Embed Size (px)
Citation preview

Respiratory Module
Lower Respiratory Tract InfectionsLecture 6

Atelectasis
• Definition– Closure or collapse of
alveoli

Atelectasis: Pathophysiology
• Can occur as a result of alveolar ventilation or
• any type of blockage • that impedes the
passage of air to and from the alveoli

Atelectasis: Etiology
• #1 post-op• secretions or mucus
plug• Chronic airway
obstruction– i.e. lung CA
• Excessive pressure on the lungs

Atelectasis: Risk Factors
• Altered breathing patterns
• Retained secretions• Pain• LOC• Immobility• Prolonged supine
position• Post-op

Atelectasis: Clinical Manifestations
• “The development of Atelectasis usually is insidious”– Cough– sputum production– low-grade fever

Atelectasis: Clinical Manifestations
• If Atelectasis involves a large amount of lung tissue S&S include– Marked resp. distress– Dyspnea (orthopnea)– Pulse?
• Tachycardia– Respiratory rate?
• Tachypnea– Pleural pain– Central cyanosis

Atelectasis: Assessment and Diagnostic Findings
• breath sounds – – Crackles
• Chest X-ray – patchy infiltrates– consolidated area

Atelectasis: Assessment and Diagnostic Findings
• SpO2 – < 90%
• PaO2 – < 80
• PaCO2– > 45
• HCO3-– to compensate
• ABG analysis– Resp. acidosis

Atelectasis: Prevention
• Frequent turning• Early mobilization• Strategies to expand the
lungs – Deep breathing – Incentive Spirometry
(IS)

Atelectasis: Prevention
• Strategies to manage secretions– Directed cough– Suctioning– Nebulizer– Chest physical
therapy– fluids

Atelectasis: Management
• Goal:– to ventilation and
secretions
• Frequent turning• Early amb.• Lung volume expansion
maneuvers

Atelectasis: Management
• Coughing• PEEP• Bronchoscope

Atelectasis: Management
• If due to bronchial obstruction– Coughing– Suctioning– Chest physiotherapy– Nebulizers– Bronchodilators– Endotracheal
intubation & mechanical ventilation

Atelectasis: Management
• If due to compression of the lung tissue– Decrease the
compression– Thoracentesis– Chest tubes

Small Group Questions
1. What can a nurse due to prevent a patient from acquiring Atelectasis?
2. Which patients are most likely to acquire Atelectasis?
3. How is Atelectasis treated?4. Describe the ABG’s of a patient with Atelectasis.5. Name 4 S&S of Atelectasis.

Acute Tracheobronchitis
AKA• Bronchitis• Acute Bronchitis

Acute Tracheobronchitis
Pathophysiology• Inflammation of the
mucous membranes of the trachea & bronchial tree
• Follows URI

Acute Tracheobronchitis
• What pathogen is most commonly responsible for tracheobronchitis?
A. BacteriaB. VirusC. FungusD. Parasite

Acute Tracheobronchitis
Etiology/Contributing factors
• Infection• Inhalation of irritants– Sulfur dioxide– Nitrogen dioxide– Air pollutants
• May be a complication of bronchial asthma

Acute TracheobronchitisClinical Manifestations• Usually self limiting• Durations
– Several days• Sputum
– Mucopurulent• Cough
– Dry, irritation, dyspnea• Pain
– Sternal soreness• Fever / chills• Headache / gen. malaise

Acute Tracheobronchitis
Diagnostic findings• Sputum C&S• Chest x-ray • Breath sounds– Sonorous wheezes– Stridor
• Symptoms

Acute Tracheobronchitis
Treatment• Symptomatic• Bed rest• Cool vapor• Steam• Moist heat to chest• If bacterial– Antibiotics

Acute TracheobronchitisNursing interventions• Enc bronchial hygiene• Enc TCDB / fluids• Position– HOB
• Caution against over exertion relaps
• Auscultate BS• Check V/S

Acute Tracheobronchitis
Prevention• Treat URIComplications• Bronchopneumonia

Small group questions???1. Describe the pathophysiology of tracheobronchitis?2. What is the usual causative agent for tracheobronchitis?3. What does self-limiting mean?4. What breath sounds are associated with
Tracheobronchitis?5. Identify a nursing diagnosis for tracheobronchitis?6. Name for nursing comfort measures for a pt. with
tracheobronchitis?

Pneumonia
Pathophysiology• An inflammatory process in which there is
consolidation – caused by exudates filling the alveolar spaces.
• Gas exchange cannot take place in consolidated area

PneumoniaCausative agents• Viral pneumonia• Bacterial Pneumonia
– Streptococcus pneumoniae– Pneumocystis Pneumonia
• Fungal pneumonia• Radiation pneumonia• Chemical pneumonitis• Aspiration pneumonia• Hypostatis pneumonia

Pneumonia
Which of the following components of respiration would pneumonia affect? (there may be more than one answer)
A. VentilationB. PerfusionC. Diffusion

Pneumonia FYI
• Most common cause of death from infectious agents
• 66,000 deaths / year• $$$

PneumoniaProgression of events• Inflammation • Exudate • movement of O2 and CO2 • WBC migrate into the alveoli • Fill air-containing spaces• ventilation • PaO2 ?–

Pneumonia - Classifications• Community-acquired pneumonia– CAP– Community or < 48 hr after hospitalization
• Hospital-acquired pneumonia– HAP– Nosocomial – (CDC: 15-20% all pt get HAP)
• Immuno-compromised host– Pneumocystis pneumonia (PCP)
• Aspiration

• Mrs. Sickly is admitted to Sierra View District Hospital on Wednesday Morning at 0930 AM for severe back pain and general declining state. She is 82 years old. On Friday morning at 0600 AM the nurse notes decreased breath sounds in the left lung, a productive cough and crackles. The doctor orders a chest x-ray which shows consolidation in the base of the left lung. She has pneumonia. What type of pneumonia does she have?
A. Community acquired pneumoniaB. Nosocomial pneumoniaC. Immuno-compromised host D. Aspiration

Pneumonia: Risk factors
• Immunosuppressant• Smoking• Prolonged immobility• Depressed cough reflex• NPO• Alcohol intoxication• Gen. anesthetic or opiod• Advanced age

Pneumonia
S&S: bacterial• Onset:
– Sudden• Pain:
– Severe chest pain– sharp– Guarding– mobility (affected side)
• Temperature– High temp (>106)– Chills
• Cough– Painful
• Sputum– Rust colored
• Breathing– Shallow– Rapid rate– Wheezing & crackles– Decreased BS
• Peristaltic activity– Slows down
• PaO2– – Cyanotic

Pneumonia: S&S: viral pneumonia
• Blood cultures:– Sterile
• Sputum– Copious
• Temperature– Seldom chills
• Respirations– Slow– Wheezing & crackles– Diminished BS
• Pulse– Slow
• PaO2– – Cyanotic
• Viral less severe than bacterial
• Mortality is low

Pneumonia
S&S Elderly• General deterioration• Weakness• Abd. Symptoms• Anorexia• Confusion• Tachycardia• Tachypnea
• Do Not C/O– Cough– Pain– Fever – Sputum

Pneumonia
Dx • Sputum C&S• CBC / WBC–
• Bacteria–
• Viral
• ABG’s• Chest x-ray
• What is a normal WBC count?– 5,000 – 10,000 mm3

Pneumonia
• What would you expect the ABG’s of a person with bacterial pneumonia to have?
• PaO2?
• PaCO2?
• pH• HCO3
- ? - Why?
• Analysis?

Pneumonia
Treatment• Antibiotics?• Rest• Fluids– – Humidifier
• Antipyretic• Anti-tussive?
• Analgesics• Anti-histamines• Nasal Decongestants• O2 • Mucolytic drug– Alivaire– Via – nebulizer

Pneumonia: Nrs. diagnosis
• Ineffective airway clearance: r/t copious secretions• Activity intolerance: r/t impaired resp. function• Risk for deficient fluid volume: r/t fever & dyspnea• Imbalanced nutrition: less than body requirement• Deficit knowledge: about the treatment regimen and
preventive health measures

Pneumonia – Nursing Interventions
• Improve airway patency– Hydration• 2-3 L/day• Humidifier
– TCDB– Lung expansion maneuvers• Incentive spirometer
– Chest physiotherapy– O2

Pneumonia – Nursing Interventions
• Promoting rest & conserving energy–Position• Semi-fowler• Affected side for pain
– Turn frequently–Moderate activity only
• Promoting fluid intake– 2 L/day

Pneumonia – Nursing Interventions
• Maintaining nutrition–Gatorade– Ensure
• Promoting the patients knowledge

Pneumonia
Prevention• Vaccine– Pneumonia– Flu
• Treat URI• Avoid irritants

Pneumonia
Complications• Shock • Respiratory failure• Atelectasis • Pleural effusion• Superinfection

Pneumonia: Small Group Questions
1. Describe the pathophysiology of pneumonia.2. What is the difference btw bacterial and viral
pneumonia?3. What causes pneumocystis carinii?4. What leads to hypostatis pneumonia?5. What lab values are associated with bacterial
pneumonia? / viral pneumonia?

Pneumonia: Small Group Questions
6. What is Nosocomial pneumonia7. Identify 5 risk factors for developing pneumonia8. What medications might be administered to treat a
pt. with pneumonia?9. What nursing education would you give to a patient
with pneumonia?10. What ABG’s are associated with pneumonia?11. What are the gerontological considerations of
caring for the elderly in regards to pneumonia?

SARS
• Severe Acute Respiratory Syndrome
• Viral respiratory illness • Caused by a coronavirus

SARS
• FYI– First reported in Asia
2003– 8098 people worldwide
dx with SARS in 2003– 774 died!

SARS
• Mode of transmission– Respiratory droplet
• When infected person coughs or sneezes
• The droplet gets on another's mucous membranes or
• On a surface that is touch by another and then they touch their own mucous membranes

SARS
S&S• Initial– High fever– H/A– Body aches– Mild resp. symptoms– After 2-7 days
• After 2-7 days– Dry cough– Progressive hypoexmia
– Pneumonia

SARS
• Treatment– Same for viral
pneumonia• Infection control– Limit transmission
• Neg pressure rooms• Protective equipment• Good cleaning or hands
and room• Contain secretions

Tuberculosis
• AKA– TB– Consumption

Tuberculosis - FYI
• Causes more death than any other disease. 2 billion world wide, 15 million in the US

Tuberculosis - FYI
• When it becomes active it kills 60% of those not treated. Amounts to about 3 million deaths each year. In the US about 20,000 TB cases become active each year.

Tuberculosis - FYI
• When treated, about 90% of those with active TB survive!

Tuberculosis
• Pathophysiology– Mycrobacterium
tuberculosis– Tubercle bacillus

Question?
• TB is caused by a(n)?A. BacteriaB. VirusC. FungusD.ParasiteE. Little green bugs!

Tuberculosis
Pathophysiology• Mode of transmission– Air-borne
• alveoli• Multiplies in alveoli

Tuberculosis
• Immune response phase– Macrophages attack TB– TB has waxy cell wall that protects it from
macrophages– Immune system surrounds the infected
macrophages– Forms a Lesion– Called a Tubercle

Tuberculosis
• Dormant /latent phase– Contagious?
• No
– Symptomatic?• No
– PPD?• positive
– chest x-ray?• Negative

Tuberculosis
• Active phase– If an infected person has a weakened immune
system, – the TB escapes and infects the body

Tuberculosis
• 5-10% become active• Only contagious when
active• Primarily affect lungs
but…– Kidneys– Liver– Brain– Bone

Tuberculosis
Etiology• Assoc. w/
– Poverty– Malnutrition– Overcrowding– Substandard housing– Inadequate health care
• Elderly• HIV• Prison

TuberculosisS&S (active phase)• NOC sweats• Low grade fever• Wt loss• Chronic productive cough
– Rust colored sputum– Thick
• Hemoptysis • SOB

Tuberculosis
Diagnostic exams• PPD – Mantoux skin test– > 10mm in diameter– induration – Indicates:
• Latent TB – Read
• 48-72 after – Intradermal: 15-degrees– Do not rub

Tuberculosis
• Diagnostic tests– X-ray
• Cavities or lesions
– Symptoms– Acid Fast Bacillus

TuberculosisTreatment• INH
– isonicotinyl hydrazine – Isoniazid – Toxic to the liver
• Rifampin– Turns urine red
• Streptomycin– Causes 8th cranial nerve damage– Acoustic nerve

Tuberculosis: treatment
• Rx toxic to liver and CNS
• Must take >6months• Usually take > one at a
time• Not contagious after
2wks of treatment

• INH - TUBERCULOSIS MEDICATIONYour positive skin test reaction shows that you have been exposed to tuberculosis at some time in the past. The tuberculosis germ is still present in your body. If your chest x-ray is normal, you do NOT have active TB disease.

• TB germs can live in your body without making you sick. This is called TB infection, and this is what you have. Your immune system has trapped the TB germs. However, if your immune system or body defenses go down, as can happen with stress, long-term illnesses, old age, or other stressors such as alcohol abuse, the TB germs may multiply and develop into active TB disease. TB germs can affect other organs besides the lungs.

• We recommend that you take preventive medicine now, before your TB infection becomes active TB disease. This medicine, taken every day for six or nine months, will kill the TB germs in your body so that you will not develop active TB disease. The medicine you will be taking is Isoniazid - also called “INH.” This medicine may deplete your body’s stores of vitamin B6, so you will also be given additional vitamin B6, to counteract possible side effects from a lack of this vitamin.

Tuberculosis
Nursing Dx• Impaired gas exchange• Ineffective airway
clearance• Anxiety• Knowledge deficit• Alt. nutrition

TuberculosisPreventative measures• Clean well ventilated living areas• Resp. isolation
– Negative pressure room
• Vaccine?– BCG– Does not prevent TB– Causes a + PPD
• If exposed take– INH

Tuberculosis
Complications• Malnutrition• S/E of medication
treatment• Multi-drug resistance• Spread of TB infection

Small Group Questions
1. What type of pathogen is TB?2. What is the mode of transmission?3. What are the classic S&S of TB ?4. How to administer and read a PPD?5. If a pt is PPD +, what does that mean?

Small Group Questions
6. What is the standard screening method of TB?
7. That medications are used to treat TB, what are their side effects?
8. Where in the US is TB most prevalent? Why?

Lung Abscess
Pathophysiology• Localized necrotic lesion of the lung
parenchyma containing purulent material • Lesion collapses and forms a cavity

Lung Abscess
Etiology / contributing factors
• Aspiration• Obstruction of the
bronchi
Risk Factors:• Any one at risk for
aspiration is at risk for lung abscess!– Impaired cough reflex– CNS disorders– NGT– Alcoholism– LOC

Lung Abscess
S&S• Most often Rt or left
side?– Right
• Varied– Dyspnea– Weakness– Fever– Malodorous sputum
– Blood sputum– Pleurisy– Anorexia

Lung Abscess
Dx• Absent / decreased BS• Chest x-ray• Sputum culture• Bronchoscopy

Lung Abscess
Tx• IV antimicrobial– Lg amounts
• Chest drainage– Chest physiotherapy– TCDB
• Diet– Protein
• ↑
– Calories• ↑
– Catabolic state• Bronchoscopy – Drain lesion
• Long recovery

Lung Abscess
Prevention• Antibiotics with dental
work• Tx pneumonia• HOB w/ NGT

Lung Abscess
Complications• Broncho-pleural fistula

Small Group Questions1. Describe the pathophysiology of a lung abscess in
your own words?2. What is the most common etiology of a lung
abscess?3. How is a lung abscess treated? – non-
pharmaceutical.4. What nursing education can a nurse give to patient
at risk of developing a lung abscess?5. What diet is usually prescribed to a patient with a
lung abscess?

Pleurisy
Pathophysiology• Pleural membranes
become inflamed• ‘catch” or rub on I• The parietal pleura has
nerve endings• The visceral pleura does
not have nerve endings

Pleurisy
Etiology/Contributing factors• Usually related to
another underlying respiratory problem/disease– Pneumonia– TB– Tumor/cancer– Trauma

Pleurisy
S&S• #1 pain – with respiration– movement– deep breath, cough,
sneeze– localized (usually one
side or the other)
– Sharp pain on inspiration– when hold their breath– as fluid develops
• Shallow-rapid breathing

Pleurisy
• Dx exams/procedures– S&S – Auscultation ?
• pleural friction rub • lower, lateral, anterior
– X-ray– Thoracentesis

Pleurisy
Tx• Underlying cause• Control pain – Analgesics– Topical application or
heat or cold– Indomethacin (Indocin)
(NSAID)– Narcotics
• Nerve block• Antibiotics

Pleurisy
Nursing intervention• Rest• Pain sympathy• Lay on ______ side
– Affected• Splint side when DB
and cough– Pillows– Hands
• Complications– Pleural effusion – Atelectasis– Empyema

Pleural Effusion: AKA - Hydrothorax
Pathophysiology• Excess fluid collects in
the pleural space • fluid • to compression of the
lung tissue • atelectasis• Effusion can be
– clear fluid – bloody – purulent

Pleural Effusion
• Pleural Fluid circulated by lymphatic system.
• Can be cause be a break in either system– Respiratory – Lymphatic

Pleural Effusion
Etiology• Symptom rather than a
disease• Generally caused by
another disorder– Heart failure– TB– Pneumonia– Pulmonary embolism– Tumors / Carcinoma

Pleural Effusion
S&S• or absent BS• SOB• Percussion– dull
• Lg amts mediastinum to shift towards…– unaffected side.
• Tracheal deviation away from…– affected side
S&S assoc. w/ the underlying cause.
• i.e. pneumonia:– fever, chills, dyspnea,
cough etc.

Pleural Effusion
DX exams/procedures• Thoracentesis – C&S fluid– Gram stain, acid-fast
bacillus stain• TB
– Cytologic analysis • malignant cells
• X-ray

Pleural Effusion: treatment
• Thoracentesis• Chest tube • Prevent re-accumulation of
fluid• Relieve comfort, dyspnea
and respiratory compromise
• pursed lip and diaphragmatic breathing
• Remove fluids Rx. – Lasix
• Anti-inflammatory + analgesics– Toradol– NSAIDS– Corticosteroids
• Treat underlying cause• Chemical pleurodesis

Pleural Effusion
Nursing intervention• Implement medical
regime• Pain management• Monitor chest tubes• Assist with
thoracentesis

EmpyemaPathophysiology• Collection of pus in the
pleural spaceEtiology• Usually secondary to
pneumonia, TB or lung abscess
Clinical manifestations and treatment
• Same as pleural effusion
• Elevated WBC

Hemothorax
Pathophysiology• Do you want to take a
stab at it?• Blood in the pleural spaceEtiology• Trauma
– #1• Lung CA• Pulm. emboli

Symptoms: • Same as pneumothoraxTreatment• Chest tube• Treat underlying issueNursing Management• Monitor chest tube• Monitor resp. status

Small Group Questions
1. Describe the difference between pleurisy, pleural effusion, hemothorax and empyema.
2. What is the etiology for each of the above disorders?
3. Describe the medical treatment for the above.4. What is the Rx treatment for each of the above?

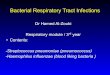
Pneumothorax
Pathophysiology:• “Accumulation of air
or gas in the pleural cavity”
• Left-sided pneumothorax (on the right side of the image) on CT scan of
the chest with chest tube in place.

Pneumothorax
Anatomy Review- Pleural cavity
• Visceral pleura– Encases lungs
• Pleural space/cavity– Area between pleura– Contains fluid (4ml)– Fluid prevents friction– Fluid circulated by…
• lymph system• Parietal pleura
– Lines chest wall

Pneumothorax
Anatomy review - Breathing• Diaphragm & accessory
muscles move outward • Negative pressure in the
thoracic cavity • Negative pressure pulls air
into the lungs via the nose and mouth
• Diaphragm & accessory muscle relax ()
• air exhaled

Pneumothorax
• If the visceral pleural is perforated or the chest wall & parietal pleural are perforated– air enters the pleural
space – negative pressure is
lost – Lung on the affected
side collapses

Pneumothorax
Classifications of pneumothorax
• Spontaneous pneumothorax– with out injury– Air enters the pleural
cavity via the airway– Farther classified as:
• Primary• Secondary

Pneumothorax
Spontaneous (Primary) Pneumothorax
• Pt. with no known lung disease.
• D/T a rupture of a bulla in the lung.
• Most often tall, thin men between 20 and 40 years old.

Pneumothorax
Spontaneous Secondary Pneumothorax
• occurs in pt. with known lung disease– most often COPD
• Other lung diseases commonly assoc. with– Tuberculosis– Pneumonia– Asthma– cystic fibrosis– lung cancer
• Often severe & life threatening

Pneumothorax
• Traumatic Pneumothorax– D/T injury to the chest
wall– Further classified as
Open or closed

Pneumothorax
Open Pneumothorax• Air enters pleural cavity via
outside• A free communication
between the exterior and the pleural space as through an open wound– blowing wound– sucking wound
• may be caused by a penetrating injury– stab wound,– gunshot wound– impaled object

Pneumothorax
Closed pneumothorax• Air enters the pleural
cavity via lungs• D/t/ blunt chest
trauma– Car crash– Fall– Crushing chest injury

Pneumothorax
Iatrogenic pneumothorax• D/T procedure /
treatment

Pneumothorax
Tension Peumothorax• air accumulates in the
pleural space with each breath.
• The remorseless increase in intrathoracic pressure
• massive shifts of the mediastinum away from the affected lung
• compressing intrathoracic vessels
• cardiovascular collapse

Pneumothorax
Tension Pneumonthorax• a piece of tissue forms
a one-way valve that allows air to enter the pleural cavity but not to escape, overpressure can build up with every breath

Pneumothorax
Etiology / Contributing factors• Spontaneous
– Lung disease - COPD– Tall, thin men
• Traumatic– A penetrating chest wound – Barotrauma
• scuba divers• Iatrogenic Pneumothorax
– * insertion of a central line – * thoracic surgery – * thoracentesis – * pleural or transbronchial
biopsy.

Pneumothorax
Clinical Manifestations (all types)
• Sudden sharp chest pain• Asymmetrical chest
expansion• dyspnea• Cyanosis• Percussion
– Hyper resonance or tympany
• Breath sounds– diminished– Absent

Pneumothorax
Clinical Manifestations (all types)
• Respiratory distress• O2 Sats– decreased
• Tachypnea• Tachycardia• Restlessness/ Anxiety

Pneumothorax
S&S of open pneumothorax
• Cripitus – (subcutaneous
emphysema)
• Sucking chest wound”

Pneumothorax
S&S Tension pneumothorax• cardiac output• Hypotension• Tachycardia (compensatory)• Tachypnea • Mediastinal shift and
tracheal deviation– To the unaffected side
• Cardiac arrest• Distended neck veins

Pneumothorax
Dx exam and tests• HX & PE• Chest x-ray• ABG’s
– Initial PaCO2• Decreased• respiratory alkalosis
– Later ABG’s• Hypoxemia• Hypercapnia• Acidosis

Pneumothorax
Treatment - First aid: Open pneumothorax
• Cover immediately with an occulsive dressing, made air-tight with petroleum jelly or clean plastic sheeting.

Pneumothorax
Tx: Small pneumothorax • Spontaneous recovery– Bed rest– resolve on its own in 1
to 2 weeks
• Remove with small bore needle inserted into the pleural space

Pneumothorax
Tx: Larger pneumothorax• Chest tube • Surgery repair• Pleurodesis
– “glue” – Very painful– Prep with analgesic
• O2• Surgery

Pneumothorax
Nursing interventions• Closely monitor resp status• Frequent assess
– LOC– Color– VS – Chest pain?– Restlessness?
• Chest Tube • Rest/Activity Balance• Sedation • Provide a means for
communicate • Educate patient & family
• Notify MD for:– SpO2 < 90% or Change
Greater Than 5% – Extubation – Respiratory Distress – Inadequate Sedation – Peak Airway Pressure
(Especially with Pressure Control Mode)

Pneumothorax
Complications• Recurrent
pneumothorax – D/C
• smoking • high altitudes• scuba diving• flying in unpressurized
aircrafts
• Cardiac damage

Question?
A client who has been on a ventilator for two days experiences acute respiratory distress accompanied by distended neck veins. The best action of the nurse is to:
A. hand ventilate the client.B. prepare for chest tube insertion.C. call the physician immediately.D. perform emergency chest decompression.

• The question is asking what the nurse should do when a client on a ventilator has these symptoms. When acute respiratory distress occurs along with neck vein distension, cyanosis and tracheal shift are evident, a tension pneumothorax has probably occurred. The client should be removed from the machine and ventilated by hand. Then the physician should be notified (option c). Equipment for chest tube insertion should be gathered (option b) so it will be ready for immediate use by the physician. Emergency chest decompression (option d) should only be attempted after specific training and if the physician will be delayed.

• A patient is being treated with chest tubes because of a pneumothorax. The nurse recognizes that chest tubes may be used to:– Prevent pleural irritation– Regain positive intra-pleural pressure– Remove air from the intra-pleural space– All of the above– None of the above

Small Group Questions
1. What is the pathophysiology of a pneumothorax?2. Describe the anatomy of the pleural membrane
(including nerves endings)3. What is a spontaneous pneumothorax?4. What are some examples of an iatrogenic
pneumothorax?5. Define an open and closed pneumothorax.

Small Group Questions
6. Describe the mediastial shift in an pneumothorax.7. 7. What is the first aid treatment of a traumatic
pneumothorax (include assessment)8. What is Pleurodesis?9. What ABG’s would you expect to see late in a
patient with a pneumothorax?