Embed Size (px)
Citation preview

THE AMERICAN JOURNAL OF CANCER
A Continuation of The Journal of Cancer Research ______ ~
-. ~ _ _ ~
VOLUME XXVII AUGIJST, 1936 NUMBER 4
ADENOCARCINOMA OF T H E CERVIX
A STUDY OF FORTY-THREE CASES
CHARLES C. NORRTS, M D
(Froin t h c Di’fiurLiuent of Ohstetrir\ and Gvtm-ology and the Gyizcccnn Ho\pztd Instit14te o] Gynernlogzr Retcurrh, linzverczty of Pennsylvania)
The history of carcinoma of the cervix is closely interwoven with the history of radium. Prior to the discovery of radium in 1898, gynecologic pathologists were generally dependent upon classification of this disease into two types : the epidermoid (epithelioma) or squamous-cell carcinoma and the adenocarcinoma or glandular form of cancer. Since that time, the treat- ment of cervical carcinoma by operative measures has gradually but steadily been replaced by irradiation, until to-day radiotherapy has become the recog- nized method of treatment in most clinics. With the employment of radium and the roentgen rays in the treatment of cervical carcinoma have come in- tensive studies of the radiosensitivity and radioresistance of the various forms of carcinoma of the cervix, Such studies have resulted in many new and more detailed classifications. Even in those days in which surgery was the only recognized method of treatment, the opinion was more or less general that adenocarcinomata were less amenable to surgical measures than were those tumors that had their origin in the stratified squamous epithelium. TO- day much difference of opinion still exists regarding the relative malignancy and radiosensitivity of these two main groups of cervical carcinomata.
Madruzza ( 1 ) asserts that Adler’s statistics show that adenocarcinomata of the uterine cervix, when treated with radium and the roentgen ray, have a less favorable prognosis than have epitheliomata of the same region. Doder- lein (25) formerly attributed this to the greater radioresistance of the adeno- carcinomata. Of Philipp’s 11 cases of adenocarcinomata, including 4 in Stages I and 11, none reached the five-year limit. Wintz (35) reported 47 per cent of five-year salvage in a series of 32 cases. Nilsson (2), of the Radiunihenimet in Stockholm, had a five-year salvage in 19.23 per cent of a series of 26 cases treated from 1916 to 1925. During the same period, the same observer secured 2 1.34 per cent of salvage for cervical cancer in general,
653
0% CIIARLES C. NORRIS
including epithelioniata and adenocarcinomata. Nilsson believes that the adenocarcinomata are as radiosensitive as are the epitheliomata. In a more recent communication ( 3 ) he reports 23 per cent five-year salvage in a series of 80 primary adenocarcinomata observed from 1916 to 1932. About half of these cases were operable, and in this group there was 35 per cent salvage,
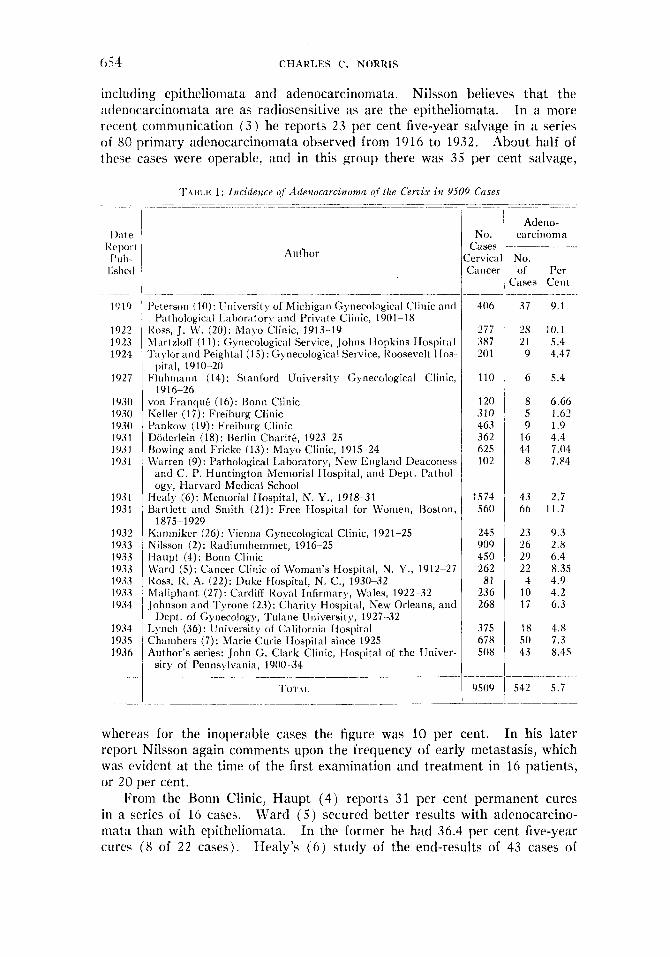
T.,\nr.a I : Incidence of Adenocarcinonza (if ilze Cervix in 9509 Cuses
1).1te IZep(1I I I’ub lishctl
_ _ _ - ~
1910
1922 1923 1924
1927
1930 1030 1 0 3 0 19.3 1 193 1 19.31
1 OJ 1 19.3 I
1932 1933 1933 1933 1933 1933 1934
1934 1935 1936
-- _.
I’rterson (10): IJniversit), of Michigan (;ynecological Clinic and
I<oss, J. M‘. (20): Mayo Clinic, 1913-19 Martzloff (1 1): Gynecological Service, Johns I Iopkiris Hospital Taylor and Peightal (15) : Gynecological Service, lbosevelt Hos-
Fluhinann (14): Stanford University Gynecological Clinic,
voii Franqui. (16): Hoiiii Clinic Keller (17): Freihurg Clinic I’aiikow (19): Freiburg Clinic 1)iitlerlein (18): Berlin Chariti., 1923- 25 Howing and Fricke (1.3): Mayo Clinic, 1915~-24 LVarren (9): Pathological laboratory, New England Deaconess
and C. P. Huntington Memorial I Iospital, and Dept. Pathol- ogy, fiarvard Medical School
1% t holog ica I 1.a hora t or !, and Private CI i 11 ic, 1 90 1 - 1 8
I ) i t al , 19 10-20
191 6-26
fiealy (6): Meniorial IIospital, N. Y., 1918-31 Bartlett and Smith (21) : Free Ilospital for Women, Boston,
I<aniniker (26): Vienna Gynecological Clinic, 1921-25 Nilsson (2): I<adiunihemniet, 1916~-25 I-Iaupt (4): Bonn Clinic C\’ard (5): Cancer Clinic of Woman’s flospital, N. Y., 1912-27 I ~ O S S , R. A. (22): Duke IIospital, N. C., 1930-32 Maliphant (27): Cardiff Royal Infirmary, Wales, 1922--32 Johnson and Tyrone (23): Charity Hospital, New Orleans, ant1
Lynch (36): University of California Hospital Ch;tinbers (7) : Marie Curie Hospital since 1925 Author’s series: John G. Clark Clinic, Hospital of the liniver-
1875 1929
Dept. of Gynecology, Tularte University, 1927-32
sity of Pennsylvania, 1900--34
-
NO. Cases krvica Cancer
406
277 387 20 1
110
120 310 463 362 625 102
1574 560
245 909 450 262 81
236 268
375 678 508
9509 -
Atleno- carcinoma
No. of Per
Cases Cent
37 9.1
28 10.1 21 5.4 9 4.47
6 5.4
8 6.66 5 1.6‘2 9 1.9
16 4.4 44 7.04 8 7.84
43 2.7 66 11.7
23 9.3 26 2.8 29 6.4 22 8.35 4 4.9
10 4.2 1 7 6.3
18 4.8 50 7.3 43 8.45
542 5.7
whereas for the inoperable cases the figure was 10 per cent. In his later report Nilsson again comments upon the frequency of early metastasis, which was evident a t the time of the first examination and treatment in 16 patients, or 20 per cent.
I+om the Bonn Clinic, Haupt (4) reports 31 per cent permanent cures in a series of 16 cases. Ward ( 5 ) secured better results with adenocarcino- mata than with epitheliomata. In the former he had 36.4 per cent five-year cures (8 of 2 2 cases). Healy’s ( 6 ) study of the end-results of 43 cases of
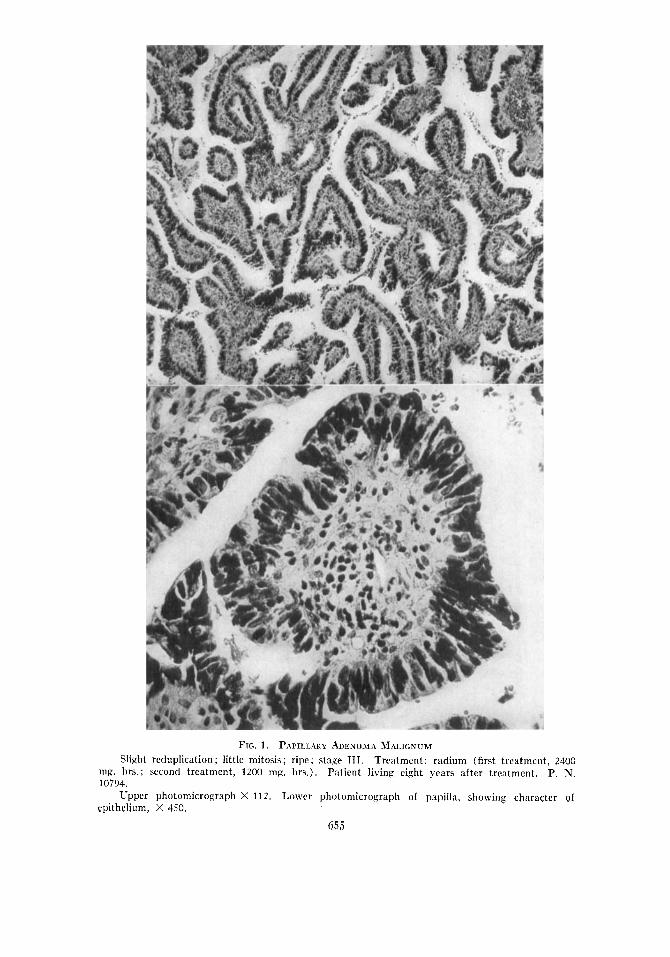
FIG. 1. PAPILLARY ADENOMA MALIGNUM Slight reduplication ; little mitosis; ripe ; stage 111. Treatment: radium (first treatment, 2400
Patient living eight years after treatment. P. N.
Upper photomicrograph X 112. Lower photomicrograph of papilla, showing character of
mg. hrs.; second treatment, 1200 mg. hrs.). 10794.
epithrlium, X 450.
655
656 CHARLES C. NORRIS
adenocarcinomata does not support the view that adenocarcinoma is more resistant to irradiation than is epithelioma, for of this series 9 (20.93 per cent) survived for five years. Chambers (7) , of the Marie Curie Hospital, found no evidence that adenocarcinoniata were insensitive to radiation.
FREQUENCY Adenocarcinoma of the cervix is relatively infrequent. The incidence as
Of the 9,509 cases of cervical reported in various series is given in Table I . carcinomata in these combined series 5.7 per cent were adenocarcinomata.
MACROSCOPIC PATHOLOGY The gross appearance of adenocarcinoma of the cervix is similar to that
of the more common epidermoid type, and the tumor cannot, as a rule, be differentiated from the latter without the aid of the microscope. I n the early stages the site of origin may be suggestive, but this is by no means a certain guide.
Adenocarcinoma may develop-(1 j from the portio; ( 2 ) from the cervical canal; ( 3 ) from the glandular epithelium in the intramural portion of the cervix; (4) from epithelial rests. Growths having their origin in the portio niay be ( a ) ulcerative, ( b ) papillary, ( c ) nodular, or ( d ) diffuse. Neoplasms springing from the cervical canal may be of similar types. I n the latter location the papillary type is prone to be flattened as a result of pressure. .In annular form is occasionally observed. Disc-like tumors, with or without preservation of the portio, are also encountered. During the advanced stage d l types tend to become ulcerative.
Those tumors springing from the intramural portion of the cervix (sub- surface epithelium) are prone to be one, of two types. ( a ) Neoplasms of the first type have their origin in the depths of a cervical gland. In the early stages such a tumor is likely to be mistaken for a nabothian cyst or a small cervical fibroma. This nodular-like variety finally invades either the canal or the portio, and until such erosion occurs the condition is practically free from symptoms and as a consequence may be far advanced before either hemorrhage or discharge develops. Fortunately this type is infrequent. ( 6 ) ‘The second type is a diffuse variety, in which almost the entire cervix appears to be involved simultaneously. The cervix is enlarged and softened, the investing epithelium is reddened and congested, and may exhibit engorged capillaries. Upon being lightly rubbed with a gauze sponge the surface may exude a little blood, but no ulcer or papilloma is observable macroscopically until the disease is in an advanced stage. The entire cervix is almost brain- like in consistency, and the tenaculum will cut through it with slight traction. The tissue is so friable that a biopsy specimen can easily be scooped out from dmost any area with a curet. These tumors apparently have their origin in the sub-surface epithelium, and under the microscope are usually highly un- differentiated. The chief feature of this variety of neoplasm is the diffuse, widespread invasion without macroscopic ulceration or papilloma upon the surface, together with great friability and vascularity of the entire cervix, the general shape of the organ being preserved or slightly flattened.
I1 P.
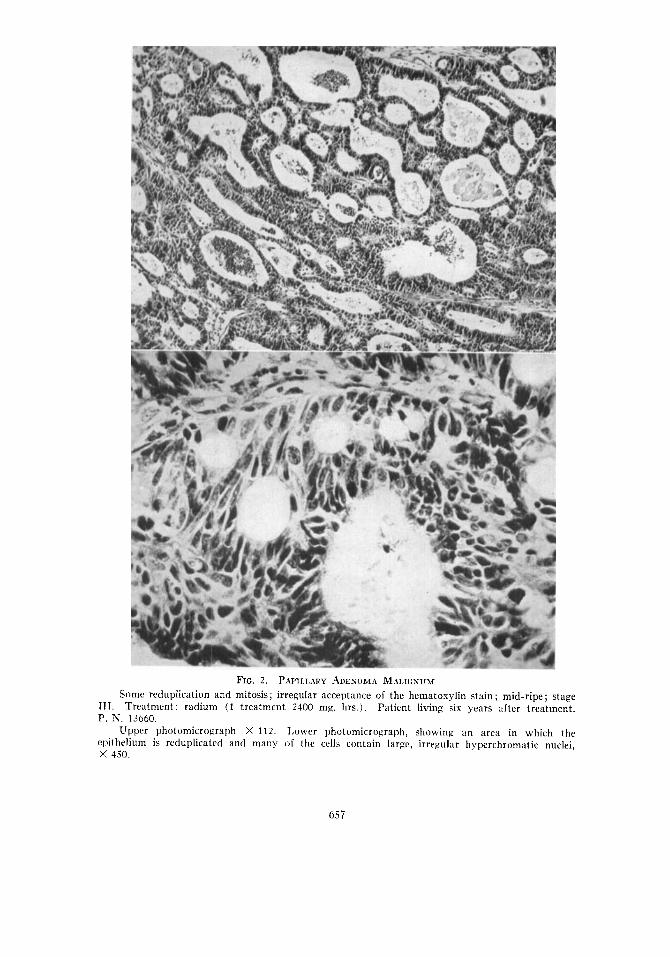
FIG. 2 . PAPILLARY ADEXOMA MALICNUM Some reduplication and mitosis; irregular acceptance of the hematoaylin stain ; mid-ripe ; stage
Patient living six years after treatment.
Upper photomicroaraph X 112. Lower photomicrograph, showing an area in which the iithelium is reduplicated and many of the cells contain larac, irregular hyperchromatic nuclei,
I. Treatment: radium (1 treatment 2400 ma. hrs.). N. 1.3660.
4.50.
65 7
65 8 CHARLES C. NORRIS
Nilsson ( 2 ) divides the adenocarcinomata into the following types: ( 1) typical endocervical growth with preserved portio contour; ( 2 ) diffuse infil- tration without cavity formation, the portio being enlarged, and with flat- tened vaginal surface (endocervical) ; (3 ) partial portio cervical infiltration ( apparently sub-epithelial) , and eventually visible ulcerations and crater formation, the configuration of the portio being preserved more or less; ( 4 ) disc-like tumor with preserved portio contour; ( 5 ) disc-like tumor with ob- literated portio contour; ( 6 ) disc-like tumor with crater and partially pre- served portio contour; ( 7 ) typical exophytic tumor.
HISTOLOGIC P A T H O L O G Y
Schottlaender and Kermauner (29) and others make the following clas- sification of adenocarcinoma of the cervix: ( a ) ripe, ( 6 ) mid-ripe, ( c ) un- ripe, according to the amount of differentiation present. This classification is useful in that, to some extent a t least, it tends to determine the relative malignancy and perhaps also the radiosensitivity of the various neoplasms.
Nilsson ( 2 ) classifies the adenocarcinomata into six groups : ( 1) papil- lomatous adenocarcinoma; ( 2 ) adenoma nialignum; ( 3 ) highly differentiated adenocarcinoma; ( 4 ) slightly differentiated adenocarcinoma (one-quarter solid) ; ( 5 ) adenocarcinoma with pavement epithelium differentiation; (6) partially solid adenocarcinoma ( more than one-fourth solid). H e points out that this classification would naturally be divided into two parts, one includ- ing groups 1, 2 , 3 and 4, and the other groups 5 and 6.
At first glance Nilsson’s classification may appear to be somewhat coni- plicated. The fact is, however, that adenocarcinoma of the cervix presents perhaps more histologic types than does any other malignant tumor that in- volves the female genital tract. Furthermore, many gradations exist between the different types. In passing, it may be stated that such classifications are prone to result in small groups, and when these are subdivided further, ac- cording to stages of advancement and different methods of treatment, a caniparison of relative malignancy and radiosensitivity becomes extremely dificult because of the sinall number of cases in each series.
The differentiation between the epidermoid neoplasm and adenocarcinoma is usually a simple matter for the experienced gynecologic pathologist; but the varying proportions of these two varieties reported from different clinics are an indication that this is not uniformly the case. Thus Bartlett and Smith ( 2 1 ) record 11.7 per cent of adenocarcinonia ainong 560 cases of carcinoma of the cervix, whereas Pankow (19), from the Freiburg clinic, found only 1.9 per cent among 463 cases.
I n reviewing our series of cases we have been impressed with the fact that in some neoplasms gland-like areas have been observed at one point, whereas in another area a somewhat typical epidermoid-like architecture may be found. Other tumors present intermediate types that cannot be classified with cer- tainty. In this connection Martzloff’s (30) experience is significant. He examined 70 whole specimens of cervical epidermoid carcinoma removed by hysterectomy and compared his findings with those secured by biopsy. He discovered that in about one-third of the cases the biopsy material was insuf-
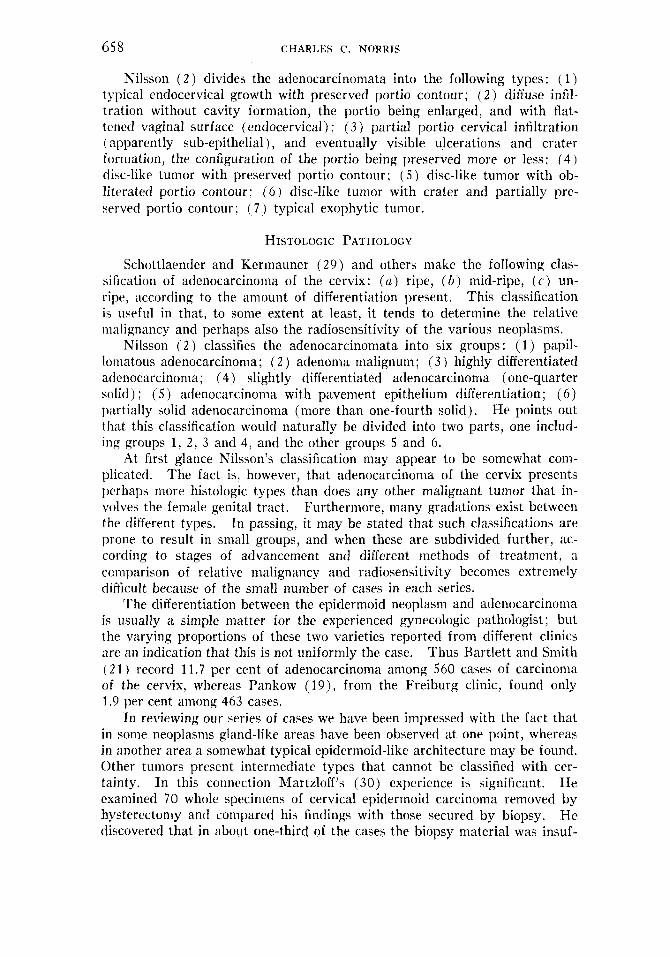
F I G . 3 . ADEXOCARCINOMA
Small Rlands ; considerable reduplication and marked penetration ; moderate amount of mi- tosis ; predominance of large cells; mid-ripe to unripe ; stage IV. Treatment: palliative radium (1 treatment, 1500 ma. hrs.).
Uppcr photomicrograph X 112. Lower photomicrograph, showing penetration, irregularity of cells, hyprrchromatosis, mitotic figures, and hydrops of certain cells, X 450.
Tenure of life, four months. P. N. 10136.
659
600 CHARLES C. NORRIS
ficient in quantity to permit definite conclusions to be drawn regarding the predominating type of cell and accurate classification was therefore impos- ~ i b l c . Martzloff’s study demonstrates the difficulty sometimes encountered i n accurate diagnosis in those cases in which only a small amount of tissue is available, and the variations which occur in different areas in the same
Regaud and Gricouroff (31) believe that many of the doubtful cases of tJpidermoid carcinomata that possess a gland-like structure are derived from the epithelium of the cervical canal, without preliminary epidermoid meta- plasia, and they suggest for this group the term pseudo-epidermoids of cervicel origin.
neoplasms,
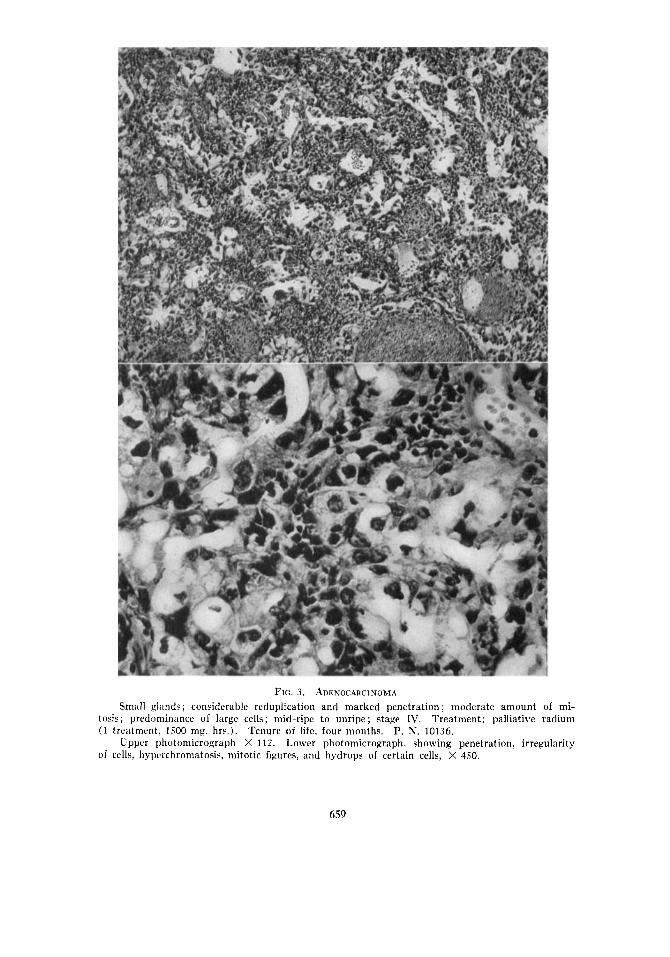
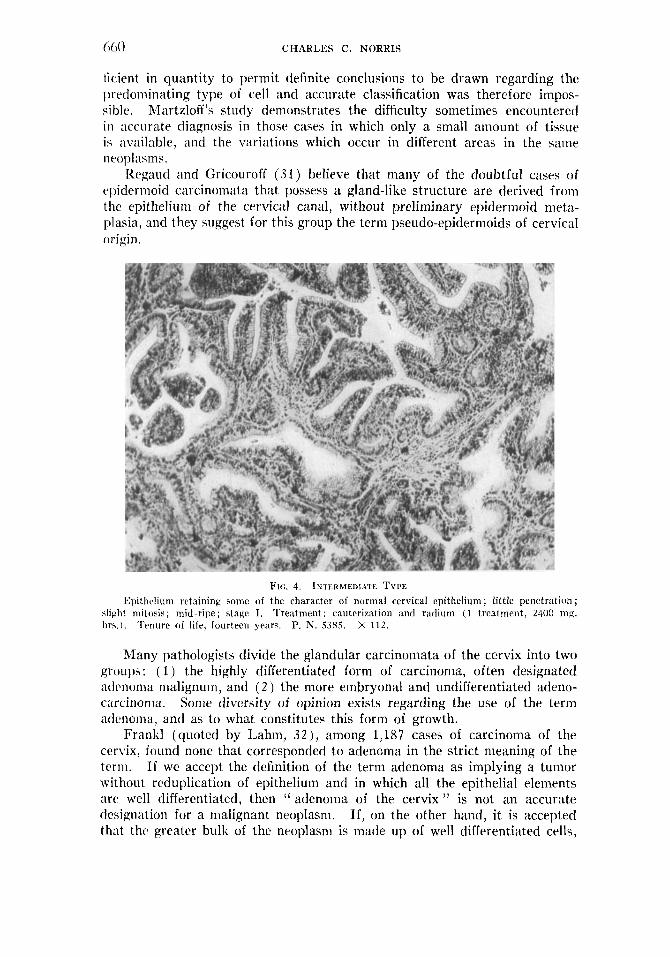
FIG. 4. INTERMEDIATE TYPE Epithelium retaining some of the character of normal cervical epithelium ; little penetration ;
slight mitosis; mid-ripe; stage I. Treatment: cautcrization and radium (1 treatment, 2400 mg. hrx . ) . Tcnure of life, fourteen years. P. N. S.<85. X 112.
Many pathologists divide the glandular carcinomata of the cervix into two groups : ( 1 ) the highly differentiated form of carcinoma, often designated :idenonia nialignum, and ( 2 ) the more embryonal and undifferentiated adeno- carcinoma. Some diversity of opinion exists regarding the use of the term ~denonia , and as to what constitutes this form of growth.
Frank1 (quoted by Lahm, 32), among 1,187 cases of carcinoma of the cervix, found none that corresponded to adenoma in the strict meaning of the term. If we accept the definition of the term adenoma as implying a tumor without reduplication of epithelium and in which all the epithelial elements arc well differentiated, then ( ‘ adenoma of the cervix ” is not an accurate tlehignation for a malignant neoplasm. If, on the other hand, it is accepted that the greater bulk of the neoplasm is made up of well differentiated cells,
ADENOCARCINOMA OF T H E CERVIX 66 1
with but little reduplication or penetration, quite a high proportion of such tumors will be found. These neoplasms are usually of relatively slow growth, display slower metastasizing characteristics, and are generally less malignant than are those of the form known as adenocarcinoma. For this reason, therefore, the division into the two types of growth seems to be a useful one.
The classifying of the tumor according to the degree of differentiation, however, as is preferred by Healy and Cutler (24) and others, in general answers the same purpose. An accurate classification of glandular carcino- mata is somewhat more difficult than that of the epidermoid cancers.
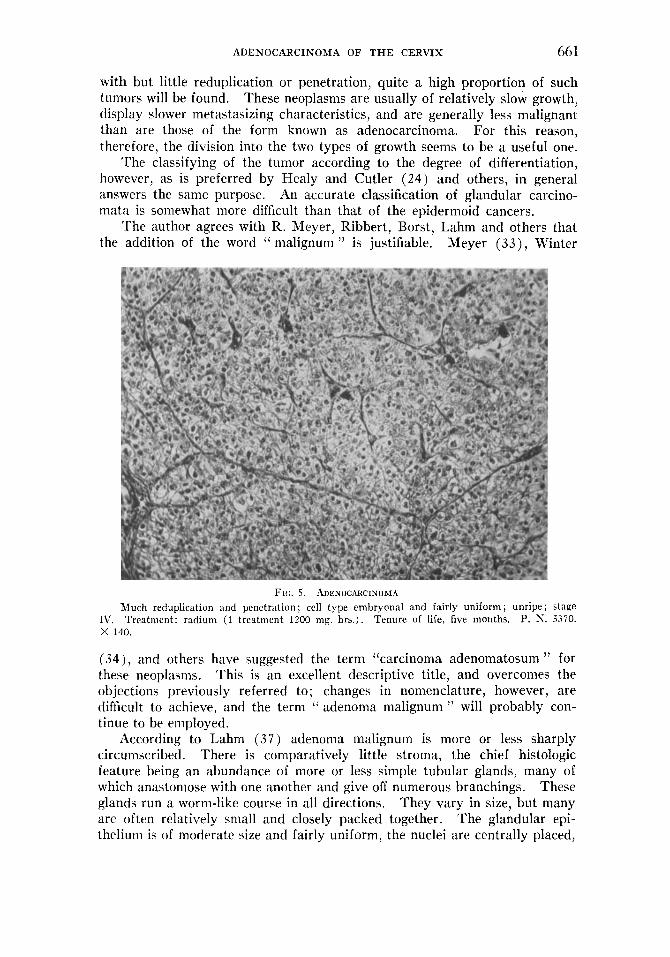
The author agrees with R. Meyer, Ribbert, Borst, Lahm and others that the addition of the word “ malignum ” is justifiable. Meyer ( 3 3 ) , Winter
FIG. 5 . ADENOCARCINOMA Much reduplication and penetration; cell type embryonal and fairly uniform; unripe; stage
P. N. 5.370. IV. X 140.
Treatment: radium (1 treatment 1200 mg. hrs.). Tenure of life, five months.
(34), and others have suggested the term “carcinoma adenomatosum ” for these neoplasms. This is an excellent descriptive title, and overcomes the objections previously referred to; changes in nomenclature, however, are difficult to achieve, and the term ‘‘ adenoma malignum ” will probably con- tinue to be employed.
According to Lahm (37) adenoma malignum is more or less sharply circumscribed. There is comparatively little stroma, the chief histologic feature being an abundance of more or less simple tubular glands, many of which anastomose with one another and give off numerous branchings. These glands run a worm-like course in all directions. They vary in size, but many are often relatively small and closely packed together. The glandular epi- thelium is of moderate size and fairly uniform, the nuclei are centrally placed,
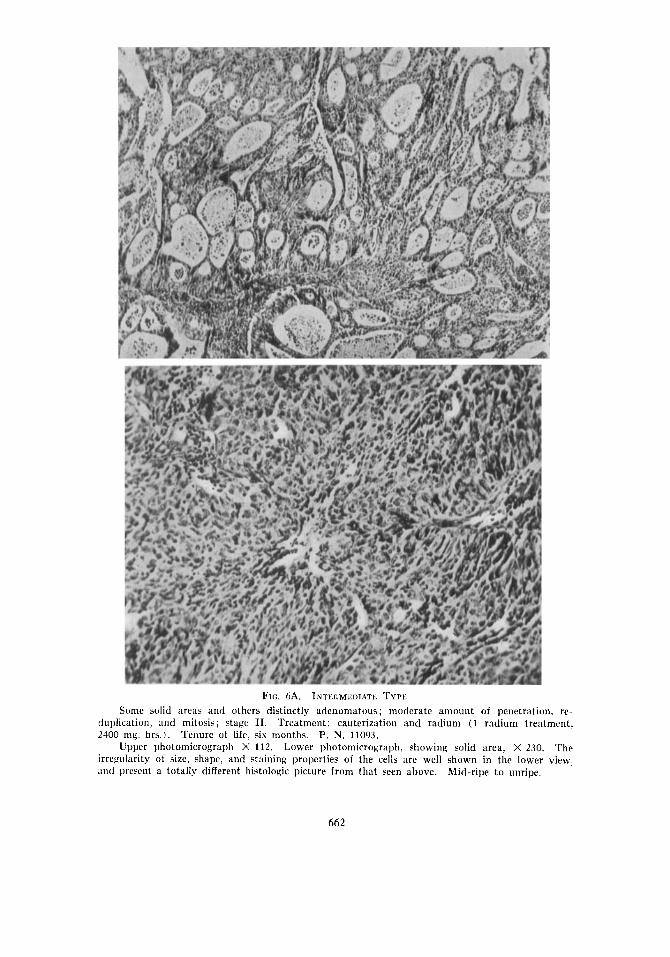
Fro. 6A. INTEI;MI:DIATE TYPE Some solid itreas and others distinctly adenomatous; moderate amount of penetration, rc-
duplication, and mitosis; stage 11. Treatment: cauterization and radium ( 1 radium treatment, 2400 nig. hrs.). Tenure of life, six months. P. N. 11093.
Upper photomicrograph X 112. Lower photomicrograph, showing solid area, X 230. The irregularity of size, shape, and staining properties of the cells are well shown in the lower view. and present a totally different histologic picture frnm that seen above. Mid-ripe to unripe.
662
ADENOCARCINOMA O F THE CERVIX 663
rich in chromatin, and take the hematoxylin stain deeply. Mitotic figures, although present, are infrequent as compared to the number found in the more embryonic adenocarcinomata. The cell protoplasm is often finely granular, and may be partially or wholly replaced by a secretion (" carci- noma gelatinosum "), which may fill the entire cell. The investing epithelium of the glands possesses few of the characteristics of malignancy and is gen- erally moderately well differentiated. Penetration of the basement membrane is infrequent. A careful search will, however, usually reveal areas exhibiting penetration or, even more commonly, cytologic changes characteristic of carcinoma.
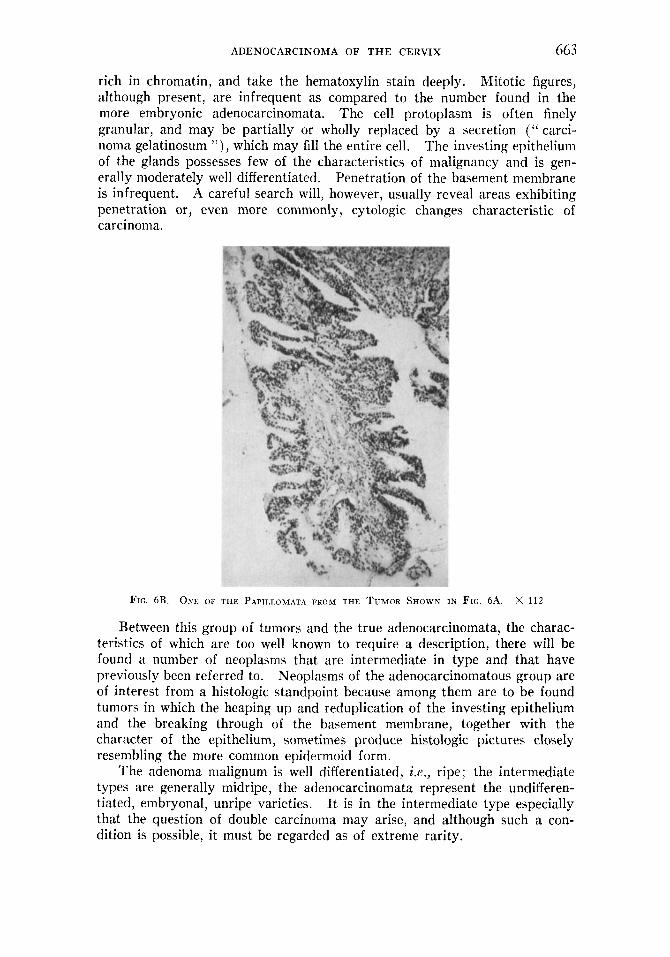
FIG. 6B ONE or THE PAPIIIOMATA FROM THE TUMOR SHOWN IN F I G 6A. x 112
Between this group of tumors and the true adenocarcinomata, the charac- teristics of which are too well known to require a description, there will be found a number of neoplasms that are intermediate in type and that have previously been referred to. Neoplasms of the adenocarcinomatous group are of interest from a histologic standpoint because among them are to be found tumors in which the heaping up and reduplication of the investing epithelium and the breaking through of the basement membrane, together with the character of the epithelium, sometimes produce histologic pictures closely resembling the more common epidermoid form.
The adenoma malignum is well differentiated, ix., ripe; the intermediate types are generally midripe, the adenocarcinomata represent the undifferen- tiated, embryonal, unripe varieties. I t is in the intermediate type especially that the question of double carcinoma may arise, and although such a con- dition is possible, it must be regarded as of extreme rarity.
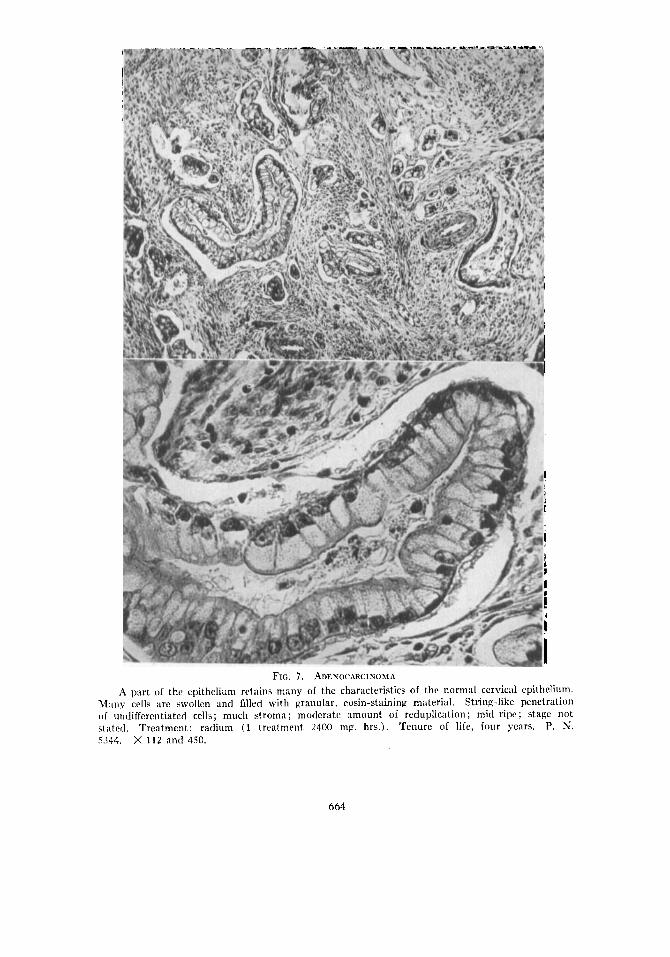
FIG. 7 . ADENOCARCINOMA A part of the epithelium retains many of the characteristics of the normal cervical epitheli
M m y cells are swollen and Glled with granular, eosin-staining material. String-like penetra of undifferentiated cells; much stroma ; moderate amount of reduplication ; mid-ripe ; stage stated. Treatment: radium (1 treatment 2400 mg hrs.). Tenure of life, four years. P. 5144. X 112 and 450.
um. tion not N.
664
ADENOCARCINOMA OF THE CERVIX 665
The proportion of mitotic figures that are present is perhaps the most valuable single histologic factor on which to judge the degree of malignancy, and is also probably important in determining the radiosensitivity, although many other factors enter into the latter criterion.
CLINICAL FEATURES
The following study includes all those cases of adenocarcinoma of the cervix that have been verified by histologic examination in the Gynecologic Service of the Department of Obstetrics and Gynecology, Hospital of the
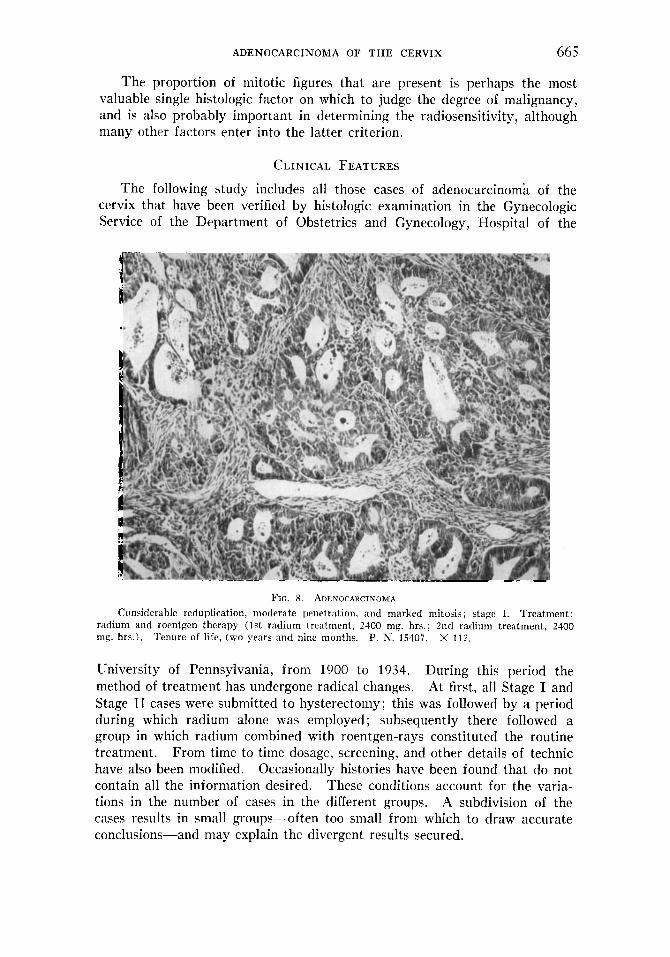
FIG. 8. ADLNOCARCINOMA Treatment:
radium and roentgen therapy (1st radium treatment, 2400 mg. hrs.; 2nd radium treatment, 2400 mg. hrs.). Tenure of life, two years and nine months. P. N. 15407. X 112.
Considerable reduplication, moderate penetration, and marked mitosis ; stage I.
University of Pennsylvania, from 1900 to 1934. During this period the method of treatment has undergone radical changes. At first, all Stage I and Stage I1 cases were submitted to hysterectomy; this was followed by a period during which radium alone was employed; subsequently there followed a group in which radium combined with roentgen-rays constituted the routine treatment. From time to time dosage, screening, and other details of technic have also been modified. Occasionally histories have been found that do not contain all the information desired. These conditions account for the varia- tions in the number of cases in the different groups. A subdivision of the cases results in small groups-often too small from which to draw accurate conclusions-and may explain the divergent results secured.
006 CHARLES C. NORRIS
Ihr ing the earlier period covered by this series the follow-up was not so strict nor efficient as it is at present, and this, combined with the fact that some of these cases were treated thirty-four years ago, adds to the difficulty of securing a satisfactory report of the end-results.
Forty-three cases of adenocarcinonia of the cervix form the basis for this study. The histologic study is based chiefly upon biopsy specimens, which adds still further to the difficulty of reaching accurate conclusions. A con- siderable number of tumors that apparently had their origin at the cervico- uterine junction were observed. Because of the doubtful origin of these neoplasms, these cases have been excluded from this series.
T.\I<LK I I : h!!arilal History iii 4.7 Cusrs oJ Adenocarcinoma 0.f the Cervix
Marr ied . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 34 (79.08%)
\i’iciow . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4 (9.3%) Not stated . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1 (2 .32%)
Single . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4 (9.3%)
The proportion of white to colored patients (Table 111) corresponds moderately accurately to the proportion of negro patients admitted to the service as a whole and suggests that race plays no particular part in the development of this tumor.
1 . u i t . r c 111: Race in 4.7 Cases of Adenocarcinonia of the Cervix
\2‘hite . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 39 (90.7%) Coloretl.. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2 (4.65%) Not stated . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2 (4.65%)
Eighty per cent of patients had been pregnant or had been submitted to some form of cervical operation prior to the development of the carcinoma (Tables IV and V ) .
T.\mi< IV: Prepzaricies in 4.1 Cases of Adenocarcinoma of the Cervix
Number of patients who had been pregnant . . . . . . . . . . . . . . . . . . 33 (76.74%) Niinrlm oT full-teriu pregnancies. . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31 (72.1%) Numher \vho have had aliortions or miscarriages, I)ut IIO full-teriii
pregnancies.. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2 ( 4.65%) I’atients who were never pregnant . . . . . . . . . . . . . . . . . . . . . . . . . . . 9 (20.93y0)
Average nunlher of pregnancies ainong those who have been pregnant . . 3.8 Nuniher of pregliartcies not stated, . . . . . . . . . . . .
T \ i i i , t % V: Data o n Preoious Operations ivi 4.7 Cases (!f Adeiiocarciizowia of the Cervix
No previous operat ions upon the cervix . . . . . . . . . . . . . . . . . . . . . . 36 (83.73’11,) I’revious operations not stated . . . . . . . . . . . . . . . . . . . . . . . . . . 3 (6.98%) I’revious supracervical hysterectomy. . . . . . . . . . . . . . . . . . . . . . . . . 1 (2 .32%) I’revious cauterization for existing carcinoma . . . . . . . . . . . . . . . . . 1 (2 .32%) Llilatation and curettage for sterility (one paticnt was never
pregnant) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2 (4.65%)
Stricture of the cervical canal and bad drainage have been suggested as a Such lesions
In this series the proportion predisposing factor to the development of carcinoma in this area. may readily result in dysmenorrhea or sterility. of such symptoms was not unduly high (Table V I ) .
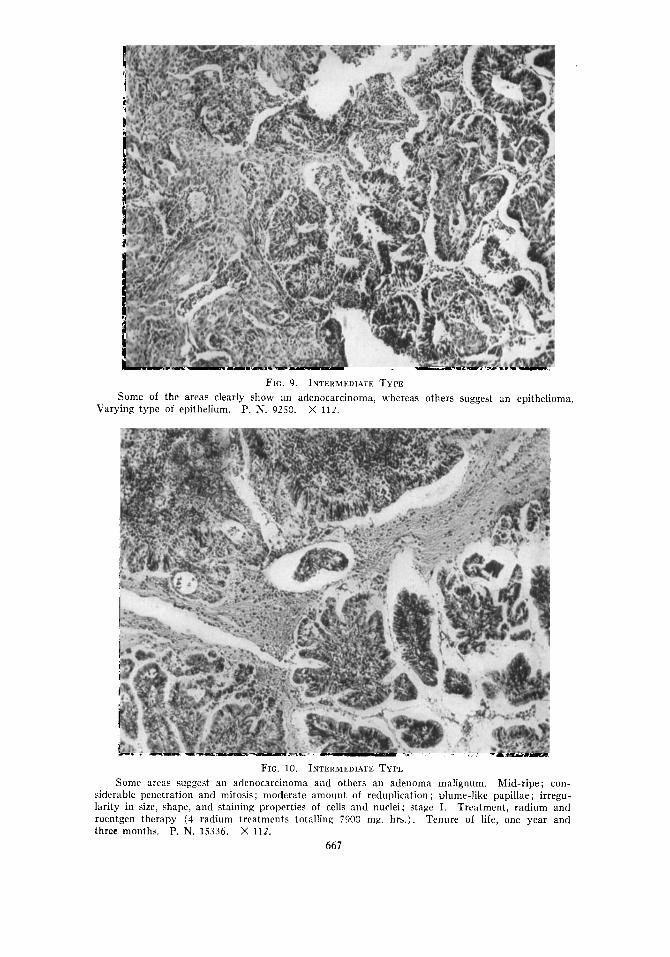
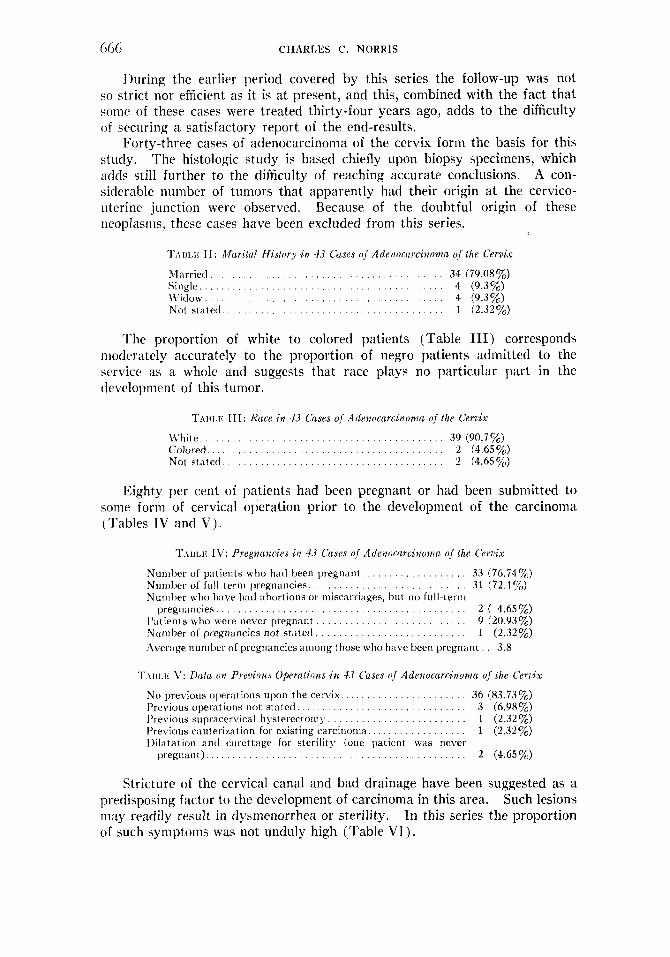
FIG. 9. INTLHMLDIAIE TYPE Some of the areas clearly show an adenocarcinoma, whereas others suggest an epithelioma.
Varying type of epithelium. P. N. 9250. X 1 1 2 .
FIG. 10. I N T ~ H M L D ~ A T E TYPL Mid-ripe ; con-
siderable penetration and mitosis; moderate amount of reduplication ; plume-like papillae; irregu- larity in size, shape, and staining properties of cells and nuclei; stage I. Treatment, radium and roentgen therapy (4 radium treatments totalling 7900 mg. hrs.). Tenure of life, one year and three months. P. N. 1.5336. X 112 .
Some areas suggest an adenocarcinoma and others an adenoma malignum.
667
668 CHARLES C. NORRIS
‘ ~ . \ I I L I ~ ; C’I : f i i s to ry of Preni~ous Dysmenorrhea or .%eri/ity in 4.7 Cades of Adenocarcinoma
No tlysmenorrhea or sterility . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28 (65.1%) I)ysnieiiorrliea o r sierilit y present . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8 (l8.6q;b) Not s ta ted. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7 (16.3%)
The average age in this series was 47.06 years; 65.1 per cent of the patients were between forty and fifty-nine years of age. The two youngest were each twenty-eight years old, and the oldest was seventy-two years of
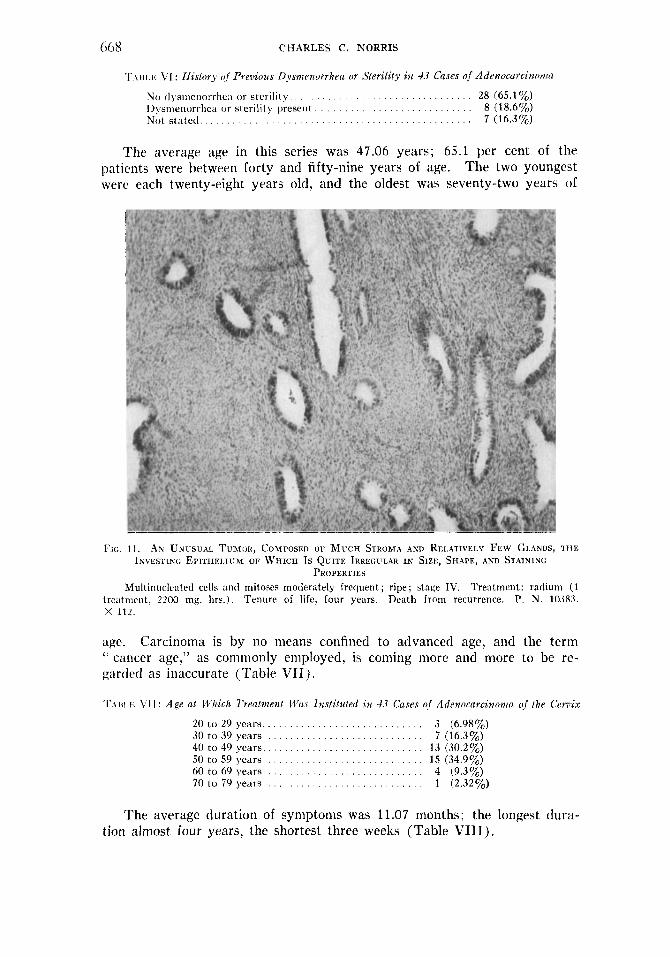
Frc. I 1 . AN UNUSUAL TUMOH, COMPOSED OF M u c ~ STHOMA AXD RELATIVELY Few GLANDS, T H E INVESTING EPITHEIJUM OF WHICH Is QUITE IRREGULAR IN SIZE, SHAPE, AND STAINING
PHOPEKTIES Multinuclrated cells and mitoses moderately frequent; ripe; stage IV. Treatment: radium (1
trc:itnirnt, 2200 mg. hrs.). Tenure of life, four years. Death from recurrence. P. N. 10383. x 112.
age. Carcinoma is by no means confined to advanced age, and the term ‘‘ cancer age,” as commonly employed, is coming more and more to be re- gorded as inaccurate (Table VII) . T.\III.K VI I : Age at I.t%ich Treatnienf l-ti(~s Instituted i n 4.7 Cases of Adtnocarcinonin o,f / h e Cervix
20 to 29 years . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3 (6.980/,) 30 to 39 y e a r s . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7 (16.3%) 40 to 49 years . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13 (30.2 %) 50 to 59 years . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15 (34.9%) 60 to 69 years 4 (9.3%) 70 to 79 y e a r s . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1 (2.3293
. . . . . . . . . . . . . . . . . . . . . . . . . . . .
The average duration of symptoms was 11.07 months; the longest dura- tion almost four years, the shortest three weeks (Table VIII).
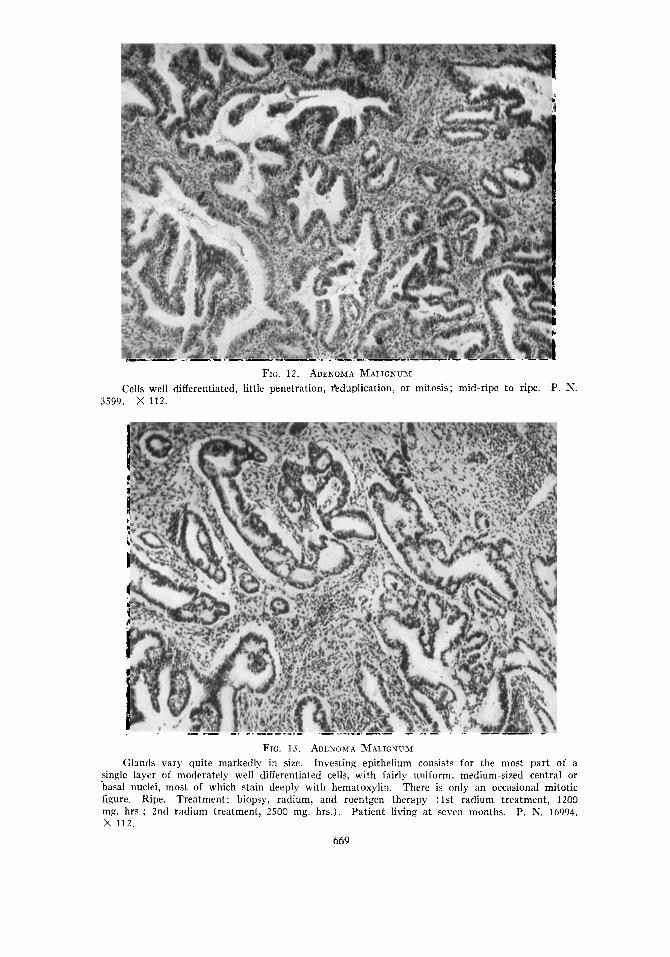
FIG. 12. ADENOMA MALIGSUM Cells well differentiated, little penetration, &duplication, or mitosis; mid-ripe to ripe. P. N.
3599. x 112.
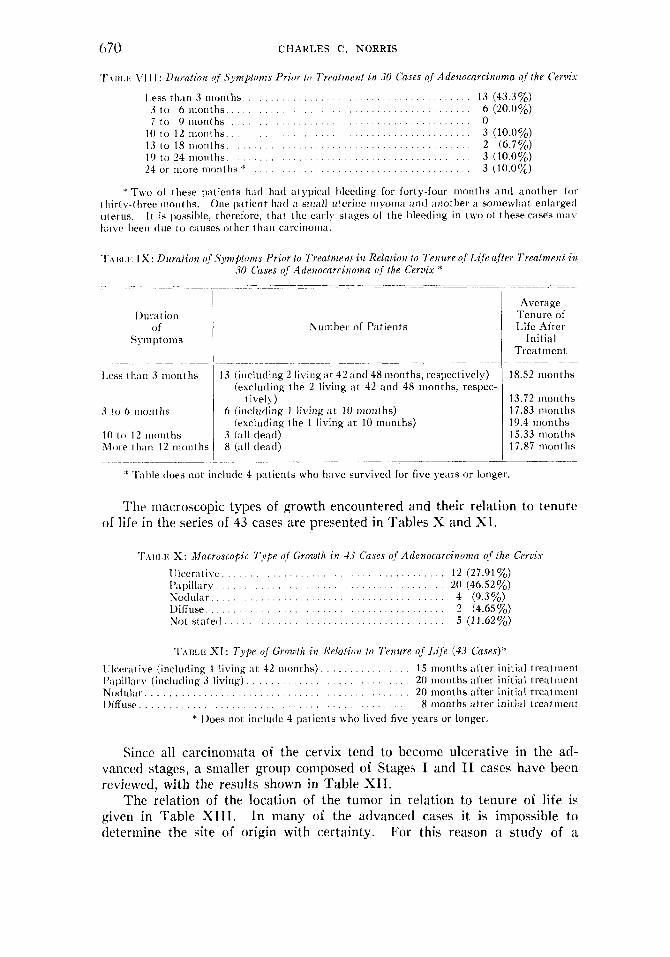
FIG. 13. ADENOMA MALIGNUM Investing epithelium consists for the most part of a
single layer of moderately well differentiated cells, with fairly uniform, medium-sized central or basal nuclei, most of which stain deeply with hematoxylin. There is only an occasional mitotic figure. Treatment: biopsy, radium, and roentgen therapy (1st radium treatment, 1200 m#. hrs.; 2nd radium treatment, 2500 mg. hrs.). Patient living a t sewn months. P. N. 16994. x 112.
Glands vary quite markedly in size.
Ripe.
669
670 CHARLES C. NORRIS
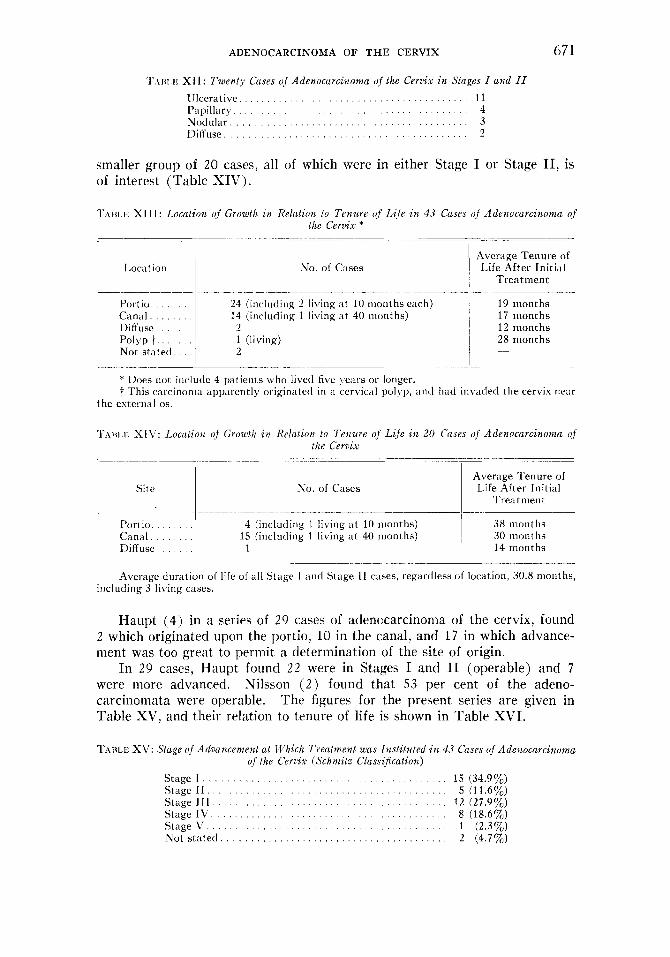
‘I‘\iti.i,: \‘I I I : L)tircz/ion of .Y+nptoms Prior to Treatmen! in .10 Cases of Adrnocarcinonza of the Crrvix
1.ess t h a n 3 Illonths . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13 (43.3%) 3 to 6 n i o n t h s . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6 (20.070) 7 t o 0 i i i o n t h s . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 0
3 (10.0%)
3 (10.0%) 3 (10.0%)
10 t o 12 n1onths.. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1 3 1 0 18 m o n t h s . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2 (6.7%) 19 t o 24 ni<)i i ths . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24 o r more months * . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
* TWO of these patients hiid had atypical hleetling for for tyfour moiiths and another for One p i t i e i i t hail i i sniall uterine niyonin and another ii soiiiewh;it enlargetl
I t is possihle, therefore, t h a t the cai-ly stages of the bleeding i n two of these cases m;i\. i l i ir ty-t hrec months. iiterus. h;ive Ijeen tlue t o causes other t hail carcinoiiin.
T.\HI,K IX : Dt~rcllion of .S’ymp/nms Prior lo l‘reatnzent iit Relalion lo Tenure o,[ L{fe after Trealmmt i n 30 Cases of Adenocarcinonia o,f the Cerziix *
~-
I.ess than 3 nionths
3 to 6 inonths
10 to 12 n i o n t h s Moi-e t hain 12 m o i i t hs
Numhrr of Patients
Average Tenure of Life After
In it ia 1 Treat mcnt
13 (iiicluding 2 living ,it 42 and 48 months, respectively) (excluding i he 2 living at 42 and 48 nionths, respec-
t ivel) ) 6 iinrluding 1 living ‘ 1 1 10 ~i~on ths )
3 ( , i l l dead) 8 (all de:id)
(excluding the 1 living .it 10 months)
18.52 inont hs
13.72 months 17.83 months 10.4 months 15.33 months 17.87 lllOIlt 11s
+ Table does not inclittle 4 patierits who have survived for five years or longer
The macroscopic types of growth encountered and their relation to tenure of life in the series of 43 cases are presented in Tables X and XI.
‘ ~ . I I I I . K X: Macrosropic Type of Growfh, in 4.1 Ccms of Adeiiocnrcinoma o,f ihr Cerzis IJlcer;itive. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12 (27.0170) 1’;ipillary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20 (46.52%)
IXl‘fuse.. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2 (4.65%) Not s ta te t l . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5 (11.62%)
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Nodular 4 (9.3%)
T,ziii.e XI: Typr of Grow,lh in Relafiiin to Tenure of Lije (4.3 Cases)* 1llccr;itive (inclutliiig 1 living ; i t 42 nionths). . . . . . . . . . . . . . . . 1.5 months after iuitial treatment 1’:ipiIl;iry (including 3 liviiig) . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20 nionths after initial treatiiicnt N~)cIu l ; i r . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20 inonths after initial treat nieiit I)ifl-use, . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8 months after initial lreatnierit
* Does not inclutle 4 patients who lived five years or longer.
Since all carcinomata of the cervix tend to become ulcerative in the ad- vanced stages, a smaller group composed of Stages I and I1 cases have been reviewed, with the results shown in Table XI I .
The relation of the location of the tumor in relation to tenure of life is given in Table XIII. In many of the advanced cases it is impossible to determine the site of origin with certainty. For this reason a study of rl.
ADENOCARCINOMA OF T H E CERVIX 671
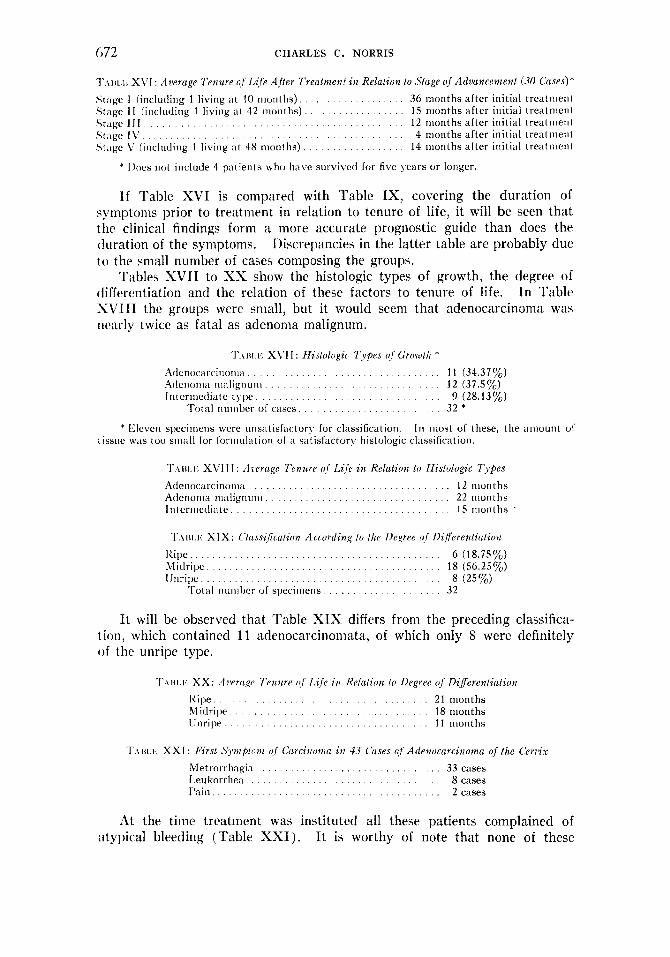
T.\BI.IC XII: Twenty Cases uf Adenocarcinoma of the Cerz~iix in Stages I a d 11 1Jlcerative . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . I I Papillary. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4 Nodular . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3 ])iffuse . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2
smaller group of 20 cases, all of which were in either Stage I or Stage 11, is of interest (Table XIV).
TIHI 14. XIII: Location of Growth z n Relation lo Tenure of Lite in 43 Cases uj Adenocarcirruma of the Cervix *
Location
Portio. . . . . . . Ca 1111 1 . . . . . . . Diffuse. . . . . Polyp t . . . . . . Not stated . .
No. of Cases
- - _____-----__ 24 (inclucliiig 2 living at 10 months each) 14 (including 1 living at 40 nionths)
2 1 (living) 2
Average Tenure of I,i fe After In it ia 1
Treatment
19 months 17 months 12 months 28 months -
* Does not include 4 patients who lived five !.ears or longer. t This carcinoma apparently originated i n a cervical polyp, and had invaded the cervix iieiir
the external 0s.
T.iici I XIY: Lucatzon of Growth $12 Relataon to Tenure of Lafe in 20 Cases of Adenncarcinuma of the Cerozx
- -~ ~ - _ _ ~
Site No. of Cases Average Tenure of Life After Initial
Treatment
I'ori io . . . . . . . 4 (iiiclutling 1 living at 10 months) . . . . . . . 15 (including 1 living a t 40 nionths) Canal.
Diffuse. . . . .
38 months 30 months 14 months
Average duration o f life of a l l Stage I and Stage I1 cases, regardless of location, 30.8 months, including 3 living cases.
Haupt ( 4 ) in a series of 29 cases of adenocarcinoma of the cervix, found 2 which originated upon the portio, 10 in the canal, and 1 7 in which advance- ment was too great to permit a determination of the site of origin.
In 29 cases, Haupt found 2 2 were in Stages I and I1 (operable) and 7 were more advanced. Nilsson ( 2 ) found that 53 per cent of the adeno- carcinomata were operable. The figures for the present series are given in Table XV. and their relation to tenure of life is shown in Table XVI.
T A I U . ~ ~ XV: .9tage of Advancement at Which Treatment was Instituted in 43 Cases of Adenocarcinoma of the Cervix (Schmitz Classi$cation)
Stage I . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15 (34.9y0) Stage 1 1 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5 (11.6%) Stage 1 1 1 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12 (27.9y0) Stage I V . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8 (18.6%) Stage\ ' . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1 (2.3%) Not stated . . . . . . . . . . . . . . . . . . . . . 2 (4.7%)
072 CHARLES C. NORRIS
T.IIII,I~. XVI : Aoerage Tenure of LiJe Afier Treatnzenf in Relaiion to Stage nf Advancement (30 Cases)* Stage I (including 1 living at 10 months). . . . . . . . . . . . . . . . . 36 months after initial treatnieni Stage I 1 (iricluding 1 living at 42 months) . . . . . . . . . . . . . . . . . 15 months after initial trcatnient Stage I I I . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12 months after initial treatnieui Stage I \ ' . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4 months after initial tre;itiiierit Si;ige 1' (iucluding 1 living a t 48 months) . . . . . . . . . . . . . . 14 nionths after initial treiitnieiil
.' Ihes i i o t include 4 patients \vho have survived lor five years or longer.
I f Table XVI is compared with Table IX, covering the duration of symptoms prior to treatment in relation to tenure of life, it will be seen that the clinical findings form a more accurate prognostic guide than does the duration of the symptoms. Discrepancies in the latter table are probably due to the small number of cases composing the groups.
Tables XVII to XX show the histologic types of growth, the degree of differentiation and the relation of these factors to tenure of life. In Table S V I I I the groups were small, but it would seem that adenocarcinonia was rienrly twice as fatal as adenonia malignum.
T.\IH,K X\rI I : ZZisfologic Q p e s i!f Growth * At1enocarcinoiii;i. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1 1 (34.377,) A(leiioiiia nialigiium . . . . . . . . . . . . . . . . . . . . . . . . 12 (37.570) Iritermetiiate t ) p . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9 (28.13%)
Total iiiuiiber of cases. . . . . . . . . . . . . . . . . . . . . . . . . 32 * * Eleveii specimens were unsntisfartory for c1;rssification. In most of these, the ;inrounl of
tissue w a s too sniall for foriiiulatiori o f i i satisfactory histologic classification.
'r.iui.i<; XVI I I : Azarage Tenure of Lije in Relation to ZZistologic Types Atlenocarcinoiiia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12 months Adenoma nialignuiii . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 22 nionths I n t erniediate . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15 nionths
'F.iut,l,: XIX: Cluss<ficntion According to thr Ile,oree of Differentiation I:il)e . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6 (18.75%) Midripe. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18 (56.25%) {Jiii-ipe.. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8 (25'%) ,. 1 otal nuiiil)er of specinlens. . . . . . . . . . . . . . . . . . . . 32
It will be observed that Table XIX differs from the preceding classifica- tion, which contained 11 adenocarcinomata, of which only 8 were definitely of the unripe type.
'r.\iii,i<: XX: Azwagr Tentire i1.f Life in Rr/(ition lo Degree nf Differentiation Kipe . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21 months Midripe. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18 months IJnripe. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1 1 months
T.\ t31 ,1*: XXI : First . S y n p / o n i (11 ci~rcinonia in 4.3 C u e s (if Adenocarciiioma of the C e r z k Metrorrhagia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 33 cases LeukorrheEi. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8 cases I'ain.. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2 cases
At the time treatment was instituted all these patients complained of I t is worthy of note that none of these atypical bleeding (Table XXI).
ADENOCARCINOMA O F T H E CERVIX 673
patients complained of menorrhagia. The bleeding caused by carcinoma is due largely to the erosive nature of the carcinoma cells and to trauma to the friable structure of the tumor, and as a result menstruation is but little affected unless there is involvement of the ovary. It is probable that if the patients forming this group had been questioned carefully, a higher proportion of cases exhibiting leukorrhea as the initial symptom would have been found. As has so often been stressed, most of these patients suffer for years before the development of the carcinoma from cervicitis, generally the result of lacerations; as a result, the leukorrhea emanating from the carcinoma is merely an augmentation or an alteration in character of a symptom that has long been present, and it is, therefore, prone to attract less attention than does the bleeding.
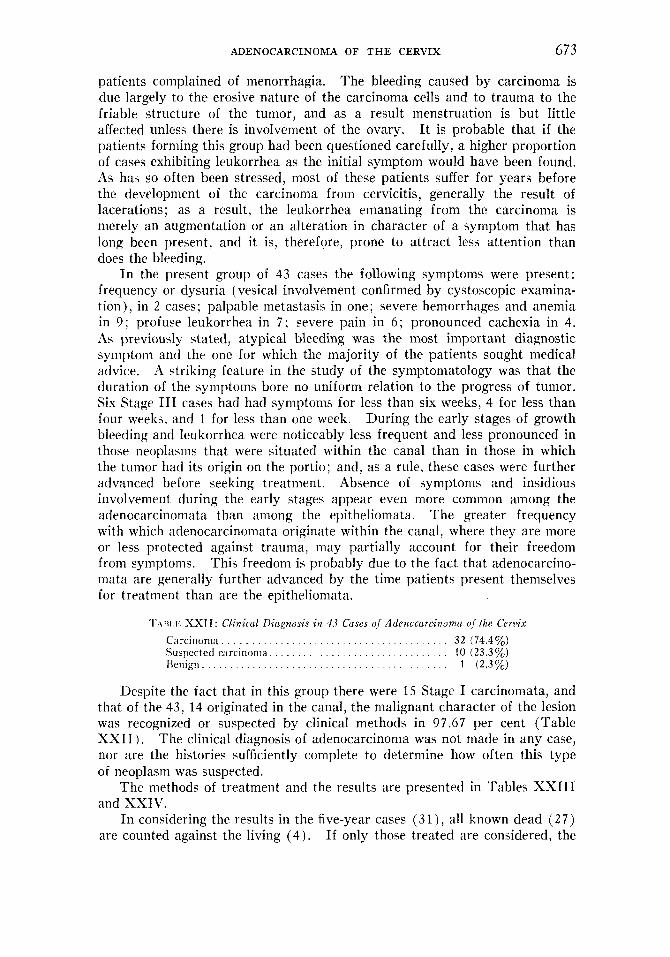
I n the present group of 43 cases the following symptoms were present: frequency or dysuria (vesical involvement confirmed by cystoscopic examina- tion), in 2 cases; palpable metastasis in one; severe hemorrhages and anemia in 9; profuse leukorrhea in 7 ; severe pain in 6 ; pronounced cachexia in 4. As previously stated, atypical bleeding was the most important diagnostic symptom and the one for which the majority of the patients sought medical advice. A striking feature in the study of the symptoniatology was that the duration of the symptoms bore no uniform relation to the progress of tumor. Six Stage I11 cases had had symptoms for less than six weeks, 4 for less than four weeks, and 1 for less than one week. During the early stages of growth bleeding and leukorrhea were noticeably less frequent and less pronounced in those neoplasms that were situated within the canal than in those in which the tumor had its origin on the portio; and, as a rule, these cases were further advanced before seeking treatment. Absence of symptoms and insidious involvement during the early stages appear even more common among the adenocarcinomata than among the epitheliomata. The greater frequency with which adenocarcinomata originate within the canal, where they are more or less protected against trauma, may partially account for their freedom from symptoms. This freedom is probably due to the fact that adenocarcino- niata are generally further advanced by the time patients present themselves for treatment than are the epitheliomata.
T.IIII,I< XXTI: Clinical Diagnosis in 4.1 Cases of Adcnccarciiiorna of the Cervix Carcinonia. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 32 (74.4%) Suspected carcinoma. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10 (23.3%) Henign.. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1 ('2.37,)
Despite the fact that in this group there were 15 Stage I carcinomata, and that of the 43, 14 originated in the canal, the malignant character of the lesion was recognized or suspected by clinical methods in 97.67 per cent (Table X X I I ) . The clinical diagnosis of adenocarcinoma was not made in any case, nor are the histories sufficiently complete to determine how often this type of neoplasm was suspected.
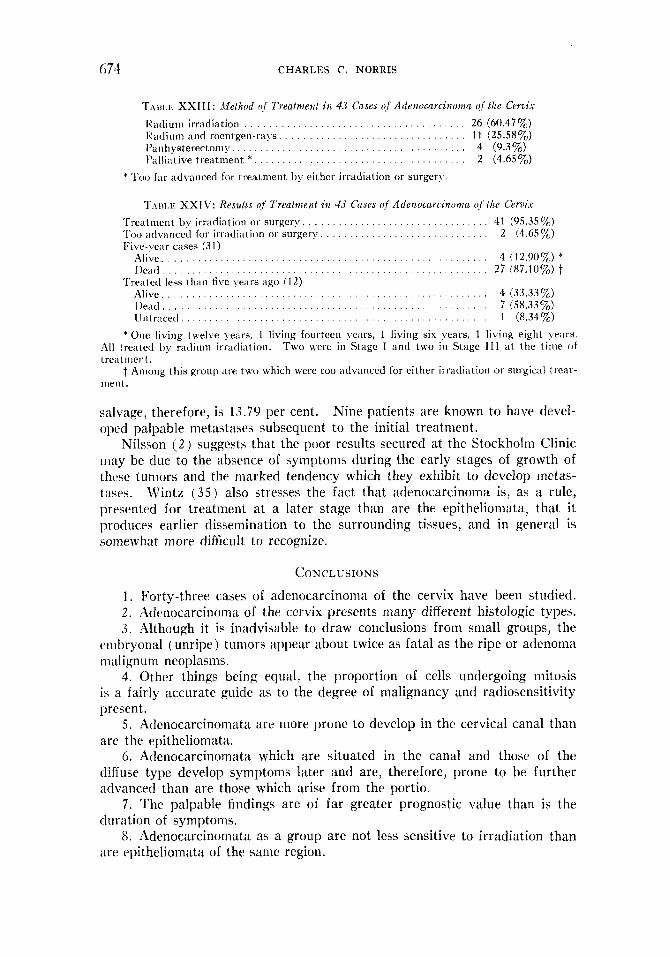
The methods of treatment and the results are presented in Tables XXIII and XXIV.
I n considering the results in the five-year cases (31), all known dead (27) are counted against the living (4) . If only those treated are considered, the
074 CHARLES C. NORRIS
TAiii.ii XXIII: Mefhod o/ Treatment it2 4.1 Cases (f Adenocarcinoma o/ the Cervix IZatlium irradiation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26 (60.47%) IZadiuin and roentgen-rays . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11 (25.5870) Panhysterectoniy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4 (9.3%) I'allintive treatiiient * . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2 (4.657,)
* Too far advanced for treatnient by either irradiation or surgery.
T.\iii,Il XXIV: Results of Treatment i n 45 Cases of Adenocarcinonza o/ the Cerzkt 'I'reatmeiit by irradiation or surgery. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 41 (95.35%) Too advanced for irradiation or surgery, . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2 (4.65%) Five-!,e;tr cases (31)
Alive.. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4 (12.90%) * I)ca[l . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 27 (87.10%)t
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4 (33.33%) 1)eatl . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7 (58.337,) lintracecl. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1 (8.34%)
Treated less than five years ago (1 2)
* One living twelve ).ears, 1 living fourteen years, 1 living six years, 1 living eight !wrs. Two were ill Stage I and two i r i Stage 111 at the time of
t Among this groul) are two which were too advanced for either irradiation or surgical treat-
.A11 treated by radium irradiation. 1re;itnient.
Inent.
salvage, therefore, is 13.79 per cent. Nine patients are known to have devel- oped palpable metastases subsequent to the initial treatment.
Nilsson ( 2 ) suggests that the poor results secured at the Stockholm Clinic may be due to the absence of symptoms during the early stages of growth of thcse tumors and the marked tendency which they exhibit to develop metas- tases. Wintz (35) also stresses the fact that adenocarcinoma is, as a rule, presented for treatment a t a later stage than are the epitheliomata, that i t produces earlier dissemination to the surrounding tissues, and in general is somewhat more difficult to recognize.
CONCLUSIONS 1. Forty-three cases of adenocarcinoma of the cervix have been studied. 2. Adenocarcinoma of the cervix presents many different histologic types. 3. Although it is inadvisable to draw conclusions from small groups, the
embryonal (unripe) tumors appear about twice as fatal as the ripe or adenoma malignutii neoplasms.
4. Other things being equal, the proportion of cells undergoing mitosis is a fairly accurate guide as to the degree of malignancy and radiosensitivity present.
5. Adenocarcinoinata are more prone to develop in the cervical canal than are the epitheliomata.
6. Adenocarcinomata which are situated in the canal and those of the diffuse type develop symptoms later and are, therefore, prone to be further advanced than are those which arise from the portio.
7. The palpable findings are of far greater prognostic value than is the duration of symptoms.
8. Adenocarcinomata as a group are not less sensitive to irradiation than are epitheliomata of the same region.
ADENOCARCINOMA O F T H E CERVIX 67 S
NOTE: Photomicrographs used in the article are by Mr. Basil Varian of the Department of Anatomy, University of Pennsylvania, through the courtesy of Dr. E. R. Clark, Professor of Anatomy.
HIBLIOGRAPIIY
1. MADRUZZA, G.: Zentralbl. f . Gynitk. 59: 19-22, 1935. 2. NILSSON, F.: Acta Radiol. 14: 283-330, 1933. 3 . NILSSON, F.: Acta Radiol. 16: 217-223, 1935. 4. HAUPT, W.: Monatschr. f . Geburtsh. u. Gyniik. 94: 364-367, 1033. 5. WARD, G. G . : Surg., Gynec. & Obst. 56: 431-436, 1933. 6 . HEALY, W. P.: J. A. M. A. 97: 1680-~1683, 1931. 7 . CHAMBERS, H.: Am. J. Cancer 23: 12, 1935. 8. WARD, G. G., AND FAKRAK, L. K. I).: Surg. Gynec. & Ohst. 52: 556-559, 1931. 9. WARREN, SHIELDS: Arch. Path. 12: 783-786, 1931.
10. PETERSON, R. : Surg. Gynec. & Obst. 29: 544-553, 1019. 11. MARTZLOFF, K. H. : Bull. Johns Hopkins Hosp. 34: 141-149, 184-195, 1923. 12. BUWING, H. H., DESJARDINS, A. U. , STACY, L. J., AND BLISS, J. H. : Am. J. Roentgenol.
13. BOWING. H. H., A N D FRICKE, R. E.: Journal-Lancet 51: 195-199, 1931. 14. FLUHMAKN, C. F.: Amer. J. Ohst. & Gynec. 13: 174-184, 1927. 15. TAYLOR, H. c., AND PEI(;HmL, T . C. : Amer. J. Obst. & Gynec. 8 : 288-297, 1924. 16. \’ON F R A N Q U ~ , 0.: In Veit-Stoeckel’s Handbuch der Gyniikologie, Ed. 3, Vol. V I / l , p.
17. KELLER, F.: Strahlentherapie 37: 349-353, 1930.
19. PANKOW, 0.: In Veit-Stoeckel’s Handbuch der Gyniikologie, Ed. 3, Vol. VI/2, 11. 642.
20. ROSS, J. W.: Canad. M. A. J. 12: 772-780, 1922. 21. BARTLETT, M. K., A N D SMITH, G. W.: Surg. Gynec. & Obst. 52: 249-253, 1931. 22. Ross, R. A.: South. Med. & Surg. 95: 487-488, 1933. 23. JOHNSON, C. G., A N D TYRONE, C. H. : Surg. Gynec. & Obst. 58: 113-115, 1931. 24. HEALY, W. P., A N D CUTLER, M.: Am. J. Obst. & Gynec. 16: 15-28, 1928. 25. DijDERLEIN, G.: Arch. f . Gyniik. 120: 201-203, 1923. 26. KAMNIKER, H.: Zentralbl. f . Gyniik. 56: 457-461, 1932. 27 . MALIPHANT, R. G.: J. Obst. & Gynaec. Brit. Emp. 40: 441-459, 1033. 28. CCTLER, M.: Surg. Gynec. & Obst. 55: 481-486, 1932. 2 0 . SCHOTTLAENDER, J., A N D KEKMAUNER, F. : Zur Keiintnis des Uteruskarzinoms, S.
30. MARTZL(JFF, K. H.: Am. J. Obst. & Gynec. 16: 578-594, 1928. 3 1 . REGALJD, C., AND GRICOUROFP, G.: Bull. Assoc. franf. p. l’ktude d. cancer 22: 285-296,
32. FRANKL: Quoted by Lahm, W., in Halban & Seitz: Biologie u. Pathologie des Weibes,
33. MEYER, R. : in Henke and Lubarsch: Handb. d. spez. pathol. Anat. und Histologie, Vol.
34. WINTER, G. : Anatomie des Carcinoma Uteri, in Veil’s Handbuch der Gyniikologie, Vol. J . I;. Bergmann, Wiesbaden, 1908.
35. WINTZ, 13.: Miinchen. med. Wchnschr. 78: 1935-1937, 1931. 36. LYNCH, F. W.: in Davis, C. H.: Gynecology and Obstetrics, Vol. 2, Chapter 13, 1934. 37. L a x r ~ , W.: in Halhan & Seitz, I3iologie und I’athologie des Weibes, Vol. IV, pp. 750-
24: 54-62, 1930.
104. J. F. Bergmann, Miinchen, 1930.
18. DijDERLEIN, G. : Zentralbl. f . Gyniik. 55: 968-981, 1931.
J. F. Bergmann, Miinchen, 1931.
Karger, Berlin, 1912.
1933.
Vol. IV. p. 751.
VI I / l . Julius Springer, Berlin, 1930.
III,:2.
Urban & Schwarzenberg, Berlin, 1928.
r v I 2 3 . Urban and Schwarzenberg. I3erlin, 1928.