Embed Size (px)
Citation preview

New Orleans, LA3/29/2018
Understanding Different Modalities (SSEP, MEP, EMG)
What They Mean, How They are Obtained
Wellington K. Hsu, MD
Clifford C. Raisbeck Distinguished Professor of Orthopaedic SurgeryDirector of Research
Department of Orthopaedic SurgeryDepartment of Neurological Surgery
Northwestern University Feinberg School of Medicine

St. Louis, MO
Wellington K. Hsu, MD
Clifford C. Raisbeck Distinguished Professor of Orthopaedic SurgeryDirector of Research, NMH Musculoskeletal Institute
Department of Orthopaedic SurgeryNorthwestern University Feinberg School of Medicine
Disclosures3/29/2018

Intraoperative Neuromonitoring (IOM)
• Goals – Identify emerging insult to
nervous system structures– Provide real-time feedback
before irreversible injury– Allow action that can be
used to reverse the insult – Monitor the efficacy of
interventional strategies
SSEP MEP
EMG

Intraoperative Neuromonitoring (IOM)
SSEP
MEP
EMG
• Somatosensory Evoked Potentials• Dorsal medial spinal tracts
• Motor Evoked Potentials• Corticospinal motor tracts
• Electromyography• Individual nerve roots

Surgeon
Anesthesia
IONM tech
IONM M.D.
Scrub tech Circulator

Neurologic insult• Mechanical
– Direct injury (contusion)– Distortion forces (corrective forces to
spinal column)– Patient positioning
• Nerve root injury• Brachial plexopathy• Quadriplegia
• Ischemia– Stretching of vascular supply– Prolonged hypotension– Ligation of anterior segmental artery

SSEP• 1st NM technique to be
developed (25 yr)• Generated by repetitive
stimulation of a peripheral mixed nerve (e.g., tibial, peroneal, ulnar/median nerve)– Signal-averages,
continuous monitoring• Recording electrodes
placed at levels cephalad to the operative level
• The more recording sites (redundant), the more reliable the monitoring
– Owen et al:Spine 20 :34-43,1995

SSEP• Delay > 1 minute while
SSEP response is averaged from background physiologic noise
• Helpful to detect sensory deficit
– Reported 100% accuracy• Not helpful for motor deficit
– 31% positive predictive value– Lags behind 16 min
(Hilibrand)• Better efficacy
– Mechanical > Ischemic• Does not assess anterior
SC

Mitigating Factors – SSEP• Anesthetics (N20, foranes, propofol) inhibit
SSEP• Etomidate may enhance SSEP• Narcotics, benzodiazepines: little or no effect• Poorly defined in
– Severe myelopathy– Spinal cord tumor– Obesity– Peripheral neuropathy

MEP• Transcranial
application of high-voltage electrical stimulus
• Stimulation sites: motor cortex or spinal cord– Electrodes placed
over scalp regions• Electrical > Magnetic
stimulation• Recording site:
– Myogenic (CMAP) recorded at muscle sites distal to the surgical level
– Neurogenic (NMEP) mixed peripheral nerve

MEP• Can have varying
degrees of variability
• Nl fluctuations of amplitude and morphology
• Most sensitive and specific for diagnosing impending SCI
• Quicker response• More technically
demanding• Affected by
Anesthetics, BP, Temp, Lytes, Meds, Equipment

Neuromonitoring principles• Evaluation
– Amplitude (voltage)– Latency (time)– Morphology (shape)
• Injury leads to a voltage drop not increased latency– Sustaining SCI without amplitude
change is unlikely
• Latency can shift with increased concentration of inhalational agents, lowering of core body temp, hypercarbia

Neuromonitoring principles• Spinal cord contusion
– Amplitude suppression (50-75%) SSEP/MEP
– Resolves 15-20 minutes– Serious injury obliterates all
signals• Ischemia
– Sensory and Motor pathways physically separate vascular supplies
– Possible to have selective loss (SSEP vs. MEP)
– MEP especially sensitive to BP changes – can be used to titrate ideal BP

Neuromonitoring principles• Positive event
– 10% increase in latency
– 50% decrease in amplitude
• > 50% loss SSEP• > 65% loss MEP
• Baseline readings critical to defining positive event

EMG• Spinal nerve root trauma
provokes ion depolarization– Recorded from muscle
innervated by nerve root• Mechanical elicitation
– Free-running EMG– For dynamic phases of
surgery (implant placement, nerve root manipulation)
• Electrical elicitation– Stimulus-evoked or
triggered EMG– Static phases (pedicle
screw stimulation)

EMG• Chronically compressed
motor nerve roots have elevated thresholds and may not fire spontaneously– False-negative result
• Baseline is no activity• Brief irritation
– Irrigation– Electrocautery– Gelfoam
• Sustained irritation– EMG train activity– Traction/pressure on nerve
root– More potential for injury

Anesthetic principles
• Inhalational agents– Reduce cortical SSEP– Reduce MEP
• Prolonged propofol– Reduce MEP signals
• Neuromuscular blockade negatively affects:– EMG– MEP
• Total intravenous anesthetic protocol
• Avoid prolonged propofol
• Avoid paralytic agents
FACT RESULT

T4 disappears with 75% blockade - 3/4 response
T3 with 80%, blockade - 2/4 response
T2 with 90% blockade - 1/4 response
T1 disappears with 100% blockade – 0/4 response
blockade
18
Train of 4 – tested with foot muscles
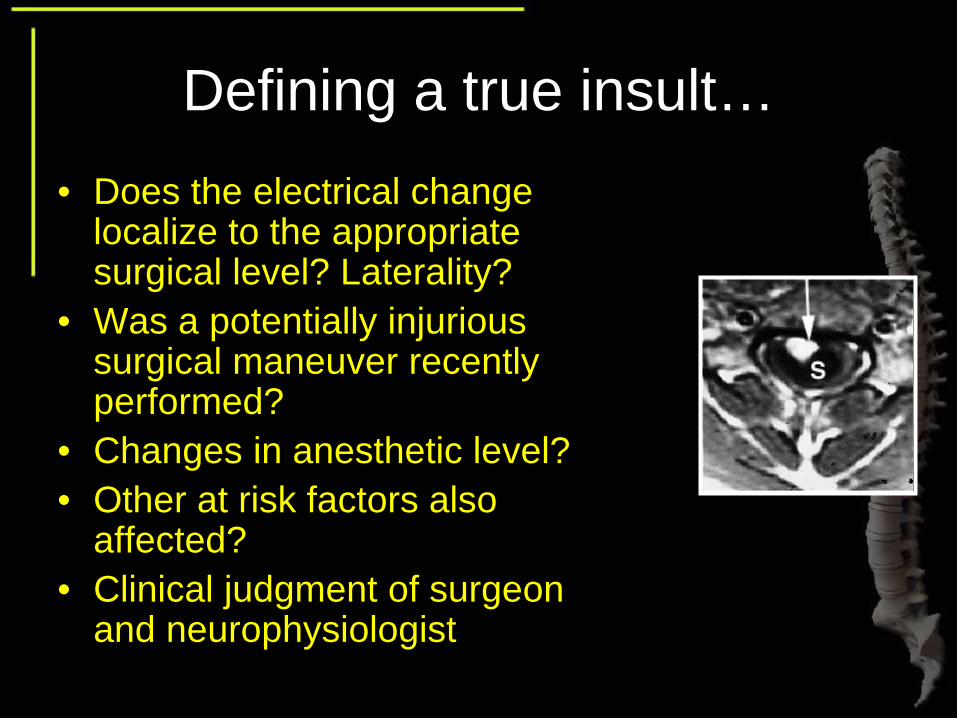
Defining a true insult…• Does the electrical change
localize to the appropriate surgical level? Laterality?
• Was a potentially injurious surgical maneuver recently performed?
• Changes in anesthetic level?• Other at risk factors also
affected?• Clinical judgment of surgeon
and neurophysiologist

Confirmatory Clinical Tests
• Stagnara Wake-up Test– Gross motor exam of
extremities– Decrease anesthesia; patient
responds to verbal commands• Ankle Clonus Test
– Reflex normally absent in the awake state
– Appears when awakening from anesthesia
– Not validated– Non-specific

Brachial plexopathy
• MEPs– Recorded over deltoid, extensor carpi radialis, and
intrinsic 1st dorsal interosseous M• Intermittent monitoring of ulnar nerve SSEPs
– Recorded from brachial plexus or cervical spine– Erb’s point

Cervical considerations• SSEP
– Ulnar SSEPs to detect position related issues– Tibial SSEPs may be delayed more than Ulnar– Identify Carotid retraction related issues
• TcMEP– Deltoid MEPs pre-incision– MEPs may be absent from the lowers with myelopathy (even in
ambulatory patient)
• EMG– Limited benefit in C5 palsy (delayed effect)– May be helpful in setting of foraminotomy

Cervical considerations• In upper cervical procedures
(C1-2)– Brainstem auditory-evoked
responses (BAERs) can be used• In procedures above C4
– Upper extremity SSEPs adequate– Median/ulnar nerve enter SC
below C4– Lower extremity SSEPs not
required

Action Items
• Positive event– Raise blood pressure– Transfuse if needed– Release correction (esp.
distraction)– Observe for positive
response 5-10 minutes– Consider wake up test

Action Items• Remove instrumentation• Induce hypertension• Avoid hypoglycemia• Initiate SCI steroid protocol• Consider options to reduce
cord insult– Drain CSF
• Abandon procedure


• Spine deformity cases – SRS– 92% sensitivity, 99% specificity– 51,263 cases
• EMG– Gunnarsson et al– 100% sensitivity, 24% specificity
• MEP– 100% sensitivity, 95% specificity, 96% PPV
• SSEP, MEP, EMG should be utilized together because alone may be unreliable
• ACDF– Risk of neuro injury (0.09-0.6%)– Increases cost by 16%
• Myelopathy patients increased neurologic risk

Summary
• Multimodality approach most efficacious for neuromonitoring
• Limitations– Patient Population– Mitigating Factors– Operator-dependence
• Be clear in action items and protocols• Cost-effectiveness?

Wellington K. Hsu, MDClifford C. Raisbeck Distinguished ProfessorDirector of ResearchDepartment of Orthopaedic SurgeryDepartment of Neurological SurgeryNorthwestern University Feinberg School of Medicinehttp://www.nwspine.org



![SSEP PROGRAM DEVELOPMENT [NAME OF TRANSIT AGENCY] will implement the following process to develop and monitor the SSEP Program: STEP 1: Participate in](https://img.pdfslide.net/doc/110x75/5515a8d4550346486b8b609b/ssep-program-development-name-of-transit-agency-will-implement-the-following-process-to-develop-and-monitor-the-ssep-program-step-1-participate-in.jpg)






![[PPT]EMG and NCV for upper extremity diagnosis NCV and SSEP for... · Web viewEMG: Recruitment When a muscle is voluntarily contracted a single motor unit may fire. As the muscle](https://img.pdfslide.net/doc/110x75/5af1abf27f8b9ad0618fb3e6/pptemg-and-ncv-for-upper-extremity-ncv-and-ssep-forweb-viewemg-recruitment.jpg)