Embed Size (px)
Citation preview

Toward a Standardized Breast Ultrasound Lexicon BI-RADS Ultrasound
Ellen B Mendelson Wendie A Berg and Christopher R B Merritt
SONOGRAPHY IS an imp0l1ant complement to mammography Analysis of sonographic
features may aid in appropriate selection of lesions for follow-up or biopsy Recognizing that consisshytent terminology and clear communication of findshyings and results directly affect patient manageshyment a validated lexicon of descriptors for breast sonography is in development This includes terms to describe shape orientation margin regularity and thickness matrix echogenicity matrix homoshygeneity acoustic attenuation and effect on surshyrounding ti ssue
With support from the Offlce on Womens Health Department of Health and Human Sershyvices the American College of Radiology (ACR) Commission on Ultrasound has developed the initial draft of a breast ultrasound lexicon to be used for standardized reporting of breast ultrashysound findings In tended to complement the ACR Breast Imaging Reporting and Data System (BIshyRADSTM) lexicon the breast ultrasound lexicon (BI-RADS Ultrasound) will undergo final review in mid 2001 and is expected to be released in December 2001 An overview of the proposed lexicon and examples of features described in the lexicon are presented
INTRODUCTION
Although mammography remains the most senshysitive method for detecting preclinical breast carshycinoma its limited specificity resu lts in need to biopsy many abnormalities to determine whether they are benign or malignant I 2 Indi cations for breast sonography include the following the in itial eva luation of palpable abnormalities in women under 30 initial identification and characterization of palpable and nonpalpable abnormalities guidshyance of interventional procedures and evaluation of problems associated with breast implants34
Several recent studies suggest that sonography in combination with mammography can reduce the number of false-positive recommendations for bishyopsyS-B Mammography remains the standard for breast screening as most ductal carc inoma in situ is missed sonographically9-1 I
The growing use of ultrasonography has created the need for a standardized method for lesion characterization descri ption and reporting1 2 The
mammography lexicon developed by the ACR the Breast Imaging Reporting and Data System (BI-RADSTM)13 provides sta ndardized assessment and associated management recommendations for masses and calcifications Based on success of BI-RADS with mammography the development of a lexicon for breast ultrasound (BIRADS Cltrashysound) and breast magnetic resonance imaging 14 has been a high priority for the ACR The lexicons are designed to use shared terminology whenever possible When com pleted the lexicons will aid refelTing physician s radiologists and patients in describing abnormalities and understanding their management implications Furthermore these lexshyicons will provide a basis for validation of outshycomes across multiple centers
A breast ultrasound lexicon_ the Breast Imaging Reporting and Data System lJtrasound is curshyrently being developed by the ACR The initial draft was prepared by the Breast Cltrasound Lexshyicon Subcommittee of an Expert Working Group to Plan and Develop Protocol s for Optimization and Clinical Testing of Breast Ultrasound supported by a contract from the Offlce of Womens Health National Institutes of Health and conducted by the Commission on Ultrasound of the ACR Techshyniques adapted from those used in the development of BI-RADS are being used in the formulation of the new ultrasound lexicon The ACR lexicon is ex pected to be completed and released j n late 200 1 follo wing its validation
Froll the Deporll11enl of Radiology Western Pennsylvania
Hospital PitTsiJurgh PA Depamnenr of Diagnostic Radiology
and Greenebawll Cancer Center UniversiT) of Maryland Baltimore MD alld The DeparTment of Radiology Thomas
j efferson UniversilY j efferson Medical College Philadelphia
PA This work Ivas supPOrTed in part by COnTract 282-97-0076
Federal Technology Tran sfer Program to Advance Novel
BreasT Imaging Technologies 15 Public HealTh Service Office
on Womens Health CS D epaJ1meJl of HealTh and Human
Senices Address reprinT requests To Ellen B Mendelson MD Deshy
palllnelll of Radiology The WeSTern Penl1Sylvania Hospital 4800 Friendship AFe PillsiJlrgh PA 15224
Copyright copy 2001 by WB Salnders Company
0037- 98x013603-0007$3500O
doi JOI053sroe200125125
Seminars in Roentgenologv Vol XXXVI No 3 (July) 2001 pp 217-225 217
218 MENDELSON BERG AND MERRITI
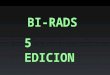
Fig 1 Shape Masses are described as round (A) oval (B) or irregular (C) A round mass is spherical ball-shaped or globular in shape An oval mass is elliptical or egg-shaped These descriptors are similar to those used in the ACR BI-RADS lexicon for mammography (A) A spherical simple cyst is shown (B) An oval fibroadenoma is shown The invasive cancer shown in C is irregular
FEATURE ANALYSIS
Lesion features include primary fea tures such as shape (Fig 1) orientation (Fig 2) margins (Figs 3 through 5) matri x echogenicity and homogeneity (Figs 6 and 7) and attenuation (Fig 8) which should be described and applied in a consistent fashion In addition secondary associated findings such as architectural distortion (Fig 9) retraction or angulation of Coopers ligaments (Fig 9B) di lated ducts calcifications (Fig 10) and changes in the ski n subcutaneous fat and pectoral muscle can be recorded as well These fea tures of masses have been enumerated previously5715 16 The utility of
each category of features requires validati on along with that of individual descriptors For example matrix homogeneity probably has less specificity and significance than description of mass marg ins The most appropriate descriptor for each category of characteristics shou ld be applied whe n desc ribshying a lesion (Table 1) Wherever poss ible fea ture descriptors similar to those used by BI-RADS fo r mammography have been imported As with mamshymography use of the lexicon is predicated on
Fig 2 Orientation Mass orientation refers to the relationshyship of the long axis of the mass to the skin This may be parallel as is common with fibroadenomas (A) or not parallel a common orientation for many cancers (B) Because round lesions do not have one axis that is longer than another they should be classified as not parallel
Fig 3 Margins The margin is the boundary between the lesion and its surroundings Several characteristics of the lesion margin are important The margin should be described as circumscribed (distinct and smooth) (A) or irregular (indisshytinct microlobulated angUlar or spiculated) (B) In A the circumscribed margin of a fibroadenoma is shown In B an invasive cancer demonstrates an ill -defined or indistinct inshyterface with the surrounding tissues As in mammography ill-defined margins are associated with higher risk of maligshynancy than circumscribed margins
exce llent sonographic technique using a linear transd ucer whose center frequency is at least 7 MHz Documentation should be performed in acshycord with the American Colleoe of Radioloayeo c
Standards Orthogonal v iews of the lesion should be obtained and the orientation of the transducer and location of the abnormality should be deshyscribed using quadran t clock-face location andlor labeled diagram of the breast ideall y including distance from the nipple
Several previous studies5 15 reach the conclushysion that multiple features must be analyzed to achie ve as great a specificity as possible in sonoshygraphic charac terizati on As an example the diagshynosis of a mass as a si mple cyst requires that the shape be rou nd oval or gently lobul ated margin circumscribed echogenicity (echo pattern) aneshychoic and that there be acoustic enhancement Based on these combined features the impress ion is that of a simple cyst (Figs 1 5 and 6) The final assessme nt for the combination of mammographic
Fig 4 Margin thickness Circumscribed margins may be thin thick or of mixed thickness The fibroadenoma (A) has a thin and distinct boundary delineating it from surrounding breast tissue The invasive cancer in 4B has generally thick margins whereas the cancer in C shows a margin composed of thick thin and indistinct segments Barely perceptible margins favor benign etiology
TOWARD A STANDARDIZED BREAST ULTRASOUND LEXICON 21 9
Fig 5 Margins The smooth barely perceptible margin of a simple cyst (A) is contrasted with the irregular margins of a small invasive cancer (B) Margin irregularities may include angular edges m icrolobulation and spiculation
and sonographic fi ndings using BI-RADS is cateshygory 2 benign with routine screening recomshymended The accuracy of sonographi c identificashyti on of cysts approaches 100 provided stric t ad herence to the classical sonographic charac teri sshytics are observed 17
t
Practical use of any lexicon req uires an undershystanding of the de fin iti ons of each term An examshypJe is complicated versus complex The presence of homogeneous low-level internal echoes throug holl t a cystic lesion that has all the other features of a sim ple cyst as above results in its designation as complicated 18 Many of these masses appear solid a lbeit benign and may be reported as comshyplicated cyst or probabl y ben ign solid lesion Often such lesions are incidentall y found during ul trasound examination peIiormed for other reashysons Recent studies cumulative ly evaluating 567 incidental compli cated cysts identifi ed only one 3-mm in situ ma lignancy (positive predictive value [PPY] 02)1 9-21 Based on these data short-term follow-up appears appropriate (BI-RADS category 3 probabJy ben ign) although further validation is
Fig 6 Echogenicityechotextureecho pattern The matrix of a mass may be homogeneous or heterogeneous Homogeshyneous masses may be anechoic hypoechoic or hyperechoic Cysts are typically anechoic (A) The echogenicity of hyposhyechoic and hyperechoic masses should be compared with the echogenicity of fibroglandular tissue In this example a hamartoma produces a homog eneous mass (arrows) that is hyperechoic compared with fat (B) Invasive cancer (C) is often hypoechoic both to fat and to glandular tissue (same lesion as in Fig 2B)
Fig 7 Echogenicityechotextureecho pattern Heterogeshyneous masses may be solid or complex conta ining a mixture of solid and cystic components The invasive cancer in A is predominantly hypoechoic but contains some areas of inshycreased echogenicity resulting in a heterogeneous echotexshyture Complex masses may be predominantly solid (B) or cystic (C both intracystic papillary carcinomas) and should be regarded as suspicious for cancer in the absence of clinical finding s suggesting an abscess
encouraged Interval enl argement (mammographishycall y or sonograph ical ly) or the presence of any suspicious features should prompt aspi ration and possible core biopsy if it proves solid 22
Suspicious features include an intracystic mass mural nodule thick septations or a thi ck or irregshyul ar wall When such fea tures are present the mass should be desc ribed as a complex cystic mass (Figs 7B and C) These lesions generall y requ ire aspiration or biopsy (BI-RADS category 4 susp ishycious)
When a so lid lesion is presen t careful analysis of contour margins matri x and attenuation may a llow classification of some nodules as BI-RADS category 3 probab ly benign and provide the opshyti on of short interva l follow-up at 6 months 12 months and 24 mon ths rather than biopsy5-7 As in ma mmography for a lesion to be assessed as probably benign it should have lt2 risk of malignancy 2324 As mentioned preliminary data suggest cysts with internal echoes can be so classhysified as can clusters of tin y cystic foci wi th thin intervening septatio ns compatible with apocrine metaplas ia 25
Fig 8 ShadOWingenhancement Enhancement may be seen with cysts (A) fibroadenomas (B) and high-grade inshyvasive cancers (C) Central shadowing is associated with the small invasive cancer is shown in C Refractive edge shadowing (present in A and B) is excluded from considershyation A single echogenic calcification is present in the fibroshyadenoma (8)
220
Fig 9 Effect on surrounding tissue Masses may affect surrounding breast tissues resulting in architectural distorshytion (A) Extensive distortion of breast architecture by a small scirrhous cancer is shown (8) A more subtle change is seen where a Cooper ligament is interrupted by a cancer (open arrows)
Stavros et a]5 proposed three categories of solid lesions that could be class ified as BI-RADS cateshygory 3 probably benign in the absence of any suspicious features (I) masses with intense and uniform hyperechogenicity re lative to fat (2) masses with an ellipsoid shape and thin echogenic capsule and (3) masses with two or three gentle lobulations and a thin echogenic capsu le Individshyually each of these characteristics had a negative predictive va lue for malignancy of 988 to 100905 Although accepted by some it is important to note that these results have not been validated across multiple centers Indeed one recent study26
suggests that not all readers achieve sufficiently high specificity to fo llow so lid lesions [n the draft BI-RADSUltrasound lexicon the concept of a thin echogenic capsule or pseudocapsule- has been replaced by that of a thin smooth margin analoshygous to a circumscribed mass mammographishycally Although palpable solid lesions are genershyally recommended for biopsy 2l24 it is not yet clear whether any size criterion or palpability of the lesion influences the absolute risk of malignancy
For solid masses irregularity of shape and margins dominate other features suggesting maligshynancy with a PPY of ma lignancy of 86 to 9357 such lesions are appropriately classified as BI-RADS category 4 or 5 with biopsy recomshymended Other features have lower specificity Orientation of the long axis of the mass nonparalshylel to the skin synonymously termed taller than wide5 has been associated with a 62 to 81 Ok likelihood of malignancy57 and is more common ly seen in cancers lt 1 cm in size Ylost fibroadenoshymas as well as many cancers are oriented with their long axes parallel to the skin (wider than tall) J I
Echotextureecho pattern appears to be less helpful in differentiating benign fro m malignan t sol id
MENDELSON BERG AND MERRITI
masses I as most masses will be hypoechoic to pare nchyma Acoustic attenuation (shadowing) is suspicious for malignancy but as many as 2 1 of benign les ions will show shadowing7 Similarly acoustic enhancement while common in benign lesions may be present in up to 42 of cancerss
Several typically benign lesions are included as special cases (Fig 11) This includes lymph nodes with a thin circumscribed capsule and centra l echogenic hi lum Foreign bodies are spec ial cases and include siliconomas and free extracapsu lar silicone (Fig 11)27 Description of vascu larity of the lesion is not a required standard (Fig 12) as no reliable distinction has yet been made between
30benign and malignant lesions on this basis 2 8shy
Vasc ularity is described as the same increased_ or decreased relative to surrounding parenchyma
Table I is a worki ng draft of a breast ultrasound lexicon including feature categories and descripshytors Although different in format this draft was based largely on the version developed by the Lexicon Committee of the Expert Working Group It is important to note that these recommendations awa it va lidation and are subject to modification before release of the final draft of the ACR BIRADSlltrasound Descriptors are illustrated in Figures 1 through 12 The illustrations show only a
Fig 10 Associated finding s Dilated ducts skin changes and calcifications associated with breast masses may be seen with ultrasonography and should be described when present (A) Macrocalcifications (~0 5 mm) associated with a fibroad shyenoma are shown (arrowheads) (8) Microcalcifications laquo05 mm) in an invasive ductal carcinoma are shown (arrows) (C) Microcalcifications not in a mass and particularly within a tubular dilated duct (curved arrow) are suspicious and may be seen in ductal carcinoma in situ as in this example
bull TC
0 f-
bull
bull
rJ
Ca
se
Re
vie
we
r o
_
gtC
LA
SS
IFIC
AT
ION
CA
TE
GO
RIE
S amp
TE
RM
S
DE
SC
RIP
TIO
N
Ta
ble
1
Dra
ft A
CR
BI-
RA
DS
Ult
raso
un
d L
exi
con
Cla
ssif
ica
tio
n F
orm
4-4
-01
~
Ma
sse
s
ArI
2sect
secto
ccup
ies
spac
e an
d sh
ould
be
seen
in
two
diffe
rent
pr
ojec
tions
Sha
pe
(sel
ect
one)
0O
val
Rou
nd
Irre
gula
r
ellip
tical
or
egg-
shap
ed (
ma
y in
clud
e tw
o o
r th
ree
undu
latio
lls
ie
lob
ular
)
sphe
rical
ba
ll-sh
aped
ci
rcul
ar
or g
lob
ula
r ne
ither
roun
d n
or o
val
Ori
enta
tion
B P
aral
lel
long
axi
s o
f les
ion
orie
nted
alo
ng s
kin
line
(w
ider
than
tal
l)
(sel
ect
one)
N
ot P
aral
lel
no lo
ng a
xis
or
axis
no
t orie
nted
alo
ng s
kin
line
(ta
ller t
han
wid
e)
Mar
gin
C
ircu
msc
ribe
d (s
elec
t al
l tha
t ap
ply)
Y
ES
(d
yes
che
ck o
ne o
ptio
n be
lOW
)0 8
No
perc
eptib
le r
im o
r th
in r
im
Thi
ck r
im
NO
(if
no
go
to i
rreg
ular
)0
IRR
EG
ULA
R (
sele
ct a
ll th
at
appl
y)
0 In
dist
inct
A
ng
ula
r M
icro
lobu
late
d S
picu
late
d ~
Ech
o P
atte
m
A
nech
oic
Hyp
erec
hoic
C
ompl
ex
Hyp
oech
oic
~ (s
elec
t on
e)
Po
ste
ri or
Aco
ustic
N
o po
ster
ior
acou
stic
fea
ture
s F
eatu
res
Enh
ance
men
t S
hado
win
g C
om
bin
ed p
atte
rn
~ S
urro
undi
ng T
issu
e 0
No
effe
ct
BIden
tifia
ble
effe
ct (
sele
ct a
ll th
at a
pp
ly)
Duc
ts
Coo
pers
liga
men
t ch
an
ge
s
0E
dem
a A
rchi
tect
ural
dis
tort
ion
Ski
n T
hick
enin
g
B S
kin
retr
actio
nflr
regu
lari
ty
Pec
tora
l m
uscl
e se
en
bu
t pl
ane
with
an
teri
or
tissu
e is
un
cle
ar
Sm
ooth
dis
tinct
mar
gin
with
thi
n t
hick
or
no p
erce
ptib
le li
near
rim
circ
umsc
ribe
d m
argi
n w
ithin
lin
ear
rim
circ
umsc
ribe
d m
argi
n w
me
asu
rab
le th
ick
rim gt
1 m
m b
etw
een
lesi
on a
nd s
urro
undi
ng t
issu
e
mar
gins
dem
onst
ratin
g a
com
bina
tion
of f
eatu
res
incl
udin
g at
leas
t 1
of t
hose
list
ed b
elow
poor
ly d
efin
ed m
argi
n pa
rt o
r al
l of t
he m
argi
n fo
rmed
by
shar
p lin
ear
inte
rsec
tions
that
form
acu
te a
ngle
s m
argi
n ch
arac
teri
zed
by b
y gt
3 sm
all
sho
rt c
ycle
und
ulat
ions
m
argi
n ch
arac
teri
zed
by
shar
p pr
ojec
ting
lines
with
out
inte
mal
ech
oe
s de
fined
rel
ativ
e to
fat
eq
ua
l to
fibro
glan
dula
r tis
sue
com
bine
d cy
stic
(an
echo
ic)
and
ech
og
en
ic c
om
po
ne
nts
de
fined
rel
ativ
e to
fib
rogl
andu
lar
tissu
e i
soec
hoic
or
hyp
oe
cho
ic to
fat
con
tain
s lo
w-l
evel
ecl
hoes
th
roug
hout
(eg
co
mpl
icat
ed c
yst o
r fib
road
enom
a)
no p
oste
rior
sha
dow
ing
or e
nh
an
cem
en
t in
crea
sed
post
erio
r ec
hoes
de
crea
sed
post
erio
r ec
hoes
ex
clud
ing
edge
sh
ad
ow
s bo
th s
hado
win
g an
d e
nh
an
cem
en
t
surr
ound
ing
tissu
e un
affe
cted
by
lesi
on
abno
rmal
cal
iber
an
do
r arb
oriz
atio
n st
raig
hten
ing
or th
icke
ning
of C
oope
rs li
gam
ents
(cu
rvili
near
co
nn
ect
ive
tissu
e b
an
ds
prov
idin
g su
ppor
t fo
r th
e br
east
s)
incr
ease
d ec
hoge
nici
ty o
f sur
roun
ding
tis
sue
ret
icul
atio
n i
nclu
des
an
gu
lar
hyp
oe
cho
ic li
nes
disr
uptio
n o
f nor
mal
ana
tom
ic p
lane
s fo
cald
iffus
e sk
in t
hick
enin
g-no
rmal
ski
n is
gt2
mm
in t
hick
ness
exc
ept i
n th
e pe
riar
eola
r ar
ea
and
low
er b
reas
ts
skin
sur
face
is c
onca
ve o
r iII
-def
ined
ap
pear
s pu
lled
in
diso
rder
ed e
cho
pa
tte
m in
volv
ing
pect
oral
mu
scle
sug
gest
ive
of i
nvas
ion
(exc
lude
tech
nica
l ca
uses
suc
h a
s im
prop
erly
pla
ced
foca
l zo
ne
) _
-shy
~ z ~ rJ o N
m
o (lJ
rJ ~ ~
c ~
rJ ampi o c z o r m
x o o z
I
I
C
LA
SS
IFIC
AT
ION
CA
TE
GO
RIE
S amp
TE
RM
S
DE
SC
RIP
TIO
N
Ca
lcif
ica
tio
ns
0 N
one
seen
C
alc
ifica
tion
s a
re p
oo
rly
cha
ract
eri
zed
with
ul
traso
und
but c
an b
e re
cogn
ized
par
ticul
arly
in a
If
pres
ent
(sel
ect a
ll th
at a
pply
) m
ass
sect Macrocalc~ications
Mic
roca
lcifi
catio
ns o
ut o
f m
ass
Mic
roca
lcifi
catio
ns in
mas
s
no c
alci
ficat
ions
see
n
~O5mm
I I I
Sp
ecia
l C
ase
s
0 N
one
Sp
eci
al
case
s ar
e th
ose
with
a u
niq
ue
dia
gn
osi
s (s
elec
t all
that
app
ly)
or
find
ing
~ Mas
s in
or
on s
kin
For
eign
bod
y Ly
mph
nod
es-in
tram
amm
ary
Lym
ph n
odes
-axi
lla
I incl
udin
g se
bace
ous
or e
pide
rmal
incl
usio
n cy
st
kelo
id
etc
in
clud
ing
clip
co
il w
ire c
athe
ter
slee
ve
silic
one
etc
in
bre
ast
incl
udin
g ax
illar
y ta
il
Va
scu
lari
ty
(sel
ect o
ne)
~ Can
not a
sses
s va
scul
arity
N
one
Sam
e as
in n
orm
al t
issu
e D
ecre
ased
In
crea
sed
colo
r flo
w n
ot d
one
or in
adeq
uate
for
inte
rpre
tatio
n no
col
or fl
ow
less
than
in n
orm
al ti
ssue
m
ore
than
in n
orm
al ti
ssue
I
Th
ere
are
lim
ite
d d
ata
to
su
pp
ort
ma
na
ge
me
nt
reco
mm
en
da
tio
ns
tor
so
lid
ma
sse
s b
ase
d o
n u
ltra
so
un
d fi
nd
ing
s a
t th
is t
ime
How
ever
w
hat
wou
ld b
e yo
ur
bes
t ass
essm
ent
an
d m
an
ag
emen
t rec
omm
enda
tion
in e
ach
case
Inco
mp
lete
Asse
ssm
en
t 0
Inco
mpl
ete
addi
tiona
l eva
luat
ion
need
ed b
efor
e fin
al a
sses
smen
t
Fin
al A
sse
ssm
en
t C
ate
go
ry
Neg
ativ
e B
enig
n fin
ding
~ Pro
babl
y be
nign
S
uspi
ciou
s ab
norm
ality
H
ighl
y su
gges
tive
of m
alig
nanc
y ------------------------------shy
no le
sion
foun
d (r
outin
e fo
llow
-up)
no
mal
igna
At f
eatu
res
ex-
cyst
(ro
utin
e fo
llow
-up)
lo
w p
roba
bilit
y o
f can
cer
ex-
fibro
aden
oma
(sho
rt in
terv
al fo
llow
-up)
in
term
edia
te p
roba
bilit
y o
f can
cer
(tis
sue
sam
plin
g)
high
pro
babi
lity
of c
ance
r (t
issu
e sa
mpl
ing)
-
Fo
r e
ach
of
the
ab
ove
ca
teg
ori
es
se
lect
the
te
rm t
ha
t b
est
de
scri
be
s th
e d
om
ina
nt
lesi
on
fe
atu
re
m
Wh
ere
ver
po
ssib
le
de
fin
itio
ns
an
d d
esc
rip
tio
ns
use
d i
n B
I-R
AO
S (
Re
sto
n
VA
) fo
r m
am
mo
gra
ph
y w
ill b
e a
pp
lied
to
ult
raso
un
d
Z o
Ple
ase
ma
rk th
e b
ox
be
sid
e y
ou
r se
lect
ion
m
r (f
JC
opyr
ight
200
1 A
mer
ican
Col
lege
of R
adio
k)gy
Bas
ed o
n F
inal
Rep
ort
of E
xper
t W
orki
ng G
roup
D
evel
oped
Un
de
r Co
ntr
act
282
-97-
0016
-B
etw
een
us
Pub
lic H
eart
h S
ervi
ce O
ffic
e o
n W
omen
s H
ealth
us
De
pa
rtm
en
t o
f Hea
lth
and
Hum
an
o S
ervi
ces
an
d t
he A
me
rica
n C
olle
ge
of R
adiO
logy
z rn
m
IJ
p tgt
Z
o
m
IJ
IJ j
f
_
rr
_
(I)
j _
~
m Q~
-
-
_ ~
0 (
) o
en
en
c--
0 (l
)
shy
~
2
r
c
nC
ll
O-C
sect8sect35~
cr
7
-
r
co
-0
Q)
0 b
~
(1)
-o~
rl
-
~
pl
-
(I)r~m
lt
~
()
223 TOWARD A STANDARDIZED BREAST ULTRASOUND LEXICON
Fig 11 Special cases Skin lesions lymph nodes and foreign bodies are also demonstrable with breast ultrasonogmiddot raphy (A) A typical intramammary lymph node with an echogenic hilum is shown (arrows) (8) Extracapsular spread of silicone gel from a ruptured silicone implant usually manmiddot ifests itself as echogenic noise or a snowstorm pattern (curved arrow)
sing le view of each lesion In prac ti ce descripto rs should be based on multiple views of masses obtained in orthogonal imaging planes in accord with the ACR Standard for the Ultrasound Exa mshyination of the Breast 3 Primary descriptors of masses (shape ori entation margin and echo patshytem ) are generall y listed in order of increasing risk of malignancy top to bottom altho ugh further validation of the risk of malignancy is needed Secshyondary features associated fi ndings or effects on sUlTounding tissue are not listed in any particular order as fLll1her assessment of the risk of mali gnancy for each feature is needed In refening to Tabk 1 it is important to re-emphasize that greatest specific ity is achieved by the evaluation of multiple features of the mass rather than any single attlibute
Certain prob le ms of descrip tion nomenclashyture a nd ca tegori za tion have no t been reso lved
Fig 12 Vascularity The role of vascularity in the characmiddot terization of breast masses is not fully defined Therefore description of vascular features is optional Vascularity asmiddot sessed with color or power Doppler is described as the same increased or decreased compared with adjacent normal breast tissue Power Doppler of a high-grade carcinoma with increased vascularity (arrowheads) is shown
Fig 13 Tubular mass A complex centrally cystic mass tubular in shape with hyperechoic indistinct rim and hetermiddot ogeneous internal echoes is noted Thi s patient is on coumamiddot din and developed a hematoma in the breast Although the features suggest potential need for biopsy the combination of clinical history and imaging findings allows classification of this finding as probably benign with shortmiddotinterval followmiddotup recommended
For example ove rl ap of shape and margin ca teshygories (eg irregular) has bee n discussed in the development of both mammography and ult ra shysound lex icons Cse of the term tu bular may be appropria te as a shape (Fig 13) o r special case (eg dil a ted duct) The benign les io n apocrine metapasia l with its characterist ic m icrolobushyla ted margin bu t otherwise iden ti fi ably benig n microcys tic components (Fig 14) might be a spec ia l case be tter includ ed and desc ri bed for its uni q ue ness than analyzed by indi vi dual desc ri pshyto rs such as irregu lar micro lobu lated and comshyplex that woul d otherwise prompt ti ssue di ag noshySIS
Another dil emma is classifica tion of lesion s by
Fig 14 Apocrine metaplasia (A) Microlobulated masses with microcysts are typical of apocrine metaplasia and may rarely contain calcifications (arrow) (8) Enhancement is sometimes evident Such lesions can be considered benign or probably benign and followed 25
l
224
Table 2 BI-RADS Ultrasound Final Assessment Categories
Assessment Categories and Codes Recommendations
O-Incomplete Needs additional imaging evaluation
1-Negative Routine follow-up for age 2-Benign finding Routine follow-up for age 3-Probably benign finding Short-term follow-up
(usually in 6 mo nths) 4-Suspicious abnormality Requires tissue sampling 5-Highly suggestive of Requires tissue sampling
malignancy
their echogenicity that is_ defined relative to fat or fibroglanduar tissue Some masses notably fibroshyadenomas are similar to fat lobules in shape and echogenicity Should they be described as hyposhyechoic using fibroglandular tissue as the basis for comparison just as fat lobules are hypoechoic to fibroglandular tissue or should they be termed isoechoic to fat) Further in need of validation are the categories of thickness of circumscribed marshygins and the characterization of solid masses by their matrix homogeneity 1any fibroadenomas are heterogeneous and some carcinomas are homoshygeneous What is the predictive value of these features alone or in combination with other feashytures
FINAL ASSESSMENT
As with mammography a Br-RADS final asshysessment and recommendation should be specified (Table 2) When breast sonography is pelformed as an adjunct to mammography one final as sessment and management recommendation should be specshyified which reflects combined mammographic and sonographic findings Final assessment and man-
MENDELSON BERG AND MERRITI TOW
agement should be predicated on the basis of the II
most suspicious feature(s) present preo Radl
I SUMMARY
solie
The approach outlined above for describing and and
reporting sonographic features of breast masses I
represents only the initial step in the development repc m
of a comprehensive system to enhance the accurate I
identification reporting and analysis of sonoshygraphic abnormalities of the breast Future revishysions with validation of interobserver consistency anal
in application of these descriptors across multiple toll
I centers with feedback from potential users in the Cha breast imaging community will undoubtedly exshy M O
pand the utility of this eff0l1 I bre
AJFACKNOWLEDGMENTS I
Participating in the development of the standardshy son
ized breast lexicon were the members of the Expert Working Group to Plan and Develop Protocols for WOI
Optimization and Clinical Testing of Breast Ultrashydial
19S sound Steering Committee-Christopher R B Menitt MD Chairman Barry B Goldberg MD con
Ellen B 1endel son MD Lexicon Subcommitshy 191
tee-Ellen B 1endelson MD chair Janet K Baum MD Christopher R B Merritt MD Eva
Inc
Rubin MD ExpeI1 Working Group-Janet K Baum MD Lawrence W Bassett MD Paul L Carson_ PhD David Cosgrove MD A Pat Romshyilly 10 Barbara S Hertzberg 10 Valerie P Jackson 10 Robert R Kuske Jr MD Helmut Madjar MD PhD Jonathan Ophir PhD Steve H Parker MD Catherine W Piccoli MD Eva Rushybin MD Gordon F Schwartz MD Edward A Sickles MD and Jonathan Sunshine PhD
REFERENCES
1 Rosenberg AL Schwanz GF Feig SA et al Clinically
occult breast les ions Localization and signincanclt Radiology
162 167-170 1987
2 Bassett LW Liu TH Giuliano AE et al The prevalence
of carcinoma in palpable vs impalpable mammog raphicaJly
detected les ions AJR Am J Roentgenol 157 21-24 1991
3 ACR Standard for the Pelformance of Breast Ultrasou nd
Examination ACR Standards Resto n V A American Coll ege
of Radiology 2000 pp 389-392
4 Merritt CRB The Breast Nodule in Ultrasound A Pracshy
tical Approach to Clinica l Problems (ch 52) in Bluth EI Ar2er
P Benson C et al (eds) A Prac ti ca l Approach to Clinical
Problems New York Thieme 2000
5 Stavros AT Thickman D Rapp CL et a1 Solid breast
nodules Use of sonog raphy to di stingui sh between beni g n and
malignant lesions Radiology 196 123-134 1995
6 Taylor KJW HOI Breast Sc reening Researc h (ATL) Can
complementary US reduce the number of biopsies of beni gn
breast massesry Radiology 189(P) 179 1993 (abstr suppl )
7 High defi niti on imag ing The ro le o f ultrasound in the
di agnosis of breast cancer Bothell WA Advanced Technology
Labo ratorie 1 99 ~
8 Zonderand HM Coerkamp EG Hem1ans J et al Diagshy
nosis of breast cancer Contribution of US as an adjuJlc t to
mammography Radiol ogy 21341 3-422 1999
9 Sickl es EA Filly RA Callen PW Breast cancer detecshy
ti o n wi th so nograph y a nd mammography Compariso n using
sta te-o f-the-a rt equipme nt AJR Am J Roenlgenol 140843shy
84 5 1983
10 Skaane P Sauer T Ultrasonograph y of malignant breast
neoplasms Anal ys is of cuc inomas missed as lumor Acta
Radiol 40376-382 1999
225 TOWARD A STANDARDI ZED BREAST ULTRASOUND LEXICON
II Berg W A Gilbrea th PL Whole breast ul trasound in preoperative evaluati on for multicentric and multi foca l cancer Radiology 2 1459-66 2000
12 Baker lA Kornguth Pl Soo MS et al Sonography of solid breast les ions Observer variability of les ion description and assessment AJR Am 1 Roentgenol 172 1621- 1625 1999
13 American Co llege of Radiology (ACR) Breast imag ing reponing and data system (BI-RADSlgtt) (ed 3) Res ton VA Ameri can College of Radiology 1998
14 Morris EA lliustrated breast MR lex icon Semin Roentshygenol 36XX 2001
15 Cole-Beuglet C Soriano RZ Kurtz B et al Ultrasound analysis of 104 primary breast carcinomas c1ass itied according to hi stopathologic type Radio logy 147 1 91-196 1983
16 Mendelson EB The Breast in Wilson S Rumack C Charboneau JW (eds ) Diagnost ic Ultrasound (ed 2) St Louis Mosby 1998 pp 75 1-789
17 Hilton SvW Leopold GR Ol son LK et al Real-time breast sonography Applica ti on in 300 consecuti ve patients AJR Am J Roentgenol 147479-486 1986
18 Jokich PM Monticciolo DL dler YT Breast ultrashysonography Radi ol Cl in North Am 30993-1009 1992
19 Kolb TM Lichy J Newhouse JH Occu lt cancer in women with dense breasts Detection with sc reening USshydi agnostic yield and tumor charac teri stics Rad iology 207 191 shy1991998
20 Venta LA Kim JP Pelloski CE et al Management of complex breast cysts AJR Am J Roentgenol 173 133 1-1 336 1999
21 Buchberger W DeKoek koek-Do ll P Springer P ct al Incidental findings on sonog raphy of the breast Clinical sigshy
ni fi cance and diagnostic worku p AJ R Am J Roentgenol 173 92 1-927 1999
22 Jackson VP Management of so lid breast nodul es What is the role of sonography~ Radiology 196 14- 15 1995 (editoshyrial )
23 Sick les EA Periodic mammographic fo ll ow-u p of prob shyab ly benign les ions Results in 3184 consecuti ve cases Radishyology 179463-468 1991
24 Sickles EA )onpalpable c ircumscribed nonca lcified so lid breast masses Like lihood of ma lignancy based on les ion size and age of patient Radiology J92439-442 1994
25 Warner lK Kum Jr 0 Berg WA Apocrine metaplas ia Mammographic and sonographic appearances AJ R m J Roentgenol 170 1375-1379 1998
26 Rahbar G Sie Ac Hansen Gc et a1 Benign versus malignant sol id breas t masses US different iation Radiology 2 13889-894 1999
27 Hanis KJv Ganon MA Shestak KC et al Si licone implant rupture Detect ion wi th US Radiology 18776 1-768 1993
28 Cosgrove DO Kedar RP Bamber Jc et al Breast di seases Color doppler US in differenti al diagnosis Radiology 18999-104 1993
29 VlcNic holas MM Mercer PM Miller JC et al Color Doppler sonography in the evaluation of palpable breast masses AJR m 1 Roentgenol 161 765-77 1 1993
30 Ra7a S Ballm JK Solid breast les ions Evaluation with power Doppler tS Radiology 203 164-168 1997
31 Skaane P Engedal K Anal ysis of sonographic features in the differentiation of fibroadenoma and invas ive ducta l carcino ma AJR m J Roentgenol 170 109- 1 14 1998

218 MENDELSON BERG AND MERRITI
Fig 1 Shape Masses are described as round (A) oval (B) or irregular (C) A round mass is spherical ball-shaped or globular in shape An oval mass is elliptical or egg-shaped These descriptors are similar to those used in the ACR BI-RADS lexicon for mammography (A) A spherical simple cyst is shown (B) An oval fibroadenoma is shown The invasive cancer shown in C is irregular
FEATURE ANALYSIS
Lesion features include primary fea tures such as shape (Fig 1) orientation (Fig 2) margins (Figs 3 through 5) matri x echogenicity and homogeneity (Figs 6 and 7) and attenuation (Fig 8) which should be described and applied in a consistent fashion In addition secondary associated findings such as architectural distortion (Fig 9) retraction or angulation of Coopers ligaments (Fig 9B) di lated ducts calcifications (Fig 10) and changes in the ski n subcutaneous fat and pectoral muscle can be recorded as well These fea tures of masses have been enumerated previously5715 16 The utility of
each category of features requires validati on along with that of individual descriptors For example matrix homogeneity probably has less specificity and significance than description of mass marg ins The most appropriate descriptor for each category of characteristics shou ld be applied whe n desc ribshying a lesion (Table 1) Wherever poss ible fea ture descriptors similar to those used by BI-RADS fo r mammography have been imported As with mamshymography use of the lexicon is predicated on
Fig 2 Orientation Mass orientation refers to the relationshyship of the long axis of the mass to the skin This may be parallel as is common with fibroadenomas (A) or not parallel a common orientation for many cancers (B) Because round lesions do not have one axis that is longer than another they should be classified as not parallel
Fig 3 Margins The margin is the boundary between the lesion and its surroundings Several characteristics of the lesion margin are important The margin should be described as circumscribed (distinct and smooth) (A) or irregular (indisshytinct microlobulated angUlar or spiculated) (B) In A the circumscribed margin of a fibroadenoma is shown In B an invasive cancer demonstrates an ill -defined or indistinct inshyterface with the surrounding tissues As in mammography ill-defined margins are associated with higher risk of maligshynancy than circumscribed margins
exce llent sonographic technique using a linear transd ucer whose center frequency is at least 7 MHz Documentation should be performed in acshycord with the American Colleoe of Radioloayeo c
Standards Orthogonal v iews of the lesion should be obtained and the orientation of the transducer and location of the abnormality should be deshyscribed using quadran t clock-face location andlor labeled diagram of the breast ideall y including distance from the nipple
Several previous studies5 15 reach the conclushysion that multiple features must be analyzed to achie ve as great a specificity as possible in sonoshygraphic charac terizati on As an example the diagshynosis of a mass as a si mple cyst requires that the shape be rou nd oval or gently lobul ated margin circumscribed echogenicity (echo pattern) aneshychoic and that there be acoustic enhancement Based on these combined features the impress ion is that of a simple cyst (Figs 1 5 and 6) The final assessme nt for the combination of mammographic
Fig 4 Margin thickness Circumscribed margins may be thin thick or of mixed thickness The fibroadenoma (A) has a thin and distinct boundary delineating it from surrounding breast tissue The invasive cancer in 4B has generally thick margins whereas the cancer in C shows a margin composed of thick thin and indistinct segments Barely perceptible margins favor benign etiology
TOWARD A STANDARDIZED BREAST ULTRASOUND LEXICON 21 9
Fig 5 Margins The smooth barely perceptible margin of a simple cyst (A) is contrasted with the irregular margins of a small invasive cancer (B) Margin irregularities may include angular edges m icrolobulation and spiculation
and sonographic fi ndings using BI-RADS is cateshygory 2 benign with routine screening recomshymended The accuracy of sonographi c identificashyti on of cysts approaches 100 provided stric t ad herence to the classical sonographic charac teri sshytics are observed 17
t
Practical use of any lexicon req uires an undershystanding of the de fin iti ons of each term An examshypJe is complicated versus complex The presence of homogeneous low-level internal echoes throug holl t a cystic lesion that has all the other features of a sim ple cyst as above results in its designation as complicated 18 Many of these masses appear solid a lbeit benign and may be reported as comshyplicated cyst or probabl y ben ign solid lesion Often such lesions are incidentall y found during ul trasound examination peIiormed for other reashysons Recent studies cumulative ly evaluating 567 incidental compli cated cysts identifi ed only one 3-mm in situ ma lignancy (positive predictive value [PPY] 02)1 9-21 Based on these data short-term follow-up appears appropriate (BI-RADS category 3 probabJy ben ign) although further validation is
Fig 6 Echogenicityechotextureecho pattern The matrix of a mass may be homogeneous or heterogeneous Homogeshyneous masses may be anechoic hypoechoic or hyperechoic Cysts are typically anechoic (A) The echogenicity of hyposhyechoic and hyperechoic masses should be compared with the echogenicity of fibroglandular tissue In this example a hamartoma produces a homog eneous mass (arrows) that is hyperechoic compared with fat (B) Invasive cancer (C) is often hypoechoic both to fat and to glandular tissue (same lesion as in Fig 2B)
Fig 7 Echogenicityechotextureecho pattern Heterogeshyneous masses may be solid or complex conta ining a mixture of solid and cystic components The invasive cancer in A is predominantly hypoechoic but contains some areas of inshycreased echogenicity resulting in a heterogeneous echotexshyture Complex masses may be predominantly solid (B) or cystic (C both intracystic papillary carcinomas) and should be regarded as suspicious for cancer in the absence of clinical finding s suggesting an abscess
encouraged Interval enl argement (mammographishycall y or sonograph ical ly) or the presence of any suspicious features should prompt aspi ration and possible core biopsy if it proves solid 22
Suspicious features include an intracystic mass mural nodule thick septations or a thi ck or irregshyul ar wall When such fea tures are present the mass should be desc ribed as a complex cystic mass (Figs 7B and C) These lesions generall y requ ire aspiration or biopsy (BI-RADS category 4 susp ishycious)
When a so lid lesion is presen t careful analysis of contour margins matri x and attenuation may a llow classification of some nodules as BI-RADS category 3 probab ly benign and provide the opshyti on of short interva l follow-up at 6 months 12 months and 24 mon ths rather than biopsy5-7 As in ma mmography for a lesion to be assessed as probably benign it should have lt2 risk of malignancy 2324 As mentioned preliminary data suggest cysts with internal echoes can be so classhysified as can clusters of tin y cystic foci wi th thin intervening septatio ns compatible with apocrine metaplas ia 25
Fig 8 ShadOWingenhancement Enhancement may be seen with cysts (A) fibroadenomas (B) and high-grade inshyvasive cancers (C) Central shadowing is associated with the small invasive cancer is shown in C Refractive edge shadowing (present in A and B) is excluded from considershyation A single echogenic calcification is present in the fibroshyadenoma (8)
220
Fig 9 Effect on surrounding tissue Masses may affect surrounding breast tissues resulting in architectural distorshytion (A) Extensive distortion of breast architecture by a small scirrhous cancer is shown (8) A more subtle change is seen where a Cooper ligament is interrupted by a cancer (open arrows)
Stavros et a]5 proposed three categories of solid lesions that could be class ified as BI-RADS cateshygory 3 probably benign in the absence of any suspicious features (I) masses with intense and uniform hyperechogenicity re lative to fat (2) masses with an ellipsoid shape and thin echogenic capsule and (3) masses with two or three gentle lobulations and a thin echogenic capsu le Individshyually each of these characteristics had a negative predictive va lue for malignancy of 988 to 100905 Although accepted by some it is important to note that these results have not been validated across multiple centers Indeed one recent study26
suggests that not all readers achieve sufficiently high specificity to fo llow so lid lesions [n the draft BI-RADSUltrasound lexicon the concept of a thin echogenic capsule or pseudocapsule- has been replaced by that of a thin smooth margin analoshygous to a circumscribed mass mammographishycally Although palpable solid lesions are genershyally recommended for biopsy 2l24 it is not yet clear whether any size criterion or palpability of the lesion influences the absolute risk of malignancy
For solid masses irregularity of shape and margins dominate other features suggesting maligshynancy with a PPY of ma lignancy of 86 to 9357 such lesions are appropriately classified as BI-RADS category 4 or 5 with biopsy recomshymended Other features have lower specificity Orientation of the long axis of the mass nonparalshylel to the skin synonymously termed taller than wide5 has been associated with a 62 to 81 Ok likelihood of malignancy57 and is more common ly seen in cancers lt 1 cm in size Ylost fibroadenoshymas as well as many cancers are oriented with their long axes parallel to the skin (wider than tall) J I
Echotextureecho pattern appears to be less helpful in differentiating benign fro m malignan t sol id
MENDELSON BERG AND MERRITI
masses I as most masses will be hypoechoic to pare nchyma Acoustic attenuation (shadowing) is suspicious for malignancy but as many as 2 1 of benign les ions will show shadowing7 Similarly acoustic enhancement while common in benign lesions may be present in up to 42 of cancerss
Several typically benign lesions are included as special cases (Fig 11) This includes lymph nodes with a thin circumscribed capsule and centra l echogenic hi lum Foreign bodies are spec ial cases and include siliconomas and free extracapsu lar silicone (Fig 11)27 Description of vascu larity of the lesion is not a required standard (Fig 12) as no reliable distinction has yet been made between
30benign and malignant lesions on this basis 2 8shy
Vasc ularity is described as the same increased_ or decreased relative to surrounding parenchyma
Table I is a worki ng draft of a breast ultrasound lexicon including feature categories and descripshytors Although different in format this draft was based largely on the version developed by the Lexicon Committee of the Expert Working Group It is important to note that these recommendations awa it va lidation and are subject to modification before release of the final draft of the ACR BIRADSlltrasound Descriptors are illustrated in Figures 1 through 12 The illustrations show only a
Fig 10 Associated finding s Dilated ducts skin changes and calcifications associated with breast masses may be seen with ultrasonography and should be described when present (A) Macrocalcifications (~0 5 mm) associated with a fibroad shyenoma are shown (arrowheads) (8) Microcalcifications laquo05 mm) in an invasive ductal carcinoma are shown (arrows) (C) Microcalcifications not in a mass and particularly within a tubular dilated duct (curved arrow) are suspicious and may be seen in ductal carcinoma in situ as in this example
bull TC
0 f-
bull
bull
rJ
Ca
se
Re
vie
we
r o
_
gtC
LA
SS
IFIC
AT
ION
CA
TE
GO
RIE
S amp
TE
RM
S
DE
SC
RIP
TIO
N
Ta
ble
1
Dra
ft A
CR
BI-
RA
DS
Ult
raso
un
d L
exi
con
Cla
ssif
ica
tio
n F
orm
4-4
-01
~
Ma
sse
s
ArI
2sect
secto
ccup
ies
spac
e an
d sh
ould
be
seen
in
two
diffe
rent
pr
ojec
tions
Sha
pe
(sel
ect
one)
0O
val
Rou
nd
Irre
gula
r
ellip
tical
or
egg-
shap
ed (
ma
y in
clud
e tw
o o
r th
ree
undu
latio
lls
ie
lob
ular
)
sphe
rical
ba
ll-sh
aped
ci
rcul
ar
or g
lob
ula
r ne
ither
roun
d n
or o
val
Ori
enta
tion
B P
aral
lel
long
axi
s o
f les
ion
orie
nted
alo
ng s
kin
line
(w
ider
than
tal
l)
(sel
ect
one)
N
ot P
aral
lel
no lo
ng a
xis
or
axis
no
t orie
nted
alo
ng s
kin
line
(ta
ller t
han
wid
e)
Mar
gin
C
ircu
msc
ribe
d (s
elec
t al
l tha
t ap
ply)
Y
ES
(d
yes
che
ck o
ne o
ptio
n be
lOW
)0 8
No
perc
eptib
le r
im o
r th
in r
im
Thi
ck r
im
NO
(if
no
go
to i
rreg
ular
)0
IRR
EG
ULA
R (
sele
ct a
ll th
at
appl
y)
0 In
dist
inct
A
ng
ula
r M
icro
lobu
late
d S
picu
late
d ~
Ech
o P
atte
m
A
nech
oic
Hyp
erec
hoic
C
ompl
ex
Hyp
oech
oic
~ (s
elec
t on
e)
Po
ste
ri or
Aco
ustic
N
o po
ster
ior
acou
stic
fea
ture
s F
eatu
res
Enh
ance
men
t S
hado
win
g C
om
bin
ed p
atte
rn
~ S
urro
undi
ng T
issu
e 0
No
effe
ct
BIden
tifia
ble
effe
ct (
sele
ct a
ll th
at a
pp
ly)
Duc
ts
Coo
pers
liga
men
t ch
an
ge
s
0E
dem
a A
rchi
tect
ural
dis
tort
ion
Ski
n T
hick
enin
g
B S
kin
retr
actio
nflr
regu
lari
ty
Pec
tora
l m
uscl
e se
en
bu
t pl
ane
with
an
teri
or
tissu
e is
un
cle
ar
Sm
ooth
dis
tinct
mar
gin
with
thi
n t
hick
or
no p
erce
ptib
le li
near
rim
circ
umsc
ribe
d m
argi
n w
ithin
lin
ear
rim
circ
umsc
ribe
d m
argi
n w
me
asu
rab
le th
ick
rim gt
1 m
m b
etw
een
lesi
on a
nd s
urro
undi
ng t
issu
e
mar
gins
dem
onst
ratin
g a
com
bina
tion
of f
eatu
res
incl
udin
g at
leas
t 1
of t
hose
list
ed b
elow
poor
ly d
efin
ed m
argi
n pa
rt o
r al
l of t
he m
argi
n fo
rmed
by
shar
p lin
ear
inte
rsec
tions
that
form
acu
te a
ngle
s m
argi
n ch
arac
teri
zed
by b
y gt
3 sm
all
sho
rt c
ycle
und
ulat
ions
m
argi
n ch
arac
teri
zed
by
shar
p pr
ojec
ting
lines
with
out
inte
mal
ech
oe
s de
fined
rel
ativ
e to
fat
eq
ua
l to
fibro
glan
dula
r tis
sue
com
bine
d cy
stic
(an
echo
ic)
and
ech
og
en
ic c
om
po
ne
nts
de
fined
rel
ativ
e to
fib
rogl
andu
lar
tissu
e i
soec
hoic
or
hyp
oe
cho
ic to
fat
con
tain
s lo
w-l
evel
ecl
hoes
th
roug
hout
(eg
co
mpl
icat
ed c
yst o
r fib
road
enom
a)
no p
oste
rior
sha
dow
ing
or e
nh
an
cem
en
t in
crea
sed
post
erio
r ec
hoes
de
crea
sed
post
erio
r ec
hoes
ex
clud
ing
edge
sh
ad
ow
s bo
th s
hado
win
g an
d e
nh
an
cem
en
t
surr
ound
ing
tissu
e un
affe
cted
by
lesi
on
abno
rmal
cal
iber
an
do
r arb
oriz
atio
n st
raig
hten
ing
or th
icke
ning
of C
oope
rs li
gam
ents
(cu
rvili
near
co
nn
ect
ive
tissu
e b
an
ds
prov
idin
g su
ppor
t fo
r th
e br
east
s)
incr
ease
d ec
hoge
nici
ty o
f sur
roun
ding
tis
sue
ret
icul
atio
n i
nclu
des
an
gu
lar
hyp
oe
cho
ic li
nes
disr
uptio
n o
f nor
mal
ana
tom
ic p
lane
s fo
cald
iffus
e sk
in t
hick
enin
g-no
rmal
ski
n is
gt2
mm
in t
hick
ness
exc
ept i
n th
e pe
riar
eola
r ar
ea
and
low
er b
reas
ts
skin
sur
face
is c
onca
ve o
r iII
-def
ined
ap
pear
s pu
lled
in
diso
rder
ed e
cho
pa
tte
m in
volv
ing
pect
oral
mu
scle
sug
gest
ive
of i
nvas
ion
(exc
lude
tech
nica
l ca
uses
suc
h a
s im
prop
erly
pla
ced
foca
l zo
ne
) _
-shy
~ z ~ rJ o N
m
o (lJ
rJ ~ ~
c ~
rJ ampi o c z o r m
x o o z
I
I
C
LA
SS
IFIC
AT
ION
CA
TE
GO
RIE
S amp
TE
RM
S
DE
SC
RIP
TIO
N
Ca
lcif
ica
tio
ns
0 N
one
seen
C
alc
ifica
tion
s a
re p
oo
rly
cha
ract
eri
zed
with
ul
traso
und
but c
an b
e re
cogn
ized
par
ticul
arly
in a
If
pres
ent
(sel
ect a
ll th
at a
pply
) m
ass
sect Macrocalc~ications
Mic
roca
lcifi
catio
ns o
ut o
f m
ass
Mic
roca
lcifi
catio
ns in
mas
s
no c
alci
ficat
ions
see
n
~O5mm
I I I
Sp
ecia
l C
ase
s
0 N
one
Sp
eci
al
case
s ar
e th
ose
with
a u
niq
ue
dia
gn
osi
s (s
elec
t all
that
app
ly)
or
find
ing
~ Mas
s in
or
on s
kin
For
eign
bod
y Ly
mph
nod
es-in
tram
amm
ary
Lym
ph n
odes
-axi
lla
I incl
udin
g se
bace
ous
or e
pide
rmal
incl
usio
n cy
st
kelo
id
etc
in
clud
ing
clip
co
il w
ire c
athe
ter
slee
ve
silic
one
etc
in
bre
ast
incl
udin
g ax
illar
y ta
il
Va
scu
lari
ty
(sel
ect o
ne)
~ Can
not a
sses
s va
scul
arity
N
one
Sam
e as
in n
orm
al t
issu
e D
ecre
ased
In
crea
sed
colo
r flo
w n
ot d
one
or in
adeq
uate
for
inte
rpre
tatio
n no
col
or fl
ow
less
than
in n
orm
al ti
ssue
m
ore
than
in n
orm
al ti
ssue
I
Th
ere
are
lim
ite
d d
ata
to
su
pp
ort
ma
na
ge
me
nt
reco
mm
en
da
tio
ns
tor
so
lid
ma
sse
s b
ase
d o
n u
ltra
so
un
d fi
nd
ing
s a
t th
is t
ime
How
ever
w
hat
wou
ld b
e yo
ur
bes
t ass
essm
ent
an
d m
an
ag
emen
t rec
omm
enda
tion
in e
ach
case
Inco
mp
lete
Asse
ssm
en
t 0
Inco
mpl
ete
addi
tiona
l eva
luat
ion
need
ed b
efor
e fin
al a
sses
smen
t
Fin
al A
sse
ssm
en
t C
ate
go
ry
Neg
ativ
e B
enig
n fin
ding
~ Pro
babl
y be
nign
S
uspi
ciou
s ab
norm
ality
H
ighl
y su
gges
tive
of m
alig
nanc
y ------------------------------shy
no le
sion
foun
d (r
outin
e fo
llow
-up)
no
mal
igna
At f
eatu
res
ex-
cyst
(ro
utin
e fo
llow
-up)
lo
w p
roba
bilit
y o
f can
cer
ex-
fibro
aden
oma
(sho
rt in
terv
al fo
llow
-up)
in
term
edia
te p
roba
bilit
y o
f can
cer
(tis
sue
sam
plin
g)
high
pro
babi
lity
of c
ance
r (t
issu
e sa
mpl
ing)
-
Fo
r e
ach
of
the
ab
ove
ca
teg
ori
es
se
lect
the
te
rm t
ha
t b
est
de
scri
be
s th
e d
om
ina
nt
lesi
on
fe
atu
re
m
Wh
ere
ver
po
ssib
le
de
fin
itio
ns
an
d d
esc
rip
tio
ns
use
d i
n B
I-R
AO
S (
Re
sto
n
VA
) fo
r m
am
mo
gra
ph
y w
ill b
e a
pp
lied
to
ult
raso
un
d
Z o
Ple
ase
ma
rk th
e b
ox
be
sid
e y
ou
r se
lect
ion
m
r (f
JC
opyr
ight
200
1 A
mer
ican
Col
lege
of R
adio
k)gy
Bas
ed o
n F
inal
Rep
ort
of E
xper
t W
orki
ng G
roup
D
evel
oped
Un
de
r Co
ntr
act
282
-97-
0016
-B
etw
een
us
Pub
lic H
eart
h S
ervi
ce O
ffic
e o
n W
omen
s H
ealth
us
De
pa
rtm
en
t o
f Hea
lth
and
Hum
an
o S
ervi
ces
an
d t
he A
me
rica
n C
olle
ge
of R
adiO
logy
z rn
m
IJ
p tgt
Z
o
m
IJ
IJ j
f
_
rr
_
(I)
j _
~
m Q~
-
-
_ ~
0 (
) o
en
en
c--
0 (l
)
shy
~
2
r
c
nC
ll
O-C
sect8sect35~
cr
7
-
r
co
-0
Q)
0 b
~
(1)
-o~
rl
-
~
pl
-
(I)r~m
lt
~
()
223 TOWARD A STANDARDIZED BREAST ULTRASOUND LEXICON
Fig 11 Special cases Skin lesions lymph nodes and foreign bodies are also demonstrable with breast ultrasonogmiddot raphy (A) A typical intramammary lymph node with an echogenic hilum is shown (arrows) (8) Extracapsular spread of silicone gel from a ruptured silicone implant usually manmiddot ifests itself as echogenic noise or a snowstorm pattern (curved arrow)
sing le view of each lesion In prac ti ce descripto rs should be based on multiple views of masses obtained in orthogonal imaging planes in accord with the ACR Standard for the Ultrasound Exa mshyination of the Breast 3 Primary descriptors of masses (shape ori entation margin and echo patshytem ) are generall y listed in order of increasing risk of malignancy top to bottom altho ugh further validation of the risk of malignancy is needed Secshyondary features associated fi ndings or effects on sUlTounding tissue are not listed in any particular order as fLll1her assessment of the risk of mali gnancy for each feature is needed In refening to Tabk 1 it is important to re-emphasize that greatest specific ity is achieved by the evaluation of multiple features of the mass rather than any single attlibute
Certain prob le ms of descrip tion nomenclashyture a nd ca tegori za tion have no t been reso lved
Fig 12 Vascularity The role of vascularity in the characmiddot terization of breast masses is not fully defined Therefore description of vascular features is optional Vascularity asmiddot sessed with color or power Doppler is described as the same increased or decreased compared with adjacent normal breast tissue Power Doppler of a high-grade carcinoma with increased vascularity (arrowheads) is shown
Fig 13 Tubular mass A complex centrally cystic mass tubular in shape with hyperechoic indistinct rim and hetermiddot ogeneous internal echoes is noted Thi s patient is on coumamiddot din and developed a hematoma in the breast Although the features suggest potential need for biopsy the combination of clinical history and imaging findings allows classification of this finding as probably benign with shortmiddotinterval followmiddotup recommended
For example ove rl ap of shape and margin ca teshygories (eg irregular) has bee n discussed in the development of both mammography and ult ra shysound lex icons Cse of the term tu bular may be appropria te as a shape (Fig 13) o r special case (eg dil a ted duct) The benign les io n apocrine metapasia l with its characterist ic m icrolobushyla ted margin bu t otherwise iden ti fi ably benig n microcys tic components (Fig 14) might be a spec ia l case be tter includ ed and desc ri bed for its uni q ue ness than analyzed by indi vi dual desc ri pshyto rs such as irregu lar micro lobu lated and comshyplex that woul d otherwise prompt ti ssue di ag noshySIS
Another dil emma is classifica tion of lesion s by
Fig 14 Apocrine metaplasia (A) Microlobulated masses with microcysts are typical of apocrine metaplasia and may rarely contain calcifications (arrow) (8) Enhancement is sometimes evident Such lesions can be considered benign or probably benign and followed 25
l
224
Table 2 BI-RADS Ultrasound Final Assessment Categories
Assessment Categories and Codes Recommendations
O-Incomplete Needs additional imaging evaluation
1-Negative Routine follow-up for age 2-Benign finding Routine follow-up for age 3-Probably benign finding Short-term follow-up
(usually in 6 mo nths) 4-Suspicious abnormality Requires tissue sampling 5-Highly suggestive of Requires tissue sampling
malignancy
their echogenicity that is_ defined relative to fat or fibroglanduar tissue Some masses notably fibroshyadenomas are similar to fat lobules in shape and echogenicity Should they be described as hyposhyechoic using fibroglandular tissue as the basis for comparison just as fat lobules are hypoechoic to fibroglandular tissue or should they be termed isoechoic to fat) Further in need of validation are the categories of thickness of circumscribed marshygins and the characterization of solid masses by their matrix homogeneity 1any fibroadenomas are heterogeneous and some carcinomas are homoshygeneous What is the predictive value of these features alone or in combination with other feashytures
FINAL ASSESSMENT
As with mammography a Br-RADS final asshysessment and recommendation should be specified (Table 2) When breast sonography is pelformed as an adjunct to mammography one final as sessment and management recommendation should be specshyified which reflects combined mammographic and sonographic findings Final assessment and man-
MENDELSON BERG AND MERRITI TOW
agement should be predicated on the basis of the II
most suspicious feature(s) present preo Radl
I SUMMARY
solie
The approach outlined above for describing and and
reporting sonographic features of breast masses I
represents only the initial step in the development repc m
of a comprehensive system to enhance the accurate I
identification reporting and analysis of sonoshygraphic abnormalities of the breast Future revishysions with validation of interobserver consistency anal
in application of these descriptors across multiple toll
I centers with feedback from potential users in the Cha breast imaging community will undoubtedly exshy M O
pand the utility of this eff0l1 I bre
AJFACKNOWLEDGMENTS I
Participating in the development of the standardshy son
ized breast lexicon were the members of the Expert Working Group to Plan and Develop Protocols for WOI
Optimization and Clinical Testing of Breast Ultrashydial
19S sound Steering Committee-Christopher R B Menitt MD Chairman Barry B Goldberg MD con
Ellen B 1endel son MD Lexicon Subcommitshy 191
tee-Ellen B 1endelson MD chair Janet K Baum MD Christopher R B Merritt MD Eva
Inc
Rubin MD ExpeI1 Working Group-Janet K Baum MD Lawrence W Bassett MD Paul L Carson_ PhD David Cosgrove MD A Pat Romshyilly 10 Barbara S Hertzberg 10 Valerie P Jackson 10 Robert R Kuske Jr MD Helmut Madjar MD PhD Jonathan Ophir PhD Steve H Parker MD Catherine W Piccoli MD Eva Rushybin MD Gordon F Schwartz MD Edward A Sickles MD and Jonathan Sunshine PhD
REFERENCES
1 Rosenberg AL Schwanz GF Feig SA et al Clinically
occult breast les ions Localization and signincanclt Radiology
162 167-170 1987
2 Bassett LW Liu TH Giuliano AE et al The prevalence
of carcinoma in palpable vs impalpable mammog raphicaJly
detected les ions AJR Am J Roentgenol 157 21-24 1991
3 ACR Standard for the Pelformance of Breast Ultrasou nd
Examination ACR Standards Resto n V A American Coll ege
of Radiology 2000 pp 389-392
4 Merritt CRB The Breast Nodule in Ultrasound A Pracshy
tical Approach to Clinica l Problems (ch 52) in Bluth EI Ar2er
P Benson C et al (eds) A Prac ti ca l Approach to Clinical
Problems New York Thieme 2000
5 Stavros AT Thickman D Rapp CL et a1 Solid breast
nodules Use of sonog raphy to di stingui sh between beni g n and
malignant lesions Radiology 196 123-134 1995
6 Taylor KJW HOI Breast Sc reening Researc h (ATL) Can
complementary US reduce the number of biopsies of beni gn
breast massesry Radiology 189(P) 179 1993 (abstr suppl )
7 High defi niti on imag ing The ro le o f ultrasound in the
di agnosis of breast cancer Bothell WA Advanced Technology
Labo ratorie 1 99 ~
8 Zonderand HM Coerkamp EG Hem1ans J et al Diagshy
nosis of breast cancer Contribution of US as an adjuJlc t to
mammography Radiol ogy 21341 3-422 1999
9 Sickl es EA Filly RA Callen PW Breast cancer detecshy
ti o n wi th so nograph y a nd mammography Compariso n using
sta te-o f-the-a rt equipme nt AJR Am J Roenlgenol 140843shy
84 5 1983
10 Skaane P Sauer T Ultrasonograph y of malignant breast
neoplasms Anal ys is of cuc inomas missed as lumor Acta
Radiol 40376-382 1999
225 TOWARD A STANDARDI ZED BREAST ULTRASOUND LEXICON
II Berg W A Gilbrea th PL Whole breast ul trasound in preoperative evaluati on for multicentric and multi foca l cancer Radiology 2 1459-66 2000
12 Baker lA Kornguth Pl Soo MS et al Sonography of solid breast les ions Observer variability of les ion description and assessment AJR Am 1 Roentgenol 172 1621- 1625 1999
13 American Co llege of Radiology (ACR) Breast imag ing reponing and data system (BI-RADSlgtt) (ed 3) Res ton VA Ameri can College of Radiology 1998
14 Morris EA lliustrated breast MR lex icon Semin Roentshygenol 36XX 2001
15 Cole-Beuglet C Soriano RZ Kurtz B et al Ultrasound analysis of 104 primary breast carcinomas c1ass itied according to hi stopathologic type Radio logy 147 1 91-196 1983
16 Mendelson EB The Breast in Wilson S Rumack C Charboneau JW (eds ) Diagnost ic Ultrasound (ed 2) St Louis Mosby 1998 pp 75 1-789
17 Hilton SvW Leopold GR Ol son LK et al Real-time breast sonography Applica ti on in 300 consecuti ve patients AJR Am J Roentgenol 147479-486 1986
18 Jokich PM Monticciolo DL dler YT Breast ultrashysonography Radi ol Cl in North Am 30993-1009 1992
19 Kolb TM Lichy J Newhouse JH Occu lt cancer in women with dense breasts Detection with sc reening USshydi agnostic yield and tumor charac teri stics Rad iology 207 191 shy1991998
20 Venta LA Kim JP Pelloski CE et al Management of complex breast cysts AJR Am J Roentgenol 173 133 1-1 336 1999
21 Buchberger W DeKoek koek-Do ll P Springer P ct al Incidental findings on sonog raphy of the breast Clinical sigshy
ni fi cance and diagnostic worku p AJ R Am J Roentgenol 173 92 1-927 1999
22 Jackson VP Management of so lid breast nodul es What is the role of sonography~ Radiology 196 14- 15 1995 (editoshyrial )
23 Sick les EA Periodic mammographic fo ll ow-u p of prob shyab ly benign les ions Results in 3184 consecuti ve cases Radishyology 179463-468 1991
24 Sickles EA )onpalpable c ircumscribed nonca lcified so lid breast masses Like lihood of ma lignancy based on les ion size and age of patient Radiology J92439-442 1994
25 Warner lK Kum Jr 0 Berg WA Apocrine metaplas ia Mammographic and sonographic appearances AJ R m J Roentgenol 170 1375-1379 1998
26 Rahbar G Sie Ac Hansen Gc et a1 Benign versus malignant sol id breas t masses US different iation Radiology 2 13889-894 1999
27 Hanis KJv Ganon MA Shestak KC et al Si licone implant rupture Detect ion wi th US Radiology 18776 1-768 1993
28 Cosgrove DO Kedar RP Bamber Jc et al Breast di seases Color doppler US in differenti al diagnosis Radiology 18999-104 1993
29 VlcNic holas MM Mercer PM Miller JC et al Color Doppler sonography in the evaluation of palpable breast masses AJR m 1 Roentgenol 161 765-77 1 1993
30 Ra7a S Ballm JK Solid breast les ions Evaluation with power Doppler tS Radiology 203 164-168 1997
31 Skaane P Engedal K Anal ysis of sonographic features in the differentiation of fibroadenoma and invas ive ducta l carcino ma AJR m J Roentgenol 170 109- 1 14 1998

TOWARD A STANDARDIZED BREAST ULTRASOUND LEXICON 21 9
Fig 5 Margins The smooth barely perceptible margin of a simple cyst (A) is contrasted with the irregular margins of a small invasive cancer (B) Margin irregularities may include angular edges m icrolobulation and spiculation
and sonographic fi ndings using BI-RADS is cateshygory 2 benign with routine screening recomshymended The accuracy of sonographi c identificashyti on of cysts approaches 100 provided stric t ad herence to the classical sonographic charac teri sshytics are observed 17
t
Practical use of any lexicon req uires an undershystanding of the de fin iti ons of each term An examshypJe is complicated versus complex The presence of homogeneous low-level internal echoes throug holl t a cystic lesion that has all the other features of a sim ple cyst as above results in its designation as complicated 18 Many of these masses appear solid a lbeit benign and may be reported as comshyplicated cyst or probabl y ben ign solid lesion Often such lesions are incidentall y found during ul trasound examination peIiormed for other reashysons Recent studies cumulative ly evaluating 567 incidental compli cated cysts identifi ed only one 3-mm in situ ma lignancy (positive predictive value [PPY] 02)1 9-21 Based on these data short-term follow-up appears appropriate (BI-RADS category 3 probabJy ben ign) although further validation is
Fig 6 Echogenicityechotextureecho pattern The matrix of a mass may be homogeneous or heterogeneous Homogeshyneous masses may be anechoic hypoechoic or hyperechoic Cysts are typically anechoic (A) The echogenicity of hyposhyechoic and hyperechoic masses should be compared with the echogenicity of fibroglandular tissue In this example a hamartoma produces a homog eneous mass (arrows) that is hyperechoic compared with fat (B) Invasive cancer (C) is often hypoechoic both to fat and to glandular tissue (same lesion as in Fig 2B)
Fig 7 Echogenicityechotextureecho pattern Heterogeshyneous masses may be solid or complex conta ining a mixture of solid and cystic components The invasive cancer in A is predominantly hypoechoic but contains some areas of inshycreased echogenicity resulting in a heterogeneous echotexshyture Complex masses may be predominantly solid (B) or cystic (C both intracystic papillary carcinomas) and should be regarded as suspicious for cancer in the absence of clinical finding s suggesting an abscess
encouraged Interval enl argement (mammographishycall y or sonograph ical ly) or the presence of any suspicious features should prompt aspi ration and possible core biopsy if it proves solid 22
Suspicious features include an intracystic mass mural nodule thick septations or a thi ck or irregshyul ar wall When such fea tures are present the mass should be desc ribed as a complex cystic mass (Figs 7B and C) These lesions generall y requ ire aspiration or biopsy (BI-RADS category 4 susp ishycious)
When a so lid lesion is presen t careful analysis of contour margins matri x and attenuation may a llow classification of some nodules as BI-RADS category 3 probab ly benign and provide the opshyti on of short interva l follow-up at 6 months 12 months and 24 mon ths rather than biopsy5-7 As in ma mmography for a lesion to be assessed as probably benign it should have lt2 risk of malignancy 2324 As mentioned preliminary data suggest cysts with internal echoes can be so classhysified as can clusters of tin y cystic foci wi th thin intervening septatio ns compatible with apocrine metaplas ia 25
Fig 8 ShadOWingenhancement Enhancement may be seen with cysts (A) fibroadenomas (B) and high-grade inshyvasive cancers (C) Central shadowing is associated with the small invasive cancer is shown in C Refractive edge shadowing (present in A and B) is excluded from considershyation A single echogenic calcification is present in the fibroshyadenoma (8)
220
Fig 9 Effect on surrounding tissue Masses may affect surrounding breast tissues resulting in architectural distorshytion (A) Extensive distortion of breast architecture by a small scirrhous cancer is shown (8) A more subtle change is seen where a Cooper ligament is interrupted by a cancer (open arrows)
Stavros et a]5 proposed three categories of solid lesions that could be class ified as BI-RADS cateshygory 3 probably benign in the absence of any suspicious features (I) masses with intense and uniform hyperechogenicity re lative to fat (2) masses with an ellipsoid shape and thin echogenic capsule and (3) masses with two or three gentle lobulations and a thin echogenic capsu le Individshyually each of these characteristics had a negative predictive va lue for malignancy of 988 to 100905 Although accepted by some it is important to note that these results have not been validated across multiple centers Indeed one recent study26
suggests that not all readers achieve sufficiently high specificity to fo llow so lid lesions [n the draft BI-RADSUltrasound lexicon the concept of a thin echogenic capsule or pseudocapsule- has been replaced by that of a thin smooth margin analoshygous to a circumscribed mass mammographishycally Although palpable solid lesions are genershyally recommended for biopsy 2l24 it is not yet clear whether any size criterion or palpability of the lesion influences the absolute risk of malignancy
For solid masses irregularity of shape and margins dominate other features suggesting maligshynancy with a PPY of ma lignancy of 86 to 9357 such lesions are appropriately classified as BI-RADS category 4 or 5 with biopsy recomshymended Other features have lower specificity Orientation of the long axis of the mass nonparalshylel to the skin synonymously termed taller than wide5 has been associated with a 62 to 81 Ok likelihood of malignancy57 and is more common ly seen in cancers lt 1 cm in size Ylost fibroadenoshymas as well as many cancers are oriented with their long axes parallel to the skin (wider than tall) J I
Echotextureecho pattern appears to be less helpful in differentiating benign fro m malignan t sol id
MENDELSON BERG AND MERRITI
masses I as most masses will be hypoechoic to pare nchyma Acoustic attenuation (shadowing) is suspicious for malignancy but as many as 2 1 of benign les ions will show shadowing7 Similarly acoustic enhancement while common in benign lesions may be present in up to 42 of cancerss
Several typically benign lesions are included as special cases (Fig 11) This includes lymph nodes with a thin circumscribed capsule and centra l echogenic hi lum Foreign bodies are spec ial cases and include siliconomas and free extracapsu lar silicone (Fig 11)27 Description of vascu larity of the lesion is not a required standard (Fig 12) as no reliable distinction has yet been made between
30benign and malignant lesions on this basis 2 8shy
Vasc ularity is described as the same increased_ or decreased relative to surrounding parenchyma
Table I is a worki ng draft of a breast ultrasound lexicon including feature categories and descripshytors Although different in format this draft was based largely on the version developed by the Lexicon Committee of the Expert Working Group It is important to note that these recommendations awa it va lidation and are subject to modification before release of the final draft of the ACR BIRADSlltrasound Descriptors are illustrated in Figures 1 through 12 The illustrations show only a
Fig 10 Associated finding s Dilated ducts skin changes and calcifications associated with breast masses may be seen with ultrasonography and should be described when present (A) Macrocalcifications (~0 5 mm) associated with a fibroad shyenoma are shown (arrowheads) (8) Microcalcifications laquo05 mm) in an invasive ductal carcinoma are shown (arrows) (C) Microcalcifications not in a mass and particularly within a tubular dilated duct (curved arrow) are suspicious and may be seen in ductal carcinoma in situ as in this example
bull TC
0 f-
bull
bull
rJ
Ca
se
Re
vie
we
r o
_
gtC
LA
SS
IFIC
AT
ION
CA
TE
GO
RIE
S amp
TE
RM
S
DE
SC
RIP
TIO
N
Ta
ble
1
Dra
ft A
CR
BI-
RA
DS
Ult
raso
un
d L
exi
con
Cla
ssif
ica
tio
n F
orm
4-4
-01
~
Ma
sse
s
ArI
2sect
secto
ccup
ies
spac
e an
d sh
ould
be
seen
in
two
diffe
rent
pr
ojec
tions
Sha
pe
(sel
ect
one)
0O
val
Rou
nd
Irre
gula
r
ellip
tical
or
egg-
shap
ed (
ma
y in
clud
e tw
o o
r th
ree
undu
latio
lls
ie
lob
ular
)
sphe
rical
ba
ll-sh
aped
ci
rcul
ar
or g
lob
ula
r ne
ither
roun
d n
or o
val
Ori
enta
tion
B P
aral
lel
long
axi
s o
f les
ion
orie
nted
alo
ng s
kin
line
(w
ider
than
tal
l)
(sel
ect
one)
N
ot P
aral
lel
no lo
ng a
xis
or
axis
no
t orie
nted
alo
ng s
kin
line
(ta
ller t
han
wid
e)
Mar
gin
C
ircu
msc
ribe
d (s
elec
t al
l tha
t ap
ply)
Y
ES
(d
yes
che
ck o
ne o
ptio
n be
lOW
)0 8
No
perc
eptib
le r
im o
r th
in r
im
Thi
ck r
im
NO
(if
no
go
to i
rreg
ular
)0
IRR
EG
ULA
R (
sele
ct a
ll th
at
appl
y)
0 In
dist
inct
A
ng
ula
r M
icro
lobu
late
d S
picu
late
d ~
Ech
o P
atte
m
A
nech
oic
Hyp
erec
hoic
C
ompl
ex
Hyp
oech
oic
~ (s
elec
t on
e)
Po
ste
ri or
Aco
ustic
N
o po
ster
ior
acou
stic
fea
ture
s F
eatu
res
Enh
ance
men
t S
hado
win
g C
om
bin
ed p
atte
rn
~ S
urro
undi
ng T
issu
e 0
No
effe
ct
BIden
tifia
ble
effe
ct (
sele
ct a
ll th
at a
pp
ly)
Duc
ts
Coo
pers
liga
men
t ch
an
ge
s
0E
dem
a A
rchi
tect
ural
dis
tort
ion
Ski
n T
hick
enin
g
B S
kin
retr
actio
nflr
regu
lari
ty
Pec
tora
l m
uscl
e se
en
bu
t pl
ane
with
an
teri
or
tissu
e is
un
cle
ar
Sm
ooth
dis
tinct
mar
gin
with
thi
n t
hick
or
no p
erce
ptib
le li
near
rim
circ
umsc
ribe
d m
argi
n w
ithin
lin
ear
rim
circ
umsc
ribe
d m
argi
n w
me
asu
rab
le th
ick
rim gt
1 m
m b
etw
een
lesi
on a
nd s
urro
undi
ng t
issu
e
mar
gins
dem
onst
ratin
g a
com
bina
tion
of f
eatu
res
incl
udin
g at
leas
t 1
of t
hose
list
ed b
elow
poor
ly d
efin
ed m
argi
n pa
rt o
r al
l of t
he m
argi
n fo
rmed
by
shar
p lin
ear
inte
rsec
tions
that
form
acu
te a
ngle
s m
argi
n ch
arac
teri
zed
by b
y gt
3 sm
all
sho
rt c
ycle
und
ulat
ions
m
argi
n ch
arac
teri
zed
by
shar
p pr
ojec
ting
lines
with
out
inte
mal
ech
oe
s de
fined
rel
ativ
e to
fat
eq
ua
l to
fibro
glan
dula
r tis
sue
com
bine
d cy
stic
(an
echo
ic)
and
ech
og
en
ic c
om
po
ne
nts
de
fined
rel
ativ
e to
fib
rogl
andu
lar
tissu
e i
soec
hoic
or
hyp
oe
cho
ic to
fat
con
tain
s lo
w-l
evel
ecl
hoes
th
roug
hout
(eg
co
mpl
icat
ed c
yst o
r fib
road
enom
a)
no p
oste
rior
sha
dow
ing
or e
nh
an
cem
en
t in
crea
sed
post
erio
r ec
hoes
de
crea
sed
post
erio
r ec
hoes
ex
clud
ing
edge
sh
ad
ow
s bo
th s
hado
win
g an
d e
nh
an
cem
en
t
surr
ound
ing
tissu
e un
affe
cted
by
lesi
on
abno
rmal
cal
iber
an
do
r arb
oriz
atio
n st
raig
hten
ing
or th
icke
ning
of C
oope
rs li
gam
ents
(cu
rvili
near
co
nn
ect
ive
tissu
e b
an
ds
prov
idin
g su
ppor
t fo
r th
e br
east
s)
incr
ease
d ec
hoge
nici
ty o
f sur
roun
ding
tis
sue
ret
icul
atio
n i
nclu
des
an
gu
lar
hyp
oe
cho
ic li
nes
disr
uptio
n o
f nor
mal
ana
tom
ic p
lane
s fo
cald
iffus
e sk
in t
hick
enin
g-no
rmal
ski
n is
gt2
mm
in t
hick
ness
exc
ept i
n th
e pe
riar
eola
r ar
ea
and
low
er b
reas
ts
skin
sur
face
is c
onca
ve o
r iII
-def
ined
ap
pear
s pu
lled
in
diso
rder
ed e
cho
pa
tte
m in
volv
ing
pect
oral
mu
scle
sug
gest
ive
of i
nvas
ion
(exc
lude
tech
nica
l ca
uses
suc
h a
s im
prop
erly
pla
ced
foca
l zo
ne
) _
-shy
~ z ~ rJ o N
m
o (lJ
rJ ~ ~
c ~
rJ ampi o c z o r m
x o o z
I
I
C
LA
SS
IFIC
AT
ION
CA
TE
GO
RIE
S amp
TE
RM
S
DE
SC
RIP
TIO
N
Ca
lcif
ica
tio
ns
0 N
one
seen
C
alc
ifica
tion
s a
re p
oo
rly
cha
ract
eri
zed
with
ul
traso
und
but c
an b
e re
cogn
ized
par
ticul
arly
in a
If
pres
ent
(sel
ect a
ll th
at a
pply
) m
ass
sect Macrocalc~ications
Mic
roca
lcifi
catio
ns o
ut o
f m
ass
Mic
roca
lcifi
catio
ns in
mas
s
no c
alci
ficat
ions
see
n
~O5mm
I I I
Sp
ecia
l C
ase
s
0 N
one
Sp
eci
al
case
s ar
e th
ose
with
a u
niq
ue
dia
gn
osi
s (s
elec
t all
that
app
ly)
or
find
ing
~ Mas
s in
or
on s
kin
For
eign
bod
y Ly
mph
nod
es-in
tram
amm
ary
Lym
ph n
odes
-axi
lla
I incl
udin
g se
bace
ous
or e
pide
rmal
incl
usio
n cy
st
kelo
id
etc
in
clud
ing
clip
co
il w
ire c
athe
ter
slee
ve
silic
one
etc
in
bre
ast
incl
udin
g ax
illar
y ta
il
Va
scu
lari
ty
(sel
ect o
ne)
~ Can
not a
sses
s va
scul
arity
N
one
Sam
e as
in n
orm
al t
issu
e D
ecre
ased
In
crea
sed
colo
r flo
w n
ot d
one
or in
adeq
uate
for
inte
rpre
tatio
n no
col
or fl
ow
less
than
in n
orm
al ti
ssue
m
ore
than
in n
orm
al ti
ssue
I
Th
ere
are
lim
ite
d d
ata
to
su
pp
ort
ma
na
ge
me
nt
reco
mm
en
da
tio
ns
tor
so
lid
ma
sse
s b
ase
d o
n u
ltra
so
un
d fi
nd
ing
s a
t th
is t
ime
How
ever
w
hat
wou
ld b
e yo
ur
bes
t ass
essm
ent
an
d m
an
ag
emen
t rec
omm
enda
tion
in e
ach
case
Inco
mp
lete
Asse
ssm
en
t 0
Inco
mpl
ete
addi
tiona
l eva
luat
ion
need
ed b
efor
e fin
al a
sses
smen
t
Fin
al A
sse
ssm
en
t C
ate
go
ry
Neg
ativ
e B
enig
n fin
ding
~ Pro
babl
y be
nign
S
uspi
ciou
s ab
norm
ality
H
ighl
y su
gges
tive
of m
alig
nanc
y ------------------------------shy
no le
sion
foun
d (r
outin
e fo
llow
-up)
no
mal
igna
At f
eatu
res
ex-
cyst
(ro
utin
e fo
llow
-up)
lo
w p
roba
bilit
y o
f can
cer
ex-
fibro
aden
oma
(sho
rt in
terv
al fo
llow
-up)
in
term
edia
te p
roba
bilit
y o
f can
cer
(tis
sue
sam
plin
g)
high
pro
babi
lity
of c
ance
r (t
issu
e sa
mpl
ing)
-
Fo
r e
ach
of
the
ab
ove
ca
teg
ori
es
se
lect
the
te
rm t
ha
t b
est
de
scri
be
s th
e d
om
ina
nt
lesi
on
fe
atu
re
m
Wh
ere
ver
po
ssib
le
de
fin
itio
ns
an
d d
esc
rip
tio
ns
use
d i
n B
I-R
AO
S (
Re
sto
n
VA
) fo
r m
am
mo
gra
ph
y w
ill b
e a
pp
lied
to
ult
raso
un
d
Z o
Ple
ase
ma
rk th
e b
ox
be
sid
e y
ou
r se
lect
ion
m
r (f
JC
opyr
ight
200
1 A
mer
ican
Col
lege
of R
adio
k)gy
Bas
ed o
n F
inal
Rep
ort
of E
xper
t W
orki
ng G
roup
D
evel
oped
Un
de
r Co
ntr
act
282
-97-
0016
-B
etw
een
us
Pub
lic H
eart
h S
ervi
ce O
ffic
e o
n W
omen
s H
ealth
us
De
pa
rtm
en
t o
f Hea
lth
and
Hum
an
o S
ervi
ces
an
d t
he A
me
rica
n C
olle
ge
of R
adiO
logy
z rn
m
IJ
p tgt
Z
o
m
IJ
IJ j
f
_
rr
_
(I)
j _
~
m Q~
-
-
_ ~
0 (
) o
en
en
c--
0 (l
)
shy
~
2
r
c
nC
ll
O-C
sect8sect35~
cr
7
-
r
co
-0
Q)
0 b
~
(1)
-o~
rl
-
~
pl
-
(I)r~m
lt
~
()
223 TOWARD A STANDARDIZED BREAST ULTRASOUND LEXICON
Fig 11 Special cases Skin lesions lymph nodes and foreign bodies are also demonstrable with breast ultrasonogmiddot raphy (A) A typical intramammary lymph node with an echogenic hilum is shown (arrows) (8) Extracapsular spread of silicone gel from a ruptured silicone implant usually manmiddot ifests itself as echogenic noise or a snowstorm pattern (curved arrow)
sing le view of each lesion In prac ti ce descripto rs should be based on multiple views of masses obtained in orthogonal imaging planes in accord with the ACR Standard for the Ultrasound Exa mshyination of the Breast 3 Primary descriptors of masses (shape ori entation margin and echo patshytem ) are generall y listed in order of increasing risk of malignancy top to bottom altho ugh further validation of the risk of malignancy is needed Secshyondary features associated fi ndings or effects on sUlTounding tissue are not listed in any particular order as fLll1her assessment of the risk of mali gnancy for each feature is needed In refening to Tabk 1 it is important to re-emphasize that greatest specific ity is achieved by the evaluation of multiple features of the mass rather than any single attlibute
Certain prob le ms of descrip tion nomenclashyture a nd ca tegori za tion have no t been reso lved
Fig 12 Vascularity The role of vascularity in the characmiddot terization of breast masses is not fully defined Therefore description of vascular features is optional Vascularity asmiddot sessed with color or power Doppler is described as the same increased or decreased compared with adjacent normal breast tissue Power Doppler of a high-grade carcinoma with increased vascularity (arrowheads) is shown
Fig 13 Tubular mass A complex centrally cystic mass tubular in shape with hyperechoic indistinct rim and hetermiddot ogeneous internal echoes is noted Thi s patient is on coumamiddot din and developed a hematoma in the breast Although the features suggest potential need for biopsy the combination of clinical history and imaging findings allows classification of this finding as probably benign with shortmiddotinterval followmiddotup recommended
For example ove rl ap of shape and margin ca teshygories (eg irregular) has bee n discussed in the development of both mammography and ult ra shysound lex icons Cse of the term tu bular may be appropria te as a shape (Fig 13) o r special case (eg dil a ted duct) The benign les io n apocrine metapasia l with its characterist ic m icrolobushyla ted margin bu t otherwise iden ti fi ably benig n microcys tic components (Fig 14) might be a spec ia l case be tter includ ed and desc ri bed for its uni q ue ness than analyzed by indi vi dual desc ri pshyto rs such as irregu lar micro lobu lated and comshyplex that woul d otherwise prompt ti ssue di ag noshySIS
Another dil emma is classifica tion of lesion s by
Fig 14 Apocrine metaplasia (A) Microlobulated masses with microcysts are typical of apocrine metaplasia and may rarely contain calcifications (arrow) (8) Enhancement is sometimes evident Such lesions can be considered benign or probably benign and followed 25
l
224
Table 2 BI-RADS Ultrasound Final Assessment Categories
Assessment Categories and Codes Recommendations
O-Incomplete Needs additional imaging evaluation
1-Negative Routine follow-up for age 2-Benign finding Routine follow-up for age 3-Probably benign finding Short-term follow-up
(usually in 6 mo nths) 4-Suspicious abnormality Requires tissue sampling 5-Highly suggestive of Requires tissue sampling
malignancy
their echogenicity that is_ defined relative to fat or fibroglanduar tissue Some masses notably fibroshyadenomas are similar to fat lobules in shape and echogenicity Should they be described as hyposhyechoic using fibroglandular tissue as the basis for comparison just as fat lobules are hypoechoic to fibroglandular tissue or should they be termed isoechoic to fat) Further in need of validation are the categories of thickness of circumscribed marshygins and the characterization of solid masses by their matrix homogeneity 1any fibroadenomas are heterogeneous and some carcinomas are homoshygeneous What is the predictive value of these features alone or in combination with other feashytures
FINAL ASSESSMENT
As with mammography a Br-RADS final asshysessment and recommendation should be specified (Table 2) When breast sonography is pelformed as an adjunct to mammography one final as sessment and management recommendation should be specshyified which reflects combined mammographic and sonographic findings Final assessment and man-
MENDELSON BERG AND MERRITI TOW
agement should be predicated on the basis of the II
most suspicious feature(s) present preo Radl
I SUMMARY
solie
The approach outlined above for describing and and
reporting sonographic features of breast masses I
represents only the initial step in the development repc m
of a comprehensive system to enhance the accurate I
identification reporting and analysis of sonoshygraphic abnormalities of the breast Future revishysions with validation of interobserver consistency anal
in application of these descriptors across multiple toll
I centers with feedback from potential users in the Cha breast imaging community will undoubtedly exshy M O
pand the utility of this eff0l1 I bre
AJFACKNOWLEDGMENTS I
Participating in the development of the standardshy son
ized breast lexicon were the members of the Expert Working Group to Plan and Develop Protocols for WOI
Optimization and Clinical Testing of Breast Ultrashydial
19S sound Steering Committee-Christopher R B Menitt MD Chairman Barry B Goldberg MD con
Ellen B 1endel son MD Lexicon Subcommitshy 191
tee-Ellen B 1endelson MD chair Janet K Baum MD Christopher R B Merritt MD Eva
Inc
Rubin MD ExpeI1 Working Group-Janet K Baum MD Lawrence W Bassett MD Paul L Carson_ PhD David Cosgrove MD A Pat Romshyilly 10 Barbara S Hertzberg 10 Valerie P Jackson 10 Robert R Kuske Jr MD Helmut Madjar MD PhD Jonathan Ophir PhD Steve H Parker MD Catherine W Piccoli MD Eva Rushybin MD Gordon F Schwartz MD Edward A Sickles MD and Jonathan Sunshine PhD
REFERENCES
1 Rosenberg AL Schwanz GF Feig SA et al Clinically
occult breast les ions Localization and signincanclt Radiology
162 167-170 1987
2 Bassett LW Liu TH Giuliano AE et al The prevalence
of carcinoma in palpable vs impalpable mammog raphicaJly
detected les ions AJR Am J Roentgenol 157 21-24 1991
3 ACR Standard for the Pelformance of Breast Ultrasou nd
Examination ACR Standards Resto n V A American Coll ege
of Radiology 2000 pp 389-392
4 Merritt CRB The Breast Nodule in Ultrasound A Pracshy
tical Approach to Clinica l Problems (ch 52) in Bluth EI Ar2er
P Benson C et al (eds) A Prac ti ca l Approach to Clinical
Problems New York Thieme 2000
5 Stavros AT Thickman D Rapp CL et a1 Solid breast
nodules Use of sonog raphy to di stingui sh between beni g n and
malignant lesions Radiology 196 123-134 1995
6 Taylor KJW HOI Breast Sc reening Researc h (ATL) Can
complementary US reduce the number of biopsies of beni gn
breast massesry Radiology 189(P) 179 1993 (abstr suppl )
7 High defi niti on imag ing The ro le o f ultrasound in the
di agnosis of breast cancer Bothell WA Advanced Technology
Labo ratorie 1 99 ~
8 Zonderand HM Coerkamp EG Hem1ans J et al Diagshy
nosis of breast cancer Contribution of US as an adjuJlc t to
mammography Radiol ogy 21341 3-422 1999
9 Sickl es EA Filly RA Callen PW Breast cancer detecshy
ti o n wi th so nograph y a nd mammography Compariso n using
sta te-o f-the-a rt equipme nt AJR Am J Roenlgenol 140843shy
84 5 1983
10 Skaane P Sauer T Ultrasonograph y of malignant breast
neoplasms Anal ys is of cuc inomas missed as lumor Acta
Radiol 40376-382 1999
225 TOWARD A STANDARDI ZED BREAST ULTRASOUND LEXICON
II Berg W A Gilbrea th PL Whole breast ul trasound in preoperative evaluati on for multicentric and multi foca l cancer Radiology 2 1459-66 2000
12 Baker lA Kornguth Pl Soo MS et al Sonography of solid breast les ions Observer variability of les ion description and assessment AJR Am 1 Roentgenol 172 1621- 1625 1999
13 American Co llege of Radiology (ACR) Breast imag ing reponing and data system (BI-RADSlgtt) (ed 3) Res ton VA Ameri can College of Radiology 1998
14 Morris EA lliustrated breast MR lex icon Semin Roentshygenol 36XX 2001
15 Cole-Beuglet C Soriano RZ Kurtz B et al Ultrasound analysis of 104 primary breast carcinomas c1ass itied according to hi stopathologic type Radio logy 147 1 91-196 1983
16 Mendelson EB The Breast in Wilson S Rumack C Charboneau JW (eds ) Diagnost ic Ultrasound (ed 2) St Louis Mosby 1998 pp 75 1-789
17 Hilton SvW Leopold GR Ol son LK et al Real-time breast sonography Applica ti on in 300 consecuti ve patients AJR Am J Roentgenol 147479-486 1986
18 Jokich PM Monticciolo DL dler YT Breast ultrashysonography Radi ol Cl in North Am 30993-1009 1992
19 Kolb TM Lichy J Newhouse JH Occu lt cancer in women with dense breasts Detection with sc reening USshydi agnostic yield and tumor charac teri stics Rad iology 207 191 shy1991998
20 Venta LA Kim JP Pelloski CE et al Management of complex breast cysts AJR Am J Roentgenol 173 133 1-1 336 1999
21 Buchberger W DeKoek koek-Do ll P Springer P ct al Incidental findings on sonog raphy of the breast Clinical sigshy
ni fi cance and diagnostic worku p AJ R Am J Roentgenol 173 92 1-927 1999
22 Jackson VP Management of so lid breast nodul es What is the role of sonography~ Radiology 196 14- 15 1995 (editoshyrial )
23 Sick les EA Periodic mammographic fo ll ow-u p of prob shyab ly benign les ions Results in 3184 consecuti ve cases Radishyology 179463-468 1991
24 Sickles EA )onpalpable c ircumscribed nonca lcified so lid breast masses Like lihood of ma lignancy based on les ion size and age of patient Radiology J92439-442 1994
25 Warner lK Kum Jr 0 Berg WA Apocrine metaplas ia Mammographic and sonographic appearances AJ R m J Roentgenol 170 1375-1379 1998
26 Rahbar G Sie Ac Hansen Gc et a1 Benign versus malignant sol id breas t masses US different iation Radiology 2 13889-894 1999
27 Hanis KJv Ganon MA Shestak KC et al Si licone implant rupture Detect ion wi th US Radiology 18776 1-768 1993
28 Cosgrove DO Kedar RP Bamber Jc et al Breast di seases Color doppler US in differenti al diagnosis Radiology 18999-104 1993
29 VlcNic holas MM Mercer PM Miller JC et al Color Doppler sonography in the evaluation of palpable breast masses AJR m 1 Roentgenol 161 765-77 1 1993
30 Ra7a S Ballm JK Solid breast les ions Evaluation with power Doppler tS Radiology 203 164-168 1997
31 Skaane P Engedal K Anal ysis of sonographic features in the differentiation of fibroadenoma and invas ive ducta l carcino ma AJR m J Roentgenol 170 109- 1 14 1998

220
Fig 9 Effect on surrounding tissue Masses may affect surrounding breast tissues resulting in architectural distorshytion (A) Extensive distortion of breast architecture by a small scirrhous cancer is shown (8) A more subtle change is seen where a Cooper ligament is interrupted by a cancer (open arrows)
Stavros et a]5 proposed three categories of solid lesions that could be class ified as BI-RADS cateshygory 3 probably benign in the absence of any suspicious features (I) masses with intense and uniform hyperechogenicity re lative to fat (2) masses with an ellipsoid shape and thin echogenic capsule and (3) masses with two or three gentle lobulations and a thin echogenic capsu le Individshyually each of these characteristics had a negative predictive va lue for malignancy of 988 to 100905 Although accepted by some it is important to note that these results have not been validated across multiple centers Indeed one recent study26
suggests that not all readers achieve sufficiently high specificity to fo llow so lid lesions [n the draft BI-RADSUltrasound lexicon the concept of a thin echogenic capsule or pseudocapsule- has been replaced by that of a thin smooth margin analoshygous to a circumscribed mass mammographishycally Although palpable solid lesions are genershyally recommended for biopsy 2l24 it is not yet clear whether any size criterion or palpability of the lesion influences the absolute risk of malignancy
For solid masses irregularity of shape and margins dominate other features suggesting maligshynancy with a PPY of ma lignancy of 86 to 9357 such lesions are appropriately classified as BI-RADS category 4 or 5 with biopsy recomshymended Other features have lower specificity Orientation of the long axis of the mass nonparalshylel to the skin synonymously termed taller than wide5 has been associated with a 62 to 81 Ok likelihood of malignancy57 and is more common ly seen in cancers lt 1 cm in size Ylost fibroadenoshymas as well as many cancers are oriented with their long axes parallel to the skin (wider than tall) J I
Echotextureecho pattern appears to be less helpful in differentiating benign fro m malignan t sol id
MENDELSON BERG AND MERRITI
masses I as most masses will be hypoechoic to pare nchyma Acoustic attenuation (shadowing) is suspicious for malignancy but as many as 2 1 of benign les ions will show shadowing7 Similarly acoustic enhancement while common in benign lesions may be present in up to 42 of cancerss
Several typically benign lesions are included as special cases (Fig 11) This includes lymph nodes with a thin circumscribed capsule and centra l echogenic hi lum Foreign bodies are spec ial cases and include siliconomas and free extracapsu lar silicone (Fig 11)27 Description of vascu larity of the lesion is not a required standard (Fig 12) as no reliable distinction has yet been made between
30benign and malignant lesions on this basis 2 8shy
Vasc ularity is described as the same increased_ or decreased relative to surrounding parenchyma
Table I is a worki ng draft of a breast ultrasound lexicon including feature categories and descripshytors Although different in format this draft was based largely on the version developed by the Lexicon Committee of the Expert Working Group It is important to note that these recommendations awa it va lidation and are subject to modification before release of the final draft of the ACR BIRADSlltrasound Descriptors are illustrated in Figures 1 through 12 The illustrations show only a
Fig 10 Associated finding s Dilated ducts skin changes and calcifications associated with breast masses may be seen with ultrasonography and should be described when present (A) Macrocalcifications (~0 5 mm) associated with a fibroad shyenoma are shown (arrowheads) (8) Microcalcifications laquo05 mm) in an invasive ductal carcinoma are shown (arrows) (C) Microcalcifications not in a mass and particularly within a tubular dilated duct (curved arrow) are suspicious and may be seen in ductal carcinoma in situ as in this example
bull TC
0 f-
bull
bull
rJ
Ca
se
Re
vie
we
r o
_
gtC
LA
SS
IFIC
AT
ION
CA
TE
GO
RIE
S amp
TE
RM
S
DE
SC
RIP
TIO
N
Ta
ble
1
Dra
ft A
CR
BI-
RA
DS
Ult
raso
un
d L
exi
con
Cla
ssif
ica
tio
n F
orm
4-4
-01
~
Ma
sse
s
ArI
2sect
secto
ccup
ies
spac
e an
d sh
ould
be
seen
in
two
diffe
rent
pr
ojec
tions
Sha
pe
(sel
ect
one)
0O
val
Rou
nd
Irre
gula
r
ellip
tical
or
egg-
shap
ed (
ma
y in
clud
e tw
o o
r th
ree
undu
latio
lls
ie
lob
ular
)
sphe
rical
ba
ll-sh
aped
ci
rcul
ar
or g
lob
ula
r ne
ither
roun
d n
or o
val
Ori
enta
tion
B P
aral
lel
long
axi
s o
f les
ion
orie
nted
alo
ng s
kin
line
(w
ider
than
tal
l)
(sel
ect
one)
N
ot P
aral
lel
no lo
ng a
xis
or
axis
no
t orie
nted
alo
ng s
kin
line
(ta
ller t
han
wid
e)
Mar
gin
C
ircu
msc
ribe
d (s
elec
t al
l tha
t ap
ply)
Y
ES
(d
yes
che
ck o
ne o
ptio
n be
lOW
)0 8
No
perc
eptib
le r
im o
r th
in r
im
Thi
ck r
im
NO
(if
no
go
to i
rreg
ular
)0
IRR
EG
ULA
R (
sele
ct a
ll th
at
appl
y)
0 In
dist
inct
A
ng
ula
r M
icro
lobu
late
d S
picu
late
d ~
Ech
o P
atte
m
A
nech
oic
Hyp
erec
hoic
C
ompl
ex
Hyp
oech
oic
~ (s
elec
t on
e)
Po
ste
ri or
Aco
ustic
N
o po
ster
ior
acou
stic
fea
ture
s F
eatu
res
Enh
ance
men
t S
hado
win
g C
om
bin
ed p
atte
rn
~ S
urro
undi
ng T
issu
e 0
No
effe
ct
BIden
tifia
ble
effe
ct (
sele
ct a
ll th
at a
pp
ly)
Duc
ts
Coo
pers
liga
men
t ch
an
ge
s
0E
dem
a A
rchi
tect
ural
dis
tort
ion
Ski
n T
hick
enin
g
B S
kin
retr
actio
nflr
regu
lari
ty
Pec
tora
l m
uscl
e se
en
bu
t pl
ane
with
an
teri
or
tissu
e is
un
cle
ar
Sm
ooth
dis
tinct
mar
gin
with
thi
n t
hick
or
no p
erce
ptib
le li
near
rim
circ
umsc
ribe
d m
argi
n w
ithin
lin
ear
rim
circ
umsc
ribe
d m
argi
n w
me
asu
rab
le th
ick
rim gt
1 m
m b
etw
een
lesi
on a
nd s
urro
undi
ng t
issu
e
mar
gins
dem
onst
ratin
g a
com
bina
tion
of f
eatu
res
incl
udin
g at
leas
t 1
of t
hose
list
ed b
elow
poor
ly d
efin
ed m
argi
n pa
rt o
r al
l of t
he m
argi
n fo
rmed
by
shar
p lin
ear
inte
rsec
tions
that
form
acu
te a
ngle
s m
argi
n ch
arac
teri
zed
by b
y gt
3 sm
all
sho
rt c
ycle
und
ulat
ions
m
argi
n ch
arac
teri
zed
by
shar
p pr
ojec
ting
lines
with
out
inte
mal
ech
oe
s de
fined
rel
ativ
e to
fat
eq
ua
l to
fibro
glan
dula
r tis
sue
com
bine
d cy
stic
(an
echo
ic)
and
ech
og
en
ic c
om
po
ne
nts
de
fined
rel
ativ
e to
fib
rogl
andu
lar
tissu
e i
soec
hoic
or
hyp
oe
cho
ic to
fat
con
tain
s lo
w-l
evel
ecl
hoes
th
roug
hout
(eg
co
mpl
icat
ed c
yst o
r fib
road
enom
a)
no p
oste
rior
sha
dow
ing
or e
nh
an
cem
en
t in
crea
sed
post
erio
r ec
hoes
de
crea
sed
post
erio
r ec
hoes
ex
clud
ing
edge
sh
ad
ow
s bo
th s
hado
win
g an
d e
nh
an
cem
en
t
surr
ound
ing
tissu
e un
affe
cted
by
lesi
on
abno
rmal
cal
iber
an
do
r arb
oriz
atio
n st
raig
hten
ing
or th
icke
ning
of C
oope
rs li
gam
ents
(cu
rvili
near
co
nn
ect
ive
tissu
e b
an
ds
prov
idin
g su
ppor
t fo
r th
e br
east
s)
incr
ease
d ec
hoge
nici
ty o
f sur
roun
ding
tis
sue
ret
icul
atio
n i
nclu
des
an
gu
lar
hyp
oe
cho
ic li
nes
disr
uptio
n o
f nor
mal
ana
tom
ic p
lane
s fo
cald
iffus
e sk
in t
hick
enin
g-no
rmal
ski
n is
gt2
mm
in t
hick
ness
exc
ept i
n th
e pe
riar
eola
r ar
ea
and
low
er b
reas
ts
skin
sur
face
is c
onca
ve o
r iII
-def
ined
ap
pear
s pu
lled
in
diso
rder
ed e
cho
pa
tte
m in
volv
ing
pect
oral
mu
scle
sug
gest
ive
of i
nvas
ion
(exc
lude
tech
nica
l ca
uses
suc
h a
s im
prop
erly
pla
ced
foca
l zo
ne
) _
-shy
~ z ~ rJ o N
m
o (lJ
rJ ~ ~
c ~
rJ ampi o c z o r m
x o o z
I
I
C
LA
SS
IFIC
AT
ION
CA
TE
GO
RIE
S amp
TE
RM
S
DE
SC
RIP
TIO
N
Ca
lcif
ica
tio
ns
0 N
one
seen
C
alc
ifica
tion
s a
re p
oo
rly
cha
ract
eri
zed
with
ul
traso
und
but c
an b
e re
cogn
ized
par
ticul
arly
in a
If
pres
ent
(sel
ect a
ll th
at a
pply
) m
ass
sect Macrocalc~ications
Mic
roca
lcifi
catio
ns o
ut o
f m
ass
Mic
roca
lcifi
catio
ns in
mas
s
no c
alci
ficat
ions
see
n
~O5mm
I I I
Sp
ecia
l C
ase
s
0 N
one
Sp
eci
al
case
s ar
e th
ose
with
a u
niq
ue
dia
gn
osi
s (s
elec
t all
that
app
ly)
or
find
ing
~ Mas
s in
or
on s
kin
For
eign
bod
y Ly
mph
nod
es-in
tram
amm
ary
Lym
ph n
odes
-axi
lla
I incl
udin
g se
bace
ous
or e
pide
rmal
incl
usio
n cy
st
kelo
id
etc
in
clud
ing
clip
co
il w
ire c
athe
ter
slee
ve
silic
one
etc
in
bre
ast
incl
udin
g ax
illar
y ta
il
Va
scu
lari
ty
(sel
ect o
ne)
~ Can
not a
sses
s va
scul
arity
N
one
Sam
e as
in n
orm
al t
issu
e D
ecre
ased
In
crea
sed
colo
r flo
w n
ot d
one
or in
adeq
uate
for
inte
rpre
tatio
n no
col
or fl
ow
less
than
in n
orm
al ti
ssue
m
ore
than
in n
orm
al ti
ssue
I
Th
ere
are
lim
ite
d d
ata
to
su
pp
ort
ma
na
ge
me
nt
reco
mm
en
da
tio
ns
tor
so
lid
ma
sse
s b
ase
d o
n u
ltra
so
un
d fi
nd
ing
s a
t th
is t
ime
How
ever
w
hat
wou
ld b
e yo
ur
bes
t ass
essm
ent
an
d m
an
ag
emen
t rec
omm
enda
tion
in e
ach
case
Inco
mp
lete
Asse
ssm
en
t 0
Inco
mpl
ete
addi
tiona
l eva
luat
ion
need
ed b
efor
e fin
al a
sses
smen
t
Fin
al A
sse
ssm
en
t C
ate
go
ry
Neg
ativ
e B
enig
n fin
ding
~ Pro
babl
y be
nign
S
uspi
ciou
s ab
norm
ality
H
ighl
y su
gges
tive
of m
alig
nanc
y ------------------------------shy
no le
sion
foun
d (r
outin
e fo
llow
-up)
no
mal
igna
At f
eatu
res
ex-
cyst
(ro
utin
e fo
llow
-up)
lo
w p
roba
bilit
y o
f can
cer
ex-
fibro
aden
oma
(sho
rt in
terv
al fo
llow
-up)
in
term
edia
te p
roba
bilit
y o
f can
cer
(tis
sue
sam
plin
g)
high
pro
babi
lity
of c
ance
r (t
issu
e sa
mpl
ing)
-
Fo
r e
ach
of
the
ab
ove
ca
teg
ori
es
se
lect
the
te
rm t
ha
t b
est
de
scri
be
s th
e d
om
ina
nt
lesi
on
fe
atu
re
m
Wh
ere
ver
po
ssib
le
de
fin
itio
ns
an
d d
esc
rip
tio
ns
use
d i
n B
I-R
AO
S (
Re
sto
n
VA
) fo
r m
am
mo
gra
ph
y w
ill b
e a
pp
lied
to
ult
raso
un
d
Z o
Ple
ase
ma
rk th
e b
ox
be
sid
e y
ou
r se
lect
ion
m
r (f
JC
opyr
ight
200
1 A
mer
ican
Col
lege
of R
adio
k)gy
Bas
ed o
n F
inal
Rep
ort
of E
xper
t W
orki
ng G
roup
D
evel
oped
Un
de
r Co
ntr
act
282
-97-
0016
-B
etw
een
us
Pub
lic H
eart
h S
ervi
ce O
ffic
e o
n W
omen
s H
ealth
us
De
pa
rtm
en
t o
f Hea
lth
and
Hum
an
o S
ervi
ces
an
d t
he A
me
rica
n C
olle
ge
of R
adiO
logy
z rn
m
IJ
p tgt
Z
o
m
IJ
IJ j
f
_
rr
_
(I)
j _
~
m Q~
-
-
_ ~
0 (
) o
en
en
c--
0 (l
)
shy
~
2
r
c
nC
ll
O-C
sect8sect35~
cr
7
-
r
co
-0
Q)
0 b
~
(1)
-o~
rl
-
~
pl
-
(I)r~m
lt
~
()
223 TOWARD A STANDARDIZED BREAST ULTRASOUND LEXICON
Fig 11 Special cases Skin lesions lymph nodes and foreign bodies are also demonstrable with breast ultrasonogmiddot raphy (A) A typical intramammary lymph node with an echogenic hilum is shown (arrows) (8) Extracapsular spread of silicone gel from a ruptured silicone implant usually manmiddot ifests itself as echogenic noise or a snowstorm pattern (curved arrow)
sing le view of each lesion In prac ti ce descripto rs should be based on multiple views of masses obtained in orthogonal imaging planes in accord with the ACR Standard for the Ultrasound Exa mshyination of the Breast 3 Primary descriptors of masses (shape ori entation margin and echo patshytem ) are generall y listed in order of increasing risk of malignancy top to bottom altho ugh further validation of the risk of malignancy is needed Secshyondary features associated fi ndings or effects on sUlTounding tissue are not listed in any particular order as fLll1her assessment of the risk of mali gnancy for each feature is needed In refening to Tabk 1 it is important to re-emphasize that greatest specific ity is achieved by the evaluation of multiple features of the mass rather than any single attlibute
Certain prob le ms of descrip tion nomenclashyture a nd ca tegori za tion have no t been reso lved
Fig 12 Vascularity The role of vascularity in the characmiddot terization of breast masses is not fully defined Therefore description of vascular features is optional Vascularity asmiddot sessed with color or power Doppler is described as the same increased or decreased compared with adjacent normal breast tissue Power Doppler of a high-grade carcinoma with increased vascularity (arrowheads) is shown
Fig 13 Tubular mass A complex centrally cystic mass tubular in shape with hyperechoic indistinct rim and hetermiddot ogeneous internal echoes is noted Thi s patient is on coumamiddot din and developed a hematoma in the breast Although the features suggest potential need for biopsy the combination of clinical history and imaging findings allows classification of this finding as probably benign with shortmiddotinterval followmiddotup recommended
For example ove rl ap of shape and margin ca teshygories (eg irregular) has bee n discussed in the development of both mammography and ult ra shysound lex icons Cse of the term tu bular may be appropria te as a shape (Fig 13) o r special case (eg dil a ted duct) The benign les io n apocrine metapasia l with its characterist ic m icrolobushyla ted margin bu t otherwise iden ti fi ably benig n microcys tic components (Fig 14) might be a spec ia l case be tter includ ed and desc ri bed for its uni q ue ness than analyzed by indi vi dual desc ri pshyto rs such as irregu lar micro lobu lated and comshyplex that woul d otherwise prompt ti ssue di ag noshySIS
Another dil emma is classifica tion of lesion s by
Fig 14 Apocrine metaplasia (A) Microlobulated masses with microcysts are typical of apocrine metaplasia and may rarely contain calcifications (arrow) (8) Enhancement is sometimes evident Such lesions can be considered benign or probably benign and followed 25
l
224
Table 2 BI-RADS Ultrasound Final Assessment Categories
Assessment Categories and Codes Recommendations
O-Incomplete Needs additional imaging evaluation
1-Negative Routine follow-up for age 2-Benign finding Routine follow-up for age 3-Probably benign finding Short-term follow-up
(usually in 6 mo nths) 4-Suspicious abnormality Requires tissue sampling 5-Highly suggestive of Requires tissue sampling
malignancy
their echogenicity that is_ defined relative to fat or fibroglanduar tissue Some masses notably fibroshyadenomas are similar to fat lobules in shape and echogenicity Should they be described as hyposhyechoic using fibroglandular tissue as the basis for comparison just as fat lobules are hypoechoic to fibroglandular tissue or should they be termed isoechoic to fat) Further in need of validation are the categories of thickness of circumscribed marshygins and the characterization of solid masses by their matrix homogeneity 1any fibroadenomas are heterogeneous and some carcinomas are homoshygeneous What is the predictive value of these features alone or in combination with other feashytures
FINAL ASSESSMENT
As with mammography a Br-RADS final asshysessment and recommendation should be specified (Table 2) When breast sonography is pelformed as an adjunct to mammography one final as sessment and management recommendation should be specshyified which reflects combined mammographic and sonographic findings Final assessment and man-
MENDELSON BERG AND MERRITI TOW
agement should be predicated on the basis of the II
most suspicious feature(s) present preo Radl
I SUMMARY
solie
The approach outlined above for describing and and
reporting sonographic features of breast masses I
represents only the initial step in the development repc m
of a comprehensive system to enhance the accurate I
identification reporting and analysis of sonoshygraphic abnormalities of the breast Future revishysions with validation of interobserver consistency anal
in application of these descriptors across multiple toll
I centers with feedback from potential users in the Cha breast imaging community will undoubtedly exshy M O
pand the utility of this eff0l1 I bre
AJFACKNOWLEDGMENTS I
Participating in the development of the standardshy son
ized breast lexicon were the members of the Expert Working Group to Plan and Develop Protocols for WOI
Optimization and Clinical Testing of Breast Ultrashydial
19S sound Steering Committee-Christopher R B Menitt MD Chairman Barry B Goldberg MD con
Ellen B 1endel son MD Lexicon Subcommitshy 191
tee-Ellen B 1endelson MD chair Janet K Baum MD Christopher R B Merritt MD Eva
Inc
Rubin MD ExpeI1 Working Group-Janet K Baum MD Lawrence W Bassett MD Paul L Carson_ PhD David Cosgrove MD A Pat Romshyilly 10 Barbara S Hertzberg 10 Valerie P Jackson 10 Robert R Kuske Jr MD Helmut Madjar MD PhD Jonathan Ophir PhD Steve H Parker MD Catherine W Piccoli MD Eva Rushybin MD Gordon F Schwartz MD Edward A Sickles MD and Jonathan Sunshine PhD
REFERENCES
1 Rosenberg AL Schwanz GF Feig SA et al Clinically
occult breast les ions Localization and signincanclt Radiology
162 167-170 1987
2 Bassett LW Liu TH Giuliano AE et al The prevalence
of carcinoma in palpable vs impalpable mammog raphicaJly
detected les ions AJR Am J Roentgenol 157 21-24 1991
3 ACR Standard for the Pelformance of Breast Ultrasou nd
Examination ACR Standards Resto n V A American Coll ege
of Radiology 2000 pp 389-392
4 Merritt CRB The Breast Nodule in Ultrasound A Pracshy
tical Approach to Clinica l Problems (ch 52) in Bluth EI Ar2er
P Benson C et al (eds) A Prac ti ca l Approach to Clinical
Problems New York Thieme 2000
5 Stavros AT Thickman D Rapp CL et a1 Solid breast
nodules Use of sonog raphy to di stingui sh between beni g n and
malignant lesions Radiology 196 123-134 1995
6 Taylor KJW HOI Breast Sc reening Researc h (ATL) Can
complementary US reduce the number of biopsies of beni gn
breast massesry Radiology 189(P) 179 1993 (abstr suppl )
7 High defi niti on imag ing The ro le o f ultrasound in the
di agnosis of breast cancer Bothell WA Advanced Technology
Labo ratorie 1 99 ~
8 Zonderand HM Coerkamp EG Hem1ans J et al Diagshy
nosis of breast cancer Contribution of US as an adjuJlc t to
mammography Radiol ogy 21341 3-422 1999
9 Sickl es EA Filly RA Callen PW Breast cancer detecshy
ti o n wi th so nograph y a nd mammography Compariso n using
sta te-o f-the-a rt equipme nt AJR Am J Roenlgenol 140843shy
84 5 1983
10 Skaane P Sauer T Ultrasonograph y of malignant breast
neoplasms Anal ys is of cuc inomas missed as lumor Acta
Radiol 40376-382 1999
225 TOWARD A STANDARDI ZED BREAST ULTRASOUND LEXICON
II Berg W A Gilbrea th PL Whole breast ul trasound in preoperative evaluati on for multicentric and multi foca l cancer Radiology 2 1459-66 2000
12 Baker lA Kornguth Pl Soo MS et al Sonography of solid breast les ions Observer variability of les ion description and assessment AJR Am 1 Roentgenol 172 1621- 1625 1999
13 American Co llege of Radiology (ACR) Breast imag ing reponing and data system (BI-RADSlgtt) (ed 3) Res ton VA Ameri can College of Radiology 1998
14 Morris EA lliustrated breast MR lex icon Semin Roentshygenol 36XX 2001
15 Cole-Beuglet C Soriano RZ Kurtz B et al Ultrasound analysis of 104 primary breast carcinomas c1ass itied according to hi stopathologic type Radio logy 147 1 91-196 1983
16 Mendelson EB The Breast in Wilson S Rumack C Charboneau JW (eds ) Diagnost ic Ultrasound (ed 2) St Louis Mosby 1998 pp 75 1-789
17 Hilton SvW Leopold GR Ol son LK et al Real-time breast sonography Applica ti on in 300 consecuti ve patients AJR Am J Roentgenol 147479-486 1986
18 Jokich PM Monticciolo DL dler YT Breast ultrashysonography Radi ol Cl in North Am 30993-1009 1992
19 Kolb TM Lichy J Newhouse JH Occu lt cancer in women with dense breasts Detection with sc reening USshydi agnostic yield and tumor charac teri stics Rad iology 207 191 shy1991998
20 Venta LA Kim JP Pelloski CE et al Management of complex breast cysts AJR Am J Roentgenol 173 133 1-1 336 1999
21 Buchberger W DeKoek koek-Do ll P Springer P ct al Incidental findings on sonog raphy of the breast Clinical sigshy
ni fi cance and diagnostic worku p AJ R Am J Roentgenol 173 92 1-927 1999
22 Jackson VP Management of so lid breast nodul es What is the role of sonography~ Radiology 196 14- 15 1995 (editoshyrial )
23 Sick les EA Periodic mammographic fo ll ow-u p of prob shyab ly benign les ions Results in 3184 consecuti ve cases Radishyology 179463-468 1991
24 Sickles EA )onpalpable c ircumscribed nonca lcified so lid breast masses Like lihood of ma lignancy based on les ion size and age of patient Radiology J92439-442 1994
25 Warner lK Kum Jr 0 Berg WA Apocrine metaplas ia Mammographic and sonographic appearances AJ R m J Roentgenol 170 1375-1379 1998
26 Rahbar G Sie Ac Hansen Gc et a1 Benign versus malignant sol id breas t masses US different iation Radiology 2 13889-894 1999
27 Hanis KJv Ganon MA Shestak KC et al Si licone implant rupture Detect ion wi th US Radiology 18776 1-768 1993
28 Cosgrove DO Kedar RP Bamber Jc et al Breast di seases Color doppler US in differenti al diagnosis Radiology 18999-104 1993
29 VlcNic holas MM Mercer PM Miller JC et al Color Doppler sonography in the evaluation of palpable breast masses AJR m 1 Roentgenol 161 765-77 1 1993
30 Ra7a S Ballm JK Solid breast les ions Evaluation with power Doppler tS Radiology 203 164-168 1997
31 Skaane P Engedal K Anal ysis of sonographic features in the differentiation of fibroadenoma and invas ive ducta l carcino ma AJR m J Roentgenol 170 109- 1 14 1998

bull
bull
rJ
Ca
se
Re
vie
we
r o
_
gtC
LA
SS
IFIC
AT
ION
CA
TE
GO
RIE
S amp
TE
RM
S
DE
SC
RIP
TIO
N
Ta
ble
1
Dra
ft A
CR
BI-
RA
DS
Ult
raso
un
d L
exi
con
Cla
ssif
ica
tio
n F
orm
4-4
-01
~
Ma
sse
s
ArI
2sect
secto
ccup
ies
spac
e an
d sh
ould
be
seen
in
two
diffe
rent
pr
ojec
tions
Sha
pe
(sel
ect
one)
0O
val
Rou
nd
Irre
gula
r
ellip
tical
or
egg-
shap
ed (
ma
y in
clud
e tw
o o
r th
ree
undu
latio
lls
ie
lob
ular
)
sphe
rical
ba
ll-sh
aped
ci
rcul
ar
or g
lob
ula
r ne
ither
roun
d n
or o
val
Ori
enta
tion
B P
aral
lel
long
axi
s o
f les
ion
orie
nted
alo
ng s
kin
line
(w
ider
than
tal
l)
(sel
ect
one)
N
ot P
aral
lel
no lo
ng a
xis
or
axis
no
t orie
nted
alo
ng s
kin
line
(ta
ller t
han
wid
e)
Mar
gin
C
ircu
msc
ribe
d (s
elec
t al
l tha
t ap
ply)
Y
ES
(d
yes
che
ck o
ne o
ptio
n be
lOW
)0 8
No
perc
eptib
le r
im o
r th
in r
im
Thi
ck r
im
NO
(if
no
go
to i
rreg
ular
)0
IRR
EG
ULA
R (
sele
ct a
ll th
at
appl
y)
0 In
dist
inct
A
ng
ula
r M
icro
lobu
late
d S
picu
late
d ~
Ech
o P
atte
m
A
nech
oic
Hyp
erec
hoic
C
ompl
ex
Hyp
oech
oic
~ (s
elec
t on
e)
Po
ste
ri or
Aco
ustic
N
o po
ster
ior
acou
stic
fea
ture
s F
eatu
res
Enh
ance
men
t S
hado
win
g C
om
bin
ed p
atte
rn
~ S
urro
undi
ng T
issu
e 0
No
effe
ct
BIden
tifia
ble
effe
ct (
sele
ct a
ll th
at a
pp
ly)
Duc
ts
Coo
pers
liga
men
t ch
an
ge
s
0E
dem
a A
rchi
tect
ural
dis
tort
ion
Ski
n T
hick
enin
g
B S
kin
retr
actio
nflr
regu
lari
ty
Pec
tora
l m
uscl
e se
en
bu
t pl
ane
with
an
teri
or
tissu
e is
un
cle
ar
Sm
ooth
dis
tinct
mar
gin
with
thi
n t
hick
or
no p
erce
ptib
le li
near
rim
circ
umsc
ribe
d m
argi
n w
ithin
lin
ear
rim
circ
umsc
ribe
d m
argi
n w
me
asu
rab
le th
ick
rim gt
1 m
m b
etw
een
lesi
on a
nd s
urro
undi
ng t
issu
e
mar
gins
dem
onst
ratin
g a
com
bina
tion
of f
eatu
res
incl
udin
g at
leas
t 1
of t
hose
list
ed b
elow
poor
ly d
efin
ed m
argi
n pa
rt o
r al
l of t
he m
argi
n fo
rmed
by
shar
p lin
ear
inte
rsec
tions
that
form
acu
te a
ngle
s m
argi
n ch
arac
teri
zed
by b
y gt
3 sm
all
sho
rt c
ycle
und
ulat
ions
m
argi
n ch
arac
teri
zed
by
shar
p pr
ojec
ting
lines
with
out
inte
mal
ech
oe
s de
fined
rel
ativ
e to
fat
eq
ua
l to
fibro
glan
dula
r tis
sue
com
bine
d cy
stic
(an
echo
ic)
and
ech
og
en
ic c
om
po
ne
nts
de
fined
rel
ativ
e to
fib
rogl
andu
lar
tissu
e i
soec
hoic
or
hyp
oe
cho
ic to
fat
con
tain
s lo
w-l
evel
ecl
hoes
th
roug
hout
(eg
co
mpl
icat
ed c
yst o
r fib
road
enom
a)
no p
oste
rior
sha
dow
ing
or e
nh
an
cem
en
t in
crea
sed
post
erio
r ec
hoes
de
crea
sed
post
erio
r ec
hoes
ex
clud
ing
edge
sh
ad
ow
s bo
th s
hado
win
g an
d e
nh
an
cem
en
t
surr
ound
ing
tissu
e un
affe
cted
by
lesi
on
abno
rmal
cal
iber
an
do
r arb
oriz
atio
n st
raig
hten
ing
or th
icke
ning
of C
oope
rs li
gam
ents
(cu
rvili
near
co
nn
ect
ive
tissu
e b
an
ds
prov
idin
g su
ppor
t fo
r th
e br
east
s)
incr
ease
d ec
hoge
nici
ty o
f sur
roun
ding
tis
sue
ret
icul
atio
n i
nclu
des
an
gu
lar
hyp
oe
cho
ic li
nes
disr
uptio
n o
f nor
mal
ana
tom
ic p
lane
s fo
cald
iffus
e sk
in t
hick
enin
g-no
rmal
ski
n is
gt2
mm
in t
hick
ness
exc
ept i
n th
e pe
riar
eola
r ar
ea
and
low
er b
reas
ts
skin
sur
face
is c
onca
ve o
r iII
-def
ined
ap
pear
s pu
lled
in
diso
rder
ed e
cho
pa
tte
m in
volv
ing
pect
oral
mu
scle
sug
gest
ive
of i
nvas
ion
(exc
lude
tech
nica
l ca
uses
suc
h a
s im
prop
erly
pla
ced
foca
l zo
ne
) _
-shy
~ z ~ rJ o N
m
o (lJ
rJ ~ ~
c ~
rJ ampi o c z o r m
x o o z
I
I
C
LA
SS
IFIC
AT
ION
CA
TE
GO
RIE
S amp
TE
RM
S
DE
SC
RIP
TIO
N
Ca
lcif
ica
tio
ns
0 N
one
seen
C
alc
ifica
tion
s a
re p
oo
rly
cha
ract
eri
zed
with
ul
traso
und
but c
an b
e re
cogn
ized
par
ticul
arly
in a
If
pres
ent
(sel
ect a
ll th
at a
pply
) m
ass
sect Macrocalc~ications
Mic
roca
lcifi
catio
ns o
ut o
f m
ass
Mic
roca
lcifi
catio
ns in
mas
s
no c
alci
ficat
ions
see
n
~O5mm
I I I
Sp
ecia
l C
ase
s
0 N
one
Sp
eci
al
case
s ar
e th
ose
with
a u
niq
ue
dia
gn
osi
s (s
elec
t all
that
app
ly)
or
find
ing
~ Mas
s in
or
on s
kin
For
eign
bod
y Ly
mph
nod
es-in
tram
amm
ary
Lym
ph n
odes
-axi
lla
I incl
udin
g se
bace
ous
or e
pide
rmal
incl
usio
n cy
st
kelo
id
etc
in
clud
ing
clip
co
il w
ire c
athe
ter
slee
ve
silic
one
etc
in
bre
ast
incl
udin
g ax
illar
y ta
il
Va
scu
lari
ty
(sel
ect o
ne)
~ Can
not a
sses
s va
scul
arity
N
one
Sam
e as
in n
orm
al t
issu
e D
ecre
ased
In
crea
sed
colo
r flo
w n
ot d
one
or in
adeq
uate
for
inte
rpre
tatio
n no
col
or fl
ow
less
than
in n
orm
al ti
ssue
m
ore
than
in n
orm
al ti
ssue
I
Th
ere
are
lim
ite
d d
ata
to
su
pp
ort
ma
na
ge
me
nt
reco
mm
en
da
tio
ns
tor
so
lid
ma
sse
s b
ase
d o
n u
ltra
so
un
d fi
nd
ing
s a
t th
is t
ime
How
ever
w
hat
wou
ld b
e yo
ur
bes
t ass
essm
ent
an
d m
an
ag
emen
t rec
omm
enda
tion
in e
ach
case
Inco
mp
lete
Asse
ssm
en
t 0
Inco
mpl
ete
addi
tiona
l eva
luat
ion
need
ed b
efor
e fin
al a
sses
smen
t
Fin
al A
sse
ssm
en
t C
ate
go
ry
Neg
ativ
e B
enig
n fin
ding
~ Pro
babl
y be
nign
S
uspi
ciou
s ab
norm
ality
H
ighl
y su
gges
tive
of m
alig
nanc
y ------------------------------shy
no le
sion
foun
d (r
outin
e fo
llow
-up)
no
mal
igna
At f
eatu
res
ex-
cyst
(ro
utin
e fo
llow
-up)
lo
w p
roba
bilit
y o
f can
cer
ex-
fibro
aden
oma
(sho
rt in
terv
al fo
llow
-up)
in
term
edia
te p
roba
bilit
y o
f can
cer
(tis
sue
sam
plin
g)
high
pro
babi
lity
of c
ance
r (t
issu
e sa
mpl
ing)
-
Fo
r e
ach
of
the
ab
ove
ca
teg
ori
es
se
lect
the
te
rm t
ha
t b
est
de
scri
be
s th
e d
om
ina
nt
lesi
on
fe
atu
re
m
Wh
ere
ver
po
ssib
le
de
fin
itio
ns
an
d d
esc
rip
tio
ns
use
d i
n B
I-R
AO
S (
Re
sto
n
VA
) fo
r m
am
mo
gra
ph
y w
ill b
e a
pp
lied
to
ult
raso
un
d
Z o
Ple
ase
ma
rk th
e b
ox
be
sid
e y
ou
r se
lect
ion
m
r (f
JC
opyr
ight
200
1 A
mer
ican
Col
lege
of R
adio
k)gy
Bas
ed o
n F
inal
Rep
ort
of E
xper
t W
orki
ng G
roup
D
evel
oped
Un
de
r Co
ntr
act
282
-97-
0016
-B
etw
een
us
Pub
lic H
eart
h S
ervi
ce O
ffic
e o
n W
omen
s H
ealth
us
De
pa
rtm
en
t o
f Hea
lth
and
Hum
an
o S
ervi
ces
an
d t
he A
me
rica
n C
olle
ge
of R
adiO
logy
z rn
m
IJ
p tgt
Z
o
m
IJ
IJ j
f
_
rr
_
(I)
j _
~
m Q~
-
-
_ ~
0 (
) o
en
en
c--
0 (l
)
shy
~
2
r
c
nC
ll
O-C
sect8sect35~
cr
7
-
r
co
-0
Q)
0 b
~
(1)
-o~
rl
-
~
pl
-
(I)r~m
lt
~
()
223 TOWARD A STANDARDIZED BREAST ULTRASOUND LEXICON
Fig 11 Special cases Skin lesions lymph nodes and foreign bodies are also demonstrable with breast ultrasonogmiddot raphy (A) A typical intramammary lymph node with an echogenic hilum is shown (arrows) (8) Extracapsular spread of silicone gel from a ruptured silicone implant usually manmiddot ifests itself as echogenic noise or a snowstorm pattern (curved arrow)
sing le view of each lesion In prac ti ce descripto rs should be based on multiple views of masses obtained in orthogonal imaging planes in accord with the ACR Standard for the Ultrasound Exa mshyination of the Breast 3 Primary descriptors of masses (shape ori entation margin and echo patshytem ) are generall y listed in order of increasing risk of malignancy top to bottom altho ugh further validation of the risk of malignancy is needed Secshyondary features associated fi ndings or effects on sUlTounding tissue are not listed in any particular order as fLll1her assessment of the risk of mali gnancy for each feature is needed In refening to Tabk 1 it is important to re-emphasize that greatest specific ity is achieved by the evaluation of multiple features of the mass rather than any single attlibute
Certain prob le ms of descrip tion nomenclashyture a nd ca tegori za tion have no t been reso lved
Fig 12 Vascularity The role of vascularity in the characmiddot terization of breast masses is not fully defined Therefore description of vascular features is optional Vascularity asmiddot sessed with color or power Doppler is described as the same increased or decreased compared with adjacent normal breast tissue Power Doppler of a high-grade carcinoma with increased vascularity (arrowheads) is shown
Fig 13 Tubular mass A complex centrally cystic mass tubular in shape with hyperechoic indistinct rim and hetermiddot ogeneous internal echoes is noted Thi s patient is on coumamiddot din and developed a hematoma in the breast Although the features suggest potential need for biopsy the combination of clinical history and imaging findings allows classification of this finding as probably benign with shortmiddotinterval followmiddotup recommended
For example ove rl ap of shape and margin ca teshygories (eg irregular) has bee n discussed in the development of both mammography and ult ra shysound lex icons Cse of the term tu bular may be appropria te as a shape (Fig 13) o r special case (eg dil a ted duct) The benign les io n apocrine metapasia l with its characterist ic m icrolobushyla ted margin bu t otherwise iden ti fi ably benig n microcys tic components (Fig 14) might be a spec ia l case be tter includ ed and desc ri bed for its uni q ue ness than analyzed by indi vi dual desc ri pshyto rs such as irregu lar micro lobu lated and comshyplex that woul d otherwise prompt ti ssue di ag noshySIS
Another dil emma is classifica tion of lesion s by
Fig 14 Apocrine metaplasia (A) Microlobulated masses with microcysts are typical of apocrine metaplasia and may rarely contain calcifications (arrow) (8) Enhancement is sometimes evident Such lesions can be considered benign or probably benign and followed 25
l
224
Table 2 BI-RADS Ultrasound Final Assessment Categories
Assessment Categories and Codes Recommendations
O-Incomplete Needs additional imaging evaluation
1-Negative Routine follow-up for age 2-Benign finding Routine follow-up for age 3-Probably benign finding Short-term follow-up
(usually in 6 mo nths) 4-Suspicious abnormality Requires tissue sampling 5-Highly suggestive of Requires tissue sampling
malignancy
their echogenicity that is_ defined relative to fat or fibroglanduar tissue Some masses notably fibroshyadenomas are similar to fat lobules in shape and echogenicity Should they be described as hyposhyechoic using fibroglandular tissue as the basis for comparison just as fat lobules are hypoechoic to fibroglandular tissue or should they be termed isoechoic to fat) Further in need of validation are the categories of thickness of circumscribed marshygins and the characterization of solid masses by their matrix homogeneity 1any fibroadenomas are heterogeneous and some carcinomas are homoshygeneous What is the predictive value of these features alone or in combination with other feashytures
FINAL ASSESSMENT
As with mammography a Br-RADS final asshysessment and recommendation should be specified (Table 2) When breast sonography is pelformed as an adjunct to mammography one final as sessment and management recommendation should be specshyified which reflects combined mammographic and sonographic findings Final assessment and man-
MENDELSON BERG AND MERRITI TOW
agement should be predicated on the basis of the II
most suspicious feature(s) present preo Radl
I SUMMARY
solie
The approach outlined above for describing and and
reporting sonographic features of breast masses I
represents only the initial step in the development repc m
of a comprehensive system to enhance the accurate I
identification reporting and analysis of sonoshygraphic abnormalities of the breast Future revishysions with validation of interobserver consistency anal
in application of these descriptors across multiple toll
I centers with feedback from potential users in the Cha breast imaging community will undoubtedly exshy M O
pand the utility of this eff0l1 I bre
AJFACKNOWLEDGMENTS I
Participating in the development of the standardshy son
ized breast lexicon were the members of the Expert Working Group to Plan and Develop Protocols for WOI
Optimization and Clinical Testing of Breast Ultrashydial
19S sound Steering Committee-Christopher R B Menitt MD Chairman Barry B Goldberg MD con
Ellen B 1endel son MD Lexicon Subcommitshy 191
tee-Ellen B 1endelson MD chair Janet K Baum MD Christopher R B Merritt MD Eva
Inc
Rubin MD ExpeI1 Working Group-Janet K Baum MD Lawrence W Bassett MD Paul L Carson_ PhD David Cosgrove MD A Pat Romshyilly 10 Barbara S Hertzberg 10 Valerie P Jackson 10 Robert R Kuske Jr MD Helmut Madjar MD PhD Jonathan Ophir PhD Steve H Parker MD Catherine W Piccoli MD Eva Rushybin MD Gordon F Schwartz MD Edward A Sickles MD and Jonathan Sunshine PhD
REFERENCES
1 Rosenberg AL Schwanz GF Feig SA et al Clinically
occult breast les ions Localization and signincanclt Radiology
162 167-170 1987
2 Bassett LW Liu TH Giuliano AE et al The prevalence
of carcinoma in palpable vs impalpable mammog raphicaJly
detected les ions AJR Am J Roentgenol 157 21-24 1991
3 ACR Standard for the Pelformance of Breast Ultrasou nd
Examination ACR Standards Resto n V A American Coll ege
of Radiology 2000 pp 389-392
4 Merritt CRB The Breast Nodule in Ultrasound A Pracshy
tical Approach to Clinica l Problems (ch 52) in Bluth EI Ar2er
P Benson C et al (eds) A Prac ti ca l Approach to Clinical
Problems New York Thieme 2000
5 Stavros AT Thickman D Rapp CL et a1 Solid breast
nodules Use of sonog raphy to di stingui sh between beni g n and
malignant lesions Radiology 196 123-134 1995
6 Taylor KJW HOI Breast Sc reening Researc h (ATL) Can
complementary US reduce the number of biopsies of beni gn
breast massesry Radiology 189(P) 179 1993 (abstr suppl )
7 High defi niti on imag ing The ro le o f ultrasound in the
di agnosis of breast cancer Bothell WA Advanced Technology
Labo ratorie 1 99 ~
8 Zonderand HM Coerkamp EG Hem1ans J et al Diagshy
nosis of breast cancer Contribution of US as an adjuJlc t to
mammography Radiol ogy 21341 3-422 1999
9 Sickl es EA Filly RA Callen PW Breast cancer detecshy
ti o n wi th so nograph y a nd mammography Compariso n using
sta te-o f-the-a rt equipme nt AJR Am J Roenlgenol 140843shy
84 5 1983
10 Skaane P Sauer T Ultrasonograph y of malignant breast
neoplasms Anal ys is of cuc inomas missed as lumor Acta
Radiol 40376-382 1999
225 TOWARD A STANDARDI ZED BREAST ULTRASOUND LEXICON
II Berg W A Gilbrea th PL Whole breast ul trasound in preoperative evaluati on for multicentric and multi foca l cancer Radiology 2 1459-66 2000
12 Baker lA Kornguth Pl Soo MS et al Sonography of solid breast les ions Observer variability of les ion description and assessment AJR Am 1 Roentgenol 172 1621- 1625 1999
13 American Co llege of Radiology (ACR) Breast imag ing reponing and data system (BI-RADSlgtt) (ed 3) Res ton VA Ameri can College of Radiology 1998
14 Morris EA lliustrated breast MR lex icon Semin Roentshygenol 36XX 2001
15 Cole-Beuglet C Soriano RZ Kurtz B et al Ultrasound analysis of 104 primary breast carcinomas c1ass itied according to hi stopathologic type Radio logy 147 1 91-196 1983
16 Mendelson EB The Breast in Wilson S Rumack C Charboneau JW (eds ) Diagnost ic Ultrasound (ed 2) St Louis Mosby 1998 pp 75 1-789
17 Hilton SvW Leopold GR Ol son LK et al Real-time breast sonography Applica ti on in 300 consecuti ve patients AJR Am J Roentgenol 147479-486 1986
18 Jokich PM Monticciolo DL dler YT Breast ultrashysonography Radi ol Cl in North Am 30993-1009 1992
19 Kolb TM Lichy J Newhouse JH Occu lt cancer in women with dense breasts Detection with sc reening USshydi agnostic yield and tumor charac teri stics Rad iology 207 191 shy1991998
20 Venta LA Kim JP Pelloski CE et al Management of complex breast cysts AJR Am J Roentgenol 173 133 1-1 336 1999
21 Buchberger W DeKoek koek-Do ll P Springer P ct al Incidental findings on sonog raphy of the breast Clinical sigshy
ni fi cance and diagnostic worku p AJ R Am J Roentgenol 173 92 1-927 1999
22 Jackson VP Management of so lid breast nodul es What is the role of sonography~ Radiology 196 14- 15 1995 (editoshyrial )
23 Sick les EA Periodic mammographic fo ll ow-u p of prob shyab ly benign les ions Results in 3184 consecuti ve cases Radishyology 179463-468 1991
24 Sickles EA )onpalpable c ircumscribed nonca lcified so lid breast masses Like lihood of ma lignancy based on les ion size and age of patient Radiology J92439-442 1994
25 Warner lK Kum Jr 0 Berg WA Apocrine metaplas ia Mammographic and sonographic appearances AJ R m J Roentgenol 170 1375-1379 1998
26 Rahbar G Sie Ac Hansen Gc et a1 Benign versus malignant sol id breas t masses US different iation Radiology 2 13889-894 1999
27 Hanis KJv Ganon MA Shestak KC et al Si licone implant rupture Detect ion wi th US Radiology 18776 1-768 1993
28 Cosgrove DO Kedar RP Bamber Jc et al Breast di seases Color doppler US in differenti al diagnosis Radiology 18999-104 1993
29 VlcNic holas MM Mercer PM Miller JC et al Color Doppler sonography in the evaluation of palpable breast masses AJR m 1 Roentgenol 161 765-77 1 1993
30 Ra7a S Ballm JK Solid breast les ions Evaluation with power Doppler tS Radiology 203 164-168 1997
31 Skaane P Engedal K Anal ysis of sonographic features in the differentiation of fibroadenoma and invas ive ducta l carcino ma AJR m J Roentgenol 170 109- 1 14 1998

C
LA
SS
IFIC
AT
ION
CA
TE
GO
RIE
S amp
TE
RM
S
DE
SC
RIP
TIO
N
Ca
lcif
ica
tio
ns
0 N
one
seen
C
alc
ifica
tion
s a
re p
oo
rly
cha
ract
eri
zed
with
ul
traso
und
but c
an b
e re
cogn
ized
par
ticul
arly
in a
If
pres
ent
(sel
ect a
ll th
at a
pply
) m
ass
sect Macrocalc~ications
Mic
roca
lcifi
catio
ns o
ut o
f m
ass
Mic
roca
lcifi
catio
ns in
mas
s
no c
alci
ficat
ions
see
n
~O5mm
I I I
Sp
ecia
l C
ase
s
0 N
one
Sp
eci
al
case
s ar
e th
ose
with
a u
niq
ue
dia
gn
osi
s (s
elec
t all
that
app
ly)
or
find
ing
~ Mas
s in
or
on s
kin
For
eign
bod
y Ly
mph
nod
es-in
tram
amm
ary
Lym
ph n
odes
-axi
lla
I incl
udin
g se
bace
ous
or e
pide
rmal
incl
usio
n cy
st
kelo
id
etc
in
clud
ing
clip
co
il w
ire c
athe
ter
slee
ve
silic
one
etc
in
bre
ast
incl
udin
g ax
illar
y ta
il
Va
scu
lari
ty
(sel
ect o
ne)
~ Can
not a
sses
s va
scul
arity
N
one
Sam
e as
in n
orm
al t
issu
e D
ecre
ased
In
crea
sed
colo
r flo
w n
ot d
one
or in
adeq
uate
for
inte
rpre
tatio
n no
col
or fl
ow
less
than
in n
orm
al ti
ssue
m
ore
than
in n
orm
al ti
ssue
I
Th
ere
are
lim
ite
d d
ata
to
su
pp
ort
ma
na
ge
me
nt
reco
mm
en
da
tio
ns
tor
so
lid
ma
sse
s b
ase
d o
n u
ltra
so
un
d fi
nd
ing
s a
t th
is t
ime
How
ever
w
hat
wou
ld b
e yo
ur
bes
t ass
essm
ent
an
d m
an
ag
emen
t rec
omm
enda
tion
in e
ach
case
Inco
mp
lete
Asse
ssm
en
t 0
Inco
mpl
ete
addi
tiona
l eva
luat
ion
need
ed b
efor
e fin
al a
sses
smen
t
Fin
al A
sse
ssm
en
t C
ate
go
ry
Neg
ativ
e B
enig
n fin
ding
~ Pro
babl
y be
nign
S
uspi
ciou
s ab
norm
ality
H
ighl
y su
gges
tive
of m
alig
nanc
y ------------------------------shy
no le
sion
foun
d (r
outin
e fo
llow
-up)
no
mal
igna
At f
eatu
res
ex-
cyst
(ro
utin
e fo
llow
-up)
lo
w p
roba
bilit
y o
f can
cer
ex-
fibro
aden
oma
(sho
rt in
terv
al fo
llow
-up)
in
term
edia
te p
roba
bilit
y o
f can
cer
(tis
sue
sam
plin
g)
high
pro
babi
lity
of c
ance
r (t
issu
e sa
mpl
ing)
-
Fo
r e
ach
of
the
ab
ove
ca
teg
ori
es
se
lect
the
te
rm t
ha
t b
est
de
scri
be
s th
e d
om
ina
nt
lesi
on
fe
atu
re
m
Wh
ere
ver
po
ssib
le
de
fin
itio
ns
an
d d
esc
rip
tio
ns
use
d i
n B
I-R
AO
S (
Re
sto
n
VA
) fo
r m
am
mo
gra
ph
y w
ill b
e a
pp
lied
to
ult
raso
un
d
Z o
Ple
ase
ma
rk th
e b
ox
be
sid
e y
ou
r se
lect
ion
m
r (f
JC
opyr
ight
200
1 A
mer
ican
Col
lege
of R
adio
k)gy
Bas
ed o
n F
inal
Rep
ort
of E
xper
t W
orki
ng G
roup
D
evel
oped
Un
de
r Co
ntr
act
282
-97-
0016
-B
etw
een
us
Pub
lic H
eart
h S
ervi
ce O
ffic
e o
n W
omen
s H
ealth
us
De
pa
rtm
en
t o
f Hea
lth
and
Hum
an
o S
ervi
ces
an
d t
he A
me
rica
n C
olle
ge
of R
adiO
logy
z rn
m
IJ
p tgt
Z
o
m
IJ
IJ j
f
_
rr
_
(I)
j _
~
m Q~
-
-
_ ~
0 (
) o
en
en
c--
0 (l
)
shy
~
2
r
c
nC
ll
O-C
sect8sect35~
cr
7
-
r
co
-0
Q)
0 b
~
(1)
-o~
rl
-
~
pl
-
(I)r~m
lt
~
()
223 TOWARD A STANDARDIZED BREAST ULTRASOUND LEXICON
Fig 11 Special cases Skin lesions lymph nodes and foreign bodies are also demonstrable with breast ultrasonogmiddot raphy (A) A typical intramammary lymph node with an echogenic hilum is shown (arrows) (8) Extracapsular spread of silicone gel from a ruptured silicone implant usually manmiddot ifests itself as echogenic noise or a snowstorm pattern (curved arrow)
sing le view of each lesion In prac ti ce descripto rs should be based on multiple views of masses obtained in orthogonal imaging planes in accord with the ACR Standard for the Ultrasound Exa mshyination of the Breast 3 Primary descriptors of masses (shape ori entation margin and echo patshytem ) are generall y listed in order of increasing risk of malignancy top to bottom altho ugh further validation of the risk of malignancy is needed Secshyondary features associated fi ndings or effects on sUlTounding tissue are not listed in any particular order as fLll1her assessment of the risk of mali gnancy for each feature is needed In refening to Tabk 1 it is important to re-emphasize that greatest specific ity is achieved by the evaluation of multiple features of the mass rather than any single attlibute
Certain prob le ms of descrip tion nomenclashyture a nd ca tegori za tion have no t been reso lved
Fig 12 Vascularity The role of vascularity in the characmiddot terization of breast masses is not fully defined Therefore description of vascular features is optional Vascularity asmiddot sessed with color or power Doppler is described as the same increased or decreased compared with adjacent normal breast tissue Power Doppler of a high-grade carcinoma with increased vascularity (arrowheads) is shown
Fig 13 Tubular mass A complex centrally cystic mass tubular in shape with hyperechoic indistinct rim and hetermiddot ogeneous internal echoes is noted Thi s patient is on coumamiddot din and developed a hematoma in the breast Although the features suggest potential need for biopsy the combination of clinical history and imaging findings allows classification of this finding as probably benign with shortmiddotinterval followmiddotup recommended
For example ove rl ap of shape and margin ca teshygories (eg irregular) has bee n discussed in the development of both mammography and ult ra shysound lex icons Cse of the term tu bular may be appropria te as a shape (Fig 13) o r special case (eg dil a ted duct) The benign les io n apocrine metapasia l with its characterist ic m icrolobushyla ted margin bu t otherwise iden ti fi ably benig n microcys tic components (Fig 14) might be a spec ia l case be tter includ ed and desc ri bed for its uni q ue ness than analyzed by indi vi dual desc ri pshyto rs such as irregu lar micro lobu lated and comshyplex that woul d otherwise prompt ti ssue di ag noshySIS
Another dil emma is classifica tion of lesion s by
Fig 14 Apocrine metaplasia (A) Microlobulated masses with microcysts are typical of apocrine metaplasia and may rarely contain calcifications (arrow) (8) Enhancement is sometimes evident Such lesions can be considered benign or probably benign and followed 25
l
224
Table 2 BI-RADS Ultrasound Final Assessment Categories
Assessment Categories and Codes Recommendations
O-Incomplete Needs additional imaging evaluation
1-Negative Routine follow-up for age 2-Benign finding Routine follow-up for age 3-Probably benign finding Short-term follow-up
(usually in 6 mo nths) 4-Suspicious abnormality Requires tissue sampling 5-Highly suggestive of Requires tissue sampling
malignancy
their echogenicity that is_ defined relative to fat or fibroglanduar tissue Some masses notably fibroshyadenomas are similar to fat lobules in shape and echogenicity Should they be described as hyposhyechoic using fibroglandular tissue as the basis for comparison just as fat lobules are hypoechoic to fibroglandular tissue or should they be termed isoechoic to fat) Further in need of validation are the categories of thickness of circumscribed marshygins and the characterization of solid masses by their matrix homogeneity 1any fibroadenomas are heterogeneous and some carcinomas are homoshygeneous What is the predictive value of these features alone or in combination with other feashytures
FINAL ASSESSMENT
As with mammography a Br-RADS final asshysessment and recommendation should be specified (Table 2) When breast sonography is pelformed as an adjunct to mammography one final as sessment and management recommendation should be specshyified which reflects combined mammographic and sonographic findings Final assessment and man-
MENDELSON BERG AND MERRITI TOW
agement should be predicated on the basis of the II
most suspicious feature(s) present preo Radl
I SUMMARY
solie
The approach outlined above for describing and and
reporting sonographic features of breast masses I
represents only the initial step in the development repc m
of a comprehensive system to enhance the accurate I
identification reporting and analysis of sonoshygraphic abnormalities of the breast Future revishysions with validation of interobserver consistency anal
in application of these descriptors across multiple toll
I centers with feedback from potential users in the Cha breast imaging community will undoubtedly exshy M O
pand the utility of this eff0l1 I bre
AJFACKNOWLEDGMENTS I
Participating in the development of the standardshy son
ized breast lexicon were the members of the Expert Working Group to Plan and Develop Protocols for WOI
Optimization and Clinical Testing of Breast Ultrashydial
19S sound Steering Committee-Christopher R B Menitt MD Chairman Barry B Goldberg MD con
Ellen B 1endel son MD Lexicon Subcommitshy 191
tee-Ellen B 1endelson MD chair Janet K Baum MD Christopher R B Merritt MD Eva
Inc
Rubin MD ExpeI1 Working Group-Janet K Baum MD Lawrence W Bassett MD Paul L Carson_ PhD David Cosgrove MD A Pat Romshyilly 10 Barbara S Hertzberg 10 Valerie P Jackson 10 Robert R Kuske Jr MD Helmut Madjar MD PhD Jonathan Ophir PhD Steve H Parker MD Catherine W Piccoli MD Eva Rushybin MD Gordon F Schwartz MD Edward A Sickles MD and Jonathan Sunshine PhD
REFERENCES
1 Rosenberg AL Schwanz GF Feig SA et al Clinically
occult breast les ions Localization and signincanclt Radiology
162 167-170 1987
2 Bassett LW Liu TH Giuliano AE et al The prevalence
of carcinoma in palpable vs impalpable mammog raphicaJly
detected les ions AJR Am J Roentgenol 157 21-24 1991
3 ACR Standard for the Pelformance of Breast Ultrasou nd
Examination ACR Standards Resto n V A American Coll ege
of Radiology 2000 pp 389-392
4 Merritt CRB The Breast Nodule in Ultrasound A Pracshy
tical Approach to Clinica l Problems (ch 52) in Bluth EI Ar2er
P Benson C et al (eds) A Prac ti ca l Approach to Clinical
Problems New York Thieme 2000
5 Stavros AT Thickman D Rapp CL et a1 Solid breast
nodules Use of sonog raphy to di stingui sh between beni g n and
malignant lesions Radiology 196 123-134 1995
6 Taylor KJW HOI Breast Sc reening Researc h (ATL) Can
complementary US reduce the number of biopsies of beni gn
breast massesry Radiology 189(P) 179 1993 (abstr suppl )
7 High defi niti on imag ing The ro le o f ultrasound in the
di agnosis of breast cancer Bothell WA Advanced Technology
Labo ratorie 1 99 ~
8 Zonderand HM Coerkamp EG Hem1ans J et al Diagshy
nosis of breast cancer Contribution of US as an adjuJlc t to
mammography Radiol ogy 21341 3-422 1999
9 Sickl es EA Filly RA Callen PW Breast cancer detecshy
ti o n wi th so nograph y a nd mammography Compariso n using
sta te-o f-the-a rt equipme nt AJR Am J Roenlgenol 140843shy
84 5 1983
10 Skaane P Sauer T Ultrasonograph y of malignant breast
neoplasms Anal ys is of cuc inomas missed as lumor Acta
Radiol 40376-382 1999
225 TOWARD A STANDARDI ZED BREAST ULTRASOUND LEXICON
II Berg W A Gilbrea th PL Whole breast ul trasound in preoperative evaluati on for multicentric and multi foca l cancer Radiology 2 1459-66 2000
12 Baker lA Kornguth Pl Soo MS et al Sonography of solid breast les ions Observer variability of les ion description and assessment AJR Am 1 Roentgenol 172 1621- 1625 1999
13 American Co llege of Radiology (ACR) Breast imag ing reponing and data system (BI-RADSlgtt) (ed 3) Res ton VA Ameri can College of Radiology 1998
14 Morris EA lliustrated breast MR lex icon Semin Roentshygenol 36XX 2001
15 Cole-Beuglet C Soriano RZ Kurtz B et al Ultrasound analysis of 104 primary breast carcinomas c1ass itied according to hi stopathologic type Radio logy 147 1 91-196 1983
16 Mendelson EB The Breast in Wilson S Rumack C Charboneau JW (eds ) Diagnost ic Ultrasound (ed 2) St Louis Mosby 1998 pp 75 1-789
17 Hilton SvW Leopold GR Ol son LK et al Real-time breast sonography Applica ti on in 300 consecuti ve patients AJR Am J Roentgenol 147479-486 1986
18 Jokich PM Monticciolo DL dler YT Breast ultrashysonography Radi ol Cl in North Am 30993-1009 1992
19 Kolb TM Lichy J Newhouse JH Occu lt cancer in women with dense breasts Detection with sc reening USshydi agnostic yield and tumor charac teri stics Rad iology 207 191 shy1991998
20 Venta LA Kim JP Pelloski CE et al Management of complex breast cysts AJR Am J Roentgenol 173 133 1-1 336 1999
21 Buchberger W DeKoek koek-Do ll P Springer P ct al Incidental findings on sonog raphy of the breast Clinical sigshy
ni fi cance and diagnostic worku p AJ R Am J Roentgenol 173 92 1-927 1999
22 Jackson VP Management of so lid breast nodul es What is the role of sonography~ Radiology 196 14- 15 1995 (editoshyrial )
23 Sick les EA Periodic mammographic fo ll ow-u p of prob shyab ly benign les ions Results in 3184 consecuti ve cases Radishyology 179463-468 1991
24 Sickles EA )onpalpable c ircumscribed nonca lcified so lid breast masses Like lihood of ma lignancy based on les ion size and age of patient Radiology J92439-442 1994
25 Warner lK Kum Jr 0 Berg WA Apocrine metaplas ia Mammographic and sonographic appearances AJ R m J Roentgenol 170 1375-1379 1998
26 Rahbar G Sie Ac Hansen Gc et a1 Benign versus malignant sol id breas t masses US different iation Radiology 2 13889-894 1999
27 Hanis KJv Ganon MA Shestak KC et al Si licone implant rupture Detect ion wi th US Radiology 18776 1-768 1993
28 Cosgrove DO Kedar RP Bamber Jc et al Breast di seases Color doppler US in differenti al diagnosis Radiology 18999-104 1993
29 VlcNic holas MM Mercer PM Miller JC et al Color Doppler sonography in the evaluation of palpable breast masses AJR m 1 Roentgenol 161 765-77 1 1993
30 Ra7a S Ballm JK Solid breast les ions Evaluation with power Doppler tS Radiology 203 164-168 1997
31 Skaane P Engedal K Anal ysis of sonographic features in the differentiation of fibroadenoma and invas ive ducta l carcino ma AJR m J Roentgenol 170 109- 1 14 1998

223 TOWARD A STANDARDIZED BREAST ULTRASOUND LEXICON
Fig 11 Special cases Skin lesions lymph nodes and foreign bodies are also demonstrable with breast ultrasonogmiddot raphy (A) A typical intramammary lymph node with an echogenic hilum is shown (arrows) (8) Extracapsular spread of silicone gel from a ruptured silicone implant usually manmiddot ifests itself as echogenic noise or a snowstorm pattern (curved arrow)
sing le view of each lesion In prac ti ce descripto rs should be based on multiple views of masses obtained in orthogonal imaging planes in accord with the ACR Standard for the Ultrasound Exa mshyination of the Breast 3 Primary descriptors of masses (shape ori entation margin and echo patshytem ) are generall y listed in order of increasing risk of malignancy top to bottom altho ugh further validation of the risk of malignancy is needed Secshyondary features associated fi ndings or effects on sUlTounding tissue are not listed in any particular order as fLll1her assessment of the risk of mali gnancy for each feature is needed In refening to Tabk 1 it is important to re-emphasize that greatest specific ity is achieved by the evaluation of multiple features of the mass rather than any single attlibute
Certain prob le ms of descrip tion nomenclashyture a nd ca tegori za tion have no t been reso lved
Fig 12 Vascularity The role of vascularity in the characmiddot terization of breast masses is not fully defined Therefore description of vascular features is optional Vascularity asmiddot sessed with color or power Doppler is described as the same increased or decreased compared with adjacent normal breast tissue Power Doppler of a high-grade carcinoma with increased vascularity (arrowheads) is shown
Fig 13 Tubular mass A complex centrally cystic mass tubular in shape with hyperechoic indistinct rim and hetermiddot ogeneous internal echoes is noted Thi s patient is on coumamiddot din and developed a hematoma in the breast Although the features suggest potential need for biopsy the combination of clinical history and imaging findings allows classification of this finding as probably benign with shortmiddotinterval followmiddotup recommended
For example ove rl ap of shape and margin ca teshygories (eg irregular) has bee n discussed in the development of both mammography and ult ra shysound lex icons Cse of the term tu bular may be appropria te as a shape (Fig 13) o r special case (eg dil a ted duct) The benign les io n apocrine metapasia l with its characterist ic m icrolobushyla ted margin bu t otherwise iden ti fi ably benig n microcys tic components (Fig 14) might be a spec ia l case be tter includ ed and desc ri bed for its uni q ue ness than analyzed by indi vi dual desc ri pshyto rs such as irregu lar micro lobu lated and comshyplex that woul d otherwise prompt ti ssue di ag noshySIS
Another dil emma is classifica tion of lesion s by
Fig 14 Apocrine metaplasia (A) Microlobulated masses with microcysts are typical of apocrine metaplasia and may rarely contain calcifications (arrow) (8) Enhancement is sometimes evident Such lesions can be considered benign or probably benign and followed 25
l
224
Table 2 BI-RADS Ultrasound Final Assessment Categories
Assessment Categories and Codes Recommendations
O-Incomplete Needs additional imaging evaluation
1-Negative Routine follow-up for age 2-Benign finding Routine follow-up for age 3-Probably benign finding Short-term follow-up
(usually in 6 mo nths) 4-Suspicious abnormality Requires tissue sampling 5-Highly suggestive of Requires tissue sampling
malignancy
their echogenicity that is_ defined relative to fat or fibroglanduar tissue Some masses notably fibroshyadenomas are similar to fat lobules in shape and echogenicity Should they be described as hyposhyechoic using fibroglandular tissue as the basis for comparison just as fat lobules are hypoechoic to fibroglandular tissue or should they be termed isoechoic to fat) Further in need of validation are the categories of thickness of circumscribed marshygins and the characterization of solid masses by their matrix homogeneity 1any fibroadenomas are heterogeneous and some carcinomas are homoshygeneous What is the predictive value of these features alone or in combination with other feashytures
FINAL ASSESSMENT
As with mammography a Br-RADS final asshysessment and recommendation should be specified (Table 2) When breast sonography is pelformed as an adjunct to mammography one final as sessment and management recommendation should be specshyified which reflects combined mammographic and sonographic findings Final assessment and man-
MENDELSON BERG AND MERRITI TOW
agement should be predicated on the basis of the II
most suspicious feature(s) present preo Radl
I SUMMARY
solie
The approach outlined above for describing and and
reporting sonographic features of breast masses I
represents only the initial step in the development repc m
of a comprehensive system to enhance the accurate I
identification reporting and analysis of sonoshygraphic abnormalities of the breast Future revishysions with validation of interobserver consistency anal
in application of these descriptors across multiple toll
I centers with feedback from potential users in the Cha breast imaging community will undoubtedly exshy M O
pand the utility of this eff0l1 I bre
AJFACKNOWLEDGMENTS I
Participating in the development of the standardshy son
ized breast lexicon were the members of the Expert Working Group to Plan and Develop Protocols for WOI
Optimization and Clinical Testing of Breast Ultrashydial
19S sound Steering Committee-Christopher R B Menitt MD Chairman Barry B Goldberg MD con
Ellen B 1endel son MD Lexicon Subcommitshy 191
tee-Ellen B 1endelson MD chair Janet K Baum MD Christopher R B Merritt MD Eva
Inc
Rubin MD ExpeI1 Working Group-Janet K Baum MD Lawrence W Bassett MD Paul L Carson_ PhD David Cosgrove MD A Pat Romshyilly 10 Barbara S Hertzberg 10 Valerie P Jackson 10 Robert R Kuske Jr MD Helmut Madjar MD PhD Jonathan Ophir PhD Steve H Parker MD Catherine W Piccoli MD Eva Rushybin MD Gordon F Schwartz MD Edward A Sickles MD and Jonathan Sunshine PhD
REFERENCES
1 Rosenberg AL Schwanz GF Feig SA et al Clinically
occult breast les ions Localization and signincanclt Radiology
162 167-170 1987
2 Bassett LW Liu TH Giuliano AE et al The prevalence
of carcinoma in palpable vs impalpable mammog raphicaJly
detected les ions AJR Am J Roentgenol 157 21-24 1991
3 ACR Standard for the Pelformance of Breast Ultrasou nd
Examination ACR Standards Resto n V A American Coll ege
of Radiology 2000 pp 389-392
4 Merritt CRB The Breast Nodule in Ultrasound A Pracshy
tical Approach to Clinica l Problems (ch 52) in Bluth EI Ar2er
P Benson C et al (eds) A Prac ti ca l Approach to Clinical
Problems New York Thieme 2000
5 Stavros AT Thickman D Rapp CL et a1 Solid breast
nodules Use of sonog raphy to di stingui sh between beni g n and
malignant lesions Radiology 196 123-134 1995
6 Taylor KJW HOI Breast Sc reening Researc h (ATL) Can
complementary US reduce the number of biopsies of beni gn
breast massesry Radiology 189(P) 179 1993 (abstr suppl )
7 High defi niti on imag ing The ro le o f ultrasound in the
di agnosis of breast cancer Bothell WA Advanced Technology
Labo ratorie 1 99 ~
8 Zonderand HM Coerkamp EG Hem1ans J et al Diagshy
nosis of breast cancer Contribution of US as an adjuJlc t to
mammography Radiol ogy 21341 3-422 1999
9 Sickl es EA Filly RA Callen PW Breast cancer detecshy
ti o n wi th so nograph y a nd mammography Compariso n using
sta te-o f-the-a rt equipme nt AJR Am J Roenlgenol 140843shy
84 5 1983
10 Skaane P Sauer T Ultrasonograph y of malignant breast
neoplasms Anal ys is of cuc inomas missed as lumor Acta
Radiol 40376-382 1999
225 TOWARD A STANDARDI ZED BREAST ULTRASOUND LEXICON
II Berg W A Gilbrea th PL Whole breast ul trasound in preoperative evaluati on for multicentric and multi foca l cancer Radiology 2 1459-66 2000
12 Baker lA Kornguth Pl Soo MS et al Sonography of solid breast les ions Observer variability of les ion description and assessment AJR Am 1 Roentgenol 172 1621- 1625 1999
13 American Co llege of Radiology (ACR) Breast imag ing reponing and data system (BI-RADSlgtt) (ed 3) Res ton VA Ameri can College of Radiology 1998
14 Morris EA lliustrated breast MR lex icon Semin Roentshygenol 36XX 2001
15 Cole-Beuglet C Soriano RZ Kurtz B et al Ultrasound analysis of 104 primary breast carcinomas c1ass itied according to hi stopathologic type Radio logy 147 1 91-196 1983
16 Mendelson EB The Breast in Wilson S Rumack C Charboneau JW (eds ) Diagnost ic Ultrasound (ed 2) St Louis Mosby 1998 pp 75 1-789
17 Hilton SvW Leopold GR Ol son LK et al Real-time breast sonography Applica ti on in 300 consecuti ve patients AJR Am J Roentgenol 147479-486 1986
18 Jokich PM Monticciolo DL dler YT Breast ultrashysonography Radi ol Cl in North Am 30993-1009 1992
19 Kolb TM Lichy J Newhouse JH Occu lt cancer in women with dense breasts Detection with sc reening USshydi agnostic yield and tumor charac teri stics Rad iology 207 191 shy1991998
20 Venta LA Kim JP Pelloski CE et al Management of complex breast cysts AJR Am J Roentgenol 173 133 1-1 336 1999
21 Buchberger W DeKoek koek-Do ll P Springer P ct al Incidental findings on sonog raphy of the breast Clinical sigshy
ni fi cance and diagnostic worku p AJ R Am J Roentgenol 173 92 1-927 1999
22 Jackson VP Management of so lid breast nodul es What is the role of sonography~ Radiology 196 14- 15 1995 (editoshyrial )
23 Sick les EA Periodic mammographic fo ll ow-u p of prob shyab ly benign les ions Results in 3184 consecuti ve cases Radishyology 179463-468 1991
24 Sickles EA )onpalpable c ircumscribed nonca lcified so lid breast masses Like lihood of ma lignancy based on les ion size and age of patient Radiology J92439-442 1994
25 Warner lK Kum Jr 0 Berg WA Apocrine metaplas ia Mammographic and sonographic appearances AJ R m J Roentgenol 170 1375-1379 1998
26 Rahbar G Sie Ac Hansen Gc et a1 Benign versus malignant sol id breas t masses US different iation Radiology 2 13889-894 1999
27 Hanis KJv Ganon MA Shestak KC et al Si licone implant rupture Detect ion wi th US Radiology 18776 1-768 1993
28 Cosgrove DO Kedar RP Bamber Jc et al Breast di seases Color doppler US in differenti al diagnosis Radiology 18999-104 1993
29 VlcNic holas MM Mercer PM Miller JC et al Color Doppler sonography in the evaluation of palpable breast masses AJR m 1 Roentgenol 161 765-77 1 1993
30 Ra7a S Ballm JK Solid breast les ions Evaluation with power Doppler tS Radiology 203 164-168 1997
31 Skaane P Engedal K Anal ysis of sonographic features in the differentiation of fibroadenoma and invas ive ducta l carcino ma AJR m J Roentgenol 170 109- 1 14 1998

l
224
Table 2 BI-RADS Ultrasound Final Assessment Categories
Assessment Categories and Codes Recommendations
O-Incomplete Needs additional imaging evaluation
1-Negative Routine follow-up for age 2-Benign finding Routine follow-up for age 3-Probably benign finding Short-term follow-up
(usually in 6 mo nths) 4-Suspicious abnormality Requires tissue sampling 5-Highly suggestive of Requires tissue sampling
malignancy
their echogenicity that is_ defined relative to fat or fibroglanduar tissue Some masses notably fibroshyadenomas are similar to fat lobules in shape and echogenicity Should they be described as hyposhyechoic using fibroglandular tissue as the basis for comparison just as fat lobules are hypoechoic to fibroglandular tissue or should they be termed isoechoic to fat) Further in need of validation are the categories of thickness of circumscribed marshygins and the characterization of solid masses by their matrix homogeneity 1any fibroadenomas are heterogeneous and some carcinomas are homoshygeneous What is the predictive value of these features alone or in combination with other feashytures
FINAL ASSESSMENT
As with mammography a Br-RADS final asshysessment and recommendation should be specified (Table 2) When breast sonography is pelformed as an adjunct to mammography one final as sessment and management recommendation should be specshyified which reflects combined mammographic and sonographic findings Final assessment and man-
MENDELSON BERG AND MERRITI TOW
agement should be predicated on the basis of the II
most suspicious feature(s) present preo Radl
I SUMMARY
solie
The approach outlined above for describing and and
reporting sonographic features of breast masses I
represents only the initial step in the development repc m
of a comprehensive system to enhance the accurate I
identification reporting and analysis of sonoshygraphic abnormalities of the breast Future revishysions with validation of interobserver consistency anal
in application of these descriptors across multiple toll
I centers with feedback from potential users in the Cha breast imaging community will undoubtedly exshy M O
pand the utility of this eff0l1 I bre
AJFACKNOWLEDGMENTS I
Participating in the development of the standardshy son
ized breast lexicon were the members of the Expert Working Group to Plan and Develop Protocols for WOI
Optimization and Clinical Testing of Breast Ultrashydial
19S sound Steering Committee-Christopher R B Menitt MD Chairman Barry B Goldberg MD con
Ellen B 1endel son MD Lexicon Subcommitshy 191
tee-Ellen B 1endelson MD chair Janet K Baum MD Christopher R B Merritt MD Eva
Inc
Rubin MD ExpeI1 Working Group-Janet K Baum MD Lawrence W Bassett MD Paul L Carson_ PhD David Cosgrove MD A Pat Romshyilly 10 Barbara S Hertzberg 10 Valerie P Jackson 10 Robert R Kuske Jr MD Helmut Madjar MD PhD Jonathan Ophir PhD Steve H Parker MD Catherine W Piccoli MD Eva Rushybin MD Gordon F Schwartz MD Edward A Sickles MD and Jonathan Sunshine PhD
REFERENCES
1 Rosenberg AL Schwanz GF Feig SA et al Clinically
occult breast les ions Localization and signincanclt Radiology
162 167-170 1987
2 Bassett LW Liu TH Giuliano AE et al The prevalence
of carcinoma in palpable vs impalpable mammog raphicaJly
detected les ions AJR Am J Roentgenol 157 21-24 1991
3 ACR Standard for the Pelformance of Breast Ultrasou nd
Examination ACR Standards Resto n V A American Coll ege
of Radiology 2000 pp 389-392
4 Merritt CRB The Breast Nodule in Ultrasound A Pracshy
tical Approach to Clinica l Problems (ch 52) in Bluth EI Ar2er
P Benson C et al (eds) A Prac ti ca l Approach to Clinical
Problems New York Thieme 2000
5 Stavros AT Thickman D Rapp CL et a1 Solid breast
nodules Use of sonog raphy to di stingui sh between beni g n and
malignant lesions Radiology 196 123-134 1995
6 Taylor KJW HOI Breast Sc reening Researc h (ATL) Can
complementary US reduce the number of biopsies of beni gn
breast massesry Radiology 189(P) 179 1993 (abstr suppl )
7 High defi niti on imag ing The ro le o f ultrasound in the
di agnosis of breast cancer Bothell WA Advanced Technology
Labo ratorie 1 99 ~
8 Zonderand HM Coerkamp EG Hem1ans J et al Diagshy
nosis of breast cancer Contribution of US as an adjuJlc t to
mammography Radiol ogy 21341 3-422 1999
9 Sickl es EA Filly RA Callen PW Breast cancer detecshy
ti o n wi th so nograph y a nd mammography Compariso n using
sta te-o f-the-a rt equipme nt AJR Am J Roenlgenol 140843shy
84 5 1983
10 Skaane P Sauer T Ultrasonograph y of malignant breast
neoplasms Anal ys is of cuc inomas missed as lumor Acta
Radiol 40376-382 1999
225 TOWARD A STANDARDI ZED BREAST ULTRASOUND LEXICON
II Berg W A Gilbrea th PL Whole breast ul trasound in preoperative evaluati on for multicentric and multi foca l cancer Radiology 2 1459-66 2000
12 Baker lA Kornguth Pl Soo MS et al Sonography of solid breast les ions Observer variability of les ion description and assessment AJR Am 1 Roentgenol 172 1621- 1625 1999
13 American Co llege of Radiology (ACR) Breast imag ing reponing and data system (BI-RADSlgtt) (ed 3) Res ton VA Ameri can College of Radiology 1998
14 Morris EA lliustrated breast MR lex icon Semin Roentshygenol 36XX 2001
15 Cole-Beuglet C Soriano RZ Kurtz B et al Ultrasound analysis of 104 primary breast carcinomas c1ass itied according to hi stopathologic type Radio logy 147 1 91-196 1983
16 Mendelson EB The Breast in Wilson S Rumack C Charboneau JW (eds ) Diagnost ic Ultrasound (ed 2) St Louis Mosby 1998 pp 75 1-789
17 Hilton SvW Leopold GR Ol son LK et al Real-time breast sonography Applica ti on in 300 consecuti ve patients AJR Am J Roentgenol 147479-486 1986
18 Jokich PM Monticciolo DL dler YT Breast ultrashysonography Radi ol Cl in North Am 30993-1009 1992
19 Kolb TM Lichy J Newhouse JH Occu lt cancer in women with dense breasts Detection with sc reening USshydi agnostic yield and tumor charac teri stics Rad iology 207 191 shy1991998
20 Venta LA Kim JP Pelloski CE et al Management of complex breast cysts AJR Am J Roentgenol 173 133 1-1 336 1999
21 Buchberger W DeKoek koek-Do ll P Springer P ct al Incidental findings on sonog raphy of the breast Clinical sigshy
ni fi cance and diagnostic worku p AJ R Am J Roentgenol 173 92 1-927 1999
22 Jackson VP Management of so lid breast nodul es What is the role of sonography~ Radiology 196 14- 15 1995 (editoshyrial )
23 Sick les EA Periodic mammographic fo ll ow-u p of prob shyab ly benign les ions Results in 3184 consecuti ve cases Radishyology 179463-468 1991
24 Sickles EA )onpalpable c ircumscribed nonca lcified so lid breast masses Like lihood of ma lignancy based on les ion size and age of patient Radiology J92439-442 1994
25 Warner lK Kum Jr 0 Berg WA Apocrine metaplas ia Mammographic and sonographic appearances AJ R m J Roentgenol 170 1375-1379 1998
26 Rahbar G Sie Ac Hansen Gc et a1 Benign versus malignant sol id breas t masses US different iation Radiology 2 13889-894 1999
27 Hanis KJv Ganon MA Shestak KC et al Si licone implant rupture Detect ion wi th US Radiology 18776 1-768 1993
28 Cosgrove DO Kedar RP Bamber Jc et al Breast di seases Color doppler US in differenti al diagnosis Radiology 18999-104 1993
29 VlcNic holas MM Mercer PM Miller JC et al Color Doppler sonography in the evaluation of palpable breast masses AJR m 1 Roentgenol 161 765-77 1 1993
30 Ra7a S Ballm JK Solid breast les ions Evaluation with power Doppler tS Radiology 203 164-168 1997
31 Skaane P Engedal K Anal ysis of sonographic features in the differentiation of fibroadenoma and invas ive ducta l carcino ma AJR m J Roentgenol 170 109- 1 14 1998

225 TOWARD A STANDARDI ZED BREAST ULTRASOUND LEXICON
II Berg W A Gilbrea th PL Whole breast ul trasound in preoperative evaluati on for multicentric and multi foca l cancer Radiology 2 1459-66 2000
12 Baker lA Kornguth Pl Soo MS et al Sonography of solid breast les ions Observer variability of les ion description and assessment AJR Am 1 Roentgenol 172 1621- 1625 1999
13 American Co llege of Radiology (ACR) Breast imag ing reponing and data system (BI-RADSlgtt) (ed 3) Res ton VA Ameri can College of Radiology 1998
14 Morris EA lliustrated breast MR lex icon Semin Roentshygenol 36XX 2001
15 Cole-Beuglet C Soriano RZ Kurtz B et al Ultrasound analysis of 104 primary breast carcinomas c1ass itied according to hi stopathologic type Radio logy 147 1 91-196 1983
16 Mendelson EB The Breast in Wilson S Rumack C Charboneau JW (eds ) Diagnost ic Ultrasound (ed 2) St Louis Mosby 1998 pp 75 1-789
17 Hilton SvW Leopold GR Ol son LK et al Real-time breast sonography Applica ti on in 300 consecuti ve patients AJR Am J Roentgenol 147479-486 1986
18 Jokich PM Monticciolo DL dler YT Breast ultrashysonography Radi ol Cl in North Am 30993-1009 1992
19 Kolb TM Lichy J Newhouse JH Occu lt cancer in women with dense breasts Detection with sc reening USshydi agnostic yield and tumor charac teri stics Rad iology 207 191 shy1991998
20 Venta LA Kim JP Pelloski CE et al Management of complex breast cysts AJR Am J Roentgenol 173 133 1-1 336 1999
21 Buchberger W DeKoek koek-Do ll P Springer P ct al Incidental findings on sonog raphy of the breast Clinical sigshy
ni fi cance and diagnostic worku p AJ R Am J Roentgenol 173 92 1-927 1999
22 Jackson VP Management of so lid breast nodul es What is the role of sonography~ Radiology 196 14- 15 1995 (editoshyrial )
23 Sick les EA Periodic mammographic fo ll ow-u p of prob shyab ly benign les ions Results in 3184 consecuti ve cases Radishyology 179463-468 1991
24 Sickles EA )onpalpable c ircumscribed nonca lcified so lid breast masses Like lihood of ma lignancy based on les ion size and age of patient Radiology J92439-442 1994
25 Warner lK Kum Jr 0 Berg WA Apocrine metaplas ia Mammographic and sonographic appearances AJ R m J Roentgenol 170 1375-1379 1998
26 Rahbar G Sie Ac Hansen Gc et a1 Benign versus malignant sol id breas t masses US different iation Radiology 2 13889-894 1999
27 Hanis KJv Ganon MA Shestak KC et al Si licone implant rupture Detect ion wi th US Radiology 18776 1-768 1993
28 Cosgrove DO Kedar RP Bamber Jc et al Breast di seases Color doppler US in differenti al diagnosis Radiology 18999-104 1993
29 VlcNic holas MM Mercer PM Miller JC et al Color Doppler sonography in the evaluation of palpable breast masses AJR m 1 Roentgenol 161 765-77 1 1993
30 Ra7a S Ballm JK Solid breast les ions Evaluation with power Doppler tS Radiology 203 164-168 1997
31 Skaane P Engedal K Anal ysis of sonographic features in the differentiation of fibroadenoma and invas ive ducta l carcino ma AJR m J Roentgenol 170 109- 1 14 1998


![QuantifyingTumorVascularHeterogeneitywithDynamic Contrast ... · 2015. 7. 29. · ACR Breast Imaging-Reporting and Data System (BI-RADS) MRI lexicon [18]. In cancer treatment, tumor](https://img.pdfslide.net/doc/110x75/5fc9df59a8ef470c23133cae/quantifyingtumorvascularheterogeneitywithdynamic-contrast-2015-7-29-acr.jpg)