Embed Size (px)
Citation preview

Tubercle 66 (1985) 179-186 0 Longman Group Ltd.
TUBERCULOSIS IN AN INDOCHINESE REFUGEE CAMP: EPIDEMIOLOGY, MANAGEMENT AND THERAPEUTIC RESULTS
Hans L. Rieder”
Thai/Swiss Red Cross TB Programme, Thai Red Cross Society, Chulalongkorn Hospital, Bangkok, Thailand
Summary In a 3-year period tuberculosis was diagnosed in 629 patients in Thailand’s largest camp for Kampuchean refugees: 62 % had pulmonary disease and 38 % extrapul- monary forms. Tuberculosis of lymph nodes was the most important extrapulmon- ary manifestation (50 %). The mean annual notification rates were 0.5 % and 0.24 % for all forms and smear-positive pulmonary tuberculosis respectively. There was a steep rise in the annual notification rate with increasing age. A 6-month course of fully supervised chemotherapy efficiently counteracted defaulting, early abscond- ing and initial drug resistance. Seventy-three per cent of all patients remained on chemotherapy for the planned period; only 2 % of the smear-positive patients failed bacteriologically on chemotherapy. Of the patients with the most common forms of extrapulmonary disease, 90 % showed a favourable response to chemotherapy.
R&urn6 En 3 ans, la tuberculose a ete diagnostiquee chez 629 malades dans le plus grand camp de refugies kampucheens en Thai’lande: 62 % avaient une forme pulmonaire et 38 % des formes extra-pulmonaires. La tuberculose des ganglions lymphatiques etait la forme extra-pulmonaire la plus importante (50 %I. Les taux moyens de declaration etaient de 0,5 % et 0,24 % par an pour la tuberculose toutes formes et pour la tuber&lose pulmonaire a frottis positifs respectivement. Le taux annuel de declaration augmentait avec I’Bge. Un traitement de 6 mois par une chimiotherapie entierement supervisee a contre efficacement les defaillances, les abandons precoces et al resistance initiale aux medicaments. Soixante-treize pour cent des malades sont rest& sous traitement pour toute la periode prevue; pour seulement 2 % des malades a frottis positifs, I’examen bacteriologique montrait un echec de la chimiotherapie. Parmi les malades ayant une tuberculose extra-pulmonaire, 90 % ont repondu favorablement a la chimiotherapie.
Resumen En un period0 de 3 arias se diagnosticaron 629 cases de tuberculosis en el campo mas grande de refugiados provenientes de Kampuchea, en Tailandia. El 62 % de estos enfermos presentaba una tuberculosis pulmonar y el 38 % una forma extra pulmonar. La localization extra pulmonar m&s importante fue la ganglionar (50 %). Las tasas anuales de notification fueron en promedio 0.5 % y 0.24 % para todas las formas y para la tuberculosis pulmonar con baciloscopia positiva, respectivamente. La tasa anual de notification aumentaba con la edad. Un tratamiento de 6 meses
*Requests for reprints should be addressed to: Dr Hans L. Rieder, Division of Tuberculosis Control, Center for Prevention Services, Centers for Disease Control, Atlanta, Georgia 30333 U.S.A.
180 Rieder
con una quimioterapia enteramente supervisada permitio controlar eficazmente 10s abandonos precoces y la resistencia initial a 10s medicamentos. El 73 % del total de 10s pacientes prosiguieron la quimioterapia durante todo el period0 previsto; solo en le 2 % de 10s pacientes con baciloscopia positiva se registrd un fracas0 desde el punto de vista bacteriologico durante la quimioterapia. En el 90 % de 10s pacientes con forma extra pulmonar importante se observe una respuesta favorable a la quimioterapia.
Introduction Organization of health services in temporary refugee settlements is becoming an increasing problem-the number of refugees in the ‘zones of crisis’ alone exceeds 3 million people [I]. The largest Holding Centre for Kampuchean Refugees in Thailand, Khao-I-Dang, was opened in November 1979 and gave shelter initially for 140 000 Kampucheans. It was originally planned to provide an area of 5.6 hectares per 1000 population, and the area of the camp was 2.3 km* in 1982-1983 when the camp census ranged from 40 000 to 68 000 refugees (3.4 to 5.7 hectares per 1000 population). The health infrastructure of the camp was provided by international agencies under the auspices of the United Nations High Commissioner for Refugees, who provided shelter, food, water, and medicaments. As tuberculosis was considered to be a major public health problem, one of the agencies, the Thai/Swiss Red Cross, was entrusted with case-finding and chemotherapy. The approach to the tuberculosis problem was determined by two major factors. First, the population census showed marked fluctuations and second, the camp had a well-defined area. The former aspect forced the planners to choose the shortest possible effective drug regimen, whereas the latter permitted, in principle, full supervision of drug administration. The results with fully supervised short-course chemotherapy over a 3-year period are presented here.
Materials and methods Background of the Tuberculosis Programme
The camp had a central hospital area offering medical services in surgery, internal medicine, obstetrics and gynaecology, paediatrics, leprosy, rehabilitation, and prosthetic limb replacement. Patients presented themselves to one of the 4 outpatient dispensaries in the camp and, if suspected as having tuberculosis, were then referred to the tuberculosis clinic, The tuberculosis hospital had 30 beds, a pharmacy, a consultation room, a dispensary for outpatients, a laboratory with facilities for direct smear microscopy by the Ziehl-Neelsen staining technique, and a home-made incubator (light bulbs as heat-source controlled by a thermostat) for incubation of inoculated Lowenstein-Jensen media. Routine patient work-up included a m-.dical history, physical examination, chest radiograph, examination of 3 to 6 smears for acid-fast bacilli of early morning sputum, and a culture from the specimen giving the first positive or last negative smear in the series in the case of adult patients with suspected pulmonary tuberculosis and children able to produce sputum. In cases of suspected extrapulmonary tuberculosis bacteriological examinations were made from accessible superficial lesions or abscesses, and in rare instances biopsy specimens were sent to Bangkok for histological examination.
Tuberculin sensitivity was tested in the majority of patients (71 %) using the Mantoux technique with 5 TU PPD RT 23, measuring the mean diameter of induration after 48 to 72 hours.
BCG was given at birth to children born in the camp and to all others under 1 year of age. No active follow-up was performed after completion of chemotherapy.
Tuberculosis in a Refugee Camp 181
Patient characteristics were analyzed with regard to form and site of tuberculosis, age, sex, and during a period of relative stability of the population census in the camp to age-specific notification rates. Patients with multiple sites of tuberculosis were classed as single cases for statistical analysis.
Chemotherapy Criteria to start chemotherapy were as follows:
Pulmonary tuberculosis
a. Adults-Positive bacteriology (smear and/or culture) or significant (IO mm or more) tuberculin skin test reaction plus clinical signs compatible with tuberculosis plus 4-8 weeks observation (the latter only in absence of gross haemoptysis). b. Children (5 to 14 years of age)-Positive bacteriology or significant tuberculin skin test reaction plus clinical signs compatible with tuberculosis. c. Children younger than 5 years of age-Positive bacteriology or significant reaction to the tuberculin skin test.
Extrapulmonary tuberculosis
Positive bacteriology or suggestive histology or significant tuberculin skin test reaction plus clinical signs compatible with tuberculosis (exception: a positive skin test was not required for treatment of suspected meningeal tuberculosis and in patients with a miliary pattern on the chest film).
Chemotherapy was routinely ambulatory after an initial hospitalization period of 2 weeks. Family contact investigations were conducted during this period. Treatment was daily and fully supervised throughout the course. Patients had to attend one of the three dispensaries (two outposts in addition to the central dispensary to facilitate access to drug administra- tion) in the camp and swallow their drugs in front of a supervisor. Urine was checked at random (at least once per month, and more often in selected cases) for the orange colouration of rifampicin. If patients missed 2 consecutive days, they were actively sought in the camp. The number of absent patient-days was calculated for a randomly selected month and in a series of patients who had completed therapy.
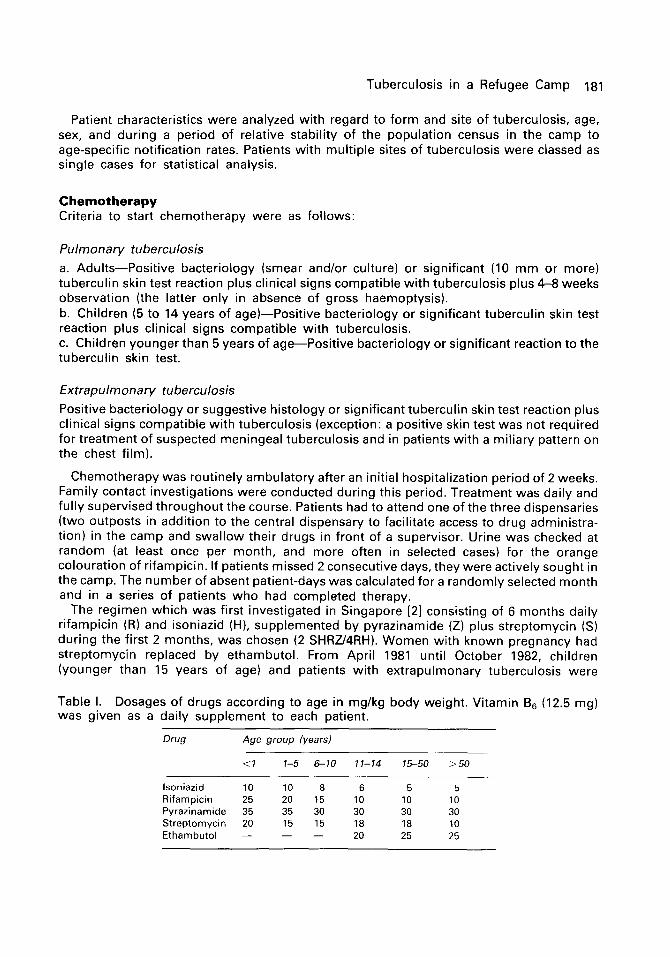
The regimen which was first investigated in Singapore [21 consisting of 6 months daily rifampicin (RI and isoniazid (H), supplemented by pyrazinamide (Z) plus streptomycin (S) during the first 2 months, was chosen (2 SHRZ/4RH). Women with known pregnancy had streptomycin replaced by ethambutol. From April 1981 until October 1982, children (younger than 15 years of age) and patients with extrapulmonary tuberculosis were
Table I. Dosages of drugs according to age in mg/kg body weight. Vitamin B6 (12.5 mg) was given as a daily supplement to each patient.
Drug Age group (year.4
<l l-5 6-10 11-14 15-50 >50
lsoniazid 10 10 8 6 5 5 Rifampicin 25 20 15 10 10 10 Pyrazinamide 35 35 30 30 30 30 Streptomycin 20 15 15 18 18 10 Ethambutol - - - 20 25 25
182 Rieder
assigned to a similar regimen, but given for 9 months and omitting pyrazinamide; subsequently, all patients were given the same regimen regardless of form and age. We gave the drugs in single daily doses according to age and body weight (Table I). Progress on chemotherapy in patients with smear-positive pulmonary tuberculosis was assessed by means of three sputum smear examinations each month, with the results quantitatively graded as recommended by the American Thoracic Society [3]. Therapeutic progress among children and patients with extrapulmonary tuberculosis was assessed clinically.
Results Patient characteristics
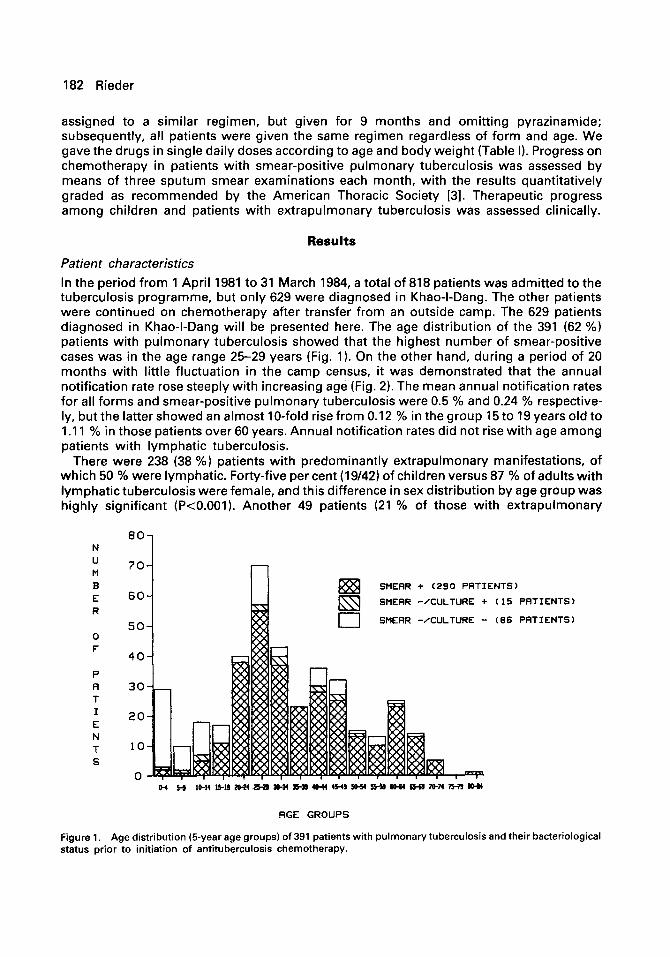
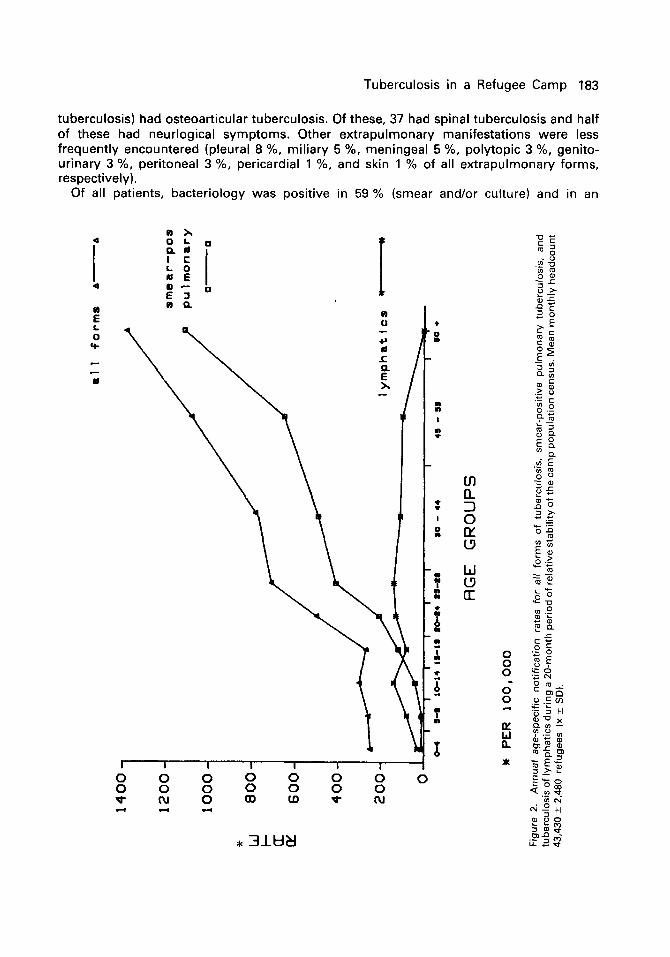
In the period from 1 April 1981 to 31 March 1984, a total of 818 patients was admitted to the tuberculosis programme, but only 629 were diagnosed in Khao-I-Dang. The other patients were continued on chemotherapy after transfer from an outside camp. The 629 patients diagnosed in Khao-I-Dang will be presented here. The age distribution of the 391 (62 %) patients with pulmonary tuberculosis showed that the highest number of smear-positive cases was in the age range 25-29 years (Fig. 1). On the other hand, during a period of 20 months with little fluctuation in the camp census, it was demonstrated that the annual notification rate rose steeply with increasing age (Fig. 2). The mean annual notification rates for all forms and smear-positive pulmonary tuberculosis were 0.5 % and 0.24 % respective- ly, but the latter showed an almost IO-fold rise from 0.12 % in the group 15 to 19 years old to 1 .I 1 % in those patients over 60 years. Annual notification rates did not rise with age among patients with lymphatic tuberculosis.
There were 238 (38 %) patients with predominantly extrapulmonary manifestations, of which 50 % were lymphatic. Forty-five per cent (19/42) of children versus 87 % of adults with lymphatic tuberculosis were female, and this difference in sex distribution by age group was highly significant (PcO.001). Another 49 patients (21 % of those with extrapulmonary
80-l
N u M
70-
B E 60- R
so- 0 F
40- P
SMERR + (290 PRTIENTS)
SMERR -/CULTURE + (15 PATIENTS)
SMEAR -/CULTURE - (66 PATIENTS)
RGE GROUPS
Figure 1. Age distribution (5-year age groups) of 391 patients with pulmonary tuberculosis and their bacteriological status prior to initiation of antituberculosis chemotherapy.
Tuberculosis in a Refugee Camp 183
tuberculosis) had osteoarticular tuberculosis. Of these, 37 had spinal tuberculosis and half of these had neurlogical symptoms. Other extrapulmonary manifestations were less frequently encountered (pleural 8 %, miliary 5 %, meningeal 5 %, polytopic 3 %, genito- urinary 3 %, peritoneal 3 %, pericardial 1 %, and skin 1 % of all extrapulmonary forms, respectively).
Of all patients, bacteriology was positive in 59 % (smear and/or culture) and in an

184 Rieder
additional 4 % a suggestive histology was reported. Bacteriological proof was most often obtained in patients with pulmonary tuberculosis (78 %), and among these more often in adults than in children (Figure 2).
The distribution of the size of tuberculin reaction by diagnostic categories is shown in Fig. 3. While few of the patients had small (5-9 mm) reactions, the percentage of patients with no reaction (O-4 mm) increased with severity of the form, so that 43 % of those with disseminated and/or meningeal tuberculosis had no reaction compared with 8 % and 2 % in patients with pulmonary and lymphatic tuberculosis respectively. The mean reaction size of those with reactions of 25 mm tended to be larger in those with lymphatic (22.1 mm) than in those with pulmonary tuberculosis (19.8 mm) (Student t test p<O.O02).
Compliance and treatment outcomes
Compliance with medication was quite good. Forty-six of 4,035 prescribed days of chemotherapy (I.14 %) were spontaneously missed by patients during a month selected at random. Of the first 49 patients who completed a 6-month course of chemotherapy for smear-positive pulmonary tuberculosis, the mean of definitely missed days was 1.62 %, the range O-5 %. Of the 558 patients who began treatment before 1 October 1983, and should have completed their course by 31 March 1984: 73 % had remained in the programme for the planned course, 15 % had been transferred to other camps, 7 % had absconded (returning to Kampuchea) and 5 % died during treatment.
TUBERCULIN SKIN TEST C5TU PPD RT 23)
P E R C E N T R G E
0 F
R E R C T 0 R s
50
40
30
20
10
0
1 6 -* LYMPHRTIC
-m PULMONRRY
__ _ __A MILIRRY/MENINGEAL/POLYTOPIC
MERN DIAMETER (MM)
Figure 3. Reaction to 5 TU PPD RT 23 (mean diameter of induration after 48-72 hours) in 463 patients: 328 patients with pulmonary tuberculosis, 107 patients with tuberculosis of lymphatics and 28 patients with miliary/polytopic/ meningeal tuberculosis. The percentage of reactors in each 5 mm group is shown.
Tuberculosis in a Refugee Camp 185
Smear-positive pulmonary tuberculosis
The mortality rate among patients with smear-positive pulmonary tuberculosis receiving any chemotherapy (at least 1 day) was 3.9 % as compared with 0 % among patients with lymphatic tuberculosis and 33 % among those with meningeal tuberculosis. In those patients who remained on chemotherapy for the planned course (183 patients) the bacteriological monthly smear results were divided into 3 categories:
1. One hundred and sixty-four (90 %) patients had a favourable bacteriological response, converting within 3 months and never showing any positive smear during the last 3 months of chemotherapy.
2. Fifteen (8 %) patients had a doubtful bacteriological response, defined as those who responded well, but had one or more occasional positive smears during the last 3 months.
3. Four (2 %) patients with bacteriological treatment failure, responding well during the intensive phase, but subsequently showing persistent acid-fast bacilli in the last 3 months.
Adverse drug reactions
Although untoward effects to drugs were common, they were usually mild and did not require a fundamental change of regimen. In smear-positive pulmonary cases, adverse reactions were reported by 48 of 183 (26 %) patients. These were attributed usually to one, but occasionally more, drugs. Although side-effects were common, only 3 % of patients required permanent withdrawal of a drug. There were 16 % with adverse reactions attributable to streptomycin; 8th cranial nerve toxicity required reducing dosage in 4 % and discontinuing streptomycin in 3 %. There were 11 % with arthralgias attributable to pyrazinamide, none of which required withdrawal of the drug. Just 2 % had reported side effects related to rifampicin (nausea), not requiring any change except ingestion of the drug after breakfast, and 2 % developed jaundice during treatment which subsided with only temporary withdrawal of the potentially hepatotoxic drugs.
Extrapulmonary tuberculosis
Seventy-two of the 79 (91 %) patients with tuberculosis of lymph nodes who remained in the programme for the planned period had a favourable clinical outcome on chemotherapy.
Of the 27 patients with tuberculosis of the spine who remained in the programme, 24 (89 %) had a favourable outcome, 2 patients died and one remained paraplegic.
The outcome in patients with other extrapulmonary manifestations was similar with the exception of those with tuberculous meningitis. Of these 12 patients, 4 died, 4 had no sequelae and 4 were left with neurological disability.
Discussion Patient compliance with antituberculous chemotherapy remains today the major problem for tuberculosis control in both technically advanced and developing countries. The problem of noncompliance may be especially great in refugee settlements [41. To overcome this problem, we chose to use a fully supervised treatment regimen of 6 months duration. In Singapore, this regimen resulted in a 98 % cure rate [21. The same regimen gave similar results in Britain [51. While 10 % of our patients had one or more positive smears in the last 3 months of the 6-month course, only 2 % definitely failed on this regimen. The evidence from quality control studies suggests that even isolated positive cultures during or after chemotherapy have little significance IS, 71, but the importance of such bacteriological
186 Rieder
findings remains controversial [81. Unfortunately, we have no long-term follow-up data on relapses.
The prevalence of resistance to isoniazid and/or streptomycin is reportedly high among Indochinese refugees [9]. The 4-drug combination apparently overcame initial drug resistance in the majority of cases. The system of daily supervision of drug administration was clearly the determining factor for the apparent high success rate in the treatment of both extrapulmonary and pulmonary tuberculosis. The short course efficiently counteracted loss of patients due to absconding and transfers to other camps.
There are dilemmas in choosing a regimen for the treatment of tuberculosis among refugees. Because rifampicin and pyrazinamide, both expensive, are important drugs to enable curtailing of the conventional 12-month regimens to 6 months, the factor of drug cost is a point of serious consideration. On the other hand, as the experience in the Somali refugee camps demonstrates [4], the use of less expensive, but longer, regimens carries with it the danger of less efficient tuberculosis control.
We feel justified in concluding, from our experience in Thailand’s largest refugee camp, that the use of a fully supervised 6-month chemotherapy regimen compensated for the additional drug expense and seemed to be the appropriate strategy for tuberculosis control in this temporary settlement for Kampuchean refugees.
Acknowledgements
The author thanks K. Trikham, P. Trikham, S. Suwanavit, and D. Pitak for their dedication to the programme; and Drs R. O’Brien, L. Farer, and D. Snider, Jr., for helpful comments on the manuscript; and B. Ledergerber and G. Caras for statistical help; and S. Hussain for typing the manuscript. This programme was made possible with financial support from the Swiss Government and Enfants du Monde.
References 1 United Nations High Commissionar for Refugees. Geographie de I’exil. Chiffres au ler Janvier 1983. 2 Singapore Tuberculosis Service/British Medical Research Council. (1981). Clinical trial of g-month and 4-month
regimens of chemotherapy in the treatment of pulmonary tuberculosis: the results up to 30 months. Tubercle, 62, 95.
3 American Thoracic Society. (1981). Diagnostic standards and classification of tuberculosis and other mycobacte- rial diseases (14th edition). American Review of Respiratory Diseases, 123, 343.
4 Shears, P. (1984). Tuberculosis control in Somali refugee camps. Tubercle, 65, 111. 5 British Thoracic Society. (1984). A controlled trial of 6 months’ chemotherapy in pulmonary tuberculosis. Final
report: results during the 36 months afterthe end of chemotherapy and beyond. BritishJournalofDiseases of the Chest, 76. 330.
6 Aber, V. R., Allen, B. W., Mitchison, D. A., Ayuma, P., Edwards, E. A., & Keyes, A. B. (1980). Quality control in tuberculosis bacteriology. 1. Laboratory studies on isolated positive cultures and the efficiency of direct smear examination. Tubercle, 61, 123.
7 Mitchison, D. A., Keyes, A. B., Edwards, E. A., Ayuma, P., Byfield, S. P., & Nunn, A. J. (1980). Quality control in tuberculosis bacteriology. 2. The origin of isolated positive cultures from the sputum of patients in four studies of short course chemotherapy in Africa. Tubercle, 61, 135.
8 Buechner, H. A. (1981). Correspondence. Short course chemotherapy for tuberculosis-a story of flawed studies. From the authors: Stead, W. W., & Dutt, A. K. In reply: Farer, L. S., Long, M. W., Snider, D. E., & Ziersky, M. In reply: Citron, K. M., Angel, J. H. & Somner, A. R. From the authors: Darbyshire, J., Fox, W., Girling, D. J., Nunn, A. J., & Mitchison, D. A. American Review of Respiratory Diseases, 124, 655.
9 Rowan, R. D., Brewin, A. W., Hopewell, P. C., Slutkin, G., Chin, J., Anderson, K., Leahy, R. H., Smith, B., &Allard, J. A. (1981). Drug resistance among Indochinese refugees with tuberculosis. Morbidity and Mortality Weekly Report, 30. 373.