Embed Size (px)
Citation preview
1
Trial of two different ESWT energy flux density levels for the treatment of
chronic patellar tendinopathy in an active population.
¹Bruce Twaddle , ²Wayne Hing, ³Kenneth Craig
¹Chief of Orthopaedic Trauma, Auckland Hospital. Department of Orthopaedics Auckland University. Sports
Orthopaedics Consultant, UniSports Medicine. ²Assoc. Professor and Head of Health and Rehabilitation Research
Institute Auckland University of Technology. ³BHSc. Podiatry, Dip. Pharmacology, PG MSK Pain Management
Studies.
Abstract
Background: Patella tendinopathy (PT) is a commonly seen condition where activity related overload of
the knee extensor mechanism is seen to be the primary cause of complaint and disability presenting a
clinical challenge in its management (Taunton, 2003; Warden & Brunker, 2003; Wang et al 2007;
Maffulli et al 2010). Despite the abundance of therapeutic options available to treat tendinopathies, the
inconsistencies, irregularities and the lack of evidence based guidelines for treating this condition (Frohm,
2006; Crossley et al 2007; Andres & Murrell, 2008; Maffulli & Longo, 2008), warrants the exploration of
a treatment modality that may help address this issue, especially in unresponsive chronic conditions.
Aim: The aim of this study is to determine if medium and high energy extracorporeal shockwaves are
effective in treating chronic patella tendinopathy versus placebo in an active population that has failed to
respond to two or more non-surgical treatment methods.
Design: Randomised double blind placebo controlled trial.
Method: 108 patients randomized equally into three groups; two treatment groups and one placebo.
Patients with clinically diagnosed chronic patella tendinopathy with a minimum disability period of 4
months who have all failed three other treatments including eccentric exercises will be referred via a
network of physiotherapist, sports physicians and orthopaedic surgeons. Baseline scores using Visual
analogue scale (VAS), Victoria Institute of Sports Assessment – Patella (VISA – P), ultrasonography,
vertical jump test (VJT), and single leg decline (SLD) will be conducted and reassessed post treatment.
One treatment group will receive a single session of high energy ESWT and the other treatment group
will receive a single session of medium energy ESWT. Control group will receive 3000 blocked impulses
(placebo). Treatments will be conducted without the use of local anesthesia or pain medication.
2
Treatment objective: To determine if medium or high energy ESWT will demonstrate a superior
outcome for treatment of patients with chronic patellar tendinopathy versus placebo. A minimum of a 15
point increase from baseline VISA - P scores will be considered a positive outcome. Other markers such
as non-dependence on pharmacogenics for increased function, VJT and SLD will be correlated with the
VISA – P scores to provide for a more accurate final descriptive of trial outcomes.
Discussion: There seems to be a dearth of quality evidence for the treatment of patella tendinopathy
despite the abundance of treatment options available to practitioners. The use of ESWT has been seen to
be effective for the treatment of chronic plantar fasciitis and Achilles tendinopathy in several studies
(Ogden et al 2002; Carter et al 2004; Ogden et al, 2004; Furia, 2006, 2008; Wang et al 2006), as well as
from our own clinical experience, suggesting that similar outcomes may be plausible when using ESWT
for chronic patella tendinopathy. While there have been some dated and recent studies investigating the
efficacy of ESWT for patella tendinopathy there is still debate as to which type of energy levels should be
utilized. Our study hopes to answer the question: Is ESWT an effective treatment for the treatment of
chronic patella tendinopathy? While comparing two different energy levels (medium and high energy), in
a placebo controlled trial. To our knowledge this will be the first study to undertake the comparison of
both medium and high energy ESWT in a placebo controlled study for patellar tendinopathy.
Trial registration No: LRS/11/02/004
Keywords: patellar tendinitis, patellar tendinopathy, tendinopathy, patellar injury, treatment for
tendinopathy, inflammation in tendinopathy, eccentric exercises, cortisone injection for tendinopathy, NSAID’s, extracorporeal shockwave therapy, aging and tendons, overuse sports injury, injury in elite
athletes.
Corresponding authors:
Twaddle, B.
71 Merton Road,
St. Johns, Auckland,
New Zealand
Hing, W.
Auckland University of Technology
90 Akoranga Drive, North Shore City,
New Zealand
Craig, K.
Level 2, 626 Great South Road,
Ellerslie, Auckland,
New Zealand
3
Introduction
Tendinopathy is a generically used term that encompasses pain and discomfort occurring around
tendons as a result of repetitive or overuse syndromes due to sports, as well as activities of daily
living. Patella tendinopathy (PT) is a commonly seen insertional tendinopathy affecting the
physically active where activity related repetitive overload of the knee extensor mechanism is
seen to be the primary cause of complaint and disability presenting a clinical challenge for its
management (Taunton, 2003; Warden & Brunker, 2003; Wang et al 2007; Maffulli et al 2010).
Despite the clinical frequency, there are many unanswered questions and conflicting opinions as
to the etiology, pathophysiology, pain mechanisms and treatment protocols for this condition
(Fredberg & Stengaard-Pederson, 2008). Historically labeled as tendinitis, this condition which
commonly affects the posterior proximal insertion of the tendon at the inferior pole of the patella
displays a degenerative histological pattern devoid of an overt inflammatory process (Alfredson
et al 2001; Hamilton & Purdam, 2004; Wilson & Best, 2005; 2006; Lian, 2005; Magra, 2006;
Crossley et al 2007; Frohm, 2006; Maffulli et al, 2010). Although greater prevalence is seen
among volleyball and basketball players, it affects athletes and enthusiasts over a wider range of
sporting activities and is also known to occur in patients with a sedentary lifestyle (Crossley et al
2007; Lian, 2005; Maffulli et al 2010).
Clinical symptoms
Clinical symptoms may range from mild to disabling with consistent symptomatic findings
commonly presenting as focal tenderness at the inferior pole upon palpation with knee in
extension, with some patients complaining of increased stiffness around the knees in the
mornings (Warden, 2003; Hamilton, 2004; Cook et al 2005; Frohm, 2006). Pain is often
insidious with increasing intensity and frequency that may ultimately interfere with activity and
performance. Other complaints include discomfort when ascending and descending stairs, with
long periods of sitting, and sleep disruption (Warden, 2003). Patients with chronic PT often
present with some or all of the above symptoms, and at times may present with noticeable
wasting of the vastus medialis obliqus muscle with or without reduced thigh circumference and
gastrocnemius atrophy (Cook et al, 2000; Pfirrmann et al 2008).
4
Etiology
The exact etiology of patellar tendinopathy is unclear however multifactorial theories such as
tensile overload, tenocyte related collagen synthesis disruption, tendon load induced ischemia,
neural sprouting, and histological adaptive compressive responses are seen to be some of the
causative factors that give rise to pain, activity disruption and disability in the active and athletic
populations (Cook, 2000; Purdam, 2003; Warden, 2003; Hamilton, 2004; Cook et al 2005; Lian,
2005; 2006; Crossley et al 2007; Frohm, Maffulli, 2008; Maffulli et al 2010). The most
commonly accepted cause for this condition however is seen to be an overuse syndrome of the
knee joint extensor mechanism in combination with intrinsic and extrinsic factors that lead to the
progressive interference or failing of the healing response ( Cook, 2000; Witvrouw et al 2001;
Richards et al 2002; Purdam, 2003; Warden, 2003; Hamilton, 2004; Cook et al 2005; Lian, 2005;
Lian, 2006; Frohm, 2006; Crossley et al 2007; Woodley et al 2007; Maffulli, 2008; Maffulli et al
2010). Chronic patellar tendinopathy as described by Kuttenen et al; is a condition where
symptoms persist for over three months and as more recently described; is devoid of
prostaglandin mediated inflammation (Alfredson et al 2001). This suggests the term tendinitis
may be a misnomer when addressing this condition, and some of the traditional treatment
modalities aimed at inflammatory control such as non-steroidal anti-inflammatory drugs
(NSAID’s) and cortisone injections may not be the most suitable options when treating this
condition especially in chronic states (Wilson 2005; Andres & Murrell, 2008; Maffulli et al
2010). However consideration must be given to the fact that although prostaglandin related
inflammation in chronic tendinopathy may be questioned, neurogenic inflammation due to
increased expressions of neurotransmitters have the potential to initiate peritendinitis, which in
turn may lead to degenerative changes in the tendon (Hart et al 1998; Sullo et al 2001; Fredberg
& Stengaard-Pederson, 2008), hence not totally eliminating the role of inflammation in
tendinopathies further emphasizing the complexity of this condition.
Tendinopathic Pain
With the exception of those with a congenial insensitivity to pain, the experience of pain is
something that humans are familiar with (Ebrahimi-Nejad, 2007; Quniter, 2008), yet this
familiarity with pain has not allowed us to fully grasp the very nature and causative factors of
pain in chronic states (Craig, 2010), as in the case of patellar tendinopathy. Traditionally it was
thought that chronic inflammation was the cause of pain in chronic overuse tendinopathies
5
however histological findings indicate the absence of inflammatory mediated markers in
tendinopathy (Kannus & Jozsa, 1991; Astrom & Rausing, 1995; Alfredson et al 1999; Alfredson
& Lorentson, 2002(a); Alfresdon et al 2002; Fredberg & Stengaard-Pederson, 2008) and as such
pain in chronic tendinopathy may originate from a combination of biochemical and mechanical
factors (Khan et al 1999; Khan et al 2002; Sharma & Maffulli, 2005). Pain in tendinopathy may
be multifactorial and is seen to be caused by chemical and neurotransmitter substances as studies
on patients with chronic Achilles and patellar tendinopaties show an increase in levels of lactate,
glutamate, substance P and calcitonin gene related peptide (CGRP) in symptomatic groups
compared to control devoid of pro-inflammatory substances (Alfredson, 1999; Alfredson et al
2002; Sharma & Maffulli, 2005; Alfredson, 2006). Neuromodulators and transmitters such as
substance P and CGRP commonly found in unmyelinated sensory fibers have been found in
increased levels in tendinopathic Achilles and patellar tendons, and elbow epicondyles (Ljung,
2004; Sharma, 2005; Alfredson, 2006). As sensory nerves transmit pain to the spinal cord, the
increased levels of neuropeptides seen in tendinopathic condition may provide some insights and
explanation to the pain associated with these conditions (Ljung, 2004). Increased
neovascularization is seen in patellar tendinopathy but the correlation between pain and
neovasuclarization has not been fully established (Lian et al, 2006; Wang et al 2007).
Treatment options
Current conservative and non-surgical treatment options available for the management and
treatment of patellar tendinopathy include: rest, ice, massage therapy, eccentric exercise,
NSAID’s, cortisone, ultrasound therapy, LIPUS, acupuncture, electrotherapy, taping, sclerosing
injections, blood injection, glyceryl trinitrate patches, and (ESWT) extracorporeal shockwave
therapy (Warden, 2003; Visnes et al 2005; Wilson, 2005; Frohm, 2006; Warden et al 2006;
Crossley et al 2007; Murrell, 2007; Visnes & Bahr, 2007; Wang et al 2007; Maffulli, 2008;
Paoloni et al 2009; Maffulli et al 2010). Despite the abundance of therapeutic options available
to treat tendinopaties, the inconsistencies, irregularities and the lack of evidence based guidelines
for treating this condition (Wilson, 2005; Frohm, 2006; Crossley et al 2007; Andres & Murrell
2008; Maffulli & Longo, 2008) warrants the exploration of a treatment modality that may help
address these issues, especially in chronic nonresponsive tendinopathies.

6
Extracorporeal shock wave therapy (ESWT).
Extracorporeal shock waves (ESW) are acoustic pulses that transmit energy from a generator
source, presented as a single positive peak pressure pulse with a rapid peak rise time of up to
100MPa, followed by a pressure decrease within nanoseconds (Chen et al 2004; Mariotto et al
2005; Angehrn, 2008). The use of ESWT in chronic musculoskeletal injuries have demonstrated
that it is a safe and effective treatment for Achilles tendinopathy, plantar heel pain, pseudo
arthrosis, and calcerea shoulder tendinitis (Ogden, 2002; Carter et al 2004; Ogden et al 2004;
Furia, 2006; Furia 2008; Cacchio, et al, 2009; Craig, 2010). Although the exact mechanism of
the impact on human tissue of ESWT is not completely understood, research has shown that dose
dependant ESWT induces progenitor cell expression, stimulation of mesenchymal stem cell
recruitment and regeneration stimulus, endothelial nitric oxide syntheses (eNOS), neural nitric
oxide syntheses (nNOS), neovascularization (increasing regional blood circulation), transforming
growth factor ß1 (TGF ß1) mediation, collagen type I & III uptake, and a cascade of endogenous
biochemical responses including the down regulation of neurogenic inflammatory substances;
promoting physiological healing in tendon, bone and wounds (Wang, 2002; Chen et al 2004;
Mariotto et al 2005; Moretti et al 2009; Notranicola et al 2010;). Use of ESWT for knee injuries
including patellar tendinopathy have been carried out with some promising results (Vara et al,
2000; Peers, 2003; Peers et al, 2003; Taunton, 2003; Vulpiani et al 2007; Wang et al 2007;
Moretti et al 2009). However, a study recently concluded by Zwerver et al (2010) on sixty four
jumping athletes with patellar tendinopathy concluded that results were disappointing. It must be
noted that there were several disparities in this study but it is not within the scope of this paper to
discuss them at this juncture.
Design
A single centre RCT with blinded assessors and participants dived into three groups. Participants
will be divided randomly into treatment groups. (1) Receiving a single session of medium energy
ESWT, (2) receiving a single session of high energy ESWT, and (3) receiving placebo.
Treatments will be run over a two week period, with a post treatment follow-up of up to 24
weeks commencing at week 4. Patient recruitment will be from an independent referral base of
physiotherapist, sports physicians and orthopaedic surgeons. Study design, and treatment
procedure will be explained to the entire study population and an informed consent will be
7
obtained prior to trial commencement. The study geography would revolve between: the ESWT
treatment centre, the research centre of the Auckland University of Technology (AUT), and
independent sports and orthopaedic clinics located in Auckland, New Zealand. The ESWT
provider will not be blinded in this study and will not be involved in the assessment of treatment
outcomes. Outcome assessors, data collectors and participants will be blinded throughout the
study period. To our knowledge this study is the first to investigate simultaneously two different
energy flux density levels using ESWT in a placebo control trial for the treatment of patellar
tendinopathy.
Sample population
108 participants will be recruited from an independent referral network comprising of both
genders engaged in multi-sports disciplines with and age range of 18 – 35 years old. Participants
would have a clinically established condition of patellar tendinopathy confirmed by ultrasound,
and must have failed to respond to a minimum of three other treatment methods including
eccentric exercises. Baseline measurements will be carried out on all selected participants then
randomized into treatment and control groups. It is our objective to obtain sample populations
with a comparatively narrow range of deviation in age, activity and clinical presentations in
order to minimize variables and reduce the potential for α and ß errors in the final analysis
(Rothman, 2010).
Inclusion and exclusion criteria
Inclusion criterion:
Male and female participants from multi-sports disciplines (aged 18 – 35).
Clinically established tendinopathy by an independent referral panel.
Failed minimum of three other on-surgical interventions including eccentric and muscle
strengthening physiotherapy.
Injury history of 4 – 8 months.
VISA – P score of 60 and below.
Ultrasound confirmation of patellar tendinopathy.
8
Exclusion criterion:
All known contraindications to ESWT (ie pregnancy, coagulative disorders, etc.).
Received a cortisone injection within 8 weeks prior to this trial
Previous knee surgery or arthroscopic investigation.
Presence of patellar fracture.
Arthritic condition of the knee.
Injury history of < 4 months
VISA – P score of > 60
Study size
Our study hypothesizes that 80% of the participants in treatment groups should improve by a 15
point difference in VISA – P scale when compared to control. Based on this expectation with a
power of 85%, a placebo factor of 30%, and a potential for dropout rate of 20%, we require 108
participants to be dived equally into 3 groups of 36 participants.
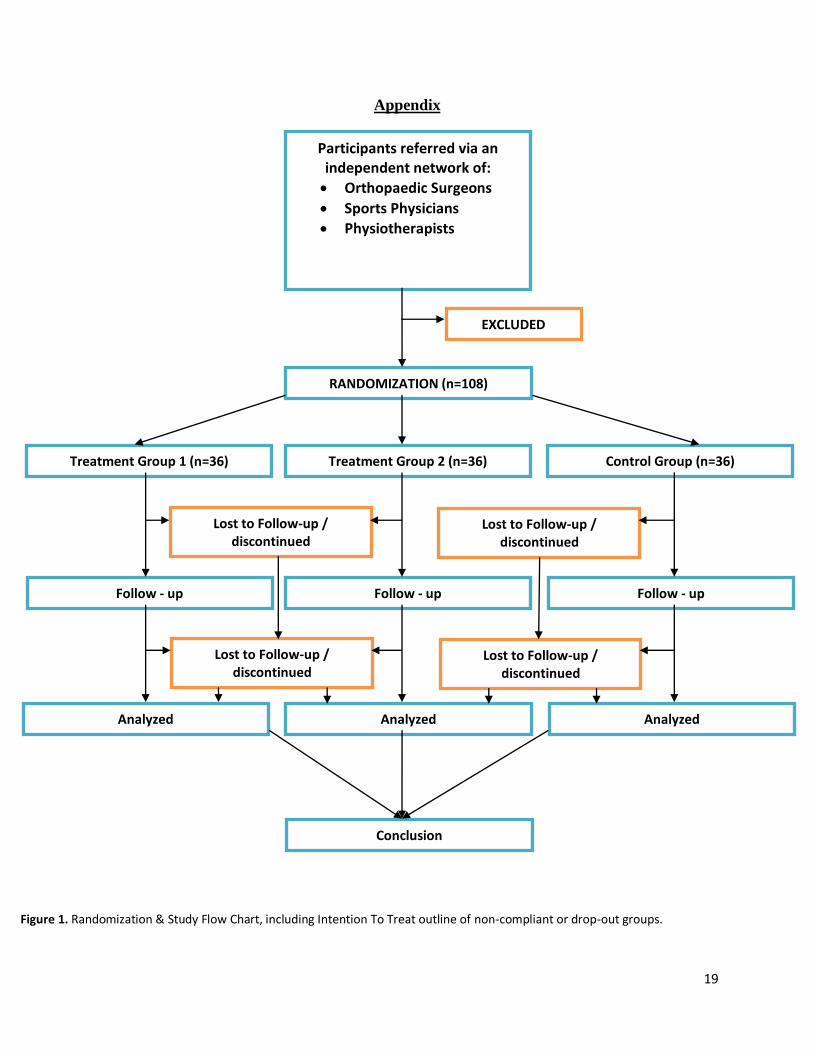
Randomization
Computer generated randomization will be carried out after final selection, briefing and informed
consent. ESWT therapist will be the only person who is not blinded to treatment groups
(Appendix Figure 1). Study will be carried out on an Intention-to-Treat (ITT) basis.
Treatment
ESWT will be conducted at a single location in Auckland by a single experienced therapist to
ensure proper and uniform ESWT application between the groups. A brief explanation of the
treatment will be provided to each participant, where they will be informed that discomfort may
be experienced and that it may vary between individuals. ESWT sessions will be carried out in
the presence of an independent senior year physiotherapy student assigned by the university to
ensure that ESWT is conducted devoid of therapist bias. All treatments will be carried out
without the use of pain medication or local anesthesia. Participants will be seated off a plinth
with knee in unsupported 90˚ flexion. Medical shockwaves will be generated by an
electrohydraulic orthopaedic device, the OrthoSpec (MediSpec Ltd., Germantown, MD). A
single session of 3000 impulses will be applied directly onto the region of interest propagated by
a water medium and coupling gel. Treatment group receiving medium energy ESWT will be
9
given 3000 impulses at energy density flux levels (EDFL) commencing at 0.12mj/mm² and
concluding at 0.22mj/mm². EDFL in group receiving medium energy will be graduated in 250
impulses increments up to 0.20mj/mm², and after 1000 impulses at 0.20mj/mm² EDFL will be
increased to 0.22mj/mm² for 1000 impulses to conclude the session. Patients receiving high
energy ESWT will receive 3000 impulses at EDFL commencing at 0.12mj/mm² and concluding
at 0.28mj/mm². EDFL graduation in this group will be graduated in 200 impulse increments up
to 0.24mj/mm², and after 1000 impulses at 0.24mj/mm² EDFL will be increased to 0.29mj/mm²
for 1000 impulses to conclude the session.
Placebo treatment
Placebo provided by the manufacturer involves a specially designed metal deflector placed inside
the treatment reflector membrane to deflect shockwaves where a non-therapeutic EDFL of below
0.02mj/mm² may be released into the focal region (Medispec, Germantown). Reflector will not
be visible to participants and sound levels during treatment will not be modified by the reflector
ensuring this aspect of uniformity between the treatment groups. Placebo group will receive 3000
impulses ranging from EDFL of 0.12mj/mm² and concluding at 0.24mj/mm², graduated at 250
pulse increments up to 0.20mj/mm², where after 1000 impulses increased to 0.24mj/mm² for
1000 impulses to conclude the session. It is to be noted that these impulses will be blocked by an
internal membrane deflector resulting in a non-therapeutic EDFL onto treatment site.
Concurrent treatment
All forms of anti-inflammatory medication will be ceased throughout the study period (although
analgesics such as paracetamol may be allowed where necessary), and participant will be
restricted to sedentary activity for 6 – 8 weeks. On week 4 graduated eccentric and strengthening
therapies may be introduced without prematurely overloading the recently rehabilitated tendon
and according to patient’s minimum threshold.
Measurement
Baseline measurements will be compared to post intervention scores commencing form week 4
post treatment, and reassessed at weeks; 8, 12 and 24. Patient data will include personal details,
10
demographics, present and past medical history leading up to the study. Adverse events will be
recorded on clinical assessment sheets should they arise.
Visual Analogue Scale (VAS)
Measures subjective activity of daily living scores and post treatment measurements such as the
vertical jump test and single leg decline on a 25˚ decline board (Purdam et al 2003).
VISA – P questionnaire
The VISA – P is a reliable instrument to measure self reported severity and changes specifically
designed for patellar tendinopathy, and has been used by many trials investigating patellar
tendinopathy internationally (Taunton, 2003; Frohm, 2006; Maffulli et al 2009, Zwerver et al
2010).
Ultrasound
The hypo-echogenity, tendon thickness and diameter, presence of neovascularization and calcific
appearance if present will be obtained and monitored by an experienced musculoskeletal
sonographer and remarked by a radiologist at baseline and at week 24. Ultrasound is more
accurate in capturing the fine internal structure and anatomic border of the patellar tendon for
confirming clinical tendinopathy (Karmel et al 2004; Warden et al 2007; Fredberg & Stengaard-
Pederson, 2008). Both sonographer and radiologist will be blinded.
Follow-up
Follow-ups will commence during weeks 4, 8, 12 and 24. Participants will be provided a journal
to record details of their treatment and injury progress on a weekly basis, these entries will be
recorded into patient files by blinded data processors.
Statistical and data analysis
Multilevel analysis will be conducted to weigh the difference between primary and secondary
endpoints of this trial and the independent variables that may occur due to the randomization
process. Further analysis will be conducted to arrive at a truly significant conclusion, where the
confidence intervals (CI) will be calculated based on both size and precision reflected by the P-
value (Rothman, 2010). Changes from baseline scores and their relevance between treatment
11
groups and placebo as well as differentials between each group will be tabulated in a 2x2
contingency table to provide greater truth when providing proof of the treatment outcomes for
this study (Bogduk, 1998). Sample size was calculated based on a power of 85% and a placebo
factor of 30% with an additional 20% dropout rate adjusted into the calculations. Based on the
participant size of each group the comparative calculations of treatment outcomes will be
calculated on a one-on-one basis; High energy vs Medium energy, High energy vs Control, and
Medium energy vs Control. At the conclusion of this study further plans to conduct longer term
follow-ups on treatment group will be planned to determine the survival curves of treatment
outcomes. ITT analysis will be conducted to reduce bias, preserve sample size, and provide for
more accurate data tabulation (Lewis & Machin, 1993; Montori & Guyatt, 2001; Sainani, 2010).
Discussion
Our study intends to investigate the efficacy of ESWT for the treatment of chronic patellar
tendinopathy unresponsive to other non-surgical methods currently used. From our personal
clinical experience of using ESWT, most of our referrals are sent for chronic unresponsive
conditions. This investigative theme and pattern is seen to be consistent when reviewing
literature investigating the use of ESWT in various tendinopathies and musculoskeletal issues.
As such the objective of our investigation using ESWT for patellar tendinopathy is thematic with
our clinical experience and published literature, and does not wish to explore the use of ESWT as
a primary therapy for patellar tendinopathy. Our study has put in place some variable controls in
order to reduce the standard deviation range, such as:
The cessation of steroidal and non-steroidal anti-inflammatory drugs (SAID’s &
NSAID’s) once participants were selected into the study. Some previous studies involving
ESWT did not allow those who were on continuous NSAID’s to participate in the study.
However our study intended to reproduce a real-life clinic situation, and therefore
allowed such participants to be included.
The equal restrictions on training and activity throughout the study period, across the
groups ensures uniformity while recognizing requirements of tendon healing.
12
Clinically diagnosed and established chronic patellar tendinopathy that have failed a
minimum of three other treatment methods. This aspect of our study removes the sole
dependence on the self reporting nature of the VISA – P instrument, reducing the
potential for α and ß errors.
This study uses two different ESWT energy levels and compares them to control; this was to
initiate an investigation that may provide greater premise and insight as to the type of energy
levels that should be selected when considering the use of ESWT for chronic patellar and other
tendinopathies.
Conclusion
Chronic patellar tendionpathy is a complex condition that causes performance disruptions and
disability especially in active populations, with the lack of an evidenced based approach for its
management and containment. When considering treatment options for overuse tendinopathies, a
thorough appreciation of the properties of a healthy tendon and the functional interplay and
mechanical properties of the musculotendon complex is necessary. The proposed mechanisms of
action of ESWT and its safety profile makes it a plausible treatment option when faced with
managing chronic tendinopathies such as patellar tendinopathy. There have been several studies
exploring the use of ESWT on patellar tendinopathy with mixed outcomes. Our study and its
design intend to integrate systemic research with a real-life clinical setting, while seeking to
demonstrate our trail objectives with a strict adherence to medical research standards. This is the
first study to compare different energy density flux levels (EDFL) with a placebo control for the
treatment of patellar tendinopathies and aims to provide some basis to establish which EDFL to
select when considering use of ESWT for this condition.
Authors: KC: Study conceptualization & design, author original manuscript, co-ethics applicant, and ESWT treatment provider. BT: Orthopaedic consultant and clinical assessor. WH: Ultrasonography, ethics applicant and clinical assessor. Conflicting interest:
KC is a Director of Kompass Health Associates,
providers of ESWT services as part of their practice.
13
Reference
Alfredson, H., Thorsen, K. & Lorentzon, R. (1999). In situ microdialysis in tendon tissue: high
levels of glutamate, but not prostaglandin E2 in chronic Achilles tendon pain. Knee Surgery,
Sports Traumatology, Arthroscopy: Official Journal of the ESSKA 7 (6) 378 – 381.
Alfredson, H., Forsgren, S., Thorsen, K. & Lorentzon, R. (2001) In vivo microdialysis and
immunohistochemical analyses of tendon tissue demonstrated high amounts of free glutamate
and glutamate NMDR1 receptors, but no signs of inflammation, in Jumper’s knee. Journal of
Orthopaedic Research 19(5) 881 – 886.
Alfredson, H., Bjur, D., Thorsen, K., Lorensen, R., Sabdstrom, P & High, P. (2002).
Intratendinous lactate levels in painful chronic Achilles tendinosis. An investigation using
microdialysis technique. Journal of Orthopaedic Research 20 (5) 934 – 938.
Alfredson, H. & Lorenson, R. (2002). Chronic tendon pain: no signs of chemical inflammation
but high concentrations of the neutransmitter glutamate. Implications for treatment? Current
Drug Targets 3(1) 43 – 54.
Alfredson, H. (2006). Strategies in treatment of tendon overuse injury. The chronic painful
Tendon. European Journal of Sports Science 6 (2) 81 – 85.
Andres, B. M. & Murrell, G. A. C. (2008). Treatment of Tendinopathy What Works, What Does
Not, and What is on the Horizon. Clinical Orthopaedics and Related Research 466 (7) 1539 –
1554.
Angehrn, F., Kuhn, C., Sonnabend, O. & Voss, A. (2008). Impact of extracorporeal shock waves
on the human skin with cellulite: A case study of an unique instance. Clinical Interventions in
Ageing, 3 (1) 175 – 182.
Astrom, M. & Rausing, A. (1995). Chronic Achilles Tendinopathy, A survey of surgical and
histological findings. Clinical Orthopaedic 12 246 – 252.
Bogduk, N. (1999). Truth in Musculoskeletal Skeletal Medicine, Truth in Therapy. Australian
Musculoskeletal Medicine. 22 - 30
Cacchio, A., Giordano, L., Colafarina, O., Rompe, J. D., Tavernese, E., Ioppolo, F., Flamini, S.,
Spacca, G. & Santilli, V. (2009). Extracorporeal Shock-Wave Therapy Compared with Surgery
for Hypertonic Long-Bone Nonunions. The Journal of Bone and Joint Surgery, 91 2589 – 2597.
Carter,M., Hall, J., Thompson, B. & Dwairy, M (2004). The Effectiveness of Extracorporeal
Shock Wave Therapy (ESWT) in the Treatment of Specific Musculoskeletal Disorders. ACC
Evidence Based Review.
14
Chen, Y. J., Wang, C. J., Yang, K. D., Kuo, Y. R., Huang, H. C., Huang, Y. T., Sun, Y. C. &
Wang, F. S.(2004). Extracorporeal shock waves promote healing of collagenase-induced
Achilles tendinitis and increase TGF-b1 and IGF-I expression. Journal of Orthopaedic Research,
22(4) 854 – 861.
Cook, J. L., Khan, K. M., Maffulli, N. & Purdam, C. (2000). Overuse Tendinosis, Not Tendinitis.
The Physician and Sports Medicine 28 (6) 2 – 12.
Cook, J. L. Malliaras, P., De Luca, J., Ptasznik, R. & Morris, M. (2005). Vascularity and pain in
the patellar tendon of adult jumping athletes: a 5 month longitudinal study. British Journal of
Sports Medicine 39 (7) 458 – 461.
Craig, K. (2010). Biopsychosocial Rehabilitation in Sports Medicine: A Case Study. NGAU
MAMAE (Real Pain) Publication of the New Zealand Pain Society, Winter – Spring.
Craig, K. (2010). Contracted treatment outcomes using extracorporeal shock wave therapy
(ESWT) 2005 – 2009: An outcomes review for the Accident Compensation Corporation.
Crossley, K. M., Thancanamootoo, Metcalf, K. B., Cook, J. L., Purdam, C. R. & Warden, S. J.
(2007). Clinical Features of Patellar Tendinopathy and Their Implications for Rehabilitation.
Journal of Orthopaedic Research 25: 1164–1175.
Ebrahimi-Nejad, G., Ebrahimi-Nejad, A., Bahrampour, A. & Kohan, S. (2007). Comparisons of
Emotion Status and Pain Perception in Neurosurgical Patients before and after Surgery. Journal
of Medical Science Research 1(1) 51 – 57.
Fredberg, U. & Stengaard-Pederson, K. (2008). Chronic tendinopathy tissue pathology, pain
mechanisms, and etiology with special focus on inflammation. The Scandinavian Journal of
Medicine & Science In Sports 18(1) 3 – 15.
Frohm, A. (2006). Patella tendinopathy – on evaluation methods and rehabilitation techniques.
Karolinska University Press, Stockholm.
Furia, J. P. (2006). High-Energy Extracorporeal Shock Wave Therapy as a Treatment for
Insertional Achilles tendinopathy. The American Journal of Sports Medicine 34(5) 733 – 740.
Furia, J. P. (2008). Jigh Energy Extracorporeal Shock Wave Therapy as a Treatment for Chronic
Non-insertional Achilles Tendinopathy. The American Journal of Sports Medicine 36(3) 502 –
508.
Hamilton, B. & Purdam, C. (2004). Patellar tendinosis as an adaptive process: a new hypothesis.
British Journal of Sports Medicine 38(6) 758 – 761.
Hart, D. A., Archambault, J. M., Kydd, A., Reno, C., Frank, C. B. & Herzog, W. (1998). Gender
and neurogenic variables in tendon biology biology and repetitive motion disorders. Clinical
Orthopaedics and Related Research 351(June) 44 – 56.
15
Kamel, M., Eid, H. & Mansour, M. (2004). Ultrasound detection of knee patellar enthesitis: a
comparison with magnetic resonance imaging. Annals of the Rheumatic Diseases 63(2) 213 –
214.
Kannus, P. & Jozsa, L. G. (1991). Histopathological changes preceding spontaneous rupture of a
tendon. A controlled study of 891 patients. Journal of Bone and Joint Surgery 73 (10)
1507 – 1525.
Kettunen, J. A., Kvist, M. K., Alanen, E. & Kujala, U. M. (2002). Long-term prognosis for
Jumper’s knee in male athletes: A prospective follow-up study. The American Journal of Sports
Medicine 30(5) 689 – 692.
Khan, K. M., Cook, J. L., Bonar, F., Harcourt, P. & Astrom, M. (1999). Histopathology of
common tendinopathies.Update and implications for clinical management. Sports Medicine 27
(6) 393 – 408.
Khan, K. M., Cook, J. L., Kannus, P., Maffulli, N. & Bonar, S. F. (2002). Time to abandon the
“tendinitis” myth. Painful, overuse tendon conditions have a non-inflammatory pathology.
British Medical Journal 16 (324) 626 – 627. Retrieved November 11, 2010 from
www.ncbi.nlm.nih.gov/pmc/articles/PMC1122566/pdf/626.pdf
Lewis, J. A. & Machin, D (1993). Intention to treat – who should use ITT?. British Journal of
Cancer 68(4) 647 – 650.
Lian, Ø. B., Engebertsen, L. & Bahr, R. (2005). Prevelance of Jumper’s Knee among elite
athletes from different sports: a cross sectional study. The American Journal of Sports Medicine
33(4) 561 – 567.
Lian, Ø., Dahl, J., Ackermann, P. W., Frihagen, F. Engebretsen, L. & Bahr, R. (2006).
Pronociceptive and antinociceptive neuromediators in patellar tendinopathy. The American
Journal of Sports Medicine 34(11):1801 – 1808.
Ljung, B. O., Alfredson, H. & Forsgren, S. (2004). Neurokinin1-receptors and sensory
neuropeptides in tendon insertions at the lateral and medial epicondyles of the humerus. Studies
on tennis elbow and medial epicondylagia. Journal of Orthopaedic Research 22 (2) 321 – 327.
Maffulli, N. & Longo, U. G. (2008). Conservative management for tendinopathy: is there enough
evidence? Rheumatology 47: 390 – 391.
Maffulli, N., Longo, U. G., Loppini, M., Spiezia, F. & Denaro, V. (2010). New options in the
management of tendinopathy. Open Access Journal of Sports Medicine 1: 29 - 37.
Maffulli, N., Longo, U. G., Loppini, M., Spiezia, F. & Denaro, V. (2010). Current treatment
options for tendinopathy. Expert Opinions in Pharmacotherapy 11(13) 2177 – 2186.
16
Maffulli, N. (2010). Disappointing results seen in randomized study of ESWT therapy for
jumper’s knee. ORTHOSuperSite http://www.orthosupersite.com/view.aspx?rid=67975
Magra, M. & Maffulli, N. (2006). Nonsteroidal antiinflammatory drugs intendinopathy: Friend
or foe. Clinical Journal of Sports Medicine16(1) 1 – 3.
Mariotto, S., Cavaleri, E., Amelio, E., Ciampa, A. R., de Pratti, A. C., Marlinghaus, E., Russo, S.
& Suzuki, H. (2005). Extracorporeal shock waves: From lithotripsy to anti-inflammatory
action by NO production. Nitric Oxide 12(2) 89 – 96.
Montori, V. M. & Guyatt, G. H. (2001). Intention-to-treat principle. Canadian Medical
Association Journal165(10) 1339 – 1341.
Moretti, B., Iannone, F., Notarnicola, A., Lapadula, G., Moretti, L., Patella, V. & Garofalo, R.
(2008). Extracorporeal shock waves down-regulate the expression of interleukin-10 and tumor
necrosis factor-alpha in osteoarthritic chondrocytes. BMC Musculoskeletal Disorders 9:16.
Retrieved September 20, 2010 from
www.biomedcentral.com/content/pdf/1471-2474-9-16.pdf
Moretti, B., Notarnicola, A., Maggio, G., Moretti, L., Pascone, M., Tafuri, S & Patella, V.
(2009). A volleyball player with bilateral knee osteochondritis dissecans treated with
extracorporeal shock wave therapy. Musculoskeletal Surgery 93(1) 37 – 41.
Murrell, G. A. C. (2007). Using Nitric oxide to treat tendinopathy. British Journal of Sports
Medicine 41: 227 – 231.
Ogden, J. A., Alvarez, R. G. & Marlow, M. E. (2002). Shockwave Therapy for Chronic Proximal
Plantar Fasciitis: A Meta Analysis.
Ogden, J. A., Alvarez, R. G., Levitt, R. L ., Johnson, J. E. & Marlow, M. E. (2004).
Electrohydraulic High-Energy Shock-Wave Treatment for Chronic Plantar Fasciitis. Journal of
Bone and Joint Surgery 86-A (10) 2216 – 2228.
Paoloni, J. A., Milne, C., Orchard, J. & Hamilton, B. (2009). Non-steroidal anti-inflammatory
drugs in sports medicine: guidelines for practical but sensible use. British Lournal of Sports
Medicine 43: 863 – 865.
Pfirrmann, C. W. A., Jost, B., Pirkl, C., Aitzetmuller, G. & Lajtai, G. (2008). Quadriceps
tendinosis and patellar tendinosis in professional beach volleyball players: sonographic findings
in correlation with clinical symptoms. European Radiology 18 (8) 1703 – 1709.
Purdam, C. R., Cook, J. L., Hopper, D. M. & Khan, K. M. (2003). Discriminate ability of
functional loading tests for adolescent jumper’s knee. Physical Therapy in Sport 4(1) 3 – 9.
17
Quinter, J. L., Cohen, M. L., Buchanan, D., Katz, J. D. & Williamson, O. D. (2008). Pain
Medicine and Its Models: Helping or Hindering? American Academy of Pain Medicine 9(7) 824
– 834.
Richards, D. P., Ajemian, S. V., Wiley, J. P., Brunet, J. A. & Zernicke, R. F. (2002) Relation
between ankle joint dynamics and patellar tendinopathy in elite volleyball players. Clinical
Journal of Sports Medicine 5 (12) 266 – 272.
Rothman, K. J. (2010). Curbing type I and type II errors. European Journal of Epidemiology 25
(4) 223 – 224.
Sainani, K. L. (2010). Making Sense of Intention-to-Treat. The American Academy of Physical
Medicine and Rehabilitation 2(3) 209 – 213.
Sullo, A., Maffulli, N., Capasso, G. & Testa, V. (2001). The effects of prolonged peritendinous
administration of PGE 1 to the rat Achilles tendon: a possible animal model of chronic Achilles
tendinopathy. Journal of Orthopaedic Science 6(4) 349 – 357.
Taunton, K. M., Taunton, J. E. & Khan, K. M. (2003). Treatment of patellar tendinopathy with
extracorporeal shock wave therapy. BC Medical Journal 45 (10) 500 – 507.
Vara, F., Garzon, N. & Ortega, N. (2000) Treatment of the patellar tendinitis with local
application of extracorporeal shock waves. Abstract from the 4th Congress of the International
Society for Musculoskeletal Shock Wave Therapy. Naples.
Visnes, H., Hoksrud, A., Cook, J. & Bahr, R. (2005). No Effect of Eccentric Training on
Jumper’s Knee in Volleyball Players During the Competitive Season A Randomized Clinical
Trial. Clinical Journal of Sports Medicine 15: 227 – 234.
Visnes, H. & Bahr, R. (2007). The evolution of eccentric training as treatment for patellar
tendinopathy (jumper’s knee): a critical review of exercise programmes. British Journal of Sports
Medicine 41: 217 – 223.
Vulpiani, M. C., Vetrano, M., Savoia, V., Di Pangrazio, E., Trischitta, D. & Ferretti, A. (2007).
Jumper's knee treatment with extracorporeal shock wave therapy: a long-term follow-up
observational study. Journal of Sports Medicine and Physical Fitness. 47(3) 323 – 328.
Wang, F. S., Yang, K. D. & Chen, R. F. (2002). Extracorporeal shock wave promotes growth
and differentiation of bone-marrow stromal cells towards osteo-progenitors associated with
induction of TGF-β1. Journal of Bone and Joint Surgery British Volume, 84(3) 457 – 461.
Wang, C. J., Ko, J. Y., Chan, Y. S., Weng, L. H., Hsu, S. L. (2007). Extracorporeal Shockwave
for Chronic Patellar Tendinopathy. The American Journal of Sports Medicine, 35(6) 972 – 978.
18
Wang, C. J., Wang, F. S., Yang, K. D., Weng, L. H. & Ko, J. Y. (2006). Long-term Results of
Extracorporeal Shockwave Treatment for Plantar Fasciitis. American Journal of Sports Medicine
34 (4) 592 - 596
Warden, S. J. & Brukner, P. (2003). Patellar Tendinopathy. Clinical Sports Medicine 22: 743 –
759.
Warden, S. J. (2003). A New Direction for Ultrasound Therapy in Sports Medicine. Sports
Medicine 33 (2) 95 – 107.
Warden, S. J., Metcalf, B. R., Kiss, Z. S., Cook, J. L., Purdam, C. R., Bennell, K. L. & Crossley,
K. M. (2006). Low-intensity pulsed ultrasound for chronic patellar tendinopathy: a randomized,
double-blind, placebo-controlled trial. Rheumatology 47 (4) 467 – 471.
Warden, S. J., Kiss, Z. S., Malara, F. A., Aoi, J. B., Cook, J. L. & Crossley, K. M. (2007).
Comparative accuracy of magnetic resonance imaging and ultrasonography in confirming
clinically diagnosed patellar tendinopathy. The American Journal of Sports Medicine 35(3) 427
– 436.
Wilson, J. J. 7 Best, T. M. (2005). Common Overuse Tendon Problems: A Review and
Recommendations for Treatment. American Academy of Family Physicians 72(5) 811 – 818.
Witvrouw, E., Bellemans, J., Lysens, R., Denneels, L. & Cambier, D. (2001) Intrinsic risk
factors for the development of patellar tendinitis in a athletic population. A two year prospective
study. The American Journal of Sports Medicine 29 (2)190 – 195.
Woodley, B. L., Newsham – West, R. J. & Baxter, G. D. (2007). Chronic tendinopathy:
effectiveness of eccentric exercise. British Journal of Sports Medicine 41: 188 – 199.
Zwerver, J., Verhagen, E., Hartgens, F., Akker-Scheek, I. & Diercks, R. L (2010). The
TOPGAME-study: effectiveness of extracorporeal shockwave therapy in jumping athletes with
patellar tendinopathy. Design for a randomized controlled trial.
BMC Musculoskeletal Disorders 11:28.
19
Appendix
Participants referred via an independent network of:
Orthopaedic Surgeons
Sports Physicians
Physiotherapists
Control Group (n=36) Treatment Group 2 (n=36) Treatment Group 1 (n=36)
Follow - up Follow - up Follow - up
RANDOMIZATION (n=108)
Lost to Follow-up / discontinued
Analyzed
Lost to Follow-up / discontinued
Analyzed
Conclusion
Analyzed
EXCLUDED
Lost to Follow-up / discontinued
Lost to Follow-up / discontinued
Figure 1. Randomization & Study Flow Chart, including Intention To Treat outline of non-compliant or drop-out groups.