Embed Size (px)
Citation preview
TRAUMATIC PARAPLEGIAHunterian Lecture delivered at the Royal College of Surgeons of England
on11th March 1954
byF. W. Holdsworth, M.Chir., F.R.C.S.
Orthopaedic Surgeon, Sheffield Royal Infirmary and Sheffield Children's Hospitaland Lecturer in Orthopaedic Surgery at Sheffield University.
PARAPLEGIA, THE RESULT of injury in civilian life, is fairly common. In areview carried out just after the last war Nicoll estimated the incidence inthe large coal fields of this country to be 1 per 100,000 and that everygeneral hospital might expect two of these patients each year. Thus,although the total number of patients is large the experience gained in thetreatment from the time of injury of 150 patients suffering from paraplegiawill perhaps not be without interest and possible value.The first really serious attempt to analyse these injuries and to work
out a rational line of treatment was made by Gordon Holmes and othersduring and immediately after the first world war on paraplegia resultingfrom gunshot wounds. These patients, however, were treated underdifficulties and, as a rule, were not seen and carefully examined untilweeks or even months after the injury. Moreover, the lesions were ofmany different types. For all these reasons conclusions as to immediatetreatment were difficult to elicit. The fact is that little general attentionwas paid to their work and up to the last war patients were, for all practicalpurposes, left to die, rotting with bedsores and wasted with protein lossand severe renal infection. During the last war the great increase innumber of paraplegic patients again stimulated interest in the problem.The establishment of spinal centres and the pioneer work of Guttmannin this country and of Munroe, Bors, Rodgers and many others in theUnited States, showed that bedsores could be healed, urinary infectioncontrolled and patients rehabilitated to a useful life. No praise is too highfor their remarkable work, indeed such praise is constantly given byall who have been privileged to visit their centres.
These centres, however, receive almost all their patients weeks or evenmonths after the injury, when the original problem is masked by thedreadful complications of huge bedsores and urinary infection. It occurredto my colleagues and myself that these complications might be avoidedif a centre were established where such patients could be admitted immedi-ately after the accident. The splendid co-operation of our colleaguesin the Sheffield region, enabled us to develop such a centre and we havenow treated 71 patients from the time of the accident. The experience wehave gained and the lessons we have learned from these patients form thesubstance of this lecture.We have, I think, clearly shown that by correct nursing and careful
attention to simple bladder drainage and by correct rehabilitation all serious
281
F. W. HOLDSWORTH
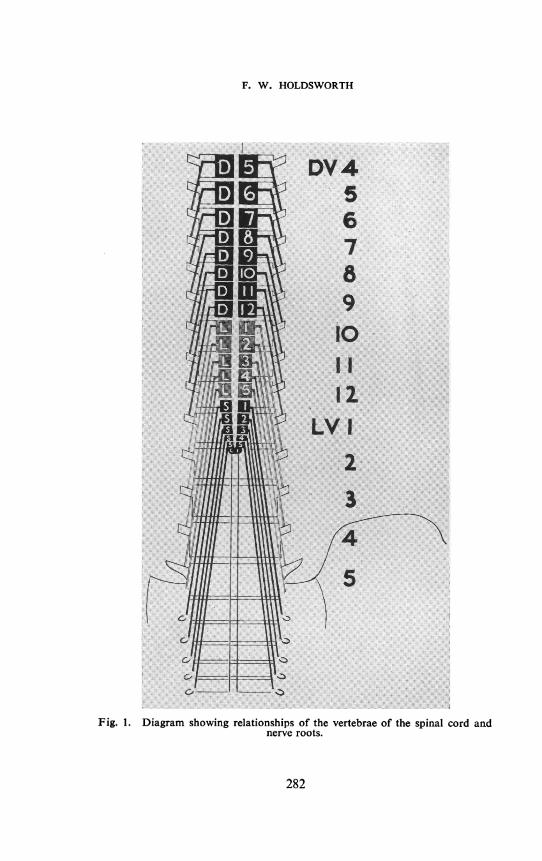
Fig. 1. Diagram showing relationships of the vertebrae of the spinal cord andnerve roots.
282
TRAUMATIC PARAPLEGIA
complications can easily be avoided, the general health of the patientmaintained and the stay in hospital cut down to nine or ten months.In the 71 patients treated from the onset there has not been one seriousbedsore and no case of urinary infection which was not easily controlled.All the patients with lumbo dorsal paraplegia have been up in threemonths and discharged home in an average of nine months.The absence of serious complications has allowed us to concentrate
attention upon the cord and vertebral injury. Careful neurological
(a)(b)(c)(d)
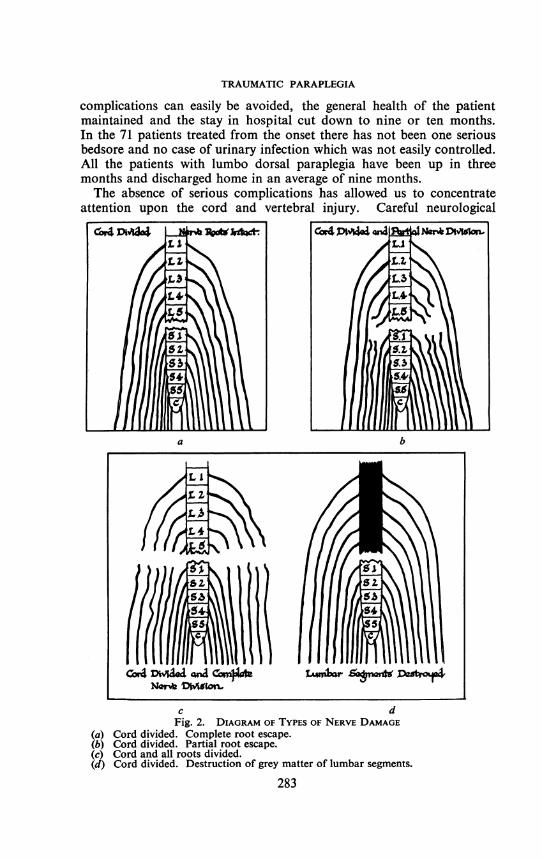
c dFig. 2. DIAGRAM OF TYPES OF NERVE DAMAGE
Cord divided. Complete root escape.Cord divided. Partial root escape.Cord and all roots divided.Cord divided. Destruction of grey matter of lumbar segments.
283
* r
ba
Cor4 DwIAed QGia c4attNor Muto
I i 4
F. W. HOLDSWORTH
examination from within a few hours of the accident and repeated through-out treatment has given us an experience probably unique, for althoughlarger series are reported in the literature, so far as we are aware, there isno comparable series treated in one centre from the time of injury.
It has been known for many years that transection of the spinal cord isan irrecoverable lesion, for the nerve fibres of the cord have no power ofregeneration. The nerve roots, however, are peripheral nerves and, undersuitable circumstances, are capable of regeneration after transection.Moreover, there is considerable evidence to show that the cord is lessresistant to injury than the nerve roots. Violence sufficient to produceirrecoverable damage to the cord may be insufficient to cause irreparabledamage to the nerve roots. Thus root and cord lesions are very differentand it is therefore important in these injuries to distinguish the one fromthe other for, in general, the prognosis of root paralysis is better than ofcord paralysis or at any rate it cannot be worse.The immediate effect of severe injury to the spinal cord is to produce a
suppression of function below the level of the lesion. The suppression offunction may not be due to anatomical division of the cord but to aphysiological division which is capable of recovery. The extent and typeof recovery depend upon the degree of anatomical injury to the cord.If the cord is intact complete recovery will occur; if partly divided partialrecovery of sensation and motor power; but if completely divided theisolated segments will recover local reflex activity and the paralysis willbecome of the upper motor neurone type, the anaesthesia remainingunchanged.The roots behave in a similar manner except that, with anatomical
division, if recovery does not occur, the paralysis remains flaccid and thereis no return of reflex activity of the affected root segments.
Thus, during the period of suppression of function it is impossible todiscover the extent of anatomical damage to the cord and so long as thiscondition persists in complete form there must be uncertainty as to thepossibility of recovery of any cord function.
It is for this reason that there is so much controversy about the initialtreatment of the injury. If the cord is divided no form of treatment canalter the prognosis. If the cord is intact recovery will occur withouttreatment and all that is necessary is to protect it from further damage.If, however, there is a partial lesion it may well be that decompressionof the cord either by laminectomy or by cordotomy may assist recovery.Faced with these difficulties of diagnosis, some surgeons, assuming all
patients with paraplegia to have some cord continuity, advocate laminec-tomy and possible exploration in all cases, others, disappointed with theresults of immediate exploration, never operate but wait until " spinalshock" has disappeared and then explore the cord in those patients withsome signs of recovery. Still others only operate upon those patients withsigns of recovery and with evidence, radiological and otherwise of thecal
284
TRAUMATIC PARAPLEGIA
block. One grave disadvantage of waiting is that the nursing necessary toprevent bedsores may cause further damage to an anatomically intactcord or transform a partial into a complete transection.
Any guide to the true nature of the cord lesion must therefore be ofgreat importance. For this purpose we believe that the deductions wehave made from this series may be of value.
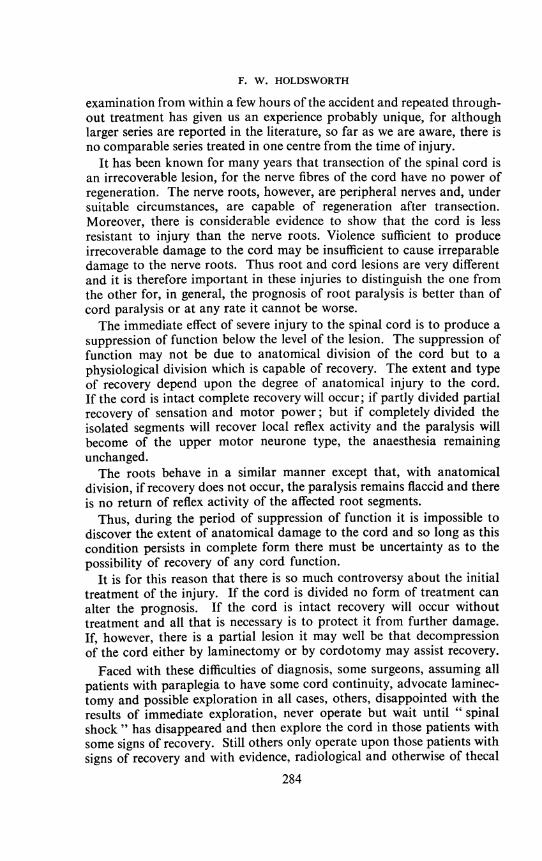
Fig. 3. The cord and cauda equina removed from a patient with complete corddivision at the level of S1. The grey matter of the lumbar segments is destroyed
and the cord replaced by a large cyst.
285
F. W. HOLDSWORTH
AnatomyThe spinal cord ends at the lower border of the first lumbar vertebra.
Below this level the vertebral canal contains the cauda equina. Thefirst sacral neurological segment lies opposite the lower border of thetwelfth dorsal vertebra and the first lumbar neurological segment probablyas high as the ninth dorsal vertebra (Fig. 1). Thus, all the lumbar cordsegments lie between D9 and D12 and all the sacral segments betweenthe lower border of D12 and the lower border of LI. The vertebralcanal, therefore, at the thoraco lumbar junction contains the cord andall the lumbar nerve roots passing down from their segments of originto their proper intervertebral foramina. Above the ninth dorsal vertebrathe nerve segments and roots are roughly opposite the appropriatevertebra.The cord is supplied with blood by several vessels. In the embryo the
longitudinal spinal arteries are reinforced by arteries which pass alongeach nerve root but in the process of development all but four or five ofthese vessels disappear. The final pattern is of longitudinal arteries rein-forced by three or four root arteries, one of which is fairly constantlyfound running with the second lumbar nerve root and therefore passingthe lumbo dorsal vertebral junction.
Dorso Lumbar InjuriesWe have paid particular attention to injuries at the thoraco-lumbar
junction. Firstly because it is the commonest level for traumatic paraplegiato occur and secondly because at this level particular conditions exist.Most of the deductions we have made for these injuries are also applicablefor cord and root injuries above and below.The level of cord injury can be determined in patients with traumatic
paraplegia by a study of the X-rays. The neurological level as determinedby clinical examination may not correspond with this. The disparityis due to root injury. Thus a dislocation between D12 and LI vertebraewill injure the cord at the SI segment but the neurological level may beas high as LI. The lumbar segmental paralysis and anaesthesia in sucha patient is due to root injury but the sacral is due to damage to the cord(Fig. 1). At higher levels the disparity becomes comparatively less whilstbelow LI vertebrae the lesion must be purely of the roots. These areextremely important facts for we believe that in many cases of lumbo-dorsal dislocation escape or recovery of one or two lumbar roots hasbeen interpreted as a partial cord lesion. In other words, that the levelof cord injury has been assumed to be that determined by the neurologicalexamination.That the cord level can be determined as opposite the vertebral injury
may appear to be an unjustifiable assumption for it disregards tractionon the cord and vascular disturbances as a cause of cord division. Itcan, however, be shown that in many of our cases the paralysis and
286
TRAUMATIC PARAPLEGIA
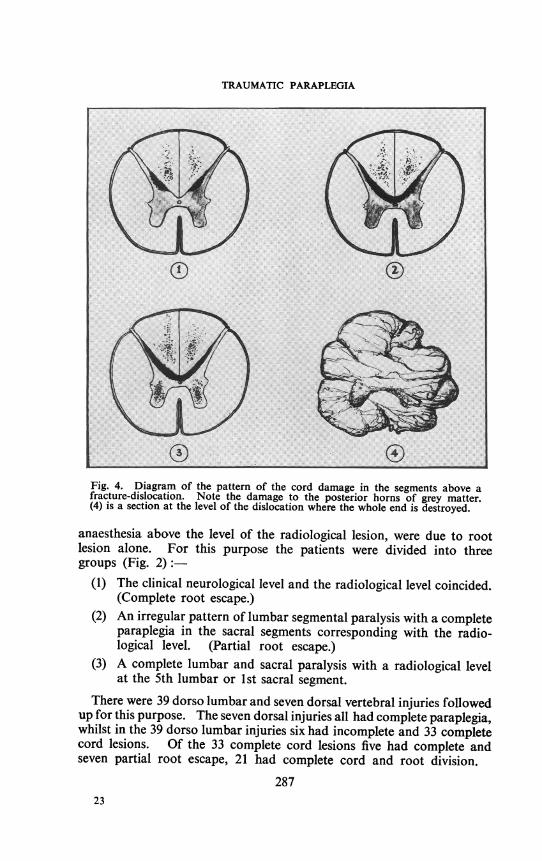
Fig. 4. Diagram of the pattern of the cord damage in the segments above afracture-dislocation. Note the damage to the posterior horns of grey matter.(4) is a section at the level of the dislocation where the whole end is destroyed.
anaesthesia above the level of the radiological lesion, were due to rootlesion alone. For this purpose the patients were divided into threegroups (Fig. 2):-
(1) The clinical neurological level and the radiological level coincided.(Complete root escape.)
(2) An irregular pattern of lumbar segmental paralysis with a completeparaplegia in the sacral segments corresponding with the radio-logical level. (Partial root escape.)
(3) A complete lumbar and sacral paralysis with a radiological levelat the 5th lumbar or 1st sacral segment.
There were 39 dorso lumbar and seven dorsal vertebral injuries followedup for this purpose. The seven dorsal injuries all had complete paraplegia,whilst in the 39 dorso lumbar injuries six had incomplete and 33 completecord lesions. Of the 33 complete cord lesions five had complete andseven partial root escape, 21 had complete cord and root division.
28723
F. W. HOLDSWORTH
In the first group the ultimate development of the classical signs of anisolated sacral cord, that is paralysis and anaesthesia with brisk reflexes,proved the lesion to be of the cord whilst the lumbar segments, with someinteresting exceptions, to be discussed later, remained normal.
In the second group a similar pattern of isolated sacral cord developedbut the lumbar paralysis either recovered to normal function or theparalysis remained flaccid with no reflex activity-proof of a lower motorneurone lesion in the lumbar segments.
In the third group the lumbar paralysis remained flaccid with no reflexactivity whilst the typical signs of upper motor neurone lesion appearedin the sacral segments fixing the cord lesion level with vertebral injury.In a few cases some normal activity returned in the lumbar segments.The recovery was never spastic.
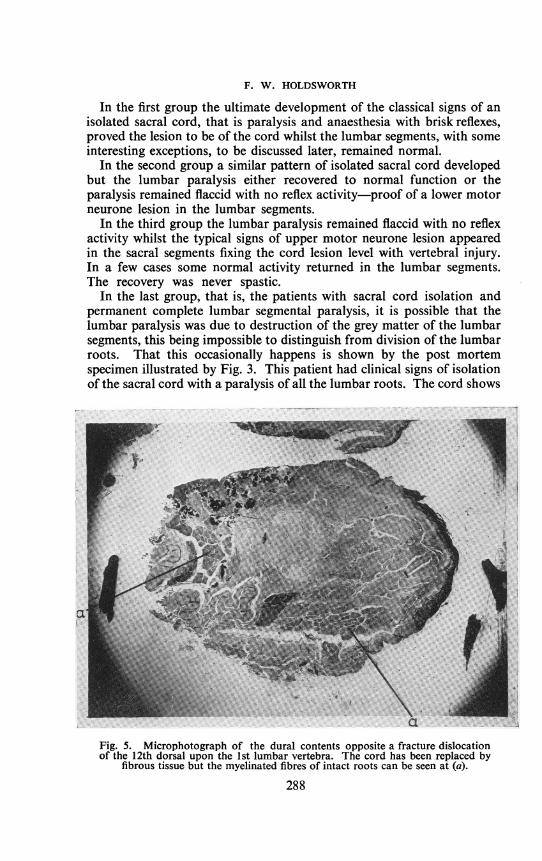
In the last group, that is, the patients with sacral cord isolation andpermanent complete lumbar segmental paralysis, it is possible that thelumbar paralysis was due to destruction of the grey matter of the lumbarsegments, this being impossible to distinguish from division of the lumbarroots. That this occasionally happens is shown by the post mortemspecimen illustrated by Fig. 3. This patient had clinical signs of isolationof the sacral cord with a paralysis of all the lumbar roots. The cord shows
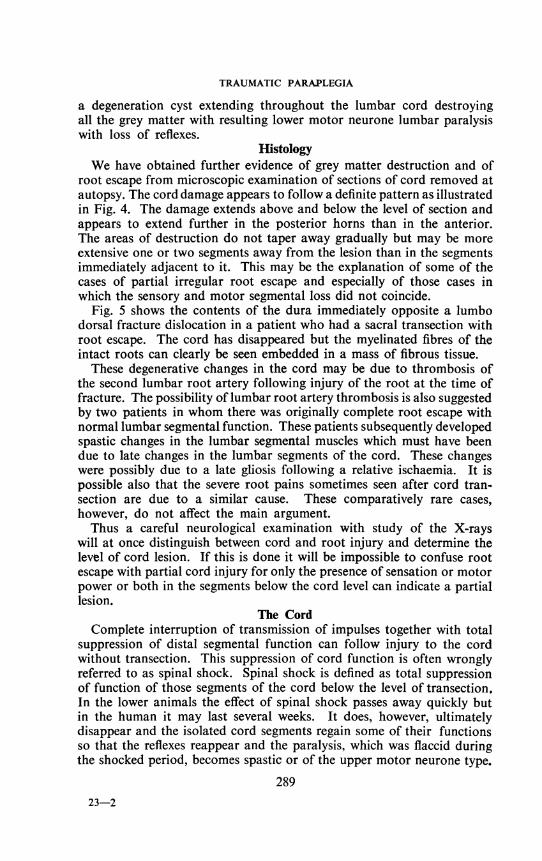
Fig. 5. Microphotograph of the dural contents opposite a fracture dislocationof the 12th dorsal upon the 1st lumbar vertebra. The cord has been replaced by
fibrous tissue but the myelinated fibres of intact roots can be seen at (a).
288
TRAUMATIC PARAPLEGIA
a degeneration cyst extending throughout the lumbar cord destroyingall the grey matter with resulting lower motor neurone lumbar paralysiswith loss of reflexes.
HistologyWe have obtained further evidence of grey matter destruction and of
root escape from microscopic examination of sections of cord removed atautopsy. The cord damage appears to follow a definite pattern as illustratedin Fig. 4. The damage extends above and below the level of section andappears to extend further in the posterior horns than in the anterior.The areas of destruction do not taper away gradually but may be moreextensive one or two segments away from the lesion than in the segmentsimmediately adjacent to it. This may be the explanation of some of thecases of partial irregular root escape and especially of those cases inwhich the sensory and motor segmental loss did not coincide.
Fig. 5 shows the contents of the dura immediately opposite a lumbodorsal fracture dislocation in a patient who had a sacral transection withroot escape. The cord has disappeared but the myelinated fibres of theintact roots can clearly be seen embedded in a mass of fibrous tissue.
These degenerative changes in the cord may be due to thrombosis ofthe second lumbar root artery following injury of the root at the time offracture. The possibility of lumbar root artery thrombosis is also suggestedby two patients in whom there was originally complete root escape withnormal lumbar segmental function. These patients subsequently developedspastic changes in the lumbar segmental muscles which must have beendue to late changes in the lumbar segments of the cord. These changeswere possibly due to a late gliosis following a relative ischaemia. It ispossible also that the severe root pains sometimes seen after cord tran-section are due to a similar cause. These comparatively rare cases,however, do not affect the main argument.Thus a careful neurological examination with study of the X-rays
will at once distinguish between cord and root injury and determine thelevel of cord lesion. If this is done it will be impossible to confuse rootescape with partial cord injury for only the presence of sensation or motorpower or both in the segments below the cord level can indicate a partiallesion.
The CordComplete interruption of transmission of impulses together with total
suppression of distal segmental function can follow injury to the cordwithout transection. This suppression of cord function is often wronglyreferred to as spinal shock. Spinal shock is defined as total suppressionof function of those segments of the cord below the level of transection.In the lower animals the effect of spinal shock passes away quickly butin the human it may last several weeks. It does, however, ultimatelydisappear and the isolated cord segments regain some of their functionsso that the reflexes reappear and the paralysis, which was flaccid duringthe shocked period, becomes spastic or of the upper motor neurone type.
28923-2
F. W. HOLDSWORTH
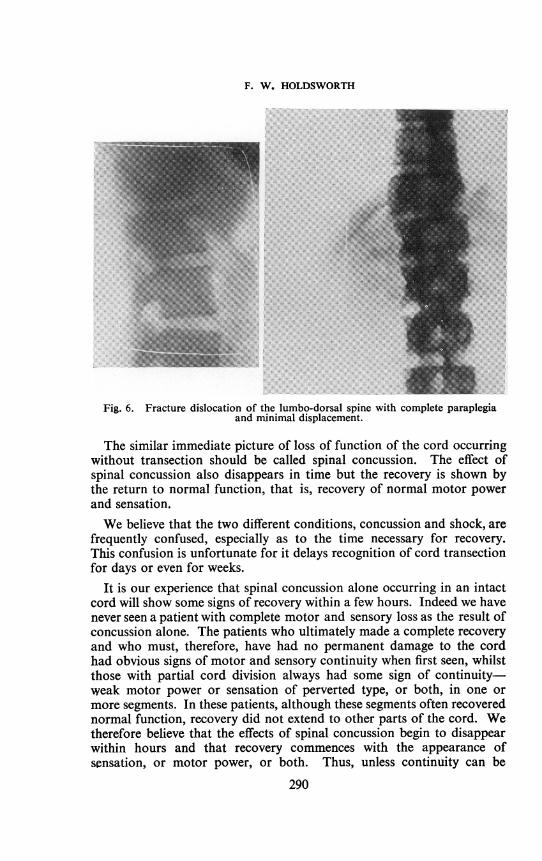
Fig. 6. Fracture dislocation of the lumbo-dorsal spine with complete paraplegiaand minimal displacement.
The similar immediate picture of loss of function of the cord occurringwithout transection should be called spinal concussion. The effect ofspinal concussion also disappears in time but the recovery is shown bythe return to normal function, that is, recovery of normal motor powerand sensation.We believe that the two different conditions, concussion and shock, are
frequently confused, especially as to the time necessary for recovery.This confusion is unfortunate for it delays recognition of cord transectionfor days or even for weeks.
It is our experience that spinal concussion alone occurring in an intactcord will show some signs of recovery within a few hours. Indeed we havenever seen a patient with complete motor and sensory loss as the result ofconcussion alone. The patients who ultimately made a complete recoveryand who must, therefore, have had no permanent damage to the cordhad obvious signs of motor and sensory continuity when first seen, whilstthose with partial cord division always had some sign of continuity-weak motor power or sensation of perverted type, or both, in one ormore segments. In these patients, although these segments often recoverednormal function, recovery did not extend to other parts of the cord. Wetherefore believe that the effects of spinal concussion begin to disappearwithin hours and that recovery commences with the appearance ofscnsation, or motor power, or both. Thus, unless continuity can be
290
TRAUMATIC PARAPLEGIA
demonstrated by the return of some sensation or motor power below thelevel of the cord lesion within a few hours, it is our experience that thecord is totally divided.
Spinal shock, on the other hand, may take days or weeks to disappear,and of course, recovery is never accompanied by sensory or motor recoverybut only by reflex activity and spasticity. Although weeks may elapsebefore full return of reflex function of the isolated cord occurs somereflexes may reappear early or never disappear, and of these the analand bulbo-cavernosus reflexes are the most constant. In 12 patients withcord transection at the S1 level these reflexes never disappeared and in 20they had returned within 12 hours.
Thus, it is our experience that if, on the initial examination within afew hours of injury, there is complete motor and sensory loss below thecord lesion, then no recovery can be expected but if there is any sign inany segment of sensation, however perverted, further recovery can beexpected. The cord is not transected. The presence of reflex activity ofany kind in the segments below the lesion without any sensation or motorpower is certain evidence of cord transection.Thus meticulous neurological examination within a few hours of injury
will determine the pattern of root and cord injury and give a useful guideto the probability or otherwise of cord transection.
.:..?&'''.".' ........................................................... - . ..... 6*:: :. :.::: .%. ...:
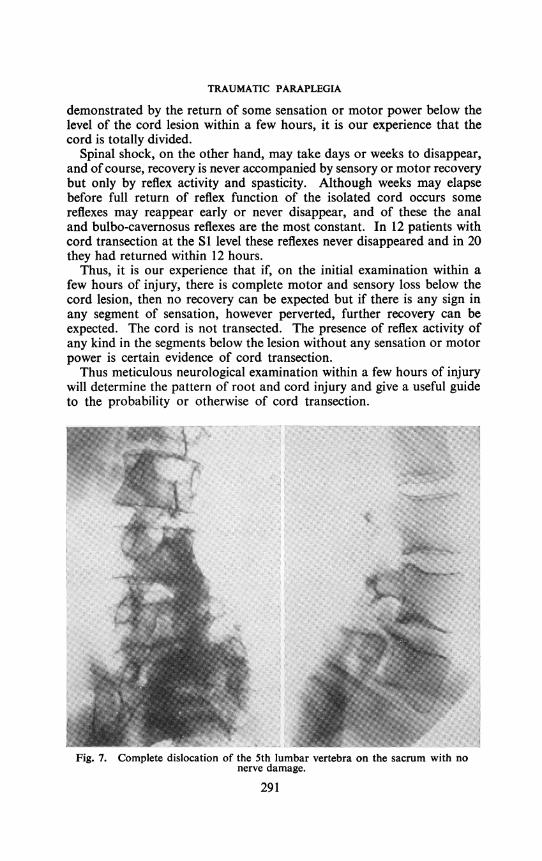
Fig. 7. Complete dislocation of the 5th lumbar vertebra on the sacrum with nonerve damage.
291
F. W. HOLDSWORTH
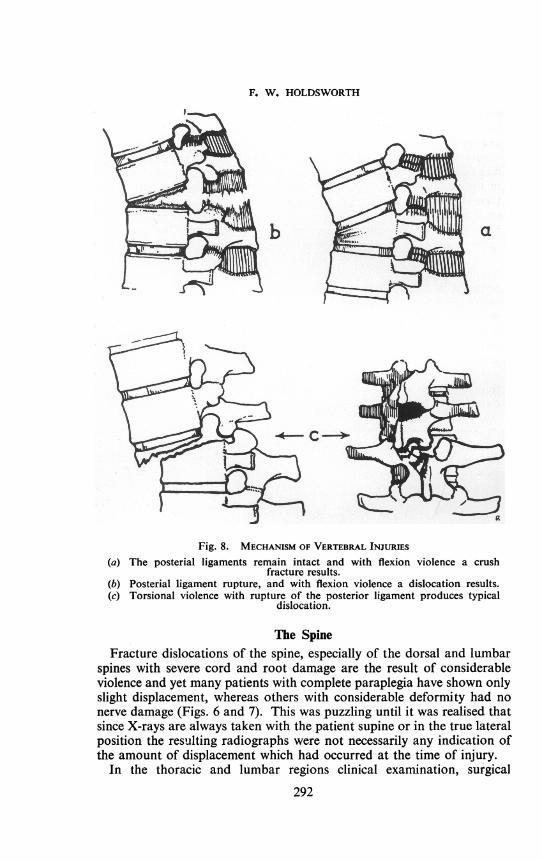
Fig. 8. MECHANISM OF VERTEBRAL INJURIES
(a) The posterial ligaments remain intact and with flexion violence a crushfracture results.
(b) Posterial ligament rupture, and with flexion violence a dislocation results.(c) Torsional violence with rupture of the posterior ligament produces typical
dislocation.
The SpineFracture dislocations of the spine, especially of the dorsal and lumbar
spines with severe cord and root damage are the result of considerableviolence and yet many patients with complete paraplegia have shown onlyslight displacement, whereas others with considerable deformity had nonerve damage (Figs. 6 and 7). This was puzzling until it was realised thatsince X-rays are always taken with the patient supine or in the true lateralposition the resulting radiographs were not necessarily any indication ofthe amount of displacement which had occurred at the time of injury.
In the thoracic and lumbar regions clinical examination, surgical
292
TRAUMATIC PARAPLEGIA
exploration and examination of post mortem specimens showed thatfractures and fracture dislocations of the spine could be divided into stableand unstable types.
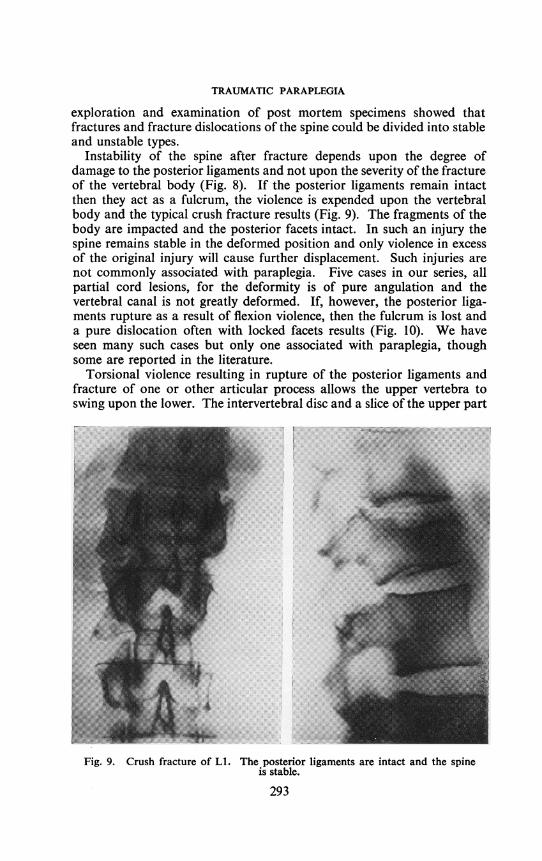
Instability of the spine after fracture depends upon the degree ofdamage to the posterior ligaments and not upon the severity of the fractureof the vertebral body (Fig. 8). If the posterior ligaments remain intactthen they act as a fulcrum, the violence is expended upon the vertebralbody and the typical crush fracture results (Fig. 9). The fragments of thebody are impacted and the posterior facets intact. In such an injury thespine remains stable in the deformed position and only violence in excessof the original injury will cause further displacement. Such injuries arenot commonly associated with paraplegia. Five cases in our series, allpartial cord lesions, for the deformity is of pure angulation and thevertebral canal is not greatly deformed. If, however, the posterior liga-ments rupture as a result of flexion violence, then the fulcrum is lost anda pure dislocation often with locked facets results (Fig. 10). We haveseen many such cases but only one associated with paraplegia, thoughsome are reported in the literature.
Torsional violence resulting in rupture of the posterior ligaments andfracture of one or other articular process allows the upper vertebra toswing upon the lower. The intervertebral disc and a slice of the upper part
... . ..............~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~.......
Fig. 9 ru r . e i n e nc e spine
.... , S _ I | Er ~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~..;.. .. . ;e .... . .3g;1...
is stable.
293
F. W. HOLDSWORTH
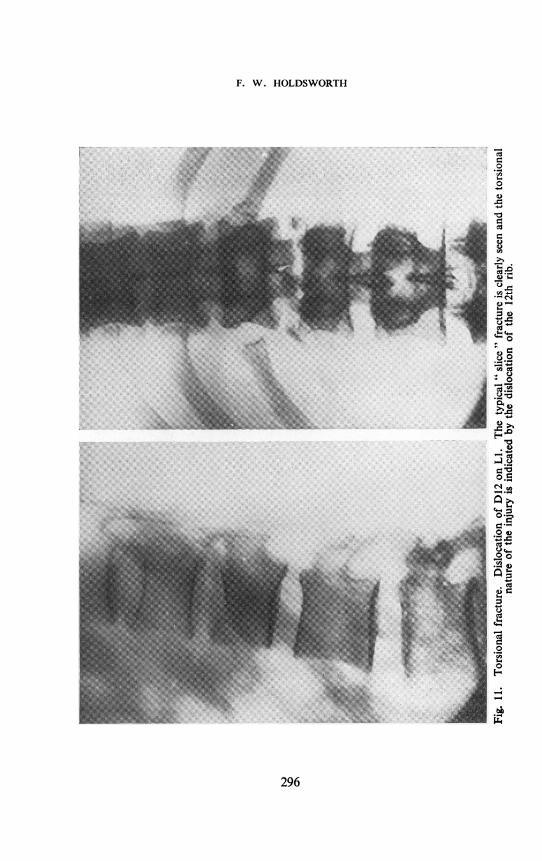
of the lower vertebra is carried with the upper vertebra (Fig. 11). Thisfracture dislocation is very unstable. The displacement can be reducedsimply by laying the patient on his back. Consequently X-rays taken withthe patient supine or in the lateral position with the pelvis and shouldersheld in line often show little displacement whereas if the torsional strainis reproduced gross displacement can be demonstrated. This has beenconfirmed in many cases at operation. This type of unstable torsionalfracture dislocation is the common cause of paraplegia at the dorso-lumbar junction, the cord being crushed between the lamina above andthe vertebral body below. It can be recognised by the lateral shift of thespinous processes together with fracture of one or both articular processesin the radiographs and also by the presence of a palpable gap between theaffected spinous processes due to rupture of the intra and supraspinousligaments.Thus by careful neurological examination and study of the X-rays a
fairly clear picture of the lesion of the nervous system can be obtainedwithin a few hours of the injury. Distinction between root and corddamage can be made accurately and in most cases transection or partialdamage of the cord can be recognised. The spinal injury can be assessedas stable or unstable. Once these facts are established they form guidesto rational early treatment.
TreatmentThe object of treatment in fracture dislocations of the spine with
paraplegia is to restore alignment and stability of the spine in preparationfor future weight bearing, to free the cord and nerve roots from possiblecompression so as to prevent any hindrance to spontaneous recovery andprevent further damage and to make nursing easy so that bedsores maybe avoided.
Restoration of Cord and Root FunctionIf the cord is anatomically divided then no recovery is possible and
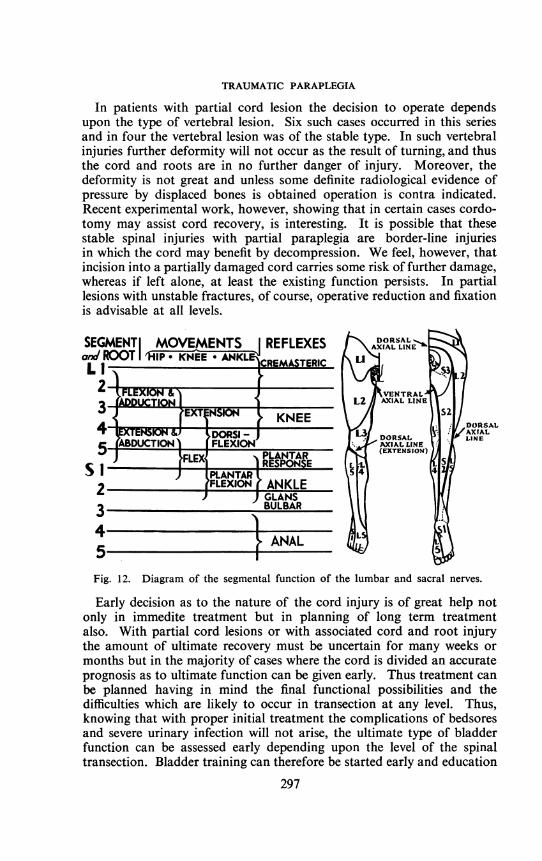
decompression or exploration of the cord is useless. Immediate completeparaplegia, therefore, indicating cord transection is in our experience acontra indication to laminectomy or exploration. Complete paralysisand anaesthesia due to root lesion is different. With root lesions recoveryis always possible and therefore if the root paralysis is extensive and theresulting loss of function from this cause is important then the rootsmust be freed from pressure and protected from further injury. Suchconditions apply in the lumbar spine and at the thoraco-lumbar junctionbut not above this level. Lumbar fracture dislocations result in pureroot lesions whilst in thoraco-lumbar dislocations the whole of the lumbarsegmental paralysis may be due to root damage. The lumbar roots are ofgreat importance for they control flexion and part of extension of the hip,extension of the knee and much of the sensation of the leg (Fig. 12).
Dislocations at or above D1O vertebra can be considered as causingpure cord lesions for the roots involved are few and their functionunimportant.
294
TRAUMATIC PARAPLEGIA
Thus with cord transection and vertebral injury at the thoraco-lumbarjunction or below attention must be focused upon the nerve roots. Ifthe vertebral deformity is severe or encroaches upon the neural canal itmust be reduced, or if, even in the absence of severe deformity thevertebral injury is of the unstable type, the spine must be supported other-wise further damage may occur during the necessary turning of nursing.If the vertebral injury is of the stable type and the canal is not grosslydeformed reduction and support are unnecessary and exploration contraindicated.
Reduction of vertebral deformity by manipulation and support byexternal splinting is often disastrous. The exact position of the damagedarticular facets is difficult and often impossible to determine on theX-rays and in view of this manipulation is bound to be a hit or missaffair fraught with danger. External splinting, such as a plaster bed should,in our opinion, never be used for out of the 16 patients admitted to thecentre late, having been nursed in plaster beds, all had large bedsores whichtook up to two years to heal.E~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~. ... ......... _..
Fig. 10. Dislocation with interlocked facets.
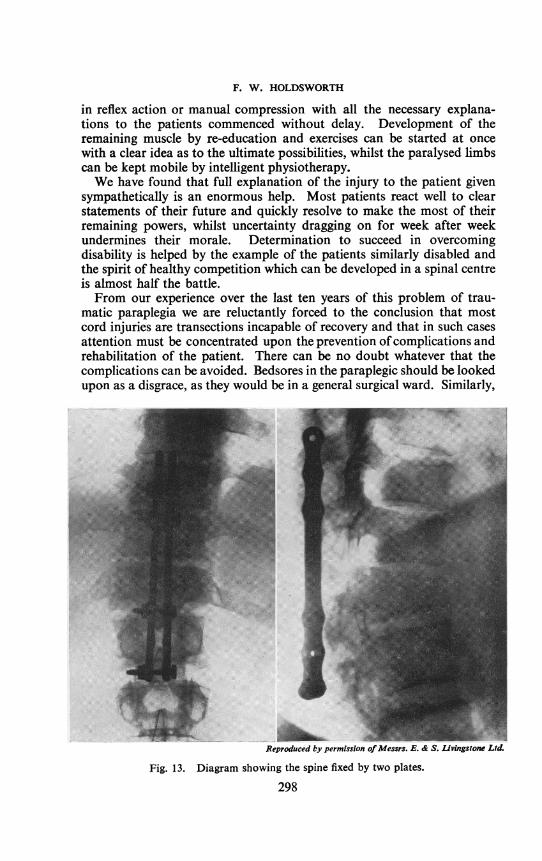
For these reasons in all our cases of this type reduction has been carriedout by open operation and the spine stabilised by internal fixation, that is,by plates bolted to the spinous processes. The operation is safe, simpleand often affords opportunity of direct inspection of the neural canal toensure that no obstruction is present (Fig. 13).
Because routine turning of the patient should start at once, for bedsoresmay be produced by continuous pressure for as little as twelve hours, theoperation should be carried out at once as an emergency.
295
F. W. HOLDSWORTH
0
Ct
.0
ca
ri.
)-4
CT
Cd
'0
* C)o
;.-a
C._
Cu
Cd
F-
.b,X
296
TRAUMATIC PARAPLEGIA
In patients with partial cord lesion the decision to operate dependsupon the type of vertebral lesion. Six such cases occurred in this seriesand in four the vertebral lesion was of the stable type. In such vertebralinjuries further deformity will not occur as the result of turning, and thusthe cord and roots are in no further danger of injury. Moreover, thedeformity is not great and unless some definite radiological evidence ofpressure by displaced bones is obtained operation is contra indicated.Recent experimental work, however, showing that in certain cases cordo-tomy may assist cord recovery, is interesting. It is possible that thesestable spinal injuries with partial paraplegia are border-line injuriesin which the cord may benefit by decompression. We feel, however, thatincision into a partially damaged cord carries some risk of further damage,whereas if left alone, at least the existing function persists. In partiallesions with unstable fractures, of course, operative reduction and fixationis advisable at all levels.
SEGMENT MOVEMENTS REFLEXES AXIAL LINEaxnlROOT KNEE * ANKL CREMASTERICLi1-
4~~~ET eSC KNEEOXEKN &J DORS - )
5 ABDUCTION FLEXIONN1 JFLEM ]~RESPONSE
PI, PLANTAR2 FLEXION ANKLE
) GLANS3 BULBAR
4 15 1NALFig. 12. Diagram of the segmental function of the lumbar and sacral nerves.
Early decision as to the nature of the cord injury is of great help notonly in immedite treatment but in planning of long term treatmentalso. With partial cord lesions or with associated cord and root injurythe amount of ultimate recovery must be uncertain for many weeks ormonths but in the majority of cases where the cord is divided an accurateprognosis as to ultimate function can be given early. Thus treatment canbe planned having in mind the final functional possibilities and thedifficulties which are likely to occur in transection at any level. Thus,knowing that with proper initial treatment the complications of bedsoresand severe urinary infection will not arise, the ultimate type of bladderfunction can be assessed early depending upon the level of the spinaltransection. Bladder training can therefore be started early and education
297
S
F. W. HOLDSWORTH
in reflex action or manual compression with all the necessary explana-tions to the patients commenced without delay. Development of theremaining muscle by re-education and exercises can be started at oncewith a clear idea as to the ultimate possibilities, whilst the paralysed limbscan be kept mobile by intelligent physiotherapy.We have found that full explanation of the injury to the patient given
sympathetically is an enormous help. Most patients react well to clearstatements of their future and quickly resolve to make the most of theirremaining powers, whilst uncertainty dragging on for week after weekundermines their morale. Determination to succeed in overcomingdisability is helped by the example of the patients similarly disabled andthe spirit of healthy competition which can be developed in a spinal centreis almost half the battle.From our experience over the last ten years of this problem of trau-
matic paraplegia we are reluctantly forced to the conclusion that mostcord injuries are transections incapable of recovery and that in such casesattention must be concentrated upon the prevention ofcomplications andrehabilitation of the patient. There can be no doubt whatever that thecomplications can be avoided. Bedsores in the paraplegic should be lookedupon as a disgrace, as they would be in a general surgical ward. Similarly,
Reproduced by permission of Messrs. E. & S. Livingstone Ltd.
Fig. 13. Diagram showing the spine fixed by two plates.
298

TRAUMATIC PARAPLEGIA
acute uncontrollable urinary sepsis with pyuria, stones, hydronephrosisand renal failure is an indication of careless treatment.To discuss as the treatment of paraplegia the healing of bedsores,
methods of overcoming severe urinary infection, correction of spinaldeformity and the mobilisation of stiff joints is as out of date as to con-sider only the treatment of severe generalised peritonitis in a discussion onacute appendicitis.To avoid these complications simply requires meticulous care and
nursing, which can only be achieved in special centres by a staff properlytrained in this work. A spinal centre should be ready and willing toaccept cases at once. There must be no delay in admission, for if there ismost cases bring their complications with them, and the average stay inhospital is about two years instead of nine months and much unnecessarywork must be done. A spinal centre is an emergency centre and mustalways have beds available. In Sheffield we have a centre of 50 beds whichis large enough to deal with the paraplegias occurring in a heavy industrialarea with a population of about two million. All the hospitals in thedistrict willingly co-operate, either sending the patient at once or, incertain cases, within a few days, having treated the patient exactly as weadvise before admission. We also admit some late cases, but theseadmissions are never allowed to fill the beds, a recent case being givenabsolute priority.With modern transport and with goodwill between hospitals the
establishment of six or eight centres in the country should present nodifficulties and should go far to ensure correct treatment for thesepatients. It would also stimulate research in the many problems ofparaplegia due to injury.
REFERENCESCOBB, S., and COLEMAN, C. C. (1921) Arch. Surg. 3, 132.COHEN. H.. and ROGERS, L. (1941) in Bailey's Surgery of modern warfare, p. 711.COLEMAN, C. C. (1925) J. Amer. med. Ass. 85, 1,106.
and MEREDITH, J. M. (1938) J. Amer. med. Ass. 111, 2,168.FRAZIER, C. H., and ALLEN, A. R. (1918) Surgery ofthe spine and spinal cord. Appleton,
New York.HEAD, H. (1920) Studies in neurology. Oxford University Press. 2, 491.HOLDSWORTH, F. W., and HARDY, A. (1953) J. Bone J. Surg., B. 35, 540.HOLMES, G. (1915) Brit. Med. J. 2, 769; 815; 855.MARTIN, J. (1947) Surg. Gynec. Obstet. 84, 403.MAYFIELD, F. H., and CAZAN, G. M. (1942) Amer. J. Surg. 55, 317.MUNRo, D. (1945) Clinics, 4, 448.NAFFZIGER, H. C. (1938) J. Bone J. Surg. 20, 444.NICOLL, E. A. (1949) J. Bone J. Surg., B. 31, 376.REYNOLDS, E. S. (1895) Brain, 18, 175.RIDDOCH, G. (1917) Brain, 40, 264.SCARF, J. E., and POOR, J. L. (1946) J. Neurosurg. 3, 285.SHERRINGTON, C. S. (1906) The integrative action of the nervous system. Harvard Univer-
sity Press.WALSHE, F. M. R. (1914) Brain, 37, 269.WATSON-JONES, R. (1943) Fractures andjoint injuries. Livingstone, Edinburgh. p. 348.
299