Embed Size (px)
Citation preview

Journal ofNeurology, Neurosurgery, andPsychiatry, 1977, 40, 937-950
Therapeutic embolisation of the external carotidarterial treeBRIAN KENDALL AND IVAN MOSELEY1
From the Lysholm Radiological Department, National Hospital for Nervous Diseases, Queen Square,London
SUMMARY Intra-arterial embolisation is a valuable adjunct to the treatment of many vascularlesions, including neoplasms such as glomus tumours or juvenile angiofibromas, and arterio-venous malformations. Its place in the management of the individual patient should beestablished before any surgical procedure is carried out, as this may prejudice the eventualresult. The indications for the procedure, the technique, and possible complications are discussedin this paper, and it is emphasised that the latter are best avoided by the use of a scrupuloustechnique and adequate technical facilities.
Therapeutic intra-arterial embolisation of vascularlesions is not a new technique; it was suggested in1930 by Brooks, at a time when carotid angio-graphy itself had been practised for only threeyears. Since then it has been used extensively asan adjunct to surgery or as definitive therapy, andthe purpose of the present article is to describesome of its applications and advantages in themanagement of vascular lesions of the neck andhead.The aim of intravascular embolisation is to
occlude the blood vessels of a tumour or othervascular lesion which is either inaccessible to sur-gery, or in which surgery could involve consider-able haemorrhage, within the lesion itself or at acritical level. Thus, in the case of a vascular mal-formation or tumour in the external carotidterritory, ligation or occlusion of feeding vesselsat some distance from the shunt or tumour bedhas repeatedly been shown to result in the rapiddevelopment of collateral supply; the placementof emboli within the pathological vessels them-selves precludes this.
In the external carotid territory embolisationmay be useful in the management of angiomas: ofthe skin, tongue, bone, or dura mater; of arterio-venous fistulae, eg caroticocavernous; and oftumours: glomus tumours, angiofibromas, menin-giomas, or malignant tumours. Similar lesions
1 Address for reprint requests: Dr I. F. Moseley, The NationalHospital, Queen Square, London WCIN 3BG.Accepted 16 April 1977
can, of course, be treated in other parts of thebody.The contraindications to embolisation include
allergy to angiographic contrast medium (but seecase 6), and atheroma of the carotid bifurcation,which precludes selective catheterisation. There islittle indication for the treatment of lesions whichpresent no difficulty at surgery and are unlikely toproduce poor cosmetic results.Brooks (1930) recommended muscle as the
embolic material, while later workers have usedradio-opaque metallic, plastic, or silicone spheres(Luessenhop, 1969) or Gelfoam fragments (Ishi-mori et al., 1967). More recently, rapidly solidify-ing liquids have been prepared for embolisation.We have consistently used fragments of Gelfoam,which is non-antigenic. These have the advantagesof being relatively cheap and simple to handle andprepare; their size can be finely adjusted to theindividual case. Injection of even large fragmentsis easy and does not require a large catheter. Al-though they appear to provide a satisfactorythrombosis, we feel that a single fragment mis-placed in a vessel which it is not intended toembolise may be less harmful than a rigid metalor plastic sphere. The use of rapidly solidifyingliquids, although very effective, may produce amore complete occlusion than is desirable of someof the tiny normal vessels arising from branchesof the external carotid artery to supply thecranial nerves.
Preparation of the patient is important. If theexternal carotid artery is to be embolised, it is
937
Protected by copyright.
on August 1, 2020 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.40.10.937 on 1 October 1977. D
ownloaded from
Brian Kendall and Ivan Moseley
essential that the patient should understand thatthere is a risk of permanent neurological deficit,very minor though this may be; full informedconsent must, therefore, be given. The proceduremay be carried out under local or general anaes-thesia: the former has the advantage that theneurological state of the patient may be monitoredcontinuously, the latter that pain on injection ofthe external carotid artery branches, which maycause the patient to move and impair the diag-nostic quality of the radiographs, is avoided.Embolisation of a complex lesion may also bea lengthy procedure. As a rule we use generalanaesthesia.The catheter through which embolisation is to
be carried out may be introduced by direct exter-nal or common carotid puncture, or by retrogradeSeldinger catheterisation of the axillary or femoralarteries. We use the last approach which has threemain advantages: it is the one through whichmanipulation of the catheter is easiest, theoperator's hands are kept far from the radiationfield, and all the head and neck vessels may beinjected after a single arterial puncture.
Adequate fluoroscopic and radiographic appara-tus is also very important. We use a caesiumiodide image intensifier which can be used in thelateral position for fluoroscopy, and the angio-graphic series are carried out with 2 X or 3 Xmagnification, using a 0.2 mm focal spot tube.Any compromise on apparatus may prejudice theefficacy and safety of the procedure.
In adults we use the standard flexible, thin-walled 5F gauge catheters, while in young child-ren, smaller tubing may be used. The first stageof the procedure is filming of the carotid bifurca-tion to exclude ulcerating or stenosing atheroma,followed by the documentation of the vascularsupply of the lesion to be embolised, and it is ourpractice to inject first those vessels of which em-bolisation is unlikely to be possible-that is, theinternal carotid and vertebral arteries. If mostof the blood supply to the lesion arises from thesevessels, or if there are widely patent anastomosesbetween them and the external carotid branches,embolisation is not feasible (Figs. 1, 2).
Next, one of the external carotid arterybranches supplying the lesion is catheterised;lateral fluoroscopy is particularly useful duringthis superselective catheterisation. An angio-graphic series is then performed and this is in-spected before embolisation to determine: (i) thedegree and nature of pathological vascularity-that is, the presence or absence of significantarteriovenous shunting: if there is no pathological
vascular bed, emboli will pass directly throughinto the venous circulation; (ii) the size of thevessels feeding the lesion and the volume of flowwithin them: this will determine the size of theemboli to be injected and the speed of the injec-tion; (iii) the presence of anastomoses with theinternal carotid or vertebrobasilar trees, whichwill contraindicate embolisation; and (iv) thesuperselectivity of the catheterisation, and lack ofreflux into the internal carotid or vertebralcirculations.
If the angiographic appearances are satisfactoryfor embolisation, small fragments of Gelfoam arecut with fine scissors, the size depending on thatof the vessels to be occluded, and suspended innon-heparinised saline. The syringes which areused for injecting the emboli are distinctivelymarked, and are used for this purpose only. Justbefore embolisation, and repeatedly during theprocedure, the catheter is inspected fluoroscopic-ally to ensure that it has not moved. Ten to 20emboli are then injected, followed by a smallquantity of contrast material to check fluoro-scopically that the vessel is still patent and thatreflux is not occurring.
This procedure is repeated, using progressivelylarger emboli, until it is clear at fluoroscopy thatthe flow in the catheterised vessel has slowedsignificantly. Another angiogram is then obtained.If this demonstrates almost complete occlusion ofthe pathological vessels, no further emboli areinjected; it is not the aim to achieve completeblockage of the feeding vessel at this stage as thismay be hazardous. If there is no flow, markedspasm, a proximal block, or obvious reflux, embo-lisation of that vessel is also terminated, for thetime being at least.
Successful embolisation depends in part on pre-ferential flow towards vascular lesions; when thisis abolished, there is no force directing the embolito their desired site. The same procedure iscarried out until all the feeding vessels have beendealt with, although with very extensive lesions itmay be necessary to carry out embolisation inseveral stages.Some workers have suggested the injection of a
sclerosant or thrombogenic agent at the end ofthe embolisation of each vessel (Djindjian, 1977)but we have not found this necessary.When embolisation appears complete, a flush
injection is made into the external carotid artery.This will demonstrate any remaining vascularlesions, and in many cases, by reflux, confirm thatthe internal carotid artery remains normallypatent.
938
Protected by copyright.
on August 1, 2020 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.40.10.937 on 1 October 1977. D
ownloaded from
Therapeutic embolisation of the external carotid arterial tree 939
__
V:t:
:t:b*: w <'w' ..... :.\ 4
*YO:"___
,l :, s'
j.a:.S
,:*#0.
A
V ,...Fig. 1 Glomus jugularetumour-vertebral angiogram.(All illustrations are lateralprojections, subtracted, theright margin being anterior.)There is massive supply to thetumour (open arrowheads).External carotid supply was
negligible, and the lesion wasnot treated by embolisation.
The following eight case reports illustrate theindications for the procedure and the modificationsto the basic technique which may be necessary.
Case 1 Facial angioma
PL, a 30 year old moneybroker, complained ofintermittent bleeding from a lump affecting theleft upper lip and alveolus. There was also recur-rent gingivitis which had caused loosening of hisfront teeth and it was now considered necessaryto remove these. Because of the danger of tor-rential haemorrhage he was referred for embo-lisation in order to reduce the blood supply to the
superior alveolus. Examination confirmed an ex-tensive angiomatous malformation of the leftupper lip and alveolus.On 14 November 1975 superselective angio-
graphy showed that the malformation was suppliedby the superior alveolar, major palatine andsphenopalatine branches of the maxillary arteries,and by branches of both facial arteries. There wasno supply from other vessels. Gelfoam emboliwere injected into the branches supplying thelesion, and repeat angiography at the terminationof the procedure showed that there was only avery minor residuum (Fig. 3).Over the 24 hours after embolisation there was
Arjo.I0 Alwx :4
Ankow,.AV.wl "
Protected by copyright.
on August 1, 2020 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.40.10.937 on 1 October 1977. D
ownloaded from

Brian Kendall and Ivan Moseley
Fig. 2 Glomus jugulare tumour-internal carotid arteriogram. There issupply (open arrows) from the internalcarotid artery which is constricted(arrow). The patient, a 19 year old girl,had minor symptoms, and it wasconsidered unjustifiable to attemptremoval of this portion of the tumour.The tumour in the neck (below dottedline) was supplied by external carotidartery branches and is opacified byreflux. This was effectively embolised.
progressive and considerable reduction in the sizeof the malformation and there were no adverseeffects. Four days later the patient complained ofa feeling of stiffness in the region of the angioma,but this soon abated. The patient's teeth wereremoved without undue haemorrhage.
Case 2 Facial angioma
AM, a 22 year old housewife, complained of a
small fluctuant swellin2 of the left eyelid and the
adjacent malar region. At angiography, carriedout before cosmetic surgery to determine theblood supply, this was seen to be an angioma,largely supplied by the superficial temporal artery,with a small contribution from the supraorbitalbranch of the ophthalmic artery.The superficial temporal artery was then
embolised (Fig. 4). The object of embolisationin this case was merely to facilitate surgery, butit was so effective that no operation wasrequired.
940
*. 041tM:,'A
Protected by copyright.
on August 1, 2020 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.40.10.937 on 1 October 1977. D
ownloaded from

Therapeutic embolisation of the external carotid arterial tree
F -.I/
{(aa (1)
Fig. 3 Case I Facial angioma-selective injection of the maxillary artery. (a) Before embolisation--massive angioma of face and upper lip, supplied by hypertrophied infraorbital and descending palatinevessels; (b) after embolisation-many normal vessels are preserved.
.4.
(I. t
Fig. 4 Case 3 Facial angioma-injection of maxillary and superficial temporal arteries. (a) Beforeembolisation-the angioma is largely fed by superficial temporal artery; main venous drainage is towardssuperior ophthalmic vein (arrows); (b) during embolisation-partial obliteration of lesion; (c) final series-only a small portion of the angiomna remains, fed by tiny collateral vessels from maxillary artery.
Case 3 Angioma of right parotid region
RN, a 30 year old housewife, complained of aswelling in the right cheek and tonsillar region fortwo and a half months. Examination had sug-gested that the swelling was within the rightparotid gland, and exploration and partial excision
showed that the lesion was an angiomatous mal-formation. An angiogram had shown that residualmalformation was supplied by branches of theexternal carotid artery and the patient was re-ferred to us for embolisation.Transfemoral superselective catheterisation of
the branches of the right external carotid artery
941
WI, *'.Il I
f.
I
Protected by copyright.
on August 1, 2020 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.40.10.937 on 1 October 1977. D
ownloaded from

942
was performed. This showed that the maxillaryartery had been ligated within the parotid gland,but that the angiomatous malformation was sup-plied from branches of the vessel arising proximalto the ligature, from tonsillar branches of thelinguo-facial trunk and from masseteric branchesof the facial artery. Virtually all the direct supplyto the angioma was occluded with Gelfoam emboli(Fig. 5). There was, however, some retrogradefilling of the part of the maxillary artery beyondthe ligature via facial collaterals. It was decidedto wait and see how much thrombosis would takeplace in the malformation as a result of the directembolisation and to deal with the collaterals at afurther session if indicated.There were no adverse effects after embolisa-
tion. Three weeks later the swelling in the regionof the right tonsil was only about half its formersize and there was further reduction over thefollowing months.
Case 4 Epistaxis from hereditary haemorrhagicteangiectasia
JB, a 54 year old male caretaker, was referred toKing's College Hospital in 1974 with a five yearhistory of daily epistaxes. The bleeding had beensevere enough to require transfusion of 500 pintsof blood over this period and had prevented himfrom working during the preceding three years.In 1972 he had a bilateral septal dermoplasty and
t
Brian Kendall and Ivan Moseley
he had been treated with oral oestrogens butneither of these procedures had any significanteffect.
Diagnosis presented no difficulty as he had thecharacteristic lesions of hereditary haemorrhagictelangiectasia over the face, lips, oral, pharyngeal,and nasal mucosa. There was a large perforationof the nasal septum as a result of previous surgery.
In January 1974 both maxillary arteries andtheir terminal branches in the nose were occludedwith silver clips. This operation caused a tempor-ary marked reduction in the frequency andseverity of the epistaxis, but by October 1974, thepatient was again requiring transfusions to main-tain his haemoglobin level. Bilateral carotid angio-graphy showed that the left maxillary artery waspatent, but that the right was occluded beyond theorigin of the middle meningeal artery. The leftethmoidal, facial, lingual, and external carotidarteries were ligated. There was again marked buttemporary reduction in the frequency and severityof the epistaxis, but they gradually returned totheir previous severity and he was requiring trans-fusion by April 1976. Repeat angiography showedthat the left external carotid artery was occludedat its origin. There was some collateral circulationinto the maxillary distribution from the ophthal-mic artery. The right maxillary artery was oc-cluded in the region of the pterygo-maxillaryfissure and there was collateral circulation to thenasal cavity from the right facial artery.
Fig. 5 Case 3 Parotid angioma-injection of linguofacial trunk. (a) Before embolisation-the angiomais supplied from facial artery. The proximally-ligated maxillary artery (long arrow) fills via collaterals(arrows); (b) during embolisation-the mass of the angioma is reduced; (c) final series-the angioma is almostcompletely obliterated. Flush injection confirms patency of internal carotid artery (arrow).
Protected by copyright.
on August 1, 2020 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.40.10.937 on 1 October 1977. D
ownloaded from

Therapeutic einbolisation of the external carotid arterial tree
On 4 June 1976 magnification angiography ofthe right maxillary artery showed telangiectasessupplied by its remaining branches. The tel-angiectases and finally the supplying vessels wereoccluded with Gelfoam emboli. A right facialarteriogram showed that the vessel supplied col-lateral circulation into some nasal telangiectases.These were similarly embolised, but one small col-lateral branch was left patent because forwardflow in the main trunk of the vessel had becomesufficiently slow to cause a dangerous degree ofreflux towards the internal carotid origin. Notelangiectases were supplied by the ascendingpharyngeal artery, and although the lingual arterydid supply some on the tongue these were notcausing haemorrhage and were not embolised.There was some pain and tenderness over the
anterior branch of the right superficial temporalartery which subsided over the next few days, butotherwise there were no symptoms due to the pro-cedure. There was immediate cessation of theepistaxes but, unfortunately, these recurred andthe patient died two months later. It should benoted that only a small proportion of the patient'slesions were amenable to embolisation because thedirect vascular supply to other lesions had beenligated proximally and they were being supplied bycollateral circulation through branches of the rightopnthalmic artery.
Case 5 Dural angiomatous malformation
JP, a 21 year old housewife, complained ofproptosis of the right eye for three years whichhad begun during pregnancy, but was non-pro-gressive. There was a past history of head injuryat the age of 14 years, which had been followedby a machinery murmur in the head. This hadlasted for one year but then disappeared. Exam-ination revealed marked proptosis with venouscongestion of the right eyelid and a bruit over theright eye. External ocular movements were full.Visual acuity was J1 in both eyes and there was nopapilloedema.
Skull radiographs showed enlargement of theright superior ophthalmic fissure and an EMIscan showed a dilated superior ophthalmic vein.Carotid angiography showed a fistula between themedial branch of the right middle meningealartery and a vein draining into the right cavernoussinus. There was no supply from the internalcarotid artery and none was evident from anyother vessel. Superselective angiography confirmedthat the fistula filled from this single vessel andshowed marked early venous drainage into thecavernous sinus and superior ophthalmic veins.
Gelfoam emboli were injected into the rightmiddle meningeal artery. These caused markedreduction in flow through the fistula and therewas no early venous drainage at the terminationof the procedure.
After embolisation the bruit disappeared andthe proptosis was less marked. The patient wasseen in the outpatient department one year later;she remains well, with no bruit and only minimalresidual proptosis.
Case 6 Post-traumatic left carotid cavernous sinusfistulae
LE, a 23 year old housewife, complained of pul-sating exophthalmos of the left eye which hadbeen increasing for 10 days. In 1970 she suffereda head injury when she was knocked down by acar and this had resulted in immediate leftproptosis and diplopia. The left internal carotidartery was ligated in the neck and the orbit vir-tually returned to normal. Ten days before admis-sion she had a sudden left frontal headacheassociated with an intermittent subjective bruitbehind the left eye.Examination revealed bruits over both orbits.
There was non-pulsatile left proptosis with en-gorgement of veins around the eye and over theforehead. Visual acuity and visual fields werenormal, but fundoscopy showed venous engorge-ment and pulsation with early papilloedema on theleft and venous engorgement on the right.On 20 May 1976 bilateral carotid angiography
was performed. After injection of contrastmedium there was immediate marked hypotensionassociated with flushing and urticaria. Only alimited study was, therefore, performed and thisrevealed occlusion of the left internal carotidartery in the neck, with cross circulation from theright internal carotid artery and retrograde fillinginto the left cavernous sinus. There was only faintfilling of the left middle cerebral artery and itsbranches.
After the angiogram the patient was neurologi-cally normal, but over the next 24 hours there wereepisodes of dysphasia and right sided weakness. By48 hours after the procedure the patient had re-turned to her preangiographic state.On 25 May 1976 the left terminal carotid artery
was occluded by clipping. The brain was noted tobe swollen with venous engorgement, especially af-fecting the Sylvian veins. There was a left posteriorcommunicating aneurysm which was clipped. Clip-ping of the terminal carotid artery caused a fall inthe Sylvian venous pressure. A vein connectingthe Sylvian vein to the cavernous sinus was clipped
B
943
Protected by copyright.
on August 1, 2020 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.40.10.937 on 1 October 1977. D
ownloaded from

Brian Kendall and Ivan Moseley
4~~~~~~.
_~~~~~.i> I AN.~~~."*ss
0*4p.
I
Fig. 6 Case 6 Post-traumatic caroticocavernous fistula-selective injection of themaxillary artery. There is filling of the dilated superior ophthalmic vein viacavernous sinus (open arrow). Catheter position is not suitable for embolisation, sincemiddle meningeal artery also supplies ophthalmic artery (arrows). Catheter tip wasadvanced beyond the origin of this vessel before embolisation.
I' .
%. .e.
......
. 9_r,f.:.ni
i. . :
Fig. 7 Case 6 (a) Injection of ascending pharyngeal artery-there is dense opacification ofvenous sinuses and superior and inferior ophthalmic veins (open arrows). Note clips oninternal carotid artery (arrow); (b) after embolisation-the shunt has been almost completelyobliterated.
944
Protected by copyright.
on August 1, 2020 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.40.10.937 on 1 October 1977. D
ownloaded from
Therapeutic embolisation of the external carotid arterial tree
4J
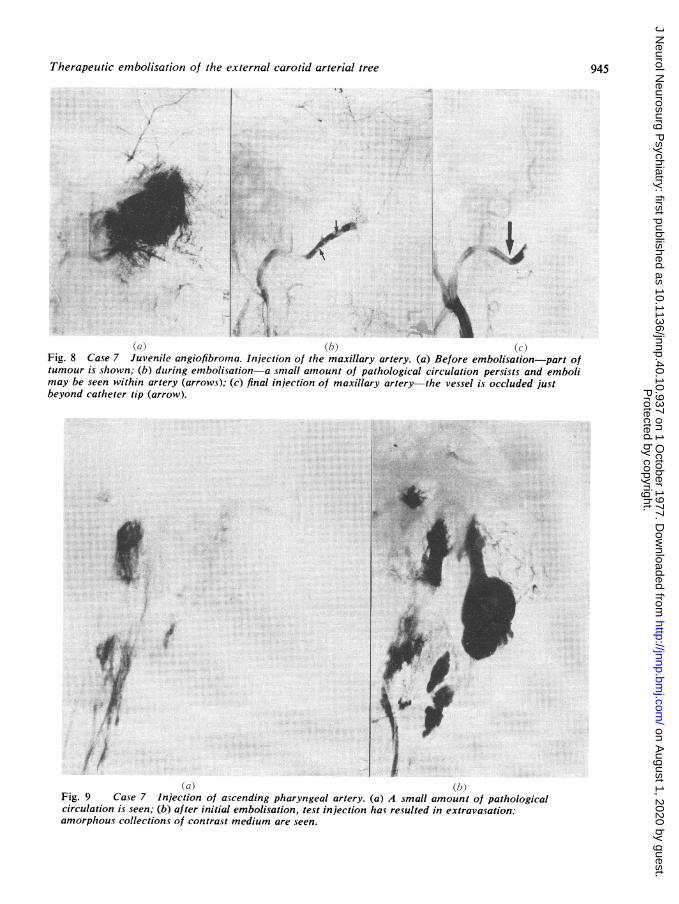
(a)} (b) (cXFig. 8 Case 7 Juvenile angiofibroma. Injection of the maxillary artery. (a) Before embolisation-part oftumour is shown; (b) during embolisation-a small amount of pathological circulation persists and embolimay be seen within artery (arrows); (c) final injection of maxillary artery-the vessel is occluded justbeyond catheter tip (arrow).
A,
a) ~~~~~~~~~~~~~~(b)Fig. 9 Case 7 Injection of ascending pharyngeal artery. (a) A small amount of pathologicalcirculation is seen; (b) after initial embolisation, test injection has resulted in extravasation:amorphous collections of contrast medium are seen.
945
.}w
Protected by copyright.
on August 1, 2020 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.40.10.937 on 1 October 1977. D
ownloaded from
Brian Kendall and Ivan Moseley
and this raised pressure in the proximal part ofthe vein, with dilatation of the veins anteriorlyin the temporal fossa, one of which ruptured.These vessels were occluded by diathermy alongthe edge of the sinus and this caused reduction inthe Sylvian venous pressure. After surgery, theorbital bruit disappeared and the proptosis wasmuch less. There was no cerebral deficit.One month later superselective injection of the
branches of the right external carotid arteryshowed that the fistula was supplied mainly fromthe right ascending pharyngeal artery, but alsobranches of the maxillary artery other than themiddle meningeal artery which supplied the oph-thalmic artery (Fig. 6). Emboli were injected intothe ascending pharyngeal artery (Fig. 7) and themaxillary artery beyond the middle meningealorigin; towards the end of the procedure it wasnecessary to use large Gelfoam fragments. Thisresulted in a marked reduction in flow through thefistula. The procedure was ended when consider-able reflux into muscular collaterals of the exter-nal carotid artery was shown and there was quiteprominent filling of the vertebrobasilar circulationfrom these.
After the embolisation, the proptosis becamegradually less prominent. The patient was con-siderably worried by painful trismus whichgradually abated over the three weeks after theprocedure. There was no other adverse effect.When seen at six monthly follow-up the patienthad no complaints and the left eye had returnedto normal.
Case 7 Angiofibroma of the nasopharynx
CS, a 12 year old schoolboy, was referred toGreat Ormond Street Hospital in September 1976.He had been seen first in September 1975, com-plaining of headaches, at which time examinationby an ear, nose, and throat surgeon was negative.He was seen again in May 1976 complaining ofsevere nose bleeds. There was necrotic mucosaon the free border of the left middle turbinatebone; this was cauterised. Complete examinationfailed to show any other abnormality.
Intermittent nose bleeds continued until Sep-tember 1976 when examination revealed a whitepolyp in the left middle meatus. Biopsy provedthis to be a juvenile angiofibroma. Radiographsshowed opacity of the left nasal space with devia-tion of the septum towards the right; the leftantrum was opaque.
Transfemoral selective internal carotid angio-graphy and supraselective angiography of themaxillary, facial and ascending pharyngeal arteries
of both sides were performed. The tumour wasvery vascular, with a pathological circulationderived mainly from the left maxillary and ascend-ing pharyngeal arteries, but with a considerablecontribution from the same vessels on the rightside. These four arteries were embolised with firstsmall and then progressively larger Gelfoam frag-ments, so as to occlude the tumour vessels them-selves and then the supplying branches (Fig. 8).Some extravasation occurred from the rightascending pharyngeal artery during a test injectionmonitoring the embolisation (Fig. 9). This was notprogressive and the procedure was otherwiseuneventful.For a few days after embolisation the patient
complained of sore throat, but there were noother symptoms. Eleven days later a transpalatalexcision of the angiofibroma was performed. Itwas attached to the roof and left lateral wall ofthe nasal cavity 10 mm anterior to the pterygoid
i
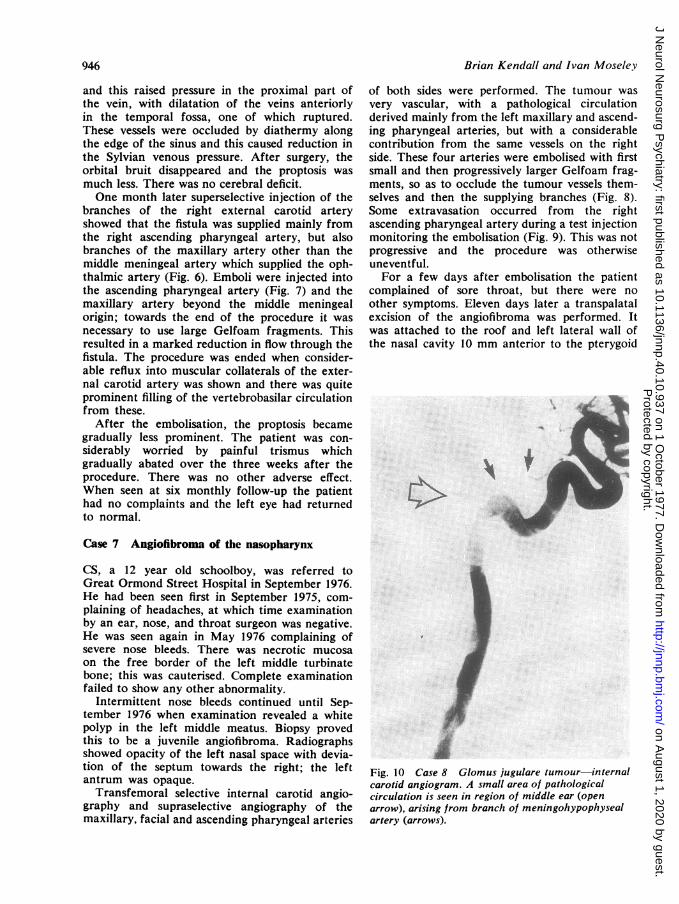
Fig. 10 Case 8 Glomus jugulare tumour-internalcarotid angiogram. A small area of pathologicalcirculation is seen in region of middle ear (openarrow), arising fromz branch of meningohypophysealartery (arrows).
94r6
Protected by copyright.
on August 1, 2020 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.40.10.937 on 1 October 1977. D
ownloaded from

Therapeu 'ic emnbolisation of the externtal carotid arterial tree
processes. It was avulsed piecemeal and the sur-geon commented on the fact that the blood losswas significantly less than usual. Recovery wasuneventful.
Case 8 Glomus jugulare tumour
EA, a 46 year old Persian businessman, com-plained of a pulsatile bruit in his right ear; thishad been present for three months, but two yearspreviously he had had one acute attack of vertigo.He had also noticed slight right sided deafness andfacial weakness, and mild dysphagia.These symptoms were confirmed on examina-
tion, which also showed a right palatal weaknessand wasting of the right side of the tongue. Theeardrum was bulging and blue. Although he gaveno hisvory of previous operation, there was a largescar overlying the right sternomastoid muscle.
Plain radiographs showed extensive erosion of
Ar
(a)
the right petrous bone. Selective injections of theright vertebral and internal carotid arteries showedvery minor contribution to the blood supply of thelesion (Fig. 10). Superselective injection of thebranches of the external carotid artery showedthe lesion to be fed by two branches of the oc-cipital artery, the ascending pharyngeal artery andthe maxillary artery. These four feeding vesselswere each selectively embolised (Figs. 11, 12).The patient was intensely nauseated for two
days after embolisation, but made a satisfactoryrecovery. His symptoms were alleviated and therewas some return of bulk to the tongue. Tenmonths after the first embolisation, he was seenagain, complaining that his swallowing haddeteriorated.
Plain radiographs indicated that the petrouscrosion had increased. Selective vertebral andinternal carotid angiograms showed some increasein the supply from these vessels. The occipital
4$
*A}J1 P
I 0,
(bi)
Fig. 11 Case 8 Selective injection of occipital artery. (a) The catheter is in main trunk of artery (arrow)froni which two branches supply a large tumour mass; (b) after embolisation the larger, posterior branch isoccluded and emboli are seen within it (arrowheads). There is still supply to the tumour from the anteriorbranch; the catheter was advanced into this for further embolisation. Note reflux into other externalcarotid branches after obliteration of a major portion of tumour.
947
Protected by copyright.
on August 1, 2020 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.40.10.937 on 1 October 1977. D
ownloaded from

Brian Kendall and Ivan Moseley
IL~~~~~~~~~~~~~~~~~~~~~~~~~~~
Fig. 12 Case 8 (a) Injection of maxillary and superficial temporal arteries after embolisation of ascendingpharyngeal-further supply to the tumour is seen; (b) after embolisation-a tiny portion of tumour remains.Flush injection shows this and confirms the patency of internal carotid and middle cerebral vessels (arrows).
artery was embolised again, and it was noted thatthe supply from the maxillary artery had not in-creased significantly. The ascending pharyngealartery, which had previously fed only a small por-tion of the lesion, was now supplying a large tu-mour mass (Fig. 13a). After the first embolisationand check angiogram of this artery (with 4 ml ofcontrast medium) it was clear that there had beenmassive extravasation of contrast medium into thesubdural space and even into the cerebral ventri-cular system (Fig. 13b). The procedure wasstopped immediately.Recovery was uneventful despite the leakage of
contrast medium, and there was some improve-ment in the patient's symptoms. The nature of theextravasation suggested that the tumour hadbroken from the confines of the petrous bone intothe subdural space, and possibly even invaded thesubarachnoid space where small veins hadruptured. This, and the obvious extension of thetumour between the two embolisations underlinethe fact that in such progressive lesions embolisa-
tion is best followed by resection when feasible,although it may not be essential (Hekster et al.,1973).
Complications
All these procedures carry the risks associatedwith general anaesthesia and arterial catheterisa-tion; since these are non-specific, they will not bedwelt on here. The specific complications arisefrom the interruption of the blood supply to nor-mal tissues, the possibility of embolisation of thecerebral vessels, and certain local complicationsof the catheter techniques.
In general, ischaemia of healthy tissues doesnot result from therapeutic embolisation becauseof the excellent collateral supply in the regionsconcerned. However, skin ulceration may occur,particularly around the pinna, and this may be adisadvantage when the procedure is largely cos-metic. Some workers have also described ulcera-tion of the tip of the tongue, a particular hazard
948
:;-
Protected by copyright.
on August 1, 2020 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.40.10.937 on 1 October 1977. D
ownloaded from

Therapeutic embolisation of the external carotid arterial tree
4..
~~) I,
Fig. 13 Case 8 Second embolisation. (a) Injection of ascending pharyngeal artery-a considerableregrowth of tumour is seen; (b) after partial embolisation-the tumour vascularity is markedly reduced.but contrast medium is seen outlining the subdural space in front of and behind lower medulla (open arrows),and lying in the dependent portion of the fourth ventricle (arrow).
with extensive bilateral embolisation of the lingualarteries (Djindjian et al., 1973a). In neither ofthese situations has the ulceration been clinicallytroublesome. Case 3 of the present paper did showsome superficial ulceration of the tonsil afterembolisation but this was not significant. In an-
other case, however, preoperative partial embo-lisation of an enormous facial and pharyngealangioma was followed 12 hours later by haemor-rhage from the larynx; this was thought to be a
result of traumatic intubation, but must be re-
garded as a complication of the procedure.Djindjian et al. (1973b) have also described facialatrophy as a laze result of embolisation of facialangiomas or lymphangiomas.
In none of our patients was there any neuro-
logical deficit after embolisation of the externalcarotid artery. Manelfe and his coworkers(Guiraud et al., 1974) described a series of 50 casesin which the internal carotid artery was injectedat the end of embolisation in the external carotidterritory. Nine cases showed some angiographic
abnormality but in only one was this symptomatic.More serious incidents have, however, been des-cribed (see Djindjian (1977) for full bibliography).We would emphasise, therefore, that it is vitalnot to proceed with embolisation unless it appearsquite safe; it is also important not to attempt toachieve complete occlusion of all feeding vesselsat the time of the procedure, as this clearly setsthe stage for reflux into the internal carotid artery.The local complications include damage to the
vessels by intimal tears during attempted super-selective catheterisation, or by rupture of smallvessels-cf cases 7 and 8 of the present series.Fortunately, neither of these phenomena appearsto be clinically significant. After embolisation,some transient pain and swelling of the areausually accompanies a successful result; slightfever is not uncommon. These symptoms are dueto thrombosis within the embolised vessels, whichusually continues for seven to 14 days after theprocedure.The lesion may become revascularised, par-
949
i
4.!..ft!
.f.w,
Protected by copyright.
on August 1, 2020 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.40.10.937 on 1 October 1977. D
ownloaded from

Brian Kendall and Ivan Moseley
ticularly if it has not been possible to deal withall the feeding vessels. If surgery is to follow em-bolisation it should, therefore, be carried outwithin seven to 10 days of the procedure. In casesin which surgery is not contemplated, it may benecessary to repeat the embolisation, possiblymore than once.
Conclusions
It would seem that embolisation represents aneffective primary mode of treatment for lesionswhich may pose problems of bleeding-spontane-ous or peroperative-and in which the feedingvessels may not be dealt with effectively andsimply by the surgeon. This is particularly relevantwhen a good cosmetic result is important. Thatembolisation should precede surgery is illustratedby cases 3 and 4 of the present report, in whichprevious surgery, while ineffective, prejudiced theresults of the radiological procedure.
Close surgical/radiological collaboration isessential to determine the relative timing and ex-tent of embolisation and surgery, and in the assess-ment of the relative benefits and possible risks ofthe procedure.
We are grateful to our colleagues at the NationalHospital for referring these cases to us and alsoto Mr R. Pracey, Mr 1. W. Broomhead, Mr J.Maynar4 and Dr R. Heirons for transferringpatients to us for the procedure. We thank theDepartment of Medical Illustration at the Instituteof Neurology for preparation of the illustrationsand Miss P. M. Hampson for secretarial assistance.
References
Brooks, B. (1930). The treatment of traumatic arterio-venous fistula. Southern Medical Journal, 23, 100-106.
Djindjian, R. (1977). Superselective Arteriography ofthe External Carotid Artery. Springer: Berlin.
Djindjian, R., Cophignon, J., Theron, J., Merland,J. J., and Houdart, R. (1973a). Embolization bysuperselectivc arteriography from the femoral routein neuroradiology. Review of 60 cases. I. Technique,indications, complications. Neuroradiology, 6, 20-26.
Djindjian, R., Cophignon, J., Rey, A., Th6ron, J.,Merland, J. J.. and Houdart, R. (1973b). Super-selective arteriographic embolization by the femoralroute in neuroradiology. Study of 50 cases. III.Embolization in craniocerebral pathology. Neuro-radiology, 6, 143-152.
Guiraud, B., Manelfe, C., Rascol. A., and Guillaume,J. (1974). Discussion of complications of embolisa-tion. Reunion interregionale de la Societe d'Oto-neuro-ophtalmologie de Toulouse: Angiographiesuperselective de la carotide externe et embolisationen oto-neuro-ophtalmologie. Toulouse, 26.10.74.
Hekster, R. E. M., Luyendijk. W., Matricali, B.(1973). Transfemoral catheter embolization: amethod of treatment of glomus jugulare tumours.Neuroradiology, 5, 208-214.
Ishimori, S., Mattori, M.. Shibatta, Y., Sizawa, H.,and Fujinaya, R. (1967). Treatment of carotidcavernous fistula by gelfoam embolization. Journalof Neurosurgery, 27, 315-319.
Luessenhop, A. J. (1969). Artificial embolization forcerebral arteriovenous malformations. Progress inNeurological Surgery. 3, 320-362.
950
Protected by copyright.
on August 1, 2020 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.40.10.937 on 1 October 1977. D
ownloaded from