Embed Size (px)
Citation preview
Online Data Supplement 1
ONLINE SUPPLEMENTARY MATERIAL
The PROactive instruments to measure physical activity in
patients with COPD
Elena Gimeno-Santos, Yogini Raste, Heleen Demeyer, Zafeiris Louvaris,
Corina de Jong, Roberto A Rabinovich, Nicholas S Hopkinson, Michael I
Polkey, Ioannis Vogiatzis, Maggie Tabberer, Fabienne Dobbels, Nathalie
Ivanoff, Willem I de Boer, Thys van der Molen, Karoly Kulich, Ignasi Serra,
Xavier Basagaña, Thierry Troosters, Milo A Puhan, Niklas Karlsson, Judith
Garcia-Aymerich on behalf of PROactive consortium
Methods – complete version ............................................................................... 4
List of proposed items for day-to-day (Daily) assessment ................................ 19
List of proposed items for Clinic visit assessment ............................................ 22
Table E1. Baseline demographic and clinical characteristics of COPD patients
stratified by sites ............................................................................................... 25
Table E2. Description of activity monitor data, stratified by visit and by site ..... 29
Table E3. Performance of all items from Daily version of PROactive Physical
Activity in COPD (D-PPAC) instrument and Dynaport prior to item reduction .. 31
Table E4. Performance of all items from Clinical visit version of PROactive
Physical Activity in COPD (C-PPAC) instrument and Dynaport prior to item
reduction........................................................................................................... 32
Online Data Supplement 2
Table E5. Reason for removing items that flagged in at least one predefined
criteria .............................................................................................................. 33
Table E6. Confirmatory factor analysis results of Daily and Clinical visit versions
of PROactive Physical Activity in COPD instruments (D-PPAC and C-PPAC,
respectively) ..................................................................................................... 52
Table E7. Performance of items from factor 1 (‘amount’) without variables from
the activity monitors ............................................. Error! Bookmark not defined.
Table E8. Scores for Daily and Clinical visit versions of PROactive Physical
Activity in COPD instruments (D-PPAC and C-PPAC, respectively), stratified by
gender and severity .......................................................................................... 55
Table E9. Daily and Clinical visit versions of PROactive Physical Activity in
COPD scores (D-PPAC and C-PPAC, respectively) according to dyspnea
groups, exacerbation status at baseline, and physical activity levels (known-
groups validity) ................................................................................................. 56
Table E10. Correlation of Daily and Clinical visit versions of PROactive Physical
Activity in COPD instruments (D-PPAC and C-PPAC, respectively) with height,
socioeconomic status and heart rate (discriminant validity) ............................. 58
Figure E1. Person-item maps and overall fit of the model for factor 1 (‘amount’)
of Daily and Clinical visit PROactive PROs (without variables from activity
monitors) ............................................................. Error! Bookmark not defined.
Figure E2. Bland-Altman test-retest reliability of Daily PROactive Physical
Activity in COPD (D-PPAC) instrument – daily values ...................................... 61
Figure E3. Bland-Altman test-retest reliability of Clinical visit version of
PROactive Physical Pctivity in COPD (C-PPAC) instrument ............................ 66

Online Data Supplement 3
Final version of the Daily of PROactive Physical Activity in COPD (D-PPAC)
instrument......................................................................................................... 67
Final version of the Clinical visit of PROactive Physical Activity in COPD (C-
PPAC) instrument ............................................................................................. 69
References ....................................................................................................... 72
Online Data Supplement 4
Methods – complete version
Study Design, Sample, and Procedures
The current study was a six-week, randomized, two-way cross-over, multi-centre
study (Figure 1). Study was conducted in five European medical centers, covering
tertiary hospitals, rehabilitation centers and primary care settings in Athens (Greece),
Edinburgh and London (UK), Leuven (Belgium), and Groningen (The Netherlands).
We recruited both stable and exacerbated patients with COPD defined by spirometry,
to cover the whole range of physical activity.
Inclusion criteria were as follows: (i) men or women at least 40 years of age, (ii) with
medical diagnosis of COPD (post bronchodilator FEV1 less than 80% and FEV1/FVC
less than 70%) confirmed by spirometry, (iii) smoking history equivalent to at least 10
pack years, (iv) able to read and write and to use electronic devices and physical
activity monitors, and (v) for the patients into stable group, COPD was defined stable
if the patient had not used systemic antibiotics nor systemic corticosteroids nor had
been hospitalized due to COPD in the previous 4 weeks; for the patients into
exacerbated group, COPD exacerbation was defined as admitted into emergency
room or hospitalized under the care of a pneumologist (irrespective of the ward).
Exclusion criteria were: (i) orthopaedic, neurological or other complaints that
significantly impair normal biomechanical movement patterns, (ii) respiratory
diseases other than COPD (e.g. asthma), (iii) COPD exacerbation within 4 weeks
prior to Visit 1 (only applicable for patients in the stable group), (iv) cognitive
impairment, (v) involvement in the planning and/or conduct of the study, and (vi)
previous randomization in the present study.
Online Data Supplement 5
Patients that fulfilled the inclusion criteria were randomized into one of the two arms
using statistical software in varying blocks of 4, 6 or 8, and separately by site and by
status (stable/exacerbated). In arm 1 (Figure 1), patients followed a sequence of a
baseline assessment (visit 1), a 14 days period during which they completed the
Daily PROactive item pool and wore the physical activity monitor devices, followed by
a second visit (visit 2) where they returned the electronic devices. After a 14-day
wash-out period, patients underwent a third visit (visit 3) in which they completed the
Clinical visit PROactive item pool, prior to start a new 14 days period during which
they wore the physical activity monitors, and then came back for visit 4, when they
again completed the Clinical visit PROactive item pool and returned the physical
activity monitors. Patients in arm 2 followed the sequence in reverse order (Figure 1).
The study was performed in accordance with ethical principles that have their origin
in the Declaration of Helsinki and are consistent with Good Clinical Practice and
applicable regulatory requirements. The study was advised and approved by the
PROactive ethics and patient advisory boards and approved by the Ethics Committee
at each center. Written consent was obtained from all patients. The study was
registered at www.clinicaltrials.gov (NCT01388218).
The PROactive project (www.proactivecopd.com) was funded through the Innovative
Medicines Initiative (IMI) supported by the European Commission and the European
Federation of Pharmaceutical Industry and Associations.
Assessments and measures
Figure 1 shows the assessments and timing for the study.
Physical activity measures. Physical activity experience was assessed using the
PROactive item pools that were self-administrated using a LogPad® (PHT
Online Data Supplement 6
Corporation, Geneva, Switzerland) handheld electronic patient-reported outcome
(PRO) device (ePRO). All the items for the PROactive PROs were previously
developed according to current European Medicines Agency (EMA) (E1) and US
Food and Drug Administration (FDA) standards (E2) in order to support claims for the
use of pharmacotherapy related to changes in domains of physical activity relevant to
patients. Their development published elsewhere (E3) was based on input from the
literature, from experts, and from patients through qualitative research using one-to-
one interviews, focus groups and cognitive debriefing interviews to measure physical
activity from the patients’ perspective on a daily basis (Daily PROactive PRO), and
during clinic visits (Clinical visit PROactive PRO). All items were linguistically adapted
or each site (E3). The Daily PROactive PRO asked patients to report their physical
activity experiences during a day. It consisted of 30 questions, where the majority of
questions were responded to on a five- or six- point Likert scale. A few questions
were dichotomous with “yes” or “no” response. It was to be completed by the patient
every evening at home between visit 1 and visit 2 for patients in arm 1, and between
visit 3 and visit 4 for patients in arm 2. The Clinical visit PROactive PRO asked
patients to report their physical activity experiences in the past 7 days. It consisted of
35 questions, where all except two dichotomous questions were responded to on a
five- or six- point Likert scale. It was to be completed by the patient at visit 1 and visit
2 for patients in arm 2, and at visit 3 and visit 4 for patients in arm 1.
Moreover, two accelerometers previously identified during a systematic review [E4]
and further validated for COPD patients against the doubly labelled water (DLW)
method [E5] and the indirect calirometry [E6] (Actigraph G3Tx, Actigraph, Pensacola,
FL, United States; and Dynaport MoveMonitor, McRoberts BV, The Hague, The
Netherlands) were used to measure the direct physical activity levels of the patient.
Online Data Supplement 7
Patients were instructed to wear both monitors at same time, at least 10 hours per
day, during 14 days from visit 1 to visit 2, and from visit 3 to visit 4 (Figure 1). From
Actigraph, we obtained the following variables: wearing time, steps per day, vector
magnitude units (VMU) daily average, and time in moderate-to-vigorous physical
activity per day. From Dynaport, the following variables were obtained: wearing time,
steps per day, time in locomotion per day, standing time per day, VMU daily average,
and intensity.
Other assessments. At baseline (visit 1), patients were evaluated for body
composition by bioelectrical impedance analysis (BIA); lung function testing by
spirometry and reversibility test and body plethysmography; gas transfer (TLCO);
pulse oxymetry (SpO2); exercise tolerance by six-minute walking test (6MWT); and
skeletal muscle function by quadriceps maximal voluntary contraction (QMVC). For
exacerbated patients group, lung function testing and 6MWT were performed at visit
4. We also recorded at baseline demographics, smoking, and patient characteristics
(including baseline exacerbation characteristics for those patients included in
exacerbated group). Clinical data (medical, surgical, COPD and COPD exacerbation
histories, and concomitant treatments) were obtained from medical records.
Socioeconomic status was defined, from questions on occupation and employment
characteristics, according to the National Statistics Socio-economic Classification
(NS-SEC) in five classes version (I Professional occupations, II Managerial and
technical occupations, III Skilled occupations (non-manual and manual), IV Partly
skilled occupations, V Unskilled occupations) (E7). Emotional status using Hospital
Anxiety and Depression Scale (HADS) (E8) was also assessed, only at baseline,
using the PHT LogPad® System. Finally, dyspnea using the modified Medical
Research Council Dyspnea scale (mMRC), and a health related quality of life
Online Data Supplement 8
package containing Chronic Respiratory Disease Questionnaire (CRQ) (E9), Clinical
COPD Questionnaire (CCQ) (E10) and COPD Assessment Test (CAT) (E11) were
assessed at all visits using the PHT LogPad® System (Figure 1). All questionnaires
were on linguistic adaptation for each site.
Safety issues. Since the study did not involve a study drug, only Serious Adverse
Events (SAE) and Discontinuation due to Adverse Events (DAE) were collected.
Statistical Analysis
Analysis Sets
The analyses sets were defined based primarily on the data of the Daily and Clinical
visit PROactive PROs, as follows:
- Full Analysis Set (FAS) was defined as the set of patients who fulfilled the
following: (i) had answered at least one question from at least one day of the
Daily PROactive PRO, or (ii) had answered at least one question from at least
one administration of the Clinical visit PROactive PRO.
- The Item Reduction Analysis Set for the Daily PROactive PRO (IRAS-D) was
defined as the subset of FAS patients who had completed all items for at least 3
(not necessarily consecutive) days during their first week of filling in the Daily
PROactive PRO. Data from all available days for each subject (maximum of 14
days for patient) were used in the analyses. The Item Reduction Analysis Set for
the Clinical visit PROactive PRO (IRAS-C) was defined as the subset of FAS
patients who had completed all the items for their first administration of the
Clinical visit PROactive PRO. Data from the two Clinical visit PRO for each
subject were used in the analyses.

Online Data Supplement 9
- The Test-Retest Analysis Set for the Daily PROactive PRO (TRAS-D) was
defined as the subset of FAS patients who had (i) answered at least one question
(and the same question) on at least 3 days (not necessarily consecutive) from
each week of filling in the Daily PROactive PRO, (ii) their daily activity had not
altered significantly between the 2 weeks, and (iii) had not suffered an
exacerbation between the 2 weeks. The Test-Retest Analysis Set for the Clinical
visit PROactive PRO (TRAS-C) was defined as the subset of FAS patients who
had (i) answered at least one question (and the same question) from both
administrations of the Clinical visit PROactive PRO, (ii) their daily activity had not
altered significantly between the 2 weeks, and (iii) had not suffered an
exacerbation between the 2 weeks.
- Construct Validity Analysis Sets (CVAS-D and CVAS-C) was defined as the
subset of IRAS-D and IRAS-C, respectively, which had data on at least one of the
following variables: FEV1, 6-min walking distance, dyspnea, quadriceps strength,
CRQ, CAT, or CCQ scores.
Sample size calculations
The sample size for this study was based on the test-retest validation analysis of the
Clinical visit PROactive PRO using the method described in Flack et al 1988 (E12).
Sample size calculations were performed to detect that the Cohen’s κ between two
separate administrations of the question was significantly greater than 0.4 with a
precision of 0.2 at the 5% level. Assuming a five-item question with item probabilities
of 0.07, 0.08, 0.10, 0.15 and 0.6, the required sample size was 166. For
convenience, this was rounded to 170 patients. Because the test-retest analysis was
to be performed using the TRAS-C, a subset of patients expected to be around 85%
of the total number of patients, we calculated the number of patients to be 200 (200 =
Online Data Supplement 10
170 + (15% of 200)). Furthermore, an additional percentage of patients was expected
from the exacerbated group who, by definition, would not be eligible for the test-retest
analysis (because their physical activity can change during the study) and who at
baseline would have virtually no physical activity at all. Data from the literature
suggests that at about 20% of COPD patients are completely inactive (E13), so the
figure of 200 was upgraded to 250 patients (250 = 200 + (20% of 250)). Finally, this
sample size was increased by approximately 10% to allow for attrition. Therefore the
final sample size was set at 280 patients.
This figure also fit well with requirements of sample size for factor analysis (one of
the main analysis to be performed), where N:p ratios above 5, being N was the
number of patients and p the number of items, were considered adequate (E14–
E16). In this study, 280 patients equated to N:p ratios of approximately 11 for the
Daily PROactive PRO (23 items) and approximately 7 for the Clinical visit PROactive
PRO (34 items).
Treatment of missing data
The electronic devices for the PROs did not allow missing values in individual items
of any of the PROactive questionnaires, so no strategies to account for missing data
were used.
Descriptive results
Baseline characteristics and physical activity monitors were summarized according to
number and percentage for qualitative variables, mean and standard deviation for
quantitative variables with normal distribution, and median and 25th-75th percentiles
for quantitative variables with non-normal distribution. Comparisons between sites
and between arms were conducted for description purposes.
Online Data Supplement 11
Item reduction – datasets and variables
The item reduction process was conducted separately for Daily and Clinical visit
versions of PROactive PROs using IRAS-D and IRAS-C, respectively. For the Daily
PROactive PRO, the analyses were performed choosing at random one day, while
for the Clinical visit PROactive PRO one of the two administrations was chosen at
random. The item reduction followed a systematic iterative process (Figure 2) that
was based on the following criteria: (i) floor and ceiling effects; (ii) fitting
unidimensionality; (iii) redundancy of items; (iv) ordering of categories; and (v)
differential item functioning. Additionally, information from patients’ interviews, focus
groups, cognitive debriefings and Advisory Board advice were considered during
personal meetings (11 May 2012 in Paris, 26-27 June 2012 in Barcelona, 18 March
2013 in Leuven, 27 June 2013 in Brussels, 10 July 2013 in London, and 18 July 2014
in Munich) and periodic phone discussions (25 April 2012, 30 May 2012, 7 June
2012, 6 July 2012, 18 July 2012, 29 August 2012, 29 November 2012, 12 December
2012, 6 February 2013, and 12 June 2013) prior to removal of items or as supportive
to keep items that statistically might not perform perfectly well (Figure 2).
We envisaged that the PROs did not capture well information on the amount of
physical activity, both Daily and Clinical visit PROs were analyzed alone and in
combination with activity data from each monitor (analyzed separately). Therefore,
the item reduction process was done with six sets of variables: (i) items from the
Daily PRO, (ii) items from the Daily PRO with variables from Dynaport activity
monitor, (iii) items from the Daily PRO with variables from Actigraph activity monitor,
(iv) items from the Clinical visit PRO, (v) items from the Clinical visit PRO with
variables from Dynaport activity monitor, and (vi) items from the Clinical visit PRO
with variables from Actigraph activity monitor. For the Daily PRO, activity monitors
Online Data Supplement 12
variables were obtained from the same exact day than PRO items; for the Clinical
visit PRO, the median values of accelerometers variables from each week of
measurement were included. For the item reduction, variables from activity monitors
were categorized both using cut-offs from the literature and quintiles (details
available from the authors). We foresaw that activity monitors data would only be
incorporated into the final PROactive Physical Activity in COPD (PPAC) instruments
if the information it provided was not redundant, according to the inter-item
correlations and infit and outfit values.
Finally, several sensitivity analyses were done using different sets of days, or
different categories of variables/items (details available from the authors).
Item reduction – statistical analysis
The following analyses were performed for each dataset of those mentioned above at
each iteration.
Floor effect and ceiling effects. Items with 50% of patients in either the top or lower
category were flagged for exclusion (E17).
Exploratory Factor Analysis. Exploratory factor analysis was performed to inform
about dimensionality of the PROs. Factors with eigenvalues>1 were retained and
considered to identify different dimensions if the ratio of first to second eigenvalue
was ≥4 (E17, E18). After promax rotation, items were assigned to a factor if the
largest factor loading was greater than |0.3| and at least twice as big as the second
largest loading (E17). Items with all factors loading smaller than |0.3| were
considered for removal.
Online Data Supplement 13
Item-to-total score correlation. Item-to-total score correlation was calculated as the
Pearson correlation coefficient between each item and the sum of all (remaining)
items. Item to total score correlation was expected to be high, so items with values
smaller than |0.5| were flagged for exclusion (E11).
Inter-item correlation. Pairwise inter-item correlations were computed using the
Pearson correlation coefficient. Items with high inter-item correlation (>|0.8|) were
flagged because they indicate potential redundancy, and those with low inter-item
correlation (<|0.2|) were flagged because they indicate that the item does not fit with
the other items (E17).
Rasch analysis. We fitted the polytomous generalization of the Rasch model, the
rating scale model (E19) and we checked the following properties: (1) Ordering of
response categories for each item: we flagged for exclusion items in which the
ordering of the thresholds did not follow the logical sequence (E20, E21); (2) Item fit
statistics: items with values <0.8 for information-weighted fit statistic (infit) and <0.7
for the outlier-sensitive fit statistic (outfit) were flagged for exclusion since they can
indicate redundancy (E21); items with values >1.2 for infit and >1.3 for outfit were
flagged for exclusion because they probably measure a different concept than the
overall scale. The chi-squared fit statistic was used to have a ranking of the least
well-fitting items (i.e., to decide which item exclude first in case several fulfilled infit
and/or outfit criteria for exclusion), because significant chi-squared statistics indicate
bad fit to the unidimensional model (E20, E21). (3) Person item map: the person item
map displays the location of items and thresholds along with the distribution of
persons along the final scale. In this plot, we checked whether the mean of items was
close to the mean of patients, indicating that the items are well targeted to the
patients (E21), whether items were located along the whole scale, thus covering a

Online Data Supplement 14
wide range, and on which part of the scale each item has more discriminating power.
(4) Overall fit of the model: the person separation index (PSI) was calculated and
indicates the ability (precision) of the instrument to differentiate between different
people’s physical activity. Values greater than 0.8 were considered to indicate good
performance of the scale, with appropriate ability to discriminate different physical
activity in the patients (E21).
Differential item functioning. We evaluated differential item functioning (DIF)
according to sex and site using a hybrid approach that combined ordinal logistic
regression and item response theory (E22). Items were flagged if they showed a p-
value less than 0.01 to any of the likelihood ratio test (uniform DIF, non-uniform DIF,
and total DIF), showed a MC Fadden pseudo R2 higher than 0.13, or a 10%
difference in the coefficient for physical activity when the group variable (sex or site)
and its interaction entered the model (E23). Content experts helped to determine
whether items with DIF were central to the meaning of the construct and needed to
be retained.
Confirmatory factor analysis. Confirmatory factor analysis (CFA) using structural
equation modeling (SEM) was used to test the fit of the final PROactive Physical
Activity in COPD (PPAC) instruments with the dimensionality identified during item
reduction process. It was done separately for Daily and Clinical visit PPAC using,
respectively, a random day not used in previous analyses, and the remaining Clinical
visit administration at visit 1 and visit 3 that was not used before in the analyses. The
SEM model imposed the following structure: a number of factors derived from
previous analysis, each item contributing to at least on factor, and allowing
correlation between factors if more than one were included. The fit of the SEM model
was evaluated using several indices commonly used in CFA, namely the root mean
Online Data Supplement 15
square error of approximation (RMSEA), the comparative fit index (CFI), the Non-
Normed Fit Index (NNFI) and the standardized root mean square residual (SRMR)
(E18, E24), considering an ideal performance if RMSEA<0.05, CFI>0.95, NNFI>0.92,
and SRMR <0.08, and no items loaded <0.3 (E18).
Developing equivalences between activity monitors.
A process was done, separately for Daily and Clinical visit versions using IRAS-D
and IRAS-C, respectively, to identify cut-offs of the variables from the activity
monitors that provided the same information to the final versions of PPAC. In order to
do so, we built regression analyses predicting the value of a physical activity variable
from one monitor (e.g., steps from Actigraph) with the same physical activity variable
from the other monitor (i.e., steps from Dynaport), after appropriate normalization if
required. Goodness of fit was assessed by means of normality of residuals,
heteroscedasticity, linearity, collinearity and identification of influential data. Then,
using the cut-offs of the final PPAC version with one of the monitors (identified as
defined above), we calculated the value of cut-offs for the other monitor and tested
performance in the Rasch model. We repeated the process using the second monitor
as the basis. After identifying cut-offs that were equivalent according to regression
models, and that provided same Rasch analysis results, we tested agreement
between such cut-offs.
Initial validation of the PROactive instruments
The initial validation involved reliability (covering internal consistency and test-retest
reliability) and construct validity (covering convergent, known-groups and
discriminant validity). All analyses were performed for the final Daily and Clinical
PPAC instruments (D-PPAC and C-PPAC, respectively), separately for each
Online Data Supplement 16
dimension in case the instruments had exhibited more than one dimension. The
following tests were performed:
Internal consistency. To evaluate internal consistency, Cronbach’s alpha was
calculated for the D-PPAC and C-PPAC, separately, using TRAS-D and TRAS-C.
Their values were considered appropriate if between 0.70 and 0.90 (E21). For the D-
PPAC, Cronbach’s alpha were calculated for each day and also using the 1-week
average of each item, resulting in two values of Cronbach’s alpha, one for the first 7
days of daily assessments (week 1 for arm 1 / week 5 for arm 2) and one for the
second week of daily assessments (week 2 for arm 1 / week 6 for arm 2). For the C-
PPAC Cronbach’s alpha were calculated for each assessment period, resulting in
two values of Cronbach’s alpha, one for the first assessment (visit 3 for arm 1 / visit 1
for arm 2) and one for the second assessment (visit 4 for arm 1 / visit 2 for arm 2).
Test-retest reliability. Test-retest for the D-PPAC was performed on the TRAS-D
dataset. For patients randomised to arm 1, the score from days 1-7, week 1 was
compared to the score from days 1-7, week 2, separately for each of the seven days.
For patients randomised to arm 2, the score from days 1-7, week 5 was compared to
the score from days 1-7, week 6, separately for each of the seven days. In addition,
the average score across the first 7 days of daily assessments (week 1/week 5) and
the average score across the 7 days of the second week of daily assessments (week
2/week 6) were calculated and tested for reliability. Test-retest reliability for the C-
PPAC was performed on the TRAS-C dataset. For patients randomised to arm 1, the
response to each item on day 1, week 1 were compared with their response to the
same score on day 7, week 2. For patients randomised to arm 2, the response to
each item on day 1, week 5 were compared with their response to the same item on
day 7, week 6. Patients from both sequences were pooled for analysis. The
Online Data Supplement 17
agreement between the final scales in the two time points (single administrations plus
1-week average for the D-PPAC and single administrations for C-PPAC) was
assessed using the intra-class correlation coefficient (ICC) and Bland-Altman plot
(E25) and considering desirable values of ICC greater than 0.8 (E21).
Construct validity refers to whether an instrument measures the unobservable
construct that it purports to measure. Several specific types of validity were explored
to support construct validity, namely: convergent, known-groups and discriminant
validity.
Convergent validity. Using the CVAS-D and CVAS-C datasets, we explored the
correlations between the PPAC instruments (and their potential dimensions
subscales) and (some dimensions of) related constructs, namely dyspnoea (mMRC),
exercise tolerance (6MWD), physical activity amount (accelerometers), and HRQL
(CRQ, CCQ, CAT). A matrix of expected correlations for each variable was built
using bibliography at the time of analysis. Pearson or Spearman correlation
coefficients were calculated. Correlations lower than 0.3 were considered weak,
correlation between 0.3 and 0.5 were considered moderate, and correlations greater
than 0.5 were considered strong. Correlations less than 0.9 were expected so that
the two measures provide different information (E21). Calculation of the correlations
was repeated for every visit in which the PROs and each construct were collected
(e.g. visits 1, 2, 3 and 4 for mMRC). Each construct was compared to the C-PPAC
obtained in the closest visit and with the closest day of the D-PPAC, as well as with
the average of the week before clinical visit.
Known-groups validity. The PPAC instruments (and their potential dimensions
subscales) were compared (i) across mMRC grades of dyspnoea (collapsing 0-1, 2-
Online Data Supplement 18
3, and 4), respectively, using ANOVA test; (ii) between stable and exacerbated
patients using a t-test; and (iii) across levels of physical activity defined according to
the monitors using a t-test, ANOVA, or other tests required depending on data
distribution. These comparisons were done for each visit where both PROactive
scores and the groups of interest are available.
Discriminant validity. The PPAC instruments (and their potential dimensions
subscales) were correlated to expected unrelated constructs, namely height, income
category or socioeconomic status. Pearson correlation coefficients were calculated.
Low correlations were expected (<0.3). Calculation of the correlations was repeated
for every visit in which the PROs and each construct were collected. Each construct
was compared to the C-PPAC obtained in the closest visit and with the closest day of
the D-PPAC, as well as with the average of the week before clinical visit.
Online Data Supplement 19
List of proposed items for day-to-day (Daily) assessment
1. How much walking did you do outside today?
2. How many chores did you do inside the house today? Some examples are
cleaning, doing the laundry or mending things.
3. How many chores did you do outside the house today? Some examples are
gardening, taking the rubbish out, or doing small errands.
4. How much physical leisure activity did you do today? Some examples are
swimming, cycling or going out.
5. How much difficulty did you have getting dressed today?
6. How much difficulty did you have with carrying things you needed to today?
7. Did you avoid climbing stairs today because of your lung problems? OR How
much difficulty did you have climbing stairs today?
8. Did your lung problems prevent you from taking a shower today? OR How
much difficulty did you have showering today?
9. Did your lung problems prevent you from taking a bath today? OR How much
difficulty did you have taking a bath today?
10. How much difficulty did you have bending over today (for instance to put on
your socks or tie your shoelaces)?
11. How much difficulty did you have washing yourself today?
12. How much difficulty did you have walking up a small slope today?
13. How much difficulty did you have when hurrying today (for instance to catch a
bus or to finish your work in time)?
14. How often did you avoid doing activities because of your lung problems today?
15. How breathless were you in general during your activities today?
Online Data Supplement 20
16. How often did you lack physical strength to do things because of your lung
problems today?
17. How often did you experience lack of strength in your legs during your
physical activities today?
18. How tired were you in general during your activities today?
19. How often did you have to take breaks during your physical activities today?
20. How often did you have to pace yourself during your physical activities today?
21. How often did your lung problems prevent you from doing activities that you
needed to do today?
22. How breathless were you when walking on level ground indoors and outdoors
today?
23. How often did you have to slow down while walking today?
24. How breathless were you when climbing stairs today?
25. How much time did you need to recover from your physical activities today?
26. Did you need to spread your activities throughout the day today because of
your lung problems?
27. Did your lung problems stop you from doing the physical activities that you
wanted to do today?
28. How many puffs of [insert name of rescue medication here] in addition to your
regularly used medication did you need to take for your physical activities
today?
29. Did you need to consider your lung problems when you planned your activities
today? Examples are a trip out, an appointment or expecting visitors.

Online Data Supplement 21
30. How much help from others did you need with any of your activities today?
Please consider all activities. Examples are household chores, shopping or
getting dressed.
Online Data Supplement 22
List of proposed items for Clinic visit assessment
1. In the past 7 days, how much walking did you do outside?
2. In the past 7 days, how many chores did you do inside the house? Some
examples are cleaning, doing the laundry or mending things.
3. In the past 7 days, how many chores did you do outside the house? Some
examples are gardening, taking the rubbish out, or doing small errands.
4. In the past 7 days, how much physical leisure activity did you do? Some
examples are swimming, cycling or going out.
5. In the past 7 days, how much difficulty did you have getting dressed?
6. In the past 7 days, how much difficulty did you have with carrying things you
needed to?
7. In the past 7 days, did you avoid climbing stairs because of your lung
problems? OR In the past 7 days, how much difficulty did you have climbing
stairs?
8. In the past 7 days, how much difficulty did you have showering?
9. In the past 7 days, how much difficulty did you have bathing?
10. In the past 7 days, how much difficulty did you have bending over (for instance
to put on your socks or tie your shoelaces)?
11. In the past 7 days, how much difficulty did you have washing yourself?
12. In the past 7 days, how much difficulty did you have walking up a small slope?
13. In the past 7 days, how much difficulty did you have getting out and about?
14. In the past 7 days, how much difficulty did you have when hurrying (for
instance to catch a bus or to finish your work in time)?
15. In the past 7 days, how often did you avoid doing activities because of your
lung problems?

Online Data Supplement 23
16. In the past 7 days, how breathless were you in general during your activities?
17. In the past 7 days, how often did you lack physical strength to do things
because of your lung problems?
18. In the past 7 days, how often did you experience lack of strength in your legs
during your physical activities?
19. In the past 7 days, how tired were you in general during your activities?
20. In the past 7 days, how often did you have to take breaks during your physical
activities?
21. In the past 7 days, how often did you have to pace yourself during your
physical activities?
22. In the past 7 days, how often did your lung problems prevent you from doing
activities that you needed to do?
23. In the past 7 days, how often did you cough during your physical activities?
24. In the past 7 days, how breathless were you when walking on level ground
indoors and outdoors?
25. In the past 7 days, how often did you have to slow down while walking?
26. In the past 7 days, how breathless were you when climbing stairs?
27. In the past 7 days, how much time did you need to recover from your physical
activities?
28. In the past 7 days, did you need to spread your activities throughout the day
because of your lung problems?
29. In the past 7 days, did your lung problems stop you from doing the physical
activities that you wanted to do?
Online Data Supplement 24
30. In the past 7 days, how many puffs of [insert name of rescue medication here]
in addition to your regularly used medication did you need to take for your
physical activities?
31. In the past 7 days, did you need to consider your lung problems when you
planned your activities because of your lung problems? Examples are a trip
out, an appointment or expecting visitors.
32. In the past 7 days, how much help from others did you need with any of your
activities? Please consider all activities. Examples are household chores,
shopping or getting dressed.
33. In the past 7 days, how often did you exercise to maintain or improve your
physical condition?
34. In the past 7 days, how often did you use aids to facilitate your physical
activities? Some examples are a wheeled walker, stair lift, or a chair in the
shower.
35. In the past 7 days, how often did you overexert yourself during your physical
activities?

Online Data Supplement 25
Table E1. Baseline demographic and clinical characteristics of COPD patients stratified by sites
Athens
(n = 49)
m (SD) / n (%)
Edinburgh
(n = 45)
m (SD) / n (%)
Groningen
(n = 39)
m (SD) / n (%)
Leuven
(n = 54)
m (SD) / n (%)
London
(n = 49)
m (SD) / n (%)
Patient status at recruitment
Stable 45 (92) 43 (96) 39 (100) 49 (91) 45 (92)
Exacerbated 4 (8) 2 (4) 0 (0) 5 (9) 4 (8)
Age (years) 66.2 (8.0) 71.7 (7.4) 64.0 (9.6) 66.3 (6.5) 68.7 (9.1)
Male 38 (78) 28 (62) 24 (62) 42 (78) 28 (57)
Primary ethnicity: White 49 (100) 45 (100) 38 (97) 54 (100) 45 (92)
Marital status:
Married 30 (62) 26 (58) 25 (64) 40 (74) 27 (55)
Single 4 (8) 2 (4) 5 (13) 2 (4) 9 (18)
Widow 8 (16) 12 (27) 5 (13) 5 (9) 5 (10)
Divorced 7 (14) 5 (11) 4 (10) 6 (11) 6 (12)
Other 0 (0) 0 (0) 0 (0) 1 (2) 2 (4)
Living:
Alone 15 (31) 17 (38) 12 (31) 54 (100) 19 (39)
Family 34 (69) 28 (62) 27 (69) 0 (0) 30 (61)
Education:
None 0 (0) 0 (0) 0 (0) 0 (0) 0 (0)
Primary school 14 (29) 0 (0) 7 (18) 20 (37) 2 (4)
Secondary school/High school 27 (55) 39 (87) 25 (64) 29 (54) 33 (67)
University 7 (14) 3 (7) 6 (15) 5 (9) 13 (27)
Post graduate 1 (2) 3 (7) 1 (3) 0 (0) 1 (2)
Socioeconomic status
I - Professional occupation 1 (2) 2 (4) 2 (5) 1 (2) 3 (6)
II - Managerial and technical occupation 11 (22) 5 (11) 13 (33) 7 (13) 21 (43)
III - Non-manual skilled occupation 5 (10) 14 (31) 10 (26) 9 (17) 8 (16)
III - Manual skilled occupation 21 (43) 13 (29) 9 (23) 27 (50) 15 (31)

Online Data Supplement 26
Athens
(n = 49)
m (SD) / n (%)
Edinburgh
(n = 45)
m (SD) / n (%)
Groningen
(n = 39)
m (SD) / n (%)
Leuven
(n = 54)
m (SD) / n (%)
London
(n = 49)
m (SD) / n (%)
IV - Partly skilled occupation 7 (14) 6 (13) 5 (13) 8 (15) 1 (2)
V - Unskilled occupation 4 (8) 5 (11) 0 (0) 2 (4) 1 (2)
Working status:
Employed 4 (8) 1 (2) 12 (31) 6 (11) 5 (10)
Unemployed 2 (4) 3 (7) 4 (10) 7 (13) 3 (6)
Retired 43 (88) 41 (91) 23 (59) 41 (76) 41 (84)
Current smoker 5 (10) 7 (16) 7 (18) 20 (37) 4 (8)
Pack-years 91.6 (51.9) 53.3 (32.0) 35.0 (21.6) 55.9 (38.0) 45.5 (24.9)
Weigth (kg) 76.8 (17.8) 80.5 (19.1) 80.0 (15.5) 76.5 (16.4) 74.3 (17.5)
Heigth (cm) 168.8 (7.6) 166.7 (10.3) 172.9 (10.3) 169.4 (7.9) 168.1 (9.2)
BMI (kg/m2) 27.0 (6.2) 28.8 (5.8) 26.6 (3.6) 26.6 (5.1) 26.3 (6.0)
FFMI (kg/m2)* 18.1 (2.3) 18.4 (3.0) 18.2 (2.7) 18.2 (3.3) 17.8 (3.5)
FEV1 (% predicted) 46.9 (15.3) 61.6 (20.3) 62.3 (15.6) 61.9 (21.9) 53.6 (23.2)
FVC (% predicted) 80.4 (19.7) 100.2 (21.1) 100.9 (14.6) 99.7 (17.6) 98.2 (16.2)
FEV1/FVC (%) 46.5 (13.4) 48.1 (12.4) 49.6 (11.3) 48.2 (12.3) 42.5 (15.2)
IC/TLC (%)* 31.5 (9.5) 38.5 (8.6) 39.2 (8.3) 31.4 (10.5) 33.6 (9.6)
RV/TLC (%)* 51.7 (12.6) 48.9 (9.3) 47.3 (10.3) 51.9 (13.0) 54.0 (9.8)
TLCO (%predicted)* 52.9 (22.9) 59.5 (19.7) 67.0 (21.4) 63.7 (22.6) 56.9 (24.2)
ATS/ERS stages*
I - mild (FEV1≥80%) 0 (0) 10 (23) 4 (10) 12 (22) 8 (16)
II - Moderate (FEV1<80% and ≥50%) 21 (43) 20 (46) 25 (64) 25 (46) 17 (35)
III - Severe (FEV1<50% and ≥30% 19 (39) 12 (27) 10 (26) 14 (26) 16 (33)
IV - very severe (FEV1<30%) 9 (18) 2 (5) 0 (0) 3 (6) 8 (16)
6-MWD (m)* 356.3 (99.2) 403.9 (124.8) 472.3 (91.7) 500.5 (135.6) 403.8 (129.9)
Quadriceps strength (kg)* 27.7 (8.2) 37.6 (12.7) 32.5 (14.8) 34.1 (10.0) 27.5 (10.4)
Previous admissions for COPD exacerbation
Yes 32 (65) 11 (24) 3 (8) 29 (54) 20 (41)
No 17 (35) 34 (76) 36 (92) 25 (46) 29 (59)
Online Data Supplement 27
Athens
(n = 49)
m (SD) / n (%)
Edinburgh
(n = 45)
m (SD) / n (%)
Groningen
(n = 39)
m (SD) / n (%)
Leuven
(n = 54)
m (SD) / n (%)
London
(n = 49)
m (SD) / n (%)
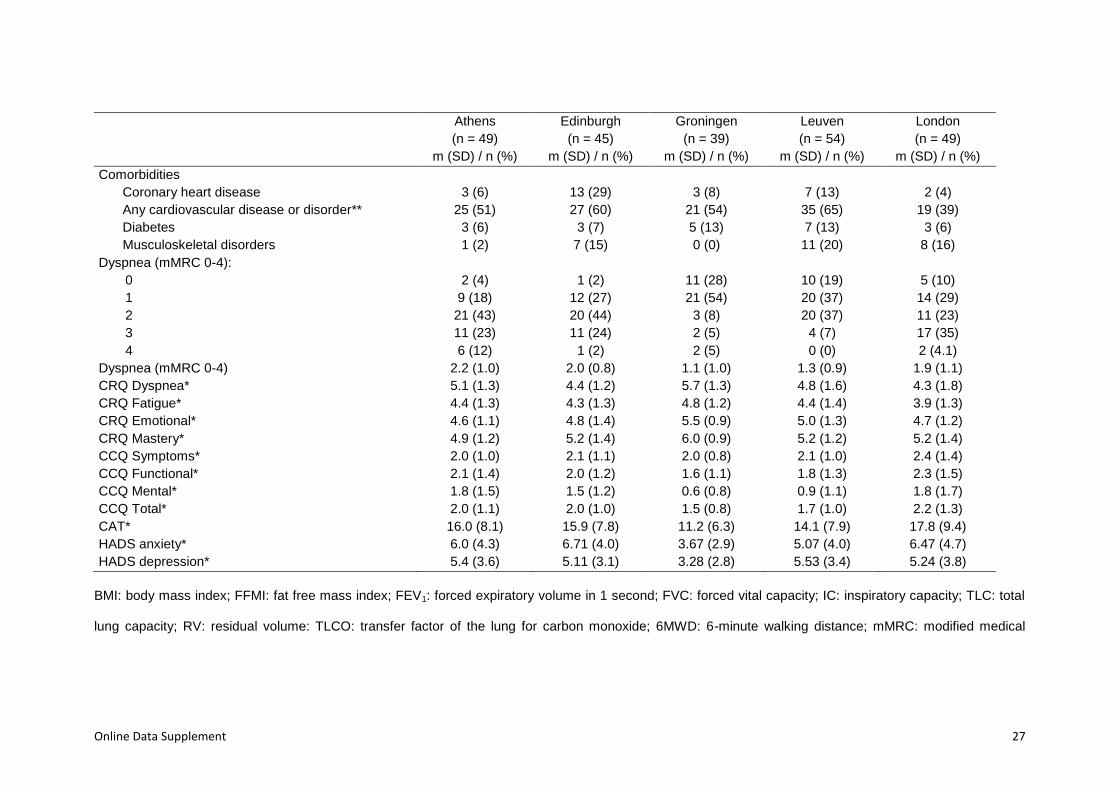
Comorbidities
Coronary heart disease 3 (6) 13 (29) 3 (8) 7 (13) 2 (4)
Any cardiovascular disease or disorder** 25 (51) 27 (60) 21 (54) 35 (65) 19 (39)
Diabetes 3 (6) 3 (7) 5 (13) 7 (13) 3 (6)
Musculoskeletal disorders 1 (2) 7 (15) 0 (0) 11 (20) 8 (16)
Dyspnea (mMRC 0-4):
0 2 (4) 1 (2) 11 (28) 10 (19) 5 (10)
1 9 (18) 12 (27) 21 (54) 20 (37) 14 (29)
2 21 (43) 20 (44) 3 (8) 20 (37) 11 (23)
3 11 (23) 11 (24) 2 (5) 4 (7) 17 (35)
4 6 (12) 1 (2) 2 (5) 0 (0) 2 (4.1)
Dyspnea (mMRC 0-4) 2.2 (1.0) 2.0 (0.8) 1.1 (1.0) 1.3 (0.9) 1.9 (1.1)
CRQ Dyspnea* 5.1 (1.3) 4.4 (1.2) 5.7 (1.3) 4.8 (1.6) 4.3 (1.8)
CRQ Fatigue* 4.4 (1.3) 4.3 (1.3) 4.8 (1.2) 4.4 (1.4) 3.9 (1.3)
CRQ Emotional* 4.6 (1.1) 4.8 (1.4) 5.5 (0.9) 5.0 (1.3) 4.7 (1.2)
CRQ Mastery* 4.9 (1.2) 5.2 (1.4) 6.0 (0.9) 5.2 (1.2) 5.2 (1.4)
CCQ Symptoms* 2.0 (1.0) 2.1 (1.1) 2.0 (0.8) 2.1 (1.0) 2.4 (1.4)
CCQ Functional* 2.1 (1.4) 2.0 (1.2) 1.6 (1.1) 1.8 (1.3) 2.3 (1.5)
CCQ Mental* 1.8 (1.5) 1.5 (1.2) 0.6 (0.8) 0.9 (1.1) 1.8 (1.7)
CCQ Total* 2.0 (1.1) 2.0 (1.0) 1.5 (0.8) 1.7 (1.0) 2.2 (1.3)
CAT* 16.0 (8.1) 15.9 (7.8) 11.2 (6.3) 14.1 (7.9) 17.8 (9.4)
HADS anxiety* 6.0 (4.3) 6.71 (4.0) 3.67 (2.9) 5.07 (4.0) 6.47 (4.7)
HADS depression* 5.4 (3.6) 5.11 (3.1) 3.28 (2.8) 5.53 (3.4) 5.24 (3.8)
BMI: body mass index; FFMI: fat free mass index; FEV1: forced expiratory volume in 1 second; FVC: forced vital capacity; IC: inspiratory capacity; TLC: total
lung capacity; RV: residual volume: TLCO: transfer factor of the lung for carbon monoxide; 6MWD: 6-minute walking distance; mMRC: modified medical
Online Data Supplement 28
research council dyspnea scale; CRQ: chronic respiratory questionnaire; CCQ: clinical chronic obstructive pulmonary disease questionnaire; CAT: chronic
obstructive pulmonary disease assessment test; HADS: hospital anxiety and depression scale.
* Some values are missing for certain variables: 9 for FFMI, 15 for IC/TLC, 14 for RV/TLC, 8 for TLCO (% pred), 1 for GOLD stages, 3 for 6-minute walking
distance, 3 for quadriceps strength, 88 for CRQ dyspnea, 3 for CRQ fatigue, 3 for CRQ emotional, 3 for CRQ mastery, 1 for CCQ, 2 for CAT, 1 for HADS
anxiety, 1 for HADS depression.
** Including coronary heart disease

Online Data Supplement 29
Table E2. Description of activity monitor data, stratified by visit and by site
All Athens Edinburgh Groningen Leuven London
VISITS 1 to 2: week 1
Dynaport n=228 n=48 n=42 n=37 n=53 n=48
Wearing time (min/day) 879 (117) 863 (136) 856 (96) 908 (121) 902 (123) 869 (95)
Time in locomotion (min/day) 60 (36) 56 (39) 45 (22) 65 (28) 77 (40) 55 (37)
Standing time (min/day) 155 (64) 148 (63) 142 (60) 175 (67) 166 (66) 145 (59)
Intensity (g) 0.184 (0.030) 0.177 (0.026) 0.176 (0.026) 0.191 (0.027) 0.186 (0.028) 0.192 (0.040)
VMU (VMU/min) 351 (232) 316 (226) 272 (160) 380 (181) 421 (267) 357 (265)
Steps per day 4763 (3129) 4400 (3176) 3477 (1791) 5127 (2433) 6072 (3430) 4525 (3627)
Actigraph n=218 n=47 n=41 n=36 n=50 n=44
Wearing time (min/day) 839 (96) 825 (103) 809 (78) 862 (109) 862 (95) 837 (87)
Time in MVPA (min/day), median (P25-P75) 5 (1-17) 3 (1-15) 3 (1-8) 7 (1-12) 7 (2-23) 9 (1-23)
VMU (VMU/min) 461 (213) 412 (221) 413 (165) 497 (194) 518 (223) 465 (231)
Steps per day 4345 (2909) 3862 (2861) 3230 (1897) 4878 (2974) 5168 (2753) 4528 (3501)
VISITS 1 to 2: week 2
Dynaport n=191 n=44 n=30 n=32 n=46 n=39
Wearing time (min/day) 893 (129) 882 (160) 866 (135) 913 (117) 908 (112) 891 (114)
Time in locomotion (min/day) 62 (35) 57 (36) 50 (21) 69 (39) 70 (34) 59 (37)
Standing time (min/day) 160 (64) 152 (64) 153 (58) 190 (69) 164 (68) 146 (55)
Intensity (g) 0.183 (0.029) 0.177 (0.026) 0.173 (0.022) 0.190 (0.027) 0.181 (0.026) 0.191 (0.037)
VMU (VMU/min) 340 (221) 305 (203) 278 (157) 397 (229) 365 (215) 351 (270)
Steps per day 4871 (3024) 4478 (2875) 3898 (1751) 5505 (3315) 5510 (2934) 4789 (3622)
Actigraph n=189 n=42 n=38 n=30 n=46 n=33
Wearing time (min/day) 840 (99) 827 (106) 806 (77) 869 (122) 869 (73) 828 (105)
Time in MVPA (min/day), median (P25-P75) 4 (1-13) 4 (1-11) 4 (0-10) 3 (1-8) 5 (2-16) 5 (1-19)
VMU (VMU/min) 450 (207) 412 (212) 424 (177) 441 (165) 500 (201) 466 (264)
Steps per day 4234 (2913) 3876 (2487) 3325 (1949) 4608 (3579) 4841 (2589) 4552 (3821)
VISITS 3 to 4: week 5
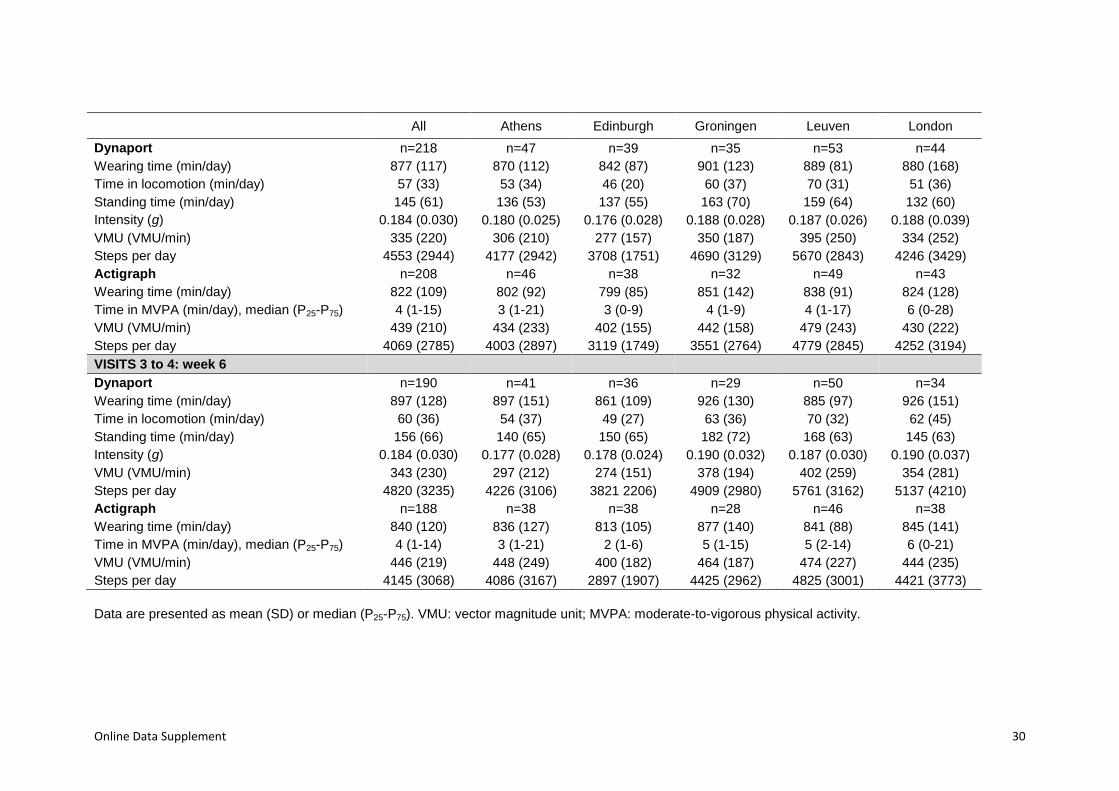
Online Data Supplement 30
All Athens Edinburgh Groningen Leuven London
Dynaport n=218 n=47 n=39 n=35 n=53 n=44
Wearing time (min/day) 877 (117) 870 (112) 842 (87) 901 (123) 889 (81) 880 (168)
Time in locomotion (min/day) 57 (33) 53 (34) 46 (20) 60 (37) 70 (31) 51 (36)
Standing time (min/day) 145 (61) 136 (53) 137 (55) 163 (70) 159 (64) 132 (60)
Intensity (g) 0.184 (0.030) 0.180 (0.025) 0.176 (0.028) 0.188 (0.028) 0.187 (0.026) 0.188 (0.039)
VMU (VMU/min) 335 (220) 306 (210) 277 (157) 350 (187) 395 (250) 334 (252)
Steps per day 4553 (2944) 4177 (2942) 3708 (1751) 4690 (3129) 5670 (2843) 4246 (3429)
Actigraph n=208 n=46 n=38 n=32 n=49 n=43
Wearing time (min/day) 822 (109) 802 (92) 799 (85) 851 (142) 838 (91) 824 (128)
Time in MVPA (min/day), median (P25-P75) 4 (1-15) 3 (1-21) 3 (0-9) 4 (1-9) 4 (1-17) 6 (0-28)
VMU (VMU/min) 439 (210) 434 (233) 402 (155) 442 (158) 479 (243) 430 (222)
Steps per day 4069 (2785) 4003 (2897) 3119 (1749) 3551 (2764) 4779 (2845) 4252 (3194)
VISITS 3 to 4: week 6
Dynaport n=190 n=41 n=36 n=29 n=50 n=34
Wearing time (min/day) 897 (128) 897 (151) 861 (109) 926 (130) 885 (97) 926 (151)
Time in locomotion (min/day) 60 (36) 54 (37) 49 (27) 63 (36) 70 (32) 62 (45)
Standing time (min/day) 156 (66) 140 (65) 150 (65) 182 (72) 168 (63) 145 (63)
Intensity (g) 0.184 (0.030) 0.177 (0.028) 0.178 (0.024) 0.190 (0.032) 0.187 (0.030) 0.190 (0.037)
VMU (VMU/min) 343 (230) 297 (212) 274 (151) 378 (194) 402 (259) 354 (281)
Steps per day 4820 (3235) 4226 (3106) 3821 2206) 4909 (2980) 5761 (3162) 5137 (4210)
Actigraph n=188 n=38 n=38 n=28 n=46 n=38
Wearing time (min/day) 840 (120) 836 (127) 813 (105) 877 (140) 841 (88) 845 (141)
Time in MVPA (min/day), median (P25-P75) 4 (1-14) 3 (1-21) 2 (1-6) 5 (1-15) 5 (2-14) 6 (0-21)
VMU (VMU/min) 446 (219) 448 (249) 400 (182) 464 (187) 474 (227) 444 (235)
Steps per day 4145 (3068) 4086 (3167) 2897 (1907) 4425 (2962) 4825 (3001) 4421 (3773)
Data are presented as mean (SD) or median (P25-P75). VMU: vector magnitude unit; MVPA: moderate-to-vigorous physical activity.
Online Data Supplement 31
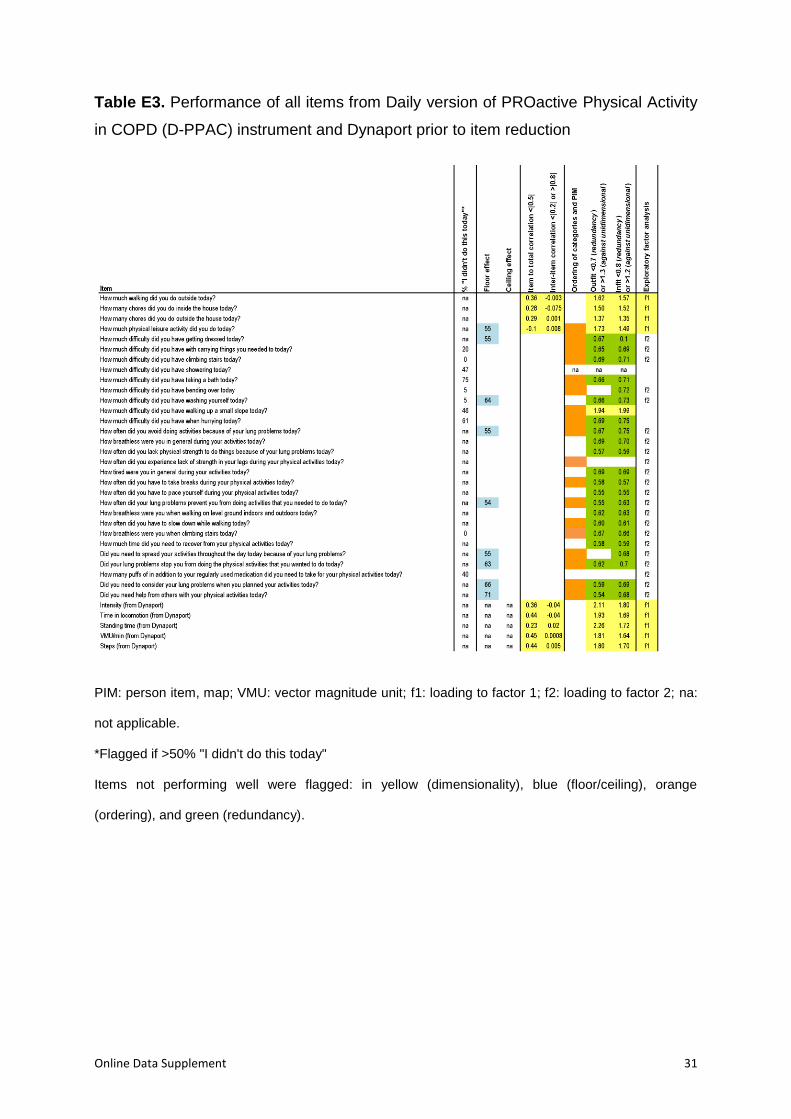
Table E3. Performance of all items from Daily version of PROactive Physical Activity
in COPD (D-PPAC) instrument and Dynaport prior to item reduction
PIM: person item, map; VMU: vector magnitude unit; f1: loading to factor 1; f2: loading to factor 2; na:
not applicable.
*Flagged if >50% "I didn't do this today"
Items not performing well were flagged: in yellow (dimensionality), blue (floor/ceiling), orange
(ordering), and green (redundancy).
Online Data Supplement 32
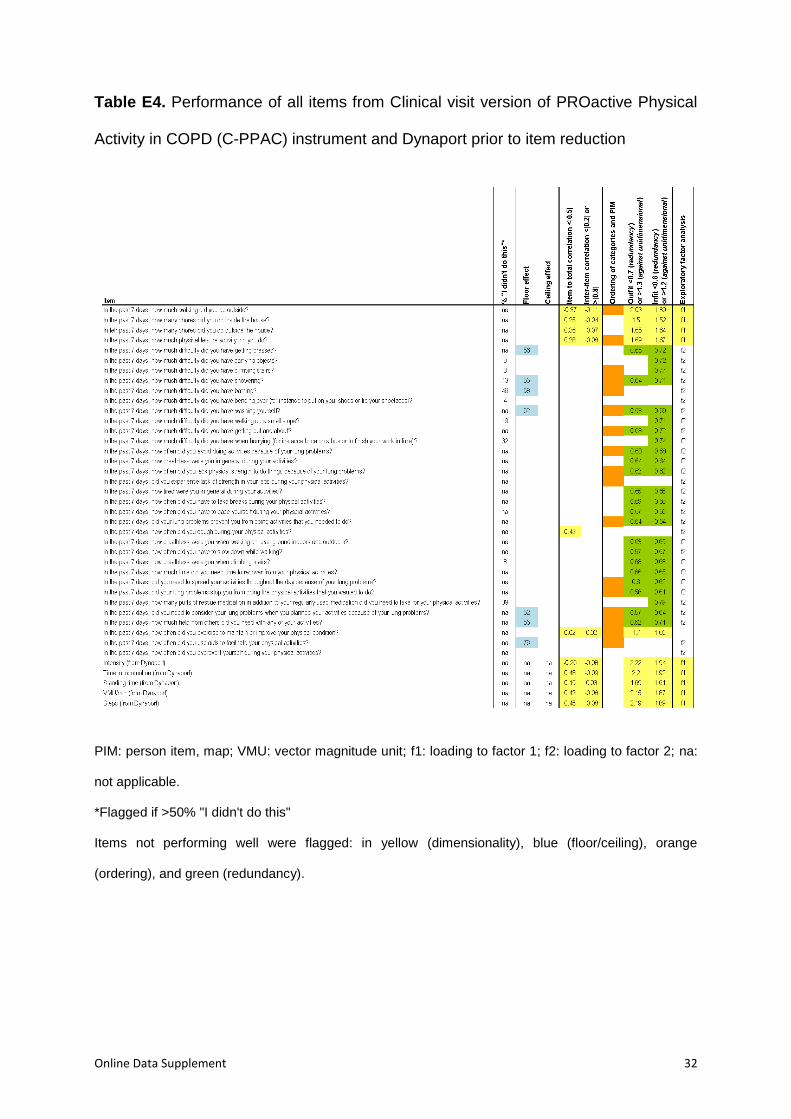
Table E4. Performance of all items from Clinical visit version of PROactive Physical
Activity in COPD (C-PPAC) instrument and Dynaport prior to item reduction
PIM: person item, map; VMU: vector magnitude unit; f1: loading to factor 1; f2: loading to factor 2; na:
not applicable.
*Flagged if >50% "I didn't do this"
Items not performing well were flagged: in yellow (dimensionality), blue (floor/ceiling), orange
(ordering), and green (redundancy).

Online Data Supplement 33
Table E5. Reason for removing items that flagged in at least one predefined criteria
Daily version of PROactive Physical Activity in COPD (D-PPAC) instrument
Factor 1 “Amount of physical activity”
Item / variable Reasons for removal
FROM PRO
How many chores did you do inside the house today?
Not fitting well with the rest of the items
Details/additional comments:
- Item not fitting well with the rest of the items:
o EFA loading <0.3
o item-to-total correlation <0.5
o inter-item correlation <0.2
o outfit >1.3
o infit >1.2
- Item exhibits differential item functioning between genders
- In patients interviews and focus groups, item reported by few percentage of patients
- In patients interviews and focus groups, item revealed differences between genders, which could make the item not applicable to men
- In cognitive debriefings, male not understanding the item (“it applies to females”, while actually it was including “mending things”)
How much physical leisure activity did you do today?
Not fitting well with the rest of the items + no proper ordering
Details/additional comments:
- Item not fitting well with the rest of the items:
o EFA loading <0.3
o outfit >1.3 in some analyses
Online Data Supplement 34
o infit >1.2 in some analyses
- Not ordering well in Rasch analysis
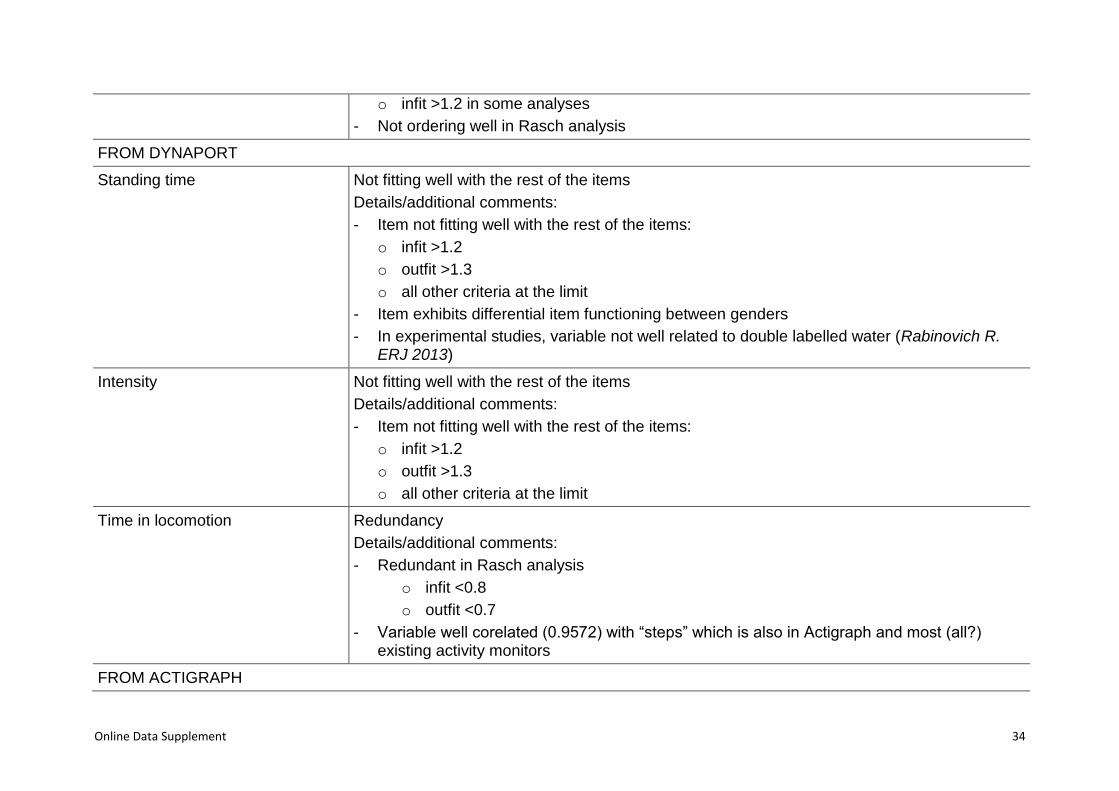
FROM DYNAPORT
Standing time Not fitting well with the rest of the items
Details/additional comments:
- Item not fitting well with the rest of the items:
o infit >1.2
o outfit >1.3
o all other criteria at the limit
- Item exhibits differential item functioning between genders
- In experimental studies, variable not well related to double labelled water (Rabinovich R. ERJ 2013)
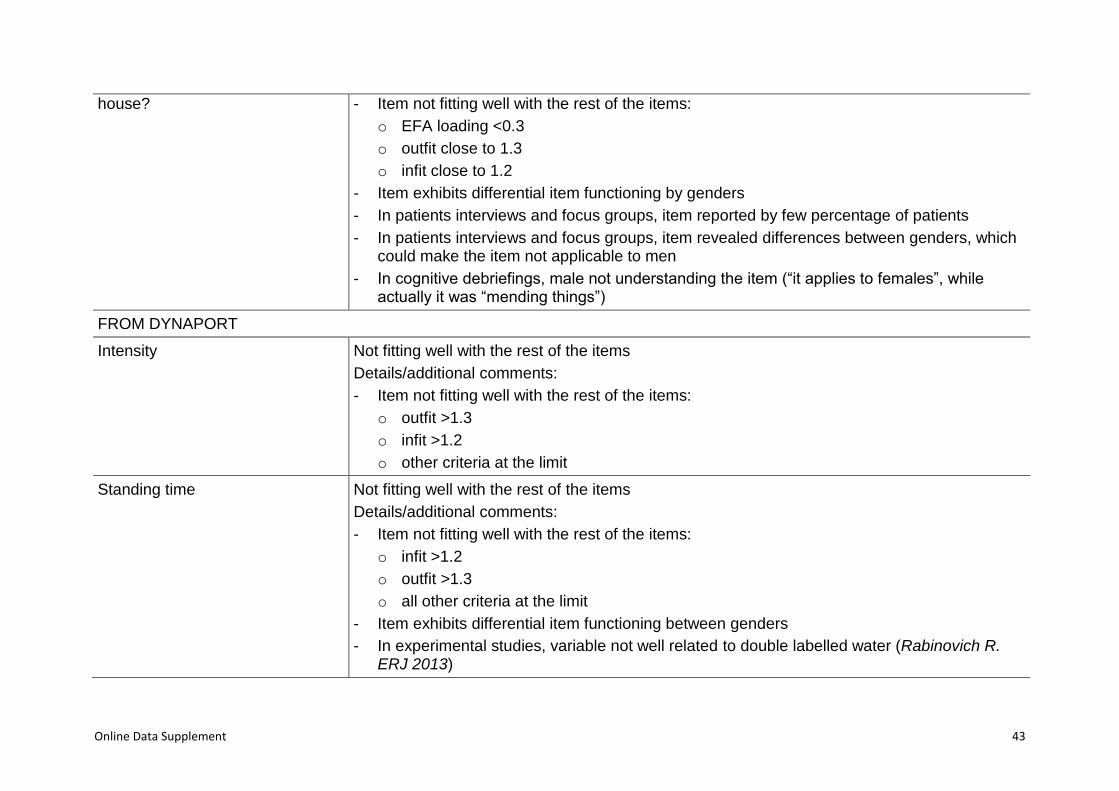
Intensity Not fitting well with the rest of the items
Details/additional comments:
- Item not fitting well with the rest of the items:
o infit >1.2
o outfit >1.3
o all other criteria at the limit
Time in locomotion Redundancy
Details/additional comments:
- Redundant in Rasch analysis
o infit <0.8
o outfit <0.7
- Variable well corelated (0.9572) with “steps” which is also in Actigraph and most (all?) existing activity monitors
FROM ACTIGRAPH
Online Data Supplement 35
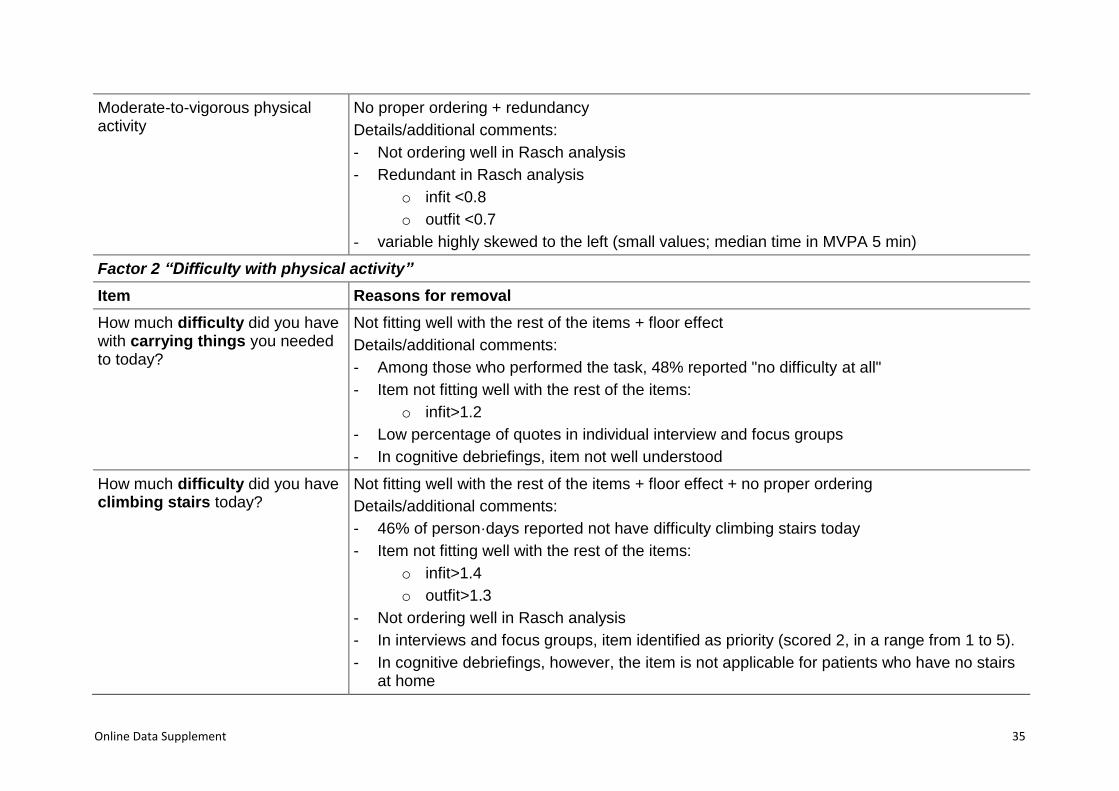
Moderate-to-vigorous physical activity
No proper ordering + redundancy
Details/additional comments:
- Not ordering well in Rasch analysis
- Redundant in Rasch analysis
o infit <0.8
o outfit <0.7
- variable highly skewed to the left (small values; median time in MVPA 5 min)
Factor 2 “Difficulty with physical activity”
Item Reasons for removal
How much difficulty did you have with carrying things you needed to today?
Not fitting well with the rest of the items + floor effect
Details/additional comments:
- Among those who performed the task, 48% reported "no difficulty at all"
- Item not fitting well with the rest of the items:
o infit>1.2
- Low percentage of quotes in individual interview and focus groups
- In cognitive debriefings, item not well understood
How much difficulty did you have climbing stairs today?
Not fitting well with the rest of the items + floor effect + no proper ordering
Details/additional comments:
- 46% of person·days reported not have difficulty climbing stairs today
- Item not fitting well with the rest of the items:
o infit>1.4
o outfit>1.3
- Not ordering well in Rasch analysis
- In interviews and focus groups, item identified as priority (scored 2, in a range from 1 to 5).
- In cognitive debriefings, however, the item is not applicable for patients who have no stairs at home
Online Data Supplement 36
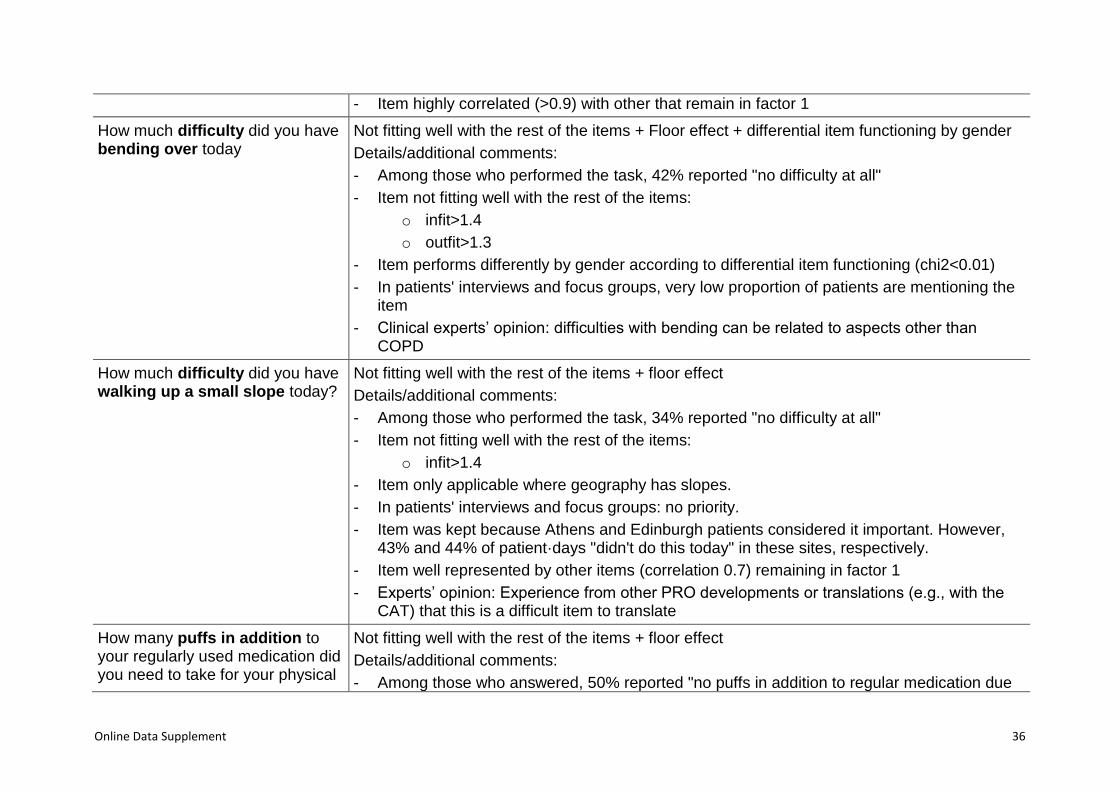
- Item highly correlated (>0.9) with other that remain in factor 1
How much difficulty did you have bending over today
Not fitting well with the rest of the items + Floor effect + differential item functioning by gender
Details/additional comments:
- Among those who performed the task, 42% reported "no difficulty at all"
- Item not fitting well with the rest of the items:
o infit>1.4
o outfit>1.3
- Item performs differently by gender according to differential item functioning (chi2<0.01)
- In patients' interviews and focus groups, very low proportion of patients are mentioning the item
- Clinical experts’ opinion: difficulties with bending can be related to aspects other than COPD
How much difficulty did you have walking up a small slope today?
Not fitting well with the rest of the items + floor effect
Details/additional comments:
- Among those who performed the task, 34% reported "no difficulty at all"
- Item not fitting well with the rest of the items:
o infit>1.4
- Item only applicable where geography has slopes.
- In patients' interviews and focus groups: no priority.
- Item was kept because Athens and Edinburgh patients considered it important. However, 43% and 44% of patient·days "didn't do this today" in these sites, respectively.
- Item well represented by other items (correlation 0.7) remaining in factor 1
- Experts’ opinion: Experience from other PRO developments or translations (e.g., with the CAT) that this is a difficult item to translate
How many puffs in addition to your regularly used medication did you need to take for your physical
Not fitting well with the rest of the items + floor effect
Details/additional comments:
- Among those who answered, 50% reported "no puffs in addition to regular medication due
Online Data Supplement 37
activities today? to activities today"
- Item not fitting well with the rest of the items:
o infit>1.4
o outfit>1.3
- According to experts opinion (Advisory Board comment): 41% not having prescribed rescue medication is not clinically believable
- According to experts opinion (Advisory Board comment): Rest of items in factor 1 fit with "ease and difficulty" while this item is an effect/result; the question may be relevant but not as a part of the tool; to be considered for validation of the tool
- In cognitive debriefings, some patients don't like the question
Did you need help from others with your physical activities today?
Not fitting well with the rest of the items + floor effect
Details/additional comments:
- In Rasch analysis, item redundant: outfit<0.6
- In Rasch analysis, person item map: narrow distribution
- In patients’ interviews and focus groups, item difficult to understand
- In patients’ interviews and focus groups, item reported together with dressing (which is kept in factor 1)
How breathless were you when climbing stairs today?
Not fitting well with the rest of the items
Additional comments:
- Item not fitting well with the rest of the items:
o infit>1.4
o outfit>1.3
- In all factor analysis, low factor load
- In patients’ interviews and focus groups, climbing stairs was reported important for those with stairs (but irrelevant for patients with no stairs)
- Item well represented by breathlessness in general, which is kept in factor 1
How often did you experience lack Not fitting well with the rest of the items
Online Data Supplement 38
of strength in your legs during your physical activities today?
Details/additional comments:
- Item not fitting well with the rest of the items:
o infit>1.4
o outfit>1.3
- In patients’ interviews and focus groups, patients report problems in legs, weakness, tiredness, soreness (but not lack of leg strength)
- In cognitive debriefings it is suggested that leg problems should be only included in clinical visit version because they are not so frequent.
How much difficulty did you have washing yourself today?
Floor effect + redundancy
Details/additional comments:
- Redundant in Rasch analysis
o outfit <0.7
- Item well represented by dressing (correlation >0.8), which remains in factor 1
- In patients’ interviews and focus groups, item reported together with dressing, which remains in factor 1
Did you need to consider your lung problems when you planned your activities today?
Floor effect + redundancy
Details/additional comments:
- Redundant in Rasch analysis
o outfit <0.7
- Item well represented by other items remaining in factor 1 (correlation >0.7)
- Item included after cognitive debriefing, not from patients’ interviews or focus groups quotes
How often did your lung problems prevent you from doing activities that you needed to do today?
Floor effect + redundancy
Details/additional comments:
- Redundant in Rasch analysis
o infit <0.8
o outfit <0.7
- Item well represented by other items remaining in factor 1 also related to planning activities
Online Data Supplement 39
(correlation >0.7)
- In patients’ interviews and focus groups, item mentioned together with other remaining items
How much difficulty did you have showering today?
Floor effect + no proper ordering
Details/additional comments:
- Among those who performed the task, 52% reported "no difficulty at all"
- Not ordering well in Rasch analysis
- In patients' interviews and focus groups, low proportion of patients are mentioning the item and represented few quotes
How much difficulty did you have taking a bath today?
Floor effect + no proper ordering
Details/additional comments:
- Among those who performed the task, 49% reported "no difficulty at all"
- In Rasch analysis, item does not order well
- In patients' interviews and focus groups, low proportion of patients are mentioning the item and represented few quotes
Did your lung problems stop you from doing the physical activities that you wanted to do today?
Floor effect + no proper ordering
Details/additional comments:
- Not ordering well in Rasch analysis
- Item well represented by most other items that remain in factor 1 (correlation >0.75)
- In patients’ interviews and focus groups, item mentioned together with other related to the planning of activities that remain in factor 1
Did you need to spread your activities throughout the day today because of your lung problems?
Floor effect + no proper ordering
Details/additional comments:
- Not ordering well in Rasch analysis
- In Rasch analysis, person item map, is very narrow. Removing it doesn't worsen PSI
- Highly correlated (>0.75) with many other remaining in factor 1, of planning and symptoms

Online Data Supplement 40
- Relevant for patients, as per patients’ interviews and focus groups.
- Experts’ opinion: item could be relevant but may be something that rather is gradually changing and not noted by patients from a day-to-day basis.
How much difficulty did you have when hurrying today?
Floor effect
Details/additional comments:
- Among those who performed the task, 41% reported "no difficulty at all"
- Item well represented by other items (correlation 0.7) remaining in factor 1
- Item difficult to interpret in COPD patients: "I didn't do this" means both severe problems to do, or not willing to do so
How much time did you need to recover from your physical activities today?
Redundancy
Details/additional comments:
- Redundant in Rasch analysis
o infit <0.8
o outfit <0.7
- Item well represented by others remaining in factor 1, in adaptations/planning and symptoms
- In cognitive debriefings, item not well understood by some patients
How often did you have to pace yourself during your physical activities today?
Redundancy
Details/additional comments:
- Redundant in Rasch analysis
o infit <0.8
o outfit <0.7
- Item well represented by others (r>0.75) remaining in factor 1
- In patients’ interviews and focus groups: item not identified by the patients; the exact wording of pacing was not used by the patients, who rather used words like doing things slower
Online Data Supplement 41
How breathless were you when walking on level ground indoors and outdoors today?
Redundancy
Details/additional comments:
- Redundant in Rasch analysis
o infit <0.8
o outfit <0.7
- Highly correlated (>0.7) with other symptoms (breathless, tiredness) and adaptations remaining in factor 1
- Experts’ opinion: Question is complex: "How breathless were you when walking on level ground indoors and outdoors today?"
- In cognitive debriefings the question (originally phrased shorter) was not well understood, and it was rephrased to an even longer sentence
How often did you have to slow down while walking today?
Redundancy
Details/additional comments:
- Redundant in Rasch analysis
o infit <0.8
o outfit <0.7
- Highly correlated with taking breaks, which remains in factor 1
- In patients’ interviews and focus groups, item reported together with taking breaks, which is kept
- Experts: one of the first problems noted by patients according to clinical experts, but could be primarily relevant for milder patients. Taking breaks is considered a clearer item since it does not have an implicit reference in terms of slowing down from what (e.g., from fast, from “normal” pace...)
How often did you lack physical strength to do things because of your lung problems today?
Redundancy
Details/additional comments:
- Redundant in Rasch analysis
o infit <0.8

Online Data Supplement 42
o outfit <0.7
- Highly correlated (>0.7) with items that remain in factor 1
- In patients’ interviews and focus groups, item considered as low priority
Clinical visit version of PROactive Physical Activity in COPD (C-PPAC) instrument
Factor 1 “Amount of physical activity”
Item/variable Reasons for removal
FROM PRO
In the past 7 days, how often did you exercise to maintain or improve your physical condition?
Not fitting well with the rest of the items + no proper ordering
Details/additional comments:
- Item not fitting well with the rest of the items:
o EFA loading <0.3
o item-to-total correlation <0.5
o inter-item correlation <0.2
o outfit >1.3
o infit >1.2
- Not ordering well in Rasch analysis
In the past 7 days, how much physical leisure activity did you do?
Not fitting well with the rest of the items + no proper ordering
Details/additional comments:
- Item not fitting well with the rest of the items:
o EFA loading <0.3
o outfit close to 1.3
o infit close to 1.2
- In Rasch analysis, item does not order well in person item map.
In the past 7 days, how many chores did you do inside the
Not fitting well with the rest of the items + differential item functioning by gender
Details/additional comments:
Online Data Supplement 43
house? - Item not fitting well with the rest of the items:
o EFA loading <0.3
o outfit close to 1.3
o infit close to 1.2
- Item exhibits differential item functioning by genders
- In patients interviews and focus groups, item reported by few percentage of patients
- In patients interviews and focus groups, item revealed differences between genders, which could make the item not applicable to men
- In cognitive debriefings, male not understanding the item (“it applies to females”, while actually it was “mending things”)
FROM DYNAPORT
Intensity Not fitting well with the rest of the items
Details/additional comments:
- Item not fitting well with the rest of the items:
o outfit >1.3
o infit >1.2
o other criteria at the limit
Standing time Not fitting well with the rest of the items
Details/additional comments:
- Item not fitting well with the rest of the items:
o infit >1.2
o outfit >1.3
o all other criteria at the limit
- Item exhibits differential item functioning between genders
- In experimental studies, variable not well related to double labelled water (Rabinovich R. ERJ 2013)
Online Data Supplement 44
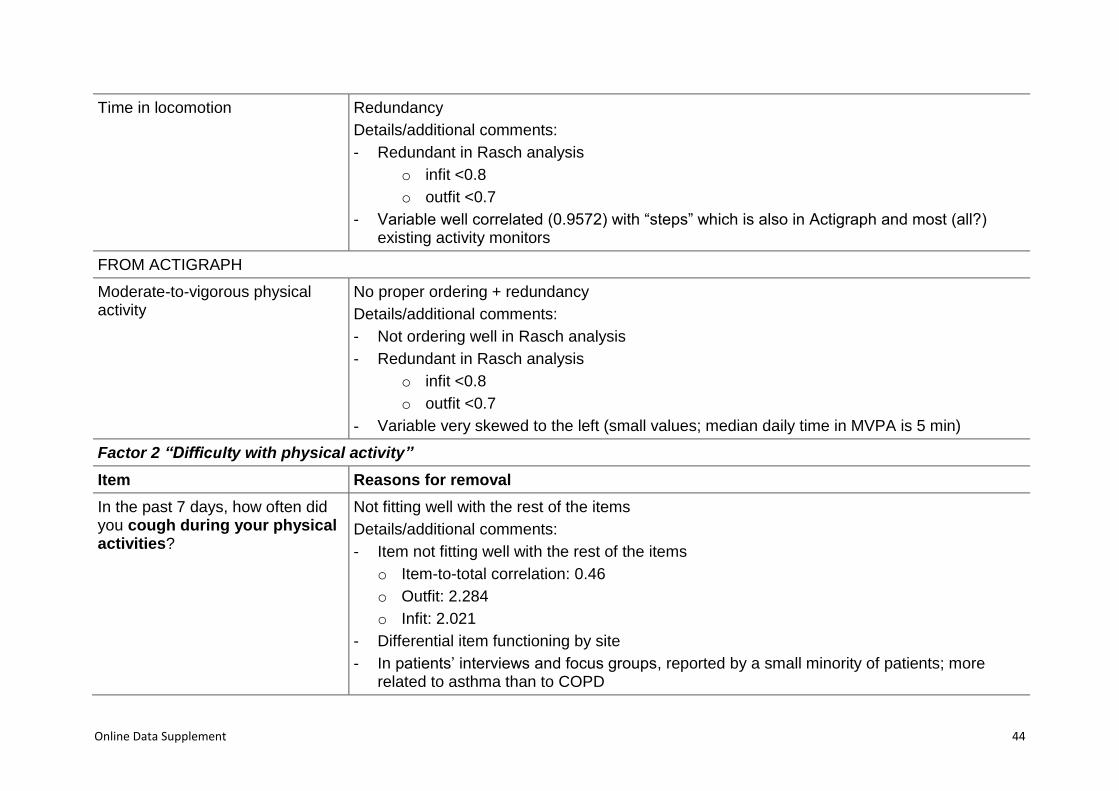
Time in locomotion Redundancy
Details/additional comments:
- Redundant in Rasch analysis
o infit <0.8
o outfit <0.7
- Variable well correlated (0.9572) with “steps” which is also in Actigraph and most (all?) existing activity monitors
FROM ACTIGRAPH
Moderate-to-vigorous physical activity
No proper ordering + redundancy
Details/additional comments:
- Not ordering well in Rasch analysis
- Redundant in Rasch analysis
o infit <0.8
o outfit <0.7
- Variable very skewed to the left (small values; median daily time in MVPA is 5 min)
Factor 2 “Difficulty with physical activity”
Item Reasons for removal
In the past 7 days, how often did you cough during your physical activities?
Not fitting well with the rest of the items
Details/additional comments:
- Item not fitting well with the rest of the items
o Item-to-total correlation: 0.46
o Outfit: 2.284
o Infit: 2.021
- Differential item functioning by site
- In patients’ interviews and focus groups, reported by a small minority of patients; more related to asthma than to COPD
Online Data Supplement 45
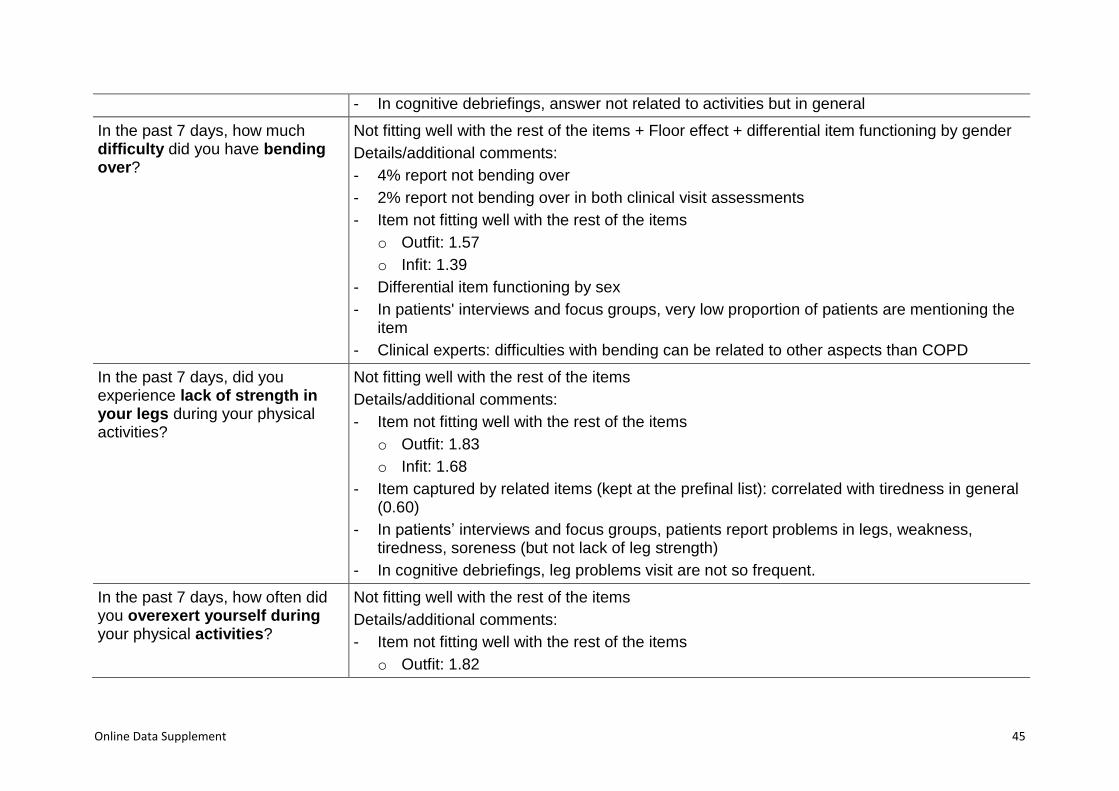
- In cognitive debriefings, answer not related to activities but in general
In the past 7 days, how much difficulty did you have bending over?
Not fitting well with the rest of the items + Floor effect + differential item functioning by gender
Details/additional comments:
- 4% report not bending over
- 2% report not bending over in both clinical visit assessments
- Item not fitting well with the rest of the items
o Outfit: 1.57
o Infit: 1.39
- Differential item functioning by sex
- In patients' interviews and focus groups, very low proportion of patients are mentioning the item
- Clinical experts: difficulties with bending can be related to other aspects than COPD
In the past 7 days, did you experience lack of strength in your legs during your physical activities?
Not fitting well with the rest of the items
Details/additional comments:
- Item not fitting well with the rest of the items
o Outfit: 1.83
o Infit: 1.68
- Item captured by related items (kept at the prefinal list): correlated with tiredness in general (0.60)
- In patients’ interviews and focus groups, patients report problems in legs, weakness, tiredness, soreness (but not lack of leg strength)
- In cognitive debriefings, leg problems visit are not so frequent.
In the past 7 days, how often did you overexert yourself during your physical activities?
Not fitting well with the rest of the items
Details/additional comments:
- Item not fitting well with the rest of the items
o Outfit: 1.82

Online Data Supplement 46
o Infit: 1.67
- In cognitive debriefing, item phrased as “overdo” and not well understood
- Clinical experts: difficult interpretation, patient may be avoiding it
In the past 7 days, did your lung problems prevent you from doing activities that you needed to do?
Redundancy + no proper ordering
Details/additional comments:
- Redundant in Rasch analysis
o infit <0.8
o outfit <0.7
- Item captured by related items (kept on prefinal list): correlated with avoid doing activities (0.79), lack physical strength (0.79).
- In patients’ interviews and focus groups, item mentioned together with other remaining items
In the past 7 days, how much difficulty did you have carrying objects?
Not fitting well with the rest of the items + differential item functioning by site + interpretation problems
Details/additional comments:
- 8% report not carrying things.
- 4% report not carrying things in both clinical visit assessments.
- Item not fitting well with the rest of the items
o Infit: 1.27
- Differential item functioning by site
- In patients’ interviews and focus groups, low percentage of quotes
- In cognitive debriefings, item not well understood
In the past 7 days, how much difficulty did you have when hurrying?
Not fitting well with the rest of the items + interpretation problems
Details/additional comments:
- 32% report not hurrying.
- 21% report not hurrying in both clinical visit assessments.
Online Data Supplement 47
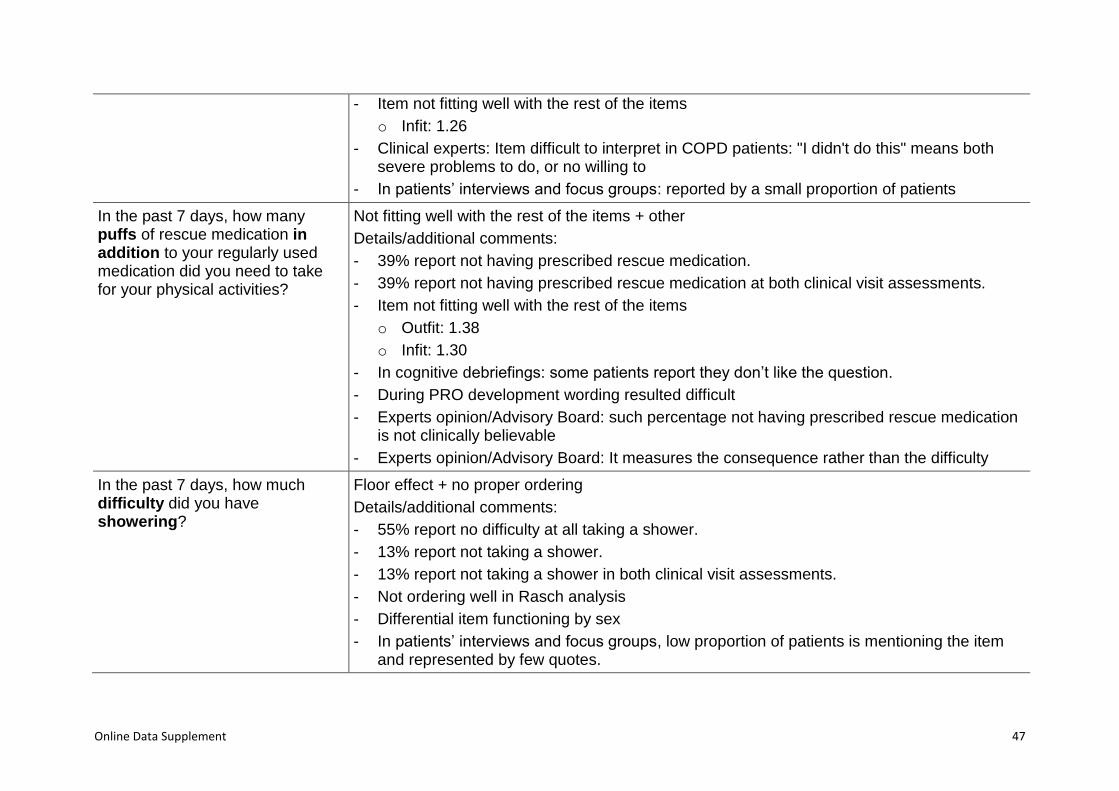
- Item not fitting well with the rest of the items
o Infit: 1.26
- Clinical experts: Item difficult to interpret in COPD patients: "I didn't do this" means both severe problems to do, or no willing to
- In patients’ interviews and focus groups: reported by a small proportion of patients
In the past 7 days, how many puffs of rescue medication in addition to your regularly used medication did you need to take for your physical activities?
Not fitting well with the rest of the items + other
Details/additional comments:
- 39% report not having prescribed rescue medication.
- 39% report not having prescribed rescue medication at both clinical visit assessments.
- Item not fitting well with the rest of the items
o Outfit: 1.38
o Infit: 1.30
- In cognitive debriefings: some patients report they don’t like the question.
- During PRO development wording resulted difficult
- Experts opinion/Advisory Board: such percentage not having prescribed rescue medication is not clinically believable
- Experts opinion/Advisory Board: It measures the consequence rather than the difficulty
In the past 7 days, how much difficulty did you have showering?
Floor effect + no proper ordering
Details/additional comments:
- 55% report no difficulty at all taking a shower.
- 13% report not taking a shower.
- 13% report not taking a shower in both clinical visit assessments.
- Not ordering well in Rasch analysis
- Differential item functioning by sex
- In patients’ interviews and focus groups, low proportion of patients is mentioning the item and represented by few quotes.

Online Data Supplement 48
In the past 7 days, how much difficulty did you have bathing?
Floor effect + no proper ordering
Details/additional comments:
- 58% report no difficulty at all taking a bath.
- 46% report not taking a bath.
- 45% report not taking a bath in both clinical visit assessments.
- Not ordering well in Rasch analysis
- In patients’ interviews and focus groups, low proportion of patients is mentioning the item and represented by few quotes.
In the past 7 days, how often did you use aids to facilitate your physical activities?
Floor effect + no proper ordering
Details/additional comments:
- 76% report never use aids.
- Not ordering well in Rasch analysis
- Item not fitting well with the rest of the items
o Outfit: 2.87
o Infit: 1.88
- Differential item functioning by site
- In cognitive debriefings, items exhibits several different interpretations by patients
In the past 7 days, how much difficulty did you have washing yourself?
Floor effect + no proper ordering
Details/additional comments:
- 62% report no difficulty at all washing.
- Not ordering well in Rasch analysis.
- Differential item functioning by sex
- In patients’ interviews and focus groups, item reported together with dressing.
In the past 7 days, how much help from others did you need with any of your activities?
Floor effect + differential item functioning by site
Details/additional comments:
- 52% report no help at all (floor effect)
Online Data Supplement 49
- Differential item functioning by site
- In patients’ interviews and focus groups, item reported together with dressing (which is kept).
- In cognitive debriefings, item difficult to understand
In the past 7 days, how much difficulty did you have climbing stairs?
No proper ordering
Details/additional comments:
- 8% report not climbing stairs.
- 4% report not climbing stairs in both clinical visit assessments.
- Item not fitting well with the rest of the items
o Infit: 1.25
- Not ordering well in Rasch analysis.
- Differential item functioning by site
- In cognitive debriefings, item not applicable for patients who have no stairs at home
- Clinical experts: the item is clinically relevant, but, if removed, the theme still captured by related items (kept on prefinal list): correlated with breathlessness on level (0.65), avoid doing activities (0.60) and time to recover (0.60)
In the past 7 days, did you need to spread your activities throughout the day because of your lung problems?
No proper ordering
Details/additional comments:
- Not ordering well in Rasch analysis.
- Experts: could be relevant but may be something that rather is gradually changing and not noted by patients.
In the past 7 days, how often did you have to pace yourself during your physical activities?
Redundancy
Details/additional comments:
- Redundant in Rasch analysis
o infit <0.8
o outfit <0.7
- Item not found in WP2b docs because the exact wording of ‘pacing’ was not used by the
Online Data Supplement 50
patients, who rather used words like ‘doing things slower’.
- Item captured by related items (kept on prefinal list): correlated with difficulty getting out and about (0.63), avoid doing activities (0.66), breathlessness in general (0.67), lack of physical strength (0.69), tiredness in general (0.67), have to take breaks (0.82), breathlessness on level (0.67), time to recover (0.68), and need to consider lung problems (0.70)
In the past 7 days, how often did you have to slow down while walking?
Redundancy
Details/additional comments:
- Redundant in Rasch analysis
o infit <0.8
o outfit <0.7
- Differential item functioning by sex
- In patients’ interviews and focus groups, item reported together with break, which is kept
- Experts: this item captures one of the first problems noted by patients but difficult to capture in a question. Taking breaks is considered a clearer item since it does not have an implicit reference in terms of slowing down from what (e.g., from fast, from “normal” pace...)
- Item captured by related items (kept on prefinal list): correlated with difficulty getting out and about (0.64), avoid doing activities (0.65), breathlessness in general (0.70), lack of physical strength (0.68), tiredness in general (0.62), have to take breaks (0.75), breathlessness on level (0.75), time to recover (0.68), and need to consider lung problems (0.68)
In the past 7 days, did your lung problems stop you from doing the physical activities that you wanted to do?
Redundancy
Details/additional comments:
- Redundant in Rasch analysis
o infit <0.8
o outfit <0.7
- Item captured by related items (kept on prefinal list): correlated with difficulty getting out and about (0.63), avoid doing activities (0.79), breathlessness in general (0.65), lack of physical strength (0.79), tiredness in general (0.60), have to take breaks (0.66), breathlessness on level (0.67), time to recover (0.61), and need to consider lung problems (0.67)
Online Data Supplement 51
- In patients’ interviews and focus groups, problems in interpretation by patients, because they adapt what they do to what they can do
In the past 7 days, how breathless were you when climbing stairs?
Other: differential item functioning by sites
Details/additional comments:
- 8% report not climbing stairs.
- 4% report not climbing stairs in both clinical visit assessments.
- Differential item functioning by site
- In cognitive debriefings, item not applicable for patients who have no stairs at home
- Clinical experts: the item is relevant because is the first symptom reported by patients. If removed, the theme is still captured by related items (kept on prefinal list): correlated with avoid doing activities (0.64), breathlessness in general (0.68), lack of physical strength (0.66), have to take breaks (0.63), breathlessness on level (0.73), time to recover (0.65), and need to consider lung problems (0.61)
In the past 7 days, how much difficulty did you have walking up a small slope?
Interpretation problems
Details/additional comments:
- 19% report no walking slope
- 9% report no walking slope in both clinical visit assessments
- In patients' interviews and focus groups: only patients from Athens and Edinburgh reported it as important.
- PRO experts: Experience from other PRO developments/translations (e.g., with the CAT) that this is a difficult item to translate
- Item well represented by others remaining in the final factor 1: correlated with breathlessness in general (0.63), lack of physical strength (0.60), have to take breaks (0.60), and breathlessness on level (0.61)

Online Data Supplement 52
Table E6. Confirmatory factor analysis results of Daily and Clinical visit versions of PROactive Physical Activity in COPD
instruments (D-PPAC and C-PPAC, respectively)
D-PPAC combined with
Dynaport (n=179) combined with
Actigraph (n=156) C-PPAC
combined with Dynaport (n=199)
combined with Actigraph (n=156)
Items Factor loadings Factor loadings
Items Factor loadings Factor loadings
Factor 1 Factor 2 Factor 1 Factor 2 Factor 1 Factor 2 Factor 1 Factor 2
Walking outside 0.51 0.52 Walking outside 0.62 0.62
Chores outside 0.41 0.39 Chores outside 0.62 0.66
Steps 0.89 0.88 Steps 0.66 0.73
Vector magnitude units 0.90 0.93 Vector magnitude units 0.73 0.61
Difficulty getting dressed 0.71 0.66 Difficulty getting dressed 0.71 0.71
Avoid activities 0.81 0.76 Difficulty getting out 0.77 0.78
Breathless in general 0.90 0.93 Avoid activities 0.83 0.83
Tired in general 0.83 0.82 Breathless in general 0.87 0.86
Take breaks 0.90 0.90 Lack physical strength 0.80 0.81
Tired in general 0.70 0.70
Take breaks 0.76 0.75
Breathless walking 0.81 0.79
Time to recover 0.82 0.79
Consider lung problems 0.77 0.78
Goodness of fit
RMSEA 0.055 0.043
Goodness of fit
RMSEA 0.035 0.038
CFI 0.987 0.992 CFI 0.992 0.989
NNFI 0.979 0.986 NNFI 0.988 0.984
SRMR 0.040 0.046 SRMR 0.035 0.033
D-PPAC: Daily version of PROactive Physical Activity in COPD instrument; C-PPAC: Clinical visit version of PROactive Physical Activity in COPD instrument;
RMSEA: root mean square error of approximation; CFI: comparative fit index; NNFI: non-normed fit index; SRMR: standardized root mean square residual.

Online Data Supplement 53
Table E7. Performance of items from factor 1 (‘amount’) without variables from the activity monitors, comparing with performance
with final factor 1 (2 items from PRO + 2 variables from the activity monitor (Dynaport)).
Flo
or
eff
ec
t
Ceil
ing
eff
ec
t
Ite
m t
o t
ota
l co
rrela
tio
n
Inte
r-it
em
co
rrela
tio
n
No
t p
rop
er
ord
eri
ng
of
ca
teg
ori
es
Ou
tfit
Infi
t
Pe
rso
n S
ep
ara
tio
n In
dex
Ex
plo
rato
ry f
ac
tor
an
aly
sis
:
fac
tor
load
ing
Ex
plo
rato
ry f
ac
tor
an
aly
sis
:
pro
po
rtio
n v
ari
an
ce
Dif
fere
nti
al It
em
Fu
nc
tio
nin
g
Daily version (factor 1)
Items from the PRO only
How much walking did you do outside today? 0.79 0.35 0.54 0.54
0.59
0.99
0.37
How many chores did you do inside the house today? 0.47 0.07 1.19 1.14 <0.1 X
How many chores did you do outside the house today? 0.72 0.29 0.69 0.71 0.58
How much physical leisure activity did you do today? 55 0.61 0.20 X 0.69 0.77 0.38
2 final items from the PRO + 2 final variables from Dynaport monitor
How much walking did you do outside today? 0.84 0.59 0.79 0.79
0.83
0.69
0.58
How many chores did you do outside the house today? 0.73 0.46 1.10 1.13 0.49
Steps (total daily) 0.85 0.60 0.63 0.62 0.89
VMU (mean vmu/min) 0.86 0.61 0.53 0.56 0.90
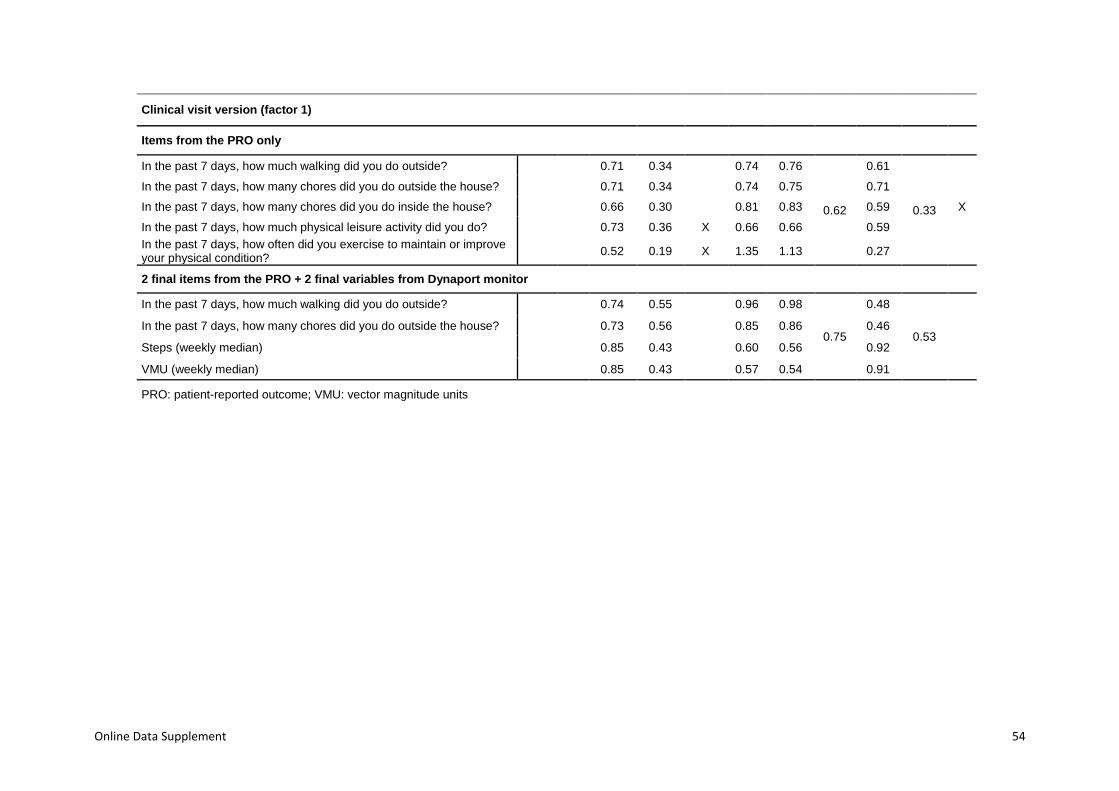
Online Data Supplement 54
Clinical visit version (factor 1)
Items from the PRO only
In the past 7 days, how much walking did you do outside? 0.71 0.34 0.74 0.76
0.62
0.61
0.33
In the past 7 days, how many chores did you do outside the house? 0.71 0.34 0.74 0.75 0.71
In the past 7 days, how many chores did you do inside the house? 0.66 0.30 0.81 0.83 0.59 X
In the past 7 days, how much physical leisure activity did you do? 0.73 0.36 X 0.66 0.66 0.59
In the past 7 days, how often did you exercise to maintain or improve your physical condition?
0.52 0.19 X 1.35 1.13 0.27
2 final items from the PRO + 2 final variables from Dynaport monitor
In the past 7 days, how much walking did you do outside? 0.74 0.55 0.96 0.98
0.75
0.48
0.53
In the past 7 days, how many chores did you do outside the house? 0.73 0.56 0.85 0.86 0.46
Steps (weekly median) 0.85 0.43 0.60 0.56 0.92
VMU (weekly median) 0.85 0.43 0.57 0.54 0.91
PRO: patient-reported outcome; VMU: vector magnitude units
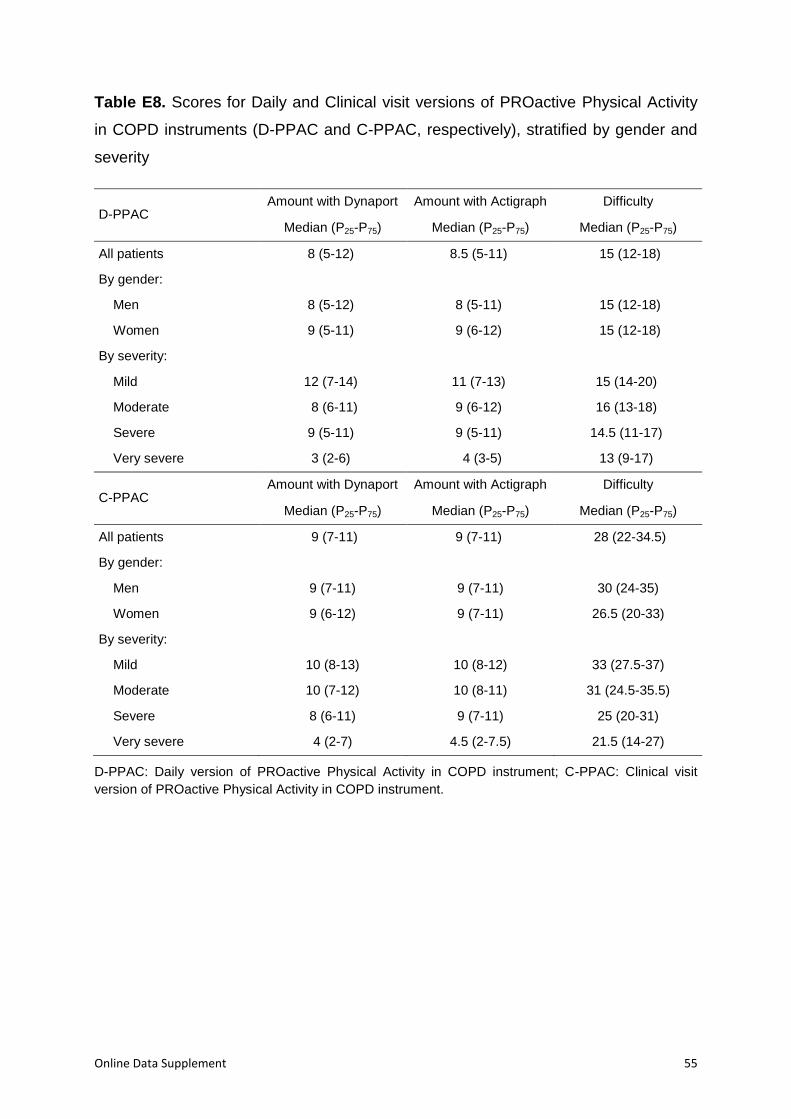
Online Data Supplement 55
Table E8. Scores for Daily and Clinical visit versions of PROactive Physical Activity
in COPD instruments (D-PPAC and C-PPAC, respectively), stratified by gender and
severity
D-PPAC Amount with Dynaport Amount with Actigraph Difficulty
Median (P25-P75) Median (P25-P75) Median (P25-P75)
All patients 8 (5-12) 8.5 (5-11) 15 (12-18)
By gender:
Men 8 (5-12) 8 (5-11) 15 (12-18)
Women 9 (5-11) 9 (6-12) 15 (12-18)
By severity:
Mild 12 (7-14) 11 (7-13) 15 (14-20)
Moderate 8 (6-11) 9 (6-12) 16 (13-18)
Severe 9 (5-11) 9 (5-11) 14.5 (11-17)
Very severe 3 (2-6) 4 (3-5) 13 (9-17)
C-PPAC Amount with Dynaport Amount with Actigraph Difficulty
Median (P25-P75) Median (P25-P75) Median (P25-P75)
All patients 9 (7-11) 9 (7-11) 28 (22-34.5)
By gender:
Men 9 (7-11) 9 (7-11) 30 (24-35)
Women 9 (6-12) 9 (7-11) 26.5 (20-33)
By severity:
Mild 10 (8-13) 10 (8-12) 33 (27.5-37)
Moderate 10 (7-12) 10 (8-11) 31 (24.5-35.5)
Severe 8 (6-11) 9 (7-11) 25 (20-31)
Very severe 4 (2-7) 4.5 (2-7.5) 21.5 (14-27)
D-PPAC: Daily version of PROactive Physical Activity in COPD instrument; C-PPAC: Clinical visit
version of PROactive Physical Activity in COPD instrument.
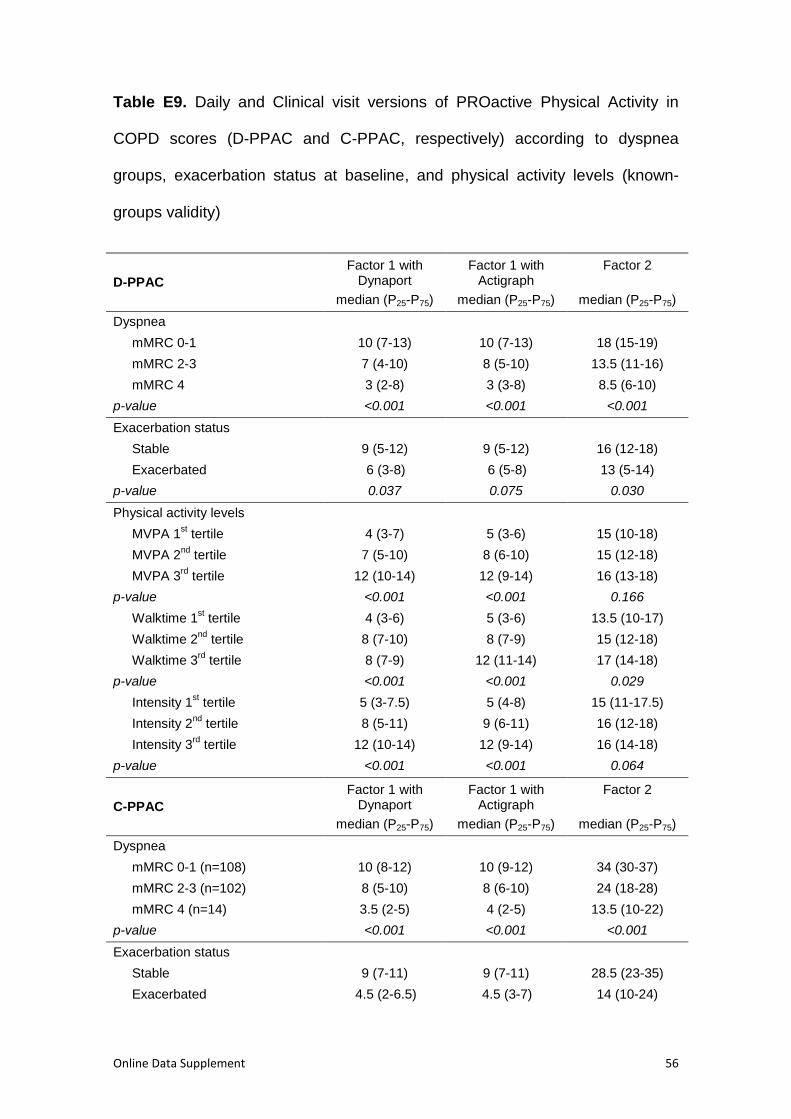
Online Data Supplement 56
Table E9. Daily and Clinical visit versions of PROactive Physical Activity in
COPD scores (D-PPAC and C-PPAC, respectively) according to dyspnea
groups, exacerbation status at baseline, and physical activity levels (known-
groups validity)
D-PPAC
Factor 1 with Dynaport
median (P25-P75)
Factor 1 with Actigraph
median (P25-P75)
Factor 2 XXXXXXX
median (P25-P75)
Dyspnea
mMRC 0-1 10 (7-13) 10 (7-13) 18 (15-19)
mMRC 2-3 7 (4-10) 8 (5-10) 13.5 (11-16)
mMRC 4 3 (2-8) 3 (3-8) 8.5 (6-10)
p-value <0.001 <0.001 <0.001
Exacerbation status
Stable 9 (5-12) 9 (5-12) 16 (12-18)
Exacerbated 6 (3-8) 6 (5-8) 13 (5-14)
p-value 0.037 0.075 0.030
Physical activity levels
MVPA 1st tertile 4 (3-7) 5 (3-6) 15 (10-18)
MVPA 2nd
tertile 7 (5-10) 8 (6-10) 15 (12-18)
MVPA 3rd
tertile 12 (10-14) 12 (9-14) 16 (13-18)
p-value <0.001 <0.001 0.166
Walktime 1st tertile 4 (3-6) 5 (3-6) 13.5 (10-17)
Walktime 2nd
tertile 8 (7-10) 8 (7-9) 15 (12-18)
Walktime 3rd
tertile 8 (7-9) 12 (11-14) 17 (14-18)
p-value <0.001 <0.001 0.029
Intensity 1st tertile 5 (3-7.5) 5 (4-8) 15 (11-17.5)
Intensity 2nd
tertile 8 (5-11) 9 (6-11) 16 (12-18)
Intensity 3rd
tertile 12 (10-14) 12 (9-14) 16 (14-18)
p-value <0.001 <0.001 0.064
C-PPAC
Factor 1 with Dynaport
median (P25-P75)
Factor 1 with Actigraph
median (P25-P75)
Factor 2 XXXXXXX
median (P25-P75)
Dyspnea
mMRC 0-1 (n=108) 10 (8-12) 10 (9-12) 34 (30-37)
mMRC 2-3 (n=102) 8 (5-10) 8 (6-10) 24 (18-28)
mMRC 4 (n=14) 3.5 (2-5) 4 (2-5) 13.5 (10-22)
p-value <0.001 <0.001 <0.001
Exacerbation status
Stable 9 (7-11) 9 (7-11) 28.5 (23-35)
Exacerbated 4.5 (2-6.5) 4.5 (3-7) 14 (10-24)
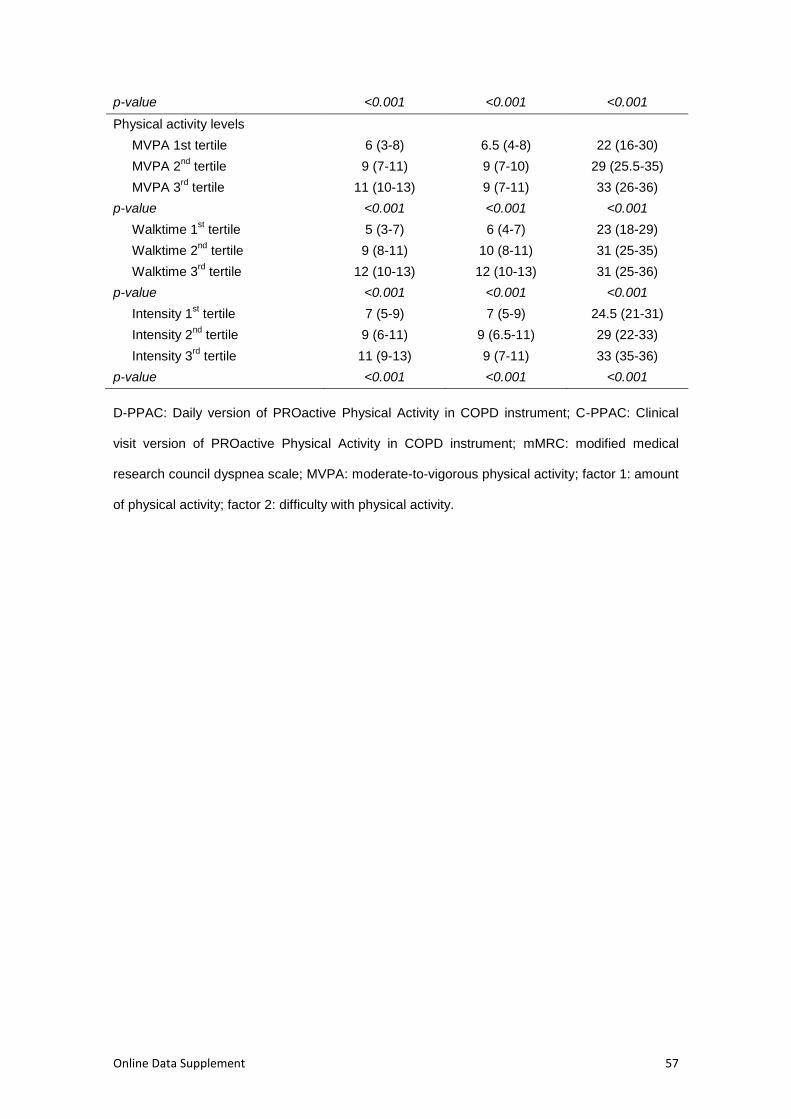
Online Data Supplement 57
p-value <0.001 <0.001 <0.001
Physical activity levels
MVPA 1st tertile 6 (3-8) 6.5 (4-8) 22 (16-30)
MVPA 2nd
tertile 9 (7-11) 9 (7-10) 29 (25.5-35)
MVPA 3rd
tertile 11 (10-13) 9 (7-11) 33 (26-36)
p-value <0.001 <0.001 <0.001
Walktime 1st tertile 5 (3-7) 6 (4-7) 23 (18-29)
Walktime 2nd
tertile 9 (8-11) 10 (8-11) 31 (25-35)
Walktime 3rd
tertile 12 (10-13) 12 (10-13) 31 (25-36)
p-value <0.001 <0.001 <0.001
Intensity 1st tertile 7 (5-9) 7 (5-9) 24.5 (21-31)
Intensity 2nd
tertile 9 (6-11) 9 (6.5-11) 29 (22-33)
Intensity 3rd
tertile 11 (9-13) 9 (7-11) 33 (35-36)
p-value <0.001 <0.001 <0.001
D-PPAC: Daily version of PROactive Physical Activity in COPD instrument; C-PPAC: Clinical
visit version of PROactive Physical Activity in COPD instrument; mMRC: modified medical
research council dyspnea scale; MVPA: moderate-to-vigorous physical activity; factor 1: amount
of physical activity; factor 2: difficulty with physical activity.
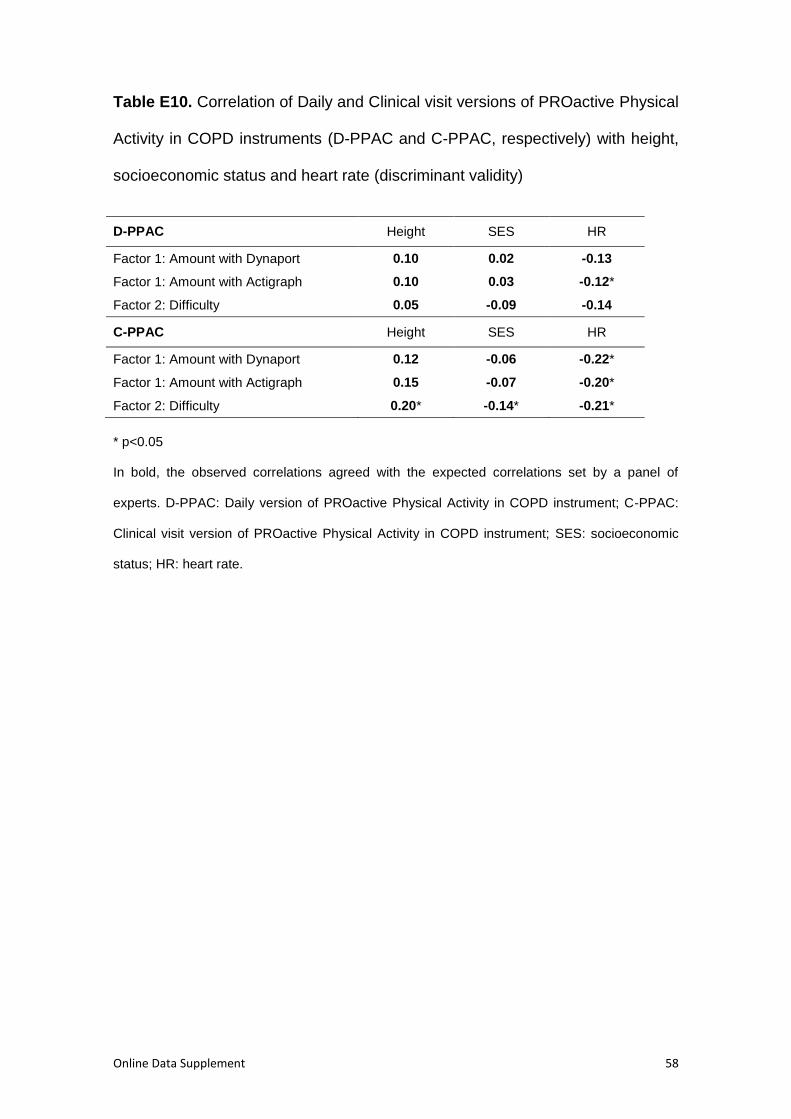
Online Data Supplement 58
Table E10. Correlation of Daily and Clinical visit versions of PROactive Physical
Activity in COPD instruments (D-PPAC and C-PPAC, respectively) with height,
socioeconomic status and heart rate (discriminant validity)
D-PPAC Height SES HR
Factor 1: Amount with Dynaport 0.10 0.02 -0.13
Factor 1: Amount with Actigraph 0.10 0.03 -0.12*
Factor 2: Difficulty 0.05 -0.09 -0.14
C-PPAC Height SES HR
Factor 1: Amount with Dynaport 0.12 -0.06 -0.22*
Factor 1: Amount with Actigraph 0.15 -0.07 -0.20*
Factor 2: Difficulty 0.20* -0.14* -0.21*
* p<0.05
In bold, the observed correlations agreed with the expected correlations set by a panel of
experts. D-PPAC: Daily version of PROactive Physical Activity in COPD instrument; C-PPAC:
Clinical visit version of PROactive Physical Activity in COPD instrument; SES: socioeconomic
status; HR: heart rate.
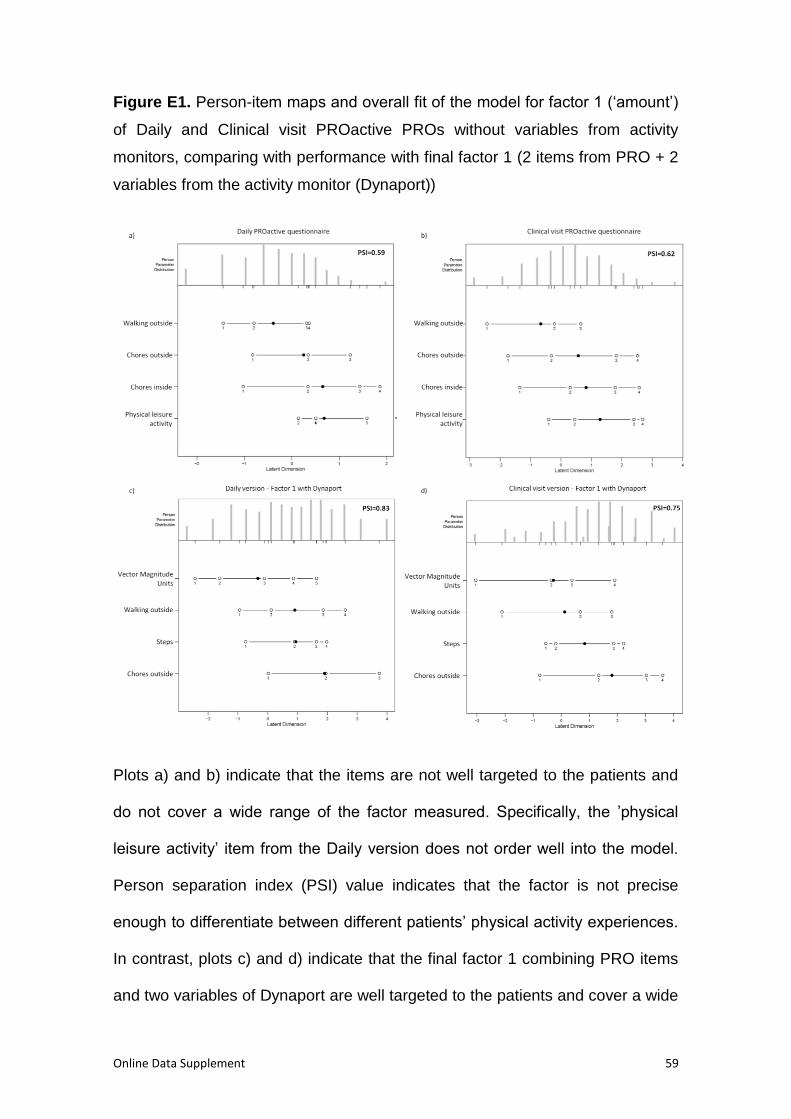
Online Data Supplement 59
Figure E1. Person-item maps and overall fit of the model for factor 1 (‘amount’)
of Daily and Clinical visit PROactive PROs without variables from activity
monitors, comparing with performance with final factor 1 (2 items from PRO + 2
variables from the activity monitor (Dynaport))
Plots a) and b) indicate that the items are not well targeted to the patients and
do not cover a wide range of the factor measured. Specifically, the ’physical
leisure activity’ item from the Daily version does not order well into the model.
Person separation index (PSI) value indicates that the factor is not precise
enough to differentiate between different patients’ physical activity experiences.
In contrast, plots c) and d) indicate that the final factor 1 combining PRO items
and two variables of Dynaport are well targeted to the patients and cover a wide

Online Data Supplement 60
range of the factor measured. Person separation index (PSI) values indicate
that the factor is precise enough to differentiate between different patients’
physical activity experiences.
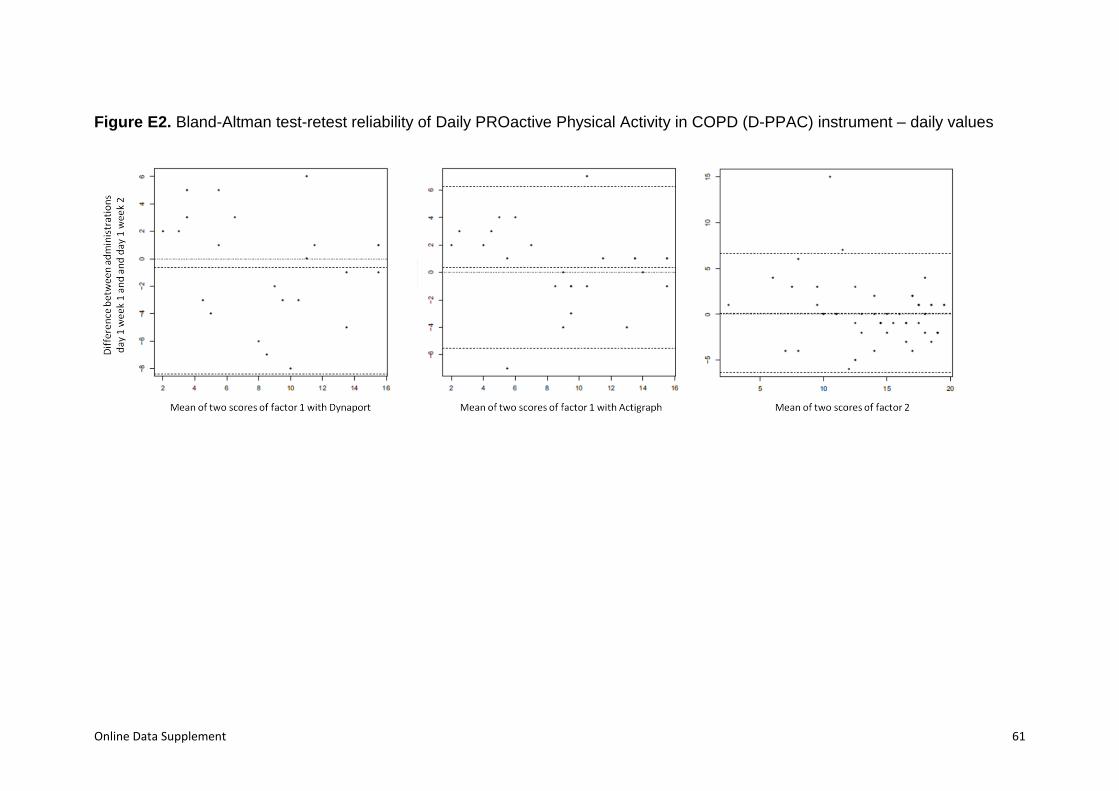
Online Data Supplement 61
Figure E2. Bland-Altman test-retest reliability of Daily PROactive Physical Activity in COPD (D-PPAC) instrument – daily values
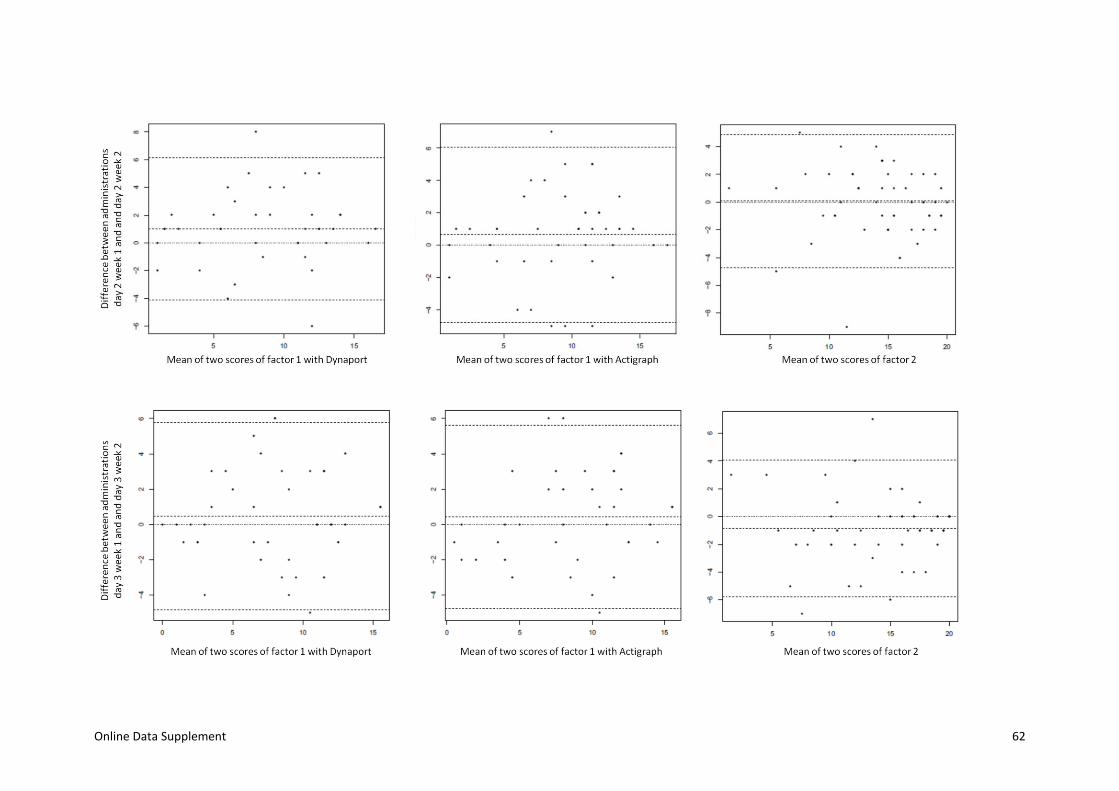
Online Data Supplement 62
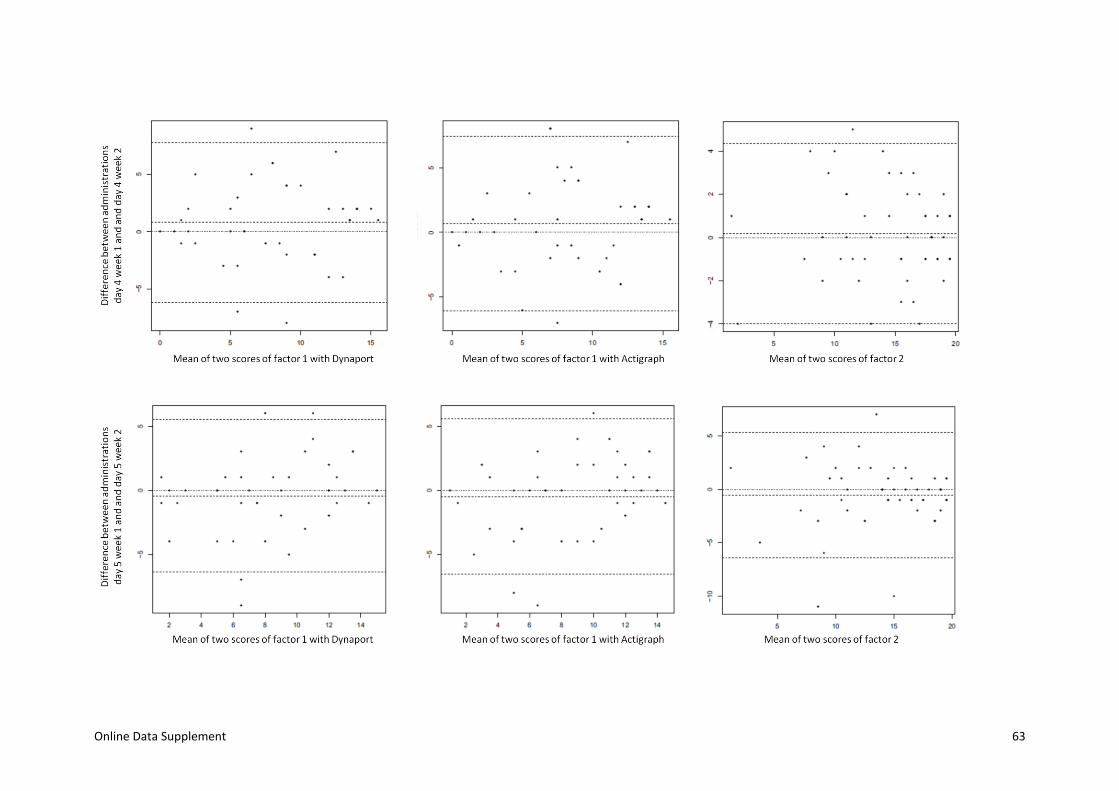
Online Data Supplement 63
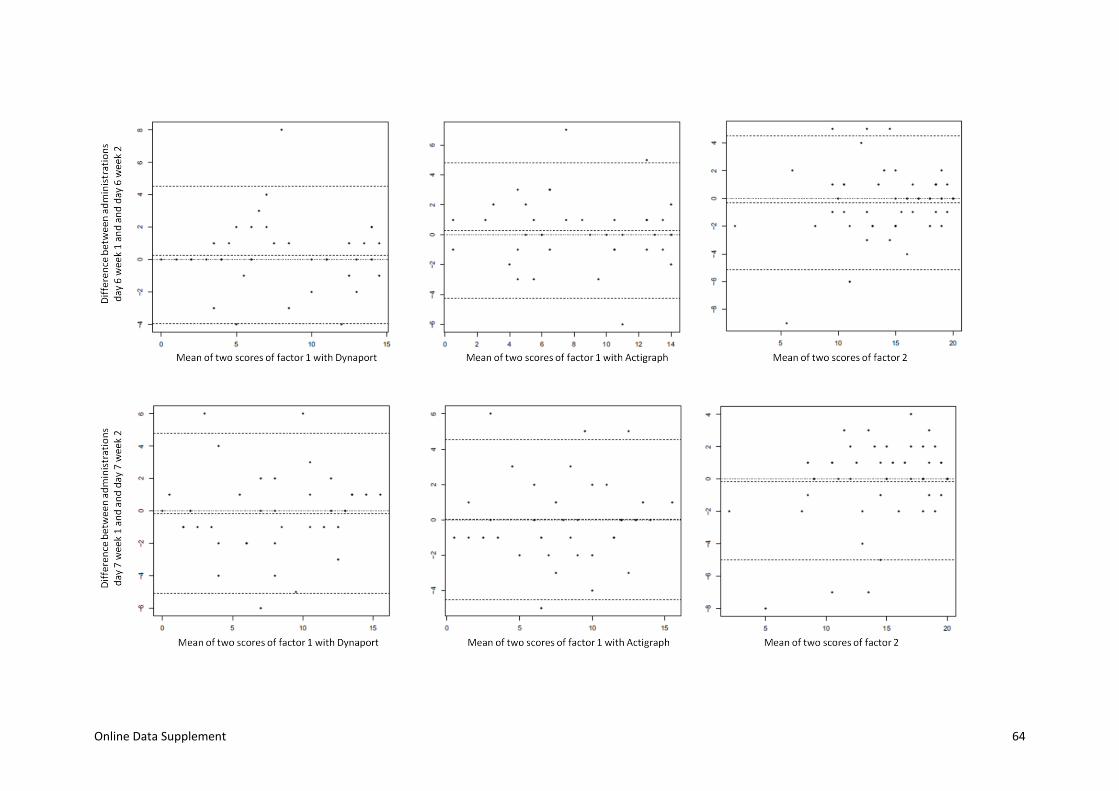
Online Data Supplement 64
Online Data Supplement 65
All Bland-Altman plots include a dotted line at value “0” and a dashed line at the value of the average of the difference. The dashed
extreme lines represent +/- 2SD. Factor 1 interpreted as ‘amount of physical activity’ and factor 2 as ‘difficulty with physical activity’.
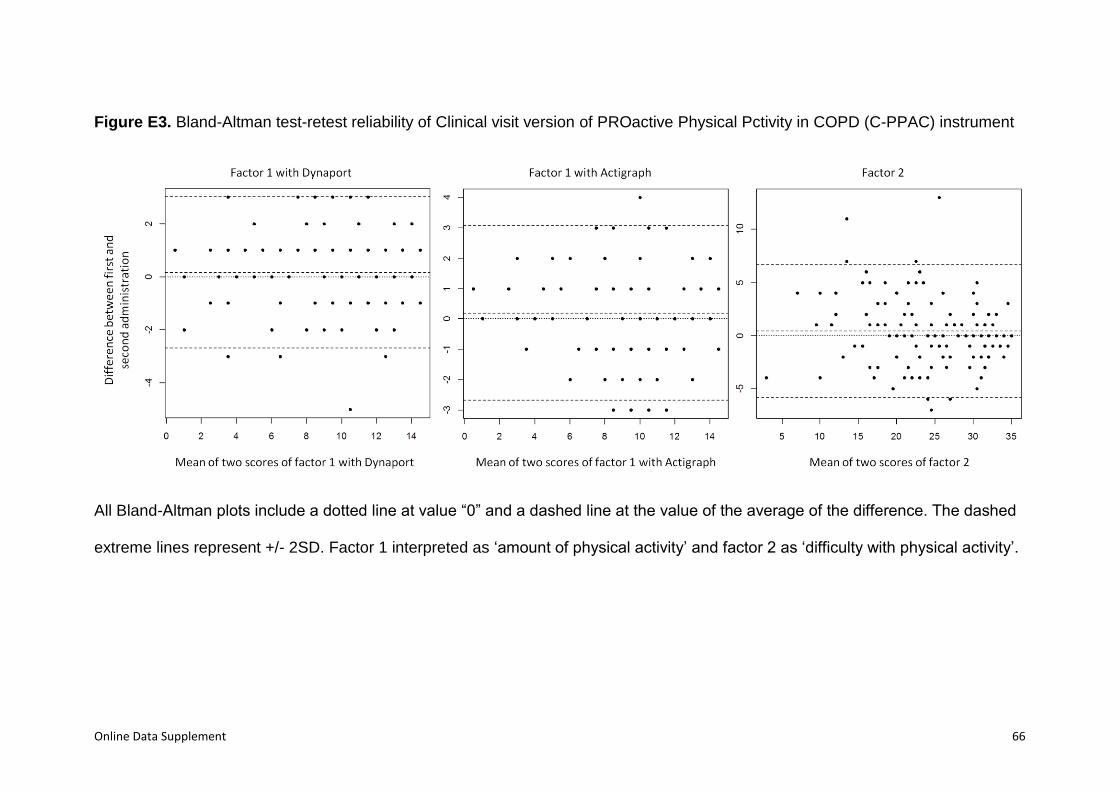
Online Data Supplement 66
Figure E3. Bland-Altman test-retest reliability of Clinical visit version of PROactive Physical Pctivity in COPD (C-PPAC) instrument
All Bland-Altman plots include a dotted line at value “0” and a dashed line at the value of the average of the difference. The dashed
extreme lines represent +/- 2SD. Factor 1 interpreted as ‘amount of physical activity’ and factor 2 as ‘difficulty with physical activity’.
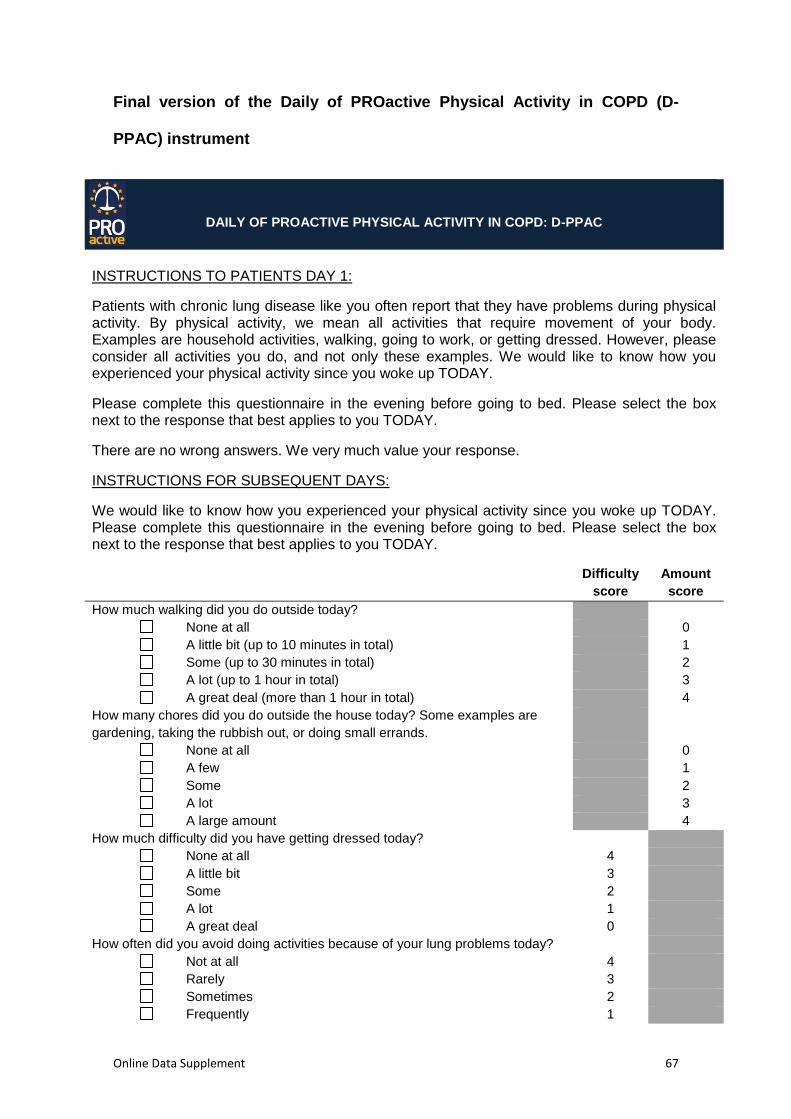
Online Data Supplement 67
Final version of the Daily of PROactive Physical Activity in COPD (D-
PPAC) instrument
DAILY OF PROACTIVE PHYSICAL ACTIVITY IN COPD: D-PPAC
INSTRUCTIONS TO PATIENTS DAY 1:
Patients with chronic lung disease like you often report that they have problems during physical activity. By physical activity, we mean all activities that require movement of your body. Examples are household activities, walking, going to work, or getting dressed. However, please consider all activities you do, and not only these examples. We would like to know how you experienced your physical activity since you woke up TODAY.
Please complete this questionnaire in the evening before going to bed. Please select the box next to the response that best applies to you TODAY.
There are no wrong answers. We very much value your response.
INSTRUCTIONS FOR SUBSEQUENT DAYS:
We would like to know how you experienced your physical activity since you woke up TODAY. Please complete this questionnaire in the evening before going to bed. Please select the box next to the response that best applies to you TODAY.
Difficulty
score
Amount
score
How much walking did you do outside today?
None at all 0
A little bit (up to 10 minutes in total) 1
Some (up to 30 minutes in total) 2
A lot (up to 1 hour in total) 3
A great deal (more than 1 hour in total) 4
How many chores did you do outside the house today? Some examples are
gardening, taking the rubbish out, or doing small errands.
None at all 0
A few 1
Some 2
A lot 3
A large amount 4
How much difficulty did you have getting dressed today?
None at all 4
A little bit 3
Some 2
A lot 1
A great deal 0
How often did you avoid doing activities because of your lung problems today?
Not at all 4
Rarely 3
Sometimes 2
Frequently 1
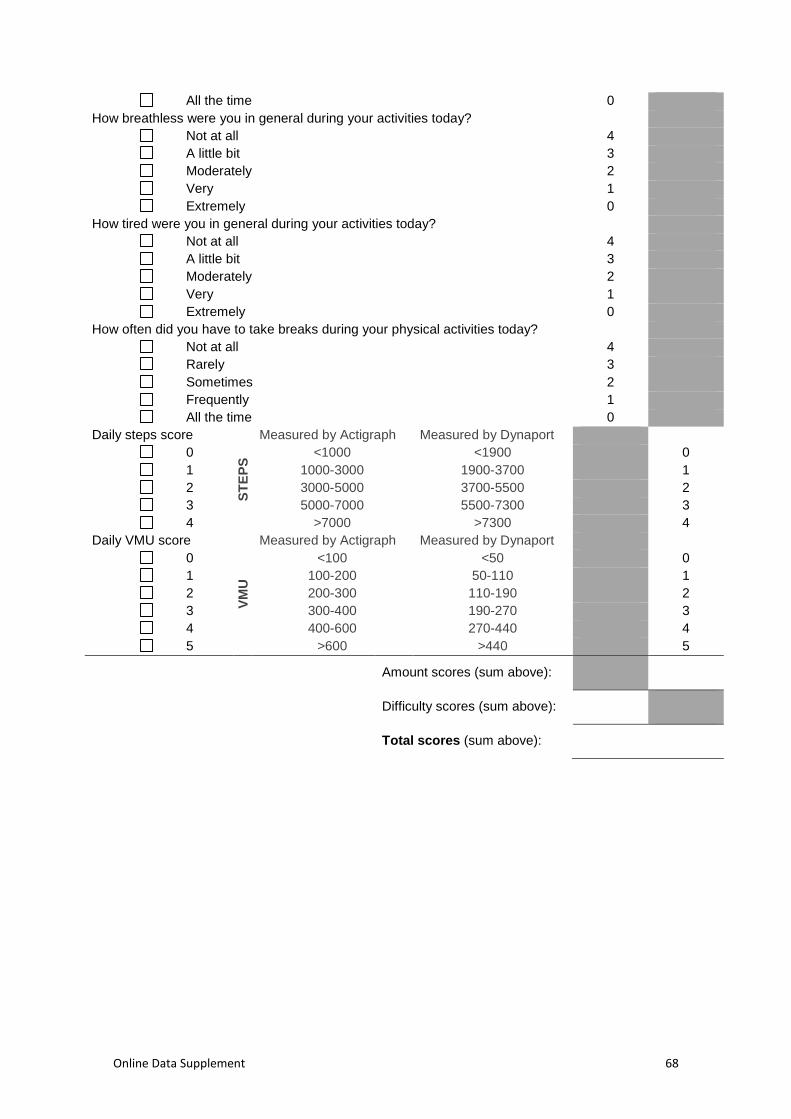
Online Data Supplement 68
All the time 0
How breathless were you in general during your activities today?
Not at all 4
A little bit 3
Moderately 2
Very 1
Extremely 0
How tired were you in general during your activities today?
Not at all 4
A little bit 3
Moderately 2
Very 1
Extremely 0
How often did you have to take breaks during your physical activities today?
Not at all 4
Rarely 3
Sometimes 2
Frequently 1
All the time 0
Daily steps score
ST
EP
S
Measured by Actigraph Measured by Dynaport
0 <1000 <1900 0
1 1000-3000 1900-3700 1
2 3000-5000 3700-5500 2
3 5000-7000 5500-7300 3
4 >7000 >7300 4
Daily VMU score
VM
U
Measured by Actigraph Measured by Dynaport
0 <100 <50 0
1 100-200 50-110 1
2 200-300 110-190 2
3 300-400 190-270 3
4 400-600 270-440 4
5 >600 >440 5
Amount scores (sum above):
Difficulty scores (sum above):
Total scores (sum above):

Online Data Supplement 69
Final version of the Clinical visit of PROactive Physical Activity in COPD
(C-PPAC) instrument
CLINICAL VISIT OF PROACTIVE PHYSICAL ACTIVITY IN COPD: C-PPAC
INSTRUCTIONS TO PATIENTS:
Patients with chronic lung disease like you often report that they have problems during physical activity. By physical activity, we mean all activities that require movement of your body. Examples are household activities, walking, going to work, or getting dressed. However, please consider all activities you do, and not only these examples. We would like to know how you experienced your physical activity IN THE PAST 7 DAYS.
Please select the box next to the response that best applies to you IN THE PAST 7 DAYS.
There are no wrong answers. We very much value your response.
Difficulty
score
Amount
score
In the past 7 days, how much walking did you do outside?
None at all 0
A little bit (about 10 minutes every day) 1
Some (about 30 minutes every day) 2
A lot (about 1 hour every day) 3
A great deal (more than 1 hour every day) 3
In the past 7 days, how many chores did you do outside the house? Some
examples are gardening, taking the rubbish out, or doing small errands.
None at all 0
A few 1
Some 2
A lot 3
A large amount 4
In the past 7 days, how much difficulty did you have getting dressed?
None at all 4
A little bit 3
Some 2
A lot 1
A great deal 0
In the past 7 days, how much difficulty did you have getting out and about?
None at all 4
A little bit 3
Some 2
A lot 1
A great deal 0
In the past 7 days, how often did you avoid doing activities because of your lung
problems?
Not at all 4
Rarely 3
Sometimes 2
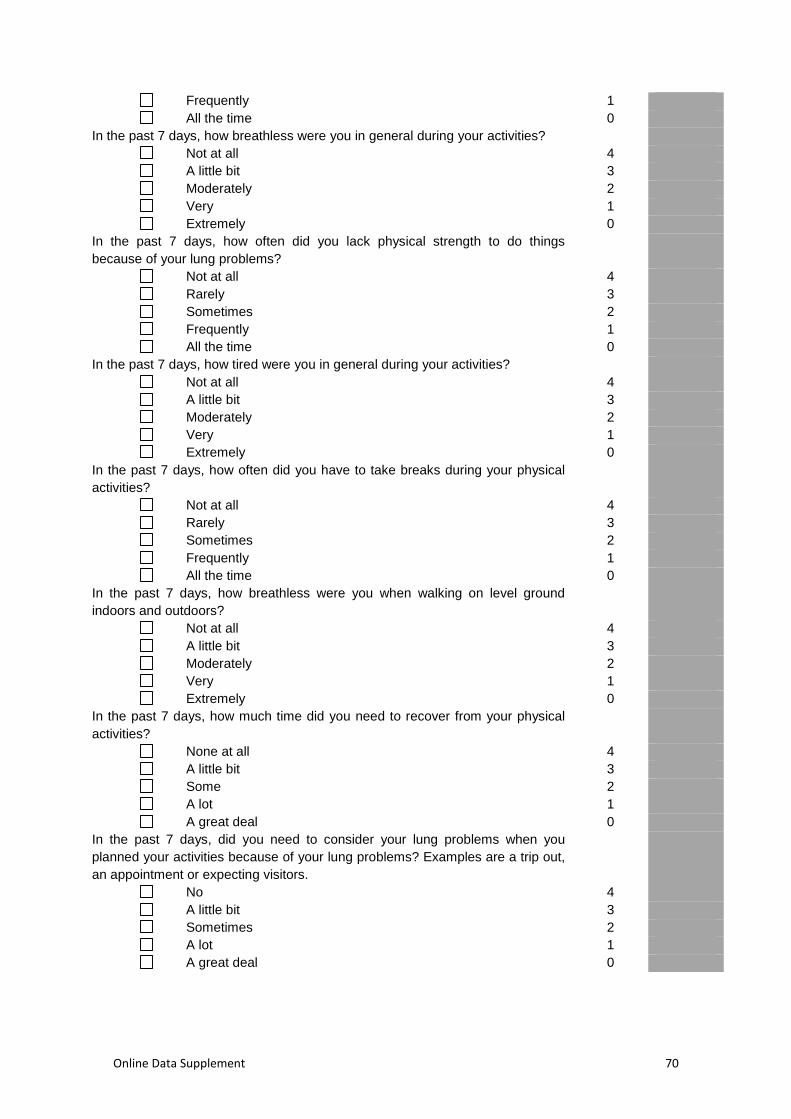
Online Data Supplement 70
Frequently 1
All the time 0
In the past 7 days, how breathless were you in general during your activities?
Not at all 4
A little bit 3
Moderately 2
Very 1
Extremely 0
In the past 7 days, how often did you lack physical strength to do things
because of your lung problems?
Not at all 4
Rarely 3
Sometimes 2
Frequently 1
All the time 0
In the past 7 days, how tired were you in general during your activities?
Not at all 4
A little bit 3
Moderately 2
Very 1
Extremely 0
In the past 7 days, how often did you have to take breaks during your physical
activities?
Not at all 4
Rarely 3
Sometimes 2
Frequently 1
All the time 0
In the past 7 days, how breathless were you when walking on level ground
indoors and outdoors?
Not at all 4
A little bit 3
Moderately 2
Very 1
Extremely 0
In the past 7 days, how much time did you need to recover from your physical
activities?
None at all 4
A little bit 3
Some 2
A lot 1
A great deal 0
In the past 7 days, did you need to consider your lung problems when you
planned your activities because of your lung problems? Examples are a trip out,
an appointment or expecting visitors.
No 4
A little bit 3
Sometimes 2
A lot 1
A great deal 0
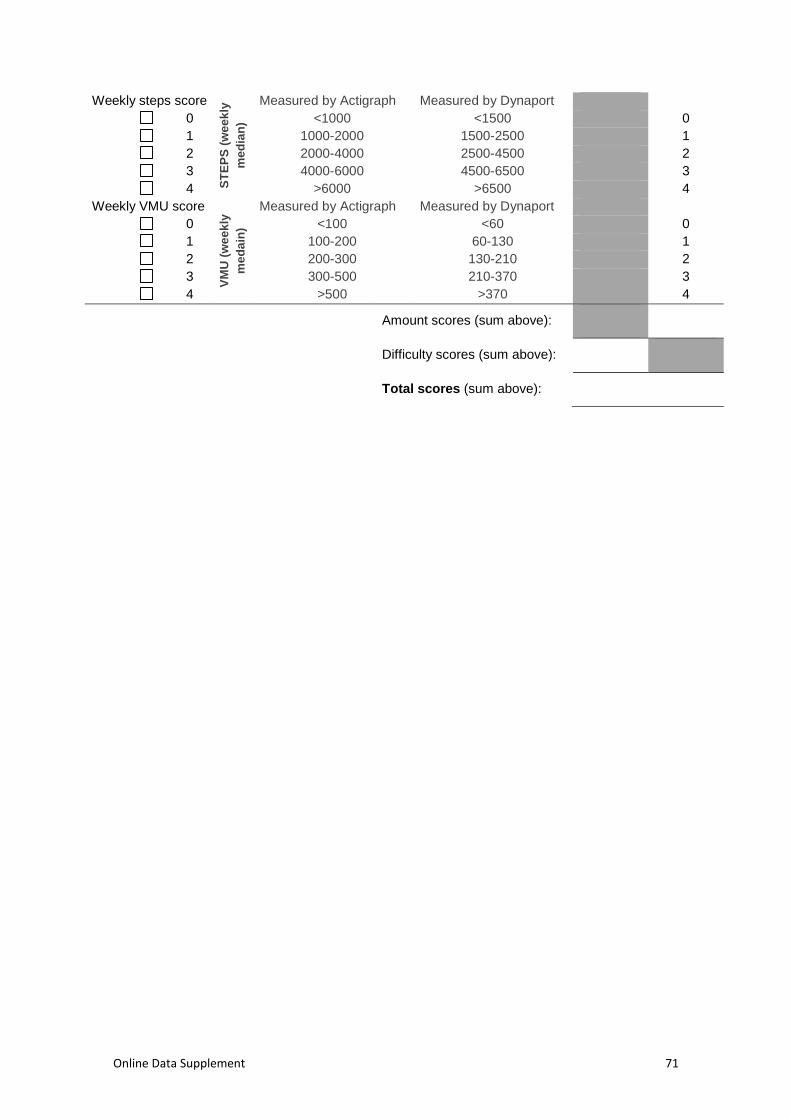
Online Data Supplement 71
Weekly steps score
ST
EP
S (
we
ek
ly
me
dia
n)
Measured by Actigraph Measured by Dynaport
0 <1000 <1500 0
1 1000-2000 1500-2500 1
2 2000-4000 2500-4500 2
3 4000-6000 4500-6500 3
4 >6000 >6500 4
Weekly VMU score
VM
U (
we
ek
ly
me
da
in)
Measured by Actigraph Measured by Dynaport
0 <100 <60 0
1 100-200 60-130 1
2 200-300 130-210 2
3 300-500 210-370 3
4 >500 >370 4
Amount scores (sum above):
Difficulty scores (sum above):
Total scores (sum above):
Online Data Supplement 72
References
E1. Committee for Medicinal products for human use (EMA). Biomarkers
Qualification: Guidance to applicants. 2008. Available from:
http://www.ema.europa.eu/ema/index.jsp?curl=pages/regulation/general/general
_content_000043.jsp
E2. Guidance for industry: patient-reported outcome measures: use in
medical product development to support labeling claims: draft guidance.
Health Qual Life Outcomes 2006;4:79.
E3. Dobbels F, de Jong C, Drost E, Elberse J, Feridou C, Jacobs L,
Rabinovich R, Frei A, Puhan MA, de Boer WI, van der Molen T, Williams
K, Pinnock H, Troosters T, Karlsson N, Kulich K, Rüdell K. The
PROActive innovative conceptual framework on physical activity. Eur
Respir J 2014; 44: 1223-1233.
E4. Van Remoortel H, Giavedoni S, Raste Y, Burtin C, Louvaris Z, Gimeno-Santos
E, Langer D, Glendenning A, Hopkinson NS, Vogiatzis I, Peterson BT, Wilson F,
Mann B, Rabinovich R, Puhan MA, Troosters T. Validity of activity monitors in
health and chronic disease: a systematic review. Int J Behav Nutr Phys Act
2012; 84-106.
E5. Rabinovich RA, Louvaris Z, Raste Y, Langer D, Van Remoortel H,
Giavedoni S, Burtin C, Regueiro EMG, Vogiatzis I, Hopkinson NS, Polkey
MI, Wilson FJ, Macnee W, Westerterp KR, Troosters T. Validity of
physical activity monitors during daily life in patients with COPD. Eur
Respir J 2013;42:1205-1215.
E6. Van Remoortel H, Raste Y, Louvaris Z, Giavedoni S, Burtin C, Langer D,
Wilson F, Rabinovich R, Vogiatzis I, Hopkinson NS, Troosters T. Validity
Online Data Supplement 73
of six activity monitors in chronic obstructive pulmonary disease: a
comparison with indirect calorimetry. PLoS One 2012;7:e39198.
E7. Office for National Statistics. The National Statistics Socio-economic
Classification. User Manual, 2005th ed. Palgrave Macmillan; 2005.
Available at www.statistics.gov.uk.
E8. Zigmond AS, Snaith RP. The Hospital Anxiety and Depression Scale.
Acta Psychiatr Scand 1983;67:361-370.
E9. Guyatt GH, Berman LB, Townsend M, Pugsley SO, Chambers LW. A
measure of quality of life for clinical trials in chronic lung disease. Thorax
1987;42:773-778.
E10. Van der Molen T, Willemse BWM, Schokker S, ten Hacken NHT, Postma
DS, Juniper EF. Development, validity and responsiveness of the Clinical
COPD Questionnaire. Health Qual Life Outcomes 2003;1:13.
E11. Jones PW, Harding G, Berry P, Wiklund I, Chen W-H, Kline Leidy N.
Development and first validation of the COPD Assessment Test. Eur
Respir J 2009;34:648-654.
E12. Flack VF, Afifi AA, Lachenbruch PA, Schouten HJA. Sample size
determinations for the two rater kappa statistic. Psychometrika
1988;53:321-325.
E13. Garcia-Aymerich J, Félez M a, Escarrabill J, Marrades RM, Morera J,
Elosua R, Antó JM. Physical Activity and Its Determinants in Severe
Chronic Obstructive Pulmonary Disease. Med Sci Sport Exerc
2004;36:1667-1673.
E14. Everitt B. Multivariate Analysis: the Need for Data, and other Problems. Br
J Psychiatry 1975;126:237-240.
Online Data Supplement 74
E15. Cattell RB. The scientific use of factor analysis in behavioral and life
sciences. New York: Plenum; 1978.
E16. Gorsuch RL. Factor Analysis, 2nd editio. Hillsdale: L. Erlbaum Associates;
1983.
E17. Jones PW, Chen W-H, Wilcox TK, Sethi S, Leidy NK. Characterizing and
quantifying the symptomatic features of COPD exacerbations. Chest
2011;139:1388-1394.
E18. Reeve BB, Hays RD, Bjorner JB, Cook KF, Crane PK, Teresi JA, Thissen
D, Revicki DA, Weiss DJ, Hambleton RK. Psychometric Evaluation and
Calibration of Health-Related Quality of Life Item Banks. Med Care
2007;45:22-31.
E19. Andrich D. A rating formulation for ordered response categories.
Psychometrika 1978;43:561-573.
E20. Meguro M, Barley E a, Spencer S, Jones PW. Development and Validation
of an Improved, COPD-Specific Version of the St. George Respiratory
Questionnaire. Chest 2007;132:456-463.
E21. Pesudovs K, Burr JM, Harley C, Elliott DB. The development,
assessment, and selection of questionnaires. Optom Vis Sci 2007;84:663-
674.
E22. Crane PK, Gibbons LE, Jolley L, Belle G Van. Differential Item
Functioning Analysis With Ordinal Logistic Regression Techniques.
DIFdetect and difwithpar. 2006;44:115-123.
E23. Choi SW, Gibbons LE, Crane PK. lordif : An R Package for Detecting
Differential Item Functioning Using Iterative Hybrid Ordinal Logistic
Online Data Supplement 75
Regression/Item Response Theory and Monte Carlo Simulations. J Stat
Softw 2011;39:1-30.
E24. Hill CD, Edwards MC, Thissen D, Langer MM, Wirth RJ, Burwinkle TM,
Varni JW. Practical Issues in the Application of Item Response Theory: A
Demonstration Using Items From the Pediatric Quality of Life (PedsQL)
4.0 Generic Core Scales. 2007;45:39-47.
E25. Altman DG, Bland JM. Measurement in Medicine : the Analysis of Method
Comparison Studies. 1983;32:307-317.