Embed Size (px)
Citation preview
J. clin. Path. (1957), 10, 46.
THE HISTOLOGICAL APPEARANCES OF CHONDRO-DERMATITIS CHRONICA HELICIS
BY
E. M. McCONNELLFrom the Department of Pathology, Liverpool Radium Institute, Liverpool
(RECEIVED FOR PUBLICATION DECEMBER 21, 1955)
Winkler (1915) described eight cases of a small,painful benign growth, occurring on or near theupper part of the free border of the helix of theauricle and suggested the name " chondroderma-titis nodularis chronica helicis" for the condition.Shortly afterwards Foerster (1917) described fourcases of a similar condition under the name of'; painful nodular growth of the ear." Furtherexamples of the condition have since been reportedby several authors.The condition usually occurs in adult males,
commonly over the age of 50 years. The patientscomplain of a small painful lump on the upper part
of the free border of one ear, usually of severalmonths' duration. The pain is aggravated if thepatient lies on the affected side, and is comparedwith the " darting" or " knife-like " pain of a corn.
There is rarely any history of bleeding or dischargefrom the lesion. On examination there is a small(usually 4-6 mm. diameter), firm, well-definedpinkish nodule, on or near the free border of theupper part of the helix, and usually immovable on
the underlying cartilage. The centre of the lesionis covered with a crust-like scale, removal ofwhich reveals a cup-shaped depression with a firmbase. Removal of the scale may be accompaniedby temporary relief of the pain.There is less agreement as to the aetio-pathology
of the condition, and the following study was
undertaken in an effort to clarify the position.Before it was completed Shuman and Helwig(1954) published in America a series of cases fromthe files of the American Armed Forces Institute ofPathology which have added considerably to theunderstanding of the condition.
Winkler considers the primary aetiological agentto be a degenerative change in the auricular car-
tilage with subsequent infection and chronicinflammatory changes. The degenerated cartilageacts as a foreign body and maintains the inflam-matory stimulus and a reactive hyperplasia occurs
in the overlying epithelium. Foerster supports thisview and considers that the anatomical peculiarities
and variation in form which occur in the scapha-helix may help to explain the location of the lesion.Ebenius (1941) considers that there are probablyseveral aetiological factors including trauma, cir-culatory disturbances, and abnormalities of theauricular skin. Carol and van Haren (1941), fromtheir study of serial sections from eight cases ofchondrodermatitis, believe the condition to be dueto a primary epithelial change, resulting in the for-mation of a clavus, pressure from which causesepithelial ulceration and necrosis of the underlyingcorium and in some instances of the cartilage also.Shuman and Helwig consider that several factors,including developmental abnormalities, poor bloodsupply, and trauma, are concerned in the aetiologyof the condition.
MaterialThe present study is based on the examination
of serial sections from 12 cases of chondroderma-titis chronica helicis excised at the LiverpoolRadium Institute during a five-year period. Thepatients were all men, the youngest of whom was40 years of age, and the duration of the conditionvaried between one month and six years.
Histological AppearancesAll of the specimens show characteristic histo-
logical features in the epithelium, connective tissue,and perichondrium. The duration of the lesiondoes not appear to alter these characteristic appear-ances.At the edge of the lesion there is a relatively
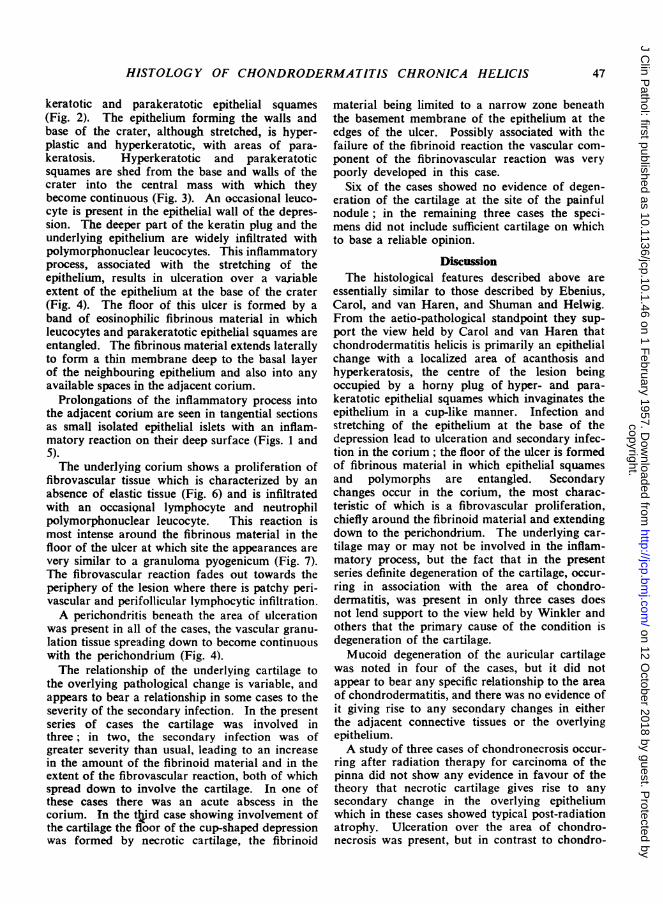
abrupt change from the normal epithelium toepithelium showing acanthosis, with irregularbroadening and deepening of the rete pegs andhyperkeratosis associated also with keratoticplugging of the follicles (Fig. 1). This epithelialhyperplasia may be so marked as to suggest anearly malignant change, particularly if seen intangential sections. In the central 1-2 mm. theepithelium is invaginated in a crater-like mannerby a keratinous plug composed chiefly of hyper-
copyright. on 12 O
ctober 2018 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.10.1.46 on 1 F
ebruary 1957. Dow
nloaded from
HISTOLOGY OF CHONDRODERMATITIS CHRONICA HELICIS
keratotic and parakeratotic epithelial squames(Fig. 2). The epithelium forming the walls andbase of the crater, although stretched, is hyper-plastic and hyperkeratotic, with areas of para-keratosis. Hyperkeratotic and parakeratoticsquames are shed from the base and walls of thecrater into the central mass with which theybecome continuous (Fig. 3). An occasional leuco-cyte is present in the epithelial wall of the depres-sion. The deeper part of the keratin plug and theunderlying epithelium are widely infiltrated withpolymorphonuclear leucocytes. This inflammatoryprocess, associated with the stretching of theepithelium, results in ulceration over a variableextent of the epithelium at the base of the crater(Fig. 4). The floor of this ulcer is formed by aband of eosinophilic fibrinous material in whichleucocytes and parakeratotic epithelial squames areentangled. The fibrinous material extends laterallyto form a thin membrane deep to the basal layerof the neighbouring epithelium and also into anyavailable spaces in the adjacent corium.
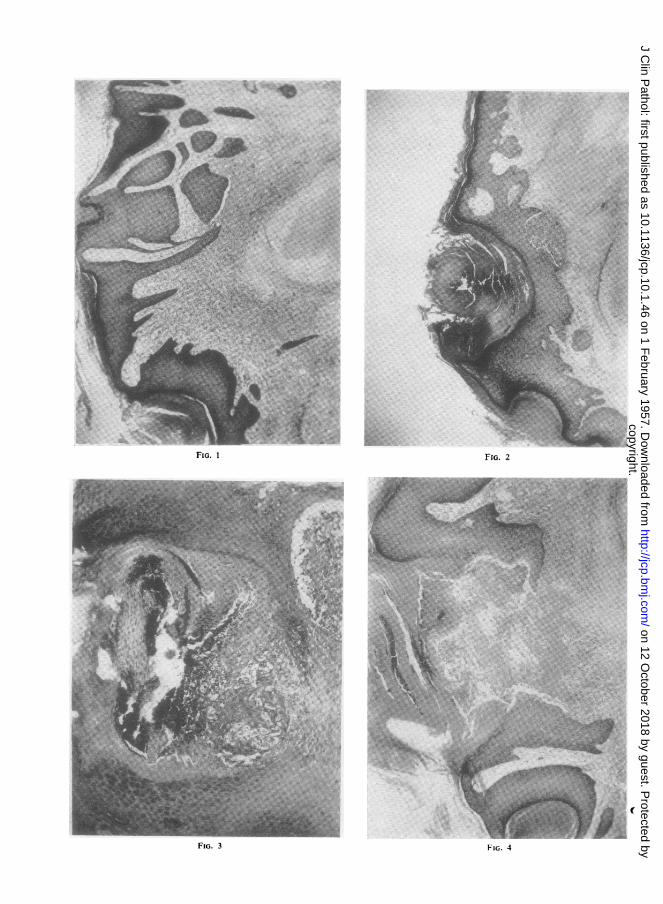
Prolongations of the inflammatory process intothe adjacent corium are seen in tangential sectionsas small isolated epithelial islets with an inflam-matory reaction on their deep surface (Figs. 1 and5).The underlying corium shows a proliferation of
fibrovascular tissue which is characterized by anabsence of elastic tissue (Fig. 6) and is infiltratedwith an occasional lymphocyte and neutrophilpolymorphonuclear leucocyte. This reaction ismost intense around the fibrinous material in thefloor of the ulcer at which site the appearances arevery similar to a granuloma pyogenicum (Fig. 7).The fibrovascular reaction fades out towards theperiphery of the lesion where there is patchy peri-vascular and perifollicular lymphocytic infiltration.A perichondritis beneath the area of ulceration
was present in all of the cases, the vascular granu-lation tissue spreading down to become continuouswith the perichondrium (Fig. 4).The relationship of the underlying cartilage to
the overlying pathological change is variable, andappears to bear a relationship in some cases to theseverity of the secondary infection. In the presentseries of cases the cartilage was involved inthree; in two, the secondary infection was ofgreater severity than usual, leading to an increasein the amount of the fibrinoid material and in theextent of the fibrovascular reaction, both of whichspread down to involve the cartilage. In one ofthese cases there was an acute abscess in thecorium. In the third case showing involvement ofthe cartilage the floor of the cup-shaped depressionwas formed by necrotic cartilage, the fibrinoid
material being limited to a narrow zone beneaththe basement membrane of the epithelium at theedges of the ulcer. Possibly associated with thefailure of the fibrinoid reaction the vascular com-ponent of the fibrinovascular reaction was verypoorly developed in this case.
Six of the cases showed no evidence of degen-eration of the cartilage at the site of the painfulnodule; in the remaining three cases the speci-mens did not include sufficient cartilage on whichto base a reliable opinion.
DiscussionThe histological features described above are
essentially similar to those described by Ebenius,Carol, and van Haren, and Shuman and Helwig.From the aetio-pathological standpoint they sup-port the view held by Carol and van Haren thatchondrodermatitis helicis is primarily an epithelialchange with a localized area of acanthosis andhyperkeratosis, the centre of the lesion beingoccupied by a horny plug of hyper- and para-keratotic epithelial squames which invaginates theepithelium in a cup-like manner. Infection andstretching of the epithelium at the base of thedepression lead to ulceration and secondary infec-tion in the corium; the floor of the ulcer is formedof fibrinous material in which epithelial squamesand polymorphs are entangled. Secondarychanges occur in the corium, the most charac-teristic of which is a fibrovascular proliferation,chiefly around the fibrinoid material and extendingdown to the perichondrium. The underlying car-tilage may or may not be involved in the inflam-matory process, but the fact that in the presentseries definite degeneration of the cartilage, occur-ring in association with the area of chondro-dermatitis, was present in only three cases doesnot lend support to the view held by Winkler andothers that the primary cause of the condition isdegeneration of the cartilage.Mucoid degeneration of the auricular cartilage
was noted in four of the cases, but it did notappear to bear any specific relationship to the areaof chondrodermatitis, and there was no evidence ofit giving rise to any secondary changes in eitherthe adjacent connective tissues or the overlyingepithelium.A study of three cases of chondronecrosis occur-
ring after radiation therapy for carcinoma of thepinna did not show any evidence in favour of thetheory that necrotic cartilage gives rise to anysecondary change in the overlying epitheliumwhich in these cases showed typical post-radiationatrophy. Ulceration over the area of chondro-necrosis was present, but in contrast to chondro-
47
copyright. on 12 O
ctober 2018 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.10.1.46 on 1 F
ebruary 1957. Dow
nloaded from
Vp,-
&A
FIG. 1
FIG. 3
FIG. 2
FIG. 4
copyright. on 12 O
ctober 2018 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.10.1.46 on 1 F
ebruary 1957. Dow
nloaded from
FIG. 5
FIG. 1.-Tangential section from the edge of the lesion showingacanthosis, hyperkeratosis and parakeratosis associated with afibrovascular reaction in the corium which is spreading down tobecome continuous with the perichondrium (x 40).
FIG. 2.-Tangential section taken from nearer the centre of the lesionshowing the " crater-like " invagination of the epithelium by thekeratin plug and a subepithelial focus of infection. (Post-radiation specimen, x 40.)
FIG. 3.-Detailed structure of the keratin plug, with parakeratoticsquames at the surface (left side of photograph) and degeneratedand infected squames at the base (x 100).
FIG. 4.-Mid-line section, showing ulceration of the epithelium at thebase of the crater; the ulcer floor is formed by hyaline fibrinousmaterial and is covered by the keratin plug (x 40).
FIG. 5.-Peripheral extension of acute infection and fibrinoid produc-tion beneath the basement membrane ofan epithelial downgrowth.(Same slide as Fig. 1, x 100.)
FIG. 6.-Characteristic fibrovascular reaction with absence of elastictissue. In this section the fibrovascular tissue is invading theelastic auricular cartilage. (Moore's elastic tissue stain, x 40.)
FIG. 7.-Fibrovascular tissue adjacent to the area of ulceration(x 400).
E riu. I
copyright. on 12 O
ctober 2018 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.10.1.46 on 1 F
ebruary 1957. Dow
nloaded from

E. M. McCONNELL
dermatitis helicis the ulcer was at the surface andnot at the base of a cup-shaped invagination, andthe horny plug and fibrovascular tissue were
absent, the granulation tissue forming the ulcerfloor being less va .ular and containing elasticfibrils.
It may be argued that the radiation had pre-
vented the normal tissue response to the presence
of degenerative cartilage. That this is not so is
suggested by the fact that the typical epithelialchanges of chondrodermatitis helicis were stillpresent in two patients in this series who had beentreated by radiotherapy before surgical excision.The presence of secondary infection may alter
the characteristic histological appearances ofchondrodermatitis chronica helicis by causing
more widespread tissue involvement, includingabscess formation in the corium and destructionof the cartilage; this may give rise to an erroneous
conception of the pathology of the condition.There is still no convincing evidence as to what
initiates the pathological change in chondro-dermatitis chronica helicis, nor its peculiar loca-
tion and predominance in males. The hi ologicalsimilarity to clavus suggests that pressure, possiblyduring sleep, may have some bearing on the con-dition.
SummaryThe histological features of 12 cases of chondro-
dermatitis chronica helicis are described. Thecondition is primarily an epithelial change withhyperkeratosis, acanthosis, and parakeratosis. Acentral keratin plug is formed which invaginatesthe epithelium in a " crater-like" manner. Theepithelium below the keratin plug becomesulcerated, associated with the production of fibrin-oid material and a fibrovascular proliferation inthe corium. Perichondritis is always present.The cartilage may or may not be involved.
REFERENCESCarol, W. L. L., and Haren, H. B. van (1941). Dermnatologia (Basel),
83, 353.Ebenius, B. (1941). Acta radiol. (Stockh.), 22, 563.Foerster, 0. H. (1917). J. cutan. Dis., 36, 154.
(1925). Arch. Derm. Syph. (Chicago), 11, 149.Shuman, R., and Helwig, E. B. (1954). Amer. J. c/in. Path., 24, 126.Winkler, M. (1915). Arch. Derin. Scph. (Berl.), 121, 278.
50
copyright. on 12 O
ctober 2018 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.10.1.46 on 1 F
ebruary 1957. Dow
nloaded from






![Evaluation of the Trivedi Effect - Energy of … symptoms include parakeratosis, hypogeusia, anorexia, dysosmia, geophagia, hypogonadism, growth retardation, etc. [5-7]. Recently,](https://img.pdfslide.net/doc/110x75/5d209b2b88c993a5378d16d5/evaluation-of-the-trivedi-effect-energy-of-symptoms-include-parakeratosis-hypogeusia.jpg)




![l c a l Derma Journal of Clinical & Experimental t i n o i ... · dermatologic conditions, including tinea pedis, seborrheic dermatitis, and axillary granular parakeratosis [14]](https://img.pdfslide.net/doc/110x75/5ce96bfc88c9932e468d82af/l-c-a-l-derma-journal-of-clinical-experimental-t-i-n-o-i-dermatologic.jpg)
















