Embed Size (px)
DESCRIPTION
Our mission is to enhance your ability to practice equine medicine by providing the latest info you need.
Citation preview

Vol 6 Issue 6 2016www.modernequinevet.com
EnterolithsHow good is your arthrocentesis technique?Genetic susceptibility to sarcoids?
Equine VetThe Modern
TreatingGastroplenic
Entrapment

2 Issue 6/2016 | ModernEquineVet.com
Table of ConTenTs
LaMenessHow accurate is your arthrocentesis technique? ..........................................................8
TecHnIcIan UpdaTeexploratory laparotomy and enterotomy for enterolith removal .............................................................................11
oncoLogy do horses have genetic susceptibility to sarcoids? ................16
newsModern horses run differently than ancient ancestors ......3oh, those aging tendons ...............................................................10The Irish take liver fluke survey .................................................15auburn gets new standing cT .......................................................18oral glucose tests repeatable in ponies .................................19
LEGAL DISCLAIMER: The content in this digital issue is for general informational purposes only. PercyBo Publishing Media LLC makes no representations or warranties of any kind about the completeness, accuracy, timeliness, reliability or suitability of any of the information, including content or advertisements, contained in any of its digital content and expressly disclaims liability of any errors or omissions that may be presented within its content. PercyBo Publishing Media LLC reserves the right to alter or correct any content without any obligations. Furthermore, PercyBo disclaims any and all liability for any direct, indirect, or other damages arising from the use or misuse of the information presented in its digital content. The views expressed in its digital content are those of sources and authors and do not necessarily reflect the opinion or policy of PercyBo. The content is for veterinary professionals. ALL RIGHTS RESERVED. Reproduction in whole or in part without permission is prohibited.
a tale of two entrapments treating gLe and eFe
coLIc:
4
Cover photo: Shutterstock/anjajuli
SalES: Matthew Todd • [email protected]
Editor: Marie Rosenthal • [email protected]
art dirEctor: Jennifer Barlow • [email protected]
contributinG writErS: paul Basillo • Kathleen ogle
coPY Editor: patty wall
Published by
p E r c y b omedia publishing
Equine VetThe Modern
advErtiSErSshanks Veterinary equipment ................................. 3Merck animal Health ................................................. 5
standlee premium western Forage ........................ 7aaeVT ...........................................................................15
PO Box 935 • Morrisville, PA 19067Marie Rosenthal and Jennifer Barlow, Publishers

ModernEquineVet.com | Issue 6/2016 3
news
Shut
terst
ock/
Olga
_i
mammals can switch between stiff-backed and flex-backed running as they increase in speed. This could be one potential model for the evolution of special-ized stiff-backed running in horses. This study reveals a new insight into a famous case-study of locomotor ad-aptation. “The findings are sig-nificant because they show how the backbone—a relatively under-studied part of the anatomy—can provide new perspectives on locomotor transitions,” Dr. Jones said. MeV
Modern horses reach top speeds using a special run-ning gait in which they hold their back stiff as they move. researchers found that tiny fossil ancestors of modern horses may have moved quite differently than their living counterparts.
Dating back more than 50 million years, the old-est horse ancestors were no bigger than a house cat. The researchers suggest that the stiff-backed gait of modern horses likely evolved to save energy while running as horses evolved into larger animals.
“For over a century, researchers studied the feet of fossil horses to explain how they evolved features specialized for running,” explained Katrina Jones, phD, a post-doctoral researcher in Harvard's Mu-seum of comparative Zoology, "but little is known about how the backbone might be involved in this famous transition.” Four-legged mammals tend to move their lower back during running to help in-crease speed and regulate breathing. but horses are unusual because they restrict the motion of their lumbar spine to a single joint near their rump.
To understand the evolution of the back in fossil hors-es, Dr. Jones first examined the anatomy and mobility of the spine in modern horses. The shape of the vertebral joints help determine how much motion occurs at each joint. Armed with this information, Dr. Jones then mea-sured the shape of vertebral joints in 16 species of fossil horses spanning their full size and age range.
She found that small fossil horses, such as Hyra-cotherium (the 'dawn horse'), had quite different anatomy of the vertebral joints than their modern equivalents. This anatomy suggests more mobility was possible in the middle and lower portions of their back. Anatomy of these joints was also linked to body size; evolutionary branches which evolved greater size tended to display more restrictive joints. Dr. Jones hypothesizes that stability of the backbone evolved as a response to the mechanical challenge of large size in horses. “The energy required for a large animal to move at high speed can be extreme, so in-creasing running efficiency by minimizing motions of the trunk makes sense,” she said, speculating that certain ancient horses may not have been run-ning in the same way as modern horses. Some living
Modern Horses run differently than ancient ancestors
For more information:
Jones KE. New insights on equid locomotor evolution from the lumbar region of fossil. Proceedings of the Royal Society B: Biological Sciences. 2016; 283 (1829): 20152947 DOI: rspb.2015.2947 10.1098/ www.shanksvet.com • [email protected]
Lifting Large Animals Since 1957

4 Issue 6/2016 | ModernEquineVet.com
B y p a u l B a s i l i o
Gastrosplenic entrapment (GLE) and epiploic foramen entrap-ment (EFE) are fairly small slices of the overall colic pie. As such, the literature to determine whether cer-tain diagnostic findings can help dif-ferentiate between the two is light, as is whether the complications and short-term survival associated with each type are similar.
This was the impetus for Isa-belle Kilcoyne, MVb, DAcVS, of the William r. pritchard Veteri-nary Medical Teaching Hospital
at University of california, Davis, and her colleagues to investigate whether GLE would have similar clinical presentation and diagnos-tic results as EFE, and whether GLE would be associated with a better short-term survival.
The populationThe retrospective study began with horses that had a definitive diagnosis of GLE or EFE based on intraoperative findings of necrop-sy at the teaching hospital during
the past 20 years. “We also looked through the
records and pulled the cases that presented for colic during that time and reviewed the signalment for those horses,” Dr. Kilcoyne said here at the 61st Annual AAEp con-vention in Las Vegas. “We found 9,755 horses that were examined because of colic during that period. There were 43 horses with GLE and 73 with EFE in that group.”
presentationTennessee Walking Horses and horses aged 8-12 years were over-represented in the GLE group, and Thoroughbreds, warmbloods, Morgan horses and horses aged 13-20 years were overrepresented in the EFE group. These findings were significantly different than the overall colic population.
“contrary to a lot of other studies, we did not find an asso-ciation between cribbing and GLE
ColiC
A tale of
The gastrosplenic ligament is a thin, broad mesenteric band that extends from the greater curvature of the stomach to the cranial edge of the spleen. The exact role of the ligament isn’t exactly known, but it is thought to provide some structural support for the abdominal viscera. It most commonly involves the small intestine, but rare cases have shown the large intestine entrapped within the ligament.
The epiploic foramen is an opening in the omental bursa that
measures 4-6 cm and separates the omental bursa from the rest of the abdominal cavity. The borders of the epiploic foramen include the caudate process of the liver and the portal vein. Recently, the literature has described a more significant role attributed the gastropancreatic fold that forms the dorsal and caudoventral borders of the foramen. Entrapment typically occurs from left to right.
anatomy lesson
entrapmentstwosh
utte
rstoc
k/an
jajuli
SafetyIn Numbers
Some dewormers claim just one dose of their product is the best way to deworm your horse, but that’s simply not true.
Demand Safety: You won’t find a laundry list of warnings and precautions on the PANACUR® (fenbendazole) POWERPAC label because fenbendazole has a unique mode of action that makes it safe for horses of all ages, sizes, and body conditions.
Demand Efficacy: PANACUR® POWERPAC is the only dewormer FDA approved to treat ALL STAGES of the encysted small strongyle.1
Other dewormers miss a critical stage, EL3, which can account for up to 75% of the encysted small strongyle burden. Plus, it’s the best choice for treating ascarids — which are not just a problem in young horses!
So when it comes to which dewormer to trust, don’t forget there’s safety in numbers.
Consult your veterinarian for assistance in the diagnosis, treatment, and control of parasitism.
Do not use in horses intended for human consumption. When using PANACUR® (fenbendazole) Paste 10% concomitantly with trichlorfon, refer to the manufacturers labels for use and cautions for trichlorfon.
1 PANACUR® (fenbendazole) POWERPAC Equine Dewormer product label.
The Science of Healthier Animals
2 Giralda Farms • Madison, NJ 07940 • merck-animal-health-usa.com • 800-521-5767Copyright © 2016 Intervet Inc., d/b/a/ Merck Animal Health, a subsidiary of Merck & Co., Inc.All rights reserved. 3290 EQ-PC-FP AD

6 Issue 6/2016 | ModernEquineVet.com
or EFE,” she said. “This was likely due to the retrospective nature of the study.”
Dr. Kilcoyne’s study did show that horses in the EFE group were significantly more likely to have had a history of prior colic surgery than horses in the GLE group.
“Horses with EFE had a signifi-cantly higher heart rate than those in the GLE group,” she noted. “That could potentially be caused by pain, but we can’t draw that conclusion because pain was not scored in our study.”
In addition, systemic lactate and peritoneal lactate were both significantly higher in the EFE group, which may indicate that these horses were more systemi-
ColiC
cally compromised. The proximity of the epiploic foramen to the liver and the pancreas could potentially have secondary effects on those organs and may impact the clini-cal presentation.
“It was interesting to note that only a small amount in both groups presented with nasogastric reflux,” Dr. Kilcoyne said. “Likewise, small intestinal involvement was only de-tected in 60% of the cases on rectal examination. Ultrasound, however, showed 92% of the GLE horses and 90% of the EFE horses had evidence of small intestinal distention. The value and sensitivity of this diag-nostic modality should lead equine practitioners to perform it in all of their colic cases.”
Treatmentof the 43 horses that presented with GLE, 32 were taken to sur-gery and 11 were euthanized. Seven of the 32 horses who were taken to surgery were euthanized on the table due to the need for re-section and anastomosis that was declined by the owner.
In the EFE group, 58 of the 73 horses were taken to surgery, and 24 were euthanized on the table. Seven of the horses eutha-nized during surgery had severe intraabdominal hemorrhage from the portal vein, caudal vena cava
or ruptured mesenteric vessels.“This emphasizes the impor-
tance of care when reducing these entrapments because of all of those anatomical structures that make up the boundaries of the fo-ramen,” Dr. Kilcoyne explained.
complicationsThere were no significant differ-ences in the complication rates (56% for GLE and 62% for EFE) between the groups postoperative-ly, which included minor or major complications.
“We had a few horses with inci-sional complications,” Dr. Kilcoyne said. “one horse had a jugular vein thrombophlebitis, three horses had postoperative hemoabdomen, and one horse developed septic peri-tonitis. The most frequent compli-cation was postoperative ileus. Six horses in each group had severe colic requiring relaparotomy.”
overall survival to discharge was 88% in the GLE group and 85% in the EFE group. Factors associated with the pooled survival included peritoneal total protein and peri-toneal lactate concentrations. post-operative ileus was a significant complication that contributed to non-survival. only 67% of horses with postoperative ileus survived compared with 100% of those with-out the complication. MeV
sign up Today * we promise not to bombard you with emails. Just a notice when new information is available. send us your email address
take-home PointsHorses with EFE were more likely to be tachycardic and have hyperlactatemia vs those with GLE.
EFE and GLE have a similar favorable short-term survival of surgery.
Middle-aged geldings seem to be predisposed to both types of colics.
Prior colic surgery may increase the risk of EFE.
The findings of the study emphasize the increased sensitivity of ultrasound for the detection of small intestinal lesions compared with the presence of nasogastric reflux or rectal findings.

Proud sponsor of:
CA_Modern_Equine.indd 1 6/2/2016 12:56:22 PM

8 Issue 6/2016 | ModernEquineVet.com
The variable clinical signs and degrees of lameness associated with the distal hock joints can be challenging to diagnose. radio-graphic guidance to confirm nee-dle placement helps, according to a recent study.
When the focus turns to local-ization to determine whether the hock is indeed the cause of lame-ness, there are several options, ac-cording to Kathryn A. Seabaugh, DVM, DAcVS (Large Animal), DAcVSMr, of the University of Georgia.
“radiography has been found to have poor correlation with disease unless there are severe osteoarthritic changes,” she said here at the 61st Annual AAEp convention in Las Vegas. “Advanced imaging has given us a wealth of knowledge, but unfor-tunately we have to localize to the region before we can pursue imaging of the area.”
Intra-articular administration of anesthesia is still the gold stan-dard for these types of patients, but the success of the procedure depends on the accuracy of the in-jection, she said.
B y p a u l B a s i l i o
arthrocentesis
laMeness
How accurate is your
technique?
Shut
terst
ock/
Abra
mov
a Kse
niya

ModernEquineVet.com | Issue 6/2016 9
arthrocentesis Dr. Seabaugh and her colleagues set out to determine the accuracy of arthrocentesis of the distal in-tertarsal (DIT) and tarsometatarsal (TMT) joints across a small group of equine veterinarians. Six vet-erinarians were recruited to inject eight joints—four DIT and four TMT. Four of the veterinarians were equine surgeons, and two were sur-gery residents. The study partici-pants were asked to use an injection technique described in Adams and Stashak’s Lameness of Horses.
“We hypothesized that the injec-tion accuracy for the TMT would be 100%, but that the accuracy for the DIT would be less,” she explained.
After the injections were com-pleted in both joints, the needles were left in place, and dorso-plantar and lateral medial views were taken. All radiographs were viewed by a board-certified radi-ologist who recorded the commu-nication of the contrast medium and the location of the injection site. The veterinarians were then interviewed to discuss their confi-dence level with the injections.
The good newsThe researchers were pleased with the accuracy of the TMT joint in-jections. Successful injections were noted in 23 of 24 joints (96%).
“The injection success matched our confidence,” Dr. Seabaugh said. “All of the successful injec-tions were in joints where the vet-erinarians said they felt confident. For the one missed injection, the veterinarian said that he was not confident in his injection.”
communication between the TMT and DIT was present in only six of 23 successful joints (26%), and the average number of re-
Here is an example of a missed distal inter tarsal injection. the star shows where they were aiming, and the line represents the misplaced needle.
Imag
es co
urte
sy of
Dr.
Kath
ryn A
. Sea
baug
h
sticks was less than one with a range of none to three.
“This indicates that the ma-jority of veterinarians placed the needle once and that was it,” she explained. “Some re-sticks were due to horses moving.”
The not-so-good newsThey were significantly less suc-cessful with the DIT. The veteri-narians were accurate in 10 of 24 joints (42%).
“The confidence and injection accuracy were also significantly less than that of the TMT joint,” Dr. Seabaugh said. “only 11 of 24 joints were confidently injected, and only six of these 11 confident injections were actually successful.”
Most of the missed DIT joints were missed proximally or even a little plantarly. The average number of re-sticks was again fewer than one, and most of these were neces-sary because the horse moved. The average number of repositions was about six, which was significantly greater than the TMT joint.
Extra-articular contrast media was noted in seven of 10 success-ful joint injections, and multiple attempts to inject had been made in three of those joints.
what It MeansThe most important take-away from this study is the accuracy, Dr. Sea-baugh said. The TMT has consistent landmarks, which leads to a high level of accuracy. The DIT joint has inconsistent landmarks, which can drag the accuracy down.
“In our survey of the operators after completion of the study, we found that many of them had de-veloped their own techniques over the years, and many of them did
not stick to the description of the injection in Adams and Stashak’s,” she noted. “one operator described using the width of his thumb cau-dal to the saphenous, and then just dorsal to the cunean tendon, and then he walked the needle in from there. That type of technique makes it hard to repeat across operators.”
Another consideration that should be made is to whether the repositioning or re-sticking of the needle could be causing joint capsule fenestration that leads to extravasion of the contrast medium. If there is extravasion or backflow of anesthetic in the TMT joint, then there is the potential for anesthetization of the lateral plantar nerve, which can con-founding the blocking pattern. MeV

10 Issue 6/2016 | ModernEquineVet.com
laMeness
Thorpe CT, Peffers MJ, Simpson D, et al. Anatomical heterogeneity of tendon: Fascicular and interfascicular tendon compartments have distinct proteomic composition. Scientific Reports. 2016;6:20455 DOI: 10.1038/srep20455. http://www.nature.com/articles/srep20455
For more information:
oh, Those aging Tendons Scientists at Queen Mary Uni-versity of London (QMUL) are one step closer to preventing the kind of injuries that affect aging race horses like champion hurdler rock on ruby, the winner of cor-al Hurdle at Ascot in 2015.
The team at QMUL's School of Engineering and Materials Science showed how the types of proteins differ in parts of the ten-don, and importantly how this changes as the tendon ages.
“When a horse runs, its mus-cles generate a massive amount of energy that is stored and released by the tendons in its legs. These can be likened to massive elastic bands that absorb energy as they are stretched, and release it again when they recoil,” said Dr. Chavaunne Thorpe, post doctoral research assistant at QMUL.
“The key to the effectiveness of tendons is the ability of the fibers that they are made up of to slide across each other. When this ability to slide is re-
duced, the energy damages the tendon instead of being stored and released by it.
“In this new study, we have identified specific proteins that help the tendon fibers to slide, and this research shows that these proteins are replaced less quickly as aging occurs. This makes inju-ries of the type that ended rock on ruby's career more likely.”
rock on ruby, the 2012 chel-tenham champion Hurdle win-ner, famously went on to win the coral Hurdle at Ascot last year despite suffering a career-ending tendon injury during the race, which resulted in the untimely re-tirement of the champion hurdler.
All tendons are made of sub-units containing rope-like collagen surrounded by a material called the interfascicular matrix (IFM), which binds them together. The IFM is a soft, extend-ible material that allows the subunits to slide past one another, enabling the whole tendon to stretch.
The researchers identified which proteins are present and how rapidly many of the proteins in the IFM are refreshed in young tendons.
As tendons become older, the IFM becomes stiffer making it harder for the subunits to slide past each other. The results of this study indicate that the rate of proteins renewal drops with aging in the IFM spe-cifically.
“our research proves that the increase in tendon injuries as horses age may be directly related to the slowdown in the renewal of specific proteins within their tendon tissues,” said co-author Hazel Screen, phD, a professor at QMUL.
Tendon injury is common in horses as well as hu-mans, with an economic impact of more than $4.104 a year in horse racing. Around 16,000 horses are in training each year, and the tendon injury rate is as high as 43% with few horses returning to racing after injury. MeV
The ifM is a soft, extendible
material that allows the subunits
to slide past one another, enabling the whole tendon
to stretch.
CliCk here To see The Video

ModernEquineVet.com | Issue 6/2016 11
Imag
es co
urte
sy of
Ms.
Larse
n
Surgery to remove the enterolith
TeChniCian updaTe
By Brandi Larsen, CVT
A 12-year-old Friesian gelding that was experi-encing intermittent, yet chronic abdominal dis-comfort and a decreased appetite over the past
month presented to the clinic. His long black mane and tail were full of shine and his coat was smooth and rich, not the typical presentation of a patient experiencing colic symptoms.
The clinician asked about his vaccination and deworming history, diet, daily routine and if there had been any environmental changes that may have triggered his symptoms. The owners stated that with IV flunixin meglumine given, his symptoms would improve for several days. With the episodes of dis-comfort becoming more frequent, the patient’s re-
exploratory laparotomy and enterotomy for the removal of an enterolith
ferring veterinarian recommended a second opin-ion to find the source of his mystery pain.
He was bright, alert and curious as to why he was at the practice, yet felt well enough to be on the un-successful hunt for a stray treat or two. His exami-nation gave no hints as to the primary cause of his symptoms. His rectal temperature, heart rate and respiratory rate were 99.6° F, 36 beats per minute (bpm) and 16 breaths per minute, respectively. His heart was auscultated and found to have a normal sinus rhythm without evidence of murmurs or ar-rhythmias. Auscultation of his lungs was also within normal limits with no crackles or rales appreciated.
Following abdominal auscultation, it was deter-mined that borborygmi was decreased in all four quadrants of the abdomen bilaterally, giving the clinician his first clue in the case. His mucous mem-branes were pink and moist. The patient’s capillary refill time was less than 2 seconds proving also to be

12 Issue 4/2016 | ModernEquineVet.com
TeChniCian updaTe
within normal limits. No heat, swelling or edema was palpated in the distal limbs and the pa-tient’s digital pulses were nor-mal. The results obtained from the primary physical examina-tion did not give the clinician enough information for a diag-nosis.
The patient appeared calm and relaxed. Transrectal pal-pation revealed small, firm fe-cal balls with a mild amount of mucous and digested blood ob-served, and he had a body con-dition score of 5 out of 9. No ec-toparasites, wounds, abrasions or significant lameness were appre-ciated. No evidence of neurologic disease, weakness, or ataxia was observed, and the patient was not actively displaying signs of ab-dominal discomfort at this time.
A veterinary technician obtained a venous blood sample to test for chagas disease, a complete blood count (cbc), chemistry 12 panel, fibrino-gen, packed cell volume (pcV) and total protein analysis. While waiting for the lab results, the pa-tient again was convinced that he has been such a great patient that he deserved a treat. Unfortunately, without answers, he would have to settle for a neck scratch and kisses from his owners.
still everything within normal limitsHis cbc was unremarkable and revealed a nor-mal pcV of 32% and total protein result of 7.4 mg/dL. His white blood cell (Wbc) count was 6.0 K/uL (neutrophils accounting for 69.7%) and the red blood cell (rbc) count was 6.48 M/uL. His chemis-try profile was also within normal limits. The clini-cian obtained a fecal sample to submit for an egg count and a free catch urine sample for a complete urinalysis, culture and sensitivity. The fecal egg count result showed the patient as a low shedder at 50 eggs/g of feces and the urinalysis had no abnor-mal findings with a specific gravity of 1.036 and no growth was observed following the urine culture and sensitivity analysis. The chagas disease serum test results were also negative.
After discussing the findings of all preliminary diagnostics with the owners, it was decided to per-form a gastroscopy to examine the esophagus and stomach. The patient’s stomach was completely
empty allowing visualization. The gastroscopy revealed no evidence of past or active equine gastric ulcer syndrome and the Margo plicatus was observed to be within normal limits with no signs of squamous ulceration, inflammation or masses. The py-lorus and cardia were also with-in normal limits with no signs of glandular ulceration. While removing the gastroscope, the esophagus was mildly distended with air and minimal bile was observed in the distal one-third of the esophagus. The clinician administered a prophylactic dose of omeprazole orally.
The clinician moved on to a more in-depth examination by performing a thoracic and ab-dominal ultrasound. His thorax
was unremarkable with no comet tails, consolida-tion, or abscessation appreciated while his abdomen revealed normal renal, splenic and liver architec-ture, with a normally sized stomach. The left colon was observed to be gas distended while the right co-lon was found to be mildly edematous. The patient’s small intestine in the ventral flank area was mildly thickened at 5.9 mm and no peritoneal fluid, masses or abscesses were noted along the visible wall. He was hospitalized under constant observation for even the slightest change in mentation or physical status.
To keep the patient hydrated and stable, he was given maintenance IV fluid via a jugular IV cath-eter. The clinician started the patient on IV crystal-loid fluids (Lactated ringer’s Solution) with calcium gluconate 23%, vitamin b complex, vitamin c and potassium chloride. He was also offered 2 lbs of purina Equine Senior Feed as a mash and started on IV antibiotics every 24 hours. When he was all settled in, the waiting game began.
At approximately 11:48 pm, the overnight vet-erinary staff noticed that the patient became alert, responsive and appeared nervous, which they had not observed before. He began to walk in a circle around his stall and positioned himself comfortably in sternal recumbency for about 30 minutes with no attempt to roll, thrash or even appear to be in distress. The staff continued to monitor him for any change and evaluated his heart rate once he stood up. His heart rate was determined to be within rela-
The 12-year-old friesian was
bright, alert and curious with a long black, shiny mane and tail. his coat was smooth and
rich—not a usual colic.

ModernEquineVet.com | Issue 6/2016 13
tively normal limits at 48 bpm. His IV catheter was flushed with heparinized saline and determined to be patent while IV fluids were continued. Since hospitalization, defecation had not been observed, however, he was displaying a moderate amount of flatulence but still no solid indications of abdominal discomfort.
The primary clinician returned in the morning following the uneventful evening hoping for news. He performed a physical examination, which to no surprise was deemed to be unremarkable with the exception of increased borborygmi in all four quad-rants of the abdomen following auscultation. The cli-nician elected to obtain a blood sample for a subse-quent cbc analysis. Frustratingly enough, the results were unremarkable aside from mild polycythemia possibly indicating GI disease of unknown origin.
The patient again began showing visible signs of abdominal discomfort around 7:00 am severe enough to warrant mild IV sedation. The staff sprang into action by performing an abdominal ultrasound during the episode in hopes of finding another piece of the puzzle, however the ultrasound revealed no new information. Fluid ingesta was ap-preciated in the colon with hypermotile small intes-tine. Transrectal palpation was then performed, and a small amount of soft feces was appreciated in the rectum. Mild gas and ingesta in the right colon led the clinician to believe the patient may be displacing his right colon. He was placed back on observation where he passed a small amount of soft feces and diarrhea.
some discomfortAfterward, the patient stood comfortably and qui-etly through most of the morning. A repeat ab-dominal ultrasound was performed again around 9:30 am and resulted in the finding of small, yet consistent colonic vessels indicative of a previous right dorsal colon displacement, finally. The patient was observed throughout the day with no signs of discomfort. He passed additional small amounts of diarrhea throughout the day but appeared relatively comfortable with all subsequent physical examina-tions within normal limits. IV fluids were continued with no change in rate without incident.
The following morning, day three of observation, at about 7:00 am, the patient was again, significantly uncomfortable and was displaying behavior associ-ated with a moderate colic episode. He was pacing, restlessly lying down and standing up, as well as pawing and kicking at his abdomen. This was the most severe episode thus far, hopefully providing
some insight to further clues. A nasogastric tube was passed through the left nares and into the stom-ach, yet no gastric reflux was appreciated. His heart rate was within normal limits at deparate 44 bpm, which did not traditionally match up with the de-gree of discomfort observed.
All findings, results and observations up until this point were discussed with the owners who opt-ed to continue monitoring the patient until he either continually improves or severely declines. Through-out day three, he displayed continued anorexia and his mentation became moderately dull, which was a new development. A physical examination was per-formed at 8:00 pm and the patient was found to be mildly febrile with a rectal temperature of 101° F. This was the first major physical change other than the discomfort.
New bloodwork showed a possible infection. With the previous examination findings possibly indicat-ing GI disease, these new results were slowly piecing together the diagnostic puzzle. The clinician admin-istered a dose of flunixin meglumine IV and every 12 hours thereafter, to combat the patient’s pyrexia. While still a mystery, he was subsequently febrile again at approximately 8:00 pm with rectal tempera-ture of 101.3° F but with an unremarkable heart rate of 42 bpm and respiratory rate of 12 breaths per min.
Febrileby the following day, the patient was still mildly fe-brile during his 7:00 am physical examination with a rectal temperature of 101.2° F but again, the remain-der of his examination was frustratingly unremark-able. The patient was referred to a facility with a ra-diologist and advanced ultrasonography equipment.
The radiology report stated that a large mass was appreciated in his GI tract that was indicative of a large enterolith symptomatically fitting the patient. After careful discussion with both the owners and surgical staff, it was elected to attempt to combat the infectious disease process with antibiotics and IV fluid therapy until the patient was normothermic and stable enough to attempt to reduce anesthetic risk and patient morbidity associated with an up-coming and imminent exploratory laparotomy.
over the next three days, tensions remained high knowing what the future would hold for this pa-tient. IV fluids were continued with additives as well as the addition of IV cefazolin every 8 hours and IV polymyxin b every 12 hours. He was started on oral probiotic paste, as well as continued omeprazole paste every 24 hours to increase his appetite and calm his abdominal discomfort until he was deemed

14 Issue 6/2016 | ModernEquineVet.com
stable enough for an exploratory laparotomy. prolonging the start of surgery was a difficult deci-sion to make, but the risks ver-sus benefits had to be weighed
weighing the benefits vs. risksThe risks of waiting included un-foreseen increase or decrease of his disease process systemically, further decline of the patient, GI rupture at an unknown location and endotoxemia. The benefits of waiting for surgical correction included less morbidity risk dur-ing general anesthesia and over-all systemic patient stabilization for a general anesthesia with less risk and postoperative recovery.
His owners visited him fre-quently and the bond between them was evident. Unfortunately, his temperature continued to rise to 103.5° F the following day after the decision to withhold an attempt at surgical cor-rection until the pyrexia had dissipated with no as-sociated signs of discomfort. IV fluid, antibiotic and GI therapies were continued and luckily, he became normothermic the following morning.
TeChniCian updaTe
prolonging the horse's surgery was a difficult
decision to make, but the risk
versus benefits had to be weighed.
It is rare to see an explorato-ry laparotomy on the practice schedule instead of by emer-gency, however, the patient was scheduled for an exploratory lap-arotomy to remove the suspected enterolith from the GI tract.
The patient was prepared for surgery by being brushed of all debris, feet cleaned and his mouth was rinsed to avoid aspiration of debris. Due to his breed and size, a real concern was the increased risk of postoperative muscle my-opathy or nerve paresis.
He was given a preanesthetic sedation combination of butor-phanol and xylazine followed by a small bolus of guaifenesin IV. The patient was induced for general anesthesia with a combination of
ketamine and midazolam IV without incident and was intubated with a size 26-mm endotracheal tube in sternal recumbency to avoid the risk of reflux. He was positioned on the operating table in dorsal recum-bency on 14-inch thickness operating table padding. Due to his already compromised state and his size, he became hypotensive with a mean arterial blood pressure (MAp) of 65 mm Hg immediately follow-ing induction at which time a dobutamine constant rate infusion (crI) was administered IV to combat his hypotension, promote organ, tissue and muscle perfusion, as well as battle postoperative muscle my-opathy. He responded well to the crI, and his MAp increased to normal limits of between 80 and 90 mm Hg throughout the remainder of the procedure. The enterolith was removed successfully and was equiva-lent to the size of a cantaloupe which would cause ob-vious discomfort to any patient.
The patient’s general anesthesia was relatively uncomplicated and, uneventful, and the patient was moved into recovery and positioned in left lateral re-cumbency. No abnormalities were appreciated on any of the arterial blood gas results obtained throughout the exploratory laparotomy proving his metabolic and respiratory status was maintained within normal limits.
While being carefully monitored in recovery, he immediately began spontaneous respirations with no increase respiratory effort. once the patient de-veloped horizontal nystagmus, he was sedated with IV romifidine to allow him sufficient time to recover from the sevoflurane gas inhalant anesthesia. He re-
necropsy resultsAlthough the clinician was confident that metabolic acidosis and respiratory distress played a major role in his death, a necropsy was performed post-mortem. Unfortunately, the primary cause of pyrexia and abdominal discomfort was the pre-existing enterolith in his GI tract, which can be a silent killer if left undiagnosed for too long. He was only clinically symptomatic for approximately 30 days prior to his diagnosis and unfortunately, that was not enough time for him to present and stay stable and healthy at the time of surgery. He became febrile, which also indicates a systemic disturbance assumably stemming from the enterolith. This large patient was adequately positioned and padded at the time of surgery to minimize postanesthetic complications. The duration of anesthesia was not abnormally increased, and he remained stable throughout the surgery.
Losing a patient is never easy, no matter what the circumstance. Members of veterinary staff develop relationships with their patients, also bonding them to owners and trainers. It is easy to feel helpless following an unpredicted death, however, working as a team, having a plan in place for postanesthetic complications and attending continuing education meetings can ensure that things go smoothly during an emergency. Sadly, the mortality rate associated with equine anesthesia should always be considered, especially during an emergency.

ModernEquineVet.com | Issue 6/2016 15
gained laryngeal function, swallowed and was extu-bated without incident.
About 30 minutes after extubation, the patient attempted to roll into sternal recumbency and stand but was repeatedly unsuccessful with increased re-spiratory effort and apparent weakness in his hind limbs. The attending surgeon, clinician and other members of the support staff calmly, carefully and quietly entered the recovery stall and upon a sub-sequent venous blood gas analysis determined the patient was experiencing severe metabolic acidosis with a pH of 6.8. The clinician began to administer sodium bicarbonate 8.4% in Lactated ringer’s Solu-tion (LrS) IV as a bolus to correct the metabolic acidosis while others staff members attempted to keep the patient calm and free from panic.
While still suffering from apparent distress, the pa-tient was intubated nasotracheally and an intranasal cannula was passed into the nasotracheal tube. once secured in place, 100% supplemental oxygen was ad-ministered to the patient. Even with the sodium bi-carbonate 8.4% supplementation, the patient was still acidotic and displayed signs of respiratory distress.
He rolled into sternal recumbency and once sta-ble enough to be manipulated, he was carefully po-sitioned in a sling to assist him to a standing posi-tion. Head and tail ropes were used and as a smooth and calm attempt was made to assist the patient into standing with the help of the sling, he became agonal and was lowered into right lateral recumbency. Epi-nephrine was administered IV and a member of the support staff attempted to thump on his chest over his heart with her body weight behind her elbow to resuscitate the patient although usually unsuccessful.
Sadly and unfortunately the attempt to resus-citate our gentle giant was unsuccessful, and he passed away in the recovery stall two hours post-operatively. The entire staff was devastated for our patient and for his owners.
This beautiful and stoic gentle giant galloped his way into the hearts of everyone involved that day and will be remembered fondly. MeV
about the author Brandi Larsen, CVT, is an independent consultant in Weatherford, Texas. She has piloted and implemented custom veterinary training programs in large animal practices in Texas as well as lent her knowledge as a speaker at veterinary conferences nationwide. She is the central region AAEVT representative.
news noTes
the irish take liver Fluke Survey Blood markers and the fecal coproantigen ELISA are not reliable tests for fluke infestation, according to a recent study in the Equine Veterinary Journal.
The recombinant CL1 ELISA has a high specificity but low sensitivity, and other methods of ante-mortem diagnosis warrant investigation, the researchers said.
The researchers determined the prevalence of Fasciola hepatica infestation in horses in Ireland, and evaluated an indirect ELISA as a diagnostic tool. Two hundred horses were selected randomly at an abattoir and were placed into four groups based on their ante-mortem health status at ante-mortem examination.
On gross post-mortem examination, liver samples were graded from 1 to 6 (1 being lack of visible pathology, through mild to moderate changes, and 6 observations of fluke in the liver. )Periductular fibrosis, periductular cellular infiltrates and hyperplastic changes in the biliary epithelium were graded from 0 to 3 giving a maximum score of 9. Blood was collected for hematology, biochemistry and an indirect ELISA test based on F. hepatica recombinant cathepsin L1 antigen (CL1) and fecal egg counts (FEC) were performed.
The prevalence of liver fluke infestation was 9.5% (19 of 200 horses). Most of the positive horses had clinical grade 2 (lesions of no clinical significance) or 3 (evidence of underlying chronic disease), with only four showing non-specific signs of current clinical disease, highlighting that liver fluke infestation is often subclinical. In 16 of the 19 positive cases, adult fluke were seen in the liver. In fluke positive horses, the mean histological score was 6.5 (of a maximum 9), compared with in the fluke-negative horses.
There was no association between fluke status and total protein, albumin/globulin ratio and eosinophilia although these variables were associated strongly with strongyle infestation. There was also no association between fluke and any of the biochemical parameters (including GGT activity) and bile acid concentrations (an indicator of liver function) were within normal limits in all horses. Importantly, this suggests that hematology and blood biochemistry are not reliable for detecting potentially affected horses.
When the recombinant CL1 ELISA results were compared with the fluke status (based on post-mortem findings and FEC), the ELISA had low sensitivity (42.1%) but high specificity (95.6%), suggesting that the immune response to fluke infestation in horses may be different to other species in which similar ELISA tests are more sensitive.
Fluke eggs were observed on fecal sedimentation in six horses, four of which also had adult fluke on gross post-mortem. The fecal coproantigen ELISA was performed on samples from 42 horses and failed to detect infestation in any of them, including six that had adult fluke on gross post-mortem, showing this to be a very unreliable diagnostic tool. MeV
For more information:
Quigley A, Sekiya M, Egan S. Prevalence of liver fluke infection in Irish horses and assessment of a serological test for diagnosis of equine fasciolosis. Equine Vet J. 2016. May 27. [Epub ahead of print].
http://onlinelibrary.wiley.com/doi/10.1111/evj.12577/abstract
a liver fluke
Imag
es co
urte
sy of
The
Equin
e Vete
rinar
y Jou
rnal

16 Issue 6/2016 | ModernEquineVet.com
AAEVT MembershipBi-Annual NewsletterWeekly “HoofBeats” Email NewsblastFull access to www.aaevt.org, including the Career Center and the LibraryUp-to-date information on the AAEVTDiscounted registration for AAEVT Regional Meetings and the annual AAEP/AAEVT ConventionNTRA, Working Advantage and Platinum Performance BenefitsThe opportunity to participate in the AAEVT Online Certification Program or to become a member of the AEVNT Academy-Specialty in Equine Veterinary Nursing Scholarship opportunities. AAEVT’s Equine Manual for Veterinary Technicians (Blackwell Publishing 20% discount on purchase price)Opportunity to attend Purina’s Annual Equine Veterinary Technician Conference - All Expenses paid!
•••••
•••
••
•
AAEVT ObjectivesProvide opportunities for CE, training, communication, and networkingEducate the equine veterinary community and the public about our professionInform Members of issues affecting our professionAssist in providing the best medical care to improve the health and welfare of the horse
••••
AAEVT Online Equine Certification ProgramA three course, 10 module, equine-only online program offered through ACTGeared toward Credentialed Veterinary Technicians, Assistants, Support staff, & StudentsAreas of study include: equine medical terminology, anatomy and physiology, parasitology, laboratory, diagnostics, equine basics (breeds, wellness, husbandry,) diagnostic procedures, emergency medicine, restraint, pharmacology, surgical assistance and anesthesia, equine office proceduresA certificate of completion is awarded to those who: Successfully complete required courses Complete the list of required skills (per a supervising DVM who is an AAEP member) Attend an AAEVT regional CE symposium and participate in the we labsThose individuals who successfully complete the programs will be recognized as AAEVT Certified Equine Veterinary Technicians / AAEVT Certified Equine Veterinary Assistants depending on their current designation. The certificate is recognized by the AAEVT and the AAEP but does not grant the credentialed status by the AVMAFor more information go to www.aaevt.4act.com or call 800-357-3182
•••
•
•
•
For more inf or mat ion vist www.aae vt.org*American Association of Equine Veterinary Technicians and Assistants
AAEVT Mission Statement: To promote the health and welfare of the horse through the education and professional enrichment of the equine veterinary technician and assistant.
AAEV T M E M b E r s h i pMembership in the AAEVT is open to all veterinary technicians, assistants, support staff and those employed in the veterinary health care industry worldwide. Student membership is open to those currently enrolled in an AVMA/CVMA accredited veterinary technology program.
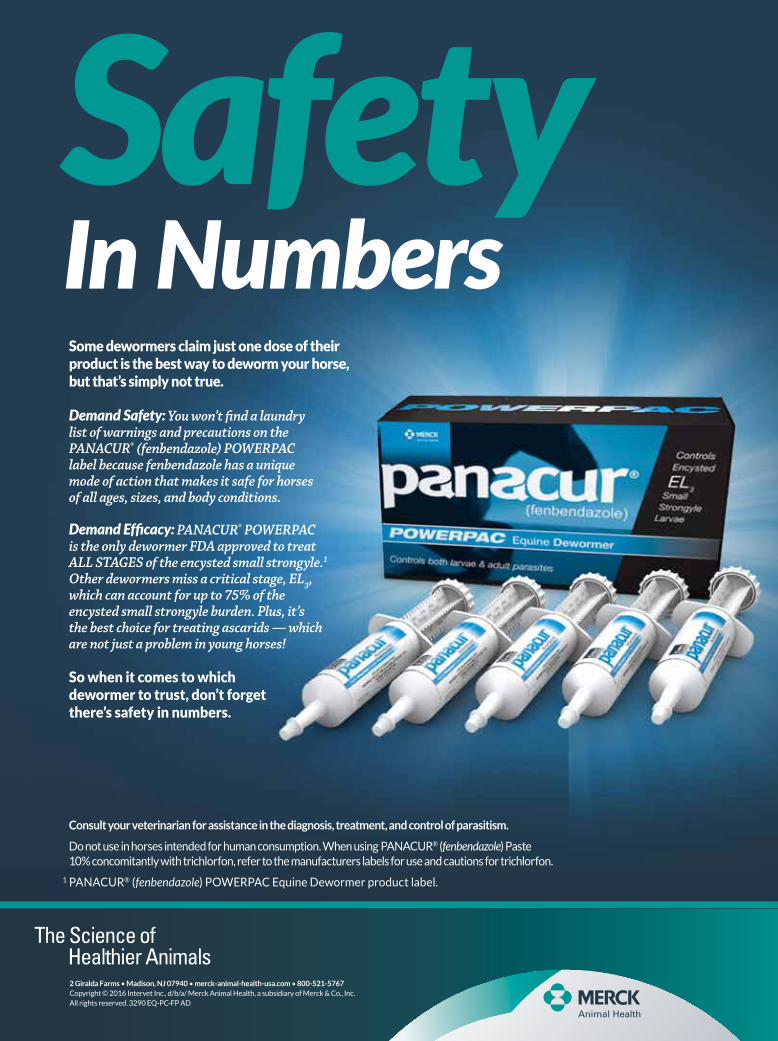
Sarcoid skin tumors are the most common form of cancer in horses, but little is known about why the papillomavirus behind them strikes some horses and not others.
A new study by an international research group led by scientists at the baker Institute for Animal Health at cornell’s college of Vet-erinary Medicine in Ithaca, Ny, shows that genetic differences in immune function among horses partly accounts for these differ-ences. The study mirrors findings in humans, as some people have a genetic susceptibility to human papillomavirus, which can cause cervical and other cancers.
“Many therapies have been proposed as the ‘best’ treatment for sarcoids,” says cornell's Doug Antczak, VMD, phD, Dorothy Havemeyer Mcconville profes-sor of Equine Medicine, who led the study. In some horses, tumors develop as small bumps under the skin or as scaly lesions that easily can be removed by a veterinarian, but in others, the problem becomes much more serious. Surgery, cryo-therapy, laser treatment, injecting the tumors with drugs to kill the cells, radiation treatment and im-munotherapy have all been shown to cure these recalcitrant tumors, “but some tumors tend to recur no matter what treatment is used, and there is no universal consensus on a uniformly successful therapy,” said Dr. Antczak.
For years, researchers have thought that bovine papillomavirus (bpV) is the most likely culprit be-hind sarcoid tumors. recent work from Europe suggests variants of the bpV have become adapted to horses and are probably the cause of most sarcoids, Dr. Antczak said.
Dr. Antczak and his team
GEnEtic
onCology
do Horses Have
T o s a R c o I d s ?SuScEPtibilitY
a 3 cm sarcoid tumor on a horse’s ear. Sarcoids often develop as small bumps under the skin or scaly lesions like the one in the photo. depending on their location on the horse’s body, tumors like these can often be removed by a veterinarian. However, in certain horses sarcoids tend to regrow after surgery, sometimes to much larger tumors that are impossible to cure.
Imag
es co
urte
sy of
Univ
esity
of Co
rnell

ModernEquineVet.com | Issue 6/2016 17
AAEVT MembershipBi-Annual NewsletterWeekly “HoofBeats” Email NewsblastFull access to www.aaevt.org, including the Career Center and the LibraryUp-to-date information on the AAEVTDiscounted registration for AAEVT Regional Meetings and the annual AAEP/AAEVT ConventionNTRA, Working Advantage and Platinum Performance BenefitsThe opportunity to participate in the AAEVT Online Certification Program or to become a member of the AEVNT Academy-Specialty in Equine Veterinary Nursing Scholarship opportunities. AAEVT’s Equine Manual for Veterinary Technicians (Blackwell Publishing 20% discount on purchase price)Opportunity to attend Purina’s Annual Equine Veterinary Technician Conference - All Expenses paid!
•••••
•••
••
•
AAEVT ObjectivesProvide opportunities for CE, training, communication, and networkingEducate the equine veterinary community and the public about our professionInform Members of issues affecting our professionAssist in providing the best medical care to improve the health and welfare of the horse
••••
AAEVT Online Equine Certification ProgramA three course, 10 module, equine-only online program offered through ACTGeared toward Credentialed Veterinary Technicians, Assistants, Support staff, & StudentsAreas of study include: equine medical terminology, anatomy and physiology, parasitology, laboratory, diagnostics, equine basics (breeds, wellness, husbandry,) diagnostic procedures, emergency medicine, restraint, pharmacology, surgical assistance and anesthesia, equine office proceduresA certificate of completion is awarded to those who: Successfully complete required courses Complete the list of required skills (per a supervising DVM who is an AAEP member) Attend an AAEVT regional CE symposium and participate in the we labsThose individuals who successfully complete the programs will be recognized as AAEVT Certified Equine Veterinary Technicians / AAEVT Certified Equine Veterinary Assistants depending on their current designation. The certificate is recognized by the AAEVT and the AAEP but does not grant the credentialed status by the AVMAFor more information go to www.aaevt.4act.com or call 800-357-3182
•••
•
•
•
For mo re in f o r mat i on vi st www.aae vt.org*American Association of Equine Veterinary Technicians and Assistants
AAEVT Mission Statement: To promote the health and welfare of the horse through the education and professional enrichment of the equine veterinary technician and assistant.
AAEV T M E M b E r s h i pMembership in the AAEVT is open to all veterinary technicians, assistants, support staff and those employed in the veterinary health care industry worldwide. Student membership is open to those currently enrolled in an AVMA/CVMA accredited veterinary technology program.

18 Issue 6/2016 | ModernEquineVet.com
onCology
applied a genomewide associa-tion study to compare the genetic makeup of horses with and with-out sarcoid tumors at more than 50,000 sites in the equine genome. They studied 82 sarcoid-bearing horses from the United States and United Kingdom and 272 carefully matched controls that did not have sarcoids. They found regions on chromosomes 20 and 22 that tend-ed to be different in horses diag-nosed with sarcoids, evidence that a horse’s genes determine, in part, how susceptible it is to sarcoids.
“This is an example of more complicated genetics – multigene susceptibility,” said Dr. Antczak. “More than one genetic region is associated with susceptibility to sarcoids, and they don’t completely determine whether or not a horse will develop the disease once it’s ex-posed to bpV.”
This genetic link implicates the
immune system in sarcoid suscep-tibility. The region of chromosome 20 associated with sarcoid devel-opment is within a portion of the genome responsible for immune
function called the major histo-compatibility complex (MHc) class II region. The MHc type as-sociated with sarcoid susceptibility is rare among Standardbred horses, a fact that may explain why sarcoid is diagnosed so rarely in this breed.
This complex mix of virus, host genes and tumor development may have relevance to a related human condition. Tumors caused by HpV account for more than 5% of cancer cases worldwide. In women with cervical cancer, an association with the MHc class II region has also been shown.
“That should make a light bulb go off,” Antczak said. “It suggests there’s a common mechanism in both species for susceptibility to tu-mor progression that may involve subversion of the host immune re-sponse. by studying this phenom-enon in horses you can learn about human cancer and vice versa.” MeV
cornell’s doug antczak, dvM, and his collaborators found that the region of chromosome 20 associated with sarcoid development is within a portion of the genome responsible for immune function.
Imag
es co
urte
sy of
Corn
ell U
niver
sity
auburn Gets new Standing ct for large animalsThe Auburn University college of Veterinary Medicine added standing commuted tomography (cT). For radiology and equine faculty, this ad-vanced diagnostic tool has already proven to make a significant difference in diagnosing and treating complicated diseases found in a horse’s neck and skull. Robert Cole, DVM, an assistant professor of radiology, said the concept behind standing cT was to allow cross sectional imaging of the horse’s head without anesthesia.
Typical cT requires anesthesia, which can be risky. The standing cT creates cross sectional images of the skull and upper part of the cervi-cal spine. Dr. cole said the machine is allowing surgeons to understand “exactly what is going on before the surgery takes place. Typically, on a lot of cases, a horse may present with a nasal discharge.
“We’d start with radiographs traditionally and we might see fluid in the sinus but we couldn't tell why it was there or the origin. The surgeon would go in and explore that sinus, not knowing exactly what they were
getting into.” The standing cT, in the same amount of time or less time, can have that cross-sectional imaging and locate the boundary of the disease process and its location. “The surgeon now knows exactly how to plan and knows what they are up against.” MeV
Staiger EA, Chia TT, Miller D, et al. Host genetic influence on papillomavirus-induced tumors in the horse. Int J Can. 2016 May 6 [Epub ahead of print]) http://onlinelibrary.wiley.com/doi/10.1002/ijc.30120/abstract
For more information:
Imag
es co
urte
sy of
Aubu
rn U
niver
sity C
olleg
e of V
eter
inary
Med
icine

ModernEquineVet.com | Issue 6/2016 19
news
Cour
tesy
of Th
e Equ
ine Ve
t Jou
rnal
de Laat MA, Sillence, MN. The repeatability of an oral glucose test in ponies. Equine Vet J. 2016. May 23. [Epub ahead of print]. http://onlinelibrary.wiley.com/doi/10.1111/evj.12579/abstract
For more information:
oral glucose tests repeatable in poniesThe oral D-glucose test has a good degree of repeat-ability in ponies under controlled conditions, and a carbohydrate-based feed is a suitable alternative test substrate, according to a recent study in the Equine Veterinary Journal.
The oral glucose tolerance test is used commonly to detect insulin dysregulation. The standard proto-col involves feeding 1g/kg bodyweight of D-glucose (dextrose) powder in bran and collecting postpran-dial blood samples for insulin. In a recent study, re-searchers from Queensland University in brisbane, Australia, used 0.75g/kg D-glucose for greater palat-ability, mixed with a fixed amount of wheat bran and lucerne chaff.
of 12 ponies originally sourced for the study, eight were finally included as they showed good ac-ceptance of the glucose test diet.
First a repeatability study was undertaken: fol-lowing overnight fasts, oral glucose tests were per-formed on two ponies at a time (to ensure consis-tent washout periods) on three separate occasions over a three-week period. blood glucose and serum insulin concentrations were taken before the glu-cose meal, and at 90 and 180 minutes and 24 hours. blood glucose levels were also measured immedi-ately after feeding.
They found that blood insulin and glucose con-centration were higher than basal concentrations after the D-glucose feed in all ponies and had re-turned to baseline 24 hours. overall, insulin con-centrations did not alter significantly in individuals among the three tests, and there was no signifi-cant difference in insulin concentrations at differ-ent points after feeding. Glucose results showed a higher degree of variability than insulin concen-trations, particularly in the post-prandial samples. overall the oral glucose test had a good degree of repeatability in most ponies. However there was a large degree of variability in one individual pony, indicating that the test may not be reliable in all in-dividuals and results must be interpreted within the individual clinical context.
The study also demonstrated that blood sam-pling at around two hours post-feeding as per the current recommendations is suitable for achieving
diagnostic results. As some ponies found the test diet unpalatable, an
alternative test diet consisting of commercial cereal-based pellets was explored. pellets containing 0.75g/kg bodyweight of non-soluble carbohydrate were mixed with wheat bran and lucerne chaff. blood glucose and serum insulin concentrations with the pellets correlat-ed well with those in the D-glucose diet and there was good agreement with improved compliance and better palatability MeV
as some ponies found the test diet unpalatable, an alternative test diet consisting of commercial cereal-based pellets was explored.

reach your veterinarians wherever they are, whenever they want.
FoR adVeRTIsIng RaTes and InFoRMaTIon, eMaILMatthew todd
Equine VetThe Modern