Embed Size (px)
Citation preview
The Vascular Exam
Jason Davis, MDJason Davis, MD
Before the Exam…Obtain historyAcute vs. Chronic symptomsDistribution of symptoms
Level(s) of extremity pain, etc.Aggravating, Relieving factors
Activity/rest, elevation/dependenceCo-morbid conditions, vitals
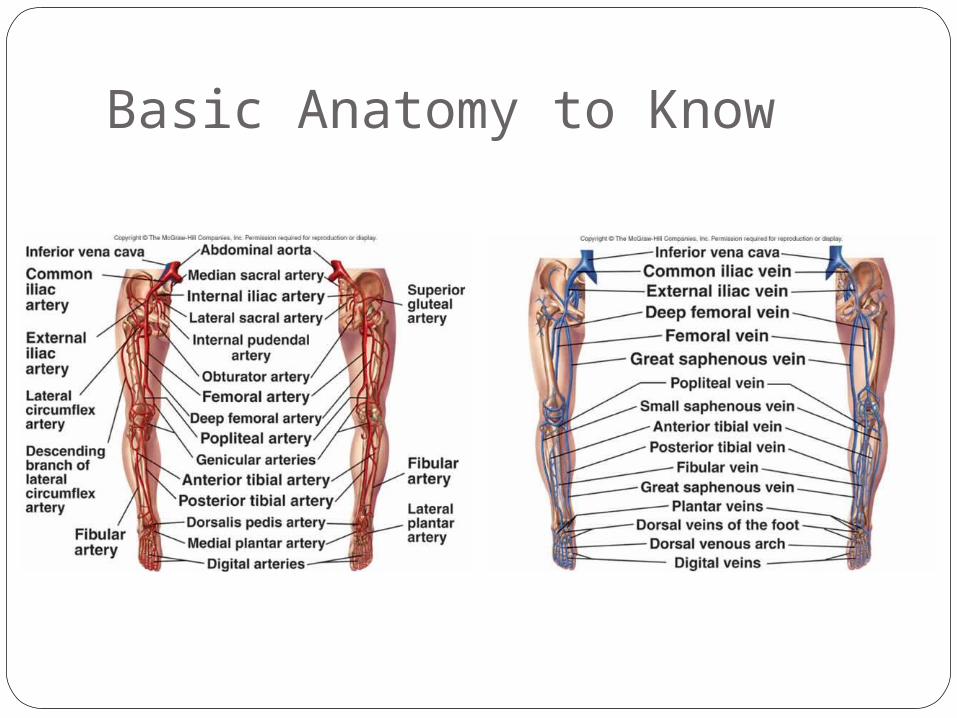
Basic Anatomy to Know

Basic Anatomy to Know
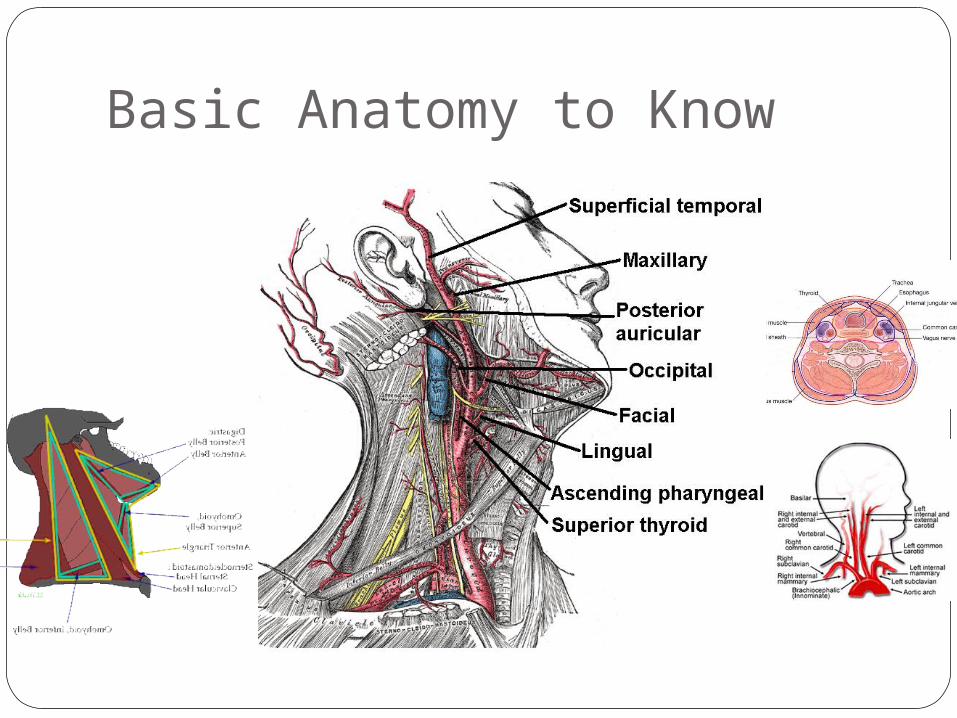
Basic Anatomy to Know
Elements of Vascular Exam
Inspect, Palpate, AuscultateSkin pallor/rubor, mottling/ cyanosis,
temperature, atrophy, hair distributionMotor function and sensory examTissue loss, ulcerationsPulse +/- doppler exam
Always compare each w/ contralateral
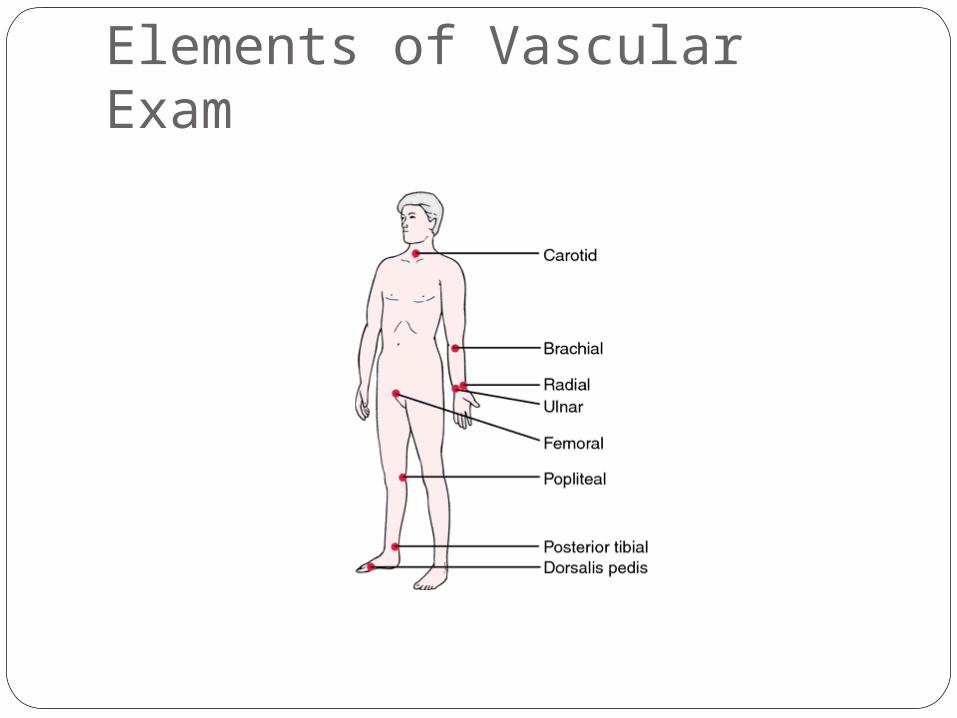
Elements of Vascular Exam
Vascular Exam tips
■ Doppler signals are NOT Pulses– Palpable pulses include carotid, brachial, radial,
ulnar, femoral, popliteal, dorsalis pedis, posterior tib
■ Bruits vs. Thrills: Audible vs. Palpable■ Characterization of Pulses
– Character (bounding, thready), Rate, Rhythm■ Characterization of Doppler Signals
– Triphasic, Biphasic, Monophasic
Trauma / Hypovolemia■ If you can palpate:
– Radial pulse, then SBP is >70 - 80– Femoral + Carotid, then SBP >50 - 70– Carotid only, then SBP >40 - 60
■ NEVER rely on pulses alone for hypovolemia assessment
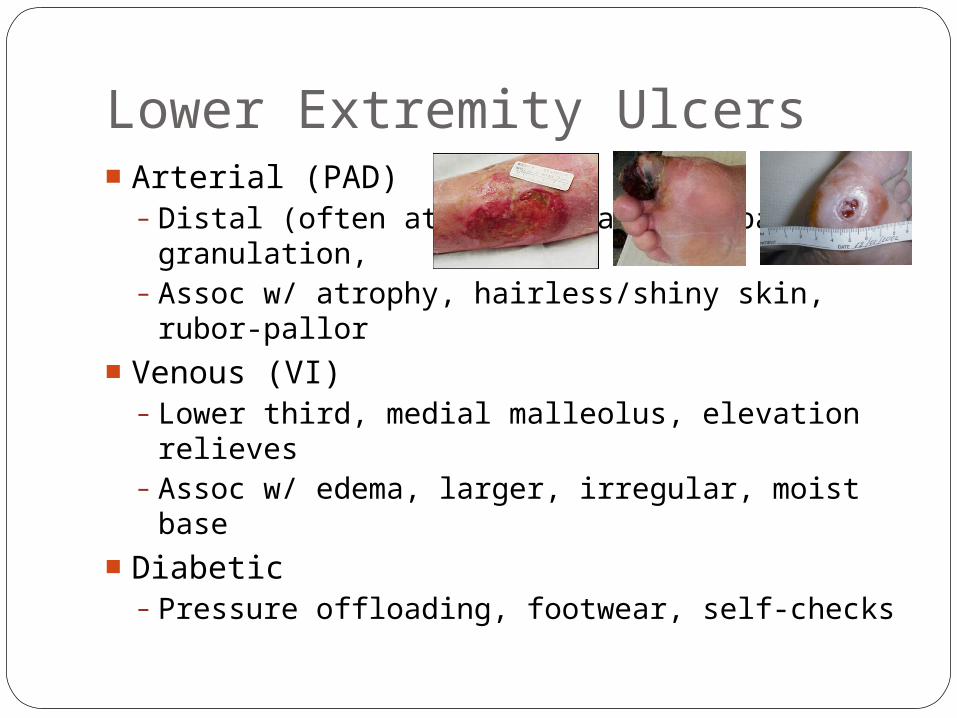
Lower Extremity Ulcers■ Arterial (PAD)
– Distal (often at toes), painful, pale granulation,
– Assoc w/ atrophy, hairless/shiny skin, rubor-pallor
■ Venous (VI)– Lower third, medial malleolus, elevation
relieves– Assoc w/ edema, larger, irregular, moist base
■ Diabetic– Pressure offloading, footwear, self-checks
Common Vascular Problems■ Peripheral arterial disease
– Thrombotic (DM, atherosclerosis)– Embolic (atrial fibrillation, Aneurysms)
■ Venous insufficiency■ DVT, thrombophlebitis■ Carotid artery stenosis■ Compartment Syndrome■ Trauma
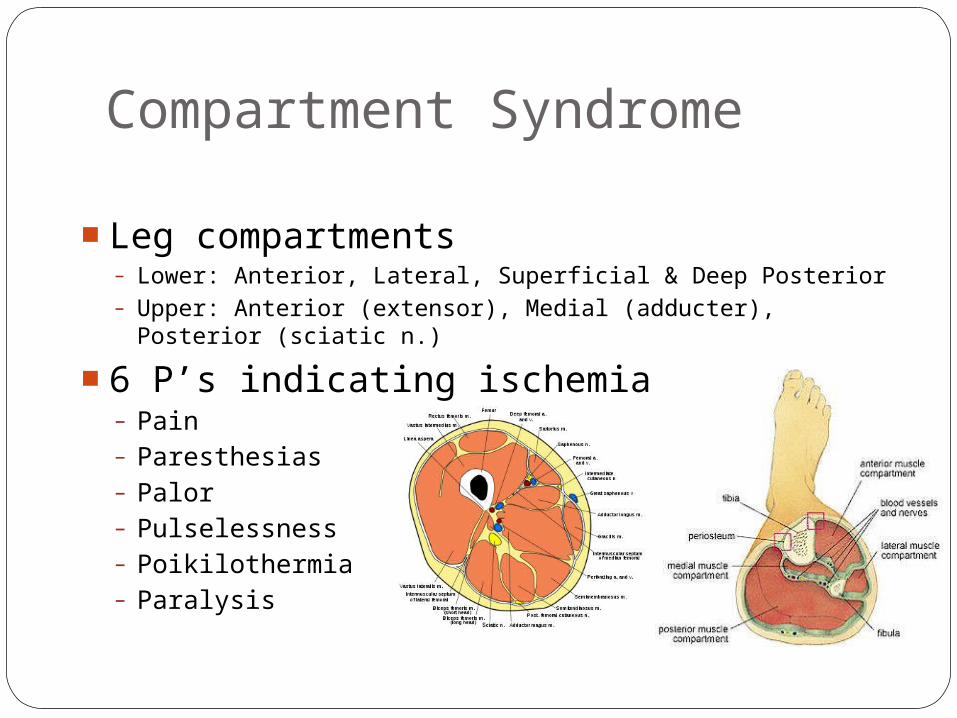
Compartment Syndrome
■ Leg compartments– Lower: Anterior, Lateral, Superficial & Deep Posterior– Upper: Anterior (extensor), Medial (adducter), Posterior
(sciatic n.)
■ 6 P’s indicating ischemia– Pain– Paresthesias– Palor– Pulselessness– Poikilothermia– Paralysis
Clinical Scenario #1■ Routine 5pm ED consult for cellulitis.
Clinical Scenario #1
■ Routine 5pm ED consult for cellulitis. ■ You see before leaving within your hrs■ On arrival, 78yo male w/ DM, CAD, +tobacco■ Also, hx of “irregular HR” with INR of 1.1■ Rt foot cooler than Lt, no palp Rt DP or PT■ Acute onset severe pain started 3hrs ago■ Embolectomy and anticoagulation
■ Don’t forget fasciotomy
Clinical Scenario #2■ New consult for non-healing ulcer, evaluate
for peripheral arterial bypass.
Clinical Scenario #2■ New consult for non-healing ulcer, evaluate
for peripheral arterial bypass.■ Obese 63yo M dialysis w/ DM, HTN■ Legs down in chair, severely edematous■ Advised to elevate and compression
garments, but does not b/c uncomfortable■ Non-tender medial malleolar ulcer x3 wk■ B/L DP and PT are palpable
Clinical Scenario #3
■ Stat consult to 3A for r/o compartment sx.■ 39yo F s/p cardiac cath via L radial artery■ Cath performed for cough, was normal■ After sheath removed, arm doubled in size■ Nurses want to know when pt going to OR
Clinical Scenario #3
■ Stat consult to 3A for r/o compartment sx.■ 39yo F s/p cardiac cath via L radial artery■ Cath performed for sneezing, found normal■ After sheath removed, arm doubled in size
■ Direct pressure applied, bleeding ceased■ Palpable distal pulses were appreciated■ Neurovascular exam intact w/ serial
exams■ Arm elevated to facilitate venous return
Berger’s Pet Peaves■ No overnight pre-op IVF unless dehydration
established or elderly pt AND afternoon case■ Reglan for N/V unless obstruction, espec DM
■ Zofran ONLY if nausea refractory to Reglan■ Only attg name on consents except as witness
■ Residents can, however, sign blood consents■ SCD’s for AAA’s only (NOT CEA’s, bypasses, etc)■ Vaseline gauze, NEVER iodoform gauze■ Do NOT elevate extremities after access cases
■ Increases steal symptoms and neuropathy■ Peri-op edema will resolve, heart level adequate
■ Dextran x24hrs for all CEA’s EXCEPT Berger’s
Vascular Studies■ Duplex
■ Doppler
■ B-mode doppler
■ ABI/PVR (LEADs)








![upper extremity exam[1] - Lincoln. B. Pain Clinic LTD • Learn to scrutinize pt for unique physical and key findings • To master the art of the upper extremity and neck neurologic](https://img.pdfslide.net/doc/110x75/5ab604b47f8b9a7c5b8d4bf1/upper-extremity-exam1-lincoln-b-pain-clinic-learn-to-scrutinize-pt-for.jpg)




















