Embed Size (px)
Citation preview

Treating Depression with Behavior Therapy:
The Implementation of Behavioral Activation
Christopher Martell, Ph.D., ABPPIndependent Practice and University of Washington
Sona Dimidjian, Ph.D.University of Colorado
as told by
Steven D. Hollon, Ph.D.
Vanderbilt University

AcknowledgementsResearch Team:
Michael AddisSandra Coffman David Dunner Robert GallopSteve Hollon Bob KohlenbergChristopher Martell Karen Schmaling
Research Staff: David Atkins
Patty Bardina
Carolyn Bea
Chris Budech
Jackie Gollan
Eric Gortner
David Markley
Melissa McElrea
Joe McGlinchey
Evelyn Mercier
Kim Nomensen
Shireen Rizvi
Lisa Roberts
Elizabeth Shilling
Mandy Steiman
Dan Yoshimoto
Clinical Staff:Sandra Coffman
Linda Cunning
Steve Dager
Kerri Halfant
Helen Hendrickson
Ruth Herman-Dunn
David Kosins
Tom Linde
Christopher Martell
Peggy Martin
Steve Sholl
Alan UnisSupport:NIMH & GlaxoSmithKline

What is Behavioral Activation?- Structured, brief psychosocial approach- Based on premise that problems in
vulnerable individuals' lives and behavioral responses reduce ability to experience positive reward from their environments
- Aims to systematically increase activation such that patients may experience greater contact with sources of reward in their lives and solve life problems
- Focuses directly on activation and on processes that inhibit activation, such as escape and avoidance behaviors and ruminative thinking
Peter M. Lewinsohn
1970s
A Brief History of the Evidence Base for Behavioral Activation

Lewinsohn
• Early models highlighted the role of lack of response-contingent reinforcement for non-depressed behavior
• Decrease in frequency or range of reinforcing stimuli or increase in frequency of punishment depression

Brief History: Ferster
“I think the conceptual formulation as well as the treatment of depression really depend upon focusing on the behaviors the patient is not engaged in … the most obvious aspect of depression is a marked reduction in the frequency of certain kinds of behavior and an increase in the frequency of others, usually avoidance and escape”
Ferster, 1974

Peter M. Lewinsohn Aaron T. Beck
19791970s

BA subsumed within CT
• “…the ultimate aim of these techniques in cognitive therapy is to produce change in the negative attitudes” (Beck et al., 1979, p.118).
• “The key point is that even when cognitive therapists are focusing on behaviors, they do so within the context of a larger model that relates those actions to the beliefs and expectations from which they arise and view them as an opportunity to test the accuracy of those underlying beliefs” (Hollon, 1999, p.306).
Positive outcomes in CT may be dependent on competence level of therapist (DeRubeis et al., 2005; Elkin et al., 1989)

Peter M. Lewinsohn
1996
Neil S. JacobsonAaron T. Beck
19791970s
What accounts for the efficacy of cognitive therapy?
Peter M. Lewinsohn
1996
Neil S. JacobsonAaron T. Beck
19791970s

Automatic Thought Strategies
Behavioral Activation Strategies
Core Belief Strategies
Facilitative Strategies
Cognitive Therapy for Depression
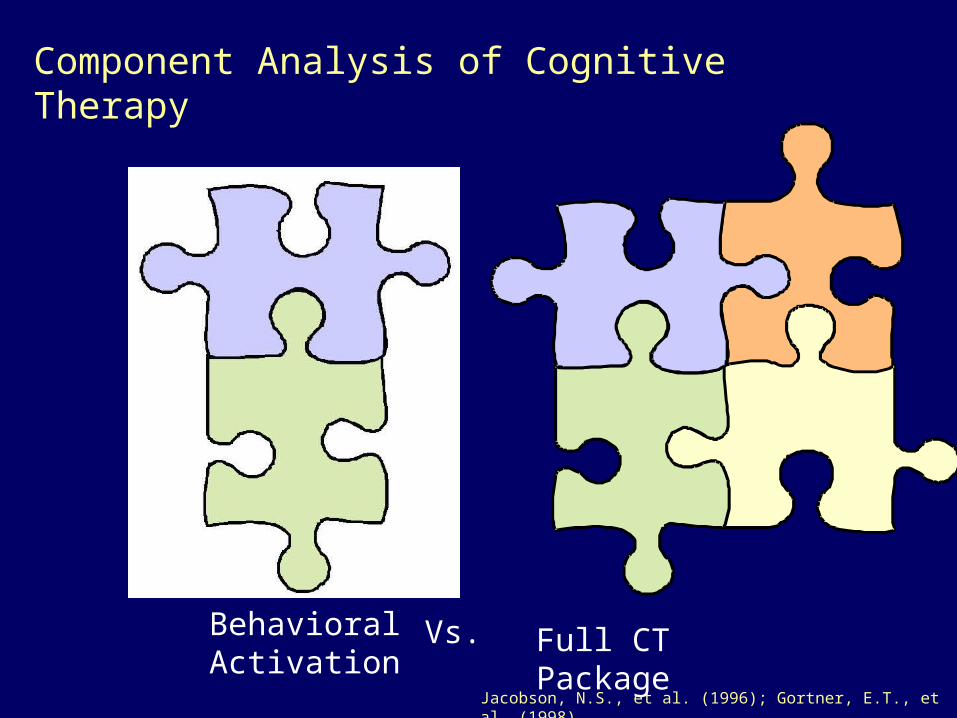
Behavioral Activation
Vs.
Jacobson, N.S., et al. (1996); Gortner, E.T., et al. (1998)
Full CT Package
Component Analysis of Cognitive Therapy

Acute Findings
0
5
10
15
20
25
30
35
Pre Post
Mea
n B
DI
CognitiveTherapyBehavioralActivation
Component Analysis of CT
Jacobson, N.S., et al. (1996); Gortner, E.T., et al. (1998)

Acute Findings
0
5
10
15
20
25
30
35
Pre Post
Mea
n B
DI
CognitiveTherapyBehavioralActivation
Follow Up Findings
0
10
20
30
40
50
60
70
80
90
100
% S
urv
iva
l (T
wo
Ye
ars
)
CognitiveTherapy
BehavioralActivation
Jacobson, N.S., et al. (1996); Gortner, E.T., et al. (1998)
Component Analysis of CT

Behavioral Activation
Findings of the component analysis study led to an expansion of BA into a stand-alone model, not solely defined by proscription of cognitive interventions (Jacobson et al., 2000; Martell et al., 2001)
Linked to earlier behavioral work on depression (Ferster, 1973; Lewinsohn, 1974)

Acute and Follow-up Design
BA
ADM-CM
CT
Acute Phase Continuation Phase Follow-Up Phase
ADM continuation
Placebo withdrawal
Intake Wk. 8 Wk. 16 Month 12 Month 24
Follow-up evaluations
Follow-up evaluations
Follow-up evaluations
Follow-up evaluations
PLA-CM
(N=43)
(N=45)
(N=100)
(N=53)

0.570.06
8.06
8.65
5.01
0.220.58
6.07
0.06
0.00
1.00
2.00
3.00
4.00
5.00
6.00
7.00
8.00
9.00
10.00
BA CT ADM
Mea
n Sc
ale
Scor
e
BEH
COG
PHARM
Assessment of Treatment AdherenceAssessment of Treatment Adherence
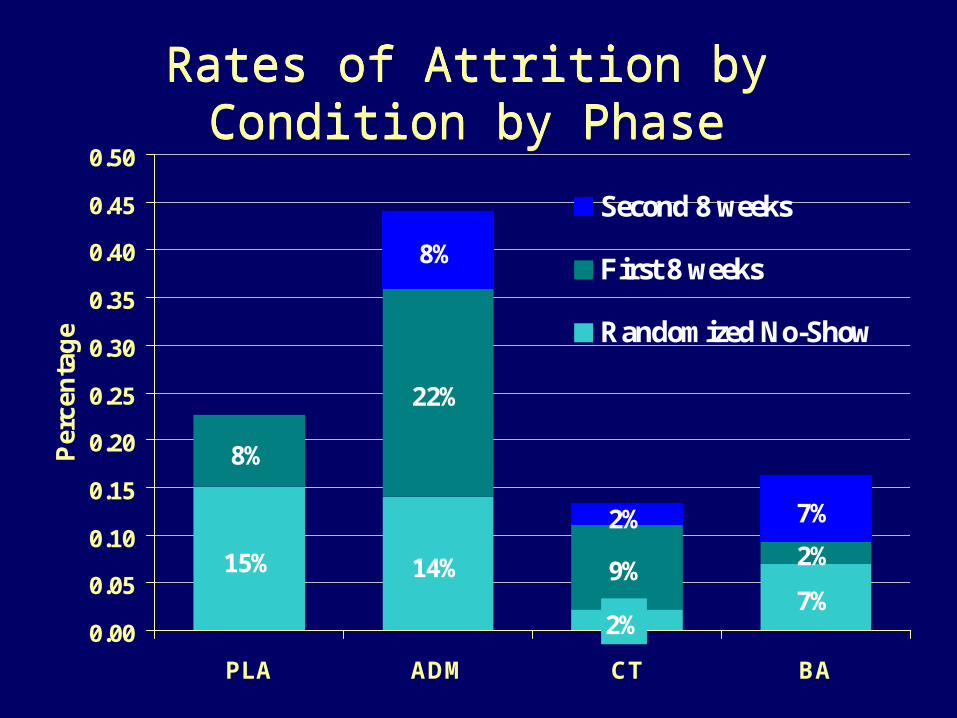
15% 14%7%
8%
22%
9%
8%
7%
2%
2%
2%
0.00
0.05
0.10
0.15
0.20
0.25
0.30
0.35
0.40
0.45
0.50
PLA ADM CT BA
Per
cen
tag
e
Second 8 weeks
First 8 weeks
Randomized No-Show
Rates of Attrition by Condition by PhaseRates of Attrition by Condition by Phase

5
10
15
20
25
30
35
40
Intake Mid-Tx Post-Tx
CT Hi
CT Lo
BA Hi
BA Lo
ADM Hi
ADM Lo
Mean BDI across acute treatment Mean BDI across acute treatment

5
10
15
20
25
Intake Mid-Tx Post-Tx
CT Hi
CT Lo
BA Hi
BA Lo
ADM Hi
ADM Lo
Mean HRSD across acute treatment Mean HRSD across acute treatment

2%
8%
0%
28%
48%
8% 8%
0%
37%
7%4%
36%
0.00
0.10
0.20
0.30
0.40
0.50
0.60
0-10 11-20 21-30 31-63
BDI
Per
cen
tag
e
ADM (N=57)
CT (N=25)
BA (N=25)
Extreme Non-Response (BDI) Extreme Non-Response (BDI)
Extreme Non-Response

0
0.2
0.4
0.6
0.8
1
Months (following end of active treatment)
% S
urv
ival
ADM-Placebo(n=21)
ADM-ADM (n=28)
Prior BA (n=27)
Prior CT (n=30)
RelapseRelapse RecurrenceRecurrence
Prevention of Relapse Following Successful Treatment- all treatment conditionsPrevention of Relapse Following Successful Treatment- all treatment conditions

0
500
1000
1500
2000
2500
3000
3500
4000
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16
Months in Treatment
Co
st
in D
olla
rs
BA/ CT
ADM-ADM
Cumulative Direct Costs of Continuation ADM and BA/CT
Note: These costs are based on $100/ session in BA and CT, versus $75/ session in Continuation ADM, plus drug costs of $125/ month; ADM sessions occurring x2/ month for 2 months & monthly thereafter.
Note: These costs are based on $100/ session in BA and CT, versus $75/ session in Continuation ADM, plus drug costs of $125/ month; ADM sessions occurring x2/ month for 2 months & monthly thereafter.

Putting it all together…
• BA emerges as a strong and promising treatment
• Challenges the idea that medication is required to treat moderately to severely depressed patients
• Challenges the idea that directly modifying cognition is necessary to treat depression
• Limitations (BA, CT, ADM)

Points of Convergence • Consistent with earlier behavioral literature (e.g.,
Lewinsohn; Ferster), more recent behavioral and activation oriented studies (e.g., Hopko et al., 2003; Stathopoulou et al., 2006 ), and dismantling studies across other disorders/ages (e.g., Scogin et al., 1989)
• Consistent with early emphasis in CT on behavioral strategies for more severely depressed patients (Beck et al., 1979)
• Consistent with key components of other behavioral treatments (DBT; Linehan, 1993; ACT; Hayes, Strosahl, & Wilson, 1999) and recent conceptualizations of integrative treatments for Axis I disorders (Barlow, Allen, & Choate, 2004)


Key elements of BA
• Stylistic strategies • Structuring strategies (including orienting to
treatment)• Assessment strategies (individualizing primary
treatment targets through behavioral assessment)
• Activation strategies (activity structuring and scheduling)
• Targeting avoidance, routine disruption, rumination

Course of BA• Orient to treatment
– Treatment rationale, including conceptualization of depression and primary treatment strategies
– Role of therapist/patient
• Develop treatment goals• Individualize treatment targets• Repeated application and troubleshooting of
activation and engagement strategies• Reviewing and consolidating treatment gains

Stylistic Strategies• Validating:
– Interested; Accurately reflects; Genuine; Maintains hope and optimism about change
• Reciprocal/responsive to client – Collaborative; Open to the client’s influence;
Awake to client’s behavior in session and modifies interventions as appropriate; Warm
• Non-judgmental and matter of fact in interactions with client
– Everything is useful, provides information; Curious—holds a problem solving mindset in relation to all new behavior


Structure of Sessions
• Set collaborative agenda
• Review homework
• Review weekly activities
• Troubleshoot problem behaviors
• Assign new homework
• Ask for feedback
Treatment Rationale • Emphasize relationships between
environment, mood, and activity• Highlight vicious cycle that can develop
between depressed mood, withdrawal/avoidance, and worsened mood
• Suggest activation as a tool to break this cycle and support problem solving
• Emphasize an “outsidein” approach: act according to a plan or goal rather than a feeling or internal state

BA Case Conceptualization
Life events
Less Rewarding Life
Sad, tired, worthless, indifferent, etc.
Stay home, stay in bed, watch TV, withdraw from social contacts, ruminate, etc.

BA Case Conceptualization
Life events
Less Rewarding Life
Sad, tired, worthless, indifferent, etc.
Stay home, stay in bed, watch TV, withdraw from social contacts, ruminate, etc.
Loss of friendships, conflict with supervisor at work, financial stress, poor health, etc.

TG 1-2, 2-2
Adolescents Taking Action Sessions 1 & 2: Getting Started
1st by identif ying what makes you feel down 2nd by learning how to tackle problems 3rd by working together with your therapist to take small steps, get active, accomplish your goals, and
Depression
What Does Behavioral Activation Mean?
Depression is a vicious cycle
Your lif e is more stressful. You begin to f eel tired, bored….lif e gets harder, you do less, pull away and may blame yourself f or not doing more….it gets harder to do things. This can create more problems with school, parents, f riends…….
BUT Behavioral Activation can break this cycle by:
BUI LD THE LI FE YOU
WANT!

Address common myths about activation and change
• Will-power or “Nike” model of change

Address common myths about activation and change
• Will-power or “Nike” model of change
• Emphasize– Role of the therapist– Focused activation
based on careful behavioral analyses
– Graded task assignment
– Difficulty of change


Individualizing activation targets
• Conduct detailed examination of what is getting in the way of feeling better
• Sounds simple, and yet in practice, we often lack awareness of these relationships

• Identify and set goals
• Define and specifically describe problems in behavioral terms
• Assesses consequences of behavior
• Examine behavioral patterns
Key Assessment Strategies
Goal Setting
• Ultimate goal of treatmentClients modify their behavior to increase contact with sources of positive reinforcement
• Typical goals relate to changing avoidance patterns and routine disruption and to changing environmental context
• Focus on acting from the “outside in”• Set priorities for long and short-term goals• Figure out what behaviors are needed to reach
goal—what, when, where, etc. Be focused, specific, and concrete!

• Basic questions:– What is maintaining the depression?– What is getting in the way of engaging and
enjoying life?– What behaviors are good candidates for
maximizing change?
• Activity/mood monitoring provides the essential information
• Utilize basic behavioral principles to answer these questions
Key Assessment Strategies
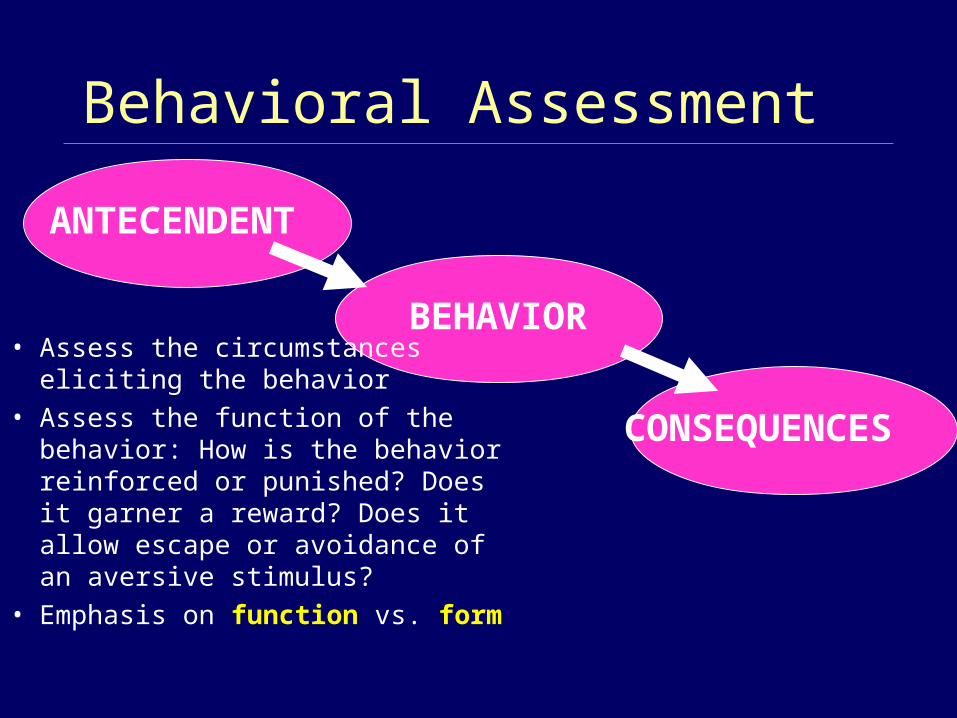
Behavioral Assessment
• Assess the circumstances eliciting the behavior
• Assess the function of the behavior: How is the behavior reinforced or punished? Does it garner a reward? Does it allow escape or avoidance of an aversive stimulus?
• Emphasis on function vs. form
ANTECENDENT
BEHAVIOR
CONSEQUENCES

Two Types of Conditioning
• Classical Conditioning: paired stimuli take on similar functions– a neutral stimulus such as a hospital paired with
grief following a loved one’s death in the hospital takes on the properties of grief, such that seeing a hospital evokes similar feelings
• Operant Conditioning: behavior is learned according to the consequences that maintain it

Understanding consequences
• Negative reinforcement: the likelihood of a behavior is increased by the removal of something from the environment (usually an aversive condition)– Watching television is negatively reinforced by reduction of
painful emotions– Negative reinforcement contingencies are frequently targets
in BA for depression• Positive reinforcement: the likelihood of a behavior is
increased by the addition of something in the environment– Going to bed early is positively reinforced by family member
offering empathy and support• Punishment: the extinguishing of a behavior by the
addition of an aversive consequence in the environment– Asking for help is punished by a judgmental and critical
reaction from others

Nuts and bolts of behavioral analysis in BA…
• The Activity Chart – Central tool!
• What does a BA therapist focus on when reviewing activity schedules?

Typical Questions to Guide Review
• What would the client be doing if he or she were not depressed (e.g., working, managing family responsibilities, exercising, socializing, engaging in leisure activities, eating, sleeping, etc.)?
• What is being avoided or from what is the client pulling away? How are these patterns related to mood?
• What is the relationship between specific activities and mood?
• What is the relationship between specific life contexts or problems and mood?
• Is the client engaging in a wide variety of activities or have his or her activities become narrow?
• Are there disruptions in normal routines?



Exercise #2: Activity Monitoring
1. Recording: Write down your activities and moods for 1-2 typical days over the past week; include enough detail to allow your partner can begin to notice some relationships
2. Role Play: Practice being the therapist and reviewing the completed log; identify “if…then” relationships between activity and mood; look for variability; help your client begin to notice these relationships

The challenge!
“There is only a modest correlation between intention and behavior. Most often, people have good intentions and fail to act on them.” (Gollwitzer, 1999)

• Problem definition
• Generate and evaluate solutions
• Practice new behaviors in session as appropriate
• Skills training as appropriate
• Troubleshooting
Problem Solving

• Increase pleasure• Increase mastery• Increase approach (vs. avoidance)
Activity Scheduling

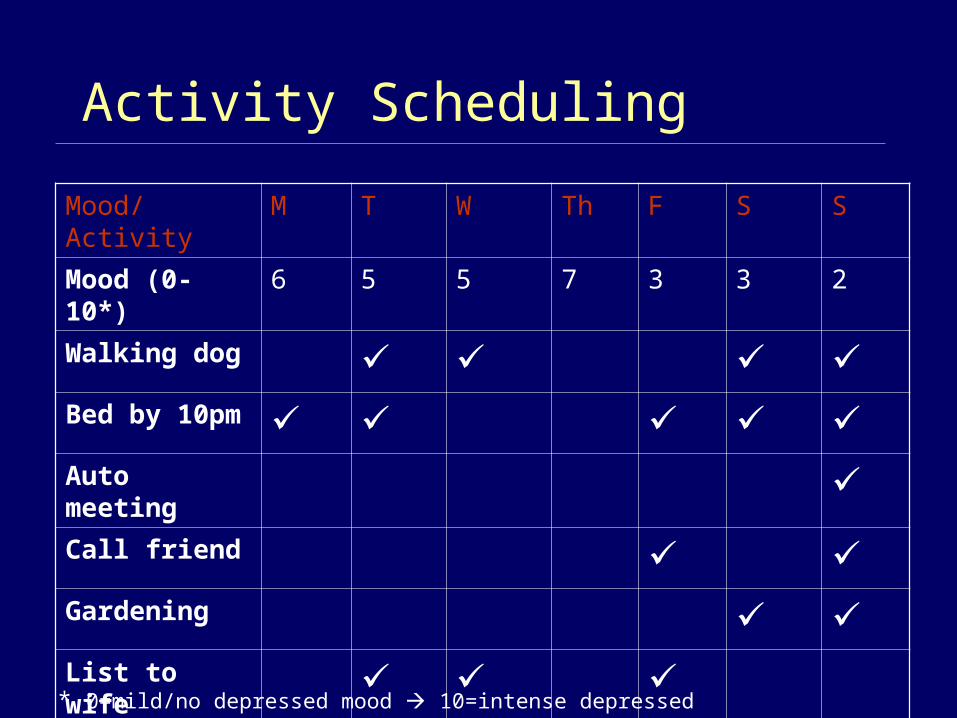
Activity Scheduling
Mood/Activity M T W Th F S S
Mood (0-10*) 6 5 5 7 3 3 2
Walking dog Bed by 10pm Auto meeting Call friend Gardening List to wife
* 0=mild/no depressed mood 10=intense depressed mood
• Break down activities into parts• Assign simple to more complex tasks in
a stepwise fashion• Design assignments so that early
success is guaranteed• Goal is not to accomplish all parts of the
activity—rather, to get started, increase activation, disrupt avoidance
• Completing one component will increase likelihood of completing others
Activity Structuring: Grading Tasks

Qualities of Effective Action Plans: Opposite Action (Linehan, 1993)
Emotions love themselves– All emotions have “action urges” – what one wants to
do or say when feeling an emotion– Action urges tend to maintain or intensify emotions
If you want to change anemotion, act opposite to the action urge
Opposite action works best if you do it “ALL THE WAY” – throwing yourself into andparticipating fully inthe opposite action
• Clearly tied to the essence of the problem (not random or arbitrary)
• Target avoidance, withdrawal, approaching important problems/modifying life context
• Includes activities that are opposite to the action urges accompanying depression
• Based on creative and collaborative problem solving
• Utilizes contingency management as needed to promote change
Qualities of Effective Action Plans
• Clear and specific (adequately detailed information about what, when, where, etc.); do you and the patient know what the plan is when the session ends?
• Do-able (adequately graded into component parts, assigning simple to more complex parts in a stepwise fashion, structured so that early success is nearly guaranteed)
Qualities of Effective Action Plans

• Informed by adequate troubleshooting--consideration of potential barriers; anything that might get in the way?
• Informed by what’s needed to maximize commitment to implementation -- public commitment, getting started in session, reminders during the week, explicit linking to long-term goals
• Includes plans for how to make new behaviors routine
• Returns to treatment rationale as needed
Qualities of Effective Action Plans

• TRAP/TRAC
• ACTION
Acronyms to Organize Action Plans



TRAP/TRAC
• T- Trigger (demands at work)
• R- Response (depressed mood/hopelessness)
• AP- Avoidance Pattern (leave work; stay at home)
• T-Trigger (demands at work)
• R- Response (depressed mood/hopelessness)
• AC- Alternative Coping (approach behaviors using graded tasks)

Trigger Response Avoidance-Pattern

Trigger Response AlternativeCoping

ACTION Strategy• A=Assess How will my behavior affect my depression?
Am I avoiding? What are my goals in this
situation?
• C=Choose I know that activating myself will increase my
chances of improving my life situation and mood.
Therefore, if I choose not to self-activate, I am choosing to take a break.
• T=Try Try the behavior I have chosen.
• I=Integrate Integrate any new activity into my daily routine.
• O=Observe Observe the result. Do I feel better or worse?
Did this action allow me to take steps toward improving my situation?
• N=Never Never give up.

• BA is not a one-size-fits-all therapy
• Not all clients will be inactive
• Need to look for subtle forms of avoidance
• Engagement as activation
• Experiencing rather than avoiding negative feelings
Experiential Avoidance (Hayes et al., 1996)
Routine Regulation
• Work with patient to develop and follow regular routine for basic life activities—eating, working, school, sleeping.
• Can only evaluate new behaviors after implemented for a period of time—make them routine, then evaluate– Use activity logs– Use the ACTION strategy

Exercise #3: Modifying Avoidance
• Break into pairs• Help your partner…
• Identify a goal for learning at ABCT (or more broadly getting the most out of your experience)
• Identify an avoidance pattern that might typically become a barrier to moving in the direction of this goal
• Identify an action plan for alternative coping that can be implemented over the next 3 days
• Troubleshoot potential problems that would interfere with the action plan
• You can use the TRAP/TRAC form or a blank activity schedule if useful




The Trouble with Ruminating
• What is ruminating?– “People with a ruminative response style think
repetitively and passively about their negative emotions, focusing on their symptoms of distress ("I feel so lousy," "I just can't concentrate") and worrying about the meanings of their distress ("Will I ever get over this?“).”
• Ruminative response styles predict higher levels of depressive symptoms over time, onset of new episodes, and episode chronicity
Nolen-Hoeksema, 2000

Targeting Ruminating
• Monitor and assess
• Focus on context and consequences of ruminating, not on the content of ruminative thoughts

Targeting Ruminating
• Practice with “attention to experience” strategies
• Notice colors, smells, noises, sights, relation to others, etc.• Notice elements of tasks (parenting, work)
• Select activities that are associated with high engagement
• Highlight negative consequences of ruminating• Be alert for partial activation and identify
specific behaviors that would maximize full engagement

A Focus on the Content of Thinking
“I was depressed all day yesterday because I was thinking about how my sister really doesn’t love me.”* What is the evidence that this thought is accurate?
* What would it mean if it were true?
* Can you think of another way to interpret what your sister said?
* Why must everyone love you?
A Focus on the Context and Consequences of Thinking
“I was depressed all day yesterday because I was thinking about how my sister really doesn’t love me.”
* When did you start thinking that?
* How long did it last?
* What were you doing while you were thinking that?How engaged were you with the activity, context, etc.?
* What were consequences of thinking about that? What might be the function?
Relapse Prevention
• Consolidate Treatment gains– What has been helpful– What has been learned
• Plan for future problems– What targets have been identified– What new responses to targets are practiced

Additional Resources Jacobson, N. S., Martell, C. R., & Dimidjian, S. (2001). Behavioral
activation treatment for depression: Returning to contextual roots. Clinical Psychology: Science and Practice, 8, 255-270.
Martell, C. R., Addis, M. E., & Jacobson, N. S. (2001). Depression in context: Strategies for guided action. New York: Norton and Co.
Addis, M.E., & Martell, C.R. (2004). Overcoming Depression One Step at a Time: The New Behavioral Activation Approach to Getting Your Life Back. New York: New Harbinger Press.
Dimidjian, S., Hollon, S.D., Dobson, K.S., Schmaling, K.B., Kohlenberg, R., Addis, M., Gallop, R., McGlinchey, J., Markley, D., Gollan, J.K., Atkins, D.C., Dunner, D.L., & Jacobson, N.S. (2006). Randomized trial of behavioral activation, cognitive therapy, and antidepressant medication in the acute treatment of adults with major depression. JCCP, 74 (4), 658-670.
Dimidjian, S., Martell, C.R., Addis, M.E., Herman-Dunn, R. (in press). Behavioral activation. In D. H. Barlow (Ed.), Clinical Handbook of Psychological Disorders, 4th Edition. NY: Guilford Press.