Embed Size (px)
Citation preview

Treatment of respiratory tract infections with fluoroquinolones in Belgium
S. Simoens
Research Centre for Pharmaceutical Care and Pharmaco-economics, Katholieke Universiteit Leuven, Onderwijs en Navorsing 2, bus 521, Herestraat 49, 3000 Leuven, Belgium
Belgian data on the treatment of respiratory tract infections with antibiotics in ambulatory care showed that fluoroquinolone use remains well controlled. Belgian guidelines have recommended moxifloxacin for CAP outpatients with comorbid conditions or outpatients in whom infection with atypical pathogens needs to be considered. Moxifloxacin is recommended in case of IgE-mediated ß-lactam allergy or severe intolerance to ß-lactam antibiotics when treating COPD exacerbations or when treating upper respiratory tract infections on the rare occasion that antibiotic treatment is warranted. The MIC distribution of moxifloxacin and levofloxacin in S. pneumoniae isolates remained stable during 2004-2009 and resistance to moxifloxacin and levofloxacin was low (≤ 1%) in Belgium. As the cost-effectiveness of moxifloxacin is influenced by the causative pathogens involved and resistance patterns, it may be advisable to identify patient subgroups in which moxifloxacin is cost-effective.
Keywords fluoroquinolones; respiratory tract infections; Streptococcus pneumoniae; consumption; resistance.
1. Introduction
Respiratory tract infections are accompanied by significant morbidity, impaired quality of life, and mortality. The World Health Organisation estimated that respiratory tract infections generated 94.6 disability-adjusted life years lost worldwide and were the fourth major cause of mortality, responsible for 4.0 million deaths or 6.9% of the global number of deaths in 2002 [1]. Respiratory tract infections are a primary driver of hospital admissions and impose a substantial economic burden on society in terms of direct health care costs (costs of medication, physician office visits, emergency room visits and hospitalisation) and indirect costs (costs of productivity losses) [2]. Antibiotics have made a significant contribution to improving the health of patients suffering from respiratory tract infections. The scientific literature and international guidelines recommend antibiotic therapy in patients with acute exacerbations of chronic obstructive pulmonary disease (AECOPD) (Gold stages II to IV and/or acute respiratory failure) and community-acquired pneumonia (CAP) [3-5]. Also, antibiotics appear effective in improving cure rates and decreasing duration of some upper respiratory tract infections in patients who have a microbiological diagnosis of bacterial infection or severe disease [6]. In fact, the added value of antibiotics for therapeutic purposes has been so persuasive that many older antibiotics never underwent controlled clinical trials [7]. On the other hand, systematic reviews published by the Cochrane Collaboration have found no benefit of antibiotic therapy in upper respiratory tract infections because the cause of such infections is generally viral and, thus, the use of antibiotics is not indicated [8,9]. A range of antibiotics such as penicillins, macrolides, cephalosporins, co-trimoxazol, tetracyclines, and fluoroquinolones can be used to treat respiratory tract infections in ambulatory care. Fluoroquinolones are a class of antibiotics developed in the 1980s. Fluoroquinolones initially demonstrated their effectiveness against Gram-negative bacteria (H. influenzae, Moraxella catarrhalis), whereas newer fluoroquinolones have increased activity against Gram-positive bacteria, including S. pneumoniae, and against atypical micro-organisms (Mycoplasma pneumoniae, Chlamydophila spp. and Legionella pneumophilia). Moreover, moxifloxacin has increased activity against Staphylococcus aureus and anaerobes. In an era of spiraling health care costs and limited resources, policy makers and health care payers are concerned about the costs of antibiotics in addition to their effectiveness. Rising consumption of antibiotics is contributing to increasing pharmaceutical expenditure [10]. Furthermore, the quality of antibiotic use has been questioned, with studies suggesting that up to 50% of antibiotic use is inappropriate [11,12]. For instance, a Belgian survey of general practitioners and pulmonologists compared actual management of AECOPD with GOLD recommendations [13]. The authors concluded that antibiotics were overused in the treatment of exacerbations and that their use should be limited to those exacerbations where bacterial infection is likely to be present. Inappropriate use of antibiotics contributes to the appearance of resistance [14]. Antibiotic resistance is associated not only with worse clinical outcomes, but also with higher treatment costs [15]. For instance, a survey of 122 U.S. hospitals revealed that antibiotic resistance was the most commonly cited reason for increases in antibiotic expenditure [16]. The resistance of respiratory pathogens to commonly prescribed antibiotics such as macrolides and tetracyclines is relatively high in Belgium, and there has been some concern about the decrease in susceptibility of S. pneumoniae to ß-lactam antibiotics [17]. Resistance to fluoroquinolones is still low, but if these antibiotics become more widely used in the community for the treatment of respiratory tract infections, resistance is expected to spread with the potential
338 ©FORMATEX 2011
Science against microbial pathogens: communicating current research and technological advances A. Méndez-Vilas (Ed.)______________________________________________________________________________
induction of cross-resistance even to the new fluoroquinolones. Resistance may also develop as a result of unnecessary antibiotic therapy and inappropriate dose, duration and/or frequency of administration of antibiotics. The aim of this chapter is to address specific aspects of the treatment of respiratory tract infections with fluoroquinolones in ambulatory care in Belgium by: a) mapping fluoroquinolone consumption in ambulatory care in Belgium over time and breaking down consumption by infection type; b) discussing the role of fluoroquinolones as recommended by Belgian guidelines on the treatment of respiratory tract infections in ambulatory care; c) documenting the level of in vitro resistance of S. pneumoniae to fluoroquinolones in Belgium over time; and d) reviewing the current evidence on the cost-effectiveness of treating respiratory tract infections with fluoroquinolones in ambulatory care in Belgium.
2. Fluoroquinolones and consumption
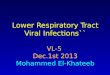
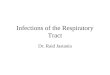
In Belguim, fluoroquinolones made up 9% of the average annual volume of antibiotic consumption [18]. The share of fluoroquinolones increased from 7% in 1993 to 12% in 2003, but then fell to 10% in 2009. The volume of fluoroquinolone consumption increased from 1.75 defined daily doses per 1,000 inhabitants per day (DID) in 1993 to 3.00 DIDs in 2003, but then fell to 2.66 DIDs in 2009 (see Figure 1).
0,0
0,5
1,0
1,5
2,0
2,5
3,0
3,5
1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009
Con
sum
ptio
n in
DID
CIPROFLOXACIN LEVOFLOXACIN MOXIFLOXACIN NORFLOXACIN OFLOXACIN PEFLOXACIN
Fig. 1 Consumption of fluoroquinolones in ambulatory care in Belgium In the 1990s, consumption was dominated by norfloxacin, although this fluoroquinolone was increasingly replaced by ciprofloxacin and ofloxacin in the second half of the 1990s. Although pefloxacin contributed to fluoroquinolone consumption in the 1990s, this antibiotic is no longer commercialized in Belgium. The growth in consumption in the 1990s originated from increased consumption of ciprofloxacin, and accelerated with the introduction of levofloxacin in 2000 and moxifloxacin in 2002. The decrease in consumption since 2003 can be attributed to falling consumption of norfloxacin and ofloxacin, although the consumption of ciprofloxacin, levofloxacin and moxifloxacin has remained relatively stable. In 2009, consumption of fluoroquinolones was made up of 1.07 DIDs of ciprofloxacin (40% of fluoroquinolone consumption), 0.78 DIDs of moxifloxacin (29%), 0.33 DIDs of levofloxacin (13%), 0.27 DIDs of norfloxacin (10%), and 0.21 DIDs of ofloxacin (8%). Looking at the annual consumption of fluoroquinolones valued at public prices, this increased from 24.1 million € in 1993 to a maximum of 44.4 million € in 2002, and then decreased to 35.0 million € in 2009. With respect to the type of infection, levofloxacin was used for treating respiratory tract infections prior to the introduction of moxifloxacin, and for treating gastro-intestinal and urinary tract infections after its introduction [18]. Moxifloxacin was typically used in the treatment of respiratory tract infections. The principal use of fluoroquinolones was in the treatment of urinary tract infections (36% of consumption, volume of 0.95 DIDs) and lower respiratory tract infections (26% of consumption, volume of 0.70 DIDs). Management of upper respiratory tract infections with fluoroquinolones amounted to 8% of consumption (volume of 0.21 DIDs). This suggests that fluoroquinolones are primarily used in those indications where they have been shown to yield clinical benefit [19,20]. Future consumption patterns of fluoroquinolones and other antibiotics are likely to be influenced by a number of factors. A recent analysis suggested that the worldwide antibiotic market is stagnating and increasingly subjected to generic substitution [21]. While little activity is taking place developing new antibiotics for the community setting, the antibiotic market is shifting towards the hospital sector. Generic competition is likely to affect older classes of antibiotics such as cephalosporins and penicillins to a greater extent than the newer class of fluoroquinolones.
339©FORMATEX 2011
Science against microbial pathogens: communicating current research and technological advances A. Méndez-Vilas (Ed.)_______________________________________________________________________________

Nonetheless, the consumption of generic fluoroquinolones in Belgium has steadily increased to 24% of consumption in DIDs and 17% of consumption in Euro in 2009 [18]. Patents covering levofloxacin and moxifloxacin will expire in the next five years. The danger exists that the lower price of generic medicines may incite physicians to increase overall consumption, thereby possibly negating the effect of Belgian information campaigns to rationalize the use of antibiotics.
3. Fluoroquinolones and guidelines
The role of fluoroquinolones in the treatment of respiratory tract infections in ambulatory care is discussed in guidelines issued by the Belgian Antibiotic Policy Coordination Committee [22] and by the Belgian Infectious Disease Advisory Board [23,24]. For patients with mild to moderate CAP who can be treated outside the hospital, the choice of antibiotics will depend on their age and the presence of comorbid illnesses. In younger (age < 65y), previously healthy patients with pneumonia (CAP1) oral amoxicillin 1g TID is the preferred choice. Oral moxifloxacin 400mg OD or telithromycin 800mg OD are proposed in case of IgE-mediated ß-lactam allergy or severe intolerance to ß-lactam antibiotics. In older (age ≥ 65y) patients and/or patients with comorbidities (CAP2) oral amoxicillin-clavulanic acid, either 875/125 mg TID or 2000/125 mg ‘Retard formulation’ BID, is recommended. Oral moxifloxacin 400mg OD is proposed in case of IgE-mediated ß-lactam allergy or severe intolerance to ß-lactam antibiotics. The use of antibiotics in AECOPD remains a subject of controversy. The Belgian Infectious Disease Advisory Board recommends oral amoxicillin-clavulanic acid, either 875/125 mg TID or 2000/125 mg ‘Retard formulation’ BID, as the preferred choice for the empiric antibiotic treatment of a AECOPD outside the hospital. Oral moxifloxacin 400mg OD is proposed as first choice in case of IgE-mediated ß-lactam allergy or severe intolerance to ß-lactam antibiotics. In COPD patients with a history of frequent exacerbations (≥ 3 in the previous year) cycling between amoxicillin-clavulanic acid and moxifloxacin is recommended. Most upper respiratory tract infections such as acute rhinosinusitis, acute pharyngitis, acute laryngitis, and acute bronchitis are self-limiting illnesses caused by viruses. Treatment with antibiotics is not warranted unless complications due to secondary bacterial infection occur (mastoiditis, meningitis, …). In more severe cases of bacterial sinusitis, antibiotic therapy can be indicated and oral amoxicillin 1g TID is recommended as the preferred choice. When clinical evolution is unfavourable after 2 days a switch to oral amoxicillin-clavulanic acid, either 875/125 mg TID or 2000/125 mg ‘Retard formulation’ BID, is advised to also cover ß-lactamase producing pathogens. Oral moxifloxacin 400mg OD is proposed in case of IgE-mediated ß-lactam allergy or severe intolerance to ß-lactam antibiotics.
4. Fluoroquinolones and resistance
Fluoroquinolones inhibit bacterial DNA synthesis by inhibiting DNA gyrase and topoisomerase IV [25]. Fluoroquinolone resistance is generally related to mutations in the Quinolone Resistance-Determining Region (QRDR). In S. pneumoniae, resistance to the new fluoroquinolones mostly requires at least two mutation events, one in DNA gyrase and one in topoisomerase IV. In Belgium, surveillance studies from 1995 to 2005 have consistently found 0% resistance of S. pneumoniae to moxifloxacin [26,27]. One of these studies focused on fluoroquinolone consumption and pneumococcal resistance rates [26]. Data on fluoroquinolones sold by wholesalers in Belgium were obtained from IMS Health. Also, the susceptibility of 600 isolates of S. pneumoniae collected from 1998 to 2003 was tested. The S. pneumoniae strains were isolated in Belgian laboratories participating in the National Surveillance Programme. The volume of consumption of fluoroquinolones in ambulatory care in Belgium nearly doubled from 1993 to 2003. The growth in consumption accelerated with the introduction of levofloxacin in 2000 and moxifloxacin in 2002. However, the use of levofloxacin and moxifloxacin, and the ongoing use of older fluoroquinolones did not lead to increased pneumococcal resistance: it remained below 1% for levofloxacin and was 0% for moxifloxacin. A more recent surveillance study of blood isolates from the Belgian Pneumococcal Reference Laboratory showed that moxifloxacin is the most potent fluoroquinolone available for treatment of lower respiratory infections in Belgium with MIC90 of 0.19 mg/L [18]. Also, the use of fluoroquinolones has not led, to date, to an increase in the rate of pneumococcal resistance to fluoroquinolones. A rightward shift in the minimum inhibitory concentration (MIC) distributions of fluoroquinolones was not observed during 2004-2009, indicating that first-step mutants have not become more prevalent in Belgian strains. Data on the activity of antibiotics (including fluoroquinolones) against non-invasive isolates of S. pneumoniae pointed to similar resistance rates as those observed in this sample of blood isolates. These results mirror the findings of a recent survey of antibiotic resistance in S. pneumoniae collected from 3,262 non-invasive clinical isolates in Belgium from 1995 to 2008 [28]. Resistance of S. pneumoniae to levofloxacin and to moxifloxacin was less than 1% and no rightward shift in the MIC distributions of the fluoroquinolones was noted. The percentage of S. pneumoniae that are not susceptible to selected antibiotics in 2008 was 29.7% for erythromycin, 22.9% for tetracycline, 11.6% for penicillin, 9.2% for cefuroxime, 5.1% for ciprofloxacin, 2.0% for cefotaxime, 0.7% for levofloxacin, 0.4% for moxifloxacin, 0% for amoxicillin, and 0% for telithromycin.
340 ©FORMATEX 2011
Science against microbial pathogens: communicating current research and technological advances A. Méndez-Vilas (Ed.)______________________________________________________________________________
Antibiotic resistance can have a substantial impact on the cost-effectiveness of treating respiratory tract infections with antibiotics (cfr. infra). For instance, four economic evaluations assessed the cost-effectiveness of moxifloxacin for CAP taking into account antibiotic resistance in CAP pathogens and multi-drug resistance in S. pneumoniae isolates [29-32]. These studies were conducted in countries with different levels of antibiotic resistance: Germany, which has a low level of antibiotic resistance in CAP pathogens; Belgium, Canada and the United States, which have an intermediate level of resistance; France and Spain, which have a high level of resistance. These studies indicated that antibiotic resistance affected costs and clinical outcomes, but first-line treatment with moxifloxacin remained more effective and less expensive than all other treatment strategies in Belgium, France, Germany, Spain and the United States. In Canada, a 50% increase in fluoroquinolone resistance would raise the incremental cost-effectiveness ratio of first-line moxifloxacin treatment as compared with azithromycin to CAN$ 101.47 per first-line clinical failure avoided. Canada has faced a steady increase in macrolide resistance in S. pneumoniae over time, and further increase in macrolide resistance rates cannot be ruled out. Increase in macrolide resistance would result in more favourable cost-effectiveness ratios for first-line treatment with moxifloxacin.
5. Fluoroquinolones and cost-effectiveness
Economic evaluation is a technique that can be used to determine whether antibiotic treatment adds sufficient value to justify its costs. An economic evaluation is a comparative analysis of at least two health technologies in terms of both their costs and outcomes. Evidence derived from economic evaluations is used to inform antibiotic pricing/reimbursement decisions in many countries. Antibiotics that provide better value for money are rewarded by means of a more favourable price/reimbursement. The requirement for economic evaluation fits within an overall trend towards evidence-based decision making in health care. An economic evaluation focused on the treatment of CAP with fluoroquinolones in ambulatory care in Belgium [30]. The study employed a decision-analytic model to evaluate the cost-effectiveness of empirical antibiotic treatment of patients suffering from mild-to-moderate CAP. Treatment strategies involved oral antibiotics (i.e. moxifloxacin, co-amoxiclav, cefuroxime or clarithromycin), were recommended by clinical practice guidelines and reflected prevailing treatment pathways in Belgium. First-line treatment was initiated in the community, with failure resulting in second-line treatment in the community or hospitalization. The analysis calculated the cost-effectiveness of antibiotic treatment in the presence of resistance. As this economic evaluation was carried out from the perspective of the third-party payer, the analysis considered direct health care costs only and did not include indirect costs due to productivity loss. The economic evaluation was based on the premise that clinical failure can occur due to two main reasons: lack of response to treatment in patients with susceptible pathogens and failure due to the presence of antibiotic-resistant pathogens. The failure rate in susceptible pathogens was estimated on the basis of antibiotic success rates from published clinical trials in CAP. The failure rate in antibiotic-resistant pathogens was estimated on the basis of antibiotic resistance data from published surveillance studies. Antibiotic resistance data related to Belgium or were derived from published sources in the absence of Belgian data. First-line treatment of CAP with moxifloxacin turned out to be more effective in terms of first-line clinical failure, need for second-line treatment, hospitalization and mortality as compared with first-line treatment with co-amoxiclav, cefuroxime or clarithromycin. The rate of first-line failure was 5%, 16%, 19% and 18% for these four treatment strategies, respectively. The rate of second-line treatment amounted to 4%, 13%, 16% and 15%, respectively. The hospitalization rate was 1%, 4%, 4% and 4%, respectively. The death rate was 0.01%, 0.04%, 0.03% and 0.03%, respectively. As a consequence, total health care costs of treating a CAP episode with moxifloxacin were lower than costs of comparator strategies, despite the higher drug cost of moxifloxacin. Costs of treating a CAP episode amounted to 144 € with moxifloxacin, 222 € with co-amoxiclav, 211 € with cefuroxime, and 193 € with clarithromycin. The extensive sensitivity analyses corroborated these results in nearly all scenarios. The authors argued that the absence of resistance to moxifloxacin and the high clinical success rate associated with moxifloxacin leads to moxifloxacin being the most effective and least expensive option in most cases. Therefore, it appears to be more cost-effective to select an antibiotic as first-line treatment that is more effective, i.e. with lower resistance and a higher clinical success rate. The decision-analytic model employed in the economic evaluation reflected empirical antibiotic treatment. However, empirical treatment does not always correspond to real clinical practice where data on the pathogen and the susceptibility may be available following first-line treatment failure. If the physician can adopt with a high degree of reliability the antibiotic treatment strategy according to the cause, the most cost-effective treatment strategy may vary. However, if the aetiology cannot be discriminated clinically, first-line treatment of CAP with moxifloxacin is the most cost-effective option. To date, economic evaluations assessing the cost-effectiveness of treating respiratory tract infections with fluoroquinolones or other antibiotics are not taken into account in Belgian (or international) clinical guidelines. In addition to the best available evidence on safety and effectiveness, treatment guidelines should take into account pharmaco-economic considerations. International evidence supports the value of treating respiratory tract infections with fluoroquinolones [33,34]. However, the cost-effectiveness of fluoroquinolones is influenced by the local frequency
341©FORMATEX 2011
Science against microbial pathogens: communicating current research and technological advances A. Méndez-Vilas (Ed.)_______________________________________________________________________________

of causative pathogens, the pattern of antibiotic resistance, and risk factors for resistant bacteria. Therefore, it may be advisable to identify patient subgroups in which treatment with fluoroquinolones is cost-effective and should be recommended by guidelines. In addition to information about the cost-effectiveness of treating respiratory tract infections with fluoroquinolones in Belgium, the budgetary impact of fluoroquinolones needs to be considered. Treatment with fluoroquinolones benefits from a lower resistance rate, an equal or higher clinical success rate, a similar or higher bacteriological eradication rate, and a shorter time to resolution of symptoms as compared with other antibiotics. This may translate into cost savings due to a shorter course of antibiotic treatment, a lower hospitalization rate, a shorter duration of intravenous therapy and hospital stay. These cost savings more than offset the higher drug acquisition costs of fluoroquinolones. Therefore, the management of respiratory tract infections with fluoroquinolones saves money, freeing up resources to be invested in other health technologies in Belgium. A recent study evaluated the impact of three interventions for physicians in order to implement guidelines for sequential therapy (i.e. intravenous to oral conversion) with fluoroquinolones in a Belgian university hospital [35]. This study was not an economic evaluation, focused on fluoroquinolone use in general (not limited to respiratory tract infections), and examined the impact of interventions for guideline implementation rather than of fluoroquinolones. The three interventions were: 1) hospital-wide publication of guidelines in local drug letter to all prescribers; 2) a once-only educational interactive session by infectious disease specialists to medical staff; and 3) a proactive conversion programme by pharmacists. The outcome measures were the ratio of intravenous versus total fluoroquinolone consumption (as measured in daily define doses per 1,000 bed days) and the number of days that intravenous therapy continued beyond the day that the patient fulfilled the criteria for sequential therapy as assessed by an expert panel. To calculate the potential financial impact, the cost of continuing intravenous therapy when oral fluoroquinolones could have been used was determined. The study did not consider other costs associated with labour in drug preparation and administration, supplies for administration, avoidance of infusion-related complications, length of hospital stay etc. It should be noted that this study had limited statistical power due to the small sample size and employed a pre- and post-study design (without control group for the second and third intervention) rather than a controlled before-and-after study design. The study observed that the mean ratio of intravenous versus total fluoroquinolone consumption decreased from 44.5% before the publication of the guidelines to 41.2% in the following 24 months (p = 0.011). This intervention had a gradual rather than an instant effect (learning effect observed following six months) which may decline over time (decay effect). The number of excess days of intravenous therapy was 4.1 days in the baseline period, 3.5 days with the educational session and 1.0 days with the conversion programme (p = 0.006). The mean additional cost for excess intravenous therapy decreased from 188 € in the baseline period to 103 € with the educational session and 44 € with the conversion programme (p = 0.037). These results show that the educational session had a clear, but not significant impact; whereas the proactive conversion programme by a pharmacist reduced the duration of intravenous treatment and antibiotic costs. Finally, the authors noted that the majority of physicians were not aware of the bio-equivalence of and the cost difference between intravenous and oral fluoroquinolones.
6. Conclusions
Belgian data on the treatment of respiratory tract infections with antibiotics in ambulatory care showed that fluoroquinolone use remains well controlled. Belgian guidelines have recommended moxifloxacin for CAP outpatients with comorbid conditions or outpatients in whom infection with atypical pathogens needs to be considered. Moxifloxacin is recommended in case of IgE-mediated ß-lactam allergy or severe intolerance to ß-lactam antibiotics when treating COPD exacerbations or when treating upper respiratory tract infections on the rare occasion that antibiotic treatment is warranted. The MIC distribution of moxifloxacin and levofloxacin in S. pneumoniae isolates remained stable during 2004-2009 and resistance to moxifloxacin and levofloxacin was low (≤ 1%) in Belgium. As the cost-effectiveness of moxifloxacin is influenced by the causative pathogens involved and resistance patterns, it may be advisable to identify patient subgroups in which moxifloxacin is cost-effective.
Acknowledgements The financial support by Bayer Schering Pharma for this study is gratefully acknowledged.
References
[1] World Health Organisation. The World Health Report 2004 - changing history. Geneva: World Health Organisation; 2004. [2] Martin SJ, Sahloff EG, Close SJ. Evaluation and cost assessment of fluoroquinolones in community-acquired respiratory
infections. Expert Opinion of Pharmacotherapy 2002;3(9):1251-1266. [3] Feldman C. Appropriate management of lower respiratory tract infections in primary care. Primary Care Respiratory Journal
2004;13(3):159-166.
342 ©FORMATEX 2011
Science against microbial pathogens: communicating current research and technological advances A. Méndez-Vilas (Ed.)______________________________________________________________________________
[4] Mandell LA, Wunderink RG, Anzueto A, Bartlett JG, Campbell GD, Dean NC, et al. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clinical and Infectious Diseases 2007;44 Suppl 2:S27-S72.
[5] Woodhead M, Blasi F, Ewig S, Huchon G, Ieven M, Ortqvist A, et al. Guidelines for the management of adult lower respiratory tract infections. European Respiratory Journal 2005;26(6):1138-1180.
[6] Wasserfallen JB, Livio F, Zanetti G. Acute rhinosinusitis : a pharmacoeconomic review of antibacterial use. Pharmacoeconomics 2004;22(13):829-837.
[7] Hulscher ME, Grol RP, van der Meer JW. Antibiotic prescribing in hospitals: a social and behavioural scientific approach. Lancet Infectious Diseases 2010;10(3):167-175.
[8] Arroll B, Kenealy T. Antibiotics for the common cold and acute purulent rhinitis. Cochrane Database of Systematic Reviews 2005;(3):CD000247.
[9] Smucny J, Fahey T, Becker L, Glazier R. Antibiotics for acute bronchitis. Cochrane Database of Systematic Reviews 2004;(4):CD000245.
[10] Organisation for Economic Co-operation and Development. Health at a glance 2007. Paris: Organisation for Economic Co-operation and Development; 2007.
[11] Dunagan WC, Woodward RS, Medoff G, Gray JL, Casabar E, Lawrenz C, et al. Antibiotic misuse in two clinical situations: positive blood culture and administration of aminoglycosides. Review of Infectious Diseases 1991;13(3):405-412.
[12] Lee KR, Leggiadro RJ, Burch KJ. Drug use evaluation of antibiotics in a pediatric teaching hospital. Infectious Control Hospital Epidemiology 1994;15(11):710-712.
[13] Decramer M, Bartsch P, Pauwels R, Yernault JC. Management of COPD according to guidelines. A national survey among Belgian physicians. Monaldi Archives of Chest Diseases 2003;59(1):62-80.
[14] Kahlmeter G. An international survey of the antimicrobial susceptibility of pathogens from uncomplicated urinary tract infections: the ECO.SENS Project. Journal of Antimicrobial Chemotherapy 2003;51(1):69-76.
[15] Holmberg SD, Solomon SL, Blake PA. Health and economic impacts of antimicrobial resistance. Review of Infectious Diseases 1987;9(6):1065-1078.
[16] Rifenburg RP, Paladino JA, Hanson SC, Tuttle JA, Schentag JJ. Benchmark analysis of strategies hospitals use to control antimicrobial expenditures. American Journal of Health System Pharmacy 1996;53(17):2054-2062.
[17] Vanhoof R, Carpentier M, Cartuyvels R. Surveillance of antibiotic resistance in non invasive clinical isolates of Streptococcus pneumoniae collected in Belgium during winters 2003 and 2004. Acta Clinica Belgica 2006;61(2):49-57.
[18] Simoens S., Verhaegen J., van Bleyenbergh P., Peetermans W., Decramer M. Consumption patterns and in vitro resistance of S. pneumoniae to fluoroquinolones. Antimicrobial Agents and Chemotherapy 2011;55(6):3051-3053.
[19] Bailey RR. Quinolones in the treatment of uncomplicated urinary tract infections. International Journal of Antimicrobial Agents 1992;2(1):19-28.
[20] Ball P. Efficacy and safety of levofloxacin in the context of other contemporary fluoroquinolones: a review. Diagnosis and Microbiology of Infectious Diseases 2003;64(9):646-661.
[21] Datamonitor. Antibacterials - opportunities in the hospital sector contrast with the lack of innovation in community market. New York: Datamonitor; 2009.
[22] De Sutter A, Chevalier P, BAPCOC. Belgische gids voor anti-infectieuze behandeling in de ambulante praktijk. 2010. [23] Valcke Y. Community-acquired pneumonia. IDAB; 2005. [24] Vincken W. Acute exacerbations of COPD. IDAB; 2007. [25] Hooper DC. Mechanisms of action of antimicrobials: focus on fluoroquinolones. Clinical and Infectious Diseases 2001;32
Suppl 1:S9-S15. [26] Simoens S, Verhaegen J, Laekeman G, Peetermans WE. Treating respiratory tract infections in ambulatory care in Belgium:
fluoroquinolone consumption and resistance development. International Journal of Antimicrobial Agents 2005;26(1):62-68. [27] Institut Pasteur. Evolution of fluoroquinolone resistance and detection of resistance mechanisms in clinical isolates of
streptococcus pneumoniae collected in Belgium in 1995 – 2005. Brussels: Institut Pasteur; 2006. [28] Vanhoof R, Van Bossuyt E, De Craeye S, Van Eldere J, Verhaegen J, Kaufman L, et al. Survey of antibiotic resistance in
Streptococcus pneumoniae collected in Belgium during winter 2008. Follow-up of resistance since 1995 and possible effects of antibiotic campaigns. 2009.
[29] Martin M, Quilici S, File T, Garau J, Kureishi A, Kubin M. Cost-effectiveness of empirical prescribing of antimicrobials in community-acquired pneumonia in three countries in the presence of resistance. Journal of Antimicrobial Chemotherapy 2007;59(5):977-989.
[30] Martin M, Moore L, Quilici S, Decramer M, Simoens S. A cost-effectiveness analysis of antimicrobial treatment of community-acquired pneumonia taking into account resistance in Belgium. Current Medical Research and Opinion 2008;24(3):737-751.
[31 ]Moore L, Martin M, Quilici S. The cost-effectiveness of targeted prescribing of antimicrobials in Canada for community-acquired pneumonia in an era of antimicrobial resistance. Value in Health 2008;11:A271-A272.
[32] Sabes-Figuera R, Segu JL, Puig-Junoy J, Torres A. Influence of bacterial resistances on the efficiency of antibiotic treatments for community-acquired pneumonia. European Journal of Health Economics 2008;9(1):23-32.
[33] Simoens S, Decramer M, Laekeman G. Economic aspects of antimicrobial therapy of acute exacerbations of COPD. Respiratory Medicine 2007;101(1):15-26.
[34] Simoens S, Decramer M. A pharmacoeconomic review of the management of respiratory tract infections with moxifloxacin. Expert Opinion of Pharmacotherapy 2008;9(10):1735-1744.
[35] Buyle F, Vogelaers D, Peleman R, Van MG, Robays H. Implementation of guidelines for sequential therapy with fluoroquinolones in a Belgian hospital. Pharmacy World and Science 2010;32(3):404-410.
343©FORMATEX 2011
Science against microbial pathogens: communicating current research and technological advances A. Méndez-Vilas (Ed.)_______________________________________________________________________________