Embed Size (px)
Citation preview
Toxicity of contrast agents
N. Grenier, Bordeaux
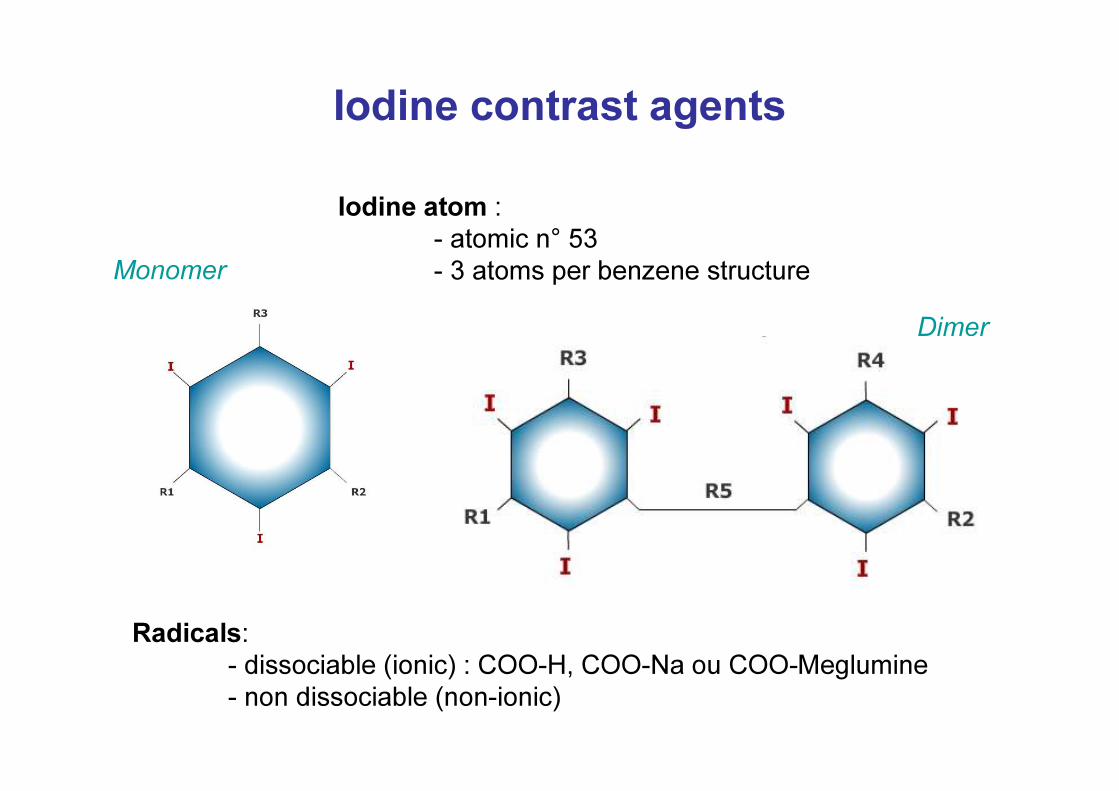
Iodine contrast agentsIodine atom :
- atomic n° 53- 3 atoms per benzene structure
Radicals: - dissociable (ionic) : COO-H, COO-Na ou COO-Meglumine- non dissociable (non-ionic)
Monomer
Dimer
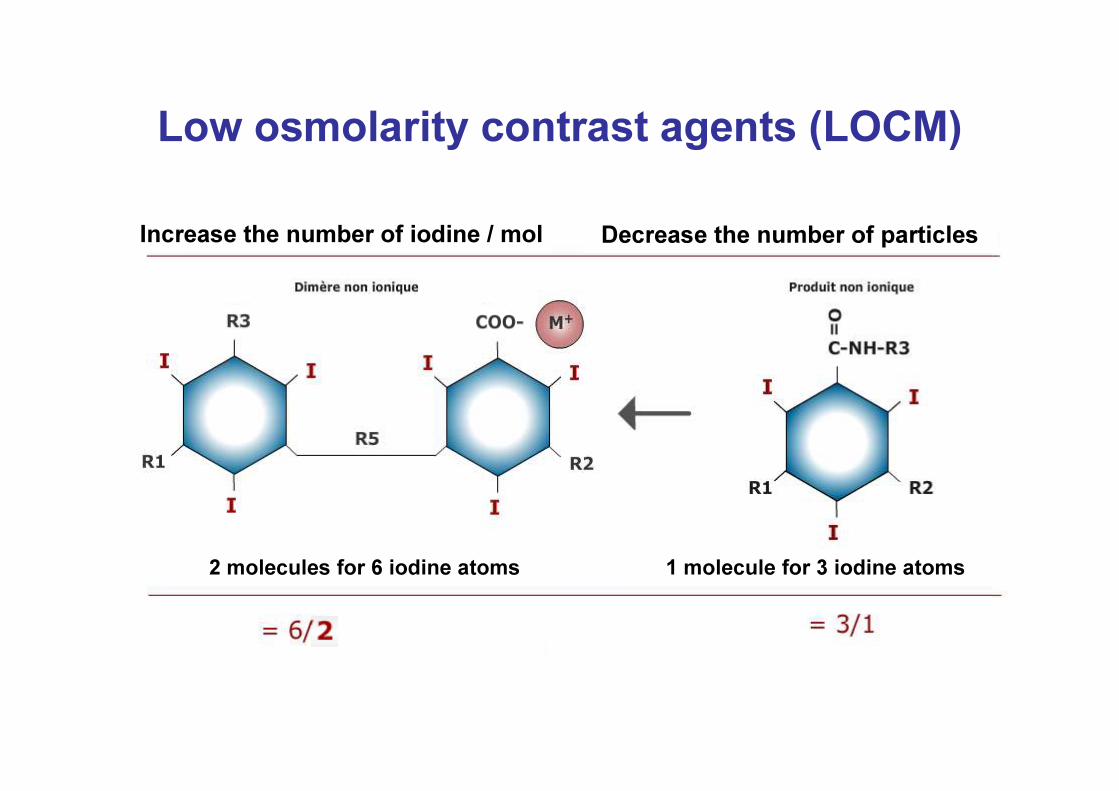
Low osmolarity contrast agents (LOCM)Increase the number of iodine / mol Decrease the number of particles
1 molecule for 3 iodine atoms2 molecules for 6 iodine atoms
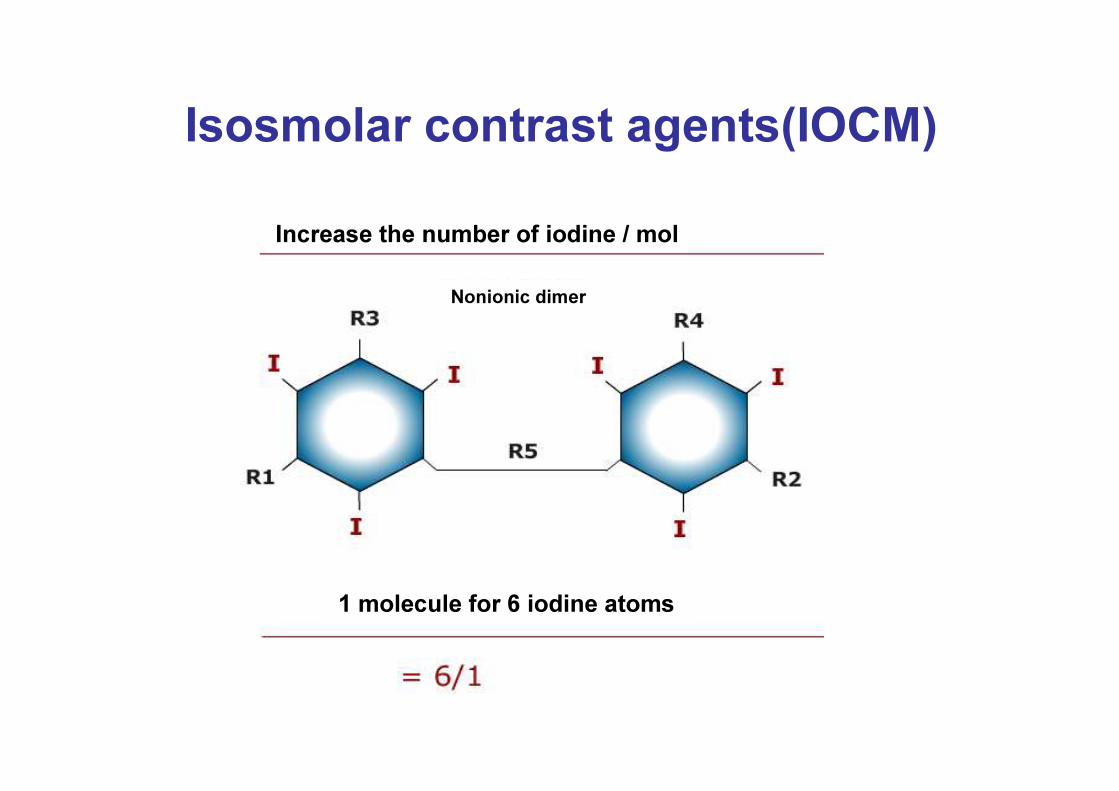
Isosmolar contrast agents(IOCM)Increase the number of iodine / mol
1 molecule for 6 iodine atoms
Nonionic dimer
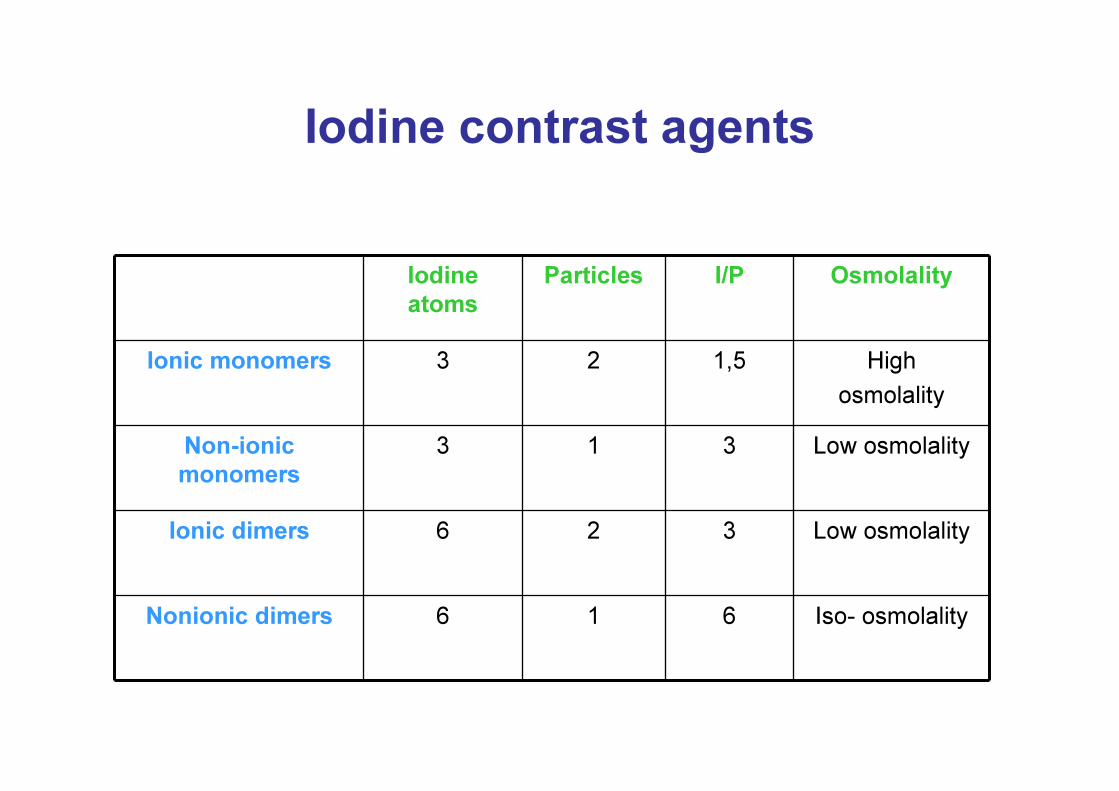
Iodine contrast agents
Iodineatoms
Particles I/P Osmolality
Ionic monomers 3 2 1,5 High osmolality
Non-ionicmonomers
3 1 3 Low osmolality
Ionic dimers 6 2 3 Low osmolality
Nonionic dimers 6 1 6 Iso- osmolality
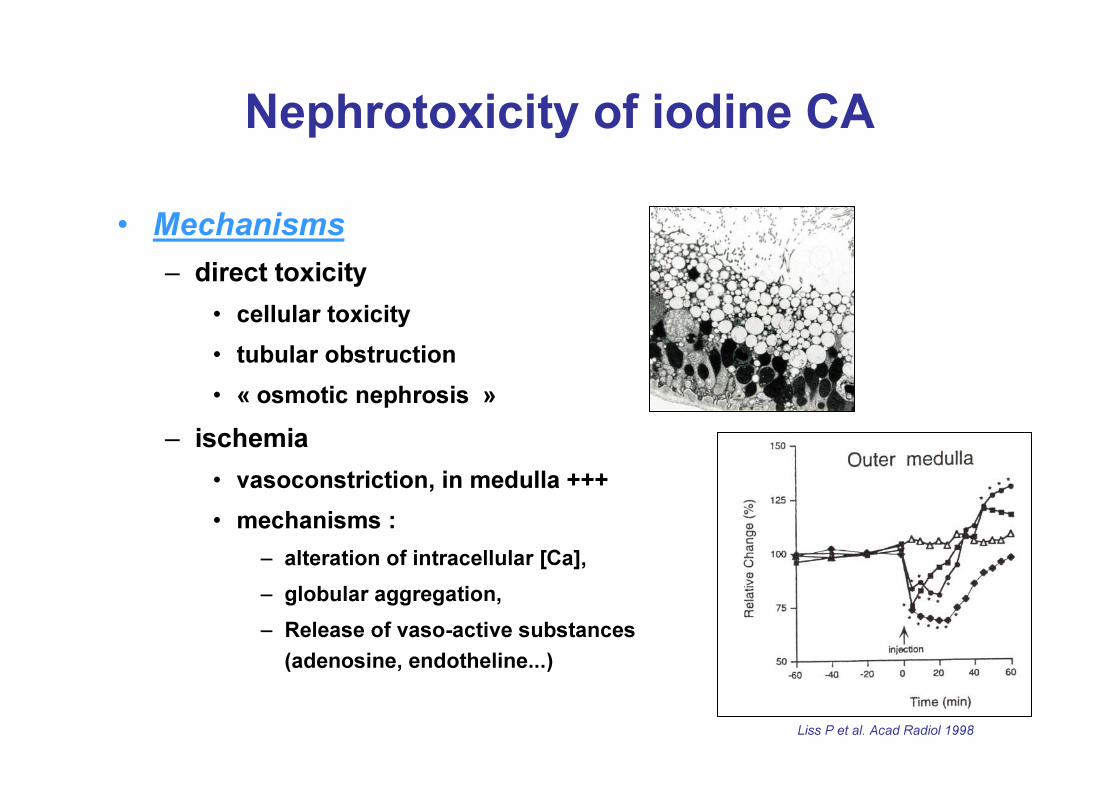
Nephrotoxicity of iodine CA• Mechanisms
– direct toxicity• cellular toxicity• tubular obstruction• « osmotic nephrosis »
– ischemia• vasoconstriction, in medulla +++• mechanisms : – alteration of intracellular [Ca], – globular aggregation, – Release of vaso-active substances
(adenosine, endotheline...)
Liss P et al. Acad Radiol 1998
Nephrotoxicity of iodine CA
• Definition :« increase of SCr within 3 days followinginjection of CA without any other cause » :- either absolute : > 44µmol/l- or relative : > 25%
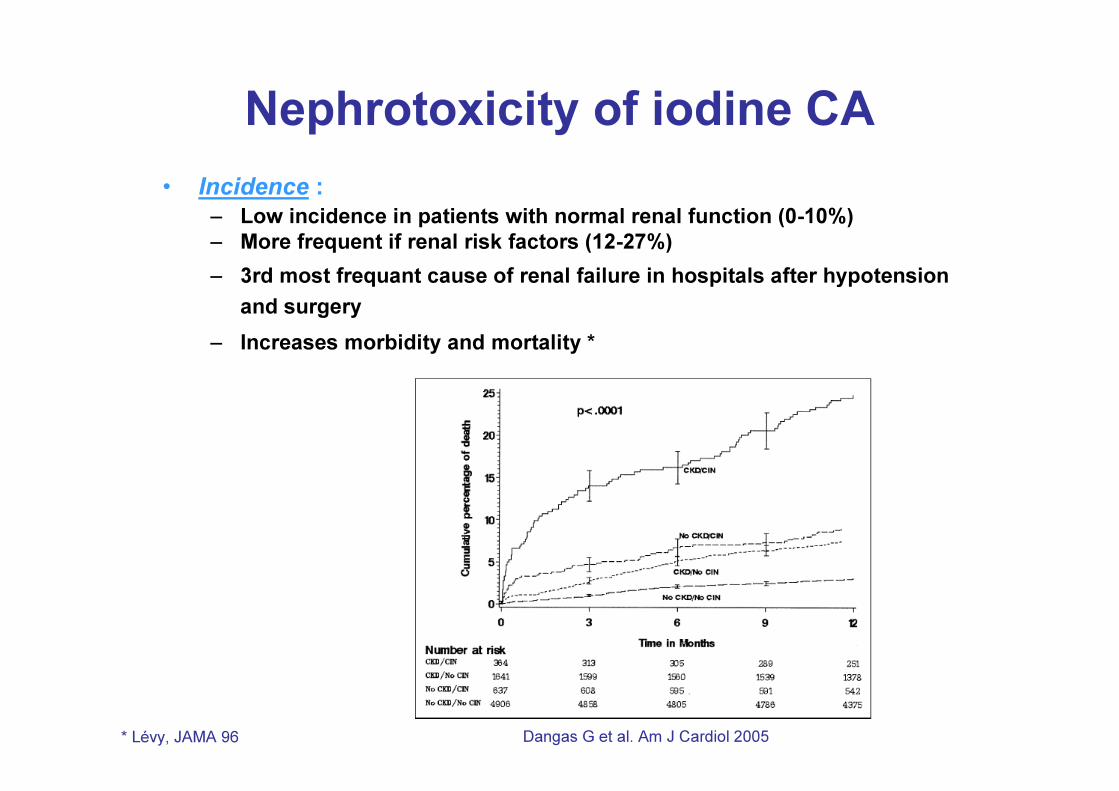
Nephrotoxicity of iodine CA• Incidence :– Low incidence in patients with normal renal function (0-10%)– More frequent if renal risk factors (12-27%)– 3rd most frequant cause of renal failure in hospitals after hypotension
and surgery– Increases morbidity and mortality *
* Lévy, JAMA 96 Dangas G et al. Am J Cardiol 2005
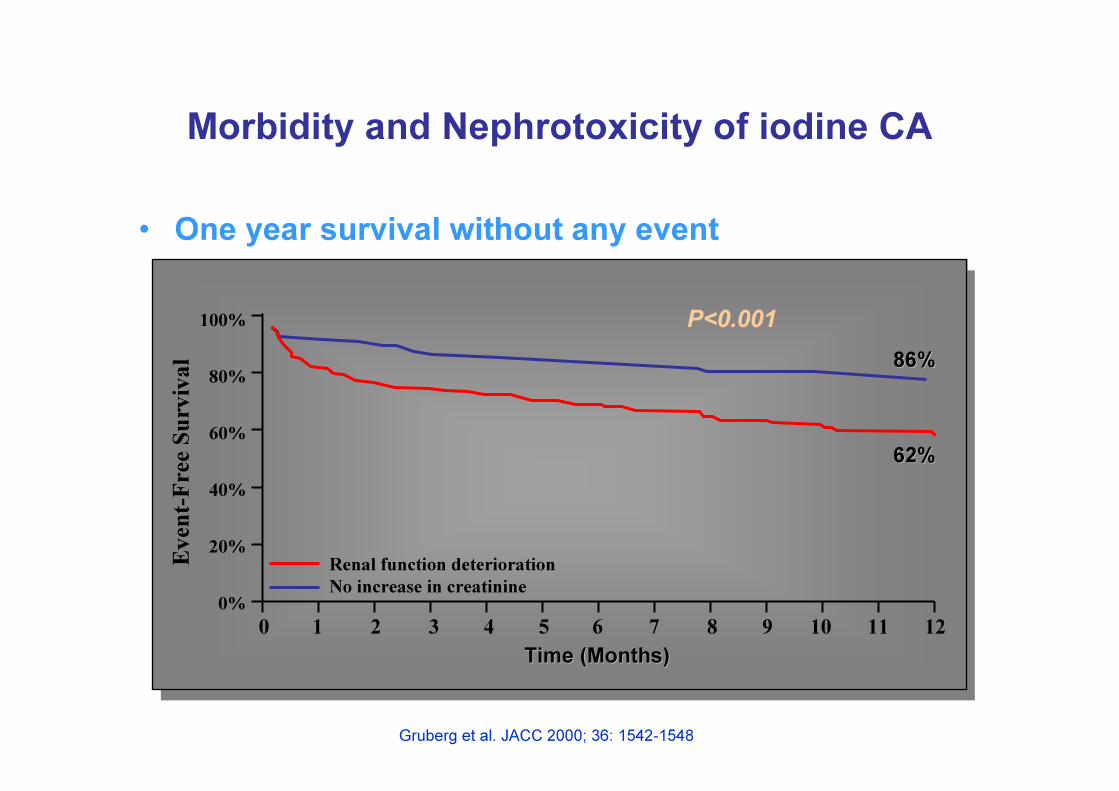
Morbidity and Nephrotoxicity of iodine CA
• One year survival without any event
00%
20%
40%
60%
80%
100%
1 2 3 4 5 6 7 8 9 10 11 12
Renal function deteriorationNo increase in creatinine
Time (Months)Time (Months)
Even
t-Fre
e Sur
viva
l 86%86%
62%62%
P<0.001
Gruberg et al. JACC 2000; 36: 1542-1548
Nephrotoxicity of iodine CA• Risk factors :
– pre-existing RF (130 µmol/l)– diabetes– Nephrotoxic drugs (Ab, NSAI +++)– dehydration– Cardiopathy with diuretics– myeloma– age > 70 years
Maximal risk : diabetes and RF +++
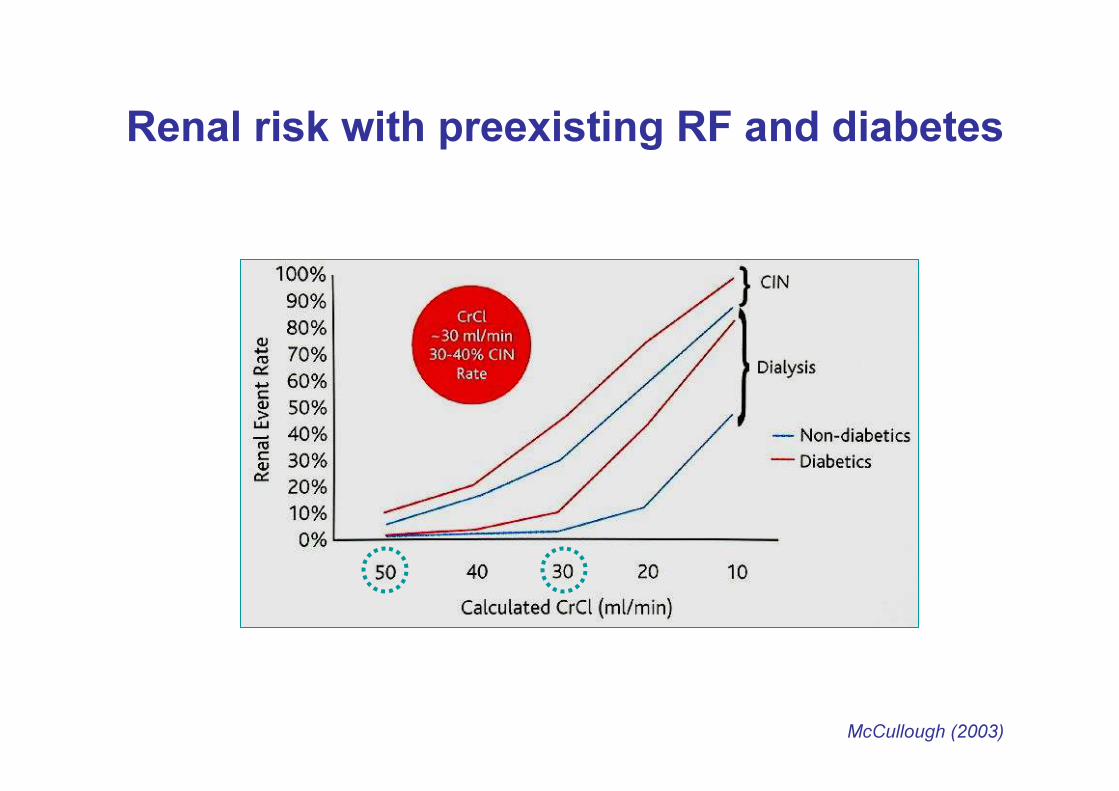
Renal risk with preexisting RF and diabetes
McCullough (2003)
Incidence of CIN• Factors of variation :
– Definition de la NCI– Type of population
• Out-patients vs in-patients• Risk factors
– Type and duration of follow-up– Hydration state– Type of CA– Doses of CA– Route of administration– …
Which incidence after IV injection?• Analysis of literature (2006) :
– Research on Medline : 3081 publications on CIN (1966-2004)
– 40 about IV injections in humans :• 9 showed no effect on renal function• 31 showed CIN
– Only 2 had a control group
– In-patients +++– No preparation
Rao QA & Newhouse JH, Radiology 2006
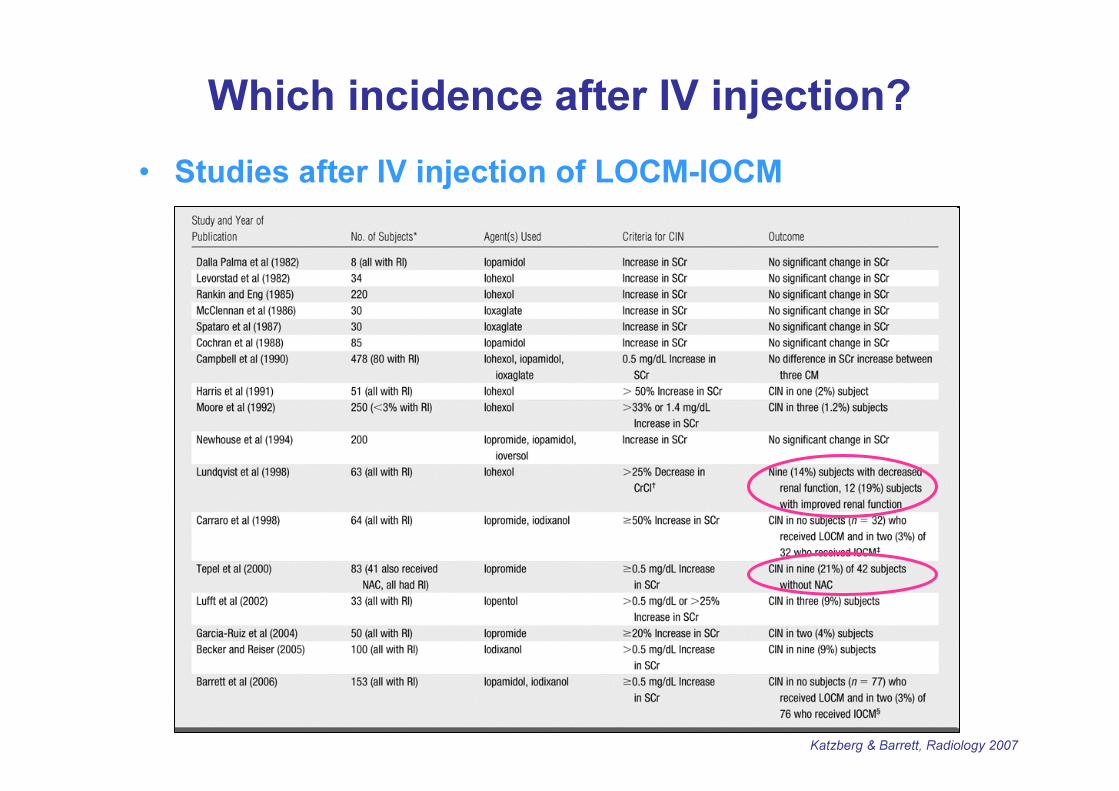
Which incidence after IV injection?• Studies after IV injection of LOCM-IOCM
Katzberg & Barrett, Radiology 2007
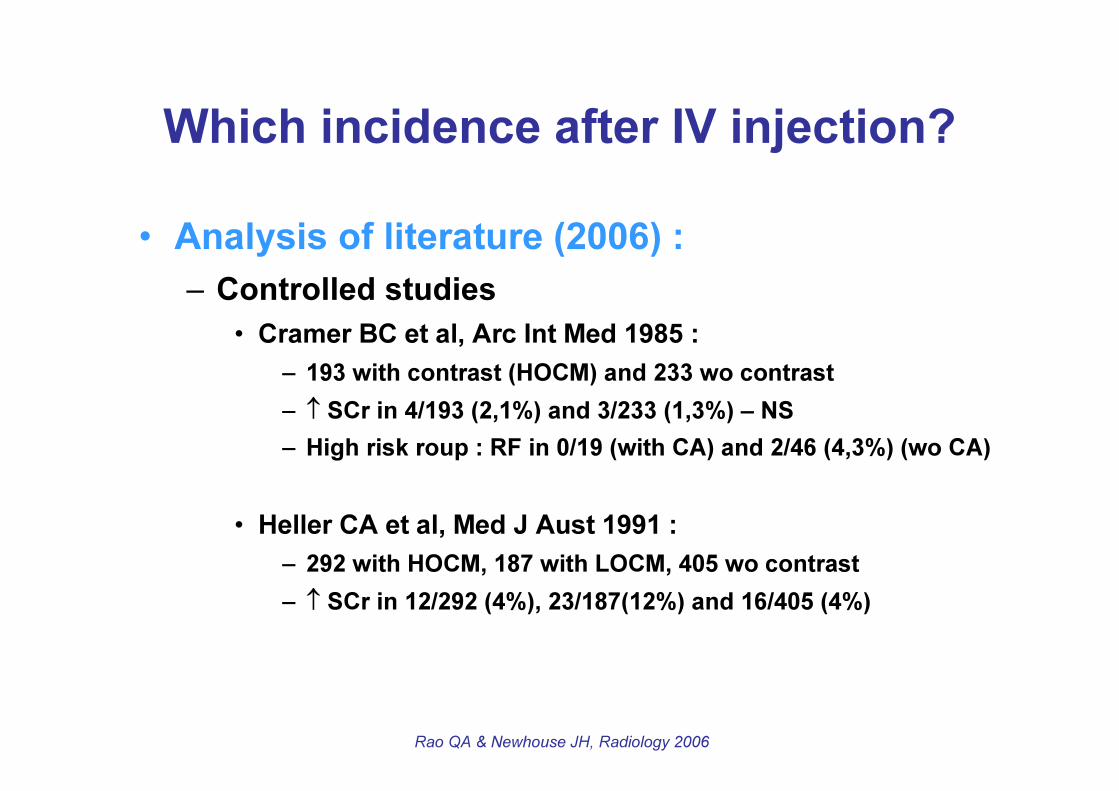
Which incidence after IV injection?• Analysis of literature (2006) :
– Controlled studies• Cramer BC et al, Arc Int Med 1985 :
– 193 with contrast (HOCM) and 233 wo contrast– ↑ SCr in 4/193 (2,1%) and 3/233 (1,3%) – NS– High risk roup : RF in 0/19 (with CA) and 2/46 (4,3%) (wo CA)
• Heller CA et al, Med J Aust 1991 :– 292 with HOCM, 187 with LOCM, 405 wo contrast– ↑ SCr in 12/292 (4%), 23/187(12%) and 16/405 (4%)
Rao QA & Newhouse JH, Radiology 2006
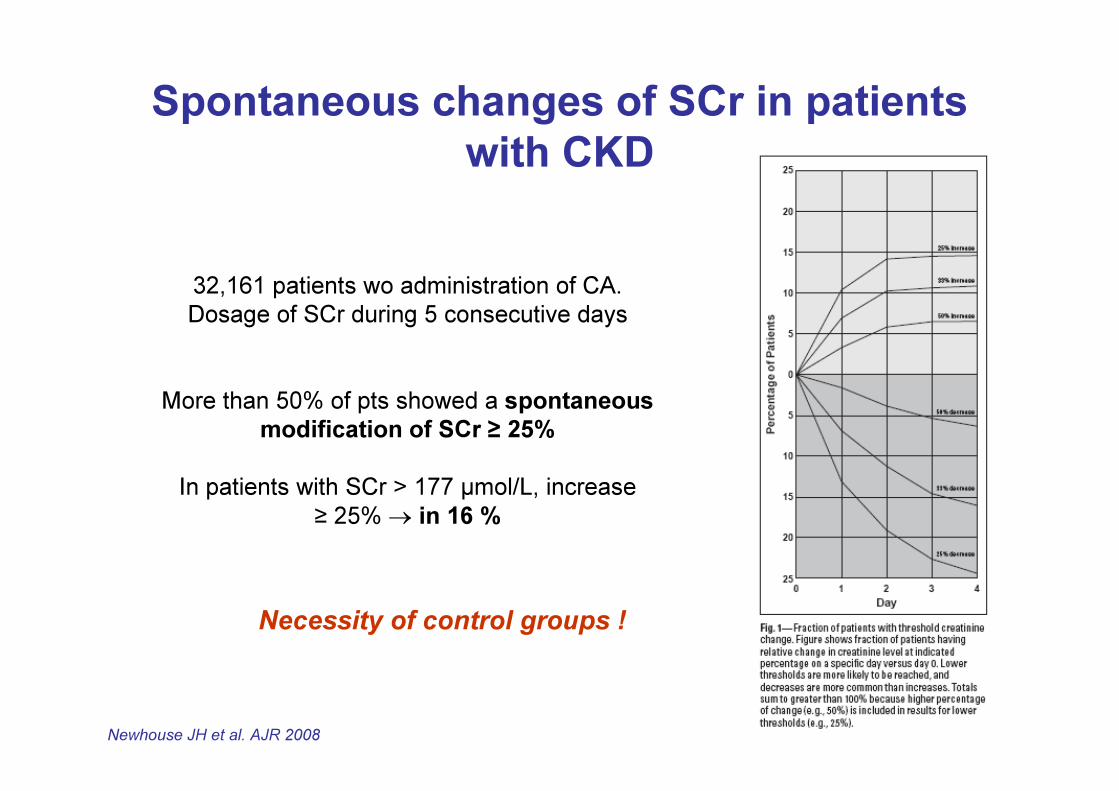
Spontaneous changes of SCr in patients with CKD
32,161 patients wo administration of CA.Dosage of SCr during 5 consecutive days
More than 50% of pts showed a spontaneousmodification of SCr ≥ 25%
In patients with SCr > 177 µmol/L, increase ≥ 25% → in 16 %
Newhouse JH et al. AJR 2008
Necessity of control groups !
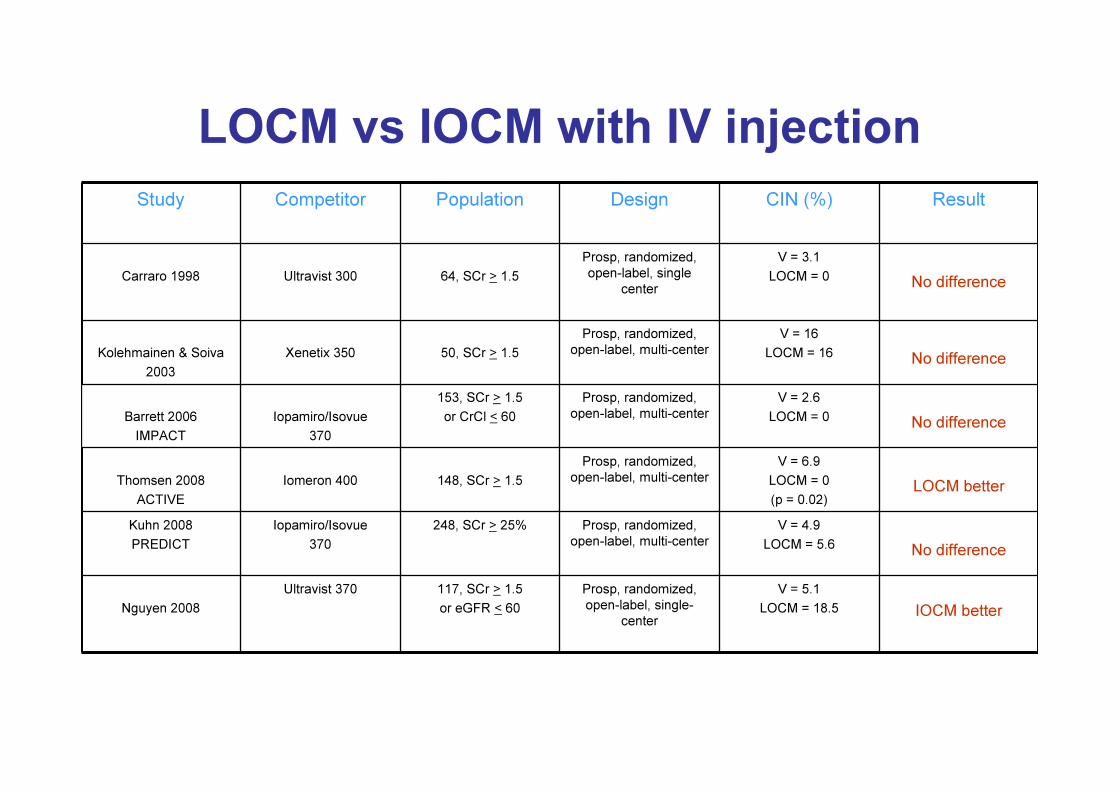
LOCM vs IOCM with IV injectionStudy Competitor Population Design CIN (%) Result
Carraro 1998 Ultravist 300 64, SCr > 1.5Prosp, randomized, open-label, single
centerV = 3.1
LOCM = 0 No difference
Kolehmainen & Soiva2003
Xenetix 350 50, SCr > 1.5Prosp, randomized,
open-label, multi-centerV = 16
LOCM = 16 No difference
Barrett 2006IMPACT
Iopamiro/Isovue370
153, SCr > 1.5or CrCl < 60
Prosp, randomized, open-label, multi-center
V = 2.6LOCM = 0 No difference
Thomsen 2008ACTIVE
Iomeron 400 148, SCr > 1.5Prosp, randomized,
open-label, multi-centerV = 6.9
LOCM = 0(p = 0.02) LOCM better
Kuhn 2008PREDICT
Iopamiro/Isovue370
248, SCr > 25% Prosp, randomized, open-label, multi-center
V = 4.9LOCM = 5.6 No difference
Nguyen 2008Ultravist 370 117, SCr > 1.5
or eGFR < 60Prosp, randomized, open-label, single-
centerV = 5.1
LOCM = 18.5 IOCM better
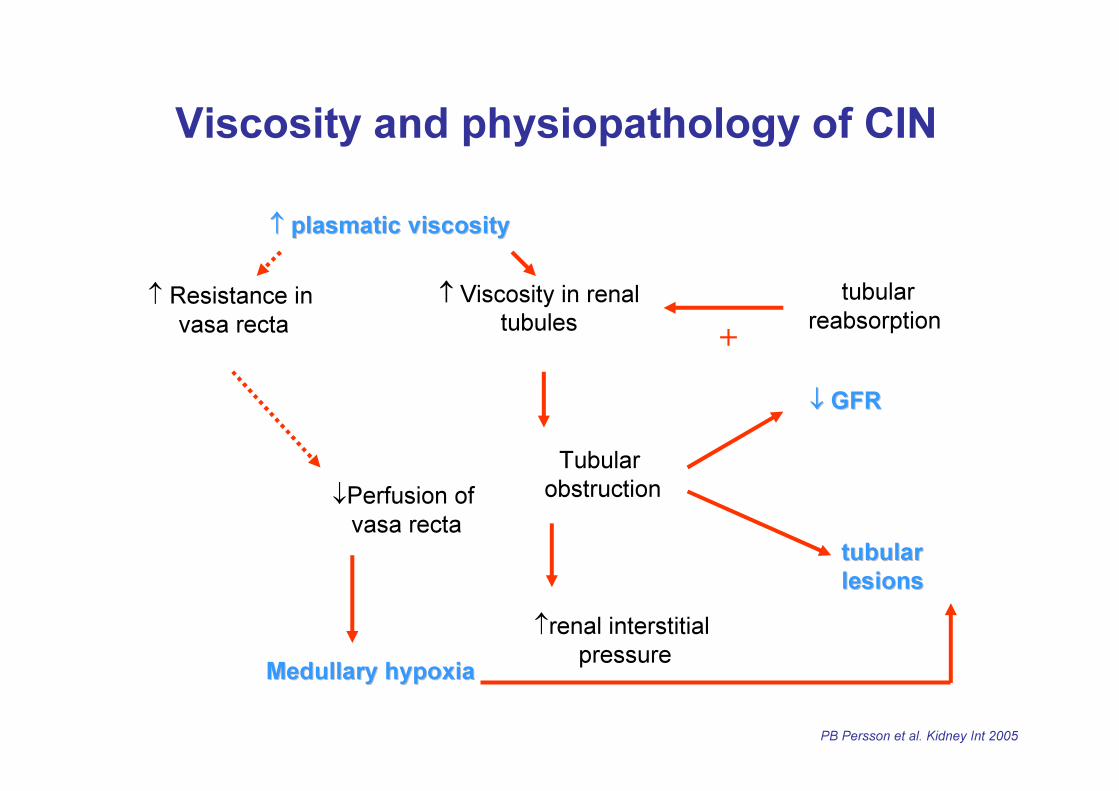
↑↑ plasmatic viscosityplasmatic viscosity
↑ Resistance in vasa recta
↓Perfusion of vasa recta
Medullary hypoxiaMedullary hypoxia
↑ Viscosity in renal tubules
Tubular obstruction
↑renal interstitial pressure
tubular tubular lesions lesions
↓↓ GFR GFR
tubularreabsorption+
Viscosity and physiopathology of CIN
PB Persson et al. Kidney Int 2005
+
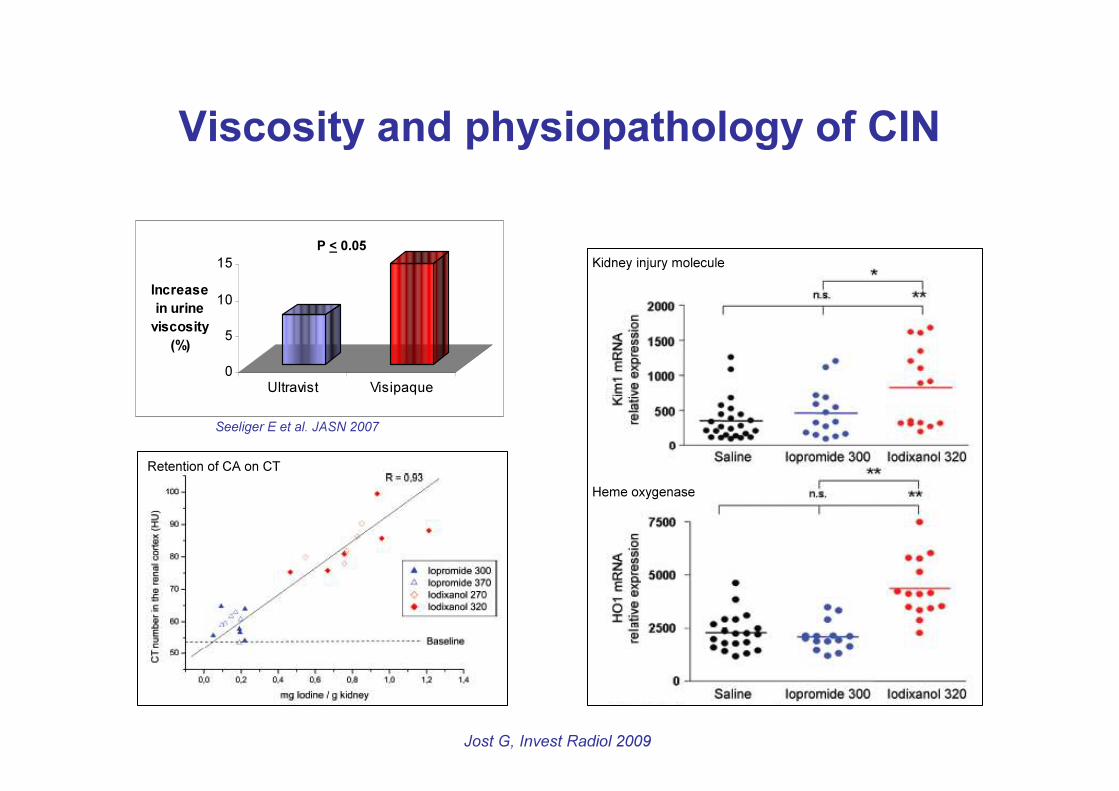
Viscosity and physiopathology of CIN
0
5
10
15Increase in urine
viscosity (%)
Ultravist Visipaque
Seeliger E et al. JASN 2007
Jost G, Invest Radiol 2009
Kidney injury molecule
Heme oxygenase
P < 0.05
Retention of CA on CT
Does that mean….
…. A lot of noise for nothing ?
Nephrotoxicity of iodine CA• Incidence :
– Probably much lower than expected after IV injection
• Prevention in risk patients :– Identification of risk patients – Search for alternative technique– Hydration +++
• 1-2 ml/kg/h of saline 0.9%o or bicarbonate• 4-6h before => 12h-24h after
– Stop all nephrotoxic drugs (24h)– Medications :
• theophylline ?• acetylcysteine (Mucomyst) ?
Toxicity of Gd-chelates• Nephrotoxicity :
– No nephrotoxicity demonstrated at recommendeddoses
– More nephrotoxic than iodine CA at equimolardose
• Nephrogenic systemic fibrosis– In patients with severely impaired renal function
NSF - History
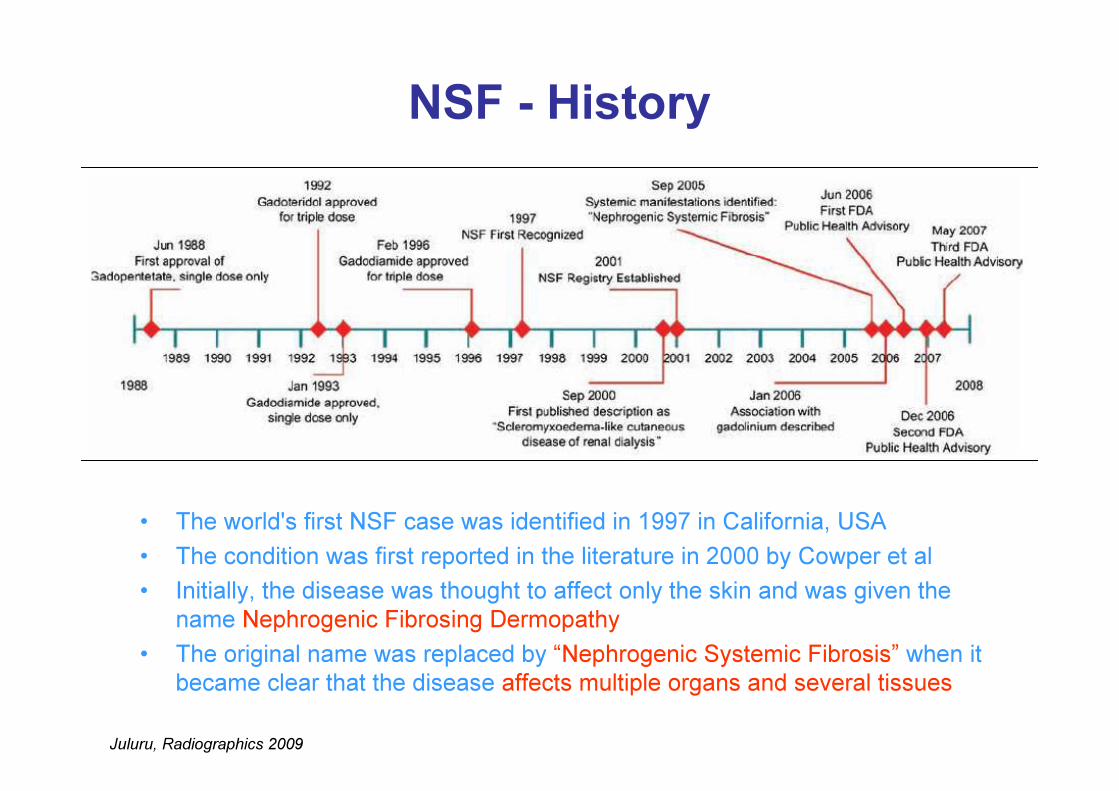
Juluru, Radiographics 2009
• The world's first NSF case was identified in 1997 in California, USA • The condition was first reported in the literature in 2000 by Cowper et al• Initially, the disease was thought to affect only the skin and was given the
name Nephrogenic Fibrosing Dermopathy• The original name was replaced by “Nephrogenic Systemic Fibrosis” when it
became clear that the disease affects multiple organs and several tissues
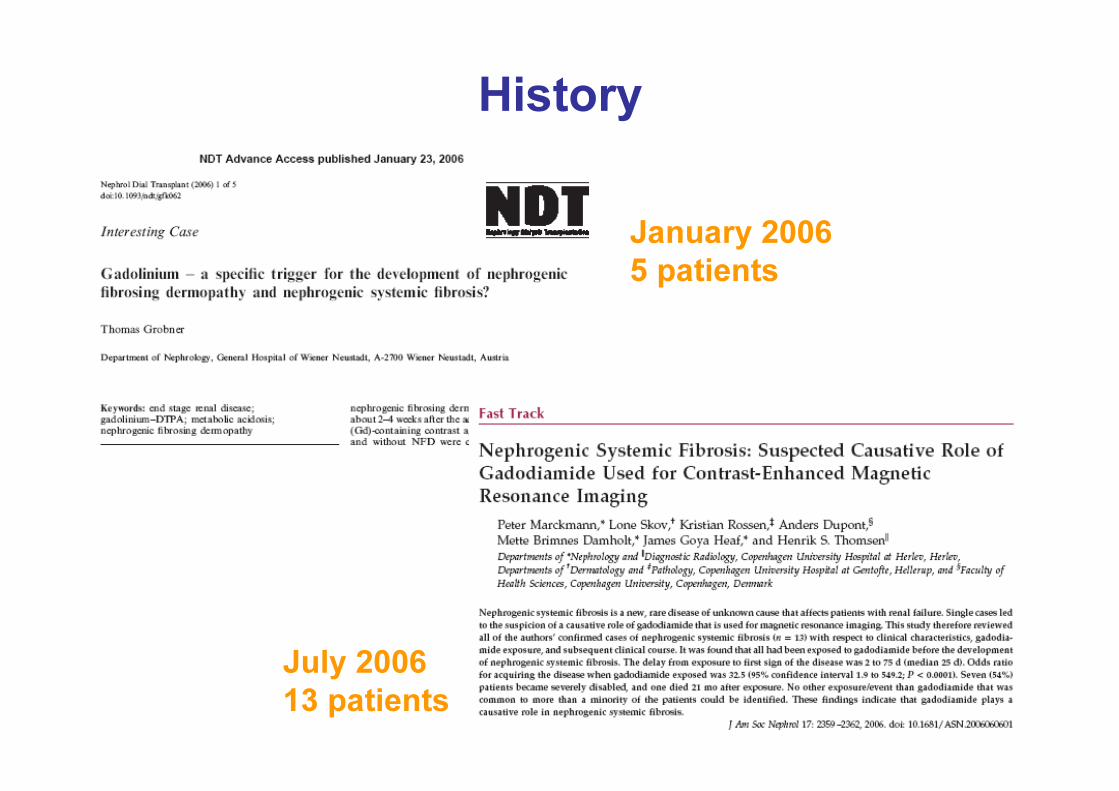
History
January 20065 patients
July 200613 patients
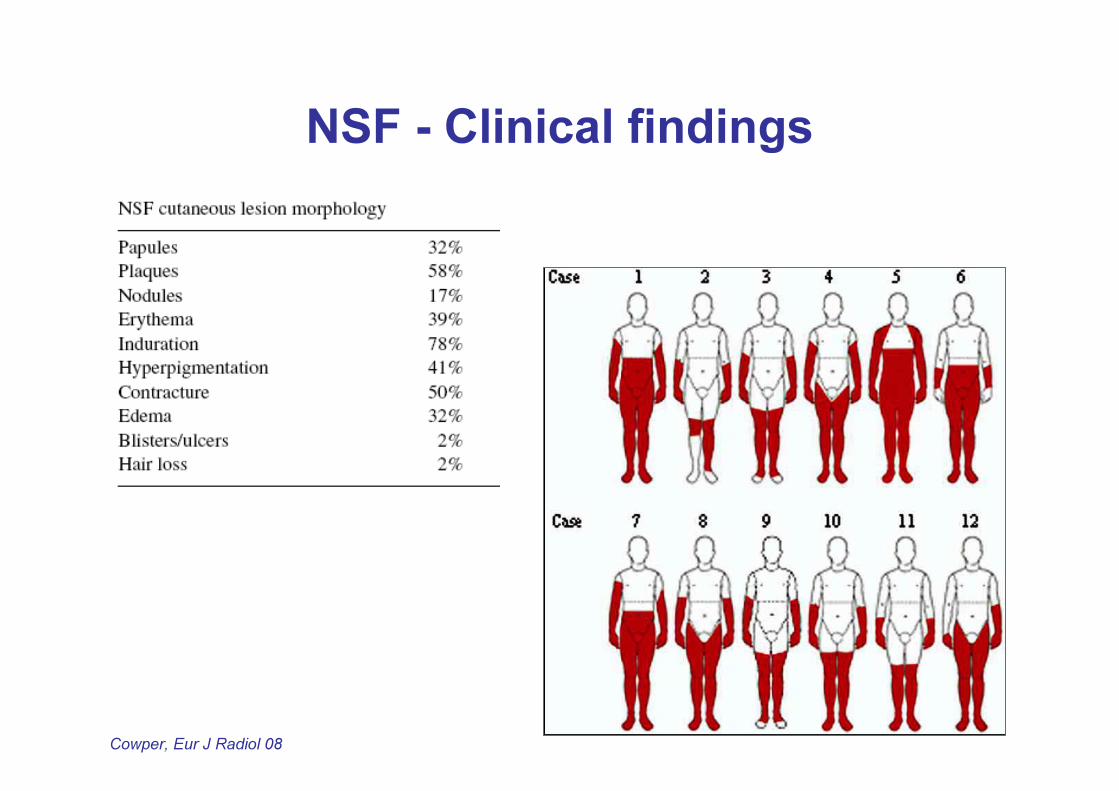
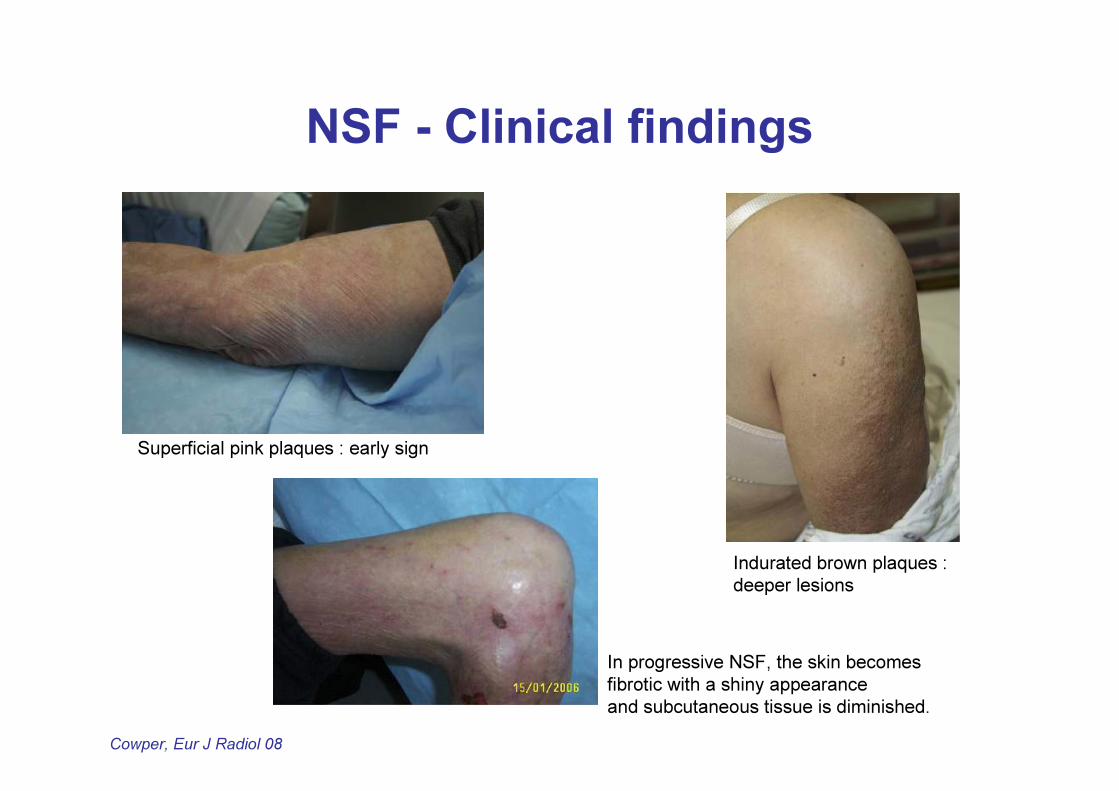
NSF - Clinical findings
Cowper, Eur J Radiol 08
NSF - Clinical findings
Cowper, Eur J Radiol 08
Superficial pink plaques : early sign
Indurated brown plaques : deeper lesions
In progressive NSF, the skin becomes fibrotic with a shiny appearanceand subcutaneous tissue is diminished.

NSF - Clinical findings
Cowper, Eur J Radiol 08
Contractures in lower distal extremity
Contractures in upper distal extremity
Prominent yellow scleral plaque
Clinical findings : outcome
• Severely affected patients are unable to walk
• NSF may cause severe morbidity and even mortality in some patients
• Improvement in a small percentage of patients following recovery of renal function
Mendoza FA. Semin Arthtitis Rheum 2003Jimenez S. Arthritis Rheum 2004
Swartz RD. Am J Med 2003
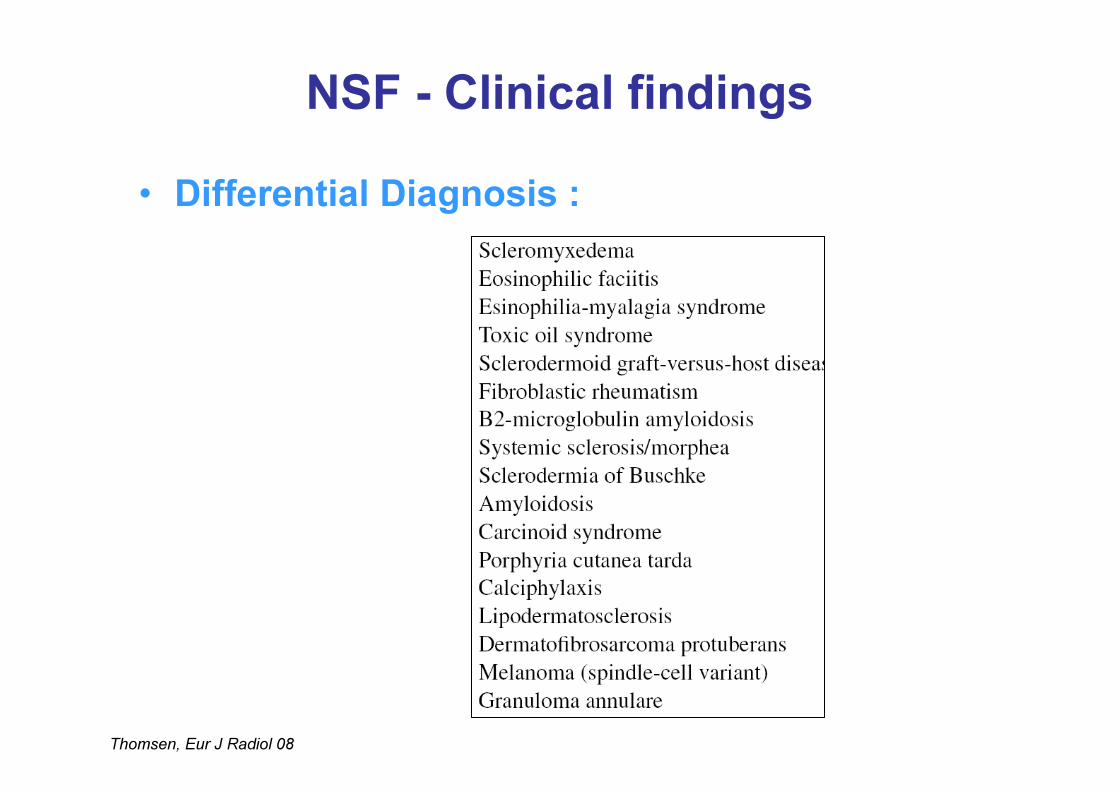
NSF - Clinical findings• Differential Diagnosis :
Thomsen, Eur J Radiol 08
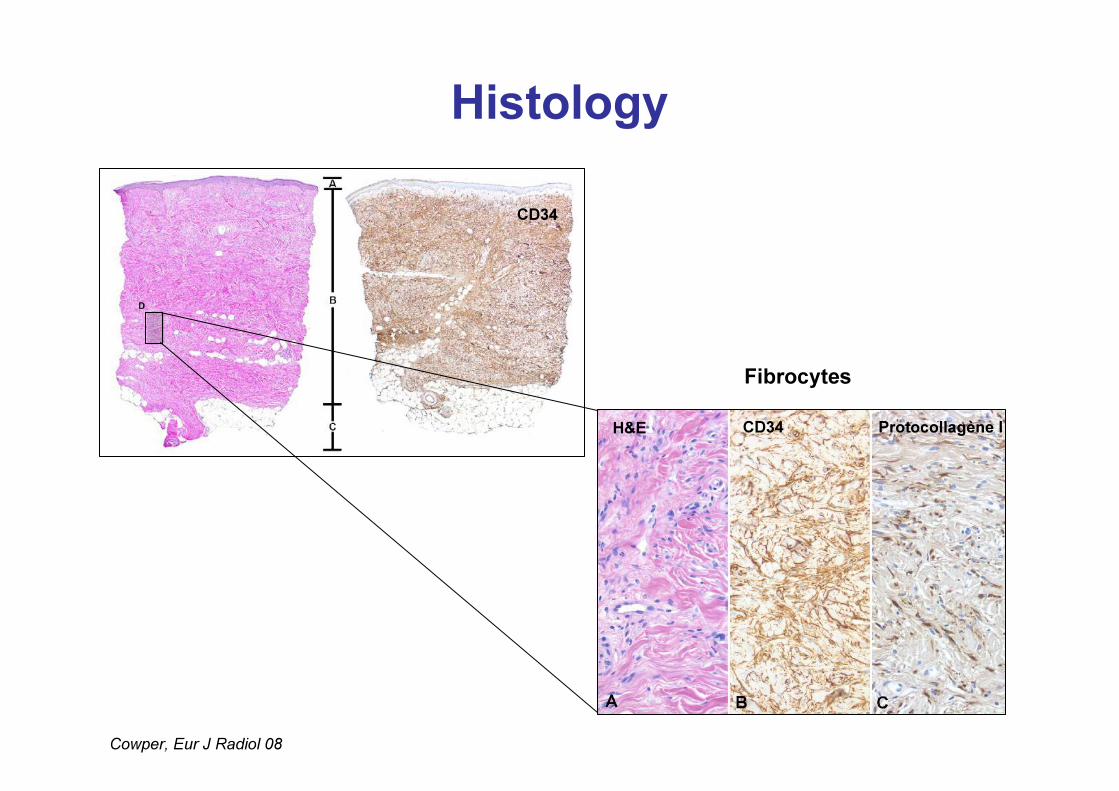
HistologyCD34
Cowper, Eur J Radiol 08
FibrocytesH&E CD34 Protocollagène I
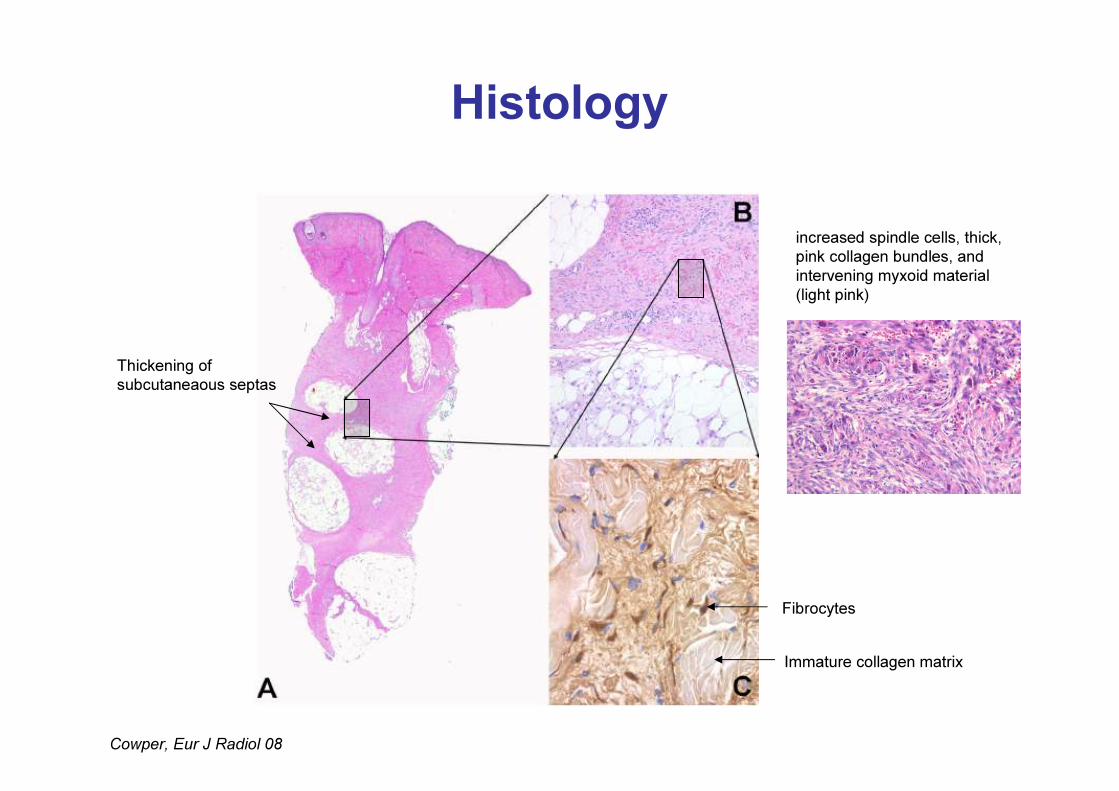
Histology
Cowper, Eur J Radiol 08
Thickening of subcutaneaous septas
Immature collagen matrix
Fibrocytes
increased spindle cells, thick, pink collagen bundles, andintervening myxoid material (light pink)
Histology• Differential Diagnosis :
Thomsen, Eur J Radiol 08
NSF and renal function• Facts :
– Patients with normal or moderate renal failure never develop NSF– The risk of developing NSF increases with severity of renal failure– Majority of risk patients do NOT develop NSF– No age, ethnic or gender preference
• Risk factors :– Patients with CKD (GFR < 30ml/min)– Patients on dialysis– Patients suffering from acute renal failure– Patients with hepato-renal syndrome – Patients requiring liver transplantation
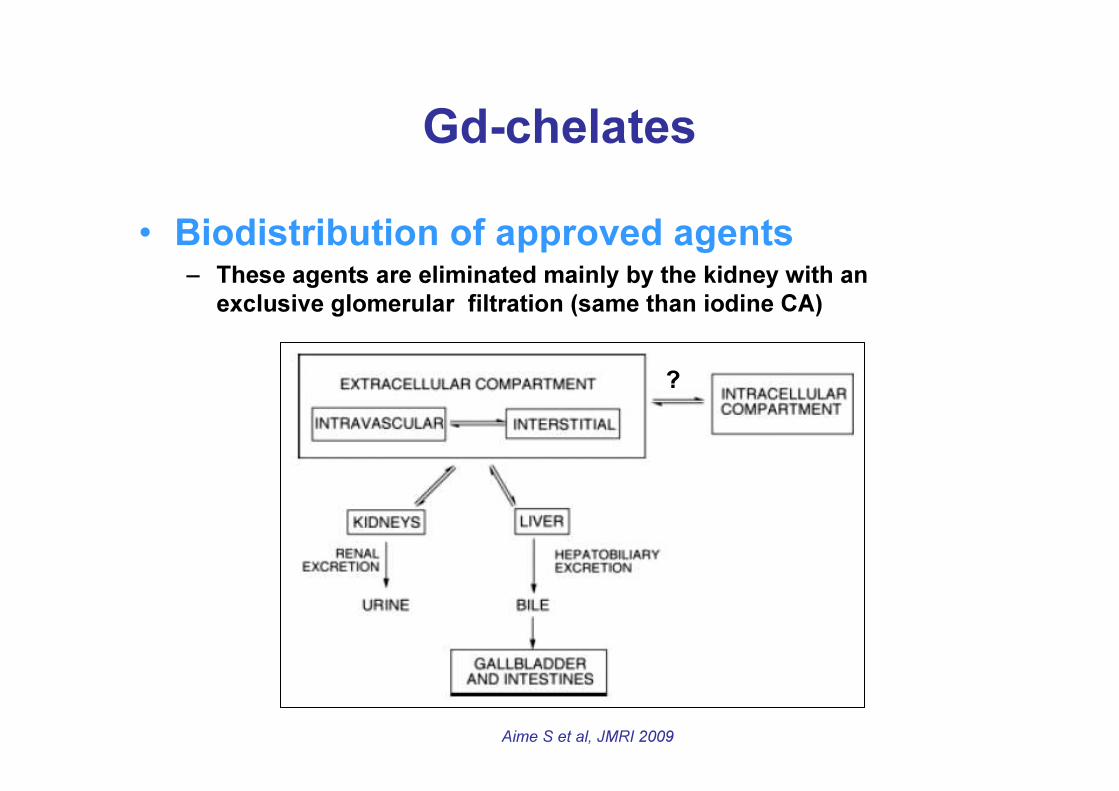
Gd-chelates• Biodistribution of approved agents
– These agents are eliminated mainly by the kidney with an exclusive glomerular filtration (same than iodine CA)
?
Aime S et al, JMRI 2009
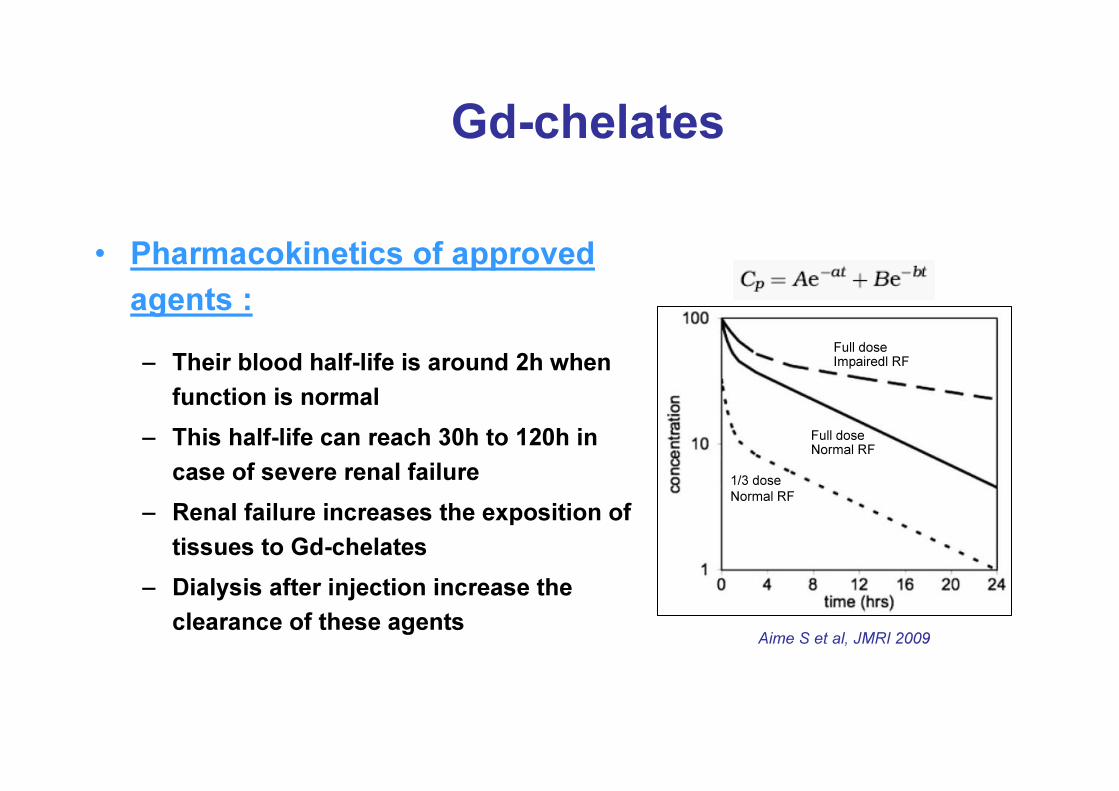
Gd-chelates
• Pharmacokinetics of approved agents :– Their blood half-life is around 2h when
function is normal– This half-life can reach 30h to 120h in
case of severe renal failure– Renal failure increases the exposition of
tissues to Gd-chelates– Dialysis after injection increase the
clearance of these agents
Full doseNormal RF
1/3 doseNormal RF
Full doseImpairedl RF
Aime S et al, JMRI 2009
Physiopathology• Possible co-factors of development of NSF :
– Repeated and increasing exposition to the CA– High blood concentration of phosphate and ionized calcium– Hypoalbuminemia – Liver insufficiency, particularly before liver transplantation– Concomitant pro-inflammatory state– Metabolic acidosis– Treatment with high doses of erythropoietin
Marckman, Eur J Radiol 08
Hypotheses
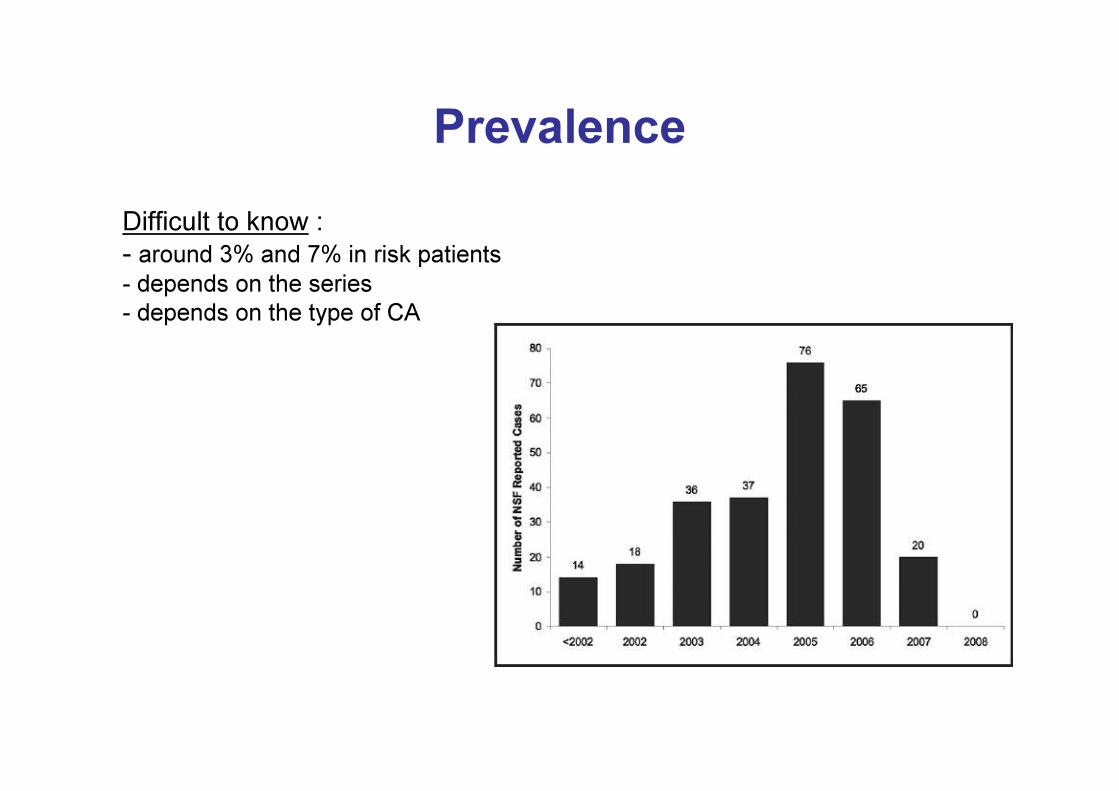
Prevalence Difficult to know :- around 3% and 7% in risk patients- depends on the series- depends on the type of CA
PrevalenceReported cases :
– Around 500 reported cases but all are not proved– In publications : 186 « non confounded » cases in 2008• 134 with Omniscan• 18 with Magnevist• 2 with Optimark• 1 with Prohance
– Other cases are « confounded »
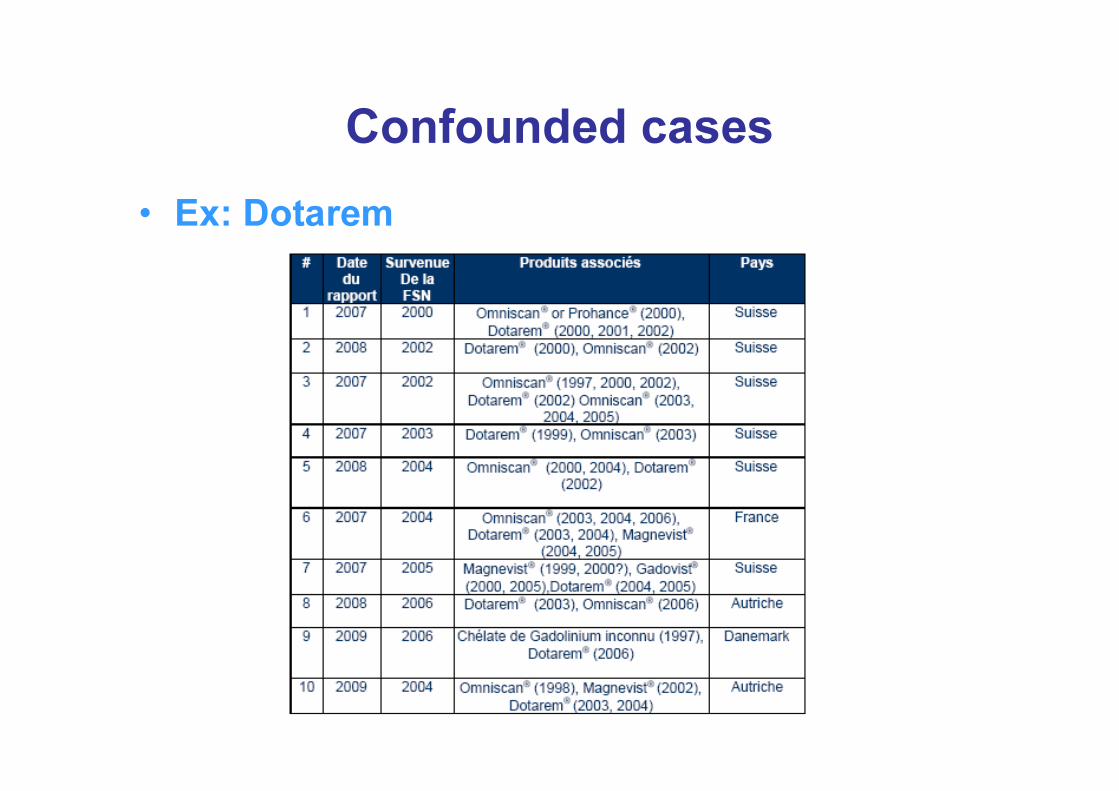
Confounded cases• Ex: Dotarem
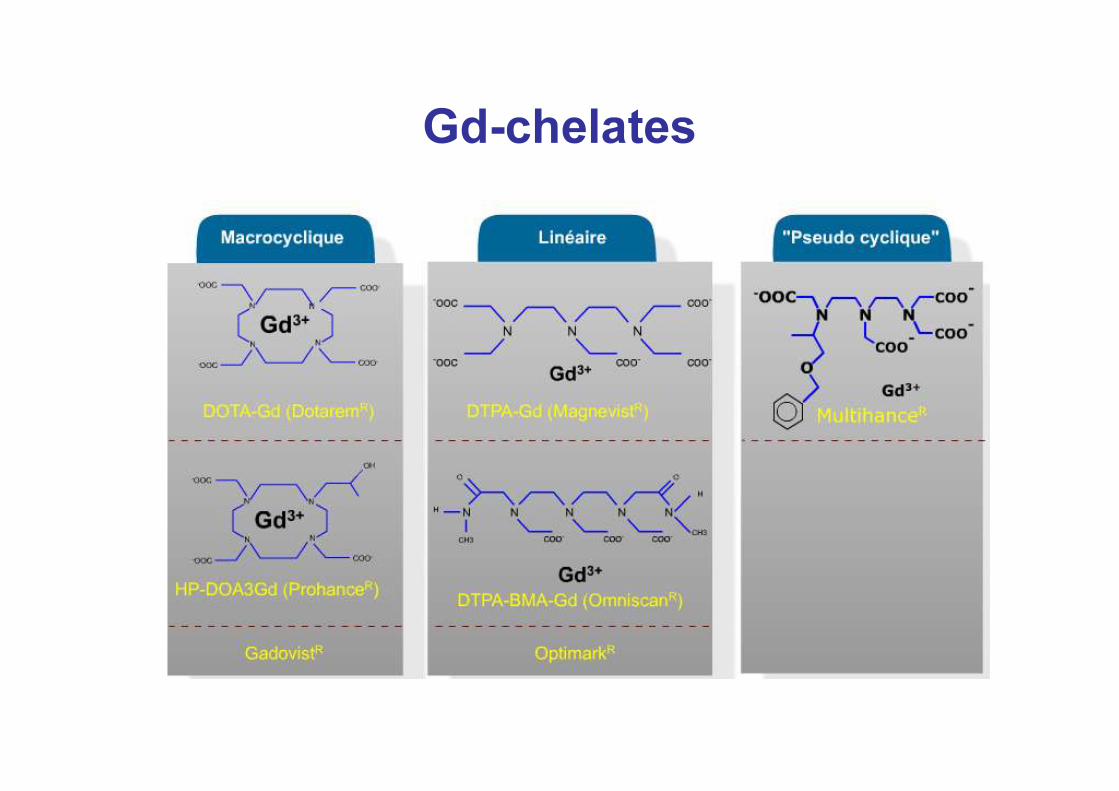
Gd-chelates
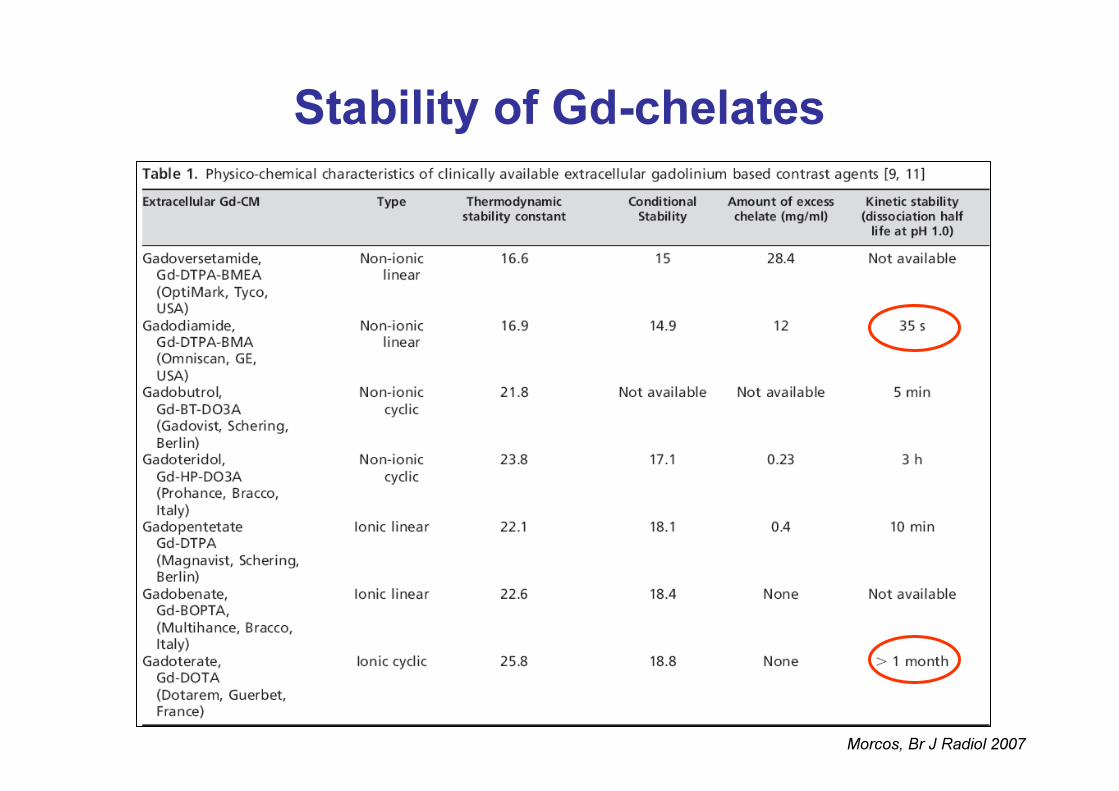
Stability of Gd-chelates
Morcos, Br J Radiol 2007

Physiopathology• Transmetallation
Tweedle MF Invest. Radiol. 1992; 27:S2-S6
Opt Mag
2000
1500
1000
500
0
nmol/Gd/g skin
Omnisc
an
Dotarem
Gadovist
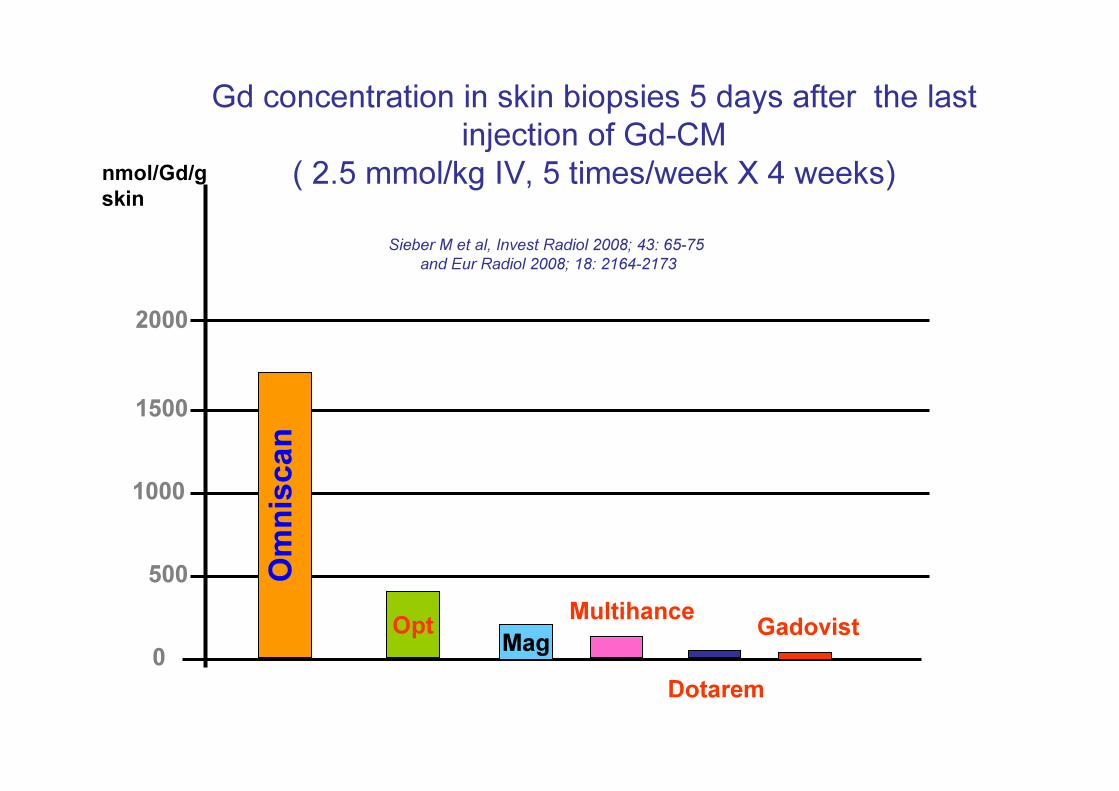
Gd concentration in skin biopsies 5 days after the last injection of Gd-CM
( 2.5 mmol/kg IV, 5 times/week X 4 weeks)
Multihance
Sieber M et al, Invest Radiol 2008; 43: 65-75 and Eur Radiol 2008; 18: 2164-2173

Physiopathology
Abraham, Eur J Radiol 08
Skin biopsy showing free gadolinium
H&S ME
Spectroscopie
Open Questions • It is unknown whether Gd deposition results in non-NSF subjects as
well, and if so, whether such deposition correlates with impaired renal function.
• In the cases of Gd deposition in NSF patients, it is likely that the Gd is no longer associated with its chelator, but this has still not been definitively shown.
• Is the form of Gd the same in skin deposits compared to internalorgans?
• If dechelation occurs, then where does it occur and how is the Gd transported to other organs?
How to reduce the Risk of NSF ?• Patients with GFR<30ml/min including those on dialysis should not
receive non-ionic linear chelates or Magnevist• The most stable Gd-CM should be used in these patients (macrocyclic Gd-CA)• The lowest possible dose• Allow at least one week before giving more Gd-CM• Patients on haemodialysis can be scheduled to have a dialysis
session shortly after the MRI examination• Patients on peritoneal dialysis should be asked to do several rapid exchanges after the examination
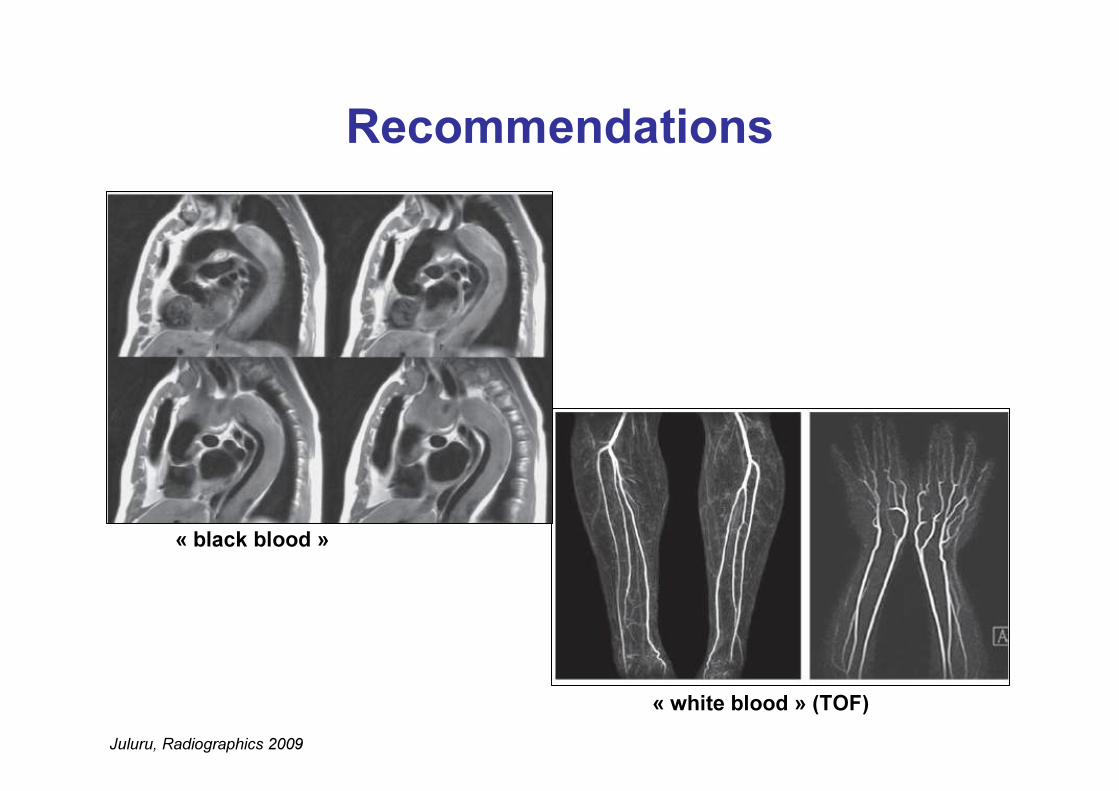
Recommendations
Juluru, Radiographics 2009
« black blood »
« white blood » (TOF)
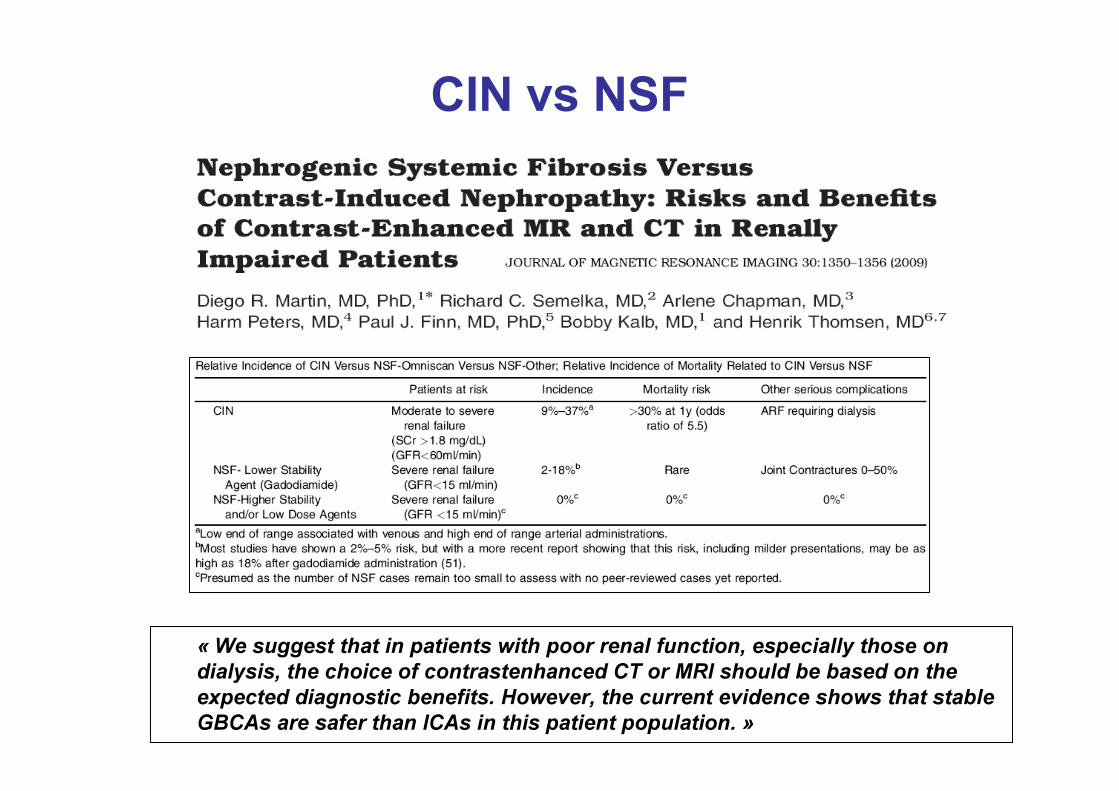
« We suggest that in patients with poor renal function, especially those on dialysis, the choice of contrastenhanced CT or MRI should be based on the expected diagnostic benefits. However, the current evidence shows that stable GBCAs are safer than ICAs in this patient population. »
CIN vs NSF
Conclusions• Iodine CA :
– Nephrotoxicity of CA is probably overestimated with IV injections
– However, detection of risk patients and prevention must stay the rule
• NSF :– It is a complication linked to unstable agents which have to be waved in risk patients
– However, use of Gd injections should be rationalized in these risk patients

ESUR Guidelines on Contrast Media
ESUR
Contrast Media Safety Committee
www.esur.org
Acknowledgments to Pr Sam K Morcos, Sheffield, UK for help