Embed Size (px)
Citation preview
Valvular Heart Disease
Part 2: Aortic Valve

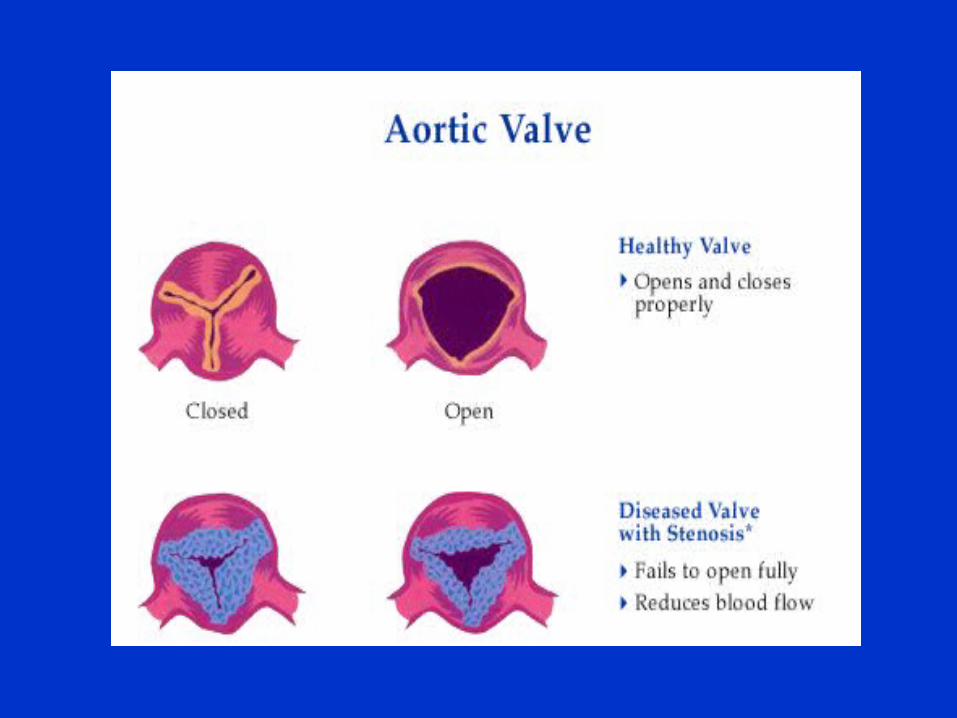

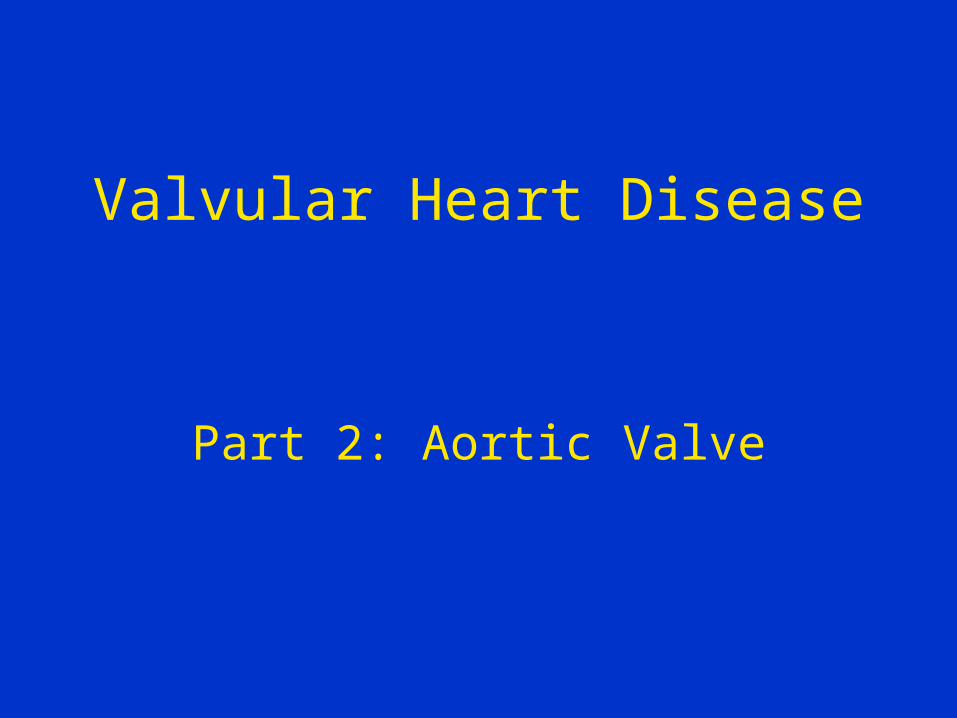
Aortic stenosis (AS)
AS-Etiology
• Senile calcification
-CAD risk factors, ? use of statins
• Congenital
- bicuspid most common, presents in adulthood
- true congenital• Rheumatic heart disease
- mitral always involved as well
AS-Pathophysiology
• Pressure overload wall stress LV hypertrophy
• LVH leads to:
1. increased oxygen demand
2. reduced LV compliance, higher diastolic pressure at same volume
3. lower aortic pressure with reduced systemic perfusion and coronary blood flow
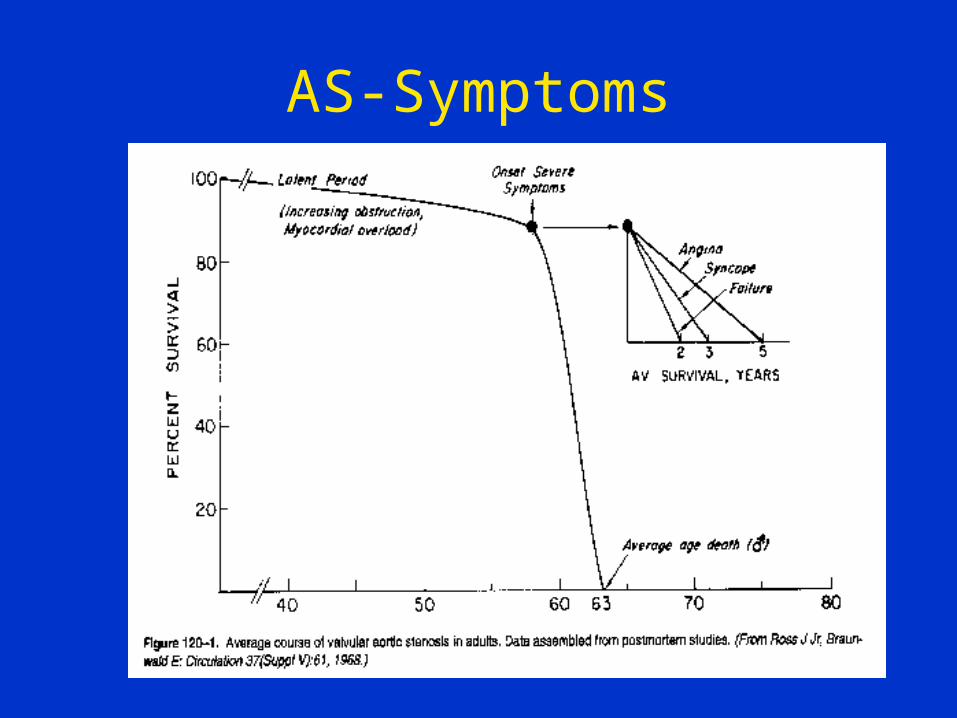
AS-Symptoms
AS-Symptoms
• Angina
Increased O2 demand, decreased supply
Mainly exertional
• Syncope
Exertional- vasodilatation with fixed output
• Congestive heart failure Reduced compliance, eventually systolic
dysfunction
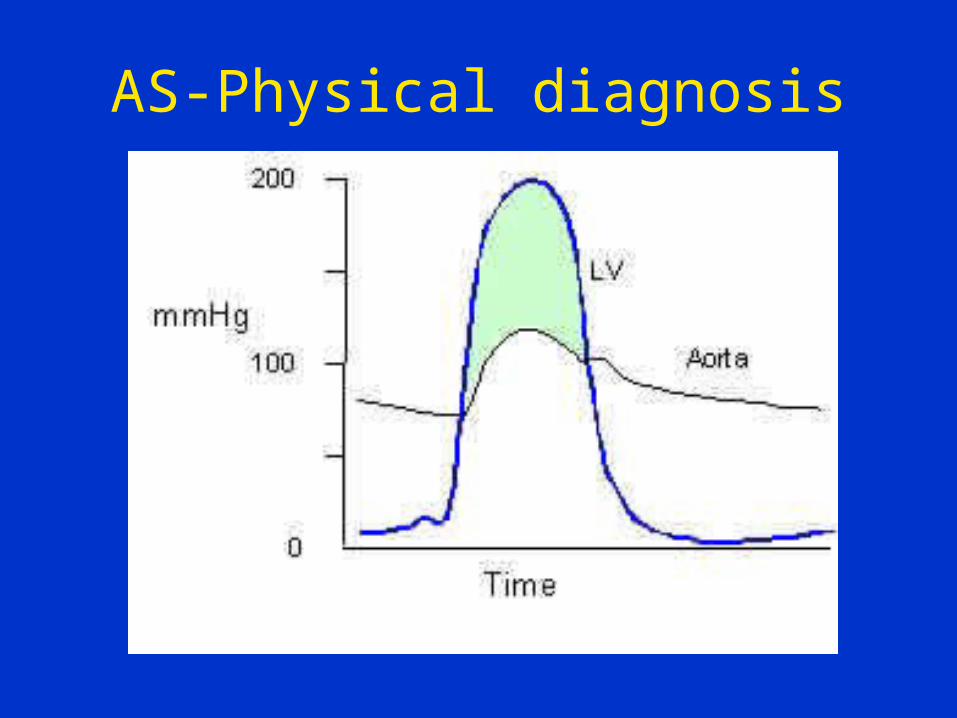
AS-Physical diagnosis
AS-Physical diagnosis
• PMI is sustained and laterally displaced
• Fourth heart sound
• Systolic murmur at base radiating to carotids, crescendo-decrescendo
• Time to peak of murmur, reduced second heart sound, pulsus parvus et tardus correlate with AS severity
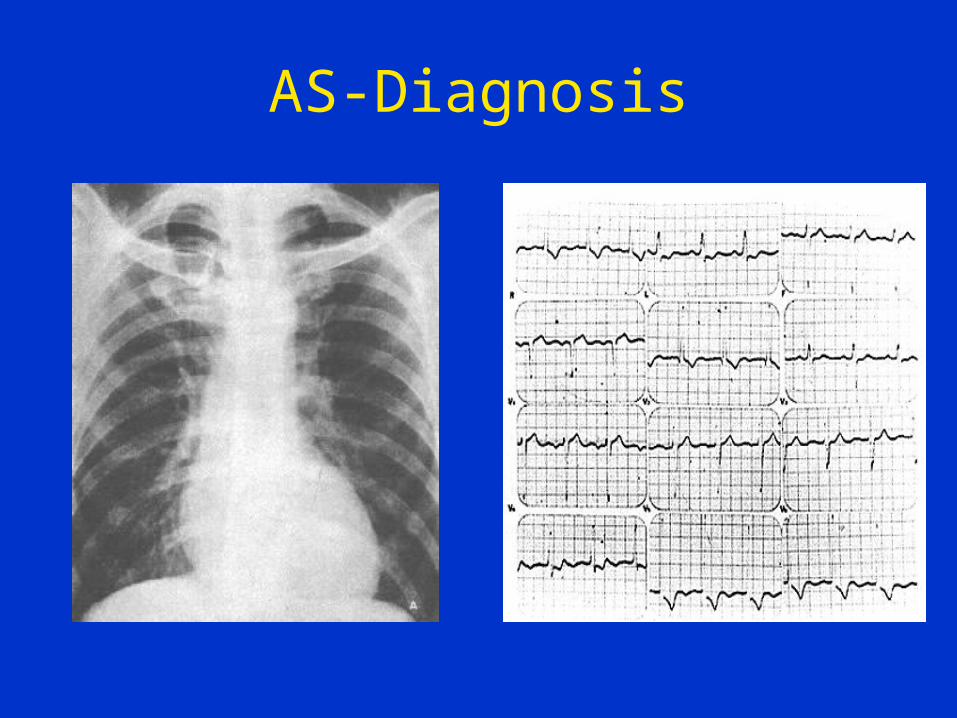
AS-Diagnosis
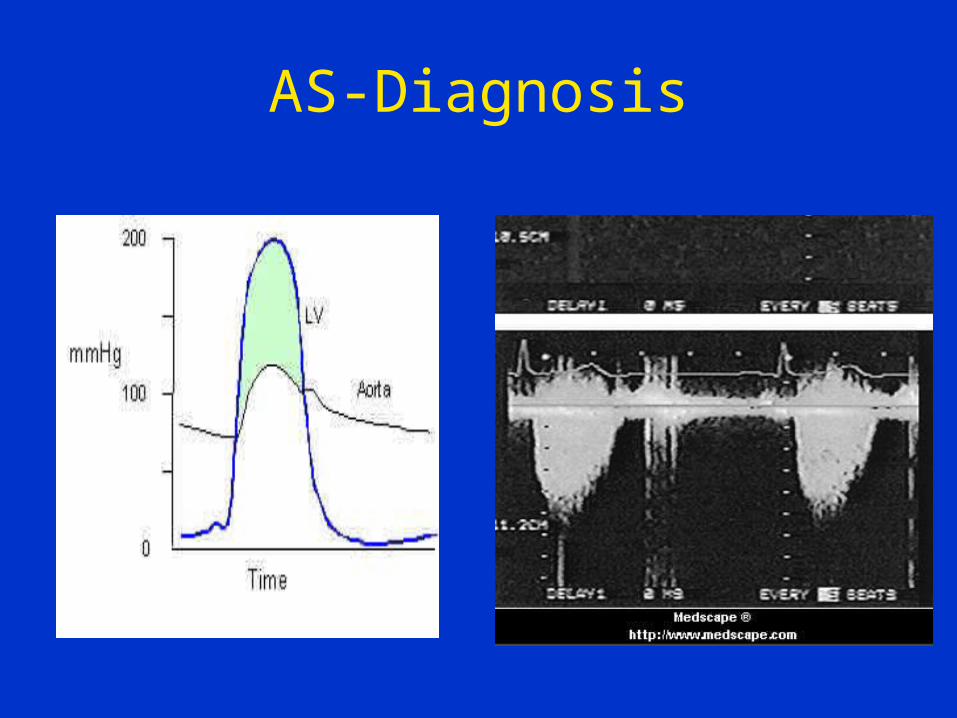
AS-Diagnosis
AS-Medical therapy
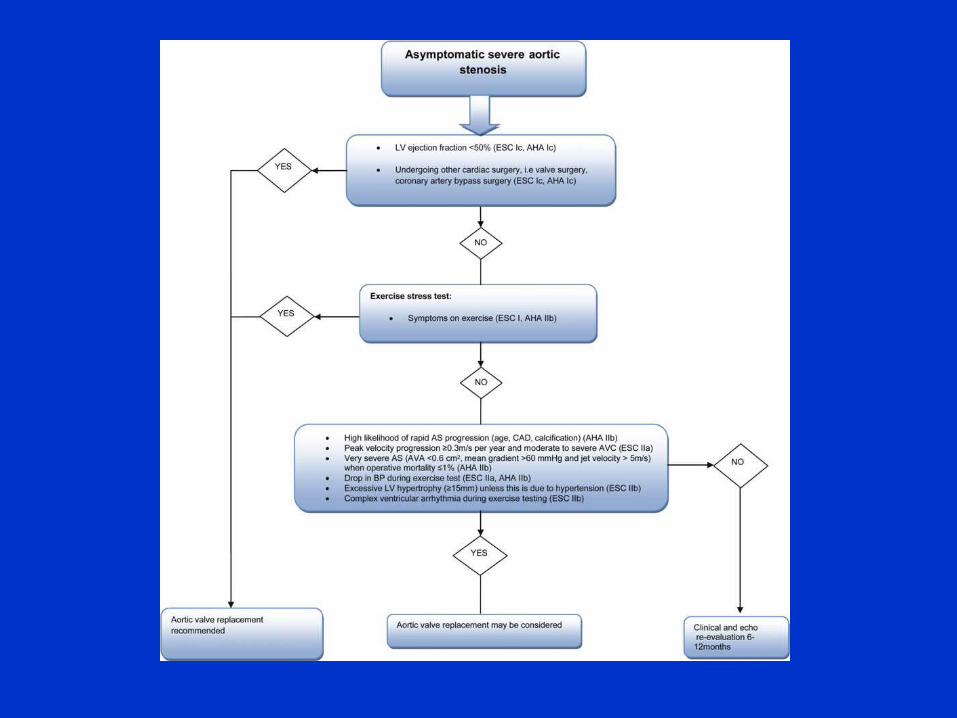
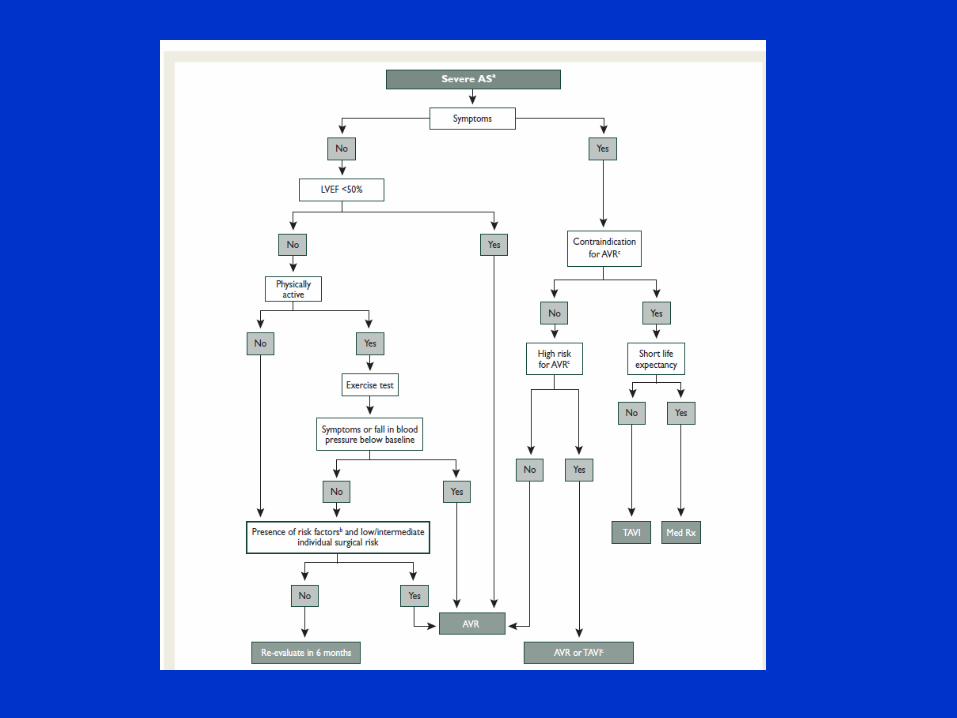
AS-Surgical intervention
• Any appearance of symptoms
• Asymptomatic pts can be followed-– Consider ETT to evaluate FC
• In general, AVR
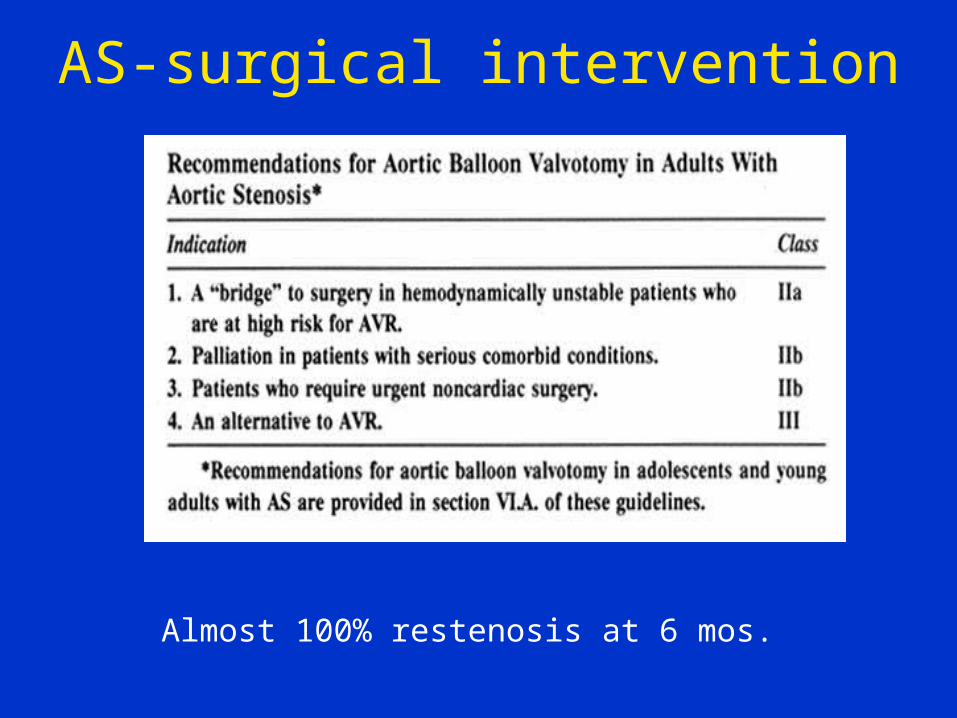
AS-surgical intervention
Almost 100% restenosis at 6 mos.
Percutaneous valve replacement
• Symptomatic AS
• Not candidates/high-risk for surgery
AR-Etiology
Diseases of the valve
1. Rheumatic heart disease
2. Calcific/degenerative
3. Rheumatoid arthritis, ankylosing spondylitis, SLE
4. Congenital-bicuspid, VSD, DSS
AR-Etiology
Diseases of the aorta
1.Marfan’s, other connective tissue disorders
2. Hypertension
3. Tertiary syphillis
4. Aortic aneurysm\dissection (acute)
AR-Pathophysiology
Extreme volume overload LV dilatation
As in MR, LV function initially preserved but gradually decreases
Unlike MR, no reduced afterload and only compensation is dilatation
AR-Pathophysiology
Increased LV mass increases O2 demand
Reduced aortic diastolic pressure leads to decreased coronary perfusion and reduced O2 supply
AR-Symptoms
• Long latent, asymptomatic period
• Symptoms generally appear after significant LV dilatation has already occurred.
• Congestive heart failure
• Rarely, angina due to decreased coronary perfusion
AR-Physical diagnosis
• Peripheral wide pulse pressure
“waterhammer” or “pistol-shot” pulses head-bobbing, “dancing” uvula
• CardiacPMI laterally and downwardly displacedDecrescendo diastolic murmur (sitting up) -duration correlated with severityApical diastolic murmur (“Austin-Flint”)
AR-Medical therapy
• Afterload reduction- ACEI, hydralazine, nifedipine
Unlike MR, randomized trials available
• Acute-immediately to OR
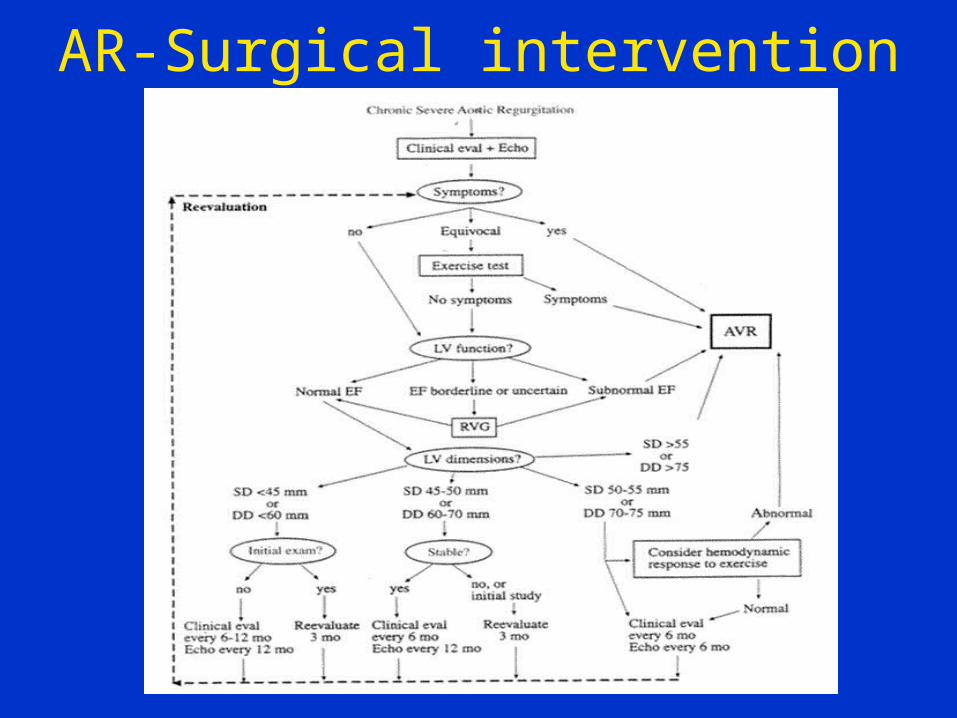
AR-Surgical intervention