Embed Size (px)
Citation preview

Ventricular Arrhythmias and
Sudden Cardiac Death
Department of Cardiology,
Arcispedale S. Anna
University of Ferrara
Matteo Bertini, MD, PhD

No conflict of interest to
declare

One of the most common causes of death:
Sudden Cardiac Arrest Statistics
• High recurrence rate
• Last ESC guidelines 2006
<5%400,0003W. Europe
5%450,0002U.S.
<1%3,000,0001Worldwide
SurvivalIncidence(cases/year)

Priori et al Eur Heart J 2015

Structure of the guidelines
18 members of Task Force
• 14 sections
• 74 peer reviewers
• 810 references
• Guidelines reviewed concerning prevention of SCD are listed in Web Table

• Less than 5% of the patients will survive an episode of SCD
• The focus is on prevention! (for potential victims or family members!)

Cardiovascular Mortality: 17 million deaths every year in the world
SCD(25%)
Non SCD

Arrhythmia and SCD
Albert CM. Circulation. 2003;107:2096-2101.
12%Other Cardiac
Cause
88%Arrhythmic
Cause
Importance and relevance
The risk of SCD is:
1. higher in men than in women,
2. increases with age due to the higher prevalence of CAD in older age.

Importance and relevance
Cardiac diseases associated with SCD differ in young vs. older individuals
– Young: channelopathies, cardiomyopathies, myocarditis and substance abuse
– Older: chronic degenerative diseases, such as CAD, valvular heart diseases and HF, predominate.
What’s hot and what’s not …
• Not much new data in ICD and ischemic heart disease and HF, as no new trial has been performed
• Currently available anti-arrhythmic drugs have not been shown in RCTs, to be effective in primary management of patients with life-threatening VA or in prevention of SCD, while each drug has a significant potential for causing adverse events, including pro-arrhythmia.

What’s hot and what’s not …
• The screening of families in which there is a sudden death.
• For the first time, recommendations on the wearable and SICD.
• Good discussion on whether LBBB / non-LBBB morphologies are important discriminators or if the absolute QRS duration is most important.
– Recommendations on the use of CRT for the primary prevention of SCD are provided, according to the NYHA of the patient and the presence of sinus rhythm vs. atrial fibrillation.
• Sections on cardiomyopathies and channellopathies.

3.2 Indications for autopsy and
molecular autopsy in sudden death
victims
The Guidelines have a well developed section of screening of families in which there is a sudden death, as well as the workup of patients at high risk.
Indications for autopsy and molecular autopsy in sudden death victims are also detailed.
For 1st time- DNA analysis should be a fundamental component of post mortem assessment in SD victims, especially in young


Diagnostic workup in patients
presenting with
sustained VT or VF



4.3 DEVICE THERAPY


New!

6. Therapies for patients with left ventricular dysfunction with or without heart failure

6. Therapies for patients with left ventricular dysfunction with or without heart failure
CRT for prevention of SCD Recommendation Class I for• LVEF < 35%, • LBBB• QRS d > 120 ms.

Inherited primary arrhythmia syndromes

Inherited primary arrhythmia syndromes
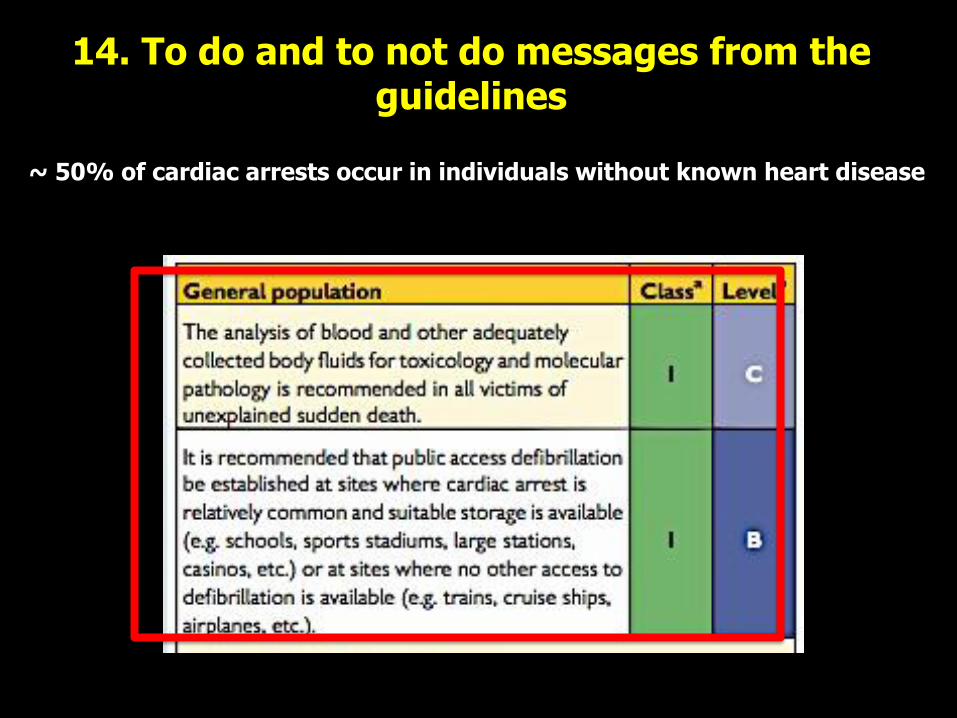
14. To do and to not do messages from the guidelines
~ 50% of cardiac arrests occur in individuals without known heart disease
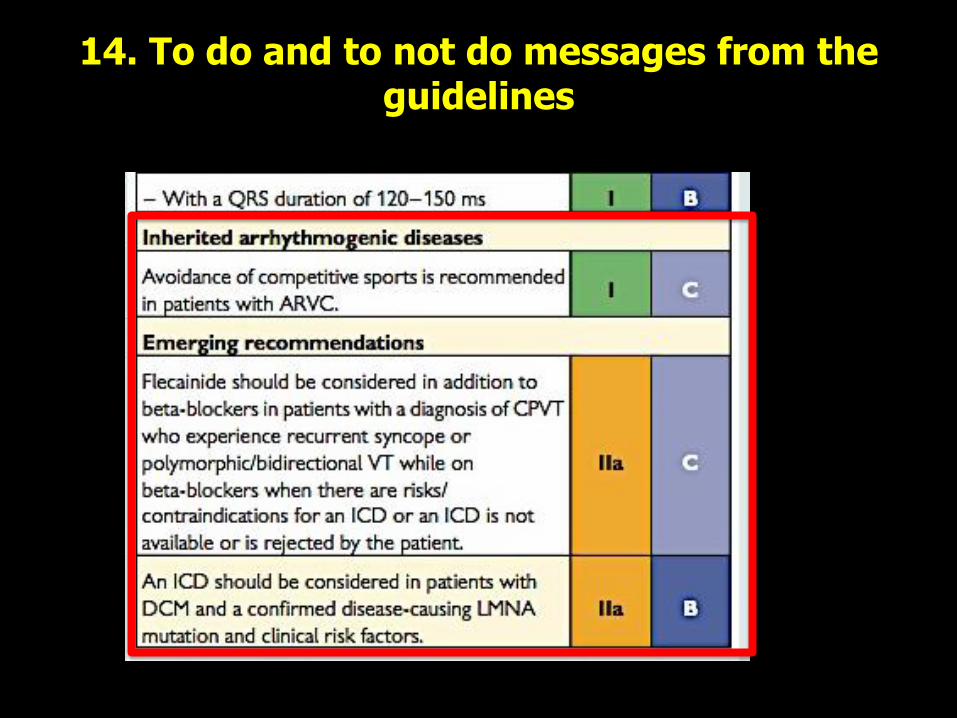
14. To do and to not do messages from the guidelines

Priori et al Eur Heart J doi:10.1093/eurheartj/ehv316

Thanks!





























