Embed Size (px)
Citation preview

1
Aortic orifice area (AOA) and blood flow velocity are often considered insufficient to characterize the severity
of aortic stenosis (AS).1,2 The increased stress on the left ven-tricle (LV) caused by AS can be highly variable and leads to a broad range of LV impairment.3,4 As a result, it is challenging to quantitatively determine the burden on the ventricle caused by AS in the individual patient. Conversely, unfavorable LV remodeling is an important prognostic factor and contributes significantly to the development of heart failure in patients with AS.5–8
See Editorial by Bäck and MarieSee Clinical Perspective
There are many attempts to better characterize the myo-cardial stress provoked by AS. Whereas a decline of LV
ejection fraction is regarded as a late sign of LV impairment, systolic longitudinal strain assessed by transthoracic echocar-diography has been proven to be a valuable marker for early LV dysfunction in AS.1,9 ECG signs of LV hypertrophy and LV strain as well as elevated blood markers such as troponin and brain natriuretic peptide have also been reported to pre-dict outcome in patients with AS.10,11 Moreover, the presence of fibrosis assessed by late gadolinium enhancement cardio-vascular magnetic resonance (CMR) is associated with poorer outcome with and without aortic valve replacement.12,13
Altered poststenotic blood flow in the presence of AS is another potential cause of elevated LV afterload.
Altered helical and vortical blood flow formations have been described to cause power loss caused by friction and viscous dissipation and to alter wall shear stress (WSS).14
Background—Aortic stenosis (AS) leads to variable stress for the left ventricle (LV) and consequently a broad range of LV remodeling. The aim of this study was to describe blood flow patterns in the ascending aorta of patients with AS and determine their association with remodeling.
Methods and Results—Thirty-seven patients with AS (14 mild, 8 moderate, 15 severe; age, 63±13 years) and 37 healthy controls (age, 60±10 years) underwent 4-dimensional-flow magnetic resonance imaging. Helical and vortical flow formations and flow eccentricity were assessed in the ascending aorta. Normalized flow displacement from the vessel center and peak systolic wall shear stress in the ascending aorta were quantified. LV remodeling was assessed based on LV mass index and the ratio of LV mass:end-diastolic volume (relative wall mass). Marked helical and vortical flow formation and eccentricity were more prevalent in patients with AS than in healthy subjects, and patients with AS exhibited an asymmetrical and elevated distribution of peak systolic wall shear stress. In AS, aortic orifice area was strongly negatively associated with vortical flow formation (P=0.0274), eccentricity (P=0.0070), and flow displacement (P=0.0021). Bicuspid aortic valve was associated with more intense helical (P=0.0098) and vortical flow formation (P=0.0536), higher flow displacement (P=0.11), and higher peak systolic wall shear stress (P=0.0926). LV mass index and relative wall mass were significantly associated with aortic orifice area (P=0.0611, P=0.0058) and flow displacement (P=0.0058, P=0.0283).
Conclusions—In this pilot study, AS leads to abnormal blood flow pattern and peak systolic wall shear stress in the ascending aorta. In addition to aortic orifice area, normalized flow displacement was significantly associated with LV remodeling. (Circ Cardiovasc Imaging. 2016;9:e004038. DOI: 10.1161/CIRCIMAGING.115.004038.)
Key Words: aorta ◼ aortic valve stenosis ◼ heart valve diseases ◼ heart ventricles ◼ magnetic resonance imaging
© 2016 American Heart Association, Inc.
Circ Cardiovasc Imaging is available at http://circimaging.ahajournals.org DOI: 10.1161/CIRCIMAGING.115.004038
Received August 25, 2015; accepted January 14, 2016.From the Working Group Cardiovascular Magnetic Resonance, Experimental and Clinical Research Center, a Joint Cooperation Between the Charité
Medical Faculty and the Max-Delbrueck Center for Molecular Medicine and HELIOS Klinikum Berlin Buch, Department of Cardiology and Nephrology, Berlin, Germany (F.v.K.-B., A.K., R.F.T., E.B., J.S.-M.); Department of Biomedical Engineering, McCormick School of Engineering, Northwestern University, Chicago, IL (A.J.B., M.M.); and Department of Radiology, Feinberg School of Medicine, Northwestern University, Chicago, IL (M.M.).
Correspondence to Florian von Knobelsdorff-Brenkenhoff, MD, Working Group Cardiovascular Magnetic Resonance, Charité Medical University Berlin, Experimental and Clinical Research Center, Lindenberger Weg 80, 13125 Berlin, Germany. E-mail [email protected]
Evaluation of Aortic Blood Flow and Wall Shear Stress in Aortic Stenosis and Its Association With Left
Ventricular RemodelingFlorian von Knobelsdorff-Brenkenhoff, MD; Achudhan Karunaharamoorthy;
Ralf Felix Trauzeddel, MD; Alex J. Barker, PhD; Edyta Blaszczyk, MD; Michael Markl, PhD; Jeanette Schulz-Menger, MD
Valvular Heart Disease
by guest on July 10, 2017http://circim
aging.ahajournals.org/D
ownloaded from

2 von Knobelsdorff-Brenkenhoff et al Aortic Blood Flow in Aortic Stenosis
Integrated over time, these losses can cause an increase in energy required for blood circulation.15 The recent use of 4-dimensional (4D) flow CMR to characterize blood flow pat-terns and the distribution of WSS is an opportunity to inves-tigate this theory.16,17 In this hypothesis-generating study, 4D flow CMR of patients with AS was used to characterize the poststenotic blood flow and to analyze the association of aor-tic hemodynamics with LV remodeling.
Methods
Study PopulationParticipants were prospectively recruited. The diagnosis of AS was based on the AOA obtained from CMR cine imaging. Severe AS was defined as AOA <1 cm2 or AOA indexed by body surface area <0.6 cm2/m2, moderate AS 1 to 1.5 cm2, and mild AS >1.5 cm2. The status healthy was based on uneventful medical history, absence of any symptoms indicating cardiovascular dysfunction, normal ECG and normal cardiac dimensions, and function proven by CMR cine imaging. Subjects with impaired LV ejection fraction <50% or with evidence of coronary artery disease by coronary angiography, non-invasive imaging, or clinical assessment were excluded. Patients with arrhythmia, greater than mild valvular disease (other than AS), or general contraindications for CMR were also excluded. For each participant, written informed consent was obtained before the study, after due approval by the local ethical committee.
Four-Dimensional Flow CMR: AcquisitionAll CMR examinations were performed with a 3T system (MAGNETOM Verio; Siemens Healthcare GmbH, Erlangen, Germany). Four-dimensional flow CMR data were acquired using a sagittal oblique volume covering the thoracic aorta. Prospective ECG gating was used in combination with a respiratory navigator placed on the lung–liver in-terface to permit data acquisition during free breathing. The following scan parameters were chosen: echo time=2.6 ms, repetition time=5.1 ms, bandwith=450 Hz/pixel, imaging acceleration using PEAK GRAPPA with a reduction factor of R=5,18 net acceleration 4.17, reference lines=20, flip angle α=7° to 9°, temporal resolution=40.8 ms, field of view (360×270) mm2, matrix (133×118), voxel size=2.7×2.3×2.6 mm3, phase encoding direction=anterior-posterior, number of slices=32, velocity encoding=1.5 (healthy controls)−2.5 m/s (AS).
Four-Dimensional Flow CMR: PostprocessingAll 4D flow data were processed as previously described and in con-cordance with current consensus recommendations.19,20 Briefly, data were corrected for Maxwell terms, eddy currents, and velocity alias-ing (MATLAB; The MathWorks, Natick, MA).21 In a second step, a 3D phase contrast angiogram was calculated based on the flow measurements to position 2D analysis planes and to aid in 3D blood flow visualization (EnSight; CEI, Apex, NC). Three planes were po-sitioned perpendicular to the longitudinal axis of the aortic wall: at the level of the sinotubular junction (S
1), in the midascending aorta
(S2), and proximal to the brachiocephalic trunk (S
3; Figure 1). These
analysis planes were exported into software for the segmentation and calculation of the blood flow parameters (MATLAB).21 A single ex-pert did this analysis with extensive experience in the assessment of 4D flow data sets strictly after standard operating procedures.
Four-Dimensional Flow: ParametersHelical and vortical blood flow formations in the ascending aorta were semiquantitatively evaluated using pathline movies and graded in: 0 (none), 1 (<360°), and 2 (>360°). A vortical flow formation was defined as revolving particles around a point within the vessel with a rotation direction deviating by >90° from the physiological flow directions. A helical flow formation was considered a regional fluid circulation around an axis parallel to bulk fluid motion (ie, along the
longitudinal axis of the vessel), thereby creating a corkscrew-like mo-tion.19 To test interobserver dependency, the analysis was repeated by a second observer for a subset of 25 randomly selected data sets.
Peak velocity blood flow was semiquantitatively graded as cen-tral, mildly eccentric, or markedly eccentric in 2D flow profiles at the midascending aorta.19,22 Central flow was defined by the high veloc-ity flow occupying the majority of the vessel. A mild eccentric flow occupied one to two thirds of the vessel and a marked eccentric flow occupied one third or less of the vessel. In addition, normalized flow displacement was calculated to quantitatively describe blood flow ec-centricity. Normalized flow displacement is defined as the distance between the center of the lumen and the center of velocity of the forward flow, normalized to the lumen diameter.23 Finally, a visualiza-tion of outflow asymmetry was created by mapping the peak systolic velocity location and the region of the upper 15th percentile of the velocities on a segmental aortic lumen map.
Quantification of peak systolic WSS (WSSpeak
in N/m2) was per-formed for 8 regional segments along the aortic circumference for each plane S
1–S
3.17 Regional WSS
peak was averaged with the preced-
ing and 3 subsequent time steps to mitigate measurement noise.
Cine CMRSteady-state free-precession cine images were obtained to assess wall motion, for cardiac chamber quantification and for planim-etry of the AOA.24 Imaging parameters were as follows: repeti-tion time=3.1 ms, echo time=1.3 ms, flip angle=45°, field of view (276×340) mm2, matrix (156×192), slice thickness 6 mm (cham-bers) and 5 mm (aortic valve), bandwidth 704 Hz/px, parallel imag-ing using GRAPPA reconstruction (R=2), 30 cardiac phases. Axial steady-state free-precession still images of the thorax were used to estimate the size of the ascending aorta at the level of the pulmo-nary bifurcation.25 Image analysis was done using CVI42 (Circle Cardiovascular Imaging, Calgary, Canada).
LV remodeling was defined based on LV mass index (LVMI) and relative wall mass (RWM=LVM divided by end-diastolic volume in g/mL).3 The categories were: (1) normal (LVMI and RWM normal), remodeling (LVMI normal and RWT ≥1.16 g/mL), hypertrophy (LVMI abnormal26 and RWM ≥1.16 g/mL). Asymmetrical remodel-ing and hypertrophy were differentiated by wall thickening ≥13 mm that was also >1.5-fold the thickness of the opposing myocardial seg-ment. RWM is reported to be more sensitive to detect LV remodeling than global LV mass or 2D diameters of the LV wall, in particular, for small concentric remodeled hearts.3
Statistical AnalysisStatistical analysis of the data as outlined in this section was per-formed using SPSS 20 (IBM, Armonk, NY) and SAS 9.4 (SAS Institute Inc., Cary, NC). Graphics were created using PRISM 5 (GraphPad Software Inc, San Diego, CA) and plug-in software for MATLAB. Categorical data are expressed as percentages; continu-ous data as mean±SD. Interobserver variability of helical and vortical flow evaluation was assessed using the intraclass correlation coef-ficient. Comparisons between the 3 severity grades of AS were made using the Jonckheere–Terpstra test when a trend across groups was of major interest,27 or the Kruskal–Wallis test when looking for any dif-ference between the groups. In case of significance, a Mann–Whitney U test was added to investigate into the actual effects. Correlation was assessed using the Spearman method.
Modeling of Flow ParametersThe flow parameters were modeled based on all available data using ordinal logistic regression or linear regression as appropriate for the parameter. The presence of a bicuspid aortic valve, aortic diameter, ejection fraction, age, AOA, AS grade, and AS (y/n) as well as the 2-way interaction between AS (y/n) and the aforementioned indepen-dent variables other than AS grade were independent variables in the models.17,28,29 Stepwise selection (P(entry)=0.15, P(stay)=0.15) was used to arrive at sparse models and to avoid spurious effects caused by correlations in the independent variables. As for some models,
by guest on July 10, 2017http://circim
aging.ahajournals.org/D
ownloaded from

3 von Knobelsdorff-Brenkenhoff et al Aortic Blood Flow in Aortic Stenosis
significant interaction terms pointed toward different effect in pa-tients and controls; models were also computed for patients only. The focus of interpretation was put into the main factors, whereas interac-tion terms will be subject to further investigation.
Modeling of Remodeling ParametersThe analysis of associations with the remodeling parameters LVMI, RWM, and presence of LV remodeling was based on patients only. Univariate linear or logistic regression models were used to assess uni-variate relationships between the remodeling parameters and the flow pa-rameters helical and vortical flow formation, eccentricity, normalized flow displacement, and WSS
peak. In a first step of multiple modeling, multiple
regression models using the influential factors systolic blood pressure, AOA, and age as independent variables were built to investigate the influ-ence of these more familiar parameters on remodeling parameters.3,30 In a second step, the models were extended by the flow parameters helical and vortical flow formations, eccentricity, and normalized flow displacement (S
1–S
3), as well as WSS
peak (S
1–S
3). Stepwise selection (P(entry=0.15,
P(stay)=0.15) was used to identify flow parameters with added value for the explanation of variability in the remodeling parameters.
As this was an exploratory study, P values were considered as de-scriptive rather than confirmatory throughout. Except for the model-ing approaches, P<0.05 were considered to be statistically significant.
ResultsStudy SampleThe study sample comprised n=37 patients with AS and n=37 healthy control subjects. All were in sinus rhythm. Tables 1 and 2 show the characteristics of the study participants.
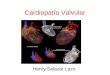
Patients with AS had a higher body mass index, higher systolic blood pressure and larger aortic diameter, higher LVMI and higher RWM, lower stroke volume index and lower LV end-diastolic volume index than controls. Furthermore, patients with AS were slightly older than controls (63 ver-sus 60 years; P=0.042), but can be regarded as being within in a similar age class. There was no difference on the sex-distribution between both groups. With increasing severity of AS, AOA, and AOA index decreased (P<0.001). RWM and LVMI was significantly higher in severe AS than in mild AS (P<0.001 and P=0.037). The prevalence of LV remodeling increased with increasing AS severity (Figure 2).
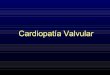
Helical and Vortical Blood Flow Formations in the Ascending AortaInterobserver variability to assess helical and vortical flow formations was low with an intraclass correlation
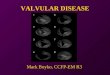
coefficient of 0.82 and 0.77, respectively. Examples for helical and vortical blood flow formations are shown in Figure 1. Marked helical and vortical flow formation were more prevalent in patients with AS than in healthy subjects, and with increasing AS severity grade the prevalence gen-erally increased (Figure 3). Table 3 summarizes all models with model estimates and their respective P values after model selection.
Helical Flow FormationsAge, ejection fraction, aortic diameter, AS grade, and AOA were not relevant with respect to the intensity of helical flow formation within the AS sample. Only when considering both
Figure 1. Schematic of the analysis planes at the sinotubular level, midascending, and distal ascending aorta (left). Examples for marked vortical and helical flow formation and eccentricity when compared with the flow of a healthy volunteer.
Table 1. Patient Characteristics
Parameter AS Healthy P Value
n 37 37
Sex (male/female) 23/14 20/17 0.48
Age, y 63±13 60±10 0.042*
Height, cm 169±9 171±13 0.25
Weight, kg 83±13 79±17 0.074
BMI, kg/m2 28.8±4.3 27.7±10.3 0.005*
BSA, m2 1.97±0.19 1.92±0.21 0.22
Systolic blood pressure, mm Hg 140±15 134±13 0.012*
Diastolic blood pressure, mm Hg 83±14 82±10 0.84
Heart rate, min−1 67±12 68±9 0.77
Aortic diameter, mm 35±7 32±3 0.016*
Aortic orifice area, cm2 1.5±0.6 3.5±0.5 <0.001*
Aortic orifice area index, cm2/m2 0.75±0.33 1.85±0.25 <0.001*
Morphology of aortic valve (tricuspid/ bicuspid)
21/16 37/0 <0.001*
LVEF, % 66±6 63±5 0.062
LVSV-index, mL/m2 44±11 48±8 0.044*
LVEDV-index, mL/cm 0.77±0.18 0.87±0.18 0.020*
LV mass index, g/cm 0.94±0.30 0.70±0.15 <0.001*
Relative wall mass, g/mL 1.25±0.38 0.81±0.13 <0.001*
The P value stems from the Mann–Whitney U test and for sex and valve morphology from the χ2 test. AS indicates aortic stenosis; BMI, body mass index; BSA, body surface area; LVEDV, left ventricular end-diastolic volume; LVEF, left ventricular ejection fraction; and LVSV, left ventricular systolic volume.
*P<0.05.
by guest on July 10, 2017http://circim
aging.ahajournals.org/D
ownloaded from

4 von Knobelsdorff-Brenkenhoff et al Aortic Blood Flow in Aortic Stenosis
patients and controls, a higher age and a smaller AOA were associated with more intense helical flow formation (P=0.14). Helical flow formation was significantly more intense for AS patients with a bicuspid aortic valve than for AS patients with a tricuspid valve (P=0.0098).
Vortical Flow FormationsWithin the AS sample, the smaller the AOA and the larger the ascending aortic diameter, the more intense the vorti-cal flow formation was (P=0.0274, P=0.14). Vortical flow formations were more pronounced for subjects with a bicus-pid aortic valve than for AS patients with a tricuspid valve (P=0.0536).
Eccentricity of the Blood Flow in the Ascending AortaAn example for marked eccentricity is shown in Figure 1. The strong eccentricity of the blood flow, which is present in all AS severity grades, is illustrated by the mapping of the peak flow velocity in Figure 4. Marked eccentricity was more prevalent in patients with AS than in healthy subjects, and with increasing AS severity grade the prevalence gener-ally increased (Figure 3). In the regression model, a lower AOA was strongly associated with a higher eccentricity (P<0.0001 in all subjects, P=0.0070 in patients). The results of the normalized flow displacement, which quantitatively describes blood flow eccentricity, are summarized in Table 4. Normalized flow displacement was strongly associated with AOA (P
S2=0.0021) and age (P
S3=0.0662) among the patients
with AS, with the smaller the AOA and the higher the age, the larger the flow displacement. The presence of a bicuspid aortic valve was weakly related to normalized flow displace-ment (P
S1=0.11).
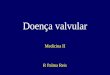
WSS in the Ascending AortaThe distribution of WSS
peak along the aortic circumference is
illustrated in Figure 5. Patients with AS exhibited an asym-metrical elevation of WSS
peak at the right/right anterior/anterior
side of the aorta at level S1. The magnitude and the asymmetry
of WSSpeak
became more marked in S2. In S
3, mild and moder-
ate AS approached the WSSpeak
of healthy controls. Severe AS still showed increased and asymmetrical WSS
peak results with
peaks at the anterior/left anterior wall (even though there was no statistical difference).
Table 2. Patient Characteristics Separated by Aortic Stenosis Severity Grade
Parameter Mild Moderate Severe P Value
n 14 8 15
Sex (male/female) 8/6 3/5 12/3 0.12
Age, y 58±17 63±13 68±8 0.13
Height, cm 168±9 169±11 172±8 0.18
Weight, kg 81±14 82±14 85±13 0.36
BMI, kg/m2 28.6±4.0 28.8±3.6 29.0±4.9 0.89
BSA, m2 1.93±0.20 1.95±0.22 2.01±0.15 0.12
Systolic blood pressure, mm Hg 140±14 143±18 140±16 0.93
Diastolic blood pressure, mm Hg 82±15 85±20 82±11 0.90
Heart rate, min−1 67±15 68±10 69±11 0.48
Aortic diameter, mm 33±7 38±7 35±6 0.52
Aortic orifice area, cm2 2.09±0.39 1.28±0.18 0.94±0.21 <0.001*
Aortic orifice area index, cm2/m2 1.10±0.24 0.66±0.06 0.47±0.11 <0.001*
Morphology of aortic valve (tricuspid/bicuspid)
11/3 5/3 5/10 0.10
LVEF, % 64±6 66±6 67±6 0.19
LVSV-index, mL/m2 45±12 42±10 44±10 0.89
LVEDV-index, mL/cm 0.80±0.20 0.75±0.15 0.76±0.18 0.63
LV mass index, g/cm 0.79±0.19 0.93±0.21 1.08±0.36 0.036*
Relative wall mass, g/mL 1.00±0.15 1.28±0.39 1.43±0.42 0.001*
The P value stems from the Jonckheere–Terpstra test and for sex and valve morphology from the χ2 test. BMI indicates body mass index; BSA, body surface area; LVEDV, left ventricular end-diastoluc volume; LVEF, left ventricular ejection fraction; and LVSV, left ventricular systolic volume.
*P<0.05.
Contro
ls
Mild AS
Modera
te AS
Severe
AS0
20
40
60
80
100
Prev
alen
ce [%
]
NoneConcentric RemodelingAsymmetric RemodelingConcentric HypertrophyAsymmetric Hypertrophy
Figure 2. Prevalence of LV remodeling in patients with aortic stenosis (AS) separated for AS severity grades. AS sever-ity grades were found statistically significant for severity of left ventricular (LV) remodeling in ordinal logistic regression (P<0.0001).
by guest on July 10, 2017http://circim
aging.ahajournals.org/D
ownloaded from

5 von Knobelsdorff-Brenkenhoff et al Aortic Blood Flow in Aortic Stenosis
In the regression model, a bicuspid aortic valve was associated with higher WSS
peak in S
2 (P=0.0926). In
patients with AS, ejection fraction correlated positively
with WSSpeak
in level S1 (P=0.0474) and S
3 (P=0.0592),
and a higher age was associated with higher WSSpeak
in level S
3 (P=0.0469).
Contro
ls
Mild AS
Modera
te AS
Severe
AS0
20
40
60
80
100
Prev
alen
ce [%
]
None Mild Marked
Contro
ls
Mild AS
Modera
te AS
Severe
AS0
20
40
60
80
100
Prev
alen
ce [%
]
None Mild Marked
Contro
ls
Mild AS
Modera
te AS
Severe
AS0
20
40
60
80
100
Central Mild Marked
Prev
alen
ce [%
]
Helical flow formation Vortical flow formation Eccentricity
Figure 3. Qualitative grades for helical flow formation, vortical flow formation, and eccentricity. Aortic stenosis (AS) severity grades were found statistically significant for helical and vortical flow formation and eccentricity in ordinal logistic regression (all P<0.0001).
Table 3. Multiple Regression Models on the Association of Flow Parameters (Helical and Vortical Flow Formation, Eccentricity, Normalized Flow Displacement, WSSpeak) With Potential Influencing Factors, Parameter Estimates, and P Values of Final Models After Stepwise Selection
Flow Parameter (Model) Independent VariableAll Subjects (n=74)
Estimate β±SE (P Value)Patients (n=37)
Estimate β±SE (P Value)
Helical flow* Age −0.04±0.02 (P=0.14)
Bicuspid morphology 0.98±0.48 (P=0.0406) 1.13±0.44 (P=0.0098)
Aortic orifice area −1.81±0.38 (P<0.0001)
Vortical flow* Bicuspid morphology 0.80±0.38 (P=0.0375) 0.74±0.38 (P=0.0536)
Aortic diameter 0.12±0.06 (P=0.0522) 0.10±0.07 (P=0.14)
Aortic orifice area −1.84±0.55 (P=0.0009) −1.42±0.64 (P=0.0274)
AS (y/n) −2.71±1.22 (P=0.0258) …
Eccentricity*,† Aortic orifice area −2.74±0.47 (P<0.0001) −2.17±0.81 (P=0.0070)
Normalized flow displacement, S1‡ Bicuspid morphology … 0.032±0.02 (P=0.11)
Ejection fraction 0.002±0.001 (P=0.0668) …
AS×aortic diameter 0.002±0.0003 (P<0.0001) …
Normalized flow displacement, S2‡ Age 0.001±0.0004 (P=0.0788)
Aortic orifice area −0.039±0.004 (P<0.0001) −0.041±0.01 (P=0.0021)
Normalized flow displacement, S3‡ Age … 0.001±0.001 (P=0.0662)
AS×age 0.002±0.0002 (P<0.0001) …
WSSpeak
, S1‡ Ejection fraction 0.01±0.01 (P=0.0269) 0.02±0.01 (P=0.0474)
AS×ejection fraction 0.01±0.001 (P<0.0001) …
WSSpeak
, S2‡ Age −0.01±0.003 (P=0.0002) …
Bicuspid morphology … 0.22±0.13 (P=0.0926)
AS×ejection fraction 0.01±0.002 (P<0.0001) …
AS×aortic orifice area −0.22±0.07 (P=0.0043) …
WSSpeak
, S3‡ Age −0.01±0.003 (P<0.0001) −0.01±0.004 (P=0.0469)
Ejection fraction … 0.02±0.01 (P=0.0592)
AS×ejection fraction 0.01±0.004 (P=0.0004) …
AS×aortic diameter −0.01±0.01 (P=0.0859) …
AS×aortic orifice area −0.13±0.07 (P=0.0540) …
Only parameters remaining in the final model are shown. AS indicates aortic stenosis; and WSSpeak
, peak systolic wall shear stress.*Ordinal logistic regression.†Model without AS (y/n) and interaction terms as introduction of these led to quasi-complete separation.‡Linear regression.…Parameter not presented to selection process.
by guest on July 10, 2017http://circim
aging.ahajournals.org/D
ownloaded from

6 von Knobelsdorff-Brenkenhoff et al Aortic Blood Flow in Aortic Stenosis
Association of Flow Parameters With Parameters of LV RemodelingThe results of the regression models are shown in Table 5. In the univariate investigation, stronger vortical flow formations were associated with higher LVMI, higher RWM, and higher probability of LV remodeling (P=0.0213, P=0.0115, and P=0.0285, respectively). Higher eccentricity was associated with higher RWM (P=0.0270). A higher normalized flow displacement in level S
2 was significantly associated with a
higher LVMI (P=0.0410), a higher RWM (P=0.0023), and with the presence of LV remodeling (P=0.0459). A higher normalized flow displacement in level S
3 was significantly
associated with higher LVMI (P=0.0056) and higher RWM (P=0.0076). A higher WSS
peak at level S
1 was significantly
associated with higher LVMI (P=0.0268).In multiple regression, LVMI, RWM, and presence of
LV remodeling were found to be significantly negatively associated with AOA. The covariates age and systolic blood pressure were not found to be significant for the remodeling parameters. The only parameter in addition to AOA that was linked to parameters of LV remodeling was the normalized flow displacement in level S
3. Its addition improved the model
for LVMI to R2=0.3108 when compared with R2=0.1083
(P=0.0058) and for RWM to R2=0.3351 (from 0.2575; P=0.0713), indicating that a larger normalized flow displace-ment was associated with a higher LVMI and RWM.
DiscussionPatients with AS exhibited a high prevalence of abnormal flow patterns with regard to helical and vortical flow formations and eccentricity. Vortical flow formation, eccentricity, and normal-ized flow displacement were strongly associated with AOA, indicating that the obstruction influences boundary layer sepa-ration and leads to significant destabilization of the antegrade blood flow. As there was no difference in the ascending aortic size between the AS severity grades as well as only a weak general association between aortic size and vortical flow for-mation, these flow abnormalities can be mainly attributed to the abnormal AOA. In addition to the mere flow obstruction, the bicuspid morphology of the valve was a relevant con-tributor to abnormal blood flow. This finding is in agreement with previous studies that demonstrated altered blood flow in bicuspid valve disease even in the absence of a stenosis.17,31
Abnormal blood flow may reflect an elevated afterload for the LV, as energy is dissipated by frictional losses associ-ated with the various flow phenomena and with the aortic wall.14 The latter hypothesis is strengthened by the observa-tion of the univariate analysis, where vortical flow forma-tion, eccentricity, and normalized flow displacement were associated with signs of LV remodeling. In the multiple model, however, normalized flow displacement was the only parameter that had impact on LV remodeling in addition to AOA. The relatively small impact of flow parameters on remodeling parameters in multiple models when compared
Figure 4. Visualization of the outflow asymmetry by mapping the peak systolic velocity location and the region of the upper 15th percen-tile of the velocities on a segmental aortic lumen map. AS indicates aortic stenosis; S1, sinotubular junction; S2, midascending aorta; and S3, distal ascending aorta.
Table 4. Normalized Flow Displacement (Mean±SD)
Aortic Level Healthy Controls Mild AS Moderate AS Severe AS
S1
0.11±0.04 0.18±0.05 0.20±0.05 0.19±0.07
S2
0.08±0.05 0.14±0.04 0.17±0.04 0.19±0.05
S3
0.04±0.01 0.12±0.06 0.16±0.04 0.14±0.07
AS indicates aortic stenosis.
by guest on July 10, 2017http://circim
aging.ahajournals.org/D
ownloaded from

7 von Knobelsdorff-Brenkenhoff et al Aortic Blood Flow in Aortic Stenosis
with univariate models might be explained by their high cor-relation to AOA (helix: r=−0.31, vortex: r=−0.52, eccentric-ity=−0.48, normalized flow displacement r=−0.56). Thus, the added value of flow parameters to models containing AOA is limited, but it was present at least for normalized flow displacement. The association of LV remodeling with AOA underlines that remodeling is a feature of AS sever-ity. Whether it is also a feature of disease progression needs confirmation in a longitudinal study.
Hypertension is another contributor to LV remodeling.32 The mean systolic blood pressure was slightly elevated in the AS group when compared with the healthy controls, whereas the various severity grades of AS did not differ on the blood pressure. Nevertheless, a comparable blood pressure in a patient with severe versus mild AS may have varying degree of LV impact, as it is the combination of vascular and valvu-lar LV hemodynamic load that is decisive. In this study, the multiple regression model on LV remodeling accounted for blood pressure and did not find a significant influence among the patients with AS.
Blood flow abnormalities are also thought to contribute to poststenotic aortic dilatation by the chronic vascular wall strain.33 Patients with AS revealed significantly elevated WSS
peak at the level of the sinotubular junction and midas-
cending aorta. This was observed similarly in all severity
grades of AS, underlining that the aortic blood flow changes as soon as the morphology of the aortic valve changes, even in the absence of a clinically relevant obstruction. Higher WSS
peak was not linked to markers of LV remodeling, but
adds knowledge to the development of poststenotic dilata-tion in AS.34
In conclusion, this hypothesis-generating study using 4D flow CMR provided new insights into the aortic blood flow in the presence of AS. Blood flow was abnormal in AS, with increasing intensity as the AOA decreased, and enhanced by the presence of a bicuspid aortic valve. In addition to AOA, the flow parameter normalized flow displacement was signifi-cantly linked to signs of LV remodeling and might therefore serve as surrogate of unfavorable blood transport and myo-cardial stress. WSS was elevated and asymmetrically distrib-uted in the aorta in all severity grades of AS. Whereas this parameter was not associated with LV remodeling, the find-ings suggested that mechanotransduction risks for postste-notic dilatation are present already in the early stages of AS. At that time, the results are mainly descriptive and add to the knowledge base surrounding flow patterns in the proximity of AS. The added clinical value of this new information still has to be proven. Yet, we speculate that the fluid dynamics infor-mation might enable a better characterization of the disease stage in the future.
Figure 5. Peak systolic wall shear stress (WSSpeak) distribution along the aortic circumference. Comparison of the aortic stenosis (AS) severity grades with healthy controls. Significant differences between the groups with *P<0.05 and **P<0.001. Tests were performed per location. A indicates anterior; L, left; LA, left anterior; LP, left posterior, P, posterior; R, right; RA, right anterior; RP, right posterior; S1, sino-tubular junction; S2, midascending aorta; and S3, distal ascending aorta. by guest on July 10, 2017
http://circimaging.ahajournals.org/
Dow
nloaded from

8 von Knobelsdorff-Brenkenhoff et al Aortic Blood Flow in Aortic Stenosis
LimitationsThere are several limitations in this work that make it a hypothesis-generating study. (1) Further studies with larger samples, more quantitative flow information and integration of multimodality information are needed to test the generated hypothesis that flow pattern and remodeling are linked and to allow adequate subgroup-analysis. (2) Helical and vorti-cal flow patterns were only assessed qualitatively. Absolute quantification of flow and energy loss might be superior and more objective; furthermore, volumetric assessments might overcome limitations of 2D analyses. However, validation using magnetic resonance imaging, CFD, and particle image velocity data has only recently emerged, with mixed results relating to segmentation and resolution-related errors.35–39 The computation of these parameters requires specialized algorithms and volumetric segmentations, neither of which were available for this study. Additional development and validation needs to be performed before the quantitative approaches can be integrated in future clinically oriented studies. After having overcome these challenges, extend-ing the definitions of the tested flow parameters from 2D to 3D and achieving a volumetric description will certainly be an important future direction. (3) Age is a known influenc-ing factor for ascending aortic hemodynamics.29 The groups
were statistically not perfectly age matched, but they were in the same age category (middle-aged adults). To account for this age difference, age was included in the regression models.
AcknowledgmentsWe acknowledge the technicians Kerstin Kretschel, Evelyn Polzin, Denise Kleindienst, and Franziska Neumann for acquiring the CMR data and the study nurses Elke Nickel-Szczech and Antje Els for as-sisting in the organization of the CMR scans. We thank Mrs Susanne Schwenke (scossis, Berlin) for her valuable support of the statistical analyses.
Sources of FundingDeutsche Stiftung für Herzforschung (Frankfurt, Germany; F/37/12; Dr von Knobelsdorff-Brenkenhoff), National Institutes of Health (NIH) K25HL119608 (Dr Barker), and NIH R01HL115828 (Dr Markl).
DisclosuresNone.
References 1. Pibarot P, Dumesnil JG. Improving assessment of aortic stenosis. J Am
Coll Cardiol. 2012;60:169–180. doi: 10.1016/j.jacc.2011.11.078.
Table 5. Univariate and Multiple Regression Models to Assess Relationships Between Parameters of LV Remodeling and Flow Parameters
Model Remodeling Parameter Independent Variable Estimate P Value
Univariate models
Linear regression LVMI Vortical flow formation 10.94±4.54 0.0213
Normalized flow displacement, S2
172.00±81.04 0.0410
Normalized flow displacement, S3
185.61±62.94 0.0056
WSSpeak
, S2
23.47±10.15 0.0268
Linear regression RWM Vortical flow formation 0.18±0.07 0.0115
Eccentricity 0.29±0.13 0.0270
Normalized flow displacement, S2
3.65±1.11 0.0023
Normalized flow displacement, S3
2.65±0.94 0.0076
Logistic regression LV remodeling Vortical flow formation 0.92±0.42 0.0285
Normalized flow displacement, S2
16.53±8.28 0.0459
Final multiple models, after stepwise selection
Linear regression LVMI Age* −0.48±0.33 0.15
Systolic blood pressure* −0.24±0.26 0.36
Aortic orifice area* −13.84±7.11 0.0611
Normalized flow displacement, S3
195.40±65.82 0.0058
Linear regression RWM Age* −0.003±0.005 0.50
Systolic blood pressure* 0.002±0.003 0.55
Aortic orifice area* −0.28±0.10 0.0058
Normalized flow displacement, S3
2.01±0.87 0.0283
WSSpeak
, S2
−0.29±0.15 0.0691
Logistic regression LV remodeling Age* 0.05±0.04 0.27
Systolic blood pressure* 0.004±0.03 0.87
Aortic orifice area* −2.27±0.97 0.0195
In univariate models, only significant associations (P<0.05) are shown. LVMI indicates left ventricular mass index; RWM, relative wall mass; and WSS
peak, peak systolic wall shear stress.
*Parameter forced into the model.
by guest on July 10, 2017http://circim
aging.ahajournals.org/D
ownloaded from

9 von Knobelsdorff-Brenkenhoff et al Aortic Blood Flow in Aortic Stenosis
2. Joint Task Force on the Management of Valvular Heart Disease of the European Society of C, European Association for Cardio-Thoracic Surgery (EACTS), Vahanian A, Alfieri O, Andreotti F, Antunes MJ, Baron-Esquivias G, Baumgartner H, Borger MA, Carrel TP, De Bonis M, Evangelista A, Falk V, Iung B, Lancellotti P, Pierard L, Price S, Schafers HJ, Schuler G, Stepinska J, Swedberg K, Takkenberg J, Von Oppell UO, Windecker S, Zamorano JL, Zembala M. Guidelines on the management of valvular heart disease (version 2012). Eur Heart J. 2012; 33:2451–2496.
3. Dweck MR, Joshi S, Murigu T, Gulati A, Alpendurada F, Jabbour A, Maceira A, Roussin I, Northridge DB, Kilner PJ, Cook SA, Boon NA, Pepper J, Mohiaddin RH, Newby DE, Pennell DJ, Prasad SK. Left ventric-ular remodeling and hypertrophy in patients with aortic stenosis: insights from cardiovascular magnetic resonance. J Cardiovasc Magn Reson. 2012;14:50. doi: 10.1186/1532-429X-14-50.
4. Dweck MR, Boon NA, Newby DE. Calcific aortic stenosis: a disease of the valve and the myocardium. J Am Coll Cardiol. 2012;60:1854–1863. doi: 10.1016/j.jacc.2012.02.093.
5. Cioffi G, Faggiano P, Vizzardi E, Tarantini L, Cramariuc D, Gerdts E, de Simone G. Prognostic effect of inappropriately high left ventricular mass in asymptomatic severe aortic stenosis. Heart. 2011;97:301–307. doi: 10.1136/hrt.2010.192997.
6. Gerdts E, Rossebø AB, Pedersen TR, Cioffi G, Lønnebakken MT, Cramariuc D, Rogge BP, Devereux RB. Relation of left ventricular mass to prognosis in initially asymptomatic mild to moderate aortic valve steno-sis. Circ Cardiovasc Imaging. 2015;8:e003644; discussion e003644. doi: 10.1161/CIRCIMAGING.115.003644.
7. Hess OM, Villari B, Krayenbuehl HP. Diastolic dysfunction in aortic ste-nosis. Circulation. 1993;87:IV73–76.
8. Paulus WJ, van Ballegoij JJ. Treatment of heart failure with normal ejec-tion fraction: an inconvenient truth! J Am Coll Cardiol. 2010;55:526–537. doi: 10.1016/j.jacc.2009.06.067.
9. Ng AC, Delgado V, Bertini M, Antoni ML, van Bommel RJ, van Rijnsoever EP, van der Kley F, Ewe SH, Witkowski T, Auger D, Nucifora G, Schuijf JD, Poldermans D, Leung DY, Schalij MJ, Bax JJ. Alterations in multi-directional myocardial functions in patients with aortic stenosis and pre-served ejection fraction: a two-dimensional speckle tracking analysis. Eur Heart J. 2011;32:1542–1550. doi: 10.1093/eurheartj/ehr084.
10. Shah AS, Chin CW, Vassiliou V, Cowell SJ, Doris M, Kwok TC, Semple S, Zamvar V, White AC, McKillop G, Boon NA, Prasad SK, Mills NL, Newby DE, Dweck MR. Left ventricular hypertrophy with strain and aortic stenosis. Circulation. 2014;130:1607–1616. doi: 10.1161/CIRCULATIONAHA.114.011085.
11. Chin CW, Shah AS, McAllister DA, Joanna Cowell S, Alam S, Langrish JP, Strachan FE, Hunter AL, Maria Choy A, Lang CC, Walker S, Boon NA, Newby DE, Mills NL, Dweck MR. High-sensitivity troponin I concentra-tions are a marker of an advanced hypertrophic response and adverse out-comes in patients with aortic stenosis. Eur Heart J. 2014;35:2312–2321. doi: 10.1093/eurheartj/ehu189.
12. Dweck MR, Joshi S, Murigu T, Alpendurada F, Jabbour A, Melina G, Banya W, Gulati A, Roussin I, Raza S, Prasad NA, Wage R, Quarto C, Angeloni E, Refice S, Sheppard M, Cook SA, Kilner PJ, Pennell DJ, Newby DE, Mohiaddin RH, Pepper J, Prasad SK. Midwall fi-brosis is an independent predictor of mortality in patients with aor-tic stenosis. J Am Coll Cardiol. 2011;58:1271–1279. doi: 10.1016/j.jacc.2011.03.064.
13. Azevedo CF, Nigri M, Higuchi ML, Pomerantzeff PM, Spina GS, Sampaio RO, Tarasoutchi F, Grinberg M, Rochitte CE. Prognostic significance of myocardial fibrosis quantification by histopathology and magnetic reso-nance imaging in patients with severe aortic valve disease. J Am Coll Cardiol. 2010;56:278–287. doi: 10.1016/j.jacc.2009.12.074.
14. Barker AJ, van Ooij P, Bandi K, Garcia J, Albaghdadi M, McCarthy P, Bonow RO, Carr J, Collins J, Malaisrie SC, Markl M. Viscous energy loss in the presence of abnormal aortic flow. Magn Reson Med. 2014;72:620–628. doi: 10.1002/mrm.24962.
15. Kheradvar A, Pedrizzetti G. Vortex formation in the cardiovascular sys-tem. Springer-Verlag; 2012.
16. Markl M, Kilner PJ, Ebbers T. Comprehensive 4D velocity mapping of the heart and great vessels by cardiovascular magnetic resonance. J Cardiovasc Magn Reson. 2011;13:7. doi: 10.1186/1532-429X-13-7.
17. Barker AJ, Markl M, Bürk J, Lorenz R, Bock J, Bauer S, Schulz-Menger J, von Knobelsdorff-Brenkenhoff F. Bicuspid aortic valve is associated with altered wall shear stress in the ascending aorta. Circ Cardiovasc Imaging. 2012;5:457–466. doi: 10.1161/CIRCIMAGING.112.973370.
18. Bauer S, Markl M, Föll D, Russe M, Stankovic Z, Jung B. K-t GRAPPA accelerated phase contrast MRI: Improved assessment of blood flow and 3-directional myocardial motion during breath-hold. J Magn Reson Imaging. 2013;38:1054–1062. doi: 10.1002/jmri.24077.
19. von Knobelsdorff-Brenkenhoff F, Trauzeddel RF, Barker AJ, Gruettner H, Markl M, Schulz-Menger J. Blood flow characteristics in the as-cending aorta after aortic valve replacement–a pilot study using 4D-flow MRI. Int J Cardiol. 2014;170:426–433. doi: 10.1016/j.ijcard.2013.11.034.
20. Dyverfeldt P, Bissell M, Barker AJ, Bolger AF, Carlhäll CJ, Ebbers T, Francios CJ, Frydrychowicz A, Geiger J, Giese D, Hope MD, Kilner PJ, Kozerke S, Myerson S, Neubauer S, Wieben O, Markl M. 4D flow car-diovascular magnetic resonance consensus statement. J Cardiovasc Magn Reson. 2015;17:72. doi: 10.1186/s12968-015-0174-5.
21. Stalder AF, Russe MF, Frydrychowicz A, Bock J, Hennig J, Markl M. Quantitative 2D and 3D phase contrast MRI: optimized analysis of blood flow and vessel wall parameters. Magn Reson Med. 2008;60:1218–1231. doi: 10.1002/mrm.21778.
22. Hope MD, Hope TA, Crook SE, Ordovas KG, Urbania TH, Alley MT, Higgins CB. 4D flow CMR in assessment of valve-related ascending aor-tic disease. JACC Cardiovasc Imaging. 2011;4:781–787. doi: 10.1016/j.jcmg.2011.05.004.
23. Sigovan M, Hope MD, Dyverfeldt P, Saloner D. Comparison of four-di-mensional flow parameters for quantification of flow eccentricity in the as-cending aorta. J Magn Reson Imaging. 2011;34:1226–1230. doi: 10.1002/jmri.22800.
24. Friedrich MG, Schulz-Menger J, Poetsch T, Pilz B, Uhlich F, Dietz R. Quantification of valvular aortic stenosis by magnetic resonance imaging. Am Heart J. 2002;144:329–334.
25. von Knobelsdorff-Brenkenhoff F, Rudolph A, Wassmuth R, Abdel-Aty H, Schulz-Menger J. Aortic dilatation in patients with prosthetic aortic valve: comparison of MRI and echocardiography. J Heart Valve Dis. 2010;19:349–356.
26. Maceira AM, Prasad SK, Khan M, Pennell DJ. Normalized left ven-tricular systolic and diastolic function by steady state free preces-sion cardiovascular magnetic resonance. J Cardiovasc Magn Reson. 2006;8:417–426.
27. Jonckheere AR. A distribution-free kappa-sample test against ordered al-ternatives. Biometrika. 1954; 41:133–145.
28. Bürk J, Blanke P, Stankovic Z, Barker A, Russe M, Geiger J, Frydrychowicz A, Langer M, Markl M. Evaluation of 3D blood flow pat-terns and wall shear stress in the normal and dilated thoracic aorta us-ing flow-sensitive 4D CMR. J Cardiovasc Magn Reson. 2012;14:84. doi: 10.1186/1532-429X-14-84.
29. van Ooij P, Garcia J, Potters WV, Malaisrie SC, Collins JD, Carr JC, Markl M, Barker AJ. Age-related changes in aortic 3d blood flow veloci-ties and wall shear stress: implications for the identification of altered hemodynamics in patients with aortic valve disease [published online ahead of print October 19, 2015]. J Magn Reson Imaging. doi: 10.1002/jmri.25081.
30. Drazner MH. The progression of hypertensive heart disease. Circulation. 2011;123:327–334. doi: 10.1161/CIRCULATIONAHA.108.845792.
31. Mahadevia R, Barker AJ, Schnell S, Entezari P, Kansal P, Fedak PW, Malaisrie SC, McCarthy P, Collins J, Carr J, Markl M. Bicuspid aortic cusp fusion morphology alters aortic three-dimensional outflow patterns, wall shear stress, and expression of aortopathy. Circulation. 2014;129:673–682. doi: 10.1161/CIRCULATIONAHA.113.003026.
32. Briand M, Dumesnil JG, Kadem L, Tongue AG, Rieu R, Garcia D, Pibarot P. Reduced systemic arterial compliance impacts significantly on left ven-tricular afterload and function in aortic stenosis: implications for diagno-sis and treatment. J Am Coll Cardiol. 2005;46:291–298. doi: 10.1016/j.jacc.2004.10.081.
33. Hope MD, Dyverfeldt P, Acevedo-Bolton G, Wrenn J, Foster E, Tseng E, Saloner D. Post-stenotic dilation: evaluation of ascending aortic dila-tion with 4D flow MR imaging. Int J Cardiol. 2012;156:e40–e42. doi: 10.1016/j.ijcard.2011.08.018.
34. Guzzardi DG, Barker AJ, van Ooij P, Malaisrie SC, Puthumana JJ, Belke DD, Mewhort HE, Svystonyuk DA, Kang S, Verma S, Collins J, Carr J, Bonow RO, Markl M, Thomas JD, McCarthy PM, Fedak PW. Valve-related hemodynamics mediate human bicuspid aortopathy: insights from wall shear stress mapping. J Am Coll Cardiol. 2015;66:892–900. doi: 10.1016/j.jacc.2015.06.1310.
35. Lorenz R, Bock J, Barker AJ, von Knobelsdorff-Brenkenhoff F, Wallis W, Korvink JG, Bissell MM, Schulz-Menger J, Markl M. 4D flow magnetic
by guest on July 10, 2017http://circim
aging.ahajournals.org/D
ownloaded from

10 von Knobelsdorff-Brenkenhoff et al Aortic Blood Flow in Aortic Stenosis
CLINICAL PERSPECTIVEAortic orifice area and blood flow velocity are sometimes considered incomplete to characterize the stress for the left ven-tricle caused by aortic stenosis, which is highly variable and leads to a broad range of ventricular impairment. Unfavorable left ventricular remodeling is an important prognostic factor and contributes significantly to the development of heart failure in patients with aortic stenosis. There are many attempts to better characterize the myocardial stress provoked by aortic stenosis. In this study, 4-dimensional flow magnetic resonance imaging was used to characterize the poststenotic blood flow in the ascending aorta, which is suspected to influence ventricular afterload and therefore ventricular remodeling. The aortic blood flow pattern in aortic stenosis was completely different when compared with healthy controls. Vortical and helical flow formations were more prevalent, the lower the orifice area was. Also, the peak blood flow velocity was more eccentric and the flow displacement higher in patients with aortic stenosis, and the wall shear stress elevated and asymmetrically distributed. In addition to aortic orifice area, flow displacement, which quantitatively describes the blood flow eccentricity, was associated with markers of left ventricular remodeling. These results are preliminary, but are hypothesis-generating and should stimulate future trials about the interplay of valvular disease, myocardial impairment, and blood flow to comprehen-sively characterize aortic valve disease.
resonance imaging in bicuspid aortic valve disease demonstrates altered distribution of aortic blood flow helicity. Magn Reson Med. 2014;71:1542–1553. doi: 10.1002/mrm.24802.
36. Morbiducci U, Ponzini R, Rizzo G, Cadioli M, Esposito A, De Cobelli F, Del Maschio A, Montevecchi FM, Redaelli A. In vivo quantification of helical blood flow in human aorta by time-resolved three-dimension-al cine phase contrast magnetic resonance imaging. Ann Biomed Eng. 2009;37:516–531. doi: 10.1007/s10439-008-9609-6.
37. Binter C, Gulan U, Holzner M, Kozerke S. On the accuracy of viscous and turbulent loss quantification in stenotic aortic flow using phase-contrast
MRI [published online ahead of print August 10, 2015]. Magn Reson Med. doi: 10.1002/mrm.25862.
38. Casas B, Lantz J, Dyverfeldt P, Ebbers T. 4d flow MRI-based pressure loss estimation in stenotic flows: Evaluation using numerical simulations [published online ahead of print May 28, 2015]. Magn Reson Med. doi: 10.1002/mrm.25772.
39. Cibis M, Jarvis K, Markl M, Rose M, Rigsby C, Barker AJ, Wentzel JJ. The effect of resolution on viscous dissipation measured with 4D flow MRI in pa-tients with Fontan circulation: evaluation using computational fluid dynamics. J Biomech. 2015;48:2984–2989. doi: 10.1016/j.jbiomech.2015.07.039.
by guest on July 10, 2017http://circim
aging.ahajournals.org/D
ownloaded from

Alex J. Barker, Edyta Blaszczyk, Michael Markl and Jeanette Schulz-MengerFlorian von Knobelsdorff-Brenkenhoff, Achudhan Karunaharamoorthy, Ralf Felix Trauzeddel,
Association With Left Ventricular RemodelingEvaluation of Aortic Blood Flow and Wall Shear Stress in Aortic Stenosis and Its
Print ISSN: 1941-9651. Online ISSN: 1942-0080 Copyright © 2016 American Heart Association, Inc. All rights reserved.
Dallas, TX 75231is published by the American Heart Association, 7272 Greenville Avenue,Circulation: Cardiovascular Imaging
doi: 10.1161/CIRCIMAGING.115.0040382016;9:e004038Circ Cardiovasc Imaging.
http://circimaging.ahajournals.org/content/9/3/e004038World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circimaging.ahajournals.org//subscriptions/
is online at: Circulation: Cardiovascular Imaging Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer information about this process is available in the
requested is located, click Request Permissions in the middle column of the Web page under Services. FurtherCenter, not the Editorial Office. Once the online version of the published article for which permission is being
can be obtained via RightsLink, a service of the Copyright ClearanceCirculation: Cardiovascular Imagingin Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on July 10, 2017http://circim
aging.ahajournals.org/D
ownloaded from