-
8/10/2019 The role of genetic polymorphisms in periodontitis
1/31
The role of geneticpolymorphisms in periodontitis
H I R O M A S A YO S H I E, T E T S U O KO B A Y A S H I, H I D
E A K I TA I & J O H N A H C. GA L I C I A
A detailed knowledge of the dynamic between the
host immune responses and oral bacteria is essential
to understand clearly the pathogenesis of periodontal
disease. Periodontopathic bacteria initiate and re-
peatedly attack the host, stimulating an immune re-
sponse, but the presence of pathogenic subgingival
flora alone does not always equate to periodontal
destruction. Although bacterial plaque is essential for
the initiation of periodontitis, the amount of plaque
does not necessarily correlate with disease severity
(178). Each person has an individual doseresponse
curve that defines host susceptibility to periodontitis
(180). Certain patients are disease-resistant and will
not progress beyond gingivitis or early periodontitis.
This places the emphasis on host response, rather
than bacterial etiology, as the principal determinant
of disease expression.
The vast number of scientific papers availablesupport the
indispensable role of genes in host re-
sponses and, consequently, in progression of the
disease. Specifically, different allelic variants can re-
sult in variations in tissue structure (innate immu-
nity), antibody responses (adaptive immunity) and
inflammatory mediators (non-specific inflammation)
(126). Genetic variations may also act as protective or
risk factors for certain conditions, including perio-
dontitis (173). For these reasons, periodontitis is
considered as a complex genetic disease whose
phenotype is determined by both the genetic makeup
and the environmental influences on the affectedindividual.
It has already been established that interindividual
variations in the host immune responses and most
human diseases have genetic components in them.
In particular, genetic differences in immune-cell
development and antigen presentation may contrib-
ute to the susceptibility to autoimmune and infec-
tious diseases (93, 194). Identifying genes can
therefore result in novel diagnostics for risk assess-
ment, early detection and individualized treatment
approaches.
Like any other complex disease, genetic variants at
multiple loci associated with periodontitis synergis-
tically contribute to the overall disease process. Re-
sults obtained from numerous genetic reports may be
utilized to identify the candidate genes for perio-
dontal disease profiling in both aggressive and
chronic periodontitis. Identifying genes that con-
tribute to the pathogenesis of periodontitis can have
significant public health, therapeutic and scientific
repercussions. Loss of teeth induced by periodontitis
has a considerable effect on the homeostasis of cra-
niofacial and oral tissues, and consequently on the
general wellbeing of the individual. This global health
concern is instrumental in the continuous quest of
the scientific field to provide evidence linking gen-
etics and periodontitis.
Evidence linking genetics andperiodontitis
Heritability of aggressive periodontitis
Aggressive periodontitis is a specific type of perio-
dontitis with clearly identifiable clinical findings, ra-
pid attachment loss and alveolar bone destruction,
which make it distinct from chronic periodontitis.
Aggressive periodontitis is subdivided into prepu-bertal,
juvenile and rapidly progressive periodontitis,
and early onset periodontitis. Familial aggregation
reports have shown clustering within families, which
strongly suggests a genetic component of the disease
(16, 17, 21, 22, 28, 65, 66, 121, 134, 149, 154, 156, 165,
181, 206, 231, 251). Although these numerous reports
support a genetic basis for aggressive periodontitis,
sufficient consideration must be placed on the extent
of the environmental effects and behavioral patterns
102
Periodontology 2000, Vol. 43, 2007, 102132
Printed in Singapore. All rights reserved
2007 The Authors.
Journal compilation 2007 Blackwell Munksgaard
PERIODONTOLOGY 2000
-
8/10/2019 The role of genetic polymorphisms in periodontitis
2/31
that families share. These include nutrition, socio-
economic status, sanitation and diseases like diabe-
tes, among others (126). In a large-scale segregation
analysis of more than 100 families, performed by
Marazita et al. (154), a 70% autosomal-dominant
transmission of periodontitis was found in both
Blacks and non-Blacks. Segregation analysis is a
method used to study families to assess the likelihood
that a certain disease is inherited as a genetic trait. Alinkage
study has identified a gene locus responsible
for aggressive periodontitis on chromosome 4 [log-
arithm of odds (LOD) score 3.0] but this finding
was later refuted with suggestions on the genetic
locus heterogeneity of aggressive periodontitis (22,
88). This means that the disease may be a result of
mutations in several loci. Very recently, aggressive
periodontitis was linked to chromosome 1q25 (LOD
score 3.48) (146). The result was established after
performing linkage analysis in four multigenerational
families exhibiting the localized aggressive perio-
dontitis phenotype. Linkage analysis is a way of
localizing a trait to a specific location along a chro-
mosome.
Heritability of chronic periodontitis
Chronic periodontitis (former name; adult perio-
dontitis) is the most frequently occurring form of
periodontitis, characterized by slowly progressing
alveolar bone destruction and attachment loss. Genes
have also been implicated to play a role in chronic
periodontitis, but in contrast to aggressive perio-dontitis,
chronic periodontitis does not typically
follow a simple pattern of familial transmission or
distribution. The twin study is probably the most
popular method that supports the genetic aspects of
chronic periodontitis. This study substantiates the
contribution that genes make vs. the environment in
a phenotypic expression. Monozygous twins, in
contrast to dizygous twins, come from a single ovum
and therefore share exactly the same genes. Dis-
cordance in the disease experience of monozygous
twins must be caused by environmental determi-
nants as seen in twins reared apart. In dizygous
twins,differences could be a result of both genetic and
environmental differences. Michalowicz et al. (166)
reported the periodontal condition of 110 pairs of
twins from 16 to 70 years old. The mean probing
depth and attachment level scores were found to vary
less in monozygous twins reared together than in
dizygous twins reared together. In a subsequent
related study of 64 monozygous and 53 dizygous
adult twin pairs, the genetic and environmental var-
iances and heritability in chronic periodontitis,
according to path models, were estimated using
maximum likelihood estimation techniques (167).
Monozygous twins were found to be more similar
than dizygous twins for all clinical measures. Statis-
tically significant genetic variance was found for both
the severity and extent of disease. Adult periodontitis
was estimated to havec. 50% heritability, which was
unaltered following adjustments for behavioral vari-ables,
including smoking. It was concluded that there
is indeed a substantial genetic basis for the risk of
chronic periodontitis. A study by Corey et al. (38)
among 4908 twin pairs revealed that of the 116
identical and 233 non-identical twins, 9% reported a
history of periodontitis. The concordance rates were
0.230.36 for monozygous twins and 0.080.16 for
dizygous twins. However, in this study, environ-
mental factors like smoking were not controlled,
thereby creating bias toward establishing a correla-
tion between twins.
Gene polymorphisms inperiodontitis: aiming at the
righttargets
Most genetic research in periodontitis has focused on
gene polymorphisms that play roles in immunoreg-
ulation or metabolism, such as cytokines, cell-surface
receptors, chemokines, enzymes and others that are
related to antigen recognition (Table 1). The follow-
ing sections discuss the different studies that wereundertaken
to further understand the roles of gene
polymorphisms in periodontitis.
Cytokine gene polymorphisms
Interleukin-1 family
The biological activity, molecular biology and clinical
relevance of the interleukin-1 family [interleukin-1ab,
interleukin-1 receptor I/II/a] have been studied
extensively and reviewed time and again (6, 46, 50,212, 261).
Interleukin-1 is a potent pro-inflammatory
agent that is released by macrophages, platelets and
endothelial cells. The gene encoding this cytokine is
assigned to chromosome 2q1321 (10, 29, 155). Based
on the number of published reports, the interleukin-1
genotypes appear to be the most studied genetic
association with periodontal disease (Table 1).
However, carriage rates of interleukin-1 alleles differ
across populations (Fig. 1). In 1997, Kornman et al.
103
Role of genetic polymorphisms in periodontitis
-
8/10/2019 The role of genetic polymorphisms in periodontitis
3/31
Table
1.
Reportsontheassociationbetweenperiodontitisandpolymorphismsingenesaffectinghostresponseandmetabolism
Gene
P
osition
Aggressiveperiodontitis*
Chronicperiodontitis*
References
IL-1cluster
a
;)889/+4845,)511
1/8,1/3
1/11,0/2
(4,8,49,74,78,80,96,
136,141,147,151)
b
;)31,+3954RNPAG
)4/10,2/4,0/6
1/1,5/14,1/1,5/10
(157,164,185,187,196,203,
207,221,237,246,259)
Otherinterleukins
2
;)330
1/1
(208)
4
;)590,VNTR
0/3,0/3
0/3,0/2
(51,79,122,168,195,209)
6
;)597,)572,)373,)190,)174
0/2,1/2,1/1,0/1,1/3
(102,133,248)
1
0;)1087,)819,)592,VNTR
)0/1
1/3,1/3,1/3,
(18,77,125,210,274)
1
8;)656,)607,)137,+113,
+127,codon35/3
Allloci0/1
(64)
TNF
a
;)1031,)863,)857,)376,
)308,)238,+489,VNTR
0/1,0/1,0/1
0/30/1,0/1
1/1,1/1,1/1,0/1
1/7,0/3,0/1,
(39,51,53,57,61,73,98,125,
135,192,217)
b
;+252
2/3
(221)
TGF-b
)
988,)800,)509,L10P,R25P
)5091/2,others0/1
(99,222)
FCGR
IIA,IIIA,IIIB
2/4,1/3,2/4
2/7,3/6,1/7
(34,36,69,127,129,130,
150,162,229,271)
MMP
1
;)1607
1/4
(101,113,223,233)
3
;)1171
0/2
(113,233)
9
;)1562
0/2
(224,233)
2
;)1575,)1306,)790,)735
0/2
(103,233)
O
thers
0/1
0/1
(233)
HLA
A
,B,Cw
1/2,0/1,0/1
1/2,1/2,1/2
(12,19,96,182,226,233,239)
D
RB1,DRB345,DRBblank
2/3,0/1
1/2,1/1,1/1
D
QA1,DQB1,DR4
0/1,4/5,0/1
1/2,1/2
VDR
A
paI,BsmI,TaqI
0/1,2/2
1/1,1/1,4/5
(46,88,108,235,236,276)
FPR1
c
.301,306,329,348,378
0/1,1/1,1/1,1/1,1/1
(85,278)
5
46,568,576
0/1,1/1,1/1
104
Yoshie et al.
-
8/10/2019 The role of genetic polymorphisms in periodontitis
4/31
(137) described a composite genotype formed by the
two polymorphic loci interleukin-1A ()889) and
interleukin-1B (+3953) single nucleotide polymor-
phisms that carry a CT transition. This was later
known as periodontitis-associated genotype (136).
The interleukin-1A ()889), however, was superseded
by analysis of the interleukin-1A (+4845) GT
dimorphism, which is technically more straightfor-
ward, as the two single nucleotide polymorphismsare in complete
linkage disequilibrium with one an-
other. Thus, analysis of the interleukin-1A (+4845)
single nucleotide polymorphism provides the same
genetic information (135, 242). The two loci compri-
sing the periodontitis-associated genotype were
found to be in linkage disequilibrium (80).
Interleukin-1 genotypes associate more with chronic
periodontitis in Caucasians. Galbraith et al. (74) and
Gore et al. (80) concurred with the 1997 report by
Kornman et al. (136) that either the smoking status or
the interleukin-1 periodontitis-associated genotype
contribute to periodontitis disease severity. Papapa-
nou et al. (185) did not find statistical difference
in the periodontitis-associated genotype between
periodontitis patients and controls, but the period-
ontitis-associated genotype correlated with the
severity of disease when assessed by clinical attach-
ment level. In addition, periodontitis-associated
genotype-positive patients had a lower systemic
immunoglobulin G response to periodontal microb-
iota than periodontitis-associated genotype-negative
patients. Laine et al. (141) investigated the distribu-tion of
polymorphisms in the interleukin-1 gene
family among periodontitis patients and controls,
taking into account both smoking and microbiological
parameters, including the presence ofPorphyromon-
as gingivalisandActinobacillus actinomycetemcomi-
tans. The results showed a higher frequency of allele 2
carriage in interleukin-1A ()889) and interleukin-1B
(+3954) single nucleotide polymorphisms and inter-
leukin-1RN variable numbers of tandem repeat poly-
morphisms in non-smoking periodontitis patients in
whom P. gingivalis and A. actinomycetemcomitans
could not be detected [odds ratio (OR) 5.7; 95%confidence
interval (CI): 1.619.8]. These results pro-
vide evidence that polymorphisms in genes of the
interleukin-1 family are associated with severe adult
periodontitis in the absence of other risk factors tested
in the patient population. The subjects enrolled in all
the studies mentioned were Caucasians. In a mixed-
population study by McDevitt et al. (157), non-
smokers and former light smokers (
-
8/10/2019 The role of genetic polymorphisms in periodontitis
5/31
increased OR of 3.75 of having moderate to severe
periodontitis (95% CI: 1.0413.50). Performing the
analysis in European Caucasians only increased the
odds ratio to 5.27. This study also demonstrated the
relationship of patients age and former smoking
history with severity of adult periodontitis. On the
other hand, Meisel et al. (164) concluded that the in-
terleukin-1 periodontitis-associated genotype in Ger-
man Caucasians displayed a strong interaction with
smoking, resulting in an increased chronic perio-dontitis risk
(OR 2.50; 95% CI: 1.215.13). Non-
smokers, even genotype-positive, were not at any in-
creased risk. Studies in Chinese, Greek, Japanese and
Thai populations did not find a relationship between
interleukin-1 genotypes and chronic periodontitis
disease susceptibility or severity (4, 8, 203, 225).
One study investigated the incidence of the inter-
leukin-1 genotypes in a population-based sample of
26-year-old New Zealanders (246). After controlling
for gender, smoking status and plaque levels, the
authors identified a high-risk group consisting of
subjects with the interleukin-1B (+3953) CC/inter-leukin-1A
(+4845) TT genotype. This high-risk
genotype was consistent with the genotype pattern
reported by Diehl et al. (49) for early onset periodon-
titis, although the New Zealand study found no
association between early onset periodontitis and
interleukin-1 genotypes. In a study of Chilean Cau-
casians, with ages ranging from 20 to 48 years, the
heterozygous form of the interleukin-1B (+3954)
genotype was significantly higher in patients than in
controls and was associated with periodontitis
(OR 3.12; 95% CI 1.596.09; P 0.001) (151).
Homozygosity for allele 1 of the interleukin-1B
(+3954) genotype was a protective factor for perio-
dontitis. The prevalence of positive genotype (at least
one allele 2 present at each locus) was significantly
higher in periodontitis patients than in controls and
was significantly associated with periodontitis, irres-
pective of the smoking status and periodontitis dis-
ease severity. A 5-year longitudinal study in a group ofsubjects
of essentially European heritage showed an
interaction of the interleukin-1 periodontitis-asso-
ciated genotype with age, smoking and P. gingivalis
(40). The authors concluded that the interleukin-1
periodontitis-associated genotype was a contributory,
but non-essential, risk factor for periodontal disease
progression.
Studies suggest that periodontitis-associated genotype
does not correlate with aggressive periodontitis. Unlike
chronic periodontitis, reports of aggressive periodon-
titis indicate that periodontitis-associated genotype isnot
associated with this disease (Table 2). Hodge et al.
(95) investigated interleukin-1A and interleukin-1B
gene polymorphisms in unrelated Scottish Caucasian
patients with generalized early onset periodontitis and
found no association between patients and controls
for the periodontitis-associated genotype. Other rela-
ted studies demonstrated similar results. For example,
the studies by Diehl et al. (49) and Parkhill et al. (187)
actually found that allele 1 rather than 2 of the
Carriage rate of IL-1 polymorphic alleles
IL-1A+4845
IL-1B -511
IL-1B +3954
IL-1RN VNTR17.9%
8.2%
20.4%
48.6%
2.1%
9.3%
27.0%
61.1%
70.5%
68.0%
59.4%
11.6%
18.6%
26.9%
37.5%
0% 10% 20% 30% 40% 50% 60% 70% 80%
CaucasianCaucasian
African-American
JapaneseJapanese
ChineseChinese
African-American
Fig. 1. Heterogeneity across the population is evident in the
distribution of single nucleotide polymorphisms identified inthe
interleukin(IL)-1 gene.
106
Yoshie et al.
-
8/10/2019 The role of genetic polymorphisms in periodontitis
6/31
Table
2.Interleukin-1(IL-1)geneclusterpolymorphismsrelatedtochronicandaggressiveperiodontitisrisk(case-controlstudy)
Disease
association
Ethnicity
IL-1A)889/
+4845GT
IL-1B
PAG+4845/
+3954
IL-1RN
VNTR
References
)511TC
)31CT
+3953/3954CT
Chronic/adultperiodontitis
Susceptibility
Caucasian
Yes(1)*;no(1)
Yes(1)*;no(2
)
Yes(1);no(1)
Insmoker
OR
2.5
Yes(1)*
(141,157,164,185)
Others
No(5)
No(5)
Yes(1);no(4)
OR
3.75
(4,8,42,203,221)
Severity
Caucasian
No(3)
No(1)
Yes(2);no(2)
OR
4.67,3.36
Yes(2);no(1)
Innon-smoker
OR
6.8
(74,80,136,185,203)
Japanese
No(1)
No(1)
No(1)
(221)
Others
No(1)
No(1)
No(1)
(4)
Aggressive/earlyonsetperiodontitis
Earlyonset
Caucasian
No(3)
No(1)
Yes(2);no(2)
Allele1:OR
2.22
No(2)
Yes(1);no(1
)
(49,79,96,187,203)
African-American
No(2)
Yes(1);no(1)
Allele1:risk
No(1)
(259)
Japanese
No(1)
No(1)
No(1)
No(1)
Yes(1)
(221,237)
Others
Yes(1);no(2)
InmalesOR
5.58
Yes(1)
Inmale
sOR
3.16
Yes(1);no(2)
OR
2.86
No(2)
No(1)
(147,196)
Numbersinparenthesesindicatethen
umberofreports.
PAG,allele2oftheIL1A+4845singlenucleotidepolymorphism(SNP)andallele2oftheIL1B+3954SNP.
*Allele2+non-smoker+noP.gingiva
lisandA.actinomycetemcomitansdetectedoddsratio(OR)
5.7.
107
Role of genetic polymorphisms in periodontitis
-
8/10/2019 The role of genetic polymorphisms in periodontitis
7/31
interleukin-1B (+3953) significantly correlated with
aggressive periodontitis. A significant difference was
found only in the interleukin-1B genotype distribu-
tion after comparison of aggressive periodontitis
smokers with control smokers. In contrast, Quappe et
al. (196) reported that Chilean subjects who were
heterozygous for allele 2 of the interleukin-1B (+3953)
showed a significant association with aggressive
periodontitis (OR 2.86; 95% CI: 1.067.71; P 0.030). In a wholly
African-American population,
Walker et al. (259) concluded that because of the high
frequency of allele 1 of the interleukin-1B (+3954)
single nucleotide polymorphism, studies of this
polymorphism could not be carried out in this
population.
A study by Tai et al. (237) showed that generalized
aggressive periodontitis in a Japanese population
failed to find any association between aggressive
periodontitis and genotypes with respect to the in-
terleukin-1B (+3954), interleukin-1B ()511) or the
interleukin-1A (+4845) single nucleotide polymorph-
isms, although there was a significant association
with the interleukin-1RN intron 2 variable numbers
of tandem repeat genotype (OR 3.81). Recently,
Scapoli et al. (207) indicated a positive association
between generalized aggressive periodontitis and the
interleukin-1RN (variable numbers of tandem repeat)
genotype in Italian Caucasians. The genotype distri-
bution was significantly different between general-
ized aggressive periodontitis and control subjects,
and the interleukin-1B (+3953) single nucleotide
polymorphism was associated with generalizedaggressive
periodontitis. Moreover, a recombination
hot spot between the interleukin-1B (+3953) and in-
terleukin-1B ()511) single nucleotide polymorphisms
was identified. However, there was no similar
association with the interleukin-1RN (variable num-
bers of tandem repeat) genotype in study of a UK
population (187). Li et al. (147) investigated the
associations of interleukin-1 gene cluster polymor-
phisms with aggressive periodontitis in a Chinese
population. There was no significant association
of interleukin-1 polymorphisms with generalized
aggressive periodontitis in unstratified subjects.However, when
subjects were stratified by gender,
the positivity and frequency of allele 2 at the inter-
leukin-1A (+4845) single nucleotide polymorphism
were significantly increased in male patients com-
pared with male controls (OR 5.58). The frequency
of the interleukin-1B ()511) heterozygote was also
significantly increased in a male generalized aggres-
sive periodontitis group. Moreover, a possible com-
bined effect of the polymorphism of interleukin-1B
()511) and smoking on generalized aggressive peri-
odontitis susceptibility was suggested.
Taken altogether, the interleukin-1 composite
genotype, along with other candidate genes, may
contribute to the pathogenesis of chronic periodonti-
tis, but seemingly not to aggressive periodontitis. The
increase in risk of the periodontitis-associated geno-
type-positive subjects was demonstrated, irrespective
of confounding factors such as smoking,P. gingivalisand age,
although periodontitis-associated genotype
was shown to interact with these confounding factors.
Owing to ethnic differences, the global applicability of
the interleukin-1 composite genotype as a periodon-
titis marker may not be established.
Interleukin-1 genotype-positive subjects exhibited in-
creased interleukin-1 protein. The number of reports
describing the functional importance of interleukin-1
gene polymorphisms is relatively few. Thus, a defin-
itive cause and effect could not be pointed out. Sev-
eral studies, however, have shown some possible
functional implications. For example, carriage of al-
lele 2 in the ()889) locus resulted in an almost four-
fold increase of interleukin-1a protein levels in
chronic periodontitis patients (219). Furthermore,
patients who were positive to the composite inter-
leukin-1A (+4845) and interleukin-1B (+3954) peri-
odontitis-associated genotype had a higher level of
interleukin-1b in gingival crevice fluid but not in
gingival tissue before and after treatment (54).
However, positivity to periodontitis-associated gen-
otype did not correlate with higher gingival crevicefluid volume
and percentage bleeding on probing in
experimental gingivitis (114). Periodontitis patients
carrying one or two copies of the rare allele of in-
terleukin-1A ()889), tumor necrosis factor ()308) or
interleukin-6 ()174) polymorphisms displayed signi-
ficantly higher serum interleukin-6 concentrations.
Similarly, subjects carrying one or two copies of the
allele 2 at interleukin-6 ()174) and interleukin-1A
()889) had significantly higher C-reactive protein
serum levels than subjects homozygous for allele 1.1
(43). The interleukin-1RN tandem repeat poly-
morphism, in contrast to the non-synonymous, in-terleukin-1B
(+3954) polymorphism, contributed to
interleukin-1b regulation in differentiating mono-
cytes (193, 217).
Tumor necrosis factor
Tumor necrosis factor is a pro-inflammatory cytokine
that possesses a wide range of immunoregulatory
functions. Tumor necrosis factor has the potential to
stimulate the production of secondary mediators,
108
Yoshie et al.
-
8/10/2019 The role of genetic polymorphisms in periodontitis
8/31
including chemokines or cyclooxygenase products,
which consequently amplifies the degree of inflam-
mation (115, 179).
Tumor necrosis factor gene polymorphisms and
periodontitis studies display conflicting results. The
tumor necrosis factor gene (TNF) is located in chro-
mosome 6 within the major histocompatibility com-
plex, in the 6p21.3 Class III human leukocyte antigenzone (148,
197). Eight single nucleotide polymorph-
isms in the promoter region of this gene have been
described at positions )1031T/C,)863C/A,)857C/T,
)575G/A, )376G/A, )308G/A, )244G/A, and )238G/A
(25, 26, 45, 92, 250, 265). Casecontrol studies ofTNF
promoter variations revealed conflicting findings.
The )380 locus was linked to chronic periodontitis
susceptibility (P < 0.01) in Czech Caucasians, but not
in Dutch, Polish, Swedish or US Caucasians (33, 51,
57, 61, 74, 217). The same locus was associated with
chronic periodontitis severity in U.S. Caucasians
(OR 10.2), but an earlier study in the same popu-
lation reported contrasting results (74, 136). Aggres-
sive periodontitis was not linked to this locus (53,
192, 217). The rest of the promoter polymorphisms
were not associated with periodontitis, except in one
study that found an association between the )1031,
)863, )857 single nucleotide polymorphisms and
chronic periodontitis severity in Japanese people (39,
53, 74, 125, 221). On the other hand, the A/A genotype
of the +252 single nucleotide polymorphism in the
tumor necrosis factor-b gene served as a protective
factor against chronic periodontitis (OR
0.08) inone study of Caucasian subjects, but this result was
not in accordance with another study of similar
subjects (57, 74). It is not clear why these studies gave
conflicting results. However, performing another
approach, such as meta-analysis, which pools all the
data to extract a common conclusion, would be
helpful. The major cellular source of tumor necrosis
factor is the monocyte/macrophage cell group,
although other cells, such as T lymphocytes and
epithelial cells, can also produce tumor necrosis
factor (120, 191). Ex vivo studies, on the correlation
between single nucleotide polymorphisms andtumor necrosis factor
production by lipopolysac-
charide stimulation of monocytes, produced varying
results. Some studies concluded that TNFpolymor-
phisms, particularly)308 G/A did not affect tumor
necrosis factor production (99, 119, 241). On the
contrary, other studies reported that the)308 A allele
correlated with higher levels of tumor necrosis factor
(58, 152, 240). The contradictory results could be
attributed to the differences in size and choice of
subjects, time periods after stimulation, concentra-
tions of stimuli used and the absolute values of tumor
necrosis factor (in pg/ml) reported (15). Tumor
necrosis factor-a production in TNF 1031/)863 or
)857 single nucleotide polymorphism variant allele
carriers tended to be elevated in healthy Japanese
subjects (221). Gene polymorphisms and periodon-
titis association ofTNFand other cytokines, and their
receptors, are summarized in Table 3.
Other cytokines
Interleukin-2. Interleukin-2 is a pro-inflammatory
cytokine produced by T-helper 1 cells. It mediates the
cellular immune response by participating in B lym-
phocyte activation and macrophage stimulation, as
well as in natural killer and T lymphocyte prolifer-
ation (186, 243, 266). Periodontitis patients have been
reported to show higher interleukin-2 levels in the
serum compared with healthy subjects (164). In
addition, interleukin-2 was found to be produced by
lymphocytes cultured from chronically inflamed
periodontal tissues (215). The interleukin-2 gene is
located in chromosome 4q26 (214). Polymorphism at
positions ()330) and (+166), relative to the tran-
scription start site, were identified by John et al.
(116). The (+166) change occurs within the leader
peptide and does not affect the amino acid sequence.
The ()330) polymorphism has two common alleles (T
and G), making it an ideal marker for genetic
association. Homozygotes of the G-allele were found
to be at increased risk of hay fever (175). In a perio-
dontal study in Caucasian subjects, the T-allelecarriers seem to
be approximately half as likely to
develop severe periodontal disease (OR 1.99; 95%
CI 1.073.7). Moreover, individuals with the TT
genotype seem to be 2.5-times less likely to develop
severe periodontitis than individuals who are het-
erozygous or GG homozygous (OR 2.57; 95%
CI 1.155.73) (208).
Interleukin-4. Multiple roles have been identified
with interleukin-4. This cytokine can rescue B
lymphocytes from apoptosis and enhance their sur-
vival, thus playing a role in promoting B-lymphocyte-mediated
autoimmunity (107, 170, 220). Interleukin-4
is also a potent down-regulator of macrophage
function (56, 87). In established and advanced
periodontitis lesions, the presence of interleukin-4-
producing cells and the percentage of interleukin-4+
cells were significantly higher in periodontitis than in
gingivitis tissues (271). Interleukin-4 levels in the
serum of patients was higher in chronic periodontitis
than in controls, although these levels did not cor-
109
Role of genetic polymorphisms in periodontitis
-
8/10/2019 The role of genetic polymorphisms in periodontitis
9/31
Table
3.
Genepolymorphismsinothercytokines,cytokinerece
ptorsandperiodontitisassociation
Gene
Chromosome
Locus
Allele
Ethnicity
Association(no.ofreports)
References
Chronic
periodo
ntitis
Aggressive
periodontitis
TNFA
6p21.3
)1031
T/C
Japanese
Yes(1)*
No(1)
(53,221)
)863
C/A
Japanese
Yes(1)*
No(1)
(53,221)
)857
C/T
Japanese
Yes(1)*
No(1)
(53,221)
)376
G/A
Caucasian
No(1)
(39)
)308
G/A
Caucasian
Yes(1);
no(5)
OR10.2,GG:risk
No(1)
(57,61,73,74,217)
Japanese
No(1)
No(1)
(53,221)
Chilean
No(1)
(192)
)238
G/A
Caucasian
No(2)
(39,73)
Japanese
No(1)
No(1)
(53,221)
+489
G/A
Caucasian
No(1)
(39)
TNFB
6p21.3
+252
A/G
Caucasian
Yes(2);
no(1)
AA:protective,OR
0.08
(57,73,98)
TNF-a
6p21.3
Microsatellite
14alleles
Caucasian
No(1)
(125)
IL-2
4q2627
)330
T/G
Brazilian
Yes(1)
OR1.99
(208)
IL-4
5q31.1
)590
C/T
Caucasian
No(2)
(79,167)
Japanese
No(1)
(79)
Brazilian
No(1)
(209)
African-Brazilian
No(1)
(195)
Korean
No(1)
(122)
VNTR
VNTR(70bp)
Caucasian
No(2)
(79,168)
Japanese
No(1)
(79)
Brazilian
No(1)
(195)
African-Brazilian
No(1)
(209)
110
Yoshie et al.
-
8/10/2019 The role of genetic polymorphisms in periodontitis
10/31
Table
3.
Continued
Gene
Chromosome
Locus
Allele
Ethnicity
Association(no.ofreports)
References
Chronic
periodontitis
Aggre
ssive
periodontitis
IL-6
7p21
)597
A/G
Caucasian
No(1)
(102)
Japanese
No(1)
(42)
)572
G/C
Caucasian
Yes
(1)
OR
0.27,GC:protective
(102)
Japanese
No(1)
(133)
)373(microsatellite)
AnTm
:3alleles
Japanese
Yes
(1)
OR
2.96,A9T11:protective
(133)
)190
C/T
Japanese
No(1)
(133)
)174
G/C
Caucasian
Yes
(1);no(1)
OR
3.0,Callele:protective
(102,248)
Japanese
No(1)
(133)
IL-10
1q3132
)1082/)1087
A/G
Caucasian
Yes
(1)
OR
2.58
(18)
Japanese
No(1)
No(1)
(273)
Brazilian
No(1)
(210)
)819/)824
C/T
Caucasian
No(1)
No(1)
(76)
Japanese
No(1)
No(1)
(273)
Brazilian
Yes
(1)
OR
3.78
(210)
)592/)597
C/A
Caucasian
No(1)
No(1)
(76)
Japanese
No(1)
No(1)
(273)
Brazilian
Yes
(1)
OR
3.35
(210)
111
Role of genetic polymorphisms in periodontitis
-
8/10/2019 The role of genetic polymorphisms in periodontitis
11/31
relate with either the degree of bone loss or pocket
formation observed clinically (158). The gene for in-
terleukin-4 is found in chromosome 5q31.1 (232).
Promoter single nucleotide polymorphism at position
()590) and a 70-bp variable numbers of tandem re-
peat polymorphism at intron 2 have been identified
(173). Casecontrol reports relating to aggressive
periodontitis and chronic periodontitis susceptibility
and severity across several populations have failed toestablish
a connection between these loci and peri-
odontal disease (79, 122, 168, 195, 209).
Interleukin-6. Essential biological activities depend
on interleukin-6. As a result of its wide range of ef-
fects, deregulated over-production of interleukin-6
causes various clinical symptoms and abnormal
laboratory findings in vivo (176). The interleukin-6
gene was demonstrated to be localized in chromo-
some 7p21 (23). Several studies have shown the
association of interleukin-6 gene polymorphisms
with some diseases or conditions such as rheumatoid
arthritis and bone mineral density (184, 189). In
periodontitis, the GC single nucleotide polymorph-
ism at the ()174) position correlated with chronic
periodontitis susceptibility in Brazilian Caucasians
(OR 3.0), but not in Czech Caucasians (57, 259).
With regard to the other interleukin-6 gene single
nucleotide polymorphism locations, the Czech study
suggested that the ()572) G/C polymorphism of the
IL-6 gene may be one of the protective factors asso-
ciated with lower susceptibility to chronic periodon-
titis (OR
0.27; 95%
CI: 0.120.61). Furthermore, thestudy did not find an association
between the ()597)
G/A locus and chronic periodontitis susceptibility.
A recent report revealed that the ()174) G/C, ()190)
C/T and ()597) G/A loci were non-polymorphic in a
Japanese population (133). However, an over-repre-
sentation of the ()373) A9T11 allele was observed
in non-chronic periodontitis subjects (P 0.008;
OR 2.96; 95% CI 1.217.43). The authors also
reported that the interleukin-6 concentration in
subjects homozygous for the C[A10T10] haplotype of
the ()572) G/C and )373 AnTm loci was significantly
higher than in heterozygotes. In another study, peri-odontitis
patients carrying one or two copies of the
rare allele in the interleukin-6 ()174) polymorphism
displayed significantly higher serum interleukin-6
and C-reactive protein concentrations (SE 0.8
1.1 ng/l, P < 0.001 for interleukin-6; SE 0.8
1.1 mg/l, P 0.023 for C-reactive protein) (43).
Cigarette smoking and carriage of the same allele was
associated with less reduction in probing depths
among chronic periodontitis patients after deliveryTable
3.
Continued
Gene
Chromosome
Locus
A
llele
Ethnicity
Association(no.ofreports)
References
Chronic
periodontitis
Aggressive
period
ontitis
TGF-b1
19q13.113.2
)800
G
/A
Caucasian
No(1)
(99,222)
)509
C
/T
Caucasian
Yes(1);no(1)
+869
T
/C
Caucasian
No(1)
+915
G
/C
Caucasian
No(1)
TNFR2
1p36.236.3
+857
T
/G(Met196Arg)
Japanese
Yes(1)
OR
2.61
(218)
CCR5
3p21
Coding()?32)
3
2-bpdeletion
Caucasian
No(1)
(59)
IFN-cR1
6q2324
Intronicmicrosatellite
1
3alleles
Caucasian
Yes(1)
OR
5.56insmoker
(67)
IL,interleukin;IFN,interferon;OR,od
dsratio;TGF,transforminggrowthfactor;TNF,tu
mornecrosisfactor.
112
Yoshie et al.
-
8/10/2019 The role of genetic polymorphisms in periodontitis
12/31
of standard non-surgical periodontal therapy (44).
It appears that interleukin-6 gene polymorphisms
affect the serum levels of circulating interleukin-6,
and consequently modify the patients response to
periodontal treatment.
Interleukin-10. Interleukin-10 stimulates the pro-
duction of protective antibodies and down-regulates
pro-inflammatory cytokines produced by monocytes(200, 256).
Periodontitis lesions demonstrated a
significantly higher messenger ribonucleic acid
expression for interleukin-10 than that in autologous
peripheral blood mononuclear cells (272). Moreover,
stimulation of peripheral blood mononuclear cells
with outer membrane antigen from P. gingivalis
induced variable but significantly higher interleukin-
10 messenger ribonucleic acid expression in perio-
dontitis patients than in healthy controls (5). These
data suggest that controlling mechanisms suppress
an excess production of inflammatory cytokines,
which could affect the inflammatory response in
periodontitis, resulting in different clinical manifes-
tations. The gene encoding interleukin-10 was map-
ped to chromosome 1q3132 (123). Three promoter
single nucleotide polymorphisms have been des-
cribed in this gene: ()1087) G/A; ()819) C/T; and
()592) C/A (139, 143). The three loci exhibit strong
LD (260). Microsatellite polymorphisms were also
identified in the 5-flanking region of the gene, but no
association with periodontitis has been established
(55, 125). The ()1087) G/A locus was not associated
with chronic periodontitis susceptibility in Japaneseand
Brazilian subjects, but was linked to chronic
periodontitis severity in Swedish Caucasians
(OR 2.58) (18, 210, 273). The ()819) C/T and ()592)
C/A loci correlated with chronic periodontitis
susceptibility in Brazilians (OR 3.04; CI 1.31
6.91 and OR 3.38; 95% CI 1.298.82, respect-
ively) but not in Japanese and German Caucasian
subjects (77, 210, 273). The ()1087) single nucleotide
polymorphism falls within a putative transcription
factor binding site and was associated with high
in vitro interleukin-10 production (55, 139). The
()819) single nucleotide polymorphism may affect an
estrogen-responsive element, and the ()
592) singlenucleotide polymorphism lies within a region with
a
negative regulatory function (139, 143).
Transforming growth factor-b1. One of the cytokines
released during tissue injury and by inflammatory
cells exposed to bacteria and their products is
transforming growth factor-b (258). This cytokine is
described as a double-edged sword, having both
therapeutic and pathologic potential (20). Perio-
dontopathic microorganisms have been reported to
induce the production, by mononuclear phagocytes,
of transforming growth factor-b in vitro, and the
transforming growth factor-b protein was detected
in the early and late stages of periodontal disease
(257).
The gene for transforming growth factor-b1
(TGFB1) is located in chromosome 19q13.1 (70). One
promoter polymorphism, the ()509) C/T, was asso-
ciated with chronic periodontitis severity in Brazilian
Caucasians (P 0.04) (224). However, this single
nucleotide polymorphism, together with the other
polymorphisms, was not related to chronic perio-
dontitis susceptibility in Czech Caucasians (100). The()509) C/T
polymorphism was significantly associ-
ated with the plasma concentration of transforming
growth factor-b1 and osteoporosis in Japanese
subjects (82, 269).
Fc R polymorphisms
FcRIIA
-H131 -R131
His131
Arg131
-158V -158F
FcRIIIA
Phe158
Val158
Cell membrane
-NA1 -NA2
FcRIIIB
Arg18
Ser18
Asn47
Asp64
Val
Ser47
Asn64
Ile88
High Low
(IgG2)
High Low
(IgG1, IgG3)
High Low
(IgG1, IgG3)
Receptor affinity
(Ligand)
GPI GPI
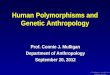
Fig. 2. Human FccR polymorph-
isms. FccRIIA alleles are distin-
guised by the presence of either Arg
or His at amino acid position 131,
whereas FccRIIIA alleles are
determined by either a Val or a Pheat position 158. The
FccRIIIB-NA1/
NA2 polymorphism results in 4
amino acid substitutions, leading to
glycosylation differences (blue cir-
cles). The FccRIIA alleles interact
differntially with human immuno-
globulin G(IgG)2, whereas FccRIIIA
and FccRIIIB affinities are different
upon interaction with human IgG1
and IgG3. GPI glycosylphosphati-
dylinositol.
113
Role of genetic polymorphisms in periodontitis
-
8/10/2019 The role of genetic polymorphisms in periodontitis
13/31
Receptor and other gene polymorphisms
Fc receptor polymorphisms
Leukocyte receptors for the constant (or Fc-) part of
immunoglobulin (FcR) link cellular and humoral
branches of the immune system, which are consid-
ered essential for the host defense against bacteria.
Strong, specific immunoglobulin G responses against
periodontopathic bacteria are observed in the gingi-val tissue
and gingival crevicular fluid (104, 160). FcR
for immunoglobulin G (FccR) may therefore play a
crucial role in the host defense against these bacteria.
FcR profile and gene polymorphisms. The human
leukocyte FccR family consists of three major classes,
and encompasses eight genes (CD64: FccRIA, IB, and
IC; CD32: FccRIIA, IIB and IIC; CD16: FccRIIIA and
IIIB), which have been mapped to the long arm of
chromosome 1 (1q21 and 1q2324) (144, 205, 238).
Most FccR subclasses consist of a separate ligand-
binding chain with an extracellular domain that
contains the immunoglobulin G-binding region, and
signaling chains essential for the initiation of signal
transduction. Neutrophil FccRIIIB is a notable
exception, as it is linked to the outer leaflet of the
lipid bilayer via a glycosyl phosphatidylinositol an-
chor.
Functional bi-allelic polymorphisms have been
identified for three FccR subclasses: FccRIIA, FccRI-
IIA, and FccRIIIB (Fig. 2) (183, 204, 267). FccRIIA
bears either an arginine (FccRIIA-R131) or a histidine
(FccRIIA-H131) at amino acid position 131 in thesecond
extracellular immunoglobulin-like domain
(261, 262). This difference strongly affects the recep-
tor affinity for immunoglobulin G2 (188). FccRIIA-H/
H131 neutrophils internalize human immuno-
globulin G2-opsonized bacteria more efficiently than
FccRIIA-R/R131 neutrophils (24). The FccRIIIA-158V
allotype exhibits higher affinity for both monomeric
and immune-complexed immunoglobulin G1 and
immunoglobulin G3 than does FccRIIIA-158F (132).
The neutrophil-specific FccRIIIB bears the NA1-NA2polymorphism
caused by four amino acid substitu-
tions within the first extracellular immunoglobulin-
like domain (183). Neutrophils from FccRIIIB-NA2
individuals bind immunoglobulin G1 or immuno-
globulin G3 less efficiently than those from FccRIIIB-
NA1 individuals (24) (Fig. 3A). In vitro findings have
suggested that inter-individual differences in the
efficacy of FccR-mediated effector functions depen-
ded on FccR polymorphisms.
Association of FcR polymorphisms with periodontitis
risk. Wilson and Kalmar (264) speculated that
FccRIIA-R/R131 subjects were more susceptible to
periodontitis as a result of the diminished capacity to
phagocytose immunoglobulin G2-opsonized perio-
dontopathic bacteria. It has been well documented
that FccR genes are associated with risk for various
types of periodontitis: aggressive periodontitis,
chronic periodontitis, and recurrent chronic perio-
dontitis (Table 4). Associations between FccR
polymorphisms and susceptibility to aggressive per-
iodontitis have been investigated in Caucasian, Asian
(Japanese and Taiwanese), and African-Americanpopulations. Loos
et al. (150) studied FccRIIA, IIIA,
Table 4. FccR genes related to periodontitis risk
Periodontitis Population FccRIIA FccRIIIA FccRIIIB
References
Aggressive
(early onset)
periodontitis
Caucasian Yes (H131: OR 3.7) Yes (158V: OR 2.6) No (150)
African-American No No Yes (NA2: OR 1.8) (69)
Japanese No No Yes (NA2: OR 2.0) (129)
Taiwanese Yes (R131: OR 2.4) Not tested No (34)
Chronic (adult)periodontitis
Caucasian Yes (H/H131) No No (150, 270)
Japanese No No No (127, 229)
Taiwanese No Not tested No (34)
Severe chronic (adult)
periodontitis
Caucasian Yes (H131: OR 2.4) Yes (158V: OR 2.9) No (150, 162,
270)
Japanese No Yes (158V: OR 2.0) No (130)
Recurrent chronic
(adult) periodontitis
Caucasian No No No (36)
Japanese No Yes (158F: OR 2.9) Yes (NA2: OR 3.3) (128, 230)
114
Yoshie et al.
-
8/10/2019 The role of genetic polymorphisms in periodontitis
14/31
and IIIB genotypes in 12 patients with aggressive
periodontitis and 61 controls of Northern European
Caucasian background. The carriage rate of FccRIIA-
H131 and FccRIIIA-158V was higher in patients with
aggressive periodontitis than in controls, respectively
(P 0.013 and P 0.044), suggesting a putative
susceptibility factor for aggressive periodontitis.
Chung et al. (34) examined FccRIIA and FccRIIIB
genotypes in 30 patients with aggressive periodontitisand 74
healthy controls in Taiwan. FccRIIA-R131 was
found more frequently in the group with aggressive
periodontitis than in the group with chronic perio-
dontitis (P 0.01), but not in the control group. In
contrast, Japanese studies have demonstrated an
over-representation of the FccRIIIB-NA2 allele in
patients with aggressive periodontitis compared to
patients with chronic periodontitis and controls (129,
277), which was in accordance with the results of
African-American patients (69). From these results, it
is conceivable that the FccR-encoding genes related
to aggressive periodontitis risk are different among
ethnic populations.
Relationships between FccR polymorphisms and
chronic periodontitis risk have also been investigated
in detail. There is only one report showing a signifi-
cant association with susceptibility to chronic
periodontitis. Yamamoto et al. (270) indicated a
difference in the FccRIIA genotype distributions
between 213 Caucasian patients with chronic perio-
dontitis and 209 race-matched controls (P 0.036),
with enrichment of the FccRIIA-H/H131 genotype in
the patients compared with the controls. However,
other work failed to show a significant associationwith chronic
periodontitis susceptibility (34, 127, 130,
162). Caucasian patients with chronic periodontitis
and FccRIIA-H/H131 were found to have more teeth
with severe periodontal breakdown than patients
carrying FccRIIA-R131 (150). Likewise, smokers with
FccRIIA-H/H131 exhibited a greater clinical attach-
ment loss than smokers with FccRIIA-R/H131 and
FccRIIA-R/R131 (270). On the other hand, Meisel
et al. (162) indicated a significant association of
FccRIIIA-158V with chronic periodontitis severity
(P 0.010), which was in accordance with a Japanese
study (130).
Three studies have investigated FccR genotype
distributions in patients with recurrent chronic per-
iodontitis. Colombo et al. (36) found no differences in
FcRIIIB polymorphism and neutrophil function
(%)50 75 100
Recurrent chronicperiodontitis (n=85)
22.3 45.9 31.8
Aggressive
periodontitis (n
=
38)
29.0 52.6 18.4
Healthy control(n=104)
11.5 52.9 35.6
Periodontitis -resistant (n=46)
43.5 56.5
Chronicperiodontitis (n=83)
48.2 36.115.7
250
5 15 25
0
20
40
60
Phagocytosis (%)
(min)
IgG1-opsonized
NA1/NA2NA2/NA2 NA1/NA1
A B
Fig. 3. (A) Diminished phagocytosis of immunoglobulin
G(IgG)1-opsonized Porphyromonas gingivalis by neu-
trophils expressing FccRIIIb-NA2/NA2 (closed circles)
compared with IIIb-NA1/NA1 (open circles) in six healthy
controls. Subjects were matched for their FccRIIA R/H131
genotypes. Values represent means standard error
(128). (B) Distribution of FccRIIIB genotypes in Japanese
patients with various types of periodontitis. FccRIIIB-NA2/
NA2 (closed bars) was found more frequently in aggressive
periodontitis patients than in healthy controls (127, 129,
230).
115
Role of genetic polymorphisms in periodontitis
-
8/10/2019 The role of genetic polymorphisms in periodontitis
15/31
FccRIIA and IIIB genotype distributions among the
32 refractory, 54 successfully treated and 27 perio-
dontally healthy groups of Caucasian background.
On the contrary, a significant over-representation of
FccRIIIB-NA2 and FccRIIIA-158F was found in 85
Japanese patients with chronic periodontitis and
disease recurrence as compared with 15 race-mat-
ched chronic periodontitis patients without recur-
rence (P 0.0003 and P 0.009) (127, 229).
Interestingly, FccRIIB polymorphisms may play
an important role in the pathogenesis of periodon-titis, because
of a large numbers of FccRII-bearing
B lymphocytes in the periodontal lesion. Yasuda
et al. (275) found a significant over-representation
of the FccRIIB-232T allele in 32 patients with
aggressive periodontitis, as compared with 72
patients with chronic periodontitis and 72 controls
(P 0.039 and P 0.006), suggesting an association
with susceptibility to aggressive periodontitis in
Japanese subjects.
Hypothetical role of FcR risk allele in periodonti-
tis. The most convincing FccR genes related to
periodontitis risk might be supported by significant
evidence provided in more than two ethnic popu-
lation studies. FccRIIIB-NA2 seems to constitute a
gene-predisposing susceptibility to aggressive peri-
odontitis (Fig. 3B), which might be explained by the
hypothesis demonstrated in Fig. 4. FccRIIIB is a
neutrophil-specific receptor and plays a crucial
role in the control of specific immunoglobulin
G-opsonized pathogens in the gingival crevice.Immunoglobulin G1-
and immunoglobulin G3-ops-
onized P. gingivalis may be more effectively
phagocytosed and killed by FccRIIIB-NA1 than
FccRIIIB-NA2 neutrophils (128). Therefore, ineffi-
cient clearance of periodontopathic bacteria by
neutrophils in FccRIIIB-NA2 subjects may result in
an increased level of bacteria in the gingival crevice,
finally leading to be relatively at high risk of
aggressive periodontitis.
Hypothetical role of FcR genotypes in susceptibility to
periodontitis
cihtapotnodoireP
airetcab
ospO zin a noit
iw th IgG
sisotycogahpdetaidem-GgI
slihportuenybAggressive periodontitis
btneiciffE y
sllec-1AN lamroN
ksiRIn ybtneiciffesllec-2AN
noitagiL of
egahporcam/etyconom
etycohpmyldnaF-NT noitcudorp1-LI/
PC
dorp-lamroN noitcu
in R1 -13 1ro lec-F85 ls
dorp-revO noitcu
in -131H or sllec-V851
lamroN
ksiR
Fig. 4. Hypothetical role of FcR genotypes in suscept-
ibility to periodontitis. Inefficient clearance of perio-
dontopathic bacteria by neutrophils expressing the
low-affinity genotype FccRIIIB-NA2/NA2 may result in an
increased level of bacteria in the gingival crevice, leading
to high susceptibility to periodontitis in younger adults.
The high affinity genotype FccRIIA-H131/H131 and
FccRIIIA-158V/158V may contribute to a strong proin-
flammatory cytokine release by monocytes/macrophages
and lymphocytes upon interaction with immunoglobulin
G(IgG), possibly leading to an increased risk for period-
ontitis in adults.
116
Yoshie et al.
-
8/10/2019 The role of genetic polymorphisms in periodontitis
16/31
Other promising genes influencing susceptibility to
chronic periodontitis are FccRIIA-H131 and FccRI-
IIA-158V. The significance of these two genes might
be related to a hypothetical role of FccRIIA-bearing
monocytes/macrophages and FccRIIIA-expressing
lymphocytes in the periodontium (Fig. 4). FccRIIAand IIIA
cross-linkings have been shown to produce
pro-inflammatory cytokines, such as tumor necrosis
factor-a and interleukin-1b (47, 156). It is therefore
proposed that the high affinity of FccRIIA-H131 and
FccRIIIA-158V to immunoglobulin G contributes to a
high level of pro-inflammatory cytokine release by
monocytes/macrophages and lymphocytes, possibly
leading to an increased risk for chronic periodontitis.
Cytokine and chemokine receptors
Receptors are important constituents of the whole
cytokine system. Through these membrane-bound orcirculating
proteins, cell responses to various cytok-
ines, such as interleukin-6 and tumor necrosis factor-
a, are either elicited or blocked (2, 72). The soluble
form of tumor necrosis factor-receptor 2 (tumor
necrosis factor-R2), which is shed from the cell sur-
face, significantly reduced the loss of connective tis-
sue and alveolar bone in experimental periodontitis
(8, 9, 48). The tumor necrosis factor-R2 (+587) T/G
polymorphism was associated with chronic perio-
dontitis severity in Japanese patients (P 0.0097;
OR 2.61) (218). Given this scenario, this variation
in the tumor necrosis factor-R2 gene could have an
effect on the ability of the receptor to block efficiently
the activity of tumor necrosis factor-a. Using an
intronic (CA)n
polymorphic microsatellite markerwithin the interferon-c
receptor 1 (IFNGR1) gene,
Fraser et al. (67) found a correlation between genetic
polymorphisms and periodontitis in Caucasians
(P 0.014; OR 5.56). It was reported that a strong
correlation exists among the IFNGR1 genotype, cel-
lular responsiveness to interferon-c and clinical dis-
ease features (52). On the other hand, the C-C
chemokine receptor 5 delta32 polymorphism was not
related to periodontitis susceptibility in German
Caucasians (59). Recent reports indicate the role of
interleukin-6 receptor gene polymorphisms in dia-
betes, obesity and serum soluble interleukin-6receptor level
(75, 86, 268). The possible role of var-
iations in the interleukin-6 receptor gene in perio-
dontitis could therefore be investigated in the future.
Metabolism-related polymorphisms
Cathepsin C polymorphisms. Cathepsin C is a prote-
inase, and is expressed in the hyperkeratotic epithe-
lial lesions such as palms, knees and oral keratinized
Possible concept for common polymorphisms
AggressiveAggressive
periodontitisperiodontitis
ChronicChronic
periodontitisperiodontitisPeriodontitisPeriodontitis
SystemicSystemic
diseasesdiseases
Master gene Minor genes Common/shared genes
Fig. 5. Both aggressive and chronic periodontitis may have
shared susceptibility genes, in the same manner as period-
ontitis may share susceptibility genes with other complex,
inflammatory or systemic diseases.
117
Role of genetic polymorphisms in periodontitis
-
8/10/2019 The role of genetic polymorphisms in periodontitis
17/31
gingiva (87). Hart et al. (89, 90) analyzed two con-
sanguineous Jordanian families, and identified a gene
on chromosome 11 (11q14) containing the cathepsin
C gene, responsible for prepubertal periodontitis as
well as Papillon-Lefevre Syndrome. All patients with
pre-pubertal periodontitis were found to be homo-
zygous for an AG mutation at gene position +1040,
resulting in a substitution of the amino acid tyrosine
by a cysteine. This gene polymorphism was shown tobe functional
as there was a diminished activity of
cathepsin C in Papillon-Lefevre Syndrome (247).
Interestingly, other mutations found in the cathepsin
C gene have been linked to Papillon-Lefevre Syn-
drome (41, 89). Recently, Cury et al. (41) demon-
strated a novel TC mutation at gene position +587 in
exon 4, causing substitution of conserved leucine, at
position 196, by a proline. Another study, by Noack
et al. (177), reported two novel gene mutations at
positions 947 and 1268, which was associated with
these two diseases. Functional mutations in the
cathepsin C gene may therefore be considered as
causative for prepubertal periodontitis and Papillon-
Lefevre Syndrome.
Vitamin D receptor polymorphisms. Vitamin D plays
a role in the metabolism of calcium and phosphorus.
The human vitamin D receptor gene is localized in
chromosome 12q12q14 (169), and exhibits func-
tional polymorphisms associated with osteocalcin
levels and bone mineral density (137, 171). Vitamin D
receptor polymorphisms may therefore play a role in
the destruction of alveolar bone. Hennig et al. (91)studied a
restriction fragment length polymorphism
(RFLP) for TaqI in exon 9 in 69 Caucasian patients
with aggressive periodontitis and 72 race-matched
controls. The authors indicated a higher prevalence
of TaqI RFLP (t) in the patients with loca-
lized aggressive periodontitis than in the controls
(P 0.017). In contrast, Yoshihara et al. (276) indi-
cated no association between the vitamin D receptor
genotypes and risk for aggressive periodontitis in the
Japanese. Tachi et al. (236) found an increased fre-
quency of the allele TaqI RFLP (T) in chronic perio-
dontitis patients compared with controls (P 0.04).Another
polymorphism for BsmI (B/b) in exon 8 was
analyzed by de Brito et al. (27), who showed that the
vitamin D receptor haplotype was a risk factor for
chronic periodontitis. Inagaki et al. (108) examined
an association of the ApaI (A/a) and TaqI (T/t)
polymorphisms and periodontal disease progression
in 125 subjects for 23 years, and showed that theApaI
A/A genotype subjects exhibited the highest rate of
the disease progression.
Matrix metalloproteinase polymorphisms. Matrix
metalloproteinases play an important role in con-
nective tissue destruction in periodontitis. Increased
levels of the gene transcript and protein for matrix
metalloproteinase-1 (interstitial collagenase) and
matrix metalloproteinase-3 (stromelysin-1, activator
of collagenase) were found in the periodontitis le-
sions. Therefore, polymorphisms in the promoter
region of matrix metalloproteinase-1 and
matrixmetalloproteinase-3 genes may contribute to sus-
ceptibility to periodontitis. de Souza et al. (223)
showed that the matrix metalloproteinase-1 ()1607)
2G/2G genotype was more frequently observed in 26
patients with severe chronic periodontitis than in 24
patients with moderate chronic periodontitis and 37
controls, all with a Brazilian background. The authors
also examined the matrix metalloproteinase-9 ()1562
C/T) promoter polymorphism, which was not asso-
ciated with susceptibility to chronic periodontitis
(224). Holla et al. (101) indicated that three matrix
metalloproteinase-1 polymorphisms ()
1607 1G/2G,
)519 A/G, and )422 A/T) showed only a small
effect on chronic periodontitis in the Czech popula-
tion. Recently, Itagaki et al. (113) studied matrix
metalloproteinase-1 ()1607 1G/2G) and matrix
metalloproteinase-3 ()1171 5A/6A) polymorphisms
in 37 patients with aggressive periodontitis, in 205
patients with chronic periodontitis, and in 142 heal-
thy controls, all with a Japanese background, but
failed to show a significant association with perio-
dontitis.
Antigen recognition-related polymorphisms.
Human leukocyte antigen polymorphisms. The major
histocompatibility complex system is a cluster of
genes encoding the human leukocyte antigens, which
are located on chromosome 6p21.3 (12). The human
leukocyte antigen region is mainly divided into two
classes: major histocompatibility complex class I
molecules (human leukocyte antigen-A, -B, and -C)
are expressed on most nucleated cells, whereas major
histocompatibility complex class II molecules (hu-
man leukocyte antigen-DP, -DQ, -DR) are expressed
on B- and T lymphocytes, and on macrophages.Shapira et al. (216)
found that human leukocyte
antigen-A9 and -B15 antigens were elevated in
patients with aggressive periodontitis as compared
with healthy controls. Takashiba et al. (239) indicated
a significant association of the human leukocyte
antigen-DQa gene with susceptibility to aggressive
periodontitis in the Japanese. The DQB1 molecule
has been shown, by Ohyama et al. (182), to be critical
in the pathogenesis of aggressive periodontitis. In
118
Yoshie et al.
-
8/10/2019 The role of genetic polymorphisms in periodontitis
18/31
contrast, Hodge et al. (94) reported no association
between the human leukocyte antigen-DQagene and
aggressive periodontitis in Caucasians. Bonfil et al.
(19) demonstrated an important role of human leu-
kocyte antigen-DR4 in susceptibility to aggressive
periodontitis, in which subtypes 0401, 0404, 0405 and
0408 can be a risk factor for the disease. Recently,
Stein et al. (226) elucidated the variety of human
leukocyte antigen associations and the difficulty ofassigning
single human leukocyte antigen markers to
periodontitis in Caucasians. A significant association
of certain human leukocyte antigen alleles (human
leukocyte antigen-A, -B, -Cw, -DRB1, -DRB3/4/5,
-DQB1) has been shown in aggressive periodontitis
and chronic periodontitis by Machulla et al. (153).
CD14 polymorphisms. The CD14 molecule is a
receptor for recognition of lipopolysaccharides, and
initiates the innate immune response to bacterial
invasion. The gene for the CD14 receptor is located
on chromosome 5q2123, consisting of c. 3900 bp
organized in two exons (81). A single nucleotide
polymorphism (CT) was identified in the promoter
region at position )159 upstream from the major
transcriptional site (110), affecting transcriptional
activity (145) and CD14 density (13). Four additional
polymorphisms have recently been identified at
positions )1619, )1359, )1145 and )809, which
influence soluble CD14 levels (254). Holla et al. (100)
found that in Czech patients, the )1359 C/T genotype
was associated with severity of chronic periodontitis,
while the)
159 G/T genotype was not. Yamazaki et al.(274) studied the )159
G/T genotype distribution in
163 Japanese patients and 104 race-matched con-
trols, and indicated that the )159 G/T genotype was
not associated with development of periodontitis, but
may be related to early disease activity. Folwaczny
et al. (62) reported that the )159 G/T genotype was
associated with periodontitis in women, but not in
men, in Germany. These results were consistent with
a recent study with Caucasian subjects by Donati
et al. (51).
n-Formyl-L-methionyl-L-leucyl-L-phenylalanine recep-tor
polymorphisms. The n-formyl-L-methionyl-L-leu-
cyl-L-phenylalanine (fMLP) is a structural analogue of
bacterial products involved in neutrophil chemotaxis.
The fMLP receptors are also involved in the activation
and subsequent response to certain chemotactic
stimuli. The fMLP receptor genes are localized in
chromosome 19 (14). Gwinn et al. (85) examined the
fMLP receptor gene, and found that two single nuc-
leotide base alterations (329 T/C and 378 C/G) were
associated with aggressive periodontitis. These
alterations resulted in amino acid changes (110 Phe/
Ser and 126 Cys/Try) in the fMLP receptor, suggest-
ing a role in ligand binding and G-protein activation.
Differences in fMLP expression levels and chemotaxis
towards fMLP were examined between the fMLP
polymorphisms by Jones et al. (118). More defective
chemotaxis was found in the 126 Cys/Try mutant
than in the 110 Phe/Ser mutant, suggesting a moresevere form of
aggressive periodontitis. In contrast,
Zhang et al. (278) found no association of these fMLP
receptor polymorphisms (329 T/C and 378 C/G) with
susceptibility to aggressive periodontitis.
Issues and concerns on thecandidate gene approach
inperiodontitis
The candidate gene approach tries to identify one
allele of a gene that is more frequently seen in sub-
jects with the disease than in subjects without the
disease. Most of the studies mentioned above have
utilized this approach. These association studies,
which may include members of an affected family or
unrelated cases and controls, can be performed rel-
atively quickly and inexpensively and may allow
identification of genes with small effects (140). Au-
thors assert that candidate gene studies are better
suited for detecting genes underlying common and
more complex disease where the risk associated withany gene is
relatively small (35).
Candidate genes are chosen on the basis of their
known or presumed functions that are thought to
have some plausible role in the disease. There are
three types of candidate genes: functional candidate
genes; positional candidate genes; and expressional
candidate genes (105). Functional candidate genes
are derived from an existing knowledge of the phe-
notype and the potential function of the gene in-
volved after clinical or physiological studies of
affected individuals. Positional candidate genes are
based on the involvement of the gene to a markedlocation after
genetic linkage analyses. Expressional
candidate genes are determined through differences
in gene expression using microarrays.
For several genes, which have been individually
sequenced for association with periodontitis, we see
a scattered picture from different studies of varied
populations and ethnicities. To produce scientifically
sound and meaningful disease-association studies,
some issues and concerns that should be addressed
119
Role of genetic polymorphisms in periodontitis
-
8/10/2019 The role of genetic polymorphisms in periodontitis
19/31
when sequencing candidate genes are discussed
below.
Ethnic heterogeneity
In designing a casecontrol study, subjects should be
carefully matched by ethno-geographic origin in
addition to other potential confounding factors in
order to avoid systematic differences in geneticcomposition
between the two groups (37). Failing to
do so could result in different frequencies of single
nucleotide polymorphism alleles and the unsuspect-
ing investigator might then draw unwarranted con-
clusions about localizations of susceptibility genes
(97). There is also a clear statement that in the pres-
ence of large biological and environmental variability,
genetic effects can differ across different populations,
or even among generations within the population
(111). Ideally, twin studies can be useful in sorting out
genetic heterogeneity and environmental factors, but
there are certain limitations in carrying out twin
studies in subjects with periodontitis (166).
Frequencies of the genetic marker of interest may
also show large heterogeneity between races (112).
Variation in genotype frequencies across diverse
populations may affect the number of individuals at
increased risk for a disease, and population substruc-
ture imbalances may create spurious differences in
genotype frequencies of the compared groupsin gene-
disease association studies (245). For example, specific
interleukin-1 gene variations of interleukin-1A+4845,
interleukin-1A-889 and interleukin-1B+3954 havebeen associated
with increased severity of periodon-
titis in multiple Caucasian studies. However, these
interleukin-1 single single nucleotide polymorphisms
are found in low prevalence among Asians, including
Japanese, Koreans, and Chinese (Fig. 1). Moreover,
association studies of the same candidate genes in
supposedly related populations or ethnicities pro-
duced mixed or conflicting results (53, 95, 96,133, 136,
187, 234). Stephens et al. (227) reported that 3899 dis-
tinct genetic variations at 313 genes exist in unrelated
individuals, including Caucasians, African-Americans,
Asians and Latinos, and thus the diagnostic use ofgenes in
periodontitis might be limited to a specific
population and may not apply globally or across an
ethnic group.
Considering the issues mentioned, it is prudent
to select a more homogenous population (age- and
race-matched), and to study, with caution, the
applicability of a certain gene marker before com-
mencing with any attempts to replicate the same
study in the population under investigation.
Clinical classification
Classifying periodontal diseases has been a long-
standing dilemma largely influenced by paradigms
that reflect the understanding of the nature of peri-
odontal diseases during a given historical period (7).
As a result of its familial tendency, aggressive perio-
dontitis generally appears in individuals before the
age of 35 years, but age alone is not sufficient toestablish
diagnosis. On the other hand, chronic
periodontitis is quite complex and much more
dependent on environmental factors that confront
the patient during his lifetime. In addition, microbial
plaque deposition, smoking and systemic diseases
largely influence the phenotypic expression of the
disease. For these combined reasons, chronic perio-
dontitis is considered to appear later in life. The
periodontist is therefore challenged regarding into
which classification a patient would properly fall.
Another critical problem related to genetics re-
search in periodontitis is the similarity of the fol-
lowing clinical findings: deepening of the periodontal
pocket; and attachment and alveolar bone loss.
Therefore, investigators should strictly adhere to the
classification set during the American Academy of
Periodontology workshop in 1999 (31). Moreover,
subjects falling into the gray zone between aggressive
and chronic periodontitis should be excluded in the
study. Aggressive and chronic periodontitis probably
share a common pathogenic pathway, so several
common polymorphisms may exist and/or overlap
between the two.
Functional polymorphisms and directevidence
In the 2001 report of the International SNP Map
Working Group, they approximated around
1.42 million single nucleotide polymorphisms in the
human genome (201). Sixty thousand of these sin-
gle nucleotide polymorphisms fall within exons.
Structural gene defects can affect the qualitative
response, and regulatory polymorphisms can alter
the response quantitatively. However, many studiesfail to
provide functional evidence for gene poly-
morphisms and periodontal diseases. The majority
only statistically demonstrated an association be-
tween polymorphisms and periodontitis. Moreover,
some of the studied alleles may not be associated
with disease themselves, but instead may be in LD
with the disease-associated allele. If so, because LD
breaks down differently in different populations,
variations in the estimated OR may reflect variable
120
Yoshie et al.
-
8/10/2019 The role of genetic polymorphisms in periodontitis
20/31
LD rather than variation in the true genetic effect
(112).
Kinane et al. (126) outlined the requirements in
providing a disease-polymorphism association: the
polymorphism must influence the gene product;
biases in the study population should be recognized
and controlled for; confounders such as smoking and
socio-economic class must be sorted out; and the
affected gene product should be part of the
diseaseetiopathology. Genetic markers for proposed gene-
disease associations vary in frequency across popu-
lations, but their biological impact on the risk for
common diseases may usually be consistent across
traditional racialboundaries (112).
Common guidelines for associationstudies
When performing candidate gene casecontrolstudies, factors such
as study design, methods of
recruitment of case and controls, selection of can-
didate genes, functional significance of polymor-
phisms chosen for study, and statistical analysis
require close attention to ensure that only genuine
associations are detected (37, 83, 84, 109, 110).
These factors are frequently debated upon in cases
of conflicting results from a similar study.
Size of study groups
One major concern related to genotype studies is thesample size
of the study subjects. Owing to limited
number of samples, most sample sizes in genetics are
small. This scenario describes very well the small
number of cases in aggressive periodontitis associ-
ation studies. The number of subjects in studies of
chronic periodontitis tends to be larger, but varia-
tions do occur. The results of small studies might
differ significantly from the results of larger studies,
but large studies with thousands of participants
might not be carried out (109). Experience from other
clinical domains suggests that small studies maymistakenly yield
more favorable outcomes than lar-
ger studies (112). Wang et al. (260) demonstrated that
if susceptibility alleles have minor allele frequencies
(MAFs) of
-
8/10/2019 The role of genetic polymorphisms in periodontitis
21/31
accuracy. A commentary by Aderem and Hood (1)
summarized the impact of the completion of the
human genome project on biology in general. They
discussed the shifting of approaches in biology, the
effect to small university-based laboratories, aca-
demic vs. industrial strengths and integrating large-
and small-scale sciences. In the succeeding parts,
we discuss several genetic methods and research
advances that could be useful in clarifying the role ofgenetic
polymorphisms in periodontitis.
Multigene model for periodontitis
From the overview of publications mentioned above,
it is reasonable to conclude that both aggressive
periodontitis and chronic periodontitis are not sin-
gle-gene but polygenic diseases. A polygenic model
for periodontitis is presented in Fig. 5. A good
example to describe this model is the risk for Alz-
heimers disease that has been considered to be
substantially influenced by a total of 10 genetic
polymorphisms of inflammation-related molecules,
including pro-inflammatory cytokines and protease
inhibitors (126). It is thought that several of these
relatively common high-risk polymorphisms may be
inherited by an individual, giving them a suscepti-
bility profile (159).
Similarly to other complex diseases, it is estimated
that between 10 and 50 genes with several major
master genes may be involved in periodontitis. So, it
would be more efficient to simultaneously analyze a
large sample size for multiple gene polymorphisms.Recently, a
large-scale investigation of genomic
markers for severe periodontitis was performed (234).
In this study, subjects were genotyped at 637 single
nucleotide polymorphisms in 244 genes using Taq-
man polymerase chain reaction. Genes encoding
gonadotropin-releasing hormone 1, phosphatidy-
linositol 3-kinase regulatory 1, dipeptidylpeptidase 4,
fibrinogen-like 2, and calcitonin receptor were found
to be associated with severe periodontitis. A previous
study performed by the same group sequenced a
total of 310 single nucleotide polymorphisms in 125
candidate genes for their association with
aggressiveperiodontitis and severe chronic periodontitis in a
Japanese population using the Taqman allelic dis-
crimination assay (233). Single nucleotide poly-
morphisms in genes encoding collagen type 4 a1,
collagen type 1 a1 and gp130, among others, were
associated with chronic periodontitis. On the other
hand, single nucleotide polymorphisms in cathepsin
D, collagen type 17 and others were linked with se-
vere chronic periodontitis. Polymorphisms in the
inflammatory mediators and structural factors of
periodontal tissues were associated with periodonti-
tis in Japanese.
Genome screening and linkage analysis
With the concerns for the candidate gene approach
and association studies (e.g. inter- and intra-popu-
lation heterogeneity of periodontitis genes), thesearch for
genes contributing to periodontitis would
be more effective using genome-wide screening and
linkage analysis of affected families or ethnic groups.
In these approaches, all genes are systematically
scanned using panels of microsatellite or single nu-
cleotide polymorphism DNA markers uniformly dis-
tributed along the entire genome.
Numerous papers have employed genomic
screening and linkage analysis as common tools in
the search for genes of other complex diseases, such
as diabetes, inflammatory bowel disease and obesity
(11, 32, 33, 174, 263, 280). The results obtained from
the screenings and analyses of the disorders men-
tioned provide promising results that are worth
considering in the search for periodontitis genes in
the future. However, practical concerns may still
surface in using these methods: models of the allelic
architecture of common diseases, sample size, map
density and sample-collection biases (260).
Other questions that arise in linkage studies of
complex diseases include the number of marker loci
that should be included in the whole genome screen,
and whether single nucleotide polymorphisms or thehighly
polymorphic microsatellite markers, which are
less common throughout the genome but are more
informative, should be preferred (198). Kruglyak (138)
concluded that single nucleotide polymorphisms
could be as informative as microsatellites when there
is a sufficiently dense map, and marker densities of
one per centimorgan or less were sufficient for an
initial screening for linkage. However, difficulties still
existed in linkage studies and the need for larger
samples was encouraged (3).
In 2003, localized aggressive periodontitis was
linked to human chromosome 1q25 (146). In thisstudy, a genetic
linkage analysis was performed first
with four multigenerational families exhibiting the
localized aggressive periodontitis phenotype. Four-
teen chromosome locations were analyzed using a
directed genomic screening approach. The localized
aggressive periodontitis phenotype was linked to a
DNA marker, D1S492, with the LAP locus spanning
about 26 million DNA base pairs between D1S196
and D1S533. In addition, a gene of major effect for
122
Yoshie et al.
-
8/10/2019 The role of genetic polymorphisms in periodontitis
22/31
prepubertal periodontitis was localized by Hart et al.
(90) in chromosome 11q14.
Haplotypes and tag single nucleotidepolymorphisms
The human genome sequence is thought to con-
tain more than 10 million single nucleotide poly-
morphisms with a frequency of >1% (244). Thecombination of
closely linked alleles observed on a
chromosome and inherited as a unit is called a
haplotype. Single nucleotide polymorphisms are
present in the millions but a limited number were
sufficient to define all of the common haplotypes,
and a collection of single nucleotide polymorphisms
can represent at least 95% of the haplotypes studied
(117). The selected limited number of single nucleo-
tide polymorphisms is termed haplotype-tagging
single nucleotide polymorphisms. Most of the genetic
variation represented by the 10 million common
single nucleotide polymorphisms in the population
could be provided by genotyping between 200,000
and 1,000,000 tag single nucleotide polymorphisms
across the genome (30, 71, 76, 190, 244). Some of the
studied alleles, however, may not be associated with
disease themselves, but instead may be in LD with
the disease-associated allele (111). Therefore, know-
ledge of LD may result in a substantial reduction in
the amount of genotyping, with little loss of infor-
mation. Wang et al. (260) placed the general con-
sensus of r2 (degree of LD between alleles) at 0.8,
which is sufficient for tag single nucleotide poly-morphism
mapping to obtain a good coverage of
untyped single nucleotide polymorphisms, allowing
genotyping of a lower number of marked single nu-
cleotide polymorphisms with relatively small losses
in power. They added that if the LD between single
nucleotide polymorphisms is strong, this could result
in the need to carry out up to 7080% less genotyp-
ing. On the other hand, if LD in a region is low,
almost every single nucleotide polymorphism might
have to be genotyped to ensure comprehensive cov-
erage of the region.
Conclusion
With the completion of the human genome project
and the availability of cutting-edge technology,
researchers have turned from studying genetic se-
quences to analyzing a larger number of proteins
encoded by them. Recent studies from multiple
groups have pointed to genetics as an important
determinant of the severity and progression of peri-
odontitis. A number of aspects of the inflammatory
and immune response that are suspected to play a
role in the development of periodontitis have a
clearly defined genetic basis. Currently, the presence
of interleukin genetic variations appears to identify
individuals who are at increased risk for more severe
chronic periodontitis and for a less predictable re-
sponse to therapy. A correlation of genetic polymor-phisms with
periodontitis, such as that demonstrated
in the Fc receptor gene, appear to provide the
promising use of genetic determinants in periodon-
titis.
Applying genetic information and tech