Embed Size (px)
Citation preview

Therapeutic Contact Lenses for Ocular Surface Disease
Lynette K. Johns, OD, FAAO, FSLS, FBCLA

Disclosure
• Clinical and education consultant for Bausch + Lomb Boston GP Division
• Adjunct Assistant Professor at the New England College of Optometry

Overview•Dry eye classification• Indications for bandage soft contact lenses• Indications for scleral lenses•Quality of Life•Long-term management•Limitations of CL and Scleral Lenses•Supplemental treatments

International Dry Eye Workshop•Expert committee including clinicians and
clinical scientists•Defined and classified dry eye disease•Epidemiology•Diagnosis, monitoring, treatment and
management•Research and clinical trials
4

Dry Eye Disease• Multifactorial
• Tears• Ocular Surface
• Symptoms• Discomfort• Visual • Tear Film Instability
• Associated Features• Increased Tear Osmolarity• Inflammation of Ocular Surface

Dry Eye Disease• Aqueous deficient
• Sjogren’s syndrome• Non-Sjogren’s (age related)
• Evaporative• Meibomitis/Posterior Blepharitis• Environmental• Contact lens related
• Post-refractive surgery• Allergic keratoconjuntivitis• Blink abnormalities

Dry Eye and Ocular Surface Disease :Classification
From 2007 report of International Dry Eye WorkShop (DEWS)Ocular surface 2007; 5 65-198.

EarlyTimeline of Contact Lenses
•1st century A.D. Celsus applied honey soaked linen to conjunctiva s/p pterygium removal
•1888-1889 Fick, Kalt and Muller report using glass scleral lenses
•1960 First publication of soft hydrogel polymers for biologic use (Wichterle O, Lim D: Hydrophilic gels for biologic use. Nature 185: 117-118.)
•1963 Fredrick Ridley reports a review of 3,000 scleral fits over 13 years. (Ridley, F. Scleral Contact Lenses: Their Clinical Significance Arch of Ophthal 70: 740-745)
•1970 First report of bandage soft contact lens use (Gasset AR, Kaufman HE: Therapeutic uses of hydrophilic contact lenses. Am J Ophthal 69: 252-259.)
•1971 first soft contact lens was FDA approved
8

Therapeutic Soft Contact Lenses
9

Therapeutic Indications of Contact Lenses
Protection from the lid•Trichiasis•Distichiasis•Keratinized lid margins

Therapeutic Indications of Contact Lenses
Protection from exposure
• Bell’s /CN VII Palsy• Acoustic Neuroma• Möbius syndrome• s/p Blepharoplasty• Orbital Disease
Neurogenic & Mechanical Exposure

Therapeutic Indications of Contact Lenses
Keratoprosthesis Type 1•Lubrication of corneal graft host•Protection from ulceration

Re-epithelialization
http://www.visiomed.co.za/prk.php
•Persistent Epithelial Defects•Post-operative protection
Therapeutic Indications of Contact Lenses

Therapeutic Indications of Contact Lenses
Pain Relief
•Filamentary Keratitis•Bullous Keratopathy•Post-operative

Piggyback Therapeutic Contact Lenses
MLADEN ANTONOV/AFP/Getty Images
15

Piggyback Contact Lens system
Therapeutic Indications of Contact Lenses

FDA Approved Silicone Hydrogel Bandage Contact LensesLotrafilcon A Balafilcon A
• AIR OPTIX® NIGHT & DAY® AQUA
• CIBA VISION®• Approved 2003• BC 8.4, 8.6• Dia 13.8• Dk 140, 24% H2O
• PureVision™• Bausch + Lomb• Approved 2005• BC 8.3, 8.6• Dia 14.0• Dk 91, 36% H2O
Senofilcon A
• ACUVUE® OASYS®
• VISTAKON®
• Approved 2007
• BC 8.4, 8.8
• Dia 14.0
• Dk 103, 38% H2O

Therapeutic Scleral Lenses
18

Therapeutic Uses of Scleral Devices• Vision Rehabilitation• Protection from Lids• Protection from Exposure• Surface Lubrication• Pain relief• Re-epithelialization

Therapeutic Benefits of Scleral Lenses
Initial Presentation After 4.5 hours scleral lens wear
Constant Surface Lubrication

Improving Quality of LifeExamples in Literature
21

Graft versus Host Disease
• Transplanted bone marrow/stem cells recognize recipient tissue as foreign
• Acute form within the first 90-100 days after transplant
• Affects skin, liver, mucosa, gastrointestinal tract• Dry eye affects 50% patients who had allogenic
bone marrow transplant

Graft versus Host Disease

Ocular Graft versus Host Disease• Keratoconjunctivitis sicca• Cicatricial lagophthalmos• Conjunctivitis• Corneal ulceration/melt• Uveitis• Ectropian• Cataract
Ogawa Y, Kuwana, M. Dry eye as a major complication of graft-versus-host disease after hematopoietic stem cell transplantation. Cornea 2003 (22) suppl. 1 S19-27

Ocular Surface Disease Index
• 12 question validated self-administerred psychometric tool
• 3 subscales▫Ocular Symptoms▫Visual Function▫Environmental Triggers
• Can be used as an endpoint in clinical trials• Aids monitoring of treatment outcomes• Available online via ALLERGAN• Scoring OSDI© = (sum of scores) x 25 (# of questions answered)Schiffman R, et al. Reliability and validity of the Ocular Surface Disease Index.
ArchOphthalmol 2000;118:615-621.

Ocular Surface Disease Index Scoring
Normal Mild Moderate Severe
0-12 13-22 23-32 33-100

Soft Contact Lenses and cGVHD
Eye & Contact Lens 33(3): 144–147, 2007
• Focus NIGHT & DAY®
• n = 8
• Continuous wear x 7 days over 1 month
• Improvement in VA
• Reduction in OSDI from 77 to 31
• Schirmer’s and Staining remained unchanged

Scleral Lenses and cGVHD
• Boston Scleral Lens
• n = 9
• Retrospective review
• Reduction in OSDI from 81 to 21 after 2 weeks
• Further reduced to 12 after 1 – 23 months
Biology of Blood and Bone Marrow Transplantation. 13: 1016-1021. 2007

Scleral Lenses and cGVHD
Eye & Contact Lens 2008 34(6): 302–305. 2008
Cornea 2007 (26) 10: 1193-1195
• n = 5
• retrospective review 2007
• 4-14 month follow-up
• Improvement in VA
• Subjective improvement in symptoms
• n = 33
• retrospective review 2002 -2005
• Survey regarding pain (52 % reduction), photophobia (63% reduction), quality of life (73 % improvement)
• 22 wearing devices for 3 months – 2 years

Long-Term Management
30

Management of Recurrent Corneal Erosions
•Recurrent epithelial erosions•Associated with trauma and anterior corneal
dystrophies•Characterized by
▫Pain (worse in mornings)▫Injection▫Tearing▫Photophobia
31

32
Management of Recurrent Corneal Erosions

Treatment of Recurrent Corneal Erosions
•Hyperosmotic agents•Lubricants•Bandage contact lenses•Tetracyclines•Superficial keratectomy•Anterior stromal puncture•Phototherapeutic keratectomy
33

Cornea (30) 2: 164-166. 2011
•Retrospective review recalcitrant RCE•n = 12•Bandage soft CL worn for 3 months (replaced every 2 weeks) with antibiotic prophylaxis•75 % of patients had no recurrence of RCE after 1 year
Management of Recurrent Corneal Erosions

Management of Recurrent Corneal Erosions
•Randomized (unmasked) Controlled Study•n = 29•Bandage soft CL worn for 3 months (replaced every 30 days) •Ocular Lubricants (Lacrilube, Celluvisc) QID for 3 mos•No difference in recurrence between groups. CL provide better initial comfort
Cornea (32) 10: 1311-1314. 2013

Management of Persistent Epithelial Defects
•Photodocumentation•Extended wear of scleral device•Daily monitoring •Antibiotic prophylaxis•Daily disinfection of device and replenishment of
fluid•Longstanding PED’s can be managed with
exchange of 2 devices q12 hours•Weekend monitoring•DOCUMENTATION!!!!!!
36

10/25/200710/27/200711/05/2007
Management of Persistent Epithelial Defects

Corneal Perforation: Symptoms, Signs
SymptomsPainImpaired vision“Excessive tearing”
SignsFlat Anterior ChamberPositive Seidel Sign (independent or with pressure)Iris Prolapse
CausesInfectiousAutoimmuneTrauma

Cases
39

56 y.o. F referred for scleral lenses for exposure keratitis and lagophthalmos
• Blepharoplasty #1 at age 32 OU UL & LL, revision 4 lids, hard palate graft, canthoplasty, hard palate grafts removed, soft palate grafts, soft palate graft removal, cheek lifts, punctal cautery x4
• Total 38 facial and oculoplastic procedures
• Systemic history of Systemic Lupus Erythematosus, Fibromyalgia, Migraine
• Systemic meds: Namenda, Verapamil, Zolazepam, Vicodin
Ocular Surface Disease Case 1

• Ocular Meds: Tobradex 2x/week OU, Lacrilube OU qhs, Vigamox prn— “when eye is red”
• Chief complaint: dryness and pain OS>OD, inability to close OS, light sensitivity soft contact lens intolerant• VA entering (specs): OD: 20/25-2 OS: 20/20• 7th nerve paresis, lagophthalmos, 2+ PEE (Oxford staining scale)• TBUT: OD: 8 seconds OS: 7 seconds• Schirmer’s: OD: 9 mm, OS: 7 mm• Fitting goals: 1. Support ocular surface, 2. Improve comfort. 3. Improve vision
•Fit OU with scleral devices OD: 20/20-2 OS: 20/15-2 No corneal or conjunctival staining after 6 hours
Case 1

61 y.o. F referred for PROSE treatment for cicatrizing conjunctivitis and dry eye (x 10 years) associated with ocular cicatricial pemphigoid
• Systemic meds: Prednisone 5 mg q.o.d., Methotrexate injection 20 mg/week, Doxycycline 200 mg/day
•Ocular Meds: Restasis BID OU
• Past ocular treatments: Punctal plugs x4, cautery inferior OU, bandage contact lenses
• Chief Complaint: Pain, Dryness, Photophobia
Ocular Surface Disease Case 2

Case 2
• Entering VA (specs): OD: 20/40 OS: 20/40-2• Superior mild injection OD, inferonasal symblepharon OS
• Bilateral 1+ PEE (Oxford grading scale)
• Schirmer’s: OD: 7 mm, OS: 3 mm
• Fitting goals: 1. Improve Comfort, 2. Improve vision
•Fit and dispensed OU with VA 20/25 OD and 20/30+1

Case 2
• September 2005• OD: 16.5 OS: 16.5
• May 2006• OD: 18.0 OS: 18.0
• October 2007• OD: 18.0 OS: 18.0
• April 2008• OD: 17.5 OS: 18.0
• November 2008•Bandage soft CL OU

Example conditions and considerationsSjögren’s syndrome
Increased risk (44x) for Mucosa-Associated Lymphoid Tissue (MALT) lymphoma—non Hodgkin’s lymphoma
SclerodermaHandling Issues
Neurotrophic KeratitisRedness is the patient’s only cue something is wrongRequires a near-flawless scleral fit
Retinal surgeryScleral device diameter and haptic issuesLimit impingement and aggravation of irregular conjunctiva
Patch graft for perforationVisual rehabilitation

Ocular Surface Disease Case 3
61 y.o. F referred for resurfacing PED 1 month s/p patch for perforation • 3 eye surgeries in prior 6m • s/p Phaco CE, PCIOL• s/p PPV/AFx/EL/16% C3F8• s/p PK Patch graft for descemetocele• Secondary Sjögren’s syndrome • Neurotrophic cornea• ? Stem cell deficient

Case 3
Current TX by specialist : Vigamox QIDPF Pred Forte BIDSerum Tears q2hDoxy 50 mg p.o QDBandage CL

Case 3
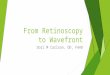
Re-surfaced after 6 days continuous wear and Vigamox in the device

Figure 2
a
b c d
Novel Applications- Drug Delivery
Keating A., Jacobs D. Anti-VEGF Treatment of Corneal Neovascularization. The Ocular Surface. 2011 9 (4): 40-51.

October 20071w after continuous then daily wear of Boston Ocular Surface Prosthesis VA =CF 6’
March 2008: VA: 20/400s/p 3 months topical Avastin in BOSP , suture removal, systemic steroid. ?PK for vision
Case 3

July 2011s/p PKP January 2011VA 20/50
•Overnight wear with device and one drop Vigamox. •Resurfaced in 24 hours
Case 3

Limitations
52

Limitations of Soft Contact Lenses
• Lens retention• Desiccation• Inability to correct irregular astigmatism• Dependency on doctor for applications• Microbial keratitis

Limitations of Scleral Lenses
• Daily wear• Surface Debris• Chamber debris• Bubbles• Suction• Handling• Microbial Keratitis

Microbial Keratitis: Risk for both soft lenses and scleral devices

Lens Management Considerations
Soft Lenses & Scleral Lenses
•Depends on patients condition•Application and removal•Overnight wear?•Prophylactic antibiotic?•Close management

Soft Lens Studies that we discussed•GVHD:
▫Continuous wear x 7 days ▫1 month▫no antibiotic
•RCE: ▫Continuous wear x 2 Weeks▫3 months▫Antibiotic prophylaxis

Supplemental Management
58

Daytime Management with Lenses/Devices Lubricants over
lenses Medications with
lenses Refreshing lenses Punctal plugs Moisture goggles

Nighttime Management: To sleep or not to sleep in the lens/device?
•Overnight ointment•Tape tarsorrhaphy•Nighttime goggles