Embed Size (px)
Citation preview
Viral Hepatitis in Pregnancy
Assoc.Prof.Pawin Puapornpong
Epidemiology
Hepatitis is the most serious Liver Disease
encountered in Pregnancy woman
There are at least 5 distinct types A , B , C
, D ( Delta Agent ) and E
Hepatitis A
Infectious Hepatitis
Cause by Human RNA Piconarvirus
Epidemiology
World wide
Low Socioeconomic
Poor Hygiene
Transmission via Fecal – Oral Route
Incubation Period 2 – 7 wks
Hepatitis A – Clinical Manifestration
Sign & Symptom aren’t specific , may present as :-
N / V
Headache
Malaise
Low grade Fever is more common with Hepatitis A
More common if there is underlying chronic
Hepatitis C
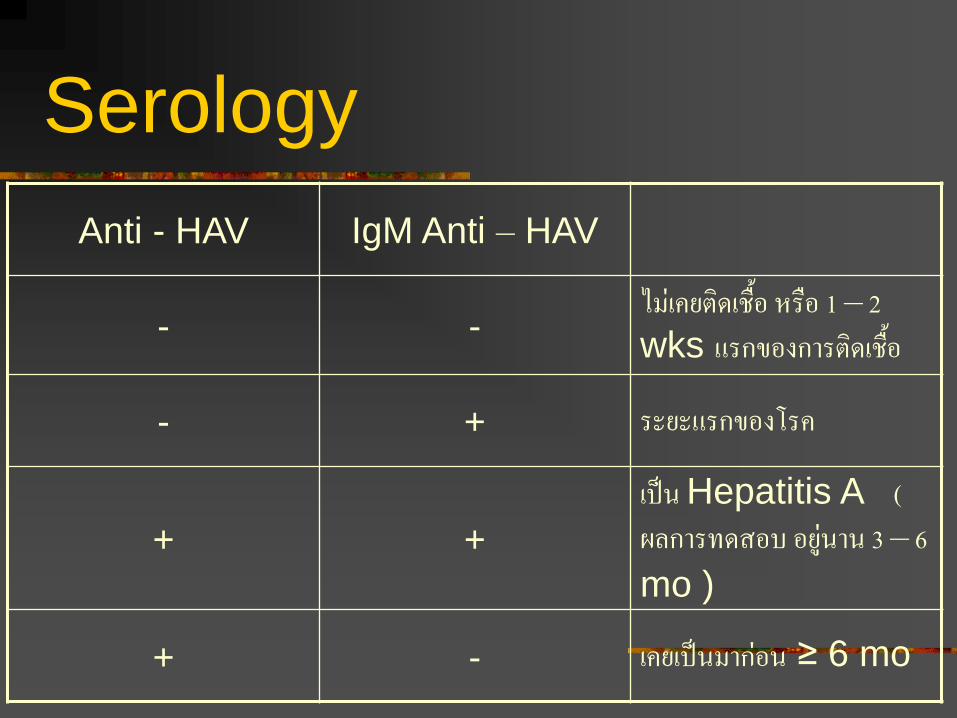
Serology
Anti - HAV IgM Anti – HAV
- - ไมเคยตดเชอ หรอ 1 – 2 wks แรกของการตดเชอ
- + ระยะแรกของโรค
+ +
เปน Hepatitis A ( ผลการทดสอบ อยนาน 3 – 6 mo )
+ - เคยเปนมากอน ≥ 6 mo
Hepatitis A And Pregnancy
Effect on pregnancy aren’t Dramatic
Both Perinatal and Maternal Death are
substantially increase
No evidence that HAV is teratogenicI
Increase Risk of preterm birth
Rarely spread through placenta
Management
ปองกนทวไป เหมอนผปวยทไมไดตงครรภ
ปองกนจ าเพาะ Passive Immunoprophylaxis
ISG
Passive Antibody จะคอยๆ ลดลงภายในขวบปแรกของทารก
ISG ประสทธภาพขนอยกบ
ปรมาณทให ขนาดของ ISG
ขนาดของ Anti – HAV
ระยะเวลาทสมผสโรคมา
อยได 3 mo
ขนาด 0.02 – 0.05 mg / kg IM ใหในรายทสมผสเชอ HAV หรออยในทองถนทมโรคชกชม หรอในสตรตงครรภ
การม Acute Hepatitis A ในระยะคลอด อาจให ISG แกทารก 0.5 ml IM
Hepatitis B
DNA – Virus
Serum Hepatitis
Epidemiology
World wide spreading but especially in
Asia and Africa
More Severe than A type
HBsAg
พบไดในสารคดหลงทกชนดของรางกาย โดยมปรมาณและความเขมขนแตกตางกนออกไป
สามารถตดตอไดทกทาง เชน การกน , SI , รอยแผล , มารดาสทารก
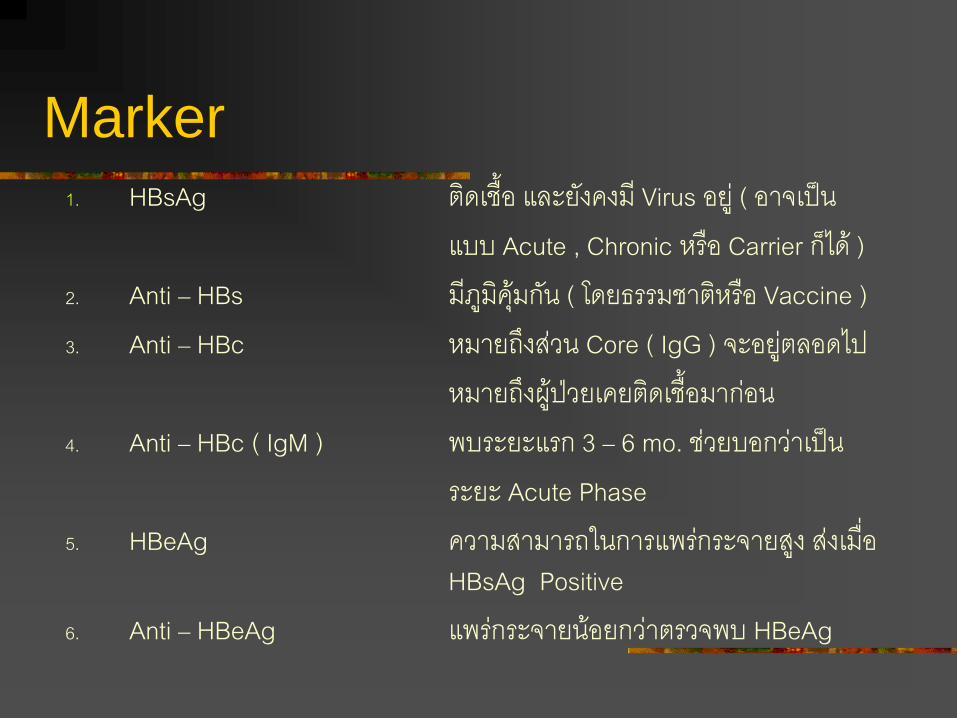
Marker 1. HBsAg ตดเชอ และยงคงม Virus อย ( อาจเปน แบบ Acute , Chronic หรอ Carrier กได ) 2. Anti – HBs มภมคมกน ( โดยธรรมชาตหรอ Vaccine ) 3. Anti – HBc หมายถงสวน Core ( IgG ) จะอยตลอดไป หมายถงผปวยเคยตดเชอมากอน 4. Anti – HBc ( IgM ) พบระยะแรก 3 – 6 mo. ชวยบอกวาเปน ระยะ Acute Phase 5. HBeAg ความสามารถในการแพรกระจายสง สงเมอ
HBsAg Positive 6. Anti – HBeAg แพรกระจายนอยกวาตรวจพบ HBeAg
Sign & Symptom
คลาย Hepatitis A
Sign & Symptom aren’t specific , may
present as :-
N / V
Headache
Malaise
ระยะ Prodrome และการตดเชอระยะแรกยาวนานกวามาก
Mode of Transmission
Transplacental viral transfer from the mother to
the fetus is associated with acute hepatitis but
not Chronic seropositivity. With acute infection in
the first Trimester ( 10 % of Fetus ) and up to 80
– 90 % of Fetus in Third Trimester
With Chronic maternal Infection, perinatal
transmission is by ingestion of infected material
during delivery or exposure subsequent to birth,
for example, Breast Feeding ( Less than Acute
Hepatitis )
Mode of Transmission
There are 3 Route to spread to Infant :-
Placenta ( Rare )
Intrapartum ( Common )
Postpartum Breast Feeding ( Maybe )
If infant present Antigen :-
within first 2 mo of Life ,so It is Congenital Infection
If 2 – 6 mo, It is Perinatal Infection
If more than 6 mo, It is postpartum Infectrion
Diagnosis
Clinical Manifestration
Liver Function Test
Marker
Clinical Manifestration
Acute Phase
Sign & Symptom
Jaundice
Incerase LFT
Present of HBsAg and HBeAg
2 – 3 % present by Fluminant Hepetitis
90 % is Fully recover
Clinical Manifestration
Chronic Phase
Carrier HBsAg Positive but asymptomatic
Persistent More common after Acute Hepatitis
Patient has Jaundice more than 2 mo
Active Prolong Rising LFT
Prolong presentation of HBsAg
Hepatitis B – In Thailand
If Mother is a Carrier then Infant 40 – 50 %
is Infected
When Male Infant Carrier grown up They
have 50 % chance to Death
15 % in Female infant
Management
1. คดกรองสตรตงครรภหาพาหะเรอรง ( ม HBsAg ) เพอปองกนการตดเชอไปทารก โดยให HB Immunoglobulin 0.06 mg / kg ( + Vaccine 3 ครง ท 0 , 1 และ 6 เดอน )
2. ชวยเหลอระยะคลอด โดยตองดดเมอกและเลอดออกจากปากทารกใหมากทสด ( การท า Cesarean Section ไมชวยลดโอกาสตดเชอของทารก )
3. การแยกมารดาและทารก ความสะอาดส าคญมากกวาการแยกทารกออกจากทารกอนๆ หรอแยกออกจากมารดา
Management
4. สามารถเลยงลกดวยนมมารดาได เนองจากน านมแมมปรมาณ Ag
ต ารวมกบถาแมเปนพาหะอย มารดากจะได HBIG รวมดวยเลย 5. ใหภมคมกนแกทารก เปน HBIG ทกรายทมารดาเปนพาหะ 3 ครง
คอตอนคลอด , 3 และ 6 เดอน จะชวยลดโอกาสตดเชอลงได ( 91
% เปน 23 % ) 6. การให Vaccine Hepatitis B แนะน าใหฉด Vaccine
รวมดวยทกราย แมวาจะได HBIG ไปแลวกตาม
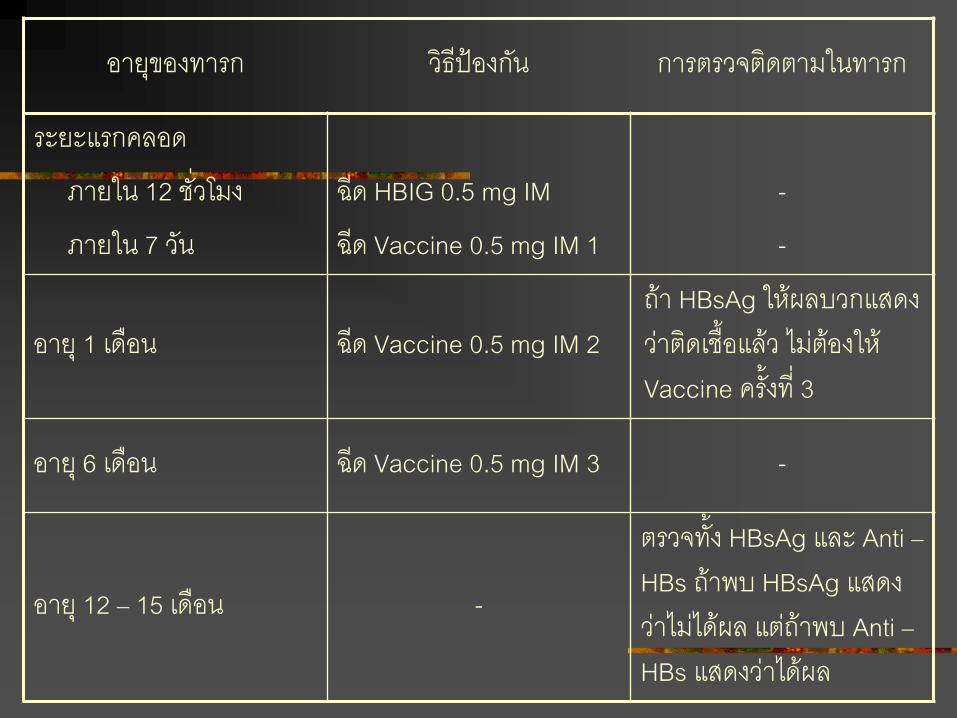
อายของทารก วธปองกน การตรวจตดตามในทารก
ระยะแรกคลอด
ภายใน 12 ชวโมง
ภายใน 7 วน
ฉด HBIG 0.5 mg IM
ฉด Vaccine 0.5 mg IM 1
-
-
อาย 1 เดอน ฉด Vaccine 0.5 mg IM 2 ถา HBsAg ใหผลบวกแสดงวาตดเชอแลว ไมตองให Vaccine ครงท 3
อาย 6 เดอน ฉด Vaccine 0.5 mg IM 3 -
อาย 12 – 15 เดอน -
ตรวจทง HBsAg และ Anti – HBs ถาพบ HBsAg แสดงวาไมไดผล แตถาพบ Anti – HBs แสดงวาไดผล

T
H
A
N
K
Y
O
U
F
O
R
Y
O
U
R
A
T
T
E
N
T
I
O
N