Embed Size (px)
Citation preview
Campbell/TnT-IES Participation Based Services January 2010 Page 1 of 27
CAREGIVER ASSESSMENT OF ACTIVITIES AND ROUTINES Learning about activities and routines allows providers to work with caregivers to:
� Help children participate successfully in activities or routines that may currently be challenging;
� Embed intervention strategies, including adaptations and AT, into activities/routines so that children have multiple learning opportunities; and
� Identify the best ways for caregivers to learn strategies to promote their children’s development.
The Importance of Activities and Routines to a Participation-Based Intervention Approach
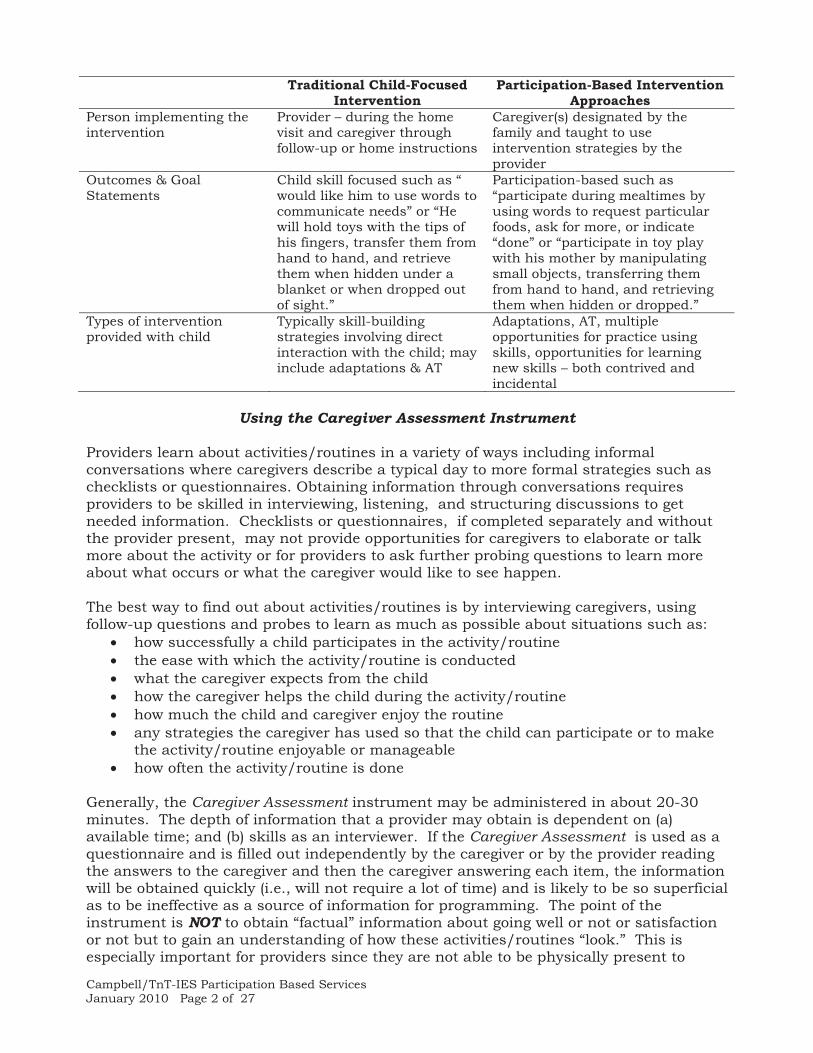
The chart below contrasts traditional child-focused intervention with participation-based approaches. In child focused intervention, teachers and therapists design or create activities to provide opportunities for a child to practice or learn an identified developmental skill. For example, an occupational therapist may structure an activity so that trucks and other vehicle toys are involved so that the child may practice a skill of pushing objects. In participation- based services, the emphasis is on: a) children’s successful participation in identified activity(ies) or routine(s); and b) embedding of intervention strategies into the activities or routines. For example, a speech and language pathologist may work with a caregiver around issues involved in having the child learn to chew and swallow a variety of foods thereby helping a child to participate successfully in mealtime. Or, opportunities to communicate particular words may be embedded into bathtime or riding in a car or other caregiver-identified activities/routines. When implementing participation-based services, developmental information is insufficient and information about participation in activities/routines must also be obtained. Traditional Child-Focused
Intervention Participation-Based Intervention
Approaches Context of Intervention Provider-designed activity
(selected by the provider) Typical family activity or routine selected by the caregiver with the provider
Length of Intervention
Length of home visit – typically an hour
Multiple hours infused throughout the week by providing learning opportunities in typically occurring activities/routines
Campbell/TnT-IES Participation Based Services January 2010 Page 2 of 27
Traditional Child-Focused Intervention
Participation-Based Intervention Approaches
Person implementing the intervention
Provider – during the home visit and caregiver through follow-up or home instructions
Caregiver(s) designated by the family and taught to use intervention strategies by the provider
Outcomes & Goal Statements
Child skill focused such as “ would like him to use words to communicate needs” or “He will hold toys with the tips of his fingers, transfer them from hand to hand, and retrieve them when hidden under a blanket or when dropped out of sight.”
Participation-based such as “participate during mealtimes by using words to request particular foods, ask for more, or indicate “done” or “participate in toy play with his mother by manipulating small objects, transferring them from hand to hand, and retrieving them when hidden or dropped.”
Types of intervention provided with child
Typically skill-building strategies involving direct interaction with the child; may include adaptations & AT
Adaptations, AT, multiple opportunities for practice using skills, opportunities for learning new skills – both contrived and incidental
Using the Caregiver Assessment Instrument
Providers learn about activities/routines in a variety of ways including informal conversations where caregivers describe a typical day to more formal strategies such as checklists or questionnaires. Obtaining information through conversations requires providers to be skilled in interviewing, listening, and structuring discussions to get needed information. Checklists or questionnaires, if completed separately and without the provider present, may not provide opportunities for caregivers to elaborate or talk more about the activity or for providers to ask further probing questions to learn more about what occurs or what the caregiver would like to see happen. The best way to find out about activities/routines is by interviewing caregivers, using follow-up questions and probes to learn as much as possible about situations such as:
� how successfully a child participates in the activity/routine � the ease with which the activity/routine is conducted � what the caregiver expects from the child � how the caregiver helps the child during the activity/routine � how much the child and caregiver enjoy the routine � any strategies the caregiver has used so that the child can participate or to make
the activity/routine enjoyable or manageable � how often the activity/routine is done
Generally, the Caregiver Assessment instrument may be administered in about 20-30 minutes. The depth of information that a provider may obtain is dependent on (a) available time; and (b) skills as an interviewer. If the Caregiver Assessment is used as a questionnaire and is filled out independently by the caregiver or by the provider reading the answers to the caregiver and then the caregiver answering each item, the information will be obtained quickly (i.e., will not require a lot of time) and is likely to be so superficial as to be ineffective as a source of information for programming. The point of the instrument is NOT to obtain “factual” information about going well or not or satisfaction or not but to gain an understanding of how these activities/routines “look.” This is especially important for providers since they are not able to be physically present to
Campbell/TnT-IES Participation Based Services January 2010 Page 3 of 27
observe every family activity/routine. For example, few providers are able to make Sunday visits to church, accompany the family when visiting relatives at night, or be present at bedtime. Information gained through the Caregiver Assessment should be as “rich” and complete as what a provider would have observed should observation have been possible.
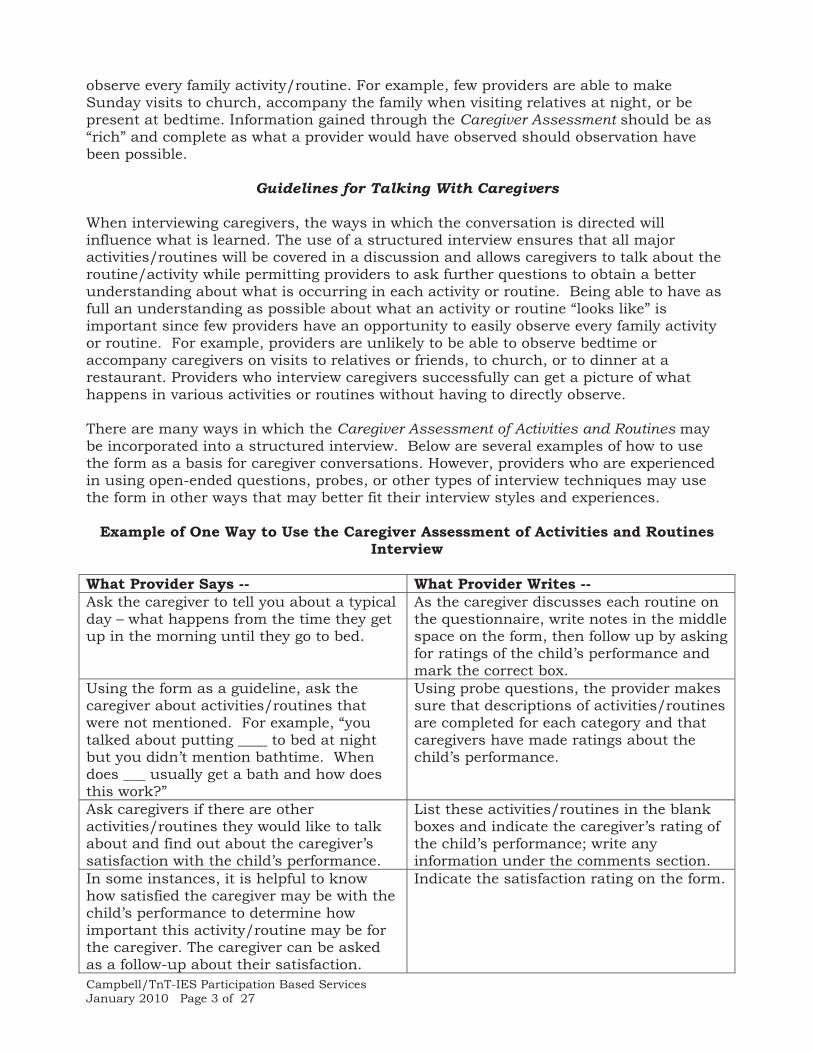
Guidelines for Talking With Caregivers When interviewing caregivers, the ways in which the conversation is directed will influence what is learned. The use of a structured interview ensures that all major activities/routines will be covered in a discussion and allows caregivers to talk about the routine/activity while permitting providers to ask further questions to obtain a better understanding about what is occurring in each activity or routine. Being able to have as full an understanding as possible about what an activity or routine “looks like” is important since few providers have an opportunity to easily observe every family activity or routine. For example, providers are unlikely to be able to observe bedtime or accompany caregivers on visits to relatives or friends, to church, or to dinner at a restaurant. Providers who interview caregivers successfully can get a picture of what happens in various activities or routines without having to directly observe. There are many ways in which the Caregiver Assessment of Activities and Routines may be incorporated into a structured interview. Below are several examples of how to use the form as a basis for caregiver conversations. However, providers who are experienced in using open-ended questions, probes, or other types of interview techniques may use the form in other ways that may better fit their interview styles and experiences.
Example of One Way to Use the Caregiver Assessment of Activities and Routines Interview
What Provider Says -- What Provider Writes -- Ask the caregiver to tell you about a typical day – what happens from the time they get up in the morning until they go to bed.
As the caregiver discusses each routine on the questionnaire, write notes in the middle space on the form, then follow up by asking for ratings of the child’s performance and mark the correct box.
Using the form as a guideline, ask the caregiver about activities/routines that were not mentioned. For example, “you talked about putting ____ to bed at night but you didn’t mention bathtime. When does ___ usually get a bath and how does this work?”
Using probe questions, the provider makes sure that descriptions of activities/routines are completed for each category and that caregivers have made ratings about the child’s performance.
Ask caregivers if there are other activities/routines they would like to talk about and find out about the caregiver’s satisfaction with the child’s performance.
List these activities/routines in the blank boxes and indicate the caregiver’s rating of the child’s performance; write any information under the comments section.
In some instances, it is helpful to know how satisfied the caregiver may be with the child’s performance to determine how important this activity/routine may be for the caregiver. The caregiver can be asked as a follow-up about their satisfaction.
Indicate the satisfaction rating on the form.

Campbell/TnT-IES Participation Based Services January 2010 Page 4 of 27
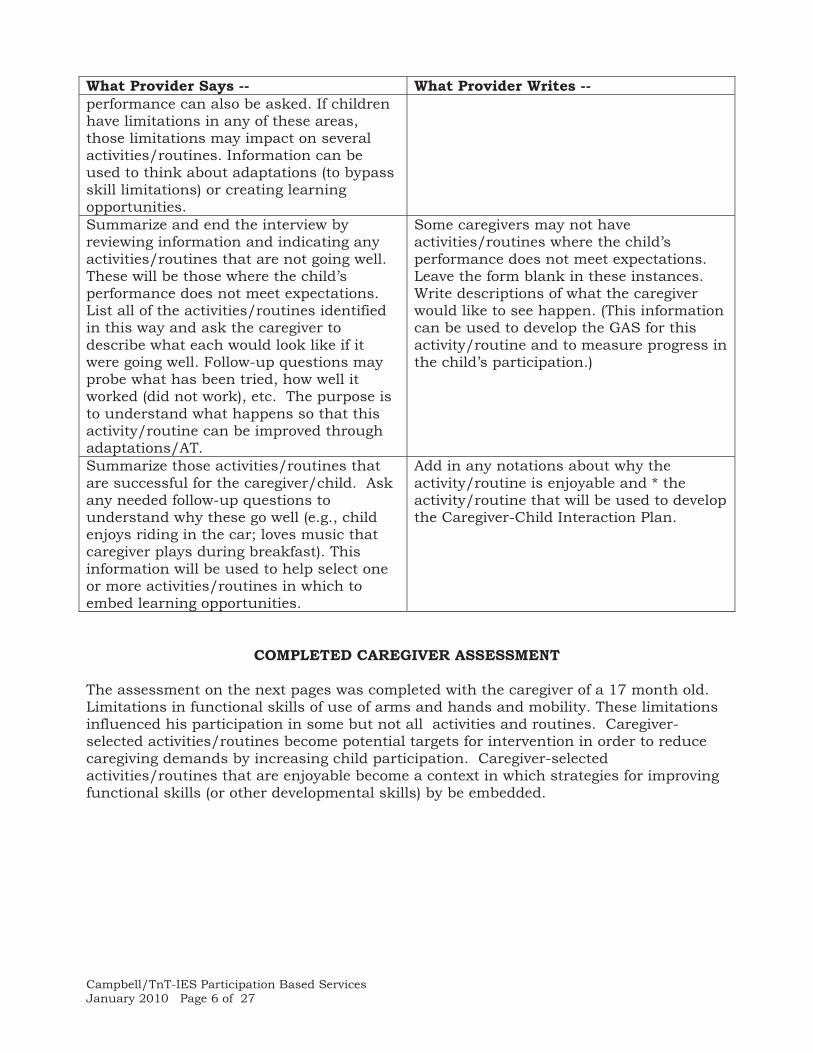
What Provider Says -- What Provider Writes -- Functional Skills: 4 overall skill areas impact on children’s performance in activities/routines. Ask caregivers to talk about the child’s performance of each of these functional skills and identify where they may negatively limit the child’s performance. The caregiver’s satisfaction with the child’s performance can also be asked. If children have limitations in any of these areas, those limitations may impact on several activities/routines. This information can be used to think about adaptations (to bypass skill limitations) or creating opportunities for the child to practice or learn to use these skills.
Fill in the caregiver’s rating and describe any key points about the skill. Satisfaction ratings may be completed if this is an area that is asked about.
Summarize and end the interview by reviewing information and indicating any activities/routines that are not going well. These will be those where the child’s performance does not meet expectations. List all of the activities/routines identified in this way and ask the caregiver to describe what this would look like if it were going well. Follow-up questions may probe what has been tried, how well it worked (did not work), etc. The purpose is to fully understand what happens so that this activity/routine can be improved through adaptations/AT.
Some caregivers may not have activities/routines where the child’s performance does not meet expectations. Leave the form blank in these instances. Write descriptions of what the caregiver would like to see happen. (This information can be used to develop the GAS for this activity/routine and to measure progress in the child’s participation.)
Summarize those activities/routines that are successful for the caregiver/child. Ask any needed follow-up questions to understand why these go well (e.g., child enjoys riding in the car; loves music that caregiver plays during breakfast). This information will be used to help select one or more activities/routines in which to embed learning opportunities.
Add in any notations about why the activity/routine is enjoyable and * the activity/routine that will be used to develop the Caregiver-Child Interaction Plan.
.
Campbell/TnT-IES Participation Based Services January 2010 Page 5 of 27
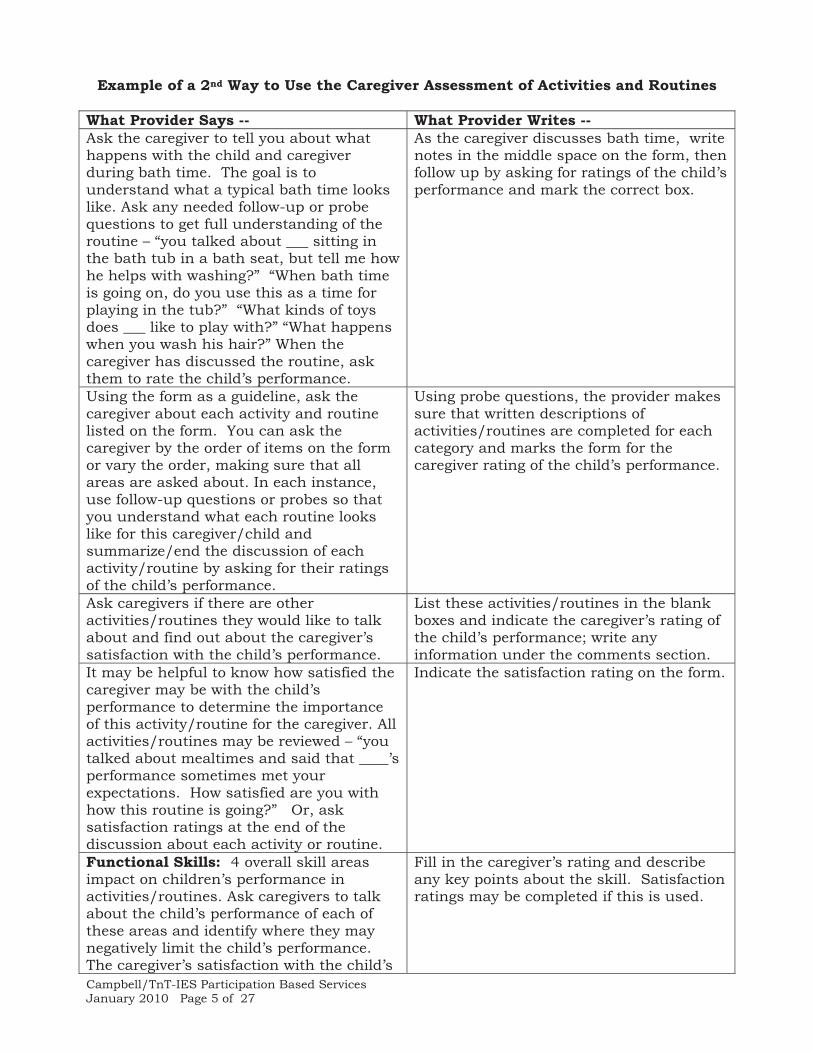
Example of a 2nd Way to Use the Caregiver Assessment of Activities and Routines What Provider Says -- What Provider Writes -- Ask the caregiver to tell you about what happens with the child and caregiver during bath time. The goal is to understand what a typical bath time looks like. Ask any needed follow-up or probe questions to get full understanding of the routine – “you talked about ___ sitting in the bath tub in a bath seat, but tell me how he helps with washing?” “When bath time is going on, do you use this as a time for playing in the tub?” “What kinds of toys does ___ like to play with?” “What happens when you wash his hair?” When the caregiver has discussed the routine, ask them to rate the child’s performance.
As the caregiver discusses bath time, write notes in the middle space on the form, then follow up by asking for ratings of the child’s performance and mark the correct box.
Using the form as a guideline, ask the caregiver about each activity and routine listed on the form. You can ask the caregiver by the order of items on the form or vary the order, making sure that all areas are asked about. In each instance, use follow-up questions or probes so that you understand what each routine looks like for this caregiver/child and summarize/end the discussion of each activity/routine by asking for their ratings of the child’s performance.
Using probe questions, the provider makes sure that written descriptions of activities/routines are completed for each category and marks the form for the caregiver rating of the child’s performance.
Ask caregivers if there are other activities/routines they would like to talk about and find out about the caregiver’s satisfaction with the child’s performance.
List these activities/routines in the blank boxes and indicate the caregiver’s rating of the child’s performance; write any information under the comments section.
It may be helpful to know how satisfied the caregiver may be with the child’s performance to determine the importance of this activity/routine for the caregiver. All activities/routines may be reviewed – “you talked about mealtimes and said that ____’s performance sometimes met your expectations. How satisfied are you with how this routine is going?” Or, ask satisfaction ratings at the end of the discussion about each activity or routine.
Indicate the satisfaction rating on the form.
Functional Skills: 4 overall skill areas impact on children’s performance in activities/routines. Ask caregivers to talk about the child’s performance of each of these areas and identify where they may negatively limit the child’s performance. The caregiver’s satisfaction with the child’s
Fill in the caregiver’s rating and describe any key points about the skill. Satisfaction ratings may be completed if this is used.
Campbell/TnT-IES Participation Based Services January 2010 Page 6 of 27
What Provider Says -- What Provider Writes -- performance can also be asked. If children have limitations in any of these areas, those limitations may impact on several activities/routines. Information can be used to think about adaptations (to bypass skill limitations) or creating learning opportunities. Summarize and end the interview by reviewing information and indicating any activities/routines that are not going well. These will be those where the child’s performance does not meet expectations. List all of the activities/routines identified in this way and ask the caregiver to describe what each would look like if it were going well. Follow-up questions may probe what has been tried, how well it worked (did not work), etc. The purpose is to understand what happens so that this activity/routine can be improved through adaptations/AT.
Some caregivers may not have activities/routines where the child’s performance does not meet expectations. Leave the form blank in these instances. Write descriptions of what the caregiver would like to see happen. (This information can be used to develop the GAS for this activity/routine and to measure progress in the child’s participation.)
Summarize those activities/routines that are successful for the caregiver/child. Ask any needed follow-up questions to understand why these go well (e.g., child enjoys riding in the car; loves music that caregiver plays during breakfast). This information will be used to help select one or more activities/routines in which to embed learning opportunities.
Add in any notations about why the activity/routine is enjoyable and * the activity/routine that will be used to develop the Caregiver-Child Interaction Plan.
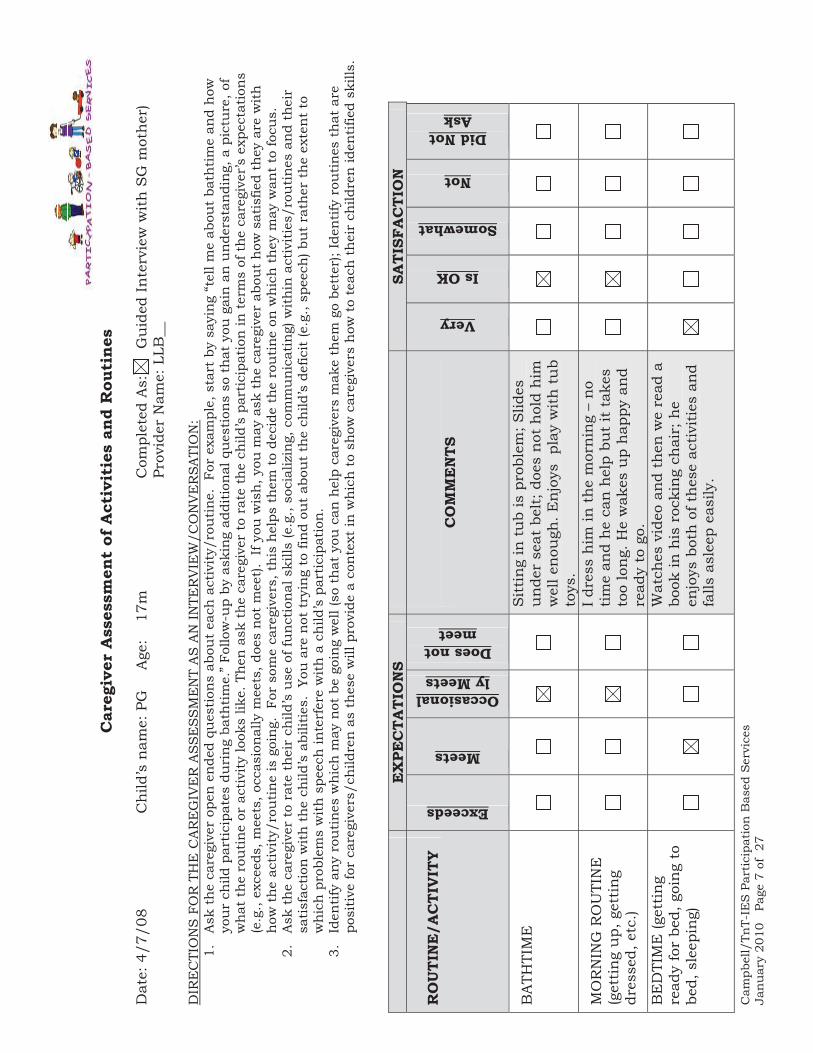
COMPLETED CAREGIVER ASSESSMENT
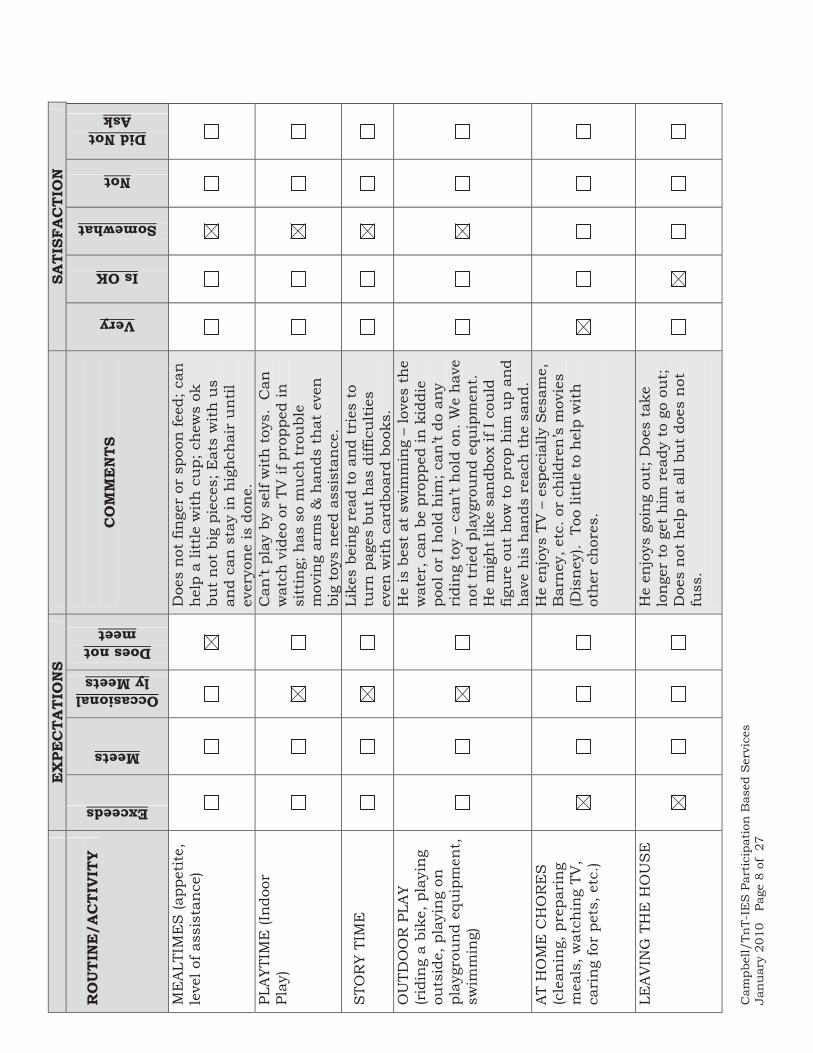
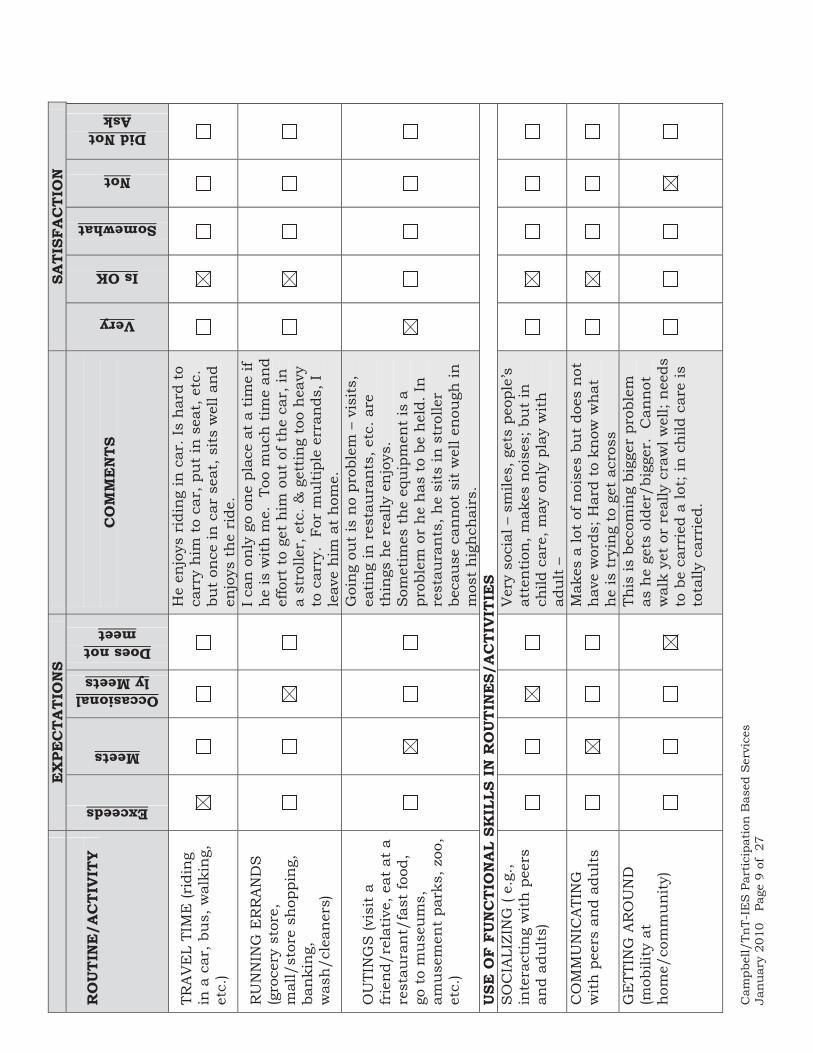
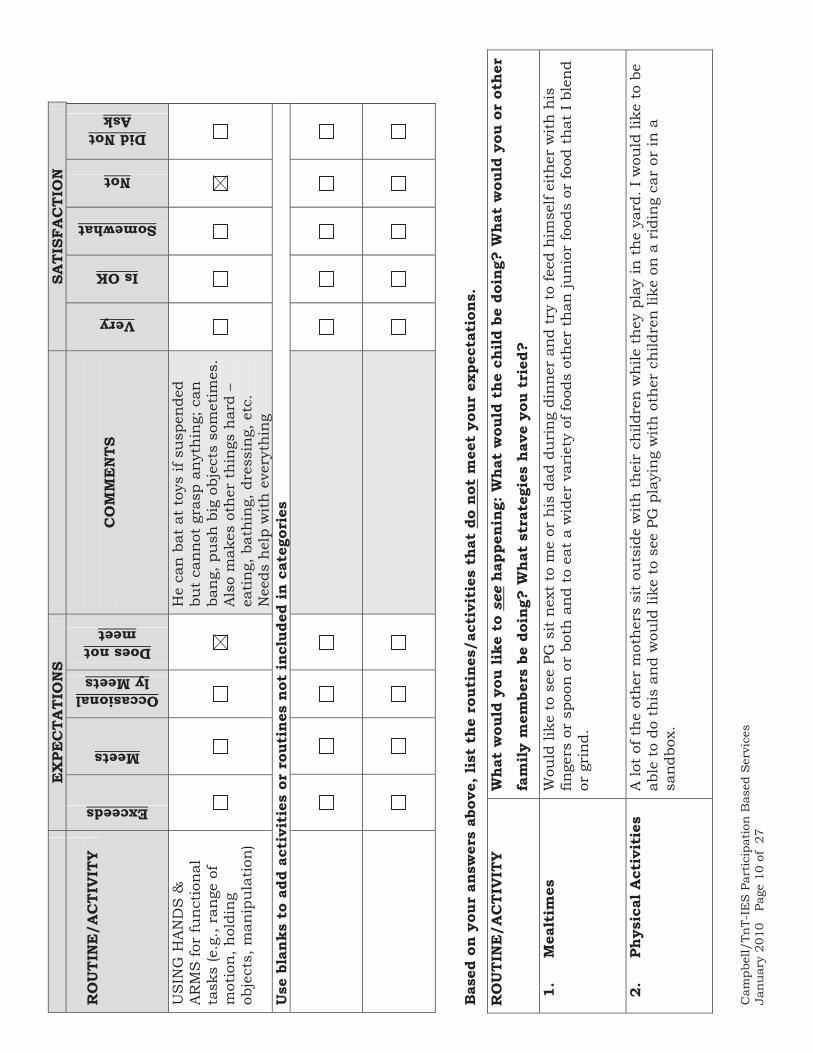
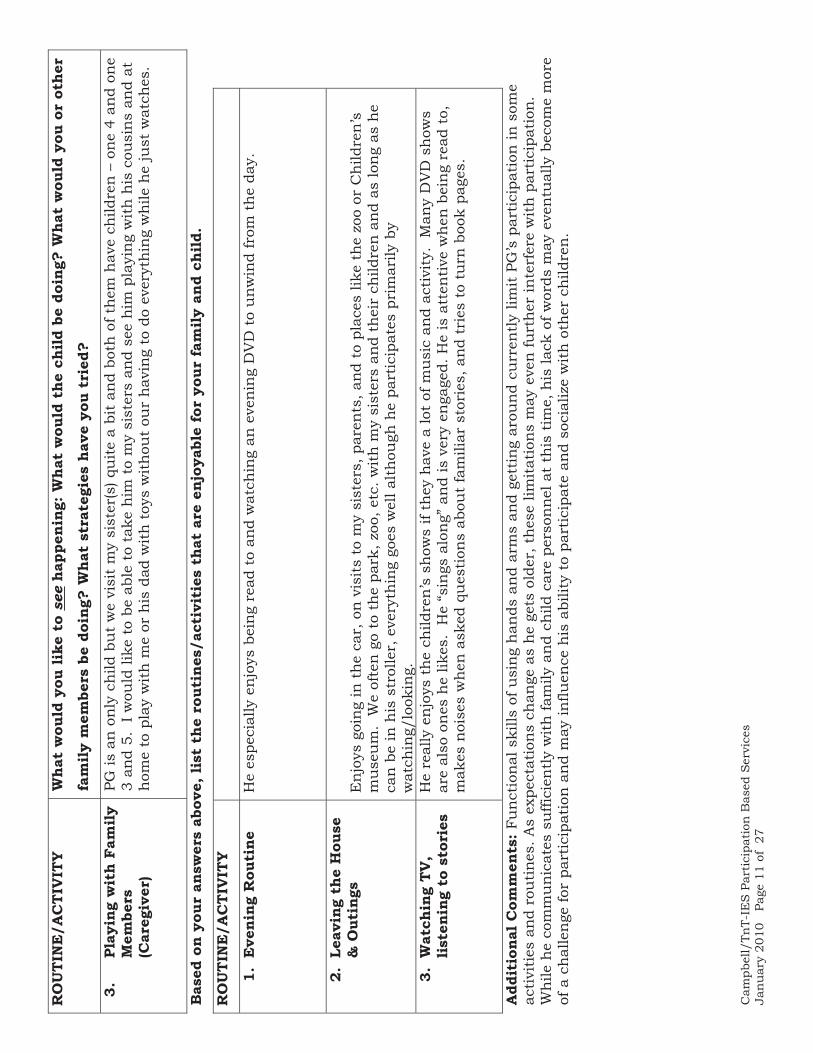
The assessment on the next pages was completed with the caregiver of a 17 month old. Limitations in functional skills of use of arms and hands and mobility. These limitations influenced his participation in some but not all activities and routines. Caregiver-selected activities/routines become potential targets for intervention in order to reduce caregiving demands by increasing child participation. Caregiver-selected activities/routines that are enjoyable become a context in which strategies for improving functional skills (or other developmental skills) by be embedded.
Cam
pbel
l/Tn
T-IE
S P
arti
cipa
tion
Bas
ed S
ervi
ces
Jan
uar
y 20
10
Page
7 o
f 27
Car
egiv
er A
sses
smen
t of
Act
ivit
ies
and
Rou
tine
s
Dat
e: 4
/7/0
8
Ch
ild’s
nam
e: P
G
Age
: 17
m
Com
plet
ed A
s: G
uid
ed I
nte
rvie
w w
ith
SG
mot
her
)
Prov
ider
Nam
e: L
LB__
D
IRE
CTI
ON
S F
OR
TH
E C
AR
EG
IVE
R A
SS
ES
SM
EN
T A
S A
N IN
TER
VIE
W/C
ON
VE
RSA
TIO
N:
1.A
sk t
he
care
give
r op
en e
nde
d qu
esti
ons
abou
t ea
ch a
ctiv
ity/
rou
tine
. Fo
r ex
ampl
e, s
tart
by
sayi
ng
“tel
l me
abou
t ba
thti
me
and
how
yo
ur
child
par
tici
pate
s du
rin
g ba
thti
me.
” Fo
llow
-up
by a
skin
g ad
diti
onal
qu
esti
ons
so t
hat
you
gai
n a
n u
nde
rsta
ndi
ng,
a p
ictu
re, o
f w
hat
th
e ro
uti
ne
or a
ctiv
ity
look
s lik
e. T
hen
ask
th
e ca
regi
ver
to r
ate
the
child
’s p
arti
cipa
tion
in t
erm
s of
th
e ca
regi
ver’
s ex
pect
atio
ns
(e.g
., ex
ceed
s, m
eets
, occ
asio
nal
ly m
eets
, doe
s no
t m
eet)
. If
you
wis
h, y
ou m
ay a
sk t
he
care
give
r ab
out
how
sat
isfie
d th
ey a
re w
ith
h
ow t
he
acti
vity
/rou
tin
e is
goi
ng.
For
som
e ca
regi
vers
, th
is h
elps
th
em t
o de
cide
th
e ro
uti
ne o
n w
hic
h t
hey
may
wan
t to
focu
s.
2.A
sk t
he
care
give
r to
rat
e th
eir
child
’s u
se o
f fu
nct
ion
al s
kills
(e.g
., so
cial
izin
g, c
omm
uni
cati
ng)
wit
hin
act
ivit
ies/
rou
tine
s an
d th
eir
sati
sfac
tion
wit
h t
he
child
’s a
bilit
ies.
You
are
not
try
ing
to fi
nd
out
abou
t th
e ch
ild’s
def
icit
(e.g
., sp
eech
) bu
t ra
ther
th
e ex
ten
t to
w
hic
h p
robl
ems
wit
h s
peec
h in
terf
ere
wit
h a
ch
ild’s
par
tici
pati
on.
3.Id
enti
fy a
ny
rou
tine
s w
hic
h m
ay n
ot b
e go
ing
wel
l (so
th
at y
ou c
an h
elp
care
give
rs m
ake
them
go
bett
er);
Iden
tify
rou
tin
es t
hat
are
po
siti
ve fo
r ca
regi
vers
/ch
ildre
n a
s th
ese
will
pro
vide
a c
onte
xt in
wh
ich
to
show
car
egiv
ers
how
to
teac
h t
hei
r ch
ildre
n id
enti
fied
skill
s.
E
XPE
CTA
TIO
NS
SATI
SFA
CTI
ON
R
OU
TIN
E/A
CTI
VIT
Y
Exceeds
Meets
Occasionally Meets
Does not meet
C
OM
ME
NTS
Very
Is OK
Somewhat
Not
Did Not Ask
BA
THTI
ME
Sit
tin
g in
tu
b is
pro
blem
; Slid
es
un
der
seat
bel
t; d
oes
not
hol
d h
im
wel
l en
ough
. En
joys
pla
y w
ith
tu
b to
ys.
MO
RN
ING
RO
UTI
NE
(g
etti
ng
up,
get
tin
g dr
esse
d, e
tc.)
I dr
ess
him
in t
he
mor
nin
g –
no
tim
e an
d h
e ca
n h
elp
but
it t
akes
to
o lo
ng.
He
wak
es u
p h
appy
an
d re
ady
to g
o.
BE
DTI
ME
(get
tin
g re
ady
for
bed,
goi
ng
to
bed,
sle
epin
g)
Wat
ches
vid
eo a
nd
then
we
read
a
book
in h
is r
ocki
ng
chai
r; h
e en
joys
bot
h o
f th
ese
acti
viti
es a
nd
falls
asl
eep
easi
ly.
Cam
pbel
l/Tn
T-IE
S P
arti
cipa
tion
Bas
ed S
ervi
ces
Jan
uar
y 20
10
Page
8 o
f 27
E
XPE
CTA
TIO
NS
SATI
SFA
CTI
ON
R
OU
TIN
E/A
CTI
VIT
Y
Exceeds
Meets
Occasionally Meets
Does not meet
C
OM
ME
NTS
Very
Is OK
Somewhat
Not
Did Not Ask
ME
ALT
IME
S (a
ppet
ite,
le
vel o
f ass
ista
nce
)
Doe
s n
ot fi
nge
r or
spo
on fe
ed; c
an
hel
p a
littl
e w
ith
cu
p; c
hew
s ok
bu
t n
ot b
ig p
iece
s; E
ats
wit
h u
s an
d ca
n s
tay
in h
igh
chai
r u
nti
l ev
eryo
ne
is d
one.
PLA
YTIM
E (I
ndo
or
Play
)
Can
’t pl
ay b
y se
lf w
ith
toy
s. C
an
wat
ch v
ideo
or
TV if
pro
pped
in
sitt
ing;
has
so
mu
ch t
rou
ble
mov
ing
arm
s &
han
ds t
hat
eve
n
big
toys
nee
d as
sist
ance
.
STO
RY
TIM
E
Li
kes
bein
g re
ad t
o an
d tr
ies
to
turn
pag
es b
ut
has
diff
icu
ltie
s ev
en w
ith
car
dboa
rd b
ooks
.
OU
TDO
OR
PLA
Y (r
idin
g a
bike
, pla
yin
g ou
tsid
e, p
layi
ng
on
play
grou
nd
equ
ipm
ent,
sw
imm
ing)
He
is b
est
at s
wim
min
g –
love
s th
e w
ater
, can
be
prop
ped
in k
iddi
e po
ol o
r I
hol
d h
im; c
an’t
do a
ny
ridi
ng
toy
– ca
n’t
hol
d on
. We
hav
e n
ot t
ried
pla
ygro
un
d eq
uip
men
t.
He
mig
ht
like
san
dbox
if I
cou
ld
figu
re o
ut
how
to
prop
him
up
and
hav
e h
is h
ands
rea
ch t
he
san
d.
AT
HO
ME
CH
OR
ES
(c
lean
ing,
pre
pari
ng
mea
ls, w
atch
ing
TV,
cari
ng
for
pets
, etc
.)
He
enjo
ys T
V –
esp
ecia
lly S
esam
e,
Bar
ney
, etc
. or
child
ren
’s m
ovie
s (D
isn
ey).
Too
litt
le t
o h
elp
wit
h
oth
er c
hor
es.
LEA
VIN
G T
HE
HO
US
E
He
enjo
ys g
oin
g ou
t; D
oes
take
lo
nge
r to
get
him
rea
dy t
o go
ou
t;
Doe
s n
ot h
elp
at a
ll bu
t do
es n
ot
fuss
.
Cam
pbel
l/Tn
T-IE
S P
arti
cipa
tion
Bas
ed S
ervi
ces
Jan
uar
y 20
10
Page
9 o
f 27
E
XPE
CTA
TIO
NS
SATI
SFA
CTI
ON
R
OU
TIN
E/A
CTI
VIT
Y
Exceeds
Meets
Occasionally Meets
Does not meet
C
OM
ME
NTS
Very
Is OK
Somewhat
Not
Did Not Ask
TRA
VE
L TI
ME
(rid
ing
in a
car
, bu
s, w
alki
ng,
et
c.)
He
enjo
ys r
idin
g in
car
. Is
har
d to
ca
rry
him
to
car,
pu
t in
sea
t, e
tc.
but
once
in c
ar s
eat,
sit
s w
ell a
nd
enjo
ys t
he
ride
.
RU
NN
ING
ER
RA
ND
S
(gro
cery
sto
re,
mal
l/st
ore
shop
pin
g,
ban
kin
g,
was
h/c
lean
ers)
I ca
n o
nly
go
one
plac
e at
a t
ime
if h
e is
wit
h m
e. T
oo m
uch
tim
e an
d ef
fort
to
get
him
ou
t of
th
e ca
r, in
a
stro
ller,
etc
. & g
etti
ng
too
hea
vy
to c
arry
. Fo
r m
ult
iple
err
ands
, I
leav
e h
im a
t h
ome.
OU
TIN
GS
(vis
it a
fr
ien
d/re
lati
ve, e
at a
t a
rest
aura
nt/
fast
food
, go
to
mu
seu
ms,
am
use
men
t pa
rks,
zoo
, et
c.)
Goi
ng
out
is n
o pr
oble
m –
vis
its,
ea
tin
g in
res
tau
ran
ts, e
tc. a
re
thin
gs h
e re
ally
en
joys
. S
omet
imes
th
e eq
uip
men
t is
a
prob
lem
or
he
has
to
be h
eld.
In
re
stau
ran
ts, h
e si
ts in
str
olle
r be
cau
se c
ann
ot s
it w
ell e
nou
gh in
m
ost
hig
hch
airs
.
USE
OF
FUN
CTI
ON
AL
SKIL
LS I
N R
OU
TIN
ES/
AC
TIV
ITIE
S S
OC
IALI
ZIN
G (
e.g.
, in
tera
ctin
g w
ith
pee
rs
and
adu
lts)
Ver
y so
cial
– s
mile
s, g
ets
peop
le’s
at
ten
tion
, mak
es n
oise
s; b
ut
in
child
car
e, m
ay o
nly
pla
y w
ith
ad
ult
–
CO
MM
UN
ICA
TIN
G
wit
h p
eers
an
d ad
ult
s
Mak
es a
lot
of n
oise
s bu
t do
es n
ot
hav
e w
ords
; Har
d to
kn
ow w
hat
h
e is
try
ing
to g
et a
cros
s
GE
TTIN
G A
RO
UN
D
(mob
ility
at
hom
e/co
mm
un
ity)
This
is b
ecom
ing
bigg
er p
robl
em
as h
e ge
ts o
lder
/big
ger.
Can
not
w
alk
yet
or r
eally
cra
wl w
ell;
nee
ds
to b
e ca
rrie
d a
lot;
in c
hild
car
e is
to
tally
car
ried
.
Cam
pbel
l/Tn
T-IE
S P
arti
cipa
tion
Bas
ed S
ervi
ces
Jan
uar
y 20
10
Page
10
of 2
7
E
XPE
CTA
TIO
NS
SATI
SFA
CTI
ON
R
OU
TIN
E/A
CTI
VIT
Y
Exceeds
Meets
Occasionally Meets
Does not meet
C
OM
ME
NTS
Very
Is OK
Somewhat
Not
Did Not Ask
US
ING
HA
ND
S &
A
RM
S fo
r fu
nct
ion
al
task
s (e
.g.,
ran
ge o
f m
otio
n, h
oldi
ng
obje
cts,
man
ipu
lati
on)
He
can
bat
at
toys
if s
usp
ende
d bu
t ca
nn
ot g
rasp
an
yth
ing;
can
ba
ng,
pu
sh b
ig o
bjec
ts s
omet
imes
. A
lso
mak
es o
ther
th
ings
har
d –
eati
ng,
bat
hin
g, d
ress
ing,
etc
. N
eeds
hel
p w
ith
eve
ryth
ing
Use
bla
nks
to a
dd a
ctiv
itie
s or
rou
tine
s no
t in
clud
ed in
cat
egor
ies
Bas
ed o
n yo
ur a
nsw
ers
abov
e, li
st t
he r
outi
nes/
acti
viti
es t
hat
do n
ot m
eet
your
exp
ecta
tion
s.
RO
UTI
NE
/AC
TIV
ITY
Wha
t w
ould
you
like
to
see
happ
enin
g: W
hat
wou
ld t
he c
hild
be
doin
g? W
hat
wou
ld y
ou o
r ot
her
fam
ily m
embe
rs b
e do
ing?
Wha
t st
rate
gies
hav
e yo
u tr
ied?
1.M
ealt
imes
W
ould
like
to
see
PG s
it n
ext
to m
e or
his
dad
du
rin
g di
nn
er a
nd
try
to fe
ed h
imse
lf ei
ther
wit
h h
is
finge
rs o
r sp
oon
or
both
an
d to
eat
a w
ider
var
iety
of f
oods
oth
er t
han
jun
ior
food
s or
food
th
at I
ble
nd
or g
rin
d.
2.Ph
ysic
al A
ctiv
itie
s A
lot
of t
he
oth
er m
oth
ers
sit
outs
ide
wit
h t
hei
r ch
ildre
n w
hile
th
ey p
lay
in t
he
yard
. I w
ould
like
to
be
able
to
do t
his
an
d w
ould
like
to
see
PG p
layi
ng
wit
h o
ther
ch
ildre
n li
ke o
n a
rid
ing
car
or in
a
san
dbox
.
Cam
pbel
l/Tn
T-IE
S P
arti
cipa
tion
Bas
ed S
ervi
ces
Jan
uar
y 20
10
Page
11
of 2
7
RO
UTI
NE
/AC
TIV
ITY
Wha
t w
ould
you
like
to
see
happ
enin
g: W
hat
wou
ld t
he c
hild
be
doin
g? W
hat
wou
ld y
ou o
r ot
her
fam
ily m
embe
rs b
e do
ing?
Wha
t st
rate
gies
hav
e yo
u tr
ied?
3.Pl
ayin
g w
ith
Fam
ily
Mem
bers
(C
areg
iver
)
PG is
an
on
ly c
hild
bu
t w
e vi
sit
my
sist
er(s
) qu
ite
a bi
t an
d bo
th o
f th
em h
ave
child
ren
– o
ne
4 an
d on
e 3
and
5. I
wou
ld li
ke t
o be
abl
e to
tak
e h
im t
o m
y si
ster
s an
d se
e h
im p
layi
ng
wit
h h
is c
ousi
ns
and
at
hom
e to
pla
y w
ith
me
or h
is d
ad w
ith
toy
s w
ith
out
our
hav
ing
to d
o ev
eryt
hin
g w
hile
he
just
wat
ches
.
Bas
ed o
n yo
ur a
nsw
ers
abov
e, li
st t
he r
outi
nes/
acti
viti
es t
hat
are
enjo
yabl
e fo
r yo
ur f
amily
and
chi
ld.
RO
UTI
NE
/AC
TIV
ITY
1.E
veni
ng R
outi
ne
He
espe
cial
ly e
njo
ys b
ein
g re
ad t
o an
d w
atch
ing
an e
ven
ing
DV
D t
o u
nw
ind
from
th
e da
y.
2.Le
avin
g th
e H
ouse
&
Out
ings
E
njo
ys g
oin
g in
th
e ca
r, o
n v
isit
s to
my
sist
ers,
par
ents
, an
d to
pla
ces
like
the
zoo
or C
hild
ren
’s
mu
seu
m.
We
ofte
n g
o to
th
e pa
rk, z
oo, e
tc. w
ith
my
sist
ers
and
thei
r ch
ildre
n a
nd
as lo
ng
as h
e ca
n b
e in
his
str
olle
r, e
very
thin
g go
es w
ell a
lth
ough
he
part
icip
ates
pri
mar
ily b
y w
atch
ing/
look
ing.
3.
Wat
chin
g TV
, lis
teni
ng t
o st
orie
s H
e re
ally
en
joys
th
e ch
ildre
n’s
sh
ows
if th
ey h
ave
a lo
t of
mu
sic
and
acti
vity
. M
any
DV
D s
how
s ar
e al
so o
nes
he
likes
. H
e “s
ings
alo
ng”
an
d is
ver
y en
gage
d. H
e is
att
enti
ve w
hen
bei
ng
read
to,
m
akes
noi
ses
wh
en a
sked
qu
esti
ons
abou
t fa
mili
ar s
tori
es, a
nd
trie
s to
tu
rn b
ook
page
s.
Add
itio
nal C
omm
ents
: Fu
nct
ion
al s
kills
of u
sin
g h
ands
an
d ar
ms
and
gett
ing
arou
nd
curr
entl
y lim
it P
G’s
par
tici
pati
on in
som
e ac
tivi
ties
an
d ro
uti
nes
. As
expe
ctat
ion
s ch
ange
as
he
gets
old
er, t
hes
e lim
itat
ion
s m
ay e
ven
furt
her
inte
rfer
e w
ith
par
tici
pati
on.
Wh
ile h
e co
mm
un
icat
es s
uffi
cien
tly
wit
h fa
mily
an
d ch
ild c
are
pers
onn
el a
t th
is t
ime,
his
lack
of w
ords
may
eve
ntu
ally
bec
ome
mor
e of
a c
hal
len
ge fo
r pa
rtic
ipat
ion
an
d m
ay in
fluen
ce h
is a
bilit
y to
par
tici
pate
an
d so
cial
ize
wit
h o
ther
ch
ildre
n.
Page 12 of 27
Campbell/TnT-IES Participation Based Services January 2010 Page 12 of 27
USING CAREGIVER ASSESSMENT RESULTS FOR DECISION-MAKING ABOUT CHILD
INTERVENTION OPPORTUNITIES
Two general types of intervention categories are identified through the caregiver assessment:
� Activities/Routines Not Going Well � Activities/Routines that Caregivers Enjoy with their Children
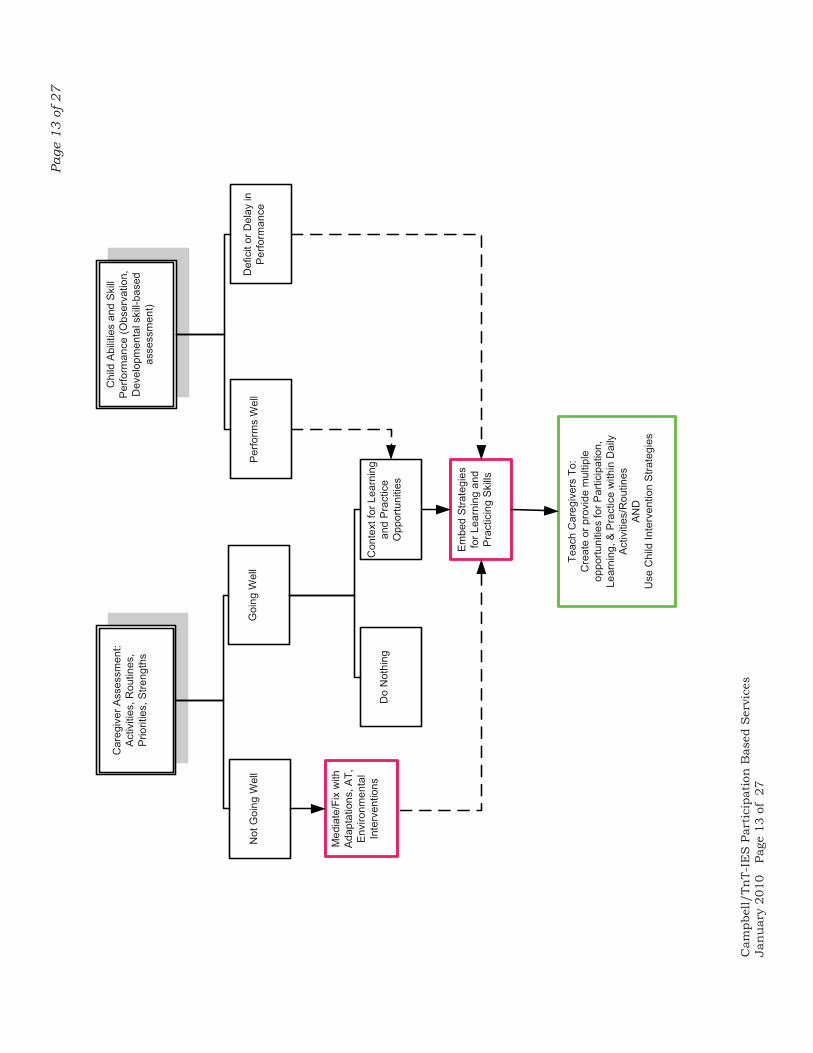
Activities/routines in both of these categories may be contexts in which children may participate, learn, or practice. Figure 1 diagrams the ways in which information from the caregiver assessment is combined with developmental performance information to figure out which activity/routine categories (well/not well) may be selected as contexts for programming.
Activities/Routines Not Going Well Children’s skills or behavior may influence the ease by which caregivers carry out activities and routines. Bathtime, for example, may be especially challenging when a child is unable to sit easily in the tub or does not like water. Families may stop doing certain activities because the child’s participation is so challenging. Sometimes, when professionals ask a simple question such as “are there things that you used to do before your child came into your family, that you are no longer able to do?” they are surprised by the number of activities that caregivers have given up because of not being able to accommodate the child. EI professionals can play a valuable role in helping caregivers continue activities they would like to (or need to) do and to make family routines go as smoothly as possible. Improving activities/routines helps make a caregiver’s life less stressful even though these improvements may not necessarily directly address a child’s skill deficits. Improving a child’s participation in activities or routines that do not go well has the benefit of not only making the activity/routine be more pleasurable and less stressful but also of making the activity/routine go well enough that it may become a future context for teaching and learning. Activities/routines that are problematic may not be optimal situations in which to embed teaching and learning strategies. When activities/routines are not going well, most caregivers cannot wait for the child to learn a whole new skill that may be necessary for optimal participation. For example, a child care teacher cannot wait for a child who is unable to hold utensils, writing tools, etc. to learn to grasp in order for child care routines such as snack or lunch to go well, or for a child to participate in child care activities such as art or inside or outside play that require manipulation of materials. In situations that do not go well and where a child’s increased participation is needed to enhance the activity or routine, adaptation interventions, including AT, should be tried before using strategies designed to help a child learn a new skill.
Page
13
of 2
7
Cam
pbel
l/Tn
T-IE
S P
arti
cipa
tion
Bas
ed S
ervi
ces
Jan
uar
y 20
10
Page
13
of 2
7
Car
egiv
er A
sses
smen
t: A
ctiv
ities
, Rou
tines
, P
riorit
ies,
Stre
ngth
s
Chi
ld A
bilit
ies
and
Ski
ll P
erfo
rman
ce (O
bser
vatio
n,
Dev
elop
men
tal s
kill-
base
d as
sess
men
t)
Not
Goi
ng W
ell
Goi
ng W
ell
Per
form
s W
ell
Def
icit
or D
elay
in
Per
form
ance
Do
Not
hing
Con
text
for L
earn
ing
and
Pra
ctic
e O
ppor
tuni
ties
Embe
d S
trate
gies
fo
r Lea
rnin
g an
d P
ract
icin
g S
kills
Teac
h C
areg
iver
s To
:C
reat
e or
pro
vide
mul
tiple
op
portu
nitie
s fo
r Par
ticip
atio
n,
Lear
ning
, & P
ract
ice
with
in D
aily
Ac
tiviti
es/R
outin
es
AN
DU
se C
hild
Inte
rven
tion
Stra
tegi
es
Med
iate
/Fix
with
A
dapt
atio
ns, A
T,
Env
ironm
enta
l In
terv
entio
ns
Page 14 of 27
Campbell/TnT-IES Participation Based Services January 2010 Page 14 of 27
Interventions using activities/routines that are not going well need to:
� Create immediate – or as immediate as possible – CHANGE � Create change using uncomplicated and easy-to-implement interventions � Provide opportunities for children to participate successfully � Enable caregivers to carry out the activity/routine easily and efficiently � Reduce or minimize caregiving demands.
A majority of the intervention strategies that “fix” activities/routines that are going poorly include environmental modifications, adaptations, and assistive technology (AT). These types of interventions are directed toward making environmental changes (e.g., changing a room arrangement; using equipment for an individual child) and using adaptations that allow a child to participate as independently as possible using materials or aids that do not involve adult assistance. For example, if a child can’t paint at the easels during art at child care because of poor standing balance, strategies such as making an adjustment in the easel height so that the child can sit to paint or using a stander so that a lot of balance is not required allow the child to be independent even though standing balance is not improved. Similarly, adaptations for eating utensils, writing tools, books, toys, or other materials can allow a child to participate without adult assistance even when the child has limited skills. Activities/routines that are not going well are NOT an optimal context in which to:
� Teach a new skill that a child is not presently able to do or able to do easily or independently (without excessive prompts);
� Embed opportunities for the child to practice something the child is able to do but not do well enough to be efficient, competent, or accurate.
Activities/Routines Caregivers Enjoy with Their Children
Many people have written about the importance of using family activities/routines as sources of natural opportunities for teaching children with disabilities. Activities/routines that are identified as a context(s) for child learning opportunities should only include those that are enjoyable for the child and caregiver and in which the child is easily engaged. If bath time, riding in a car, going to the library, or visiting grandma, are things that a caregiver and child enjoy doing, then these are appropriate activities/routines in which to embed opportunities for the child to practice or learn a specific skill. Interventions using activities/routines that caregivers enjoy with their children need to:
� Embed opportunities for a child to practice an existing skill that needs to be performed more fluently, efficiently, quickly, consistently etc. OR
� Embed opportunities for a child to learn a new skill – actually do a skill that is not easily within the child’s repertoire with or without specific intervention;
� Embed specific (differentiated) intervention strategies that allow a child to demonstrate/perform a new skill that the child is unable to perform
� Result in child practice or learning; � Embed opportunities for practice or new skill learning in ways that caregivers can
implement easily (i.e., are not complicated or too “artificial” and that don’t
Page 15 of 27
Campbell/TnT-IES Participation Based Services January 2010 Page 15 of 27
significantly detract from the efficiency, enjoyment, or other characteristics of the activity/routine;
� Enable caregivers to and children to continue to enjoy the activity/routine. Together, the caregiver and EI provider decide what activity/routine to use as a source of opportunities for learning and what skill(s) will be targeted. The family’s evening routine may include book reading before bed, an activity that may provide opportunities for using hands and arms, listening, or verbally or non-verbally identifying objects, colors, or other basic concepts. The caregiver and EI provider together decide what skills are important to be practiced or learned , then the EI provider decides strategies to be used and teaches these to the caregiver, optimally within the selected activity or routine. In this example, the EI provider is unlikely to be able to make a home visit during bedtime, however, the provider and the caregiver could practice bookreading with the child at another time during the day such as nap time. The provider would ask the caregiver to read to the child the same way s/he might when the child is getting ready to go to bed. Then, the provider and caregiver would identify strategies the caregiver might use to help the child acquire or practice the targeted skill. For example, the provider might demonstrate for the caregiver how to use facilitation to help the child reach and point or turn pages of the book and then have the caregiver use the facilitation with the child and verify the caregiver’s correct use (i.e., reinforce the caregiver for using this strategy well) or provide suggestions about how caregiver use might be improved. Some situations where a child is learning a new skill(s) within the context of an activity or routine may involve the use of both teaching strategies (such as facilitation, hand-over-hand guidance, systematic reinforcement) and adaptation interventions. For example, in the above example, the provider might help the caregiver to select cardboard-paged books with simple pictures spaced far enough apart for the child to successfully point or fasten page turners made of cardboard or another material onto the book pages so that the child can turn the pages without adult assistance. Adaptations should always be considered even when “special” therapeutic or educational strategies will be taught to caregivers. These simple modifications, for example, in material or the overall activity may make the activity/routine easier to use as a context for teaching and learning a new skill.
DEVELOPING INTERVENTION DESIGNED TO “FIX” PROBLEMMATIC ACTIVITIES OR ROUTINES
The age of a child and, therefore, typical developmental expectations as well as the child’s degree of disability/delay influence the extent to which caregivers experience activities/routines that are problematic. For example, few participation expectations are generally present when children are under the age of a year. Caregivers don’t expect infants to participate in morning routines, for example, or bathing but may have expectations about participation in play or travel time. Not every caregiver identifies an activity/routine as going poorly. However, when activities/routines are identified, providers should help design strategies that will work quickly to make the identified activity/routine more manageable and easy to carry out. In improving or fixing an activity/routine that is going poorly, providers help families to be raise their children more easily (with fewer caregiver demands) and increase children’s
Page 16 of 27
Campbell/TnT-IES Participation Based Services January 2010 Page 16 of 27
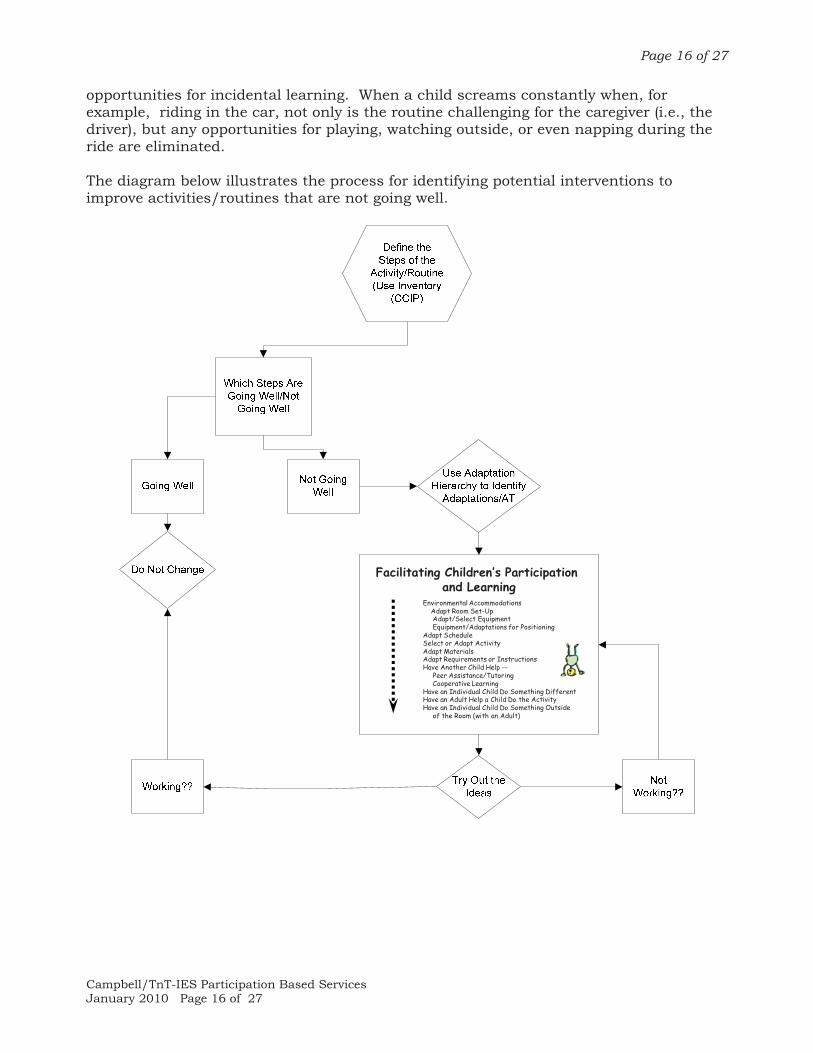
opportunities for incidental learning. When a child screams constantly when, for example, riding in the car, not only is the routine challenging for the caregiver (i.e., the driver), but any opportunities for playing, watching outside, or even napping during the ride are eliminated. The diagram below illustrates the process for identifying potential interventions to improve activities/routines that are not going well.
Environmental AccommodationsAdapt Room Set-UpAdapt/Select EquipmentEquipment/Adaptations for Positioning
Adapt ScheduleSelect or Adapt ActivityAdapt MaterialsAdapt Requirements or InstructionsHave Another Child Help --
Peer Assistance/TutoringCooperative Learning
Have an Individual Child Do Something DifferentHave an Adult Help a Child Do the ActivityHave an Individual Child Do Something Outside
of the Room (with an Adult)
Facilitating Children’s Participation and Learning
Page 17 of 27
Campbell/TnT-IES Participation Based Services January 2010 Page 17 of 27
Designing strategies to improve an activity/routine includes the following components: � Caregiver-identification of an activity/routine which is not going well and for
which the CCIP will be developed and adaptation/AT interventions will be used. � Completing an analysis of the activity
o Identifying which steps of the activity are a problem o Figuring out adaptations or assistive technology to try o Deciding what the adult (usually the caregiver) will do during the
activity/routine o Outlining what the child will be expected to do
� Teaching the caregiver how to implement adaptations/AT or other types of intervention
� Regularly reviewing the effectiveness of the intervention and trying other adaptations, AT, or child interventions if the ones initially planned are no longer effective.
Activity Analysis: The Caregiver-Child Interaction Plan (CCIP)
An analysis of the activity/routine is completed jointly by the caregiver and the provider to identify which aspects are really a problem and to then plan interventions. The plan is developed using discussion between the caregiver and the provider or through observation by the provider while the caregiver performs the activity/routine. Developing the CCIP takes between 20-30 minutes. The framework includes:
Steps Problem? Adaptation/AT What Caregiver Will Do
What Child Will Do
Steps of the Activity/Routine: Watch the caregiver do the routine/activity with the child and write down the steps. If you are unable to observe the activity/routine, then spend some time talking to the caregiver to discuss how the activity/routine takes place and write the steps on the CCIP. For example, for bathtime, the steps might be 1) place the child on the bed, remove clothing, go to the bathroom, run the water in the tub, place child in tub, etc. Every routine or activity has a beginning and an end. In this example, the beginning may be getting undressed and the end may be getting into P.J.’s or into bed/crib. Different caregivers may have different ways of doing an activity/routine so the steps may differ from person to person. Identifying the steps of an activity/routine seems to be the most difficult part of completing the CCIP. Use the Participation-Based Services Step-By-Step Resource Guide to find examples of activities/routines that have been broken into steps and to see if the steps written on the CCIP are really naturally occurring activity steps. Problem? Think about the steps and decide whether each step is or is not a problem. Adaptation/AT: Frequently adaptations or AT can be used to address a particular problem. For example, if washing the body is a problem, a child may be able to help or wash independently (dependent on age) by using a bath mitt instead of a washcloth. For each problem step, describe one or more adaptations/AT that might be tried. The
Page 18 of 27
Campbell/TnT-IES Participation Based Services January 2010 Page 18 of 27
Participation-Based Services Step-By-Step Resource Guide includes suggestions for adaptations/AT matched to the 12 routines (e.g., bathtime, mealtime, etc.) on the Caregiver Assessment. What the Caregiver Will Do: For each step, describe what the adult will do to help. This help may include verbal directions/reinforcement, physical guidance, placement of objects, time delay, or other child intervention strategies. What the Child Will do: Again, for each step, describe the expectations for the child. What do the adult(s) (provider and caregiver) expect that the child will be able to do (e.g., in this example, sit, wash self, or play with toys).
Tips for Writing the CCIP REMEMBER TO FOCUS ON THE STEPS (A LIST) OF AN ACTIVITY/ROUTINE AS IT
TYPCALLY OCCURS
� This does not mean directions for the caregiver (e.g., mother will lift child onto changing table; dad puts child into bumbo seat) but means the actual steps of the activity – i.e., 1) child crawls to bedroom, 2) lifted onto changing table; 3) placed onto back; ETC.)
� This is not home program instructions (e.g., during diapering, place John on back, give him a toy to play with, etc. does not mean what the child will do). This is not what the provider wants another adult or the child to do.
� It is a description of an activity/routine as it typically occurs without any intervention, structure, etc. manipulation, changing around, etc.
IDENTIFY WHETHER EACH INDIVIDUAL STEP IS OR IS NOT A PROBLEM
� When an activity/routine is not going well, individually identifying problem steps makes the “solution” easier to identify, find, or create. Only solutions need to be found for steps that are problems.
FIND ADAPTATIONS/AT TO MAKE THE IDENTIFIED PROBLEM STEP “GO WELL”
� When individual steps are identified as problems, adaptations or AT may frequently be used so that the step is no longer a problem
� Adaptations or AT are various solutions that come about by using special devices or materials, rearranging the environment, finding positioning, changing the way in which directions given to a child, using visual schedules, etc.
IDENTIFY EXPECTATIONS. WRITE DOWN WHAT THE CAREGIVER AND CHILD
WILL DO
� When an activity/routine is not going well, adaptations/AT should reduce what the caregiver needs to do. For example, in bathtime, a bath seat means that the adult does not need to hold the child in the tub.
� Adaptations/AT should also improve the child’s participation (use bath mitt to help wash self rather than hold washcloth independently)
Teaching and Reviewing with the Caregiver: Implementing the CCIP
The CCIP is a plan for the strategies that will be tried to improve an activity/routine that is not going well (or plan for embedding when activities/routines are going well).
Page 19 of 27
Campbell/TnT-IES Participation Based Services January 2010 Page 19 of 27
� The plan is implemented by the caregiver every day or whenever the
activity/routine occurs. � The provider supports the caregiver’s implementation by:
o Teaching the caregiver to use the adaptations/AT within the targeted activity/routine;
o Asking how the plan is working; o Reviewing to make sure the plan is revised when timely to do so (e.g.,
the number of supports may be reduced because less adaptation is needed; or planned adaptations are not working and others need to be tried); and
o Providing feedback, encouragement, etc. as the plan is implemented over time.
Various teaching strategies may be used to help caregivers learn to use adaptations/AT within an activity/routine that is not going well. Providers may not be able to observe the caregiver actually doing the routine but can engage in regular discussion and problem-solving to make sure that things are improving and to gage the caregivers’ expectation and degree of satisfaction.
Example Of A CCIP For Activity/Routine Not Going Well
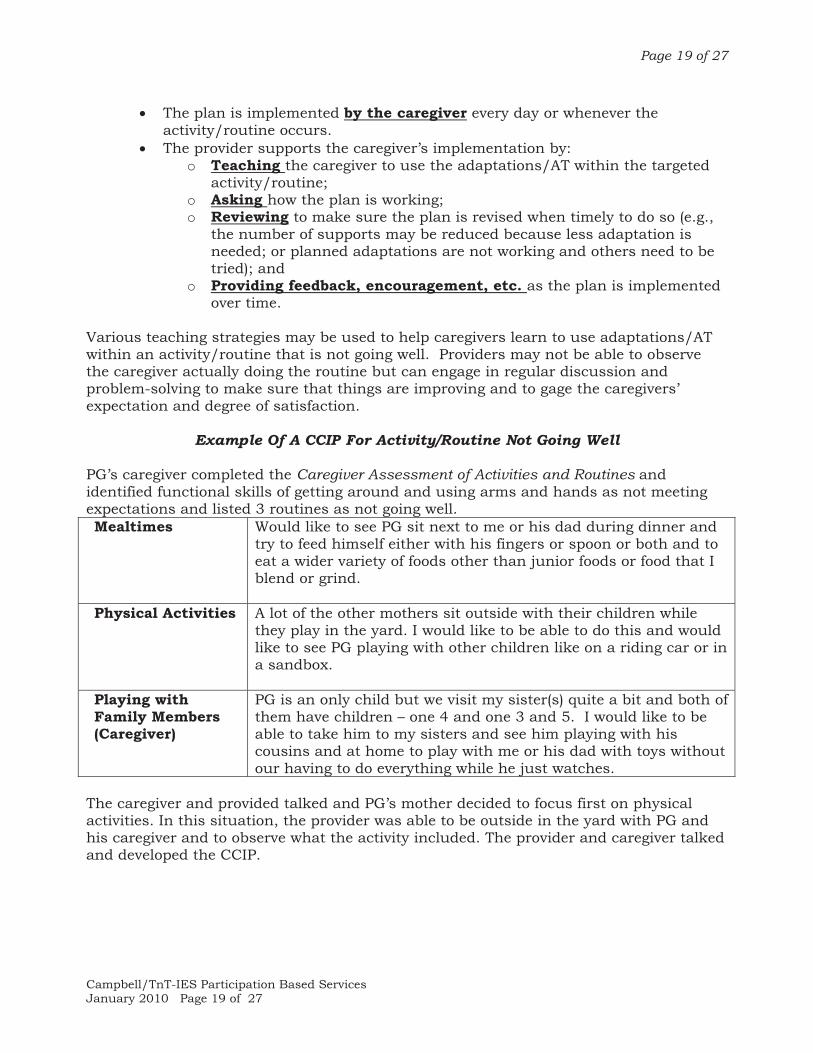
PG’s caregiver completed the Caregiver Assessment of Activities and Routines and identified functional skills of getting around and using arms and hands as not meeting expectations and listed 3 routines as not going well. Mealtimes Would like to see PG sit next to me or his dad during dinner and
try to feed himself either with his fingers or spoon or both and to eat a wider variety of foods other than junior foods or food that I blend or grind.
Physical Activities A lot of the other mothers sit outside with their children while they play in the yard. I would like to be able to do this and would like to see PG playing with other children like on a riding car or in a sandbox.
Playing with Family Members (Caregiver)
PG is an only child but we visit my sister(s) quite a bit and both of them have children – one 4 and one 3 and 5. I would like to be able to take him to my sisters and see him playing with his cousins and at home to play with me or his dad with toys without our having to do everything while he just watches.
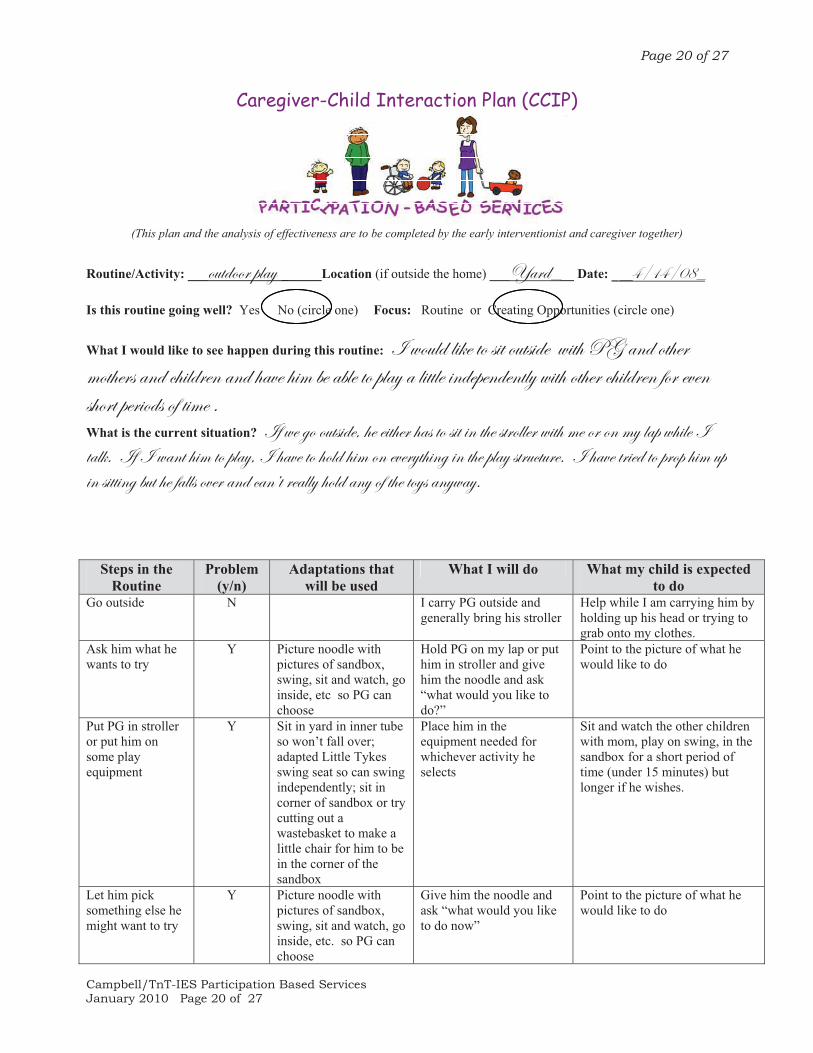
The caregiver and provided talked and PG’s mother decided to focus first on physical activities. In this situation, the provider was able to be outside in the yard with PG and his caregiver and to observe what the activity included. The provider and caregiver talked and developed the CCIP.
Page 20 of 27
Campbell/TnT-IES Participation Based Services January 2010 Page 20 of 27
Caregiver-Child Interaction Plan (CCIP)
(This plan and the analysis of effectiveness are to be completed by the early interventionist and caregiver together)
Routine/Activity: ___ÉâàwÉÉÜ ÑÄtç ______Location (if outside the home) ___ltÜwr__ Date: _rGBDGBCKr
Is this routine going well? Yes No (circle one) Focus: Routine or Creating Opportunities (circle one)
What I would like to see happen during this routine: \ ãÉâÄw Ä|~x àÉ á|à Éâàá|wx ã|à{ cZ tÇw Éà{xÜ ÅÉà{xÜá tÇw v{|ÄwÜxÇ tÇw {täx {|Å ux tuÄx àÉ ÑÄtç t Ä|ààÄx |ÇwxÑxÇwxÇàÄç ã|à{ Éà{xÜ v{|ÄwÜxÇ yÉÜ xäxÇ á{ÉÜà ÑxÜ|Éwá Éy à|Åx A What is the current situation? \y ãx zÉ Éâàá|wx? {x x|à{xÜ {tá àÉ á|à |Ç à{x áàÜÉÄÄxÜ ã|à{ Åx ÉÜ ÉÇ Åç ÄtÑ ã{|Äx \ àtÄ~A \y \ ãtÇà {|Å àÉ ÑÄtç? \ {täx àÉ {ÉÄw {|Å ÉÇ xäxÜçà{|Çz |Ç à{x ÑÄtç áàÜâvàâÜxA \ {täx àÜ|xw àÉ ÑÜÉÑ {|Å âÑ |Ç á|àà|Çz uâà {x ytÄÄá ÉäxÜ tÇw vtÇËà ÜxtÄÄç {ÉÄw tÇç Éy à{x àÉçá tÇçãtçA
Steps in the Routine
Problem(y/n)
Adaptations that will be used
What I will do What my child is expected to do
Go outside N I carry PG outside and generally bring his stroller
Help while I am carrying him by holding up his head or trying to grab onto my clothes.
Ask him what he wants to try
Y Picture noodle with pictures of sandbox, swing, sit and watch, go inside, etc so PG can choose
Hold PG on my lap or put him in stroller and give him the noodle and ask “what would you like to do?”
Point to the picture of what he would like to do
Put PG in stroller or put him on some play equipment
Y Sit in yard in inner tube so won’t fall over; adapted Little Tykes swing seat so can swing independently; sit in corner of sandbox or try cutting out a wastebasket to make a little chair for him to be in the corner of the sandbox
Place him in the equipment needed for whichever activity he selects
Sit and watch the other children with mom, play on swing, in the sandbox for a short period of time (under 15 minutes) but longer if he wishes.
Let him pick something else he might want to try
Y Picture noodle with pictures of sandbox, swing, sit and watch, go inside, etc. so PG can choose
Give him the noodle and ask “what would you like to do now”
Point to the picture of what he would like to do
Page 21 of 27
Campbell/TnT-IES Participation Based Services January 2010 Page 21 of 27
Steps in the Routine
Problem(y/n)
Adaptations that will be used
What I will do What my child is expected to do
Put him in 2nd
choice activity Y Sit in yard in inner tube
so won’t fall over; adapted Little Tykes swing seat so can swing independently; sit in corner of sandbox or try cutting out a wastebasket to make a little chair for him to be in the corner of the sandbox
Place him in the equipment needed for whichever activity he selects
Sit and watch the other children with mom, play on swing, in the sandbox for a short period of time (under 15 minutes) but longer if he wishes.
Continue choicemaking, activity sequence until it is time to go inside
Y Continue to use choice noodle for choices & positioning to enable participation
Allow him to use noodle to make choices; place him in equipment needed for whichever activity he selects
Sit and watch the other children with mom, play on swing, in the sandbox for a short period of time (under 15 minutes) but longer if he wishes.
Go Inside N Carry PG inside when we are done playing with other children
Be carried inside – helping by holding on, holding head, etc.
Note: If the routine is not going well, planning focuses on completing the routine; if the routine is going well, planning focuses on embedding learning opportunities within the routine
EMBEDDING ADAPTATIONS/AT INTO ACTIVITIES/ROUTINES
Both families and EI providers are likely to focus on developmental skills that infants and toddlers may need to learn. Caregivers may identify talking or walking or behaving better or eating independently. Many of these skills are functional –meaning that they are essential to children’s abilities to interact with their physical and social worlds and caregivers will have reported their perceptions about the extent to which children’s overall functional skills meet caregiver expectations and satisfaction. Opportunities for children to acquire developmental/functional skills are present in activities/routines that are going well and can occur systematically when opportunities are planned. There are two basic types of learning opportunities: (a) planned; (b) incidental. In planned learning opportunities, a specific opportunity to perform a particular skill is created. Children learn when multiple opportunities are provided – within one activity/routine or within many different activities/routines. Making a written plan helps the caregiver, child care provider, or adult who is with the child during the activity/routine know what to do, when to provide learning opportunities, and what types of opportunities to provide to help children to demonstrate a particular skill. Planned learning opportunities include 3 general types:
1. Practice: Skill performance without adult assistance (child is able to do something without any more help than another child of the same chronological age but needs opportunities to practice for the skill to become integrated)
2. New Learning with Adaptations/AT: Skill performance using an adaptation or AT intervention and no more adult assistance than another child of the same chronological age; AND
Page 22 of 27
Campbell/TnT-IES Participation Based Services January 2010 Page 22 of 27
3. New Learning with Adult-Provided Intervention: Skill performance with the support of specially-designed instructional strategies such as antecedent arrangements, prompts and supports, or consequences.
Incidental learning refers to opportunities that are naturally available (not specifically designed) within the activities and routines in which children participate. Incidental learning best occurs when children are interested and engaged and participating in an activity/routine. The CCIP may also be used to design planned learning opportunities and to help identify child intervention strategies to be embedded within the activity/routine learning opportunities. The same components as used to plan for improving activities/routines that are not going well are included:
� Caregiver-identification of an enjoyable activity/routine for which the CCIP will be developed and in which instructional strategies will be embedded
� Completing an analysis of the activity o Identifying which steps of the activity are a problem (should be few to none
for an activity/routine that is enjoyable and going well.] o Figuring out adaptations or assistive technology to try, as necessary o Deciding what the adult (usually the caregiver) will do during the
activity/routine including the learning opportunities to be provided and interventions to be embedded
o Outlining what the child will be expected to do � Teaching the caregiver how to implement learning opportunities/instructional
supports � Regularly reviewing the effectiveness of the intervention and trying other
adaptations, AT, or child interventions if the ones initially planned are no longer effective.
Example Of A CCIP For An Enjoyable Activity/Routine In Which Learning
Opportunities will be Provided and Specially-Designed Interventions Embedded
PG’s caregiver completed the Caregiver Assessment of Activities and Routines and identified functional skills of getting around and using arms and hands as not meeting expectations and listed 3 enjoyable activities/routines. Evening Routine He especially enjoys being read to and watching an evening DVD to
unwind from the day.
Leaving the House & Outings
Enjoys going in the car, on visits to my sisters, parents, and to places like the zoo or Children’s museum. We often go to the park, zoo, etc. with my sisters and their children and as long as he can be in his stroller, everything goes well although he participates primarily by watching/looking.
Watching TV, listening to stories
He really enjoys the children’s shows if they have a lot of music and activity. Many DVD shows are also ones he likes. He “sings along” and is very engaged. He is attentive when being read to, makes noises when asked questions about familiar stories, and tries to turn book pages.
Page 23 of 27
Campbell/TnT-IES Participation Based Services January 2010 Page 23 of 27
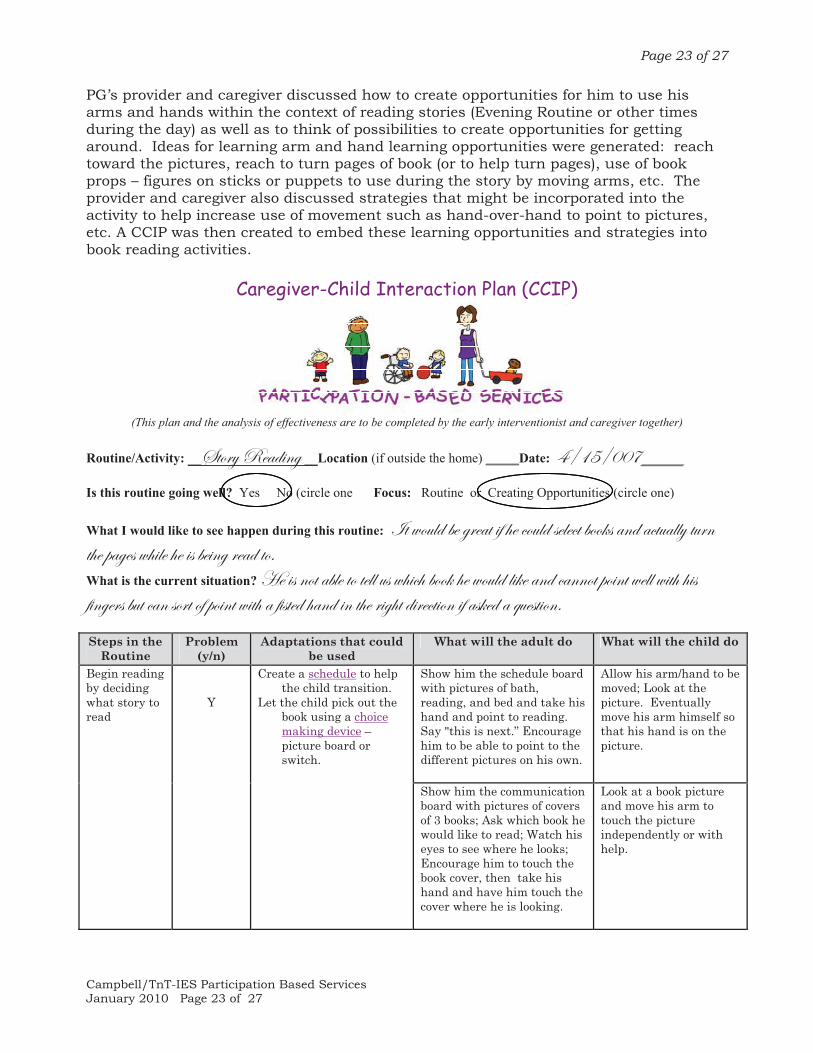
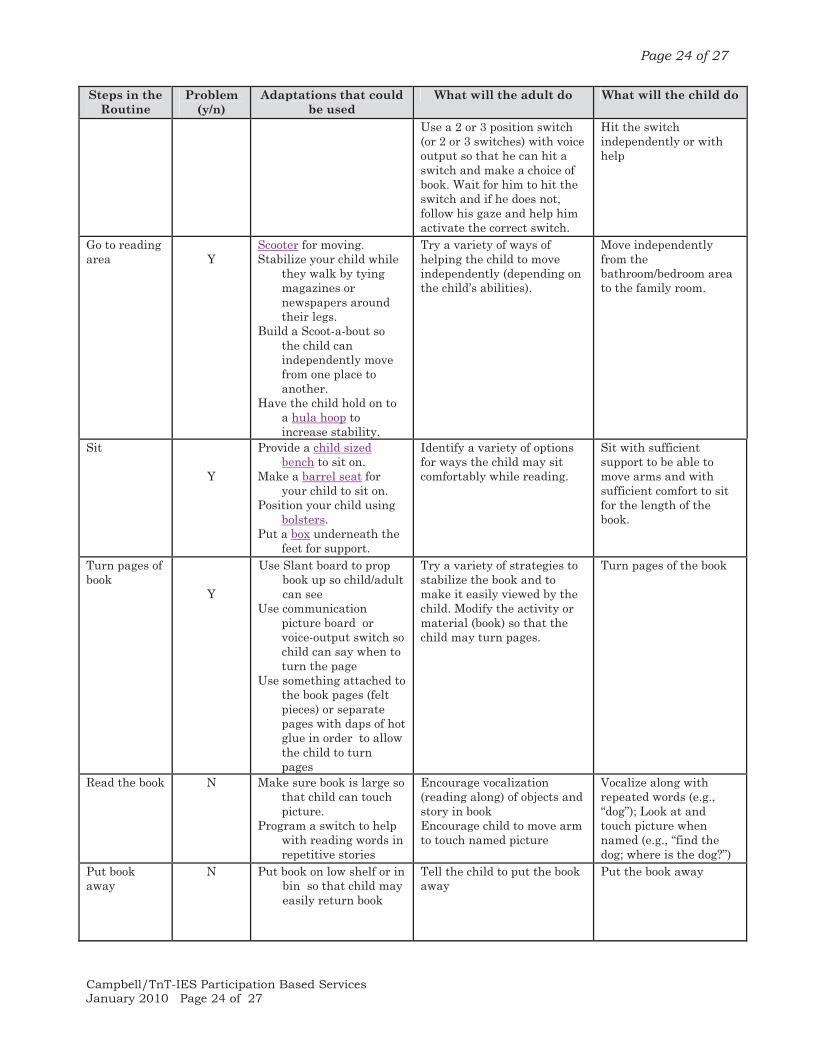
PG’s provider and caregiver discussed how to create opportunities for him to use his arms and hands within the context of reading stories (Evening Routine or other times during the day) as well as to think of possibilities to create opportunities for getting around. Ideas for learning arm and hand learning opportunities were generated: reach toward the pictures, reach to turn pages of book (or to help turn pages), use of book props – figures on sticks or puppets to use during the story by moving arms, etc. The provider and caregiver also discussed strategies that might be incorporated into the activity to help increase use of movement such as hand-over-hand to point to pictures, etc. A CCIP was then created to embed these learning opportunities and strategies into book reading activities.
Caregiver-Child Interaction Plan (CCIP)
(This plan and the analysis of effectiveness are to be completed by the early interventionist and caregiver together)
Routine/Activity: __fàÉÜç extw|Çz __Location (if outside the home) _____Date: GBDHBCCJrrrr
Is this routine going well? Yes No (circle one Focus: Routine or Creating Opportunities (circle one)
What I would like to see happen during this routine: \à ãÉâÄw ux zÜxtà |y {x vÉâÄw áxÄxvà uÉÉ~á tÇw tvàâtÄÄç àâÜÇ à{x Ñtzxá ã{|Äx {x |á ux|Çz Üxtw àÉA What is the current situation? [x |á ÇÉà tuÄx àÉ àxÄÄ âá ã{|v{ uÉÉ~ {x ãÉâÄw Ä|~x tÇw vtÇÇÉà ÑÉ|Çà ãxÄÄ ã|à{ {|á y|ÇzxÜá uâà vtÇ áÉÜà Éy ÑÉ|Çà ã|à{ t y|áàxw {tÇw |Ç à{x Ü|z{à w|Üxvà|ÉÇ |y tá~xw t Öâxáà|ÉÇA
Steps in the Routine
Problem(y/n)
Adaptations that could be used
What will the adult do What will the child do
Show him the schedule board with pictures of bath, reading, and bed and take his hand and point to reading. Say "this is next.” Encourage him to be able to point to the different pictures on his own.
Allow his arm/hand to be moved; Look at the picture. Eventually move his arm himself so that his hand is on the picture.
Begin reading by deciding what story to read
Y
Create a schedule to help the child transition.
Let the child pick out the book using a choice making device – picture board or switch.
Show him the communication board with pictures of covers of 3 books; Ask which book he would like to read; Watch his eyes to see where he looks; Encourage him to touch the book cover, then take his hand and have him touch the cover where he is looking.
Look at a book picture and move his arm to touch the picture independently or with help.
Page 24 of 27
Campbell/TnT-IES Participation Based Services January 2010 Page 24 of 27
Steps in the Routine
Problem(y/n)
Adaptations that could be used
What will the adult do What will the child do
Use a 2 or 3 position switch (or 2 or 3 switches) with voice output so that he can hit a switch and make a choice of book. Wait for him to hit the switch and if he does not, follow his gaze and help him activate the correct switch.
Hit the switch independently or with help
Go to reading area
Y
Scooter for moving.Stabilize your child while
they walk by tying magazines or newspapers around their legs.
Build a Scoot-a-bout so the child can independently move from one place to another.
Have the child hold on to a hula hoop to increase stability.
Try a variety of ways of helping the child to move independently (depending on the child’s abilities).
Move independently from the bathroom/bedroom area to the family room.
Sit Y
Provide a child sized bench to sit on.
Make a barrel seat for your child to sit on.
Position your child using bolsters.
Put a box underneath the feet for support.
Identify a variety of options for ways the child may sit comfortably while reading.
Sit with sufficient support to be able to move arms and with sufficient comfort to sit for the length of the book.
Turn pages of book
Y
Use Slant board to prop book up so child/adult can see
Use communication picture board or voice-output switch so child can say when to turn the page
Use something attached to the book pages (felt pieces) or separate pages with daps of hot glue in order to allow the child to turn pages
Try a variety of strategies to stabilize the book and to make it easily viewed by the child. Modify the activity or material (book) so that the child may turn pages.
Turn pages of the book
Read the book N Make sure book is large so that child can touch picture.
Program a switch to help with reading words in repetitive stories
Encourage vocalization (reading along) of objects and story in bookEncourage child to move arm to touch named picture
Vocalize along with repeated words (e.g., “dog”); Look at and touch picture when named (e.g., “find the dog; where is the dog?”)
Put book away
N Put book on low shelf or in bin so that child may easily return book
Tell the child to put the book away
Put the book away
Page 25 of 27
Campbell/TnT-IES Participation Based Services January 2010 Page 25 of 27
Steps in the Routine
Problem(y/n)
Adaptations that could be used
What will the adult do What will the child do
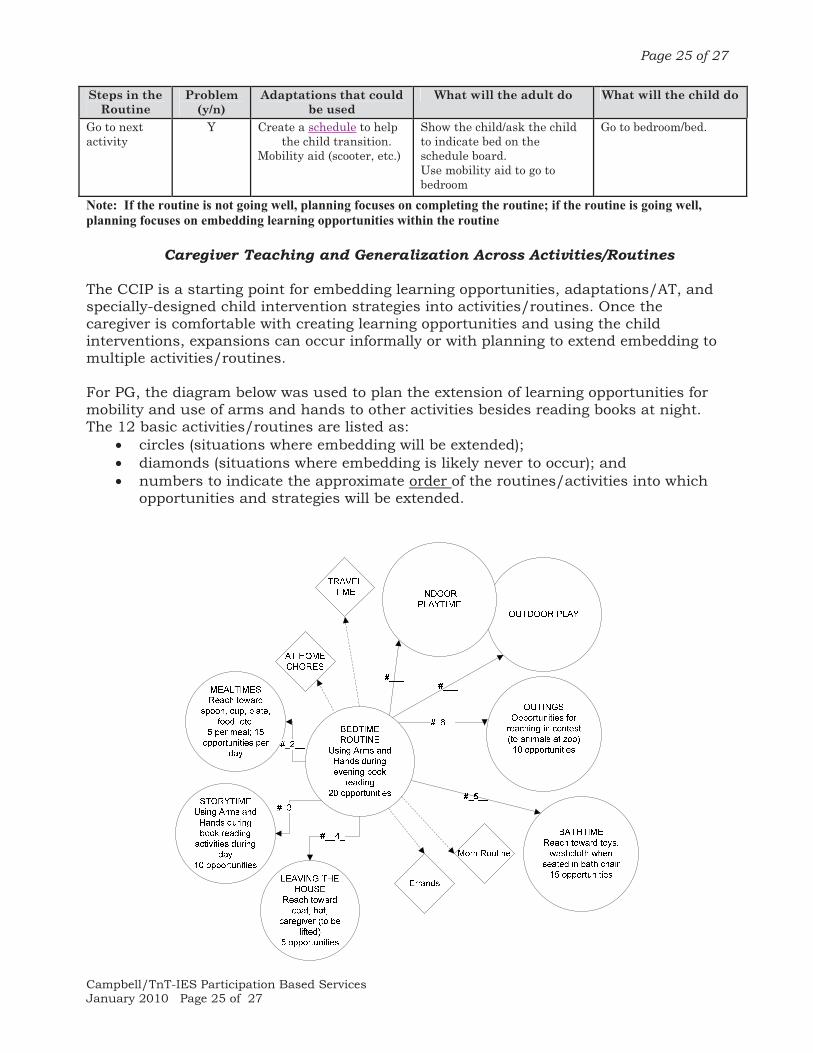
Go to next activity
Y Create a schedule to help the child transition.
Mobility aid (scooter, etc.)
Show the child/ask the child to indicate bed on the schedule board.Use mobility aid to go to bedroom
Go to bedroom/bed.
Note: If the routine is not going well, planning focuses on completing the routine; if the routine is going well, planning focuses on embedding learning opportunities within the routine
Caregiver Teaching and Generalization Across Activities/Routines
The CCIP is a starting point for embedding learning opportunities, adaptations/AT, and specially-designed child intervention strategies into activities/routines. Once the caregiver is comfortable with creating learning opportunities and using the child interventions, expansions can occur informally or with planning to extend embedding to multiple activities/routines. For PG, the diagram below was used to plan the extension of learning opportunities for mobility and use of arms and hands to other activities besides reading books at night. The 12 basic activities/routines are listed as:
� circles (situations where embedding will be extended); � diamonds (situations where embedding is likely never to occur); and � numbers to indicate the approximate order of the routines/activities into which
opportunities and strategies will be extended.
Page 26 of 27
Campbell/TnT-IES Participation Based Services January 2010 Page 26 of 27
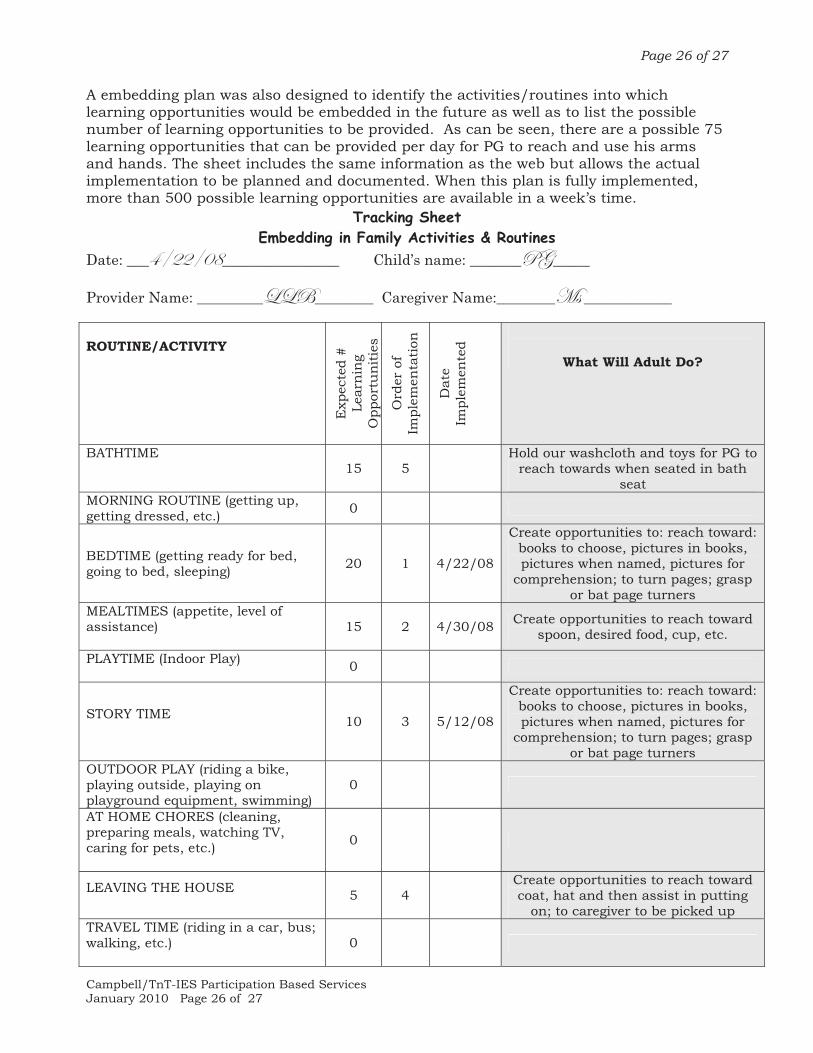
A embedding plan was also designed to identify the activities/routines into which learning opportunities would be embedded in the future as well as to list the possible number of learning opportunities to be provided. As can be seen, there are a possible 75 learning opportunities that can be provided per day for PG to reach and use his arms and hands. The sheet includes the same information as the web but allows the actual implementation to be planned and documented. When this plan is fully implemented, more than 500 possible learning opportunities are available in a week’s time.
Tracking Sheet Embedding in Family Activities & Routines
Date: ___GBEEBCK________________ Child’s name: _______cZ_____
Provider Name: ___________U________ Caregiver Name:________`á ____________
ROUTINE/ACTIVITY
Exp
ecte
d #
Le
arn
ing
Opp
ortu
nit
ies
Ord
er o
f Im
plem
enta
tion
Dat
e Im
plem
ente
d
What Will Adult Do?
BATHTIME
15 5 Hold our washcloth and toys for PG to
reach towards when seated in bath seat
MORNING ROUTINE (getting up, getting dressed, etc.) 0
BEDTIME (getting ready for bed, going to bed, sleeping) 20 1 4/22/08
Create opportunities to: reach toward: books to choose, pictures in books, pictures when named, pictures for
comprehension; to turn pages; grasp or bat page turners
MEALTIMES (appetite, level of assistance)
15 2 4/30/08 Create opportunities to reach toward spoon, desired food, cup, etc.
PLAYTIME (Indoor Play) 0
STORY TIME 10 3 5/12/08
Create opportunities to: reach toward: books to choose, pictures in books, pictures when named, pictures for
comprehension; to turn pages; grasp or bat page turners
OUTDOOR PLAY (riding a bike, playing outside, playing on playground equipment, swimming)
0
AT HOME CHORES (cleaning, preparing meals, watching TV, caring for pets, etc.)
0
LEAVING THE HOUSE 5 4
Create opportunities to reach toward coat, hat and then assist in putting
on; to caregiver to be picked up TRAVEL TIME (riding in a car, bus; walking, etc.)
0
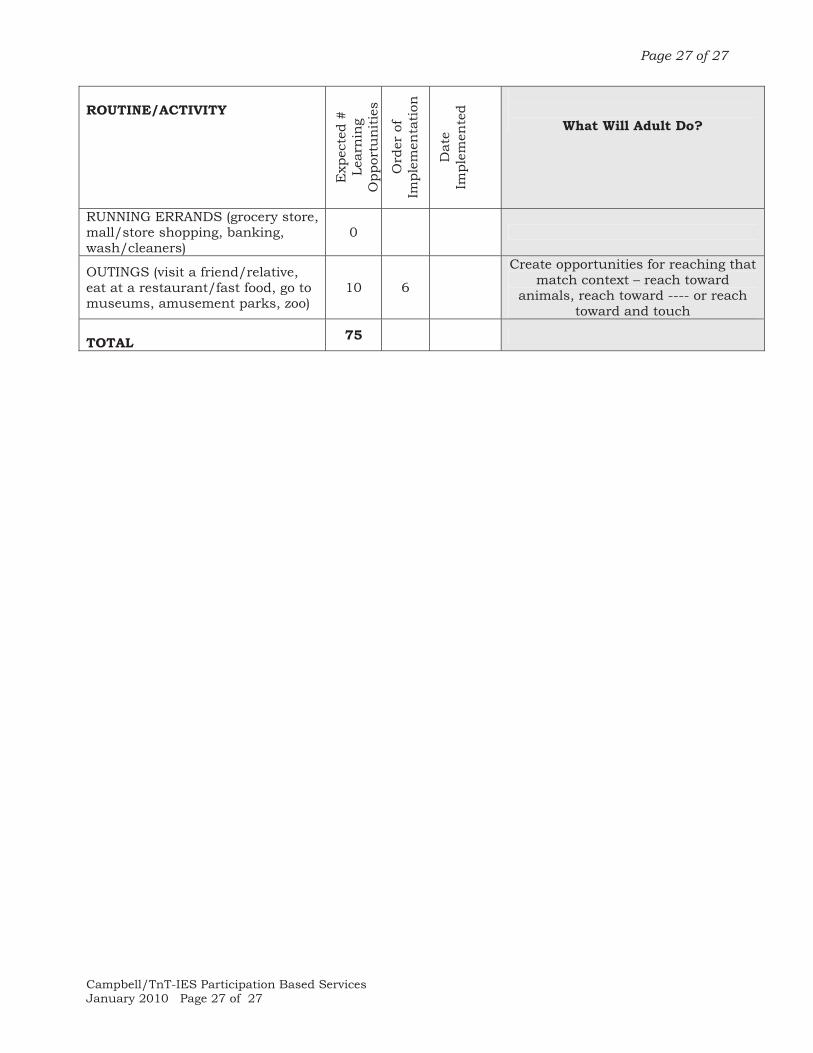
Page 27 of 27
Campbell/TnT-IES Participation Based Services January 2010 Page 27 of 27
ROUTINE/ACTIVITY
Exp
ecte
d #
Le
arn
ing
Opp
ortu
nit
ies
Ord
er o
f Im
plem
enta
tion
Dat
e Im
plem
ente
d
What Will Adult Do?
RUNNING ERRANDS (grocery store, mall/store shopping, banking, wash/cleaners)
0
OUTINGS (visit a friend/relative, eat at a restaurant/fast food, go to museums, amusement parks, zoo)
10 6
Create opportunities for reaching that match context – reach toward
animals, reach toward ---- or reach toward and touch
TOTAL 75