Embed Size (px)
Citation preview

i
THE MECHANISM OF ADENOSINERGIC
REGULATION OF T-CELL MEDIATED
ACUTE HEPATITIS
THESIS PRESENTED
BY
MEENAKSHI SUBRAMANIAN
ADVISORS: Dr. MICHAIL SITKOVSKY and Dr. AKIO OHTA
THE BOUVE΄ GRADUATE SCHOOL OF HEALTH SCIENCES
DEPARTMENT OF PHARMACEUTICAL SCIENCES
NORTHEASTERN UNIVERSITY
113 MUGAR LIFE SCIENCES BUILDING
BOSTON, MA-02115
AUGUST, 2012

ii
Department of Pharmaceutical Science Thesis Proposal, Northeastern University
Thesis Title: The mechanism of adenosinergic regulation of T-cell mediated
acute hepatitis
Author: Meenakshi Subramanian
Program: Pharmaceutical Sciences with Specialization in Immunology
Approved for Thesis Requirement of the Doctor of Philosophy Degree in Pharmaceutical
Sciences
Thesis Committee:
Chair Date:
Member Date:
Member Date:
Member Date:
Member Date:
Member Date:
Director of Bouvѐ College Graduate School:

iii
ABSTRACT
Endogenous immune regulatory mechanisms exist to protect healthy tissue from collateral
damage by overactive immune cells during inflammation. It has been found that extracellular
adenosine can suppress pro-inflammatory activities through A2A adenosine receptors (A2ARs)
on immune cells. This function of endogenous adenosine is non-redundant and has been regarded
recently as a critical immune-regulatory negative feedback mechanism. Inflammatory responses
in the liver have been shown to be under the control of A2AR-mediated anti-inflammatory
pathway. The current study was designed to investigate the critical target of adenosine-mediated
regulation of acute hepatitis. Experiments employing a murine model of acute hepatitis indicated
exacerbated liver damage accompanied by exaggerated levels of cytokines TNF-α, IL-4 and IFN-
γ in A2AR-deficient (A2ARKO) mice as compared to the wild type (WT) control animals. Since
natural killer T cells (NKT cells) are responsible for the early production of these cytokines in
this model of hepatitis, NKT cells were suspected to be under the physiological control of the
‘adenosine-A2AR anti-inflammatory pathway’. Indeed, activation of NKT cells was susceptible
to A2AR stimulation, and more importantly, NKT cells from A2ARKO mice produced higher
levels of cytokines in vivo and induced stronger liver damage as compared to WT NKT cells.
Analysis of adenosine receptors in NKT cells suggested their expression of A2B adenosine
receptors (A2BRs) along with A2AR. Studies using A2BRKO mice also showed exaggerated
NKT cell responses in vivo as were observed in A2ARKO NKT cells. These results demonstrate
the involvement of A2ARs and A2BRs in the physiological regulation of NKT cell activation.
Levels of extracellular adenosine have been known to increase in response to hypoxia.
Therefore, it was suspected that hypoxia could negatively regulate NKT cell activation through
adenosine production. As expected, NKT cells were found to be susceptible to hypoxia both in

iv
vivo and in vitro. The mechanism of hypoxic suppression of NKT cell activation was partially
mediated by adenosine. Results obtained in the current study provide evidence that the
immunoregulatory hypoxia-adenosine pathway negatively regulates NKT cell activation, at least
in part via A2AR.

v
ACKNOWLEDGEMENTS
I wish to take this opportunity to thank all those people who have helped immensely throughout
my doctoral study.
Firstly, I wish to thank Dr. Michail Sitkovsky for giving me the opportunity to work in his lab
and learn immunology. He has been a constant source of encouragement and support. I really
admire his commitment to scientific research for developing cancer immunotherapy.
I sincerely owe my thanks to my mentor, Dr. Akio Ohta, for teaching me all that I know today in
Immunology. He has constantly mentored me during the initial stages of my training,
encouraging me to develop scientific thought and approach and has supported me throughout my
PhD training. He has always been my inspiration and I will strive to be a researcher like him.
I wish to sincerely express my gratitude to other members of my PhD thesis committee; Dr.
Richard Deth, Dr. Samuel Gatley, Dr. David Janero and Dr. Mark Exley for giving me their
valuable time, suggestions and guiding me through my thesis.
I want to sincerely thank Akiko Ohta who has been a constant source of support and who has
taught me ever since I joined NEITPI during master’s program in Pharmaceutical sciences. I
wish to thank senior lab members, Dr. Lukashev and Dr. Kjaergaard for providing me with their
professional advice. I also wish to thank Susan for being so kind and supportive to me always.
I wish to express my heartfelt gratitude to my colleagues; Steve, Manasa, Bob, Peter, Shalini,
Molly for their encouragement and support. I have truly enjoyed working with them.

vi
I cannot thank my best friend and colleague, Radhika enough for being such a great support to
me at all times. I am blessed to have such a great friend in my life. Last but not the least; I do not
have words to express my heartfelt thanks to my parents, grandparents, Shreedhar, Subbu and
extended family who have been immensely supportive during my education. My parents have
strived to ensure that I seek the best education and have always encouraged me to pursue my
dreams. I wish to dedicate my thesis to my mother and father.

vii
Table of Contents
Page Number
Abstract Iii
Acknowledgements V
List of figures viii
Abbreviations Xi
Statement of the problem 1
Specific Aims 2
Background and Significance 4
Materials and Methods 21
Results 28
Discussion 60
References 67

viii
LIST OF FIGURES
Fig. 1 Hypoxia driven ‘adenosine-A2AR’ mediated anti-inflammatory pathway……….............7
Fig. 2 A2ARs act as ‘sensors’ of the critical ‘tissue protective negative feedback signal’ in acute
hepatitis……………………………………………………………………………………………9
Fig. 3 Effector functions of hepatic NKT cells…………………………………………………..14
Fig. 4 Schematic representation of the proposed mechanism of Con A induced hepatitis……...18
Fig. 5 A2AR stimulation inhibits induction of hepatitis……………………………………......28
Fig. 6 Suppression of NKT cell activation by the injection of CGS…………………………….29
Fig. 7 Adenosine-A2AR signaling suppresses NKT cell activation……………………….…….31
Fig. 8 Pathophysiological regulation of inflammation by endogenously produced adenosine via
A2AR…………………………………………………………………………………………….31
Fig. 9 Flowcytometric analysis of NKT cells in the liver mononuclear cell preparation…….…32
Fig. 10 Exaggerated activation of NKT cells in A2AR-deficient mice………………………....33
Fig. 11 A2ARKO NKT cells caused exaggerated hepatitis in RAG1-KO recipient mice…...….34
Fig. 12 A2BR stimulation is suppressive to the activation of NKT cells………………………..36
Fig. 13 A2BR mRNA levels were quantified by real-time PCR………………….……………..37
Fig. 14 Functional expression of A2BR on NKT cells…………………………..………………38

ix
Fig. 15 Exacerbation of inflammatory liver damage in the absence of A2BR…………….…….39
Fig. 16 Exaggerated inflammatory response in A2BRKO mice………………………………....40
Fig. 17 Flowcytometric analysis of NKT cells from the liver…………………………….……..41
Fig. 18 Enhanced production of IL-4 by A2BRKO NKT cells…………………….……………42
Fig. 19 Endogenous adenosine regulates NKT cells via A2BRs………………..……………….43
Fig. 20 A2BRKO NKT cells caused exaggerated hepatitis in RAG2-KO recipient mice……....44
Fig. 21 Hypoxia is suppressive to NKT cell activation………………………………….….…...45
Fig. 22 Basal level of CD69 and CD40L expression on splenic NKT cells...............................46
Fig. 23 Hypoxia alone upregulates CD69 expression on NKT cells.........................................47
Fig. 24 Hypoxia mediated regulation of NKT cell activation in vivo……………….……..……48
Fig. 25 Hypoxia mediated regulation of NKT cell activation in vivo……………………...……49
Fig. 26 Hypoxia mediated suppression of NKT cell function in vivo…………………………...50
Fig. 27 Hypoxia mediated suppression of serum IL-4 levels after α-GalCer treatment...............51
Fig. 28 Hypoxia mediated suppression of NKT cell function in vivo………………….………..52
Fig. 29 Hypoxia regulates WT and A2ARKO NKT cell activation in vivo……………….….…53
Fig. 30 A2AR involves partly in the mechanism of hypoxia mediated suppression of NKT cell
function in vivo…………………………………………………………………………………..55

x
Fig. 31 A2AR involves partly in the mechanism of hypoxia mediated suppression of NKT cell
function in vivo……………………………………………………………………………..……56
Fig. 32 Hypoxia regulates WT and A2BRKO NKT cell activation in vivo………….………….57
Fig. 33 A2BR does not involve in the mechanism of hypoxia-mediated suppression of NKT cell
function in vivo……………………………………………………………………………….….58

xi
Abbreviations:
A2AR (A2A adenosine receptor)
A2BR (A2B adenosine receptor)
A2ARKO mice (A2A adenosine receptor gene deficient mice)
A2BRKO mice (A2B adenosine receptor gene deficient mice)
ALT (alanine amino transferase)
CCPA (2-chloro-N6-cyclopentyladenosine)
CD40L (CD40 ligand)
CGS (CGS21680)
Cl-IB-MECA 1-[2-chloro-6-[[(3-iodophenyl)methyl]amino]-9H-purin-9-yl]-1-deoxy-N-methyl-
-D-ribofuranuronamide)
Con A (concanavalin A)
DCs (dendritic cells)
FasL (Fas ligand)
α-GalCer (α-galactosylceramide)
MRS (MRS1754)
NECA (5’-N-ethylcarboxamidoadenosine)
NKT cells (here, invariant natural killer T cells)
RAG1KO mice (recombinase activating gene 1 deficient mice)
WT mice (wild-type mice)
ZM-ZM241385

1
Statement of the problem
Improper or prolonged inflammation leads to tissue damage and is the leading cause of many
diseases. Extracellular adenosine that accumulates in the inflamed tissue signals through A2ARs
on immune cells and terminates inflammation (Sitkovsky and Ohta, 2005). ‘Adenosine-A2AR’
signaling was found to be critical for limiting immune responses in the liver and is
hepatoprotective during acute hepatitis (Ohta and Sitkovsky, 2001). However, the critical cellular
target of ‘adenosine-A2AR’ anti-inflammatory pathway in the liver was not known. Also, the
involvement of other adenosine receptors in the regulation of hepatitis was not understood. The
current study was designed to understand the mechanism of endogenous regulation of
inflammation during acute hepatitis.

2
1. SPECIFIC AIMS:
SPECIFIC AIM 1: To investigate the critical target of the adenosine-A2AR mediated anti-
inflammatory mechanism in acute hepatitis.
1. To pharmacologically evaluate A2ARs on NKT cells by combining receptor specific
agonists and antagonists with in vitro activation of NKT cells.
2. To determine the physiological role of the ‘adenosine-A2AR’ pathway in activation of
NKT cells using a NKT cell-specific ligand, α-galactosylceramide (α-GalCer).
3. To confirm the immunoregulatory role of A2AR on NKT cells in the induction of liver
injury after intra-hepatic transfer of WT or A2ARKO NKT cells.
SPECIFIC AIM 2: To determine if the A2BR is involved in hepatic inflammation via
the regulation of NKT cell activation.
1. To induce acute hepatitis in A2BR-deficient mice and examine the involvement of A2BR
in the adenosine-mediated immunoregulatory mechanism.
2. To determine the expression of functional A2BRs and their role in NKT cell activation.
3. To confirm the role of A2BRKO NKT cells in acute hepatitis by intra-hepatic transfer of
WT or A2BRKO NKT cells.
SPECIFIC AIM 3: To investigate hypoxia mediated regulation of NKT cell activation.
1. To determine if NKT cells are susceptible to hypoxia by culturing the cells under 1 %
oxygen.

3
2. To test NKT cell activation under hypoxia in vivo by whole body exposure of α-GalCer
treated mice to 10% oxygen containing inspired gas mixture.
3. To test the involvement of A2AR in hypoxia mediated regulation of NKT cell function.
4. To test the involvement of A2BR in hypoxia mediated regulation of NKT cell function.

4
2. BACKGROUND AND SIGNIFICANCE:
The process of inflammation is a physiological response to an inciting stimulus such as infection
or tissue injury. A microbial infection or chemical injury or surgical trauma to the tissue will
activate the release of mediators of inflammation that provide chemical cues for leukocyte
chemotaxis to the site of tissue injury (Serhan et al., 2007). Cytokines that are released at the site
of infection or tissue injury cause the circulating immune cells to adhere to the vascular
endothelium, roll over and extravasate into the tissue space (Kuby Immunology 6th
Edition). An
‘acute’ inflammation has rapid onset, lasts for a short duration followed by a resolution phase
(Kuby Immunology 6th
Edition). The beginning of an acute inflammatory response is marked by
neutrophillic infiltration into the tissue followed by monocytes, lymphocytes and other cells of
the innate immune system. Immune cells secrete various pro-inflammatory cytokines and
cytotoxic molecules in order to destroy pathogens or pathogen infected cells. This comprises the
acute phase response during acute inflammation which is followed by a phase of resolution of
inflammation and repair of the inflamed tissue so that it’s normal physiological function can be
restored (Serhan et al., 2007). Certain conditions can result in ‘chronic’ inflammation such as
persistence of pathogens due to incomplete clearance or presentation of an immunogenic self
antigen leading to an auto-immune response (Kuby Immunology 6th
Edition). For instance, in
humans the high frequency or persistence of hepatitis C virus (HCV) infection tends to cause
chronic hepatitis (Nuti et al., 1998). Interestingly, the virus has been found to replicate in spite of
the presence of cellular and humoral immune responses. Also, the HCV itself is not ‘cytopathic’
meaning the viral replication is found to occur in the hepatocytes without causing hepatocyte
damage (Cerny and Chisari, 1999). However, an exaggerated necrotic inflammatory response
develops during ‘chronic’ HCV resulting in damage to both virally infected and non-infected

5
liver cells which contributes largely to the liver damage associated with hepatitis C pathogenesis.
(Nuti et al., 1998; Cerny and Chisari, 1999; Lucas et al., 2003).
The cellular organization of organs is not designed to sustain repeated inflammatory insults.
Persistent activity of immune cells in the tissue stimulates fibroblasts to proliferate and produce
collagen at the site of chronic inflammation. Fibrosis is an attempt to heal the inflamed tissue
which results in loss of functional organ cells and compromised organ function in the long run:
cirrhosis in the liver. Chronic inflammation underlies the pathophysiology of many disease states
and is a vital factor predisposing to carcinogenesis. It is, hence, important to understand the
physiological mechanisms that regulate inflammation.
Hypoxia driven adenosine-mediated physiological regulation of inflammation
The resolution of inflammation was thought to be a passive process that involves the
normalization of chemokine gradients and decline of the survival signals from supporting
stromal cells which causes leukocytes to retreat from the inflamed tissue (Serhan et al., 2007).
However, resolution of inflammation is now thought to be a very tightly controlled and timed
process (Sitkovsky and Ohta, 2005). The pharmacological evaluation of factors that could
suppress activated immune cells led to the discovery that certain chemicals released as a
response to neuroendocrine stress such as catecholamines, neuropeptides, prostaglandins of E
and I series are immunosuppressive (Sitkovsky et al., 2004). Many of these molecules cause
immunosuppression by activating adeynylyl cyclase and elevating cAMP in the immune cells.
This led to further understanding that certain factors may be produced within the inflamed tissue
microenvironment that can inhibit the activity of immune cells.

6
It has been found that the inflamed tissue microenvironment is often hypoxic due to the
disruption of tissue microcirculation during inflammation (Linden 2001, Sitkovsky 2003).
Several studies have demonstrated the anti-inflammatory effects of hypoxia (Eltzschig et al.,
2005, Thiel et al., 2005, Rosenberger et al., 2009), where local hypoxia in the tissue was found to
suppress inflammatory damage. For instance, mice exposed to 10% oxygen resisted lung damage
by bacterial toxins, whereas exposure to 100% oxygen exacerbated the lung damage by
abolishing the hypoxia driven tissue-protective mechanism (Thiel et al., 2005).
Deprivation of oxygen can cause dramatic changes in cellular metabolism. Hypoxia has been
found to elevate the levels of extracellular adenosine in the inflamed tissue (Driver et al., 1993,
Martin et al., 2000). Even brief duration of hypoxic exposure can lead to decreased production of
ATP and a reciprocal accumulation of AMP which can be further metabolized to adenosine by
cytosolic 5’-nucleotidase (Sitkovsky et al., 2004). Adenosine can shunt between intracellular and
extracellular compartments by means of equilibrative nucleoside transporters (ENTs). Hypoxia
has been shown to decrease adenosine uptake by the ENTs (Eltzschig et al., 2005). Also, ATP is
thought to be released into the extra-cellular space during inflammatory tissue damage. In the
extracellular space, ATP or ADP is metabolized to AMP by the activity of ectonucleoside
triphosphate diphosphohydrolase (CD39) and AMP is further converted to adenosine in the
extracellular space by ecto-5’-nucleotidase (CD73). The hypoxic microenvironment within the
inflamed tissue is conducive to the activity of hypoxia inducible factor, HIF-1α, that upregulates
the surface expression of CD73 (Synnestvedt et al., 2002). Hypoxia also induces CD39, and
therefore promotes accumulation of extracellular adenosine. In addition, hypoxia inhibits
adenosine kinase and prevents the reutilization of adenosine to produce AMP (Decking et al.

7
1997, Kobayashi et al. 2000). All these events lead to the enhanced production and accumulation
of extracellular adenosine under hypoxia.
Fig. 1. Hypoxia driven ‘adenosine-A2AR’ mediated anti-inflammatory pathway:
Inflammatory tissue damage leads to direct cell injury and hypoxia in the inflamed tissue which
facilitates the accumulation of extracellular adenosine. The extracellular adenosine signals
through Gs coupled A2A and A2B adenosine receptors on activated immune cells causing an
elevation in intracellular cAMP. Increase in intracellular cAMP acts as a ‘stop signal’ to further
inflammatory activity by interrupting intracellular signaling pathways that lead to pro-
inflammatory processes in immune cells. The hypoxia driven ‘adenosine-A2AR’ pathway serves
as a delayed negative feedback mechanism to stop the activity of immune cells in the inflamed
tissue (Sitkovsky and Ohta, 2005).
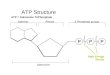
Extra-cellular adenosine is the endogenous ligand to purinergic G protein coupled receptors.
Upon binding to the receptor, adenosine signals through heterotrimeric G proteins that can either

8
stimulate (Gs) or inhibit (Gi) the enzyme, adenylyl cyclase that catalyzes the formation of cAMP
(Sitkovsky et al., 2004). Four adenosine receptors have been characterized: A1, A2A, A2B and
A3. Depending upon the agonist potencies at these receptors with regard to intracellular
production of cAMP, the receptors have been classified as high affinity A2AR and low affinity
A2BR, that couple with Gs protein to induce cAMP formation and high affinity A1R and low
affinity A3R, that couple with Gi to inhibit adenylyl cyclase activity (Sitkovsky et al., 2004). Of
these, A2ARs are most abundantly expressed on T lymphocytes.
Adenosine can suppress a wide variety of immune responses such as the oxidative burst in
neutrophils (Cronstein et al., 1990), activation of monocytes (Link et al., 2000). Also, adenosine
induces immunosuppressive IL-10 from macrophages (Okusa et al., 1999). A2AR activation and
subsequent elevation of intracellular cAMP leads to activation of protein kinase A (PKA). In T
lymphocytes, PKA can modulate T cell receptor (TCR) signaling at multiple levels, most
importantly, by the phosphorylation of carboxy terminal Src Kinase (CsK) which inhibits
proximal TCR signaling by inactivating Lck and Fyn that play pivotal role in the initial events of
T cell signaling. PKA also phosphorylates CREB (cAMP response element binding protein) that
upon binding to CRE (cAMP response element) in the DNA prevents the transcription of NFkB
and NFAT, nuclear factors needed to initiate T cell proliferation and cytokines production upon
TCR stimulation (Tasken and Ruppelt, 2006). Combining A2AR stimulation with T cell
activation can severely inhibit T cell effector functions namely, cytotoxicity and cytokines
production and to a lesser extent, T cell proliferation (Ohta et al., 2009).
However, for immune cells to be regulated by the ‘adenosine–A2AR’ pathway, the level of
extracellular adenosine in the inflamed tissue must be sufficiently high, which may be
determined by the extent of tissue damage and resultant hypoxia. Also, this mechanism will be

9
affected by the number of A2ARs expressed on the immune cells. Thus, extra-cellular adenosine
acts as a ‘reporter’ of the extent of tissue injury while A2ARs on immune cells act as ‘sensors’
for this anti-inflammatory signal in order to terminate the immune response only upon
considerable inflammatory tissue damage, which perhaps allows time for immune cell mediated
pathogen destruction (Sitkovsky et al., 2004).
2.2 Regulation of hepatitis by endogenous ‘adenosine-A2AR’ mediated anti-inflammatory
signaling
Fig. 2. A2ARs act as ‘sensors’ of the critical ‘tissue protective negative feedback signal’ in
acute hepatitis: During liver inflammation, endogenous adenosine acts as a ‘reporter’ of the
extent of tissue damage and A2ARs on immune cells can sense this signal to stop further
inflammation (Ohta and Sitkovsky, 2001). (Left) Extracellular adenosine binds to high affinity
Gs coupled A2ARs on immune cells and causes an elevation of intracellular cAMP. This leads to

10
inhibition of T cell effector functions. (Right) Immune cells at the inflamed tissue can be relieved
of adenosine mediated inhibition by interfering with ‘adenosine-A2AR signaling’ by genetic
deletion of A2ARs on immune cells or by pharmacological antagonism by receptor specific
antagonist.
The above schematic representation (Fig. 2) summarizes the work done by Ohta and Sitkovsky
in 2001. Using a model of acute hepatitis, the authors showed that sub-optimal doses of an
inflammatory stimulus that caused only minimal tissue damage in the wild-type mice were
sufficient to cause extensive liver damage as evidenced by exaggerated serum alanine amino
transferase (ALT) levels and prolonged, elevated serum levels of pro-inflammatory cytokines:
TNF-α, IFN-γ and IL-4 in the A2ARKO littermates (Ohta and Sitkovsky, 2001). Also,
pharmacological antagonism of A2AR using ZM 241385 caused exaggerated liver damage in
WT mice (Ohta and Sitkovsky, 2001). Tumor microenvironment also contains higher levels of
extracellular adenosine than the surrounding normal tissue (Ohta et al., 2006). Improvement of
tumor rejection in A2ARKO mice or by A2AR antagonist indicated a vital role of the
‘adenosine-A2AR’ pathway as an immunosuppressive mechanism in tumor microenvironment
preventing successful tumor immunotherapy (Ohta et al., 2006). These experiments demonstrate
that the lack of the adenosine-A2AR pathway results in much exaggerated inflammation because
no other endogenous anti-inflammatory mechanism could fully compensate for the deficiency of
A2AR.
Inflammatory responses in the liver are under the control of adenosine. Divergent roles of
extracellular adenosine have been observed in the course of hepatitis. Anti-inflammatory nature
of adenosine, mostly through A2AR, has been demonstrated by the suppression of acute hepatitis
induced by Con A (Ohta and Sitkovsky, 2001), D-galactosamine+LPS (Odashima et al., 2005) or

11
ischemia-reperfusion (Harada et al., 2000). Formation of extracellular adenosine is indispensable
as a physiological stop signal to prevent excess inflammation as evidenced by much exaggerated
hepatitis in A2AR-deficient mice (Ohta and Sitkovsky, 2001). T cells, which play a major role in
the pathogenesis of viral and autoimmune hepatitis, express A2ARs and T cell functions are
susceptible to adenosine-A2AR inhibitory signal (Ohta et al., 2009). These studies can explain an
anti-inflammatory mechanism of adenosine in T cell-dependent induction of acute hepatitis. In
the resolution phase of hepatitis, however, the inactivation of adenosine-A2AR signaling
prevented the induction of cirrhosis (Chan et al., 2006, Feoktistov et al., 2009). Indeed,
adenosine was found to facilitate fibrosis through the induction of collagen (Chan et al., 2006).
Thus, adenosine involves in hepatitis from the inhibition of immune responses in the priming
phase to tissue remodeling in the resolution phase of inflammation.
A2BR is another Gs protein-coupled adenosine receptor, which is capable of increasing cAMP
levels. Recently, adenosine signaling through A2BR has been reported to modulate inflammatory
responses. Studies using A2BR-selective agents and A2BRKO mice, however, have been
showing controversial roles of A2BR in inflammation. On one hand, A2BR stimulation can
enhance IL-6 production (Ryzhov et al., 2008) and is reported to augment pulmonary
inflammation and colitis (Sun et al., 2006, Mustafa et al., 2007, Kolachala et al., 2008). But, on
the other hand, A2BR is demonstrated to attenuate vascular, pulmonary, and gastrointestinal
inflammation (Yang et al., 2006, Eckle et al., 2008, Frick et al., 2009; Zhou et al., 2009). The
reason underlying these controversial pro-/anti-inflammatory actions of A2BR is not clear.

12
2.3. Natural Killer T cells:
Natural Killer T (NKT) cells are a group of lymphocytes that express both functional T cell
receptor and NK receptors (Kronenberg and Gapin, 2002, Swain, 2008). Most NKT cells bear
invariant TCR chain (V14J18 in mice and V24J18 in humans) and limited variations of
TCR chain. These are called as invariant NKT cells (iNKT cells). In the current study, by
mentioning NKT cells, I refer to iNKT cell population. They can co-ordinate between the
adaptive and innate immunity (Swain, 2008). NKT cells rapidly activate upon recognition of self
and foreign glycolipid antigens presented on MHC class I-like molecule, CD1d, and produce
large amounts of cytokines including IL-4 and IFN. During a screen for molecules that could
prevent metastases to the liver, α-galactosyl ceramide (α-GalCer) was first isolated from a sea
sponge named Agelas mauritianus (Morita et al., 1995). The bacteria, Sphingomonas breeding in
the sponge is thought to produce α-GalCer. α-GalCer is a glycolipid that binds to CD1d molecule
and can selectively activate mouse and human NKT cells (Linsen et al., 2005). It is thought that
α-GalCer mimics self glycolipid antigen recognized by NKT cells since α-glycosphingolipids
cannot be synthesized in mammals (Gapin, 2010).
Though also present in other lymphoid organs with T cells, NKT cells are enriched in the liver.
In both mice and humans, the liver has the highest NKT cell to conventional T cell ratio (Swain,
2008). α-GalCer loaded, soluble, CD-1d tetramers are used to identify the invariant NKT cells
(Benlagha et al., 2000). Using such staining it has been reported that most of the NKT cells
(approximately 50% of intrahepatic lymphocytes) bear the invariant TCR in the mouse.
However, invariant NKT cells are rare in the human liver. 0.03%-0.34% invariant NKT cells are
present in the human liver (Exley et al., 2002).

13
Extensive lipid metabolism occurs in the liver. Also, CD1d is found to be expressed on
hepatocytes, Kupffer cells, hepatic dendritic cells and the endothelial cells lining the sinusoids
(Exley et al., 2002). As NKT cells recognize and activate in response to endogenous or
exogenous lipid antigens expressed on CD1d molecules, they are thought to be best suited
immune cells for surveillance in the liver (Swain, 2010). Lysosomal glycosphingolipid,
isoglobotrihexosylceramide (iGb3) has been found to activate mouse and human NKT cells
(Gapin, 2010). However, endogenous glycolipid ligands for NKT cells have not yet been
identified.
Leukocyte trafficking is controlled by small chemotactic proteins called as ‘chemokines’. NKT
cells express chemokine receptors CXCR3 and CXCR6 which are important for the enrichment
and perhaps, the retention of NKT cells in the liver (Swain, 2010; Geissmann et al., 2005). NKT
cells perform immune surveillance while residing within the vasculature itself. In other lymphoid
organs like the spleen and lymph nodes, the lymphocytes interact closely with antigen presenting
cells in compartments that are protected from the flow rate of the blood. In the liver, however,
most cells are in close contact with the blood. NKT cells do not extravasate into the liver tissue
like other immune effector cells but patrol while residing within the vascular space. The NKT
cells stop moving once their TCR is activated by a ligand (Geissmann et al., 2005).
NKT cells can initiate immune response to bacterial infections (Linsen et al., 2005). Gram
negative, lipopolysaccharide (LPS) containing bacteria like Salmonella typhimurium indirectly
activate NKT cells (Brigl et al., 2003). The LPS in the bacteria activates Toll like receptors on
dendritic cells which then produce IL-12. This along with presentation of the endogenous
lysosomal glycosphingolipid, iGb3, by LPS-activated dendritic cells causes CD1d dependent
activation of NKT cells (Brigl et al., 2003, Mattner et al, 2005). Another mechanism of NKT

14
activation is observed in LPS negative bacterial infections. Glycosylceramides from the cell wall
of gram negative, LPS negative bacteria belonging to the class of alpha-Proteobacteria like
Ehrlichia muris and Sphingomonas capsulata cause direct activation of the T cell receptor of
NKT cells (Mattner et al, 2005). Thus NKT cells extend the repertoire of lymphocytes that
provide anti-microbial defense. NKT cells also involve in tumor immunesurveillance. IFNγ from
activated NKT cells and secondary transactivation of anti-tumor effector cells such as NK cells
and CD8+ T cells mainly contribute to NKT cell mediated anti-tumor immunity (Linsen et al.,
2005).
2.4. Role of NKT cells in regulating hepatic immune responses
Reference: Swain, M.G (2008). “Hepatic NKT cells: friend or foe?” Clin. Sci. (Lond.) 114:457-466.
Fig. 3 Effector functions of hepatic NKT cells: NKT cells activate upon recognition of
glycolipid antigen presented by CD1d on dendritic cells. Upon TCR activation, NKT cells

15
respond by rapid and explosive production of Th1 and Th2 cytokines (Wingender et al., 2011).
Activation induces upregulation of CD40L on NKT cells that interacts with CD40 on dendritic
cells (Kitamura et al., 1999). This interaction is important for dendritic cell maturation and IL-12
production (Swain, 2008). IL-12 produced from dendritic cells further activates NKT cells. IL-4
produced by NKT cells acts in an autocrine manner to upregulate FasL on NKT cells. FasL
interacts with Fas expressed on hepatocytes leading to hepatocyte apoptosis (Kaneko et al.,
2000). Also, NKT cells can cause cytotoxicity by release of preformed perforin and granzyme
(Swain, 2010).
Cytokines produced from activated NKT cells can regulate subsequent immune responses by
direct cellular effects or in an indirect manner by inducing production of chemokines that recruit
inflammatory effector cells or regulatory cells into the liver (Swain, 2010). The scheme above
(Fig. 3) explains the effector functions of hepatic NKT cells. Dendritic cells can process and
present endogenous or exogenous glycolipid antigens on CD1d. The T cell receptor of NKT cells
can recognize and activate to glycolipids presented in this way. Upon TCR activation, NKT cells
can secrete copious amounts of various cytokines of Th1 (IFNγ and TNFα), Th2 (IL-4, IL-5, IL-
10, IL-13) and Th17 (IL-17) lineages (Swain, 2010). IL-4 secreted from the activated NKT cells
acts on the NKT cells itself causing an upregulation of Fas ligand (FasL). The FasL on NKT
cells interacts with Fas expressed on hepatocytes and contributes largely to hepatocyte apoptosis
in the induction of liver damage (Kaneko et al., 2000). IL-4 from activated NKT cells also
augmented the expression of granzyme B in an autocrine manner which was important for NKT
cell-mediated cytotoxicity (Kaneko et al., 2000). Also, IFNγ and IL-4 secreted by activated NKT
cells stimulated IFNγ release from NK cells. IFNγ was found to be important in NKT cell
mediated clearance of hepatitis C virus and also for anti-tumor immune responses in the liver

16
(Swain, 2010). Upon activation, NKT cells upregulate CD40 ligand (CD40L) which interacts
with CD40 molecule expressed on dendritic cell surface. CD40-CD40L interaction is important
for the maturation of dendritic cells which then secrete IL-12 (Kitamura et al., 1999). IL-12
secreted from dendritic cells in turn further activates NKT cells that upregulate IL-12 receptor on
their surface (Kitamura et al., 1999).
NKT cells also have hepatoprotective functions. NKT cells activated by in vivo administration of
α-GalCer produce IL-17, during the early phase of the immune response which regulates the
recruitment of monocytes and neutrophils into the liver (Wondimu et al., 2010). Neutralization of
IL-17 after α-GalCer administration causes extensive monocyte and neutrophil infiltration
leading to extensive liver damage (Wondimu et al., 2010). Also, rapid production of IFNγ from
NKT cells after α-GalCer stimulation induces chemokine CXCL10 that recruits regulatory T
cells into the liver (Santodomingo-Garzon et al., 2009). Thus, depending on the stimulus for
NKT cells and the immune context into which these cytokines are released, NKT cells can play
both pro-inflammatory and anti-inflammatory roles and potently regulate hepatic immune
response (Swain, 2010).
Evidences for the involvement of hepatic NKT cells in various forms of hepatitis
Direct activation of NKT cells by -GalCer injection induces acute liver injury suggesting NKT
cell-initiated pathogenesis of acute hepatitis (Osman et al., 2000). α-GalCer activated NKT cells
produce IFNγ and transactivate NK cells that produce IFNα/β. These cytokines suppress
replication of hepatitis B virus (HBV) within 24 hrs of α-GalCer injection to HBV transgenic
mice (Kakimi et al., 2000). The study suggested the potential of NKT cells to inhibit HBV
replication in the liver during a natural infection. One of the striking features of chronic HCV

17
infection is the presence of liver-infiltrating lymphocytes (Cerny and Chisari, 1999). The intra
hepatic lymphocytes (IHLs) in the HCV infected patient livers largely contained Th1 polarized
NKT cells (Nuti et al., 1998, Exley et al., 2002). Higher frequency of NKT cells have been
observed in auto-immune liver diseases especially near the area of inflammation suggesting their
role in auto-immune hepatitis. Higher frequency of NKT cells were found in the livers of patients
with primary biliary cirrhosis as compared to the livers of healthy individuals (Kita et al., 2002).
Wilson disease is an autosomal recessive disorder resulting in abnormal copper transport causing
toxic accumulation of copper in the liver and brain. The absolute number and frequency of NKT
cells was found to be increased in the patients with fulminant Wilsonian hepatitis (Kinebuchi et
al., 2005). Chronic consumption of alcohol leads to an increase in hepatic NKT cells and also
sensitizes hepatocytes to NKT cell mediated cytotoxicity (Minagawa et al., 2004). On the other
hand hepatic NKT cells are found to be protective in high fat diet induced non-alcoholic
steatohepatitis (Li et al., 2005). Thus hepatic NKT cells involve in most forms of hepatic
disorders and this motivated the need to understand the mechanism of physiological regulation of
NKT cells during acute hepatitis in the current study.

18
2.5. The T cell mediated model of acute hepatitis:
IFN-
TNF-IL-4
FasL
IL-12
T cell
NKT cellKupffer cell
Hepatocyte Damage
Concanavalin A
IFN-
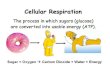
Fig. 4. Schematic representation of the proposed mechanism of Con A induced hepatitis:
Intravenous injection of concanavalin A (Con A) leads to activation of NKT cells and T cells in
the liver. NKT cells participate in the early stages of inflammation producing large amounts of
cytokines, IFN-γ and IL-4. The cytokines produced from NKT cells recruit other immune cells,
including Kupffer cells which are resident macrophages in the liver to orchestrate an immune
response leading to liver damage. Activated NKT cells also express FasL and cause Fas
mediated apoptosis of hepatocytes. NKT cells are major producers of IL-4 and are indispensible
for the induction of acute hepatitis by Con A.
Concanavalin A is a plant protein belonging to the class of ‘lectins’. The lectin specifically binds
to certain alpha-mannosyl residues of oligosaccharides on the surface of T cells and is a T
lymphocyte mitogen. Intravenous injection of Con A in mice causes acute hepatitis that
resembles viral and autoimmune hepatitis, involving T cells, NKT cells and Kupffer cells (Tiegs

19
et al., 1992, Toyabe et al., 1997, Kaneko et al., 2000, Herkel et al., 2005) (Figure 3).
Experiments using NKT cell-depleted/deficient mice have demonstrated that the lack of NKT
cells completely abolished Con A-induced liver damage. In these experiments, IL-4 production
from NKT cells was crucial in the induction of hepatitis (Toyabe et al., 1997, Kaneko et al.,
2000).
In 2000, Harada et al. reported the reduction of ischemia/reperfusion injury of rat liver by A2AR
agonist mediated inhibition of leukocyte activation (Harada et al., 2000). Subsequently, NKT
cells were found to be essential to the induction of hepatic ischemia/reperfusion injury (Lappas et
al., 2006). In the same study, A2AR specific agonist, ALT146e, could suppress
ischemia/reperfusion injury in RAG-1KO mice that received adoptive transfer of NKT cells, thus
confirming A2AR expression on NKT cells and its negative role in NKT cell activation (Lappas
et al., 2006).
The current study focuses on investigating the mechanism of adenosine-mediated regulation of
hepatic inflammation. Much exaggerated liver inflammation in A2ARKO has demonstrated the
hepatoprotective role of endogenously produced adenosine; however, cellular target of A2AR-
mediated anti-inflammatory effects is not clear. NKT cells could be the target because these cells
play a critical role in the induction of acute hepatitis. NKT cells are reported to express A2AR;
however, it is not known whether endogenously produced adenosine controls intensity of NKT
cell activation. To address this question, the intensity of NKT activation and subsequent liver
damage were studied in A2ARKO mice (Specific Aim #1). As it was observed in A2AR, similar
immunoregulatory roles could be expected for A2BR. However, previous studies have provided
controversial results and the role of A2BR in inflammation is not clear. To establish the role of
A2BR in hepatic inflammation, extent of liver damage was compared between WT and

20
A2BRKO mice together with the A2BR-mediated regulation of NKT cell activation. (Specific
Aim #2). The results from Specific Aim #1 and 2 showed exaggeration of NKT cell responses in
the absence of A2AR or A2BR indicating NKT cell regulation by endogenous adenosine.
2.6. Hypoxia mediated regulation of NKT cell activation
Since hypoxia is conductive to the accumulation of extra-cellular adenosine, it was hypothesized
that tissue hypoxia also regulates NKT cell activation. NKT cell activation was examined
whether it is under control of the hypoxia-adenosine axis of immune regulation (Specific Aim
#3).

21
3. MATERIALS AND METHODS:
3.1. Mice
C57BL/6 mice were obtained from Charles River Laboratories (Wilmington, MA). C57BL/6-
background A2ARKO mice were backcrossed 11 times to C57BL/6 mice (Chen J 1999).
C57BL/6-background A2BRKO mice were developed by Ozgene Pty. Ltd. (Bentley, Australia)
using C57BL/6 embryonic stem (ES) cells.
The mice were housed in the animal facility of Northeastern University and were used at 8-10
weeks of age in accordance with institutional animal care guidelines.
3.2. Concanavalin A (Con A)-induced hepatitis
Con A (Sigma, St. Louis, MO) was injected intravenously to induce acute liver injury (Tiegs et
al., 1992). The blood samples were collected at 8 or 24 h after Con A injection and liver damage
was evaluated by serum ALT levels. ALT activity was measured by using a kit from Teco
Diagnostics (Anaheim, CA). Serum levels of TNF- and IL-4 after 1.5 h and serum IFN- levels
after 8 h were determined using ELISA kits obtained from R&D Systems (Minneapolis, MN).
The liver tissue was fixed in 10% formalin-PBS 24 h after Con A injection, and the paraffin-
embedded tissue slice was stained with hematoxyline-eosin (Mass Histology Service, Worcester,
MA). Some wild-type mice received intraperitoneal injection of A2AR specific agonist CGS
21680 (2mg/kg) or A2BR antagonist MRS1754 (2 mg/kg) 10 min before Con A.

22
3.3. Flowcytometric analysis to evaluate NKT cell-surface expression of FasL, CD40L and IL-4
production from NKT cells.
Liver mononuclear cells were prepared by density centrifugation using Percoll (GE Healthcare,
Upsalla, Sweden). The liver was pressed through stainless steel mesh (#200) and washed by
centrifugation. The pellet was resuspended in 40 % Percoll and centrifuged at 500 x g for 15 min
at room temperature to isolate liver mononuclear cells from parenchymal hepatocytes and cell
debris. The pellet was collected, treated with ACK lysing buffer (Invitrogen), and washed using
RPMI1640 medium containing 10 % FCS.
Activation-induced surface expression of CD40L and FasL on NKT cells were evaluated by
staining with fluorochrome-conjugated antibodies for NK1.1, CD3, CD40L and FasL and
analyzing by FACSCalibur (BD Biosciences).
IL-4 production from NKT cells was analyzed 2 h after Con A injection. Surface staining of the
cells with FITC-conjugated anti-NK1.1 and allophycocyanin-conjugated anti-TCR mAbs was
followed by fixation and permeabilization (Ohta et al., 2009). Cells were fixed with 4 %
parafolmaldehyde-PBS for 15 min. After washing with PBS, cells were treated with
permeabilizing buffer (50 mM sodium chloride, 5 mM EDTA, 0.02 % sodium azide, 0.5 %
Triton X-100, 10 mM Tris-HCl, pH 7.5) for 15 min. Intracellular IL-4 was stained with PE-
conjugated anti-IL-4 mAb, and the IL-4 expression in NK1.1+ TCR
+ cells was analyzed by
FACSCalibur (BD Biosciences). All antibodies were obtained from BD Biosciences.
3.4. Purification of NKT cells
Mice were pretreated by intraperitoneal injection of anti-asialo GM1 Ab (50 g/mouse; Wako
Chemicals, Richmond, VA) to deplete NK cells. After 2 days, splenocytes were labeled with

23
FITC-conjugated anti-NK1.1 mAb (BD Biosciences, San Jose, CA) and with anti-FITC
microbeads (Miltenyi Biotec, Auburn, CA). NKT cells were purified by positive selection of
NK1.1+ cells using AutoMACS separator (Miltenyi Biotec). Purity of NK1.1
+ CD3
+ cells was
higher than 90 %.
3.5. Real-time PCR
RNA was extracted from unseparated lymph node cells, purified T cells, NK cells, NKT cells
and dendritic cells using RNA STAT-60 (Tel-Test, Friendswood, TX). CD4+ T cells were
purified by a combination of FITC-conjugated anti-CD4 mAb and anti-FITC magnetic beads
(purity: >98 %). NK cells were also extracted from the spleen of RAG2-/-
mice by positive
selection of NK1.1+ cells (purity: >97 %). Dendritic cells were prepared from the bone marrow
as described below. cDNA was synthesized with random hexaprimers using Superscript first-
strand synthesis kit (Invitrogen, Carlsbad, CA). Real-time PCR was performed using SYBR
Green PCR Master Mix (Applied Biosystems, Foster City, CA) on the Applied Biosystems 7300
Real-Time PCR System (Lukashev et al., 2003). Levels of A2BR mRNA were normalized to the
amount of L32 mRNA. Primers are as follows: A2BR, ACGTGGCCGTGGGACTC and
GCAGAAGCCCAAGCTGATG;L32, AGCAACAAGAAAACCAAGCACAT and
TTGACATTGTGGACCAGGAACT.
3.6. cAMP assay
Induction of cAMP in response to adenosine receptor agonists was measured as described
previously (Ohta et al., 2009). Purified NKT cells (1 x 105) were incubated with NECA or
CGS21680 (10 M) for 15 min at 37 C in a total volume of 0.2 ml. Adenosine receptor
antagonist, ZM241385 was used at 1 M. After the incubation, 25 l of 1N hydrochloric acid

24
was added and the samples were stored at –80 C. cAMP levels were determined by ELISA (GE
Healthcare, Buckinghamshire, UK).
3.7. Bone-marrow dendritic cells
The bone marrow cells were prepared from the femur bone of C57BL/6 mice by flushing out the
bone marrow into a sterile petri dish using a syringe filled with PBS. The cells were collected in
a tube and spun down. The pellet was re-suspended in 1ml of ACK buffer and incubated for
approximately 3 min. After centrifugation, the bone marrow cells so obtained were suspended in
RPMI1640 medium containing 10 % FCS and cultured with GM-CSF (10 ng/ml) and IL-4 (10
ng/ml) in a plastic cell culture plate. Non-adherent cells were removed on the next day. After 5-7
days, the adherent cells were collected and washed at least twice with the culture media to
remove any IL-4 or GM-CSF and used to stimulate NKT cells isolated from WT, A2ARKO,
A2BRKO mice.
3.8. In vitro stimulation of NKT cells
Purified NKT cells (1.5 x 105 cells) were stimulated by -GalCer (100 ng/ml; Biomol
International, Plymouth Meeting, PA) in the presence of bone marrow-derived dendritic cells (3
x 105 cells). Following adenosine receptor agonists were added in the culture at 100 nM: 2-
chloro-N6-cyclopentyladenosine (CCPA, A1 adenosine receptor-selective agonist), CGS21680
(CGS, A2AR-selective agonist), 5’-N-ethylcarboxamidoadenosine (NECA, non-specific
adenosine receptor agonist), 1-[2-chloro-6-[[(3-iodophenyl)methyl]amino]-9H-purin-9-yl]-1-
deoxy-N-methyl--D-ribofuranuronamide (Cl-IB-MECA, A3 adenosine receptor-selective
agonist). Cells were briefly pretreated with 100nM concentration of antagonists, ZM241385
(ZM, A2AR/A2BR-selective antagonist) and MRS1754 (MRS, A2BR-selective antagonist)

25
before treatment with A2AR and A2BR agonists. CCPA, CGS, Cl-IB-MECA and ZM were
obtained from Tocris (Ellisville, MO). NECA and MRS are from Sigma (St. Louis, MO). The
cells were cultured for 24 h, and cytokine levels in the supernatant were determined by ELISA.
The affinity of the various adenosine receptor agonists and antagonists (Jacobson and Guo, 2006)
used in the current study, at the four adenosine receptor subtypes is given in the table below:
Receptor subtype compound Ki value for adenosine receptor (nM)
Agonists
A1 CCPA 0.83
A2A CGS21680 27
A3 Cl-IB-MECA 1.4
A1, A2A, A2B, A3 NECA 14(A1R) 20(A2AR) 140(A2BR) 25(A3R)
Antagonists
A2A, A2B ZM241385 1.6(A2AR) 75(A2BR)
A2B MRS1754 2
3.9. -galactosylceramide-induced hepatitis
-GalCer (2 g/mouse) was injected intravenously and serum IL-4 and IFN- levels were
determined after 2 and 6 h, respectively (Kitamura H 1999). Liver damage was assessed 24 h
after the injection by serum ALT levels and histochemistry as described for Con A-induced
hepatitis.

26
3.10. NKT cell transfer into RAG-KO mice
WT, A2ARKO and A2BRKO mice were treated with intra-peritoneal injection of anti-asialo
GM1 Ab (50 g/mouse; Wako Chemicals, Richmond, VA) to deplete NK cells. On day 2 of anti-
asialo GM1 Ab treatment, NK1.1+ cells were isolated from the splenocytes of WT and
A2ARKO mice by magnetic cell sorting. Percentage purity of NK1.1+ cells was approximately
30-35 % each time. The cell suspension was completely depleted of T cells and NK cells. WT or
A2ARKO NKT cells, thus isolated, were transferred intra-hepatically, as focal injection, into the
livers of recipient RAG1-KO or RAG2-KO mice. Each RAG-KO recipient received 2.5*10^6
(for experiment with A2ARKO) or 3.5*10^6 (for experiment with A2BRKO) cells. The RAG-
KO recipients were then challenged with Con A (20 mg/kg). The serum ALT levels were
measured at 8 hrs and 24 hrs post Con A treatment.
3.11. Exposure to Hypoxic Atmosphere
WT mice were allowed to inspire 21% O2 or 10% O2 (hypoxic atmosphere) for 1 hr prior to -
GalCer injection (i.v.) and continued hypoxia treatment after -GalCer treatment for the entire
duration till the time point of NKT cell ex-vivo analysis. For exposure to hypoxic atmosphere,
the mice were placed in air-tight modular incubation chambers (Billups-Rothenberg, San Diego,
CA, USA). Ex-vivo analysis of splenic NKT cells for surface activation markers and intracellular
cytokines production was conducted at 1 hr or 2 hrs post -GalCer (2 µg) treatment. Serum IL-4
levels were measured at 2 hrs after -GalCer treatment. For in vitro experiments, whole
splenocytes from C57Bl/6 mice were stimulated with immobilized CD1d/Fc (2 µg/ml) + -
GalCer (2 µg/ml) and cultured at either 21% oxygen or 1% oxygen. Supernatant from the
cultures were analyzed for IFN-γ after 48 hrs.

27
3.12. Statistics
Data represent mean SD. Statistical calculations were performed using Student’s t-test.
Statistical significance was accepted for p values less than 0.05.

28
4. RESULTS:
4.1 NKT cell-dependent exacerbation of liver inflammation in A2A adenosine receptor-
deficient mice
4.1.1 A2AR stimulation inhibits Con A-induced liver injury in wild type mice
With its T cell-dependent pathogenesis, Con A-induced hepatitis has been used as a model of
acute viral hepatitis (Tiegs et al., 1992, Herkel et al., 2005). The concurrent administration of
A2AR specific agonist, CGS21680 (2mg/kg) to the Con A treated WT mice significantly
suppressed serum ALT levels (Fig. 5). After injection of Con A, serum levels of IL-4 and TNF-
peaked early preceding a rise of transaminase levels. CGS also significantly suppressed the early
production (1.5hrs after Con A injection) of IL-4 and TNF-α (Fig. 5). Pharmacological
stimulation of A2ARs can protect wild type mice from Con A induced liver damage by
suppression of proinflammatory responses.
Fig 5. A2AR stimulation inhibits induction of hepatitis. Serum ALT levels were determined at
8 h. CGS treatment blocked early (1.5 h) upregulation of IL-4 and TNF-, which are necessary
to optimal induction of liver damage. ** P < 0.001 vs Con A alone. Data represent average SD
(n = 5).

29
4.1.2 NKT cells are sensitive to adenosine-A2AR inhibitory signal
Since A2AR stimulation could suppress the early production of IL-4 and TNF-α, which are
produced by NKT cells after Con A treatment (Tiegs et al., 1992, Ajuebor et al., 2003, Herkel et
al., 2005), NKT cells were examined for the susceptibility to A2AR stimulation. Activation of
NKT cells was analyzed by flowcytometry to evaluate the expression of CD40L and FasL. CGS
co-treatment was found to decrease the expression of CD40L and FasL on NKT cells, thus
causing the early inhibition of NKT cell activation (Fig. 6). The result suggests that NKT cells
are sensitive to adenosine-A2AR signal and the early inhibition of NKT cell activation may be
important to the observed suppression of Con A-induced liver injury by CGS.
Fig 6. Suppression of NKT cell activation by the injection of CGS. Panels represent CD40
ligand and Fas ligand expression on splenic NKT cells examined 1.5 h after Con A injection. The
data shown here is gated for NK1.1+ CD3
+ cells.
4.1.3 Pharmacological stimulation of A2AR suppresses NKT cell activation in vitro
To determine the adenosine receptor subtypes that are responsible for the regulation of NKT cell
activation, NK1.1+ cells were isolated from the spleen of WT C57BL/6 mice. These cells were

30
then specifically stimulated with a NKT cell ligand, α-GalCer in the presence of A1R specific
agonist (CCPA), A3R specific agonist (Cl-IB-MECA), A2AR specific agonist (CGS) and non-
specific adenosine receptor agonist (NECA).
A2AR specific agonist, CGS, could suppress IFN-γ production by NKT cells and this could be
almost completely reversed by specific antagonist, ZM241385 (Fig. 7). The non-specific agonist,
NECA could also suppress cytokine production that was reversible by ZM (Fig. 7). This
suggested that A2AR stimulation is inhibitory to NKT cell activation. However, A1 specific
agonist, CCPA did not suppress cytokine production. A3 specific agonist, IB-MECA could
suppress cytokine production to some extent but was not significant (Fig. 7). Forskolin that
directly stimulates adenylate cyclase and increases intracellular cAMP could also significantly
suppress IFN-γ production by NKT cells, indicating cAMP mediated suppression of NKT
activation (Fig. 7). The data from this experiment indicates that NKT cells may bear functional
A2ARs and that pharmacological stimulation of A2ARs on NKT cells can inhibit NKT cell
activation.

31
Fig 7. Adenosine-A2AR signaling suppresses NKT cell activation. WT splenic NK1.1+
cells
(1.5 x 105 cells) were culture-activated by -GalCer (100 ng/ml) in the presence of bone
marrow-derived dendritic cells (2 x 105 cells). Effects of adenosine receptor stimulation on NKT
activation were tested using agonist of adenosine receptors (100 nM) and antagonists (100nM).
* p < 0.01, ** p < 0.001 vs Con A alone. Data represent average SD (n = 3-5).
4.1.4. Exacerbated liver injury accompanied by exaggerated cytokines induction in Con A-
treated A2ARKO mice
To determine if endogenous adenosine regulates NKT cell activation through A2AR, A2ARKO
mice were employed. Administration of Con A to A2ARKO mice produced serum ALT levels,
approximately 5 times greater than that observed in WT mice (Fig. 8). Exacerbation of Con A-
induced liver injury in A2ARKO mice implies that endogenous adenosine produced during
hepatic inflammation can downregulate inflammation through A2AR signaling in the wild type
mice. Correspondingly, early production of cytokines, IL-4 and TNF-α was also enhanced in
A2ARKO mice (Fig. 8).

32
Fig 8. Pathophysiological regulation of inflammation by endogenously produced adenosine
via A2AR. Serum ALT levels at 8 h are shown. IL-4 and TNF- levels after Con A injection
(1.5 h) were greater in A2ARKO mice. * P < 0.01, ** P < 0.001 vs Con A alone. Data represent
average SD (n = 5).
4.1.5 NKT cell population in the liver
Since NKT cells plays a major role in Con A-induced liver injury, the exaggerated liver damage
in A2ARKO mice might be due to a qualitative or quantitative difference in the NKT cells.
Flowcytometric analysis of NK1.1+ CD3+ cell population in liver mononuclear cell preparation
revealed that the proportion of NKT cell population was almost identical in WT and A2ARKO
mice (Fig. 9). In addition, total cell numbers were comparable, ruling out the possibility of a
quantitative difference being responsible for the observed exaggerated liver damage in the
A2ARKO animals. This led us to suspect a qualitative difference in the NKT cells.

33
Fig 9. Flowcytometric analysis of NKT cells in the liver mononuclear cell preparation. The
numbers represent percentages of NK1.1+ CD3
+ cells.
4.1.6 Physiological adenosine controls NKT cell activation through A2AR signaling
To test if physiological levels of adenosine can regulate the activation of NKT cells through
A2AR, NKT cells in WT and A2ARKO mice were directly activated in-vivo by intravenous
injection of α-GalCer. α-GalCer injection produced higher serum levels of IL-4 and IFN-γ and
exaggerated serum ALT levels in A2ARKO mice as compared to the WT controls (Fig. 10). The
exaggerated NKT cell activation in vivo in the absence of A2AR signaling suggested the
pathophysiological regulation of NKT cell activation by endogenous adenosine via A2AR.
Fig 10. Exaggerated activation of NKT cells in A2AR-deficient mice. WT and A2ARKO
mice received intravenous injection of α-GalCer (2 g/mouse). (A, B) Early production of IL-4
and IFN-γ from NKT cells. (C) Liver damage as indicated by serum ALT levels 24 hrs after -
GalCer injection. * P < 0.05, ** P < 0.01, *** P < 0.001 vs WT mice. Data represent average
SD (n = 4-5).

34
4.1.7. Role of A2AR deficient NKT cells in exaggerated Con-A induced liver injury
In order to confirm the role of A2ARKO NKT cells in causing exacerbated Con A-induced
hepatitis in A2ARKO mice, it was necessary to exclude the possibility of the involvement of
other immune cells in this reaction. For this purpose, WT or A2ARKO NK1.1+ cells were
transferred into the livers of recipient RAG1-KO mice, which lack T cells, B cells and NKT
cells. The RAG1-KO recipients were then challenged with Con A (20 mg/kg). The RAG1KO
mice that received the A2AR-deficient NKT cells had higher serum ALT levels (Fig. 11). The
result confirms the crucial role of A2AR-deficient NKT cells in causing exacerbated liver
damage in A2AR-deficient mice.
Fig. 11 A2ARKO NKT cells caused exaggerated hepatitis in RAG1-KO recipient mice. WT
or A2ARKO NKT cells were transferred intra-hepatically into RAG1-KO mice (2.5*10^6
cells/RAG1-KO mouse). The RAG1-KO recipients were then challenged with Con A (20
mg/kg). The serum ALT levels were measured at 8 hrs post Con A treatment. Data represent
average SD of 3 mice and is representative of 2 independent experiments. *, p < 0.05

35
Based upon the results obtained in chapter 4.1, the following can be inferred:
1. NKT cells have functional expression of A2A adenosine receptor and the stimulation of
A2AR results in down-regulation of NKT cell activation.
2. A2AR deficiency results in exaggerated activation of NKT cells during hepatitis.
3. Endogenous adenosine can regulate activation of NKT cells through A2A receptor
signaling.
4.2 Immunoregulation by physiological levels of adenosine via A2B adenosine receptor
4.2.1 In vitro evidence of A2BR-mediated inhibition of NKT cell activation
To analyze the functional expression of A2BR on NKT cells, NKT cells were directly stimulated
in vitro with -GalCer together with various adenosine receptor agonists. In the WT NKT cells,
a non-specific adenosine receptor agonist NECA strongly inhibited NKT cell activation as
indicated by the suppression of IFN- production (Fig. 12A). Corresponding to A2AR expression
in NKT cells as shown previously, A2AR selective agonist CGS blocked IFN- production from
WT and A2BRKO NKT cells, but not A2ARKO cells (Fig. 12B,C,D). In addition,
A2AR/A2BR-selective antagonist ZM241385, but not A2BR-selective antagonist MRS1754,
completely abolished the suppressive effect of NECA in wild-type NKT cells (Fig. 12B). These
results again confirmed immunosuppressive role of A2AR on NKT cells.
To specifically determine A2BR-mediated response, NKT cells were examined to see if NECA
was inhibitory even in the absence of immunosuppressive effect of A2AR. Interestingly,
A2ARKO NKT cells were still vulnerable to NECA as shown by a 50 % reduction in IFN-
production (Fig 12C). Since A1 and A3 adenosine receptors are not involved in this inhibition

36
(Fig12A), A2BR was suspected to be suppressive to NKT cell activation. (Fig 12B,C,D)
Importantly, MRS1754 (A2BR-selective antagonist) blocked NECA-mediated inhibition of
A2ARKO NKT cells supporting immunosuppressive role of A2BR in NKT cells.
Fig 12. A2BR stimulation is suppressive to the activation of NKT cells. (A) Purified WT
NKT cells were stimulated by -GalCer in the presence of DCs cells. IFN- levels in the culture
supernatant were determined after 24 hrs. (B,C,D) NKT cells were purified from WT, A2ARKO,
and A2BRKO mice. Data represent average SD of triplicate samples and are representative of
3 independent experiments. *, p < 0.05; **, p < 0.01 vs controls.
4.2.2 Expression of A2BR mRNA in NKT cells
Expression of A2BR mRNA was also tested in NKT cells. For verification of real-time PCR
assay, dendritic cells which are known to express A2BR (Novitsky et al., 2008; Haskó et al.,

37
2009), were employed as a positive control. Real-time PCR confirmed A2BR mRNA at high
levels in dendritic cells, whereas the A2BR mRNA content was much lower in unseparated
lymph node cells (Fig. 13). A2BR mRNA levels were further analyzed in purified lymphocyte
subsets. Comparing to low levels of expression in conventional T cells and NK cells, A2BR
mRNA levels were notably higher in NKT cells (Fig. 13) suggesting relatively abundant
expression of A2BR in NKT cells.
Fig 13. A2BR mRNA levels were quantified by real-time PCR. Samples are unseparated
lymph node cells (LN), purified CD4+ T cells (Th), purified NK cells (NK), purified NKT cells
(NKT) and dendritic cells (DC). A2BR mRNA levels were standardized on the basis of L32
mRNA levels.
4.2.3 Functional expression of A2BR on NKT cells
To test if NKT cells express functional A2BRs, cAMP responses after A2BR stimulation were
tested. WT NKT cells increased cAMP in response to non-selective adenosine receptor agonist,

38
NECA (Fig. 14). A2AR/A2BR-selective antagonist ZM241385 blocked this increase. A2AR-
selective stimulation by CGS21680 induced cAMP in WT NKT cells, but not in A2ARKO cells,
confirming A2AR expression on NKT cells. A2ARKO NKT cells were still able to increase
cAMP levels in response to NECA (Fig. 14) suggesting cAMP induction via A2BR. Since
ZM241385 blocked this increase, it suggests that A2BRs expressed on NKT cells are
functionally active and can signal by the upregulation of intracellular cAMP.
Fig 14. Functional expression of A2BR on NKT cells. Purified NKT cells were incubated with
CGS21680 (A2AR-selective agonist) or NECA (non-specific adenosine receptor agonist), and
cAMP levels were determined by ELISA. ZM241385 (A2AR/A2BR antagonist) blocked cAMP
induction by NECA. Data represent average SD of triplicate samples and are representative of
2 independent experiments. *, p < 0.05 vs untreated NKT cells. †, p < 0.05 vs NECA-treated
NKT cells.

39
4.2.4 Exacerbation of inflammatory liver damage in the absence of A2BR
NKT cells were found to express A2AR and A2BR and stimulation of both receptors are
inhibitory to NKT cell activation. As it was observed with A2AR, similar immunoregulatory role
could be expected for A2BR on NKT cells. Indeed, intravenous injection of Con A (13 mg/kg)
induced quite stronger liver damage in A2BRKO mice as compared to intermediate liver damage
in WT mice (Fig. 15).
The enhanced liver damage was reproducible in WT mice co-treated with A2BR-selective
antagonist, MRS 1754. Intravenous injection of Con A into MRS 1754-treated C57BL/6 mice
resulted in stronger liver damage than control mice (Fig. 15). These results suggested that Con A
induced hepatitis is under the physiological regulation of adenosine-A2BR signaling and the
interruption of this pathway by genetic deletion or pharmacological antagonism of the receptor
resulted in exacerbation of liver damage.

40
Fig 15. Exacerbation of inflammatory liver damage in the absence of
A2BR. (A) Exaggerated Con A-induced acute hepatitis in A2BRKO mice. A2BRKO and WT
mice (n = 5) received intravenous injection of Con A (13 mg/kg). Serum ALT levels were
determined after 8 and 24 h. (B) A2BR antagonist MRS1754 (2 mg/kg, i.p.) enhanced Con A-
induced liver injury in WT mice. Serum ALT levels were determined 8 h after Con A injection.
Data represent average ± SD of 5 mice and are representative of 4 independent experiments. The
statistical significance was calculated by Student’s t-test: *, p < 0.05; **, p < 0.01.
4.2.5 Exaggerated cytokines induction in Con A-treated A2BR-KO mice
In Con A-injected A2BRKO mice, cytokines production was also found to increase (Fig 16),
suggesting that exaggerated inflammatory responses in A2BRKO mice resulted in the
exacerbation of liver damage. Robust increase of Con A-induced cytokines production including
IL-4 in A2BRKO mice (Fig. 16) suggested the enhancement of NKT cell activation in A2BRKO
mice as it was the case in A2ARKO mice (Fig 8).
Fig 16. Exaggerated inflammatory response in A2BRKO mice. Serum cytokine levels in Con
A-injected mice were determined after 1.5 h (IL-4 and TNF-) and 8 h (IFN-). Black bars, WT
C57BL/6 mice; gray bars, A2BRKO mice. Data represent average SD of 5 mice and are

41
representative of 4 independent experiments. The statistical significance was calculated by
Student’s t-test: *, p < 0.05; **, p < 0.01.
4.2.6 Identical percentage of NKT cells in WT and A2BRKO mice
Flowcytometric analysis showed that WT and A2BRKO mice contain equivalent proportion of
NKT cells in the liver (Fig. 17). Since the total cell numbers were comparable, it was confirmed
that there was no numerical difference in NKT cells of these mice.
Fig 17. Flowcytometric analysis of NKT cells from the liver. NKT cells were observed at
similar frequency in WT and A2BRKO mice. The numbers represent percentages of NK1.1+
CD3+ cells.
4.2.7 Enhanced IL-4 production from NKT cells in A2BRKO mice
Although no quantitative difference was observed, there was a qualitative difference in NKT cell
response. Two hours after the injection of Con A, cellular IL-4 production was immediately
analyzed by intracellular staining. Increases in IL-4 production were detectable in NKT cells
from both WT and A2BRKO mice, but Con A injection induced higher levels of IL-4 from

42
A2BRKO NKT cells (Fig. 18). The result suggested that early activation and resultant cytokine
production from NKT cells is under the regulation of adenosine-A2BR signal.
Fig 18. Enhanced production of IL-4 by A2BRKO NKT cells. Two hours after Con A
injection, IL-4 was detected by intracellular staining ex vivo. The data shown here is gated for
NK1.1+ TCR
+ cells. Control cells are from untreated WT mouse.
4.2.8 Physiological adenosine controls NKT cell activation through A2BR
To test whether physiological levels of adenosine can regulate NKT cell activation via A2BR
stimulation, WT and A2BRKO mice received intravenous injection of -GalCer (2µg/mouse). It
was found that direct stimulation of A2BRKO NKT cells in vivo induced stronger
proinflammatory cytokines resulting in more extensive hepatic damage (Fig. 19). This implies
the pathophysiological regulation of NKT cell activation by endogenous adenosine via A2BR on
NKT cells.

43
Fig. 19 Endogenous adenosine regulates NKT cells via A2BRs. (Left and center panels) -
GalCer (2 g/mouse) was injected intravenously and the increase of serum IL-4 and IFN- levels
was monitored after 2hrs and 6 hrs, respectively. (Right panel) -GalCer-induced hepatic
damage was evaluated after 24 hrs by serum ALT levels. Black bars, WT C57BL/6 mice; gray
bars, A2BRKO mice. Data represent average SD of 5 mice and are representative of 4
independent experiments. *, p < 0.05; **, p < 0.01.
4.2.9. Role of A2BR deficient NKT cells in exaggerated Con A induced liver injury
In order to confirm the role of A2BRKO NKT cells in causing exaggerated Con A-induced
hepatitis in A2BRKO mice, WT or A2BRKO NK1.1+ cells were transferred into the livers of
recipient RAG2-KO mice. After the injection of Con A, the RAG2KO mice that received the
A2BR-deficient NKT cells had higher serum ALT levels (Fig. 20). The result confirms the
crucial role of A2BR-deficient NKT cells in the exacerbated liver damage in A2BR-deficient
mice.

44
Fig. 20. A2BRKO NKT cells caused exaggerated hepatitis in RAG2-KO recipient mice. WT
or A2BRKO NKT cells were transferred intra-hepatically into RAG2-KO mice (3.5*10^6
cells/RAG2-KO mouse). The RAG2-KO recipients were then challenged with Con A (16
mg/kg). The serum ALT levels were measured at 8 hrs post Con A treatment. Data represent
average SD of 3 mice and is representative of 2 independent experiments. *, p < 0.05.
Based upon the results for chapters 4.1 and 4.2, the following can be inferred:
1. NKT cells express functional A2A and A2B adenosine receptors.
2. Stimulation of A2AR and A2BR on NKT cells suppresses NKT cell activation.
3. Adenosine-A2AR/A2BR signaling pathway is involved in the physiological regulation of
NKT cell activation during acute hepatitis.

45
4.3 Hypoxia mediated regulation of NKT cell activation.
4.3.1 In-vitro evidence for hypoxia mediated suppression of NKT cell activation.
The results from chapters 4.1 and 4.2 provide evidence for adenosine mediated regulation of
NKT cell activation. Since hypoxia regulates extracellular adenosine levels, we investigated the
effect of hypoxia on NKT cell activation. To determine the effect of hypoxia on NKT cell
activation in vitro, whole splenocytes from C57Bl/6 mice were stimulated by immobilized
CD1d/Fc + α Gal Cer in either 21% O2 or 1% O2. The NKT cell culture activated under hypoxia
produced lower levels of IFN-γ (Fig. 21). Hypoxia was found to be suppressive to NKT cell
activation in vitro.
Fig. 21. Hypoxia is suppressive to NKT cell activation. Whole splenocytes from C57Bl/6 mice
were culture activated by immobilized CD1d/Fc + α Gal Cer (4:1). Cells were cultured in either
21% O2 or 1% O2. IFN-γ levels in the 48hr culture supernatant were measured by ELISA. Data
represent average SD of triplicate samples and are representative of 2 independent
experiments. * p < 0.05

46
4.3.2 Hypoxia is suppressive to the early activation of NKT cells iv vivo after α-GalCer
treatment.
To determine the effect of hypoxia on NKT cell activation in vivo, C57BL/6 mice were allowed
to inspire 10% O2 and received α-GalCer (2µg) injection. Control C57BL/6 mice were allowed
to inspire 21% O2. Activation markers CD69 and CD40L were analyzed on splenic NKT cells.
Untreated C57Bl/6 splenocytes were analyzed to estimate the basal levels of CD69 and CD40L
expression on NKT cells. Approximately 35% of splenic NKT cells from untreated mice were
found to constitutively express CD69 and 1-2% splenic NKT cells were found to express CD40L
(Fig. 22). Surprisingly, it was found that hypoxia treatment alone upregulated CD69 expression
on NKT cells from mice that were not treated with α-GalCer. CD40L expression was not
affected by hypoxia alone (Fig. 23).
Fig. 22 Basal level of CD69 and CD40L expression on splenic NKT cells. Panel on the left
represents basal level of CD69 expression on splenic NKT cells. Panel on right represents basal
level of CD40L expression on splenic NKT cells. The numbers represent the percentage of NKT
cells in each quadrant.

47
Fig. 23 Hypoxia alone upregulates CD69 expression on NKT cells. WT mice were exposed to 10%
oxygen for 1 hr. Panel on the left represents CD69 expression on splenic NKT cells. Panel on right
represents CD40L expression on splenic NKT cells. The numbers represent the percentage of
NKT cells in each quadrant. Panels representative of 3 mice.
CD69 was upregulated within 1 hr of α-GalCer treatment and continues to increase at 2 hrs (Fig.
24). NKT cells in the hypoxia treated mice also activated in response to α-GalCer. However,
hypoxic treatment suppressed the activation of NKT cells as seen by lower percentage of CD69+
NKT cells after hypoxic exposure (Fig. 24). It should be noted that hypoxia treatment alone
could increase CD69 expression (Fig. 23). After subtraction of hypoxia-induced CD69 as
background levels, normoxia versus hypoxia difference in CD69+ cells after α-GalCer might be
more distinct.

48
Fig. 24. Hypoxia mediated regulation of NKT cell activation in vivo. C57Bl/6 mice were
allowed to inspire 21% O2 or 10% O2 and were challenged with α-GalCer (2µg). CD69
upregulation on splenic NKT cells was analyzed at 1 hr and 2 hrs after α-GalCer injection. The
numbers represent the percentage of NKT cells in each quadrant. The panel is representative of 3
mice. The percentage of CD69+ cells was calculated within NK1.1+ CD3+ cells. The statistical
significance was calculated by Student’s t-test: * P< 0.05 vs 21% O2.
α-GalCer treatment increased CD40L+ NKT cells after 1 hr and the levels remained almost
constant when measured at 2 hrs (Fig. 25). However, hypoxic treatment significantly delayed the
upregulation of CD40L on NKT cells after α-GalCer treatment (Fig. 25).

49
Fig. 25. Hypoxia mediated regulation of NKT cell activation in vivo. C57Bl/6 mice were
allowed to inspire 21% O2 or 10% O2 and were challenged with α-GalCer (2µg). CD40L
upregulation on splenic NKT cells was analyzed at 1 hr and 2 hrs after α-GalCer injection. The
numbers represent the percentage of NKT cells in each quadrant. The panel is representative of 7
mice. The percentage of CD40L+ cells was calculated within NK1.1+ CD3+ cells. The statistical
significance was calculated by Student’s t-test: * p< 0.05 vs 21% O2.
4.3.3 Hypoxia is suppressive to cytokines production from NKT cells.
To determine the effect of hypoxia on NKT cell function in vivo, analysis for intracellular IL-4
and IFN-γ production from splenic NKT cells was done post α-GalCer treatment. IL-4 producing

50
NKT cells were detectable as early as 1 hr after α-GalCer treatment. The percentage of IL-4
producing NKT cells increased even more at 2 hrs after α-GalCer treatment (Fig. 26). However,
hypoxic exposure suppressed IL-4 production from NKT cells. Correspondingly, hypoxia treated
mice had lower serum IL-4 levels when measured at 2 hrs after α-GalCer treatment (Fig. 27).
Fig. 26. Hypoxia mediated suppression of NKT cell function in vivo. C57Bl/6 mice were
allowed to inspire 21% O2 or 10% O2 and were challenged with α-GalCer (2µg). Intracellular
IL-4 production from splenic NKT cells was analyzed at 1 hr and 2 hrs after α-GalCer injection.
The numbers represent the percentage of NKT cells in each quadrant. The panel is representative
of 3 mice. The percentage of IL-4+ cells was calculated within NK1.1+ CD3+ cells. The
statistical significance was calculated by Student’s t-test: * p< 0.05 vs 21% O2.

51
Fig. 27. Hypoxia mediated suppression of serum IL-4 levels after α-GalCer treatment.
C57Bl/6 mice were allowed to inspire 21% O2 or 10% O2 and were challenged with α-GalCer
(2µg). Serum IL-4 levels were measured at 2 hrs after α-GalCer injection by ELISA. Data
represent average SD of 3 mice. The statistical significance was calculated by Student’s t-test:
* p< 0.05 vs 21% O2.
Intracellular IFN-γ production from NKT cells could be detected as early as 2 hrs post α-GalCer
treatment. Hypoxia severely suppressed IFN-γ production from NKT cells in response to α-
GalCer induced activation (Fig. 28).

52
Fig. 28. Hypoxia mediated suppression of NKT cell function in vivo. C57Bl/6 mice were
allowed to inspire 21% O2 or 10% O2 and were challenged with α-GalCer (2µg). Intracellular
IFN-γ production from splenic NKT cells was analyzed at 2 hrs after α-GalCer injection. The
numbers represent the percentage of NKT cells in each quadrant. The panel is representative of 3
mice. The percentage of IFN-γ+ cells was calculated within NK1.1+ CD3+ cells. The statistical
significance was calculated by Student’s t-test: * p< 0.05 vs 21% O2.
The results obtained in the current study show hypoxia mediated suppression of NKT cell
activation in vitro and in vivo in response to -GalCer. The whole body exposure of C57Bl/6
mice to hypoxia inhibited -GalCer induced early upregulation of activation markers and
cytokines production.
4.3.4 Partial involvement of A2AR in the inhibition of NKT cells by hypoxia.
Since in the current study, NKT cells were found to be under the physiological regulation of
adenosine-A2AR/A2BR pathway (chapters 4.1 and 4.2) and since whole body exposure to
hypoxic air has been found to elevate blood adenosine levels (Chouker et al., 2008), it was
reasonable to speculate that adenosine-A2AR/A2BR signaling could be one possible mechanism

53
by which hypoxia could exert suppressive effect on NKT cell activation. To test this hypothesis,
WT and A2ARKO mice were allowed to inspire hypoxic atmosphere and received α-GalCer
(2µg) injection. Activation marker CD40L was analyzed on splenic NKT cells 1 hr after α-
GalCer treatment. As observed previously (Fig. 25), hypoxia was suppressive to the upregulation
of CD40L on WT NKT cells as compared to 21% oxygen (Fig. 29). Interestingly, hypoxia also
suppressed CD40L upregulation in A2ARKO NKT cells as compared to 21% oxygen (Fig. 29).
The result implied that hypoxia is suppressive to NKT cell activation irrespective of A2AR
expression.
Fig. 29. Hypoxia regulates WT and A2ARKO NKT cell activation in vivo. WT and
A2ARKO mice were allowed to inspire 21% O2 or 8% O2 and were challenged with α-GalCer
(2µg). CD40L upregulation on splenic NKT cells was analyzed at 1 hr after α-GalCer injection.
The numbers represent the percentage of NKT cells in each quadrant. The panel is representative

54
of 4 mice. The percentage of CD40L+ cells was calculated within NK1.1+ CD3+ cells. The
statistical significance was calculated by Student’s t-test: * p< 0.05 vs 21% O2.
The effect of hypoxia on cytokines production from WT and A2ARKO NKT cells was tested. In
21% oxygen group, A2ARKO NKT cells produced more IFNγ than WT NKT cells (Fig. 30).
Correspondingly, serum IFNγ levels in A2ARKO mice were higher than WT mice (Fig. 31)
which is consistent with the previous finding that A2AR deficiency causes exaggerated NKT
cells activation (Fig. 10). In these experiments, exposure to hypoxic air very strongly suppressed
IFNγ production from WT NKT cells (Fig. 30), however, there were still massive IFNγ-
producing NKT cells in hypoxia-treated A2ARKO mice (Fig. 30). Consistent with this result,
A2ARKO mice breathing hypoxic air showed significantly higher serum IFNγ levels as
compared to the WT mice (Fig. 31). The fact that hypoxia could not reduce NKT cell function of
A2ARKO mice to the levels of WT mice strongly suggests the involvement of A2AR-mediated
mechanism downstream hypoxia. However, participation of A2AR-mediated mechanism in
hypoxia-triggered NKT suppression was partial because hypoxia could largely suppress NKT
cell activation even in the absence of A2AR.

55
Fig. 30. A2AR involves partly in the mechanism of hypoxia mediated suppression of NKT
cell function in vivo. WT and A2ARKO mice were allowed to inspire 21% O2 or 8% O2 and
were challenged with α-GalCer (2µg). Intracellular IFNγ production from splenic NKT cells
was analyzed at 2 hrs after α-GalCer injection. The numbers represent the percentage of NKT
cells in each quadrant. The panel is representative of 4 mice. The percentage of IFN-γ+ cells was
calculated within NK1.1+ CD3+ cells. The statistical significance was calculated by Student’s t-
test: * p< 0.05 vs 21% O2.

56
Fig. 31. A2AR involves partly in the mechanism of hypoxia mediated suppression of NKT
cell function in vivo. WT and A2ARKO mice were allowed to inspire 21% O2 or 8% O2 and
were challenged with α-GalCer (2µg). Serum IFNγ levels were measured at 2 hrs after α-GalCer
injection by ELISA. Data represent average SD of 4 mice. The statistical significance was
calculated by Student’s t-test: * p< 0.05 vs 21% O2.

57
A2BR does not involve in the regulation of NKT cells by hypoxia
Another possible cause of hypoxia-mediated regulation of NKT cells activation was A2BR-
mediated inhibition. To test this hypothesis, WT and A2BRKO mice were allowed to inspire
hypoxic atmosphere and received α-GalCer (2µg) injection. As observed previously (Fig. 25),
hypoxia was suppressive to the upregulation of CD40L on WT NKT cells as compared to 21%
oxygen (Fig. 32). Hypoxia also suppressed CD40L upregulation in A2BRKO NKT cells as
compared to 21% oxygen (Fig. 32). The result implied that hypoxia is suppressive to NKT cell
activation irrespective of A2BR expression.

58
Fig. 32. Hypoxia regulates WT and A2BRKO NKT cell activation in vivo. WT and
A2BRKO mice were allowed to inspire 21% O2 or 8% O2 and were challenged with α-GalCer
(2µg). CD40L upregulation on splenic NKT cells was analyzed at 1 hr after α-GalCer injection.
The numbers represent the percentage of NKT cells in each quadrant. The panel is representative
of 4 mice. The percentage of CD40L+ cells was calculated within NK1.1+ CD3+ cells. The
statistical significance was calculated by Student’s t-test: * p< 0.05 vs 21% O2.
The effect of hypoxia on cytokines production from WT and A2BRKO NKT cells was also
tested. Exposure to hypoxic air strongly suppressed IFNγ production from both WT and
A2BRKO NKT cells (Fig. 33.) The fact that hypoxia could suppress NKT cell function in
A2BRKO mice to similar extent as in WT mice implies that A2BR does not involve in the
hypoxia triggered downregulation of NKT cells.

59
Fig. 33. A2BR does not involve in the mechanism of hypoxia mediated suppression of NKT
cell function in vivo. WT and A2BRKO mice were allowed to inspire 21% O2 or 8% O2 and
were challenged with α-GalCer (2µg). Intracellular IFNγ production from splenic NKT cells
was analyzed at 2 hrs after α-GalCer injection. The numbers represent the percentage of NKT
cells in each quadrant. The panel is representative of 4 mice. The percentage of IFN-γ+ cells was
calculated within NK1.1+ CD3+ cells. The statistical significance was calculated by Student’s t-
test: * p< 0.05 vs 21% O2.

60
Discussion
For the induction of liver diseases, immunoregulatory roles for adenosine have been described in
various experimental models. Treatment of animals with A2AR agonists blocked induction of
hepatitis and upregulation of proinflammatory cytokines (Harada et al., 2000; Ohta and
Sitkovsky, 2001; Odashima et al., 2005). Previous studies have demonstrated the exaggeration of
hepatitis by the lack of adenosine-A2AR signaling by using pharmacological antagonism of
A2AR as well as genetic deletion of A2AR, suggesting critical contribution of the adenosine-
mediated physiological immunoregulatory mechanism in the liver (Ohta and Sitkovsky, 2001;
Ohta et al., 2007). However, the critical cellular target of ‘adenosine-A2AR’ anti-inflammatory
pathway in acute hepatitis is not known. The current study was conducted to understand the
mechanism of adenosine mediated hepatoprotection during acute hepatitis.
Since NKT cells play a central role in the pathogenesis of acute hepatitis, it was hypothesized in
the current study that NKT cells may be under the control of adenosine mediated anti-
inflammatory signaling during hepatitis. The present findings provide evidence that endogenous
adenosine signaling through A2AR is suppressive to the activation of NKT cells. Lappas et al.
(2006) showed the suppression of NKT cell-dependent induction of hepatic ischemia-reperfusion
injury by A2AR agonist. In an agreement with this report, A2AR agonists induced cAMP in
NKT cells (Fig. 14) and inhibited NKT cell activation (Fig. 12A, 12B). The inhibition of
cytokines production and NKT cell activation as shown by the decrease of CD40L and FasL
expression showed that NKT cells are indeed sensitive to adenosine-A2AR inhibitory signal
(Fig. 6).

61
However, it was not known whether A2AR plays role in pathophysiological regulation of NKT
cells. Exaggerated pro-inflammatory cytokines production along with exaggerated liver damage
in α-GalCer treated A2AKO mice demonstrated physiological control of NKT cell activation
through A2AR (Fig. 10). The current study confirmed the important role of A2AR deficient
NKT cells in the exacerbation of Con A induced liver injury (Fig. 11).
Although adenosine has been known to modulate liver diseases via A2AR, the involvement of
A2BR was not known. The current study provides evidence that endogenous adenosine signaling
through A2BR, in addition to A2AR, is suppressive to the induction of acute hepatitis. A series
of in vitro studies strongly suggested the inhibitory role of A2BR on NKT cells. Being coupled
to Gs-protein like A2AR, A2BR could inhibit NKT cells possibly through the upregulation of
immunosuppressive cAMP. Indeed, cAMP induction by an adenylate cyclase activator forskolin
strongly inhibited NKT cell activation (Fig. 12A), and A2BR stimulation increased cAMP levels
in NKT cells (Fig. 14).
Exacerbation of Con A-induced liver injury by blocking adenosine-A2BR signalling
demonstrated that A2BR is also involved in the physiological regulation of hepatitis (Fig. 15).
Robust increase of Con A-induced cytokines production including IL-4 in A2BRKO mice (Fig.
16) suggested the enhancement of NKT cell activation in A2BRKO mice as it was the case in
A2ARKO mice (Fig 8). This result was supported by the enhanced production of IL-4 from Con
A stimulated A2BRKO NKT cells (Fig. 18). Exaggerated liver damage accompanied by
enhanced production of cytokines upon direct activation of NKT cells in vivo by -GalCer in
A2BRKO mice demonstrated that physiological levels of adenosine controlled NKT cell
activation through A2BR in the WT mice (Fig. 19). Importantly, the extent of NKT cell
activation and subsequent liver damage in A2BRKO mice were augmented even though the mice

62
still express A2AR. It was further confirmed that A2BR-deficiency on NKT cells could, at least
in part, account for the exacerbation of Con A-induced liver injury (Fig. 20). The results strongly
suggest non-redundancy of A2BR in the negative regulation of NKT cells and hepatic
inflammation.
For the confirmation of the role of A2AR-deficient and A2BR-deficient NKT cells, it was
necessary to exclude immune cells that could involve in the reaction. For this purpose, WT or
A2ARKO or A2BRKO NKT cells were isolated and transferred intra-hepatically into RAG1KO
mice. The transferred cell suspension was completely devoid of NK cells and T cells and was
enriched in NKT cells. However, the transferred cell suspension still contained about 65% non-
NKT cells. Although these contaminated cells are not likely to contribute to the induction of Con
A-hepatitis (Kaneko et al., 2000), purer NKT cell suspension should be used in order to
completely rule out the possibility of participation of other cells.
Recent studies have revealed significant involvement of A2BR in vascular, pulmonary and
intestinal inflammation (Sun et al., 2006; Yang et al., 2006; Mustafa et al., 2007; Eckle et al.,
2008; Kolachala et al., 2008; Frick et al., 2009; Zhou et al., 2009); however, papers reported
controversial roles for A2BR, i.e. pro- and anti-inflammatory. The reason for this discrepancy is
not known, but it may be due to involvement of various cell types that respond to A2BR
stimulation in different ways. A variety of cell types are expressing functional A2BR, e.g.
endothelial cells, epithelial cells, fibroblasts, macrophages and mast cells (Haskó et al., 2009).
A2BR affects cellular functions in various ways dependent on cell types. Differences in the
involvement of these cells in each disease model may affect overall pro- or anti-inflammatory
roles of A2BR. For example, A2BR may play a proinflammatory role in mast cells because

63
A2BR stimulation may contribute to allergic asthma through the induction of IL-13 and vascular
endothelial growth factor (VEGF) in mast cells (Ryzhov et al., 2008), although mast cells from
A2BRKO mice are also reported to increase sensitivity to IgE-mediated anaphylaxis (Hua et al.,
2007). In macrophages and dendritic cells, A2BR stimulation enhances IL-6 production in
response to inflammatory stimuli (Ryzhov et al., 2008). However, it is important to note that the
same treatment of dendritic cells also induces various immunoregulatory molecules including IL-
10, TGF-, cyclooxygenase-2 and indoleamine-2,3-dioxygenase (Novitskiy et al., 2008).
Correspondent to the induction of anti-inflammatory molecules, A2BR stimulation reduced the
capacity of antigen-presenting cells to activate T cells (Novitskiy et al., 2008). A2BR also
positively regulate IL-10 production from intestinal epithelium (Frick et al., 2009).
The direct effect of A2BR on lymphocytes is not known. The current study demonstrates the
expression of functional A2BR on NKT cells and inactivation of NKT cells by direct stimulation
of A2BR. The elevation of intracellular cAMP by activation of Gs-coupled A2BR certainly
seems to be one mechanism of negative regulation of NKT cell activation. Another mechanism
could be A2BR mediated induction of IL-6 production. Pre-exposure to IL-6 is known to
inactivate NKT cells and to suppress subsequent Con A-induced liver injury (Nishikage et al.,
1999; Sun et al., 2004). Interestingly, A2BR stimulation can enhance IL-6 production (Ryzhov et
al., 2008). Therefore, it is also possible that A2BR indirectly suppresses NKT cell activation by
increasing IL-6 levels.
Taken together, NKT cells express functional A2AR and A2BR and endogenously produced
adenosine signals through these receptors to negatively regulate NKT cell activation. Interruption
of such adenosine signaling results in much exaggerated activation of NKT cells during hepatitis.
Thus, adenosine can regulate activation of NKT cells in vivo.

64
The current study showed that both A2AR and A2BR are non-redundantly involved in the
endogenous regulation of NKT during hepatitis. However, it is unclear why both A2AR and
A2BR would be needed for regulating NKT cell activity in vivo. There is a question if A2AR and
A2BR mediated suppression of NKT cell activation are two independent mechanisms or if the
receptors can compensate for one another or if they can cooperate to cause an additive or
synergistic suppression of NKT cell activation. It may be possible to speculate that since A2AR
is a high affinity adenosine receptor, it may be recruited earlier during inflammation and as
adenosine levels increase during the course of inflammation, low affinity-A2BR may also be
recruited in the regulation of NKT cells. Together A2AR and A2BR may increase the threshold
for NKT cell activation in the presence of endogenous adenosine which may critically suppress
NKT cell-mediated hepatic inflammation. Another possibility is that A2AR and A2BR may form
homo or heterodimers. The dimers may have different signalling pathway downstream as
compared to the individual receptors. It is interesting to investigate if adenosine receptors
dimerize and if receptor dimers can regulate NKT cells activation.
Hypoxic environment has been known to be suppressive to certain immune functions. The extent
of activation of immune cells is thought to change depending on the oxygen tension surrounding
the cells (Ohta et al, 2011). T cell proliferation was significantly decreased when cultured at
physiologically relevant levels of oxygen (1-5% oxygen) when compared to proliferation at 21%
oxygen (Loeffler et al., 1992; Naldini et al., 1997; Atkuri et al., 2005, 2007; Larbi et al., 2010).
Low oxygen tension during culture suppressed IL-2 and IFNγ production from activated T cells
(Zuckerberg et al, 1994; Caldwell et al., 2001; Kim et al., 2008; Roman et al., 2010). Also, the
development of cytotoxic T cells in the mixed lymphocyte culture was suppressed by less
oxygenated culture condition (Yang et al., 2009; Wang et al., 2010). A recent study

65
demonstrated that T cell activation in vivo correlated positively with oxygen tension. In the
study, whole body exposure of mice to hypoxic air (8% oxygen) suppressed but hyperoxic air
(100% oxygen) enhanced T cell activation as compared to 21% oxygen (Ohta et al., 2011).
In those animals exposed to hypoxic atmosphere, there was an increase in blood adenosine levels
and strongly suppressed the induction of Con A-induced liver injury in an A2AR-dependent
manner (Chouker et al., 2008). The current findings demonstrate that hypoxia can strongly
suppress activation of NKT cells both in vivo and in vitro. Since NKT cell activation is crucial to
the induction of Con A hepatitis, hypoxic immunosuppression targeting NKT cells is likely to
play a role in the inhibition of hepatitis induction.
Hypoxia triggers the accumulation of extracellular adenosine by accelerating the breakdown of
ATP (Sitkovsky et al., 2004). In the current study, NKT cells were found to be under the control
of adenosine-A2AR/A2BR signaling. Therefore, the ‘adenosine-A2AR/A2BR’ pathway was
suspected to contribute to the observed suppression of NKT cells activation by hypoxic
exposure. A2AR was involved in the mechanism of hypoxic NKT cell suppression, but its
contribution was limited. Indeed, hypoxia could suppress NKT cells activation irrespective of the
presence of A2AR to some extent. This result suggested that hypoxia renders strong inhibitory
effects on NKT cell activation partly through A2AR-dependent mechanism. For the ‘A2AR-
independent’ portion of hypoxia-triggered NKT cell suppression, it was examined whether the
‘adenosine-A2BR’ pathway contributed or not. Previous studies have demonstrated hypoxia-
mediated induction of A2BR on endothelial cells (Kong et al., 2006) and involvement of A2BR
in the hypoxia-mediated inhibition of neutrophil transepithelial migration (Rosenberger et. al.
2008). Together with these previous studies, the current study suggested possible involvement of

66
A2BR downstream hypoxia; however, A2BR was not found to involve in hypoxia-mediated
suppression of NKT cell activation.
The ‘A2AR-independent’ pathway of hypoxia-mediated NKT cell regulation may involve
several other possibilities that need to be explored. One possibility is the involvement of the
transcription factor, hypoxia inducible factor-1α, (HIF-1α). Under hypoxic conditions, HIF-1α is
stabilized and it helps cells to adapt to hypoxia by switching the energy metabolism from
oxidative phosphorylation to anaerobic metabolism (Majmundar et al., 2010). The reduced
supply of ATP from the anerobic pathway might be one reason why activation of lymphocytes is
compromised under hypoxic condition. HIF-1α has been shown to suppress T cell signaling after
TCR crosslinking (Neumann et al., 2005). Also, deletion of HIF-1α from T cells resulted in
increased IFNγ production from these cells (Lukashev et al., 2006; Guo et al., 2009).
In conclusion, the current study demonstrates that NKT cells are under the control of endogenous
adenosine during hepatitis. Endogenous adenosine signals through A2AR and A2BR to down
regulate NKT cell activation during hepatitis. In addition, the current study also demonstrates
that hypoxia is suppressive to NKT cell activation and function. Taken together, ‘hypoxia-
adenosine anti-inflammatory pathway’ may play a crucial role in the pathogenesis of acute
hepatitis.

67
REFERENCES:
Ajuebor, M.N., Hogaboam, C.M., Le, T., and Swain, M.G. (2003). “C-C chemokine ligand
2/monocyte chemoattractant protein-1 directly inhibits NKT cell IL-4 production and is
hepatoprotective in T cell-mediated hepatitis in the mouse.” J. Immunol. 170: 5252-5259.
Andreas Cerny and Francis. V. Chisari. (1999). “Pathogenesis of Chronic Hepatitis C:
Immunological Features of Hepatic Injury and Viral ersistence.” Hepatology. 30, 595-601.
Atkuri, K.R., Herzenberg, L.A., and Herzenberg, L.A. (2005). “Culturing at atmospheric oxygen
levels impacts lymphocyte function.” Proc.Natl.Acad.Sci.U.S.A. 102, 3756–3759.
Atkuri, K.R., Herzenberg, L.A., Niemi, A.K., Cowan, T., and Herzenberg, L.A. (2007).
“Importance of culturing primary lymphocytes at physiological oxygen levels.”
Proc.Natl.Acad.Sci.U.S.A. 104, 4547–4552.
Benlagha, K., Weiss, A., Beavis, A., Teyton, L., and Bendelac, A. (2000). “In vivo identification
of glycolipid antigen specific T cells using fluorescent CD1d tetramers.” J Exp. Med. 191, 1895-
1903.
Brigl. M., Bry, L., Kent, S.C., Gumperz, J.E., and Brenner, M.B. (2003). “Mechanism of CD1d-
restricted natural killer T cell activation during microbial infection.” Nat. Immunol. 4, 1230–
1237.
Caldwell, C.C., Kojima, H., Lukashev, D., Armstrong, J., Farber, M., Apasov, S. G., and
Sitkovsky, M.V. (2001). “Differential effects of physiologically relevant hypoxic conditions on
T lymphocyte development and effector functions.” J. Immunol. 167, 6140– 6149.

68
Chan, E.S., Montesinos, M.C., Fernandez, P., Desai, A., Delano, D.L., Yee, H., Reiss, A.B.,
Pillinger, M.H., Chen, J.F., Schwarzschild, M.A., Friedman, S.L., and Cronstein, B.N. (2006).
“Adenosine A(2A) receptors play a role in the pathogenesis of hepatic cirrhosis.” Br. J.
Pharmacol. 148:1144-1155.
Choukèr, A., Thiel, M., Lukashev, D., Ward. J.M., Kaufmann, I., Apasov, S., Sitkovsky, M.V.,
and Ohta, A. (2008).“Critical role of hypoxia and A2A adenosine receptors in liver tissue-
protecting physiological anti-inflammatory pathway.” Mol Med. 14(3-4), 116-23.
Cronstein, B.N., Daguma, L., Nichols, D., Hutchison, A.J., and Williams, M. (1990). “The
adenosine/neutrophil paradox resolved: human neutrophils possess both A1 and A2 receptors
that promote chemotaxis and inhibit O2 generation, respectively.” J. Clin. Invest. 85, 1150-1157.
Decking, UK., Schlieper, G., Kroll, K., and Schrader, J. (1997). “Hypoxia-induced inhibition of
adenosine kinase potentiates cardiac adenosine release.” Circ Res. 81(2), 154-64
Driver, A.G., Kukoly, C.A., Ali, S., and Mustafa, S.J. (1993). “Adenosine in bronchoalveolar
lavage fluid in asthma.” Am. Rev. Respir. Dis. 148, 91-97.
Eckle, T., Grenz, A., Laucher, S., and Eltzschig, H.K. (2008). “A2B adenosine receptor
signaling attenuates acute lung injury by enhancing alveolar fluid clearance in mice.” J. Clin.
Invest. 118, 3301-3315.
Eltzschig, H.K., Abdulla, P., Hoffman, E., Hamilton, K.E., Daniels, D., Schönfeld, C., Löffler,
M., Reyes, G., Duszenko, M., Karhausen, J., Robinson, A., Westerman, K.A., Coe, I.R., and
Colgan, S.P (2005). “HIF-1-dependent repression of equilibrative nucleoside transporter (ENT)
in hypoxia.” J. Exp. Med. 202, 1493–1505.

69
Eltzschig, H.K., and Collard, C.D. (2004). “Vascular ischaemia and reperfusion injury.” Br.
Med. Bull. 70, 71–86.
Eltzschig, H.K., Thompson, L.F., Karhausen, J., Cotta, R.J., Ibla, J.C., Robson, S.C., and
Colgan, S.P. (2004). “Endogenous adenosine produced during hypoxia attenuates neutrophil
accumulation: coordination by extracellular nucleotide metabolism.” Blood 104, 3986-3992.
Exley, M. A., He, Q., Cheng, O., Wang, R., Cheney, C. P., Balk, S. P., and Koziel, M. J. (2002).
“Cutting Edge: Compartmentalization of Th1-Like Noninvariant CD1d-Reactive T Cells in
Hepatitis C Virus-Infected Live.” The Journal of Immunology. 168, 1519–1523.
Feoktistov, I., Biaggioni, I., and Cronstein, B.N. (2009). “Adenosine receptors in wound
healing, fibrosis and angiogenesis.” Handb. Exp. Pharmacol. 193, 383-397.
Frick, J.S., MacManus, C.F., Scully, M., Glover, L.E., Eltzschig, H.K., and Colgan, S.P.
(2009). “Contribution of adenosine A2B receptors to inflammatory parameters of experimental
colitis.” J. Immunol. 182, 4957-4964.
Geissmann, F., Cameron, T. O., Sidobre, S., Manlongat, N., Kronenberg, M., Briskin, M. J.,
Dustin, M. L., and Littman, D. R. (2005).” Intravascular Immune Surveillance by CXCR6+ NKT
Cells Patrolling Liver Sinusoids.” PLoS Biol 3(4), 0650-0661.
Goldsby, R.A., Kindt, T.J., and Osborne, B.A. “Kuby Immunology”, 6th
Edition.
Guo, J., Lu, W., Shimoda, L.A., Semenza, G. L., and Georas, S.N. (2009). “Enhanced interferon-
gamma gene expression in T cells and reduced ovalbumin dependent lung eosinophilia in
hypoxia inducible factor-1 alpha deficient mice.” Int. Arch.AllergyImmunol. 149, 98–102.

70
Harada, N., Okajima, K., Murakami, K., Usune, S., Sato, C., Ohshima, K., and Katsuragi, T.
(2000). “Adenosine and selective A(2A) receptor agonists reduce ischemia/reperfusion injury of
rat liver mainly by inhibiting leukocyte activation.” J. Pharmacol. Exp. Ther. 294, 1034-1042.
Haskó, G., Csóka, B., Németh, Z.H., Vizi, E.S., and Pacher, P. (2009). “A(2B) adenosine
receptors in immunity and inflammation.” Trends Immunol. 30, 263-270.
Herkel, J., Schuchmann, M., Tiegs, G., and Lohse, A.W. (2005).” Immune-mediated liver
injury.” J. Hepatol. 42, 920-923.
Hua, X., Kovarova, M., Chason, K.D., Nguyen, M., Koller, B.H., and Tilley, S.L. (2007).
“Enhanced mast cell activation in mice deficient in the A2b adenosine receptor.” J. Exp. Med.
204, 117-128.
Jacobson, A.K., and Gao, Z. (2006). “Adenosine receptors as therapeutic targets.” Nat. Rev.
Drug Discov. 5, 247-264.
Kakimi.K ., Guidotti, L. G., Koezuka, Y., and Chisari, F. V. (2000). “Natural Killer T Cell
Activation Inhibits Hepatitis B Virus Replication In Vivo.” J. Exp. Med. 192, 921–930.
Kaneko, Y., Harada, M., Kawano, T., Yamashita, M., Shibata, Y., Gejyo, F., Nakayama, T., and
Taniguchi, M. (2000). “Augmentation of Valpha14 NKT cell-mediated cytotoxicity by
interleukin 4 in an autocrine mechanism resulting in the development of concanavalin A-induced
hepatitis.” J. Exp. Med. 191, 105-114.
Karhausen, J., Haase, V. H., and Colgan, S.P. (2005). “Inflammatory hypoxia: role of hypoxia-
inducible factor.” Cell Cycle 4, 256-258.
Kawamura, T., Seki, S., Takeda, K., Narita, J., Ebe, Y., Naito, M., Hiraide, H., and Abo, T.
(1999). “Protective effect of NK1.1(+) T cells as well as NK cells against intraperitoneal tumors

71
in mice.” Cell Immunol. 193(2), 219-25.
Kim, H., Peng, G., Hicks, J.M., Weiss, H. L., VanMeir, E.G., Brenner, M. K., and Yotnda, P.
(2008). “Engineering human tumor specific cytotoxic T cells to function in a hypoxic
environment.” Mol.Ther. 16, 599–606.
Kinebuchi, M., Matsuura, A., Ohya, K., Abo, W., and Kitazawa, J. (2005). “Contribution of Vα
24+Vβ11+ natural killer T cells in Wilsonian hepatitis.” Clin Exp Immunol. 139, 144–151.
Kinjo, Y., Wu, D., Kim, G., Xing, G., Poles, M.A., Ho, D., Tsuji, M., Kawahara, K., Wong, C.,
and Kronenberg, M. (2005).“Recognition of bacterial glycosphingolipids by natural killer T
cells.” Nature. 434, 520-524.
Kita. H., Naidenko, O.V., Kronenberg, M., Ansari, A. A., Rogers, P., He, X., Koning, F.,
Mikayama, T.,Van de Water, J., Coppel, R. L., Kaplan, M., and Gershwin, M.E. (2002).
“Quantitation and phenotypic analysis of natural killer T cells in primary biliary cirrhosis using a
human CD1d tetramer.” Gastroenterology. 123(4), 1031-1043.
Kitamura, H., Iwakabe, K., Yahata, T., Nishimura, S., Ohta, A., Ohmi, Y., Sato, M., Takeda,
K., Okumura, K., Van Kaer, L., Kawano, T., Taniguchi, M., and Nishimura, T. (1999). “The
natural killer T (NKT) cell ligand alpha-galactosylceramide demonstrates its immunopotentiating
effect by inducing interleukin (IL)-12 production by dendritic cells and IL-12 receptor
expression on NKT cells.” J. Exp. Med. 189, 1121-1128.
Kolachala V.L., Vijay-Kumar, M., Dalmasso, G., Yang, D., Linden, J., Wang, L., Gewirtz, A.,
Ravid, K., Merli, D., and Sitaraman, S.V. (2008). “A2B adenosine receptor gene deletion
attenuates murine colitis.” Gastroenterology 135, 861-870.

72
Kronenberg, M., and Gapin, L. (2002). “The unconventional lifestyle of NKT cells.” Nat. Rev.
Immunol. 2, 557-568.
Lappas, C.M., Day, Y.J., Marshall, M.A., Engelhard, V.H., and Linden, J. (2006).
“Adenosine A2A receptor activation reduces hepatic ischemia reperfusion injury by inhibiting
CD1d-dependent NKT cell activation.” J. Exp. Med. 203, 2639-2648.
Larbi, A., Zelba, H., Goldeck, D., and Pawelec, G. (2010). “Induction of HIF-1alpha and the
glycolytic pathway alters apoptotic and differentiation profiles of activated human Tcells.” J.
Leukoc.Biol. 87, 265–273.
Li, Z., Soloski, M. J., and Mae Diehl, A. (2005). “Dietary factors alter hepatic innate immune
system in mice with nonalcoholic fatty liver disease.”Hepatology. 42(4), 880-885.
Linden J. (2001). “Molecular approach to adenosine receptors: receptor-mediated mechanisms of
tissue protection.” Annu.Rev. Pharmacol. Toxicol. 41, 775–87
Link, A.A., Kino, T., Worth, J.A., McGuire, J.L., Crane, M.L., Chrousos, G.P., Wilder, R.L., and
Elenkov, I.J. (2000). “Ligand-activation of the adenosine A2a receptors inhibits IL-12
production by human monocytes.” J. Immunol. 164, 436-442.
Linsen, L., Somers, V., and Stinissen, P. (2005). “Immunoregulation of Autoimmunity by
Natural Killer T Cells.” Human Immunol. 66, 1193–1202.
Loeffler, D.A., Juneau, P.L., and Masserant, S. (1992). “Influence of tumour physico-chemical
conditions on interleukin-2-stimulated lymphocyte proliferation.” Br.J.Cancer 66, 619–622.
Lucas. M., Gadola, S., Meier, U.,Young, N. T., Harcourt, G., Karadimitris, A., Coumi, N.,
Brown, D., Dusheiko, G., Cerundolo, V. and Klenerman, P. (2003).“Frequency and Phenotype of

73
Circulating V α24/V β11 Double-Positive Natural Killer T Cells during Hepatitis C Virus
Infection.” J Virol. 77(3), 2251-2257.
Lukashev, D.E., Smith, P.T., Caldwell, C.C., Ohta, A., Apasov, S.G., and Sitkovsky, M.V.
(2003). “Analysis of A2a receptor-deficient mice reveals no significant compensatory increases
in the expression of A2b, A1, and A3 adenosine receptors in lymphoid organs.” Biochem.
Pharmacol. 65, 2081-2090.
Lukashev, D., Klebanov, B., Kojima, H., Grinberg, A., Ohta, A., Berenfeld, L., Wenger, R.H.,
Ohta, A., and Sitkovsky, M. (2006). “Cutting edge: hypoxia-inducible factor 1alpha and its
activation-inducible short isoform I.1 negatively regulate functions of CD4+ and CD8+ T
lymphocytes.” J. Immunol. 177, 4962–4965.
Majmundar, A.J., Wong, W.J., and Simon, M.C. (2010). “Hypoxia inducible factors and the
response to hypoxic stress.” Mol.Cell 40, 294– 309.
Martin, C., Leone, M., Viviand, X., Ayem, M.L., and Guieu, R., (2000).” High adenosine plasma
concentration as a prognostic index for outcome in patients with septic shock.” Crit. Care Med.
28, 3198-3202.
Mattner, J., DeBord, K. L., Ismail, N., Goff, R. D., Cantu, C., Zhou, D., Saint-Mezard, P.,
Wang, V., Gao, Y., Yin, N., Hoebe, K., Schneewind, O., Walker, D., Beutler, B., Teyton, L.,
Savage, P. B., and Bendelac, A. (2005). “Exogenous and endogenous glycolipid antigens
ctivate NKT cells during microbial infections.” Nature. 434, 525-529.
Michiels, C. (2004). “Physiological and pathological responses to hypoxia.” Am. J. Pathol. 164,
1875-1882.

74
Minagawa, M., Deng, Q., Liu, Z., Tsukamoto, H., and Dennert, G. (2004). “Activated
natural killer T cells induce liver injury by Fas and tumor necrosis factor-α during alcohol
consumption.” Gastroenterology. 126(5), 1387-1399.
Morita. M., Motoki, K., Akimoto, K., Natori, T., Sakai, T., Sawa, E., Yamaji, K., Koezuka, Y.,
Kobayashi, E., and Fukushima, H. (1995). “Structure-activity relationship of alpha-
galactosylceramides against B16-bearing mice.” J.Med.Chem. 38 (12), 2176-87.
Mustafa, S.J., Nadeem, A., Fan, M., Zhong, H., Belardinelli, L., and Zeng, D. (2007). “Effect of
a specific and selective A(2B) adenosine receptor antagonist on adenosine agonist AMP and
allergen-induced airway responsiveness and cellular influx in a mouse model of asthma.” J.
Pharmacol. Exp. Ther. 320, 1246-1251.
Naldini, A., Carraro, F., Silvestri, S., and Bocci, V. (1997). “Hypoxia affects cytokine production
and proliferative responses by human peripheral mononuclear cells.” J. Cell.Physiol. 173, 335–
342.
Neumann, A.K., Yang, J., Biju, M.P., Joseph, S.K., Johnson, R.S., Haase, V.H., Freedman, B.D.,
and Turka, L. A. (2005). “Hypoxia inducible fac tor1alpha regulates T cell receptor signal
transduction.” Proc.Natl.Acad. Sci.U.S.A. 102, 17071–17076.
Niinikoski, J., Hunt, T.K., and Dunphy, J.E. (1972). “Oxygen supply in healing tissue.”
Am.J.Surg. 123, 247–252.
Nishikage, T., Seki, S., Toyabe, S., Abo, T., Kagata, Y., Iwai, T., and Hiraide, H. (1999).
“Inhibition of concanavalin A-induced hepatic injury of mice by bacterial lipopolysaccharide via

75
the induction of IL-6 and the subsequent reduction of IL-4: the cytokine milieu of concanavalin
A hepatitis.” J. Hepatol. 31, 18-26.
Novitskiy, S.V., Ryzhov, S., Zaynagetdinov, R., Goldstein, A.E., Huang, Y., Tikhomirov, O.Y.,
Blackburn, M.R., Biaggioni, I., Carbone, D.P., Feoktistov, I., and Dikov, M.M. (2008).
“Adenosine receptors in regulation of dendritic cell differentiation and function.” Blood 112,
1822-1831.
Nowak, M., Lynch, L., Yue, S., Ohta, A., Sitkovsky, M., Balk, S.P., and Exley, M.A. (2010).
“The A2aR adenosine receptor controls cytokine production in iNKT cells.” Eur. J. Immunol. 40,
682-687.
Nuti, S., Rosa, D., Valiante, N. M., Saletti, G., Caratozzolo, M., Dellabona, P., Barnaba, V., and
Abrignani, S. (1998). “Dynamics of intra-hepatic lymphocytes in chronic hepatitis C: enrichment
for Vα24+ T cells and rapid elimination of effector cells by apoptosis.” Eur. J. Immunol. 28,
3448–3455.
Odashima, M., Otaka, M., Jin, M., Komatsu, K., Wada, I., Matsuhashi, T., Horikawa, Y.,
Hatakeyama, Oyake, J., Ohba, R., Linden, J., and Watanabe, S. (2005). “Selective A2A
adenosine agonist ATL-146e attenuates acute lethal liver injury in mice.” J. Gastroenterol. 40,
526-529.
Ohta, A., and Sitkovsky, M. (2001). “Role of G-protein-coupled adenosine receptors in
downregulation of inflammation and protection from tissue damage.” Nature. 414, 916–920.
Ohta, A., Gorelik, E., Prasad, S.J., Ronchese, F., Lukashev, D.., Wong, M.K., Huang, X.,
Caldwell, S., Liu, K., Smith, P., Chen, J.F., Jackson, E.K., Apasov, S., Abrams, S., and

76
Sitkovsky, M. (2006). “A2A adenosine receptor protects tumors from antitumor T cells.” Proc.
Natl. Acad. Sci. U. S. A. 103, 13132-13137.
Ohta, A., Lukashev, D., Jackson, E. K., Fredholm, B. B., and Sitkovsky, M. (2007). “1,3,7-
trimethylxanthine (caffeine) may exacerbate acute inflammatory liver injury by weakening the
physiological immunosuppressive mechanism.” J. Immunol. 179, 7431-7438.
Ohta, A., Ohta, A., Madasu, M., Kini, R., Subramanian, M., Goel, N., and Sitkovsky, M. (2009).
“A2A adenosine receptor may allow expansion of T cells lacking effector functions in
extracellular adenosine-rich microenvironments.” J. Immunol. 183, 5487-5493.
Ohta. A., Diwanji, R., Kini, R., Subramanian, M., Ohta, A., and Sitkovsky, M. (2011). “Invivo
Tcell activation in lymphoid tissues is inhibited in the oxygen-poormicroenvironment.” Front.
Immun. 2, 1-10.
Okusa, M.D., Linden, J., Macdonald, T., and Huang, L. (1999). “Selective A2A adenosine
receptor activation reduces ischemia-reperfusion injury in rat kidney. “Am. J. Physiol. 277,
F404-412.
Osman, Y., Kawamura, T., Naito, T., Takeda, K., Van Kaer, L., Okumura, K., and Abo, T.
(2000). “Activation of hepatic NKT cells and subsequent liver injury following administration of
alpha-galactosylceramide.” Eur. J. Immunol. 30, 1919-1928.
Peters, C.L., Morris, C.J., Mapp, P. I., Blake, D.R., Lewis, C.E., and Winrow, V.R. (2004). “The
transcription factors hypoxia-inducible factor 1alpha and Ets-1 colocalize in the hypoxic
synovium of inflamed joints in adjuvant-induced arthritis.” Arthritis Rheum. 50, 291–296.

77
Roman, J., Rangasamy, T., Guo, J., Sugunan, S., Meednu, N., Packirisamy, G., Shimoda, L.A.,
Golding, A., Semenza, G., and Georas, S.N. (2010). “T-cell activation under hypoxic conditions
enhances IFN-gamma secretion.” Am.J.Respir.Cell Mol.Biol. 42, 123–128.
Rosenberger, P., Schwab, J.M., Mirakaj, V., Masekowsky, E., Mager, A., Morote-Garcia, J.C.,
Unertl, K., and Eltzschig, H.K. (2009). “Hypoxia-inducible factor-dependent induction of netrin-
1 dampens inflammation caused by hypoxia.” Nat. Immunol. 10, 195-202.
Ryzhov, S., Zaynagetdinov, R., Goldstein, A.E., Novitskiy, S.V., Blackburn, M.R., Biaggioni, I.,
and Feoktistov, I. (2008). “Effect of A2B adenosine receptor gene ablation on adenosine-
dependent regulation of proinflammatory cytokines.” J. Pharmacol. Exp. Ther. 324, 694-700.
Ryzhov, S., Zaynagetdinov, R., Goldstein, A.E., Novitskiy, S.V., Dikov, M.M., Blackburn,
M.R., Biaggioni, I., and Feoktistov, I. (2008).“Effect of A2B adenosine receptor gene ablation on
proinflammatory adenosine signaling in mast cells.” J. Immunol. 180, 7212-7220.
Santodomingo-Garzon, T., Han, J., Le, T., Yang,Y., and Swain, M. G. (2009). “Natural Killer T
Cells Regulate the Homing of Chemokine CXC Receptor 3-Positive Regulatory
Semenza, G.L. (2003). “Angiogenesis in ischemic and neoplastic disorders”. Annu. Rev. Med.
54, 17-28.
Serhan, C. N., Brain, S. D., Buckley, C. D., Gilroy, D. W., Haslett, C., O’Neill, L. A. J., Perretti,
M., Rossi, A.G., and Wallace, J. L. (2007). “Resolution of inflammation: state of the art,
definitions and terms.” Faseb J. 21, 325–332.
Sitkovsky, M.V. (2003). “Use of the A2A adenosine receptor as a physiological
immunosuppressor and to engineer inflammation in vivo.” Biochem. Pharmacol. 65, 493–501.

78
Sitkovsky, M.V., and Ohta, A. (2005). “The 'danger' sensors that STOP the immune response:
the A2 adenosine receptors?” Trends Immunol. 26, 299-304.
Sitkovsky, M.V., Lukashev, D., Apasov, S., Kojima, H., Koshiba, M., Caldwell, C., Ohta, A.,
and Thiel, M. (2004). “Physiological control of immune response and inflammatory tissue
damage by hypoxia-inducible factors and adenosine A2A receptors.” Annu. Rev. Immunol. 22,
657–682.
Sun, C.X., Zhong, H., Mohsenin, A., Morschl, E., Chunn, J.L., Molina, J.G., Belardinelli, L.,
Zeng, D., and Blackburn, M.R. (2006). “Role of A2B adenosine receptor signaling in adenosine-
dependent pulmonary inflammation and injury.” J. Clin. Invest. 116, 2173-2182.
Sun, R., Tian, Z., Kulkarni, S., and Gao, B. (2004). “IL-6 prevents T cell-mediated hepatitis via
inhibition of NKT cells in CD4+ T cell- and STAT3-dependent manners.” J. Immunol. 172,
5648-5655.
Swain, M.G (2008). “Hepatic NKT cells: friend or foe?” Clin. Sci. (Lond.) 114, 457-466.
Swain, M.G (2010). “Natural Killer T cells within the liver: Conductors of hepatic immune
orchestra.” Digestive Diseases. 28, 7-13.
Synnestvedt, K., Furuta, G., Comerford, KM., Louis, N., Karhausen, J., Eltzschig, H.K., Hansen,
K.R., Thompson, L.F., and Colgan, S.P. (2002). “Ecto-5′-nucleotidase (CD73) regulation by
hypoxia-inducible factor-1 mediates permeability changes in intestinal epithelia.” J Clin Invest.
110(7), 993–1002.
Tasken, K., and Anja Ruppelt (2006). “Negative regulation of T-cell receptor activation by the
cAMP-PKA-Csk signaling pathway in T-cell lipid rafts.” Frontiers in Bioscience. 11, 2929-2939

79
Terabe, M., and Berzofsky., J. A. (2008). “The role of NKT cells in tumor immunity.” Adv
Cancer Res. 101, 277-348.
Thiel, M., Caldwell, C.C., Kreth, S., Kuboki, S., Chen, P., Smith, P., Ohta, A., Lentsch, A.B.,
Lukashev, D., and Sitkovsky, M. V. (2007). “Targeted deletion of HIF-1alpha gene in Tcells
prevents their inhibition in hypoxic inflamed tissues and improves septic mice survival.”
PLoSONE 2, e853.
Thiel, M., Chouker, A., Ohta, A., Jackson, E., Caldwell, C., Smith, P., Lukashev, D., Bittmann,
I., and Sitkovsky, M.V. (2005). “Oxygenation inhibits the physiological tissue-protecting
mechanism and thereby exacerbates acute inflammatory lung injury.” PLoS Biol. 3:e174.
Tianqing, K., Westerman, K.A., Faigle, M., Eltzschig, H.K., and Colgan, S.P. (2006). “HIF-
dependent induction of adenosine A2B receptor in hypoxia.” FASEB J. 20,
Tiegs, G., Hentschel, J., and Wendel, A. (1992). “A T cell-dependent experimental liver injury in
mice inducible by concanavalin A.” J. Clin. Invest. 90, 196-203.
Toyabe, S., Seki, S., Iiai, T., Takeda, K., Shirai, K., Watanabe, H., Hiraide, H., Uchiyama, M.,
and Abo, T. (1997). “Requirement of IL-4 and liver NK1+ T cells for concanavalin A-induced
hepatic injury in mice.” J. Immunol. 159, 1537-1542.
Wang, Q., Liu, C., Zhu, F., Liu, F., Zhang, P., Guo, C., Wang, X., Li, H., Ma, C., Sun, W.,
Zhang, Y., Chen, W., and Zhang, L. (2010). “Reoxygenation of hypoxia-differentiated dentritic
cells induces Th1 and Th17 cell differentiation.” Mol.Immunol. 47, 922–931.

80
Wingender, G., Rogers, P., Batzer, G., Lee, M. S., Bai, D., Pei, B., Khurana, A., Kronenberg, M.
and Horner, A. A. (2011). “Invariant NKT cells are required for airway inflammation induced by
environmental antigens.” J. Exp. Med. 208, 1151-1162.
Wondimu, Z., Santodomingo-Garzon, T., Le, T. and Swain, M. G. (2010). “Protective Role of
Interleukin-17 in Murine NKT Cell-Driven Acute Experimental Hepatitis.” Am J Pathol. 177(5),
2334-2346.
Yang, D., Zhang, Y., Nguyen, H.G., Koupenova, M., Chauhan, A.K., Makitalo, M., Jones, M.R.,
St Hilaire, C., Seldin, D.C., Toselli, P., Lamperti, E., Schreiber, B.M., Gavras, H., Wagner,
D.D., and Ravid, K. (2006). “The A2B adenosine receptor protects against inflammation and
excessive vascular adhesion.” J. Clin. Invest. 116, 1913-1923.
Yang, M., Ma, C., Liu, S., Sun, J., Shao, Q., Gao, W., Zhang, Y., Li, Z., Xie, Q., Dong, Z., and
Qu, X. (2009). “Hypoxia skews dendritic cells to a T helper type 2-stimulating phenotype and
promotes tumour cell migration by dendritic cell-derived osteopontin.” Immunology. 128, e237–
e249.
Zhou, Y., Mohsenin, A., Morschl, E., Young, H.W., Molina, J.G., Ma, W., Sun, C.X., Martinez-
Valdez, H., and Blackburn, M.R. (2009). “Enhanced airway inflammation and remodeling in
adenosine deaminase-deficient mice lacking the A2B adenosine receptor.” J. Immunol. 182,
8037-8046.
Zuckerberg, A.L., Goldberg, L. I., and Lederman, H.M. (1994). “Effects of hypoxia on
interleukin-2 mRNA expression by T lymphocytes.” Crit. Care Med. 22, 197–203.