-
8/4/2019 The Problem of Osteoporotic Hip Fracture in
Australia
1/32
bu
lletin
76
Bulletin 76 March 2010
Te problem of osteoporotichip fracture in Australia
Key points
eage-adjustedincidencerateofosteoporotichipfractureinAustraliadecreasedoverthe10yearsto200607,by14%amongmalesandby20%amongfemales.However,theactualnumberofcasescontinuedtoincreaseinbothsexesduetopopulationgrowthandageing.
erewereanestimated16,518osteoporotichipfracturesamongAustraliansaged40yearsoroverin200607(175per100,000persons).Almostthree-quartersoftheseoccurredinfemales,whoonaveragewereaged83years(comparedwith81yearsformales).
Around1in9peoplehospitalisedwiththeprincipaldiagnosisofosteoporotichipfracturein200607weredischargedtoaresidentialagedcareservice,wherethishadnotpreviouslybeentheirplaceofresidence.
AboriginalandTorresStraitIslanderAustraliansweremuchmorelikelythanotherAustralianstobehospitalisedforanosteoporotichipfracture.eywerealsoonaveragemuchyoungeratthetimeoftheirfracture.
Osteoporosisandosteoporoticfracturescanbepreventedthroughlifestylechangesandbytakingactiontoreducetheriskoffalls.
Malesinparticularmaybenetfromincreasedattentiontohipfractureprevention.
Contents
Key points ......................... ...........................
............................ ............................
........................... ............................
............................ .... 1
Introduction .........................
............................ ............................
........................... ............................
............................ ........................... 2
Osteoporotic hip ractures in 200607 ..........................
............................ ...........................
............................ ...........................
.............. 5
Trends
.......................................................................................................................................................................................................14
Preventing osteoporotic hip ractures........................
........................... ............................
........................... ............................
................ 20
Conclusions ...........................
............................ ............................
........................... ............................
............................ ......................... 21
Appendix 1: Methods and data sources ..........................
............................ ...........................
............................ ...........................
............ 22
Appendix 2: Data tables ..........................
........................... ............................
........................... ............................
............................ ....... 26
Abbreviations .......................
............................ ............................
........................... ............................
............................ ......................... 27
Reerences ........................ ...........................
............................ ............................
........................... ............................
............................ .. 28
Acknowledgments .........................
........................... ............................
............................ ...........................
............................ ................ 29
-
8/4/2019 The Problem of Osteoporotic Hip Fracture in
Australia
2/32
Teproblemofosteoporo
tichipfractureinAustralia
2
Introduction
Everyday,morethan40Australiansbreaktheirhip.Mostareaged65yearsorover,andmorethanhalfareaged85orover.Virtuallyallofthesepeoplewillbeadmittedtohospital,andmostwillhavesomekindofsurgery.Twopeoplewilldieinthehospital,andatleastfourwillneedtogointoaresidentialagedcarefacility,eitherwhiletheyrecoverorpermanently.Ayearlater,lessthanhalfofthoseoriginal40peoplewillbeabletowalkaswellastheydidbeforethefracture,andanothersixorsevenwillhavedied.
OsteoporotichipfracturesareaconsiderableburdenonAustraliansandtheAustralianhealthsystem.Becausetheyaremorecommoninolderpeople,theageingofthe
Australianpopulationmeansthatovertimemorepeoplewillbeatriskofhavingahipfracture.Despitethis,however,theincidencerateofosteoporotichipfractureisfalling.
isbulletinpresentsthelatestdataontheincidenceofosteoporotichipfractureinAustralia,aswellaskeyconsequencesofthefracturesuchassurgery,placementinaresidentialagedcarefacilityanddeath.Informationaboutrecenttrendsinosteoporotichipfractureincidenceandvariationacrossthepopulationisalsopresented.
What is an osteoporotic hip fracture?
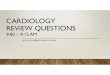
Ahipfractureisabreakoccurringatthetopofthethighbone(femur),nearthehip(Figure1).Inapersonwithhealthybones,astrongforceisusuallyneededtocausea
fracture.Butsomediseasesandconditionscanmakebonesfragile,sothatafracturecanoccurwithasmallamountofforceforexample,afallfromastandingheightorless.istypeoffractureiscalledaminimaltraumafracture.
Figure 1: Bones o the hip and sites o hip racture
Osteoporosisisaconditionwherethebonesweakenandlosetheirstructuralintegrity.Itismostcommoninolderfemalesbutalsoaectsmales.Peoplewhohaveosteoporosis
areathighriskofminimaltraumafractures,whicharethereforesometimescalledosteoporoticfractures.etermosteoporotichipfractureisusedinthisreporttomeanahipfracturethathasoccurredwitharelativelysmallamountofforce.
-
8/4/2019 The Problem of Osteoporotic Hip Fracture in
Australia
3/32
Bulletin 76 March 2010
3
Althoughosteoporoticfracturescanoccuranywhereinthebody,theyoccurmorefrequentlyatcertainsites,suchasthehip,pelvis,spine,wristandforearm.Hipfracturesaregenerallymoreseriousanddebilitatingthanfracturesatothersites.eyaredividedintothreesubtypesdependingonwherethethighbonebreaks:femoralneckfracture,pertrochantericfractureandsubtrochantericfracture(Figure1).
Causes and risk factors
Mostosteoporotichipfracturesresultfromafall(Cummings&Melton2002;Kannusetal.2005;Reginsteretal.2005).Othersarecausedwhenthehipstrikes(orisstruckby)asolidobjectforexample,collidingwithatable.Sometimesthefractureoccurswithout
obvioustrauma,whenanordinaryactivitymayputstrainonabone(suchaswhengettingupfromachair).isismorelikelytohappeninpeoplewithsevereosteoporosis.
Risk actors or alls
Riskfactorsforfallsmaybeintrinsic(factorsrelatedtotheindividual)orextrinsic(factorsrelatingtoapersonsenvironment).Intrinsicriskfactorsincludeproblemswithvision,muscleweakness,poorbalance,olderage,cognitiveimpairment,ahistoryoffalling,fearoffalling,useofmedicationscausingdrowsinessorconfusionandconditionsaectingbonestructure(suchasosteoporosis)(Stevens&Olson2000).Extrinsicriskfactorsincludetrippinghazards(suchasunevenground,looserugsorclutter),wetorslipperysurfaces,
slipperyfootwear,poorlightingandlackofhandrailsonstairs(AIHW2008a;Kanisetal.2004;OsteoporosisAustralia2006;Stevens&Olson2000).
Risk actors or osteoporosis
emodiableriskfactorsforosteoporosisincludecalciumandvitaminDdeciencies,physicalinactivity,smokingandbeingsubstantiallyunderweight.Non-modiableriskfactorsincludeafamilyhistoryofthecondition,olderageandgeneticpredisposition.Certaindiseasesandconditionsalsoincreasetheriskofosteoporosis,eitherasadirectcomplicationofthediseaseorasaside-eectofthemedicationusedtomanageit(AIHW2008a).eseincluderheumatoidarthritis,chronickidneydisease,eatingdisorders,
coeliacdiseaseandasthma.
Other risk actors or hip racture
Factorsthatincreasetheriskofhipfractureindependentlyofanyeectonosteoporosisandfallsincludeahistoryofcorticosteroiduseandpreviousminimaltraumafractures.Peoplewhohavehadaminimaltraumafractureareatincreasedriskofsubsequentfractures,aneectknownasthefracturecascade.DatafromtheDubboOsteoporosisEpidemiologyStudyshowthattheincreaseinriskpersistsforupto10years,andthat40%ofwomenand60%ofmenwillexperienceasecondfracturewithinthisperiod(Centeretal.2007)
-
8/4/2019 The Problem of Osteoporotic Hip Fracture in
Australia
4/32
Teproblemofosteoporo
tichipfractureinAustralia
4
Consequences
Hipfracturescauseconsiderablefunctionalimpairmentandnearlyalwaysrequiresurgery.eymayalsogiverisetoongoingpainanddisabilitylessthan50%ofindividualsregaintheirpre-fracturewalkingabilityoneyearaftersuchfractures(Osnesetal.2004;Sernbo&Johnell1993).Qualityoflifemaybesubstantiallyreduced,particularlyinrelationtophysicalfunction,socialfunctionandroleresponsibilities(Hallbergetal.2004;Randelletal.2000;Willigetal.2001).eabilitytoundertakeactivitiesofdailylivingmaybecompromisedand,forsome,thismaynecessitateamovefromindependentaccommodationtoaresidentialagedcarefacility,achangethatmayleadtoreducedsocialinteraction,emotionaldistress,reducedself-condenceandlossofdignity(Illinois
CouncilonLongTermCare2008;Osnesetal.2004).Anxietyabouthavinganotherfractureandfearoftheconsequencesoffracture,suchasdependenceandinstitutionalisation,maybeconsiderable(Salkeldetal.2000).Insomecases,thepersonmaydevelopafearoffallingandrestricttheiractivitiestoavoidfurtherfalls.Furthermore,theriskofdeathisraisedforseveralyearsfollowingahipfracture,particularlyinmen(Bliucetal.2009;Farahmandetal.2005;Johnelletal.2004;Piirtolaetal.2008).
Costs
Hipfracturesareexpensivetotreat,withhospitalepisodesforproceduressuchaspartialjointreplacementcostingonaverage$15,500$19,500(Table1).Hipfracturesalsoincurindirectcostsforrehabilitation,outpatientvisitsforfollow-uptreatment,temporaryresidentialagedcarefacilityplacementifrequired,andassistancewithactivitiesofdailylivingathomeduringtherecoveryperiod.Forthosewhosefractureresultsinlong-termfunctionallimitationsordisability,thecostofpermanentresidentialagedcarefacilityplacementorhelptoliveindependentlymaybeconsiderable.
NoAustraliandataontheoverallcostsofhipfracturearecurrentlyavailable.In2000,SteveParrottestimatedthatthetotalannualcosttosocietyintheUKassociatedwithhipfractureswas726million(AU$1,832million)(Parrott2000).isgurerepresentsanexpenditureof31(AU$78)perpersonaged45andover.etotalcostiscomprisedof32%indirecthospitalandambulancecosts,1%inotherhealthservicecostsand67%insocialcarecosts(includingresidentialcareandsocialsupportservicesforthoseathome).
-
8/4/2019 The Problem of Osteoporotic Hip Fracture in
Australia
5/32
Bulletin 76 March 2010
5
Table 1: Estimated cost o hospital treatment or osteoporotic hip
racture, by sector, 200607Public hospitals Private hospitals
DRG(a)
Number ohip racture
separations(b)Average lengtho stay (days)(c)
Average cost orthis DRG (AU$)(d)
Number ohip racture
separations(b)Average lengtho stay (days)(c)
Average cost orthis DRG (AU$)(d)
I03B 2,775 14.4 19,472 583 16.6 19,100
I03C 1,393 8.8 15,587 480 10.7 17,719
I08A 4,486 14.4 18,743 803 17.7 14,235
I08B 2,844 8.6 11,321 705 10.8 7,128
I78A 1,386 13.9 7,244 196 16.0 6,841
I78B 3,062 4.1 2,182 270 7.7 3,068
(a) DRG = diagnosis related groupa way o classiying hospital
admissions into groups with similar clinical conditions and
resource usage.
(b) Number o separations or osteoporotic hip racture assigned to
this DRG.
(c) Average length o stay associated with separations in
previous column.
(d) Average cost or all separations assigned to this DRG.
Note:Data or the top 6 DRGs are presented, accounting or 97% o
osteoporotic hip racture separations in 200607.
I03Bhip replacement with complications or uncomplicated revision
hip replacement
I03Cuncomplicated hip replacement
I08Aother hip and emur procedures with complications
I08Bother uncomplicated hip and emur procedures
I78Aracture o neck o emur with complications (no procedures)
I78Buncomplicated racture o neck o emur (no procedures)
Source:
AIHW National Hospital Morbidity Database and DoHA 2008.
Osteoporotic hip fractures in 200607
Incidence
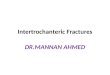
erewereanestimated16,518hospitalisationsforosteoporotichipfractureamongAustraliansaged40yearsoroverin200607,equatingto175per100,000persons.Almostthree-quartersofthese(12,006fractures)occurredinfemales.eincidencewas
higheramongfemalesthanmalesacrossallagegroupsexcept4049years,wheretherateinmaleswasaroundtwicethatinfemales(seeAppendix2,TableA2.1).
eaverageageathospitalisationwas81yearsformalesand83yearsforfemales.
-
8/4/2019 The Problem of Osteoporotic Hip Fracture in
Australia
6/32
Teproblemofosteoporo
tichipfractureinAustralia
6
0
500
1,000
1,500
2,000
2,500
3,000
FemalesMales
85+808475797074656960645559505445494044
Age
Number per 100,000 population
Note: Persons aged 40 years or over.
Source: AIHW National Hospital Morbidity Database.
Figure 2: Estimated incidence o osteoporotic hip racture,
200607
Fracture site
emostcommonfracturesiterecordedwasneckoffemur,accountingforaround53%ofallcases.Pertrochantericfracturesaccountedforanother43%ofcases,withsubtrochantericfracturestheleastcommonat4%.eseproportionsdidnotvarybetweenmalesandfemales,butdidvarysomewhatbyage,withatendencyforpertrochantericfracturestobecomemorecommonwithage(Figure3).Peoplewithpertrochantericfractureswere83yearsoldonaverage,comparedwith82and81yearsforneckoffemurandsubtrochantericfractures,respectively.
-
8/4/2019 The Problem of Osteoporotic Hip Fracture in
Australia
7/32
Bulletin 76 March 2010
7
Per cent
Age
0 10 20 30 40 50 60 70 80 90 100
SubtrochantericPertrochantericNeck of femur
4049
5054
5559
6064
6569
7074
7579
8084
85+
Notes
1. Persons aged 40 years or over.
2. The age groups 4044 years and 4549 years have been combined
due to the small number o cases.
Source: AIHW National Hospital Morbidity Database.
Figure 3: Distribution o sites o hip racture, by age, 200607
Events causing ractures
emostcommonlyrecordedexternalcausesofosteoporotichipfracturesin200607werefallonsamelevelfromslipping,trippingandstumbling(38%ofcases),otherfallonsamelevel(21%ofcases)andunspeciedfall
(30%ofcases).Fallsfromabedorchairaccountedformostoftheremainingcases(9%),withotherevents(suchascollisionwithanotherperson,ananimalorotherfurniture)makingupjust2%ofthetotal.Recordingofunspeciedfallbecameslightlymorecommonwithage.
Place o occurrence
emajorityoffracturesoccurredatthepersonsplaceofresidence,withalmosthalf(47%)happeninginprivatehomes(Figure4).Afurther32%ofcasesoccurredinresidentialcarefacilities(includingresidentialagedcarefacilitiesandretirementvillages).Inalmost600cases(3%),theplaceofoccurrencewasahealthfacility,suchasahospital,healthcentreoroutpatientclinic.
-
8/4/2019 The Problem of Osteoporotic Hip Fracture in
Australia
8/32
Teproblemofosteoporo
tichipfractureinAustralia
8
0
10
20
30
40
50
UnspeciedOtherStreet orfootpath
Health facilityPublic ortrade area
Aged carefacility
Private home
Place
Per cent
Notes
1. Public or trade areas include shops, oces, train stations,
restaur ants, sporting and recreat ional acilities, schools,
librari es and places o worship. Other
places include industrial premises, construction sites, arms,
prisons, beaches and bushland.
2. Persons aged 40 years or over.
Source: AIHW National Hospital Morbidity Database.
Figure 4: Place o occurrence o osteoporotic hip ractures,
200607
Population variation
Healthstatusanduseofhealthservicesvariesacrossthepopulation.InAustralia,groupswhooftenhaverelativelypoorhealthoraredisadvantagedinrelationtoaccesstohealthservicesincludepeoplelivinginremoteareas,thosewhoaresocioeconomicallydisadvantaged,overseas-bornpersonsandAboriginalandTorresStraitIslanderpeople.eincidenceofosteoporotichipfractureacrosssomeofthesepopulationgroupsisdescribedbelow.
Remoteness
Femaleslivingoutsideofthemajorcitieswereslightlymorelikelytohaveanosteoporotichipfracturecomparedwithfemalesinmajorcities(Table2).Ratesamongmalesdidnotvarysignicantlybyremoteness.oselivinginremoteAustraliatendedtobeyoungeratthetimeoftheirfracture,75yearsformalesand79yearsforfemales,comparedwith81and83yearsformalesandfemales,respectively,innon-remoteareas.
-
8/4/2019 The Problem of Osteoporotic Hip Fracture in
Australia
9/32
Bulletin 76 March 2010
9
Table 2: Incidence o osteoporotic hip racture by remoteness,
200607Observed number Expected number(a) Rate ratio(b) (95%
confdence interval)
Region Males Females Males Females Males Females
Major cities 2,980 7,989 . . . . 1.00 1.00
Regional Australia 1,449 3,820 1,440 3,558 1.01 (0.96, 1.05)
1.07 (1.05, 1.10)
Remote Australia 63 149 65 132 0.97 (0.78, 1.19) 1.13 (0.98,
1.30)
. . not applicable
(a) Number o cases that would be expected i people in the area
experienced the same age- and sex-specifc racture rates as those
living in major cities.
(b) Ratio o the number o cases observed to the number
expected.
Note:Persons aged 40 years or over.
Source: AIHW National Hospital Morbidity Database.
Socioeconomic disadvantage
erewasasmallbutsignicantdierencebetweentheleastdisadvantagedandsecondmostdisadvantagedgroupsforfemales(Table3).Formales,thoseinthemostdisadvantagedgroupandthemiddlegroupweresignicantlymorelikelytohaveanosteoporotichipfracturethanthoseintheleastdisadvantagedgroup,butagainthedierencesweresmall.However,ageatfracturedidincreasewithdecreasinglevelofdisadvantage.Atthetimeoffracture,maleswereaged79yearsonaverageinthemostdisadvantagedgroupand82yearsonaverageintheleastdisadvantagedgroup.Femaleswereaged82yearsonaverageinthemostdisadvantagedgroupand84yearsonaverageintheleastdisadvantagedgroup.
Table 3: Incidence o osteoporotic hip racture by socioeconomic
disadvantage, 200607
Socioeconomiccategory
Obser ved number Expec ted number(a) Rate ratio(b) (95%
confdence interval)
Males Females Males Females Males Females
Least disadvantaged 960 2,854 . . . . 1.00 1.00
Second leastdisadvantaged 746 2,079 739 2,047 1.01 (0.95, 1.07)
1.02 (0.98, 1.05)
Middle group 944 2,285 826 2,253 1.14 (1.08, 1.21) 1.01 (0.98,
1.05)
Second mostdisadvantaged 920 2,460 891 2,352 1.03 (0.98, 1.09)
1.05 (1.01, 1.08)
Most disadvantaged 922 2,280 848 2,269 1.09 (1.03, 1.15) 1.01
(0.97, 1.04)
. . not applicable
(a) Number o cases that would be expected i people in each group
experienced the same age- and sex-specifc racture rates as people
in the least
disadvantaged group.
(b) Ratio o the number o cases observed to the number
expected.
Note:Persons aged 40 years or over.
Source: AIHW National Hospital Morbidity Database.
-
8/4/2019 The Problem of Osteoporotic Hip Fracture in
Australia
10/32
Teproblemofosteoporo
tichipfractureinAustralia
0
Indigenous status
AboriginalandTorresStraitIslanderpeopleweremorelikelytobehospitalisedforanosteoporotichipfracturethanotherAustralians.Inthetwo-yearperiod200507,IndigenousmalesweretwiceaslikelytohaveahipfractureasotherAustralianmales,whereasIndigenousfemaleswere26%morelikelytohaveahipfracturethanotherAustralianfemales(Table4).
IndigenousAustralianswereonaveragemuchyoungerthanotherAustraliansatthetimeoftheirhipfracture,aged65years(comparedwith81years)formalesand74years(comparedwith83years)forfemales.
Table 4: Incidence o osteoporotic hip racture by Indigenous
status, 200507
Observed number Expected number(a) Rate ratio(b) (95% confdence
interval)
Indigenous status Males Females Males Females Males Females
Other Australians 8,492 22,761 . . . . 1.00 1.00
Indigenous Australians 73 113 35 90 2.01 (1.70, 2.54) 1.26
(1.07, 1.47)
. . not applicable
(a) Number o cases that would be expected i Indigenous people
experienced the same age- and sex-specifc racture rates as other
Australians.
(b) Ratio o the number o cases observed to the number
expected.
Notes
1. Data are or New South Wales, Victori a, Queensland, South
Australia, Western Australia and public hospitals in the Norther n
Territory only, and may not be
representative o other jurisdictions.
2. Persons aged 40 years or over.
3. The group other Australians includes both those indentifed as
non-Indigenous and those whose Indigenous status was unknown.
Source: AIHW National Hospital Morbidity Database.
Interventions and outcomes
Treatment provided in hospital
Asinglefracturecangeneratemorethanonediscreteepisodeofcareinhospital(eachknownasaseparation),astheinjuredpersonistransferredbetweenhospitalsandfrom
onetypeofcaretoanother.efulltreatmentforasinglefracturemayberecordedacrossseveralseparationsinthehospitalsdatabase.Becausethedatabasedoesnotincludeanyidentifyinginformation,itisnotpossibletolinkseparationstogethertoexaminetheoveralltreatmentforeachfracture.isanalysisthereforelooksattreatmentsprovidedasaproportionofallhipfractureseparationsandnotasaproportionofallhipfractures.
Notealsothattheanalysisinthissectionreferstohospitalseparationswiththeprincipaldiagnosisofhipfracture.Apersoninitiallyhospitalisedforosteoporotichipfracturemaygenerateanotherseparationwithadierentprincipaldiagnosis,forexample,whentheyaretransferredtoarehabilitationunit.einabilitytolinkindividualseparationstogethermeansthatitisnotpossibletoexaminetheinterventionsandoutcomesofthese
otherseparationsaspartofthisanalysis.
-
8/4/2019 The Problem of Osteoporotic Hip Fracture in
Australia
11/32
Bulletin 76 March 2010
11
e16,518osteoporotichipfracturesin200607generated19,611hospitalseparationswiththeprincipaldiagnosisofhipfracture.Surgicalprocedureswerecarriedoutinmorethanthree-quartersoftheseseparations.emostcommonwere:
xationofthefracturedbone(46%ofseparations)thisinvolvesaproceduretoholdtheendsoftheboneinplacetohelpithealcorrectly
primaryorrevisionjointreplacement(28%ofseparations)thersttimeajointreplacementoccursitiscalledaprimaryjointreplacement,andanysubsequentreplacementprocedureonthesamesiteiscalledarevisionjointreplacement.
Jointreplacementwasmostcommoninpeoplewithneckoffemurfractures.reetypesofjointreplacementsurgerycanbeperformedforahipfracture.Hemiarthroplasty
involvesthereplacementoftheheadofthefemur.Partialarthroplastyinvolvespartialreplacementorresurfacingoftheheadofthefemur.Totalarthroplastyinvolvesthereplacementoftheheadofthefemur,aswellasthehipsocket.Hemiarthroplastywasthemostcommontypeofprimaryjointreplacementperformed,accountingfor83%ofsuchprocedures.
Alliedhealthinterventionswerealsofrequentlyprovidedinseparationsforosteoporotichipfracture.Physiotherapy(in78%ofseparations),occupationaltherapy(36%),socialworkanddietetics(each20%)werethemostcommonalliedhealthinterventionsprovided.
Short-term outcomes
Attheconclusionofahospitalepisode,personsmaybetransferredtoanothertypeofcarewithinthesamehospital,movedtoanotherhospitalorhealthservice,dischargedtoaresidentialagedcareservice(asanewresident)ordischargedtotheirusualresidence(whichmayhavebeenaresidentialcarefacilityorwelfareinstitution).Someleavehospitalagainstmedicaladviceandsomedieinhospital.epatternoftheseshort-termoutcomesfortheestimated16,518incidenthipfracturecasesin200607isdescribedbelow.
-
8/4/2019 The Problem of Osteoporotic Hip Fracture in
Australia
12/32
Teproblemofosteoporo
tichipfractureinAustralia
2
Discharge to usualresidence 30%
Death 6%
Transfer to otherhealth service 53%
Discharge toresidential care 11%
Notes:
1. Persons aged 40 years or over.
2. The group discharge to usual residence includes those persons
who let against medical advice.
3. Only includes separations with the principal diagnosis o hip
racture.
Source: AIHW National Hospital Morbidity Database.
Figure 5: Outcomes o hospitalisation or osteoporotic hip
racture, 200607
Discharge
Inalmost11%(1,757)ofcases,thepatientwasdischargedtoaresidentialagedcareservicewherethishadnotpreviouslybeentheirplaceofresidence.eaverageageofthesepatientswas86years.Itwasnotpossibletodeterminewhethertheplacementwastemporaryorpermanent.
Injustover30%ofcases,thepersonwasdischargedtotheirusualplaceofresidence,orleftthehospitalagainstmedicaladvice.
In-hospital deaths
erewere1,029people(6%)withtheprincipaldiagnosisofosteoporotichipfracturein200607whodiedinhospital.Maleswerealmosttwiceaslikelytodieasfemales(9%comparedwith5%).eaverageageofthosewhodiedinhospitalwas85years,comparedwith82yearsfortheremainingcases.
Transer to other health care services
Justoverhalf(53%)ofpeoplewiththeprincipaldiagnosisofosteoporotichipfractureweretransferredtootherhealthcareservices.Almostthree-quartersoftheseweretransferredtoanotheracutehospital,andone-quarterweremovedtoanothertypeofcare
withinthesamehospital(forexample,totherehabilitationunit).Asmallproportionweremovedtonon-hospitalhealthcarefacilities.
-
8/4/2019 The Problem of Osteoporotic Hip Fracture in
Australia
13/32
Bulletin 76 March 2010
13
Althoughthemajorityofpeopletransferredbetweenorwithinhospitalsaftertheirhipfracturewouldhaveeventuallybeendischarged,theprincipaldiagnosis(thatis,theproblemchieyresponsiblefortheepisodeofcare)recordedfortheirlaterseparationswouldnotnecessarilyhavebeenhipfracture.Forexample,theymaystayinhospitalchieyforrehabilitation,ortheymaybewaitingforaplacetobecomeavailableinanappropriateoutsidecarefacility.Aspreviouslynoted,itisnotpossible,usingthesedata,todeterminetheeventualoutcomeofthesecasesbecausetheseparationscannotbelinkedtotrackindividualsthroughthehospitalsystem.
Hip fracture mortality
Accordingtothecodingrulesusedfordeathsdata,injuriescannotbelistedastheunderlying(primary)causeofdeath.Rather,theconditionoreventleadingtotheinjuryforexample,afallislistedastheunderlyingcauseandtheinjuryasanassociatedcause.Hipfracturewasrecordedasanassociatedcauseof1,448deathsamongpeopleaged40yearsoroverin2006,arateof14deathsper100,000persons.Deathratesweresimilarbetweenthesexes,thoughslightlyhigheramongfemalesintheoldestagegroup(Figure6).
evastmajorityofdeaths(98%)wereofpeopleaged65yearsorover,with63%ofdeathsinpeopleaged85yearsorover.eaverageageatdeathwas87yearsforfemalesand84yearsformales.
Commonunderlyingcausesrecordedinthesecasesincludedcardiovasculardisease(in25%ofdeaths),minimaltraumafalls(24%)andexposuretounspeciedfactor(18%).PreviousinvestigationbytheAIHWNationalInjurySurveillanceUnithasestablishedthatmostdeathsatolderageswithexposuretounspeciedfactorastheunderlyingcauseandafractureasanassociatedcauseprobablyinvolvedafall(Kreisfeld&Harrison2005).
Veryfewdeaths(lessthan0.5%)weretheresultofmajortrauma(suchastransportaccidentsorhighfalls).
-
8/4/2019 The Problem of Osteoporotic Hip Fracture in
Australia
14/32
Teproblemofosteoporo
tichipfractureinAustralia
4
0
50
100
150
200
250
300
FemalesMales
85+808475797074656960645559505445494044
Age
Deaths per 100,000 population
Note: Persons aged 40 years or over.
Source: AIHW National Mortality Database.
Figure 6: Deaths with hip racture as an associated cause,
2006
Trends
Incidence
eestimatedincidencerateofosteoporotichipfractureinAustraliaisonthedecline.Overthe10-yearperiod199798to200607,theage-standardisedratefellby14%inmales(from133to114per100,000)andby20%infemales(from246to198)(Figure7;TableA2.2).edecreasesmainlyoccurredamongmalesaged6584yearsandfemalesaged60yearsorover;littlechangewasseeninthe4059yearsagegroup,thoughthenumberofcasesinpeopleofthisagewasrelativelysmall.eaverageageathospitalisationincreasedfrom78to81inmalesandfrom81to83infemales.
-
8/4/2019 The Problem of Osteoporotic Hip Fracture in
Australia
15/32
Bulletin 76 March 2010
15
0
50
100
150
200
250
300
FemalesMales
200607200506200405200304200203200102200001199900199899199798
Year
Number per 100,000 population
Notes
1. Data have been age-standardised to the Australian population
at 30 June 2001.
2. Persons aged 40 years or over.
Source: AIHW National Hospital Morbidity Database.
Figure 7: Trends in osteoporotic hip racture incidence, 199798
to 200607
erateoffracturesatallthreesites(neckoffemur,pertrochantericandsubtrochanteric)
decreasedsignicantlyinfemalesovertheperiod,andtherewasasignicantdecreaseinneckoffemurfracturesinmales.
Number of cases
Althoughtheage-standardisedrateofosteoporotichipfracturehasfallenovertimeinbothsexes,theactualnumberofcaseshascontinuedtoriseasaresultofgrowthofthepopulationatrisk.Ageingofthepopulationhasincreasedthenumberofpeopleaged40yearsoroverby23%overthe10yearperiod,fromalmost7.6millionin1997toover9.3millionin2006.eincreaseamongthoseaged75yearsoroverhasbeenevengreaterat35%(from948,000toalmost1.3million).esepopulationincreaseshaveledtoa
riseinthenumberofosteoporotichipfracturecasesinbothsexesbetween199798and200607,by22%inmalesand7%infemales,or11%overall(Figure8;TableA2.2).
-
8/4/2019 The Problem of Osteoporotic Hip Fracture in
Australia
16/32
Teproblemofosteoporo
tichipfractureinAustralia
6
0
2,000
4,000
6,000
8,000
10,000
12,000
14,000
FemalesMales
200607200506200405200304200203200102200001199900199899199798
Year
Number of cases
Note: Persons aged 40 years or over.
Source: AIHW National Hospital Morbidity Database.
Figure 8: Trends in the number o osteoporotic hip ractures,
199798 to 200607
Interventions and outcomes
Duetochangesincodingovertime,hospitaltreatmentsandmostshort-termoutcomes
wereonlyabletobecomparedfortheperiod200001to200607.In-hospitaldeathwastheonlyoutcomeabletobecomparedforthefulldecadefrom199798to200607.
Treatment provided in hospital
Allied health interventions
Provisionofalliedhealthinterventionsinseparationswiththeprincipaldiagnosisofosteoporotichipfracturesignicantlyincreasedbetween200001and200607,from76%to81%ofseparations.Inparticular,occupationaltherapy,dieteticsandphysiotherapybecamemorecommon(Figure9).
-
8/4/2019 The Problem of Osteoporotic Hip Fracture in
Australia
17/32
Bulletin 76 March 2010
17
Year
Per cent
0
10
20
30
40
50
60
70
80
90DieteticsSocial workOccupational therapyPhysiotherapyAny
AHI
200607200506200405200304200203200102200001
AHI - allied health intervention
Notes
1. Per cent o osteoporotic hip racture separations (not cases)
where the procedure was perormed.
2. Persons aged 40 years or over.
Source: AIHW National Hospital Morbidity Database.
Figure 9: Trends in allied health interventions or osteoporotic
hip racture, 200001 to 200607
Joint replacement
Asdescribedearlier,eachfracturecangeneratemorethanonehospitalseparation,andtreatmentmaybeprovidedinanyoftheseseparations.Sometreatments,likephysiotherapy,maybeprovidedmorethanonceforasinglefracture.Othertreatments,likejointreplacement,willonlyoccuronceperfracture,sowecanassumethateachoccurrenceofthesetreatmentscorrespondstoasinglefracture.Inthissituationitispossibletoconsidertreatmentsprovidedasaproportionofallhipfractures.
-
8/4/2019 The Problem of Osteoporotic Hip Fracture in
Australia
18/32
Teproblemofosteoporo
tichipfractureinAustralia
8
0
5
10
15
20
25
30
35
Total arthroplastyPartial arthroplastyHemiarthroplasty
200607200506200405200304200203200102200001
Per cent
Year
Notes
1. Per cent o osteoporotic hip ractures where the procedure was
perormed.
2. Persons aged 40 years or over.
Source: AIHW National Hospital Morbidity Database.
Figure 10: Trend in use o joint replacement or osteoporotic hip
racture, 200001 to 200607
euseofjointreplacementincreasedslightlybetween200001and200607,from
31.0%to32.4%ofallhipfractures.Hemiarthroplastywasbyfarthemostcommontype,anditsusewasfairlyconstantataround27%ofcases(Figure10).eproportionofcaseswherepartialandtotalarthroplastywereperformedincreasedovertheperiod,from1.1%to1.9%andfrom2.2%to3.5%,respectively.
Short-term outcomes
Discharge to residential aged care services
eproportionofosteoporotichipfracturecaseswherethepatientwastransferredtoaresidentialagedcareservice(asanewresident)fellsignicantlybetween200001and
200607,from12.5%to10.6%.eaverageageofpeopletransferredtoresidentialcarerosesignicantlyovertheperiod,from84.8to85.6years.
In-hospital deaths
eproportionofosteoporotichipfracturesinwhichthepatientdiedinhospitalincreasedslightlybetween199798and200607,from5.8%to6.2%.eaverageageat
in-hospitaldeathalsoincreased,from83.7to85.5years.
-
8/4/2019 The Problem of Osteoporotic Hip Fracture in
Australia
19/32
Bulletin 76 March 2010
19
Transfer to other health care services
eproportionofpersonswithosteoporotichipfracturethatweretransferredtootherhealthcareservicesincreasedfrom48.5%in200001to53.1%in200607.istrendwaslargelydrivenbyanincreaseinthenumberofpatientstransferredbetweenacutehospitals.
Hip fracture mortality
Overthe10yearsfrom1997to2006,theage-standardisedrateofdeathswithhipfractureasanassociatedcausedecreasedby20.6%amongmales,from18to14deathsper100,000population(Figure11;TableA2.3).edeathrateamongfemalesdecreasedby24.0%,from19to15per100,000.
Duringthisperiod,theproportionofthesedeathsassignedtovariousunderlyingcauseschangedconsiderably.eproportionofdeathswithanunderlyingcauseofaminimaltraumafallrosefrom4%to24%,whiletheproportionwithanunderlyingcauseofexposuretounspeciedfactorfellfrom35%to18%.eproportionofdeathsattributedtocardiovasculardiseasealsodecreased,from34%to25%.ebulkoftheseshiftsoccurredtowardtheendoftheperiod,andarelikelytoberelatedtochangesindeathcerticationpracticesinAustraliainrecentyears,aswellasincreasedawarenessamongmedicalprofessionalsofosteoporosisandassociatedhipfractures.
AccordingtotheAIHWNationalInjurySurveillanceUnit,intheearlypartofthedecade,mosthipfracturedeathswerecertiedbyamedicalpractitionerratherthanbyacoroner,whichwascontrarytotheusualpracticeforotherinjurydeaths(Kreisfeld&Newson2006).Overthepastfewyearssomejurisdictionshavechangedtheircoronialreferralrequirements;consequentlymorehipfracturedeathswouldnowbecertiedbyacoroner.ismayhaveledtomoreinformationbeingmadeavailableaboutthecircumstancesofdeath,thusreducingthenumberofdeathsbeingassignedtheunderlyingcauseofexposuretounspeciedfactor.
-
8/4/2019 The Problem of Osteoporotic Hip Fracture in
Australia
20/32
Teproblemofosteoporo
tichipfractureinAustralia
20
Year
Deaths per 100,000 population
0
5
10
15
20
25
2006200520042003200220012000199919981997
FemalesMales
Notes
1. Rates have been age-standardised to the Australian population
at 30 June 2001.
2. Persons aged 40 years or over.
Source: AIHW National Mortality Database.
Figure 11: Hip racture as an associated cause o death, 1997 to
2006
Preventing osteoporotic hip fractures
epreventionofosteoporotichipfracturesliesintwomainstrategies:topreventthemostcommoneventresultinginfracturenamely,fallsandtodecreasetheriskofthebonebreakingifafallshouldoccur,mainlybypreventingorappropriatelymanagingosteoporosis.
Preventing falls
Aspreviouslynoted,manythingscanleadtofalls.Preventionthereforemayinclude:
exercisestoimprovebalanceandposture
areviewofmedications,assomemaycausedizzinessordrowsiness
attendingafallspreventionclass
repairing/removingtriphazardsandinstallingsafetyrailsandnon-slipoorstripsasappropriate
avoidingexcessivealcoholintake.
MoreinformationaboutpreventingfallsisavailablefromtheAustralianGovernmentDepartmentofHealthandAgeing(www.health.gov.au),HealthInsite(www.healthinsite.
gov.au)orOsteoporosisAustralia(www.osteoporosis.org.auorfreecall1800242141).
-
8/4/2019 The Problem of Osteoporotic Hip Fracture in
Australia
21/32
Bulletin 76 March 2010
21
Preventing and managing osteoporosis
Preventionofosteoporosiscentresaroundlifestylefactors:ahealthydietandregularexercise.Adietthatincorporatessucientamountsofcalciumisvital,asthismineralhelpsbuildandmaintainbonedensity.Calciumisfoundindairyproducts,shwithediblebonesand,insmalleramounts,inplantfoodssuchasgreenleafyvegetables.
Judiciousexposuretosunlight(keepinginmindtheriskofskincancer)isnecessaryforproducingvitaminD,whichenablesthebodytousecalcium.DietaryintakesofcalciumandvitaminDlevelscanbeincreasedthroughsupplementationifnecessary.Regularweight-bearingexercisealsohelpstostrengthenthebonesandmusclesand,combinedwithabalanceddiet,willhelptoachieveandmaintainahealthyweight.
esefactorsareimportantthroughoutlife,butparticularlyinchildhoodandadolescence,whenlargeamountsofboneareformed.Bonemassanddensityaregenerallymaintainedataconstantlevelduringearly-tomid-adulthood,butbegintodeclinefromaroundtheageof50years.Achievingahighbonedensityearlyinlifemeansthatthisprogressivelossdoesnotrapidlyreachosteoporoticlevels.
Forthosewhohaveosteoporosis,managementstrategiesincorporateboththepositivelifestylechoicesnotedabove,aswellastheuseofmedicationsthatcanhelpmaintainorimprovebonedensity.Bisphosphonatemedications(forexample,alendronateandrisedronate)reducetherateofbonelossbyslowingthereabsorptionofmineralsfromthebones.SucientlevelsofcalciumandvitaminDarealsoneededandcombination
bisphosphonatesarenowavailablethatincorporateacalciumand/orvitaminDsupplement.Morerecently,medicationsthatdirectlypromoteboneformationhavebecomeavailable:strontiumranelateandparathyroidhormone.
Fallpreventionmeasuresarealsoanimportantaspectofmanagingosteoporosis.
Conclusions
eage-standardisedincidenceofhipfractureinAustraliaisfalling,thoughpopulation
growthmeansthattheactualnumberofcasescontinuestorise.ehipfracturedeathratehasalsodecreasedsignicantlyinbothsexessince1997.
isbulletinhighlightsseveralimportantdierencesinhipfractureincidencebetweenmalesandfemales:
ehipfractureincidencerateamongmaleshasdecreasedmoreslowlythanamongfemalesinthelastdecade.
IndigenousAustralianmalesaretwiceaslikelytohaveahipfractureasotherAustralianmales,whereasthecorrespondinggapbetweenIndigenousandotherAustralianfemalesisonly26%.
Malesinthemostdisadvantagedandmiddlesocioeconomicgroupsaremorelikely
tohaveahipfracturethanthoseintheleastdisadvantagedgroup,butnosuchsocioeconomic-relateddierencesareseenamongfemales.
-
8/4/2019 The Problem of Osteoporotic Hip Fracture in
Australia
22/32
Teproblemofosteoporo
tichipfractureinAustralia
22
Inallpopulationgroups,malesaresignicantlyyoungerthanfemalesatthetimeoftheirhipfracture.
In-hospitalmortalityfollowinghipfractureismorecommoninmalesthaninfemales.
eseresults,inconjunctionwithotherAustraliandatashowingthatmalesarelesslikelythanfemalestoundergobonedensitometrytesting(Ewaldetal.2009)ortotakeactiontomanagediagnosedosteoporosis(AIHW2008c),suggestthatmalesshouldbeafocusfortargetedhipfracturepreventioneortsinthefuture.
Appendix 1: Methods and data sources
Methods
Virtuallyallhipfracturesrequirehospitalcare.erefore,hospitalseparationsdatacanbereliablyusedtoestimatetheincidenceofosteoporotichipfractureinAustralia.DatawereobtainedfromtheAIHWNationalHospitalMorbidityDatabase(NHMD)forthenancialyears199798to200607.Casesofosteoporotichipfracturewereidentiedbyselectingseparationsofpersonsaged40yearsoroverwheretheprincipaldiagnosiswasfractureoftheupperfemurandtheexternalcausecodeindicatedalowtraumaevent.
Apersonmayhavemorethanoneseparationdirectlyfollowingonfromtheirinitialadmissiontohospitalforagivenfractureforexample,whentheyaretransferredtoanotherhospitalforfurthertreatment.Toestimateincidence,recordswherethepatienthadbeentransferredinfromanotherhospitalwereexcludedtominimisedouble-counting.However,allrecordswereincludedinanalysisofhospitalproceduresandinterventions,asthesemayoccuratanypointduringthetimespentinhospital.ismethodisconsistentwiththatusedbytheNationalInjurySurveillanceUnit(Kreisfeld&Newson2006).
OutcomesofthestayinhospitalwerederivedfromthemodeofseparationrecordedintheNHMD.Outcomesconsideredweredeath,dischargetoaresidentialagedcarefacility(wherethepersonwasnotpreviouslyresident),transferstoothermedicalcare,andother
(includingdischargetousualresidence).RelevantICD-10-AMcodesfordiagnosesandproceduresarelistedinTableA1.1.
Simplelinearregressionswereappliedtoexaminetrendsovertime(Boyle&Parkin1991).
Comparing diferent populations
eStatisticalLocalAreacodeforeachseparationwasmappedtotheAustralianStandardGeographicClassicationRemotenessStructureandtotheIndexofDisadvantage,asdenedbytheAustralianBureauofStatistics(ABS2004;2005).ismappingallowsassignmentoftheremotenessandrelativelevelofdisadvantageofthepersonsareaofresidence.
-
8/4/2019 The Problem of Osteoporotic Hip Fracture in
Australia
23/32
Bulletin 76 March 2010
23
Foranalysisbyremoteness,Australiawasdividedintothreeregions:majorcities,regionalAustraliaandremoteAustralia.eincidenceofosteoporotichipfractureineachregionwasindirectlyage-standardisedtothemajorcitiesregionandrateratioscalculated.
Foranalysisbylevelofdisadvantage,comparisonsweremadebetweenthemostandleastdisadvantagedfthsofthepopulation.erateswereindirectlyage-standardisedtotheleastdisadvantagedfthandrateratioscalculated.
ForanalysisofvariationbyIndigenousstatus,datafortwonancialyearswerecombinedinordertoobtainasucientsamplesizeforreliableestimates.ereliabilityofIndigenousidenticationvariesacrossjurisdictions;theresultspresentedhereexcludetheAustralianCapitalTerritory,TasmaniaandprivatehospitalsintheNorthernTerritory
astheIndigenousidentierwasnotconsideredsucientlyreliableforanalysisinthesejurisdictions.
Forallthreeanalyses,95%condenceintervalsfortherateratioswerecalculatedusingthesquareroottransformmethod(AIHW2008a;Breslow&Day1987).
Counting deaths
Forthisanalysis,recordsofdeathsofpersonsaged40yearsoroverwherehipfracturewasrecordedasanassociatedcauseofdeathwereextractedfromtheAIHWNationalMortalityDatabase.eunderlyingcausesofdeathwerebroadlygroupedasminimal
traumafalls,exposuretounspeciedfactor,otherexternalcauses,cardiovasculardisease,respiratorydisease,cancerandothercauses.
Deathsregisteredinthecalendaryears1997to2006wereanalysed.Simplelinearregressionswereappliedtoexaminetrendsindeathratesandassignmentofunderlyingcausesofdeath(Boyle&Parkin1991).
Data sources
edatausedinthisstudywerederivedfromtheNHMDandtheNationalMortalityDatabase.eanalysiswasrestrictedtopeopleaged40yearsandover,aslessthan1%ofminimaltraumahipfracturesoccurinpeopleyoungerthan40years.
The National Hospital Morbidity Database
eNHMD,maintainedattheAIHW,coversalmostallpublicandprivatehospitalsinAustralia(AIHW2008b).edataaresuppliedtotheAIHWbystateandterritoryhealthauthoritiesandtheDepartmentofVeteransAairsusingstandarddenitionscontainedintheNationalHealthDataDictionary.einformationintheNHMDisnotperson-based;insteaditrelatestoepisodesofcareinahospital,knownashospitalseparations.Anindividualattendinghospitalmorethanoncewillgeneratemultiplerecordswithinthedatabase.
InformationavailablewithintheNHMDincludesdatesandmodesofadmissionandseparation,diagnoses,proceduresperformed,andpatientdemographicsincludingage,sex,
-
8/4/2019 The Problem of Osteoporotic Hip Fracture in
Australia
24/32
Teproblemofosteoporo
tichipfractureinAustralia
24
Indigenousstatusandareaofresidence.DiagnosesandproceduresarecodedbasedontheInternationalStatisticalClassicationofDiseasesandRelatedHealthProblems,ClinicalModication,9thRevisionfrom199394to199899andAustralianModication,10thRevisionfrom199899onwards(ICD-9-CMandICD-10-AM).
The National Mortality Database
eAIHWNationalMortalityDatabasecontainsinformationaboutdeathsregisteredinAustralia.Deathsareregisteredbythestateandterritoryregistrarsofbirths,deathsandmarriages.einformationisprovidedtotheAustralianBureauofStatisticsforcodingofthecauseofdeathandcompilationintoaggregatestatistics.
Informationavailableincludessex,ageatdeath,dateofdeath,areaofusualresidence,Indigenousstatus,countryofbirthandcauseofdeath.ecauseofdeathiscertiedbythemedicalpractitionerorthecoronerandcodedusingtheInternationalClassicationofDiseases,9thRevisionfrom1979to1996and10thRevisionfrom1997(ICD-9andICD-10).Multiplecausesofdeath,includingtheunderlyingandallassociatedcausesofdeathrecordedonthedeathcerticate,areavailablefrom1997onwards.
-
8/4/2019 The Problem of Osteoporotic Hip Fracture in
Australia
25/32
Bulletin 76 March 2010
25
Table A1.1: ICD codes used or data extraction and analysisICD-10
or ICD-10-AM code ICD-9 or ICD-9-CM code Defnition
Injury
S72.0 820.0, 820.1, 820.8, 820.9 Fracture o neck o emur
S72.1 820.20, 820.21, 820.30, 820.31 Pertrochanteric racture
S72.2 820.22, 820.32 Subtrochanteric racture
External cause o injury
W00 E888(a) Fall on same level involving ice and snow
W01 E885 Fall on same level rom slipping, tripping and
stumbling
W03 E886Other all on same level due to collision with, or
pushing by, anotherperson
W04 E888(a) Fall while being carried or supported by other
personsW05 E884.6 Fall involving wheelchair
W06 E884.4 Fall involving bed
W07 E884.2 Fall involving chair
W08 E884.9 Fall involving other urniture
W18 E884.7, E888(a) Other all on same level
W19 E888(a) Unspecifed all
W22 E917.2, E917.9(a) Striking against or struck by other
objects
W50 E917.9(a) Hit, struck, kicked, twisted, bitten or scratched
by another person
W51 E917.9(a) Striking against or bumped into by another
person
W54.8 E906.0 Struck by dog
Procedures andinterventions
47522-00 81.52 Hemiarthroplasty o hip
49315-00 81.52 Partial arthroplasty o hip
49318-00 81.51 Total arthroplasty o hip, unilateral
49319-00 81.51 Total arthroplasty o hip, bilateral
95550-00 Not comparable Allied health intervention,
dietetics
95550-01 Not comparable Allied health intervention, social
work
95550-02 Not comparable Allied health intervention, occupational
therapy
95550-03 Not comparable Allied health intervention,
physiotherapy
(a) The ICD-10 coding system provides fner detail or alls
compared with ICD-9. Separation o ICD-9 codes which span multiple
ICD-10 categories is notpossible.
-
8/4/2019 The Problem of Osteoporotic Hip Fracture in
Australia
26/32
Teproblemofosteoporo
tichipfractureinAustralia
26
Appendix 2: Data tables
Table A2.1: Estimated incidence o osteoporotic hip racture, by
age, 200607
Males Females Persons
Age Number Rate(a) Number Rate(a) Number Rate(a)
4044 26 3 11 1 37 2
4549 43 6 26 3 69 5
5054 58 8 89 13 147 11
5559 92 15 155 24 247 19
6064 161 31 219 43 380 37
6569 201 51 442 110 643 817074 374 122 725 219 1,099 172
7579 689 272 1,599 535 2,288 415
8084 1,133 670 2,827 1,175 3,960 966
85+ 1,735 1,589 5,913 2,642 7,648 2,297
40+ (crude rate) 4,512 99 12,006 247 16,518 175
(a) Number o cases per 100,000 population within age group.
Note: Persons aged 40 years or over.
Source: AIHW National Hospital Morbidity Database.
Table A2.2: Estimated incidence o osteoporotic hip racture,
199798 to 200607
Males Females Persons
Year Number Rate(a) Number Rate(a) Number Rate(a)
199798 3,706 133 11,186 246 14,892 204
199899 3,547 123 11,124 236 14,671 193
199900 3,906 131 11,406 234 15,312 194
200001 3,918 126 11,348 223 15,266 186
200102 3,978 122 11,714 222 15,692 184
200203 4,005 119 11,705 217 15,710 179
200304 4,113 119 11,913 216 16,026 177
200405 4,197 116 11,650 205 15,847 170
200506 4,367 116 11,755 200 16,122 167
200607 4,512 114 12,006 198 16,518 164
(a) Number o cases per 100,000 population, age-standardised to
the Australian population at 30 June 2001.
Note: Persons aged 40 years or over.
Source: AIHW National Hospital Morbidity Database.
-
8/4/2019 The Problem of Osteoporotic Hip Fracture in
Australia
27/32
Bulletin 76 March 2010
27
Table A2.3: Deaths with hip racture as an associated cause o
death, 1997 to 2006Males Females Persons
Year Number Rate(a) Number Rate(a) Number Rate(a)
1997 445 18 880 19 1,325 19
1998 504 19 882 19 1,386 19
1999 522 19 927 19 1,449 19
2000 502 18 832 16 1,334 17
2001 507 17 904 17 1,411 17
2002 599 19 1076 19 1,675 19
2003 551 17 916 16 1,467 16
2004 528 16 941 16 1,469 16
2005 546 16 955 16 1,501 16
2006 521 14 927 15 1,448 14
(a) Number o deaths per 100,000 population, age-standardised to
the Australian population at 30 June 2001.
Note:Persons aged 40 years or over.
Source: AIHW National Mortality Database.
Abbreviations
ABS AustralianBureauofStatistics
AHI alliedhealthintervention
AIHW AustralianInstituteofHealthandWelfare
DRG diagnosisrelatedgroup
ICD-9 InternationalClassicationofDiseases,9thRevision
ICD-9-CM
InternationalStatisticalClassicationofDiseasesandRelatedHealthProblems,9thRevision,ClinicalModication
ICD-10 InternationalClassicationofDiseases,10thRevision
ICD-10-AM
InternationalStatisticalClassicationofDiseasesandRelatedHealthProblems,10thRevision,AustralianModication
NHMD NationalHospitalMorbidityDatabase
-
8/4/2019 The Problem of Osteoporotic Hip Fracture in
Australia
28/32
Teproblemofosteoporo
tichipfractureinAustralia
28
ReferencesABS(AustralianBureauofStatistics)2004.Censusofpopulationandhousing:socio-economic
indexesforareas(SEIFA)Australia2001.ABScat.no.2039.0.55.001.Canberra:ABS.ABS2005.AustralianStandardGeographicalClassication(ASGC).ABScat.no.1216.0.
Canberra:ABS.AIHW(AustralianInstituteofHealthandWelfare)2008a.Arthritisandosteoporosisin
Australia2008.Cat.no.PHE106.Canberra:AIHW.AIHW2008b.Australianhospitalstatistics200607.Cat.no.HSE55.Canberra:AIHW.AIHW2008c.ApictureofosteoporosisinAustralia.Cat.no.PHE99.Canberra:AIHW.BliucD,NguyenND,MilchV,NguyenTV,EismanJA&CenterJR2009.Mortalityrisk
associatedwithlow-traumaosteoporoticfractureandsubsequentfractureinmenandwomen.
JournaloftheAmericanMedicalAssociation301:51321.BoyleP&ParkinDM1991.Statisticalmethodsforregistries.In:JensonOM,ParkinDM,
MacLennanR,MuirC&SkeetR(eds).Cancerregistration:principlesandmethods.London:OxfordUniversityPress,1402.
BreslowNE&DayNE1987.Statisticalmethodsincancerresearch.VolumeIIthedesignandanalysisofcohortstudies.London:OxfordUniversityPress,6972.
CenterJ,BliucD,NguyenT&EismanJ2007.Riskofsubsequentfractureafterlow-traumafractureinmenandwomen.297:38794.
CummingsS&MeltonLJ,3rd2002.Epidemiologyandoutcomesofosteoporoticfractures.Lancet359:17617.
DoHA(DepartmentofHealthandAgeing)2008.Nationalhospitalcostdatacollection.Round11costreport.Canberra:DoHA.Viewed12March2009,.EwaldDP,EismanJA,EwaldBD,WinzenbergTM,SeibelMJ,EbelingPRetal.2009.
PopulationratesofbonedensitometryuseinAustralia,20012005,bysexandruralversusurbanlocation.MedicalJournalofAustralia190:1268.
FarahmandBY,MichaelssonK,AhlbomA,LjunghallS&BaronJA2005.Survivalafterhipfracture.OsteoporosisInternational16:158390.
HallbergI,RosenqvistAM,KartousL,LfmanO,WahlstrmO&TossG2004.Health-relatedqualityoflifeafterosteoporoticfractures.OsteoporosisInternational15:83441.
IllinoisCouncilonLongTermCare2008.Understandingthetransitiontolifeinanursinghome.Chicago,Illinois:IllinoisCouncilonLongTermCare.Viewed31January2008,.
JohnellO,KanisJ,OdnA,SernboI,Redlund-JohnellI,PettersonCetal.2004.Mortalityafter
osteoporoticfractures.OsteoporosisInternational15:3542.KanisJ,JohanssonH,OdnA,JohnellO,DeLaetC,MeltonLJ,3rdetal.2004.Ameta-analysis
ofpriorcorticosteroiduseandfracturerisk.JournalofBoneandMineralResearch19:8939.KannusP,Uusi-RasiK,PalvanenM&ParkkariJ2005.Non-pharmacologicalmeanstoprevent
fracturesamongolderadults.AnnalsofMedicine37:30310.KreisfeldR&HarrisonJ2005.Injurydeaths,Australia,1999.Cat.no.INJCAT67.Canberra:
AIHW.KreisfeldR&NewsonR2006.Hipfractureinjuries.Cat.no.INJCAT93.Canberra:AIHW.OsnesEK,LofthusCM,MeyerHE,FalchJA,NordslettenL,CappelenIetal.2004.
Consequencesofhipfractureonactivitiesofdailylifeandresidentialneeds.OsteoporosisInternational15:56774.
OsteoporosisAustralia2006.Managingosteoporosis.Sydney:OsteoporosisAustralia.Viewed25July2006,.
ParrottS2000.eeconomiccostofhipfractureintheUK.York:eUniversityofYork.
-
8/4/2019 The Problem of Osteoporotic Hip Fracture in
Australia
29/32
Bulletin 76 March 2010
29
PiirtolaM,VahlbergT,LppnenM,RihI,IsoahoR&KivelS2008.Fracturesaspredictorsofexcessmortalityintheagedapopulation-basedstudywitha12-yearfollow-up.European
JournalofEpidemiology23:74755.RandellAG,NguyenTV,BhaleraoN,SilvermanSL,SambrookPN&EismanJA2000.
Deteriorationinqualityoflifefollowinghipfracture:aprospectivestudy.OsteoporosisInternational11:4606.
ReginsterJ-Y,SarletN&LecartM-P2005.Fracturesinosteoporosis:thechallengeforthenewmillennium.OsteoporosisInternational16:S1S3.
SalkeldG,CameronID,CummingRG,EasterS,SeymourJ,KurrleSEetal.2000.Qualityofliferelatedtofearoffallingandhipfractureinolderwomen:atimetradeostudy.BritishMedical
Journal320:3416.SernboI&JohnellO1993.Consequencesofahipfracture:aprospectivestudyover1year.
OsteoporosisInternational3:14853.StevensJA&OlsonS2000.Reducingfallsandresultinghipfracturesamongolderwomen.
MorbidityandMortalityWeeklyReport49:112.WilligR,Keinanen-KuikaaniemiS&JalovaaraP2001.Mortalityandqualityoflifeafter
trochanterichipfracture.PublicHealth115:3237.
Acknowledgments
isbulletinwaspreparedbyTracyDixonandAliceCrispoftheAIHWNational
CentreforMonitoringArthritisandMusculoskeletalConditions.
eauthorsthankcolleaguesDrKuldeepBhatia,GeorgeBodilsen,SallyBullock,RobertvanderHoek,SusanKillion,DrPaulMagnusandDrIndraniPieris-Caldwellfortheirhelpfulcommentsondraftsofthisbulletin.MembersoftheNationalCentresSteeringCommittee/DataWorkingGroupalsoprovidedvaluableinput.
isprojectwasfundedbytheAustralianGovernmentDepartmentofHealthandAgeing.
-
8/4/2019 The Problem of Osteoporotic Hip Fracture in
Australia
30/32
-
8/4/2019 The Problem of Osteoporotic Hip Fracture in
Australia
31/32
-
8/4/2019 The Problem of Osteoporotic Hip Fracture in
Australia
32/32
Australian Institute o Health and Welare 2010
This work is copyright. Apart rom any use as permitted under the
Copyright Act 1968, no part may be reproduced
without prior written permission rom the Australian Institute o
Health and Welare. Requests and enquiriesconcerning reproduction
and rights should be directed to the Head, Media and Communications
Unit, Australian
Institute o Health and Welare, GPO Box 570, Canberra ACT
2601.
This publication is part o the Australian Institute o Health and
Welares Bulletin series. A complete list o the
Institutes publications is available on the Institutes website
.
Cat. no. AUS 121
ISSN 1446-9820
ISBN 978 1 74024 992 8
Suggested citation
AIHW (Australian Institute o Health and Welare) 2010. The
problem o osteoporotic hip racture in Australia.
Bulletin no. 76. Cat. no. AUS 121. Canberra: AIHW.
Australian Institute o Health and Welare
Board Chair Director
Hon. Peter Collins, AM, QC Penny Allbon
Any enquiries or comments on this publication should be directed
to:
Australian Institute o Health and Welare
GPO Box 570
Canberra ACT 2601Phone (02) 6244 1000