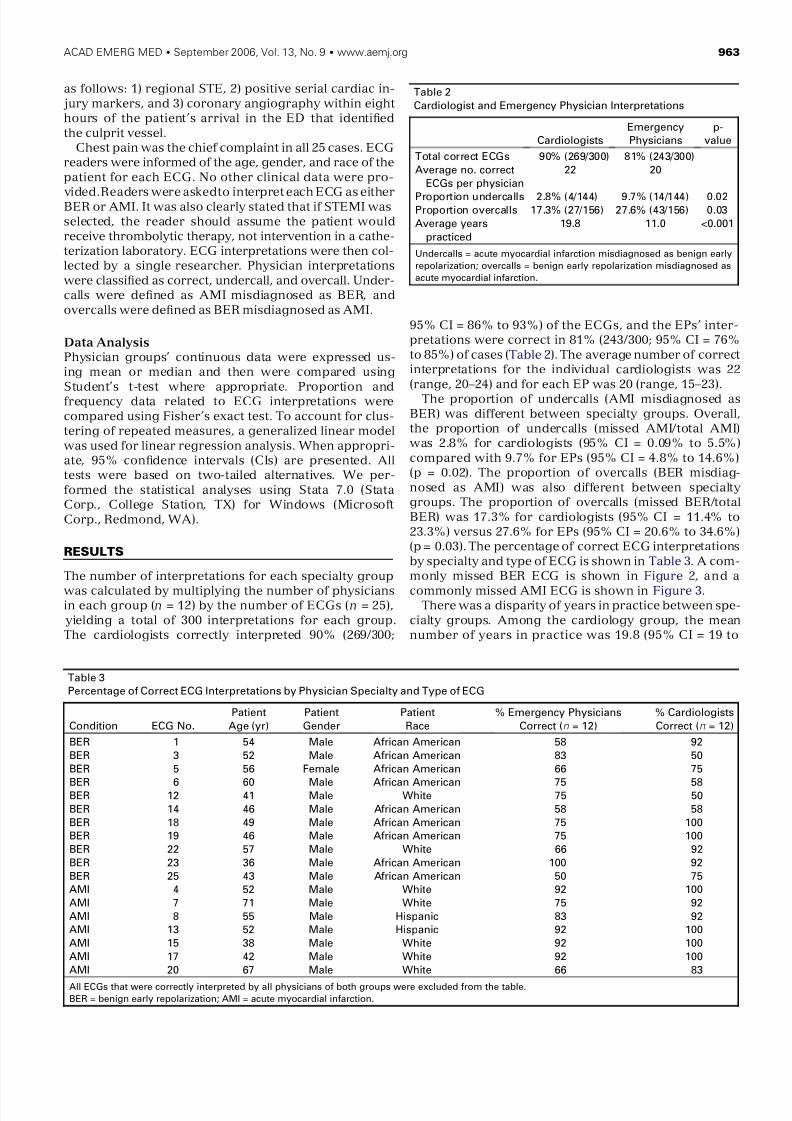
Figure 2. A commonly misdiagnosed electrocardiogram with benign early repolarization. The incorrect diagnosis of acute
myocardial infarction was made by 38% of all physician readers in the study.
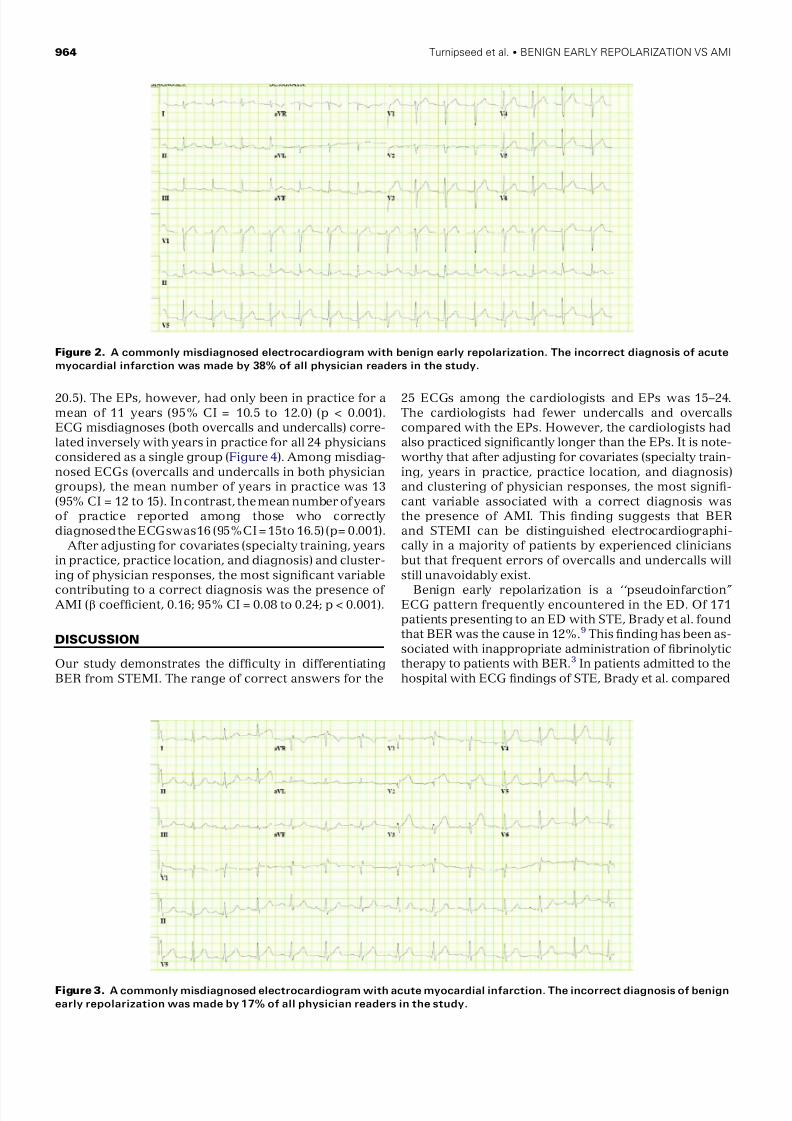
Figure 3. A commonly misdiagnosed electrocardiogram with acute myocardial infarction. The incorrect diagnosis of benign
early repolarization was made by 17% of all physician readers in the study.
964 Turnipseed et al. BENIGN EARLY REPOLARIZATION VS AMI
8/3/2019 Electrocardiogram Differentiation of Benign Early Re Polarization Versus Acute Myocardial Infarction by Emergency P…
http://slidepdf.com/reader/full/electrocardiogram-differentiation-of-benign-early-re-polarization-versus-acute 5/6
the interpretation of STE by EPs with the cardiologists’
final interpretation that was supported by clinical test-
ing. The rate of ECG STE misinterpretation was 6% by
the EPs.10 A survey involving hypothetical patients with
chest pain and ECGs that demonstrated different etiolo-
gies of STE such as AMI, left ventricular hypertrophy,
and BER was administered to 458 attending and resi-
dent physicians. These physicians were asked to decide
whether fibrinolytic therapy should be given (assumingno contraindications), and it was selected appropriately
in 83% (1,525/1,832) of cases. BER was the diagnosis in
23% of cases in which fibrinolytic therapy was given
inappropriately.11
Despite the clinical importance of differentiating BER
from STEMI, the literature pertaining to this problem is
limited. Regional STE defines STEMI in a patient with
compatible symptoms until proven otherwise and recip-
rocal ST depression further supports the diagnosis.12
Although both AMI and non-AMI causes of STE may
demonstrate a similar number of leads with STE,2 STE
in BER is less likely to be isolated to one ECG region
than is AMI.
13
Additionally, the use of current computer-ized ECG retrieval allows the clinician to readily access
previous ECGs in cases where they are in fact available.
Comparative ECGs are invaluable in distinguishing
BER from AMI.
Patients whose ECGs demonstrate BER should be
encouraged to carry a wallet-sized ECG.14 However,
when only the ED ECG is available, a number of steps
in interpretation are helpful in arriving at the correct di-
agnosis. Serial ECGs that show no change suggest BER.
In a report by Sharkey et al. of patients presenting with
AMI, 16% did not exhibit STE until the second or third
ECG.3 In addition, the presence of at least four of the
five criteria in Table 1 supports BER. It should be noted,
however, that although a notch in the J point (usually in
the precordial leads) has been considered indicative of
BER, this finding has not been systematically studied.15
The value of upward concavity of elevated ST segments
was assessed by Brady et al. In their study, nonconcave
ST elevation had a sensitivity and specificity for AMI of
77% and 97%, respectively, and a positive and negativ e
predictive value for AMI of 94% and 88%, respectively.9
If these steps are performed and the diagnosis remains
unclear, a review of the ECG, faxed to the on-call cardi-ologist, may be of benefit.
Immediate coronary angiography affords a definitive
diagnosis in patients with chest pain and STE of uncer-
tain etiology. In the absence of a cardiac catheterization
laboratory, echocardiography may be helpful in detect-
ing wall motion abnormalities in patients presenting
with AMI. However, emergency echocardiography is
limited by its inability to define the age of a wall motion
abnormality. When the diagnosis remains unclear and
neither angiography nor echocardiography is available,
consideration can be given to transfer a stable patient
to an institution with these capabilities. While several di-
agnostic tools may be available to distinguish the etiol-
ogy of STE, ECG interpretation remains fundamental.
This study demonstrates that both cardiologists and
EPs have difficulty differentiating BER from AMI elec-
trocardiographically. As shown in Table 3, only seven
ECGs were correctly diagnosed by all physicians in
both groups. Thus, physicians must have heightened
awareness that one of these entities may ‘‘masquerade’’
as the other and thus attempt to optimize the use of avail-
able resources to establish the correct diagnosis.
LIMITATIONS
A limitation of our study was the use of a hypothetical sit-
uation wherein the ECG reader did not have the advan-tage of a history and examination of the patient, serial
or previous ECGs, or the ability to obtain consultation.
However, it was our specific purpose to isolate and eval-
uate the success rate of the ECG interpretation among
groups of experienced clinicians. It is clear from prior lit-
erature that the miss rate of AMI is lower when the over-
all clinical picture is available.16 A further limitation is
the relatively small number of readers. However, to our
knowledge, this is the first study to compare ECG inter-
pretation of STE between physicians of different special-
ties in different practice settings. Finally, our findings
may not apply to other institutions.
CONCLUSIONS
In conclusion, 1) BER, a common ECG finding, can be
difficult to distinguish from AMI, 2) cardiologists who
had significantly more years of clinical practice had
fewer undercalls and overcalls than EPs in distinguishing
BER from AMI electrocardiographically, and 3) clinical
experience may be an important factor in differentiating
BER from AMI on ECG.
References
1. Brady WJ, Perron AD, Martin ML, Beagle C, Aufder-
heide TP. Cause of ST segment abnormality in ED
chest pain patients. Am J Emerg Med. 2001; 19:25–8.
Figure 4. Physician years of experience versus number of
missed diagnoses (benign early repolarization + acute myo-
cardial infarction) of the 25 study electrocardiograms.
ACAD EMERG MED September 2006, Vol. 13, No. 9 www.aemj.org 965

8/3/2019 Electrocardiogram Differentiation of Benign Early Re Polarization Versus Acute Myocardial Infarction by Emergency P…
http://slidepdf.com/reader/full/electrocardiogram-differentiation-of-benign-early-re-polarization-versus-acute 6/6
2. Brady WJ, Perron AD, Ullman EA, et al. Electrocar-
diographic ST segment elevation: a comparison of
AMI and non-AMI ECG syndromes. Am J Emerg
Med. 2002; 20:609–12.
3. Sharkey SW, Berger CR, Brunette DD, Henry TD.
Impact of the electrocardiogram on the delivery of
thrombolytic therapy for acute myocardial infarction.
Am J Cardiol. 1994; 73:550–3.4. Mehta MC, Jain AC. Early repolarization on scalar
electrocardiogram. Am J Med Sci. 1995; 309:
305–11.
5. Thomas J, Harris E, Lassiter G. Observations on the
T wave and S-T segment changes in the precordial
electrocardiogram of 320 young Negro adults. Am J
Cardiol. 1960; 5:468–74.
6. Klatsky AL, Oehm R, Cooper RA, Udaltsova N, Arm-
strong MA. The early repolarization normal variant
electrocardiogram: correlates and consequences.
Am J Med. 2003; 115:171–7.
7. Weaver WD, Simes RJ, Betriu A, et al. Comparison of
primary coronary angioplasty and intravenous throm-
bolytic therapy for acute myocardial infarction. JAMA.
1997; 278:2093–8.
8. Brady WJ, Chan TC. Electrocardiographic manifes-
tations: benign early repolarization. J Emerg Med.
1999; 17:473–8.
9. Brady WJ, Syverud SA, Beagle C, et al. Electrocardio-
graphic ST-segment elevation: the diagnosis of acute
myocardial infarction by morphologic analysis of the
ST segment. Acad Emerg Med. 2001; 8:961–7.
10. Brady WJ, Perron A, Ullman E. Errors in emergency
physician interpretation of ST-segment elevation in
emergency department chest pain patients. Acad
Emerg Med. 2000; 7:1256–60.
11. Brady WJ, Perron AD, Chan T. Electrocardiographic
ST-segment elevation: correct identification of acutemyocardial infarction (AMI) and non-AMI syndromes
by emergency physicians. Acad Emerg Med. 2001; 8:
349–60.
12. Brady WJ, Peron AD, Syverud SA, et al. Reciprocal
ST segment depression: impact on the electrocardio-
graphic diagnosis of ST segment elevation acute my-
ocardial infarction. Am J Emerg Med. 2002; 20:35–8.
13. Brady WJ. Benign early repolarization: electrocardio-
graphic manifestations and differentiation from other
ST segment elevation syndromes. Am J Emerg Med.
1998; 16:592–7.
14. Smith SW. ST-elevation acute myocardial infarction:
a critical but difficult electrocardiographic diagnosis.
Acad Emerg Med. 2001; 8:382–5.
15. Mehta M, Jain AC, Mehta A. Early repolarization.
Clin Cardiol Rev. 1999; 22(2):59–65.
16. McCarthy BD, Beshansky JR, D’Agostino RB, Selker
HP. Missed diagnoses of acute myocardial infarction
in the emergency department: results from a multi-
center study. Ann Emerg Med. 1993; 22:579–82.
Please see accompanying video Data Supplement available at www.aemj.org .
Colles Fracture Reduction Using Ultrasound
Case: A 28-year-old intoxicated woman presented to the emer-
gency department with right wrist pain and deformity after a
fall during an altercation. We confirmed a Colles fracture with
x-rays (Figure 1). The fracture was also visualized using a 7.5-
MHz ultrasound probe (Figure 2). After adequate sedation, the
fracture was reduced and visualized at the bedside using ultra-
sound, which revealed persistent, slight malalignment (Figure 3).
Further reduction and utilization of repeat ultrasound visuali-zation efficiently achieved optimal alignment (Figure 4), which
was confirmed by standard post-reduction x-rays (Figure 5).
The four-minute video available as a Data Supplement ( http://
www.aemj.org/cgi/content/full/j.aem.2006.07.013/DC1) explains
in detail the use of ultrasound during Colles fracture reduction.
Nate Unkefer, MD
Scott Joing, MD
Rob Reardon, MD
Hennepin County Medical Center
Minneapolis, MN
Figure 1. X-ray showing the initial diagnosis of the Colles
fracture.
966 Turnipseed et al. BENIGN EARLY REPOLARIZATION VS AMI