Embed Size (px)
Citation preview

J. clin. Path., 29, Suppl. (Roy. Coil. Path.), 10, 111-131
Trophoblastic tumours
The histopathology of trophoblastic tumoursC. W. ELSTON
From the Department ofPathology, City Hospital, Nottingham
Two important advances in the last 40 years havehad a profound effect on the prognosis of patientswith trophoblastic tumours. In the first place theapplication of gonadotrophin assay, initially bybiological methods and then by the more accurateradioimmunological methods, to the diagnosticproblems of patients with trophoblastic disease hasmade their management considerably easier. Sec-ondly the discovery that choriocarcinoma, previouslyamong the most rapidly fatal of all tumours, wasamenable to treatment with cytotoxic agents hasrevolutionized therapy, with a reduction in thecrude death rate from over 85% to less than 20 %.
It has been increasingly suggested that with thegrowing use of diagnostic aids such as gonado-trophin assay, arteriography and radiography, theusefulness of histological examination has diminished.In some cases this is true; for instance, in thefollow up of a patient with hydatidiform mole, when,in the face of a persistently raised gonadotrophinexcretion, it may be inadvisable to delay treatmentby waiting for histological confirmation of thediagnosis. Nevertheless, curettage is still widelyused as the initial diagnostic procedure in theinvestigation of uterine bleeding, and it is in thissituation that the histopathologist will be con-fronted by the problem of the difficult trophoblasticcuretting. Furthermore, the final diagnosis of malig-nancy, with trophoblastic as with any other tumour,should still ideally be made on histological grounds.Failure to recognize this has resulted in exaggeratedclaims for cure rates, by including in a malignantcategory, without histological proof, cases whichhave pursued an apparently benign course.A major drawback in investigating these tumours
fully has been the difficulty in collecting togetherenough cases for a detailed study. For instance, inBritain most clinicians and pathologists are unlikelyto see more than two or three cases of chorio-carcinoma in their professional lives. The authorwas particularly fortunate in being associated withDr Kenneth Bagshawe's Unit at Charing CrossHospital, London, for a number of years, with
access to the pathological material and case recordsof over 200 patients with trophoblastic disease. It ison this material that the current review of thepathological aspects of trophoblastic disease is based.
Classification of Trophoblastic Disease
Although there are those who maintain that inclassifying diseases we conceal more than weclarify, most accept that some form of classificationis necessary. This is particularly true in the case ofneoplasms, where an ideal classification carries animplication of prognosis, and the choice of therapymay depend on the tumour type. The basis ofmodernclassifications of trophoblastic neoplasia was pro-vided by Ewing (1910) who thought that moreimportance could be attached to histologicalappearances in relation to the degree of malignancythan had previously been claimed. He grouped alltrophoblastic tumours under the general term'chorioma' and recognized the following sub-divisions: (1) hydatid mole, (2) chorioadenomadestruens, (3) choriocarcinoma, (4a) syncytialendometritis, (4b) syncytioma.At first sight it may seem incongruous to include
hydatidiform mole in a classification of tropho-blastic tumours, since a mole is essentially a parti-cular type of abortion, and in the great majority ofcases there are no neoplastic sequelae. Theoreticalconsiderations of the malignant potential of molartrophoblastic hyperplasia have received muchattention (Hertig and Sheldon, 1947; Schopper andPliess, 1949; Park, 1971), but the important practicalpoint is that in at least 50% of cases choriocarcinomais preceded by a hydatidiform mole. This undoubtedclose association makes it eminently sensible toplace the two lesions together in the same classi-fication.The precise status of Ewing's second group of
chorioma, the chorioadenoma destruens, has alsobeen questioned. In the first place the term itself,derived from the idea that the chorionic villus is agland, and the lesion relatively benign, has not found
111
copyright. on O
ctober 23, 2020 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.s3-10.1.111 on 1 January 1976. D
ownloaded from

C. W. Elston
universal favour. This has been more fully discussedby Park (1971) who argues persuasively in favour of'invasive hydatidiform mole' as an alternative. Amore important point is the question of its neoplasticpotential. Tow (1966) considered that invasive moleshould be renamed 'villous choriocarcinoma' andthat choriocarcinoma be called 'avillous chorio-carcinoma'. He argued that the villous form wasmerely an early stage of the avillous form and that, inhis practice at least, both lesions received essentiallythe same type of treatment. This, of course, is notthe case in Europe and the United States, and Tow'sclassification has not been well received (Bagshawe,1969; Park, 1971). This point will be referred toagain, but from the practical point of view therecertainly seem to be good grounds for retaining thedistinction between the two lesions.
INTERNATIONAL UNION AGAINST CANCERCLASSIFICATION OF TROPHOBLASTICNEOPLASIA A = GESTATIONAL; B = NON-GESTATIONALPark (1971) has recently made a plea for the moregeneral adoption of the classification, proposed by acommittee of the International Union againstCancer (1967), which has the advantage of bothclinical and pathological categories, as shown below:
Clinical Diagnosis Morphological Diagnosis
1 Non-metastatic 1 Hydatidiform mole2 Metastatic a Non-invasive
a Local (pelvic) b Invasiveb Extrapelvic 2 Choriocarcinoma
3 Uncertain
A disadvantage of this classification is the'uncertain' category which will probably be thelargest group in the present era when so manypatients receive chemotherapy before a tissuediagnosis is established. Elston and Bagshawe haveused the terms 'persistent trophoblastic prolifera-tion' and 'persistent trophoblastic disease' in anattempt to be more precise (Elston, 1970; Elstonand Bagshawe, 1972a and b), and the latter isperhaps less cumbersome. The classification by theInternational Union against Cancer deliberatelyexcludes 'syncytioma' or 'syncytial endometritis'from the spectrum of trophoblastic neoplasia, and,although Ewing (1910) and Hertig and Sheldon(1947) considered these lesions to be chorio-carcinomas of limited malignancy, there is noconvincing evidence for this view, and they are bestregarded as an exaggerated form of placental sitereaction. Nevertheless, placental site reaction, andthe exaggerated form in particular, may cause signi-ficant diagnostic difficulty, both clinically andpathologically, and for this reason, and for the sake
of completeness, the following modification of themorphological classification by the InternationalUnion against Cancer is offered:
MODIFIED PATHOLOGICAL CLASSIFICATION OFGESTATIONAL TROPHOBLASTIC DISEASE1 Placental site reaction
a Normalb Exaggerated
2 Hydatidiform molea Non-invasiveb Invasive
3 Persistent trophoblastic disease4 Choriocarcinoma.
Hydatidiform Mole
A hydatidiform mole is an abnormal product ofgestation, usually associated with a blighted ovum.The morphological features of the 'classical' mole
are so well described in the standard textbooks ofpathology and gynaecology that they need littlediscussion here. It is recognized grossly by its
,AAS:4'"h_
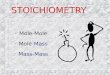
Fig 1 Hydatidiform mole, with marked stromal hydropicchange, absent stromal blood vessels and slight tropho-blastic hyperplasia. H & E x 50.
112
copyright. on O
ctober 23, 2020 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.s3-10.1.111 on 1 January 1976. D
ownloaded from

The histopathology of trophoblastic tumours
typical 'bunch of grapes' appearance and the micro-scopical features (fig 1) are: (a) hydropic swelling ofthe villous stroma giving rise to vesicles (thesevarying from 0 1 to 3 cm in diameter); (b) absence,or virtual absence, of fetal stromal blood vessels;(c) a variable degree of trophoblastic hyperplasia.
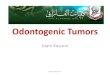
HYDROPIC CHANGE IN THE PLACENTAAlthough no difficulty should be experienced indistinguishing a typical hydatidiform mole from'normal' placental tissue derived from a spontaneousor therapeutic abortion (fig 2), a 'hydropic abortion'may give rise to diagnostic problems. In the latterthere are no obvious gross abnormalities (or at mostan occasional vesicle is seen), but microscopically avariable number of hydropic chorionic villi ispresent. Such hydropic change in placental tissuehas long been recognized as a relatively commonfinding in abortuses (Meyer, 1919) and has beeninvestigated in detail by Hertig and Edmonds (1940)and by Nilsson (1957). The practical implications ofthe problem are quite clear (Park, 1971). If theprocess that causes the hydropic abortion is thesame biologically as that which causes the classicalhydatidiform mole, then the lesion is important, andthe same close follow up which is given to patientswith the classical lesion should also be applied tothose with a hydropic abortion. If the process is notthe same then the lesion is insignificant. Unless thisquestion can be answered satisfactorily there willalways be the danger of inadequate follow up ofpatients who are at risk of developing postmolarchoriocarcinoma or over supervision of patients whohave no likelihood of developing choriocarcinoma.From their comprehensive investigation into thegenesis of hydatidiform mole Hertig and Edmonds(1940) had no doubt that focal hydropic change inabortuses was part of a spectrum of changes leadingup to the classical hydatidiform mole. They founda high incidence of 'blighted ova' in products ofspontaneous abortion, with hydropic change in67% of those with pathological ova and only 12%of those with non-pathological ova. These findingshave been substantially confirmed by Nilsson (1957),who also found hydropic change to be more frequentwith abnormal ova. Hertig and Edmonds concludedthat the primary abnormality was early death of thefetus with failure of development of the chorionicblood vessels, leading to accumulation of fluid inthe stroma in the presence of continuing secretoryactivity by the trophoblast. They introduced theconcept of the 'transitional hydatidiform mole' inwhich the embryo is either abnormal or absent,grossly the placental tissue shows only occasionalvesicles, and yet microscopically there is widespreadhydatidiform degeneration of the villi, with focal
113
Fig 2 Normal chorionic villifrom a therapeutic abortionat seven weeks' gestation. Note the regular two-layeredtrophoblastic layer, and the nucleated fetal red cells instromal blood vessels. Haematoxylin and eosin x 175.
trophoblastic hyperplasia.Park, who has long maintained his opposition to
the concept that molar change is caused by earlyfetal death (Park, 1959, 1967, 1971), feels that toomuch emphasis has been placed on the hydropicdegeneration and too little attention paid to thetrophoblastic hyperplasia. He has proposed that thetrophoblastic proliferation may be the primarylesion, with oversecretion by the abnormal tropho-blast leading to villous hydrops and thus vascularobliteration and blighting of the embryo. Whichevertheory is correct, if we return to the practicalimplications of the problem, it is certainly true thatthe significant feature shared by hydatidiform moleand choriocarcinoma is the epithelial (trophoblastic)abnormality. Park (1971) has therefore suggestedthat in these lesions the state of the epitheliumshould be given priority as follows:1 Where hydrops of the villus, whether it amounts
At
copyright. on O
ctober 23, 2020 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.s3-10.1.111 on 1 January 1976. D
ownloaded from

C. W. Elston
XI
#.a"..t 0
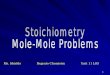
Fig 4Fig 3Fig 3 Chorionic villifrom a spontaneous abortion at nine weeks' gestation. There is hydropic change in the stroma withabsent blood vessels, and the trophoblast is two-layered but attenuated. H & E x 175.Fig 4 Same case as that shown in figure 2. In this field there is marked trophoblastic hyperplasia. H & E x 175.
to frank liquefaction of the stroma or not, is accom-panied by hyperplasia of the trophoblast, the con-ceptus should be designated 'hydatidiform mole'.2 Where villi with this type of stromal change haveno associated trophoblastic hyperplasia, the con-ceptus should be designated 'hydropic abortion'.3 No distinction should be drawn between villoushydrops visible macroscopically as distinct vesiclesand villous hydrops visible only macroscopically.
This is an arbitrary procedure, but on a practicalbasis it seems to work. Essentially similar criteriahave been used for several years in our departmentat the City Hospital, Nottingham, in the examinationof many thousands of gestational products. So far,no case of choriocarcinoma has occurred in a patientwhose original products of conception were des-cribed as a simple hydropic abortion, and this is inaccord with Park's experience (1971).Although the criteria outlined above are relatively
straightforward, difficulty in assessing trophoblasticproliferation may be experienced in some cases.Figure 3 shows a representative area from a hydropicabortus. No embryo could be identified, andalthough there was widespread hydropic change,most of the trophoblast was regular and two-layered. However, there was quite definite tropho-blastic hyperplasia in other areas (fig 4) and althoughthe overall appearances were not those of molarchange, the patient was followed uip. In the eventurinary gonadotrophin levels rapidlybecamenormal,and there were no sequelae. It is in the occasionalborderline case such as this that our knowledge islacking, and if there is any degree of uncertaintyfollow up with gonadotrophin assay is recommended.
PROGNOSIS OF HYDATIDIFORM MOLE: THEROLE OF HISTOLOGICAL GRADINGIn the United Kingdom choriocarcinoma is preceded
114
copyright. on O
ctober 23, 2020 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.s3-10.1.111 on 1 January 1976. D
ownloaded from

The histopathology of trophoblastic tumours
by a hydatidiform mole in about 50% of cases.Conversely, less than 5% of patients who abort ahydatidiform mole later develop choriocarcinoma,and fewer than 10% require treatment to eliminatetrophoblastic disease. The clinical problem is thenthat, whilst the great majority of patients who aborta hydatidiform mole have no further trouble, asmaller proportion will inevitably require cytotoxictherapy. Management would be considerablysimplified if this potentially malignant group couldbe identified at the time of molar abortion. Thepossibility that the malignant potential of thetrophoblast of a hydatidiform mole could bepredicted from its original histological appearanceswas first suggested by Hertig (1937). In a later study(Hertig and Sheldon, 1947), six histological gradeswere identified, relating increasing trophoblastichyperplasia and anaplasia to increasing malignantbehaviour. Hertig and Mansell (1956) subsequentlymodified the classification to include only threegrades. Hunt et al (1953), using the criteria of Hertigand Sheldon, found that although a histologicalclassification could be made the results were notdefinitive enough to determine treatment. This viewwas also held by Smalbraak (1957), Coppleson(1958), Logan and Motyloff (1958) and by Tow andYung (1967), but Schiffer et al (1960) and Douglas(1962) considered histological grading to be ofprognostic value. Park (1959) assessed the risk ofmalignant change as ranging from 1 % with minimaltrophoblastic hyperplasia to 10% with markedhyperplasia, and later stated that 'the correlationbetween degree of overgrowth and likely clinicalbehaviour is certainly low, but not entirely lacking'(Park, 1971).As part of a wider study of the pathology of
trophoblastic disease (Elston, 1970) an attempt wasmade to resolve these differences, particularly as thefollow up given to many patients can still be in-fluenced by the histological report on the originalhydatidiform mole. The results have been publishedmore fully elsewhere (Elston and Bagshawe, 1972a),but a summary of the findings is relevant here. Thestudy was based on histological material obtainedfrom 70 patients treated at Charing Cross (Fulham)Hospital. The criteria of Hertig and Mansell wereused, giving three grades of trophoblastic hyper-plasia and anaplasia. This was a selected group ofpatients in which there was a bias towards thosewho developed choriocarcinoma. Whereas onlyabout 2% of hydatidiform moles are followed bychoriocarcinoma in European populations (Kolstadand Hognestad, 1965; Ringertz, 1970) this occurredin at least 21 % in our study. If the Hertig thesiswere valid two trends would have been expected, anexcess of grade 3 moles in the series as a whole, and
115
an excess of choriocarcinomas arising in thosepatients who did have grade 3 moles. In fact, theincidence of grade 3 moles (18.5%) was less thanwould have been expected by chance alone (33 3 %).Further, the number of patients in each grade whosubsequently developed choriocarcinoma was ap-proximately that which would have been expected ifthe histological appearances had no influence onsubsequent malignancy (grade 1, observed eight,expected 6-6; grade 2, observed four, expected 5 5;grade 3, observed three, expected 2-8). It wasconcluded that there was no value in attempting toassess potential malignant behaviour from thehistological appearances of a hydatidiform mole.Indeed it may be an extremely dangerous practice,with delay in the diagnosis of choriocarcinomaarising from grade 1 moles or overdignosis ofmalignancy in grade 3 moles.
It seems clear that, in the absence of strongalternative evidence, attempts to identify thepotentially malignant group of hydatidiform molesfrom their histological appearances should beabandoned. Indeed, this type of analysis has beensuperseded by the development of the relativelycheap and highly accurate radioimmunoassaymethod for estimating gonadotrophin levels. Thereis no substitute for careful follow up of all patientswith hydatidiform mole (Bagshawe, 1969), and thisshould be based on regular clinical examination,with urinary gonadotrophin assay, radiographs ofthe chest, and, when indicated, histological exam-ination of uterine curettings. The microscopicalappearances of the original hydatidiform moleshould not influence future treatment, and theterms 'malignant mole' and 'choriocarcinoma in situ'should never be used.
INVASIVE HYDATIDIFORM MOLEAn invasive mole may be defined as a hydatidiformmole in which molar villi have penetrated themyometrium or its blood vessels. Apart fromvillous penetration of the uterus itself, an invasivemole may also produce villous or trophoblastic'metastases'.Ewing (1910) was the first to separate invasive
mole from choriocarcinoma on clinicopathologicalgrounds, because the average 'chorioadenoma'offered a hopeful prognosis, while choriocarcinomadid not. Since then there have been numerousreviews of invasive mole (Novak and Seah, 1954b;Hertig and Mansell, 1956; Greene, 1959; Acosta-Sison, 1960; Park, 1971), with general agreementthat the entity is a useful one. However, Tow (1966)and Brewer (1967) have questioned this, consideringthat the separation of the two lesions is artificial, thecharacteristics of the trophoblast being of more
copyright. on O
ctober 23, 2020 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.s3-10.1.111 on 1 January 1976. D
ownloaded from

C. W. Elston
importance than the presence or absence of villi. Ithas further been stated that since a patient witheither lesion is going to receive essentially the sametreatment the precise histological diagnosis is notimportant. This is not necessarily true, and patientswho have undergone surgical treatment for chorio-carcinoma usually need follow-up cytotoxic therapy,which is rarely necessary in the case of invasive mole.Ewing's (1910) observation still holds good, andPark (1971) has suggested that trophoblast of thelocally invasive lesion, which is capable of formingvilli, is biologically different from that of themetastasizing malignant type that we recognize aschoriocarcinoma. The question of so-called meta-stases in invasive mole is discussed later, but in viewof the undoubtedly less aggressive behaviour of thiscondition,,and the presence of villi as a distinctivemarker, there are excellent reasons for retaining itas an entity separate from choriocarcinoma.
There are no typical macroscopic features ininvasive mole, as there are with choriocarcinoma.The gross appearance depends on the extent ofinvasion; the uterus may show little abnormalityapart from a small haemorrhagic focus, or theremay be a large cavitating haemorrhagic lesionextending deeply into the muscle. More rarely theserosal surface of the uterus is breached. Occasion-ally, the original hydatidiform mole is still retainedwithin the uterine cavity.
Microscopical examination of invasive molesmust, by definition, reveal chorionic villi within themyometrium. The trophoblast exhibits no specificfeatures; although in the majority of cases there ismoderate or marked hyperplasia, in a significantminority little trophoblastic proliferation is seen.Three degrees of invasion can be recognized.
1 In a small proportion of cases invasion is limitedand although molar villi and hyperplastic tropho-
vi, V;'* ;h\Rp
t 4
** t a
4Wst\Es,4S*4Xi; * 9 Xs'pW
jw>s^<>@X;4X
.. I~~~~~~~~.A
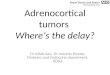
Fig 5 Fig 6Fig 5 Hydatidiform mole with limited invasion. Molar chorionic villi are attached to degenerate decidua.H&E x 100.
*
.r.
.,.
Fig 6 Same case asfigure 5. In thisfield hyperplastic trophoblast at the top is attached directly to myometrialfibres at the bottom, with conspicuous giant trophoblastic cells in the centre. H & E x 200.
116
copyright. on O
ctober 23, 2020 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.s3-10.1.111 on 1 January 1976. D
ownloaded from

The histopathology of trophoblastic tumours
wz;w S ye-OPA,- % 9-,@w,
Fig 7 Invasive hydatidiform mole, with molar villilying within a dilated venous sinus deep in the myometrium.H&E x 40.
blast are attached directly to subendometrialmyometrium (figs 5 and 6), without interveningdecidua, there is no deeper invasion of the uterus byvilli or trophoblast.
2 In the majority of cases there is deep penetra-tion by molar villi into, but not through, the myo-metrium (fig 7). This penetration appears to takeplace almost invariably within dilated venoussinuses. The molar villi vary considerably in size,and occasionally are inconspicuous, so that theexamination of any uterus containing a proliferatingtrophoblastic lesion requires a careful search forvilli to avoid an erroneous diagnosis of chorio-carcinoma. Placental site reaction is variable, andtrophoblastic emboli in myometrial vessels are notinfrequently seen.
3 In a minority of cases molar villi have penetratedthrough the full thickness of the myometrium, withperforation of the uterus or penetration into thebroad ligament.
Hertig (1950) regarded these three degrees ofinvasion as the placenta accreta, increta and percreta
of the molar placenta. He found (Hertig andMansell, 1956) that the sooner a hysterectomy wasperformed after diagnosis of a mole the more likelywas evidence of local invasion to be found, and it isprobable that all moles are at least minimallyinvasive (Gore and Hertig, 1967). Wilson et al (1961)and Gore and Hertig (1967) have commented onthe difficulty of establishing the diagnosis in invasivemole, partly because of the scarcity of well formedvilli in pathological material. It is possible that villiwill only be present in a minority of the blockstaken, and for this reason multiple blocks should beexamined.The highest recorded mortality in invasive mole
is 20% (Prawirohardjo et al, 1957) in the Far East,while in the United States, Greene (1959) found amortality of 14% in a study of 42 selected cases. Inmany of the reported cases the precise cause ofdeath is uncertain, because adequate necropsyrecords are lacking, but the impression gained isthat the mortality is related more to local complica-tions such as haemorrhage or uterine perforationthan to progressive metastatic disease. There wereno deaths in the 10 patients from the Charing Crossseries studied personally (Elston, 1970), and nonehave occurred subsequently in a much larger groupof patients (Bagshawe, 1976). These results serve toemphasize the essentially limited aggressiveness ofinvasive mole.
'METASTASES' IN HYDATIDIFORM MOLEA hydatidiform mole should be placed in the'invasive' category not only when there is clearevidence of myometrial penetration but also in thepresence of 'metastases'. As Park has pointed out(Park, 1971), the term 'metastasis' need not besynonymous with 'malignant neoplastic metastasis',and deportation of 'benign trophoblast' to thelungs in eclamptic and other maternal deaths is welldocumented (Schmorl, 1893; Veit, 1901; Bardawiland Toy, 1959). There have been numerous reportsof metastasis in molar pregnancies, with frequen-cies of 24% (Greene, 1959), 27%/ (Acosta-Sison,1960) and 40% (Wilson et al, 1961). Tow (1966),in a review of the world literature, found an overallfigure of 35%, and this is in close accord with theestimated 36% in the selected series of hydatidiformmoles examined by Elston (1970). The majority ofreports refer to lung metastases confirmed only byradiographs of the chest, but several authors haverecorded cases with histological proof of the molaror trophoblastic nature of the lesions (Delfs, 1957;Reed et al, 1959; Jacobson and Enzer, 1959; Wilsonet al, 1961; Ring, 1972). Villous metastases havebeen recorded only rarely outside the pelvis andlungs (paraspinal connective tissue, Delfs, 1957;
117
copyright. on O
ctober 23, 2020 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.s3-10.1.111 on 1 January 1976. D
ownloaded from

118
spinal cord, Hsu et al, 1962; and brain, Ishizuka,1967). From a clinical point of view the importanceof metastases in molar trophoblastic disease iswhether or not their presence implies that 'pro-gressive' malignant change has developed. Biopsymay show unequivocal choriocarcinoma, in whichcase the diagnosis is certain, or it may show simpledeported trophoblast or villi. Several authors havestressed the essentially non-malignant nature ofsuch deported trophoblast or villi (Thiele andAlvarez, 1962; Hsu et al, 1962; Ring, 1972) ascompared with choriocarcinoma.
In the patients treated at Charing Cross Hospitalwe did not have the opportunity to obtain biopsiesfrom lung lesions except in cases of confirmedchoriocarcinoma. Lung 'metastases' were thereforeassumed from radiographic evidence, and the casesdesignated as 'persistent trophoblastic disease,metastatic'. There were no deaths in these patients,although some needed treatment with cytotoxicagents in order to obtain regression of the lungnodules. We did, however, have the opportunity tostudy the histological aspects of a number ofvaginal 'metastases' which developed in patientswith hydatidiform mole. It is appropriate to discussthe findings here, because, from a study of the earlymanagement of these patients, it is apparent that thepresence of a vaginal nodule is frequently taken toindicate an unfavourable prognosis. Vaginal nodulesdeveloped in seven out of 72 patients with hydatidi-form mole. In three cases the vaginal nodule wasthe presenting lesion, in two cases the nodulebecame apparent at the time of diagnosis, and in theother two cases the vaginal metastasis developedafter abortion of the mole. In none of the patientswas there any clinical or radiological evidence ofother metastases. Choriocarcinoma did not developin any of the patients: three required no therapyat all; one, who had a hysterectomy (performedmainly because a diagnosis of choriocarcinoma hadbeen made from the presenting vaginal nodule),required no subsequent treatment; three were givenup to four months' treatment with chemotherapeuticagents, an average course for postmolar tropho-blastic disease.
In five of the seven patients a biopsy was taken,and the findings were as follows:
Case 65Two months after her last period this patientdeveloped vaginal bleeding, and was found to havean enlarged uterus with several vaginal nodules.Histological sections from one of the nodules werereported as choriocarcinoma, and she was trans-ferred to Charing Cross Hospital. Treatment withintraarterial methotrexate was started, but the
C. W. Elston
. _
9,..1..
.. 14.0 '. I
,- 44rl4ow
0
Fig 8 Molar villus with adjacent vaginal mucosa, obtainedat biopsy ofa vaginal nodule in a patient with hydatidiformmole.H&E x 50.
uterine bleeding continued, and one month afterthe vaginal biopsy a hydatidiform mole was ex-pelled spontaneously. The patient is well 11 yearslater.The original diagnosis of choriocarcinoma was
incorrect, since the biopsy specimen containedhydropic chorionic villi (fig 8). Had this been madeapparent at the time the delay in the diagnosis of thein-situ hydatidiform mole might not have occurred.
Case 67During her first pregnancy this patient developedbleeding from a nodule in the vagina. Sections fromthe biopsy showed a deposit of molar villi in thevaginal mucosa. Two weeks later abdominalhysterotomy revealed a typical hydatidiform mole.As a pregnancy test was still positive one monthlater she was referred to Charing Cross Hospitalfor assessment. No treatment was given and thegonadotrophin excretion fell to normal over the nextthree months. The patient is well 10 years later.
copyright. on O
ctober 23, 2020 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.s3-10.1.111 on 1 January 1976. D
ownloaded from

The histopathology of trophoblastic tumours
5,~~~~~~~~~O,~
U~ ~ ~~~9 xr r.
%,q II ,tr,... a
VA ~ ,xa
tt ,' St a~~~~~~~~~~~~~~~~~~~~~~~W44'-~~~~~~~~~~~~~ 1~~~~~~~~~~&p
W.. -
14~~~~~~~~ %ILf
V. W 4.AK~ ~ ~ ~ ~ ~ .
-A' ~ ~~~ aY
te,J~~~~~~~A -a~~~~r *r%~~~Yi , --'-x2-'itt-'~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~;v.t{4~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~$-'#'4~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~I ~ ~ ~ ~ ~ ~ ~
Fig9 Fig10~~~~~~~~OVFig9Vaginal nodule in hydatid~3ifr moeAsalcvt 'tth otmrgtiurone4yifamtrcellsandanoccasionallargetrophoblastic cell H & E x 80~~~~~~~~~~~~~~~~~~~~~~~~~:Fig10Highermagnificationof nodule shown in figure 9 There are scanty pyknotic trophoblastic cells butno~~~~~~~~~~~~~~~~~~~~~~~~~~~I.organizedpatternisseenandthere are no chorionic villi H & E x 160~~~~~~~~~~Ax
Case 76This patient was found to have a vaginal nodulefollowing an 18-week period of amenorrhoea.Sections from the biopsy were reported as 'verystrongly suspicious of choriocarcinoma'. Becauseof this she was referred to Charing Cross Hos-pital and hysterectomy was performed. Exam-ination of the excised uterus showed a hydatidiformmole in situ, with very early myometrial invasion.No further treatment was required and the patientremains well nine years later.
Sections from the original vaginal biopsy showed ahaemorrhagic nodule, at the periphery of whichwere scattered small numbers of rather pyknotictrophoblastic cells (figs 9 and 10). There were nochorionic villi and the appearances were those of atrophoblastic deportation nodule.
Case 79This patient had a hysterectomy for hydatidiformmole at 24 weeks' gestation. Examination of theexcised uterus showed a typical hydatidiform mole,with no evidence of invasion. Six weeks later shedeveloped vaginal bleeding and was found to have ahaemorrhagic nodule in the vagina. Needle aspira-ation yielded clumps of trophoblastic cells whichwere considered to be suspicious ofchoriocarcinoma.The patient was referred to Charing Cross Hospitalfor treatment. A further vaginal biopsy revealedtypical hydropic chorionic villi. The diagnosiswas therefore established as locally metastatichydatidiform mole, and the patient was treatedwith chemotherapeutic agents. She remains welland free from trophoblastic disease eight years later.The original histological sections were obtained
119
copyright. on O
ctober 23, 2020 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.s3-10.1.111 on 1 January 1976. D
ownloaded from

120
and examination showed not only fragments oftrophoblast but also typical molar villi, the latterprecluding a diagnosis of choriocarcinoma.
Case 83Two months after stopping oral contraceptives thispatient had a spontaneous abortion. Histologicalsections were reported as simple products of con-ception. Five weeks later further bleeding occurredand examination revealed a vaginal nodule. Abiopsy was taken, and the specimen examined by adifferent pathologist who reported that the diagnosiswas metastatic choriocarcinoma. The patient wasreferred to Charing Cross Hospital for furthertreatment, but before this was instituted the path-ologist was informed of the previous biopsy andexamined sections himself. He realized that therewas hydatidiform degeneration of the chorionicvilli and changed his diagnosis to metastatic hyda-tidiform mole. The patient remains well sixyearslater.The diagnosis of choriocarcinoma need not have
been made in the first place. Although the appearanceof some of the trophoblast in the vaginal deposit wassimilar to choriocarcinoma (fig 11) hydropicchorionic villi were also present (fig 12). As theoriginal products ofconception were morphologicallysmall fragments this is an example of a 'transitional'mole with vaginal metastasis.Of the five cases in which biopsies were taken, four
of the vaginal nodules were true metastases of molartissue while the fifth was an example of tropho-
C. W. Elston
blastic deportation. All the metastases behaved in abenign way, and the most disturbing aspect is thefact that a diagnosis of choriocarcinoma was eithersuggested or firmly made in four out of the fivecases, the correct diagnosis being made in only one.The basic presumption seems to have been that thedevelopment of vaginal nodules inhydatidiformmoleis in itself indicative of malignant change. Thismisconception is dangerous, and can easily lead tothe patient receiving unnecessary surgical orcytotoxic therapy. The essentially benign nature ofvaginal nodules has been stressed repeatedly (Haines,1955; Bardawil et al, 1957; Thiele and Alvarez, 1962),and Dinh-De and Minh (1961) have publisheddetails of a patient with hydatidiform mole andrecurrent vaginal nodules in whom recovery wascomplete. Hsu et al (1962) found vaginal metastasesin eight out of 14 cases, with one death, and statedthat metastases to the vagina did not carry a hopelessimplication. Gore and Hertig (1967) consideredthat vaginal nodules following a normal pregnancywere virtually always choriocarcinoma, but in thecase of hydatidiform mole, unless the trophoblastwas very abundant or had the classical appearancesof choriocarcinoma, it was better to assume that itwas merely deported trophoblast.To summarize, the presence of vaginal metastases
in hydatidiform mole should not be regarded asevidence of malignancy, unless there is unequivocalhistological confirmation. It is indefensible toinstitute potentially dangerous therapy for a simple
Fig 11 Fig 12Fig 11 Fragment oftrophoblastfrom a vaginal nodule in a patient with a 'transitional' hydatidiform mole. Thehistological appearances, with differentiated cytotrophoblast and syncytiotrophoblast, are not dissimilar to thoseofchoriocarcinoma. H& E x 100.Fig 12 Fragments ofhydropic chorionic villifrom the same vaginal nodule as that shown infigure 11, ruling out adiagnosis of choriocarcinoma. H & E x 60.
copyright. on O
ctober 23, 2020 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.s3-10.1.111 on 1 January 1976. D
ownloaded from

The histopathology oftrophoblastic tumours
hydatidiform mole when conservative managementof local metastases is sufficient, and the pathologistbears a considerable responsibility in his assessmentof these lesions.
Choriocarcinoma
Choriocarcinoma can be defined as 'a malignanttumour occurring as a result of a gestation, andcomposed only of cytotrophoblast and syncytio-trophoblast, which, if not treated, will almost in-variably cause death'. Clinically, the most remarkablefeature of choriocarcinoma is that this highlyaggressive malignant tumour is now eminentlycurable. Indeed, so successful may treatment bethat, if the uterus is preserved, a subsequent normalgestation is possible (Bagshawe, 1969).The typical histopathological appearances have
MA
!ar,XNS..-
, e.il.; 9 j
lffiS°8scm
Fig 13 Hemisected uterus showing multiple darkhaemorrhagic nodules of choriocarcinoma in the body andcervix.
been so well described in the past (Teacher, 1903;Ewing, 1910; Park and Lees, 1950; Novak and Seah,1954a; Ober et al, 1971; Park, 1971) that little morethan a brief outline will be given here. Grossly thereis remarkable consistency in the findings. Thetumour nodule varies considerably in size, from 0 5cm up to more than 5 cm in diameter, and is com-posed of a central brownish area of haemorrhageand necrosis with a surrounding rim of purpletrophoblast. The nodules may be single or multiple(fig 13), deep in the myometrium, or projecting intothe uterine cavity. At metastatic sites the samehaemorrhagic nodular structure is still apparent;in the lung the nodules are often situated sub-pleurally, but rarely the tumour is entirely intra-vascular.
Microscopically the malignant trophoblast issituated at the periphery of the nodule and little isfound in the central part. This is mainly due to thefact that, unlike any other tumour, choriocarcinomacontains no inherent stromal vasculature. Thetumour cells thus rely on permeation of the 'host'blood vessels for nutrition, and these vessels are onlypresent at the tumour-host interface. In this respectthe malignant trophoblast of choriocarcinomabehaves in exactly the same way as normal tropho-blast. The tumour tissue is usually organized intocentral cores of cytotrophoblast-like cells surroundedby a peripheral rim of syncytiotrophoblast-like cellswith the latter often arranged around blood-filledspaces resembling the normal intervillous space(figs 14 and 15). Variation from this typical patternoccurs, and occasionally one or other elementpredominates, whilst in parts of most tumours theclear distinction between cytotrophoblast andsyncytiotrophoblast is lost. Unlike normal tropho-blast there is considerable variation in size and shapeof nuclei, and nucleoli are often multiple. Mitoticactivity is also variable, but rarely excessive.Although there is little myometrial necrosis, in-vasion through the uterine wall is particularlyconspicious. This invasion is very rarely directlythrough muscle fibres, but is almost entirely intra-vascular, and a striking feature of the uterine venoussinuses in choriocarcinoma is their great dilatation.The combination of the unique lack of tumourstromal vessels and permeation of dilated maternalvessels is associated with a high proportion of blood-borne metastases. The relative frequency of meta-stases at different sites in a necropsy study of 27patients dying from choriocarcinoma (Elston, 1970)is shown in table I. It will be noted that in none ofthe cases was lymph node involvement found, andPark and Lees (1950) and Novak and Koff (1930)found lymph node metastases in only 6% and 4%respectively.
121
copyright. on O
ctober 23, 2020 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.s3-10.1.111 on 1 January 1976. D
ownloaded from

C. W. Elston
Fig 14 Fig 15
Fig 14 Choriocarcinoma, composed of sheets of cytotrophoblast and syncytiotrophoblast, invading myometriumH&E x 100.Fig 15 Higher magnification ofanother choriocarcinoma. Note the organized pattern, with syncytiotrophoblastlining pseudo-intervillous spaces containing maternal red cells. H& E x 400.
Organ Percentage Involvement
Lung 80Brain 40Vagina 25Liver 20Kidney 20Intestines 15
Table I Metastatic sites at necropsy in 27 patients withgestational choriocarcinoma
As a point of distinction from invasive mole,molar chorionic villi are absent. In one case in theseries examined by Elston (1970) chorionic villi wereseen in or close to the tumour. Those quite separatefrom the tumour were degenerate and surroundedby inflammatory cells; they appeared to be under-going resorption (fig 16). The villus within thetumour was histologically well preserved with a
double layer of normal trophoblast around it:malignant trophoblast did not arise from the villus,nor did the villus appear to be invading the myo-metrium (fig 17). This choriocarcinoma occurredseven weeks after a spontaneous abortion, and noevidence of molar change was seen in the originalproducts of conception. There is no reason whyvestiges of the villi from the trophoblast of which thetumour has arisen should not occasionally persist,but the occurrence seems to be rare. MacRae (1951),Driscoll (1963) and Brewer and Gerbie (1966) havedescribed very early choriocarcinomas found inotherwise normal placentas. In Driscoll's case therewere no metastatic sequelae, but Brewer and Gerbiepresented three patients, all of whom died frommetastatic choriocarcinoma in which villi were notfound. All these tumours arose from non-molargestations. The arguments relating to the wisdom of
122
copyright. on O
ctober 23, 2020 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.s3-10.1.111 on 1 January 1976. D
ownloaded from

The histopathology of trophoblastic tumours
Fig 16 Fig 17Fig 16 Degenerate, but not hydropic, chorionic villus by surrounded inflammatory cells, lying in the myometriumadjacent to a choriocarcinoma. H & E x 140.Fig 17 Chorionic villus lying close to an area ofchoriocarcinoma. The neoplastic trophoblast is not arisingfromthe villus, nor is the latter invasive. Same case asfigure 16. H & E x 100.
retaining invasive mole as an entity separate fromchoriocarcinoma on the basis of its villous structurehave already been discussed; suffice it to say that itseems illogical to use the phenomena described abovein support of the 'villous' and 'avillous choriocar-cinoma' concept, when the villi are an incidentalfinding. The presence of a number of degeneratevilli, not obviously invasive in themselves, shouldnot invalidate a diagnosis of choriocarcinoma in theface of separate sheets of typical invasive malignanttrophoblast.
The Diagnosis of Trophoblastic Lesions in UterineCurettings
Since the advent of accurate methods for estimatinggonadotrophins and the introduction of cytotoxic
agents, there has been a decline in the use of histo-pathological methods in the management of estab-lished cases of trophoblastic disease (Hammondet al, 1967). However, in the majority of patientswho develop trophoblastic disease an importantpresenting symptom is uterine bleeding, and themost widely used diagnostic tool in this situation ishistological examination of uterine curettings.Indeed, curettings containing chorionic villi orfragments of trophoblast are among the commonerdiagnostic problems in routine gynaecologicalhistopathological practice. Most of the tissue issimple retained products of conception, but in somethe trophoblast appears abnormal, and the possibilityof choriocarcinoma must be considered. Thehistopathologist, therefore, continues to be facedwith the problem of trophoblastic curettings, and
123
copyright. on O
ctober 23, 2020 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.s3-10.1.111 on 1 January 1976. D
ownloaded from

C. W. Elston
his report may have a profound effect on primarytreatment. This is reflected in the material seen inthe Charing Cross series, which was derived fromover 30 hospitals in the United Kingdom.The reliability of the diagnosis of choriocarcinoma
fromuterine curettings has been questioned by someauthors (Novak, 1922; Mathieu, 1939), although inseveral reports (Teacher, 1935; Park and Lees, 1950;Sta. Cruz, 1959; Novak and Seah, 1954a; Novakand Woodruff, 1974) curettage was found to beuseful in a proportion of cases. Because chorio-carcinoma is rare in the United Kingdom mosthistopathologists have a limited experience, andthere seems to be a tendency towards overdiagnosis,particularly in curetted material. This, on occasion,has led to patients receiving unnecessarily radicaltherapy, particularly operative surgery. It must notbe forgotten that the majority of patients withtrophoblastic disease are young and wish to bearchildren; the pathologist has a duty to ensure thathe is not responsible for the unnecessary curtailmentof this function.
4,~~~~~~~~~~o
41.14~~ ~ ~ ~ ~ '
*,, *,4 w
t. s .
,4'.zC::. *
The pathological material from the patientstreated at Charing Cross Hospital has been used byElston and Bagshawe (1972b) to define the histo-logical criteria and suggest general principles for thereporting of uterine curettings in trophoblasticdisease. They examined curettings from 54 patients;in 38 the curettings were obtained during follow upof a patient with hydatidiform mole, in 12 patientsfollowing a normal pregnancy and in four after aspontaneous abortion. Excluding curettings in whichno trophoblastic tissue was found, three histologicalgroups could be identified:
VILLOUSIn this study all the villous curettings came frompostmolar cases, and the villi showed hydropicchange with variable trophoblastic hyperplasia.Occasionally villi were inconspicuous and scanty.
SIMPLE OR SUSPICIOUS TROPHOBLASTThe appearances of the trophoblast in this categorywere of two main types. In one the fragments of
,IAI
Ai ..AMf*~~~~~~ ; .*..,t
. "4 "Ed.% s S
v 4, ._ .u ,4- *4; t
Awk.
ei 'o 4
*at* v' 4.4ssS
I .f.
4V^ .
.' I
.1 ?
s
I
Fig 18 Simple trophoblast. There are smallfragments oftrophoblast with pyknotic nuclei, but no clear differentia-tion into cytotrophoblast or syncytiotrophoblast. H & Ex 120.
'4 '1.
4 9
4'
;.
F:4
Fig 19 Suspicious trophoblast. Although cytotrophoblastand syncytiotrophoblast can be identified separately, theoverallpattern is disorganized. There is no invasion.H& Ex 150.
124
I
-
"'. t., N-`..-""'i
.9
copyright. on O
ctober 23, 2020 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.s3-10.1.111 on 1 January 1976. D
ownloaded from

The histopathology of trophoblastic tumours
trophoblast were small, and clear differentiation intocytotrophoblast and syncytiotrophoblast was poor(fig 18); nuclei were often hyperchromatic andirregular, appearances which could lead the unwaryinto a mistaken diagnosis of malignancy. In theother there were larger sheets of trophoblast, anddifferentiation into cytotrophoblast and syncytio-trophoblast was usually seen (fig 19). The tropho-blast in some of these cases resembled that ofchoriocarcinoma, but in none of the curettings wasthere evidence of invasion. Chorionic villi wereabsent.
TROPHOBLAST DIAGNOSTIC OF CHORIO-CARCINOMACurettings were only considered to be diagnostic ofchoriocarcinoma when there was invasion of endo-metrium and myometrium by large sheets oftrophoblast having a typical, well organized pattern.Nuclei were vesicular, with prominent and oftenmultiple nucleoli. No chorionic villi were seen.When the type of trophoblast in the curettings was
,,+s * 402w 7*vi S< '+
-.,_
p as tr b amyometrium.mac s
c a i E
Fig 20 Hyperplastic trophoblast attached directly to
myometrium. From a postmolar curetting which also
contained molar villi. H & E x 90.
matched with antecedent gestation and subsequenttrophoblastic disease several practical points emer-ged. In this series all the villous curettings wereobtained in the follow up of a hydatidiform mole.Chorionic villi are not infrequently present incurettings taken after a normal term pregnancy or aspontaneous abortion, but they are virtually alwaysdegenerate, and the question of abnormal tropho-blastic proliferation seldom arises. After a hydatidi-form mole the problem is more difficult because ofthe undoubted malignant potential of molar tropho-blast. Nevertheless, Elston and Bagshawe (1972b)considered that a diagnosis of choriocarcinomamust not be made in the presence of villous curettings.Most of the patients in this group pursued a rela-tively benign course, requiring only short courses ofchemotherapy or no treatment at all, and in only asmall proportion (10 %) was a definite tissue diagnosisof choriocarcinoma subsequently established. Thisis not to say that the finding of villi should beignored. This indicates that active trophoblasticproliferation is still continuing, and adequate
S-14. 2 ,
i tX; b * ..*t
_ ^+s , 4 *4_ .
S~~~ V.'g ps ,
*-%~\t...X> f '4 jte*,
*V~~~
a-~~~~~~~~~~w
q~~~~~~~~~~~~~~~~~~~~.~~~~~~~~4,. i* t* a,', #
>, ,,,,*+ } ;S.
tSAX '$ S \r.
Fig 21 Higher magnification of myometrium infigure 20,showing the typical giant cells ofplacental site reaction.H&E x 180.
125
copyright. on O
ctober 23, 2020 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.s3-10.1.111 on 1 January 1976. D
ownloaded from

126
follow up should be carried out. Furthermore, sincethe presence of formed villi is an indication of arelatively more favourable prognosis, great careshould be taken not to overlook them.
In the case of curettings containing simple orsuspicious trophoblast the nature of the antecedentgestation was found to be of great importance. Aswith the villous group, if simple or suspiciouscurettings are obtained after the abortion of ahydatidiform mole, the findings should be inter-preted with caution: careful follow up is essential,but a definite histological diagnosis cannot be made.If the preceding gestation was a normal pregnancyor a spontaneous abortion simple or suspicioustrophoblast has a far more serious implication. Inthe series of Elston and Bagshawe all the patientsin this group had malignant or potentially malignantdisease needing chemotherapy, and it is a goodworking rule to assume that the presence of non-villous trophoblastic proliferation following anormal pregnancy or a spontaneous abortion meansthat the patient has developed choriocarcinomaunless proved otherwise.A number of mononuclear and multinucleated
trophoblastic cells is normally found in the endo-metrium and myometrium at the implantation sitein normal gestations. Unfortunately, the sameappearances may be mistaken for invasive chorio-carcinoma in curettings following molar gestations.Although the trophoblastic infiltration can beunusually florid in a postmolar curetting (figs 20and 21), there is no evidence to suggest that itspresence has any sinister implications. The exag-gerated form of placental site reaction, first describedby Marchand (1898) as 'atypical choriocarcinoma'and later called 'syncytial endometritis' by Ewing(1910), presents a more difficult problem. BothMarchand and Ewing commented on the widespreadpermeation of the uterine musculature by giantmononuclear cells apparently derived from thesyncytium; in Ewing's opinion the prognosis wasmuch more favourable than that of typical chorio-carcinoma. Others do not consider the lesion to be atrue neoplasm (Novak and Seah, 1954b; Ober et al,1971; Elston and Bagshawe, 1972b) but rather anabnormal persistence of placental site cells. Never-theless, both clinically and histologically there arefeatures which may closely mimic choriocarcinoma.In uterine curettings containing myometrium theremay be numerous trophoblastic cells infiltratingbetween muscle bundles (fig 22) and in hysterectomyspecimens these cells can extend out to the serosa.Indeed, in a patient at present being treated atCharing Cross Hospital similar cells were alsopresent in one ovary, and in the face of such exten-sive spread it is difficult to exclude completely the
C. W. Elston
ty..- W.M a *, w . (.
.*t *s~~~~~~~CN.
~~, ,.T*6'a:r<:,.-X-~~ ~V.\iKS .,<XX5 W
.A .g. .
b> . E t*s s.t ....... 18.0..
\ f *~~~~~~~~P
v A
I'
Fig 22 Myometrium in which there is an exaggeratedplacental site reaction with trophoblastic cells infiltratingbetween muscle bundles. H& E x 180.
possibility of a malignant proliferation. Despite this,in most of the cases recorded in the literature, and ina small series studied personally, the condition israrely if ever fatal.One further source of diagnostic difficulty should
always be considered, and that is the occurrence of'new' pregnancy in the follow-up period of aspontaneous or molar abortion. This may initiallybe detected as a rise in gonadotrophin excretion,but if a curettage is performed it is important toremember that early trophoblast is histologicallyvery similar to choriocarcinoma.
In the assessment of curettings containing tropho-blastic tissue overdiagnosis rather than under-diagnosis is the commonest error, and the patho-logist must be aware that a definite diagnosis ofchoriocarcinoma can only be made in a limitednumber of cases. In this sphere more than in manyothers, meticulous care must be taken both in the
copyright. on O
ctober 23, 2020 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.s3-10.1.111 on 1 January 1976. D
ownloaded from

The histopathology of trophoblastic tumours
Fig 23 Infiltrating choriocarcinoma on the left issurrounded by an intense inflammatory cell infiltrate.H&E x 100.
examination of the tissue and in its correlation withclinical data. In most patients the correct manage-ment depends not only on the histological findingsbut also on a full consideration of clinical, hormonaland radiological factors.
Cellular Reaction Studies in Trophoblastic Disease
In many papers concerned with the histopathologyof choriocarcinoma no mention is made of a cellularreaction to the tumours (Marchand, 1898; Teacher,1903; Park and Lees, 1950; Hertig and Mansell,1956; Smalbraak, 1957; Park, 1959), whilst in othersthe presence of inflammatory cells is described inoccasional cases, with little or no reference to itspossible significance (Ewing, 1910; Novak and Seah,1954a; Hunter and Dockerty, 1955; Ober etal, 1971).In a discussion of the immunological aspects of thematernofetal relationship, with particular referenceto choriocarcinoma, Strauss et al (1967) described a
patient with metastatic malignant trophoblast in thepulmonary vasculature (p 513). Collections oflymphocytes and plasma cells were present at pointswhere tumour appeared to break through the vesselwall. The authors suggested that this cellular res-ponse may occur because of immunological recog-nition ofcytotrophoblast at these sites, but concludedthat supporting evidence was lacking. Conversely,the absence of an inflammatory cell reaction againstdeeply infiltrating or metastatic trophoblast in 30cases of choriocarcinoma and invasive mole wascited by Iliya et al (1967) in support of their con-tention that choriocarcinoma behaves as a successfulallograft.
Following an observation in 1966 that an intensecellular reaction was present in the hysterectomyspecimens from several patients who had respondedrapidly to chemotherapy, Elston published thepreliminary results of a formal study of this pheno-menon in 1969. Histological material from 38patients with gestational choriocarcinoma wasexamined. The cellular infiltrates (fig 23) werecomposed of small and large lymphoid cells, plasmacells and histiocytes, with occasional eosinophilpolymorphonuclear leucocytes. Neutrophil poly-morphonuclear leucocytes were only rarely seen inthese infiltrates, being found more commonly inareas of necrotic tumour. Two main cellular reactiongroups could be identified, 'mild' and 'severe', andwhen the histological findings were correlated withresponse to treatment a remarkable differencebetween the two groups was found. Of the 29 patientsin whom the primary tumour was examined, onlysix out of the 18 in the mild reaction group survived,against nine out of the 11 patients in the severereaction group (X2 = 4; ldf; P = < 0-025). It wasconcluded that there was a significantly betterresponse to treatment in the patients with a severecellular reaction. A more comprehensive study wasthen carried out, and the cellular reaction assessedin 40 patients with gestational choriocarcinoma, 10patients with invasive mole and 13 with malignantteratoma trophoblast of testis or ovary (Elston andBagshawe, 1973). Although found in eight of the 10cases of invasive mole the cellular reaction wasconsidered to have no clinical significance. Thereaction to trophoblastic teratomata was generallypoor, but there was a marked cellular infiltrate inone male patient who has enjoyed a sustainedremission. In the patients with gestational chorio-carcinoma the same significant difference in responseto treatment persisted, and if the reaction to tumoursat primary and metastatic sites was included theassociation was even stronger (18 out of 20 in the'severe' group survived compared with five out of 20in the 'mild' group). Other histological features,
127
copyright. on O
ctober 23, 2020 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.s3-10.1.111 on 1 January 1976. D
ownloaded from

C. W. Elston
such as tumour necrosis, ratio of syncytiotropho-blast to cytotrophoblast and degree of vascularinvasion by tumour, were correlated with cellularreaction, but no significant associations were found,nor was there any correlation with such clinicalfactors as maternal age, gravidity, type of antecedentgestation, time interval between antecedent gestationand diagnosis and extent of metastases at diagnosis.
It is now possible to bring these results up to date.None of the patients included in the original serieshas died, and the minimum follow-up period fromthe end of treatment is five years. Sections from anadditional 17 patients have been examined, bringingthe total to 57. The intensity of the cellular reactionto tumours at different sites is shown in table II.
There are 33 patients in the 'mild' reaction groupand 24 in the 'severe' group, and the number ofsurvivors is, respectively, 10 and 21 (table III).Table 1V shows the relationship between cellularreaction and response to treatment in the 42 patientsin whom the primary tumour was removed before
Site Intensity ofCellular Reaction
Mild Severe Total
Primary 26 17 43Metastatic 6 5 11Primary and
Metastatic 1 2 3Total 33 24 57
Table II Intensity ofcellular reaction atprimary andmetastatic sites in 57 cases ofgestational choriocarcinoma
Response to Treatment Intensity ofCellular Reaction
Mild Severe Total
Incomplete-all died 23 3 26Complete remission 10 21 31Total 33 24 57
x2 = 16-09; ldf; P = < 0.001
Table III Comparison ofcellular reaction to gestationalchoriocarcinoma in two groups ofpatients: free fromtumour and dying during treatment
Response to Treatment Intensity ofCellular Reaction
Mild Severe Total
Incomplete-all died 15 3 18Complete remission 9 15 24Total 24 18 42
x: = 7.05; ldf; P = < 0.01
Table IV Comparison of cellular reaction to the primarytumour removed before chemotherapy in two groups ofpatients with gestational choriocarcinoma: freefromtumour and dying during treatment
treatment with cytotoxic agents. These resultscontinue to confirm that the patient has a significantlybetter chance of surviving if there is a markedcellular reaction to the tumour tissue. Elston (1970)has also made a study in material obtained atnecropsy, and found only one case out of 17 inwhich the cellular reaction could be placed in the'severe' group.
Little attempt has been made by others to confirmthese findings. Park (1971) has carried out aninvestigation based on material in the UK Registryfor Diseases of Trophoblast. He examined sectionsfrom either the excised uterus or necropsy materialin 50 patients with choriocarcinoma, and showedthat a cellular reaction was present in 45, beingmarked in 20, with a general tendency for non-fatalcases to have a more pronounced reaction thanfatal ones. Mogensen and Olsen (1973) found acellular reaction in 22 out of 23 patients studied,with a significantly better response to treatment inthose patients with a moderate or marked reaction.
It is clear from these studies that, contrary to thefindings of Iliya et al (1967), a cellular infiltrate ofvariable degree is present in many cases in thetissues around deposits of choriocarcinoma, bothprimary and metastatic. There also seems to be littledoubt that response to treatment is more favourablein the presence of an intense reaction. The biologicalsignificance of the cellular infiltrates is less easy toexplain from the morphological appearances alone.The cells participating in the reactions are certainlythe same as those seen in cell-mediated immunemechanisms (Waksman, 1960) and solid allograftrejection (Gowans, 1965), and Elston and Bagshawe(1973) have suggested that they represent an attemptat tumour rejection on an immunological basis. Ifthis is correct, then there are three possible sourcesfor a presumed antigen. Choriocarcinoma mightcontain tissue specific antigens for trophoblast, andalthough such antigens are thought to be present innormal human (Krieg, 1972) and animal trophoblast(Beer, et al, 1972), they have not yet been con-clusively demonstrated in malignant trophoblast.Secondly, antigens related to malignant trans-formation may be expressed (Laurence and Neville,1972), but again there has been no convincingevidence in support of this. It is of interest in thiscontext that similar cellular reactions occur in otherhuman tumours, particularly gastric carcinoma(Black et al, 1954) and carcinoma of breast (Blacket al, 1956). Finally, since choriocarcinoma is, ineffect, a malignant allograft, it may also exhibitindividual specific or transplantation antigens, in-herited from the male parent of the antecedentgestation.The evidence in this area is conflicting, and it is
128
copyright. on O
ctober 23, 2020 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.s3-10.1.111 on 1 January 1976. D
ownloaded from

The histopathology of trophoblastic tumours
important to remember that in none of the studiesso far have ABO blood group substances or HL-Aantigens been measured in tumour tissue, but inthe red cells, leucocytes and serum of those beingexamined. Various authors have studied the bloodgroups of patients with trophoblastic disease.Schmidt and Hertz (1961) found no variation fromthe normal ABO groups in 28 patients and a similarfinding was reported by Lewis (1973) in a study of31 patients and their families. Conversely, Llewellyn-Jones (1965) showed a shift away from group 0towards groups A and AB in Malayan Chinesepatients with trophoblastic disease, while in a laterstudy from Singapore Dawood et al (1971) found asignificant increase in blood group A in patientswith choriocarcinoma. Bagshawe et al (1971) haveshown that choriocarcinoma may arise from con-ceptions which are Rh or ABO incompatible withthe host, with an excess risk associated with A Y xO d matings compared with A V x A & matings(Bagshawe, 1973). Furthermore, patients of groupAB appear to have a particularly high mortality, apoint also noted by Dawood et al (1971).Mogensen and Kissmeyer-Nielsen (1968, 1971)
have studied HL-A data in patients with chorio-carcinoma and concluded that generalized diseaseoccurs when there is compatibility between host andconceptus at one or both HL-A loci, with onlylocalized disease when there is patient-husbandincompatibility at both loci. This has not beenconfirmed by other workers and in most series asubstantial proportion of patients with chorio-carcinoma demonstrate HL-A incompatibility withthe antecedent gestation (Rudolph and Thomas,1970; Lawler et al, 1971; Lewis and Terasaki, 1971).Bagshawe (1973) has concluded that although thereis an indication from ABO blood group studies thatgenetic factors may play a part in the causation ofchoriocarcinoma, the immunological implicationsare unclear, and the HL-A data are remarkable forthe apparent lack of effect of these antigens. Becauseof insufficient data it has not so far been possible tocorrelate ABO blood group and HL-A status withcellular reaction, and this and a search for thepresence of antigens in tumour tissue itself areobvious areas for further investigation.
References
Acosta-Sison, H. (1960). Chorioadenoma destruens: a reportof 41 cases. Amer. J. Obstet. Gynec., 80, 176-179.
Bagshawe, K. D. (1969). Choriocarcinoma: The ClinicalBiology of the Trophoblast and its Tumours. Arnold,London.
Bagshawe, K. D. (1973). Recent observations related to thechemotherapy and immunology of gestational chorio-carcinoma. Advanc. Canc. Res., 18, 231-263.
Bagshawe, K. D. (1976). Personal communication.
129
Bagshawe, K. D., Rawlins, G., Pike, M. C., and Lawler,S. D. (1971). ABO blood-groups in trophoblastic neo-plasia. Lancet, 1, 553-557.
Bardawil, W. A., Hertig, A. T., and Velardo, J. T. (1957).Regression of trophoblast. 1. Hydatidiform mole: a caseof unusual features, possible metastasis and regression;review of literature. Obstet. and Gynec., 10, 614-625.
Bardawil, W. A., and Toy, B. L. (1959). The natural historyof choriocarcinoma: problems of immunity and spon-taneous regression. Ann. N. Y. Acad. Sci., 80, 197-261.
Beer, A. E., Billingham, R. E., and Yang, S. L. (1972).Further evidence concerning the autoantigenic status ofthe trophoblast. J. exp. Med., 135, 1177-1184.
Black, M. M., Opler, S. R., and Speer, F. D. (1954). Micro-scopic structure of gastric carcinomas and their regionallymph nodes in relation to survival. Surg. Gynec. Obstet.,98, 725-734.
Black, M. M., Speer, F. D., and Opler, S. R. (1956). Struc-tural representations of tumor-host relationships inmammary carcinoma. Biologic and prognostic significance.Amer. J. clin. Path., 26, 250-265.
Brewer, J. I. (1967). Light microscopy of gestational tropho-blastic disease. In Transcript of 4th Rochester TrophoblastConference, edited by C. W. Lund and J. W. Choate, pp.6-24. Rochester, New York.
Brewer, J. I., and Gerbie, A. B. (1966). Early development ofchoriocarcinoma. Amer. J. Obstet. Gynec., 94, 692-710.
Coppleson, M. (1958). Hydatidiform mole and its com-plications. J. Obstet. Gynaec. Brit. Emp., 65, 238-252.
Dawood, M. Y., Teoh, E. S.,and Ratnam, S. S. (1971).ABO blood group in trophoblastic disease. J. Obstet.Gynaec. Brit. Cwlth, 78, 918-923.
Delfs, E. (1957). Quantitative chorionic gonadotrophin:prognostic value in hydatidiform mole and chorionepi-thelioma. Obstet. and Gynec., 9, 1-24.
Dinh-De, T., and Minh, H. N. (1961). Hydatidiform molewith recurrent vaginal metastasis. Amer. J. Obstet. Gynec.,82, 660-663.
Douglas, G. W. (1962). Malignant change in trophoblastictumors. Amer. J. Obstet. Gynec., 84, 884-894.
Driscoll, S. G. (1963). Choriocarcinoma: an 'incidentalfinding' within a term placenta. Obstet. and Gynec., 21,96-101.
Elston, C. W. (1969). Cellular reaction to choriocarcinoma.J. Path., 97, 261-268.
Elston, C. W. (1970). A Histopathological Study of Tropho-blastic Tumours: with Special Reference to the CellularReaction to Choriocarcinoma. MD Thesis, University ofLondon.
Elston, C. W., and Bagshawe, K. D. (1972a). The value ofhistological grading in the management of hydatidiformmole. J. Obstet. Gynaec. Brit. Cwlth, 79, 717-724.
Elston, C. W., and Bagshawe, K. D. (1972b). The diagnosisof trophoblastic tumours from uterine curettings. J. dlin.Path., 25, 111-118.
Elston, C. W., and Bagshawe, K. D. (1973). Cellular reactionin trophoblastic tumours. Brit. J. Cancer, 28, 245-256.
Ewing, J. (1910). Chorioma: a clinical and pathologicalstudy. Surg. Gynec. Obstet., 10, 366-392.
Gore, H., and Hertig, A. T. (1967). Problems in!the histologicinterpretation of the trophoblast. Clin. Obstet. Gynec., 10,269-289.
Gowans, J. L. (1965). The role of lymphocytes in the des-truction of homografts. Brit. med. Bull., 21, 106-110.
Greene, R. R. (1959). Chorioadenoma destruens. Ann. N. Y.Acad. Sci., 80, 143-151.
Haines, M. (1955). Hydatidiform mole and vaginal nodules.J. Obstet. Gynaec. Brit. Emp., 62, 6-11.
Hammond, C. B., Hertz, R., Ross, G. T., Lipsett, M. B., andOdell, W. D. (1967). Diagnostic problems of chorio-
copyright. on O
ctober 23, 2020 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.s3-10.1.111 on 1 January 1976. D
ownloaded from

C. W. Elston
carcinoma and related trophoblastic neoplasms. Obstet.and Gynec., 29, 224-229.
Hertig, A. T. (1937). In Discussion of paper by Phaneuf, L. E.Hydatidiform mole and chorionepithelioma. New Engl. J.Med., 217, 775.
Hertig, A. T. (1950). Hydatidiform mole and chorionepi-thelioma. In Progress in Gynecology, edited by J. V. Meigsand S. H. Sturgis, Vol. 2, pp. 372-394. Greene and Stratton,New York; Heinemann, London.
Hertig, A. T., and Edmonds, H. W. (1940). Genesis ofhydatidiform mole. Arch. Path., 30, 260-291.
Hertig, A. T., and Mansell, H. (1956). Tumors of the FemaleSex Organs, Part 1, Hydatidiform Mole and Choriocar-cinoma. (Atlas of Tumor Pathology, Sect. 9, fasc. 33).Armed Forces Institute of Pathology, Washington, D.C.
Hertig, A. T., and Sheldon, W. H. (1947). Hydatidiform mole:a pathologico-clinical correlation of 200 cases. Arner. J.Obstet. Gynec., 53, 1-36.
Hsu, C. T., Huang, L. C., and Chen, T. Y. (1962). Metastasesin benign hydatidiform mole and chorioadenoma destruens.Amer. J. Obstet. Gynec., 84, 1412-1424.
Hunt, W., Dockerty, M. B., and Randall, L. M. (1953).Hydatidiform mole: a clinico-pathologic study involving'grading' as a measure of possible malignant change.Obstet. and Gynec., 1, 593-609.
Hunter, J. S., Jr., and Dockerty, M. B. (1955). Choriocar-cinoma. Obstet. and Gynec., 5, 598-611.
Iliya, F. A., Williamson, S., and Azar, H. A. (1967). Chorio-carcinoma in the Near East: consanguinity as a possibleetiologic factor. Cancer (Philad.), 20, 144-149.
International Union against Cancer (1967). Choriocarcinoma:Transactions of a Conference of the International Unionagainst Cancer, edited by J. F. Holland and M. M. Hresh-chyshyn, Appendix 1. Spriniger, Berlin.
Ishizuka, N. (1967). Chemotherapy of chorionic tumours.In Choriocarcinoma: Transactions of a Conference of theInternational Union against Cancer, edited by J. F. Hollandand M. M. Hreshchyshyn, pp. 116-118. Springer, Berlin.
Jacobson, F. J., and Enzer, N. (1959). Hydatidiform molewith 'benign' metastasis to lung. Amer. J. Obstet. Gynec.,78, 868-875.
Kolstad, P., and Hognestad, J. (1965). Trophoblastic tumoursin Norway. Acta obstet. gynaec. scand., 44, 80-88.
Krieg, H. (1972). Antigenicity of human chorionic villoustissue. Int. J. Gynec. Obstet., 10, 144-155.
Laurence, D. J. R., and Neville, A. M. (1972). Foetalantigens and their role in the diagnosis and clinicalmanagement ofhuman neoplasms: a review. Brit. J. Cancer,26, 335-355.
Lawler, S. D., Klouda, P. T., and Bagshawe, K. D. (1971).The HL-A system in trophoblastic neoplasia. Lancet, 2,834-837.
Lewis, J. L., Jr (1973). Human leukocyte antigens and ABOblood groups in gestational trophoblastic neoplasms. Proc.nat. Canc. Confr., 7, 205-211.
Lewis, J. L., Jr, and Terasaki, P. T. (1971). HL-A leukocyteantigen studies in women with gestational trophoblasticneoplasms. Amer. J. Obstet. Gynec., 111, 547-554.
Llewellyn-Jones, D. (1965). Trophoblastic tumours: geo-graphical variations in incidence and possible aetiologicalfactors. J. Obstet. Gynaec. Brit. Cwlth, 72, 242-248.
Logan, B. J., and Motyloff, L. (1958). Hydatidiform mole:a clinical and pathological study of 72 cases, with referenceto their malignant tendencies. Amner. J. Obstet. Gynec., 75,1134-1148.
MacRae, D. J. (1951). Chorionepithelioma occurring duringpregnancy. J. Obstet. Gynaec. Brit. Emp., 58, 373-380.
Marchand, F. (1898). Ueber das maligne Chorion-Epitheliom,nebst Mittheilung von 2 neuen Fallen. Z. Geburtsh. Gyndk.,39, 173-258.
Mathieu, A. (1939). Hydatidiform mole and chorio-epithel-ioma: collective review of the literature for the years 1935,1936, 1937. Int. Abstr. Surg., 68, 52-70, 181-198.
Meyer, A. W. (1919). Hydatidiform degeneration in tubalpregnancy: a report of 48 new cases. Surg. Gynec. Obstet.,28, 293-302.
Mogensen, B., and Kissmeyer-Nielsen, F. (1968). Histo-compatibility antigens of the HL-A locus in generalizedgestational choriocarcinoma. Lancet, 1, 721-725.
Mogensen, B., and Kissmeyer-Nielsen, F. (1971). Currentdata on HL-A and ABO typing in gestational chorio-carcinoma and invasive mole. Transplant. Proc., 3,1267-1269.
Mogensen, B., and Olsen, S. (1973). Cellular reaction togestational choriocarcinoma and invasive mole. Acta path.microbiol. scand., Sect. A, 81, 453-456.
Nilsson, L. (1957). Hydatidiform degeneration in abortedova: a histopathological and clinical study. Acta obstet.gynaec. scand., 36, Suppl. 7.
Novak, E. (1922). Hydatidiform mole and chorioepithelioma:a clinical and pathologic study. J. Amer. med. Ass., 78,1771-1779.
Novak, E., and Koff, A. K. (1930). Chorioepithelioma withespecial reference to disappearance of primary uterinetumour. Amer. J. Obstet. Gynec., 20, 153-164.
Novak, E., and Seah, C. S. (1954a). Choriocarcinoma of theuterus: study of 74 cases from the Mathieu MemorialChorionepithelioma Registry. Amer. J. Obstet. Gynec., 67,933-957.
Novak, E., and Seah, C. S. (1954b). Benign trophoblasticlesions in Mathieu Chorionepithelioma Registry (hydatidi-form mole, syncytial endometritis). Amer. J. Obstet. Gynec.,68, 376-390.
Novak, E. R., and Woodruff, J. D. (1974). Hydatidiformmole and choriocarcinoma. In Novak's Gynecologic andIn Obstetric Pathology, 7th edn, pp. 599-633. Saunders,Phildaelphia.
Ober, W. B., Edgcomb, J. H., and Price, E. B., Jr (1971).The pathology of choriocarcinoma. Ann. N. Y. Acad. Sci.,172, 299-426.
Park, W. W. (1959). Disorders arising from the humantrophoblast. In Modern Trends in Pathology, edited byD. H. Collins, pp. 180-211. Butterworth, London.
Park, W. W. (1967). The pathology of trophoblastic tumours.In Choriocarcinoma: Transactions of a Conference of theInternational Union against Cancer, edited by J. F. Hollandand M. M. Hreshchyshyn, pp. 3-8. Springer, Berlin.
Park, W. W. (1971). Choriocarcinoma: A study of its Patho-logy. Heinemann, London; Davis, Philadelphia.
Park, W. W., and Lees, J. C. (1950). Choriocarcinoma: ageneral review, with an analysis of 516 cases. Arch. Path.,49, 73-104 and 205-241.
Prawirohardjo, S., Martiono, K. S., and Sutomo, T. (1957).Hydatidiform mole and choriocarcinoma in Indonesia.In Proceedings of the First Asiatic Congress ofObstetricsand Gynecology, Tokyo, pp. 112-129.
Reed, S., Coe, J. I., and Bergquist, J. (1959). Invasive hyda-tidiform mole metastatic to the lungs: report of a case.Obstet. and Gynec., 13, 749-753.
Ring, A. M. (1972). The concept of benign metastasizinghydatidiform moles. Amer. J. clin. Path., 58, 111-117.
Ringertz, N. (1970). Hydatidiform mole, invasive mole andchoriocarcinoma in Sweden, 1958-1965. Acta obstet.gynaec. scand., 49, 195-203.
Rudolph, R. H., and Thomas, E. D. (1970). Histocompati-bility studies in patients with trophoblastic tumors. Amer.J. Obstet. Gynec., 108, 1126-1129.
Schiffer, M. A., Pomerance, W., and Mackles, A. (1960).Hydatidiform mole in relation to malignant disease of thetrophoblast. Amer. J. Obstet. Gynec., 80, 516-531.
130
copyright. on O
ctober 23, 2020 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.s3-10.1.111 on 1 January 1976. D
ownloaded from

The histopathology of trophoblastic tumours
Schmidt, P. J., and Hertz, R. (1961). Blood group factors inwomen with choriocarcinoma as compared with those oftheir husbands. Amer. J. Obstet. Gynec., 82, 651-653.
Schmorl, G. (1893). Pathologisch-anatomische Untersuch-ungen uber Puerperal-Eklampsie. Vogel, Leipzig.
Schopper, W., and Pliess, G. (1949). Ober Chorionepithel-iosis: ein Beitrag zur Genese, Diagnostik und Bewertungektopischer chorionepithelialer Wucherungen. Virchow'sArch. path. Anat., 317, 347-384.
Smalbraak, J. (1957). Trophoblastic Grow,ths: A Clinical,Hormonal and Histo-Pathologic Study of HydatidiformMole and Choriocarcinoma. Elsevier, Amsterdam.
Sta. Cruz, J. Z. (1959). The pathological diagnosis of chorio-carcinoma from endometrial scraping. J. Philip. med. Ass.,35, 805-809.
Strauss, F., Benirschke, K., and Driscoll, S. G. (1967).Placenta Handbuch der speziellen pathologischen Anatomieund Histologie, edited by 0. Lubarsch and F. Henke,Bd. VII, Teil 5. Springer, Berlin.
Teacher, J. H. (1903). On chorionepithelioma and theoccurrence of chorionepitheliomatous and hydatidiformmole-like structures in teratomata. J. Obstet. Gynaec. Brit.
Emp., 4, 1-64, 145-199.Teacher, J. H. (1935). A Manual of Obstetric and Gynaeco-
logical Pathology, edited by A. J. Marshall, p. 148. OxfordUniversity Press, London.
Thiele, R. A., and de Alvarez, R. R. (1962). Metastasizingbenign trophoblastic tumors. Amner. J. Obstet. Gynec., 84,1395-1406.
Tow, W S. H. (1966). The classification of malignant growthsof the chorion. J. Obstet. Gynaec. Brit. Cwlth, 73, 1000-1001
Tow, W. S. H., and Yung, R. H. (1967). The value of histo-logical grading in prognostication of hydatidiform mole.J. Obstet. Gynaec. Brit. Cwlth, 74, 292-293.
Veit, J. (1901). Ueber Deportation von Chorionzotten.Z. Geburtsh. Gyndk, 44,466-504.
Waksman, B. H. (1960). A comparative histopathologicalstudy of delayed hypersensitivity reactions. In CibaFoundation Symposium on Cellular Aspects of Immunity,edited by G. E. W. Wolstenholme and M. O'Connor,pp. 280-329. Churchill, London.
Wilson, R. B., Hunter, J. S., Jr, and Dockertv, M. B. (1961).Chorioadenoma destruens. Amer. J. Obstet. Gynec., 81,546-559.
131
copyright. on O
ctober 23, 2020 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.s3-10.1.111 on 1 January 1976. D
ownloaded from