Embed Size (px)
Citation preview

188
TABLE II-CLASSIFIED RESULTS
Progress was assessed according to the lessening ofattacks in duration and frequency, the lessening of theneed for antispasmodic material, and the improvementin health and mobility. The dosage was so small that noside-effects of steroid therapy arose.
Results
The details of our patients are shown in table i. Ourresults are shown in table 11. The cases treated with
hydrocortisone are analysed in table ill. The details ofthe successful cases do not materially differ from those ofthe unsuccessful; the patients tended to be a little youngerbut more chronic.The duration of the remissions was precisely similar
for the much improved and improved groups, varyingfrom two weeks to four months (average six weeks).5 patients returned to hydrocortisone inhalations-3 withimprovement, 2 without. These latter thought that thematerial obtained from the chemist was not the same aswe had provided.To assess our results statistically we grouped the much
improved and the improved cases together and comparedthem with the number of failures.
It appears that the hydrocortisone produces significantbenefit; the probability that results as good as theseshould have occurred by chance alone is only 0-028.The number of patients treated with prednisolone is toosmall to lead to firm conclusions. There is no evidence of
improvement over the placebo, but the results are
significantly inferior to the hydrocortisone (P=0029).Discussion
The dosage of hydrocortisone acetate given by inhala-tion in our patients was so small that the beneficial effectsmust have resulted from a local action on the bronchialtree and not to a systemic effect after absorption. Thisaction is presumably similar to that of steroids appliedtopically in skin diseases. When used in this way in
dermatology hydrocortisone is superior to prednisolone(Frank and Stritzler 1955). The reason for this is not
clear, but it may explain why there was no significantbenefit in our patients treated with prednisolone inhala-tions. Difference in solubility of the two steroids willnot readily explain the different results, because hydro-cortisone acetate is said to be insoluble in water, whereas
prednisolone is almost insoluble (British PharmaceuticalCodex 1954: Supplement 1957, pp. 29 and 60). The lackof solubility of hydrocortisone acetate, however, mayexplain why the powder gave a beneficial effect by inhala-tion whereas none was demonstrated in our previous trial
TABLE III-ANALYSIS OF PATIENTS TREATED WITH HYDROCORTISONE
using a solution of hydrocortisone hemisuccinate. Thesolution may well have been rapidly absorbed withoutthere being sufficiently long contact between the hydro-cortisone and the bronchial mucosa for any beneficialeffect to result.
Summary and ConclusionsThe value of hydrocortisone acetate and prednisolone
powder inhalations in the treatment of chronic asthmahas been assessed by a blind trial method.Of 24 patients receiving the hydrocortisone acetate
powder 17 were improved or much improved, a statis-
tically significant figure compared with the results obtainedin 13 patients with a blank inert powder.There was no evidence in 7 patients that prednisolone
was of any value when used in this way.In our opinion this simple method of administering
hydrocortisone acetate is well worthy of trial in the lesssevere cases of asthma.We are grateful to Dr. Avery Cotton, of the Upjohn Company of
America, for sending us the material; and to Dr. E. W. Emery,lecturer in medical physics, and Dr. S. W. Stanbury, lecturer inmedicine, for their help.
REFERENCES
Brockbank, W., Brebner, H., Pengelly, C. D. R. (1956) Lancet, ii, 807.Frank, L., Stritzler, C. (1955) Arch. Derm., Chicago, 72, 547.
TIME OF RECURRENCE OR CURE OF
TUMOURS IN CHILDHOOD
W. EUGENE KNOXM.D. Harvard
ASSISTANT PROFESSOR OF BIOLOGICAL CHEMISTRY, HARVARD MEDICAL
SCHOOL, AT THE NEW ENGLAND DEACONESS HOSPITAL, BOSTON
ELIZABETH M. KINGSLEY PILLERS *M.D. Cantab., D.C.H., D.M.R.T.
CLINICAL RESEARCH ASSOCIATE IN MEDICINE (TUMOUR THERAPY), THECHILDREN’S MEDICAL CENTER, BOSTON
From the Cancer Research Institute, New England Deaconess Hospital,the Department of Biological Chemistry, Harvard Medical School,and the Children’s Cancer Research Foundation, the Children’s Medical
Center, Boston, Massachusetts
* Present address : Department of Radiotherapeutics, Universityof Cambridge, England.
Collins et al. (1956) have given theoretical reasons whythe period is limited within which a treated neoplasmmay recur (the
" period of risk "). They showed thatthis held true in the results with 206 children fromseveral series treated for Wilms’ tumour (embryoma).There were no deaths or recurrences after the definedperiod of risk had ended. Patients surviving after theperiod of risk could be presumed to be cured accordingto a definite biological criterion. The existence of sucha limit to the time within which treated tumours mightrecur would be clinically useful, and important in thestudy of the natural history of neoplasms. The presentstudy was undertaken to see whether the experience withthree types of childhood tumours (Wilms’ tumour,neuroblastoma, and rhabdomyosarcoma) in a total of244 children seen in a single institution confirmed thefindings of Collins et al.
Method
Determination of the period when recurrence is possibleis based on knowledge of the growth-rate of a tumourbefore treatment and extrapolation of this rate aftertreatment for a period long enough for even a single cellleft behind to regrow to a tumour of diagnosable size.This time after treatment is the " period of risk ". The

189
choice of children as subjects for this study follows theingenious use, by Collins et al., of the results with Wilms’tumour to test their hypothesis. The growth-rate of
tumours before treatment is not generally known for anygroup of patients, but in children this rate can be assumedwithin relatively narrow limits. The tumour can have
grown only since conception, or later, to reach its par-ticular size at the time of treatment. The continued
growth at the same rate of even a single cell for a periodequal to that designated by the age of the child at
treatment (plus nine months’ gestation) would result ina tumour mass at least equal to that originally presentat treatment. Therefore, if there is to be a recurrence itshould appear before the end of the period of risk, at
which time the child will be twice the age (plus ninemonths) that he was at the time of treatment. For
example, a child treated at one year of age will reach theend of the period of risk one year and nine months later,or at the age of two years and nine months; a child fiveyears old, at ten years and nine months of age. Tumoursthat develop later than conception, or that increase theirgrowth-rate, would recur well before the end of the periodof risk, as defined here. Slowing of growth-rate, spon-taneously or as a result of treatment, could result inrecurrence after the end of the period of risk and wouldnegate the prediction.Two time-periods were ascertained for each patient: (1) the
time before treatment (age plus nine months’ gestation), and(2) the time after treatment until the first recurrence of thetumour or the last negative follow-up. Periods were deter-mined to the nearest month. In some patients in whom deathfollowed shortly after the recognised recurrence and early inthe period of risk, the time of death was accepted in lieu of fix-ing exactly the time of recurrence. In patients surviving lateinto the period of risk, the time of recurrence was fixed moreexactly by the date of the first objective signs found by radio-graphic, or, less commonly by clinical, examination. A fewpatients with documented recurrences late in the period ofrisk survived well beyond the end of the period of risk, some-times with supplementary or palliative treatment. The delayeddeaths of these patients did not vitiate the prediction of thetime of their recurrences, since they had already shown evidenceof recurrence of malignancy within the period of risk.
Patients
Records were found for a total of 244 patients treatedat the tumour therapy clinic of the Children’s MedicalCenter, Boston, during the past two decades, for thethree types of tumours selected. These particulartumours were selected simply because they are common.The diagnoses in all patients in this study were confirmedby histological examination. In each group the ages of
patients ranged from newborn to about 16 years. Noselection was made as to the mode of therapy.
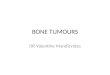
Wilms’ tumour.-This was diagnosed in 92 patients. Thetreatment was generally that of Gross and Neuhauser (1950).5 patients were lost to follow-up immediately after hospitaldischarge, while still apparently well, and these were not
incorporated in the series. Of the 87 remaining patients27 were alive and without recurrence at the last follow-up,and 60 had died or had had recurrences. There was objectiveevidence from biopsy, necropsy, or X-ray examination, in58 of the 60, for the presence of recurrent Wilms’ tumour.2 other patients died at home of recurrences diagnosed solelyon clinical grounds. 15 of the patients without recurrenceswere beyond risk.Neuroblastoma.-126 patients with this diagnosis attended
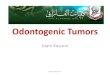
the tumour therapy clinic. Nearly all of them receivedchemotherapy, usually after surgery and radiotherapy, as
TABLE I-SUMMARY OF RESULTS IN ALL PATIENTS STUDIED
indicated. At the time of the last follow-up, 18 patients werealive, with no evidence of recurrence, and 108 had alreadyhad recurrences. 14 patients were beyond risk.Rhabdomyosarcoma.-31 patients with this diagnosis were
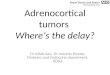
studied. The therapy was the same as that described for theprevious group. At the time of the last follow-up, 7 werestill alive (4 of them beyond risk), and 24 were dead or hadrecurrences.
Results
The overall results are shown in table i. Separategraphs have been made for the three different tumours(figs. 1-3). The time before treatment (age plus ninemonths) was graphed against the time after treatmentto recurrence or last follow-up for each of the patients.A line drawn at 45° through the origin separates theperiod of risk from the safe period, and all recurrencescan be seen to fall wholly within the period of risk. Thepatients followed long enough to be in the safe periodwithout recurrence are presumambly cured. Those withthe period of risk, but negative at the last follow-up, arecritical cases which should be followed closely until theyare beyond risk.
Discussion
The results in three of the commonest tumours ofchildhood confirmed the observations by Collins et al.
in a heterogeneous collection of 206 cases of Wilms’tumour. There were no recurrences after the safe periodwas reached. A single recurrence in the safe period would
Fig. 1-87 cases of Wilms’ tumour.

190
disprove the thesis of an invariably constant or increasingrate of growth in tumours despite therapy. The resultsobtained are consistent with this thesis though they donot supply positive proof of it. The qualitative dichotomyof the post-treatment time into two periods-a period ofrisk and a safe period-is clear and arresting.There is a highly significant difference in the results
during these two periods by the x2 test, but it is difficultto prove that this distribution did not arise by chance,because all tumours tend to recur early, long before theend of the period of risk. It is possible only to show,as did Collins et al. (1956), that the number of individualscured by their criterion (i.e., reaching the safe period)was equal to that fraction of the whole group who weredying at a normal rate instead of an accelerated rate
(i.e., equal to the " proportion cured," calculated fromthe statistics of the whole group by the method of Boag[1949]). The essential value of these results, however, isthe application of a criterion of cure to an individual.The combined experience with a total of 293 Wilms’tumours, for example, strongly suggests that the criterionof cure discussed here is reliable.The existence of a biological criterion of cure applicable to
individuals treated for neoplasms will have important uses,even if applied empirically without reference to its theoreticalbasis. Even more important issues arise from the theoreticalconsiderations. The criterion was developed from the reason-able assumption that neoplastic cells, like other populations,will tend to grow logarithmically at a constant rate under
optimal conditions, so that their number (and therefore theirmass) doubles in each interval of time. An interval of time aftertreatment, equal to that period when the tumour could haveexisted before treatment, therefore limits the period withinwhich a recognisable tumour would recur. These results pro-vide no direct evidence for the way tumours grow, and onlycircumstantial evidence for the theory itself. The results are
Fig. 2.-126 cases of neuroblastoma.
Fig. 3-31 cases of rhabdomyosarcoma.
consistent with this theory, since in no instance was a tumourfound to grow more slowly after treatment. Such exceptionswould be of particular interest in guiding tumour therapy.
Positive evidence for the theory may be obtained by theresults of longer follow-ups of larger numbers of patients, orby direct determination of tumour growth-rates in individualsof different ages. In either of these ways an important implica-tion of the theory could be tested-viz., that the tumour whichgrows to a recognisable mass in a young child is growing morerapidly than one attaining a similar mass in an older child. Ina series sufficiently large to include late recurrences at each age,it should be possible to show that the disease in younger chil-dren usually recurred earlier than in older children. Also, bydirect radiological measurement, metastases in young childrenshould be found to grow more rapidly than those in older chil-dren. In adults the possible long time-span of tumour growthwould prevent significant use of this theory, unless based onactual measurements of growth-rates of the individual tumours.
If the results of this study are accepted, one of theconsequences should be the adoption of a sliding time-scale for the follow-up of patients after treatment.
Definitive results can be known quickly in young children,but for older children the usual follow-up period shouldbe extended, commensurate with their age at treatment.
SummaryThe hypothesis that a treated neoplasm will recur only
within a defined period of risk after treatment was
tested and confirmed by the results in 244 children withtumours (Wilms’ tumour, neuroblastoma, and rhab-domyosarcoma).
All tumour recurrences developed before the end ofthe period of risk, defined as twice the age at treatmentplus nine months.
In 192 cases there was a recurrence. Of the 52 casesin which there was no evidence of recurrence at the last
follow-up, 19 were still within the period of risk. The
remaining 33 were beyond risk and therefore could beassumed to be cured.
Support is acknowledged from U.S. Atomic Energy Commis-sion grant AT (30-1)-901, and U.S. Public Health Service grant

191
A567 to the New England Deaconess Hospital and U.S. PublicHealth Service grant CY-3335 to the Children’s Cancer ResearchFoundation.
REFERENCES
Boag, J. W. (1949) J. R. statist. Soc. B, 11, 15.Collins, V. P., Loeffler, R. K., Tivey, H. (1956) Amer. J. Roentgenol.
Radium Therapy and Nuclear Medicine, 76, 988.Gross, R. E., Neuhauser, E. B. D. (1950) Pediatrics, 6, 843.
TREATMENT OF UNDULANT FEVER
J. TORRES GOSTDIRECTOR, HOSPITAL DEL REY PARA ENFERMEDADES INFECCIOSAS,
MADRID, SPAIN
Up to a few months ago we did not have a specific andefficacious antibiotic with which to treat undulant fever.Neither streptomycin nor aureomycin, let alone vaccines,gold compounds, &c., was surely therapeutic in thisinfectious disease; and invariably the end-results, after
treating the patients with these antibiotics, were completefailures, because almost constantly the disease recurred.Even without complications-e.g., spondylitis, which
cripples for life-undulant fever used to last a year or two.Some months ago a new antibiotic, Cathomycin " was
supplied to us for treating infections resistant to penicillin.For various reasons and of my own initiative I used it totreat patients with undulant fever. After treating the firstfew cases, I realised that cathomycin is a specific effectiveantibiotic in undulant fever. Up to now we have treated26 patients, who have been discharged from hospitalcompletely cured, and not one has had a recurrence.
Of the 26 patients treated 20 had produced a positiveblood-culture on admission and the remaining 6 had apositive agglutination test. Only the 20 patients with apositive blood-culture are discussed here. Their detailsare shown in the accompanying table. We treated the
patients only when the undulant fever was at its height.The constant effect of cathomycin was remarkable (see
figure). During the first five days’ treatment no changeis apparent; the pyrexia continues as before, and thesymptoms remain just the same; but almost always on thefifth day the pyrexia resolves by crisis and all the symp-toms (headache, insomnia, articular pain, anorexia,sweating, &c.) disappear. Splenomegaly also disappears,and by the end of the treatment the spleen has returnedto its normal size and shape, no matter how large it was.None of the patients relapsed.Dosage.-A capsule containing 0-25 gs. was given
four-hourly until the day after the crisis (usually the sixthday) and then six-hourly for nine days to a total of 18 g.Of course this dosage applies only to adults.
Typical chart of temperature and pulse-rate in undulant fever beforeand during treatment with cathomycin.
ANALYSIS OF CASBS OF UNDULANT FEVER AND TREATMENT
Laboratory Findings.-On the third day of treatmentliver-function tests (Kunkel’s, Maclagan’s, Hanger’s, andWuhrmann’s), which were frequently made, were alwaysnegative. The leucopenia, which sometimes was verysevere, rapidly disappeared. Anxmia, which also iscommon in undulant fever, gradually returned to normal.The platelet count was usually normal and did not varyin any way during the treatment. No organic alterationswere found.
Psychology.-The patient’s state of mind was much
improved as soon as his temperature had returned to normal.Many of the chronic patients who had become pessimisticbecame cheerful and self-confident again after losing theirfever and pain.
Side-effects.-A quarter of the patients manifestedintolerance of cathomycin.
Case 10 (see table) during the first three days of treatmenthad hyperchlorhydia, which was relieved by alkalis withoutstopping the treatment.
Case 5 had a generalised urticarial rash, with pyrexia up to104°F, but with the patient’s cooperation we did not withholdcathomycin but gave him the full fifteen days’ treatment. Onthe day that he stopped having cathomycin his temperaturereturned to normal; two days later the exanthema disappeared,and he was discharged completely cured.
Case 6 was treated for ten days. On the eighth day an urti-carial eruption appeared, causing him so much discomfortthat we had to withhold cathomycin for two days, during whichtime the rash disappeared. We gave him cathomycin again,but after the third capsule the exanthema reappeared, accom-panied by pyrexia up to 103°F. Since the patient asked us notto stop the treatment, we carried on for the remaining fourdays. Two days later all his ailments disappeared, and on thethird day he was discharged home completely cured.
In case 8 urticaria appeared on the eighth day of treatment,but the treatment was continued to the tenth day, when wehad to withhold cathomycin because the patient could nolonger bear the itching caused by the rash. Four days later,when the urticarial rash had subsided, we continued the
treatment, but at the third capsule the exanthema reappeared,this time with such severe symptoms that we had to abandontreatment with cathomycin. Although the patient had hadonly 10 days’ treatment he was definitely cured, and threedays later he was discharged.
So far the urticarial eruption has been the only incon-venience caused by cathomycin.
Conclusion
In all our knowledge and experience of undulant feverwe have never seen or achieved such good results. Thisinfectious disease is completely cured in about five days