Embed Size (px)
Citation preview
2/11/2014
1
The Neuro-ophthalmologyof Concussion
Leonard V. Messner, OD, FAAODanielle Leong, OD, FAAO
Financial Disclosure
Dr. Messner has received honoraria from Carl Zeiss Meditec. He is on the speakers’ bureau for Carl Zeiss Meditec.
Dr. Leong is employed by King-Devick Test, LLC as the Director of Research.
Chris Nowinski
Trainers rushed to Johnson's aid. Minutes later, they led him from the field. Upon reaching the sideline, Johnson
fell to his knees and clutched his head. If ever there was a defining image of the epidemic of concussions
sweeping the NFL, Johnson embodied it.
What happened next shows the NFL - despite a lot of talk, a national television campaign hailing its devotion
to improved safety and a $30 million donation to the National Institutes of Health to study brain trauma - still
cannot claim to have a coherent , effective way of dealing with concussions, let alone adequate tools for
diagnosing them on the field.
Just 11 minutes and 44 seconds after taking a hit that should have ended his game, Johnson returned to the
field. It was the fourth quarter, after all, and the Lions were down 14 points to a division rival. There was no
question he'd play. "It's a part of football ," Johnson told Detroit's WXYT-FM the following day. "You get
concussed , you gotta keep on playing."
The NFL'S Rush to Build
Unbreakable Players
Even more stunning, Johnson and his own coach can't agree on
what happened . Four days after the Sept. 30 matchup,
Johnson announced he'd finished the game with a concussion .
Not so, insists Lions head coach Jim Schwartz, who asserted
at a press conference that Johnson "was thoroughly checked"
on the sideline and cleared to resume playing.
MORE ON SPORTS CONCUSSIONS
The only thing more troubling than the hit that rattled Calvin Johnson's brain was what happened when he finally
got back up.
2/11/2014
2
9 7
VIDEO
Weather hard to c./1 through thJs
fog
POLmcs SPORTS BUSINESS SCIENCE/TECH LOCAL
Super Bowl Confetti Made Entirely From ShreddedConcussion StudiesPHOTO FINISH Sports·NFL Football • Super Bowi • ISSUE50•04 ·Feb 2, 2014
Concussive Sports Injuries
• School sport concussions drawing national attention
• Collegiate, high school
• NFL interest in chronic traumatic encephalopathy
• 20 to 30% of Alzheimer’spatients report head traumavs. 8 to 10% of controls
State concussion bill closer to realityHouse panel agrees on plan to protect kids
L'l See More
Youth sports leagueshave grown into a $5billion industry withvirtually no regulat on. Kids suffer injuries at analarming rate, and someorganizers are abusingboth children and leaguefunds. In the five-dayseries "Utt le leagues, bigcosts," The Dispatch explores where youthsports have taken wrongturns in recent years.
By Jim Siegel
The Columbus Dispatch - Wednesday June 13, 2012 7:59 AM
Abill designed to educate coaches and ensure that young Ohio athletes are
pulled from competition when they show concussion-like symptoms passed
a House committee yesterday after 1 0 revisions and several
months of debate.
There has been general agreement that more needs to be done to protect
youths from the dangers of concussions, but legislators have struggled to
balance issues regarding liability and who is responsible for allowing a
player to return to action. Some members still expressed reservations
yesterday.
Concussion
• Complex pathophysiological process resulting from traumatic biomechanical forces
• Functional rather than structural injury
• Mild traumatic brain injury (mTBI) –Diffuse axonal injury
• Loss of consciousness in less than 10%
Br J Sports Med 2005;39:196
Epidemiology• 300,000 to nearly 4 million per year
• Problem of under-reporting and debateregarding definition
• Multiple studies suggest rate on rise
• Girls have a higher rate of concussion
• Boys’ High school football followedby girls' soccer lead the list
• Nearly 85% of concussions may go undiagnosed
JAMA, October 27, 2010American College of Sports Medicine
High School Concussions(per 100,000)
• Football: Between 60 and 76• Girl's soccer: Between 33 and 35• Boys' lacrosse: Between 30 and 46• Girls' lacrosse: Between 20 and 31• Boys' soccer: Between 17 and 19• Boys' wrestling: Between 17 and 23• Girls' basketball: Between 16 and 18• Softball: Between 11 and 16• Boys' basketball: Between 11 and 21• Girls' field hockey: Between 10 and 24• Cheerleading: 11• Girls' volleyball: Between 5 and 8• Boys' baseball: Between 4 and 6
Halstead M, et al. Pediatrics 2010Meehan WP, et al. Am J Sports Med 2011
2/11/2014
3
Hockey Concussion Education Project(HCEP)
• 67 male hockey players (ages 16-21)• Prospective, physician-observed surveillance
for concussion (2009-2010)• 17 players sustained 21 concussions (25%)• 5/17 (29%) sustained a second concussion• 15/17 (88%) players admitted to prior
concussion• Concussion by position:
– 71% forwards– 29% defensemen
Neurological Focus 2010
Youth Sports & Concussion
• Children are more susceptible to headinjury than adults and require a longerperiod of recovery
Kirkwood MJ, et al. Pediatrics 2006
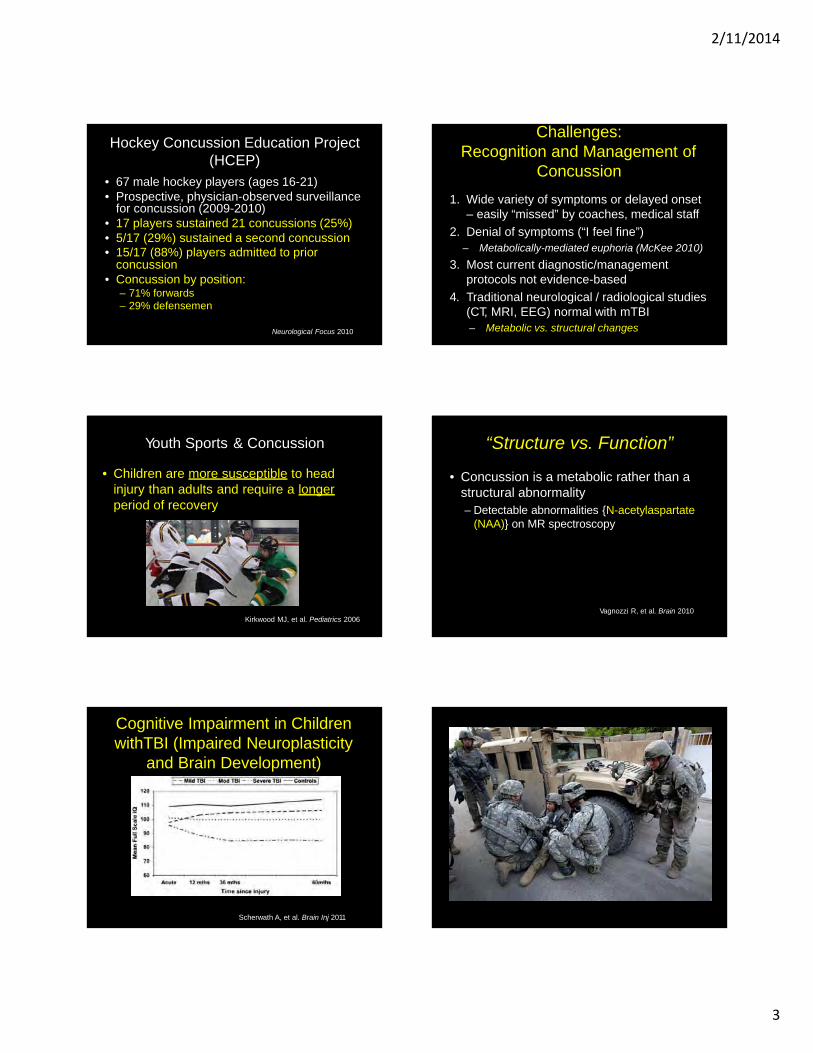
Cognitive Impairment in ChildrenwithTBI (Impaired Neuroplasticity
and Brain Development)
Scherwath A, et al. Brain Inj 2011
Challenges: Recognition and Management of
Concussion
1. Wide variety of symptoms or delayed onset– easily “missed” by coaches, medical staff
2. Denial of symptoms (“I feel fine”)– Metabolically-mediated euphoria (McKee 2010)
3. Most current diagnostic/managementprotocols not evidence-based
4. Traditional neurological / radiological studies (CT, MRI, EEG) normal with mTBI– Metabolic vs. structural changes
“Structure vs. Function”
• Concussion is a metabolic rather than astructural abnormality– Detectable abnormalities {N-acetylaspartate
(NAA)} on MR spectroscopy
Vagnozzi R, et al. Brain 2010
2/11/2014
4
WWI• Advent of trench
warefare and continuous shelling
• 10% overall fatalities due to shrapnel/indirect trauma
• Term “shell shock” used to describe psychiatric findings Battle of Ypres - 1917
Major Frederick Mott
• British neuropathologist who proposed studying brains of deceased WWIsoldiers
• Questioned link between“shell shock” andorganic brain disease
• In 1917, British Army bans further use ofterm “shell shock”
WWII• Finnish psychiatrist Dr. Harry Federley
adopts term LMF (Lacks Moral Fibre) for combat-related neuroses
• German psychiatrist Dr. Rudolph Brickenstein: “…that if a soldier did break down and could not continue fighting, it was a leadership problem, not one for medical personnel or psychiatrists. Breakdown (he said) usually took the form of unwillingness to fight or cowardice.”
Combat-Related TBI
• Most deployed soldiers report one or moreblast injuries
• TBI proposed as “signature injury” of modern combat
• Limited data on prevalence
• Potential link to post-traumatic stressdisorder (PTSD)
mTBI in Soldiers Returning from Iraq
• Survey of 2525 Army soldiers 3-4 mosafter return from deployment– 4.9% reported injury with LOC
• 43.9% with PTSD
– 10.3% injury with altered mental status• 27.3% with PTSD
Hoge CW et al. N Engl J Med 2008
PTSD & Post-TraumaticHeadache
• Retrospective analysis of 270 soldiers withpost-traumatic headache
• 105 (39%) met criteria for PTSD
Rosenthal JF, et al. Headache 2013
2/11/2014
5
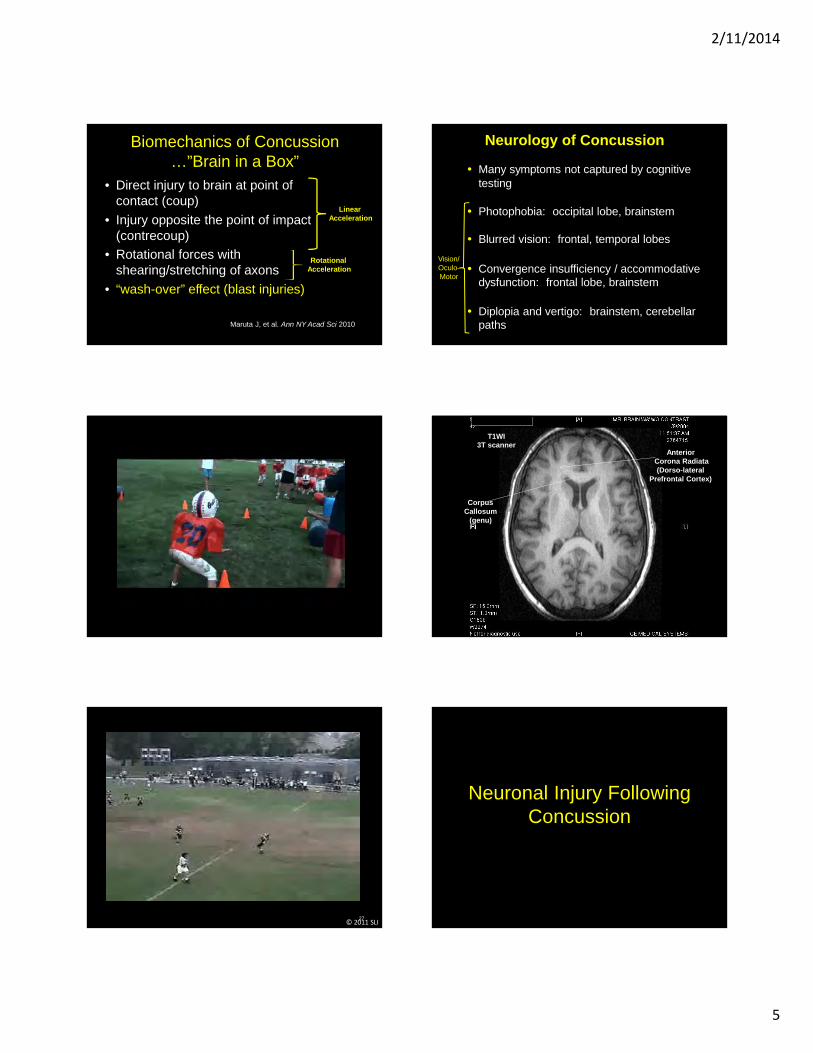
Biomechanics of Concussion…”Brain in a Box”
• Direct injury to brain at point ofcontact (coup)
• Injury opposite the point of impact (contrecoup)
• Rotational forces withshearing/stretching of axons
• “wash-over” effect (blast injuries)
Maruta J, et al. Ann NY Acad Sci 2010
Linear Acceleration
Rotational Acceleration
27© 2011 SLI
Neurology of Concussion
• Many symptoms not captured by cognitivetesting
• Photophobia: occipital lobe, brainstem
• Blurred vision: frontal, temporal lobes
• Convergence insufficiency / accommodativedysfunction: frontal lobe, brainstem
• Diplopia and vertigo: brainstem, cerebellarpaths
Vision/ Oculo-Motor
T1WI3T scanner
AnteriorCorona Radiata (Dorso-lateral
Prefrontal Cortex)
Corpus Callosum
(genu)
Neuronal Injury FollowingConcussion
2/11/2014
6
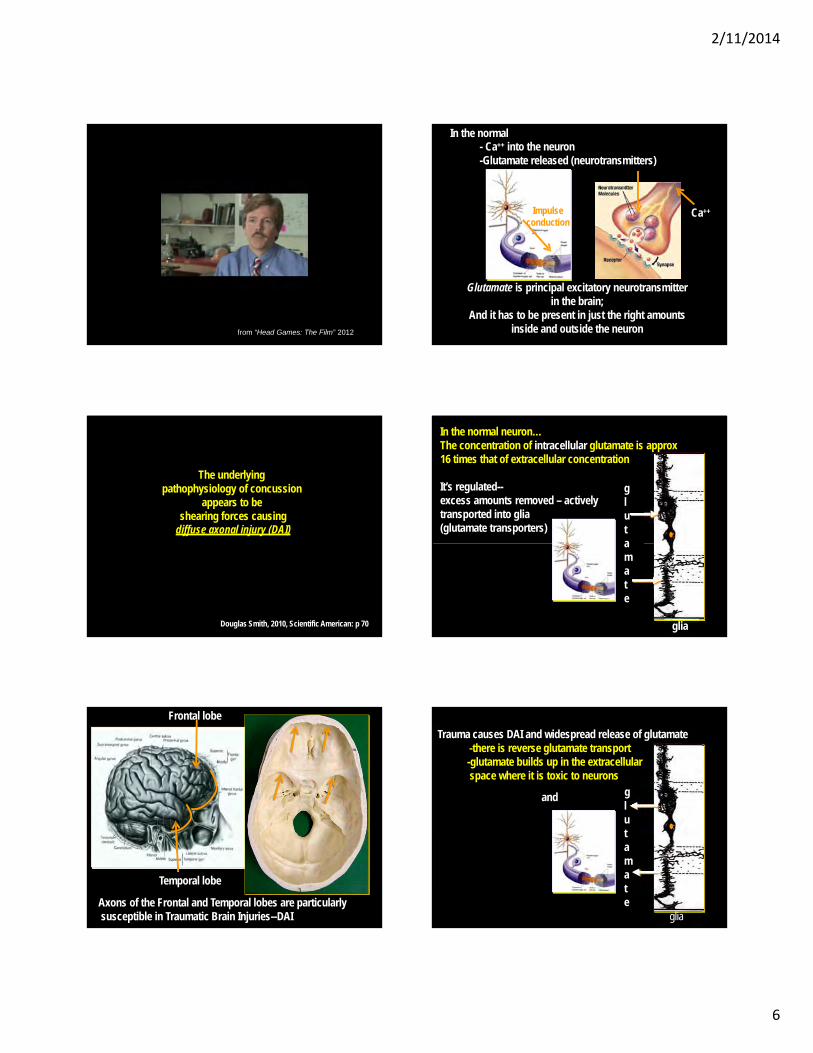
from “Head Games: The Film” 2012
The underlyingpathophysiology of concussion
appears to beshearing forces causing
diffuse axonal injury (DAI)
Douglas Smith, 2010, Scientific American: p 70
Frontal lobe
Temporal lobe
Axons of the Frontal and Temporal lobes are particularlysusceptible in Traumatic Brain Injuries--DAI
In the normal- Ca++ into the neuron-Glutamate released (neurotransmitters)
Ca++Impulseconduction
Glutamate is principal excitatory neurotransmitterin the brain;
And it has to be present in just the right amounts inside and outside the neuron
In the normal neuron…The concentration of intracellular glutamate is approx 16 times that of extracellular concentration
It’s regulated--excess amounts removed – activelytransported into glia(glutamate transporters)
glut ama t e
glia
-there is reverse glutamate transport-glutamate builds up in the extracellularspace where it is toxic to neurons
glut ama t e
glia
Trauma causes DAI and widespread release of glutamate
and
2/11/2014
7
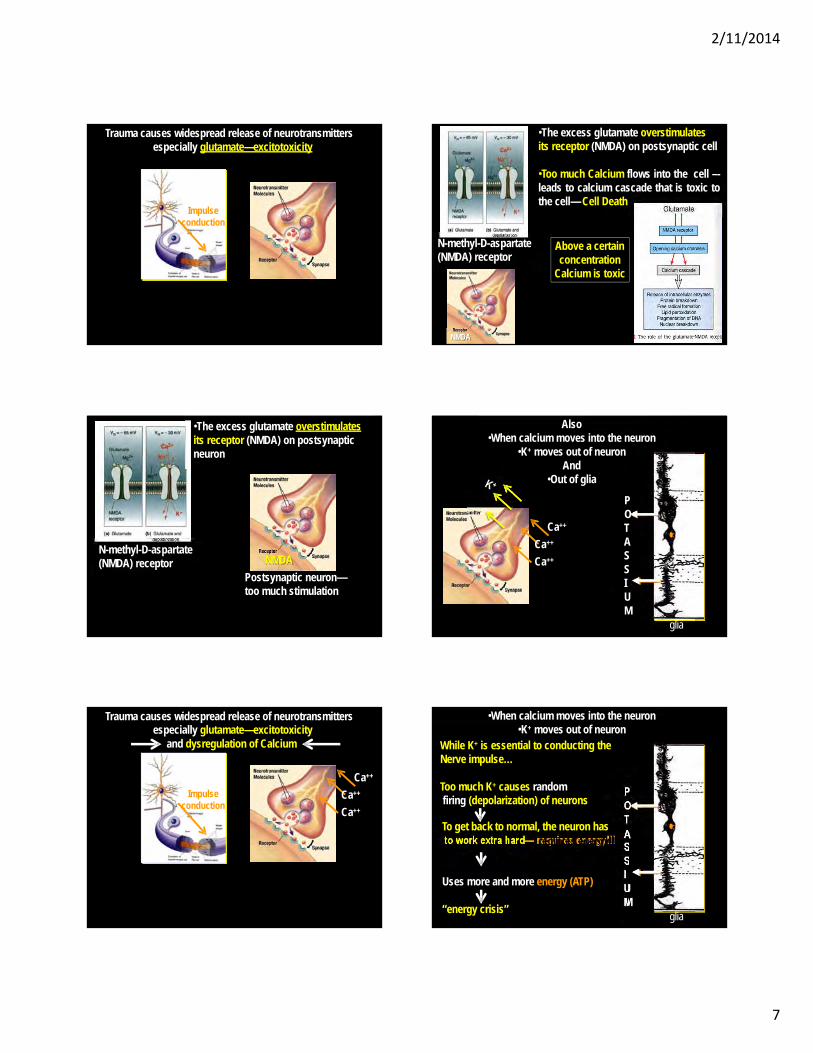
Trauma causes widespread release of neurotransmittersespecially glutamate—excitotoxicity
Impulseconduction
N-methyl-D-aspartate (NMDA) receptor
•The excess glutamate overstimulatesits receptor (NMDA) on postsynaptic neuron
NMDA
Postsynaptic neuron—too much stimulation
Trauma causes widespread release of neurotransmittersespecially glutamate—excitotoxicity
and dysregulation of Calcium
Ca++
Ca++
Ca++
Impulseconduction
N-methyl-D-aspartate (NMDA) receptor
•The excess glutamate overstimulatesits receptor (NMDA) on postsynaptic cell
•Too much Calcium flows into the cell –-leads to calcium cascade that is toxic tothe cell— Cell Death
NMDA
Above a certain concentration
Calcium is toxic
Also•When calcium moves into the neuron
•K+ moves out of neuron And
•Out of glia
POT A S SIU M
glia
Ca++
Ca++
Ca++
POT
to work extra hard— requires energy!!! ASSIU M
glia
•When calcium moves into the neuron•K+ moves out of neuron
While K+ is essential to conducting theNerve impulse…
Too much K+ causes randomfiring (depolarization) of neurons
To get back to normal, the neuron has
Uses more and more energy (ATP)
“energy crisis”
2/11/2014
8
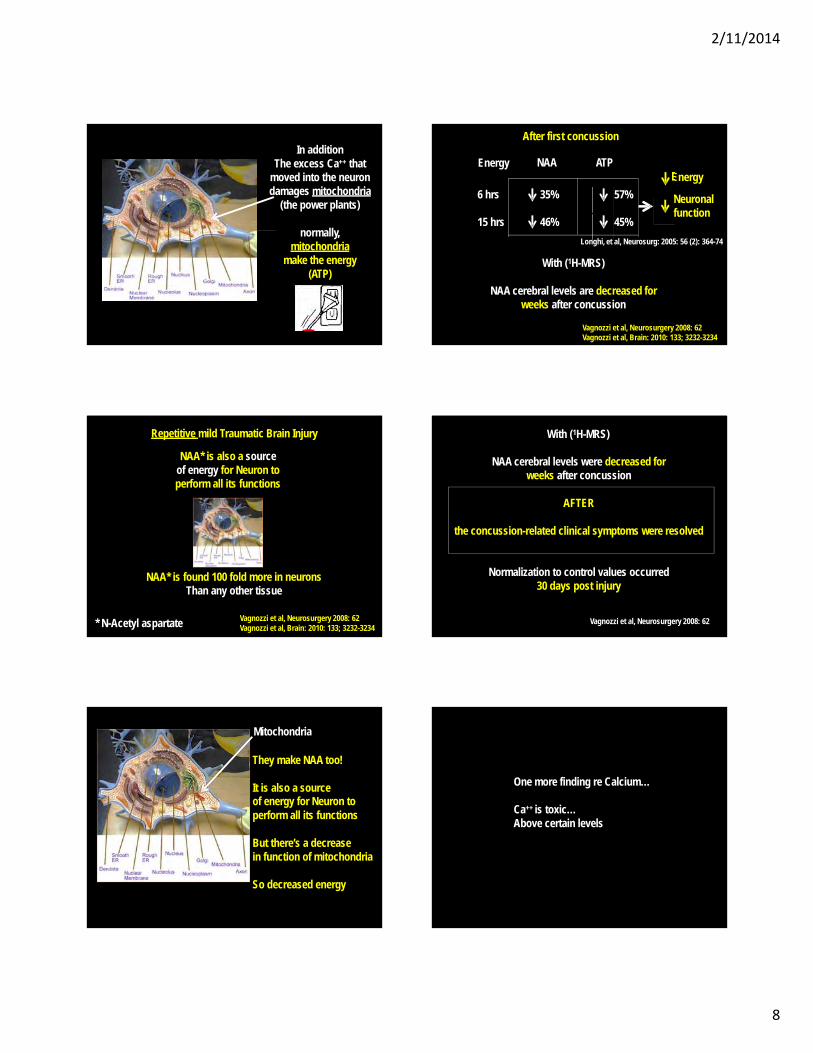
In additionThe excess Ca++ that
moved into the neurondamages mitochondria
(the power plants)
normally, mitochondria
make the energy(ATP)
NAA* is also a sourceof energy for Neuron to perform all its functions
* N-Acetyl aspartate
Repetitive mild Traumatic Brain Injury
Vagnozzi et al, Neurosurgery 2008: 62Vagnozzi et al, Brain: 2010: 133; 3232-3234
NAA* is found 100 fold more in neuronsThan any other tissue
Mitochondria
They make NAA too!
It is also a sourceof energy for Neuron to perform all its functions
But there’s a decreasein function of mitochondria
So decreased energy
Energy NAA ATP
6 hrs
15 hrs
35%
46%
57%
45%
After first concussion
Longhi, et al, Neurosurg: 2005: 56 (2): 364-74
With (1H-MRS)
NAA cerebral levels are decreased forweeks after concussion
Vagnozzi et al, Neurosurgery 2008: 62Vagnozzi et al, Brain: 2010: 133; 3232-3234
Energy
Neuronalfunction
With (1H-MRS)
NAA cerebral levels were decreased forweeks after concussion
AFTER
the concussion-related clinical symptoms were resolved
Normalization to control values occurred30 days post injury
Vagnozzi et al, Neurosurgery 2008: 62
One more finding re Calcium…
Ca++ is toxic…Above certain levels
2/11/2014
9
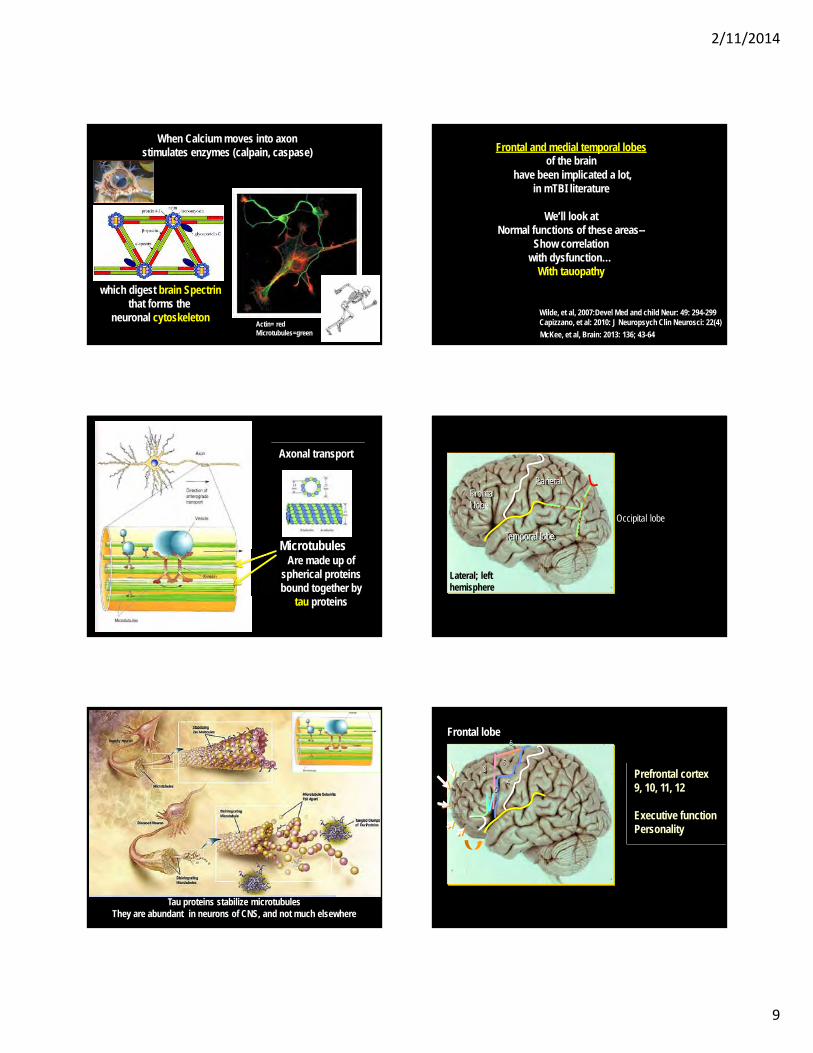
Actin= redMicrotubules=green
When Calcium moves into axonstimulates enzymes (calpain, caspase)
which digest brain Spectrinthat forms the
neuronal cytoskeleton
Axonal transport
MicrotubulesAre made up of
spherical proteins bound together by
tau proteins
Tau proteins stabilize microtubulesThey are abundant in neurons of CNS, and not much elsewhere
Frontal and medial temporal lobesof the brain
have been implicated a lot,in mTBI literature
We’ll look atNormal functions of these areas--
Show correlationwith dysfunction…
With tauopathy
Wilde, et al, 2007:Devel Med and child Neur: 49: 294-299 Capizzano, et al: 2010: J Neuropsych Clin Neurosci: 22(4)
McKee, et al, Brain: 2013: 136; 43-64
Occipital lobe
Frontal lobe
Temporal lobe
Lateral; left hemisphere
Parietal
6
68
46
Prefrontal cortex9, 10, 11, 12
Executive function Personality
Frontal lobe
2/11/2014
10
6
68?
46
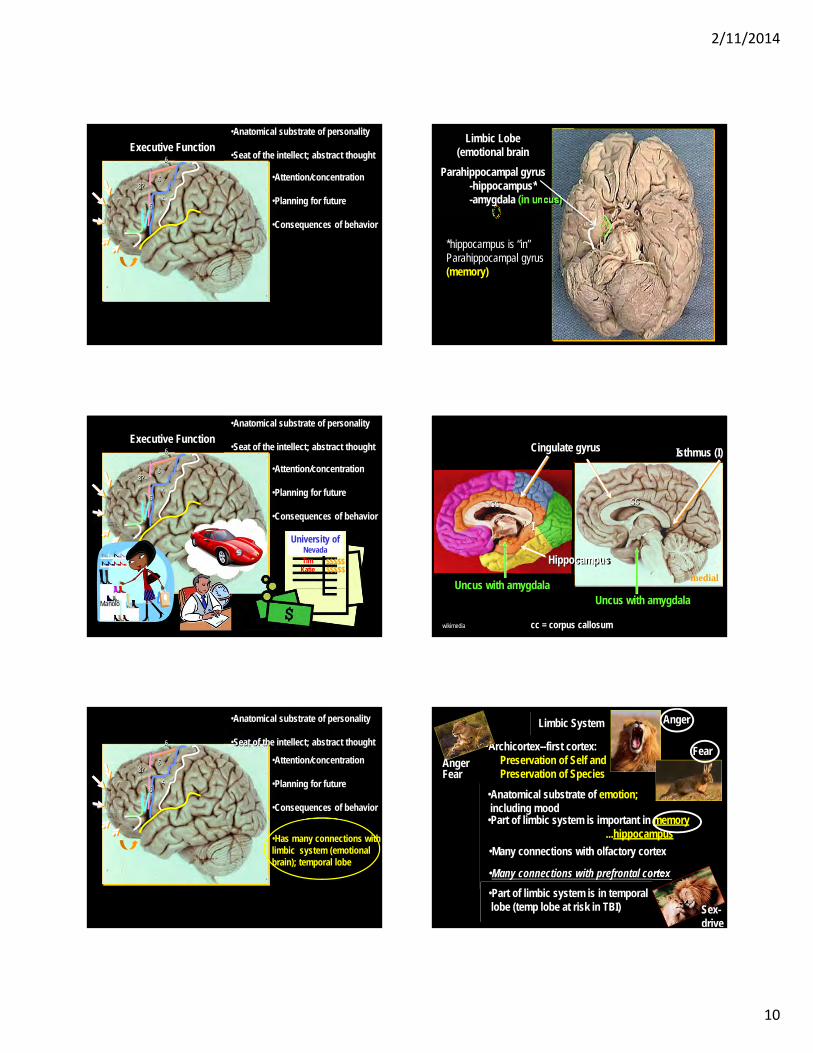
•Anatomical substrate of personality
•Seat of the intellect; abstract thought
•Attention/concentration
•Planning for future
•Consequences of behavior
Executive Function
6
68?
46
•Anatomical substrate of personality
Tim Katie
Manolo
$$$$$$$$$$
•Seat of the intellect; abstract thought
•Attention/concentration
•Planning for future
•Consequences of behavior
University ofNevada
Executive Function
6
68?
46
•Anatomical substrate of personality
•Seat of the intellect; abstract thought
•Attention/concentration
•Planning for future
•Consequences of behavior
•Has many connections with limbic system (emotional brain); temporal lobe
Limbic Lobe (emotional brain
Parahippocampal gyrus-hippocampus*-amygdala (in uncus)
*hippocampus is “in” Parahippocampal gyrus(memory)
cc
cc = corpus callosum
Cingulate gyrus Isthmus (I)
medial
Uncus with amygdala
wikimedia
Uncus with amygdala
cc
I
Hippocampus
Limbic System
•Archicortex--first cortex: Preservation of Self and Preservation of Species
•Anatomical substrate of emotion;including mood
•Part of limbic system is important in memory...hippocampus
•Many connections with olfactory cortex
•Many connections with prefrontal cortex
•Part of limbic system is in temporallobe (temp lobe at risk in TBI)
Fear
Anger
AngerFear
Sex-drive
2/11/2014
11
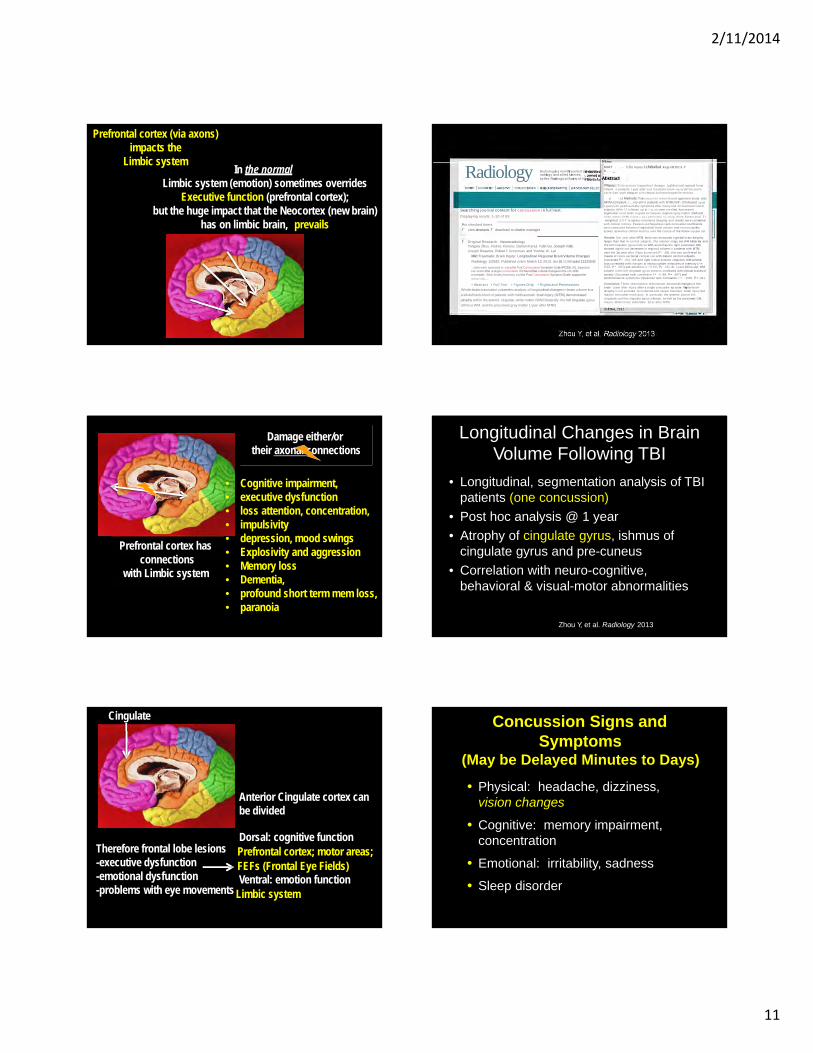
In the normalLimbic system (emotion) sometimes overrides
Executive function (prefrontal cortex);but the huge impact that the Neocortex (new brain)
has on limbic brain, prevails
Prefrontal cortex (via axons)impacts the
Limbic system
Prefrontal cortex hasconnections
with Limbic system
Damage either/ortheir axonal connections
• Cognitive impairment,• executive dysfunction• loss attention, concentration,• impulsivity• depression, mood swings• Explosivity and aggression• Memory loss• Dementia,• profound short term mem loss,• paranoia
Anterior Cingulate cortex canbe divided
Dorsal: cognitive functionPrefrontal cortex; motor areas; FEFs (Frontal Eye Fields)Ventral: emotion function
Cingulate
-problems with eye movements Limbic system
Therefore frontal lobe lesions-executive dysfunction-emotional dysfunction
Radiology RadiologyIs a monthly joumzl de••ote'c:lradiology and allied sciences,by the Radiological Society of North
Searching j ournal content for concussion in fu l l text.
Displaying results 1-10 of 89
For checked items
r view abstracts r download to citation manager
r Original Research - NeuroradiologyYongxia Zhou, Andrea Klerans, Damon Kenul, Yulin Ge, Joseph Rath,Joseph Reaume, Robert I.Grossman, and Yvonne W. Lui
Mild Traumatic Brain Injury: Longitudinal Regional Brain Volume Changes
Radiology 122542; Published online March 12, 2013, doi:10.1148/radiol.13122542
...state were assessed by using the Post Concussion Symptom Scale (PCSS) (41...injurybutcan occur after asingleconcussion.We found that volumechanges inthe rACWMcorrelated...Beck Anxiety Inventory ard the Post Concussion Symptom Scale, support thenotionthat...
• Abstract • Full Text • Figures Only • Rights and Permissions
Whole-brain automated volumetric analysis of longitudinal changes in brain volume in a
well-defined cohort of patients with mildtraumatic brain injury (MTBI) demonstrated
atrophy within the anterior cingulate white matter (WM) bilaterally, the left cingulate gyrus
isthmus WM, and the precuneal gray matter 1 year after MTBI.
MildT . . - lrlln Injury. l.cJntltudinal RegioMIIr l ln Yo . . . _
PWpose:::To lnvestioatt longnud•naJ changes 1n global and regional brain YOiurnt: n patients 1 year aner mid traumatic bram •njury (MTBI) and tocorre:Jatt such chang.es with chnic:al and neurocognrtiVe metrics.
s - .c t Methods:Thisinsuuuonal review board- approved study wasHIPAAcompliant. r...,nry-ei!t>t patients with NTBI(With 19 followed up at 1 year) with posttraumatic symptoms after inJury and 22 matched controlsubjects (Whh 12 fo llowec up at I ye_at) v.oere enrolled. Automatedsegmentat on of bc'ain re.g•ons to compute re-gJonaJ gray m atter (GM) andw h ite matter (WM) volumt.s wa.s performed by using three- d ime ns iona l T 1-weighted 3.0-T m.agneuc resonance 1maging, and results wer e correlatedwith clinical mttrics. Pearson and Spearman rank corre ation coefficientswere computed between longitud naJ brain volume and neurocognitivescores, as wel l as chnlcal metrics. over the course of the follow- up per od.
Results: One year after MTBI, the1e was measurab e global brain atrophy, larger than that In control subjects. The anterior cingu ate WM b ilaterally andthe left cingulate gyrus lsthrrus WM, as well as the right precuneal GM,showed significant decreases in regionaJ volume in patients with MTBIover the 1st year after ll'ljury (conected P< .05); this was confirm ed bymeans of cross-sectional compat son with data in control subjects(corrected P< .05). le ft and right rostral anterior cingulum WM volum eloss correlated with changes in neurocognitive m easures of m emory ( r =0.65, P • .005) and attention ( r • 0.60, Pc .01). At 1-year follow-u p, WMvolume in the left clngulate gyrus isthmus correlated with c linical scores of anxiety (S p urman rank correlation r• - 0 .68, P= .007) andpostconcussive symptoms (Spearman rank correlation r = - 0.65, P = .01).
Conclusion: These observations demonstrate structural changes to thebrain 1 year after Injury after a single concussive ep sode. Regional brainatrophy is not exclusive to moderate and severe traumatic brain injury butmay be seen after mdd injury . In panicular, the anterior pan of thecingulum and the cingulate gyrus isthmus, as well as the precuneal GM, may be distinctively vulnerable 1'(tar after MTSI.
Longitudinal Changes in BrainVolume Following TBI
• Longitudinal, segmentation analysis of TBIpatients (one concussion)
• Post hoc analysis @ 1 year
• Atrophy of cingulate gyrus, ishmus ofcingulate gyrus and pre-cuneus
• Correlation with neuro-cognitive, behavioral & visual-motor abnormalities
Zhou Y, et al. Radiology 2013
Concussion Signs and Symptoms
(May be Delayed Minutes to Days)
• Physical: headache, dizziness,vision changes
• Cognitive: memory impairment,concentration
• Emotional: irritability, sadness
• Sleep disorder
2/11/2014
12
Complications of Concussion
• Second-impact syndrome (SIS)
• Postconcussion syndrome (PCS)
• Chronic traumatic encephalopathy (CTE)
Second-Impact Syndrome
• Sustaining a second concussion before“recovery” from first concussion
• Majority in pediatric/adolescent populations (< 20 yrs.)
• Enhancement of cerebrovascularcongestion (?)– Diffuse cerebral edema
– Death (within minutes to days!)
Cantu RC, et al. Phys Sportsmed 1995
Montclair High School football player RyneDougherty died on Oct. 15, 2008, two days after collapsing in a junior varsity game against DonBosco Prep.The family of a Montclair High School footballplayer who died two days after collapsing in a2008 junior varsity game agreed Monday to settleits lawsuit against the school and the township’s Board of Education for $2.8 million, the family’slawyer said.
Nj.com September 9, 2013
Postconcussion Syndrome
• 3 months duration of three or more offollowing:– Fatigue– Disordered sleep– Irritability / aggressiveness– Anxiety / depression– Personality changes / apathy– Impaired attention / memory– Impaired eye tracking
Diagnostic and Statistical Manual of Mental Disorders. Fourth EditionHeitger MH et al. Brain 2009
Crosby progressing slowly; return not setTuesday, January 25, 2011
By Dave Molinari, Pittsburgh Post-Gazette
Vs. Capitals January 1, 2011
Vs. Lightning January 6, 2011
Chronic Traumatic Encephalopathy(CTE)
• Historical evidence of progressive neurologicdisability in boxers:– “punch drunk” (Martland 1928)– “dementia pugilistica” (Millspaugh 1937)
• Signs & symptoms:– Memory disturbance, confusion,
behavioral/personality changes, Parkinsonism and speech/gait abnormalities
• Average age of diagnosis = 43 yrs.• Average age of death = 54 yrs.
Roberts GW, et al. J Neurol Neurosurg and Psych 1990
2/11/2014
13
Neuropathology of CTE
• Atrophy of cerebral hemispheres, temporallobe, mammillary bodies & brainstem
• Ventricular dilatation
• Fenestration of septum pelucium
• Marked accumulation of tau-immunoreactive astrocytes
McKee AC, et al. J Neuropathol Exp Neurol 2009
Mlcrotubutes
Microtubule SubunilsFall Apart
Disintegrating
Microt u bTangledClumpsol TauProteins
DisintegratingMlcrotubules
McKee AC, et al. J Neuropathol Exp Neurol 2009
100
Dave Duerson
Mr. Duerson’s Clinical History
• Long-standing complaints of headaches since NFL and onward.
• Over the ~5 years prior to death, he had worsening short-term memory difficulties, as well as problems with language and “vision”
• Increasingly out of control:– Short fuse– Hot tempered– Physically abusive– Verbally abusive
, j
(,.
' l •
Dave Duerson
Department ofVeterans Affairs '
\ ,s p o r t s l e g a c y
I N S T I T U T E
/
2/11/2014
14
\ r r
,Dave Duerson
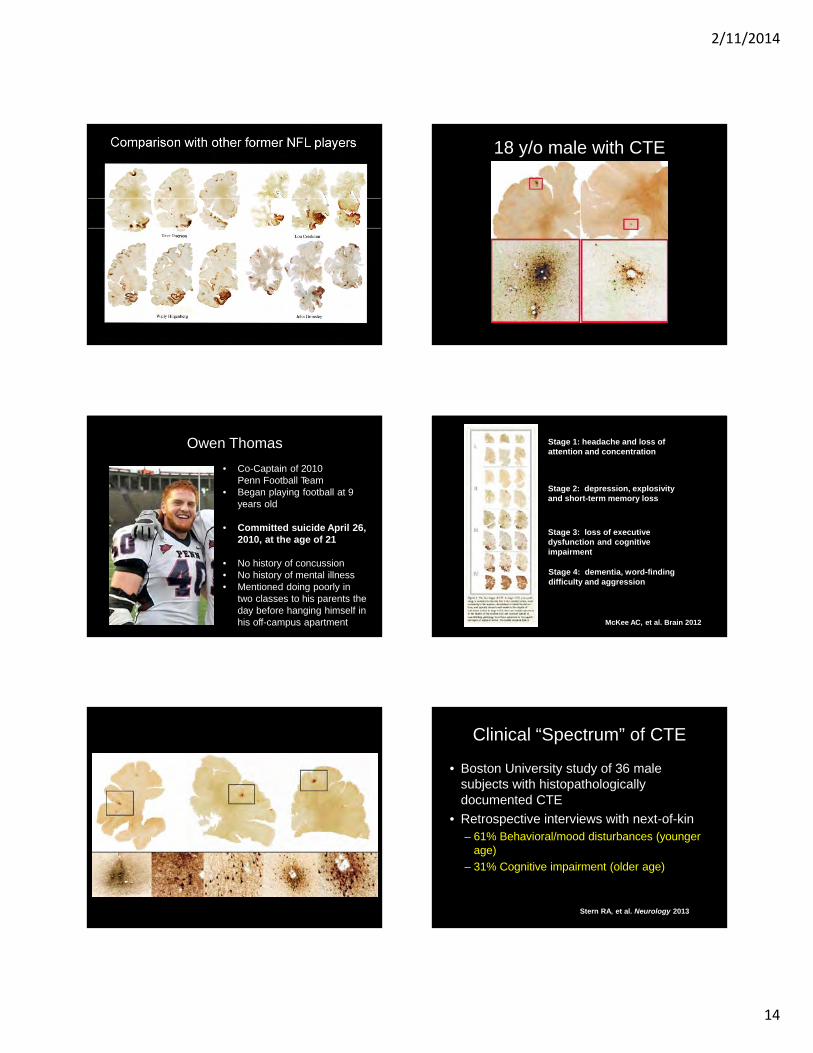
• Co-Captain of 2010Penn Football Team
• Began playing football at 9years old
• Committed suicide April 26, 2010, at the age of 21
• No history of concussion• No history of mental illness• Mentioned doing poorly in
two classes to his parents the day before hanging himself in his off-campus apartment
Owen Thomas
18 y/o male with CTE
Stage 1: headache and loss of attention and concentration
Stage 2: depression, explosivity and short-term memory loss
Stage 3: loss of executivedysfunction and cognitiveimpairment
Stage 4: dementia, word-finding difficulty and aggression
McKee AC, et al. Brain 2012
Clinical “Spectrum” of CTE
• Boston University study of 36 male subjects with histopathologically documented CTE
• Retrospective interviews with next-of-kin– 61% Behavioral/mood disturbances (younger
age)
– 31% Cognitive impairment (older age)
Stern RA, et al. Neurology 2013
2/11/2014
15
CTE is a disease of progressive neurologic & psychologic dysfunction
with increasing CNS deposition of tau related torepetitive head blows over
time.
CTE Masquerades
• Alzheimer disease
• Progressive supranuclear palsy
• Parkinsonism
• Amyotrophic lateral sclerosis (Lou Gehrig’s Disease)
JNeuropatholExpNeurolCopyright©2010bytheAmerican Association ofNeuropatholosts, Inc.
Vol.69,No.9September2010
pp.918929
ORIGINALARTICLE
TDP-43Proteinopathy andMotorNeuronDiseaseinChronicTraumatic Encephalopathy
AnnC. McKee MD,BrandonE.Gavett,PhD,RobertA.Stem,PhD,ChristopherJ.Nowinski,AB, RobertC.Cantu,MD,NeilW.Kowall, MD,Daniel P. Perl,MD E.TessaHedley-Whyte, MD,BrucePrice, MD,ChrisSullivan,PeterMorin MD,PhD Hyo-SoonLee MD,CarolineA.Kubilus
DanielH.Daneshvar,MA MeganWulff MPH andAndrewE.Budson MD
The Search for SurrogateBiomarkers
• PET scans of retired NFL players reveals FDDNP signals in areas of histopathologic documentation of Tau (Small GW, et al. Am J Geriatr Psychiatry 2013)
• OCT abnormalities in veterans with TBI vs. age-matched controls (Kardon R, et al. ARVO 2013)
The Search for SurrogateBiomarkers (cont.)
• Retinal deposition of hyperphosphorylated tau (McKee A. personal communication 2012)
• Potential for OCT and other visual tests as surrogate biomarkers of CTE
2/11/2014
16
Why Do We Need a Rapid SidelineTest for Concussion?
• Detecting early signs of concussion mayimprove outcomes in athletes with mild closed head trauma
• Possible devastating long-term disability
• Following a concussion, you are 3 times morelikely to have another one
• Need an easy objective test since qualifiedpersonnel not always available
Am J Sports Med 2000;28:643-650
New Rapid Sideline Tests
What is the Evidence?
• Management is largely guided by expertopinion or retrospective data
• Levels of evidence in medicine: 5 levels– Highest: prospective study, established
criteria
– Lowest: expert opinion
• Formal research testing is the only way to get evidence that a test works!
Levels of Evidence
•
Expert Opinion and Clinical Observation
are the LOWEST forms of evidence •
Concussion Tests: 2 Types
• Testing for diagnosis: King-Devick (K-D) test, Standardized Assessment of Concussion (SAC),SCAT3, MACE
• Testing for management: ImPACT, other computerized testing
Initial Assessment: SCAT3
2/11/2014
17
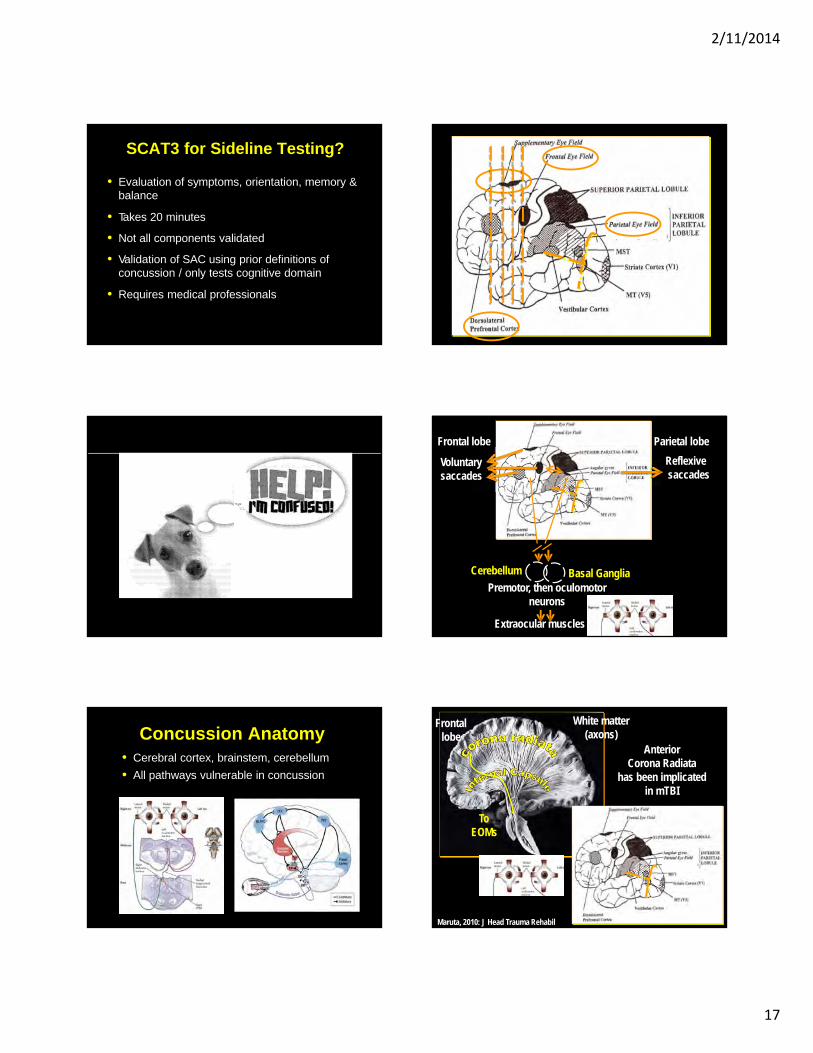
SCAT3 for Sideline Testing?
• Evaluation of symptoms, orientation, memory &balance
• Takes 20 minutes
• Not all components validated
• Validation of SAC using prior definitions ofconcussion / only tests cognitive domain
• Requires medical professionals
"""" \},'"*'""'\iT""'\i"
""""""\ "
Concussion Anatomy• Cerebral cortex, brainstem, cerebellum
• All pathways vulnerable in concussion
Parietal lobe
Reflexivesaccades
Frontal lobe
Voluntary saccades
Premotor, then oculomotorneurons
Extraocular muscles
Cerebellum Basal Ganglia
White matter (axons)
Frontallobe
AnteriorCorona Radiata
has been implicatedin mTBI
Maruta, 2010: J Head Trauma Rehabil
ToEOMs
2/11/2014
18
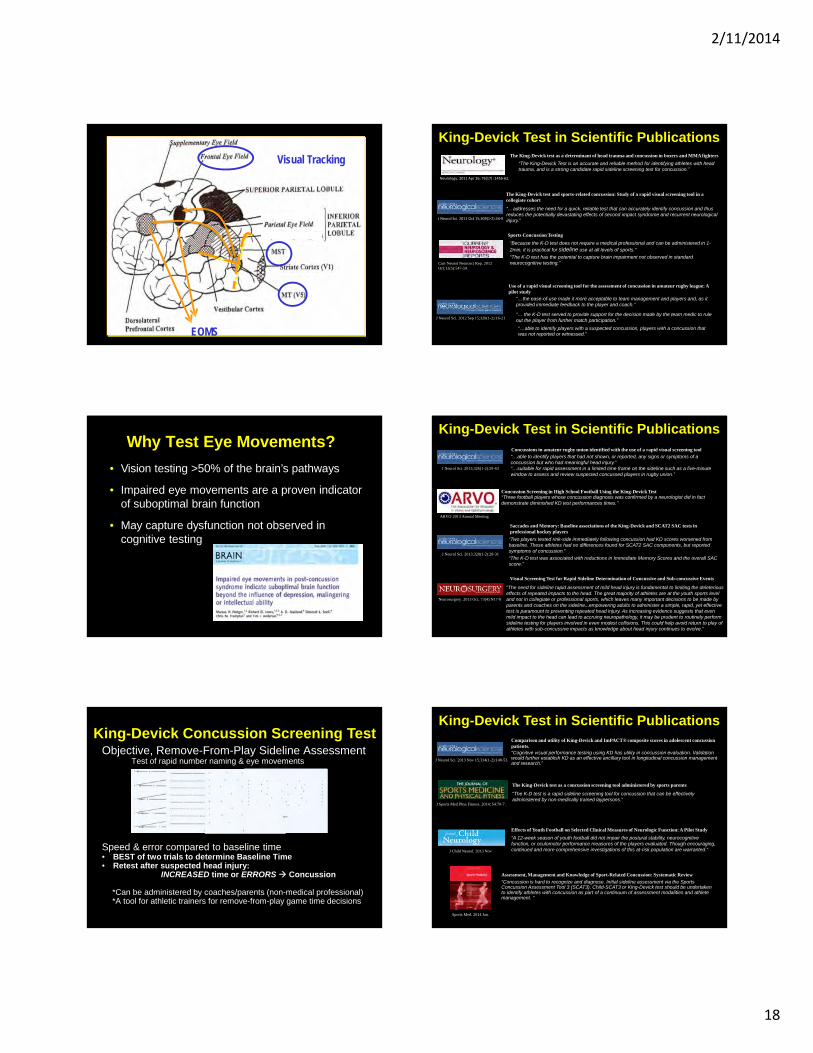
Visual Tracking
EOMS
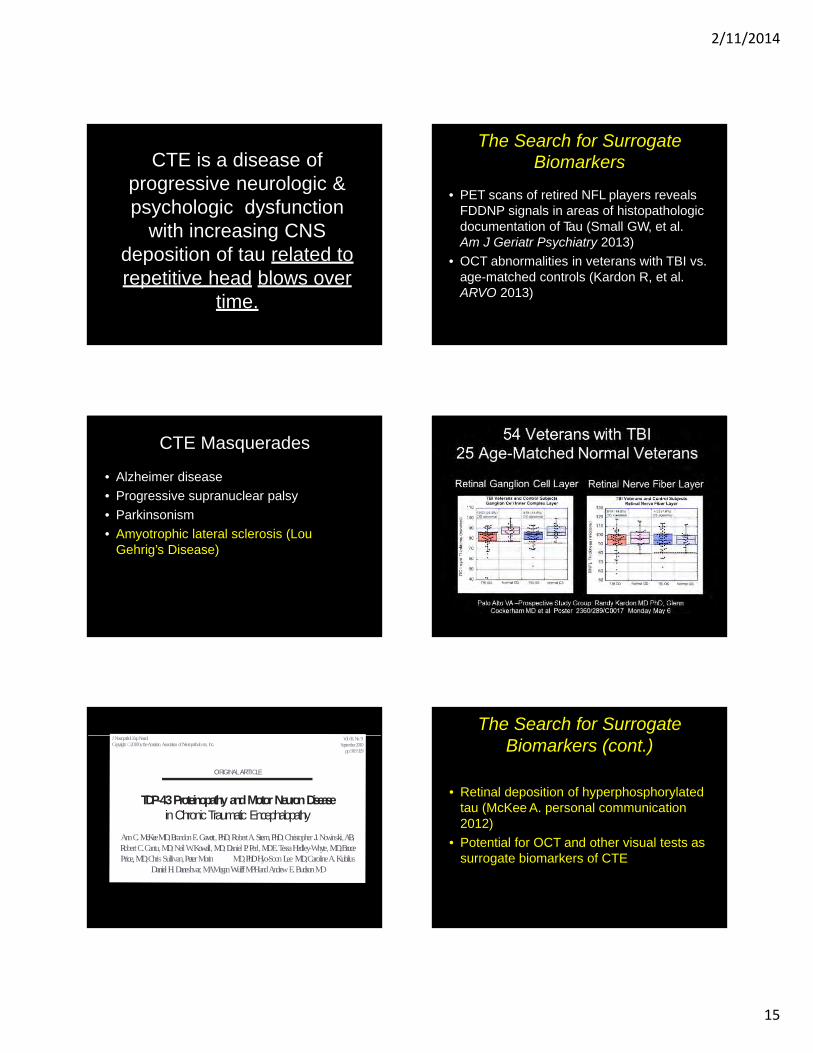
Why Test Eye Movements?
• Vision testing >50% of the brain’s pathways
• Impaired eye movements are a proven indicator of suboptimal brain function
• May capture dysfunction not observed in cognitive testing
Objective, Remove-From-Play Sideline AssessmentTest of rapid number naming & eye movements
Speed & error compared to baseline time• BEST of two trials to determine Baseline Time• Retest after suspected head injury:
INCREASED time or ERRORS Concussion
*Can be administered by coaches/parents (non-medical professional)*A tool for athletic trainers for remove-from-play game time decisions
King-Devick Concussion Screening Test
King-Devick Test in Scientific PublicationsThe King-Devick test as a determinant of head trauma and concussion in boxers and MMA fighters
“The King-Devick Test is an accurate and reliable method for identifying athletes with head trauma, and is a strong candidate rapid sideline screening test for concussion.”
The King-Devick test and sports-related concussion: Study of a rapid visual screening tool in a collegiate cohort
“…addresses the need for a quick, reliable test that can accurately identify concussion and thus reduces the potentially devastating effects of second impact syndrome and recurrent neurological injury.”
“Because the K-D test does not require a medical professional and can be administered in 1-2min, it is practical for sideline use at all levels of sports.”
“The K-D test has the potential to capture brain impairment not observed in standard neurocognitive testing.”
Sports Concussion Testing
“…able to identify players with a suspected concussion, players with a concussion that was not reported or witnessed.”
Use of a rapid visual screening tool for the assessment of concussion in amateur rugby league: A pilot study
“…the ease-of-use made it more acceptable to team management and players and, as it provided immediate feedback to the player and coach.”
“… the K-D test served to provide support for the decision made by the team medic to rule out the player from further match participation.”
Neurology. 2011 Apr 26; 76(17) :1456‐62.
J Neurol Sci. 2011 Oct 15;309(1‐2):34‐9
Curr Neurol Neurosci Rep. 2012 Oct;12(5):547-59.
J Neurol Sci. 2012 Sep 15;320(1-2):16-21
Concussions in amateur rugby union identified with the use of a rapid visual screening tool
“…able to identify players that had not shown, or reported, any signs or symptoms of a concussion but who had meaningful head injury.”“…suitable for rapid assessment in a limited time frame on the sideline such as a five-minute window to assess and review suspected concussed players in rugby union.”
Concussion Screening in High School Football Using the King-Devick Test“Three football players whose concussion diagnosis was confirmed by a neurologist did in fact demonstrate diminished KD test performances times.”
Saccades and Memory: Baseline associations of the King-Devick and SCAT2 SAC tests in professional hockey players
“Two players tested rink-side immediately following concussion had KD scores worsened from baseline. These athletes had no differences found for SCAT2 SAC components, but reported symptoms of concussion.”
“The K-D test was associated with reductions in Immediate Memory Scores and the overall SAC score.”
Visual Screening Test for Rapid Sideline Determination of Concussive and Sub-concussive Events
“The need for sideline rapid assessment of mild head injury is fundamental to limiting the deleterious effects of repeated impacts to the head. The great majority of athletes are at the youth sports level and not in collegiate or professional sports, which leaves many important decisions to be made by parents and coaches on the sideline...empowering adults to administer a simple, rapid, yet effective test is paramount to preventing repeated head injury. As increasing evidence suggests that even mild impact to the head can lead to accruing neuropathology, it may be prudent to routinely perform sideline testing for players involved in even modest collisions. This could help avoid return to play of athletes with sub-concussive impacts as knowledge about head injury continues to evolve.”
Neurosurgery. 2013 Oct; 73(4):N17-8
J Neurol Sci. 2013;328(1-2):28-31
ARVO 2013 Annual Meeting
J Neurol Sci. 2013;326(1-2):59-63
King-Devick Test in Scientific Publications
The King-Devick test as a concussion screening tool administered by sports parents
“The K-D test is a rapid sideline screening tool for concussion that can be effectively administered by non-medically trained laypersons.”
Effects of Youth Football on Selected Clinical Measures of Neurologic Function: A Pilot Study
“A 12-week season of youth football did not impair the postural stability, neurocognitivefunction, or oculomotor performance measures of the players evaluated. Though encouraging, continued and more comprehensive investigations of this at-risk population are warranted.”
Assessment, Management and Knowledge of Sport-Related Concussion: Systematic Review
“Concussion is hard to recognize and diagnose. Initial sideline assessment via the Sports Concussion Assessment Tool 3 (SCAT3), Child-SCAT3 or King-Devick test should be undertaken to identify athletes with concussion as part of a continuum of assessment modalities and athlete management. “
Comparison and utility of King-Devick and ImPACT® composite scores in adolescent concussion patients.“Cognitive visual performance testing using KD has utility in concussion evaluation. Validation would further establish KD as an effective ancillary tool in longitudinal concussion management and research.”
J Neurol Sci. 2013 Nov 15;334(1-2):148-53.
J Sports Med Phys Fitness. 2014; 54:70-7.
J Child Neurol. 2013 Nov
Sports Med. 2014 Jan.
King-Devick Test in Scientific Publications

2/11/2014
19
Sports-Related Concussions in Youth: Improving the Science, Changing the Culture.
“The King-Devick Test… such tools as well as balance tests may be used either by trained responders as part of an acute sideline or in-field assessment or by health care providers during subsequent clinical evaluation”
In the Clinic: Concussion
"For the oculomotor examination, an additional test that may be used is the King–Devick test, which is a tool that rapidly assesses eye movement and can be used in the office or on the sideline to determine impairment in eye movements associated with an acute concussion. This has been found to be potentially useful as a tool to determine removal from play. The 1-minute test involves reading single digits displayed on cards; any slowing of time to complete the test, ideally compared with the athlete’s baseline, is suggestive of concussion."
Consensus Statement on Concussion in Sport: the 4th International Conference on Concussion in Sport held in Zurich, November 2012.
“How can the SCAT2 be improved? Future research should consider the efficacy for inclusion of vision tests such as the King Devick Test and clinical reaction time tests. Recent studies suggest that these may be useful additions to the sideline assessment of concussion.
British J Sports Med. 2013, 47:250-258.
Institute of Medicine (US), National Research Council (US). Washington (DC): National Academies Press (US); 2013
Ann Intern Med. 2014 Feb; 160(3):ITC2-1-1.
King-Devick Test in Scientific Publications
According to the Research• High test retest reliability
(ICC =0.97)
• Can screen for witnessed and un-witnessed/un-reported concussions
• Quick, objective sideline test
• Can be administer by non-medical professionals
• Shown to be robust to fatigue
• Known learning effect
• Able to detect visual and cognitive function in:
Hypoxia, Parkinson’s Disease, Multiple Sclerosis, Extreme Sleep Deprivation and Learning Disability
Source: Galetta, K et al. Neurology 2011; J Neuro Sci 2011-13; Curr Neurol Neurosci 2012
K-D Test For Witnessed and Un-Witnessed, Un-Reported Concussion
Amateur Rugby League New ZealandPilot Study:Participants: 50 athletes over 12 matchesConcussions: 5
3 witnessed/self reported2 un-witnessed/un-reported(detected on post-game assessment with King-Devick test)
• Follow-up Study:Participants: 37 athletes over 24 matches Concussions: 22
5 witnessed/self reported17 un-witnessed/un-reported
(detected on post-game assessment with King-Devick test)
Source: King, D et al. J Neurol Sci. 2012; King D et al., J Neurol Sci. 2013
A Rapid Sideline Test
Professional Ice Hockey: Philadelphia Flyers
• 27 athletes, 2011-2012 pre-season
• Worse KD scores associated with:– Lower SCAT2 SAC Memory score – Lower overall SAC score
For every 1 point reduction in SAC Immediate Memory Score, corresponding worsening of KD by 7.3s
• 2 concussed athletes exhibited:– Abnormal K-D test– Normal SCAT2 SAC test– Increased Symptoms
Working memory and saccades share closely related anatomical structures, including the dorsolateral prefrontal cortex (DLPFC)
A composite of brief rapid sideline tests, including SAC and K-D (and balance testing for non-ice hockey sports), is likely to provide an effective clinical tool to assess the athlete with suspected concussion
Source: Galetta MS, et al. J Neurol Sci 2013
Concussion Sideline Assessment:Composite Measure?
• Standardized Assessment of Concussion (SAC)
• Balance Error Scoring System (BESS)
• King-Devick Test
CollegiateFootball, Soccer & Lacrosse
Prospective longitudinal study of sideline concussion screening
• 52% of concussions identified using SAC (> 2pt worsening)• 79% of concussions identified using KD• 89% of concussions identified combining: KD & SAC• 100% of concussions screened using a composite of
sideline tests: KD test, SAC, BESS
Marinides Z et al. Neurology Clinical Practice 2014, In Press

2/11/2014
20
• Cohort of amateur boxers
• Laypersons administered pre-fight and post-fight K-D Test
• Masked to head trauma status
• Matches watched by ringside physician and boxing trainer
• Athletes with suspected head trauma received MACE administered by ringside physician
• Athletes with concussion compared to athletes screened using K-D Test
• Masked layperson K-D Testers accurately identified concussed athlete due to worsening in K-D Test compared to baseline
(3.2 seconds + increased errors)
• 6 boxers in multiple bouts showed no worsening of K-D times
• Scores were not affected by fatigue
Layperson Test Administrators
Source: J Sports Med Phys Fitness 2013.
Examining Effects of Concussion & Exercise on KD test performanceFootball, Basketball, Soccer, Rugby, Boxing
K-D scores worse after concussionK-D scores not worse after exercise
Fatigue Trials
Source: J Neurol Sci 2011; 2013.
p=0.009 vs. baselinefollowing concussion
3040
5060
70
Baseline K-D (sec) Sideline K-D (sec)
n = 10 n = 10
p=0.0003 vs. baselinefollowing exercise
3040
5060
70
Baseline (sec) Post-scrimmage (sec)
n = 18 n = 18
Consensus statement on concussion in sport: the 4th International Conference on Concussion in Sport held in
Zurich, November 2012
How can the SCAT2* be improved?(Sport Concussion Assessment Tool)
Future research should consider the efficacy for inclusion of vision tests such as the King Devick Test and clinical reaction time tests. Recent studies suggest
that these may be useful additions to the sideline assessment of concussion.
Source:Br J Sports Med 2013;47:250-258 doi:10.1136/bjsports-2013-092313 *Now SCAT3
When is it acceptable for an athlete to return to play
following a concussion?
Graduated Return to Play Protocol
AAN Clinical Practice Reference Sheet for Clinicians, 2011.
Rehabilitation Stage Functional Exercise at Each Stage of Rehabilitation
(1) No activity Complete physical, cognitive rest
(2) Light aerobic exercise Walking, swimming, stationary bike
(3) Sport-specific exercise Running drills in soccer, skating drills in hockey, etc.
(4) Noncontact drills More complex training drills, may start resistance training
(5) Full-contact practice With medical clearance, participate in normal training activities
(6) Return to play Normal game play
Future Research:Visual Structure & Functional Abnormalities
with Contact Sports Athletes (VICTORS)
• Study sites:
– Illinois Eye Institute @ Illinois College ofOptometry
– NYU Langone Medical Center @ NYUSchool of Medicine
– Center for the Study of TraumaticEncephalopathy @ BU School of Medicine
2/11/2014
21
• Cross sectional & longitudinal analysis of ocular structure and functional findings among retired NFL players as compared to age-matched norms
• Testing protocol:– SD-OCT (RNFL & GCC)
– Low contrast acuity
– King Devick
VICTORS study (cont.)
Questions to be Answered
• What are the best tests to diagnose andmanage concussions?
• Can we use ocular morphology and visual-motor testing as surrogate biomarkers for CTE?
• In what ways can we lead the effort toreduce effects of concussion?
There’s No Such Thing as aTough Brain
NFL Hall of Fame-Class of 1997Mike Haynes, far left
King-Devick Test RepresentativeMike Webster (1952-2002), far rightSuffered From Dementia, Amnesia and Depression






![Bryan Concussion General Audience - 2015.pptx [Read-Only] · 2015-09-03 · CONCUSSION ‐16,400,000 MTBI and Post‐Concussion Syndrome ‐ 141,000 Concussion Management ‐1,550,000](https://img.pdfslide.net/doc/110x75/5fb548e39d237d0cb0684f4f/bryan-concussion-general-audience-2015pptx-read-only-2015-09-03-concussion.jpg)