Embed Size (px)
Citation preview
Hand Surgery
UHPHERBERT-ULNAKOPFPROTHESE®
HERBERT ULNAR HEAD PROSTHESIS®
Störungen des distalen Radioulnargelenkesund Notwendigkeit einer UlnakopfprotheseTimothy -J. Herbert/Jörg van Schoonhoven
Disorders of the Distal Radio-Ulnar Joint andthe Need for a New Ulnar Head ProsthesisTimothy -J. Herbert/Jörg van Schoonhoven
Einleitung
Störungen des distalen Radioulnargelenkes sind häufig.Klinisch steht eine schmerzhafte Einschränkung der Unter-armdrehung mit Kraftverlust und möglicher Instabilität desdistalen Radioulnargelenkes im Vordergrund. Ziel der chirurgi-schen Behandlung muss die Wiederherstellung einer schmerz-freien Unterarmdrehung bei gleichzeitiger Stabilität desdistalen Radioulnargelenkes sowie des ulnaren Handgelenk-kompartimentes sein. Bis heute gibt es kein einziges chirur-gisches Verfahren, das sowohl eine schmerzfreie Unterarmro-tation garantiert als auch gleichzeitig eine Längendiskrepanzvon Radius und Ulna oder eine Instabilität behebt. Ausdiesem Grunde ist die Behandlung des distalen Radioulnar-gelenkes bislang umstritten.
Die Ulnakopfprothese wurde entwickelt, um eine schmerz-freie Beweglichkeit wiederherzustellen. Zur selben Zeitkann unter Verwendung der Ulnakopfprothese das Längen-verhältnis von Radius und Ulna wiederhergestellt werden.Die Stabilität des distalen Radioulnargelenkes wird durcheine Weichteilrekonstruktion unter Verwendung eines spezi-ellen ulnargestielten Weichteillappens mit gleichzeitigerRekonstruktion des ulnokarpalen Komplexes (TFCC)erreicht.
Anatomie
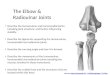
Das distale Radioulnargelenk ist ein flachschaliges Kugel-gelenk zwischen dem Ulnakopf und der Incisura ulnaris desRadius. Dieses Gelenk ermöglicht eine Unterarmrotationvon 180° (Radius um Ulna, Abb. 1), die für den normalen,uneingeschränkten Gebrauch der Hand entscheidend ist.
Der ulnokarpale Bandkomplex fungiert als Puffer zwischenUlnakopf und proximaler Handwurzelreihe. Seine starkenAnsatzstellen an der Basis des Processus styloideus ulnaeund der Kapsel des distalen Radioulnargelenkes machenihn zusätzlich zum Hauptstabilisator des distalen Radio-ulnargelenkes. In ähnlicher Weise gehen seine distalen Aus-läufer in die Handgelenkskapsel über und bewirken so eineulnarseitige Stabilisierung der Handwurzel am Handgelenk.Dies ermöglicht am ulnokarpalen Gelenk eine freie Beugung,Streckung, ulnare und radiale Deviation.
Bowers (1991) gibt einen hervorragenden Überblick überdie anatomischen Verhältnisse mit einer Beschreibung derFunktion des distalen Radioulnargelenkes bei normalemsowie instabilem Handgelenk.
Introduction
Disorders of the distal radio-ulnar joint (DRUJ) are commonand are usually associated with pain, weakness, instabilityand loss of forearm rotation. The aim of surgical treatmentis to restore a painfree range of forearm rotation with a sta-ble ulna and wrist. Today, there is no single surgical proce-dure which can be guaranteed to restore painfree rotationand at the same time correct any underlying instability oflength discrepancy. For this reason treatment of the DRUJremains controversial.
The ulnar head prosthesis has been designed to restorepainfree forearm rotation at the same time as any lengthdiscrepancy is corrected, stability is achieved by means of asimple soft tissue repair (so called “ulnar-flap”), which iscombined with a reconstruction of the triangular fibro-carti-lage complex (TFCC).
Anatomy
The DRUJ consists of a shallow “ball and socket” articulati-on between the head of the ulna and the sigmoid fossa ofthe radius. This articulation allows for 180 degrees of fore-arm rotation (radius on ulna, Fig. 1), which is essential fornormal function of the hand.
The TFCC acts as a cushion between the head of the ulnaand the proximal row of the carpus. By means of its strongsoft tissue attachments to the apex of the ulnar head andthe capsule of the DRUJ, it is also the major stabiliser ofthe DRUJ. Similarly, its distal expansions merge with thewrist capsule to stabilise the ulnar side of the carpus onthe wrist. It allows for a free range of flexion, extension,ulnar deviation and radial deviation at the ulno-carpal joint.
Bowers (1991) provides an excellent review of the anatomyand function of the DRUJ in the normal and unstable wrist.
33
Dorsal
Dorsal
Volar
Volar
DorsalVolar
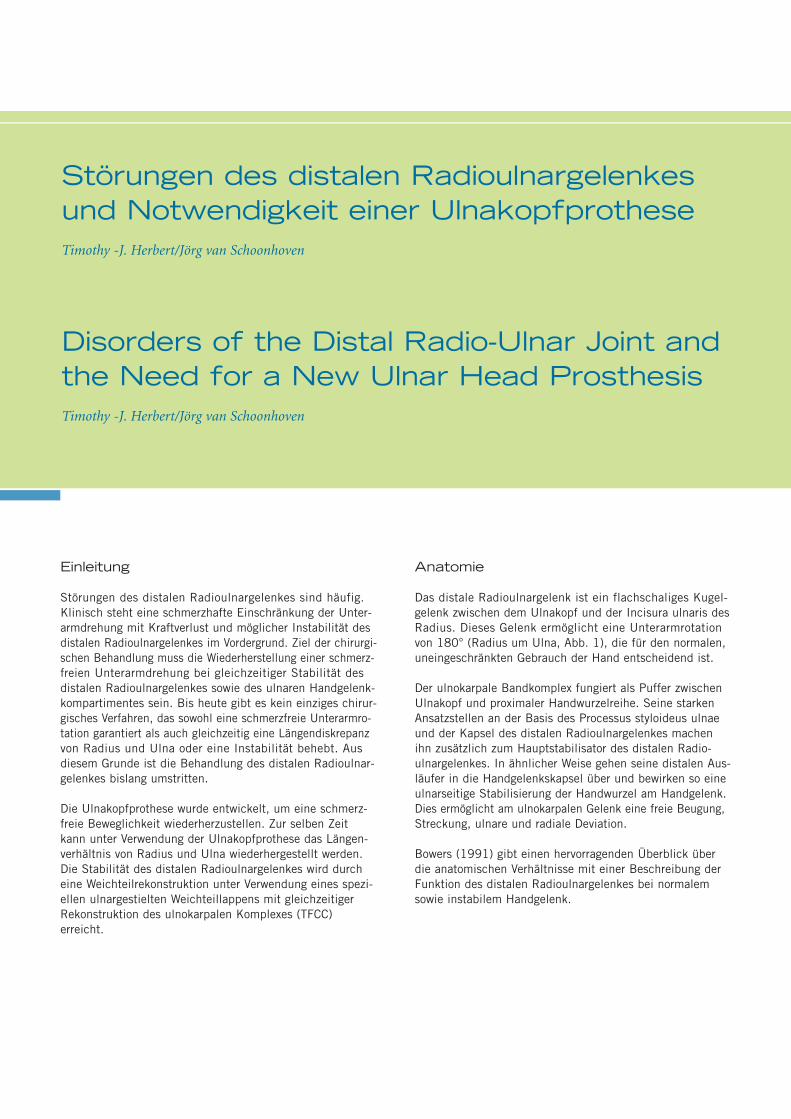
Pronation Midrotation Supination
Abb. 1: Rotation des Radius um die Ulna. Aus: Bowers WH: Das distaleRadioulnargelenk. In: Green DP, ed Operative Hand Surgery. 2nd. ed.New York: Churchill Livingston, 1988: 939-990.
Fig. 1: Rotation of the radius on the ulna. From: Bowers WH The distalradio-ulnar joint. In: Green DP, ed Operative Hand Surgery. 2nd. ed.New York: Churchill Livingston, 1988: 939-990.

Erkrankungen des distalen Radio-ulnargelenkes
Jeder Kongruitätsverlust zwischen Incisura ulnaris des Radi-us und Ulnakopf hat eine schmerzhafte Einschränkung derUnterarmdrehung zur Folge und führt in der Regel langfri-stig zur Arthrose des distalen Radioulnargelenkes. Dieskann verschiedene Ursachen haben: angeborene Deformi-täten wie die Madelung’sche Deformität, Radiusfrakturen,rheumatoide Arthritis oder degenerative Arthrose als Folgevon Einrissen im ulnokarpalen Bandkomplex.
Einrisse im ulnokarpalen Bandkomplex treten extrem häufigauf, vor allem bei Patienten mit einer Ulna-Plus-Situation(81%, Palmer und Werner 1981). Solche Einrisse könnenvon einem akuten oder chronischen Trauma herrühren undverursachen Schmerzen und Bewegungsverlust am ulnarenHandgelenk.Ein Kontinuitätsverlust des ulnokarpalen Bandkomplexesführt zu einer Instabilität sowohl des distalen Radioulnarge-lenkes als auch des ulnokarpalen Gelenkes. Im Laufe derZeit entwickelt sich daraus zumeist eine fixierte Deformitätmit der Konsequenz einer sekundären Arthrose.
Mit zunehmendem Funktionsverlust des ulnokarpalen Band-komplexes geht das normale Alignement von Radius undUlna verloren. Die dadurch bedingte radiologisch zuneh-mende Ulna-Plus-Situation am ulnokarpalen Handgelenkführt zum Anschlagen des Ulnakopfes gegen den Os trique-trum und Os lunatum. Dieses sogenannte Impaction-Syn-drom kann eine lunotriquetrale Instabilität mit ulnokarpalerArthrose hervorrufen. Die häufigste Ursache für diesen Pro-zess stellt die distale Radiusfraktur dar. Die gleichzeitigeAbrissfraktur des Processus styloideus ulnae kann zu einerfunktionellen Instabilität des ulnokarpalen Bandkomplexesführen. Am häufigsten führt jedoch eine in Fehlstellung ver-heilte distale Radiusfraktur zu einer sekundären Ulna-Plus-Deformität. Gelegentlich kann zusätzlich die direkte Beschä-digung der Incisura ulnaris zur Entwicklung einer sekun-dären Arthrose des distalen Radioulnargelenkes führen.
Eine weitere Ursache ist die traumatische Luxation desdistalen Radioulnargelenkes, gelegentlich in Verbindung miteiner Radiusköpfchen-Fraktur und Verletzung der Membranainter-ossea (Essex-Lopresti-Läsion).
Andere Ursachen, die die Funktion des distalen Radioulnar-gelenkes und ulnokarpalen Bandkomplexes betreffen, sindWachstumsstörungen (Madelung’sche Deformität), primäreArthrose des distalen Radioulnargelenkes, Stoffwechsel-störungen (z.B. Gicht) oder die rheumatoide Arthritis.
Zudem zeigt sich bei vielen Patienten eine schmerzhafte In-stabilität infolge vorausgegangener Operationen am distalenRadioulnargelenk.
Disorders of the DRUJ
Any loss of congruity between the sigmoid fossa and theulnar head will result in painful loss of forearm rotation.Causes include congenital abnormalities such as Madelung’sdeformity, radial fractures, inflammatory arthritis or degene-rative arthrosis as a consequence of tears of the TFCC.
Tears of the TFCC are extremely common, particularly inpatients with ulnar plus variance (81%, Palmer and Werner1981). Tears may be due to acute or chronic trauma, andlead to pain and loss of motion in the ulnar side of thewrist; loss of integrity of the TFCC results in instability ofboth the DRUJ and the ulno-carpal joint. In time, this islikely to become a fixed deformity leading to secondaryosteoarthritis.
As the TFCC fails, the normal alignment between thedistal radius and ulna is lost and x-rays will show evidenceof increasing ulnar plus deformity to the extent that theulna starts to impact on the lunate and/or triquetrum. Thisimpaction may result in triquetro-lunate instability andulno-carpal osteoarthritis.The commonest cause of these problems is fracture of thedistal radius. This may be associated with avulsion fractureof the ulnar styloid process, leading to functional instabilityof the TFCC. More commonly, radial malunion results in asecondary ulnar plus deformity. Occasionally direct damageto the sigmoid fossa may lead to the development of secon-dary osteo-arthritis.
Furthermore trauma may result in acute dislocation of theDRUJ itself, often in association with radial head fractureand tear of the interosseous membrane (Essex-Lopresti lesion).
Other conditions affecting the DRUJ and TFCC includegrowth disorders (Madelung’s deformity), primary osteo-arthritis, metabolic disorders (e.g. gout), rheumatoid arthritis.Finally, many patients present with painful instability follo-wing previous surgical procedures on the DRUJ.

UU
55
Derzeit gebräuchliche Operationsverfahren beiStörungen des distalenRadioulnargelenkes
1. Die Exzision des Ulnakopfes nach Dar-rach (Tulipan et al. 1991, Abb. 1) destabili-siert den ulnokarpalen Bandkomplex. Die Abwesenheit des Ulnakopfes führt oft-mals zu einem schmerzhaften radioulnarenImpingement.
Current operations forDRUJ disorders
1. Excision of the ulnar head (Darrach’sprocedure Tulipan et al. 1991, Fig. 1) desta-bilizes the TFCC leading to ulno-carpal andradio-ulnar instability. Absence of the ulnarhead often results in painful radio-ulnarimpingement.
2. Beim Verfahren von Bowers (Bowers1985, Abb. 2) können einige der beim Dar-rach-Verfahren auftretenden Probleme ver-mieden werden. Indem die Verbindung desulnokarpalen Bandkomplexes mit dem Pro-cessus styloideus ulnae erhalten bleibt, istein gewisses Maß an Stabilität gegeben.Allerdings ist die Weichteilinterposition zwi-schen Incisura ulnaris des Radius und Ulna-Resektionsfläche selten kräftig genug, umeine parallele Ausrichtung von Radius undUlna zu gewährleisten, was letztendlich wie-derum zur ulnokarpalen und radio-ulnarenInstabilität führt. Außerdem kommt es imFalle einer Ulna-Plus-Situation zu einemulnokarpalen Impaction, sofern nicht gleich-zeitig auch die Ulna verkürzt wird.
2. Bowers procedure (Bowers 1985, Fig. 2)attempts to overcome the problems associa-ted with Darrach’s procedure as outlinedabove. By preserving the attachment of theTFCC to the ulnar styloid process, some sta-bility is retained. However, soft tissue inter-position between the sigmoid fossa and theresected surface of the ulna is seldom strongenough to prevent some degree of ulno-carpaland radio-ulnar instability, due to loss of thenormal alignment between the radius andthe ulna. Furthermore, in cases of ulnar plusvariance, ulno-carpal impaction will occurunless the ulna is shortened at the sametime.
3. Bei Durchführung der Operation nachSauve-Kapandji (Sanders et. al. 1991, Abb. 3)in korrekter Weise wird ein ulnokarpalesImpaction vermieden, wobei gleichzeitig derulnokarpale Bandkomplex funktionsfähigbleibt. Die Wiederherstellung der Rotationwird hier allerdings auf Kosten einer instabi-len Ulna-Pseudoarthrose erkauft, die in derRegel zu einem schmerzhaften radio-ulnarenImpingement führt. Außerdem ist die exaktePositionierung der distalen radio-ulnarenArthrodese problematisch, was dazu führt,dass viele Patienten persistierende ulnokar-pale Probleme im Sinne eines Impaction-Syndroms behalten.
3. The Sauve-Kapandji procedure (Sanderset. al. 1991, Fig. 3), if performed correctly,will relieve any ulno-carpal impaction whilstmaintaining function of the TFCC. However,rotation is only restored at the expense of anunstable ulnar pseudoarthrosis which com-monly results in painful radio-ulnar impinge-ment. Furthermore the exact positioning ofthe radio-ulnar fusion is difficult, with theresult that many patients still have ulno-carpal impaction and TFCC problems.
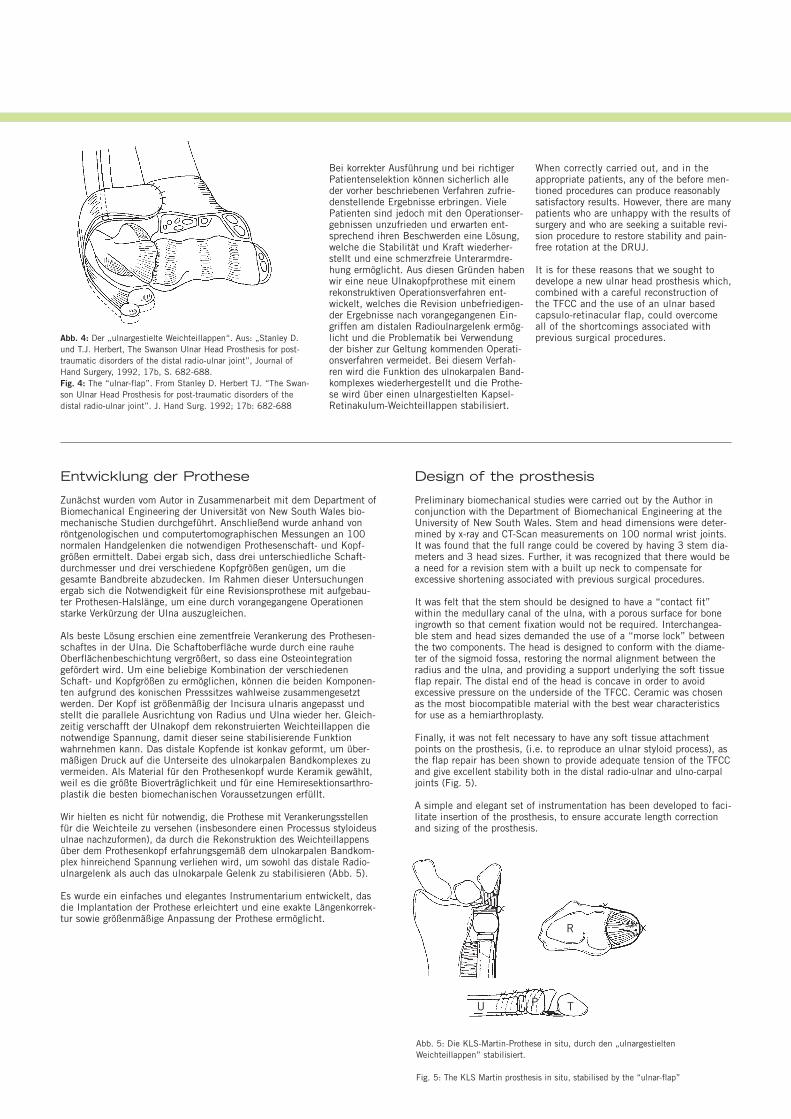
4. Der Ulnakopfersatz durch Silikonplatzhal-ter (Swanson 1973) wurde entwickelt, umeine radioulnare Instabilität nach erfolgterUlnakopfresektion zu verhindern. Durch diezuvor beschriebenen Operationsmodifikatio-nen (Stanley und Herbert 1992, Abb. 4)ermöglicht dieses Verfahren auch eine Re-konstruktion des ulnokarpalen Bandkomple-xes mit Beseitigung der ulnokarpalen Insta-bilität. Der hohe Silikonabrieb mit Silikon-synovitis sowie der häufige Prothesenbruchführten dazu, dass viele dieser Prothesenwieder entfernt werden mussten, was letzt-endlich wieder eine schmerzhafte ulnokar-pale Instabilität zur Folge hatte.
Die zur Zeit von den meisten Chirurgenfavorisierten Verfahren sind sicherlich dieHIT nach Bowers sowie die Arthrodese desdistalen Radioulnargelenkes mit Segmentre-sektion aus der Ulna nach Sauve-Kapandji.Die Indikation zur Ulnakopfresektion nachDarrach ist lediglich noch für Patienten mitgeringen Anforderungen an das Handgelenkgegeben (z.B. bei rheumatoider Arthritis).Die Swanson-Prothese findet aufgrund derzuvor geschilderten Problematik keine An-wendung mehr.
4. Silastic ulna head replacement (Swanson1973) was designed to prevent radio-ulnarinstability following ulnar head resection.With modifications previously described(Stanley and Herbert 1992, Fig. 4) it mayalso allow for reconstruction of the TFCCand restoration of ulno-carpal instability.However, the silastic prosthesis is subject to excessive wear which may be complicatedby the development of silicone synovitis.Many of these prostheses have had to beremoved resulting in painful ulno-carpalinstability.
At the present time, most surgeons prefereither the Bowers or the Sauve-Kapandjiprocedure. Darrach’s procedure is normallyreserved for low demand patients (e.g. rheu-matoid arthritis), whilst the Swanson pros-thesis is no longer available and has fallenout of favour.
Abb. 1: Ulnakopfresektion nach Darrach. R=Radius, U=Ulna,T=TriquetrumFig. 1: Darrach’s procedure. R=radius, U=ulna, T=triquetrum
R
TU
U
Abb. 2: Hemiresektions-Interpositions-Technik nach Bowers mitLängenkorrektur der Ulna.Fig. 2: Bowers’ procedure with correction of ulnar length
R
UT
UU
Abb. 3: Arthrodese des distalen Radioulnargelenkes mit Segment-resektion aus der distalen Ulna nach Sauve-Kapandji.Fig. 3: Sauve-Kapandji procedure
R
U T
Bei korrekter Ausführung und bei richtigerPatientenselektion können sicherlich alleder vorher beschriebenen Verfahren zufrie-denstellende Ergebnisse erbringen. VielePatienten sind jedoch mit den Operationser-gebnissen unzufrieden und erwarten ent-sprechend ihren Beschwerden eine Lösung,welche die Stabilität und Kraft wiederher-stellt und eine schmerzfreie Unterarmdre-hung ermöglicht. Aus diesen Gründen habenwir eine neue Ulnakopfprothese mit einemrekonstruktiven Operationsverfahren ent-wickelt, welches die Revision unbefriedigen-der Ergebnisse nach vorangegangenen Ein-griffen am distalen Radioulnargelenk ermög-licht und die Problematik bei Verwendungder bisher zur Geltung kommenden Operati-onsverfahren vermeidet. Bei diesem Verfah-ren wird die Funktion des ulnokarpalen Band-komplexes wiederhergestellt und die Prothe-se wird über einen ulnargestielten Kapsel-Retinakulum-Weichteillappen stabilisiert.
When correctly carried out, and in theappropriate patients, any of the before men-tioned procedures can produce reasonablysatisfactory results. However, there are manypatients who are unhappy with the results ofsurgery and who are seeking a suitable revi-sion procedure to restore stability and pain-free rotation at the DRUJ.
It is for these reasons that we sought todevelope a new ulnar head prosthesis which,combined with a careful reconstruction ofthe TFCC and the use of an ulnar basedcapsulo-retinacular flap, could overcome all of the shortcomings associated with previous surgical procedures.
Entwicklung der Prothese
Zunächst wurden vom Autor in Zusammenarbeit mit dem Department ofBiomechanical Engineering der Universität von New South Wales bio-mechanische Studien durchgeführt. Anschließend wurde anhand vonröntgenologischen und computertomographischen Messungen an 100normalen Handgelenken die notwendigen Prothesenschaft- und Kopf-größen ermittelt. Dabei ergab sich, dass drei unterschiedliche Schaft-durchmesser und drei verschiedene Kopfgrößen genügen, um diegesamte Bandbreite abzudecken. Im Rahmen dieser Untersuchungenergab sich die Notwendigkeit für eine Revisionsprothese mit aufgebau-ter Prothesen-Halslänge, um eine durch vorangegangene Operationenstarke Verkürzung der Ulna auszugleichen.
Als beste Lösung erschien eine zementfreie Verankerung des Prothesen-schaftes in der Ulna. Die Schaftoberfläche wurde durch eine rauheOberflächenbeschichtung vergrößert, so dass eine Osteointegrationgefördert wird. Um eine beliebige Kombination der verschiedenenSchaft- und Kopfgrößen zu ermöglichen, können die beiden Komponen-ten aufgrund des konischen Presssitzes wahlweise zusammengesetztwerden. Der Kopf ist größenmäßig der Incisura ulnaris angepasst undstellt die parallele Ausrichtung von Radius und Ulna wieder her. Gleich-zeitig verschafft der Ulnakopf dem rekonstruierten Weichteillappen dienotwendige Spannung, damit dieser seine stabilisierende Funktionwahrnehmen kann. Das distale Kopfende ist konkav geformt, um über-mäßigen Druck auf die Unterseite des ulnokarpalen Bandkomplexes zuvermeiden. Als Material für den Prothesenkopf wurde Keramik gewählt,weil es die größte Bioverträglichkeit und für eine Hemiresektionsarthro-plastik die besten biomechanischen Voraussetzungen erfüllt.
Wir hielten es nicht für notwendig, die Prothese mit Verankerungsstellenfür die Weichteile zu versehen (insbesondere einen Processus styloideusulnae nachzuformen), da durch die Rekonstruktion des Weichteillappensüber dem Prothesenkopf erfahrungsgemäß dem ulnokarpalen Bandkom-plex hinreichend Spannung verliehen wird, um sowohl das distale Radio-ulnargelenk als auch das ulnokarpale Gelenk zu stabilisieren (Abb. 5).
Es wurde ein einfaches und elegantes Instrumentarium entwickelt, dasdie Implantation der Prothese erleichtert und eine exakte Längenkorrek-tur sowie größenmäßige Anpassung der Prothese ermöglicht.
Design of the prosthesis
Preliminary biomechanical studies were carried out by the Author inconjunction with the Department of Biomechanical Engineering at theUniversity of New South Wales. Stem and head dimensions were deter-mined by x-ray and CT-Scan measurements on 100 normal wrist joints.It was found that the full range could be covered by having 3 stem dia-meters and 3 head sizes. Further, it was recognized that there would bea need for a revision stem with a built up neck to compensate forexcessive shortening associated with previous surgical procedures.
It was felt that the stem should be designed to have a “contact fit”within the medullary canal of the ulna, with a porous surface for boneingrowth so that cement fixation would not be required. Interchangea-ble stem and head sizes demanded the use of a “morse lock” betweenthe two components. The head is designed to conform with the diame-ter of the sigmoid fossa, restoring the normal alignment between theradius and the ulna, and providing a support underlying the soft tissueflap repair. The distal end of the head is concave in order to avoidexcessive pressure on the underside of the TFCC. Ceramic was chosenas the most biocompatible material with the best wear characteristicsfor use as a hemiarthroplasty.
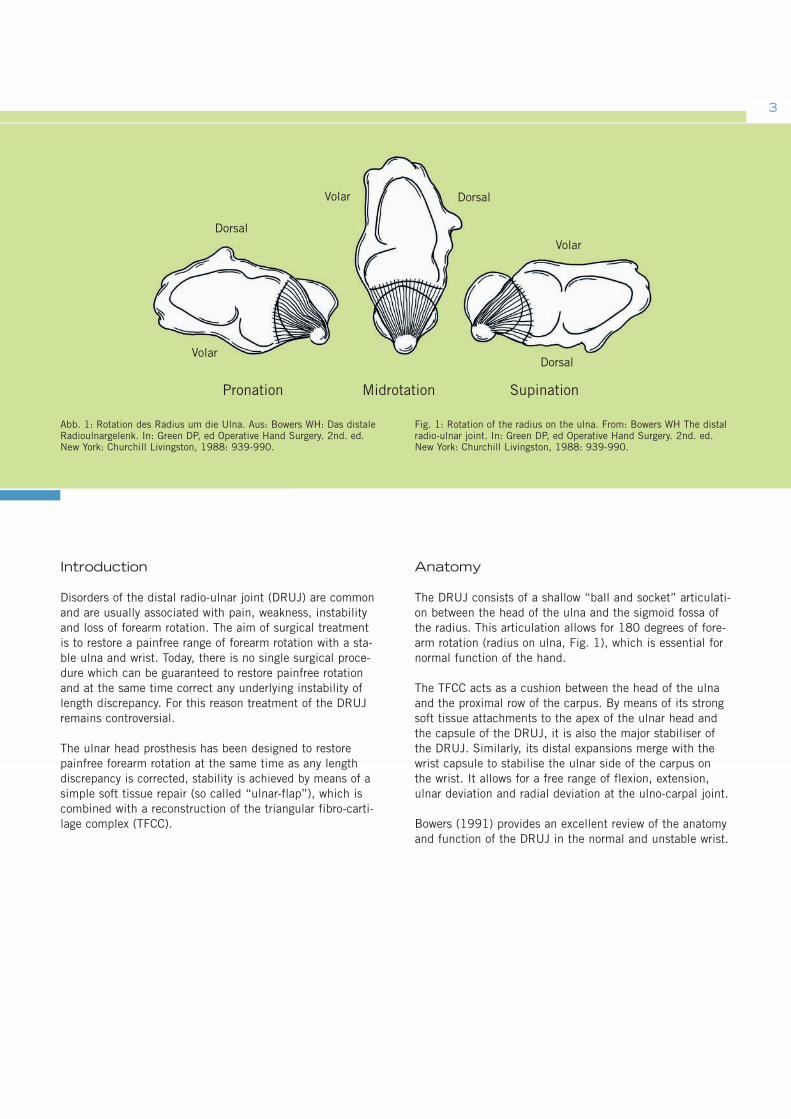
Finally, it was not felt necessary to have any soft tissue attachmentpoints on the prosthesis, (i.e. to reproduce an ulnar styloid process), asthe flap repair has been shown to provide adequate tension of the TFCCand give excellent stability both in the distal radio-ulnar and ulno-carpaljoints (Fig. 5).
A simple and elegant set of instrumentation has been developed to faci-litate insertion of the prosthesis, to ensure accurate length correctionand sizing of the prosthesis.
Abb. 5: Die KLS-Martin-Prothese in situ, durch den „ulnargestieltenWeichteillappen” stabilisiert.
Fig. 5: The KLS Martin prosthesis in situ, stabilised by the “ulnar-flap”
R
U TPP
Abb. 4: Der „ulnargestielte Weichteillappen“. Aus: „Stanley D.und T.J. Herbert, The Swanson Ulnar Head Prosthesis for post-traumatic disorders of the distal radio-ulnar joint”, Journal ofHand Surgery, 1992, 17b, S. 682-688.Fig. 4: The “ulnar-flap”. From Stanley D. Herbert TJ. “The Swan-son Ulnar Head Prosthesis for post-traumatic disorders of thedistal radio-ulnar joint”. J. Hand Surg. 1992; 17b: 682-688
7
Van Schoonhoven J, Lanz U:Rettungsoperationen und deren Differenzialindikation am distalen RadioulnargelenkOrthopäde 2004; 33: 704-714
Van Schoonhoven J, Herbert TJ, Fernandez DL, Prommersberger KJ, Krimmer H:UlnakopfprotheseOrthopäde 2003; 32: 809-815
Pillukat T, Stütz N, Van Schoonhoven J, Krimmer H: Hangelenk und FingergelenkeOP-JOURNAL 2003; 19: 210-215
Barisani G, Schwendenwein E, Vécsei V:Die Ulnakopfprothese nach Timothy J. Herbert.Osteosynthese International 2001; 9: 124-127.
Van Schoonhoven J, Herbert TJ, Krimmer H:Neue Konzepte der Endoprothetik des distalen RadioulnargelenksHandchir. Mikrochir. Plast. Chir. 30 1998; 387-392
LiteraturReference List
•
•
•
•
•
Herbert TJ, van Schoonhoven J: Ulnar Head Replacement Techniques in Hand and Upper Extremity Surgery 2007;11(1):98-108
Van Schoonhoven, Herbert TJ:The Dorsal Approach to the Distal Radioulnar JointTechniques in Hand and Upper Extremity Surgery 2004; 8(1): 11-15
Grechening W, Peicha G, Fellinger M:Primary Ulnar Head Prosthesis for Treatment of an Irreparable Ulnar Head Fracture Dislocation.Journal of Hand Surgery 2001; 26B: 3: 269-271.
Herbert TJ, van Schoonhoven J:Ulnar Head Prosthesis: A new solution for problems at the distal radioulnar joint.Hand Anthroplasties 2000; 145-149.
van Schoonhoven J, Fernandez DL, Bowers WH, Herbert TJ:Salvage of Failed Resection Arthroplasties of the DistalRadioulnar Joint using a new Ulnar Head Prosthesis.Journal of Hand Surgery 2000; 25-A: 3: 438-446.
Fernandez DL:Acute and Chronic Derangement of the Distal Radio Ulnar Joint after Fractures of the Radius.EFORT 1999; 41-53
Stanley D, Herbert TJ: The Swanson ulnar head prosthesis for post-traumatic disorders of the distal radio-ulnar joint. Journal of Hand Surgery 1992; 17B: 682-688.
Bowers WH: Instability of the distal radio-ulnar articulation. Hand Clinics 1991; 7: 311-327.
Sanders RA, Frederick HA, Hontas RB: The Sauve-Kapandji procedure: A salvage operation for the distal radio-ulnar joint. Journal of Hand Surgery 1991; 1125-1129.
Tulipan DJ, Eaton RG, Eberhart RE.: The Darrach procedure defended: Technique redefined and long-term follow up. Journal of Hand Surgery 1991; 16A: 438-444.
Bowers WH: Distal radio-ulnar joint arthroplasty: The hemiresection-interposition technique. Journal of Hand Surgery 1985; 10A: 169-178.
Palmer AK, Werner FW: The triangular fibrocartilage complex of the wrist – Anatomy and function. Journal of Hand Surgery 1981; 6: 153-162.
Swanson AB: Implant arthroplasty for disabilities of the distal radio-ulnarjoint: Use of a silicone rubber capping implant following resection of the ulnar head. Orthop. Clinics 1973; 4: 373-382.
•
•
•
•
•
•
•
•
•
•
•
•
•

Ulnakopfprothese bei Störungendes distalen Radioulnargelenkes
Indikationen:
• Revision bei unbefriedigenden Resultaten nach:- Darrach-Operation- Bowers-Operation- Sauve-Kapandji-Operation
• Primäre Arthrose
• Posttraumatische Arthrose nach:- Radiusfrakturen- Einrissen im ulnokarpalen Bandkomplex- Ulna-Impaction-Syndrom
• Rheumatoide Arthritis
• Tumore
Kontraindikationen:
• Ausgeprägte Radiusdeformität
• Ungenügende Knochenstruktur
• Insuffiziente Weichteilverhältnisse
Präoperative Untersuchung
Es ist eine sorgfältige klinische Untersuchung erforderlich, um das Ausmaß der Ulna- und/oder Karpusinstabilität exaktfestzustellen. Eine fixierte Deformität oder Dislokation musserkannt werden, da diese bei der Operation korrigiert wer-den muss. Bei Vorliegen einer dorsalen oder palmaren Sub-luxation der Ulna aufgrund einer Radiusfehlstellung oderRadiusdeformität muss diese mit einer entsprechendenRadiuskorrekturosteotomie korrigiert werden.
Vor der Operation sind normale 90/90-Röntgenaufnahmenvon beiden Unterarmen und Handgelenken anzufertigen.Anhand der geeigneten Röntgenschablone (unter Berück-sichtigung eines Vergrößerungsfaktors von 1 :1,1) solltendann das optimale Resektionsniveau sowie die vermutlichbenötigten Kopf- und Schaftgrößen ermittelt werden. Derdirekte Vergleich mit dem gegenseitigen, gesunden Handge-lenk ist bei der Ermittlung des exakten Resektionsniveaushilfreich.
Ulnar Head Prosthesis for Disorders of the Distal Radio-Ulnar Joint
Indications:
• Salvage of:- Darrach- Bowers- Sauve-Kapandji
• Primary osteoarthritis
• Post-traumatic osteoarthritis:- Radial fractures- TFCC tears- Ulnar impingement
• Rheumatoid Arthritis
• Tumors
Contraindications:
• Excess radial deformity
• Inadequate bone stock
• Inadequate soft tissues
Pre-operative assessment
Careful clinical examination is required in order to assess acutely the extent of instability of the ulna and/or the car-pus. Similarly it is important to recognize any fixed defor-mity or dislocation, as this will need to be corrected at thetime of surgery. If dorsal or volar dislocation of the ulnarhead is due to an underlying radial deformity, this shouldbe corrected by means of an appropriate radial osteotomybefore proceeding to ulnar head replacement.
Standard 90/90 degree x-rays of both forearms and wristshave to be obtained preoperatively. The appropriate x-raytemplate, (allow for magnification factor, normally 1 :1.1),should then be used to assess optimum resection level andlikely size of head and stem required. Comparison with theopposite normal wrist is the most helpful way to determinethe appropriate resection level.
OperationsverfahrenOperative Technique
9
Abb. 1/Fig. 1
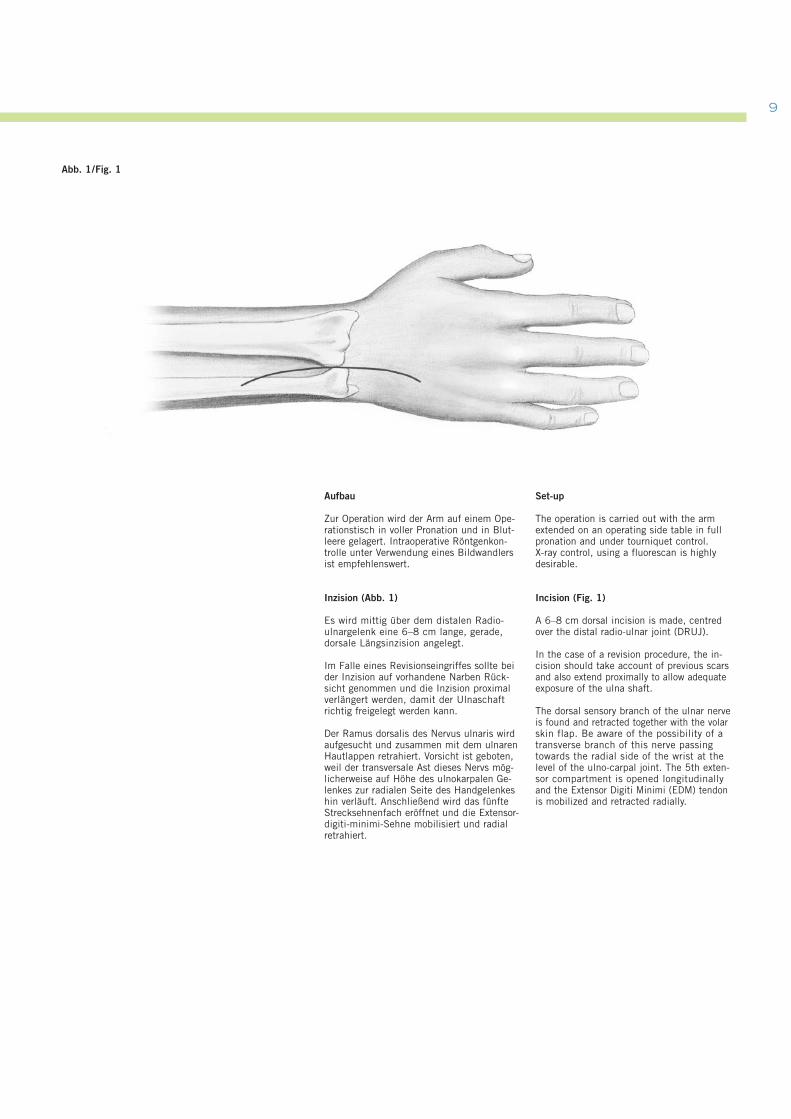
Aufbau
Zur Operation wird der Arm auf einem Ope-rationstisch in voller Pronation und in Blut-leere gelagert. Intraoperative Röntgenkon-trolle unter Verwendung eines Bildwandlersist empfehlenswert.
Inzision (Abb. 1)
Es wird mittig über dem distalen Radio-ulnargelenk eine 6–8 cm lange, gerade,dorsale Längsinzision angelegt.
Im Falle eines Revisionseingriffes sollte beider Inzision auf vorhandene Narben Rück-sicht genommen und die Inzision proximalverlängert werden, damit der Ulnaschaftrichtig freigelegt werden kann.
Der Ramus dorsalis des Nervus ulnaris wirdaufgesucht und zusammen mit dem ulnarenHautlappen retrahiert. Vorsicht ist geboten,weil der transversale Ast dieses Nervs mög-licherweise auf Höhe des ulnokarpalen Ge-lenkes zur radialen Seite des Handgelenkeshin verläuft. Anschließend wird das fünfteStrecksehnenfach eröffnet und die Extensor-digiti-minimi-Sehne mobilisiert und radialretrahiert.
Set-up
The operation is carried out with the armextended on an operating side table in fullpronation and under tourniquet control. X-ray control, using a fluorescan is highlydesirable.
Incision (Fig. 1)
A 6–8 cm dorsal incision is made, centredover the distal radio-ulnar joint (DRUJ).
In the case of a revision procedure, the in-cision should take account of previous scarsand also extend proximally to allow adequateexposure of the ulna shaft.
The dorsal sensory branch of the ulnar nerveis found and retracted together with the volarskin flap. Be aware of the possibility of atransverse branch of this nerve passingtowards the radial side of the wrist at thelevel of the ulno-carpal joint. The 5th exten-sor compartment is opened longitudinallyand the Extensor Digiti Minimi (EDM) tendonis mobilized and retracted radially.
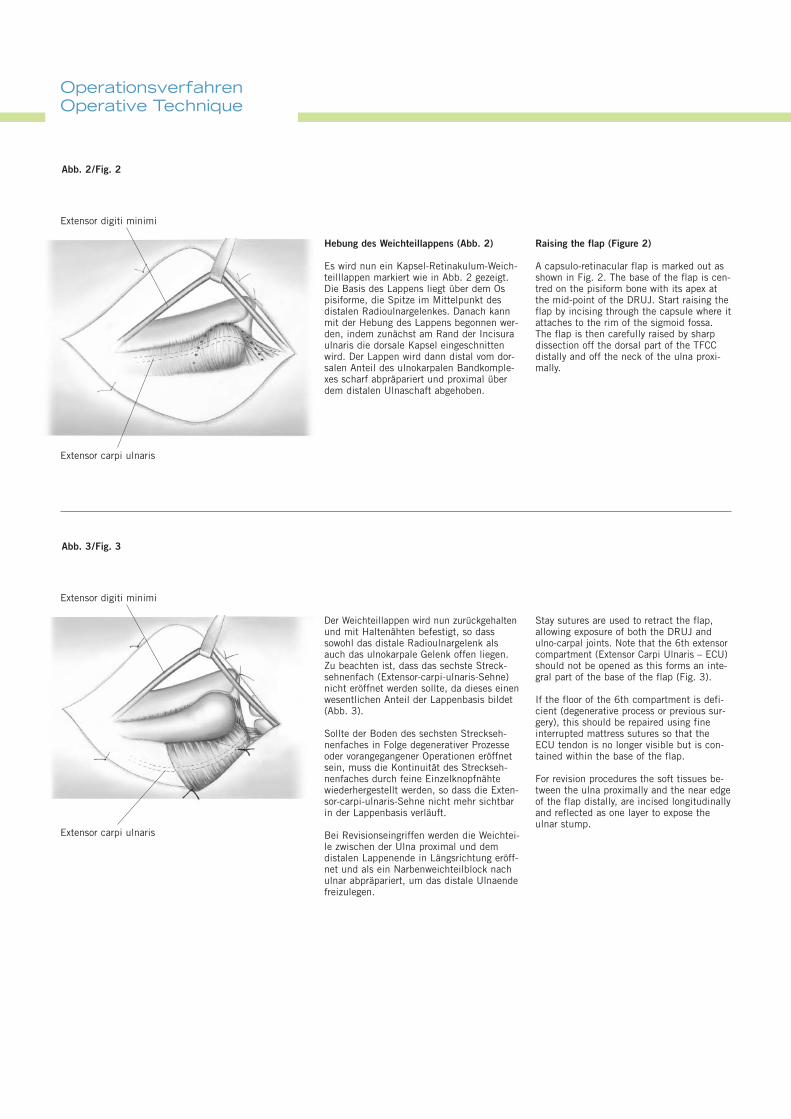
Hebung des Weichteillappens (Abb. 2)
Es wird nun ein Kapsel-Retinakulum-Weich-teilllappen markiert wie in Abb. 2 gezeigt.Die Basis des Lappens liegt über dem Ospisiforme, die Spitze im Mittelpunkt desdistalen Radioulnargelenkes. Danach kannmit der Hebung des Lappens begonnen wer-den, indem zunächst am Rand der Incisuraulnaris die dorsale Kapsel eingeschnittenwird. Der Lappen wird dann distal vom dor-salen Anteil des ulnokarpalen Bandkomple-xes scharf abpräpariert und proximal überdem distalen Ulnaschaft abgehoben.
Raising the flap (Figure 2)
A capsulo-retinacular flap is marked out asshown in Fig. 2. The base of the flap is cen-tred on the pisiform bone with its apex atthe mid-point of the DRUJ. Start raising theflap by incising through the capsule where itattaches to the rim of the sigmoid fossa.The flap is then carefully raised by sharpdissection off the dorsal part of the TFCCdistally and off the neck of the ulna proxi-mally.
Extensor carpi ulnaris
Extensor digiti minimi
Abb. 2/Fig. 2
Der Weichteillappen wird nun zurückgehaltenund mit Haltenähten befestigt, so dasssowohl das distale Radioulnargelenk alsauch das ulnokarpale Gelenk offen liegen.Zu beachten ist, dass das sechste Streck-sehnenfach (Extensor-carpi-ulnaris-Sehne)nicht eröffnet werden sollte, da dieses einenwesentlichen Anteil der Lappenbasis bildet(Abb. 3).
Sollte der Boden des sechsten Streckseh-nenfaches in Folge degenerativer Prozesseoder vorangegangener Operationen eröffnetsein, muss die Kontinuität des Streckseh-nenfaches durch feine Einzelknopfnähtewiederhergestellt werden, so dass die Exten-sor-carpi-ulnaris-Sehne nicht mehr sichtbarin der Lappenbasis verläuft.
Bei Revisionseingriffen werden die Weichtei-le zwischen der Ulna proximal und demdistalen Lappenende in Längsrichtung eröff-net und als ein Narbenweichteilblock nachulnar abpräpariert, um das distale Ulnaendefreizulegen.
Stay sutures are used to retract the flap,allowing exposure of both the DRUJ andulno-carpal joints. Note that the 6th extensorcompartment (Extensor Carpi Ulnaris – ECU)should not be opened as this forms an inte-gral part of the base of the flap (Fig. 3).
If the floor of the 6th compartment is defi-cient (degenerative process or previous sur-gery), this should be repaired using fineinterrupted mattress sutures so that theECU tendon is no longer visible but is con-tained within the base of the flap.
For revision procedures the soft tissues be-tween the ulna proximally and the near edgeof the flap distally, are incised longitudinallyand reflected as one layer to expose theulnar stump.
Extensor carpi ulnaris
Extensor digiti minimi
Abb. 3/Fig. 3
OperationsverfahrenOperative Technique
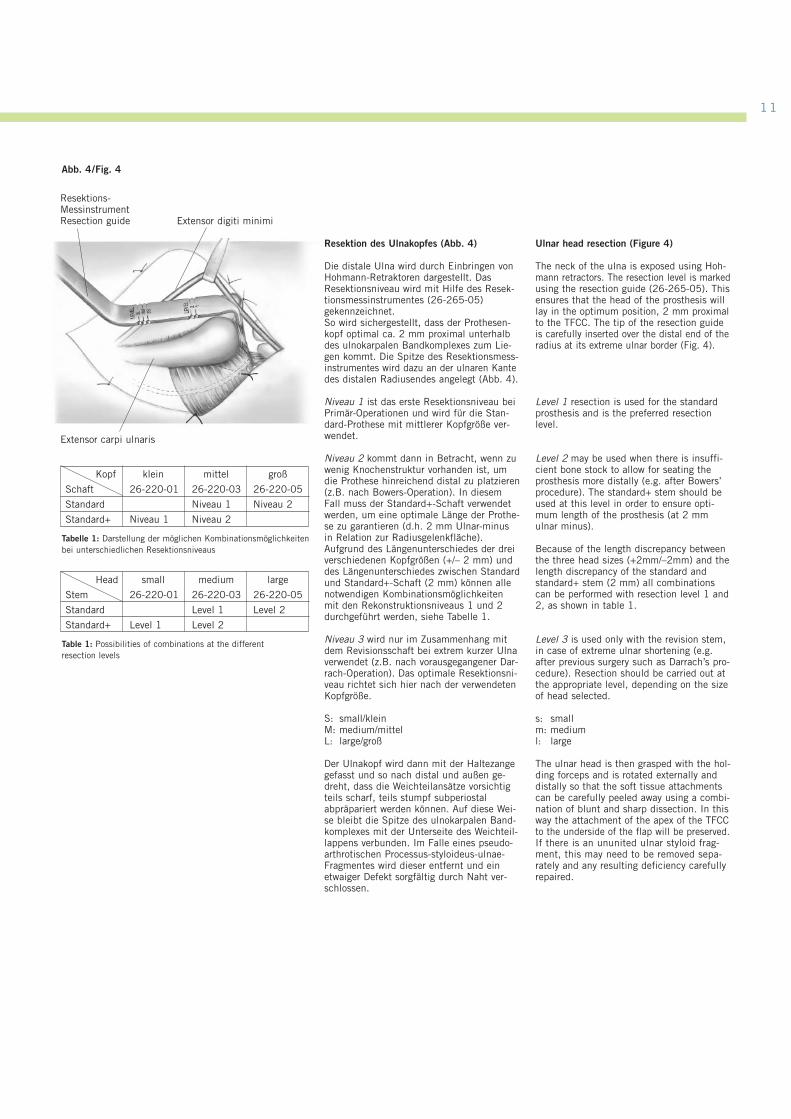
Resektion des Ulnakopfes (Abb. 4)
Die distale Ulna wird durch Einbringen vonHohmann-Retraktoren dargestellt. DasResektionsniveau wird mit Hilfe des Resek-tionsmessinstrumentes (26-265-05)gekennzeichnet. So wird sichergestellt, dass der Prothesen-kopf optimal ca. 2 mm proximal unterhalbdes ulnokarpalen Bandkomplexes zum Lie-gen kommt. Die Spitze des Resektionsmess-instrumentes wird dazu an der ulnaren Kantedes distalen Radiusendes angelegt (Abb. 4).
Niveau 1 ist das erste Resektionsniveau beiPrimär-Operationen und wird für die Stan-dard-Prothese mit mittlerer Kopfgröße ver-wendet.
Niveau 2 kommt dann in Betracht, wenn zuwenig Knochenstruktur vorhanden ist, umdie Prothese hinreichend distal zu platzieren(z.B. nach Bowers-Operation). In diesemFall muss der Standard+-Schaft verwendetwerden, um eine optimale Länge der Prothe-se zu garantieren (d.h. 2 mm Ulnar-minusin Relation zur Radiusgelenkfläche).Aufgrund des Längenunterschiedes der dreiverschiedenen Kopfgrößen (+/– 2 mm) unddes Längenunterschiedes zwischen Standardund Standard+-Schaft (2 mm) können allenotwendigen Kombinationsmöglichkeitenmit den Rekonstruktionsniveaus 1 und 2durchgeführt werden, siehe Tabelle 1.
Niveau 3 wird nur im Zusammenhang mitdem Revisionsschaft bei extrem kurzer Ulnaverwendet (z.B. nach vorausgegangener Dar-rach-Operation). Das optimale Resektionsni-veau richtet sich hier nach der verwendetenKopfgröße.
S: small/kleinM: medium/mittelL: large/groß
Der Ulnakopf wird dann mit der Haltezangegefasst und so nach distal und außen ge-dreht, dass die Weichteilansätze vorsichtigteils scharf, teils stumpf subperiostalabpräpariert werden können. Auf diese Wei-se bleibt die Spitze des ulnokarpalen Band-komplexes mit der Unterseite des Weichteil-lappens verbunden. Im Falle eines pseudo-arthrotischen Processus-styloideus-ulnae-Fragmentes wird dieser entfernt und einetwaiger Defekt sorgfältig durch Naht ver-schlossen.
Ulnar head resection (Figure 4)
The neck of the ulna is exposed using Hoh-mann retractors. The resection level is markedusing the resection guide (26-265-05). Thisensures that the head of the prosthesis willlay in the optimum position, 2 mm proximalto the TFCC. The tip of the resection guideis carefully inserted over the distal end of theradius at its extreme ulnar border (Fig. 4).
Level 1 resection is used for the standardprosthesis and is the preferred resection level.
Level 2 may be used when there is insuffi-cient bone stock to allow for seating theprosthesis more distally (e.g. after Bowers’procedure). The standard+ stem should beused at this level in order to ensure opti-mum length of the prosthesis (at 2 mmulnar minus).
Because of the length discrepancy betweenthe three head sizes (+2mm/–2mm) and thelength discrepancy of the standard andstandard+ stem (2 mm) all combinationscan be performed with resection level 1 and2, as shown in table 1.
Level 3 is used only with the revision stem,in case of extreme ulnar shortening (e.g.after previous surgery such as Darrach’s pro-cedure). Resection should be carried out atthe appropriate level, depending on the sizeof head selected.
s: smallm: mediuml: large
The ulnar head is then grasped with the hol-ding forceps and is rotated externally anddistally so that the soft tissue attachmentscan be carefully peeled away using a combi-nation of blunt and sharp dissection. In thisway the attachment of the apex of the TFCCto the underside of the flap will be preserved.If there is an ununited ulnar styloid frag-ment, this may need to be removed sepa-rately and any resulting deficiency carefullyrepaired.
Extensor carpi ulnaris
Extensor digiti minimi
Abb. 4/Fig. 4
Resektions-MessinstrumentResection guide
Tabelle 1: Darstellung der möglichen Kombinationsmöglichkeitenbei unterschiedlichen Resektionsniveaus
Kopf klein mittel groß
Schaft 26-220-01 26-220-03 26-220-05
Standard Niveau 1 Niveau 2
Standard+ Niveau 1 Niveau 2
Table 1: Possibilities of combinations at the different resection levels
Head small medium large
Stem 26-220-01 26-220-03 26-220-05
Standard Level 1 Level 2
Standard+ Level 1 Level 2
11
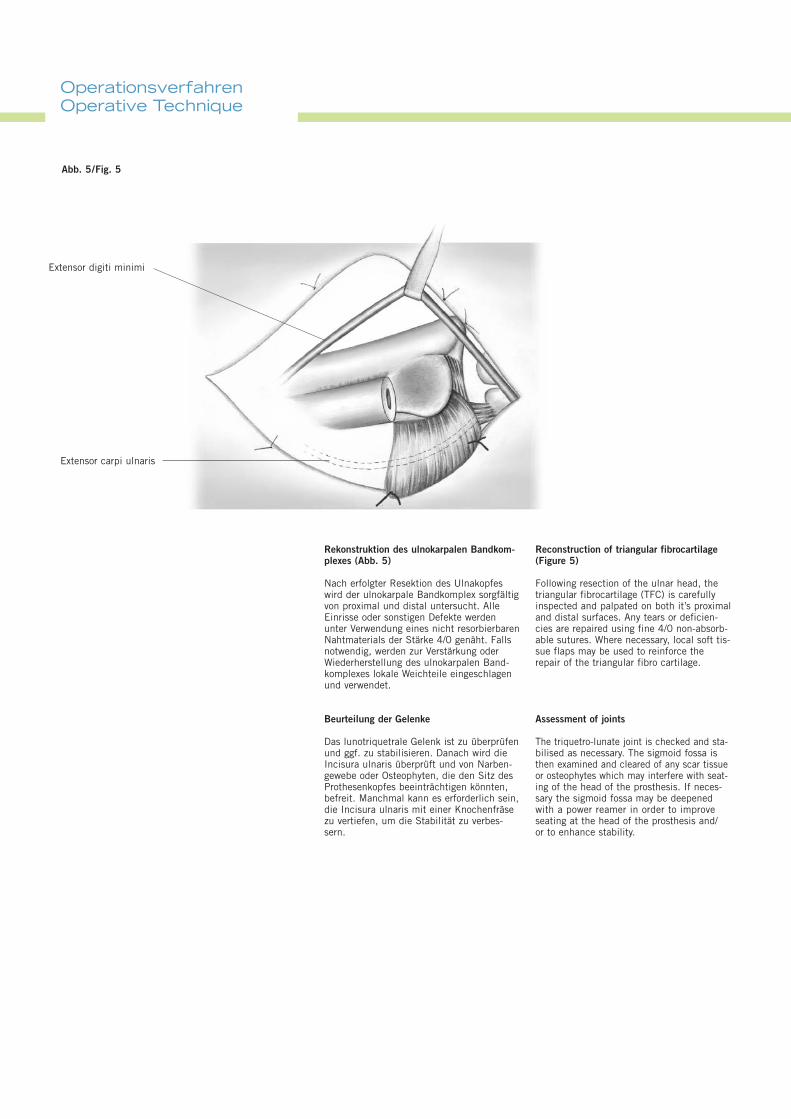
Rekonstruktion des ulnokarpalen Bandkom-plexes (Abb. 5)
Nach erfolgter Resektion des Ulnakopfeswird der ulnokarpale Bandkomplex sorgfältigvon proximal und distal untersucht. AlleEinrisse oder sonstigen Defekte werdenunter Verwendung eines nicht resorbierbarenNahtmaterials der Stärke 4/0 genäht. Fallsnotwendig, werden zur Verstärkung oderWiederherstellung des ulnokarpalen Band-komplexes lokale Weichteile eingeschlagenund verwendet.
Beurteilung der Gelenke
Das lunotriquetrale Gelenk ist zu überprüfenund ggf. zu stabilisieren. Danach wird dieIncisura ulnaris überprüft und von Narben-gewebe oder Osteophyten, die den Sitz desProthesenkopfes beeinträchtigen könnten,befreit. Manchmal kann es erforderlich sein,die Incisura ulnaris mit einer Knochenfräsezu vertiefen, um die Stabilität zu verbes-sern.
Reconstruction of triangular fibrocartilage(Figure 5)
Following resection of the ulnar head, thetriangular fibrocartilage (TFC) is carefullyinspected and palpated on both it’s proximaland distal surfaces. Any tears or deficien-cies are repaired using fine 4/0 non-absorb-able sutures. Where necessary, local soft tis-sue flaps may be used to reinforce therepair of the triangular fibro cartilage.
Assessment of joints
The triquetro-lunate joint is checked and sta-bilised as necessary. The sigmoid fossa isthen examined and cleared of any scar tissueor osteophytes which may interfere with seat-ing of the head of the prosthesis. If neces-sary the sigmoid fossa may be deepenedwith a power reamer in order to improveseating at the head of the prosthesis and/or to enhance stability.
Extensor carpi ulnaris
Abb. 5/Fig. 5
Extensor digiti minimi
OperationsverfahrenOperative Technique
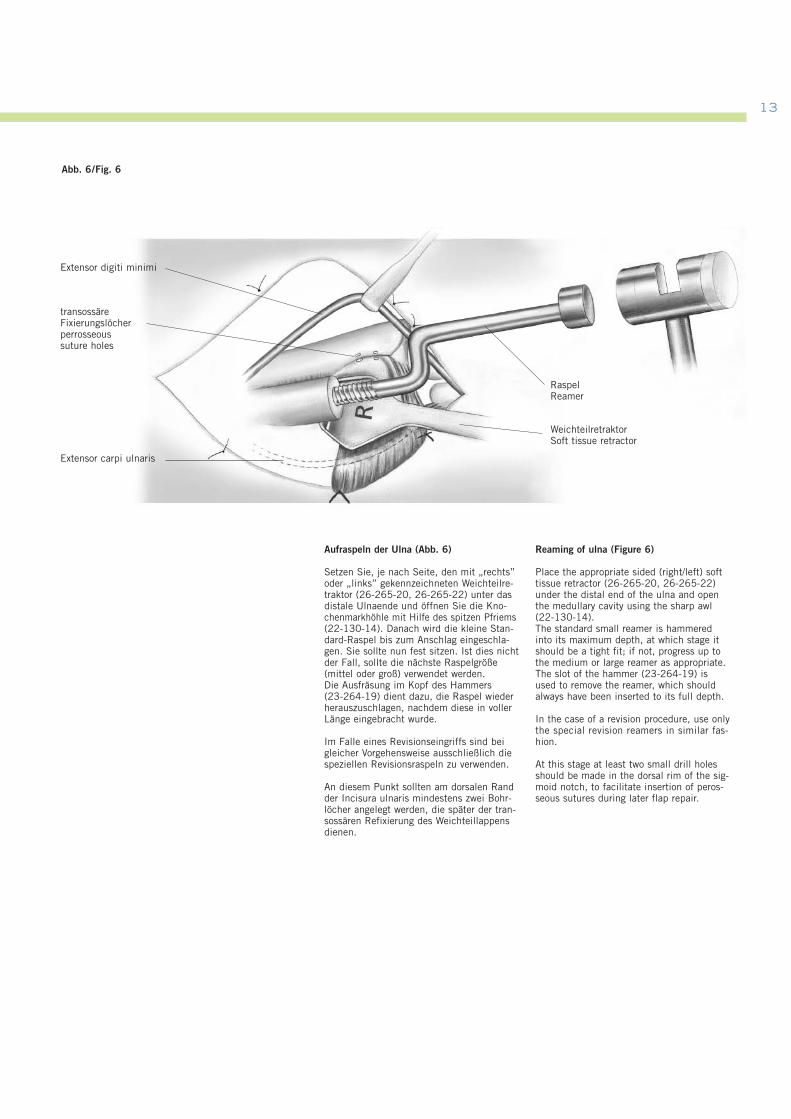
Abb. 6/Fig. 6
transossäreFixierungslöcherperrosseous suture holes
Extensor carpi ulnaris
Extensor digiti minimi
WeichteilretraktorSoft tissue retractor
RaspelReamer
13
Aufraspeln der Ulna (Abb. 6)
Setzen Sie, je nach Seite, den mit „rechts”oder „links” gekennzeichneten Weichteilre-traktor (26-265-20, 26-265-22) unter dasdistale Ulnaende und öffnen Sie die Kno-chenmarkhöhle mit Hilfe des spitzen Pfriems(22-130-14). Danach wird die kleine Stan-dard-Raspel bis zum Anschlag eingeschla-gen. Sie sollte nun fest sitzen. Ist dies nichtder Fall, sollte die nächste Raspelgröße(mittel oder groß) verwendet werden.Die Ausfräsung im Kopf des Hammers (23-264-19) dient dazu, die Raspel wiederherauszuschlagen, nachdem diese in vollerLänge eingebracht wurde.
Im Falle eines Revisionseingriffs sind beigleicher Vorgehensweise ausschließlich diespeziellen Revisionsraspeln zu verwenden.
An diesem Punkt sollten am dorsalen Randder Incisura ulnaris mindestens zwei Bohr-löcher angelegt werden, die später der tran-sossären Refixierung des Weichteillappensdienen.
Reaming of ulna (Figure 6)
Place the appropriate sided (right/left) softtissue retractor (26-265-20, 26-265-22)under the distal end of the ulna and openthe medullary cavity using the sharp awl(22-130-14). The standard small reamer is hammeredinto its maximum depth, at which stage itshould be a tight fit; if not, progress up tothe medium or large reamer as appropriate.The slot of the hammer (23-264-19) isused to remove the reamer, which shouldalways have been inserted to its full depth.
In the case of a revision procedure, use onlythe special revision reamers in similar fas-hion.
At this stage at least two small drill holesshould be made in the dorsal rim of the sig-moid notch, to facilitate insertion of peros-seous sutures during later flap repair.

Reposition der Probeprothese undBeurteilung
Setzen Sie den geeigneten Probeschaft und -kopf ein. PrüfenSie, ob der Schaft gut sitzt und der Kopf sich in korrekterPosition (etwa 2 mm unterhalb des ulnokarpalen Band-komplexes) befindet. Diese Überprüfung sollte radiologischunter Verwendung des Bildwandlers bei maximaler Pronationdes Handgelenkes verifiziert werden.
Führen Sie dann den Weichteillappen radial über den Ulna-kopf, um zu prüfen, ob er zum einen wieder gut am Radiusbefestigt werden kann und zum anderen für genügend Sta-bilität sorgt. Erscheint der Lappen zu straff, sollte der kleine Kopf auspro-biert werden. Bei Verwendung des kleinen Kopfes muss derStandard-Schaft gegen einen Standard+-Schaft ausgetauschtwerden, damit die Länge der Prothese wieder stimmt.Erscheint der Lappen hingegen zu locker, sollte der großeKopf verwendet werden. In diesem Fall muss dann die Ulnaauf Niveau 2 verkürzt werden, damit eine optimale Prothesen-länge garantiert ist (2 mm Ulnar-minus).
Nun ist die Unterarmrotation zu überprüfen. Findet sicheine Limitierung, muss die Ursache analysiert und beseitigtwerden (z.B. Blockierung durch Osteophyten, kontrakteMembrana interossea, etc.).
Die Probeprothese wird nun, ggf. unter Zuhilfenahme des Explantationsmeißels (26-265-35, 26-265-37) entferntund die Wunde und der Knochenmarkkanal gut gespült.
Einbringen der endgültigen Prothese
Nach Auswahl der geeigneten Schaft- (Standard, Standard+oder Revision) und Kopfgröße (klein, mittel oder groß) wirdnun der Schaft mit Hilfe des konischen Einschlaginstrumen-tariums (26-265-30) vorsichtig eingebracht. Das konischeEnde des Prothesenhalses sollte sauber und trocken sein,bevor der Keramikkopf durch einen leichten Schlag ange-bracht wird.
An diesem Punkt der Operation ist dann anhand von Röntgen-aufnahmen sicherzustellen, dass die Prothese optimal sitzt.
Warnung:Beim Einschlagen der Prothese sollte niemals übermäßigeKraft angewendet werden. Wenn der Schaft beim Einschla-gen zu klemmen scheint, sollte er noch einmal entferntund der Markraum der Ulna weiter aufgeraspelt werden.
Entfernen der Prothese
Falls die Prothese in Sonderfällen noch einmal herausge-nommen werden muss, kann dazu der im Operationsset vor-handene Schaftextraktor (26-265-07) verwendet werden.
Trial reduction and assessment
Insert the appropriate trial stem and head. Check that thestem fits snugly and that the head lies at the appropriatelevel (approx. 2 mm) below the TFCC. This should be checkedfluorescopically with the wrist in full pronation.
Advance the flap radially over the ulnar head to check thatthis can be re-attached to the radius and provide adequatestability. If the flap is too tight, a smaller head should be tried. Ifthis is selected, then the standard stem should be changedto a standard+ stem in order to ensure optimum length ofthe prosthesis.If the flap is too loose, a larger head may be selected. Inthis case, the ulna must be shortened back to level 2 inorder to ensure optimum length of the prosthesis (2 mmulnar minus).
Range of forearm rotation is assessed at this stage, and if itremains limited, the cause should be sought and dealt withas appropriate (e.g. osteophyte block; contracture of intero-sseous membrane, etc.).
The trial prosthesis is removed, using the explantation chisels(26-265-35, 26-265-37) and the wound and medullary canalare irrigated.
Inserting the definitive prosthesis
The appropriate stem (standard, standard+ or revision) andhead (small, medium or large) are selected. The stem iscarefully hammered into position using the conical impactor(26-265-30). The conical end of the stem should be cleanand dry before the ceramic head is impacted.
At this stage, intra-operative x-rays are used to confirm thatthe prosthesis is in optimum position.
Warning:Excessive force should never be used during insertion ofthe definitive prosthesis. If the stem appears to “lock”during insertion, it should be removed and further reamingcarried out.
Removal of prosthesis
If for any reason it is necessary to remove the prosthesis,this can be done using the stem extractor (26-265-07)provided in the set.
OperationsverfahrenOperative Technique
15
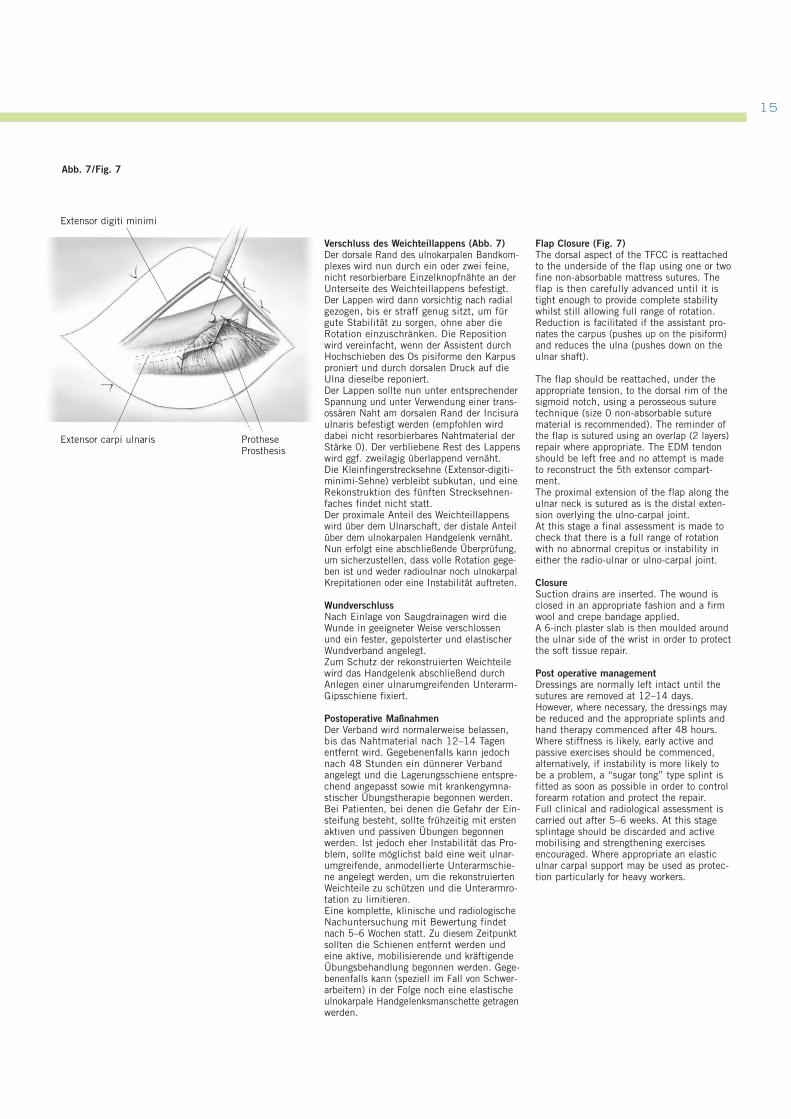
Verschluss des Weichteillappens (Abb. 7)Der dorsale Rand des ulnokarpalen Bandkom-plexes wird nun durch ein oder zwei feine,nicht resorbierbare Einzelknopfnähte an derUnterseite des Weichteillappens befestigt.Der Lappen wird dann vorsichtig nach radialgezogen, bis er straff genug sitzt, um fürgute Stabilität zu sorgen, ohne aber dieRotation einzuschränken. Die Repositionwird vereinfacht, wenn der Assistent durchHochschieben des Os pisiforme den Karpusproniert und durch dorsalen Druck auf dieUlna dieselbe reponiert.Der Lappen sollte nun unter entsprechenderSpannung und unter Verwendung einer trans-ossären Naht am dorsalen Rand der Incisuraulnaris befestigt werden (empfohlen wirddabei nicht resorbierbares Nahtmaterial derStärke 0). Der verbliebene Rest des Lappenswird ggf. zweilagig überlappend vernäht. Die Kleinfingerstrecksehne (Extensor-digiti-minimi-Sehne) verbleibt subkutan, und eineRekonstruktion des fünften Strecksehnen-faches findet nicht statt. Der proximale Anteil des Weichteillappenswird über dem Ulnarschaft, der distale Anteilüber dem ulnokarpalen Handgelenk vernäht.Nun erfolgt eine abschließende Überprüfung,um sicherzustellen, dass volle Rotation gege-ben ist und weder radioulnar noch ulnokarpalKrepitationen oder eine Instabilität auftreten.
WundverschlussNach Einlage von Saugdrainagen wird dieWunde in geeigneter Weise verschlossenund ein fester, gepolsterter und elastischerWundverband angelegt.Zum Schutz der rekonstruierten Weichteilewird das Handgelenk abschließend durchAnlegen einer ulnarumgreifenden Unterarm-Gipsschiene fixiert.
Postoperative MaßnahmenDer Verband wird normalerweise belassen,bis das Nahtmaterial nach 12–14 Tagenentfernt wird. Gegebenenfalls kann jedochnach 48 Stunden ein dünnerer Verbandangelegt und die Lagerungsschiene entspre-chend angepasst sowie mit krankengymna-stischer Übungstherapie begonnen werden.Bei Patienten, bei denen die Gefahr der Ein-steifung besteht, sollte frühzeitig mit erstenaktiven und passiven Übungen begonnenwerden. Ist jedoch eher Instabilität das Pro-blem, sollte möglichst bald eine weit ulnar-umgreifende, anmodellierte Unterarmschie-ne angelegt werden, um die rekonstruiertenWeichteile zu schützen und die Unterarmro-tation zu limitieren.Eine komplette, klinische und radiologischeNachuntersuchung mit Bewertung findetnach 5–6 Wochen statt. Zu diesem Zeitpunktsollten die Schienen entfernt werden undeine aktive, mobilisierende und kräftigendeÜbungsbehandlung begonnen werden. Gege-benenfalls kann (speziell im Fall von Schwer-arbeitern) in der Folge noch eine elastischeulnokarpale Handgelenksmanschette getragenwerden.
Flap Closure (Fig. 7)The dorsal aspect of the TFCC is reattachedto the underside of the flap using one or twofine non-absorbable mattress sutures. Theflap is then carefully advanced until it istight enough to provide complete stabilitywhilst still allowing full range of rotation.Reduction is facilitated if the assistant pro-nates the carpus (pushes up on the pisiform)and reduces the ulna (pushes down on theulnar shaft).
The flap should be reattached, under theappropriate tension, to the dorsal rim of thesigmoid notch, using a perosseous suturetechnique (size 0 non-absorbable suturematerial is recommended). The reminder ofthe flap is sutured using an overlap (2 layers)repair where appropriate. The EDM tendonshould be left free and no attempt is madeto reconstruct the 5th extensor compart-ment.The proximal extension of the flap along theulnar neck is sutured as is the distal exten-sion overlying the ulno-carpal joint.At this stage a final assessment is made tocheck that there is a full range of rotationwith no abnormal crepitus or instability ineither the radio-ulnar or ulno-carpal joint.
ClosureSuction drains are inserted. The wound isclosed in an appropriate fashion and a firmwool and crepe bandage applied.A 6-inch plaster slab is then moulded aroundthe ulnar side of the wrist in order to protectthe soft tissue repair.
Post operative managementDressings are normally left intact until thesutures are removed at 12–14 days.However, where necessary, the dressings maybe reduced and the appropriate splints andhand therapy commenced after 48 hours.Where stiffness is likely, early active andpassive exercises should be commenced,alternatively, if instability is more likely tobe a problem, a “sugar tong” type splint isfitted as soon as possible in order to controlforearm rotation and protect the repair.Full clinical and radiological assessment iscarried out after 5–6 weeks. At this stagesplintage should be discarded and activemobilising and strengthening exercisesencouraged. Where appropriate an elasticulnar carpal support may be used as protec-tion particularly for heavy workers.
Extensor carpi ulnaris
Extensor digiti minimi
Abb. 7/Fig. 7
ProtheseProsthesis
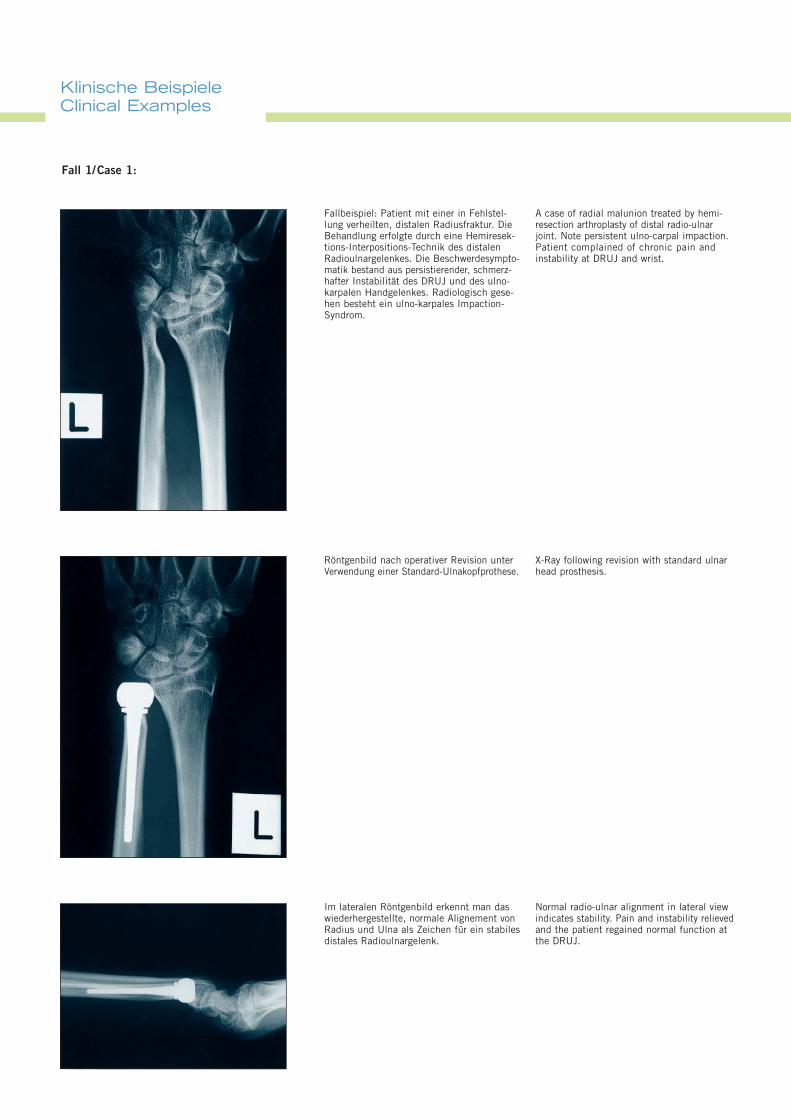
Fallbeispiel: Patient mit einer in Fehlstel-lung verheilten, distalen Radiusfraktur. DieBehandlung erfolgte durch eine Hemiresek-tions-Interpositions-Technik des distalenRadioulnargelenkes. Die Beschwerdesympto-matik bestand aus persistierender, schmerz-hafter Instabilität des DRUJ und des ulno-karpalen Handgelenkes. Radiologisch gese-hen besteht ein ulno-karpales Impaction-Syndrom.
Röntgenbild nach operativer Revision unterVerwendung einer Standard-Ulnakopfprothese.
Klinische BeispieleClinical Examples
Fall 1/Case 1:
Im lateralen Röntgenbild erkennt man daswiederhergestellte, normale Alignement vonRadius und Ulna als Zeichen für ein stabilesdistales Radioulnargelenk.
A case of radial malunion treated by hemi-resection arthroplasty of distal radio-ulnarjoint. Note persistent ulno-carpal impaction.Patient complained of chronic pain andinstability at DRUJ and wrist.
X-Ray following revision with standard ulnar head prosthesis.
Normal radio-ulnar alignment in lateral viewindicates stability. Pain and instability relievedand the patient regained normal function atthe DRUJ.
17
Fall 2 /Case 2:
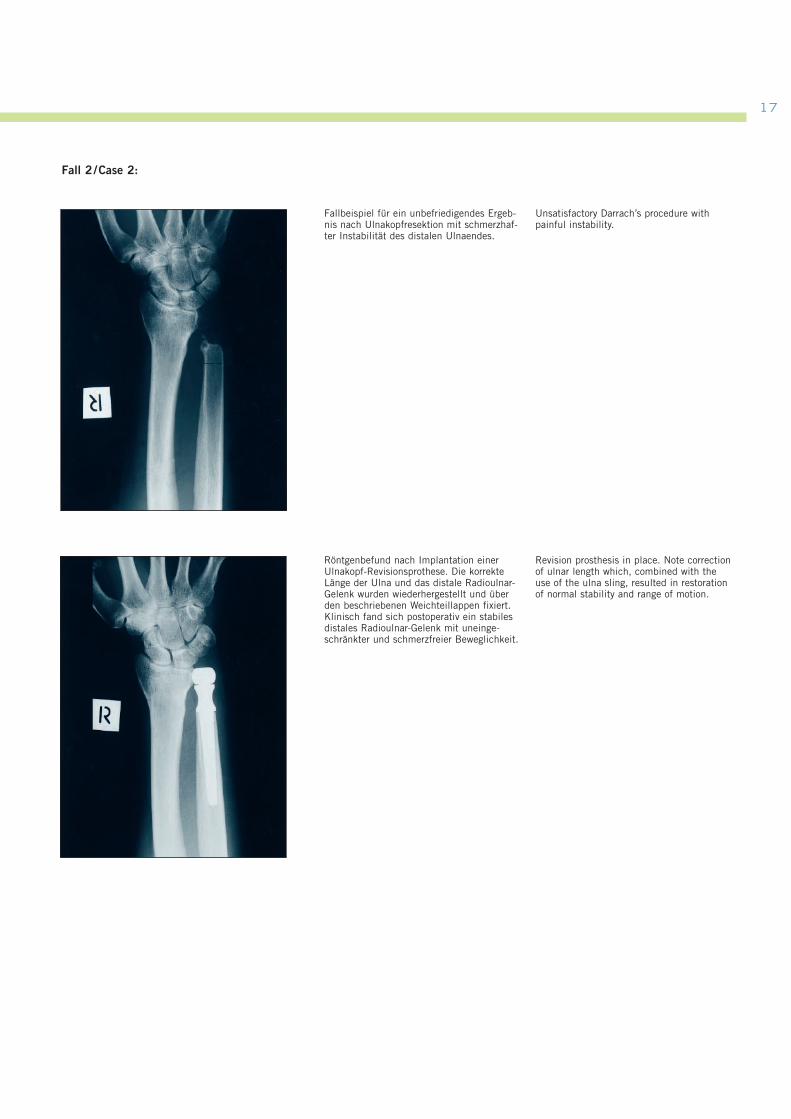
Fallbeispiel für ein unbefriedigendes Ergeb-nis nach Ulnakopfresektion mit schmerzhaf-ter Instabilität des distalen Ulnaendes.
Röntgenbefund nach Implantation einerUlnakopf-Revisionsprothese. Die korrekteLänge der Ulna und das distale Radioulnar-Gelenk wurden wiederhergestellt und überden beschriebenen Weichteillappen fixiert.Klinisch fand sich postoperativ ein stabilesdistales Radioulnar-Gelenk mit uneinge-schränkter und schmerzfreier Beweglichkeit.
Unsatisfactory Darrach’s procedure withpainful instability.
Revision prosthesis in place. Note correctionof ulnar length which, combined with theuse of the ulna sling, resulted in restorationof normal stability and range of motion.
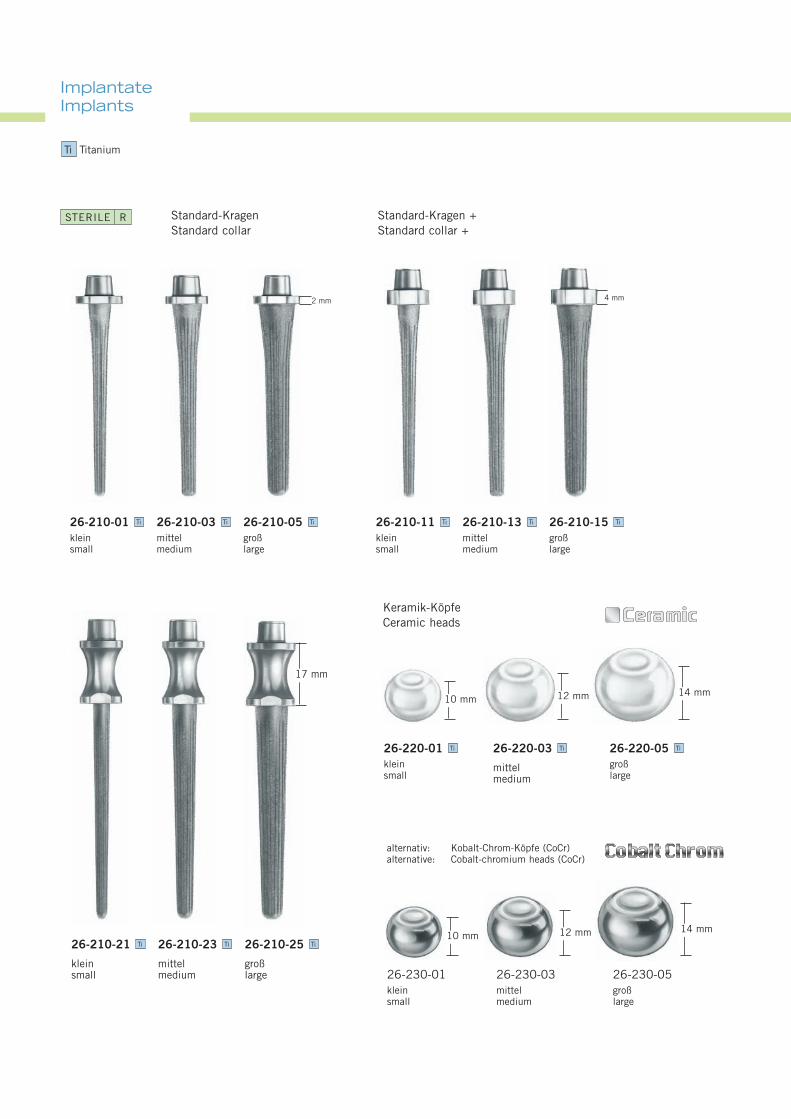
ImplantateImplants
10 mm 12 mm 14 mm
Keramik-KöpfeCeramic heads
26-210-21
kleinsmall
Ti 26-210-23
mittelmedium
Ti 26-210-25
großlarge
Ti
26-220-01kleinsmall
Ti 26-220-03
mittelmedium
Ti 26-220-05großlarge
Ti
17 mm
10 mm 12 mm 14 mm
26-210-01kleinsmall
Ti 26-210-03mittelmedium
Ti 26-210-05großlarge
Ti 26-210-11kleinsmall
Ti 26-210-13mittelmedium
Ti 26-210-15großlarge
Ti
2 mm 4 mm
Standard-KragenStandard collar
Standard-Kragen +Standard collar +
alternativ: Kobalt-Chrom-Köpfe (CoCr)alternative: Cobalt-chromium heads (CoCr)
26-230-01kleinsmall
26-230-03mittelmedium
26-230-05großlarge
Ti Titanium
STERILE R
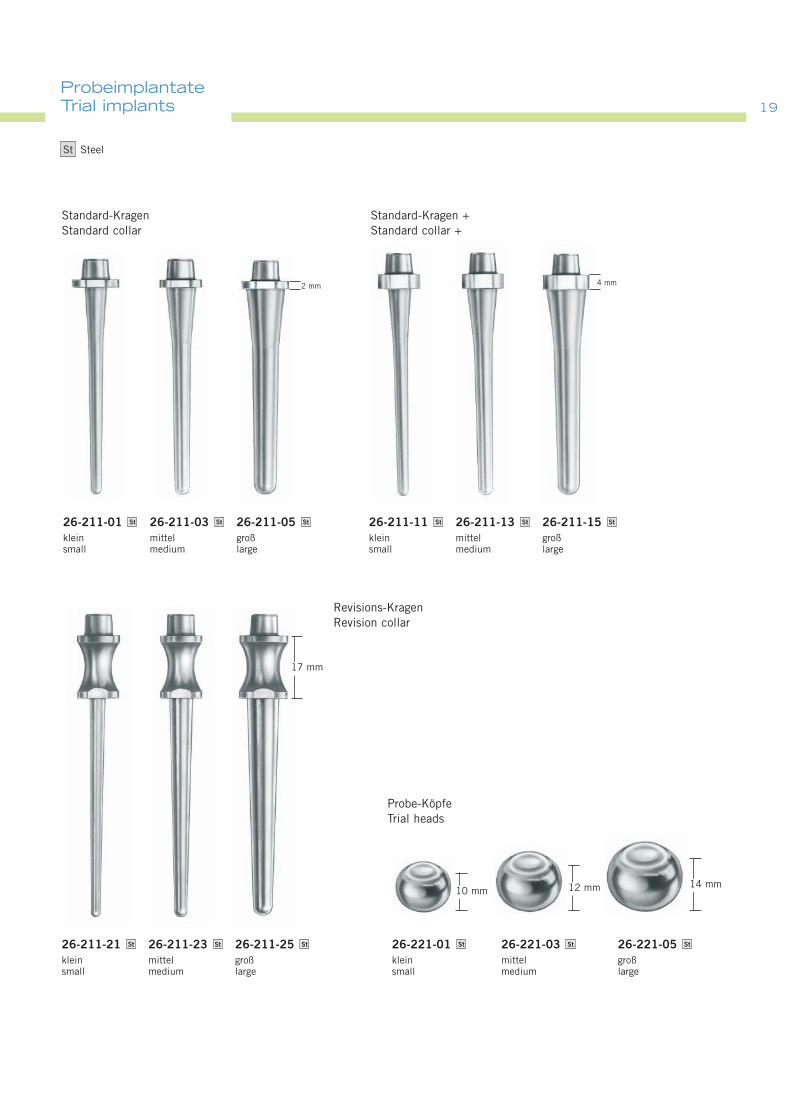
1919ProbeimplantateTrial implants
Probe-KöpfeTrial heads
26-211-21kleinsmall
St 26-211-23mittelmedium
St 26-211-25großlarge
St 26-221-01kleinsmall
St 26-221-03mittelmedium
St 26-221-05großlarge
St
10 mm 12 mm 14 mm
17 mm
Revisions-KragenRevision collar
26-211-01kleinsmall
St 26-211-03mittelmedium
St 26-211-05großlarge
St 26-211-11kleinsmall
St 26-211-13mittelmedium
St 26-211-15großlarge
St
2 mm 4 mm
Standard-KragenStandard collar
Standard-Kragen +Standard collar +
St Steel
1⁄2
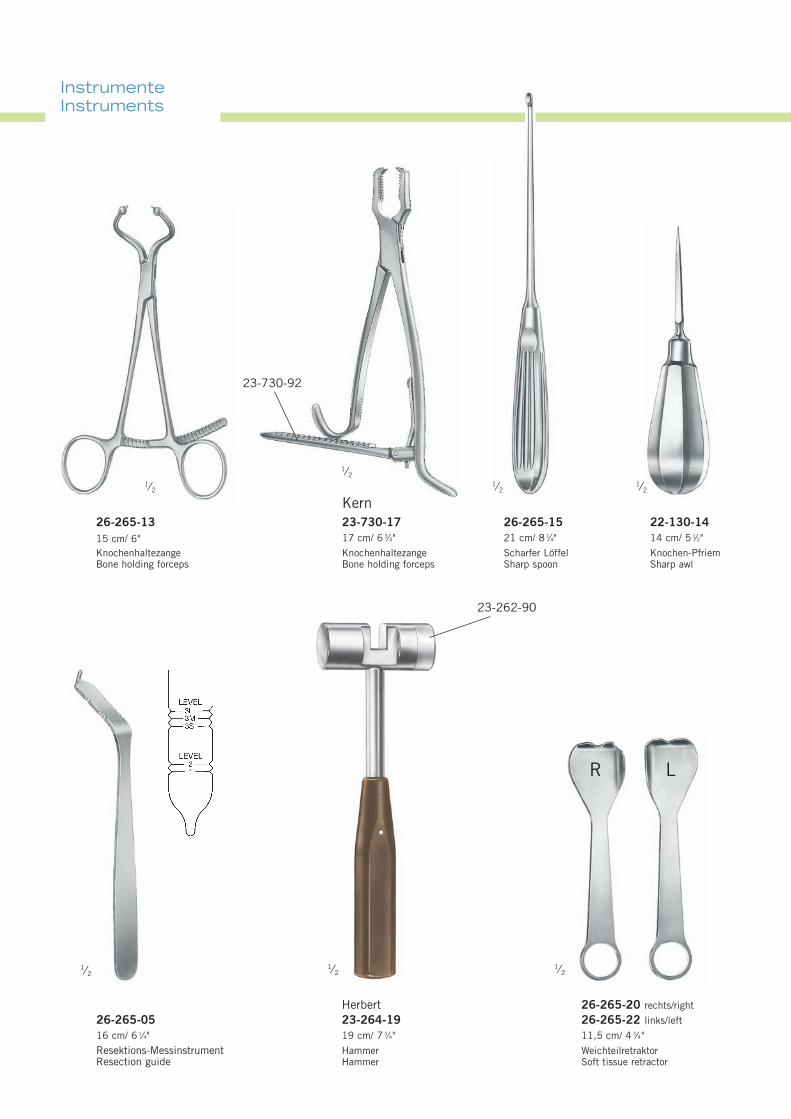
Herbert23-264-1919 cm/ 7 3⁄4"
HammerHammer
InstrumenteInstruments
1⁄2
22-130-1414 cm/ 5 1⁄2"
Knochen-PfriemSharp awl
1⁄2
Kern23-730-1717 cm/ 6 3⁄4"
KnochenhaltezangeBone holding forceps
23-730-92
1⁄2
26-265-0516 cm/ 6 1⁄4"
Resektions-MessinstrumentResection guide
26-265-1315 cm/ 6"KnochenhaltezangeBone holding forceps
1⁄2 1⁄2
26-265-1521 cm/ 8 1⁄4"
Scharfer LöffelSharp spoon
1⁄2
26-265-20 rechts/right
26-265-22 links/left
11,5 cm/ 4 3⁄4"
WeichteilretraktorSoft tissue retractor
R L
23-262-90
2121
1⁄2 1⁄2
1⁄2
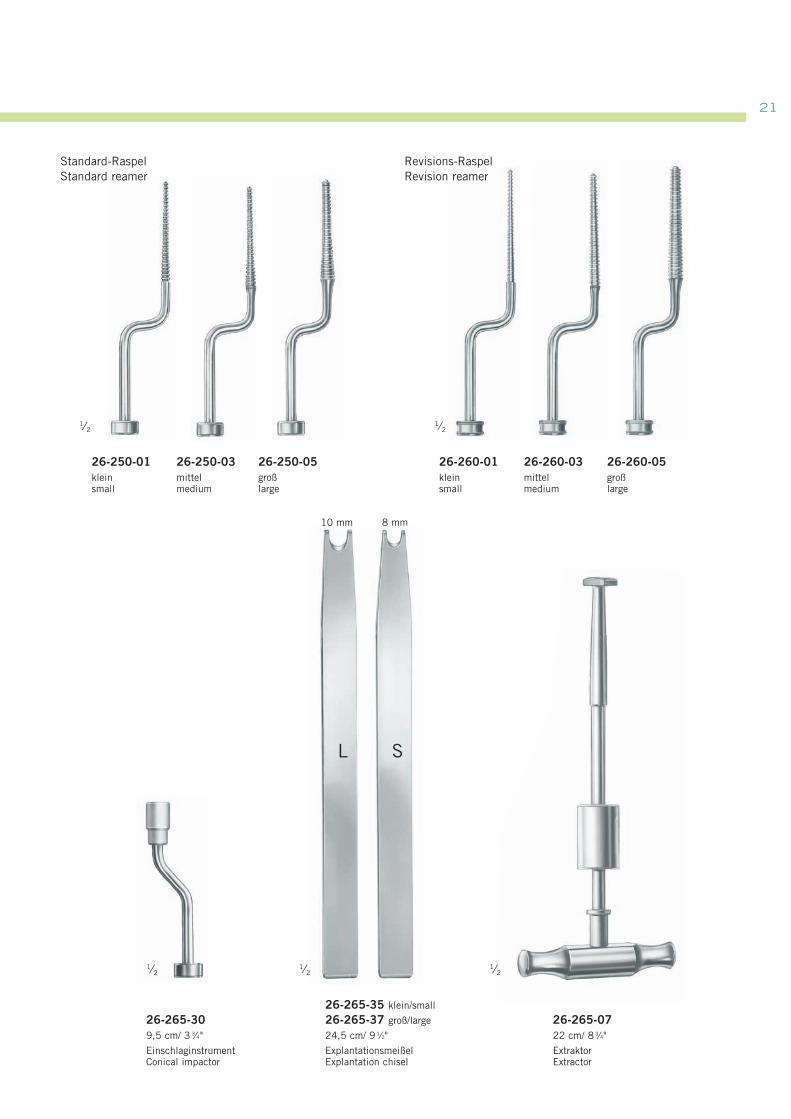
26-265-0722 cm/ 8 3⁄4"
ExtraktorExtractor
Standard-RaspelStandard reamer
Revisions-RaspelRevision reamer
26-250-01kleinsmall
26-250-05großlarge
26-250-03mittelmedium
26-260-01kleinsmall
26-260-05großlarge
26-260-03mittelmedium
1⁄2
26-265-309,5 cm/ 3 3⁄4"
EinschlaginstrumentConical impactor
1⁄2
8 mm10 mm
L S
26-265-35 klein/small
26-265-37 groß/large
24,5 cm/ 9 1⁄2"
ExplantationsmeißelExplantation chisel

SatzzusammenstellungSet Recommendation
Probe-Implantate1 x 26-211-01 Probe-Standard-Schaft, klein1 x 26-211-03 Probe-Standard-Schaft, mittel1 x 26-211-05 Probe-Standard-Schaft, groß1 x 26-211-11 Probe-Standard+-Schaft, klein1 x 26-211-13 Probe-Standard+-Schaft, mittel1 x 26-211-15 Probe-Standard+-Schaft, groß1 x 26-211-21 Probe-Revisions-Schaft, klein1 x 26-211-23 Probe-Revisions-Schaft, mittel1 x 26-211-25 Probe-Revisions-Schaft, groß1 x 26-221-01 Probe-Prothesenkopf Metall, klein1 x 26-221-03 Probe-Prothesenkopf Metall, mittel1 x 26-221-05 Probe-Prothesenkopf Metall, groß
Instrumente1 x 22-130-14 Knochen-Pfriem1 x 23-264-19 Herbert-Hammer1 x 23-730-17 Knochen-Haltezange1 x 26-265-13 Knochen-Haltezange1 x 26-250-01 Standard-Raspel, klein1 x 26-250-03 Standard-Raspel, mittel1 x 26-250-05 Standard-Raspel, groß1 x 26-260-01 Revisions-Raspel, klein1 x 26-260-03 Revisions-Raspel, mittel1 x 26-260-05 Revisions-Raspel, groß1 x 26-265-05 Resektionsmessinstrument1 x 26-265-07 Extraktor1 x 26-265-15 Scharfer Löffel1 x 26-265-20 Weichteilretraktor, rechts1 x 26-265-22 Weichteilretraktor, links1 x 26-265-30 Einschlaginstrument1 x 26-265-35 Explantationsmeißel, klein1 x 26-265-37 Explantationsmeißel, groß
Lagerung1 x 55-864-01 Codierschild mit Beschriftung, ohne Loch1 x 55-864-13 Logistik-Rähmchen, blau1 x 55-869-13 Container 140 x 300 x 600 mm1 x 55-910-16 Revisions-Implantate-Rack1 x 55-910-17 Standard-Implantate-Rack1 x 55-910-18 Instrumenten-Rack1 x 90-666-52 Röntgen-Schablone Standard1 x 90-667-52 Röntgen-Schablone Standard+1 x 90-668-52 Röntgen-Schablone Revision
26-200-00 Set
Trial Implants1 x 26-211-01 Trial standard stem, small1 x 26-211-03 Trial standard stem, medium1 x 26-211-05 Trial standard stem, large1 x 26-211-11 Trial standard+ stem, small1 x 26-211-13 Trial standard+ stem, medium1 x 26-211-15 Trial standard+ stem, large1 x 26-211-21 Trial revision stem, small1 x 26-211-23 Trial revision stem, medium1 x 26-211-25 Trial revision stem, large1 x 26-221-01 Trial metallic head, small1 x 26-221-03 Trial metallic head, medium1 x 26-221-05 Trial metallic head, large
Instruments1 x 22-130-14 Sharp awl1 x 23-264-19 Herbert hammer1 x 23-730-17 Bone holding forceps1 x 26-265-13 Bone holding forceps1 x 26-250-01 Standard reamer, small1 x 26-250-03 Standard reamer, medium1 x 26-250-05 Standard reamer, large1 x 26-260-01 Revision reamer, small1 x 26-260-03 Revision reamer, medium1 x 26-260-05 Revision reamer, large1 x 26-265-05 Resection guide1 x 26-265-07 Extractor1 x 26-265-15 Sharp spoon1 x 26-265-20 Soft tissue retractor, right1 x 26-265-22 Soft tissue retractor, left1 x 26-265-30 Cone impactor1 x 26-265-35 Explantation chisel, small1 x 26-265-37 Explantation chisel, large
Storage1 x 55-864-01 Coding labels lettered, no hole1 x 55-864-13 Logistic framelets, blue1 x 55-869-13 Container 140 x 300 x 600 mm1 x 55-910-16 Sterilisation tray for trial revision implants1 x 55-910-17 Sterilisation tray for trial standard implants 1 x 55-910-18 Sterilisation tray for instruments 1 x 90-666-52 X-Ray template Standard1 x 90-667-52 X-Ray template Standard+1 x 90-668-52 X-Ray template Revision
26-200-00 Set
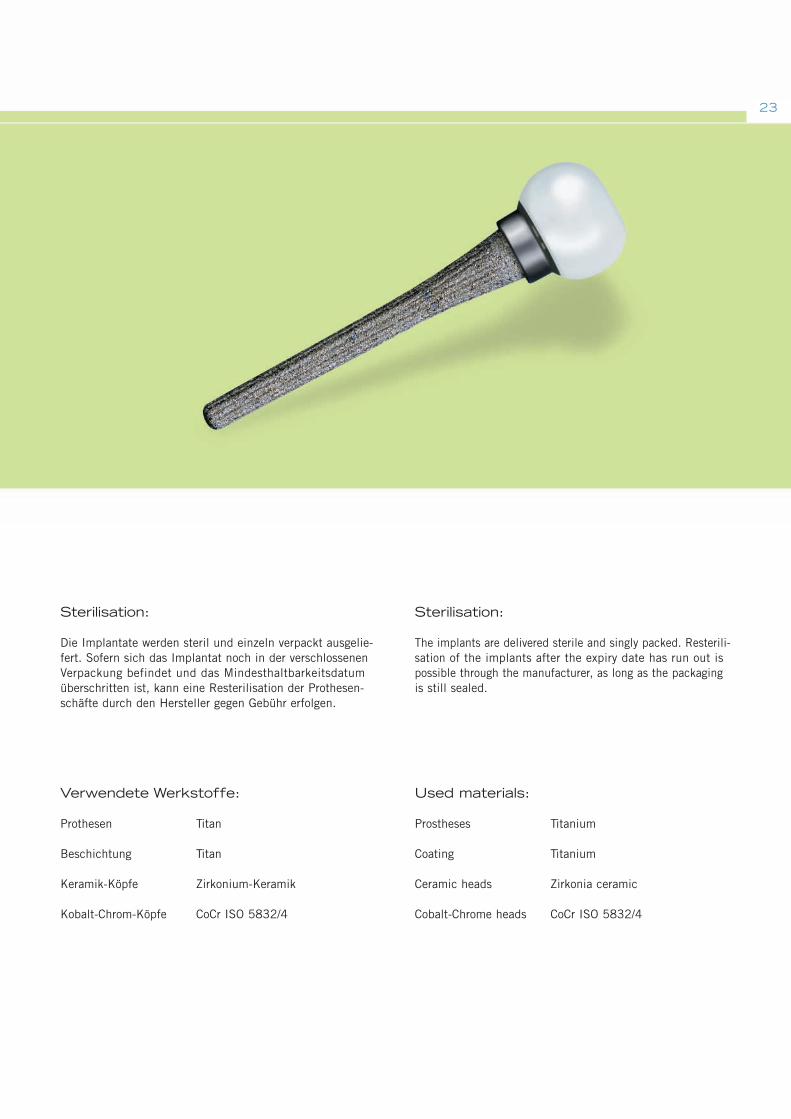
Sterilisation:
Die Implantate werden steril und einzeln verpackt ausgelie-fert. Sofern sich das Implantat noch in der verschlossenenVerpackung befindet und das Mindesthaltbarkeitsdatumüberschritten ist, kann eine Resterilisation der Prothesen-schäfte durch den Hersteller gegen Gebühr erfolgen.
Verwendete Werkstoffe:
Prothesen Titan
Beschichtung Titan
Keramik-Köpfe Zirkonium-Keramik
Kobalt-Chrom-Köpfe CoCr ISO 5832/4
Sterilisation:
The implants are delivered sterile and singly packed. Resterili-sation of the implants after the expiry date has run out ispossible through the manufacturer, as long as the packagingis still sealed.
Used materials:
Prostheses Titanium
Coating Titanium
Ceramic heads Zirkonia ceramic
Cobalt-Chrome heads CoCr ISO 5832/4
23
05.07 . 90-665-16-05 . Printed in Germany · Copyright by Gebrüder Martin GmbH & Co. KG · Alle Rechte vorbehalten · Technische Änderungen vorbehaltenWe reserve the right to make alterations · Cambios técnicos reservados · Sous réserve de modifications techniques · Ci riserviamo il diritto di modifiche tecniche
Gebrüder Martin GmbH & Co. KGA company of the KLS Martin GroupLudwigstaler Str. 132 · D-78532 TuttlingenPostfach 60 · D-78501 TuttlingenTel. +49 7461 706-0 · Fax +49 7461 [email protected] · www.klsmartin.com
KLS Martin Subsidiaries
KLS Martin France SARL 3, Rue Gambetta 68000 Colmar France Tel. +33 3 89 21 6601 Fax +33 3 89 23 6514 [email protected]
Martin Italia S.r.l.Via Paracelso, 18Palazzo Andromeda, Ingresso 2 20041 Agrate Brianza (Mi) ItalyTel. +39 039 605 6731 Fax +39 039 605 [email protected]
Martin Nederland/Marned B.V.Vissersstraat 9a1271 VE HuizenP.O. Box 2781270 AG HuizenThe NetherlandsTel. +31 35 523 45 38Fax +31 35 523 53 [email protected]
Nippon Martin K.K.6 Fl., 4-6-16 Hiranomachi541-0046 Chuo-ku,Osaka 541-0046JapanTel. +81 6 62 28 9075Fax +81 6 62 28 [email protected]
Orthosurgical Implants Inc. 12244 SW 130 Street Miami, Fl 33186USAOffice phone +1 305 969 45 45Office fax +1 305 969 45 46Toll free +1 888 305 45 [email protected] www.orthosurgical.com
KLS Martin L.P.11239-1 St. John`s Industrial Parkway SouthJacksonville, Fl 32246USAOffice phone +1 904 641 7746Office fax +1 904 641 7378Toll free +1 800 625 [email protected] www.klsmartinusa.com