Embed Size (px)
Citation preview


Laboratory of Parasitology Faculty of Veterinary Medicine Department of
Virology, Parasitology and Immunology
Prevalence and zoonotic potential of
Cryptosporidium spp and Giardia duodenalis in
different host species in Greece
Despoina Kostopoulou
Promoters:
Prof. Dr. E. Claerebout
Dr. S. Sotiraki
Dissertation submitted in fulfillment of the requirements for the degree of
Doctor in Philosophy (PhD) in Veterinary Sciences.
2018
2
This research was funded by a grant of the State Scholarships
Foundation (IKY)

3
“Reach what you cannot”
N. Kazantzakis
4
To my parents
5
TABLE OF CONTENTS
List of abbreviations 8
Chapter 1. Literature review 11
Chapter I.1. Giardia spp 12
1.1 Introduction 12
1.2 Taxonomy 12
1.3 Morphology 14
1.4 Life cycle 15
1.5 Pathogenesis 16
1.6 Immunity 17
1.7 Giardiosis in dogs and cats 18
1.8 Giardiosis in ruminants 18
1.9 Giardiosis in horses 19
1.10 Giardiosis in humans 19
1.11 Diagnosis 22
1.12 Treatment 24
1.12.1 Dogs and cats 24
1.12.2 Ruminants 24
1.12.3 Horses 25
1.12.4 Humans 25
1.13 Epidemiology and zoonotic potential 25
Chapter I.2. Cryptosporidium spp 30
2.1 Introduction 30
2.2 Taxonomy 30
2.3 Morphology 32
2.4 Life cycle 32
2.5 Pathogenesis 33
2.6 Immunity 33
2.7 Cryptosporidiosis in dogs and cats 34
2.8 Cryptosporidiosis in ruminants 35
2.9 Cryptosporidiosis in horses 35
2.10 Cryptosporidiosis in pigs 35
2.11 Cryptosporidiosis in humans 36
2.12 Diagnosis 37
2.13 Treatment 38
2.13.1 Dogs and cats 38
2.13.2 Ruminants 39
2.13.3 Horses 39
2.13.4 Pigs 39
6
2.13.5 Humans 39
2.14 Epidemiology and zoonotic potential 39
Prevention of Giardia spp and Cryptosporidium spp infections 43
Spatio-temporal patterns in Giardia spp and Cryptosporidium spp infection 45
References 47
Objectives 65
References 68
Chapter 2. The occurrence and genetic characterization of Cryptosporidium and Giardia species in foals 69
in Belgium, The Netherlands, Germany and Greece
Introduction 70
Materials and Methods 71
Results 73
Discussion 76
References 79
Chapter 3. Abundance, zoonotic potential and risk factors of intestinal parasitism amongst dog and cat 87
populations: The scenario of Crete, Greece
Introduction 88
Materials and Methods 89
Results 93
Discussion 104
References 110
Chapter 4. Human enteric infections by parasites in Greece, with focus on Giardia and Cryptosporidium 119
Introduction 120
Materials and Methods 121
Results 123
Discussion 124
References 129
Chapter 5. General discussion 135
Introduction 136
Giardia and Cryptosporidium in animals 138
Giardia and Cryptosporidium in humans 140
Zoonotic transmission of Giardia? 142
Zoonotic transmission of Cryptosporidium? 144
Conclusions 145
Opportunities of future studies 147
References 150
7
Summary 159
Samenvatting 163
Acknowledgements 169
8
List of abbreviations
bg beta giardin
BSA bovine serum albumin
CD4+ cluster of differentiation 4
COWP cryptosporidium oocyst wall protein
CPG cysts per gram of faeces
DALYs disability-adjusted life years
DMSO dimethyl sulfoxide
DNA deoxyribonucleic acid
ef1a elongation factor 1 alpha
EIAs enzyme immunoassays
ELISA enzyme-linked immunosorbent assay
ESCCAP european scientific counsel companion animal parasites
gdh glutamate dehydrogenase
GLORF-C4 giardia lamblia open reading frame –C4
gp60 60-kDa glycoprotein
HIV human immunodeficiency virus
HSP70 70kDa heat shock protein
IFA immunofluorescence assay
IFN-γ γ-interferon
IgA immunoglobulin A
IgE immunoglobulin E
IgG immunoglobulin G
IgM immunoglobulin M
9
IL interleukin
ITS internal transcribed spacers of ribosomal DNA
miRNA micro ribonucleic acid
MLB mannose-binding lectin
MLG multilocus genotyping
NGS next generation sequencing
OPG oocysts per gram of faeces
PCR polymerase chain reaction
RNA ribonucleic acid
SIgA anti-Giardia secretory immunoglobulin A
SSU rRNA small subunit ribosomal RNA
TLR4 toll-like receptor 4
TNF-α tumor necrosis factor- α
TF-test Three Faecal test
tpi triose phosphate isomerase
vsp surface protein
WHO World Health Organization

Chapter I
Literature review

12
Worldwide the parasitic protozoa Giardia spp and Cryptosporidium spp are a major cause of
diarrhoea in humans and several animal species. The last few decades a public health concern
referring to these protozoa has arisen, not only for the significance of the infection they cause to
their hosts, but mainly for their routes of transmission and their potential zoonotic risk. In this
context, in the text to follow, we aimed to present an up-to-date literature review providing
critical information that deals with those parasites and the disease they cause in both animals
and humans; focusing especially on their epidemiology and zoonotic potential which were
analysed in greater depth.
CHAPTER I.1. Giardia spp
1.1 Introduction
The genus Giardia is a single-celled protistan parasite which comprises many species that inhabit
the intestinal tract of a series of vertebrate hosts including humans, domestic animals, rodents
and wildlife. However, one species, Giardia duodenalis (synonymous with G. intestinalis and G.
lamblia), is known to infect and cause giardiosis in humans and mammals, suggesting a zoonotic
transmission (Di Genova and Tonelli, 2016).
Although Giardia was first observed in 1681 by Antonie van Leeuwenhoek, the first detailed
description of this protist was not published until 1859 and its zoonotic significance was
controversial until the World Health Organization (WHO) recognized it as a zoonotic agent in
1979 (Abeywardena et al. 2015).
1.2 Taxonomy
According to Plutzer et al., 2010, Giardia’s taxonomy is as follows:
Phylum: Metamonada
Subphylum: Trichozoa
Superclass: Eopharyngia
Class: Trepomonadea
Subclass: Diplozoa
Order: Giardiida
Family: Giardiidae
13
Giardia
Species Major hosts
G. duodenalis (= Assemblage A) Humans and other primates, dogs, cats,
livestock, rodents and other wild mammals
G. enterica (= Assemblage B) Humans, ruminants and other hoofed livestock, dogs, rabbits, marsupials, marine mammals, rodents, ferrets, rock hyrax, non-human primates, chicken, ostrich, gull
G. canis (= Assemblage C, D) Dogs
G. bovis (= Assemblage E) Cattle and other hoofed livestock
G. cati (= Assemblage F) Cats
G. simondi (= Assemblage G) Rats, mice
Assemblage H Marine mammals
G. agilis Amphibians
G. muris Rodents
G. psittaci Birds
G. ardeae Birds
G. microti Voles and muskrats
G. varani Lizzards
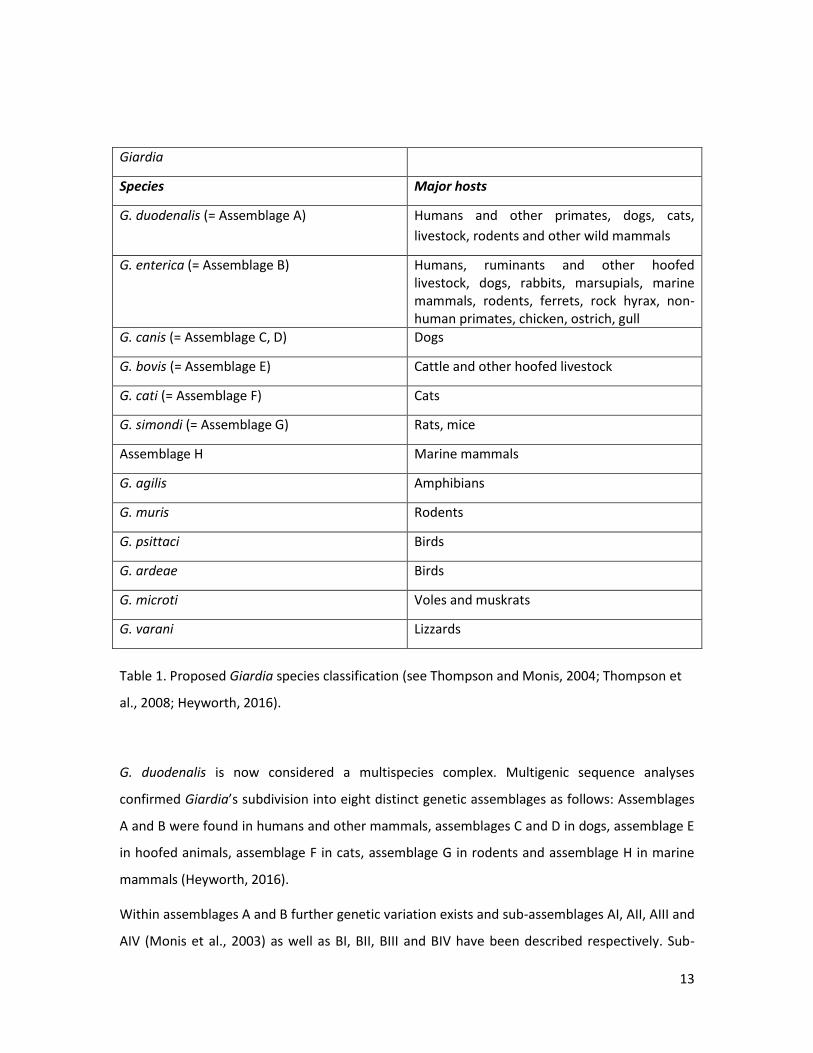
Table 1. Proposed Giardia species classification (see Thompson and Monis, 2004; Thompson et
al., 2008; Heyworth, 2016).
G. duodenalis is now considered a multispecies complex. Multigenic sequence analyses
confirmed Giardia’s subdivision into eight distinct genetic assemblages as follows: Assemblages
A and B were found in humans and other mammals, assemblages C and D in dogs, assemblage E
in hoofed animals, assemblage F in cats, assemblage G in rodents and assemblage H in marine
mammals (Heyworth, 2016).
Within assemblages A and B further genetic variation exists and sub-assemblages AI, AII, AIII and
AIV (Monis et al., 2003) as well as BI, BII, BIII and BIV have been described respectively. Sub-

14
assemblage AII has been isolated mainly from humans whereas AI, AIII and AIV have been found
mainly in animals. Similarly, sub-assemblages BIII and BIV have been described in human isolates
whereas BI and BII belonged to animals (Ryan and Caccio, 2013).
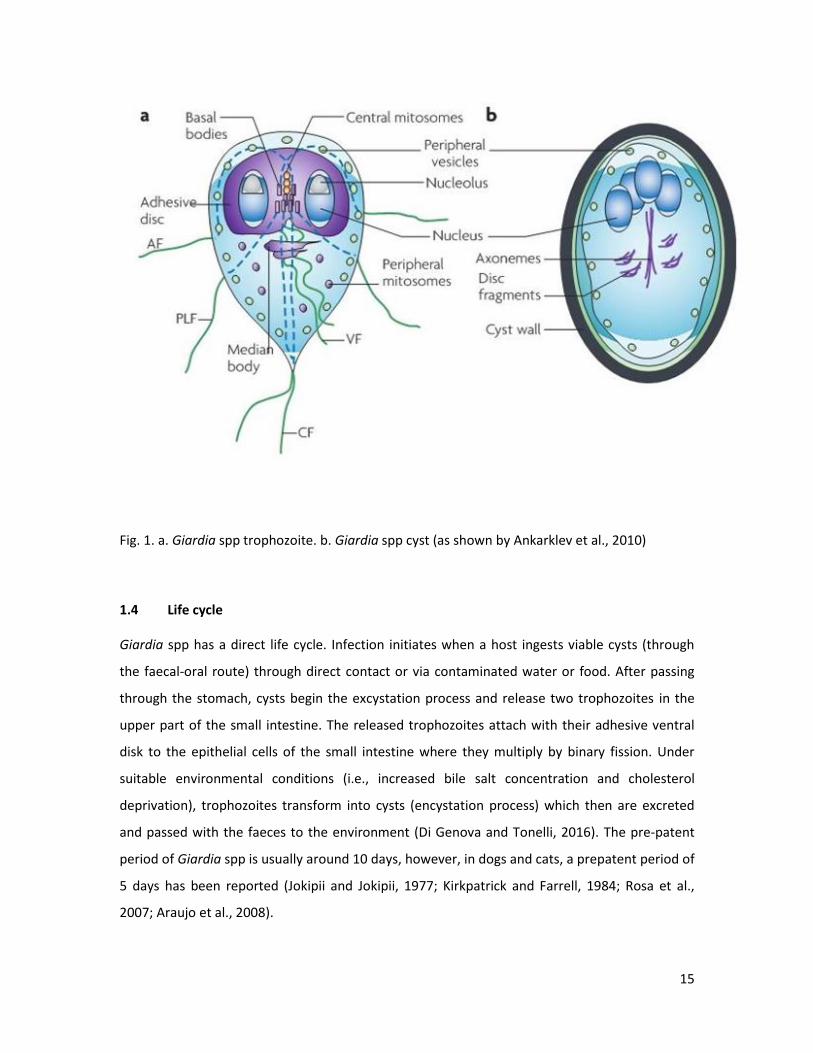
1.3 Morphology
Morphologically, Giardia consists of two stages: the motile one, the trophozoite and the non-
motile environmentally resistant stage, the cyst. Trophozoites are pear-shaped and are
approximately 12 to 15 μm long and 5 to 9 μm wide. Their cytoskeleton includes a median body,
four pairs of flagella (anterior, posterior, caudal and ventral), and a ventral adhesive disk with
which they attach to the intestinal wall, where they obtain the necessary nutrients and avoid
transport beyond the jejunum. They have two nuclei without nucleoli that are located at the
anterior part and are symmetric with respect to the long axis. Cysts are egg shaped,
approximately 5 by 7 to 10 μm in diameter and are covered by a wall that is 0.3 to 0.5 μm thick
and composed of an outer filamentous layer and an inner membranous layer with two
membranes. The internal portion includes two trophozoites with four nuclei, which are released
at the excystation phase. Cysts are excreted with the faeces to the environment where they can
survive for a long time period (Adam, 2001).
15
Fig. 1. a. Giardia spp trophozoite. b. Giardia spp cyst (as shown by Ankarklev et al., 2010)
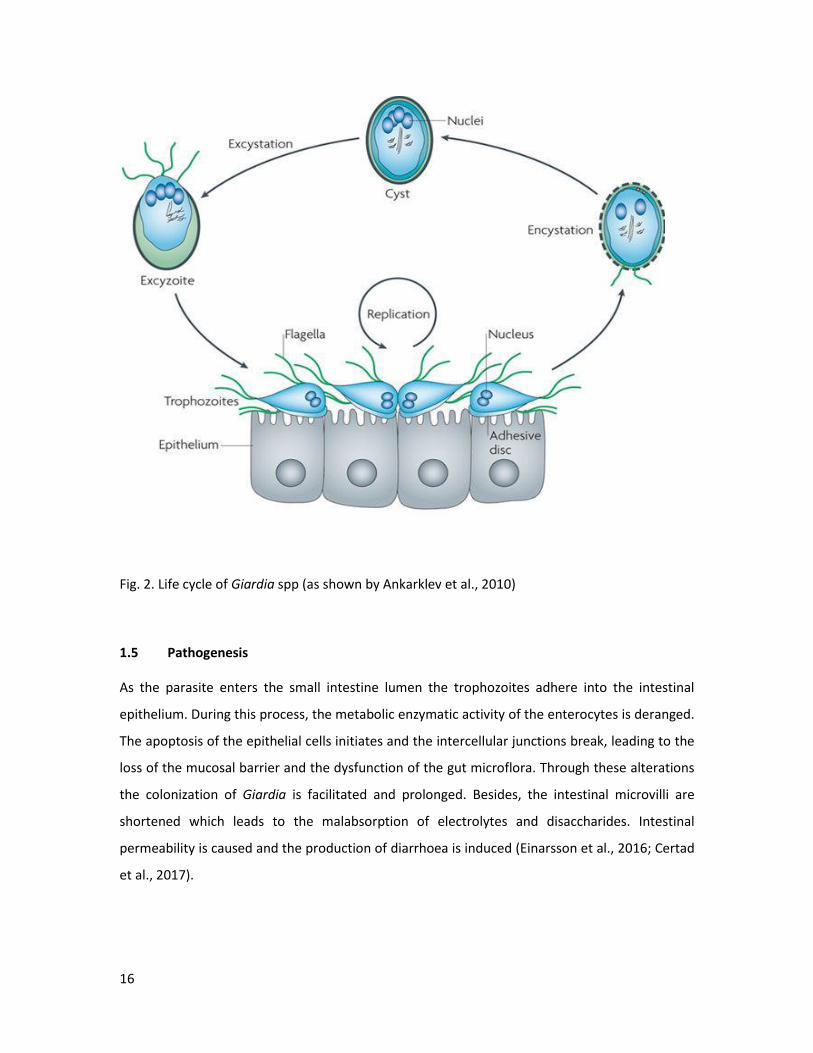
1.4 Life cycle
Giardia spp has a direct life cycle. Infection initiates when a host ingests viable cysts (through
the faecal-oral route) through direct contact or via contaminated water or food. After passing
through the stomach, cysts begin the excystation process and release two trophozoites in the
upper part of the small intestine. The released trophozoites attach with their adhesive ventral
disk to the epithelial cells of the small intestine where they multiply by binary fission. Under
suitable environmental conditions (i.e., increased bile salt concentration and cholesterol
deprivation), trophozoites transform into cysts (encystation process) which then are excreted
and passed with the faeces to the environment (Di Genova and Tonelli, 2016). The pre-patent
period of Giardia spp is usually around 10 days, however, in dogs and cats, a prepatent period of
5 days has been reported (Jokipii and Jokipii, 1977; Kirkpatrick and Farrell, 1984; Rosa et al.,
2007; Araujo et al., 2008).
16
Fig. 2. Life cycle of Giardia spp (as shown by Ankarklev et al., 2010)
1.5 Pathogenesis
As the parasite enters the small intestine lumen the trophozoites adhere into the intestinal
epithelium. During this process, the metabolic enzymatic activity of the enterocytes is deranged.
The apoptosis of the epithelial cells initiates and the intercellular junctions break, leading to the
loss of the mucosal barrier and the dysfunction of the gut microflora. Through these alterations
the colonization of Giardia is facilitated and prolonged. Besides, the intestinal microvilli are
shortened which leads to the malabsorption of electrolytes and disaccharides. Intestinal
permeability is caused and the production of diarrhoea is induced (Einarsson et al., 2016; Certad
et al., 2017).

17
1.6 Immunity
Despite a number of studies which provide valuable data about immune responses against
Giardia spp mainly based on studies in mice, still, host defense mechanisms against this parasite
have not been totally understood. Similarly to other infections, the composition of intestinal
microbiota can play a significant role in the establishment of giardiosis. Thus, enriched
commensal microbiota can either eliminate Giardia’s colonization by for instance, providing a
toxic environment to trophozoites or may have a protective role through the maintenance of
the gut integrity during infection (Lopez-Romero et al., 2015; Fink and Singer, 2017). Apart from
the mucus and the peristaltic movements of the intestine which constitute mechanical barriers
to trophozoites’ attachment, several cytokines or other proteins and compounds are produced
by the intestinal epithelial and immune cells during infection (Lopez-Romero et al., 2015). For
example, the release of antimicrobial peptides can reduce the number of G. muris trophozoites
or the increased production of nitric oxide inhibits the excystation process and also prevents the
G. duodenalis trophozoites’ multiplication (Lopez-Romero et al., 2015).
Not only innate defense mechanisms but also acquired humoral and cell-mediated immune
responses protect against Giardia infections (Faubert 2000), including CD4+ T cells and their
cytokines as well as B cells and their antibodies i.e. specific IgA or IgG (Abdul-Wahid and Faubert,
2008; Singer and Nash, 2000; Lopez-Romero et al., 2015). In fact, IgA is considered a major
contributor to protective immunity against giardiosis (Taherkhani et al., 2009; Grit et al., 2012)
with the anti-Giardia secretory IgA being detected in human saliva and breast milk (El-Gebaly et
al., 2012). Elimination of the parasite has been achieved in animal models at approximately 3-5
weeks post-infection via humoral immunity. Also, it has been reported that repeated infections
in both humans and animals lead to the development of immunity or to the display of less
severe clinical manifestations (Lopez-Romero et al., 2015). Besides, the IL-17 production by CD4+
T cells seems to play significant a role in the development of protective immunity against G.
duodenalis (Grit et al., 2014; Paerewijck et al., 2017). Specifically, Giardia infection upregulates
IL-17A cytokine which activates the IL-17RA gene and as a result induces the production of a
wide array of antimicrobial proteins and complement factors, which in combination with an
intestinal IgA response seems to be important to confer protection against Giardia (Paerewijck
et al., 2017).
18
1.7 Giardiosis in dogs and cats
Giardia is considered one of the most common intestinal parasites of dogs and cats in developed
countries (Palmer et al., 2008; Thompson et al., 2008; Claerebout et al., 2009; Scaramozzino et
al., 2009; Ballweber et al., 2010; Epe et al., 2010; Barutzki et al., 2011; Polak et al., 2014; Zanzani
et al., 2014; Osman et al., 2015; Pallant et al., 2015).
Prevalence rates for Giardia infection in dogs and cats vary substantially from one study to
another. The study population, the study area, the diagnostic method used and the health status
of the animal are factors which contribute to this variation. The prevalence rates most often
range between 5.0% and 15.0% in healthy or clinically ill dogs or cats (Tangtrongsup and Scorza,
2010) however, recent studies in Europe reported infection rates between 20.0% and 25.0% in
both species (Baneth et al., 2016).
Giardia infection is common in companion animals presented mainly as a sub-clinical,
asymptomatic disease. According to textbooks Giardia infections can cause chronic diarrhoea
and clinical manifestations similar to other species like abdominal pain, malodorous and soft to
watery diarrhoea (which can be self-limiting in immunocompetent animals), and weight loss.
The severity of such signs depends on several factors such as the Giardia assemblage, the
immune condition and the age of the animal, its’ lifestyle, physical stress, malnutrition and the
co-presence of other pathogens (Thompson et al., 2008; Tangtrongsup and Scorza, 2010; Tysnes
et al. 2014; Adell-Aledón et al. 2018). However, there are limited data proving that Giardia
infection was the main cause of diarrhoea in the infected animals (Westermarck, 2016).
1.8 Giardiosis in ruminants
Giardiosis is also common in ruminants. In both cattle and small ruminants (sheep and goats),
significant variability in the prevalence of Giardia is observed, depending on the age of the
animals, the housing, feeding and management practices as well as the diagnostic methods
used, reaching up to 100.0% infection in some cases (Robertson, 2009; Geurden et al., 2010a;
Feng and Xiao, 2011).
19
Young animals seem to be more susceptible to the disease (Geurden et al., 2010b; Abeywardena
et al., 2015). Infections are mostly asymptomatic but can be associated with mild diarrhoea and
ill thrift leading to production losses (Feng and Xiao, 2011; Abeywardena et al., 2015).
1.9 Giardiosis in horses
The prevalence of Giardia has been reported in horses from various locations with considerable
variation (0.5-35.0%) (Pavlasek et al., 1995; Olson et al., 1997; Atwill et al., 2000; De Souza et al.,
2009; Veronesi et al., 2010; Traversa et al., 2012; Santin et al., 2013).
Although the presence of this protozoan parasite in horses with diarrhoea has been reported
(Kirkpatrick and Skand, 1985), horses infected with Giardia rarely show any associated clinical
signs of diarrhoea, colic, lethargy and anorexia (Manahan, 1970; Santin et al., 2013).
As with other animals, foals seem to be more prone to infection (Xiao and Herd, 1994; Johnson
et al., 1997; Veronesi et al., 2010). However, there are studies which showed that the
prevalence of Giardia was not significantly associated with age (Olson et al., 1997; Santin et al.,
2013; Qi et al., 2015).
1.10 Giardiosis in humans
G.duodenalis is one of the most common human intestinal parasites. About 280 million people
are being infected every year (Lane and Lloyd, 2002). According to World Health Organisation
(WHO) estimates, in 2010, giardiosis had a burden of 171,100 disability-adjusted life years
(DALYs) (Kirk et al., 2015). Infection of humans by Giardia are reported globally, showing lower
rates in developed countries (ranging from 0.4% to 7.5%), compared to the ones in the
developing world where the infection rates can reach up to 30.0% (Feng and Xiao, 2011).
The parasite has been responsible for 37.0% of the waterborne disease outbreaks reported
during the last 6 years worldwide (Efstratiou et al., 2017). It is estimated that only in the United
States, 1.2 million cases of the disease and 3,581 hospitalizations occur annually (Scallan et al.,
2011). Besides, according to the Centres for Disease Control and Prevention, 242 outbreaks had
been reported from 1971 to 2011 in this country (Adam et al., 2016).
20
The disease is also present in Europe, with reported outbreaks in Nordic countries, the
Netherlands, Belgium, UK, and Greece (Hadjichristodoulou et al., 1998; Hardie et al., 1999;
Smith et al., 2006a; Braeye et al., 2015; Guzman-Herrador et al., 2015). In Denmark, Finland,
Norway and Sweden the prevalence in asymptomatic and symptomatic human populations was
estimated to be 3.0% (2.6-3.3) and 6.0% (5.3-6.3), respectively. It was also estimated that for
each registered Giardia clinical case, an estimated 867 unregistered symptomatic cases occur
annually, per 100,000 inhabitants in Finland, 634 in Norway, and 254 in Sweden (Escobedo et al.,
2014). In Germany, on average, 3,806 notified giardiosis cases (range 3,101-4,626) were
reported between 2001 and 2007, which corresponded to an average incidence of 4.6
cases/100,000 population. Much higher incidence rates were reported for some other countries.
In the Netherlands, there were 11,600 cases in 2004, corresponding to 69.9 cases/100,000
population (Baneth et al., 2016) whereas in Belgium the reported cases were 10.1/100,000
population (source EPISTAT, 2018).
Giardia is also considered to be the most common cause of acute diarrhoea in travellers mainly
those returning from developing countries (Lebbad et al., 2011; Gautret et al., 2012; Muhsen
and Levine, 2012; Broglia et al., 2013; Bartelt and Sartor, 2015).
For all the above reasons, WHO regards giardiosis a Neglected disease since 2004 (WHO, 2004;
Savioli et al., 2006).
Giardia infection is typically characterized by gastrointestinal symptoms including diarrhoea
(watery, fatty or mucous), bloating, abdominal cramps, nausea, vomiting, weight loss and
malabsorption (vitamins A and B12, d-xylose, iron and zinc as well as lactase deficiency in 20.0-
40.0% of symptomatic cases) but asymptomatic infections can also occur (Nash et al., 1987;
Huang and White, 2006; Robertson et al., 2010; Bartelt and Sartor, 2015). The first clinical signs
appear after 1-2 weeks of infection and vary from mild and self-limiting to severe with no
response to commonly applied treatment (Einarsson et al., 2016). In some cases, the host fails to
eradicate the parasite, which leads to a chronic infection (Feng and Xiao, 2011). Children and
immunodeficient patients are more vulnerable to clinical manifestations (Haliez and Buret,
2013; Soares and Tasca, 2016). However, children in developing countries seem to be protected
against symptomatic disease and specifically against acute diarrhoea, either because they
acquire immunity in their first weeks of age through breastfeeding, or due to malnutrition and
potentially to an already developed environmental enteropathy which makes their small
21
intestine characterized by hypercellularity (high numbers of lamina propria lymphocytes) and
bacterial overgrowth. It has been suggested that Giardia’s invasion may modulate the innate
immune system and mucosal environment to such extent that, partially, protection is also
offered against diarrhoea caused by other enteropathogens (Muhsen and Levine, 2012).
In various studies, the prevalence of Giardia infection has been found statistically significantly
higher among HIV seropositive patients compared to HIV seronegative patients, although there
are studies which support that HIV infection does not affect the frequency or severity of clinical
disease (Escobedo et al., 2014). It has been also reported that previous exposure to the parasite
seems to have a protective role and results in less serious manifestations (Halliez and Buret,
2013).
Furthermore, apart from the common symptoms, giardiosis may lead to post-infectious
complications such as irritable bowel syndrome, chronic fatigue, malnutrition and cognitive
impairment. Also extra-intestinal manifestations may be observed mostly as a result of
immunologic reaction, such as food allergy, urticaria, reactive arthritis, and inflammatory ocular
manifestations. These symptoms can manifest even without the presence of the parasite in the
intestine (Robertson et al., 2010; Wensaas et al., 2012; Naess et al., 2012; Halliez and Buret,
2013; Mørch et al., 2013; Bartelt and Sartor, 2015). However, the mechanisms responsible for
post-infectious and extra-intestinal manifestations in giardiosis remain obscure (Halliez and
Buret, 2013).
The broad spectrum of the clinical symptoms the disease shows could be attributed to various
factors. One of them is the difference in virulence among Giardia assemblages. Genotyping of G.
duodenalis isolates obtained from humans with Giardia infection has shown that assemblages A
and B are predominantly associated with human infections (Lebbad et al., 2011; Muhsen and
Levine, 2012; Heyworth, 2016), although there have been occasional reports of the isolation,
from human subjects, of G. duodenalis organisms that have genetic markers characteristic of
non-A, non-B, assemblages (Lebbad et al., 2011; Heyworth, 2016). However, the association
between clinical disease and the assemblage type is rather vague (Cotton et al., 2015; Einarsson
et al., 2016). Some studies reported that assemblage A isolates were more virulent than
assemblage B isolates. Assemblage A is often associated with the presence of symptoms, while
assemblage B is more often associated with asymptomatic infection (Feng and Xiao, 2011). On
the other hand, according to other studies, assemblage B isolates are linked to disease
22
appearance (Bartelt and Sartor, 2015). Some investigations support that assemblage A is
associated with intermittent diarrhoea whereas assemblage B with duodenal inflammation,
nausea and persistent symptoms (Feng and Xiao, 2011) as well as flatulence in children under 5
years of age (Lebbad et al., 2011). However, others claim that symptoms’ development does not
necessarily depend on Giardia’s strains (Lebbad et al., 2011), since even among family members
who share the same genotypes not all individuals developed symptoms (Lebbad et al., 2011).
The host nutritional status also influences the symptoms display. For example, protein energy
malnutrition, zinc deficiency and vitamin A deficiency may increase susceptibility to Giardia.
Besides, the parasite infective dose (in humans, ingestion of ten Giardia cysts has been shown to
cause infection), the age and the immunity status of the patient, possible co-existing infections
as well as the composition and function of resident microbiota contribute to the variability of
clinical manifestation of giardiosis (Lebbad et al., 2011; Bartelt and Sartor, 2015; Adam et al.,
2016).
1.11 Diagnosis
Over the years, several diagnostic techniques have been proposed for the diagnosis of Giardia
spp derived from either animals or humans. Traditionally, the identification of the parasite’s
trophozoites or cysts has been performed by microscopic examination of faeces through direct
smears or wet mounts.
Passive faecal flotation, sedimentation (acid/ether) technique, centrifugal faecal flotation (zinc
sulphate or sugar solutions are the most commonly used flotation liquids) and most recently IFA
(direct immunofluorescence assay) are the most common diagnostic methods used
(Tangtrongsup and Scorza, 2010; Koehler et al., 2014).
Among these procedures, IFA is considered the most sensitive assay for the detection of Giardia
spp (Gotfred-Rasmussen et al., 2016). It is a fluorescein-labeled monoclonal antibody system
that contains monoclonal antibodies that react with Cryptosporidium spp oocysts and Giardia
spp cysts (Tangtrongsup and Scorza 2010). The sensitivity and specificity of this test have been
evaluated through various studies in humans and in different animal species. According to the
manufacturer, sensitivity and specificity of IFA in human samples is estimated to 100.0% and
99.8% respectively (Tangtrongsup and Scorza, 2010). Immunofluorescence is considered the
23
reference standard assay for the detection of Giardia spp in dog and cat faeces (Tangtrongsup
and Scorza, 2010). Geurden et al., 2008b, have confirmed using a Bayesian approach, that IFA is
one of the most sensitive and specific tests for the detection of Giardia spp in dogs. Specifically,
they demonstrated 90.0% sensitivity and 94.0% specificity as well as 91.0% sensitivity and 94.0%
specificity in epidemiological and clinical studies respectively. Similarly in calves, IFA proved to
be a highly sensitive technique (Se=88.0%) and an ideal diagnostic key for clinical giardiosis
(Geurden et al., 2010a). However, in a previous study, ELISA was evaluated as the most sensitive
(Se=89.0%) but IFA as the most specific (Sp=95.0%) diagnostic technique for the detection of G.
duodenalis in dairy calves (Geurden et al., 2004).
Since IFA is a quite complicated technique and a time-consuming procedure which requires
expensive equipment (fluorescence microscope), it is mainly recommended for research needs
and not for routine diagnosis of giardiosis. For that reason, rapid tests (immunochromatographic
tests) are widely used although they are usually reported to be less sensitive. For example, in
dogs, their sensitivity has been evaluated in different studies to 48.0% and 67.0% (Geurden et
al., 2008b; Costa et al., 2016). In calves rapid tests demonstrated even lower sensitivity
estimated to 26.0% and 28.0% (Geurden et al., 2010a).
ELISA (enzyme-linked immunosorbent assay) is another commonly used assay which identifies
Giardia antigens in faeces. In calves, ELISA has been evaluated as a more sensitive (Se=89.0%)
but less specific (Sp=90.0%) technique compared to IFA (Geurden et al., 2004). Also in dogs,
ELISA is regarded as a useful diagnostic tool (Se =88.9% and Sp=95.8%) for the diagnosis of
giardiosis (Panini et al., 2013).
PCR assays are performed for the amplification of Giardia DNA in faeces (Koehler et al., 2014).
However, due to the presence of multiple PCR inhibitors in faecal material, DNA amplification
can be difficult, leading to false negative results (Tangtrongsup and Scorza 2010). Since there are
several genes which can be targeted through PCR [β-giardin (bg), triose phosphate isomerase
(tpi), glutamate dehydrogenase (gdh), the small subunit ribosomal RNA (SSU rRNA), elongation
factor 1 alpha (ef1a) gene, variable surface protein (vsp), the G. lamblia open reading frame –C4
(GLORF-C4) and the internal transcribed spacers (ITS) of ribosomal DNA] (Koehler et al., 2014),
the selection of the desirable genetic locus should be done based on the purpose of the use of
the method. For example, molecular techniques for diagnostic reasons usually focus on
multicopy genes like SSU-rDNA, so that high sensitivity is ensured, whereas for Giardia
24
assemblage determination more variable genes are used (Thompson and Ash, 2016). The
genetic markers with the highest polymorphism are tpi and gdh followed by bg and C4 (Caccio
and Ryan 2008). Besides, for more accurate differentiation and identification of the origin of the
assemblages (zoonotic or not), Multilocus Genotyping (MLG) should follow (Tangtrongsup and
Scorza, 2010; Feng and Xiao, 2011; Koehler et al., 2014).
1.12 Treatment
1.12.1 Dogs & Cats
Several drugs have been licensed for the treatment of giardiosis in companion animals. Of them,
benzimidazoles (albendazole, fenbendazole, oxfendazole), nitroimidazoles (metronidazole,
ronidazole), furazolidone and quinacrine have been used in dogs, whereas nitroimidazoles
(metronidazole, secnidazole), quinacrine and furazolidone have been indicated for Giardia
infections in cats (Thompson et al., 2008; Da Silva et al., 2011; Fiechter et al., 2012).
Together with chemotherapy, giardiosis can be effectively treated with the implementation of
dietary and environmental control measures. These measures include the addition of fibre to
the diet which can enrich the gut microbiota or inhibit the attachment of the parasite to
microvilli (Tangtrongsup and Scorza, 2010), and also the cleaning and disinfection of the
environment as well as the thorough shampooing of the animal in order to prevent re-infection
through contaminated environment or fur (Zajac et al., 1998; Payne et al., 2002; Geurden and
Olson, 2011).
1.12.2 Ruminants
Several compounds like fenbendazole (Geurden et al., 2006a), albendazole (O’Handley et al.,
2000; Xiao et al., 1996), and paromomycin (Geurden et al., 2006b) can be used for treatment of
giardiosis in calves.
Also in lambs, fenbendazole and secnidazole have been suggested as effective treatment
options against Giardia (Geurden et al., 2011; Ural et al., 2014).
Because only a low number of Giardia cysts is needed for infection (Caccio et al., 2005) and a
specific immune response against Giardia infection develops slowly in ruminants (Yanke et al.,
25
1998; O’Handley et al., 2003), it has been suggested that environmental disinfection in
combination with animal treatment is necessary (Xiao et al., 1996; O’ Handley et al., 2000;
Geurden et al., 2006a).
1.12.3 Horses
The administration of metronidazole suspension per os, is suggested for the treatment of
giardiosis in horses (Kirkpatrick and Skand, 1985).
1.12.4 Humans
Treatment of giardiosis in humans is based on various compounds such as nitroimidazoles
(metronidazole, tinidazole, secnidazole), benzimidazoles (albendazole, mebendazole),
quinacrine, nitazoxanide, furazolidone and paromomycin (Escobedo et al., 2016a) implemented
either alone or as a combined therapy (Escobedo et al., 2016b). However, the need for the
development of more effective and less toxic drugs against this protozoan parasite has aroused.
Recently, artemisinin and its derivatives have been suggested as an alternative treatment of
giardiosis in humans (Ni Loo et al., 2016).
1.13 Epidemiology and zoonotic potential
As mentioned above Giardia spp is highly abundant, worldwide distributed and is among the
most common intestinal parasitic infections of humans and animals. Since it has a direct life
cycle, faecal-oral transmission seems to be very common especially in individual cases. However,
regarding outbreaks, massive transmission occurs mainly through water and/or food (Adam et
al., 2016).
Infected hosts may excrete very high numbers of cysts (up to billions) each day (Robertson,
2009; Adam et al., 2016). Cysts are robust, moderately resistant to chlorine disinfection (Adam
et al., 2016) and can survive for weeks to months in the environment, especially in cool and
damp areas. In cattle faeces they can remain infectious for a week (Olson et al., 1999). In soil,
cyst infectivity was reduced by only 11.0% after 49 days at 4 °C and was non-infective after 7
days at 25 °C. In cold water Giardia cysts can survive for a long period of time, i.e. 56-84 days at
0 °C to 4 °C, while survival time is shorter at higher temperatures (Olson et al., 1999; Feng and
Xiao, 2011).
26
Environmental contamination can lead to the contamination of drinking water and food. In fact,
contaminated drinking water has been indicated as the vehicle of transmission in most
outbreaks of giardiosis (Marshall et al., 1997; Ryan and Caccio, 2013). Also, treated (swimming
pools) and untreated (lakes, rivers, streams) recreational water has been associated with Giardia
outbreaks (Marshall et al., 1997; Adam et al., 2016). In fact, Giardia was the aetiological agent in
37.0% of the waterborne outbreaks that occurred between 2011 and 2016 worldwide
(Efstratiou et al., 2017), whereas it was implicated in 35.2% of the waterborne outbreaks
documented between 2004 and 2010 (Baldursson and Karanis, 2011). In the United States,
74.8% of the 242 Giardia outbreaks that have been reported from 1971 to 2011, affecting
around 41,000 people, were associated with water. Of them 74.6% were linked to contaminated
drinking water, whereas 18.2% were associated with recreational water (Adam et al., 2016).
Again in the United States, between 2013 and 2014, 46.7% of the waterborne outbreaks
reported were caused by Giardia spp (McClung et al., 2017). Also in Europe, waterborne
outbreaks related to Giardia infection have been documented (Braeye et al., 2015;
Hadjichristodoulou et al., 1998; Hardie et al., 1999; Nygard et al., 2006; Smith et al., 2006a;
Guzman-Herrador et al., 2015). However, despite Giardia spp has been implicated in several
outbreaks associated with water as described above, our knowledge regarding the sources of
water contamination in the specific cases is with some exceptions (Robertson et al., 2006),
inadequate and thus, further investigation should have been followed for the clarification and
the detection of the primary origin of the contamination.
Also, important Giardia outbreaks associated with food have been reported globally, either as a
result of water contamination or after direct contact with an infected individual (Osterholm et
al., 1981; White et al., 1989; Espelage et al., 2010; Figgatt et al., 2017). For instance, in the
United States, more than 20,000 laboratory confirmed cases were documented in 2006 (Scallan
et al., 2011).
Animal contact has been also regarded as a risk factor of human giardiosis (Heyworth, 2016),
however, the situation remains vague as it is not sure if transmission between animals and
humans occurs via direct contact or if the presence of a common contaminated source initiates
infection (Baneth et al., 2016). In general, the role of animals in the transmission of Giardia to
humans is under debate (Caccio and Ryan, 2008; Sprong et al., 2009). According to some studies,
exposure to farm animals and household pets was not associated with the occurrence of human
27
giardiosis (Espelage et al., 2010), but on the other hand, other reports implicate animals in the
transmission cycle of the disease in humans either through direct contact or via an indirect
mode of transmission e.g. contamination of food (Traub et al., 2003; Smith et al., 2006b; Feng
and Xiao, 2011; Khan et al., 2011; Budu-Amoako et al., 2012; García-Cervantes et al., 2017;
Murray et al., 2017).
Not only animal-to-human but also human-to-animal transmission is possible (Sprong et al.,
2009). Apart from pets who share the same household with people, also wild animals can be
infected from humans via contaminated environment, with the beaver’s case in Canada as the
most wellknown example (Thompson et al., 2009, Prystajecky et al., 2015).
Undoubtedly, people also commonly infect each other (Baneth et al., 2016). Several outbreaks
resulting from person-to-person transmission have been documented (Feng and Xiao, 2011).
Foodborne outbreaks of giardiosis linked to infected food handlers (Figgatt et al., 2017) and
food handlers who changed diapers of infected children prior to handling food have been
reported (Osterholm et al., 1981; White et al., 1989). Outbreaks resulting from person-to-person
transmission in child care centres are common (Enserink et al., 2015a, Enserink et al., 2015b,
Pijnackeret al., 2016).
Community-wide outbreaks might be waterborne initially but might spread subsequently by
person-to-person transmission (Feng and Xiao, 2011).
About the seasonality of giardiosis, most human cases are reported from June to October,
probably due to increased exposure to recreational waters (Esch and Petersen, 2013).
Genotyping tools have helped us to evaluate the distribution of G.duodenalis strains in humans
and in various animal species.
In humans, Giardia infections are characterized by the presence of assemblages A and B. Sub-
typing of assemblage A isolates revealed the existence of both sub-assemblages AI and AII in
human isolates, with AII being the most common (Feng and Xiao, 2011). Worldwide assemblage
B is predominant in human giardiosis cases with around 58.0% prevalence compared to the
37.0% occurrence of the assemblage A, with no difference in distribution between developed
and developing countries (Einarsson et al., 2016). However, the only difference that has been
observed is the prevalence of mixed infections which are more frequent in developing
28
communities (5.2% prevalence compared to 3.2% detected in industrialized areas) (Ryan and
Caccio, 2013; Einarsson et al., 2016).
Dogs are commonly infected with the host specific assemblages C and D; however, there are
reports which have shown infection with the potentially zoonotic assemblage A, mainly the sub-
assemblage AI, and less frequently the presence of assemblage B. In cats, the assemblages A and
F seem to be predominant, with the cat-specific assemblage F being more frequently found. Of
the assemblage A cat isolates, the sub-assemblage AI is the most frequent, however, AII and AIII
were also reported (Feng and Xiao, 2011). Few studies have identified assemblage B or
assemblage D in cats (Ryan and Caccio, 2013). The type of the Giardia assemblage that might
dominate in dogs and cats could be determined by their living environment, that is the hosts
and the genotypes that circulate and co-exist. For instance, household pets are mostly infected
with assemblages A and B whereas shelter animals tend to be more commonly infected with the
host restricted assemblages (Berrilli et al., 2004; Lalle et al., 2005; Leonhard et al., 2007; Szenasi
et al., 2007; Claerebout et al., 2009; Ballweber et al., 2010; Upjohn et al., 2010). However, other
studies on household dogs identified mainly assemblages C and D and shelter dogs were shown
to be infected predominantly with assemblage A (Ryan and Caccio, 2013).
In livestock, assemblages A, B and E are more common either as mono-infection or as mixed
infection, with E being the most frequently found, followed by A and B which is the less
commonly reported assemblage (Geurden et al., 2008b; Robertson, 2009; Feng and Xiao, 2011;
Abeywardena et al., 2015). Most of the assemblage A isolates belong to sub-assemblage AI
(Feng and Xiao, 2011). Zoonotic transmission has been reported either via direct animal to
human contact or through contamination of water or food (Ryan and Caccio, 2013).
In horses, molecular data is limited. However, some studies show the predominance of
assemblages A, both sub-assemblages AI and AII, and B (Traversa et al., 2012; Ryan and Caccio,
2013; Santin et al., 2013; Qi et al., 2015) and some others the hoofed livestock-specific
assemblage E (Veronesi et al., 2010).
Generally, among human or animal populations, mixed infections with more than one
assemblage or sub-assemblage of G.duodenalis are possible (Sprong et al., 2009; Heyworth,
2016).
Through the evaluation of Giardia’s assemblages’ distribution in various hosts, we gain
significant knowledge about the transmission patterns of this parasite, the sources of

29
contamination and the zoonotic risk that may arise. Until some years ago, genotyping of Giardia
isolates was limited only to the use of 18 SSU-rRNA gene due to its multicopy nature and the
high degree of sequence homology (Caccio and Sprong, 2010). But, the fact that 18 SSU-rRNA is
a conserved gene and shows little variability, in combination with our increased need to clarify
the transmission scenarios of Giardia and evaluate its zoonotic potential, led to the use of other
markers with high genetic polymorphism which would let us proceed to the genetic
characterization of the isolates up to sub-assemblage level. Thus, sub-assemblages AI, AII, BIII
and BIV have been identified and regarded as potentially zoonotic, whereas sub-assemblage AIII
was found exclusively in animals (Sprong et al., 2009).
However, since genetic variability has been observed within sub-assemblages, each sub-
assemblage was further discriminated into subtypes (Sprong et al., 2009). Among assemblage A
and B subtypes several genetic differences have been observed in human and animal isolates
(Caccio and Ryan, 2008). In general, assemblage B demonstrates higher allelic sequence
heterozygosity compared to assemblage A (Caccio et al., 2005; Caccio and Sprong, 2010). This
high genetic diversity among Giardia assemblages led to the generation of multilocus genotypes
(MLGs) originating from the combination of subtypes in different loci (Caccio and Ryan, 2008).
Thus, through the use of multilocus genotyping, concrete results regarding the epidemiology
and the potential zoonotic transmission patterns of Giardia spp could be obtained (Caccio et al.,
2008).
30
CHAPTER I.2. Cryptosporidium spp
2.1 Introduction
Cryptosporidium spp is an intestinal protozoan which affects vertebrates including humans and
which is responsible for several waterborne and foodborne outbreaks worldwide (Thompson et
al., 2005; Chalmers and Katzer, 2013).Due to the severity of the symptoms that it can cause in
the hosts, and subsequently to the economic losses that are related to Cryptosporidium
infection, cryptosporidiosis has been included in the Neglected Diseases Initiative of the World
Health Organization (WHO) (Chalmers and Katzer, 2013). Therefore, it has been estimated by
WHO that in 2010 cryptosporidiosis resulted in 2,159,331 DALYs due to foodborne infections
(Kirk et al., 2015).
2.2 Taxonomy
According to Ryan et al., 2016b, Cryptosporidium spp current taxonomy is as follows:
Phylum: Apicomplexa
Class: Gregarinomorphea
Subclass: Cryptogregaria
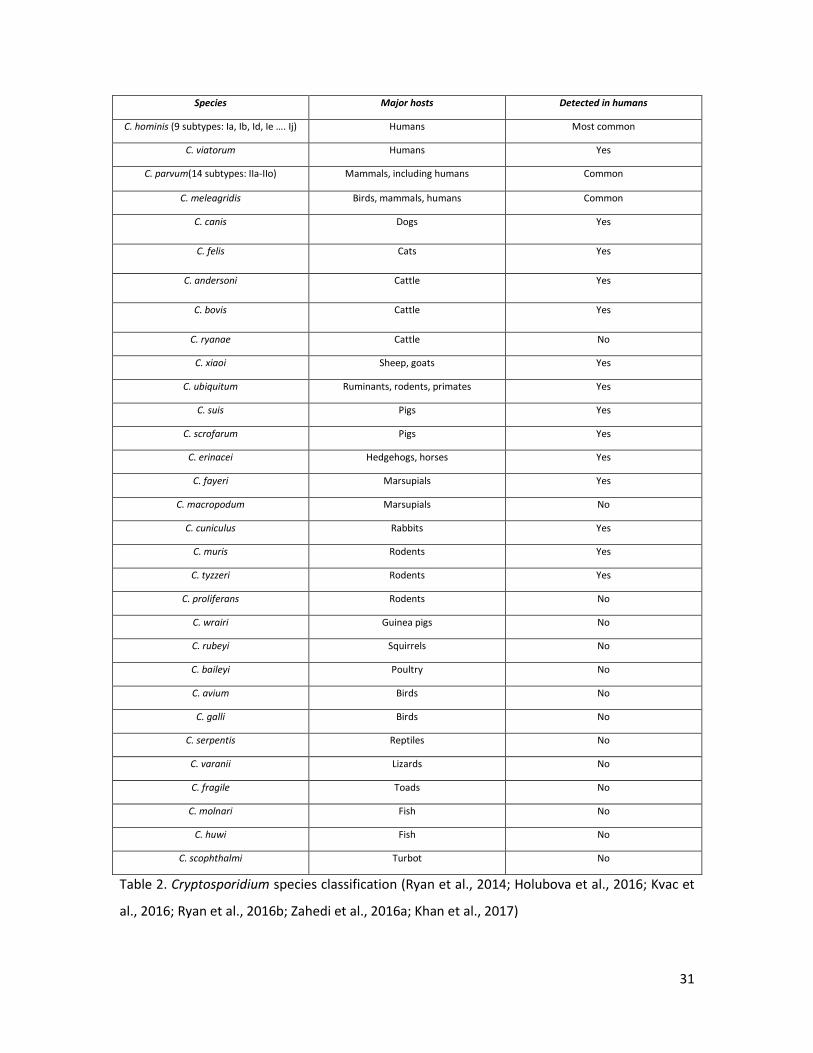
Thirty-one Cryptosporidium species and more than 70 genotypes have been recognized (Fayer,
2010; Certad et al., 2017) (Table 2).
31
Species Major hosts Detected in humans
C. hominis (9 subtypes: Ia, Ib, Id, Ie …. Ij) Humans Most common
C. viatorum Humans Yes
C. parvum(14 subtypes: IIa-IIο) Mammals, including humans Common
C. meleagridis Birds, mammals, humans Common
C. canis Dogs Yes
C. felis Cats Yes
C. andersoni Cattle Yes
C. bovis Cattle Yes
C. ryanae Cattle No
C. xiaoi Sheep, goats Yes
C. ubiquitum Ruminants, rodents, primates Yes
C. suis Pigs Yes
C. scrofarum Pigs Yes
C. erinacei Hedgehogs, horses Yes
C. fayeri Marsupials Yes
C. macropodum Marsupials No
C. cuniculus Rabbits Yes
C. muris Rodents Yes
C. tyzzeri Rodents Yes
C. proliferans Rodents No
C. wrairi Guinea pigs No
C. rubeyi Squirrels No
C. baileyi Poultry No
C. avium Birds No
C. galli Birds No
C. serpentis Reptiles No
C. varanii Lizards No
C. fragile Toads No
C. molnari Fish No
C. huwi Fish Νο
C. scophthalmi Turbot No
Table 2. Cryptosporidium species classification (Ryan et al., 2014; Holubova et al., 2016; Kvac et
al., 2016; Ryan et al., 2016b; Zahedi et al., 2016a; Khan et al., 2017)
32
2.3 Morphology
Cryptosporidium spp consists of various morphological features depending on the stage of the
life cycle. These stages include sporozoites, trophozoites, merozoites, microgametocytes,
macrogametocytes and oocysts which are released in the environment through faeces
(Thompson et al., 2005). Since many species of Cryptosporidium exist, the oocysts of each
species display morphological differences such as different size and shape, some are small and
spherical whereas others are larger and more oval (Chalmers and Katzer, 2013; Zahedi et al.,
2016a). However, regardless the species, although Cryptosporidium belongs to apicomplexan
parasites which carry the apicoplast organelle, it is characterized by the absence of apicoplasts
and mitochondria (Bouzid et al., 2013; Ryan et al., 2015).
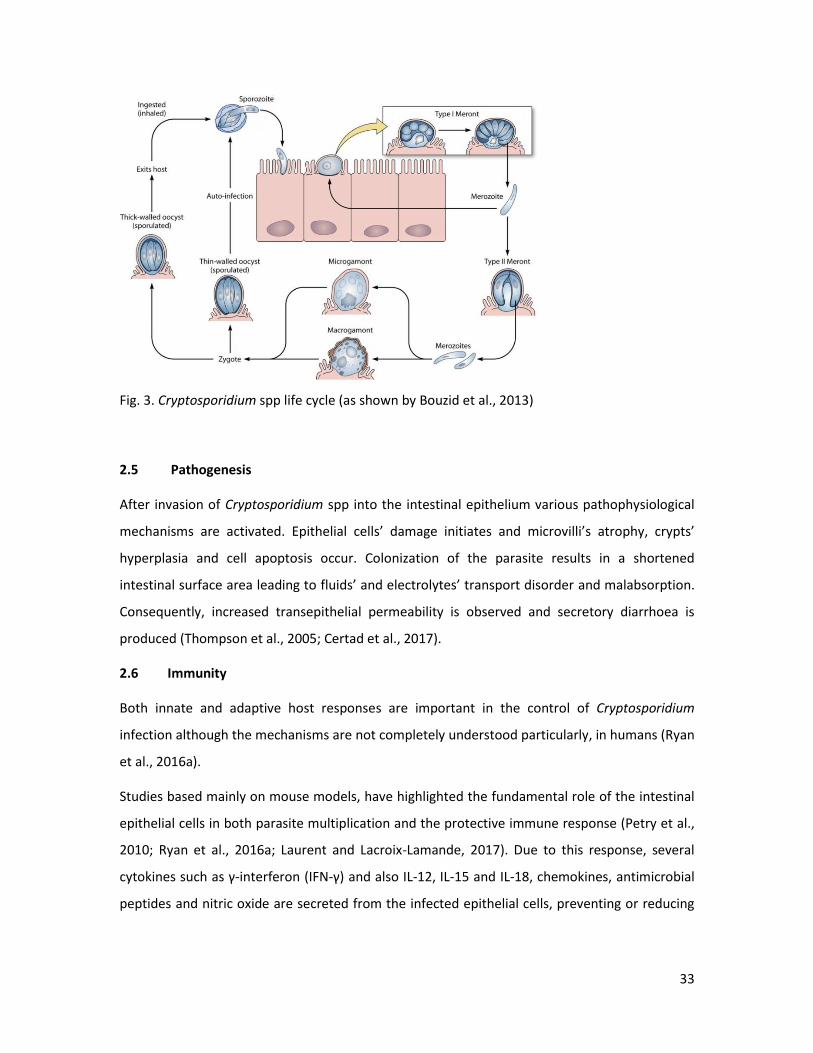
2.4 Life cycle
The life cycle of Cryptosporidium is complicated, consisting of both sexual and asexual
developmental stages. Infection begins with the ingestion by the host of the sporulated oocysts
through contaminated water or food or directly via the faecal-oral route. Inhalation of the
oocysts can also occur. Each oocyst contains four sporozoites which after excystation in the
intestinal lumen or the respiratory tract, emerge and invade the epithelial cells and develop into
trophozoites. Trophozoites undergo asexual division (merogony) and form Type I Meronts
consisting of 8 merozoites. Some of these merozoites form Type II meronts which contain 4
merozoites and initiate the sexual phase of the life cycle. Macrogametocytes and
microgametocytes are formed, fertilize and produce the zygote. Most of the zygotes develop
into oocysts, the thick ones with a two-layered wall which are released to the environment, and
the thin-walled oocysts which facilitate autoinfection. The prepatent period for Cryptosporidium
parvum for example, ranges from 7 to 21 days (Thompson et al., 2005).
33
Fig. 3. Cryptosporidium spp life cycle (as shown by Bouzid et al., 2013)
2.5 Pathogenesis
After invasion of Cryptosporidium spp into the intestinal epithelium various pathophysiological
mechanisms are activated. Epithelial cells’ damage initiates and microvilli’s atrophy, crypts’
hyperplasia and cell apoptosis occur. Colonization of the parasite results in a shortened
intestinal surface area leading to fluids’ and electrolytes’ transport disorder and malabsorption.
Consequently, increased transepithelial permeability is observed and secretory diarrhoea is
produced (Thompson et al., 2005; Certad et al., 2017).
2.6 Immunity
Both innate and adaptive host responses are important in the control of Cryptosporidium
infection although the mechanisms are not completely understood particularly, in humans (Ryan
et al., 2016a).
Studies based mainly on mouse models, have highlighted the fundamental role of the intestinal
epithelial cells in both parasite multiplication and the protective immune response (Petry et al.,
2010; Ryan et al., 2016a; Laurent and Lacroix-Lamande, 2017). Due to this response, several
cytokines such as γ-interferon (IFN-γ) and also IL-12, IL-15 and IL-18, chemokines, antimicrobial
peptides and nitric oxide are secreted from the infected epithelial cells, preventing or reducing
34
the severity of infection (Ryan et al., 2016a; Laurent and Lacroix-Lamande, 2017; Lemieux et al.,
2017).
Also other mechanisms are implicated in the host immunity during Cryptosporidium infection.
MicroRNA (miRNA), which are small RNA molecules of 23 nucleotides that result in gene
silencing via translational suppression or mRNA degradation, target Toll-like receptor 4 (TLR4)
and regulate TLR4-mediated anti-C. parvum defense as well as alter C. parvum infection burden
in vitro (Ryan et al., 2016a).
Mannose-binding lectin (MBL), which is an evolutionarily conserved protein secreted by
hepatocytes that functions in human innate immunity by binding to microbial surfaces and
promoting opsonophagocytosis, has been shown to be important in the protection against
cryptosporidiosis, as children and HIV-infected adults with mannose-binding lectin deficiency
have increased susceptibility to cryptosporidiosis and more severe diseases (Ryan et al., 2016a).
Regarding cellular adaptive immunity, CD4+ T cells seem to be essential to the eradication of the
parasite (Lemieux et al., 2017). Therefore, it has been shown that low counts of CD4+ T cells
recorded in AIDS patients, made them more vulnerable to Cryptosporidium infection (Lemieux et
al., 2017).
The role of humoral immunity in the protection from cryptosporidiosis is vague (Ryan et al.,
2016a; Lemieux et al., 2017), however, the antibodies that have been linked to Cryptosporidium
infection are serum IgM and IgG as well as serum and secretory IgA. Antibodies may support
protection as it has been shown in the case of bovine cryptosporidiosis where hyperimmune
bovine colostrum had prophylactic and therapeutic effects (Lemieux et al., 2017).
2.7 Cryptosporidiosis in dogs and cats
Cryptosporidiosis is a parasitosis that concerns dogs and cats worldwide, with prevalence rates
reported between 0.0% and 29.4% in cats and 0.5% and 44.1% in dogs (Lucio-Forster et al.,
2010). Although many of the infected animals are characterized by asymptomatic infection,
severe manifestations can also be displayed. The most common symptoms include watery
diarrhoea, anorexia and weight loss and are more frequent in young, mainly less than 6 months
of age, and immunocompromised animals (Scorza and Tangtrongsup, 2010). Oocyst shedding
35
lasts for months in cats and for more than 80 days in dogs (Thompson et al., 2005; Hamnes et
al., 2007; Santin, 2013).
2.8 Cryptosporidiosis in ruminants
Cryptosporidium spp is widely endemic in ruminants and it is considered as one of the most
frequently diagnosed enteropathogens in these animals.
Among Cryptosporidium species that infect cattle, C. parvum is linked to clinical disease
(Thomson et al., 2017). Infection occurs in neonatal calves and oocyst shedding can initiate even
in 2 days-old animals (Thompson et al., 2005). Clinical manifestations include profuse watery
diarrhoea, abdominal pain, anorexia and weight loss and can lead to death as a result of severe
dehydration (Santin, 2013). Infected animals can excrete a large number of oocysts per day (>
1010) and parasite’s shedding can occur even during asymptomatic infection (Thomson et al.,
2017).
Cryptosporidium spp also infect young sheep and goats, mainly at ages between 1 to 3 weeks
(Santin, 2013). The prepatent period is approximately 4 days (Thompson et al., 2005). Similar to
bovine cryptosporidiosis, clinical symptoms in lambs and goat kids are characterized by
diarrhoea which can be yellow pasty to watery, anorexia and illthrift. As in cattle, large numbers
of oocysts (108-1010) are excreted each day through faeces for a long time even from
asymptomatic animals (Thompson et al., 2005; Santin, 2013).
2.9 Cryptosporidiosis in horses
Cryptosporidiosis is also prevalent in horses. Infected animals can be asymptomatic but also
severe diarrhoea can occur in foals of a few weeks of age and in immunocompromised animals
(Thompson et al., 2005; Veronesi et al., 2010; Santin, 2013).
2.10 Cryptosporidiosis in pigs
Cryptosporidium has been detected in pigs of all ages worldwide (Farzan et al., 2011; Yui et al.,
2014; Lin et al., 2015; Petersen et al., 2015; Schubnell et al., 2016), however, Petersen et al.,
2015 have reported that piglets before weaning are more vulnerable to infection and more
36
intensely infected than older animals. The Cryptosporidium species/genotypes adapted to pigs
are C. scrofarum and C. suis, but C. parvum, C. muris, C. andersoni and C. tyzzeri have been also
isolated from these animals (Kvac et al., 2013; Santin, 2013; Yui et al., 2014). Cryptosporidium
suis seems to be more common in young pigs, whereas C. scrofarum is more frequently found in
older animals (>5 weeks) (Langkjaer et al., 2007; Johnson et al., 2008; Kváč et al., 2009b;
Jenikova et al., 2011; Kváč et al., 2014; Yui et al., 2014).
Although cryptosporidiosis in pigs is usually subclinical (Xiao, 2010), clinical manifestations can
occur including diarrhoea, anorexia and vomiting. Severity of clinical signs seem to depend on
the Cryptosporidium species that cause infection and co-infection with other enteropathogens
(Santin, 2013), however, the pathogenicity of the disease in pigs has not been clarified yet (Yui
et al., 2014).
2.11 Cryptosporidiosis in humans
Cryptosporidium is the most common diarrhoea-causing protozoan parasite worldwide,
especially in developing countries, as it is less frequently observed in areas where hygiene,
water quality and nutrition are adequate (Ryan et al., 2016a; Squire and Ryan, 2017).
Nevertheless, Cryptosporidium is considered as the leading agent of waterborne disease
outbreaks in the United States (Painter et al., 2016) and Europe (Semenza and Nichols, 2007;
Hajdu et al., 2008; Guzman-Herrador et al., 2015; Utsi et al., 2016) causing high rates of
morbidity and even mortality in children and immunocompromised individuals. The prevalence
of cryptosporidiosis in HIV-infected patients with diarrhoea has been reported to range from
3.0% to 16.0% in developed countries (Putignani and Menichella, 2010).
Clinical signs appear between 2 and 14 days from the time of infection and can persist for 3
weeks (Thompson et al., 2005; Chalmers and Giles, 2010). However, severity and duration of
symptoms vary with age and immune status of the host (Thompson et al., 2005). Young children
and immunocompromised and malnourished individuals are more susceptible to
cryptosporidiosis (Thompson et al., 2005; Bouzid et al., 2013; Ryan et al., 2016a; Caccio and
Chalmers, 2016) and may excrete a high number of oocysts ranging between 5.0 x 103 to 9.2 x
105 oocysts/mL (Goodgame et al., 1993). On the contrary, disease in immunocompetent
individuals is mainly characterized by self-limiting symptoms and even asymptomatic shedding
of oocysts (Thompson et al., 2005; Bouzid et al., 2013; Caccio and Chalmers, 2016).
37
The most common clinical sign is diarrhoea which can be severe and watery to mild and
intermittent (Thompson et al., 2005). Other clinical signs include general malaise, fever, fatigue,
loss of appetite, nausea and vomiting. Infrequently, symptoms associated with cholecystitis,
hepatitis, pancreatitis, reactive arthritis and respiratory problems are observed (Thompson et
al., 2005).
Among the above species, C. hominis subtype Id, C. parvum, C. canis and C. felis have been
associated with a more severe disease in HIV/AIDS patients. The risk of diarrhoea was higher in
patients infected with C. hominis subtype Id compared to those infected with the subtype Ib
whereas no diarrhoea was observed in patients infected with subtype Ia. Subjects infected with
C. meleagridis showed no clinical signs and excreted a small number of oocysts. Long-term
sequelae of infection, including ocular and articular pain, headache and fatigue, have been
associated with C. hominis but not with C. parvum (Certad et al., 2017). Also, C. hominis has
been responsible for more outbreaks than C. parvum in most regions (Ryan et al., 2016a).
2.12 Diagnosis
Cryptosporidium oocysts can be detected in faecal samples by a variety of diagnostics tests
including direct microscopy, antigen detection methods and molecular techniques.
Several staining techniques have been used for the microscopic identification of
Cryptosporidium spp with acid fast-modified Ziehl-Neelsen staining being the most common
one. Other stains include Kinyoun (Lennette et al., 1985), negative malachite green staining
(Elliot et al., 1999), negative carbol fuchsine staining (Casemore et al., 1985; Kuhnert-Paul et al.,
2012), safranin methylene blue (Garcia, 2007, 2009) and trichrome (Garcia, 2007, 2009).
Recently, the TF-test (Three Faecal Test) Coccidia parasitological technique has been validated
for the detection of Cryptosporidium oocysts using a new dye, a combination of modified
D’Antoni’s iodine solution and modified Masson’s trichome composition, with promising results
(Inacio et al., 2016).
Above all microscopic techniques, the direct immunofluorescent antibody assay (IFA) that
simultaneously detects Giardia cysts and Cryptosporidium oocysts is considered as the most
sensitive and specific test. Specifically, it offers about 97.0% sensitivity compared to 75.0%
sensitivity of acid-fast staining in human samples (Ryan et al., 2016a).

38
Apart from IFA, other immunoassays have been also evaluated and are widely used for the
detection of Cryptosporidium spp. These include enzyme-linked immunosorbent assays (ELISAs),
enzyme immunoassays (EIAs) and immunochromatographic (dipstick) assays (Ryan et al.,
2016a). Similarly, compared to other antigen detection tests, IFA remains the most sensitive
method and is also highly specific (Se: 97.4% & Sp: 94.8% in calves, Se: 97.4% & Sp: 100% in
human samples) (Geurden et al., 2008a; Chalmers et al., 2011a). Biosensor chips, that detect
and quantify C. parvum in real-time via anti-C. parvum IgM binding, have also been developed,
however detection limits are relatively high (100 or more oocysts) and they have yet to be fully
evaluated on water or faecal samples (Campbell et al., 2008; Kang et al., 2008).
Another major limitation of both conventional microscopy and antigen detection methods is
that they cannot identify to species or subtype level, which is essential for understanding
transmission dynamics and outbreaks, in particular for zoonotic species (Ryan et al., 2016a).
PCR-based methods have also been developed for the diagnosis and the determination of
Cryptosporidium species/genotypes and C. parvum and C. hominis subtypes. The SSU-rRNA is the
most widely used marker since it is semi-conserved, and it has hyper-variable regions and a
multi-copy nature. Other genes are also used such as 70kDa heat shock protein (HSP70) (Morgan
et al., 2001), Cryptosporidium oocyst wall protein (COWP) (Xiao et al., 2000) and actin (Sulaiman
et al., 2002). The 60-kDa glycoprotein (gp60) gene is a commonly used subtyping tool for the
identification of C. parvum and C. hominis subtypes (Xiao, 2010).
2.13 Treatment
2.13.1 Dogs and cats
Paromomycin, an aminoglycoside drug, is regarded the drug of choice for the treatment of
cryptosporidiosis in dogs and cats (Barr et al., 1994; Scorza and Lappin, 2006; Shahiduzzaman
and Daugschies, 2012). Apart from paromomycin, two macrolides, azithromycin and tylosin,
have been also suggested with azithromycin being better tolerated by cats (Scorza and Lappin,
2006). Besides, nitazoxanide, previously approved for use in the treatment of giardiosis and
cryptosporidiosis in humans has been administered to dogs and cats (Scorza and Lappin, 2006;
Moron-Soto et al., 2017), however, it is not effective in immunocompromised animals
(Shahiduzzaman and Daugschies., 2012). Together with the administration of drugs for the
39
effective elimination of the parasite, supportive therapy may also be needed for rehydration or
the eradication of possible secondary infections that may co-exist (Thompson et al., 2008).
2.13.2 Ruminants
Several drugs have been tested for the treatment of cryptosporidiosis in ruminants. However,
only a few have proved to control the parasite effectively and thus are widely used.
Halofuginone lactate which has a cryptosporidiostatic activity on the sporozoite and merozoite
stages of C. parvum, is quite effective against bovine cryptosporidiosis (Naciri et al., 1993;
Thompson et al., 2008; De Waele et al., 2010) and also against Cryptosporidium infection in
lambs and goat kids (Giadinis et al., 2007; Petermann et al., 2014). Paromomycin is suggested as
an efficient drug in both prevention and treatment of cryptosporidiosis, mainly administered to
small ruminants (Fayer and Ellis, 1993; Mancassola et al., 1995; Chartier et al., 1996; Viu et al.,
2000; Shahiduzzaman and Daugschies, 2012).
2.13.3 Horses
Treatment of equine cryptosporidiosis is mainly based on supportive therapy since there is no
licensed drug for this indication. However, the administration of nitazoxanide and paromomycin
in combination with azithromycin has been documented (Shahiduzzaman and Daugschies,
2012).
2.13.4 Pigs
Control of cryptosporidiosis in pigs is quite complicated. The use of paromomycin seems to have
promising results but not for severe cases. Besides, nitazoxanide can be partially effective to
infected piglets but only in low doses.
2.13.5 Humans
Nitazoxanide is widely used for the treatment of human cryptosporidiosis, however, this
compound is not efficient in HIV patients (Ryan et al., 2016b).
2.14 Epidemiology and zoonotic potential
Transmission of Cryptosporidium spp can be either direct by human-to-human or animal-to-
human contact or indirectly via contaminated water or food (Ryan et al., 2016a). Also,
40
mechanical transmission is possible by vectors such as arthropods or birds (Thompson et al.,
2005).
Infected hosts excrete large numbers of highly infectious and robust oocysts through their
faeces (Ryan et al., 2016a; Certad et al., 2017). Oocysts proved to be viable for more than 12
weeks at -4 °C in water and cattle faeces and for 10 weeks in soil (Olson et al., 1999), however, it
has been shown that temperature affects their viability and they become more susceptible as
temperature raises (Olson et al. 1999; Peng et al., 2008).
Cryptosporidium is regarded as one of the most important causes of waterborne disease
outbreaks worldwide. It has been responsible for around 60.0% of the reported waterborne
disease outbreaks between 2004 and 2010 (Baldursson and Karanis, 2011). Waterborne
infections involve drinking water, recreational waters such as swimming pools and waterparks
and surface waters including water catchments and irrigation waters (Baldursson and Karanis,
2011; Ryan et al., 2017). Besides to prolonged survival in the environment, Cryptosporidium
oocysts are also highly resistant to common disinfectants such as chlorine (Ryan et al., 2016a).
Thus, the parasite cannot be inactivated with water treatments and transmission via drinking
and recreational water is favoured (Ryan et al., 2016a). Surface waters can be contaminated by
infected people or animals, particularly wildlife and livestock whose contaminated manure left
can end up in rivers or lakes through run-off (Hofstra et al., 2013).
Foodborne outbreaks associated with Cryptosporidium infection have also been reported
(Putignani and Menichella, 2010; Robertson and Chalmers, 2013). Food contamination can occur
either from infected food handlers or from contaminated water during the preparation process
(Ryan et al., 2016a). Vegetables are more likely to be contaminated as they might be fertilized
with contaminated manure, watered with contaminated irrigation water or contaminated by
infected animals’ faeces (Ryan et al., 2016a). Besides, marine molluscan bivalve shellfish could
constitute a source of human infection (Robertson, 2007). Their capacity to filter water can lead
to their contamination with Cryptosporidium oocysts and as a result they may pose a public
health risk when consumed raw or lightly cooked (Robertson, 2007).
Human-to-human transmission can occur after direct contact with infected people in
combination with inadequate sanitation. Apart from the human-to-human transmission, people
can be infected by animals (Caccio and Chalmers, 2016). Direct contact with animals’ faeces and
lack of hygiene measures can lead to infection (Ryan et al., 2016a).

41
Molecular diagnostic tools have helped us to better understand the transmission patterns of
Cryptosporidium and evaluate its zoonotic or anthroponotic nature. Although more than 17
species have been identified in humans (Table 2), C. hominis and the zoonotic C. parvum are the
most commonly detected species associated with human infections, followed by C. meleagridis
which is primarily found in birds (Chalmers and Giles, 2010; Zahedi et al., 2016a). Besides, C.
hominis and C. parvum are responsible for the majority of the waterborne outbreaks reported
worldwide with the exception of one outbreak occurred in UK for which C. cuniculus, the rabbit
species, was incriminated (Chalmers and Giles, 2010; Zahedi et al., 2016a).
Sequence analysis of the 60kDa glycoprotein (gp60 or gp40/15) gene has revealed the presence
of several subtypes of C. hominis and C. parvum. Specifically, nine subtypes of C. hominis, from
Ia, Ib, Id to Ij, and 14 subtypes of C. parvum, from IIa to IIo, have been detected (Ryan et al.,
2014). Among those, C. parvum subtype IIa and IId have been identified in both humans and
animals (ruminants) and are considered zoonotic, whereas type IIc has only been found in
humans (Xiao and Feng, 2008; Widmer and Lee, 2010; Xiao, 2010). On the contrary, C. hominis is
considered a human pathogen (Xiao, 2010; Ryan et al., 2014; Khan et al., 2017). However,
recently it has been reported in numerous wildlife hosts including a dugong and non-human
primates and also its subtype IbA10G2 has been found in marsupials and cattle in Australia
(Zahedi et al., 2016b).
The distribution of C. hominis and C. parvum in humans varies by geographic region. C. hominis
tends to predominate in most parts of the world, especially in developing countries, while C.
parvum is more frequent in the Middle East and both species are common in Europe (Shirley et
al., 2012). C. hominis is more common in urban areas whereas C. parvum in rural areas with
lower human population densities but high livestock density. The temporal distribution of both
species is also different. Studies have seen more C. parvum in spring (lambing time) and more C.
hominis in autumn (Chalmers et al., 2009; Pollock et al., 2010; The ANOFEL Cryptosporidium
National Network, 2010).
The C. hominis subtypes Ia, Ib, Id and Ie, which are responsible for the majority of the human
cases worldwide, have been all identified in developing countries. Subtype Ib is considered the
main cause of diarrhoea in immunocompetent people in Europe and the USA (Khan et al., 2017).
C. parvum subtype families IIa, IIb, IIc and IIe have also been isolated from humans in developing

42
countries, although less frequently, due to the dominance of C. hominis in these areas (Akiyoshi
et al., 2006; Muthusamy et al., 2006; Cama et al., 2007; Essid et al., 2018).
Ruminants are reported to be the major source of C. parvum transmission to humans. Cattle,
sheep and goats have especially been implicated in human outbreaks (Shahiduzzaman and
Daugschies, 2012). However, bovine cryptosporidiosis has been also linked to C. andersoni,
which although not a human pathogen, has been documented in humans (Ryan et al., 2016a) as
well as C. bovis and C. ryanae (Chako et al., 2010; Ryan et al., 2014) which mainly appear as age
increases compared to infection with C. parvum which is most prevalent in neonatal animals
(Chalmers and Giles, 2010).
In sheep, C. parvum, C. xiaoi and C. ubiquitum are mostly frequently identified although C.
hominis, C. andersoni, C. suis, C. fayeri and C. scrofarum have been also reported (McLauchlin et
al., 2000; Santin et al., 2007; Geurden et al., 2008b; Mueller-Doblies et al., 2008; Quilez et al.,
2008; Fayer and Santin, 2009; Ryan et al., 2014; Tzanidakis et al., 2014).
In goats, mainly C. parvum and to a lesser extent C. xiaoi have been detected together with C.
hominis and C. ubiquitum (Geurden et al., 2008b; Quilez et al., 2008; Fayer and Santin, 2009;
Ryan et al., 2014; Tzanidakis et al., 2014). The presence of C. hominis and C. parvum in small
ruminants in combination with the fact that C. ubiquitum has been detected in human cases of
cryptosporidiosis (Ryan et al., 2016a), considers these animals a possible zoonotic reservoir for
Cryptosporidium.
The zoonotic C. parvum and the equine-specific Cryptosporidium horse genotype have been
mainly detected in horses (Smith et al., 2010; Caffara et al., 2013; Laatamna et al., 2015; Qi et
al., 2015), but, occasionally, the human species C. hominis and C. erinacei have been also found
(Kvac et al., 2014; Laatamna et al., 2015).
Although uncommon, the pig species C. scrofarum and C. suis have been documented in human
cryptosporidiosis cases infecting both immunocompetent and immunocompromised individuals
(Kvac et al. 2009a, Wang et al. 2013, Bodager et al. 2015). Among these reported cases, C.
scrofarum has been detected in an immunocompetent man with diarrhoea who however, was
co-infected with Giardia duodenalis, assemblage A. Thus, due to the co-presence of Giardia, C.
scrofarum was not confirmed to be the primary cause of the gastroenteritis of that patient (Kvac
et al., 2009a).

43
C. muris, mainly found in rodents, has been indicated as the cause of human infection in several
cases (Ryan et al., 2016a).
The role of companion animals in the zoonotic transmission of Cryptosporidium seems to be
limited. Dogs and cats are primarily infected with the host-specific species C. canis and C. felis
respectively (Thompson et al., 2008; Abeywardena et al., 2015), however, other species have
been also detected such as C. parvum in dogs (Abeywardena et al., 2015) and C. muris in cats
(Santin et al., 2006; Pavlasek and Ryan, 2007). The canine- and feline- specific species have been
implicated in human cases of clinical cryptosporidiosis mainly in developing countries but at a
low rate, indicating that a minimal risk for public health exists (Thompson et al., 2008; Lucio-
Forster et al., 2010).
Prevention of Giardia spp and Cryptosporidium spp infections
Since Giardia and Cryptosporidium are highly infectious organisms whose transmission can occur
through many cycles, where humans, animals and the environment are involved, a holistic
approach is needed for the prophylaxis and the control of these parasites.
In order to avoid person-to-person transmission, people should follow good hygiene practices.
These include thorough hand washing before and during food preparation and eating, after
using the toilet, after changing diapers or after caring for a patient who is suffering from
diarrhoea. Besides, hygiene measures after contact with animals’ faeces would protect from
possible zoonotic transmission (Baneth et al., 2016; Ryan et al., 2016a; Currie et al., 2017).
Recently, breast-feeding has been considered a protection weapon against clinical giardiosis.
Specifically, the presence of high titers of anti-Giardia secretory immunoglobulin A (SIgA) in
breast milk, seems to protects infants and young children from displaying symptoms. However,
infection cannot be prevented (Muhsen and Levine 2012; Squire and Ryan, 2017). Clinical
cryptosporidiosis could also be prevented via breast-feeding (Squire and Ryan, 2017). It has
been reported that breast-feeding decreases intensity of parasite infection and it has been
associated with low serum levels of IgE and TNF-α (Abdel-Hafeez et al., 2013).
Since water acts as a vehicle of transmission of giardiosis and cryptosporidiosis and as a result
numerous waterborne outbreaks have been reported worldwide (Karanis et al., 2007;
Baldursson and Karanis, 2011), preventive measures should also focus on this risk factor. Thus,

44
adequate treatment of drinking water should be provided (Peletz et al., 2013; Speich et al.,
2016). Because Giardia cysts and Cryptosporidium oocysts are highly resistant to chlorination
(Korich et al., 1990; Winiecka-Krusnell and Linder, 1998), the use of filters is recommended
(Baneth et al., 2016; Ryan et al., 2017). Besides, untreated water from lakes, rivers, springs,
ponds, streams or shallow wells should not be consumed unless it is boiled or filtered before.
Also, raw vegetables and fruits should be washed thoroughly with uncontaminated water
(Chalmers and Giles, 2010; Adam et al., 2016; Baneth et al., 2016; Caccio and Chalmers, 2016;
Ryan et al., 2016a). Sanitation and hygiene measures should be also implemented in
recreational water environments as globally many outbreaks are associated with exposure to
recreational water activities (Causer et al., 2006; Jones et al., 2006; Wheeler et al., 2007;
Hopkins et al., 2013; Adam et al., 2016; de Gooyer et al., 2017; Moreira and Bondelid, 2017;
Ryan et al., 2017). Besides, healthy swimming behaviour is required. People with diarrhoea,
especially children in diapers, should not swim at recreational water venues so that water
contamination is prevented (Ryan et al., 2016a; Ryan et al., 2017).
Preventive measures should be also taken in order to reduce the risk of environmental
contamination and therefore human infection, from animals. Since livestock constitutes a
potential source of environmental contamination including surface water catchments (Wells,
2015), access of productive animals to these areas should be monitored (Castro-Hermida et al.,
2009). Besides, manure should be properly managed by farmers, that is, stored for more than 12
weeks, decomposed and treated e.g. through anaerobic digestion (Garces et al., 2006), before
use as a fertilizer for crops (Olson et al., 1999; Castro-Hermida et al., 2009; Grit et al., 2012;
Vermeulen et al., 2017).
Preventive management measures should also include thorough cleaning and disinfection of the
housing facilities (stables, farms, kennels, catteries) using products such as ammonia, chlorine
dioxide and hydrogen dioxide or ozone, as well as the maintenance of a dry environment inside
the buildings, a condition which would block the parasites development (Geurden et al., 2010b;
Saleh et al., 2016).
Regarding prevention through vaccination, efficient vaccines against Giardia and
Cryptosporidium are not available. Recently, a novel oral vaccine against Giardia for dogs and
cats has been tested with promising results (Serradell et al., 2016).

45
Spatio-temporal patterns in Giardia spp and Cryptosporidium spp infection
Despite the abundance of Giardia spp and Cryptosporidium spp and their significant implication
in human and veterinary medicine, little is known about the spatial and temporal patterns of
these parasites. Understanding geographical and seasonal viaribility of risk factors which favour
their prevalence, especially under the burden of the constant global environmental changes,
would be a valuable knowledge about the locations and the time periods of increased risk and
would contribute to the better prevention and control of the diseases caused by Giardia spp and
Cryptosporidium spp (Jones et al., 2013). Besides, identifying the peaks in giardiosis and
cryptosporidiosis incidence would be significant information that could be related to the
occurrence of outbreaks (Valcour et al., 2016).
Globally, there are limited studies which have investigated the spatio-temporal clusters of
Giardia spp cases (Lal and Hales, 2015; Asher et al., 2016; Valcour et al., 2016; Lal et al., 2018).
According to these studies, giardiosis tends to occur predominantly in urban areas indicating an
anthroponotic pathway of transmission (Lal and Hales, 2015; Lal et al., 2018). Attendance at day
care centres and changing diapers have been identified as important risk factors for giardiosis in
metropolitan regions, supporting the above hypothesis (Hoque et al., 2003; Sagebiel et al., 2009;
Pijnacker et al., 2016).
However, in cases where human populations live in close proximity to animals, the detection of
the Giardia spp zoonotic assemblages have been reported in both populations (people and
animals) suggesting potential for cross-species transmission (Delport et al., 2014; Ng et al., 2011;
Asher et al., 2016).
Regarding seasonality, most human cases are reported from June to October, probably due to
increased exposure to recreational waters (Esch and Petersen, 2013). However, spatio-temporal
studies that were conducted in New Zealand (Lal and Hales, 2015; Lal et al., 2018), indicated that
Giardia spp cases showed no seasonality. On the contrary, a similar study in Canada reported a
spring peak for Giardia spp suggesting run-off from spring snow melt as a possible reason
(Valcour et al., 2016).
Contrary to Giardia’s trend, Cryptosporidium spp infections seem to be more oriented to
agricultural and livestock-dominated areas displaying a constant spring peak (Lal and Hales,

46
2015; Lal et al., 2018). Recurrent Cryptosporidium clusters in spring indicate a common
environmental exposure and can be related to the high number of livestock births and as a
result a high rate of Cryptosporidium spp oocysts shedding, occurring during this time period (Lal
and Hales, 2015). Reported outbreaks associated with contact with livestock support this
suggestion (Stefanogiannis et al., 2001; Grinberg et al., 2011). For that reason, C. parvum
zoonotic genotype is more prevalent in spring, whereas the anthroponotic and more frequent in
urban areas C. hominis is most commonly detected in autumn, possibly following the high
contact of humans with recreational waters (Pollock et al., 2010; Chalmers et al., 2011b) .
47
References
Abdel-Hafeez E.H., Belal U.S., Abdellatif M.Z., Naoi K., Norose K. Breast-feeding protects infantile diarrhea caused by intestinal protozoan infections. Korean J Parasitol. 2013;51:519-24.
Abdul-Wahid A., Faubert G. Characterization of the local immune response to cyst antigens during the acute and elimination phases of primary murine giardiasis. Int J Parasitol. 2008;38:691-703.
Abeywardena H., Jex A.R., Gasser R.B. A perspective on Cryptosporidium and Giardia, with an emphasis on bovines and recent epidemiological findings. Adv Parasitol. 2015;88:243-301.
Adam R.D. Biology of Giardia lamblia. Clin Microbiol Rev. 2001;14:447-75.
Adam E.A., Yoder J.S., Gould L.H., Hlavsa M.C., Gargano J.W. Giardiasis outbreaks in the United States, 1971-2011. Epidemiol Infect. 2016;144:2790-801.
Adell-Aledón M., Köster P.C., de Lucio A., Puente P., Hernández-de-Mingo M., Sánchez-Thevenet P., Dea-Ayuela M.A., Carmena D. Occurrence and molecular epidemiology of Giardia duodenalis infection in dog populations in eastern Spain. BMC Vet Res. 2018;14:26.
Akiyoshi D.E., Tumwine J.K., Bakeera-Kitaka S., Tzipori S. Subtype analysis of Cryptosporidium isolates from children in Uganda. J Parasitol. 2006;1097-1100.
Ankarklev J., Jerlström-Hultqvist J., Ringqvist E., Troell K., Svärd S.G. Behind the smile: cell biology and disease mechanisms of Giardia species. Nat Rev Microbiol. 2010;8:413-22.
Araújo N.S., Mundim M.J., Gomes M.A., Amorim R.M., Viana J.C., Queiroz R.P., Rossi M.A., Cury M.C. Giardia duodenalis: pathological alterations in gerbils, Meriones unguiculatus, infected with different dosages of trophozoites. Exp Parasitol. 2008;118(4):449-57.
Asher A.J., Hose G., Power M.L.. Giardiasis in NSW: Identification of Giardia duodenalis assemblages contributing to human and cattle cases, and an epidemiological assessment of sporadic human giardiasis. Infect Genet Evol. 2016;44:157-161.
Atwill E.R., McDougald N.K., Perea L. Cross-sectional study of faecal shedding of Giardia duodenalis and Cryptosporidium parvum among packstock in the Sierra Nevada Range. Equine Vet. J. 2000;32: 247–252.
Baldursson S., Karanis P. Waterborne transmission of protozoan parasites: review of worldwide outbreaks - an update 2004-2010. Water Res. 2011;45:6603-14.
Ballweber L.R., Xiao L., Bowman D.D., Kahn G., Cama V.A. Giardiasis in dogs and cats: update on epidemiology and public health significance. Trends Parasitol. 2010;26:180-189.
Baneth G., Thamsborg S.M., Otranto D., Guillot J., Blaga R., Deplazes P., Solano-Gallego L. Major parasitic zoonoses associated with dogs and cats in Europe. J Comp Pathol. 2016;155:S54-74.
Barr S.C., Jamrosz G.F., Hornbuckle W.E., Bowman D.D., Fayer R. Use of paromomycin for treatment of cryptosporidiosis in a cat. J Am Vet Med Assoc. 1994;205(12):1742-3.
48
Bartelt L.A., Sartor R.B. Advances in understanding Giardia: determinants and mechanisms of chronic sequelae. F1000Prime Rep. 2015;7:62.
Barutzki D., Schaper R. Results of parasitological examinations of faecal samples from cats and dogs in Germany between 2003 and 2010. Parasitol Res. 2011;109:S45–60.
Berrilli F., Di Cave D., De Liberato C., Franco A., Scaramozzino P., Orecchia P. Genotype characterisation of Giardia duodenalis isolates from domestic and farm animals by SSU-rRNA gene sequencing. Vet Parasitol. 2004;122:193-199.
Bodager J.R., Parsons M.B., Wright P.C., Rasambainarivo F., Roellig D., Xiao L., Gillespie T.R. Complex epidemiology and zoonotic potential for Cryptosporidium suis in rural Madagascar. Vet Parasitol. 2015;207: 140–143.
Bouzid M., Hunter P.R., Chalmers R.M., Tyler K.M. Cryptosporidium pathogenicity and virulence. Clin Microbiol Rev. 2013;26:115-34.
Braeye T., De Schrijver K., Wollants E., van Ranst M., Verhaegen J. A large community outbreak of gastroenteritis associated with consumption of drinking water contaminated by river water, Belgium, 2010. Epidemiol Infect. 2015;143:711-719.
Broglia A., Weitzel T., Harms G., Cacció S.M., Nöckler K. Molecular typing of Giardia duodenalis isolates from German travellers. Parasitol Res. 2013;112:3449-56.
Budu-Amoako E., Greenwood S.J., Dixon B.R., Sweet L., Ang L., Barkema H.W., McClure J.T. Molecular epidemiology of Cryptosporidium and Giardia in humans on Prince Edward Island, Canada: evidence of zoonotic transmission from cattle. Zoonoses Public Health. 2012;59:424-33.
Caccio S.M., Thompson R.C.A., McLauchlin J., Smith H.V. Unravelling Cryptosporidium and Giardia epidemiology. Trends Parasitol. 2005;21:430-437.
Cacciò S.M., Ryan U. Molecular epidemiology of giardiasis. Mol Biochem Parasitol. 2008;160:75-80.
Cacciò S.M., Beck R., Lalle M., Marinculic A., Pozio E. Multilocus genotyping of Giardia duodenalis reveals striking differences between assemblages A and B. Int J Parasitol. 2008;38(13):1523-31.
Cacciò S.M., Sprong H. Giardia duodenalis: genetic recombination and its implications for taxonomy and molecular epidemiology. Exp Parasitol. 2010;124(1):107-12.
Caccio S.M., Chalmers R.M. Human cryptosporidiosis in Europe. Clin Microbiol Infect. 2016;22:471-480.
Caffara M., Piva S., Pallaver F., Iacono E., Galuppi R. Molecular characterization of Cryptosporidium spp. from foals in Italy. Vet J. 2013;198:531-3.
Cama V.A., Ross J.M. Crawford S., Kawai V., Chavez-Valdez R., Vargas D., Vivar A., Ticona E., Navincopa M., Williamson J., Ortega Y., Gilman R.H., Bern C., Xiao L. Differences in clinical manifestations among Cryptosporidium species and subtypes in HIV-infected person. J Infect Dis. 2007;196:684-691.
Campbell G.A., Mutharasan R. Near real-time detection of Cryptosporidium parvum oocyst by IgM-functionalized piezoelectric-excited millimeter-sized cantilever biosensor. Biosens Bioelectron. 2008;23:1039–1045.
49
Casemore D.P., Armstrong M., Sands R.L. Laboratory diagnosis of cryptosporidiosis. J Clin Pathol. 1985;38:1337-41.
Castro-Hermida J.A., Garcia-Presedo I., Almeida A., Gonzalez-Warleta M., Correia Da Costa J.M., Mezo M. Detection of Cryptosporidium spp and Giardia duodenalis in surface water: A health risk for humans and animals. Water Res. 2009;43:4133-42.
Causer L.M., Handzel T., Welch P., Carr M., Culp D., Lucht R., Mudahar K., Robinson D., Neavear E., Fenton S., Rose C., Craig L., Arrowood M., Wahlquist S., Xiao L., Lee Y.M., Mirel L., Levy D., Beach M.J., Poquette G., Dworkin M.S. An outbreak of Cryptosporidium hominis infection at an Illinois recreational waterpark. Epidemiol Infect. 2006;134:147-56.
Certad G., Viscogliosi E., Chabé M., Cacciò S.M. Pathogenic mechanisms of Cryptosporidium and Giardia. Trends Parasitol. 2017;33:561-576.
Chako C.Z., Tyler J.W., Schultz L.G., Chiguma L., Beerntsen B.T. Cryptosporidiosis in people: It’s not just about cows. J Vet Intern Med. 2010;24:37-43.
Chalmers R.M., Elwin K., Thomas A.L., Guy E. C., Mason B. Long-term Cryptosporidium typing reveals the aetiology and species-specific epidemiology of human cryptosporidiosis in England and Wales, 2000 to 2003. Euro Surveill. 2009;14(2):pii=19086.https://doi.org/10.2807/ese.14.02.19086-en
Chalmers R.M., Giles M. Zoonotic cryptosporidiosis in the UK - challenges for control. J Appl Microbiol. 2010;109:1487-97.
Chalmers R.M., Campbell B.M., Crouch N., Charlett A., Davies A.P. Comparison of diagnostic sensitivity and specificity of seven Cryptosporidium assays used in the UK. J Med Microbiol. 2011a;60(Pt 11):1598-604.
Chalmers R.M., Smith R., Elwin K., Clifton-Hadley F.A., Giles M. Epidemiology of anthroponotic and zoonotic human cryptosporidiosis in England and Wales, 2004-2006. Epidemiol Infect. 2011b;139:700-712.
Chalmers R.M. and Katzer F. Looking for Cryptosporidium: the application of advances in detection and diagnosis. Trends Parasitol. 2013;29:237-51.
Chartier C., Mallereau M.P., Naciri M. Prophylaxis using paromomycin of natural cryptosporidial infection in neonatal kids. Prev Vet Med. 1996;25:357-361.
Claerebout E., Casaert S., Dalemans A.C., De Wilde N., Levecke B., Vercruysse J., Geurden T. Giardia and other intestinal parasites in different dog populations in Nothern Belgium. Vet Parasitol. 2009;161:41–6.
Costa M., Clarke C., Mitchell S., Papasouliotis K. Diagnostic accuracy of two point-of-care kits for the diagnosis of Giardia species infection in dogs. J Small Anim Pract. 2016;57:318-22.
Cotton J.A., Amat C.B., Buret A.C. Disruptions of host immunity and inflammation by Giardia duodenalis: Potential consequences for co-infections in the gastro-intestinal tract. Pathogens. 2015;4:764-792.
Currie S.L., Stephenson N., Palmer A.S., Jones B.L., Alexander C.L. Under-reporting giardiasis: time to consider the public health implications. Epidemiol Infect. 2017;7:1-5.
50
Da Silva A.S., Castro V.S., Tonin A.A., Brendler S., Costa M.M., Jaques J.A., Bertoletti B., Zanette R.A., Raiser A.G., Mazzanti C.M., Lopes S.T., Monteiro S.G. Secnidazole for the treatment of giaridiasis in naturally infected cats. Parasitol Int. 2011;60:429-32.
De Gooyer T.E., Gregory J., Easton M., Stephens N., Fearnley E., Kirk M. Waterparks are high risk for cryptosporidiosis: A case-control study in Victoria, 2015. Commun Dis Intell Q Rep. 2017;41:E142-E149.
De Souza P.N., Bomfim T.C., Huber F., Abboud L.C., Gomes R.S. Natural infection by Cryptosporidium sp., Giardia sp. and Eimeria leuckarti in three groups of equines with different handlings in Rio de Janeiro. Braz Vet Parasitol. 2009;160, 327–333.
De Waele V., Speybroeck N., Berkvens D., Mulcahy G., Murphy T.M. Control of cryptosporidiosis in neonatal calves: use of halofuginone lactate in two different calf rearing systems. Prev Vet Med. 2010;96(3-4):143-51.
Delport T.C., Asher A.J., Beaumont L.J., Webster K.N., Harcourt R.G., Power M.L. Giardia duodenalis and Cryptosporidium occurrence in Australian sea lions (Neophoca cinerea) exposed to varied levels of human interaction. Int J Parasitol Wildl. 2014;3:269-275.
Di Genova B.M, Tonellli R.R. Infection strategies of intestinal parasite pathogens and host cell responses. Front Microbiol. 2016;7:256.
Efstratiou A., Ongerth J.E., Karanis P. Waterborne transmission of protozoan parasites: Review of worldwide outbreaks – An update 2011-2016. Water Res. 2017;114;14-22.
Einarsson E., Ma’ayeh S., Svärd S.G. An up-date on Giardia and giardiasis. Curr Opin Microbiol. 2016;34:47-52.
El-Gebaly N.S., Halawa E.F., Moussa H.M., Rabia I., Abu-Zekry M. Saliva and sera IgA and IgG in Egyptian Giardia-infected children. Parasitol Res. 2012;111(2):571-5.
Elliot A., Morgan U.M., Thompson R.C. Improved staining method for detecting Cryptosporidium oocysts in stools using malachite green. J Gen Appl Microbiol. 1999;45:139-142.
Enserink R., Mughini-Gras L., Duizer E., Kortbeek T., Van Pelt W. Risk factors for gastroenteritis in child day care. Epidemiol Infect. 2015a;143(13):2707-20.
Enserink R., van den Wijngaard C., Bruijning-Verhagen P., van Asten L., Mughini-Gras L., Duizer E., Kortbeek T., Scholts R., Nagelkerke N., Smit H.A., Kooistra-Smid M., van Pelt W. Gastroenteritis attributable to 16 enteropathogens in children attending day care: significant effects of rotavirus, norovirus, astrovirus, Cryptosporidium and Giardia. Pediatr Infect Dis J. 2015b;34:5-10.
Epe C., Rehkter G., Schnieder T., Lorentzen L., Kreienbrock L. Giardia in symptomatic dogs and cats in Europe – results of a European study. Vet Parasitol. 2010; 173:32–38.
EPISTAT Belgian Infectious Diseases (https://epistat.wiv-isp.be) accessed 02 January 2018.
Esch K.J., Petersen C.A. Transmission and epidemiology of zoonotic protozoal diseases of companion animals. Clin Microbiol Rev. 2013;26:58-85.
Escobedo A.A., Hanevik K., Almirall P., Cimerman S., Alfonso M. Management of chronic Giardia infection. Expert Rev Anti Infect Ther. 2014;12:1143-57 .
51
Escobedo A.A., Ballesteros J., González-Fraile E., Almirall P. A meta-analysis of the efficacy of albendazole compared with tinidazole as treatments for Giardia infections in children. Acta Trop. 2016a;153:120-7.
Escobedo A.A., Lalle M., Hrastnik N.I., Rodríguez-Morales A.J., Castro-Sánchez E., Cimerman S., Almirall P., Jones J. Combination therapy in the management of giardiasis: What laboratory and clinical studies tell us, so far. Acta Trop. 2016b;162:196-205.
Espelage W., an der Heiden M., Stark K., Alpers K. Characteristics and risk factors for symptomatic Giardia lamblia infections in Germany. BMC Public Health. 2010;10:41.
Essid R., Menotti J., Hanen C., Aoun K., Bouratbine A. Genetic diversity of Cryptosporidium isolates from human populations in an urban area of Northern Tunisia. Infect Genet Evol. 2018;58:237-242.
Farzan A., Parrington L., Coklin T., Cook A., Pintar K., Pollari F., Friendship R., Farber J., Dixon B. Detection and characterization of Giardia duodenalis and Cryptosporidium spp. on swine farms in Ontario, Canada. Foodborne Pathog Dis. 2011;8(11):1207-13.
Faubert G. Immune response to Giardia duodenalis. Clin Microbiol Rev. 2000;13:35-54.
Fayer R., Ellis W. Paromomycin is effective as prophylaxis for cryptosporidiosis in dairy calves. J Parasitol. 1993;79(5):771-4.
Fayer R., Santín M. Cryptosporidium xiaoi n. sp. (Apicomplexa: Cryptosporidiidae) in sheep (Ovis aries). Vet Parasitol. 2009;164:192-200.
Fayer R. Taxonomy and species delimitation in Cryptosporidium. Exp Parasitol. 2010;124:90-7.
Feng Y., Xiao L. Zoonotic potential and molecular epidemiology of Giardia species and giardiasis. Clin Microbiol Rev. 2011;24:110-140.
Fiechter R., Deplazes P., Schnyder M. Control of Giardia infections with ronidazole and intensive hygiene management in a dog kennel. Vet Parasitol. 2012;187:93-98.
Figgatt M., Mergen K., Kimelstein D., Mahoney D.M., Newman A., Nicholas D., Ricupero K., Cafiero T., Corry D., Ade J., Kurpiel P., Madison-Antenucci S., Anand M. Giardiasis Outbreak Associated with Asymptomatic Food Handlers in New York State, 2015. J Food Prot. 2017;12:837-841.
Fink M.Y., Singer S.M. The Intersection of Immune Responses, Microbiota, and Pathogenesis in Giardiasis. Trends Parasitol. 2017;33(11):901-913.
Garcés G., Effenberger M., Najdrowski M., Wackwitz C., Gronauer A., Wilderer P.A., Lebuhn M. Quantification of Cryptosporidium parvum in anaerobic digesterstreating manure by (reverse-transcription) quantitative real-time PCR, infectivity and excystation tests. Water Sci Technol. 2006;53(8):195-202.
Garcia L.C. Diagnosis Medical Parasitology. (5. ed.) A.S.M. Press, Washington. 2007.
Garcia L.C. Practical Guide to Diagnostic Parasitology. (2. ed.) A.S.M. Press, Washington. 2009;288–289.
52
García-Cervantes P.C., Báez-Flores M.E., Delgado-Vargas F., Ponce-Macotela M., Nawa Y., De-la-Cruz-Otero M.D., Martínez-Gordillo M.N., Díaz-Camacho S.P. Giardia duodenalis genotypes among school children and their families and pets in urban and rural areas of Sinaloa, Mexico. J Infect Dev Ctries. 2017;11:180-187.
Gautret P., Cramer J.P., Field V., Caumes E., Jensenius M., Gkrania-Klotsas E., de Vries P.J., Grobusch M.P., Lopez-Velez R., Castelli F., Schlagenhauf P., Hervius Askling H., von Sonnenburg F., Lalloo D.G., Loutan L., Rapp C., Basto F., Santos O'Connor F., Weld L., Parola P.; EuroTravNet Network. Infectious diseases among travellers and migrants in Europe, Euro Trav Net 2010. Euro Surveill. 2012;17.
Geurden T., Claerebout E., Vercruysse J., Berkvens D. Estimation of diagnostic test characteristics and prevalence of Giardia duodenalis in dairy calves in Belgium using a Bayesian approach. Int J Parasitol. 2004;34:1121-7.
Geurden T., Vercruysse J., Claerebout E. Field testing of a fenbendazole treatment combined with hygienic and management measures against a natural Giardia infection in calves. Vet Parasitol. 2006a;142:367-371.
Geurden T., Claerebout E., Dursin L., Deflandre A., Bernay F., Kaltsatos V., Vercruysse J. The efficacy of an oral treatment with paromomycin against an experimental infection with Giardia in calves. Vet Parasitol. 2006b;135(3-4):241-7.
Geurden T., Claerebout E., Vercruysse J., Berkvens D. A Bayesian evaluation of four immunological assays for the diagnosis of clinical cryptosporidiosis in calves. Vet J. 2008a;176:400-2.
Geurden T., Thomas P., Casaert S., Vercruysse J., Claerebout E. Prevalence and molecular characterization of Cryptosporidium and Giardia in lambs and goat kids in Belgium. Vet Parasitol. 2008b;155:142-145.
Geurden T., Levecke B., Pohle H., De Wilde N., Vercruysse J., Claerebout E. A Bayesian evaluation of two dip-stick assays for the on-site diagnosis of infection in calves suspected of clinical giardiasis. Vet Parasitol. 2010a;172(3-4):337-40.
Geurden T., Vercruysse J., Claerebout E. Is Giardia a significant pathogen in production animals? Exp Parasitol. 2010b;124:98-106.
Geurden T., Olson M.E. 2011. Giardia in pets and farm animals, and their zoonotic potential. In: Lujàn H.D., Svärd S. (Eds.), Giardia – A Model Organism. Springer Wien NewYork, Wien. pp: 71–92.
Geurden T., Pohle H., Sarre C., Dreesen L., Vercruysse J., Claerebout E. The efficacy of a treatment with fenbendazole against an experimental Giardia duodenalis infection in lambs. Small Rumin Res. 2011;96:211-215.
Giadinis N.D., Papadopoulos E., Panousis N., Papazahariadou M., Lafi S.Q., Karatzias H. Effect of halofuginone lactate on treatment and prevention of lamb cryptosporidiosis: an extensive field trial. Vet Pharmacol Ther. 2007;30(6):578-82.
Goodgame R.W., Genta R.M., White A.C., Chappell C.L. Intensity of infection in AIDS-associated cryptosporidiosis. J Infect Dis. 1993;167:704-9.
53
Gotfred-Rasmussen H., Lund M., Enemark H.L., Erlandsen M., Petersen E. Comparison of sensitivity and specificity of 4 methods for detection of Giardia duodenalis in feces: immunofluorescence and PCR are superior to microscopy of concentrated iodine-stained samples. Diagn Microbiol Infect Dis. 2016;84(3):187-90.
Grinberg A., Pomroy W.E., Squires R.A., Scuffham A., Pita A., Kwan E. Retrospective cohort study of an outbreak of cryptosporidiosis caused by a rare Cryptosporidium parvum subgenotype. Epidemiol Infect. 2011;139(10):1542-50.
Grit G.H., Bénéré E., Ehsan A., De Wilde N., Claerebout E., Vercruysse J., Maes L., Geurden T. Giardia duodenalis cyst survival in cattle slurry. Vet Parasitol. 2012;184:330-4.
Grit G.H., Van Coppernolle S., Devriendt B., Geurden T., Dreesen L., Hope J., Vercruysse J., Cox E., Geldhof P., Claerebout E. Evaluation of cellular and humoral systemic immune response against Giardia duodenalis infection in cattle. Vet Parasitol. 2014;202:145-155.
Guzman-Herrador B., Carlander A., Ethelberg S., Freiesleben de Blasio B., Kuusi M., Lund V., Löfdahl M., MacDonald E., Nichols G., Schönning C., Sudre B., Trönnberg L., Vold L., Semenza J.C., Nygård K. Waterborne outbreaks in the Nordic countries, 1998 to 2012. Euro Surveill. 2015;18:20.
Hadjichristodoulou C., Gkikas A., Pediatidis Y., Tselentis Y. Outbreak of giardiasis among English tourists in Crete. Lancet. 1998;351:65-6.
Halliez M.C., Buret A.G. Extra-intestinal and long term consequences of Giardia duodenalis infections. World J Gastroenterol. 2013;19(47):8974-85.
Hajdu A., Vold L., Østmo T.A., Helleve A., Helgebostad S.R., Krogh T., Robertson L., de Jong B., Nygård K. Investigation of Swedish casesreveals an outbreak of cryptosporidiosis at a Norwegian hotel with possible links to in-house water systems. BMC Infect Dis. 2008;8:152.
Hamnes I.S., Gjerde B.K., Robertson L.J. A longitudinal study on the occurrence of Cryptosporidium and Giardia in dogs during their first year of life. Acta Vet Scand. 2007;49:22.
Hardie R.M., Wall P.G., Gott P., Bardhan M., Bartlett L.R. Infectious diarrhoea in tourists staying in a resort hotel. Emerg Infect Dis. 1999;5:168-71.
Heyworth M.F. Giardia duodenalis genetic assemblages and hosts. Parasite. 2016;23:13.
Hofstra N., Bouwman A.F., Beusen A.H., Medema G.J. Exploring global Cryptosporidium emissions to surface water. Sci Total Environ. 2013;442:10-9.
Holubova N., Sak B., Horcickova M., Hlaskova L., Kvetonova D., Menchaca S., McEvoy J., Kvac M. Cryptosporidium avium n. Sp. (Apicomplexa: Cryptosporidiidae) in birds. Parasitol. Res. 2016;115:2243-2251.
Hopkins J., Hague H., Hudgin G., Ross L., Moore D. An outbreak of Cryptosporidium at a recreational water park in Niagara Region, Canada. J Environ Health. 2013;75:28-33.
Hoque M., Hope V., Scragg R., Kjellstrom T. Children at risk of giardiasis in Auckland: a case-control analysis. Epidemiol Infect. 2003;131:655-662.
Huang D.B., White A.C. An updated review on Cryptosporidium and Giardia. Gastroenterol Clin North Am. 2006;35:291-314.
Inácio S.V., Gomes J.F., Oliveira B.C.,Falcão A.X., Suzuki C.T., Dos Santos B.M., de Aquino M.C., de Paula Ribeiro R.S., de Assunção D.M., Casemiro P.A., Meireles M.V., Bresciani K.D.
54
Validation of a new technique to detect Cryptosporidium spp. oocysts in bovine feces. Prev Vet Med. 2016;134:1-5.
Jenikova M., Nemejc K., Sak B., Kvetonova D., Kvac M. New view on the age-specificity of pig Cryptosporidium by species-specific primers for distinguishing Cryptosporidium suis and Cryptosporidium pig genotype II. Vet Parasitol. 2011;176:120-125.
Johnson E., Atwill E.R., Filkins M.E., Kalush J. The prevalence of shedding of Cryptosporidium and Giardia spp based on a single faecal sample collection from each of 91 horses used for back country recreation. J Vet Diagn Invest. 1997;9:56-60.
Johnson J., Buddle R., Reid S., Armson A., Ryan U.M. Prevalence of Cryptosporidium genotypes in pre and post- weaned pigs in Australia. Exp Parasitol. 2008;119:418-421.
Jokipii A.M., Jokipii L. Prepatency of giardiasis. Lancet. 1977;1(8021):1095-7.
Jones M., Boccia D., Kealy M., Salkin B., Ferrero A., Nichols G., Stuart J.M. Cryptosporidium outbreak linked to interactive water feature, UK: importance of guidelines. Euro Surveill. 2006;11:126-8.
Jones B.A., Grace D., Kock R., Alonso S., Rushton J., Said M.Y., McKeever D., Mutua F., Young J., McDermott J., Pfeiffer D.U. Zoonosis emergence linked to agricultural intensification and environmental change. Proc Natl Acad Sci U S A. 2013;356:983-989.
Kang C.D., Cao C., Lee J., Choi I.S., Kim B.W., Sim S.J. Surface plasmon resonance-based inhibition assay for real-time detection of Cryptosporidium parvum oocysts. Water Res. 2008;42:1693–1699.
Karanis P., Kourenti C., Smith H. Waterborne transmission of protozoan parasites: a worldwide review of outbreaks and lessons learnt. J Water Health. 2007;5(1):1-38.
Khan S.M., Debnath C., Pramanik A.K., Xiao L., Nozaki T., Ganguly S. Molecular evidence for zoonotic transmission of Giardia duodenalis among dairy farm workers in West Bengal, India. Vet Parasitol. 2011;178:342-345.
Khan A., Shaik J.S., Grigg M.E. Genomics and molecular epidemiology of Cryptosporidium species. Acta Trop. 2017;pii: S0001-706X(17)30889-6.
Kirk M.D., Pires S.M., Black R.E., Caipo M., Crump J.A., Devleesschauwer B., Döpfer D., Fazil A., Fischer-Walker C.L., Hald T., Hall A.J., Keddy K.H., Lake R.J., Lanata C.F., Torgerson P.R., Havelaar A.H., Angulo F.J. World Health Organization Estimates of the Global and Regional Disease Burden of 22 Foodborne Bacterial, Protozoal, and Viral Diseases, 2010: A Data Synthesis. PLoS Med. 2015;12(12):e1001921.
Kirkpatrick C.E., Farrell J.P. Feline giardiasis: observations on natural and induced infections. Am J Vet Res. 1984;45(10):2182-8.
Kirkpatrick C.E., Skand D.L. Giardiasis in a horse. J Am Vet Med Assoc. 1985;187:163-4.
Koehler A.V., Jex A.R., Haydon S.R., Stevens M.A., Gasser R.B. Giardia/giardiasis- a perspective on diagnostic and analytical tools. Biotechnol Adv. 2014;32:280-9.
Korich D.G., Mead J.R., Madore M.S., Sinclair N.A., Sterling C.R. Effects of ozone, chlorine dioxide, chlorine, and monochloramine on Cryptosporidium parvum oocyst viability. Appl Environ Microbiol. 1990;56:1423-8.
55
Kuhnert-Paul Y., Bangoura B., Dittmar K., Daugschies A., Schmäschke R. Cryptosporidiosis: comparison of three diagnostic methods and effects of storage temperature on detectability of cryptosporidia in cattle faeces. Parasitol Res. 2012;111:165-71.
Kváč M., Kvetonová D., Sak B., Ditrich O. Cryptosporidium pig genotype II in immunocompetent man. Emerg Infect Dis. 2009a;15:982-3.
Kváč M., Hanzlikova D., Sak B., Kvetonova D. Prevalence and age-related infection of Cryptosporidium suis, C. muris and Cryptosporidium pig genotype II in pigs on a farm complex in the Czech Republic. Vet Parasitol. 2009b;160:319-322.
Kváč M., Kestřánová M., Pinková M., Květoňová D., Kalinová J., Wagnerová P., Kotková M., Vítovec J., Ditrich O., McEvoy J., Stenger B., Sak B. Cryptosporidium scrofarum n. sp. (Apicomplexa: Cryptosporidiidae) in domestic pigs (Sus scrofa). Vet Parasitol. 2013;191(3-4):218-27.
Kváč M., Nemejc K., Kestranova M., Kvetonova D., Wagnerova P., Kotkova M., Rost M., Samkova E., McEvoy J., Sak B. Age related susceptibility of pigs to Cryptosporidium scrofarum infection. Vet Parasitol. 2014;202:330-334.
Kváč M., Havrdova N., Hlaskova L., Dankova T., Kandera J., Jezkova J. Vitovec J., Sak B., Ortega Y., Xiao L., Modry D., Chelladurai J.R., Prantlova V., McEvoy J. Cryptosporidium proliferans n. sp. (apicomplexa: Cryptosporidiidae): molecular and biological evidence of cryptic species within Gastric Cryptosporidium of mammals. PLoS One. 2016;11.
Laatamna A.E., Wagnerova P., Sak B., Kvetonova D., Xiao L., Rost M., Mc Evoy J., Saadi A.R., Aissi M., Kvac M. Microsporidia and Cryptosporidium in horses and donkeys in Algeria: detection of novel Cryptosporidium hominis subtype family (Ik) in a horse. Vet Parasitol. 2015;208:135-142.
Lal A., Hales S. Heterogeneity in hotspots: spatio-temporal patterns in neglected parasitic diseases. Epidemiol Infect. 2015;143(3):631-9.
Lal A., Marshall J., Benschop J., Brock A., Hales S., Baker M.G., French N.P.. A Bayesian spatio-temporal framework to identify outbreaks and examine environmental and social risk factors for infectious diseases monitored by routine surveillance. Spat Spatiotemporal Epidemiol. 2018;25:39-48.
Lalle M., Jimenez-Cardosa E., Caccio S.M., Pozio E. Genotyping of Giardia duodenalis from humans and dogs from Mexico using a beta-giardin nested polymerase chain reaction assay. J Parasitol. 2005;91:203-205.
Lane S., Lloyd D. Current trends in research into the waterborne parasite Giardia. Crit Rev Microbiol. 2002;28:123-47.
Langkjaer R.B., Vigre H., Enemark H.L., Maddox-Hyttel C. Molecular and phylogenetic characterization of Cryptosporidium and Giardia from pigs and cattle in Denmark. Parasitology. 2007;134:339-350.
Laurent F., Lacroix-Lamandé S. Innate immune responses play a key role in controlling infection of the intestinal epithelium by Cryptosporidium. Int J Parasitol. 2017;47(12):711-721.
Lebbad M., Petersson I., Karlsson L., Botero-Kleiven S., Andersson J.O., Svenungsson B., Svärd S.G. Multilocus genotyping of human Giardia isolates suggests limited zoonotic
56
transmission and association between assemblage B and flatulence in children. PLoS Negl Trop Dis. 2011;5:e1262.
Lemieux M.W., Sonzogni-Desautels K., Ndao M. Lessons Learned from Protective Immune Responses to Optimize Vaccines against Cryptosporidiosis. Pathogens. 2017;7(1). pii: E2.
Lennette E.H., Balows A., Hausler W.J., Truant J.P. -Manual of Clinical Microbiology.4. ed. Washington, American Society for Microbiology, 1985.
Leonhard S., Pfister K., Beelitz P., Wielinga C., Thompson R.C. The molecular characterisation of Giardia from dogs in southern Germany. Vet Parasitol. 2007;150:33-38.
Lin Q., Wang X.Y., Chen J.W., Ding L., Zhao G.H. Cryptosporidium suis infection in post-weaned and adult pigs in Shaanxi province, northwestern China. Korean J Parasitol. 2015;53(1):113-7.
Lopez-Romero G., Quintero J., Astiazarán-García H., Velazquez C. Host defences against Giardia lamblia. Parasite Immunol. 2015;37(8):394-406.
Lucio-Forster A., Griffiths J.K., Cama V.A., Xiao L., Bowman D.D. Minimal zoonotic risk of cryptosporidiosis from pet dogs and cats. Trends Parasitol. 2010;26:174-9.
Manahan F.F. Diarrhoea in horses with particular reference to a chronic diarrhoea syndrome. Aust Vet J. 1970;46:231-4.
Mancassola R., Reperant J.M., Naciri M., Chartier C. Chemoprophylaxis of Cryptosporidium parvum infection with paromomycinin kids and immunological study. Antimicrob Agents Chemother. 1995;39:75-78.
Marshall M., Naumovitz D., Ortega Y., Sterling C. Waterborne protozoan pathogens. Clin Microbiol Rev. 1997;10:67-85.
McClung R.P., Roth D.M., Vigar M., Roberts V.A., Kahler A.M., Cooley L.A., Hilborn E.D., Wade T.J., Fullerton K.E., Yoder J.S., Hill V.R. Waterborne Disease Outbreaks Associated With Environmental and Undetermined Exposures to Water - United States, 2013-2014. MMWR Morb Mortal Wkly Rep. 2017;66:1222-1225.
McLauchlin J., Amar C., Pedraza-Diaz S., Nichols G.L. Molecular epidemiological analysis of Cryptosporidium spp in the United Kingdom: Results of genotyping Cryptosporidium spp in 1,705 faecal samples from humans and 105 faecal samples from livestock animals. J Clin Microbiol. 2000;38:3984-3990.
Monis P.T., Andrews R.H., Mayrhofer G., Ey P.L. Genetic diversity within the morphological species Giardia intestinalis and its relationship to host origin. Infect Genet Evol. 2003;3:29-38.
Mørch K., Hanevik K., Rivenes A.C., Bødtker J.E., Næss H., Stubhaug B., Wensaas K.A., Rortveit G., Eide G.E., Hausken T., Langeland N. Chronic fatigue syndrome 5 years after giardiasis: differential diagnoses, characteristics and natural course. BMC Gastroenterol. 2013;13:28.
Moreira N.A., Bondelind M. Safe drinking water and waterborne outbreaks. J Water Health. 2017;15(1):83-96.
57
Morgan U.M., Monis P.T., Xiao L., Limor J., Sulaiman I., Raidal S., O'Donoghue P., Gasser R., Murray A., Fayer R., Blagburn B.L., Lal A.A., Thompson R.C. Molecular and phylogenetic characterisation of Cryptosporidium from birds. Int J Parasitol. 2001;31:289-96.
Moron-Soto M., Gutierrez L., Sumano H., Tapia G., Alcala-Canto Y. Efficacy of nitazoxanide to treat natural Giardia infections in dogs. Parasit Vectors. 2017;10(1):52.
Mueller-Doblies D., Giles M., Elwin K., Smith R.P., Clifton-Hadley F.C., Chalmers R.M. Distribution of Cryptosporidium species in sheep in the UK. Vet Parasitol. 2008;154:214–219.
Muhsen K., Levine M.M. A systematic review and meta-analysis of the association between Giardia lamblia and endemic pediatric diarrhea in developing countries. Clin Infect Dis. 2012;55.
Murray R., Tataryn J., Pintar K., Thomas M.K. Estimates of the burden of illness for eight enteric pathogens associated with animal contact in Canada. Epidemiol Infect. 2017;145:3413-3423.
Muthusamy D., Rao S.S., Ramani S., Monica B., Banerjee I., Abraham O.C., Mathai D.C., Primrose B., Muliyil J., Wanke C.A., Ward H.D., Kang G. Multilocus genotyping of Cryptosporidium sp. isolates from human immunodeficiency virus-infected individuals in South India. J Clin Microbiol. 2006;44:632-634.
Naciri M., Mancassola R., Yvore P., Peeters J.E. The effect of halofuginone lactate on experimental Cryptosporidium parvum infections in calves. Vet Parasitol. 1993;45:199-207.
Naess H., Nyland M., Hausken T., Follestad I., Nyland H.I. Chronic fatigue syndrome after Giardia enteritis: clinical characteristics, disability and long-term sickness absence. BMC Gastroenterol. 2012;12:13.
Nash T.E., Herrington D.A., Losonsky G.A., Levine M.M. Experimental human infections with Giardia lamblia. J Infect Dis. 1987;156:974-84.
Ng J., Yang R., Whiffin V., Cox P., Ryan U. Identification of zoonotic Cryptosporidium and Giardia genotypes infecting animals in Sydney’s water catchments. Exp Parasitol. 128;138-144.
Ni Loo C.S., Kei Lam N.S., Yu D., Su X.Z., Lu F. Artemisinin and its derivatives in treating protozoan infections beyond malaria. Pharmacol Res. 2016;117:192-217.
Nygård K., Schimmer B., Søbstad Ø., Walde A., Tveit I., Langeland N., Hausken T., Aavitsland P. A large community outbreak of waterborne giardiasis-delayed detection in a non-endemic urban area. BMC Public Health. 2006;6:141.
O’ Handley R.M., Cockwill C., Jelinski M., McAllister T.A., Olson M.E. Effects of repeat fenbendazole treatment in dairy calves with giardiosis on cyst excretion, clinical signs and production. Vet Parasitol. 2000;89:209-218.
O’Handley R.M., Ceri H., Anette C., Olson M.E. Passive immunity and serological immune response in dairy calves associated with natural Giardia duodenalis infections. Vet Parasitol. 2003;113:89-98.
Olson M.E., Thorlakson C.L., Deselliers L., Morck D.W., McAllister T.A. Giardia and Cryptosporidium in Canadian farm animals. Vet Parasitol. 1997;68:375-81.
58
Olson M.E., Goh J., Phillips M., Guselle N., Mc Allister T.A. Giardia cyst and Cryptosporidium oocyst survival in water, soil, and cattle faeces. J Environ Qual. 1999;28:1991-1996.
Osman M., Bories J., El Safadi D., Poirel M., Gantois N., Benamrouz-Vanneste S., Delhaes L., Hugonnard M., Certad G., Zenner L., Viscogliosi E. Prevalence and genetic diversity of the intestinal parasites Blastocystis sp. and Cryptosporidium spp. in household dogs in France and evaluation of zoonotic transmission risk. Vet Parasitol. 2015;214:167–70.
Osterholm M.T., Forfang J.C., Ristinen T.L., Dean A.G., Washburn J.W., Godes J.R., Rude R.A., McCullough J.G. An outbreak of foodborne giardiasis. N Engl J Med. 1981;304:24-8.
Paerewijck O., Maertens B., Dreesen L., Van Meulder F., Peelaers I., Ratman D., Li R.W., Lubberts E., De Bosscher K., Geldhof P. Interleukin-17 receptor A (IL-17RA) as a central regulator of the protective immune response against Giardia. Sci Rep. 2017;7(1):8520.
Painter J.E., Gargano J.W., Yoder J.S., Collier S.A., Hlavsa M.C. Evolving epidemiology of reported cryptosporidiosis cases in the United States, 1995-2012. Epidemiol Infect. 2016;144:1792-802.
Pallant L., Barutzki D., Schaper R., Thompson R.C. The epidemiology of infections with Giardia species and genotypes in well cared for dogs and cats in Germany. Parasit Vectors. 2015;8:2.
Palmer C.S., Thompson R.C.A., Traub R.J., Rees R., Robertson I.D. National study of the intestinal parasites of dogs and cats in Australia. Vet Parasitol. 2008;151:181–90.
Panini R., Carreras G., Marangi M., Mancianti F., Giangaspero A. Use of a commercial enzyme-linked immunosorbent assay for rapid detection of Giardia duodenalis in dog stools in the environment: a Bayesian evaluation. J Vet Diagn Invest. 2013;25:418-422.
Payne P.A., Ridley R.K., Dryden M.W., Bathgate C., Milliken G.A., Stewart P.W. Efficacy of a combination febantel–praziquantel–pyrantel product, with or without vaccination with a commercial Giardia vaccine, for treatment of dogs with naturally occurring giardiasis. J Am Vet Med Assoc. 2002;220:330–333.
Pavlásek I., Hess L., Stehlík I., Stika V. The first detection of Giardia spp. in horses in the Czech Republic. Vet Med. 1995;40:81–86.
Pavlasek I., Ryan U. The first finding of a natural infection of Cryptosporidium muris in a cat. Vet Parasitol. 2007;144:349-52.
Peletz R., Mahin T., Elliott M., Montgomery M., Clasen T. Preventing cryptosporidiosis: the need for safe drinking water. Bull World Health Organ. 2013;91:238-8A.
Peng X., Murphy T., Holden N.M. Evaluation of the effect of temperature on the die-off rate for Cryptosporidium parvum oocysts in water, soils, and feces. Appl Environ Microbiol. 2008;74:7101-7.
Petermann J., Paraud C., Pors I., Chartier C. Efficacy of halofuginone lactate against experimental cryptosporidiosis in goat neonates. Vet Parasitol. 2014;202(3-4):326-9.
Petersen H.H., Jianmin W., Katakam K.K., Mejer H., Thamsborg S.M., Dalsgaard A., Olsen A., Enemark H.L. Cryptosporidium and Giardia in Danish organic pig farms: Seasonal and age-
59
related variation in prevalence, infection intensity and species/genotypes. Vet Parasitol. 2015;214(1-2):29-39.
Petry F., Jakobi V., Tessema T.S. Host immune response to Cryptosporidium parvum infection. Exp Parasitol. 2010;126(3):304-9.
Pijnacker R., Mughini-Gras L., Heusinkveld M., Roelfsema J., van Pelt W., Kortbeek T. Different risk factors for infection with Giardia lamblia assemblages A and B in children attending day-care centres. Eur J Clin Microbiol Infect Dis. 2016;35(12):2005-2013.
Plutzer J., Ongerth J. and Karanis P. Giardia taxonomy, phylogeny and epidemiology: Facts and open questions. J Hyg Environ Health. 2010;213:321-333.
Polak K.C., Levy J.K., Crawford P.C., Leutenegger C.M., Moriello K.A. Infectious diseases in large-scale cat hoarding investigations. Vet J. 2014;201:189–95.
Pollock K.G., Ternent H.E., Mellor D.J., Chalmers R.M., Smith H.V., Ramsay C.N., Innocent G.T. Spatial and temporal epidemiology of sporadic human cryptosporidiosis in Scotland. Zoonoses Public Health. 2010;57(7-8):487-92.
Prystajecky N., Tsui C.K., Hsiao W.W., Uyaguari-Diaz M.I., Ho J., Tang P., Isaac-Renton J. Giardia spp. Are Commonly Found in Mixed Assemblages in Surface Water, as Revealed by Molecular and Whole-Genome Characterization.Appl Environml Microbiol. 2015;81(14):4827–4834.
Putignani L., Menichella D. Global distribution, public health and clinical impact of the protozoan pathogen Cryptosporidium. Interdiscip Perspect Infect Dis. 2010;2010.
Qi M., Zhou H., Wang H., Wang R., Xiao L., Arrowood M.J., Li J., Zhang L. Molecular identification of Cryptosporidium spp and Giardia duodenalis in grazing horses from Xinjiang, China. Vet Parasitol. 2015;209:169-172.
Quilez J., Torres E., Chalmers R.M., Hadfield S.J., Cacho E., Sanchez-Acedo C. Cryptosporidium genotypes and subtypes in lambs and goat kids in Spain. Appl Environ Microbiol. 2008;74:6026–6031.
Robertson L.J., Hermansen L., Gjerde B.K. Occurrence of Cryptosporidium oocysts and Giardia cysts in sewage in Norway. Appl Environ Microbiol. 2006;72(8):5297-303.
Robertson L.J. The potential for marine bivalve shellfish to act as transmission vehicles for outbreaks of protozoan infections in humans: a review. Int J Food Microbiol. 2007;120:201-16.
Robertson L.J. Giardia and Cryptosporidium infections in sheep and goats: a review of the potential for transmission to humans via environmental contamination. Epidemiol Infect. 2009;137:913-921.
Robertson L.J., Hanevik K., Escobedo A.A., Morch K., Langeland N. Giardiasis- why do the symptoms sometimes never stop? Trends Parasitol. 2010;26:75-82.
Robertson L.J., Chalmers R.M. Foodborne cryptosporidiosis: is there really more in Nordic countries? Trends Parasitol. 2013;29:3-9.
60
Rosa L.A., Gomes M.A., Mundim A.V., Mundim M.J., Pozzer E.L., Faria E.S., Viana J.C., Cury M.C. Infection of dogs by experimental inoculation with human isolates of Giardia duodenalis: clinical and laboratory manifestations. Vet Parasitol. 2007;145(1-2):37-44.
Ryan U., Caccio S.M. Zoonotic potential of Giardia. Int J Parasitol. 2013;43:943-956.
Ryan U., Fayer R., Xiao L. Cryptosporidium species in humans and animals: current understanding and research needs. Parasitology. 2014;141:1667-85.
Ryan U., Paparini A., Tong K., Yang R., Gibson-Kueh S., O'Hara A., Lymbery A., Xiao L. Cryptosporidium huwin. sp. (Apicomplexa: Eimeriidae) from the guppy (Poecilia reticulata). Exp Parasitol. 2015;150:31-5.
Ryan U., Zahedi A., Paparini A. Cryptosporidium in humans and animals-a one health approach to prophylaxis. Parasite Immunol. 2016a;38:535-47.
Ryan U., Paparini A., Monis P., Hijjawi N. It’s official- Cryptosporidium is a gregarine: What are the implications for the water industry? Water Res. 2016b;105:305-313.
Ryan U., Lawler S., Reid S. Limiting swimming pool outbreaks of cryptosporidiosis - the roles of regulations, staff, patrons and research. J Water Health. 2017;15:1-16.
Sagebiel D., Weitzel T., Stark K., Leitmeyer K. Giardiasis in kindergartens: prevalence study in Berlin, Germany, 2006. Parasitol Res. 2009;105(3):681-7.
Saleh M.N., Gilley A.D., Byrnes M.K., Zajac A.M. Development and evaluation of a protocol for control of Giardia duodenalis in a colony of group-housed dogs at a veterinary medical college. J Am Vet Med Assoc. 2016;249(6):644-9.
Santín M., Trout J.M., Vecino J.A., Dubey J.P., Fayer R. Cryptosporidium, Giardia and Enterocytozoon bieneusi in cats from Bogota (Colombia) and genotyping of isolates. Vet Parasitol. 2006;141(3-4):334-9.
Santin M., Trout J.M., Fayer R. Prevalence and molecular characterization of Cryptosporidium and Giardia species and genotypes in sheep in Maryland. Vet Parasitol. 2007;146:17–24.
Santin M. Clinical and subclinical infections with Cryptosporidium in animals. N Z Vet J. 2013;61:1-10.
Santin M., Cortes Vecino J.A., Fayer R. A large scale molecular study of Giardia duodenalis in horses from Colombia. Vet Parasitol. 2013;196, 31–36.
Savioli L., Smith H., Thomson A. Giardia and Cryptosporidium join the ‘Neglected Diseases Initiative’. Trends Parasitol. 2006;22:203-208.
Scallan E., Hoekstra R.M., Angulo F.J., Tauxe R.V., Widdowson M., Roy S.L., Jones J.L., Griffin P.M. Foodborne illness acquired in the United States-Major pathogens. Emerg Infect Dis. 2011;17:7-15.
Scaramozzino P., Di Cave D., Berrilli F., D’Orazi C.D., Spaziani A., Mazzanti S., Scholl F., De Liberato C.A. Study of the prevalence and genotypes of Giardia duodenalis infecting kenneled dogs. Vet J. 2009;182:231–4.
61
Schubnell F., von Ah S., Graage R., Sydler T., Sidler X., Hadorn D., Basso W. Occurrence, clinical involvement and zoonotic potential of endoparasites infecting Swiss pigs. Parasitol Int. 2016;65(6 Pt A):618-624.
Scorza A.V., Lappin M.R. An update in three important protozoan parasitic infections in cats: cryptosporidiosis, giardiasis, and tritrichomoniasis. Vet Med. 2006;18-32.
Scorza V., Tangtrongsup S. Update on the diagnosis and management of Cryptosporidium spp infections in dogs and cats. Top Companion Anim. 2010;25:163-9.
Semenza J.C., Nichols G. Cryptosporidiosis surveillance and water-borne outbreaks in Europe. Euro Surveill. 2007;12:E13-4.
Serradell M.C., Saura A., Rupil L.L., Gargantini P.R., Faya M.I., Furlan P.J., Lujan H.D. Vaccination of domestic animals with a novel oral vaccine prevents Giardia infections, alleviates signs of giardiasis and reduces transmission to humans. Npj Vaccines. 2016;1:16018.
Shahiduzzaman M.d, Daugschies A. Therapy and prevention of cryptosporidiosis in animals. Vet Parasitol. 2012;188:203-214.
Shirley D.A.T., Moonah S.N., Kotloff K.L. Burden of disease from Cryptosporidiosis. Curr Opin Infect Dis. 2012;25(5): 555–563.
Singer S.M., Nash T.E. T–cell-dependent control of acute Giardia lamblia infections in mice. Infect. Immun. 2000;68:170-175.
Smith A., Reacher M., Smerdon W., Adak G.K., Nichols G., Chalmers R.M. Outbreaks of waterborne infectious intestinal disease in England and Wales, 1992-2003. Epidemiol Infect. 2006a;134:1141-1149.
Smith H.V., Caccio S.M., Tait A., McLauchlin J., Thompson R.C. Tools for investigating the environmental transmission of Cryptosporidium and Giardia infections in humans. Trends Parasitol. 2006b;22:160-167.
Smith R.P., Chalmers R.M., Mueller-Doblies D., Clifton-Hadley F.A., Elwin K., Watkins J., Paiba G.A., Hadfield S.J., Giles M. Investigation of farms linked to human patients with cryptosporidiosis in England and Wales. Prev Vet Med. 2010;94:9-17.
Soares R., Tasca T. Giardiasis: an update review on sensitivity and specificity of methods for laboratorial diagnosis. J Microbiol Methods. 2016;129:98-102.
Speich B., Croll D., Fürst T., Utzinger J., Keiser J. Effect of sanitation and water treatment on intestinal protozoa infection: a systematic review and meta-analysis. Lancet Infect Dis. 2016;16:87-99.
Sprong H., Cacciò S.M., van der Giessen J.W.; ZOOPNET network and partners. Identification of zoonotic genotypes of Giardia duodenalis. PLoS Negl Trop Dis. 2009;3(12):e558.
Squire S.A., Ryan U. Cryptosporidium and Giardia in Africa: current and future challenges. Parasit Vectors. 2017;10:195.
Stefanogiannis N., McLean M., Van Mil H. Outbreak of cryptosporidiosis linked with a farm event. N Z Med J. 2001;114:519-521.
Sulaiman I.M., Lal A.A., Xiao L. Molecular phylogeny and evolutionary relationships of Cryptosporidium parasites at the actin locus. J Parasitol. 2002;88:388-94.
62
Szenasi Z., Marton S., Kuscera I., Tanczos B., Horvath K., Orosz E., Lucacs Z., Szeidemann. Preliminary investigation of the prevalence and genotype distribution of Giardia intestinalis in dogs in Hungary. Parasitol Res. 2007;101:S145-S152.
Taherkhani H., Hajilooi M., Fallah M., Khyanbanchi O., Haidari M. Gene polymorphism in transforming growth factor-beta codon 10 is associated with susceptibility to giardiasis. Int J Immuogenet. 2009;36:345-349.
Tangtrongsup S., Scorza V. Update on the diagnosis and management of Giardia spp infections in dogs and cats. Top Companion Anim Med. 2010;25:155-162.
The ANOFEL Cryptosporidium National Network. Laboratory-based surveillance for Cryptosporidium in France, 2006-2009. Euro Surveill. 2010;15(33):pii=19642 http://www.eurosurveillance.org.
Thompson R.C., Monis P.T. Variation in Giardia: implications for taxonomy and epidemiology. Adv Parasitol. 2004;58:69-137.
Thompson R.C.A., Olson M.E., Zhu G., Enomoto S., Abrahamsen M.S., Hijjawi N.S. Cryptosporidium and Cryptosporidiosis. Adv. Parasitol. 2005;59:77-158.
Thompson A.R.C., Palmer C.S., O’Handley R. The public health and clinical significance of Giardia and Cryptosporidium in domestic animals. Vet. J. 2008;177:18-25.
Thompson R.C.A., Kutz S.J., Smith A. Parasite zoonoses and wildlife: emerging issues. Int J Env Res Pub Hlth. 2009; 6:678-693.
Thompson R.C., Ash A. Molecular epidemiology of Giardia and Cryptosporidium infections. Infect Genet Evol. 2016;40:315-23.
Thomson S., Hamilton C.A., Hope J.C., Katzer F., Mabbott N.A., Morrison L.J., Innes E.A. Bovine cryptosporidiosis: impact, host-parasite interaction and control strategies. Vet Res. 2017;48:42.
Traub R.J., Robertson P., Irwin P., Mencke N., Monis P., Thompson R.C. Humans, dogs and parasitic zoonoses-unravelling the relationships in a remote endemic community in northeast India using molecular tools. Parasitol Res. 2003;90:156-157.
Traversa D., Otranto D., Milillo P., Latrofa M.S., Giangaspero A., Di Cesare A., Paoletti B. Giardia duodenalis sub-assemblage of animal and human origin in horses. Infect Genet Evol. 2012;12, 1642–1646.
Tysnes K.R., Skancke E., Robertson L. Subclinical Giardia in dogs: a veterinary conundrum relevant to human infection. Trends in Parasitology. 2014;30 (11):520-527.
Tzanidakis N., Sotiraki S., Claerebout E., Ehsan A., Voutzourakis N., Kostopoulou D., Stijn C., Vercruysse J., Geurden T. Occurrence and molecular characterization of Giardia duodenalis and Cryptosporidium spp. in sheep and goats reared under dairy husbandry systems in Greece. Parasite. 2014;21:45.
Upjohn M., Cobb C., Monger J., Geurden T., Claerebout E., Fox M. Prevalence, molecular typing and risk factor analysis for Giardia duodenalis infections in dogs in a central London rescue shelter. Vet Parasitol. 2010;172(3-4):341-6.
63
Ural K., Aysul N., Voyvoda H., Ulutas B., Aldemir O.S., Eren H. Single dose of secnidazole treatment against naturally occurring Giardia duodenalis infection in Sakiz lambs. Revista MVZ Cordoba. 2014;19:4023-4032.
Utsi L., Smith S.J., Chalmers R.M., Padfield S. Cryptosporidiosis outbreak in visitors of a UK industry-compliant petting farm caused by a rare Cryptosporidium parvum subtype: a case-control study. Epidemiol Infect. 2016;144:1000-9.
Valcour J.E., Charron D.F., Berke O., Wilson J.B., Edge T., Waltner-Toews D. A descriptive analysis of the spatio-temporal distribution of enteric diseases in New Brunswick, Canada. BMC Public Health. 2016;16:204.
Vermeulen L., Benders J., Medema G., Hofstra N. Global Cryptosporidium loads from livestock manure. Environ Sci Technol. 2017;51:8663-8671.
Veronesi F., Passamonti F., Caccio S., Diaferia M., Fioretti D.P. Epidemiological survey on equine Cryptosporidium and Giardia infections in Italy and molecular characterization of isolates. Zoonoses Public Health. 2010;57:510-7.
Viu M., Quílez J., Sánchez-Acedo C., del Cacho E., López-Bernad F. Field trial on the therapeutic efficacy of paromomycin on natural Cryptosporidium parvum infections in lambs. Vet Parasitol. 2000;90(3):163-70.
Wang L., Zhang H., Zhao X., Zhang L., Zhang G., Guo M., Liu L., Feng Y., Xiao L. Zoonotic Cryptosporidium species and Enterocytozoon bieneusi genotypes in HIV-positive patients on antiretroviral therapy. J Clin Microbiol. 2013; 51:557–563.
Wells B. Controlling Cryptosporidium in the environment. Vet Rec. 2015;176:615-6.
Wensaas K.A., Langeland N., Hanevik K., Mørch K., Eide G.E., Rortveit G. Irritable bowel syndrome and chronic fatigue 3 years after acute giardiasis: historic cohort study. Gut. 2012;61(2):214-9.
Westermarck E. Chronic Diarrhea in Dogs: What Do We Actually Know About It? Topics in Compan An Med. 2016;31:78-84.
Wheeler C., Vugia D.J., Thomas G., Beach M.J., Carnes S., Maier T., Gorman J., Xiao L., Arrowood M.J., Gilliss D., Werner S.B. Outbreak of cryptosporidiosis at a California waterpark: employee and patron roles and the long road towards prevention. Epidemiol Infect. 2007;135:302-10.
White K.E., Hedberg C.W., Edmonson L.M., Jones D.B., Osterholm M.T., MacDonald K.L. An outbreak of giardiasis in a nursing home with evidence for multiple modes of transmission. J Infect Dis. 1989;160:298-304.
WHO 2004. Global Burden of Disease. http://www.who.int/ healthinfo/ global_burden_disease/ GPD_report_2004 update_part2.pdf.
Widmer G., Lee Y. Comparison of single- and multilocus genetic diversity in the protozoan parasites Cryptosporidium parvum and C. hominis. Appl Environ Microbiol. 2010;76(19):6639-44.
Winiecka-Krusnell J., Linder E. Cysticidal effect of chlorine dioxide on Giardia intestinalis cysts. Acta Trop. 1998;70(3):369-72.
64
Xiao L., Herd R.P. Epidemiology of equine Cryptosporidium and Giardia infections. Equine Vet J. 1994;26:14-7.
Xiao L., Saeed K., Herd R.P. Efficacy of albendazole and fenbendazole against Giardia infection in cattle. Vet Parasitol. 1996;61:165-170.
Xiao L., Limor J., Morgan U.M., Sulaiman I.M., Thompson R.C., Lal A.A. Sequence differences in the diagnostic target region of the oocyst wall protein gene of Cryptosporidium parasites. Appl Environ Microbiol. 2000;66:5499-502.
Xiao L. and Feng Y. Zoonotic cryptosporidiosis. FEMS Immunol Med Microbiol. 2008;52:309-23.
Xiao L. Molecular epidemiology of cryptosporidiosis: an update. Exp Parasitol. 2010;124:80-9.
Yanke S.J., Ceri H., Mc Allister T.A., Morck D.W., Olson M.E. Serum immune response to Giardia duodenalis in experimentally infected lambs. Vet Parasitol. 1998;75:9-19.
Yui T., Nakajima T., Yamamoto N., Kon M., Abe N., Matsubayashi M., Shibahara T. Age-related detection and molecular characterization of Cryptosporidium suis and Cryptosporidium scrofarum in pre- and post-weaned piglets and adult pigs in Japan. Parasitol Res. 2014;113(1):359-65.
Zahedi A., Paparini A., Jian F., Robertson I., Ryan U. Public health significance of zoonotic Cryptosporidium species in wildlife: Critical insights into better drinking water management. Int J Parasitol Parasites Wildl. 2016a;5:88-109.
Zahedi A., Monis P., Aucote S., King B., Paparini A., Jian F., Yang R., Oskam C., Ball A., Robertson I., Ryan U. Zoonotic Cryptosporidium species in animals inhabiting Sydney water catchments. PLos One. 2016b;11(12):e0168169.
Zajac A.M., La Branche T.P., Donoghue A.R., Chu T.C. Efficacy of fenbendazole in the treatment of experimental Giardia infection in dogs. Am J Vet Res. 1998;59, 61–63.
Zanzani S.A., Gazzonis A.L., Scarpa P., Berrilli F., Manfredi M.T. Intestinal parasites of owned dogs and cats from metropolitan and micropolitan areas: prevalence, zoonotic risks, and pet owner awareness in nothern Italy. BioMed Res Int. 2014;2014:696508
Objectives
66
Both Giardia and Cryptosporidium are important parasites in human and veterinary medicine,
causing diarrhoea in humans and in different animal species. Although outbreaks have been
reported (Painter et al., 2016; Ryan et al., 2016; Utsi et al., 2016; Efstratiou et al., 2017; McClung
et al., 2017), only limited information is available on the prevalence of Giardia and
Cryptosporidium in humans and animals in Greece, about risk factors associated with infection
and about their clinical importance.
Based on the official records, as presented by the Hellenic Centre for Disease Control and
Prevention, there are limited reports of human parasitic diseases in Greece even when, in case
of zoonoses, there are well documented data for the infections in animals. This for example is
the case of cystic echinococcosis, for which Greece is considered highly endemic. However,
although infection rates in livestock reach up to 39.3% for sheep and 14.7% for goats (Sotiraki
and Chaligiannis, 2010), there are no official data about the disease prevalence in humans since
2009. This can be attributed either to underreporting (possibly due to misdiagnosed cases) or to
the actual fact that indeed the number of infections is low because of proper control measures.
Underreporting is unfortunately a fact in Greece as confirmed by Gibbons et al., 2014, providing
salmonellosis and campylobacteriosis as an example. According to that study, Greece appears to
be a country with high extent of underestimated (underreported and under-ascertained)
infections, more than several other European countries. If this is the case when it comes to
diseases like salmonellosis and campylobacteriosis with acute and severe clinical signs which
force infected individuals to urgently seek for medical help, we can imagine the high rates of
underestimation in case of giardiosis and cryptosporidiosis where clinical signs are often mild
and self-limiting.
With animal infections being very common, Cryptosporidium and Giardia are considered to be
zoonotic parasites, but both human-to-human and animal-to-human transmission cycles exist.
However, and especially concerning Giardia, the importance of zoonotic transmission has been
widely debated (Ryan and Caccio, 2013), mainly due to recent advances in genotyping.
Therefore, identifying and understanding transmission cycles of those parasites between
different host species is highly important to minimize disease burden and suggest appropriate
preventive measures.
Crete island in Greece, has been selected for this study because it offers an interesting case to
study transmission of Cryptosporidium and Giardia: Crete is a geographically restricted area,
67
densely populated (623,000 residents recorded in 2011), with a large tourist population, a high
number of farm and companion animals (Hellenic Ministry of Rural Development and Food:
http://minagric.gr), and proximity to both Europe and Africa. The presence of Cryptosporidium
and Giardia has been studied in small ruminant farming systems on the island (Tzanidakis et al.,
2014), prior to this thesis, using the same methodology. The results of that preliminary study,
showing high infection rates of Cryptosporidium and Giardia in small ruminants, were an extra
clue for us to expand these investigations to different hosts, as they confirmed the presence of
the two protozoa in the area.
Specifically, the objectives of this Ph.D. thesis were:
To estimate the occurrence of Giardia and Cryptosporidium in humans and different
animal species such as horses and dogs and cats. Especially in the case of dogs and cats,
we focused on household, shelter and shepherd (dogs) populations. In humans, we
targeted different groups i.e. people with and without gastrointestinal symptoms as well
as adults and children. Thus, we could evaluate and form a better view of which risk
factors favour or not the prevalence of Giardia and Cryptosporidium in humans and
companion animals.
To identify, through the performance of the molecular methods, the Giardia
assemblages and the Cryptosporidium species/genotypes/subtypes and therefore,
detect the transmission cycles of the parasites (human-to-human, animal-to-animal,
animal-to-human) to evaluate their zoonotic potential and investigate the sources of
infection.
68
References
Efstratiou A., Ongerth J.E., Karanis P. Waterborne transmission of protozoan parasites: Review of worldwide outbreaks – An update 2011-2016. Water Res. 2017;114;14-22.
Hellenic Ministry of Rural Development and Food: http://minagric.gr accessed 11 March 2018.
Gibbons C.L., Mangen M.J., Plass D., Havelaar A.H., Brooke R.J., Kramarz P., Peterson K.L., Stuurman A.L., Cassini A., Fèvre E.M., Kretzschmar M.E. Burden of Communicable diseases in Europe (BCoDE) consortium. Measuring underreporting and under-ascertainment in infectious disease datasets: a comparison of methods. BMC Public Health. 2014;14:147.
McClung R.P., Roth D.M., Vigar M., Roberts V.A., Kahler A.M., Cooley L.A., Hilborn E.D., Wade T.J., Fullerton K.E., Yoder J.S., Hill V.R. Waterborne Disease Outbreaks Associated With Environmental and Undetermined Exposures to Water - United States, 2013-2014. MMWR Morb Mortal Wkly Rep. 2017;66(44):1222-1225.
Painter J.E., Gargano J.W., Yoder J.S., Collier S.A., Hlavsa M.C. Evolving epidemiology of reported cryptosporidiosis cases in the United States, 1995-2012. Epidemiol Infect. 2016;144:1792-802.
Ryan U., Cacciò S.M. Zoonotic potential of Giardia. Int J Parasitol. 2013;43(12-13):943-56.
Ryan U., Zahedi A., Paparini A. Cryptosporidium in humans and animals-a one health approach to prophylaxis. Parasite Immunol. 2016;38:535-47.
Sotiraki S., Chaligiannis I. Cystic echinococcosis in Greece. Past and present. Parasite. 2010;17(3):205-10.
Tzanidakis N., Sotiraki S., Claerebout E., Ehsan A., Voutzourakis N., Kostopoulou D., Stijn C., Vercruysse J., Geurden T. Occurrence and molecular characterization of Giardia duodenalis and Cryptosporidium spp. in sheep and goats reared under dairy husbandry systems in Greece. Parasite. 2014;21:45.
Utsi L., Smith S.J., Chalmers R.M., Padfield S. Cryptosporidiosis outbreak in visitors of a UK industry-compliant petting farm caused by a rare Cryptosporidium parvum subtype: a case-control study. Epidemiol Infect. 2016;144:1000-9.
Chapter II
Based on:
The occurrence and genetic characterization of Cryptosporidium and
Giardia species in foals in Belgium, The Netherlands, Germany and
Greece
D. Kostopoulou, S. Casaert, N. Tzanidakis, D. van Doorn, J. Demeler, G. von Samson-Himmelstjerna, A.
Saratsis, N. Voutzourakis, A. Ehsan, T. Doornaert, M. Looijen, N. De Wilde, S. Sotiraki, E. Claerebout, T.
Geurden
In: Veterinary Parasitology. 2015;211:170-174

70
Introduction
Cryptosporidium spp and Giardia spp are protozoan parasites that have been reported worldwide in a
wide range of hosts, including horses.
In horses, excretion of Cryptosporidium oocysts has been reported in different geographical areas, with
infection rates ranging between 0.75% (De Souza et al., 2009) and 25.0% (Smith et al., 2010). In some
studies, the prevalence was higher in foals (Veronesi et al., 2010), while in other studies, the peak
prevalence was observed in adult animals (Majewska et al., 1999, 2004). Part of this variation may be
due to differences in study design, the limited number of animals and/or farms in the study, and the
diagnostic technique that was used. Although an impact of Cryptosporidium infection on horse health
has been reported (Netherwood et al., 1996; Majewska et al., 2004; Grinberg et al., 2008; Frederick et
al., 2009), it seems to be less important compared to ruminants and especially intensively reared calves,
in which infection with Cryptosporidium parvum is an important cause of neonatal diarrhoea (de Graaf
et al., 1999).
Similarly, the prevalence of Giardia duodenalis has been reported in horses from various locations with
considerable variation (0.5–35.0%) (Pavlásek et al., 1995; Olson et al., 1997; Atwill et al., 2000; De Souza
et al., 2009; Veronesi et al., 2010; Traversa et al., 2012; Santin et al., 2013), but the number of studies on
the prevalence of G. duodenalis in foals is more limited compared to studies on Cryptosporidium.
Moreover, the impact of Giardia infection on equine health remains undefined, in contrast to calves and
lambs, where Giardia infections have been associated with a decreased growth and diarrhoea (Olson et
al., 1995; Geurden et al., 2010).
The relevance of animal infections is not only limited to the impact on animal health or production, but
should also be considered from a public health point of view as they may also be a source of infection,
either by infecting people by direct contact or by contaminating water supplies, since many outbreaks of
infections by both parasites are waterborne (Baldursson and Karanis, 2011). An increasing number of
studies seems to indicate a public health relevance of equine Cryptosporidium infections. Horses were
frequently infected with the zoonotic C. parvum (Ryan et al., 2003; Grinberg et al., 2008; Imhasly et al.,
2009; Smith et al., 2010; Laatamna et al., 2015) and occasionally the human species Cryptosporidium
hominis was detected in horses (Laatamna et al., 2015). Similarly for G. duodenalis, the assemblages A
71
and B have been identified, although the zoonotic potential of G. duodenalis in horses remains largely
unexplored (Traub et al., 2005; Traversa et al., 2012; Santin et al., 2013).
In Europe, with the exception of Italy – where extensive studies have been performed (Veronesi et al.,
2010; Traversa et al., 2012; Caffara et al., 2013) – there are only limited data on the prevalence of both
protozoal infections in horses as well as their zoonotic importance. The objective of the present study
was to acquire additional data on the occurrence and genotypes of Cryptosporidium and Giardia in foals
in regions of Europe where no records were available.
Materials and methods
Sampling
Convenience samples were collected from animals that belonged either to individual owners or to larger
farms/properties in four different countries, 3 countries situated in Western Europe (i.e. Belgium, The
Netherlands and Germany) and one Mediterranean country, i.e. Greece. The samples were collected
from 51 sites in Belgium, 30 in The Netherlands, 2 sites in Germany and 82 different sites from all over
Greece. Sampling was performed in spring and summer, i.e. shortly after the foaling season. Individual
faecal samples were collected from foals between 1 week and 6 months of age. The faecal samples were
collected directly from the rectum and immediately transported to the participating lab in each country
where they were stored at 4°C and examined within 4 days of sampling. When a sample was found to be
positive by coproscopic analysis for one of the two parasites, the sample was withheld for DNA
extraction and molecular genotyping.
For every horse/sample, a data form was completed by interviewing the owner, providing information
on age, breed, sex and presence or absence of diarrhoea (up to a maximum of 15 days before sampling).
Detection of Cryptosporidium and Giardia
A quantitative direct immunofluorescence assay (IFA) based on the commercial MERIFLUOR
Cryptosporidium/Giardia kit (Meridian Diagnostics Inc., Cincinnati, Ohio) was performed. Briefly, one
gram of the faecal material was suspended in 100 ml of distilled water and strained through a layer of
surgical gauze. After sedimentation for 1 h and centrifugation at 3000 × g for 5 min, the sediment was
resuspended in distilled water up to a volume of 1 ml. After thorough vortexing, an aliquot of 20 μl was
pippeted onto a treated IFA-slide. After staining of the slide, as instructed by the manufacturer, the

72
entire smear was examined at a 400× magnification under a fluorescence microscope. The number of
Cryptosporidium oocysts per gram of faeces (OPG) and Giardia cysts per gram of faeces (CPG) was
obtained by multiplying the total number of cysts on the smear by 50.
Molecular identification
DNA was extracted from the 1 ml faecal sample using the QIAamp® Stool Mini Kit (Qiagen) according to
the manufacturer’s instructions, incorporating an initial step of 3 freeze-thaw cycles (freezing in liquid
nitrogen for 5 min and heating at 95°C for 5 min) in the protocol to maximise disruption of (oo) cysts.
For the amplification of the Cryptosporidium 18S ribosomal DNA gene (18S rDNA) and HSP70 gene,
previously described PCR protocols were used (Morgan et al., 2001; Xiao et al., 2001). For the
identification of Giardia DNA, the β-giardin gene (Lalle et al., 2005) and the triose phosphate isomerase
(TPI) gene (Geurden et al., 2008) were used. In all above-mentioned PCR reactions, bovine serum
albumin (BSA) was added to a final concentration of 0.1 μg BSA/μl reaction mixture. Amplification
products were visualised on 1.5% agarose gels with ethidium bromide. A positive (genomic DNA from a
positive faecal sample) and negative (PCR water) control sample were included in each PCR reaction.
PCR products were purified using the Qiaquick PCR purification kit (Qiagen) and fully sequenced using
the Big Dye Terminator v.3.1 Cycle sequencing Kit (Applied Biosystems). Sequencing reactions were
analysed on a 3100 Genetic Analyzer (Applied Biosystems) and assembled with the program Seqman II
(DNASTAR, Madison WI, USA). To determine the genotypes and subgenotypes, the fragments were
aligned with the homologous sequences available in the GenBank database, using MegAlign (DNASTAR,
Madison WI, USA). The β-giardin, TPI, 18S rDNA and HSP70 nucleotide sequences obtained in this study
were deposited in GenBank under accession numbers KM926502–KM926526, KM926527–KM926548,
KM926549 and KM926550–KM926551, respectively.
Statistical analysis
Univariate analysis was carried out by descriptive statistics and results were expressed as mean (M),
standard deviation (SD), median (Mdn) and minimum (min) and maximum (max) values. Within the
Giardia infected animals, the association between age and CPG values was analysed by the non-
parametric Spearman’s rho correlation coefficient. In addition, the non-parametric Mann–Whitney test
was utilised to compare the age of foals with and without diarrhoea. Finally, a multivariable logistic
regression model was constructed to assess the main effects of age and CPG values and their interaction
73
on the status (presence/absence of diarrhoea) of foals. Data were analysed using the SPSS statistics
software (version 19.0).
Results
Occurrence of Cryptosporidium and Giardia
In total, 398 foals from 4 different countries were examined in the present study, i.e. 134 in Belgium, 44
in The Netherlands, 30 in Germany and 190 in Greece. The mean age was 64 days (SD ± 56.24), the
median age was 31 days with a range of 5–180 days. Of the foals, 163 were male and 191 were female.
For 44 foals, gender was not recorded (Table 1).
Eight foals were found positive for Cryptosporidium (2.0%) and the oocyst excretion ranged from 50 to
2450 OPG with a median excretion of 750 OPG. For Giardia, 49 foals (12.3%) were found to excrete
cysts, with a range of 50–4,000,000 CPG, and a median excretion of 450 CPG. Four of these foals were
co-infected with Giardia and Cryptosporidium, all less than 1 month of age.
The age distribution of Giardia infected animals was: 55.6% (25/45) for animals aged 1–30 days, 15.6%
(7/45) for animals aged 31–60 days, 13.3% (6/45) for animals aged 61–90 days, 6.7% (3/45) for animals
aged 91–120 days and 8.9% (4/45) for animals aged 121–180 days. The Spearman’s correlation
coefficient revealed a statistically significant negative association between “the age of the foal” (in days)
and CPG values (r(42)=−0.306, p=0.049). The parasitic burden (expressed as median value of CPG per
age group) was also higher in younger animals, i.e. 1700 CPG for foals aged up to 60 days, 550 CPG for
foals between 61 and 120 days old and 150 CPG for 121–180 days old foals.
Eleven out of 88 foals (12.5%) that showed diarrhoea at or shortly before sampling were positive for
Giardia and only 1 (1.1%) was positive for Cryptosporidium. However, no significant correlation was
found between “history of diarrhoea” and infection intensity (expressed as CPG or OPG values). Similar
results were obtained when intensity of infection was collated to “the age of the foals”. In the above
mentioned correlation, the samples from Germany were not included because the factor “history of
diarrhoea” was not recorded. Within the Giardia infected animal population, the 42 animals/cases were
split, 31 without “history of diarrhoea” and 11 with “history of diarrhoea”. There was a statistically
significant difference in the distributions of “age of the foal” between subjects “without history of
diarrhoea” (Mdn=60; range 7–180) and subjects “with history of diarrhoea” (Mdn=21; range 10–30)
(Z=−3.116, p=0.002). Finally, in the multivariable binary logistic regression model, there was no
statistically significant main effect of age (in days) (χ2=2.582, p=0.108 with df=1) and CPG values

74
(χ2=1.007, p=0.316 with df=1) on the outcome of the dependent variable “history of diarrhoea”. In
addition, there was no statistically significant interaction effect of age and CPG values on the outcome of
the dependent variable (χ2=1.132, p=0.287 with df=1).
Genotyping
Six out of the 8 Cryptosporidium, positive samples did not amplify or yielded poor sequences. The
remaining 2 samples belonged to Cryptosporidium horse genotype (Table 1). Most Giardia positive
samples were identified as assemblage AI (n=9) or BIV (-like) (n=12). Additional genotypes were
assemblage A (n=1), AII (n=4), B (n=2) and E (n=3). Mixed infections of assemblages A and B were also
detected in 8 samples (2 from Belgium and 6 from Greece).
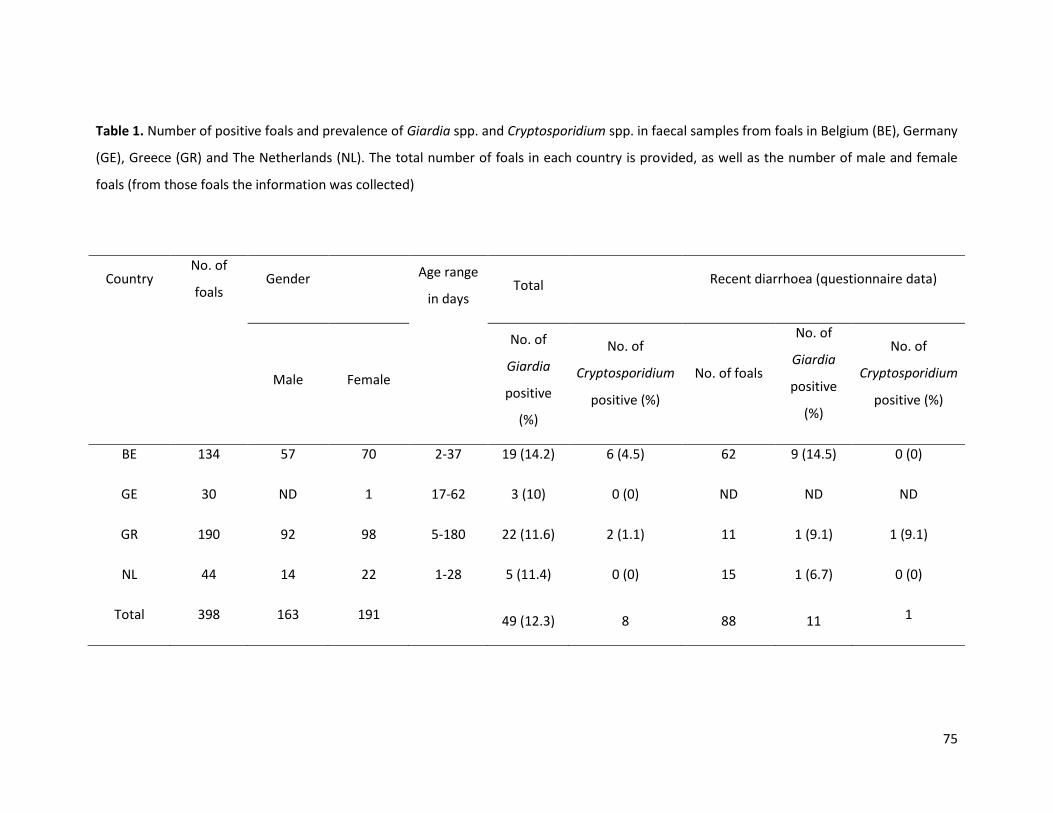
75
Table 1. Number of positive foals and prevalence of Giardia spp. and Cryptosporidium spp. in faecal samples from foals in Belgium (BE), Germany
(GE), Greece (GR) and The Netherlands (NL). The total number of foals in each country is provided, as well as the number of male and female
foals (from those foals the information was collected)
Country No. of
foals Gender
Age range
in days Total Recent diarrhoea (questionnaire data)
Male Female
No. of
Giardia
positive
(%)
No. of
Cryptosporidium
positive (%)
No. of foals
No. of
Giardia
positive
(%)
No. of
Cryptosporidium
positive (%)
BE 134 57 70 2-37 19 (14.2) 6 (4.5) 62 9 (14.5) 0 (0)
GE 30 ND 1 17-62 3 (10) 0 (0) ND ND ND
GR 190 92 98 5-180 22 (11.6) 2 (1.1) 11 1 (9.1) 1 (9.1)
NL 44 14 22 1-28 5 (11.4) 0 (0) 15 1 (6.7) 0 (0)
Total 398 163 191 49 (12.3) 8 88 11 1
76
Discussion
Infections with Giardia spp and Cryptosporidium spp were identified in foals aged up to 6 months, from
Belgium, Germany, Greece and The Netherlands.
The overall detection rate of Cryptosporidium spp was 2.0%. The infection rates for Cryptosporidium spp
were low in Belgium (4.5%) and Greece (1.1%), whereas no positive samples were found in Germany and
The Netherlands. The latter, taking also into account the lower number of foals sampled in these
countries, may suggest an overall low prevalence in those countries. Excretion of Cryptosporidium
oocysts was previously reported to range between 0.75% (De Souza et al., 2009) and 25.0% (Smith et al.,
2010). The low occurrence and level of oocyst excretion may be indicative for a low infection pressure at
the different sites participating in this study, as horses usually are not as intensively kept as livestock.
Similarly, Cryptosporidium was also reported to occur less frequently in calves kept under extensive
farming conditions compared to intensive farming (Geurden et al., 2006). In ruminants, the prevalence
of Cryptosporidium most often peaks within the first few weeks after birth (Geurden et al., 2008). Similar
to what has been found in ruminants, in the present study, all Cryptosporidium positive foals were aged
less than 37 days. This is in agreement with a higher prevalence in foals as observed by Veronesi et al.
2010, while in other studies, the prevalence peaked in adult horses (Majewska et al., 1999, 2004).
The public health and the veterinary importance of equine Cryptosporidium infections have been
discussed in previous studies (Grinberg et al., 2008, 2009; Robinson et al., 2008; Imhasly et al., 2009;
Xiao et al., 2009; Smith et al., 2010; Perrucci et al., 2011; Santin et al., 2013), however, morphological
and biological data are not yet sufficient available for horse genotypes (Ryan et al., 2014). In the present
study, the zoonotic potential of Cryptosporidium infections (e.g. through contamination of surface
water) could not be evaluated, due to the limited number of isolates and the poor amplification and
sequencing results, presumably as a consequence of the low oocyst excretion found in the samples
examined.
G. duodenalis infection rates were comparable in all countries (Table 1). The overall infection rate of G.
duodenalis found in the present study (12.3%) is in line with previous reports (0.50–35.0%) in horses
(Pavláseket al., 1995; Olson et al., 1997; Atwill et al., 2000; De Souza et al., 2009; Veronesi et al., 2010;
Santin et al., 2013). Despite the extensive rearing described above, high cyst excretion was sometimes
observed, especially in younger animals. Co-infections with Giardia and Cryptosporidium were detected
only in foals aged less than 30 days, since Cryptosporidium infection was only recorded in animals of that
age. No association was found between G. duodenalis cyst counts and diarrhoea. This agrees with
77
previous findings where Giardia infection was not correlated with the presence of diarrhoea in horses
(Xiao and Herd, 1994; Veronesi et al., 2010; Santin et al., 2013). The finding of the apparent lack of any
correlation between Giardia and diarrhoea could also be due to the experimental design, since the
animals were only sampled once, and Giardia cyst shedding can be intermittent (Patton, 2013). Within
the Giardia infected animals, the presence of diarrhoea was significantly correlated with the age of the
foal, as diarrhoea was present only in animals less than one month old.
Genetic characterization of the Giardia isolates found in this study indicated that G. duodenalis A and B
assemblages were the predominant genotypes. These assemblages with zoonotic potential are common
in humans in Europe (e.g. Geurden et al., 2009; Lebbad et al., 2011; Alexander et al., 2014; Mateo et al.,
2014) and have been identified in foals in Italy, The United States and Australia (Ey et al., 1997; Traub et
al., 2005; Traversa et al., 2012; Santin et al., 2013).
Assemblage B was found to be the most prevalent genotype. Genotyping revealed high sequence
heterogeneity in assemblage B, with many samples identified as (or closely related to) BIV or BIV-like
sub-assemblages. Genetic heterogeneity within assemblage B is a well documented phenomenon but it
is still not known if this genetic heterogeneity is due to high allelic sequence heterozygosity in such
parasites and/or due to common mixed infections with different sub-groups of isolates (Ankarklev et al.,
2012). Accordingly, it remains difficult to assign specific assemblage B isolates to different sub-
genotypes and no clear distinction between zoonotic and host-adapted genotypes can be made for
assemblage B (Sprong et al., 2009). Within assemblage A, sub-assemblages AI and AII were identified.
Although both of them have been found in humans and animals, sub-assemblage AI is mainly seen in
livestock and pets, whereas sub-assemblage AII is predominantly seen in humans. According to Sprong
et al. 2009, isolates found in both humans and animals are not always epidemiologically linked, and
finding similar sub-assemblages simply highlights the global distribution of those genotypes, providing
little evidence for zoonotic transmission. Assemblage E was also found in two samples from Greece.
Assemblage E is a non-zoonotic genotype and is usually detected in hoofed livestock (Thompson, 2004;
Geurden et al., 2008; Tzanidakis et al., 2014). Assemblage E has been reported in horses in previous
studies in Italy (Veronesi et al., 2010; Traversa et al., 2012).
To conclude, in the present study, a low Cryptosporidium and a moderate occurrence of G. duodenalis in
foals in all 4 countries involved were detected. This to an extent correlates to the detection method; i.e.
prevalence of both parasites could have been higher if real-time PCR was used for the initial detection
(Boadi et al., 2014; Operario et al., 2015). The low infection rates of these two protozoa could be due to
the living and management conditions of the horses which are in general less intensive than in farm
78
animals. Most of the G. duodenalis isolates were assemblage AI and BIV (like), which are found
predominantly in animals, or the hoofed livestock-specific assemblage E. This, combined with the
presence of Cryptosporidium horse genotype, suggests a low risk for zoonotic transmission concerning
both parasites in the context of horses. At the same time, it illustrates the difficulty of evaluating a
potential public health threat based solely on genetic data without considering the epidemiological
background of human clinical infections.
Acknowledgements
The authors would like to thank the Hellenic Scholarship Foundation for supporting Mrs.
Kostopoulou’s PhD thesis. Moreover, we are grateful to all the vets that helped during sampling and
especially Dr. A. Stefanakis, Dr. E. Fragkiadaki, Mrs. A. Mitsoura and Mr. A. Malamas.
Appendix A. Supplementary data
Additional file 1. Table S1. Number of Giardia cysts and Cryptosporidium oocysts detected by IFA and
Giardia duodenalis assemblages identified by sequence analysis frompositive foals examined in
Belgium (BE), Germany (GE), Greece (GR) and the Netherlands (NL). (TPI: Triosephosphate isomerase
gene; ND: no data).
79
References
Alexander C., Jones B., Inverarity D., Pollock K.G. Genotyping of Giardia isolates in Scotland: a descriptive epidemiological study. Epidemiol Infect. 2014;142, 1636-1639.
Ankarklev J., Svärd S.G., Lebbad M. Allelic sequence heterozygosity in single Giardia parasites. BMC Microbiol. 2012;12:65.
Atwill E.R., McDougald N.K., Perea L. Cross-sectional study of faecal shedding of Giardia duodenalis and Cryptosporidium parvum among packstock in the Sierra Nevada Range. Equine Vet. J. 2000;32:247-52.
Baldursson S., Karanis P. Waterborne transmission of protozoan parasites: Review of worldwide outbreaks – An update 2004-2010. W Res. 2011;45:6603-6614.
Boadi S., Polley S.D. Kilburn S., Mills G.A., Chiodini P.L. A critical assessment of two real-time PCR assays targeting the (SSU) rRNA and gdh genes for the molecular identification of Giardia intestinalis in a clinical laboratory. J Clin Pathol. 2014;67, 811-816.
Caffara M., Piva S., Pallaver F., Iacono E., Galuppi R. Molecular characterization of Cryptosporidium spp. from foals in Italy. Vet. J. 2013;198:531-533.
de Graaf D.C., Vanopdenbosch E., Ortega-Mora L.M., Abbassi H., Peeters J.E. A review of the importance of cryptosporidiosis in farm animals. Int J Parasitol. 1999;29:1269-1287.
De Souza P.N., Bomfim T.C., Huber F., Abboud L.C., Gomes R.S. Natural infection by Cryptosporidium sp., Giardia sp. and Eimeria leuckarti in three groups of equines with different handlings in Rio de Janeiro, Brazil. Vet Parasitol. 2009;160:327-333.
Ey P., Mansouri M., Kulda J., Nohynkova E., Monis P.T., Andrews R.H., Mayrhofer G. Genetic analysis of Giardia from hoofed farm animals reveals artiodactyls specific and potentially zoonotic genotypes. J Eukaryot Microbiol. 1997;44:626-635.
Frederick J., Giquere S., Sanchez L.C. Infectious agents detected in the feces of diarrheic foals: a retrospective study of 233 cases (2003-2008). J Vet Intern Med. 2009;23:1254-1260.
Geurden T., Goma F.Y., Siwila J., Phiri I.G., Mwanza A.M., Gabriel S., Claerebout E., Vercruysse J. Prevalence and genotyping of Cryptosporidium in three cattle husbandry systems in Zambia. Vet Parasitol. 2006;138:217-222.
Geurden T., Geldhof P., Levecke B., Martens C., Berkvens D., Casaert S., Vercruysse J., Claerebout E. Mixed Giardia duodenalis assemblage A and E infections in calves. Int J Parasitol. 2008;38: 259-264.
Geurden T., Levecke B., Cacció S., Visser A., De Groote G., Casaert S., Vercruysse J., Claerebout E. Multilocus genotyping of Cryptosporidium and Giardia in non outbreak related cases of diarrhea in human patients in Belgium. Parasitol. 2009;136:1161-1168.
Geurden T., Vandenhoute E., Pohle H., Casaert S., De Wilde N., Vercruysse J., Claerebout E. The effect of a fenbendazole treatment on cyst excretion and weight gain in calves experimentally infected with Giardia duodenalis. Vet Parasitol. 2010;169:18-23.
Grinberg A., Learmonth J., Kwan E., Pomroy W., Lopez Villalobos N., Gibson I., Widmer G. Genetic diversity and zoonotic potential of Cryptosporidium parvum causing foal diarrhea. J Clin Microbiol. 2008;46:2396-2398.
Grinberg A., Pomroy W.E., Carslake H.B., Shi Y., Gibson I.R., Drayton B.M. A study of neonatal cryptosporidiosis of foals in New Zealand. N Z Vet J. 2009;57:284- 289.
Imhasly A., Frey C.F., Mathis A., Straub R., Gerber V. Cryptosporidiose (C. parvum) in a foal with diarrhea. Schweiz. Arch. Tierheilkd. 2009;151:21-26.
Laatamna A.E. ,Wagnerova P., Sak B., Kvetonova D., Xiao L. , Rost M., Mc Evoy J., Saadi A.R., Aissi M., Kvac M. Microsporidia and Cryptosporidium in horses and donkeys in Algeria: detection of a novel Cryptosporidium hominis subtype family (ik) in a horse. Vet Parasitol. 2015;208:135-42.
80
Lalle M., Pozio E., Capelli G., Bruschi F., Crotti D., Caccio S.M. Genetic heterogeneity at the beta-giardin locus among human and animal isolates of Giardia duodenalis and identification of potentially zoonotic subgenotypes. Int J Parasitol. 2005;35:207-213.
Lebbad M., Petersson I., Karlsson L., Botero-Kleiven S., Andersson J.O., Svenungsson B., Svärd S.G. Multilocus genotyping of human Giardia isolates suggests limited zoonotic transmission and association between assemblage B and flatulence in children. PLoS Negl Trop Dis. 2011;5:1262.
Majewska A.C., Werner A., Sulima P., Luty T. Survey on equine cryptosporidiosis in Poland and the possibility of zoonotic transmission. Ann Agric Environ Med. 1999;6:161-165.
Majewska A.C., Solarczyk P., Tamang L., Graczyk T.K. Equine Cryptosporidium parvum infections in western Poland. Parasitol Res. 2004;93:274-278.
Mateo M., Mateo M., Montoya A., Bailo B., Saugar J.M., Aguilera M., Fuentes I., Carmena D. Detection and molecular characterization of Giardia duodenalis in children attending day care centers in Majadahonda, Madrid, Central Spain. Medicine (Baltimore). 2014;93(15):e75.
Morgan U.M., Monis P.T., Xiao L., Limor J., Sulaiman I., Raidal S., O’ Donoghue P., Gasser R., Murray A., Fayer R., Blagburn B.L., Lal A.A., Thomson R.C. Molecular and phylogenetic characterisation of Cryptosporidium from birds. Int J Parasitol. 2001;31:289-296.
Netherwood T., Wood J.L., Townsend H.G., Mumford J.A., Chanter N. Foal diarrhoea between 1991 and 1994 in the United Kingdom associated with Clostridium perfringens, rotavirus, Strongyloides westeri, and Cryptosporidium spp. Epidemiol Infect. 1996;117:375-383.
Olson M.E., McAllister T.A., Deselliers L., Morck D.W., Cheng K.J., Buret A.G., Ceri H. Effects of giardiasis on production in a domestic ruminant (lamb) model. Am J Vet Res. 1995;56:1470-1474.
Olson M.E., Thorlakson C.L., Deselliers L., Morck D.W., McAllister T.A. Giardia and Cryptosporidium in Canadian farm animals. Vet Parasitol. 1997;68:375-381.
Operario D.J., Bristol L.S., Liotta J., Nydam D.V., Houpt E.R. Correlation between diarrhea severity and oocyst count via quantitative PCR or fluorescence microscopy in experimental cryptosporidiosis in calves. Am J Trop Med Hyg. 2015;92:45-49.
Patton P. Overview of Giardiasis. 2013. In Merck Veterinary Manual of diagnosis and therapy (19th ed.). Whitehouse Station, N.J.: Merck Research Laboratories.
Pavlásek I., Hess L., Stehlík I., Stika V. The first detection of Giardia spp. in horses in the Czech Republic. Vet Med. 1995;40:81-86.
Perrucci S., Buggiani C., Sgorbini M., Cerchiai I., Ontranto D., Traversa D. Cryptosporidium parvum infection in a mare and her foal with foal heat diarrhoea. Vet Parasitol. 2011;182:333-336.
Robinson G., Elwin K., Chalmers R.M., 2008. Unusual Cryptosporidium genotypes in human cases of diarrhea. Emerg Infect Dis. 2008;14: 1800-1802.
Ryan U., Xiao L., Read C., Zhou L., Lal A.A., Pavlasek I. Identification of novel Cryptosporidium genotypes from the Czech Republic. Appl Environ Microbiol. 2003;69:4302-4307.
Ryan U., Fayer R., Xiao L. 2014. Cryptosporidium species in humans and animals: current understanding and research needs. Parasitology. 2014;141:1667 – 1685.
Santin M., Cortes Vecino J.A., Fayer R. A large scale molecular study of Giardia duodenalis in horses from Colombia. Vet Parasitol. 2013;196:31-36.
Smith R.P., Chalmers R.M., Mueller-Doblies D., Clifton-Hadley F.A., Elwin K., Watkins J., Paiba G.A., Hadfield S.J., Giles M. Investigation of farms linked to human patients with cryptosporidiosis in England and Wales. Prev Vet Med. 2010;94:9- 17.
Sprong H., Caccio S.M., van der Giessen J.W.B. Identification of zoonotic genotypes of Giardia duodenalis. PLoS Negl Trop Dis. 2009;3:558.
Thompson R.C.A. The zoonotic significance and molecular epidemiology of Giardia and giardiasis. Vet Parasitol. 2004;126:15-35.
81
Traub R., Wade S., Read C., Thompson A., Mohammed H. Molecular characterization of potentially zoonotic isolates of Giardia duodenalis in horses. Vet Parasitol. 2005;130:317-321.
Traversa D., Otranto D., Milillo P., Latrofa M.S., Giangaspero A., Di Cesare A., Paoletti B. Giardia duodenalis sub-Assemblage of animal and human origin in horses. Infect Genet Evol. 2012;12, 1642–1646.
Tzanidakis N., Sotiraki S., Claerebout E., Ehsan A., Voutzourakis N., Kostopoulou D., Stijn C., Vercruysse J., Geurden T. Occurrence and molecular characterization of Giardia duodenalis and Cryptosporidium spp. in sheep and goats reared under dairy husbandry systems in Greece. Parasite. 2014;21:45.
Veronesi F., Passamonti F., Cacciò S., Diaferia M., PiergiliFioretti D. Epidemiological survey on equine Cryptosporidium and Giardia infections in Italy and molecular characterization of isolates. Zoonoses Public Health. 2010;57:510-517.
Xiao L., Herd R.P. Epidemiology of equine Cryptosporidium and Giardia infections. Equine Vet J. 1994;26:14-17.
Xiao L., Singh A., Limor J., Graczyk T.K., Gradus S., Lal A.A. Molecular characterization of Cryptosporidium oocysts in samples of raw surface water and wastewater. Appl Environ Microbiol. 2001;6:1097–1101.
Xiao L., Hlavsa M.C., Yoder J., Ewers C., Dearen T., Yang W., Nett R., Harris S., Brend S.M., Harris M., Onischuk L., Valderrama A.L., Cosgrove S., Xavier K., Hall N., Romero S., Young S., Johnston S.P., Arrowood M., Roy S., Beach M.J. Subtype analysis of Cryptosporidium specimens from sporadic cases in Colorado, Idaho, New Mexico, and Iowa in 2007: widespread occurrence of one Cryptosporidium hominis subtype and case history of an infection with the Cryptosporidium horse genotype. J Clin Microbiol. 2009;47: 3017-3020.
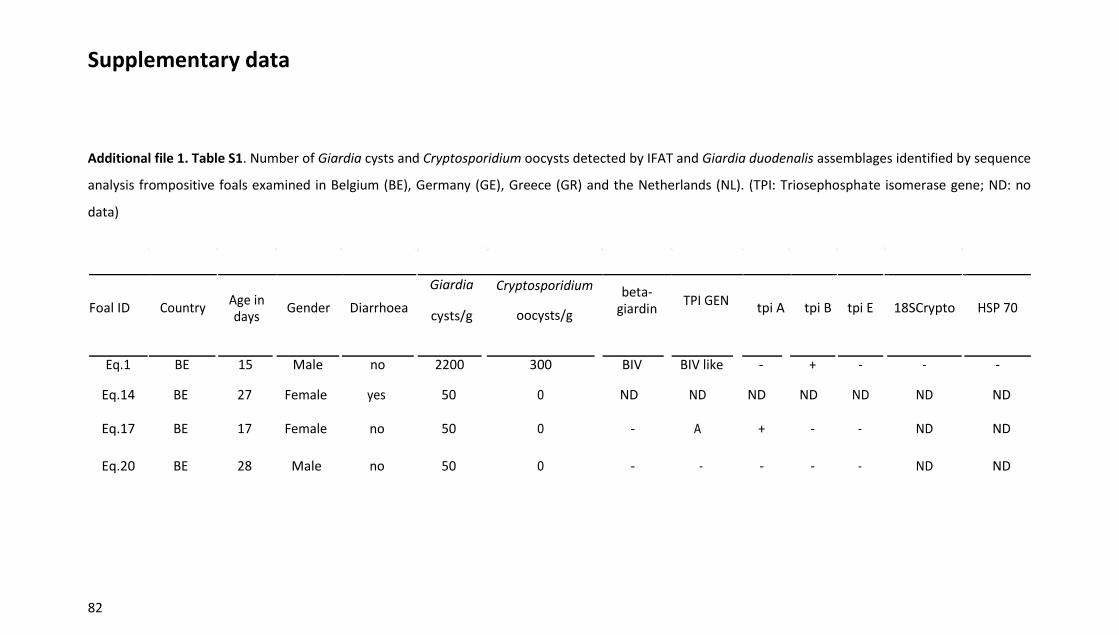
82
Supplementary data
Additional file 1. Table S1. Number of Giardia cysts and Cryptosporidium oocysts detected by IFAT and Giardia duodenalis assemblages identified by sequence
analysis frompositive foals examined in Belgium (BE), Germany (GE), Greece (GR) and the Netherlands (NL). (TPI: Triosephosphate isomerase gene; ND: no
data)
Foal ID Country Age in days
Gender Diarrhoea
Giardia
cysts/g
Cryptosporidium
oocysts/g
beta-giardin
TPI GEN tpi A tpi B tpi E 18SCrypto HSP 70
Eq.1
BE
15
Male
no
2200
300
BIV
BIV like
-
+
-
-
-
Eq.14 BE 27
Female yes 50
0
ND ND ND ND ND
ND
ND
Eq.17 BE 17
Female no 50
0
-
A +
-
-
ND
ND
Eq.20 BE 28
Male no 50
0
-
-
-
-
-
ND
ND
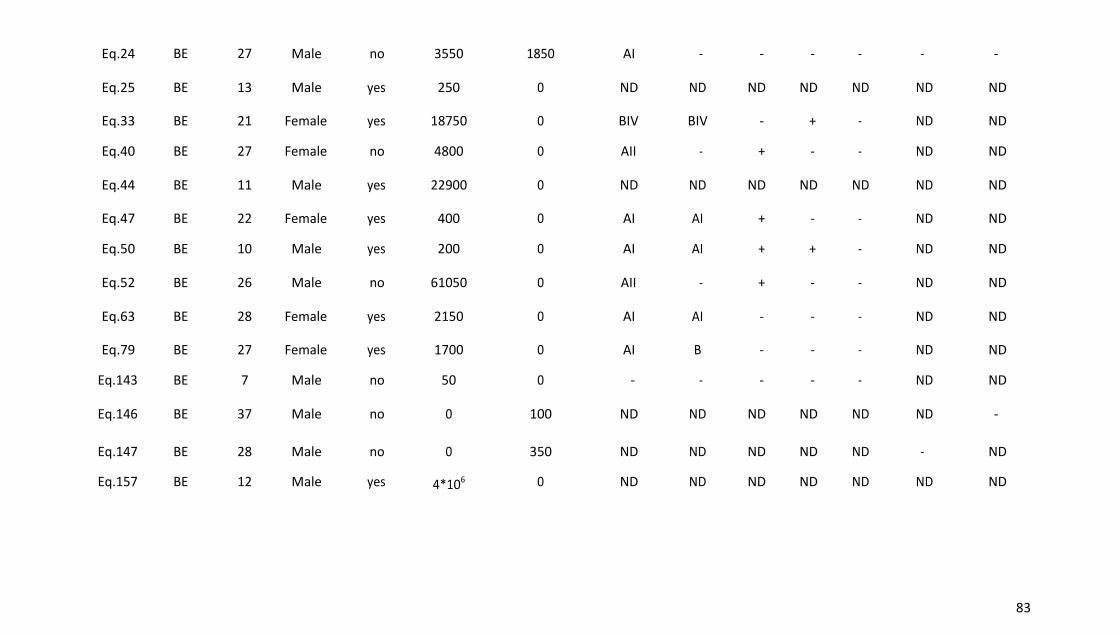
83
Eq.24 BE 27 Male no 3550 1850 AI - - - - - -
Eq.25 BE 13
Male yes 250
0
ND ND ND ND ND
ND
ND
Eq.33 BE 21
Female yes 18750
0
BIV BIV -
+
-
ND
ND
Eq.40 BE 27
Female no 4800
0
AII -
+
-
-
ND
ND
Eq.44 BE 11
Male yes 22900
0
ND ND ND ND ND
ND
ND
Eq.47 BE 22
Female yes 400
0
AI AI +
-
-
ND
ND
Eq.50 BE 10
Male yes 200
0
AI AI +
+
-
ND
ND
Eq.52 BE 26
Male no 61050
0
AII -
+
-
-
ND
ND
Eq.63 BE 28
Female yes 2150
0
AI AI -
-
-
ND
ND
Eq.79 BE 27
Female yes 1700
0
AI B -
-
-
ND
ND
Eq.143 BE 7
Male no 50
0
-
-
-
-
-
ND
ND
Eq.146 BE 37
Male no 0
100
ND ND ND ND ND
ND -
Eq.147 BE 28
Male no 0
350
ND ND ND ND ND -
ND
Eq.157 BE 12
Male yes 4*106
0
ND ND ND ND ND
ND
ND
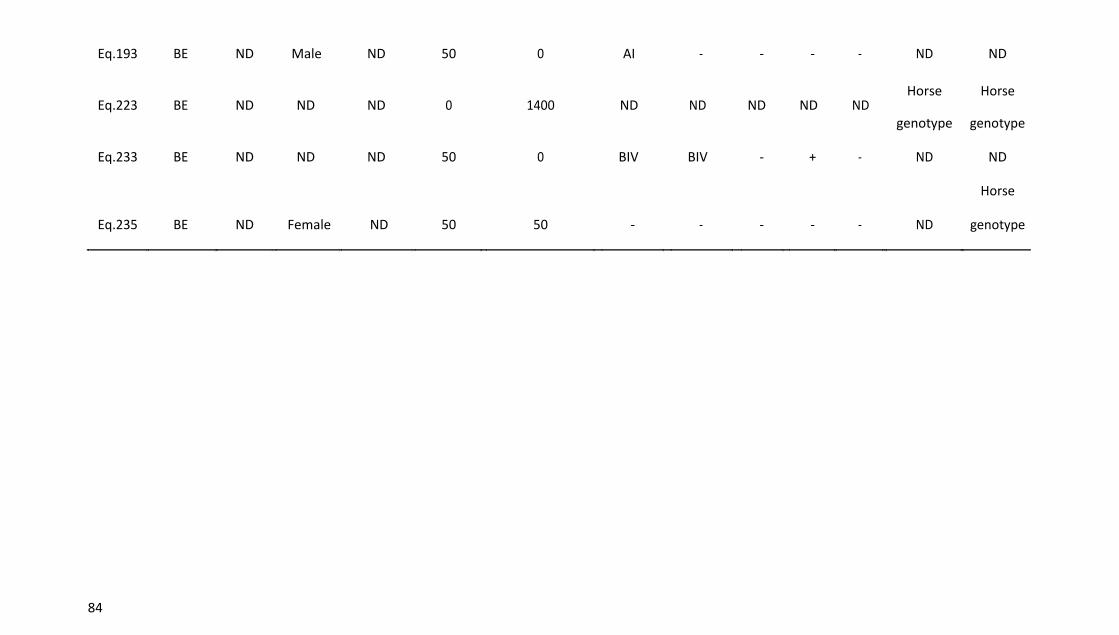
84
Eq.193 BE
ND Male ND 50
0
AI -
-
-
-
ND
ND
Eq.223 BE ND ND ND 0 1400 ND ND ND ND
ND Horse
Horse
genotype genotype
Eq.233 BE
ND ND ND 50
0
BIV BIV -
+
-
ND
ND
Eq.235 BE
ND Female ND 50
50
-
-
-
-
-
ND
Horse
genotype
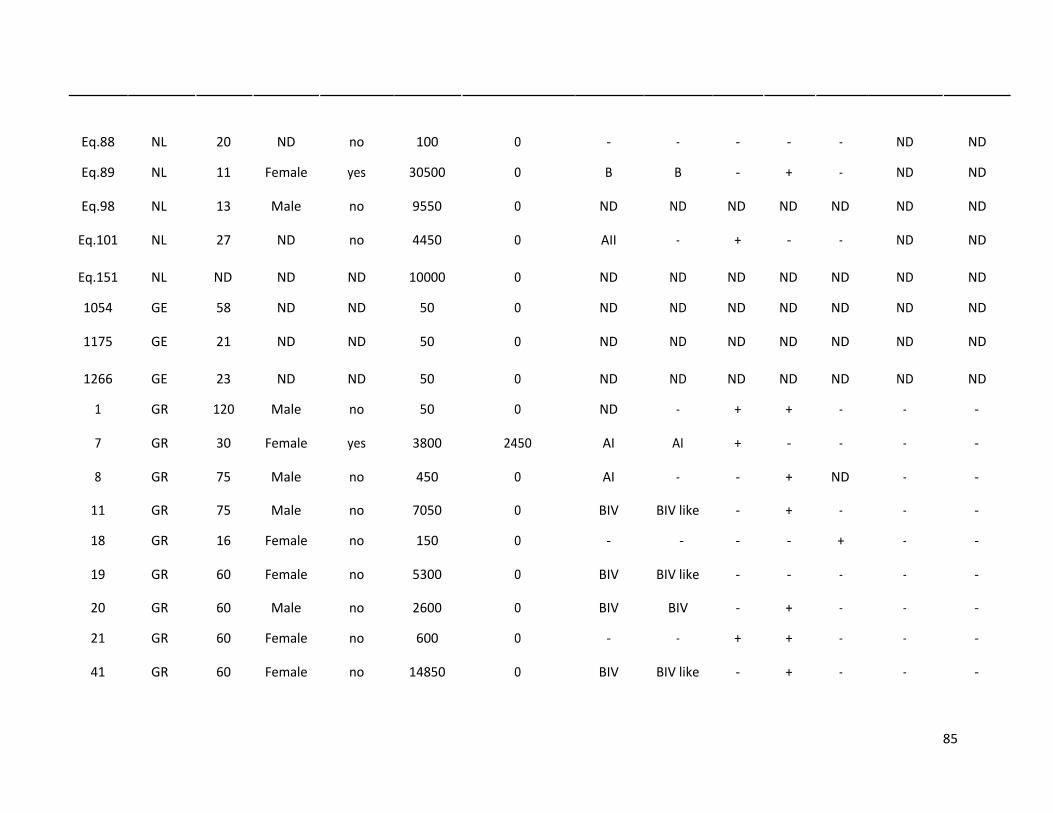
85
Eq.88 NL 20
ND
no 100 0 - - - - - ND
ND
Eq.89 NL 11
Female
yes 30500 0 B B - + - ND
ND
Eq.98 NL 13
Male
no 9550 0 ND ND ND ND ND ND
ND
Eq.101 NL 27
ND
no 4450 0 AII - + - - ND
ND
Eq.151 NL ND ND
ND 10000 0 ND ND ND ND ND ND
ND
1054 GE 58
ND
ND 50 0 ND ND ND ND ND ND
ND
1175 GE 21
ND
ND 50 0 ND ND ND ND ND ND
ND
1266 GE 23
ND
ND 50 0 ND ND ND ND ND ND
ND
1 GR 120
Male
no 50 0 ND - + + - - -
7 GR 30
Female
yes 3800 2450 AI AI + - - - -
8 GR 75
Male
no 450 0 AI - - +
ND - -
11 GR 75
Male
no 7050 0 BIV BIV like - + - - -
18 GR 16
Female
no 150 0 - - - - + - -
19 GR 60
Female
no 5300 0 BIV BIV like - - - - -
20 GR 60
Male
no 2600 0 BIV BIV - + - - -
21 GR 60
Female
no 600 0 - - + + - - -
41 GR 60
Female
no 14850 0 BIV BIV like - + - - -
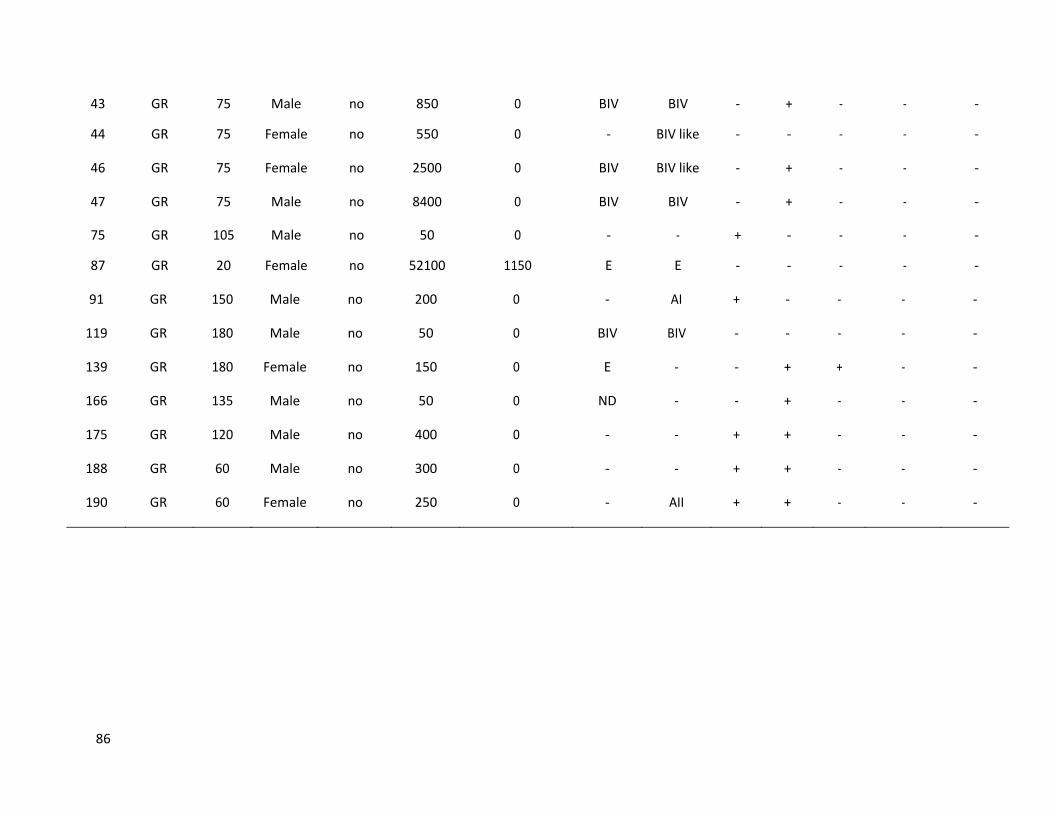
86
43 GR 75
Male
no 850 0 BIV BIV - + - - -
44 GR 75
Female
no 550 0 - BIV like - - - - -
46 GR 75
Female
no 2500 0 BIV BIV like - + - - -
47 GR 75
Male
no 8400 0 BIV BIV - + - - -
75 GR 105
Male
no 50 0 - - + - - - -
87 GR 20
Female
no 52100 1150 E E - - - - -
91 GR 150
Male
no 200 0 - AI + - - - -
119 GR 180
Male
no 50 0 BIV BIV - - - - -
139 GR 180
Female
no 150 0 E - - + + - -
166 GR 135
Male
no 50 0 ND - - + - - -
175 GR 120
Male
no 400 0 - - + + - - -
188 GR 60
Male
no 300 0 - - + + - - -
190 GR 60
Female
no 250 0 - AII + + - - -

Chapter III
Based on:
Abundance, zoonotic potential and risk factors of intestinal parasitism
amongst dog and cat populations: The scenario of Crete, Greece
D. Kostopoulou, E. Claerebout, D. Arvanitis, P. Ligda, N. Voutzourakis, S. Casaert, S. Sotiraki
In: Parasites & Vectors. 2017;10:43
88
Introduction
Intestinal parasite infections are still abundant in companion animals, despite all the highly efficient drug
formulations available and the control measures taken by owners and veterinarians (Capelli et al., 2003;
Palmer et al., 2008; Claerebout et al., 2009; Joffe et al., 2011; Ortuno and Castella, 2011; Riggio et al.,
2013; Itoh et al., 2015; Nijsse et al., 2016). Moreover, parasites are responsible for some of the most
important and well-recognized zoonoses transmitted from companion animals to man globally such as
Giardia spp, Cryptosporidium spp, Toxocara spp, hookworms and Echinococcus granulosus (Lee et al.,
2010; Deplazes et al., 2011; Chen et al., 2012; Mcpherson et al., 2013; Pereira et al., 2016).
Nowadays, changes due to climate alterations and social behaviour that affect humans’ lives and
consequently the lives of the animals which live close to them (Sutherst et al., 2004; Tabachnick, 2010),
alter the interactions between humans and pathogens leading to (re)emergence of several diseases,
including zoonotic ones (Jones et al., 2008; Otranto and Eberhard, 2011).
The distribution of zoonoses associated with companion animals is highly affected by animals’
movements (between regions, countries and continents) which in fact are the means to relocate
pathogens and vectors they harbour. The above is becoming more and more important since human
travel continues to increase in parallel with the population and financial status increase, and when
humans travel, they often take their companion animals, particularly dogs.
All the above is in fact unfolding the reasons why it is crucial to fill the gaps on the current distribution of
these diseases in a constantly changing environment and to describe the risks associated with pet
infection in order to assure their well-being and to prevent the free movement of zoonotic pathogens.
The aim of our study was to investigate the presence and infection intensity of intestinal parasites in
dogs and cats, the risk factors (such as lifestyle, veterinary care, etc.) that influence those infections and
their zoonotic potential. This was done by performing a cross-sectional epidemiological study within a
defined animal/human community, i.e. the island of Crete, as a case scenario.

89
Materials and methods
Populations studied
Faecal samples were collected from different dog populations (shelter, household and shepherd) as well
as shelter and household cats in Crete Island in Southern Greece (Figure 1), from October 2011 to
January 2015.
Crete is the largest and most densely populated island of Greece (623,000 residents recorded in 2011)
with a population well distributed in urban and rural areas. The island is also a highly popular tourist
destination (approximately 3.5 million international tourist passengers’ arrivals in 2013) (Region of
Crete: www.crete.gov.gr). Moreover in Crete, in addition to the high number of companion animals,
there is a significant livestock and wildlife population (Hellenic Ministry of Rural Development and Food:
http://minagric.gr).
Since data on the precise population of pets in the location were not available, the sample size was
determined estimating the dog and cat population size as “infinite”. The prevalence of intestinal
parasitism in different dog and cat studies in Europe varies enormously depending on the sampled
animal population and the diagnostic techniques that were used (Dubna et al., 2007; Martinez-Moreno
et al., 2007; Claerebout et al., 2009; Overgaauw et al., 2009; Riggio et al., 2013; Beugnet et al., 2014;
Ortuno et al., 2014; Zanzani et al., 2014; Simonato et al., 2015). In this study, in order to calculate the
sample size (with a precision of 5% and a 95% confidence interval) we selected to relate our “expected
prevalence” values to recent reports of Giardia prevalence in Europe. Therefore, the targeted sample
size was defined as follows: for household dogs up to 200 dogs (reported prevalence 10–20%); for
shelter dogs up to 400 dogs (reported prevalence 20–50%); for household cats 138 cats (reported
prevalence < 10%) and for shelter cats 385 cats (reported prevalence 10–50%) (Dubna et al., 2007;
Hamnes et al., 2007; Leonhard et al., 2007; Martinez-Moreno et al., 2007; Papazahariadou et al., 2007;
Claerebout et al., 2009; Barutzki et al., 2011; Ortuno and Castella, 2011). For shepherd dogs there is
little information available and given the difficulties in approaching and handling such dogs we aimed at
collecting the maximum feasible number of samples. In order to achieve the most accurate coverage of
the whole island, the animals enrolled in our study were allocated proportionally to the four different
counties of the island according to the inhabitant’s population density (Figure 1).
Individual rectal faecal samples were randomly collected from dogs and cats of all ages with or without
intestinal symptoms from 561 households, 11 shelters and 29 sheep and goat farms. After collection,

90
the samples were immediately transported under vacuum (Rinaldi et al., 2011) to the laboratory where
they were stored at 4 °C and examined within 2 days. When a sample was found to be positive by
coproscopic analysis for Giardia spp or Cryptosporidium spp, it was stored at -20°C until DNA extraction
was performed and molecular genotyping followed.
For every animal/sample, a data-form was completed by interviewing the owner or in case of shelters
the person who was responsible for the animals, providing information on age, sex, breed, living
conditions (indoors or outdoors), presence of other animals, the presence or absence of diarrhoea (up
to maximum 1 month before sampling), if the animal had travelled recently and the antiparasitic
treatment plan followed (including time of last treatment). Faecal consistency was recorded for all
faecal samples. The consistency of individual faecal samples was scored using the following scale: 1,
formed; 2, soft; 3, diarrhoea; 4, haemorrhagic diarrhoea.
Parasitological techniques
The presence of worm eggs and protozoan oocysts was determined by applying two different methods,
i.e. a sedimentation (acid/ether) and a sedimentation/flotation technique (using a saturated sugar salt
solution as a flotation fluid with 1.28 specific gravity) (MAFF, 1986). For the detection of Giardia spp and
Cryptosporidium spp (oo)cysts a quantitative direct immunofluorescence assay (IFA) based on the
commercial MERIFLUOR Cryptosporidium/Giardia kit (Meridian Diagnostics Inc., Cincinnati, Ohio) was
used (Geurden et al., 2008a; Kostopoulou et al., 2015).
Molecular analyses
DNA was extracted from the positive Giardia spp and Cryptosporidium spp faecal samples using the
QIAamp® Stool Mini Kit (Qiagen, Hilden, Germany) according to the manufacturer’s instructions. For the
amplification of the Cryptosporidium 18S ribosomal RNA gene (rDNA18S) and HSP70 gene, previously
described PCR protocols were used (Morgan et al., 2001; Xiao et al., 2001). For the identification of
Giardia DNA, the Giardia rRNA 18S gene (rDNA 18S) (Hopkins et al., 1997), the β-giardin gene (Lalle et
al., 2005), the triose phosphate isomerase (TPI) gene (Geurden et al., 2008b) and the glutamate
dehydrogenase (GDH) gene (Read et al., 2004) were used. Amplification products were visualised on
1.5% agarose gels with ethidium bromide. A positive (genomic DNA from a positive faecal sample) and
negative (PCR water) control sample were included in each PCR reaction.
91
PCR products were purified and sequenced from both strands. PCR products were purified using the
Qiaquick PCR purification kit (Qiagen) and fully sequenced using the Big Dye Terminator V3.1 Cycle
sequencing Kit (Applied Biosystems, California, USA). Sequencing was performed by an external
company (GATC Biotech) using the Big dye Terminator V3.1 Cycle sequencing Kit (Applied Biosystems)
and the reactions were analyzed using a 3730xl DNA Analyzer (ThermoFisher Scientific). Sequences were
assembled using Seqman 5.0 Software (Lasergene DNASTAR) and were aligned using the Basic Local
Alignment Search Tool (BLAST) as well as compared with reference sequences using MegAlign
(Lasergene DNASTAR). For multilocus genotyping Clustal X, 2.0.11 software was used and reference
sequences were selected according to Caccio et al. 2008.
Statistical analysis
Descriptive statistical analyses and multivariate methodologies were performed using the statistical
language R (R Core Team, 2013) and the pscl package (Jackman, 2008). Two approaches were applied as
follows.
Multivariate binary logistic models
The effect of the independent variables (age in months, gender, food, travel, neutering, living
conditions, living with other animals, antiparasitic treatment, time between treatment and sampling
date, diarrhoea during the last month, faecal score and type) on a sample being or not infected by a
parasite was studied through the utilization of multivariate logistic models with forward LR selection.
Initially, a test of the full model against a constant only model was performed in order to assess whether
there was a statistically significant effect of the examined independent predictors on the response
variable through the utilization of the Omnibus Tests of Model Coefficients, which uses the Chi-square
test to see if there is a significant difference between the log-likelihood (-2LL) of the baseline model
(constant model) and the model with the predictors. In addition, the Hosmer & Lemeshow (H-L) test was
performed to test whether the model provides a good fit to the data. (Additional file 2: Table S1).
Multivariate zero-inflated models
The effect of the independent variables on the parasitic infection intensity (egg/(oo)cyst counts per
gram) was studied through the utilization of a zero-inflated negative binomial model (Lambert, 1992)
due to the excess of zero counts and over dispersion of the data. In this analysis the group of shepherd
dogs were not included due to the limited number of samples examined. (Additional file 2: Table S2).
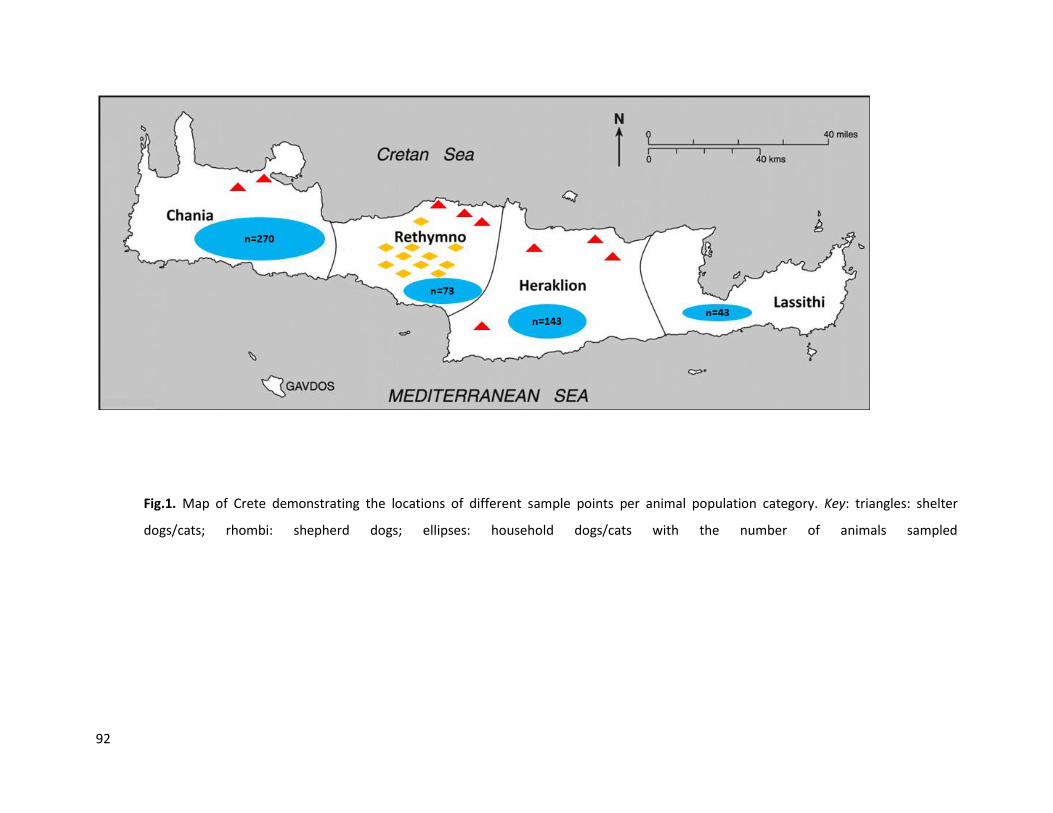
92
Fig.1. Map of Crete demonstrating the locations of different sample points per animal population category. Key: triangles: shelter
dogs/cats; rhombi: shepherd dogs; ellipses: household dogs/cats with the number of animals sampled
93
Results
Dogs
A total of 879 faecal samples from dogs were investigated for the presence of intestinal parasites. Of
these samples, 278 were derived from shelter dogs, 529 from household dogs and 72 from shepherd
dogs (Table 1). In total, 38.3% of dogs were found harbouring at least one intestinal parasite. Precisely,
25.5% were harbouring one parasite, 8.9% two and the rest 3-6 different species. The overall infection
rate was 25.2% (CI: 22.4–28.1) for Giardia spp; 9.2% (CI: 7.3-11.1) for Ancylostoma/Uncinaria spp; 7.6%
(CI: 5.9-9.4) for Toxocara spp; 5.9% (CI: 4.4-7.5) for Cryptosporidium spp; 4.6% (CI: 3.2-5.9) for
Cystoisospora spp; 2.7% (1.7-3.8) for Toxascaris leonina; 1.7% (CI: 0.9-2.6) for Capillaria spp; 0.8% (CI:
0.2-1.4) for taenid eggs, 0.2% (CI: 0-0.5) for Dipylidium caninum; and 0.1% (CI: 0-0.3) for Strongyloides
stercoralis. The results for the different dog populations are shown in Table 1.
Among the different canine populations studied, shelter dogs had the highest infection rates. In
particular, 62.9% of the shelter dogs were infected with at least one species of endoparasite compared
to 51.4% of the shepherd dogs and 23.8% of the household dogs. According to the multivariate binary
logistic model analysis, the odds ratio (OR) of Giardia infection was higher in shelter dogs than
household dogs (11.24 times higher) and shepherd dogs (15.63 times higher). However, based on the
multivariate zero-inflated model, among Giardia-infected individuals, household dogs had generally
higher cyst counts than shelter dogs (OR = 1.602). Regarding Cryptosporidium, and according to the
multivariate zero-inflated model, the odds ratio in favour of zero Cryptosporidium OPG for household
dogs was 8.248 times higher than that for shelter dogs, suggesting that household dogs were less prone
to Cryptosporidium infection than shelter dogs. However, Cryptosporidium-positive household dogs shed
more oocysts than infected shelter dogs (OR = 12.182). No statistically significant correlations between
infection with the other parasites and their living conditions were detected in both models (Table 2).
94
The mean age of the sampled dogs was approximately 3 years (39.5 months ± 41.8, SD). The majority of
the dogs were adults (≥ 12 months, n = 642), while 229 of them were younger than 12 months and 8
were of unspecified age. There was a significant correlation between age and Giardia infection (Figure 2)
and between age and T. leonina infection intensity. According to the multivariate binary logistic model
analysis, as age increased by one month, the odds of detecting Giardia cysts decreased by
1.9% = [(0.981–1) × 100] which is also confirmed by the multivariate zero-inflated model, according
which the odds of absence of Giardia cysts are increased by one unit increase of age. Similarly, according
to the multivariate zero-inflated model, as age increased by one month, the odds of detecting T. leonina
eggs decreases by 7% = [(0.93–1) × 100]. Regarding the other parasites studied, their correlation with
age was not statistically significant.
Of the dogs which had a history of recent diarrhoea, 43.1% were positive for at least one intestinal
parasite. However, faecal consistency was not significantly associated with parasitic infection. The
statistical analyses showed that signs of diarrhoea (based on faeces consistency) were significantly more
often present in younger animals (U = 100,667, P = < 0.001). Moreover, there was a statistically
significant association between the factors “recent record of diarrhoea” and “live with other animals”,
(χ2(6, N= 1138) = 29.495, P = <0.001).
On average, all of the dogs sampled received 2.1 anthelmintic treatments/year (range 0–6). The
arithmetic mean of anthelmintic treatments/year was 2.3 for household dogs, 2.2 for shelter dogs and
0.5 for shepherd dogs. Information about anthelmintic treatments was not defined in 48 cases (5.5%).
The frequency of antiparasitic treatment was also associated with diarrhoea and more specifically, the
effect of the odds of one treatment per year increase resulted in a decrease by 0.828 times in the trace
of “recent record of diarrhoea”, implying diarrhoea to be caused by parasite infestation. However, the
number of antiparasitic treatments/year received was not statistically associated with parasitic
infection.
The risk analyses of all the other factors which were evaluated in this study, such as the gender of the
animals, their living conditions (indoors/outdoors), the type of food, and recent travelling, showed no
statistically significant correlation with parasitic infection. Since almost all shelter dogs had access to the
external environment and the shepherd dogs were also living outside, the risk factor “living
indoors/outdoors” was assessed only for household dogs. The risk factor “recent travelling” was also not
analysed since only 4.2% of the dogs had been travelling during the last months before sampling,
including within counties. The same applied for the “type of food” factor, since the majority of the dogs
95
were eating industrial/cooked food and only 28 were fed with raw meat/offal, 64% of these being
shepherd dogs.
Giardia spp was the most prevalent parasite in all dogs (25.2%) and also in shelter (54.3%) and
household (12.9%) dogs in particular. The range of the cysts being shed by the infected animals varied
from 100 to 275,800 cysts per gram of faeces with 6,855 cysts shed on average. In the samples derived
from shelter and household dogs, the dog-specific assemblages C and D were dominating, either alone
(n = 72) or in mixed infections (n = 15). A limited number of dogs were infected with assemblage A
(n = 2), assemblage AI (n = 1), assemblage AII (n = 1) or a mixture of A with C or D (n = 5) or BIV-like and C
(n = 1) (Table 3). Regarding shepherd dogs, no positive PCR products were sequenced successfully.
Multilocus genotyping was performed from one dog sample which was classified as sub-assemblage AI
using 3 genetic loci (bg, TPIGEN and GDH). Alignment analysis of the isolate showed 100% homology
when compared to reference sequences A5 for bg; A1 for TPIGEN and A1 for GDH (Caccio et al., 2008),
resulting in multilocus genotype MLGA1 (Wang et al., 2016).
The PCR results for Cryptosporidium positive samples showed that the HSP70 gene amplified 23.6% of
the samples, whereas the 18S rDNA gene amplified 5.6%. Sequencing revealed the presence of
Cryptosporidium canis in 2 household dogs and C. scrofarum in a shelter dog.
Cats
In total, 264 faecal samples from cats were collected; 59 samples from shelters and 205 from owned
cats. Unfortunately, it was not possible to reach the target of 385 shelter cats. Overall, 38.1% of the cats
were harbouring at least one intestinal parasite. Precisely 26.4% were harbouring one parasite, 8.3%
two and the rest 3–4 different species. The prevalence was 20.5% (CI: 15.6–25.3) for Giardia spp; 9.5%
(CI: 5.9–13.0) for Cystoisospora spp; 8.3% (CI: 5.0–11.7) for Toxocara spp; 7.6% (CI: 4.4–10.8) for
Ancylostoma/Uncinaria spp; 6.8% (CI: 3.8–9.9) for Cryptosporidium spp; 4.2% (CI: 1.8–6.6) for Capillaria
spp; 0.8% (CI: 0.0–1.8) for taeniid eggs; and 0.4% (CI: 0–1.1) for Hammondia/Toxoplasma. The results
among different feline populations are shown in Table 4.
The mean age of the sampled cats was 3.4 years (40.8 months ± 48.9, SD). The majority of the cats were
adults (≥ 12 months, n = 161), while 97 of them were younger than 12 months and 6 were of unspecified
age.

96
Among the different feline populations studied, shelter cats had the highest infection rates. Specifically,
55.9% of the shelter cats were infected with at least one species of intestinal parasite compared to
33.2% of the household cats. However, infection rates of the different parasites were not statistically
different between different cat populations.
Of the cats which had a history of diarrhoea (30.9%), 32.9% were infected with at least one parasite. On
average, all cats sampled received 2.3 anthelmintic treatments/year (range 0–6). The mean number of
anthelmintic treatments/year was 1.9 for household cats and 2.7 for shelter cats. Information about
anthelmintic treatments was unknown in one case. Only 1.5% of the cats had been travelling during the
last months including within counties. No significant associations were found between parasite
infections and risk factors or between parasite infections and diarrhoea.
Giardia spp was the most prevalent parasite (20.5%), both in shelter cats (39.0%) and household cats
(15.6%). When targeting the 18S rRNA gene, assemblage A was identified in 10 cat samples. In 6 of these
samples, no amplification was obtained with the other genes, while in 4 samples only assemblage F was
detected in at least one of the other loci. Assemblage F was also found alone in 2 samples. Also, in two
different cases, the typing revealed the presence of assemblage BIV-like (n = 1) or the dog specific
assemblage C (n = 1) (Table 4).
Genotyping of Cryptosporidium positive samples showed the presence of the feline specific species
Cryptosporidium felis (n = 4).
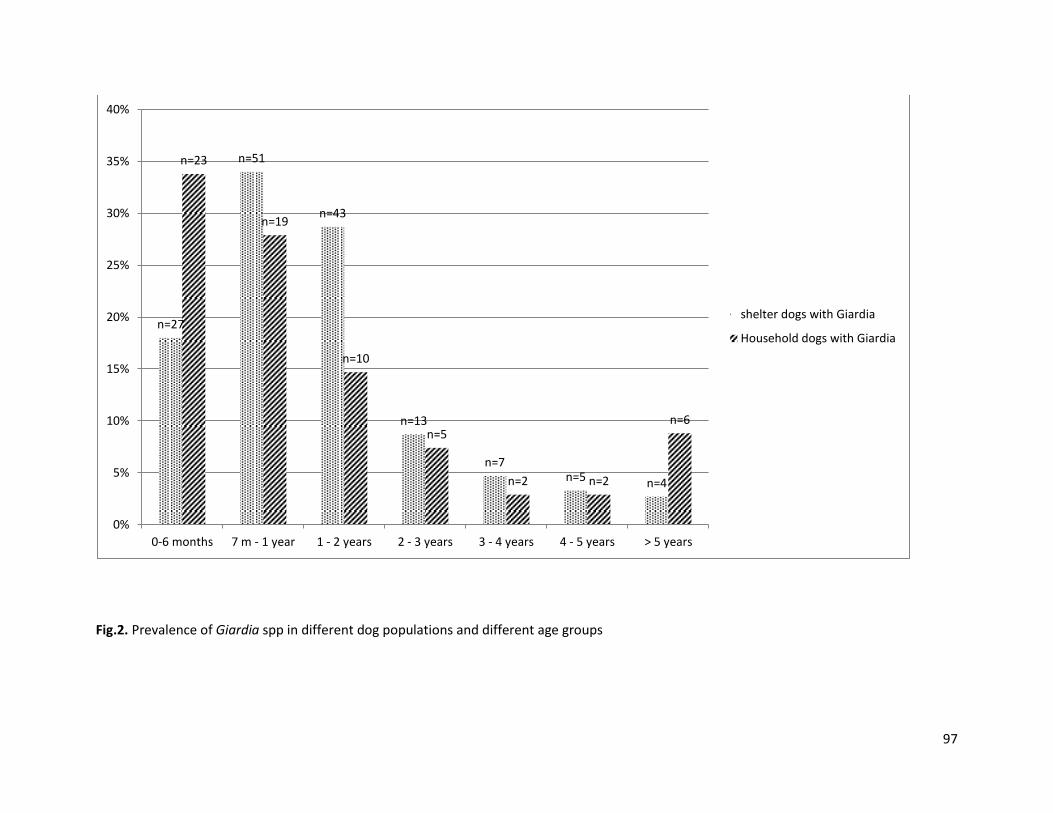
97
Fig.2. Prevalence of Giardia spp in different dog populations and different age groups
n=27
n=51
n=43
n=13
n=7 n=5 n=4
n=23
n=19
n=10
n=5
n=2 n=2
n=6
0%
5%
10%
15%
20%
25%
30%
35%
40%
0-6 months 7 m - 1 year 1 - 2 years 2 - 3 years 3 - 4 years 4 - 5 years > 5 years
shelter dogs with Giardia
Household dogs with Giardia
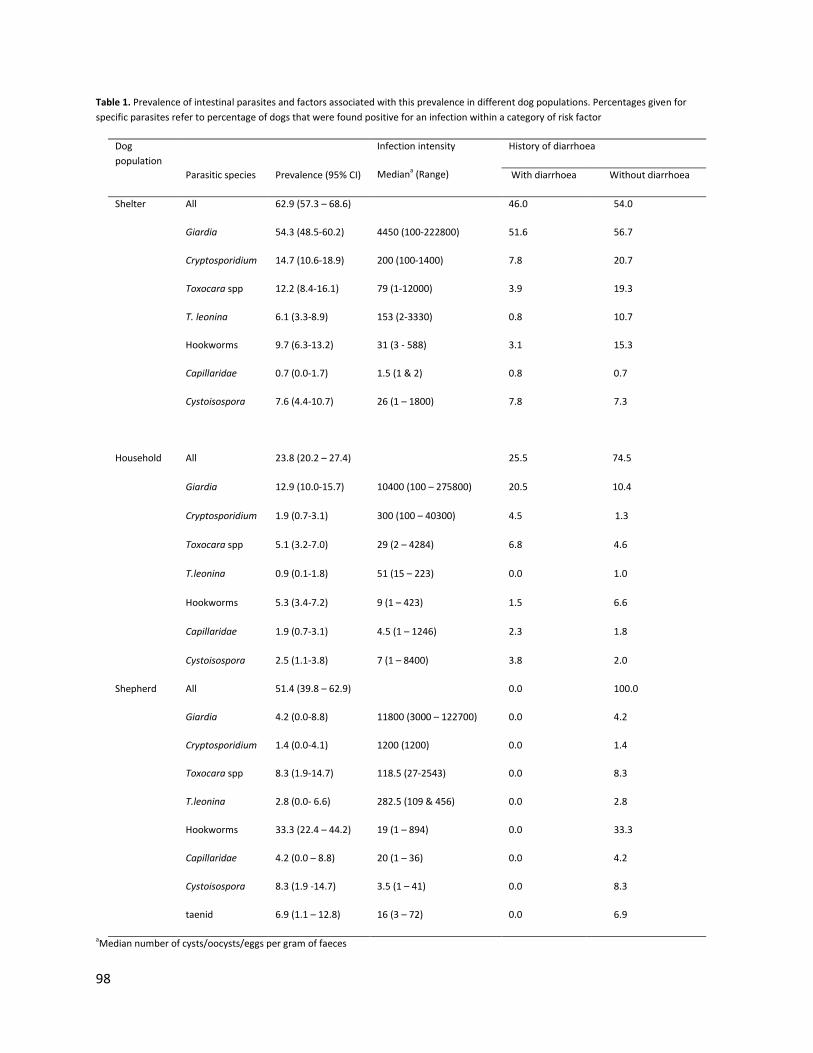
98
Table 1. Prevalence of intestinal parasites and factors associated with this prevalence in different dog populations. Percentages given for
specific parasites refer to percentage of dogs that were found positive for an infection within a category of risk factor
Dog
population
Infection intensity
Mediana (Range)
History of diarrhoea
Parasitic species Prevalence (95% CI) With diarrhoea Without diarrhoea
Shelter
Household
All
Giardia
Cryptosporidium
Toxocara spp
T. leonina
Hookworms
Capillaridae
Cystoisospora
62.9 (57.3 – 68.6)
54.3 (48.5-60.2)
14.7 (10.6-18.9)
12.2 (8.4-16.1)
6.1 (3.3-8.9)
9.7 (6.3-13.2)
0.7 (0.0-1.7)
7.6 (4.4-10.7)
4450 (100-222800)
200 (100-1400)
79 (1-12000)
153 (2-3330)
31 (3 - 588)
1.5 (1 & 2)
26 (1 – 1800)
46.0
51.6
7.8
3.9
0.8
3.1
0.8
7.8
54.0
56.7
20.7
19.3
10.7
15.3
0.7
7.3
All 23.8 (20.2 – 27.4) 25.5 74.5
Giardia 12.9 (10.0-15.7) 10400 (100 – 275800) 20.5 10.4
Cryptosporidium 1.9 (0.7-3.1) 300 (100 – 40300) 4.5 1.3
Toxocara spp 5.1 (3.2-7.0) 29 (2 – 4284) 6.8 4.6
T.leonina 0.9 (0.1-1.8) 51 (15 – 223) 0.0 1.0
Hookworms 5.3 (3.4-7.2) 9 (1 – 423) 1.5 6.6
Capillaridae 1.9 (0.7-3.1) 4.5 (1 – 1246) 2.3 1.8
Cystoisospora 2.5 (1.1-3.8) 7 (1 – 8400) 3.8 2.0
Shepherd All
Giardia
Cryptosporidium
Toxocara spp
51.4 (39.8 – 62.9)
4.2 (0.0-8.8)
1.4 (0.0-4.1)
8.3 (1.9-14.7)
11800 (3000 – 122700)
1200 (1200)
118.5 (27-2543)
0.0
0.0
0.0
0.0
100.0
4.2
1.4
8.3
T.leonina 2.8 (0.0- 6.6) 282.5 (109 & 456) 0.0 2.8
Hookworms 33.3 (22.4 – 44.2) 19 (1 – 894) 0.0 33.3
Capillaridae 4.2 (0.0 – 8.8) 20 (1 – 36) 0.0 4.2
Cystoisospora
taenid
8.3 (1.9 -14.7)
6.9 (1.1 – 12.8)
3.5 (1 – 41)
16 (3 – 72)
0.0
0.0
8.3
6.9
aMedian number of cysts/oocysts/eggs per gram of faeces
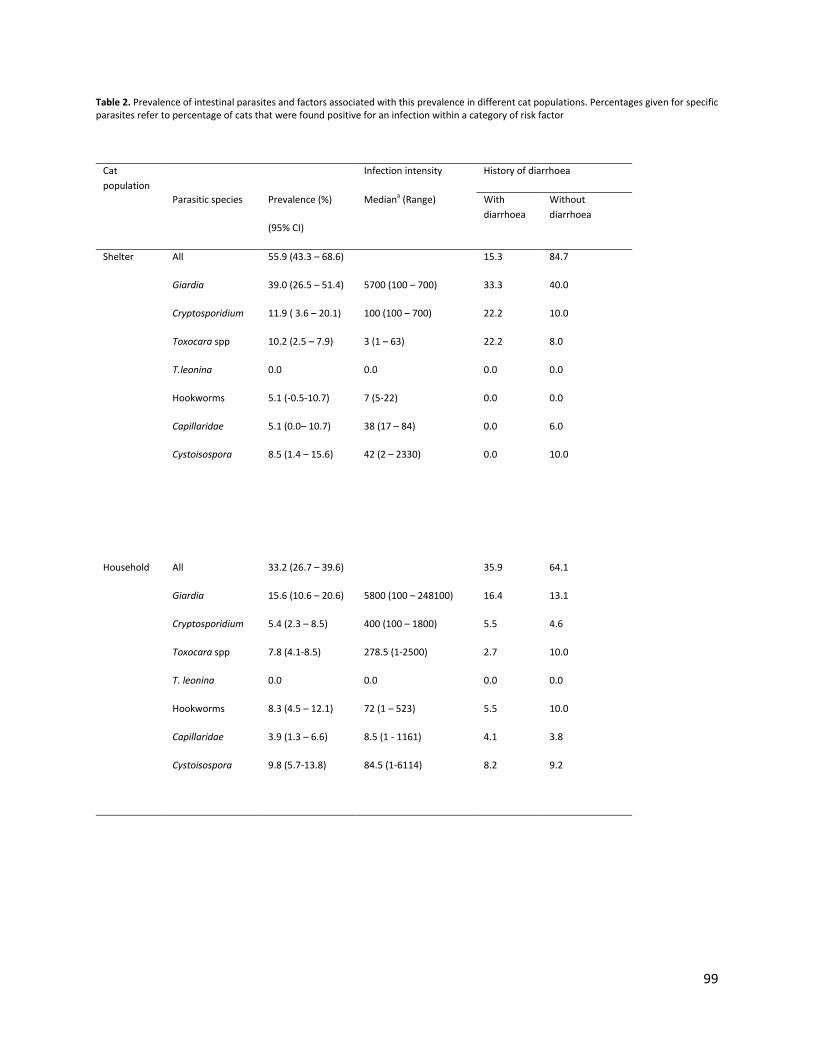
99
Table 2. Prevalence of intestinal parasites and factors associated with this prevalence in different cat populations. Percentages given for specific parasites refer to percentage of cats that were found positive for an infection within a category of risk factor
Cat
population
Infection intensity History of diarrhoea
Parasitic species Prevalence (%)
(95% CI)
Mediana (Range) With
diarrhoea
Without
diarrhoea
Shelter All
Giardia
Cryptosporidium
Toxocara spp
T.leonina
Hookworms
Capillaridae
Cystoisospora
55.9 (43.3 – 68.6)
39.0 (26.5 – 51.4)
11.9 ( 3.6 – 20.1)
10.2 (2.5 – 7.9)
0.0
5.1 (-0.5-10.7)
5.1 (0.0– 10.7)
8.5 (1.4 – 15.6)
5700 (100 – 700)
100 (100 – 700)
3 (1 – 63)
0.0
7 (5-22)
38 (17 – 84)
42 (2 – 2330)
15.3
33.3
22.2
22.2
0.0
0.0
0.0
0.0
84.7
40.0
10.0
8.0
0.0
0.0
6.0
10.0
Household All
Giardia
Cryptosporidium
Toxocara spp
T. leonina
33.2 (26.7 – 39.6)
15.6 (10.6 – 20.6)
5.4 (2.3 – 8.5)
7.8 (4.1-8.5)
0.0
5800 (100 – 248100)
400 (100 – 1800)
278.5 (1-2500)
0.0
35.9
16.4
5.5
2.7
0.0
64.1
13.1
4.6
10.0
0.0
Hookworms 8.3 (4.5 – 12.1) 72 (1 – 523) 5.5 10.0
Capillaridae
Cystoisospora
3.9 (1.3 – 6.6)
9.8 (5.7-13.8)
8.5 (1 - 1161)
84.5 (1-6114)
4.1
8.2
3.8
9.2
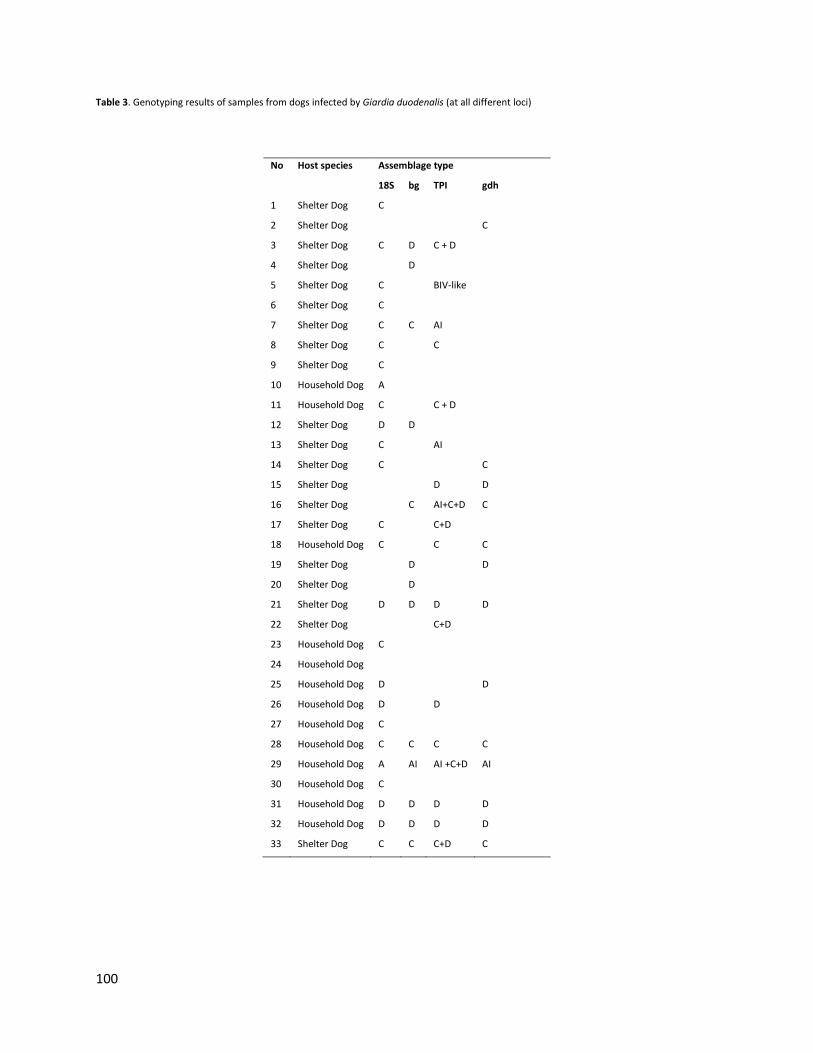
100
Table 3. Genotyping results of samples from dogs infected by Giardia duodenalis (at all different loci)
No Host species Assemblage type
18S bg TPI gdh
1 Shelter Dog C
2 Shelter Dog
C
3 Shelter Dog C D C + D
4 Shelter Dog
D
5 Shelter Dog C
BIV-like
6 Shelter Dog C
7 Shelter Dog C C AI
8 Shelter Dog C
C
9 Shelter Dog C
10 Household Dog A
11 Household Dog C
C + D
12 Shelter Dog D D
13 Shelter Dog C
AI
14 Shelter Dog C
C
15 Shelter Dog
D D
16 Shelter Dog
C AI+C+D C
17 Shelter Dog C
C+D
18 Household Dog C
C C
19 Shelter Dog
D
D
20 Shelter Dog
D
21 Shelter Dog D D D D
22 Shelter Dog
C+D
23 Household Dog C
24 Household Dog
25 Household Dog D
D
26 Household Dog D
D
27 Household Dog C
28 Household Dog C C C C
29 Household Dog A AI AI +C+D AI
30 Household Dog C
31 Household Dog D D D D
32 Household Dog D D D D
33 Shelter Dog C C C+D C
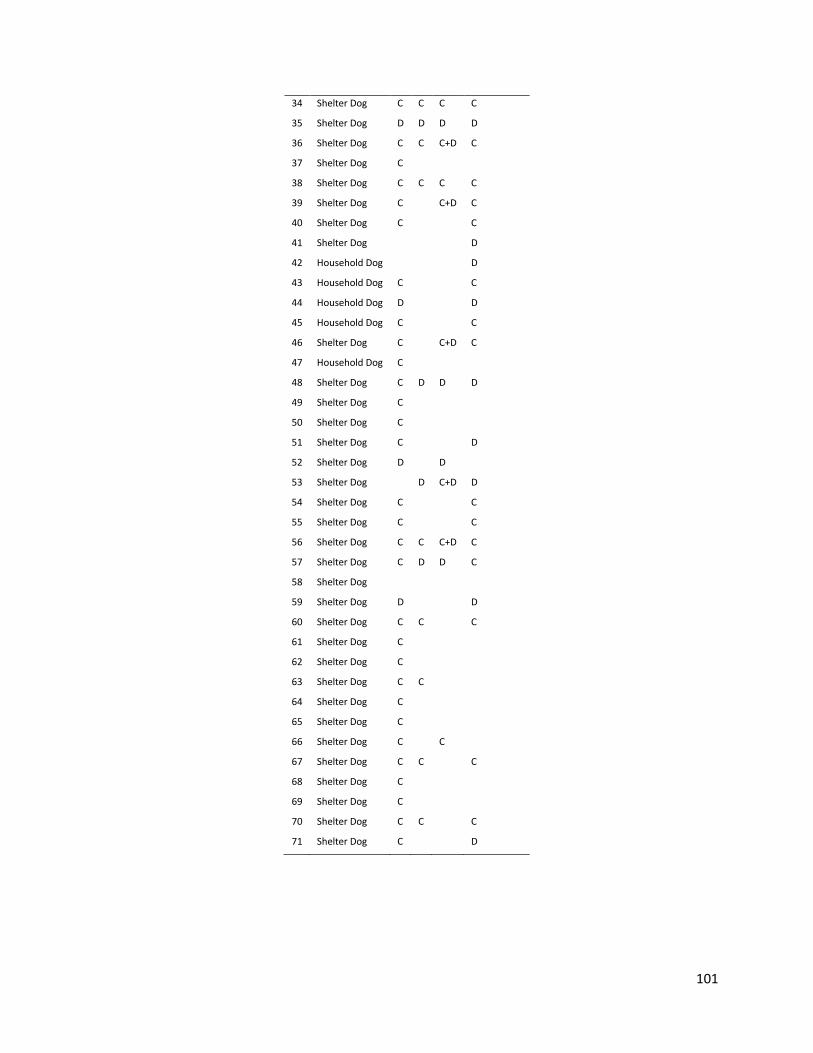
101
34 Shelter Dog C C C C
35 Shelter Dog D D D D
36 Shelter Dog C C C+D C
37 Shelter Dog C
38 Shelter Dog C C C C
39 Shelter Dog C
C+D C
40 Shelter Dog C
C
41 Shelter Dog
D
42 Household Dog
D
43 Household Dog C
C
44 Household Dog D
D
45 Household Dog C
C
46 Shelter Dog C
C+D C
47 Household Dog C
48 Shelter Dog C D D D
49 Shelter Dog C
50 Shelter Dog C
51 Shelter Dog C
D
52 Shelter Dog D
D
53 Shelter Dog
D C+D D
54 Shelter Dog C
C
55 Shelter Dog C
C
56 Shelter Dog C C C+D C
57 Shelter Dog C D D C
58 Shelter Dog
59 Shelter Dog D
D
60 Shelter Dog C C
C
61 Shelter Dog C
62 Shelter Dog C
63 Shelter Dog C C
64 Shelter Dog C
65 Shelter Dog C
66 Shelter Dog C
C
67 Shelter Dog C C
C
68 Shelter Dog C
69 Shelter Dog C
70 Shelter Dog C C
C
71 Shelter Dog C
D
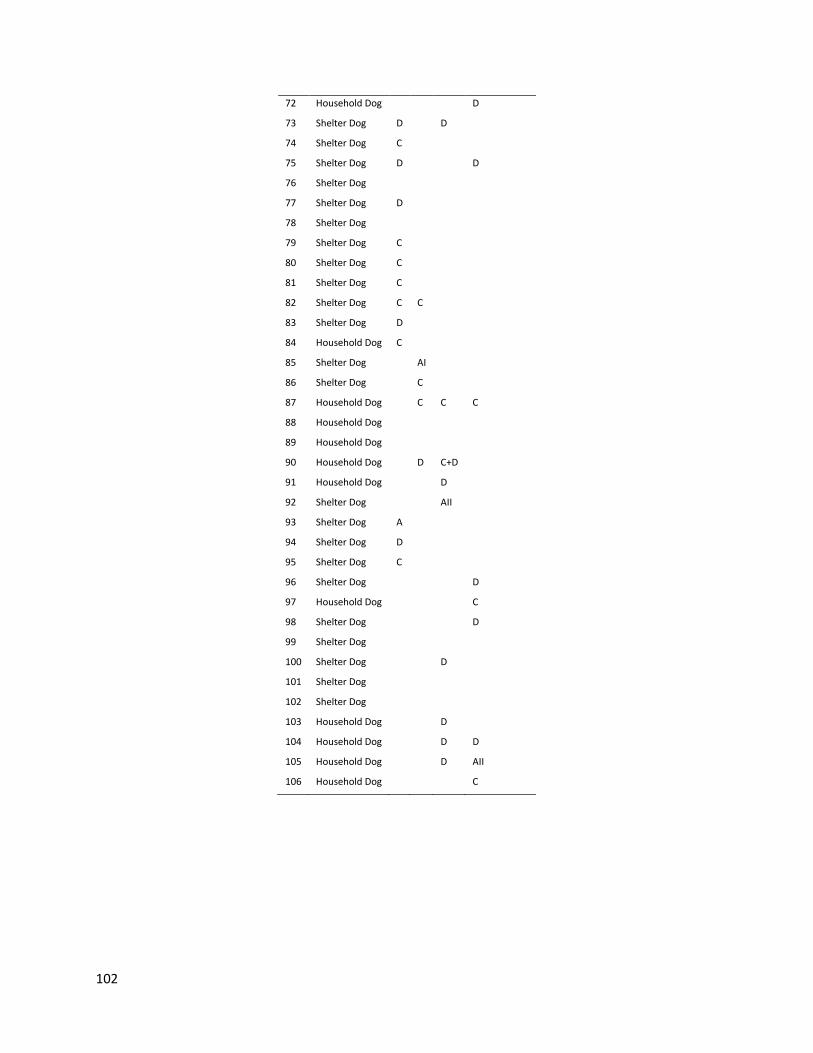
102
72 Household Dog
D
73 Shelter Dog D
D
74 Shelter Dog C
75 Shelter Dog D
D
76 Shelter Dog
77 Shelter Dog D
78 Shelter Dog
79 Shelter Dog C
80 Shelter Dog C
81 Shelter Dog C
82 Shelter Dog C C
83 Shelter Dog D
84 Household Dog C
85 Shelter Dog
AI
86 Shelter Dog
C
87 Household Dog
C C C
88 Household Dog
89 Household Dog
90 Household Dog
D C+D
91 Household Dog
D
92 Shelter Dog
AII
93 Shelter Dog A
94 Shelter Dog D
95 Shelter Dog C
96 Shelter Dog D
97 Household Dog C
98 Shelter Dog D
99 Shelter Dog
100 Shelter Dog D
101 Shelter Dog
102 Shelter Dog
103 Household Dog D
104 Household Dog D D
105 Household Dog D AII
106 Household Dog C
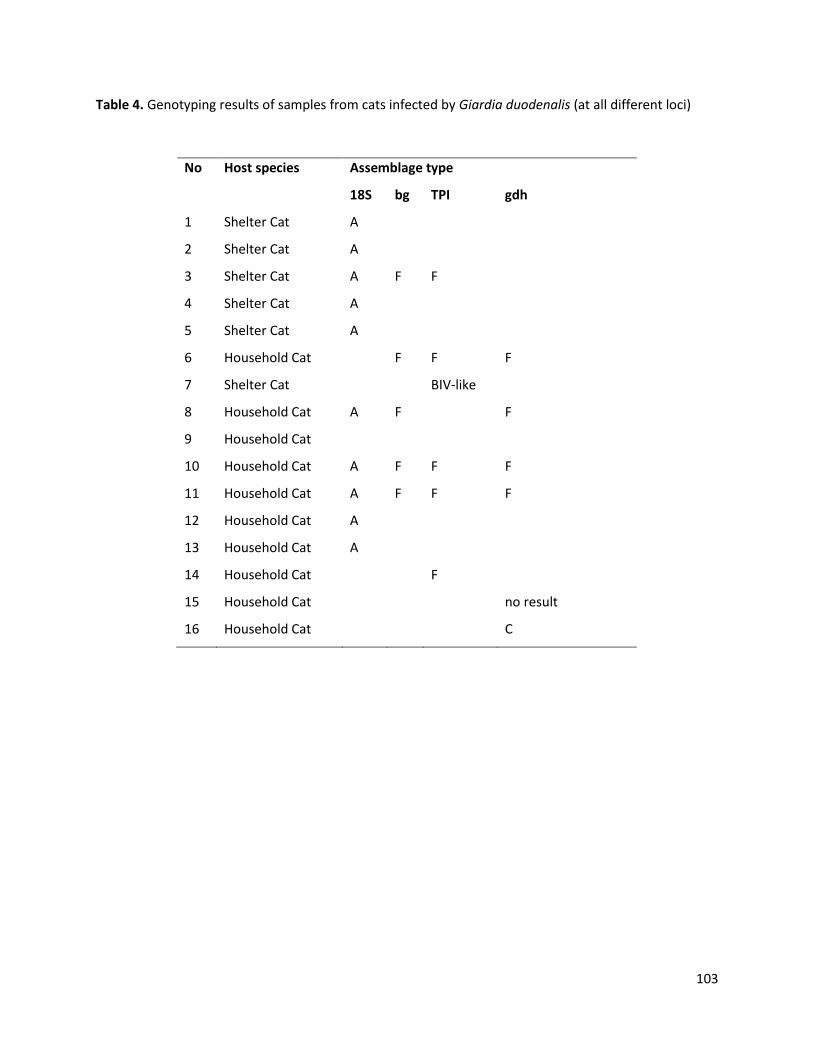
103
Table 4. Genotyping results of samples from cats infected by Giardia duodenalis (at all different loci)
No Host species Assemblage type
18S bg TPI gdh
1 Shelter Cat A
2 Shelter Cat A
3 Shelter Cat A F F
4 Shelter Cat A
5 Shelter Cat A
6 Household Cat
F F F
7 Shelter Cat
BIV-like
8 Household Cat A F
F
9 Household Cat
10 Household Cat A F F F
11 Household Cat A F F F
12 Household Cat A
13 Household Cat A
14 Household Cat
F
15 Household Cat
no result
16 Household Cat
C
104
Discussion
The infection rates of intestinal parasites detected in this study, revealed a high prevalence of parasitic
infections (38.2%) and the presence of different species of endoparasites in both dogs and cats. These
infection rates were equally distributed within animal species (38.3% for dogs and 38.1% for cats)
involved in the study. With the exception of shepherd dogs, Giardia spp was the most prevalent parasite
detected in the dog and cat populations followed by significant prevalences of ascarids, hookworms and
taeniid infections. These results are also reported in other studies which consider Giardia the most
common enteric parasite of dogs and cats in developed countries (Palmer et al., 2008; Thompson et al.,
2008; Claerebout et al., 2009; Scaramozzino et al., 2009; Ballweber et al., 2010; Barutzki et al., 2011;
Polak et al., 2014; Zanzani et al., 2014; Osman et al., 2015). In shepherd dogs, hookworms were the
most prevalent parasite species detected.
Among the targets of this study was to investigate the potential effect of animal lifestyle to parasitism so
animals living in households, shelters or farms were included. The results showed that more than half of
the shelter dogs and cats were infected with at least one species of endoparasite, which was more or
less expected, taking into consideration the less hygienic conditions that those animals are living in
combined with a high population density that usually exists in shelters. A high level of parasitism has
been previously reported in shelter dogs (Claerebout et al., 2009; Ortuno and Castella, 2011; Ortuno et
al., 2014; Simonato et al., 2015) while in shelter cats the prevalence observed in other studies was lower
(Becker et al., 2012; Ito et al., 2016).
More than half of the shepherd dogs (51.4%) were positive for at least one species of intestinal parasite.
The infection rate of intestinal parasites estimated in shepherd dogs in this study was higher than in a
previous record from Greece (26.0%) (Papazahariadou et al., 2007). Such differences are expected in
cross-sectional studies especially given time and region differences. However, our results were in
agreement with a study conducted in farm dogs in Portugal (57.4%) (Mateus et al., 2014).
Shepherd/farm dogs often receive less veterinary care and preventive treatments. Compared to a
general average of more than 2 anthelmintic treatments per year, shepherd dogs in our study received
only 0.5 treatments per year.
Although the prevalence of intestinal parasites in household dogs was lower than in shelters, although
not statistically significant for many species, the percentage of individuals infected was still noteworthy
105
(23.8%). In similar studies conducted in Italy the prevalence of intestinal parasites in household dogs
was even higher, reaching 57.0% of the animals (Riggio et al., 2013; Zanzani et al., 2014). In our study
there was no difference in the risk of infection between dogs living in an apartment with no access to a
yard or a garden and dogs living in a house with access to outdoors. A reason for that could be that even
dogs that are kept permanently indoors are regularly being walked by their owners in public places
getting in close contact with other dogs (including stray ones) or their contaminated faeces. Similar
results were recorded in the household cats studied, but this was probably due to the fact that the
majority of them also live partially outdoors. The parasitism reported in household cats in this study is in
agreement with the infection rates reported in Austria, Belgium, the Netherlands, France, Hungary, Italy,
Romania and Spain (Riggio et al., 2013; Beugnet et al., 2014; Nijsse et al., 2016).
Although both household and shelter dogs received regular anthelmintic treatments (i.e. an average of
2.3 for household dogs and 2.2 for shelter dogs per year), this seemed not to control parasitism
efficiently. This is in agreement with the general recommendation by ESCCAP for roundworms in which
it is suggested that annual or twice yearly treatments do not have a significant impact on the prevalence
of patent infections within a population, and therefore a treatment frequency of at least 4 times per
year is recommended (Worm Control in Dogs and Cats - ESCCAP, www.esccap.org). Recent modeling
indicated that the environmental Toxocara contamination by dogs can only be reduced significantly if
compliance to the four times a year treatment advice is sufficiently high (90.0%) or if at least half of the
dog owners consistently remove their dog’s faeces (Nijsse et al., 2015). In cats, the frequency of
anthelmintic treatment differed between categories, with shelter cats being more frequently treated
(i.e. an average of 1.9 for household cats and 2.7 for shelter cats per year). This could be explained by a
misconception of the cat owners that indoor cats do not need preventive treatments (Matos et al.,
2015).
Despite the high prevalence of parasitic infections, most animals were healthy with no obvious signs of
suffering probably due to the low parasitic burden, as at least suggested by the low number of
egg/(oo)cyst output recorded in most cases (even if usually there is not a clear correlation between
numbers of eggs/(oo-)cysts and clinical signs). It was not statistically proven that recent records of
diarrhoea were correlated to parasitism as also shown previously (Hill et al., 2000; Hackett et al., 2003)
although there was evidence that anthelmintic treatment had a positive effect on reducing such records.
A supporting argument for the absence of clinical disease could be that the majority of animals were
adults at the time of sampling. Young animals are more sensitive to parasitism (Gates et al., 2009) but
106
although in this study there was a tendency of older animals (>2 year-old dogs and > 1 year-old cats) to
be less infected, this was not statistically significant for most parasites. The only statistically proven facts
were that the chance to get infected by Giardia spp and the infection intensity of T. leonina was
negatively correlated to age in dogs.
Given the high prevalence and the potential zoonotic importance, Giardia and Cryptosporidium positive
samples were further investigated by PCR and sequencing of the positive PCR products. In dogs, the
host-specific assemblages C and D dominated, which has been described before in various studies
(Sulaiman et al., 2003; Berilli et al., 2004; Lalle et al., 2005; Barutzki et al., 2007; Souza et al., 2007;
Scorza et al., 2012; Zanzani et al., 2014; Pallant et al., 2015; Simonato et al., 2015). Few dogs were (co)-
infected with assemblage A, and the majority of these were identified as sub-assemblage AI. Sub-
assemblage AI is frequently found in animals, while humans are most frequently infected with sub-
assemblage AII (Xiao and Fayer, 2008; Minetti et al., 2015). The sequence analysis in one G. duodenalis
sample further revealed a multilocus genotype (MLG) which was previously described in calves in China
(Wang et al., 2016). Together, these results suggest that there is no significant risk for zoonotic
transmission of Giardia infections from dogs in Crete.
In cats, the genotyping results seemed to indicate the dominance of the potentially zoonotic assemblage
A in shelter animals and the co-infection of assemblages A and the feline specific assemblage F in
household cats. However, the zoonotic assemblage A was identified only at the 18S rDNA locus, while
only assemblage F was identified at the other loci. Since no distinction could be made between
assemblages A and F in the amplified region of the conserved rRNA 18S gene, it cannot be excluded that
(some of) the samples that were amplified with rDNA 18S gene were assemblage F instead of A.
Therefore, no conclusion can be drawn on the zoonotic risk associated with Giardia infections in cats.
Regarding Cryptosporidium, the dog specific C. canis was identified in only two household dogs and the
pig specific C. scrofarum in one shelter dog. Cryptosporidium canis has been also detected in household
dogs in other studies (Lucio-Forster et al., 2010; Ryan et al., 2014; Osman et al., 2015) and isolated in
humans, mainly children and immunocomprimised individuals in developing countries (Xiao et al., 2007;
Bowman et al., 2010), suggesting its potential public health impact. To our knowledge, this is the first
case of C. scrofarum infection reported in a dog. Since keeping backyard pigs is quite a common practice
in the area, it is possible that this dog ingested the oocysts before being transferred to the shelter. In
such a scenario this could be a case of pseudoparasitism, given that this dog was 2.5 month-old and only
recently introduced to the shelter. In cats, sequencing was not efficient; nevertheless, it revealed the
107
presence of the feline-specific C. felis. Since our genotyping results revealed the presence of host-
specific Cryptosporidium species in both dogs and cats which have been implicated in very few human
infections and mainly in developing countries, we could suggest that the zoonotic potential of
Cryptosporidium from dogs and cats in the study area is low.
Apart from Giardia and Cryptosporidium, ascarids, hookworms and taeniids are also considered to be
zoonotic (Dakkak, 1992; Caccio and Ryan, 2008; Thompson and Smith, 2011; Traversa, 2012;
Macpherson, 2013). The two major ascarid species T. canis and T. cati (to a lesser extent) are
responsible for human infections (Traversa, 2012; Macpherson, 2013). In our study the prevalence of
Toxocara spp in dogs and cats was 7.6 and 8.3%, respectively. In dogs, we characterised all Toxocara
eggs found as Toxocara spp since those infections were only microscopically diagnosed and as
previously suggested they could either belong to T. canis or T. cati since coprophagy is not unusual for
dogs and the presence of T. cati eggs in dog faeces might in fact relate to pseudoparasitism (Fahrion et
al., 2011; Nijsse et al., 2014). The infection rates found in the present study are similar to those reported
in Europe which vary from 3.5 to 34.0% for T. canis in dogs from different epidemiological environments
and from 7.2 to 76.0% for T. cati in cats (Parsons, 1987; Fok et al., 2001; Habluetzel et al., 2003; Le Nobel
et al., 2004; Dubna et al., 2007; Martinez-Carrasco et al., 2007; Lee et al., 2010; Nijsse et al., 2015; Nijsse
et al., 2016). The Toxocara infection was high, especially in shelter dogs and cats, as also reported
before (Haralambidis, 1993; Simonato et al., 2015; Villeneuve et al., 2015). Although mainly T. canis is
considered responsible for human toxocarosis (Fisher, 2003), the role of T. cati in human toxocarosis
should not be underestimated (Overgaauw, 1997; Fisher, 2003; Smith et al., 2006). In Greece,
toxocarosis in humans has not been studied extensively since published data are restricted only to some
sporadic cases (Xinou et al., 2003; Haralambidou et al., 2005) and one study regarding the
seroprevalence of T. canis in children (Theodoridis et al., 2001). Our results combined to all European
studies presented above strongly suggest that more information is needed.
Hookworm infection rates were 9.2% in dogs and 7.6% in cats. The highest infection rates of hookworms
were identified in shepherd dogs (33.3%) similar to the study of Mateus et al. 2014 in Portugal (31.0%).
Since different hookworm species were not differentiated, the zoonotic risk associated with hookworm
infections could not be determined.
The detection of taeniid eggs in shepherd dogs is worth mentioning. Unlike shelter and household dogs,
shepherd dogs seem to be more prone to taeniid infection, which possibly is due to the frequent
consumption of raw meat and carcasses (Jenkins et al., 2006; Palmer et al., 2008). Echinococcosis is still
108
endemic in Greece with a high prevalence reported in livestock (Sotiraki and Chaligiannis, 2010;
Katzoura et al., 2013; Chaligiannis et al., 2015). However, there are no recent reports regarding the
prevalence of taeniids in dogs. Taking into consideration our results in combination with the high
prevalence of E. granulosus in livestock, which is transmitted through dogs, we could assume that
shepherd dogs in Greece could be a reservoir for human infections.
Conclusions
In conclusion, we have recorded high levels of (multi)-parasitism in both dogs and cats in the study area.
Most of the animals were harbouring different species of parasites sometimes in high numbers
according to the egg/(oo)cyst counts. This is proof that those parasites are greatly abundant within
animal populations regardless of lifestyle. Thus, the results of our study stress the need for better
anthelmintic control schemes and control of intestinal protozoa in dogs and cats, tailored to their
individual needs, in order to safeguard animal and public health. Thus, a holistic approach for the
management of endoparasites in companion animals should be implemented including for instance,
proper administration of the drugs e.g. dose and frequency of administration.
Aknowledgements
This work is a part of a phD scholarship funded by the Greek State Scholarships Foundation. The authors
will also like to thank all the veterinarians, the shelter owners, Dr Alexandros Stefanakis, Mr Anastasios
Anastasiades and other colleagues in Crete who contributed in this study.
Funding
This work is a part of a PhD scholarship funded by the Greek State Scholarships Foundation.
Authors’ contributions
This study was conducted by DK as part of her PhD thesis. Also, DK participated in the data collection
and analysis and developed the first draft of the manuscript. All other authors played a role in data
collection and analysis, and interpretation of findings (EC, DA, PL, NV, SC and SS). All authors read and
approved the final manuscript.
109
Competing interests
The authors declare that they have no competing interests.
Consent for publication
Not applicable.
Ethical considerations
The study was carried out in compliance with the national animal welfare regulations. Diagnostic
veterinary procedures are not within the context of relevant EU legislation for animal experimentations
(Directive 86/609/EC) and may be performed in order to diagnose animal diseases and improve animal
welfare. Samples were collected by registered veterinarians who ensured owners consent and caused
no suffering.
Appendix A. Supplementary data
Additional file 1: Table S1: Binary logistic model for Giardia spp infection rate in dogs.
Table S2: Zero-inflation negative binomial model for parasite infection intensity in dog samples.
110
References
Ballweber L.R., Xiao L., Bowman D.D., Kahn G., Cama V.A. Giardiasis in dogs and cats: update on
epidemiology and public health significance. Trends Parasitol. 2010;26:180-189. Barutzki D., Thompson R.C., Wielinga C., Parka U., Schaper R. Observations on Giardia infection
in dogs from veterinary clinics in Germany. Parasitol Res. 2007;101:153-156. Barutzki D., Schaper R. Results of parasitological examinations of faecal samples from cats and
dogs in Germany between 2003 and 2010. Parasitol Res. 2011;109:S45-60. Becker A.C., Rohen M., Epe C., Schnieder T. Prevalence of endoparasites in stray and fostered
dogs and cats in Northern Germany. Parasitol Res. 2012;111:849-857. Berilli F., Di Cave D., De Liberato C., Franco A., Scaramozzino P., Orecchia P. Genotype
characterization of Giardia duodenalis isolates from domestic and farm animals by SSU-rRNA gene sequencing. Vet Parasitol. 2004;122:193-199.
Beugnet F., Bourdeau P., Chalvet-Monfray K., Cozma V., Farkas R., Guillot J., Halos L., Joachim A., Losson B., Miro G., Otranto D., Renaud M., Rinaldi L. Parasites of domestic owned cats in Europe: co-infestations and risk factors. Parasit Vectors. 2014;7:291.
Bowman D.D., Lucio-Forster A. Cryptosporidiosis and giardiasis in dogs and cats: veterinary and public health importance. Exp Parasitol. 2010;124:121-127.
Caccio S.M., Beck R., Lalle M., Marinculic A., Pozio E. Multilocus genotyping of Giardia duodenalis reveals striking differences between assemblages A and B. Int J Parasitol. 2008;38:1523-31.
Caccio S., Ryan U. Molecular epidemiology of giardiasis. Mol Biochem Parasitol. 2008;160:75-80. Capelli G., Paoletti B., Iorio R., Frangipane di Regalbono A., Pietrobelli M., Bianciardi P.,
Giangaspero A. Prevalence of Giardia spp. In dogs and humans in nothern and central Italy. Parasitol Res. 2003;90:S154-S155.
Chaligiannis I., Maillard S., Boubaker G., Spiliotis M., Saratsis A., Gottstein B., Sotiraki S. Echinococcus granulosus infection dynamics in livestock of Greece. Acta Trop. 2015;150:64-70.
Chen J., Xu M.J., Zhou D.H., Song H.Q., Wang C.R., Zhu X.Q. Canine and feline parasitic zoonoses in China. Parasit Vectors. 2012;5:152.
Claerebout E., Casaert S., Dalemans A.C., De Wilde N., Levecke B., Vercruysse J., Geurden T. Giardia and other intestinal parasites in different dog populations in Nothern Belgium. Vet Parasitol. 2009;161:41-46.
Dakkak A. Guidelines for diagnosis, surveillance and control of echinococcosis. Veterinary Public Health, World Health Organization, Geneva Switzerland; 1992.Echinococcus-hydatidiosis in North Africa: geographical distribution of species and strains and prevalence in man and animals.
Deplazes P., Van Knapen F., Schweiger A., Overgaauw P.A.M. Role of pet dogs and cats in the transmission of helminthic zoonoses in Europe, with a focus on echinococcosis and toxocarosis. Vet Parasitol. 2011;182:41-53.
Dubna S., Langrova I., Napravnik J., Jankovska I., Vadlejch J., Pekar S., Fechtner J. The prevalence of intestinal parasites in dogs from Prague, rural areas, and shelters of the Czech Republic. Vet Parasitol. 2007;145:120-128.
Fahrion A.S., Schnyder M., Wichert B., Deplazes P. Toxocara eggs shed by dogs and cats and their molecular and morphometric species-specific identification: is the finding of T.cati eggs shed by dogs of epidemiological relevance? Vet Parasitol. 2011;177:186-9.
Fisher M. Toxocara cati: an underestimated zoonotic agent. Trends Parasitol. 2003;19:167-70. Fok E., Szatmari V., Busak K., Rozqonyi F. Prevalence of intestinal parasites in dogs in some
urban and rural areas of Hungary. Vet Q. 2001;23:96-8.
111
Gates M.C. and Nolan T.J. Endoparasite prevalence and recurrence across different age groups of dogs and cats. Vet Parasitol. 2009;166(1-2):153-158.
Geurden T., Berkvens D., Casaert S., Vercruysse J., Claerebout E. A Bayesian evaluation of three diagnostic assays for the detection of Giardia duodenalis in symptomatic and asymptomatic dogs. Vet parasitol. 2008a;157(1-2):14-20.
Geurden T., Geldhof P., Levecke B., Martens C., Berkvens D., Casaert S., Vercruysse J., Claerebout E. Mixed Giardia duodenalis assemblage A and E infections in calves. Int J Parasitol. 2008b;38:259-264.
Habluetzel A., Traldi G., Ruggieri S., Attili A.R., Scuppa P., Marchetti R., Menghini G., Esposito F. An estimation of Toxocara canis prevalence in dogs, environmental egg contamination and risk of human infection in the Marche region of Italy. Vet Parasitol. 2003;113:243-52.
Hackett T., Lappin M.R. Prevalence of enteric pathogens in dogs of north-central Colorado. J Am Anim Hosp Assoc. 2003;39:52–56.
Hamnes I.S., Gjerde B.K., Robertson L.J. A longitudinal study on the occurrence of Cryptosporidium and Giardia in dogs during their first year of life. Acta Vet Scand. 2007;49:22.
Haralambidis S.T. Toxocarosis. In: Haralambidis S.T., ed. Issues of Parasitology that Concern Public Health in Thessaloniki. Thessaloniki, Greece: University Studio Press; 1993:41-45.
Haralambidou S., Vlachaki E., Ioannidou E., Milioni V., Haralambidis S., Klonizakis I. Pulmonary and myocardial manifestations due to Toxocara canis infection. Eur J Intern Med. 2005;16:601-2.
Hill S.L., Cheney J.M., Taton-Allen G.F., Reif J.S., Bruns C., Lappin M.R. Prevalence of enteric zoonotic organisms in cats.J Am Vet Med Assoc. 2000;216:687–692.
Hopkins R.M., Meloni B.P., Groth D.M., Wetherall J.D., Reynoldson J.A., Thompson R.C.A. Ribosomal RNA sequencing reveals differences between the genotypes of Giardia isolates recovered from humans and dogs living in the same locality. J Parasitol. 1997;83:44-51.
Ito Y., Itoh N., Kimura Y., Kanai K. Prevalence of intestinal parasites in breeding cattery cats in Japan. J Feline Med Surq. 2016;18:834-837.
Itoh N., Kanai K., Kimura Y., Chikazawa S., Hori Y., Hoshi F. Prevalence of intestinal parasites in breeding kennel dogs in Japan. Parasitol Res. 2015;114(3):1221-4.
Jackman S. pscl: Classes and Methods for R Developed in the Political Science Computational Laboratory, Stanford University. Department of Political Science, Stanford University, Stanford, California. R package version 0.95, URL http:// CRAN.R-project.org/ package=pscl. Accessed 25 Aug 2016.
Jenkins D.J., Mckinlay A., Duolong H.E., Bradshaw H., Craig P.S. Detection of Echinococcus granulosus coproantigens in faeces from naturally infected rural domestic dogs in south eastern Australia. Aust Vet J. 2006;84:12-16.
Joffe D., Van Niekerk D., Gagne F., Gilleard J., Kutz S., Lobingier R. The prevalence of intestinal parasites in dogs and cats in Calgary, Alberta. Can Vet J. 2011;52:1323-1328.
Jones K.E., Patel N.G., Levy M.A., Storeygard A., Balk D., Gittleman J.L., Daszak P. Global trends in emerging infectious diseases. Nature. 2008;451:990-994.
Katzoura V., Diakou A., Kouam M.K., Feidas H., Theodoropoulou H., Theodoropoulos G. Seroprevalence and risk factors associated with zoonotic parasitic infections in small ruminants in the Greek temperate environment. Parasitol Int. 2013;62:554-560.
Kostopoulou D., Casaert S., Tzanidakis N., van Doorn D., Demeler J., von Samson-Himmelstjerna G., Saratsis A., Voutzourakis N., Ehsan A., Doornaert T., Looijen M., De Wilde N., Sotiraki S., Claerebout E., Geurden T. The occurrence and genetic characterization of Cryptosporidium and Giardia species in foals in Belgium, The Netherlands, Germany and Greece. Vet Parasitol. 2015;211(3-4):170-4.
112
Lalle M., Pozio E., Capelli G., Bruschi F., Crotti D., Caccio S.M. Genetic heterogeneity at the beta-giardin locus among human and animal isolates of Giardia duodenalis and identification of potentially zoonotic subgenotypes. Int J Parasitol. 2005;35:207-213.
Lambert D. Zero-inflated Poisson Regression, With an Application to Defects in Manufacturing. Technometrics. 1992;34:1-14.
Le Nobel W.E., Robben S.R., Döpfer D., Hendrikx W.M., Boersema J.H., Fransen F., Eysker M. Infections with endoparasites in dogs in Dutch animal shelters. Tijdschr Diergeneeskd. 2004;129:40-4.
Lee A.C.Y., Shantz P.M., Kazacos K.R., Montgomery S.P., Bowman D.D. Epidemiologic and zoonotic aspects of ascarid infection of dogs and cats. Trends Parasitol. 2010;26:155-161.
Leonhard S., Pfister K., Beelitz P., Wielinga C., Thompson R.C.A. The molecular characterization of Giardia from dogs in southern Germany. Vet Parasitol. 2007;150:33-38.
Lucio-Forster A., Griffiths J.K., Cama V.A., Xiao L., Bowman D.D. Minimal zoonotic risk of cryptosporidiosis from pet dogs and cats. Trends Parasitol. 2010;26:174-179.
Macpherson C.N.L. The epidemiology and public health importance of toxocariasis: A zoonosis of global importance. Int J Parasitol. 2013;43:999-1008.
MAFF. 1986. Manual of veterinary parasitology laboratory techniques. Ministry of Agriculture, Fisheries and Food.
Martínez-Carrasco C., Berriatua E., Garijo M., Martínez J., Alonso F.D., de Ybáñez R.R. Epidemiological study of non-systemic parasitism in dogs in southeast Mediterranean Spain assessed by coprological and post-mordem examination. Zoonoses Public Health. 2007;54:195-203.
Martinez-Moreno F.J., Hernandez S., Lopez-Cobos E., Becerra C., Acosta I., Martinez-Moreno A. Estimation of canine intestinal parasites in Cordoba (Spain) and their risk to public health. Vet Parasitol. 2007;143:7-13.
Mateus T.L., Castro A., Ribeiro J.N., Vieira-Pinto M. Multiple zoonotic parasites identified in dog feces collected in Ponte de Lima, Portugal- A potential threat to human health. Int J Environ Res Public Health. 2014;11:9050-9067.
Matos M., Alho A.M., Owen S.P., Nunes T. Parasite control practices and public perception of parasitic diseases: A survey of dog and cat owners. Prev Vet Med. 2015;122:174-80.
Minetti C., Lamden K., Durband C., Cheesbrough J., Fox A., Wastling J.M. Determination of Giardia duodenalis assemblages and multi-locus genotypes in patients with sporadic giardiasis from England. Parasit Vectors. 2015;8:44.
Morgan U.M., Monis P.T., Xiao L., Limor J., Sulaiman I., Raidal S., O’Donoghue P., Gasser R., Murray A., Fayer R., Blagburn B.L., Lal A.A., Thompson R.C. Molecular and phylogenetic characterization of Cryptosporidium from birds. Int J Parasitol. 2001;31:289-296.
Nijsse R., Mughini-Gras L., Wagenaar J.A., Ploeger H.W. Coprophagy in dogs interferes in the diagnosis of parasitic infections by faecal examination. Vet Parasitol. 2014;204:304-309.
Nijsse R., Mughini-Gras L., Wagenaar J.A., Franssen F., Ploeger H.W. Environmental contamination with Toxocara eggs: a quantitative approach to estimate the relative contributions of dogs, cats and foxes, and to assess the efficacy of advised interventions in dogs. Parasit Vectors. 2015;8:397.
Nijsse R., Ploeger H.W., Wagenaar J.A., Mughini-Gras L. Prevalence and risk factors for patent Toxocara infections in cats and cat owners’ attitude towards deworming. Parasitol Res. 2016;115:4519-4525.
Ortuno A and Castella J. Intestinal Parasites in Shelter Dogs and Risk Factors Associated with the Facility and its Management. Isr J Vet Med. 2011;66:103-107.
Ortuno A., Scorza V., Castella J., Lappin M. Prevalence of intestinal parasites in shelter and hunting dogs in Catalonia, Northeastern Spain. The Vet J. 2014;199:465-467.
113
Osman M., Bories J., El Safadi D., Poirel M., Gantois N., Benamrouz-Vanneste S., Delhaes L., Huggonard M., Certad G., Zenner L., Viscogliosi E. Prevalence and genetic diversity of the intestinal parasites Blastocystis sp. and Cryptosporidium spp. in household dogs in France and evaluation of zoonotic transmission risk. Vet Parasitol. 2015;214:167-170.
Otranto and Eberhard. Zoonotic helminths affecting the human eye. Parasit Vectors. 2011;4:41. Overgaauw P.A. Aspects of Toxocara epidemiology: human toxocarosis. Crit Rev Microbiol.
1997;23:215-31. Overgaauw P.A.M., van Zutphen L., Hoek D., Yaya F.O., Roelfsema J., Pinelli E., van Knapen F.,
Kortbeek L.M. Zoonotic parasites in fecal samples and fur from dogs and cats in the Netherlands. Vet Parasitol. 2009;163: 115-122.
Pallant L., Barutzki D., Schaper R., Thompson R.C.A. The epidemiology of infections with Giardia species and genotypes in well cared for dogs and cats in Germany. Parasit Vectors. 2015;8:2.
Palmer C.S., Thompson R.C.A., Traub R.J., Rees R., Robertson I.D. National study of the gastrointestinal parasites of dogs and cats in Australia. Vet Par. 2008;151:181-190.
Papazahariadou M., Founta A., Papadopoulos E., Chliounakis S., Antoniadou-Sotiriadou K., Theodorides Y. Gastrointestinal parasites of shepherd and hunting dogs in the Serres Prefecture, Northern Greece. Vet Parasitol. 2007;148:170-173.
Parsons J.C. Ascarid infections of cats and dogs. Vet Clin North Small Anim Pract. 1987;17:1307-39.
Pereira A., Martins A., Brancal H., Vilhena H., Silva P., Pimenta P., Diz-Lopes D., Neves N., Coimbra M., Alves A.C., Cardoso L., Maia C. Parasitic zoonoses associated with dogs and cats: a survey of Portuguese pet owners’ awareness and deworming practices. Parasit Vectors. 2016;9:245.
Polak K.C., Levy J.K., Crawford P.C., Leutenegger C.M., Moriello K.A. Infectious diseases in large-scale cat hoarding investigations. The Vet J. 2014;201:189-195.
R Core Team. R: A language and environment for statistical computing. 2013. R Foundation for Statistical Computing, Vienna, Austria.
Read C.M., Monis P.T., Thompson R.C. Discrimination of all genotypes of Giardia duodenalis at the glutamate dehydrogenase locus using PCR-RFLP. Infect Genet Evol. 2004;4:125-30.
Riggio F., Mannella R., Ariti G., Perrucci S. Intestinal and lung parasites in owned dogs and cats from Central Italy. Vet Parasitol. 2013;193:78-84.
Rinaldi L., Coles G.C., Maurelli M.P., Musella V., Cringoli G. Calibration and diagnostic accuracy of simple flotation, McMaster and Flotac for parasite egg counts in sheep. Vet Parasitol. 2011;177:345-352.
Ryan U., Fayer R., Xiao L. Cryptosporidium species in humans and animals: current understanding and research needs. Parasitology. 2014;11:1-19.
Scaramozzino P., Di Cave D., Berrilli F., D’Orazi C.D., Spaziani A., Mazzanti S., Scholl F., De Liberato C.D. A study of the prevalence and genotypes of Giardia duodenalis infecting kenneled dogs. Vet J. 2009;182:231-234.
Scorza A.V., Ballweber L.R., Tangtrongsup S., Panuska C., Lappin M.R. Comparisons of mammalian Giardia duodenalis assemblages based on the β-giardin, glutamate dehydrogenase and triose phosphate isomerase genes. Vet Parasitol. 2012;189:182-188.
Simonato G., Frangipane di Regalbono A., Cassini R., Traversa D., Beraldo P., Tessarin C., Pietrobelli M. Copromicroscopic and molecular investigations on intestinal parasites in kenneled dogs. Parasitol Res. 2015;114:1963-1970.
Smith H., Noordin R. 2006. Diagnostic limitations and future trends in the serodiagnosis of human toxocariasis. In: Holland, C.V., Smith, H.V. (Eds.), Toxocara: The Enigmatic Parasite. CABI Publishing, CAB International, Wallingford, Oxfordshire, UK, pp. 89–112.
Sotiraki S., Chaligiannis I. Cystic echinococcosis in Greece. Parasite. 2010;17:205-10.
114
Souza S.L., Gennari S.M., Richtzenhain L.J., Pena H.F., Funada M.R., Cortez A., Gregori F., Soares R.M. Molecular identification of Giardia duodenalis isolates from humans, dogs, cats and cattle from the state of Sao Paulo, Brazil, by sequence analysis of fragments of glutamate dehydrogenase (gdh) coding gene. Vet Parasitol. 2007;149:258-264.
Sulaiman I.M., Fayer R., Bern C., Gilman R.H., Trout J.M., Schantz P.M., Das P., Lal A.A., Xiao L. Triosephospate isomerase gene characterization and potential zoonotic transmission of Giardia duodenalis. Emerg Infect Dis. 2003;9:1444-1452.
Sutherst R.W. Global change and human vulnerability to vector-borne diseases. Clin Microbiol Rev. 2004;17:136-73.
Tabachnick W.J. Challenges in predicting climate and environmental effects on vector-borne disease episystems in a changing world. J Exp Biol. 2010;213:946-54.
Theodoridis I., Frydas S., Papazahariadou M., Hatzistilianou M., Adamama-Moraitou K.K., Di Gioacchino M., Felaco M. Toxocarosis as zoonosis. A review of literature and the prevalence of Toxocara canis antibodies in 511 serum samples. Int J Immunopathol Pharmacol. 2001;14:17-23.
Thompson R.C., Palmer C.S., O’Handley R. The public health and clinical significance of Giardia and Cryptosporidium in domestic animals. Vet J. 2008;177;18-25.
Thompson R.C.A., Smith A. Zoonotic enteric protozoa. Vet Parasitol. 2011;182:70-78. Traversa D. Pet roundworms and hookworms: A continuing need for global worming. Parasit
Vectors. 2012;5:91. Villeneuve A., Polley L., Jenkins E., Schurer J., Gilleard J., Kutz S., Conboy G., Benoit D., Seewald
W., Gagne F. Parasite prevalence in fecal samples from shelter dogs and cats across the Canadian provinces. Parasit Vectors. 2015;8:281.
Wang X.T., Wang R.J., Ren G.J., Yu Z.Q., Zhang L.X., Zhang S.Y., Lu H., Peng X.Q., Zhao G.H. Multilocus genotyping of Giardia duodenalis and Enterocytozoon bieneusi in dairy and native beef (Qinchuan) calves in Shaanxi province, northwestern China. Parasitol Res. 2016;115:1355-61.
Xiao L., Singh A., Limor J., Graczyk T.K., Gradus S., Lal A.A. Molecular characterization of Cryptosporidium oocysts in samples of raw surface water and wastewater. Appl Environ Microbiol. 2001;6:1097-1101.
Xiao L., Cama V.A., Cabrera L., Ortega Y., Pearson J., Gilman R.H. Possible transmission of Cryptosporidium canis among children and a dog in a household. J Clin Microbiol. 2007;45:2014-2016.
Xiao L., Fayer R. Molecular characterisation of species and genotypes of Cryptosporidium and Giardia and assessment of zoonotic transmission. Int J Parasitol. 2008;38:1239–1255.
Xinou E., Lefkopoulos A., Gelagoti M., Drevelegas A., Diakou A., Milonas I., Dimitriadis A.S. CT and MR imaging findings in cerebral toxocaral disease. Am J Neuroradiol. 2003;24:714-8.
Zanzani S.A., Gazzonis A.L., Scarpa P., Berrilli F., Manfredi M.T. Intestinal parasites of owned dogs and cats from metropolitan and micropolitan areas: Prevalence, zoonotic risks, and pet owner awareness in nothern Italy. BioMed Res Int. 2014;2014:696508.
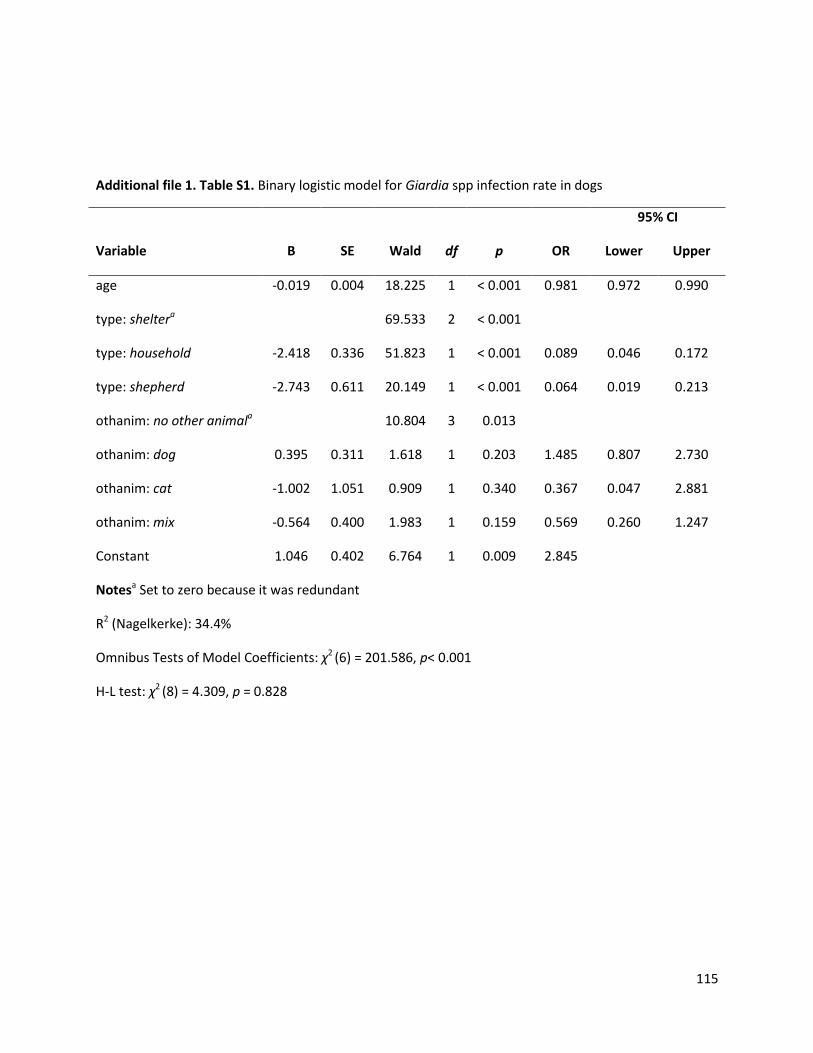
115
Additional file 1. Table S1. Binary logistic model for Giardia spp infection rate in dogs
Variable B SE Wald df p OR
95% CI
Lower Upper
age -0.019 0.004 18.225 1 < 0.001 0.981 0.972 0.990
type: sheltera
69.533 2 < 0.001
type: household -2.418 0.336 51.823 1 < 0.001 0.089 0.046 0.172
type: shepherd -2.743 0.611 20.149 1 < 0.001 0.064 0.019 0.213
othanim: no other animala
10.804 3 0.013
othanim: dog 0.395 0.311 1.618 1 0.203 1.485 0.807 2.730
othanim: cat -1.002 1.051 0.909 1 0.340 0.367 0.047 2.881
othanim: mix -0.564 0.400 1.983 1 0.159 0.569 0.260 1.247
Constant 1.046 0.402 6.764 1 0.009 2.845
Notesa Set to zero because it was redundant
R2 (Nagelkerke): 34.4%
Omnibus Tests of Model Coefficients: χ2 (6) = 201.586, p< 0.001
H-L test: χ2 (8) = 4.309, p = 0.828
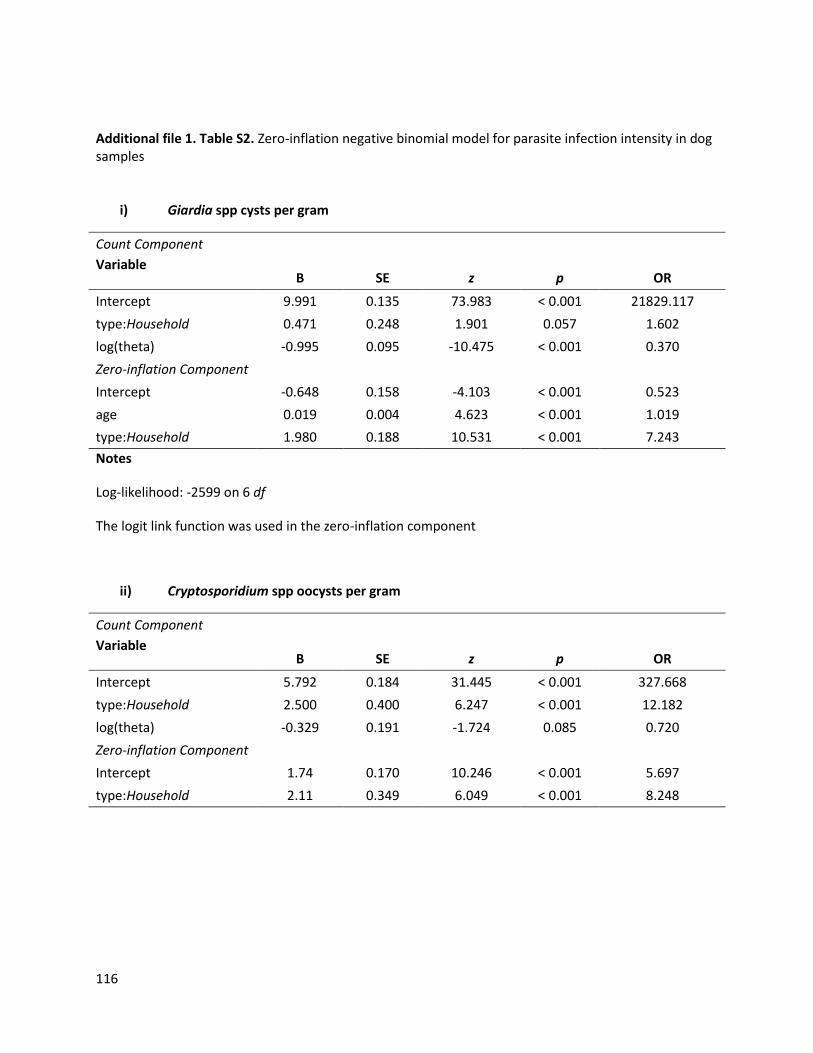
116
Additional file 1. Table S2. Zero-inflation negative binomial model for parasite infection intensity in dog samples
i) Giardia spp cysts per gram
Count Component
Variable B SE z p OR
Intercept 9.991 0.135 73.983 < 0.001 21829.117
type:Household 0.471 0.248 1.901 0.057 1.602
log(theta) -0.995 0.095 -10.475 < 0.001 0.370
Zero-inflation Component
Intercept -0.648 0.158 -4.103 < 0.001 0.523
age 0.019 0.004 4.623 < 0.001 1.019
type:Household 1.980 0.188 10.531 < 0.001 7.243
Notes
Log-likelihood: -2599 on 6 df
The logit link function was used in the zero-inflation component
ii) Cryptosporidium spp oocysts per gram
Count Component
Variable B SE z p OR
Intercept 5.792 0.184 31.445 < 0.001 327.668
type:Household 2.500 0.400 6.247 < 0.001 12.182
log(theta) -0.329 0.191 -1.724 0.085 0.720
Zero-inflation Component
Intercept 1.74 0.170 10.246 < 0.001 5.697
type:Household 2.11 0.349 6.049 < 0.001 8.248
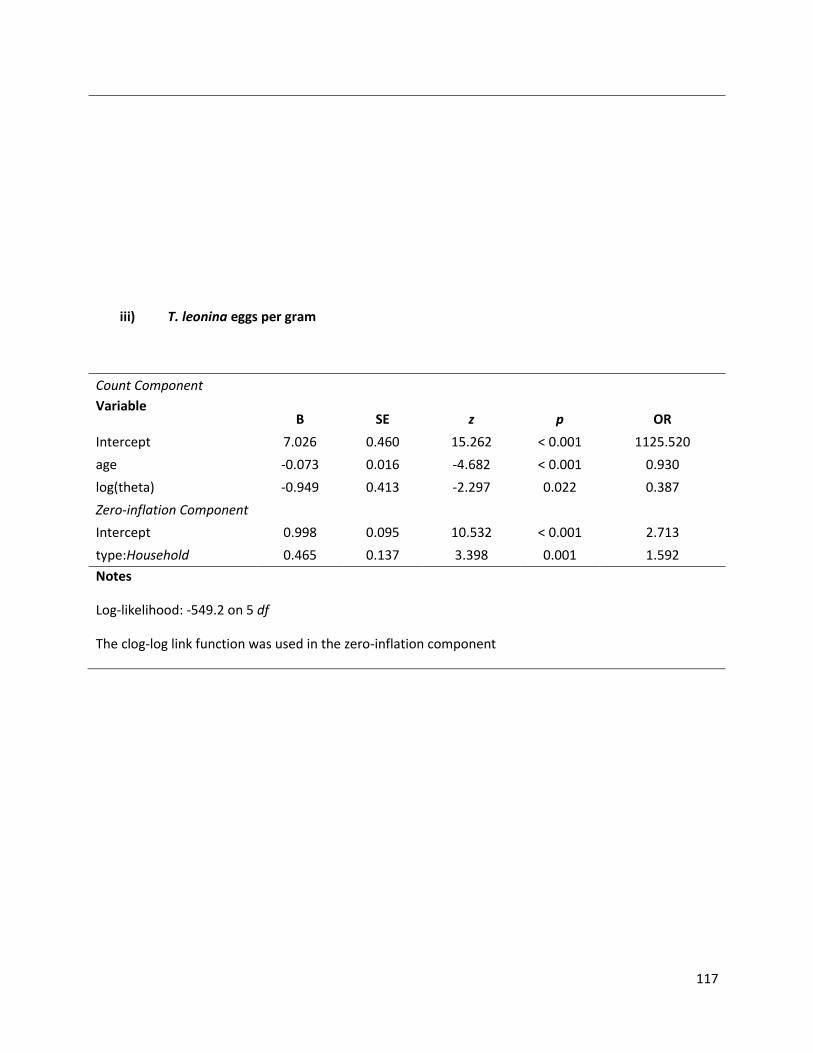
117
iii) T. leonina eggs per gram
Count Component
Variable B SE z p OR
Intercept 7.026 0.460 15.262 < 0.001 1125.520
age -0.073 0.016 -4.682 < 0.001 0.930
log(theta) -0.949 0.413 -2.297 0.022 0.387
Zero-inflation Component
Intercept 0.998 0.095 10.532 < 0.001 2.713
type:Household 0.465 0.137 3.398 0.001 1.592
Notes
Log-likelihood: -549.2 on 5 df
The clog-log link function was used in the zero-inflation component

Chapter IV
Based on:
Human enteric infections by parasites in Greece, with focus on Giardia
and Cryptosporidium
D. Kostopoulou, E. Claerebout, D. Arvanitis, P. Ligda, S. Casaert, S. Sotiraki
Submitted in Hippokratia Medical Journal

120
Introduction
Pieces of evidence of the presence of parasites in humans have been recorded even in prehistoric times.
Through history, people have been infected with a variety of parasitic species and in different intensity,
depending on the lifestyle during each time period (Mitchell, 2015). In the modern world, parasites are
most abundant in developing countries, but are also present in developed communities, having
significant consequences on public health and the economy. According to World Health Organization
estimates, foodborne parasitic diseases resulted in 48.4 million cases and 59,724 deaths annually
resulting in 8.78 million Disability Adjusted Life Years (DALYs), from 2010 to 2015 globally (Torgerson et
al., 2015).
Poor hygiene and sanitation conditions and exposure to animals are factors thought to affect parasite
transmission (Fletcher et al., 2012). This may be explained a) by the fact that parasite life cycles often
involve several hosts like people, animals, vectors, and transmission routes like food, water, surfaces, air
and b) by the ability of parasite’s life stages to survive adverse environmental conditions. Research
interest in health issues shared among people, animals and the environment has increased rapidly in
recent years, as emerging zoonotic infections like giardiosis and cryptosporidiosis have been recognized
as a global public health concern being responsible for several outbreaks worldwide. Cryptosporidium is
being considered as the leading agent of waterborne disease outbreaks in the United States (Painter et
al., 2016) and Europe (Efstratiou et al., 2017), causing high rates of morbidity and even mortality in
children or immunocompromised individuals. Infection by Giardia duodenalis on the other hand has
been responsible for a significant number of outbreaks within the US (Adam et al., 2016) and Europe
(Hadjichristodoulou et al., 1998; Braeye et al., 2015; Enserik et al., 2015; Guzman-Herrador et al. 2015).
Although several studies on parasitic infections in Greece have been published, most of these papers are
case reports and/or refer to a single parasite species (Kouklakis et al., 2007; Vassalos et al., 2009; Panidis
et al., 2011; Arkoulis et al., 2012; Gialamas et al., 2012; Printza et al., 2013; Mentessidou et al., 2016;
Patsantara et al., 2016). Available information referring to gastrointestinal parasitic infection rates is
limited (Papazahariadou et al., 2004), stressing the need for updated information on parasite
abundance.
Data on the abundance of intestinal parasites is considered critical for public health protection, showing
more than local interest, since Greece is an important first country of arrival in Europe for migrants and

121
asylum seekers, serving as a transit country in the migratory journey to Northern Europe and large
numbers of tourists visit Greece annually from all over the world.
The aim of this study was to update and compile the current knowledge on the abundance of intestinal
parasites in Greece in order to provide useful estimates for surveillance and control activities as well as
to advance the knowledge of the zoonotic relevance of Giardia and Cryptosporidium species, since they
are among the most commonly detected pathogens associated with diarrhoea in humans (Baldursson
and Karanis, 2011).
The data presented in this paper are a component of a larger coordinated endeavour undertaken by the
authors to study the occurrence of Giardia and Cryptosporidium in humans (current study) as well as in
livestock and companion animals (Tzanidakis et al., 2014; Kostopoulou et al., 2015; Kostopoulou et al.,
2017), in an effort to uncover parasite transmission pathways and provide clues for holistic parasite
control strategies, in a ‘One Health’ approach. The latter also justifies the stronger focus given in the
sample analyses for those parasites.
Materials and Methods
Stool samples were randomly collected from humans [children (<18 years old) and adults] in selected
areas in Greece, i.e. the Regions of West Macedonia, Central Macedonia and East Macedonia and Thrace
(referred to as Northern Greece and neighbouring the Balkans) and Region of Crete in the south
(neighbouring the Middle East and North Africa) over a period of almost 3 years. Samples were collected
from a State General Hospital and 2 private practitioners located in Northern Greece and 1 State
General Hospital, 4 Private Clinics and 10 private practitioners in Crete.
After collection, the samples were immediately transported under vacuum to the laboratory, where
they were stored at 4 °C and examined within 2 days.
The study was carried out in compliance with the National and Institutional ethical regulations. For every
individual, a data-form was completed after their consent or in case of children after the consent of
their parents, providing information on age, sex, reason of consulting a doctor, absence or presence of
gastrointestinal symptoms and specification of the symptoms, general health status (focusing on
possible immunodeficiency signs), any recent contact with animals and which species and travel history.
122
Parasitological techniques
Faecal consistency was recorded for all stool samples. The consistency of individual faecal samples was
scored using the following scale: 1=formed; 2=soft; 3=diarrhoea; 4=haemorrhagic diarrhoea.
The presence of worm eggs and protozoal (oo)cysts was determined by applying 2 different
concentration methods, i.e. a sedimentation (acid/ether) and a sedimentation/flotation technique
(using a saturated sugar salt solution as a flotation fluid with 1.28 specific gravity) (MAFF, 1986). For the
detection of Giardia spp and Cryptosporidium spp (oo)cysts, a quantitative direct immunofluorescence
assay (IFA) based on the commercial MERIFLUOR Cryptosporidium/Giardia kit (Meridian Diagnostics Inc.,
Cincinnati, Ohio) was used (Panidis et al., 2011).
Statistical analysis
Statistical analysis was performed using SPSS ver. 21.0. Binary and/or ordinal logistic regression analyses
were used to estimate the effects of parasitism and parasitic burden on the occurrence and severity of
diarrhoea and to investigate correlations between risk factors and parasitism. Values of P < 0.05 were
considered significant.
Molecular analyses
DNA was extracted from the positive Giardia spp and Cryptosporidium spp stool samples using the
QIAamp® Stool Mini Kit (Qiagen) according to the manufacturer’s instructions. For the amplification of
the Cryptosporidium 18S ribosomal DNA gene (18S rDNA) and HSP70 gene, previously described PCR
protocols were used (Kostopoulou et al., 2017).For the identification of Giardia DNA, the Giardia 18S
ribosomal DNA gene (18S rDNA), the β-giardin gene the triose phosphate isomerase (TPI) gene and the
glutamate dehydrogenase (GDH) gene were used (Kostopoulou et al., 2017). Amplification products
were visualized on 1.5% agarose gels with ethidium bromide. A positive (genomic DNA from a positive
faecal sample) and negative (PCR water) control sample were included in each PCR reaction.
PCR products were purified and sequenced from both strands. PCR products were purified using the
Qiaquick PCR purification kit (Qiagen) and fully sequenced by an external company (GATC Biotech) using
the Big dye Terminator V3.1 Cycle sequencing Kit (Applied Biosystems) whereas the reactions were
analysed using a 3730xl DNA Analyzer (ThermoFisher Scientific). Sequences were assembled using
123
Seqman 5.0 Software (Lasergene DNASTAR) and aligned using the Basic Local Alignment Search Tool
(BLAST) as well as compared with reference sequences using MegAlign (Lasergene DNASTAR). For
multilocus genotyping Clustal X, 2.0.11 Software was used using reference sequences according to
Caccio et al., 2008 (Caccio et al., 2008).
Results
Overall, 876 stool samples were collected in Greece. Specifically, the samples were originated from 822
adults and 54 children from Northern Greece (n=436) and Crete region (n=440), and in total samples
coming from males (n=586) were twice the number of the ones from females (n=290). Among the
sampled adults 156 had a record of gastrointestinal symptoms, but the majority (n=666) did not have
any clinical sign. The healthy adults were mostly professionals in the food sector obliged by the Greek
State to undergo regular parasitological stool examinations, in order to acquire a health certificate. Of
the children examined, 20 had a recent history of clinical signs from the gastrointestinal tract.
Thirty-six (4.1%) of the individuals examined harboured at least one intestinal parasite, 3 were children
and the other 33 were adults. In particular, 33 (3.8%) were found positive for protozoa. The protozoa
recorded were Blastocystis hominis (1.8%), Giardia duodenalis (1.3%), Cryptosporidium spp (0.6%),
Entamoeba coli (0.2%) and Entamoeba spp (0.1%). Among the above infections, the following co-
infections were detected: two cases of G. duodenalis and Cryptosporidium spp co-existence, one case of
G. duodenalis and B. hominis and one of E. coli plus Entamoeba spp. Four people (0.5%) were infected
with helminths, 2 of which were positive for Enterobius vermicularis, 1 for Taenia sp and 1 for
hookworms.
Of the individuals examined, 20.0% (n=175) displayed gastrointestinal symptoms according to the
questionnaire. Of them, 8.0% (n=14) were positive for parasites. No significant correlation was observed
between gastrointestinal symptoms and parasite infection (P > 0.05). However, for some parasites, most
infected people did show clinical disease. Both patients with enterobiosis, aged 9 and 15 years, suffered
from abdominal pain. Five people were infected with Cryptosporidium spp, two of whom were also
positive for G. duodenalis. One of the Cryptosporidium infected who had symptoms of severe diarrhoea
was immune-suppressed since he had recently undergone kidney transplantation. No significant
correlation was observed between Cryptosporidium infection levels and diarrhoea (P > 0.05). Five out of
124
11 (45.5%) G. duodenalis positive individuals displayed gastrointestinal symptoms. Three of them, all
adults, had diarrhoea, whereas a 9-year-old boy, also co-infected with Cryptosporidium spp, complained
about abdominal pain. No significant correlation was observed between G. duodenalis cyst counts and
diarrhoea (P > 0.05). Details about G. duodenalis and Cryptosporidium spp infections are presented in
Table 1.
Most of the Blastocystis infected people were asymptomatic, except for a 9 year-old girl who had a
history of eosinophilia in a blood examination a week before the faecal sample was taken.
A patient infected with both Entamoeba spp and E. coli had severe diarrhoea which did not respond to
antibiotics treatment. People infected with E. coli alone, taeniid and hookworm eggs did not report any
gastrointestinal symptoms.
No association between parasitism and age, occupation or pet ownership was found (P > 0.05).
Genotyping results
Seven G. duodenalis positive samples were successfully genotyped. Sequencing results are presented in
Table 2. Multilocus genotyping was performed for two samples which were classified as sub-
assemblages AII using 3 genetic loci (bg, TPIGEN and GDH). Alignment analysis of the isolates showed
100% homology when compared to reference sequences A2 for bg and A2 for TPIGEN ,however, there
was one SNP at the gdh locus (a “T” instead of a “C” in position 237), resulting in a new MLG. As for
Cryptosporidium, the HSP70 gene was amplified for one sample, however sequencing was not
successful.
Discussion
Intestinal parasitic infections are distributed throughout the world; however, their prevalence differs
from region to region due to different environmental, social and geographical factors. The results of the
current study confirmed the presence of different intestinal parasitic species in humans in Greece,
though in low abundance, which is more or less expected in developed countries where hygiene and
sanitation standards are high. The prevalence of intestinal parasites in humans in Greece has been
evaluated previously showing infection in 11.4% (Papazahariadou et al., 2004) of the studied population.
125
Of the parasitic infections detected, protozoans (3.8%) were more common than helminths (0.5%). This
has been also reported before in other studies worldwide (Dagnew et al., 2012; Colli et al., 2014; Kiani et
al., 2016), including Greece (Papazahariadou et al., 2004).
Blastocystis hominis (1.8%) was the most common parasite found which is in line with other studies
(Masucci et al., 2011). Our findings were closer to the lower level (1.8%), possibly due to the fact that
80.0% of the people who participated in the study were clinically healthy, which is in accordance with
previous findings in Greece (Vassalos et al., 2009; Papazahariadou et al., 2004).
G. duodenalis was the second most common parasite (1.3%). This result is in line with other European
studies where however, the prevalence of Giardia infection varies depending on the study population
and the diagnostic techniques used (Okulewicz et al., 1998; Werner et al., 2001; Crotti et al., 2005;
Giangaspero et al., 2007; Davies et al., 2009; Sagebiel et al., 2009). In Northern Greece, an infection rate
of 2.3% was previously reported (Papazahariadou et al., 2004). Giardiosis was previously confirmed in
0.5% (Kafetzis et al., 2001) and 3.0% (Maltezou et al., 2001) of children with acute diarrhoea in Greece.
Although there was also an obvious trend towards the presence of diarrhoea in Giardia infected
individuals in the present study, the number of Giardia cysts in faeces was not significantly different
between healthy individuals harbouring the parasite and individuals with diarrhoea. Asymptomatic
carriers having high parasitic burden is not an unusual finding (Feng and Xiao, 2011). Travel history and
close contact with animals (pets/farm animals) were not associated with infection in this study. All
Giardia positive samples were identified as sub-assemblage AII, which predominantly infects humans
(Feng and Xiao, 2011). Although sub-assemblage AII can also be found in different animal species, it is
predominantly found in humans (Sprong et al., 2009). Moreover, previous studies in Greece indicated
that mainly assemblage E is present in ruminants (Tzanidakis et al., 2014) sub-assemblages AI and BIV-
like in horses (Kostopoulou et al., 2015) assemblage C and D in dogs and assemblage F in cats
(Kostopoulou et al., 2017), which suggests that human-to-human transmission of Giardia was more
likely to be the source of infection in the present study. Similar conclusions (as regards travel and
contact with animals) were also reported from a previous study in Germany referring to symptomatic
patients (Espelage et al., 2010), whereas travel was characterized as a risk factor for giardiosis in
returning UK travelers but only returning from long trips from South/South East Asia and Africa (Takaoka
et al., 2016).
Cryptosporidium spp were found in 0.6% of the samples. In Greece, Cryptosporidium was detected
before in 2.7% of the study population (Papazahariadou et al., 2004) and was also implicated together
126
with Giardia, in an outbreak of diarrhoea in Crete (Hadjichristodoulou et al., 1998). Besides, a few case
reports of cryptosporidiosis have been published in Greece (Printza et al., 2013; Megremis et al., 2004).
The results of the current study showed an evident clinical appearance in the majority of
Cryptosporidium infected cases.
Only two individuals (0.2%) were found harbouring pinworm eggs and both of them were children. A
low infection rate for E. vermicularis could be due to the fact that the worm’s eggs are sticky and adhere
to the perianal skin or clothing so that only few of them pass to the faeces and consequently are not
recorded in coproscopic analysis. In Greece, 1.1% of the population was found infected (Papazahariadou
et al., 2004) while in another study, a prevalence of 48.8% in children was found using haematological
and serological parameters (Patsantara et al., 2016). Most studies regarding E. vermicularis in Greece
are case reports where the parasite is commonly associated with acute appendicitis and less often with
other pathological or clinical findings (Kollias et al., 1992; Batistatou et al., 2002; Tsibouris et al., 2005;
Kouklakis et al., 2007; Zahariou et al., 2007; Panidis et al., 2011; Arkoulis et al., 2012; Gialamas et al.,
2012; Mentessidou et al., 2016). Similarly, in our study, both infected children suffered from abdominal
pain.
Taeniid and Hookworm eggs were detected once each in stool samples from an immigrant from India
and a native woman, both originating from Crete. As regards human hookworm infection, there are no
data recording such infection in Greece whereas human taeniosis has been previously reported although
only in sporadic cases due to Taenia saginata infection (Papazahariadou et al., 2004; Paterakis et al.,
2007; Papageorgiou et al., 2009). Unfortunately, in the present case we did not succeed to characterise
the species of the parasite.
Conclusions
Overall, the results of the current study indicate that there is not an increased infection rate of
parasitism compared to previous published data. Since in the current study participants consisted mainly
of healthy adults, the real prevalence of intestinal parasitism in Greece was maybe underestimated.
Although the results cannot be extrapolated to the general population in Greece, they suggest that
increased migration and tourism had no major impact on parasitism in the studied areas. Besides, in the
majority of the cases, both parasitism and symptoms were not related to travel but acquired
indigenously and individuals were just visiting a doctor as part of a routine health screen. The above
127
confirms the status of Greece as a “low-risk” country concerning intestinal parasitic infections
(http://www.who.int/ith).
There were no indications of significant zoonotic parasite transmission. Specifically referring to Giardia
infections, genotyping results demonstrated the dominance of sub-assemblage AII in infected
individuals, indicating a human to human transmission cycle. A novel multi-locus genotype was
identified, which has not been described in humans or animals previously.
The absence of a significant association between parasitism and clinical disease was probably due to the
low number of positive samples. However, we should not underrate the clinical importance of such
infections, given the high proportion of gastrointestinal signs for some parasitic infections, such as
Giardia (36% diarrhoea in infected people), Cryptosporidium (80% diarrhoea) and pinworms (100%
abdominal pain).
Aknowledgements
The authors would like to thank the Hellenic Scholarship Foundation for supporting Mrs. Kostopoulou
thesis. We would also like to thank all the medical doctors who participated in the study as well as Dr A.
Gelasaki, Mr. N. Voutzouraki, Mrs. K. Saratsi and Mrs K. Antoniadou who contributed to the completion
of this work.
Funding
This work is a part of a PhD scholarship funded by the Greek State Scholarships Foundation.
Authors’ contributions
This study was conducted by DK as part of her PhD thesis. Also, DK participated in the data collection
and analysis and developed first draft manuscript. All other authors played a role in data collection and
analysis and interpretation of findings (EC, DA, PL, CS, SS). All authors read and approved the final
manuscript.
Competing interests
The authors declare that they have no competing interests.
128
Consent for publication
Not applicable.
Ethical considerations
This study was carried out in compliance with the National and Institutional ethical regulations.
129
References
Adam E.A., Yoder J.S., Gould L.H., Hlavsa M.C., Gargano J.W. Giardiasis outbreaks in the United States, 1971-2011. Epidemiol Infect. 2016;144:2790-2801.
Arkoulis N., Zerbinis H., Simatos G., Nisiotis A. Enterobius vermicularis (pinworm) infection of the liver mimicking malignancy: Presentation of a new case and review of current literature. Int J Surg Case Rep. 2012;3:6-9.
Baldursson S., Karanis P. Waterborne transmission of protozoan parasites: review of worldwide outbreaks—an update 2004–2010. Water Res. 2011;45:6603–6614.
Batistatou A., Zolota V., Scopa C.D. Images in pathology: Oxyuris (enterobius) vermicularis in human cecum and appendix. Int J Surg Pathol. 2002;10:58.
Braeye T., De Schrijver K., Wollants E., van Ranst M., Verhaegen J.. A large community outbreak of gastroenteritis associated with consumption of drinking water contaminated by river water, Belgium, 2010. Epidemiol Infect. 2015; 143:711-719.
Caccio S.M., Beck R., Lalle M., Marinculic A., Pozio E. Multilocus genotyping of Giardia duodenalis reveals striking differences between assemblages A and B. Int J Parasitol. 2008;38:1523-1531.
Colli C.M., Mizutani A.S., Martins V.A., Ferreira E.C., Gomes M.L. Prevalence and risk factors for intestinal parasites in food handlers, southern Brazil. Int J Environ Health Res. 2014;24:450-458.
Crotti D., D’ Annibale M.L., Fonzo G., Lalle M., Caccio S.M., Pozio E. Dientamoeba fragilis is more prevalent than Giardia duodenalis in children and adults attending a day care centre in Central Italy. Parasite. 2005;12:165-170.
Dagnew M., Tiruneh M., Moges F., Tekeste Z. Survey of nasal carriage of Staphylococcus aureus and intestinal parasites among food handlers working at Gondar University, Northwest Ethiopia. BMC Public Health. 2012;12:837.
Davies A.P., Campbell B., Evans M.R., Bone A., Roche A., Chalmers R.M. Asymptomatic carriage of protozoan parasites in children in day care centers in the United Kingdom. Pediatr Infect Dis J. 2009;28:838-840.
Efstratiou A., Ongerth J.E., Karanis P. Waterborne transmission of protozoan parasites: Review of worldwide outbreaks - An update 2011-2016. Water Res. 2017;114:14-22.
Enserink R., van den Wijngaard C., Bruijning-Verhagen P., van Asten L., Mughini-Gras L., Duizer E., Kortbeek T., Scholts R., Nagelkerke N., Smith H.A., Kooistra-Smid M., van Pelt W. Gastroenteritis attributable to 16 enteropathogens in children attending day care: significant effects of rotavirus, norovirus, astrovirus, Cryptosporidium and Giardia. Pediatric Infect Dis J. 2015;34:5-10.
Espelage W., an der Heiden M., Stark K., Alpers K. Characteristics and risk factors for symptomatic Giardia lamblia infections in Germany. BMC Public Health. 2010;10:41.
Feng Y., Xiao L. Zoonotic potential and molecular epidemiology of Giardia species and giardiasis. Clin Microbiol Rev. 2011;24:110-140.
Fletcher S.M., Stark D., Harkness J., Ellis J. Enteric protozoa in the developed world: a public health perspective. Clin Microbiol Rev. 2012;25:420–449.
130
Gialamas E., Papavramidis T., Michalopoulos N., Karayannopoulou G., Cheva A., Vasilaki O., Kesisoglou I., Papavramidis S. Enterobius vermicularis: a rare cause of appendicitis. Turkiye Parazitol Derg. 2012;36:37-40.
Giangaspero A., Berrilli F., Brandonisio O. Giardia and Cryptosporidium and public health: the epidemiological scenario from the Italian perspective. Parasitol Res. 2007;101:1169-1182.
Guzman-Herrador B., Carlander A., Ethelberg S., Freiesleben de Blasio B., Kuusi M., Lund V., Löfdahl M., MacDonald E., Nichols G., Schönning C., Sudre B., Trönnberg L., Vold L., Semenza J.C., Nygård K.Waterborne outbreaks in the Nordic countries, 1998 to 2012. Euro Surveill. 2015;18:20.
Hadjichristodoulou C., Gkikas A., Pediatidis Y., Tselentis Y. Outbreak of giardiasis among English tourists in Crete. Lancet. 1998;351:65-66.
Kafetzis D.A., Maltezou H.C., Zafeiropoulou A., Attilakos A., Stavrinadis C., Foustoukou M. Epidemiology, clinical course and impact on hospitalization costs of acute diarrhea among hospitalized children in Athens, Greece. Scand J Infect Dis. 2001;33:681-685.
Kiani H., Haghighi A., Rostami A., Azargashb E., Seyyed Tabaei S.J., Solgi A., Zebardast N. Prevalence, risk factors and symptoms associated to intestinal parasite infections among patients with gastrointestinal disorders in Nahavand, Western Iran. Rev Inst Med Trop Sao Paulo. 2016;58:42.
Kollias G., Kyriakopoulos M., Tiniakos G. Epididymitis from Enterobius vermicularis: case report. J Urol. 1992;147:1114-1116.
Kostopoulou D., Casaert S., Tzanidakis N., van Doorn D., Demeler J., von Samson-Himmelstjerna G., Saratsis A., Voutzourakis N., Ehsan A., Doornaert T., Looijen M., De Wilde N., Sotiraki S., Claerebout E., Geurden T. The occurrence and genetic characterization of Cryptosporidium and Giardia species in foals in Belgium, The Netherlands, Germany and Greece. Vet Parasitol. 2015;211:170-174.
Kostopoulou D., Claerebout E., Arvanitis D., Ligda P., Voutzourakis N., Casaert S., Sotiraki S. Abundance, zoonotic potential and risk factors of intestinal parasitism amongst dog and cat populations: The scenario of Crete, Greece. Parasit Vectors. 2017;10:43.
Kouklakis G., Mpoumponaris A., Moschos J., Koulaouzidis A., Bhat S., Efremidou E., Lyratzopoulos N. An unusual complication of a usually 'innocent' parasitic worm. Dig Surg. 2007;24:177-178.
MAFF. Manual of veterinary parasitology laboratory techniques. Ministry of Agriculture, Fisheries and Food;1986.
Maltezou H.C., Zafiropoulou A., Mavrikou M., Bozavoutoglou E., Liapi G., Foustoukou M., Kafetzis D.A. Acute diarrhoea in children treated in an outpatient setting in Athens, Greece. J Infect. 2001;43:122-7.
Masucci L., Graffeo R., Bani S., Bugli F., Boccia S., Nicolotti N., Fiori B., Fadda G., Spanu T. Intestinal parasites isolated in a large teaching hospital, Italy, 1 May 2006 to 31 December 2008. Euro Surveill. 2011;16:24.
Megremis S., Segkos N., Daskalaki M., Tzortzakakis E., Paspatis G., Zois E., Sfakianaki E. Gall bladder cryptosporidiosis in a patient with acquired immunodeficiency syndrome: sonographic evaluation of the disease's course. J Ultrasound Med. 2004;23:137-140.
Mentessidou A., Theocharides C., Patoulias I., Panteli C. Enterobius vermicularis-Associated Pelvic Inflammatory Disease in a Child. J Pediatr Adolesc Gynecol. 2016;29:e25-7.
131
Mitchell P.D. Human parasites in Medieval Europe: Lifestyle, Sanitation and Medical Treatment. Adv Parasitol. 2015;90:389-420.
Okulewicz J., Lucinska A., Galary E. Occurrence of Giardia intestinalis in hospitalized children and in children from orphanages. Ann Parasitol. 1998;44:322.
Painter J.E., Gargano J.W., Yoder J.S., Collier S.A., Hlavsa M.C. Evolving epidemiology of reported cryptosporidiosis cases in the United States, 1995-2012. Epidemiol Infect. 2016;144:1792-1802.
Panidis S., Paramythiotis D., Panagiotou D., Batsis G., Salonikidis S., Kaloutsi V., Michalopoulos A. Acute appendicitis secondary to Enterobius vermicularis infection in a middle-aged man: a case report. J Med Case Rep. 2011;5:559.
Papageorgiou S.G., Kolovou D., Bonakis A., Kontaxis T., Moulopoulou A., Kalfakis N. Concommitant appearance of glioblastoma multiforme and neurocysticercosis in a nonendemic country: a case report. Neurologist. 2009;5:293-295.
Papazahariadou M.G., Papadopoulos E.G., Frydas S.E., Mavrovouniotis Ch., Constantinidis T.C., Antoniadou-Sotiriadou K., Siochu A.E. Prevalence of gastrointestinal parasites in the Greek population: local people and refugees. Ann Gastroenterol. 2004;17:194-198.
Paterakis K.N., Kapsalaki E., Hadjigeorgiou G.M., Barbanis S., Fezoulidis I., Kourtopoulos H. Primary spinal intradural extramedullary cysticercosis. Surg Neurol. 2007;68:309-311.
Patsantara G.G., Piperaki E.T., Tzoumaka-Bakoula C., Kanariou M.G. Immune responses in children infected with the pinworm Enterobius vermicularis in central Greece. J Helminthol. 2016;90:337-341.
Printza N., Sapountzi E., Dotis J., Papachristou F. Hemolytic uremic syndrome related to Cryptosporidium infection in an immunocompetent child. Pediatr Int. 2013;55:788-790.
Sagebiel D., Weitzel T., Stark K., Leitmeyer K. Giardiasis in kindergartens: prevalence study in Berlin, Germany. Parasitol Res. 2009;105:681-687.
Sprong H., Caccio S.M., van der Giessen J.W. Identification of zoonotic genotypes of Giardia duodenalis. PLoS Negl Trop Dis. 2009;3:e558.
Takaoka K., Gourtsoyannis Y., Hart J.D., Armstrong M., Daniel A., Mewse E, Phillips D., Bailey R.L. Incidence rate and risk factors for giardiasis and strongyloidiasis in returning UK travelers. J Travel Med. 2016;23:1–6.
Torgerson P.R., Devleesschauwer B., Praet N., Speybroeck N., Willingham A.L., Kasuga F., Rokni M.B., Zhou X.N., Fèvre E.M., Sripa B., Gargouri N., Fürst T., Budke C.M., Carabin H., Kirk M.D., Angulo F.J., Havelaar A., de Silva N. World Health Organization Estimates of the Global and Regional Disease Burden of 11 Foodborne Parasitic Diseases, 2010: A Data Synthesis. PLoS Med. 2015;12(12):e1001920.
Tsibouris P., Galeas T., Moussia M., Sotiropoulou M., Michopoulos S., Kralios N. Two cases of eosinophilic gastroenteritis and malabsorption due to Enterobious vermicularis. Dig Dis Sci. 2005;50:2389-2392.
Tzanidakis N., Sotiraki S., Claerebout E., Ehsan A., Voutzourakis N., Kostopoulou D. Stijn C., Vercruysse J., Geurden T. Occurrence and molecular characterization of Giardia duodenalis and Cryptosporidium spp. in sheep and goats reared under dairy husbandry systems in Greece Parasite. 2014;21:45.
132
Vassalos C.M., Petropoulou D.M., Ganteris G., Lada H.M., Vakalis N., Stefanou S.L., Papadopoulou C. New trends on Blastocystis sp. Infection. Acta Microbiol Hel. 2009;54:70-78.
Werner A., Majewska A.C., Slodkowicz A. Prevalence of intestinal protozoan parasites in humans from the Poznan area. Ann Parasitol. 2004;4:51.
Zahariou A., Karamouti M., Papaioannou P. Enterobius vermicularis in the male urinary tract: a case report. J Med Case Rep. 2007;1:137.
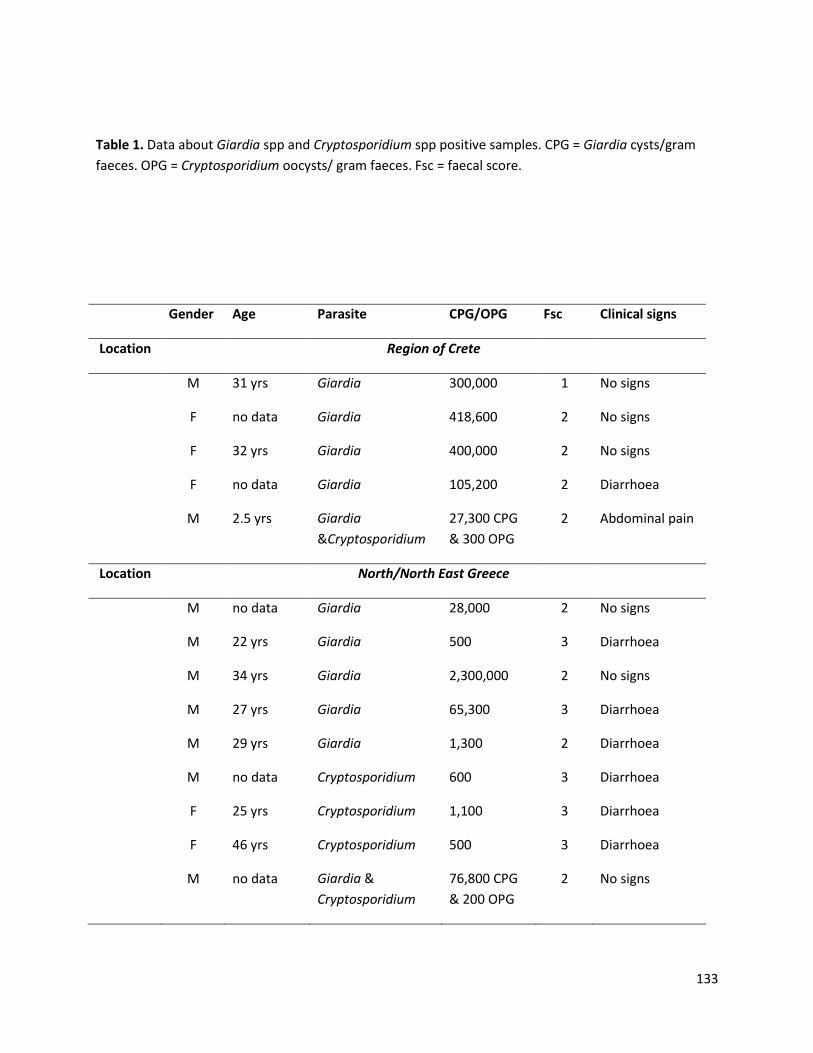
133
Table 1. Data about Giardia spp and Cryptosporidium spp positive samples. CPG = Giardia cysts/gram
faeces. OPG = Cryptosporidium oocysts/ gram faeces. Fsc = faecal score.
Gender Age Parasite CPG/OPG Fsc Clinical signs
Location Region of Crete
M 31 yrs Giardia 300,000 1 No signs
F no data Giardia 418,600 2 No signs
F 32 yrs Giardia 400,000 2 No signs
F no data Giardia 105,200 2 Diarrhoea
M 2.5 yrs Giardia
&Cryptosporidium
27,300 CPG
& 300 OPG
2 Abdominal pain
Location North/North East Greece
M no data Giardia 28,000 2 No signs
M 22 yrs Giardia 500 3 Diarrhoea
M 34 yrs Giardia 2,300,000 2 No signs
M 27 yrs Giardia 65,300 3 Diarrhoea
M 29 yrs Giardia 1,300 2 Diarrhoea
M no data Cryptosporidium 600 3 Diarrhoea
F 25 yrs Cryptosporidium 1,100 3 Diarrhoea
F 46 yrs Cryptosporidium 500 3 Diarrhoea
M no data Giardia &
Cryptosporidium
76,800 CPG
& 200 OPG
2 No signs
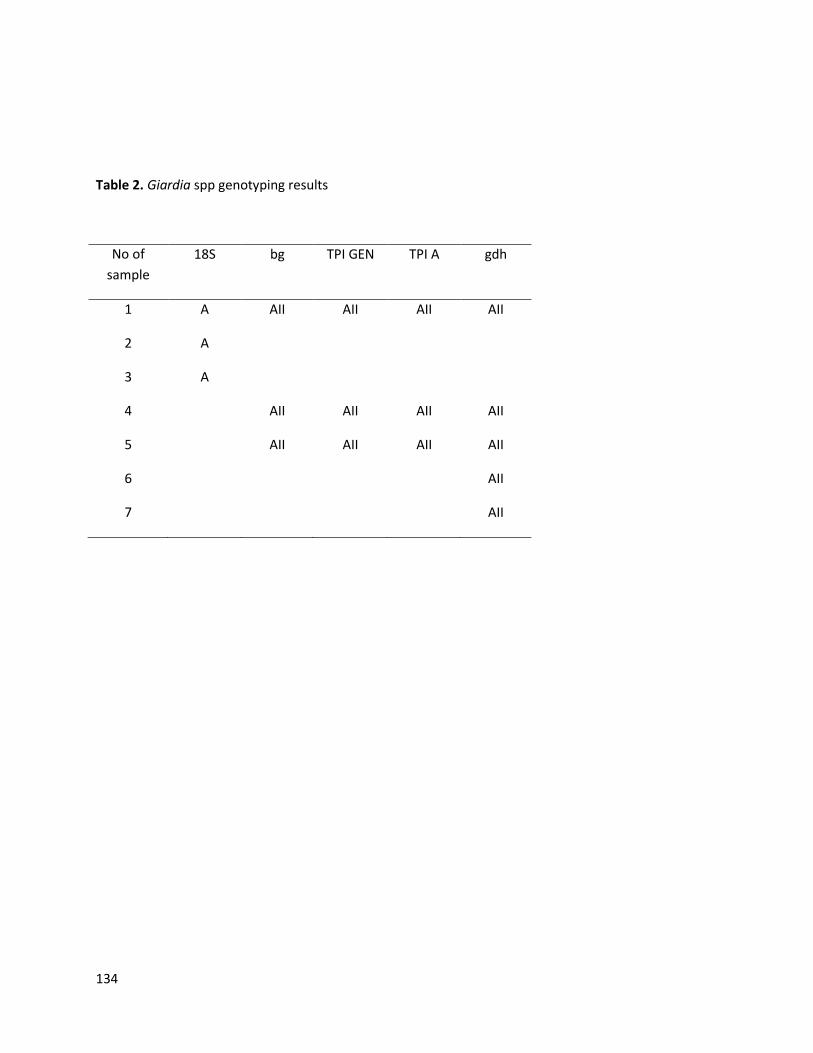
134
Table 2. Giardia spp genotyping results
No of
sample
18S bg TPI GEN TPI A gdh
1 A AII AII AII AII
2 A
3 A
4 AII AII AII AII
5 AII AII AII AII
6 AII
7 AII
135
Chapter V
General discussion
136
Introduction
Giardia and Cryptosporidium have received much attention not only for their prevalence and virulence
in various animal species, but also in humans. Several recent epidemics (Wang et al., 2013; Guzman-
Herradoret al., 2015; Painter et al., 2016; Efstratiou et al., 2017) caused by these two protozoa have
been reported worldwide, linked mainly to water contamination in both developing and developed
communities.
During the last decades numerous studies have been conducted, which led to a greater understanding
of their worldwide distribution and disease burden caused. According to WHO estimates, in 2010,
giardiosis resulted in 171,100 disability-adjusted life years (DALYs) and cryptosporidiosis in 2,159,331
DALYs (Kirk et al., 2015).
Moreover, by the application of modern biological techniques, several diagnostic assays have been
developed and validated with different sensitivity and specificity, which are performed either as a part
of routine diagnostic services or at a research level. Despite these advancements, still, there is a big
debate related to their transmission pathways within and between host species and their interactions,
especially concerning Giardia. What has being discussed is whether Giardia can be potentially zoonotic
and subsequently, which transmission cycles are implicated in human infections and in water or food
sources’ contamination.
We have tried to fill in these “gaps” of knowledge by studying the abundance of both parasites in
Greece and by characterizing them at a subspecies/assemblage level within major host species (humans,
dogs, cats, horses, small ruminants). Despite the wide distribution of Giardia and Cryptosporidium in
both animals and humans globally, little is known about the presence of these protozoa in animal and
human populations in Greece. There were 456 outbreaks of waterborne and foodborne diseases
reported by the Hellenic Center for Disease Control and Prevention between 2004 and 2017
(http://www.keelpno.gr). For 64.5% of the above outbreaks (n=294), Salmonella spp were considered as
the primary aetiological cause, followed by other bacteria or viruses. On the contrary, parasites were
implicated in only one outbreak during this time period but any further information about the
responsible parasitic species is not provided. Our interest to conduct this study in Greece arised largely
by the geographical location of the country (at the South end of Europe bordering the Balcans, Africa
and the Middle-East), which attracts immigrants and refugees especially during the last decades. This
geographical location and the climatic conditions are also responsible for the very intense touristic
137
activity of the country which translates to millions of tourists visiting various Greek destinations annually
from all over the world, often together with their pets. All the above favours the invasion of new
parasitic species with potential public health risk not necessary restricted to the area. Therefore, our
target was to better understand the routes of transmission of zoonotic parasites focusing on Giardia and
Cryptosporidium among various host populations living in close proximity and the possible existence of a
zoonotic risk.
In an effort to reduce as much as possible environmental factors affecting our results i.e surface waters
(rivers) originating from other regions or neighbouring countries, we focused our studies on a controlled
(restricted) area such as the island of Crete. Crete was also the study area for a preliminary study that
we had carried out in order to evaluate the prevalence and the zoonotic potential of Giardia spp and
Cryptosporidium spp in small ruminants (Tzanidakis et al., 2014). Following this study and in order to
have a complete view of the prevalence of these two protozoa also in other animal species, we
proceeded (as part of this thesis) to the estimation of the parasitism in companion animals (dogs and
cats) and foals of the island. In a “One Health” approach we continued our survey in the human
populations of Crete.
However, due to the difficulties we met during our sampling such as the low number of foals in the
island and the low correspondence of individuals who were willing to participate in the study, we
expanded our sampling area to various parts of Greece regarding foals, and to Nothern Greece regarding
humans. The number of samples collected from Crete is mentioned in Table 1.
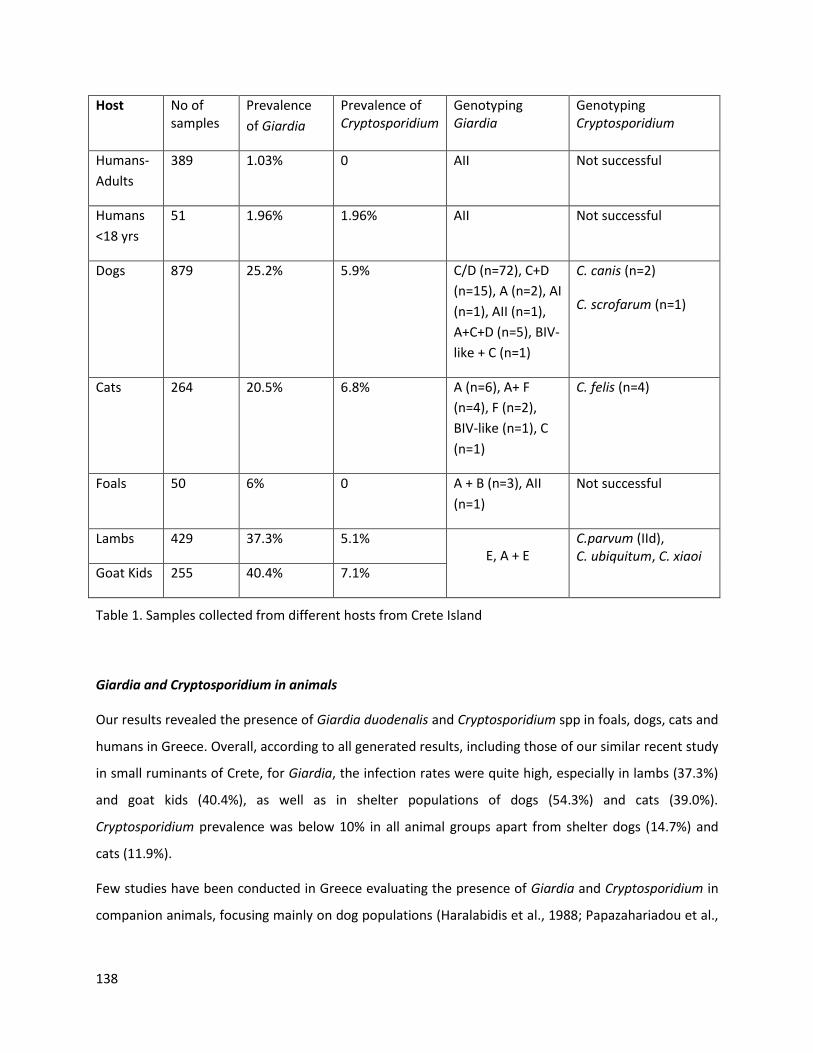
138
Host No of samples
Prevalence
of Giardia
Prevalence of Cryptosporidium
Genotyping Giardia
Genotyping Cryptosporidium
Humans-
Adults
389 1.03% 0 AII Not successful
Humans
<18 yrs
51 1.96% 1.96% AII Not successful
Dogs 879 25.2% 5.9% C/D (n=72), C+D
(n=15), A (n=2), AI
(n=1), AII (n=1),
A+C+D (n=5), BIV-
like + C (n=1)
C. canis (n=2)
C. scrofarum (n=1)
Cats 264 20.5% 6.8% A (n=6), A+ F
(n=4), F (n=2),
BIV-like (n=1), C
(n=1)
C. felis (n=4)
Foals 50 6% 0 A + B (n=3), AII
(n=1)
Not successful
Lambs 429 37.3% 5.1% E, A + E
C.parvum (IId), C. ubiquitum, C. xiaoi
Goat Kids 255 40.4% 7.1%
Table 1. Samples collected from different hosts from Crete Island
Giardia and Cryptosporidium in animals
Our results revealed the presence of Giardia duodenalis and Cryptosporidium spp in foals, dogs, cats and
humans in Greece. Overall, according to all generated results, including those of our similar recent study
in small ruminants of Crete, for Giardia, the infection rates were quite high, especially in lambs (37.3%)
and goat kids (40.4%), as well as in shelter populations of dogs (54.3%) and cats (39.0%).
Cryptosporidium prevalence was below 10% in all animal groups apart from shelter dogs (14.7%) and
cats (11.9%).
Few studies have been conducted in Greece evaluating the presence of Giardia and Cryptosporidium in
companion animals, focusing mainly on dog populations (Haralabidis et al., 1988; Papazahariadou et al.,
139
2007; Symeonidou et al., 2017; Symeonidou et al., 2018), with estimated infection rates similar to our
findings in most cases, although different diagnostic tools were applied.
Giardia and Cryptosporidium have been also found in dogs and cats in several other countries in Europe
including those located in the Mediterranean basin (Causape et al., 1996; Dubna et al., 2007; Claerebout
et al., 2009; Overgaauw et al., 2009; Epe et al., 2010; Upjohn et al., 2010; Dupont et al., 2013; Zanzani et
al., 2014; Osman et al., 2015; Paoletti et al., 2015; Piekarska et al., 2016; de Lucio et al., 2017; Ferreira et
al., 2017; Hinney et al., 2017; Adell-Aledon et al., 2018). Our results (Chapter 3) are in agreement with
the published data, however, variations in infection rates have been observed and maybe attributed to
the differences in the type of studies (cross-sectional vs longitudinal studies), the sample size and the
diagnostic methods used.
As expected due to their living conditions, shelter dogs and cats tend to be highly infected with both
Giardia and Cryptosporidium, not only in Greece but also in other European countries (Causape et al.,
1996; Claerebout et al., 2009; Scaramozzino et al., 2009; Ferreira et al., 2011; Dado et al., 2012; Ortuno
et al., 2014; Simonato et al., 2015; Gil et al., 2017). However, especially in the case of catteries, the
observed infection rates were significantly higher than those reported in other studies (Robben et al.,
2004; Ferreira et al., 2011; Gil et al., 2017).
Regarding production animals, investigations have been previously conducted in Greece with focus on
cryptosporidiosis in ruminants. Since the herds included in those studies had a history of diarrhoea or
the animals were diarrhoeic at the time of sampling, the infection rates reported in both cattle (Panousis
et al., 2007; Arsenopoulos et al., 2017) and small ruminants (Panousis et al., 2008; Giadinis et al., 2015)
were much higher than our records (Tzaniidakis et al., 2014). Comparing our results with other studies in
Europe, it seems that the high prevalence of Giardia reported in lambs and goat kids in Crete is in line
with these surveys (Gomez-Mucoz et al., 2009; Geurden et al., 2010; Castro-Hermida et al., 2011).
However, regarding Cryptosporidium, in our case, by testing animals of a similar age results showed
lower levels of infection compared to other European studies (Geurden et al., 2008; Robertson et al.,
2010; Kaupke et al., 2017a), probably due to differences in breed or management and husbandry
practices (e.g. less intensified systems prevailing in Crete) (Mahfouz et al., 2014).
Since as already mentioned, a significant part of our studies has been focused on studying the
epidemiological scenario on Crete island, we decided not to proceed with studies investigating the
occurrence of Giardia and Cryptosporidium in bovines, because contrary to the large numbers of sheep
140
and goats living all over the island (according to Official National Statistical data they are a population of
over 1,500,000 individuals), cattle herds are almost absent.
Especially for foals, our studies included horse samples not only from Greece (the majority of the
samples) but also from Belgium, Germany and the Netherlands as part of a larger survey. The infection
rates found, were similar among countries but lower than in other studies conducted in Italy in which a
higher prevalence of both Giardia and Cryptosporidium, has been found (Veronesi et al., 2010).
In general, taking into consideration our results in animals and comparing them with similar studies in
Europe (Geurden et al., 2008; Paoletti et al., 2008; Claerebout et al., 2009; Geurden et al., 2010; Tysnes
et al., 2011; de Lucio et al., 2017; Gil et al., 2017), we could assume that high infection rates of Giardia
spp exist in different animal populations (companion animals and livestock) in Greece. On the contrary,
in the case of Cryptosporidium spp, among the different animal species that were tested in the current
study, only shelter dogs and cats seem to be highly infected.
The above protozoal infections in all animal species have detained us mainly for their public health
significance and to a lesser extent for their impact on animals’ health. However, although in most cases
the infections are asymptomatic or the symptoms are self-limited in both companion and production
animals, they may have severe economic consequences especially in livestock (Tangtrongsup and
Scorza, 2010; Xiao, 2010; Feng and Xiao, 2011; Santin, 2013; Abeywardena et al., 2015). That includes
economic losses due to animals’ death, treatment costs and reduced productivity (weigh losses and
reduced carcass quality) (Geurden et al., 2010; Sweeny et al., 2011; Thomson et al., 2017).
Giardia and Cryptosporidium in humans
Apart from a previously reported outbreak of giardiosis in a hotel in Crete (Hadjichristodoulou et al.,
1998; Hardie et al., 1999), there were no epidemiological data available for the human population in
Greece. Despite the high infection rates in the studied animal species we have recorded, which are
indicative of the presence and the circulation of Giardia and Cryptosporidium in the environment, the
occurrence of parasitism in humans was low (1.3% Giardia & 0.6% Cryptosporidium). This is in
agreement with the absence of any report of outbreaks caused by Giardia spp and/or Cryptosporidium
spp by the Hellenic Center for Disease Control and Prevention between 2004 and 2017
(http://www.keelpno.gr). As previously mentioned, only one waterborne/foodborne outbreak of
parasitic origin was recorded in 2010 and without any clarification of the responsible parasitic species.

141
Giardia spp and Cryptosporidium spp infections are commonly underreported by the surveillance
systems possibly because they are misdiagnosed by the medical doctors in Greece either because of lack
of background epidemiological knowledge of the presence of those parasites (which most often co-exist
with other enteropathogens), or because the diagnostic techniques routinely performed are of limited
sensitivity failing to detect the responsible parasitic agent.
In the current study, only 11 people out of 876 were found infected with Giardia, two of whom were co-
infected with Cryptosporidium. Since it is obvious from our results that the two protozoa do exist in the
environment and are present in animal populations, a reason for the low prevalence in humans could be
that Giardia and Cryptosporidium infections may be underestimated, since many of the individuals
participating in our study were immunocompetent and clinically healthy people (80.1%), and most of
them were adults (93.8%). According to the literature, children and immunocompromised individuals
are more vulnerable to Giardia and Cryptosporidium infection (Thompson et al., 2005; Haliez and Buret,
2013; Ryan et al., 2016; Soares and Tasca, 2016). In our study we had chosen not to focus on
immunocompromised or clinically ill individuals because this was not the main objective of the study.
Our main interest was to investigate the presence of those parasites amongs the general human
population and to genetically characterise the strains found in order to trace the route of infection.
However, although we managed to follow a predefined sampling strategy in the case of dogs and cats,
this was not possible with foals’ and humans’ sampling as previously mentioned. Thus, especially in the
case of humans, we were more restricted to samples obtained through medical doctors, though mostly
from clinically healthy individuals (food workers). Our study population was randomly selected since we
could not include a predefined target group. This approach could influence our results although there
was an equal geographical distribution of the samples through Crete and also in Nothern Greece.
Of course contact with animals could have been an important risk factor, which could have led to the
transmission of Giardia spp and Cryptosporidium spp especially to pet owners. However none of the
infected participants reported any contact with animals, but then again, the low number of infected
individuals is restricting further analyses and risk factor characterization.
Greece is a country that sufficient sanitary conditions are ensured. This is confirmed by the low infection
rates of the parasites that were detected in humans in the current study, contrary to what has been
found in animal populations, including zoonotic assemblages/genotypes. Thus, the risk factor “hygiene
measures” seems not to exist in our case. Similarly, another possible risk factor could have been
contaminated water through which Giardia spp and Cryptosporidium spp are frequently transmitted.

142
However, it seems that adequate treatment to water supplies is provided following the European Union
Regulation 2015/1787(L260, 7.10.2015) and under this condition any possible transmission is prevented.
This is reinforced by the limited (only one) unofficial record of any waterborne/foodborne outbreak
caused by Giardia and/or Cryptosporidium in Greece.
Zoonotic transmission of Giardia?
Overall, despite animal infections being very common, the importance of zoonotic transmission of
Giardia has been widely debated. The most popular hypothesis is that animals tend to be largely, but
not exclusively, infected with their ‘own’ animal-specific Giardia isolates that have no, or very limited,
impact on human health (Tysnes et al., 2014; Caccio et al., 2017) and this hypothesis is supported by the
genotyping results of our studies. Humans are mainly infected with the anthroponotic assemblages A
and B (Caccio et al. 2017), which is also the case in our survey. Although assemblages A and B have also
been isolated from animals, especially dogs and cats, we cannot fully justify that these isolates are
responsible for transmission to humans (Thompson and Ash, 2016). However, there are reports
suggesting that assemblage A is mainly associated with human infections caused by dogs and cats, and
that assemblage B is mostly related to anthroponotic transmission (Anuar et al., 2014; Minetti et al.,
2015; Pijnacker et al., 2016; Caccio et al., 2017). In contrast, some studies report the presence of animal
specific assemblages in human isolates and the detection of non-adapted assemblages among different
animal species, such as for instance, the presence of feline specific assemblage/genotype of Giardia and
Cryptosporidium in cattle in Spain (Cardona et al., 2015). However, the possibility of passive carriage of
cysts instead of real infection cannot be excluded (Caccio et al., 2017).
In the present study, in agreement with several published data from Europe, the canine and feline
assemblages were the dominant ones in companion animals (Sprong et al., 2009; Feng and Xiao, 2011;
Beck et al., 2012; Ortuno et al., 2014; Pallant et al., 2015; Sommer et al., 2015; Piekarska et al., 2016; de
Lucio et al., 2017; Adell-Aledon et al., 2018; Sommer et al., 2018). However, Giardia zoonotic
assemblages were also isolated from dogs and cats (AI, AII, BIV-like). Similar recent studies conducted in
Spain support that such isolates are not epidemiologically linked to human derived sequences and this
because they have recorded a high genetic diversity in AII sequences derived from canine isolates but
not from human origin ones (Adell-Aledon et al., 2018). Unfortunately, in our study, a multi-locus
genotyping approach was achieved only for one dog sample where assemblage A was assigned in three

143
markers and classified as multilocus genotype MLGA1, previously described only in calves in China
(Wang et al., 2016). Altogether, data from both our work and other studies reinforce the suggestion that
dogs are not a significant reservoir of zoonotic Giardia assemblages.
In cats, the zoonotic assemblage A was identified exclusively at the 18 SSU-rRNA locus while the feline
assemblage F was detected at other loci even in the same samples. Since 18 SSU-rRNA is a conserved
gene, we could not make a distinction between the above assemblages and we cannot exclude the
possibility that the isolated assemblage A is in fact assemblage F. Although according to the literature,
cats are known carriers of assemblage A and F, but not of assemblage B (Xiao and Fayer, 2008; Gil et al.,
2017), we detected assemblage BIV-like from a shelter cat. The inability to distinguish the two
assemblages in cats through 18 SSU-rRNA locus has been also reported in another survey (Sommer et
al., 2018). Thus, the potential zoonotic risk from Giardia infected cats cannot be evaluated in the
present study. Cats have been implicated in the animal to human transmission cycle of Giardia as
subtypes of assemblages F and MLG belonging to sub-assemblage AII have been also found in human
isolates (Sprong et al., 2009).
In foals, apart from the detection of the hoofed livestock-specific assemblage E, we also identified
assemblage B, which in fact was the most prevalent assemblage, and sub-assemblage AI. Both of the
latter two (sub)assemblages have proven zoonotic relevance and this was not a completely new finding
since similar results have been also reported from other researchers (Veronesi et al., 2010; Traversa et
al., 2012; Ryan and Caccio, 2013; Santin et al., 2013). However, since multilocus genotyping was not
possible in our studies, similarly as with other species, the role of equidae in the transmission of Giardia
in humans remains unclear and needs to be further investigated.
As regards small ruminants, assemblage A (no further characterised into sub-assemblages) was isolated
in a limited number of animals in our earlier study in Crete, which again was more or less expected since
it has been previously isolated from livestock in Europe (Gomez-Munoz et al., 2012; Minetti et al., 2014).
Although such findings suggest that there is a potential for Giardia spp to be transmitted from small
ruminants to humans in the island of Crete, evidence remains weak and has to be further clarified.
In the human Giardia positive samples, PCR and sequencing revealed only the presence of assemblage
AII, which is primarily a human-adapted assemblage, although it has been also isolated from animals
(Wang et al., 2014; Pallant et al., 2015; Thompson and Ash, 2016; Xu et al., 2016). Further investigation,
through multi-locus genotyping (MLG), confirmed these results and provided no evidence for Giardia
transmission from animals to humans or vice versa. However, MLG was performed only for a very low

144
number of samples (n=2), so these results cannot be indicative of the whole study. Contrary to what has
been documented at the literature referring to the dominance of assemblage B (~58%) over assemblage
A (~37%) in human isolates from various regions in the world (Ryan and Caccio, 2013), in our study we
have no evidence of the presence of assemblage B in humans. This could be a consequence of the low
prevalence of the parasite in the participating individuals. However, there are reports worldwide, which
are in line with our findings and mention the mere existence or predominance of assemblage A in
human samples (Babaei et al., 2008; Yong et al., 2000; Wang et al., 2011; Wang et al., 2013; Azcona-
Gutiérrez et al., 2017).
Zoonotic transmission of Cryptosporidium?
Similarly to Giardia, the presence of animal specific Cryptosporidium species/genotypes e.g. C. canis, C.
felis and Cryptosporidium horse genotype in dogs, cats and foals respectively, illustrates a low risk for
zoonotic infections. These results are in line with other studies in Europe (Caffara et al., 2013; de Lucio
et al., 2017; Gil et al., 2017; Kvac et al., 2017). However, our previous findings in small ruminants in the
area, with the detection of C. parvum (subtype IId), C. ubiquitum and C. xiaoi, suggest an existing,
although limited, zoonotic risk. These results are similar to a recent study in Spain (Diaz et al., 2018) and
correspond to what has been previously published in the literature,i.e. Cryptosporidium infections in
humans can belinked to infected livestock (Fayer et al., 2000; Stantic-Pavlinic et al., 2003; Thompson et
al., 2008; Ibrahim et al., 2016; Conrad et al., 2017; Vermeulen et al., 2017).
Nevertheless, although as shown above, our genotyping results were rather anticipated, there were
cases of contradictory findings such as the isolation of the canine assemblage C from a household cat
which however, had unlimited access to the external environment, and the pig-specific Cryptosporidium
scrofarum genotype from a shelter dog, which may have occurred due to accidental ingestion of cysts
and oocysts respectively and these animals could act as passive carriers of the parasites.
The amplification and sequencing of the human Cryptosporidium positive sample was not successful.
The presence of PCR inhibitors in stool specimens in combination with the robust cell walls of the
Cryptosporidium oocysts and the low infection intensity (300 oocysts per gram of faeces) detected with
the immunofluorescence assay, could influence in a negative way the efficacy of the molecular
techniques performed (Oikarinen et al., 2009; Surl et al., 2011; Schrader et al., 2012). Thus, in
combination to the fact that we have only one positive sample, we cannot draw any conclusions about
zoonotic transmission of Cryptosporidium in humans. Overall, we could conclude that there is minimal

145
zoonotic risk taking also into account the results drawn from the animal studies, which showed the
presence of mainly host-specific Cryptosporidium species/genotypes. However, although unusual,
globally, species/genotypes such as C. meleagridis, C. felis, C. canis, Cryptosporidium horse, skunk and
rabbit genotype as well as cervine genotypes, have been implicated in human cases of clinical
cryptosporidiosis, even in immunocompetent individuals, but at a low rate and mainly in developing
countries (Robinson et al., 2008; Thompson et al., 2008; Xiao et al., 2009; Lucio-Forster et al., 2010;
Beser et al., 2015; González-Díaz et al., 2016). Unlike small ruminants and foals, where we met no
difficulties in genotyping either Giardia or Cryptosporidium positive faecal samples, our amplification
and sequencing results in dog and cat samples did not have the expected success rates, especially in the
case of Cryptosporidium (10% success for 18 SSU-rRNA and 13% success for HSP70 gene). This
phenomenon has been documented before mainly in isolates of canine and feline origin and could be
interpreted as a result of the presence of PCR inhibitors in dog and cat faeces and the low number of
Giardia and Cryptosporidium (oo)cysts detected by immunofluorescence (Tangtrongsup and Scorza,
2010; de Lucio et al., 2016; Cardona et al., 2015; Gil et al., 2017; Adell-Aledon et al., 2018). In our case
the parasitic burden in dogs ranged from 100 to 275.800 CPG, but the genotyping results were
inconsistent showing often positive outcome when CPG was low and vice-versa.
Conclusions
In general, our results, in an effort to evaluate the epidemiologic scenario of Giardia and
Cryptosporidium among people and various animal species who co-exist and interact in the same
environment, support the fact that transmission cycles between animals and humans remain separated
especially to what Giardia infections concerns (Figure 1).
The high infection rates of Giardia and Cryptosporidium in animals and therefore the high rates of
environmental contamination that may exist, in combination with the low parasitism which was
detected in humans who share this contaminated habitat, support that conclusion. The predominance
of non- zoonotic genotypes of both Giardia and Cryptosporidium makes the transmission scenario of
these protozoa from animals to humans rather faint. Thus, animals seem to share their own animal-
specific assemblages/genotypes and humans the anthroponotic ones.
Despite the isolation of zoonotic assemblages from Giardia infected companion and productive animals,
overall this evidence was rather weak allowing us to conclude that animals were not actively involved in
the spread of the two parasites to humans. Therefore, we are more oriented to the human-to-human
cycle as the most possible and predominant mode of transmission in humans in the present study, while
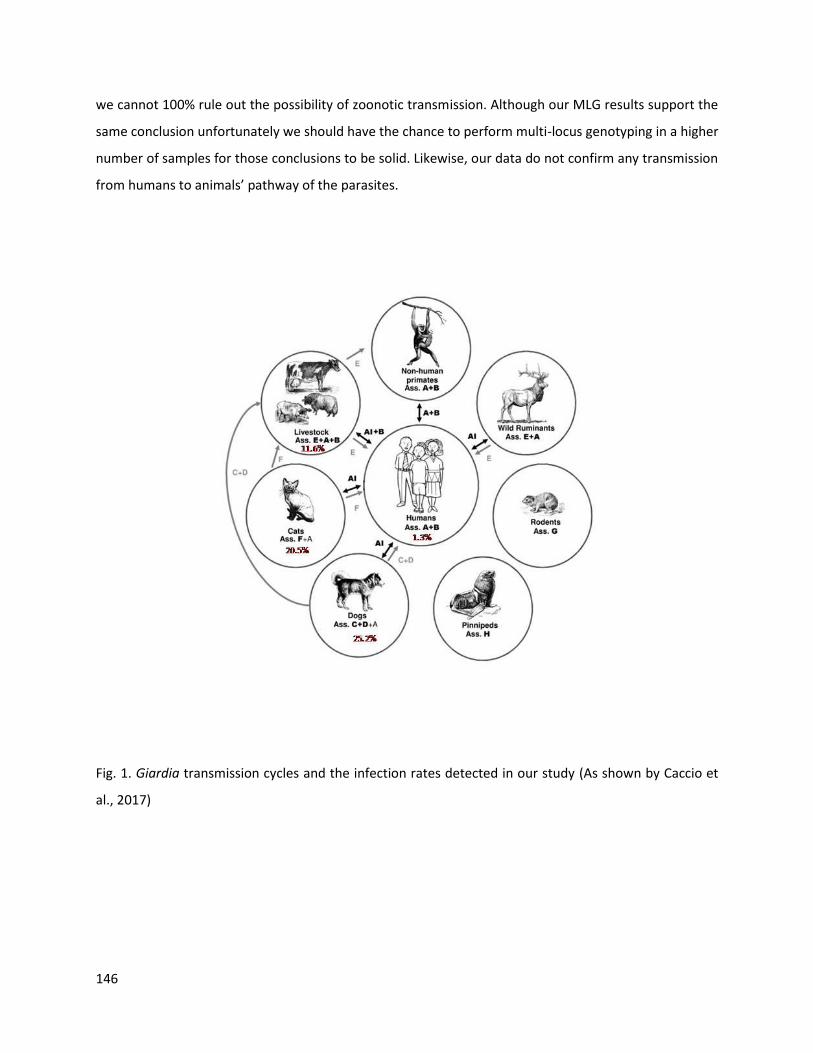
146
we cannot 100% rule out the possibility of zoonotic transmission. Although our MLG results support the
same conclusion unfortunately we should have the chance to perform multi-locus genotyping in a higher
number of samples for those conclusions to be solid. Likewise, our data do not confirm any transmission
from humans to animals’ pathway of the parasites.
Fig. 1. Giardia transmission cycles and the infection rates detected in our study (As shown by Caccio et
al., 2017)

147
Opportunities for future studies
Our work was based on cross-sectional studies. Ideally, the transmission dynamics of Giardia and
Cryptosporidium could have been better clarified if we could perform a longitudinal surveillance, which
would allow identification of temporal-spatial peaks of prevalence and the infection dynamics’
seasonality of the parasites. Based on our results in humans and the different animal populations, a
longitudinal survey could be supported by a further investigation of the parasites’ prevalence in sheep
and goats in Crete. In our preliminary study in small ruminants, high prevalence of Giardia was detected
including the zoonotic assemblage A, which therefore was not further characterized. Besides, sheep and
goats graze the pastures which surround the drinking water basins of the island so a simultaneous
investigation of the natural water sources of the area would provide valuable knowledge in an effort to
investigate the epidemiological patterns of Giardia infection and assess the potential risk for public
health. Inclusion of humans in the longitudinal study would be ideal, however, the significant difficulties
we met during sampling process remains a discouraging scenario.
Infections in humans could have occurred after direct contact with already infected individuals or via
contaminated water or food e.g. raw vegetables and fruits. In an attempt to obtain evidence of zoonotic
transmission, we designed a simultaneous sampling of humans and domestic animals living in localised
foci, although we did not preclude the investigation of the occurrence of Giardia and Cryptosporidium in
water sources (treated or untreated) or in drinking water or vegetables in the area, but this is something
that should be taken into consideration and probably performed in future studies. Specifically for the
Crete island and due to the constant tourism growth, the evaluation of the water contamination of the
swimming pools in the tourists’ accommodation spots would constitute significant data about the
possible “import” and “export” of Giardia and Cryptosporidium in the island.
Similarly, as Crete receives refugees continuously, a surveillance of Giardia and Cryptosporidium
infection level in these individuals would be also valuable.
In addition, our survey could have expanded via the investigation of environmental contamination, to
the possible infection of wildlife especially in the case of Giardia where zoonotic species have been
implicated in cases of giardiosis of wildlife species (Thompson and Ash, 2016). Crete is characterized by
a wide variety of wildlife. This wildlife includes many mammals some of which are the Cretan Agrimi
Wild Goat also known as “Kri-Kri”, the Cretan Wild Cat, the Cretan White-toothed Shrew, the Cretan
Spiny Mouse, high numbers of weasels, hedgehogs, Brown Hares and European rabbits. Also, many

148
flocks of free roaming wild sheep and goats exist in the island. Through the evaluation of the parasitism
of wildlife species we can have a more complete view of the transmission patterns of Giardia and
Cryptosporidium in the area and reach more precise conclusions.
Reffering back to the difficulties we met during sample processing procedures specifically in acquiring a
satisfactory DNA quality to run the PCR protocols it would be important to perform studies aiming to
overcome such problems. During our studies and in order to increase our success rates we proceeded to
some modifications of the selected protocols like for example altering the performance of the PCR mix
by adding Bovine Serum Albumine (BSA) and by replacing BSA with Dimethyl Sulfoxide (DMSO). During
this effort we performed multiple reactions trying different concentrations of BSA and DMSO each time.
Both BSA and DMSO boost PCR and increase PCR robustness and are recommended for difficult (low
purity) templates (Abu Al-Soud and Rådström, 2000). In addition, we tried to alter the concentration of
MgCl2. For instance, by increasing the MgCl2 concentration Taq DNA polymerase’s activity is increased
and sensitivity is higher, whereas lower MgCl2 concentration lowers Taq’s activity but increases
specificity (Roux, 1995). Moreover we changed the annealing temperature of the reactions by
decreasing the temperature in order to increase sensitivity (Roux, 1995) and tried to amplify all the
genes that are recommended by publications for the detection of Giardia and Cryptosporidium.
However, and in spite all our efforts, there is still need for improvement and it would be crucial for
similar future studies to introduce an improved sample treatment in order to acquire better purified
DNA product and therefore better-quality PCR results. Purification could be done after floatation of the
Giardia and/or Cryptosporidium positive faecal samples and selection of the concentrated cysts and/or
oocysts. DNA could be then extracted by these purified cysts and/or oocysts. Another helpful tool that
we could use in the future and could increase PCR success is DNA cloning.
Further investigations on the Giardia and Cryptosporidium genome would enable us to better
understand their transmission dynamics. The use of a more recently introduced molecular technique
(like for example Next Generation Sequencing) could lead to a better identification and clarification of
the parasites’ subtypes. This could also help to the better detection of Giardia and Cryptosporidium
species in case of mixed infections where dominant strains might competitively exclude others. Besides,
as already done in human and pig Cryptosporidium isolates (Paparini et al., 2015; Kaupke et al., 2017b),
NGS could allow species identification in samples with low abundance of parasite DNA. Regarding
Giardia, as the whole genome of assemblages A, B and E has been analysed showing similarities

149
between A and E (Caccio et al., 2017), it would be of great interest to establish genome sequences of the
other animal-specific Giardia assemblages (Caccio et al., 2017).
In summary, our study indicates that companion animals and livestock can act as significant contributors
to Giardia cyst and Cryptosporidium oocyst environmental contamination in Greece. Infections are also
present in people although in low rates. Zoonotic risk of Giardia spp and Cryptosporidium spp seems to
be limited, however, it should not be neglected. Further investigations of water sources in the area
would be valuable and could also provide interesting data about the occurrence and the epidemiology
of the parasites in the rich wildlife of the island.
150
References
Abeywardena H., Jex A.R., Gasser R.B. A perspective on Cryptosporidium and Giardia, with an emphasis on bovines and recent epidemiological findings. Adv Parasitol. 2015;88:243-301.
Abu Al-Soud W., Rådström P. Effects of amplification facilitators on diagnosticPCR in the presence of blood, feces, and meat. J Clin Microbiol. 2000;38(12):4463-70.
Adell-Aledón M., Köster P.C., de Lucio A., Puente P., Hernández-de-Mingo M., Sánchez-Thevenet P., Dea-Ayuela M.A., Carmena D. Occurrence and molecular epidemiology of Giardia duodenalis infection in dog populations in eastern Spain. BMC Vet Res. 2018;14(1):26.
Anuar T.S., Azreen S.N., Salleh F.M., Moktar N. Molecular epidemiology of giardiasis among Orang Asli in Malaysia: application of the triosephosphate isomerase gene. BMC Infect Dis. 2014;14:78.
Arsenopoulos K., Theodoridis A., Papadopoulos E. Effect of colostrum quantity and quality on neonatal calf diarrhoea due to Cryptosporidium spp. infection. Comp Immunol Microbiol Infect Dis. 2017;53:50-55.
Azcona-Gutiérrez J.M., de Lucio A., Hernández-de-Mingo M., García-García C., Soria-Blanco L.M., Morales L., Aguilera M., Fuentes I., Carmena D. Molecular diversity and frequency of the diarrheagenic enteric protozoan Giardia duodenalis and Cryptosporidium spp. in a hospital setting in Northern Spain. PLoS One. 2017;12(6):e0178575.
Babaei Z., Oormazdi H., Akhlaghi L., Rezaie S., Razmjou E., Soltani-Arabshahi S.K., Meamar A.R., Hadighi R. Molecular characterization of the Iranian isolates of Giardia lamblia: application of the glutamate dehydrogenase gene. Iran J Public Health. 2008;37:75-82.
Beck R., Sprong H., Pozio E., Cacciò SM. Genotyping Giardia duodenalis isolates from dogs: lessons from a multilocus sequence typing study. Vector Borne Zoonotic Dis. 2012;12(3):206-213.
Beser J., Toresson L., Eitrem R., Troell K., Winiecka-Krusnell J., Lebbad M. Possible zoonotic transmission of Cryptosporidium felis in a household. Infect Ecol Epidemiol. 2015;5:28463.
Cacciò S.M., Lalle M., Svärd S.G. Host specificity in the Giardia duodenalis species complex. Infect Genet Evol. 2017. pii: S1567-1348(17)30418-5.
Caffara M., Piva S., Pallaver F., Iacono E., Galuppi R. Molecular characterization of Cryptosporidium spp. from foals in Italy.Vet J. 2013;198:531-533.
Cardona G.A., de Lucio A., Bailo B., Cano L., de Fuentes I., Carmena D. Unexpected finding of feline-specific Giardia duodenalis assemblage F and Cryptosporidium felis in asymptomatic adult cattle in Northern Spain. Vet Parasitol. 2015;209(3-4):258-263.
Castro-Hermida J.A., Garcı´a-Presedo I., Almeida A., Gonza´lezWarleta M., Correia Da Costa J.M., Mezo M. Cryptosporidium spp. and Giardia duodenalis in two areas of Galicia (NW Spain). Sci Total Environ. 2011;409:2451–2459.
Causapé A.C., Quílez J., Sánchez-Acedo C., del Cacho E. Prevalence of intestinal parasites, including Cryptosporidium parvum, in dogs in Zaragoza city, Spain. Vet Parasitol. 1996;67(3-4):161-167.
Claerebout E., Casaert S., Dalemans A.C., De Wilde N., Levecke B., Vercruysse J., Geurden T. Giardia and other intestinal parasites in different dog populations in Nothern Belgium. Vet Parasitol. 2009;161:41–6.
151
Conrad C.C., Stanford K., Narvaez-Bravo C., Callaway T., McAllister T. Farm Fairs and Petting Zoos: A Review of Animal Contact as a Source of Zoonotic Enteric Disease. Foodborne Pathog Dis. 2017;14(2):59-73.
Cooper M.A., Sterling C.R., Gilman R.H., Cama V., Ortega Y., Adam R.D. Molecular analysis of household transmission of Giardia lamblia in a region of high endemicity in Peru. J Infect Dis. 2010;202(11):1713-1721.
Dado D., Montoya A., Blanco M.A., Miró G., Saugar J.M., Bailo B., Fuentes I. Prevalence and genotypes of Giardia duodenalis from dogs in Spain: possible zoonotic transmission and public health importance. Parasitol Res. 2012;111(6):2419-2422.
de Lucio A., Martínez-Ruiz R., Merino F.J., Bailo B., Aguilera M., Fuentes I., Carmena D. Molecular genotyping of Giardia duodenalis isolates from symptomatic individuals attending two major public hospitals in Madrid, Spain. PLoS One. 2015;10(12):e0143981.
de Lucio A., Amor-Aramendía A., Bailo B., Saugar J.M., Anegagrie M., Arroyo A., López Quintana B., Zewdie D., Ayehubizu Z., Yizengaw E., Abera B., Yimer M., Mulu W., Hailu T., Herrador Z., Fuentes I., Carmena D. Prevalence and genetic diversity of Giardia duodenalis and Cryptosporidiumspp among school children in a rural area of the Amhara region, North-West Ethiopia. PLoS One. 2016;11: e0159992.
de Lucio A., Bailo B., Aguilera M., Cardona G.A., Fernández-Crespo J.C., Carmena D. No molecular epidemiological evidence supporting household transmission of zoonotic Giardiaduodenalis and Cryptosporidium spp. from pet dogs and cats in the province of Álava, Northern Spain. Acta Trop. 2017;170:48-56.
Diaz P., Navarro E., Prieto A., Perez-Creo A., Vina M., Diaz-Cao J.M., Lopez C.M., Panadero R., Fernandez G., Diez-Banos P., Morrondo P. Cryptosporidium species in post-weaned and adult sheep and goats from N.W. Spain: Public and animal health significance. Vet Parasitol. 2018;254:1-5.
Dubná S., Langrová I., Nápravník J., Jankovská I., Vadlejch J., Pekár S., Fechtner J. The prevalence of intestinal parasites in dogs from Prague, rural areas, and shelters of the Czech Republic. Vet Parasitol. 2007;145(1-2):120-128.
Dupont S., Butaye P., Claerebout E., Theuns S., Duchateau L., Van de Maele I., Daminet S. Enteropathogens in pups from pet shops and breeding facilities. J Small Anim Pract. 2013;54(9):475-480.
Efstratiou A., Ongerth J.E., Karanis P. Waterborne transmission of protozoan parasites: Review of worldwide outbreaks – An update 2011-2016. Water Res. 2017;114;14-22.
Epe C., Rehkter G., Schnieder T., Lorentzen L., Kreienbrock L. Giardia in symptomatic dogs and cats in Europe--results of a European study. Vet Parasitol. 2010;173(1-2):32-38.
Fayer R., Morgan U., Upton S.J. Epidemiology of Cryptosporidium: transmission, detection and identification. Int J Parasitol. 2000;30(12-13):1305-1322.
Feng Y., Xiao L. Zoonotic potential and molecular epidemiology of Giardia species and giardiasis. Clin Microbiol Rev. 2011;24:110-140.
Ferreira F.S., Pereira-Baltasar P., Parreira R., Padre L., Vilhena M., TávoraTavira L., Atouguia J., Centeno-Lima S. Intestinal parasites in dogs and cats from the district of Évora, Portugal. Vet Parasitol. 2011;179(1-3):242-245.
152
Ferreira A., Alho A.M., Otero D., Gomes L., Nijsse R., Overgaauw P.A.M., Madeira de Carvalho L. Urban Dog Parks as Sources of Canine Parasites: Contamination Rates and Pet Owner Behaviours in Lisbon, Portugal. J Environ Public Health. 2017;2017:5984086.
Geurden T., Thomas P., Casaert S., Vercruysse J., Claerebout E. Prevalence and molecular characterisation of Cryptosporidium and Giardia in lambs and goat kids in Belgium. Vet Parasitol. 2008;155(1-2):142-145.
Geurden T., Vercruysse J., Claerebout E. Is Giardia a significant pathogen in production animals? ExpParasitol. 2010;124:98-106.
Giadinis N.D., Papadopoulos E., Lafi S.Q., Papanikolopoulou V., Karanikola S., Diakou A., Vergidis V., Xiao L., Ioannidou E., Karatzias H. Epidemiological Observations on Cryptosporidiosis in Diarrheic Goat Kids in Greece. Vet Med Int. 2015;2015:764193.
Gil H., Cano L., de Lucio A., Bailo B., de Mingo M.H., Cardona G.A., Fernández-Basterra J.A., Aramburu-Aguirre J., López-Molina N., Carmena D. Detection and molecular diversity of Giardia duodenalis and Cryptosporidium spp. in sheltered dogs and cats in Northern Spain. Infect Genet Evol. 2017;50:62-69.
Gómez-Muñoz M.T., Navarro C., Garijo-Toledo M.M., Dea-Ayuela M.A., Fernández-Barredo S., Pérez-Gracia M.T., Domínguez-Márquez M.V., Borrás R. Occurrence and genotypes of Giardia isolated from lambs in Spain. Parasitol Int. 2009;58(3):297-299.
Gómez-Muñoz M.T., Cámara-Badenes C., Martínez-Herrero Mdel C., Dea-Ayuela M.A., Pérez-Gracia M.T., Fernández-Barredo S., Santín M., Fayer R. Multilocus genotyping of Giardia duodenalis in lambs from Spain reveals a high heterogeneity. Res Vet Sci. 2012;93(2):836-842.
González-Díaz M., Urrea-Quezada A., Villegas-Gómez I., Durazo M., Garibay-Escobar A., Hernández J., Xiao L., Valenzuela O. Cryptosporidium canis in two Mexican toddlers. Pediatr Infect Dis J. 2016;35(11):1265-1266.
Guzman-Herrador B., Carlander A., Ethelberg S., Freiesleben de Blasio B., Kuusi M., Lund V., Löfdahl M., MacDonald E., Nichols G., Schönning C., Sudre B., Trönnberg L., Vold L., Semenza J.C., Nygård K. Waterborne outbreaks in the Nordic countries, 1998 to 2012. Euro Surveill. 2015;18:20.
Hadjichristodoulou C., Gkikas A., Pediatidis Y., Tselentis Y. Outbreak of giardiasis among English tourists in Crete. Lancet. 1998;351:65-66.
Halliez M.C., Buret A.G. Extra-intestinal and long term consequences of Giardia duodenalis infections. World J Gastroenterol. 2013;19(47):8974-8985.
Haralabidis S.T., Papazachariadou M.G., Koutinas A.F., Rallis T.S. A survey on the prevalence of gastrointestinal parasites of dogs in the area of Thessaloniki, Greece. J Helminthol. 1988;62(1):45-49.
Hardie R.M., Wall P.G., Gott P., Bardhan M., Bartlett L.R. Infectious diarrhoea in tourists staying in a resort hotel. Emerg Infect Dis. 1999;5:168-171.
Hinney B., Gottwald M., Moser J., Reicher B., Schäfer B.J., Schaper R., Joachim A., Künzel F. Examination of anonymous canine faecal samples provides data on endoparasite prevalence rates in dogs for comparative studies.Vet Parasitol. 2017;245:106-115.
Ibrahim M.A., Abdel-Ghany A.E., Abdel-Latef G.K., Abdel-Aziz S.A., Aboelhadid S.M. Epidemiology and public health significance of Cryptosporidium isolated from cattle, buffaloes, and humans in Egypt. Parasitol Res. 2016;115(6):2439-2448.
153
Kaupke A., Michalski M.M., Rzeżutka A. Diversity of Cryptosporidium species occurring in sheep and goat breeds reared in Poland. Parasitol Res. 2017a;116(3):871-879.
Kaupke A., Gawor J., Rzeżutka A., Gromadka R. Identification of pig-specific Cryptosporidium species in mixed infections using Illumina sequencing technology. Exp Parasitol. 2017b;182:22-25.
Kirk M.D., Pires S.M., Black R.E., Caipo M., Crump J.A., Devleesschauwer B., Döpfer D., Fazil A., Fischer-Walker C.L., Hald T., Hall A.J., Keddy K.H., Lake R.J., Lanata C.F., Torgerson P.R., Havelaar A.H., Angulo F.J. World Health Organization Estimates of the Global and Regional Disease Burden of 22 Foodborne Bacterial, Protozoal, and Viral Diseases, 2010: A Data Synthesis. PLoS Med. 2015;12(12):e1001921.
Kvac M., Hofmannova L., Ortega Y., Holubova N., Horcickova M., Kicia M., Hlaskova L., Kvetonova D., Sak B., McEvoy J. Stray cats are more frequently infected with zoonotic protists than pet cats. Folia Parasitol (Praha). 2017;64.
Lucio-Forster A., Griffiths J.K., Cama V.A., Xiao L., Bowman D.D. Minimal zoonotic risk of cryptosporidiosis from pet dogs and cats. Trends Parasitol. 2010;26:174-179.
Mahfouz M.E., Mira N., Amer S. Prevalence and genotyping of Cryptosporidium spp. in farm animals in Egypt. J Vet Med Sci. 2014;76:1569–1575.
Minetti C., Taweenan W., Hogg R., Featherstone C., Randle N., Latham S.M., Wastling J.M. Occurrence and diversity of Giardia duodenalis assemblages in livestock in the UK. Transbound Emerg Dis. 2014;61(6):e60-7.
Minetti C., Lamden K., Durband C., Cheesbrough J., Platt K., Charlett A., O'Brien S.J., Fox A., Wastling J.M. Case-Control study of risk factors for sporadic giardiasis and parasite assemblages in North West England. J Clin Microbiol. 2015;53(10):3133-40.
Oikarinen S., Tauriainen S., Viskari H., Simell O., Knip M. PCR inhibition in stool samples in relation to age of infants. J Clin Virol. 2009;44:211–221.
Ortuño A., Scorza V., Castellà J., Lappin M. Prevalence of intestinal parasites in shelter and hunting dogs in Catalonia, Northeastern Spain. Vet J. 2014;199(3):465-7.
Osman M., Bories J., El Safadi D., Poirel M.T., Gantois N., Benamrouz-Vanneste S., Delhaes L., Hugonnard M., Certad G., Zenner L., Viscogliosi E. Prevalence and genetic diversity of the intestinal parasites Blastocystis sp. and Cryptosporidium spp. in household dogs in France and evaluation of zoonotic transmission risk. Vet Parasitol. 2015;214(1-2):167-70.
Overgaauw P.A., van Zutphen L., Hoek D., Yaya F.O., Roelfsema J., Pinelli E., van Knapen F., Kortbeek L.M. Zoonotic parasites in fecal samples and fur from dogs and cats in The Netherlands. Vet Parasitol. 2009;163(1-2):115-22.
Painter J.E., Gargano J.W., Yoder J.S., Collier S.A., Hlavsa M.C. Evolving epidemiology of reported cryptosporidiosis cases in the United States, 1995-2012. Epidemiol Infect. 2016;144:1792-802.
Pallant L., Barutzki D., Schaper R., Thompson R.C. The epidemiology of infections with Giardia species and genotypes in well cared for dogs and cats in Germany. Parasit Vectors. 2015;8:2.
Panousis N., Diakou A., Papadopoulos E., Giadinis N., Karatzias H., Haralampidis S. Prevalence of Cryptosporidium infection in dairy farms with a history of calves’ diarrhoea. Cattle Pract. 2007;15:89–92.
Panousis N., Diakou A., Giadinis N., Papadopoulos E., Karatzias H., Haralampidis S. Prevalence of Cryptosporidium infection in sheep flocks with a history of lambs' diarrhoea. Rev Med Vet. 2008;159:528–531.
154
Paoletti B., Iorio R., Capelli G., Sparagano O.A., Giangaspero A. Epidemiological scenario of giardiosis in dogs from central Italy. Ann N Y Acad Sci. 2008;1149:371-4.
Paoletti B., Otranto D., Weigl S., Giangaspero A., Di Cesare A., Traversa D. Prevalence and genetic characterization of Giardia and Cryptosporidium in cats from Italy. Res Vet Sci. 2011;91(3):397-9.
Paoletti B., Traversa D., Iorio R., De Berardinis A., Bartolini R., Salini R., Di Cesare A. Zoonotic parasites in feces and fur of stray and private dogs from Italy. Parasitol Res. 2015;114(6):2135-41.
Paparini A., Gofton A., Yang R., White N., Bunce M., Ryan U.M. Comparison of Sanger and next generation sequencing performance for genotyping Cryptosporidium isolates at the 18S rRNA and actin loci. Exp Parasitol. 2015;151-152:21-7.
Papazahariadou M., Founta A., Papadopoulos E., Chliounakis S., Antoniadou-Sotiriadou K., Theodorides Y. Gastrointestinal parasites of shepherd and hunting dogs in the Serres Prefecture, Northern Greece. Vet Parasitol. 2007;148(2):170-3.
Piekarska J., Bajzert J., Gorczykowski M., Kantyka M., Podkowik M. Molecular identification of Giardia duodenalis isolates from domestic dogs and cats in Wroclaw, Poland. Ann Agric Environ Med. 2016;23(3):410-5.
Pijnacker R., Mughini-Gras L., Heusinkveld M., Roelfsema J., van Pelt W., Kortbeek T. Different risk factors for infection with Giardia lamblia assemblages A and B in children attending day-care centres. Eur J Clin Microbiol Infect Dis. 2016;35(12):2005-2013.
Robben S.R., le Nobel W.E., Döpfer D., Hendrikx W.M., Boersema J.H., Fransen F., Eysker M.E. Infections with helminths and/or protozoa in cats in animal shelters in the Netherlands. Tijdschr Diergeneeskd. 2004;129(1):2-6.
Robertson L.J., Gjerde B.K., Furuseth Hansen E. The zoonotic potential of Giardia and Cryptosporidium in Norwegian sheep: a longitudinal investigation of 6 flocks of lambs. Vet Parasitol. 2010;171(1-2):140-5.
Robinson G., Elwin K., Chalmers R.M. Unusual Cryptosporidium genotypes in human cases of diarrhea. Emerg Infect Dis. 2008;14(11):1800-2.
Roux K.H. Optimization and troubleshooting in PCR. PCR Methods Appl. 1995;4(5):S185-94.
Ryan U., Caccio S.M. Zoonotic potential of Giardia. Int J Parasitol. 2013;43:943-956.
Ryan U., Zahedi A., Paparini A. Cryptosporidium in humans and animals-a one health approach to prophylaxis. Parasite Immunol. 2016;38:535-47.
Santin M. Clinical and subclinical infections with Cryptosporidium in animals. N Z Vet J. 2013;61:1-10.
Santín M., Cortés Vecino J.A., Fayer R. A large scale molecular study of Giardia duodenalis in horses from Colombia.Vet Parasitol. 2013;196(1-2):31-6.
Scaramozzino P., Di Cave D., Berrilli F., D'Orazi C., Spaziani A., Mazzanti S., Scholl F., De Liberato C. A study of the prevalence and genotypes of Giardia duodenalis infecting kennelled dogs. Vet J. 2009;182(2):231-4.
Schrader C., Schielke A., Ellerbroek L., Johne R. PCR inhibitors - occurrence, properties and removal. J Appl Microbiol. 2012;113:1014–1026.
155
Simonato G., Frangipane di Regalbono A., Cassini R., Traversa D., Beraldo P., Tessarin C., Pietrobelli M. Copromicroscopic and molecular investigations on intestinal parasites in kenneled dogs.Parasitol Res. 2015;114(5):1963-1970.
Soares R., Tasca T. Giardiasis: an update review on sensitivity and specificity of methods for laboratorial diagnosis. J Microbiol Methods. 2016;129:98-102.
Sommer M.F., Beck R., Ionita M., Stefanovska J., Vasić A., Zdravković N., Hamel D., Rehbein S., Knaus M., Mitrea I.L., Shukullari E., Kirkova Z., Rapti D., Capári B., Silaghi C. Multilocus sequence typing of canine Giardia duodenalis from South Eastern European countries. Parasitol Res. 2015;114(6):2165-2174.
Sommer M.F., Rupp P., Pietsch M., Kaspar A., Beelitz P. Giardia in a selected population of dogs and cats in Germany-diagnostics, coinfections and assemblages. Vet Parasitol. 2018;249:49-56.
Sprong H., Cacciò S.M., van der Giessen J.W.; ZOOPNET networkand partners. Identification of zoonotic genotypes of Giardia duodenalis. PLoSNegl Trop Dis. 2009;3(12):e558.
Surl C.G., Jung B.D., Park B.K., Kim H.C. Resistance of Cryptosporidium parvum oocysts following commercial bleach treatment. Korean J Vet Res. 2011;51:101–105.
Sweeny J.P., Ryan U.M., Robertson I.D., Jacobson C. Cryptosporidium and Giardia associated with reduced lamb carcase productivity. Vet Parasitol. 2011;182(2-4):127-139.
Symeonidou I., Gelasakis A.Ι., Arsenopoulos K.V., Schaper R., Papadopoulos E. Regression models to assess the risk factors of canine gastrointestinal parasitism. Vet Parasitol. 2017;248:54-61.
Symeonidou I., Gelasakis A.I., Arsenopoulos K., Angelou A., Beugnet F., Papadopoulos E. Feline gastrointestinal parasitism in Greece: emergent zoonotic species and associated risk factors. Parasit Vectors. 2018;11:227.
Stantic-Pavlinic M., Xiao L., Glaberman S., Lal A.A., Orazen T., Rataj-Verglez A., Logar J., Berce I. Cryptosporidiosis associated with animal contacts. Wien Klin Wochenschr. 2003;115(3-4):125-127.
Tangtrongsup S., Scorza V. Update on the diagnosis and management of Giardia spp infections in dogs and cats. Top Companion Anim Med. 2010;25:155-162.
Thompson R.C.A., Olson M.E., Zhu G., Enomoto S., Abrahamsen M.S., Hijjawi N.S. Cryptosporidium and Cryptosporidiosis. Adv. Parasitol. 2005;59:77-158.
Thompson A.R.C., Palmer C.S., O’Handley R. The public health and clinical significance of Giardia and Cryptosporidium in domestic animals. Vet. J. 2008;177:18-25.
Thompson R.C.A. and Ash A. Molecular epidemiology of Giardia and Cryptosporidium infections. Infect Genet Evol. 2016;40:315-323.
Thomson S., Hamilton C.A., Hope J.C., Katzer F., Mabbott N.A., Morrison L.J., Innes E.A. Bovine cryptosporidiosis: impact, host-parasite interaction and control strategies. Vet Res. 2017;48(1):42.
Traversa D., Otranto D., Milillo P., Latrofa M.S., Giangaspero A., Di Cesare A., Paoletti B. Giardia duodenalis sub-assemblage of animal and human origin in horses. Infect Genet Evol. 2012;12:1642–1646.
Tysnes K., Gjerde B., Nødtvedt A., Skancke E. A cross-sectional study of Tritrichomonas foetus infection among healthy cats at shows in Norway. Acta Vet Scand. 2011;53:39.
156
Tysnes K.R., Skancke E., Robertson L.J. Subclinical Giardia in dogs: a veterinary conundrum relevant to human infection. Trends Parasitol. 2014;30(11):520-527.
Tzanidakis N., Sotiraki S., Claerebout E., Ehsan A., Voutzourakis N., Kostopoulou D., Stijn C., Vercruysse J., Geurden T. Occurrence and molecular characterization of Giardia duodenalis and Cryptosporidium spp. in sheep and goats reared under dairy husbandry systems in Greece. Parasite. 2014;21:45.
Upjohn M., Cobb C., Monger J., Geurden T., Claerebout E., Fox M. Prevalence, molecular typing and risk factor analysis for Giardiaduodenalis infections in dogs in a central London rescue shelter. Vet Parasitol. 2010;172(3-4):341-346.
Utsi L., Smith S.J., Chalmers R.M., Padfield S. Cryptosporidiosis outbreak in visitors of a UK industry-compliant petting farm caused by a rare Cryptosporidium parvum subtype: a case-control study. Epidemiol Infect. 2016;144:1000-1009.
Veronesi F., Passamonti F., Caccio S., Diaferia M., Fioretti D.P. Epidemiological survey on equine Cryptosporidium and Giardia infections in Italy and molecular characterization of isolates. Zoonoses Public Health. 2010;57:510-517.
Vermeulen L., Benders J., Medema G., Hofstra N. Global Cryptosporidium loads from livestock manure. Environ Sci Technol. 2017;51:8663-8671.
Wang R., Zhang X., Zhu H., Zhang L., Feng Y., Jian F., Ning C., Qi M., Zhou Y., Fu K., Wang Y., Sun Y., Wang Q., Xiao L. Genetic characterizations of Cryptosporidium spp and Giardia duodenalis in humans in Henan, China. Exp Parasitol. 2011;127:42-45.
Wang L., Xiao L., Duan L., Ye J., Guo Y., Guo M., Liu L., Feng Y. Concurrent infections of Giardia duodenalis, Enterocytozoon bieneusi, and Clostridium difficile in children during a cryptosporidiosis outbreak in a pediatric hospital in China. PloS Negl Trop Dis. 2013;7(9):e2437.
Wang H., Zhao G., Chen G., Jian F., Zhang S., Feng C., Wang R., Zhu J., Dong H., Hua J., Wang M., Zhang L. Multilocus genotyping of Giardia duodenalis in dairy cattle in Henan, China. PLoS One. 2014;9(6):e100453.
Wang X.T., Wang R.J., Ren G.J., Yu Z.Q., Zhang L.X., Zhang S.Y., Lu H., Peng X.Q., Zhao G.H. Multilocus genotyping of Giardia duodenalis and Enterocytozoon bieneusi in dairy and native beef (Qinchuan) calves in Shaanxi province, northwestern China. Parasitol Res. 2016;115:1355–1361.
Xiao L., Fayer R. Molecular characterisation of species and genotypes of Cryptosporidium and Giardia and assessment of zoonotic transmission. Int J Parasitol. 2008;38(11):1239-1255.
Xiao L., Hlavsa M.C., Yoder J., Ewers C., Dearen T., Yang W., Nett R., Harris S., Brend S.M., Harris M., Onischuk L., Valderrama A.L., Cosgrove S., Xavier K., Hall N., Romero S., Young S., Johnston S.P., Arrowood M., Roy S., Beach M.J. Subtype analysis of Cryptosporidium specimens from sporadic cases in Colorado, Idaho, New Mexico, and Iowa in 2007: widespread occurrence of one Cryptosporidium hominis subtype and case history of an infection with the Cryptosporidium horse genotype. J Clin Microbiol. 2009;47(9):3017-3020.
Xiao L. Molecular epidemiology of cryptosporidiosis: an update. ExpParasitol. 2010;124:80-89.
Xu H., Jin Y., Wu W., Li P., Wang L., Li N., Feng Y., Xiao L. Genotypes of Cryptosporidium spp., Enterocytozoon bieneusi and Giardia duodenalis in dogs and cats in Shanghai, China. Parasit Vectors. 2016;9:121.

157
Yong T.S., Park S.J., Hwang U.W., Yang H.W., LeeK W., Min D.Y., Rim H.J., Wang Y., Zheng F. Genotyping of Giardia lamblia isolates from humans in China and Korea using ribosomal DNA Sequences. J Parasitol. 2000;86(4):887-891.
Zanzani S.A., Gazzonis A.L., Scarpa P., Berrilli F., Manfredi M.T. Intestinal parasites of owned dogs and cats from metropolitan and micropolitan areas: prevalence, zoonotic risks, and pet owner awareness in northern Italy. Biomed Res Int. 2014;2014:696508.

Summary
160
Giardia spp and Cryptosporidium spp are two important parasitic protozoa which affect various hosts,
including humans. Globally, about 280,000 human cases of giardiosis and 748,000 cases of
cryptosporidiosis are reported every year. The fact that these two protozoa are widespread and
abundant not only in the developing world but also in developed countries, together with their
implication in several disease outbreaks and their zoonotic potential, urged us to study their prevalence
and transmission scenarios in Greece, and specifically in a region that has not previously been
investigated. Selection of Crete island as the study area was based on its high human population density
and the large numbers of companion animals and livestock who share the same restricted environment
and thus would enable us to better investigate the transmission dynamics of the two parasites.
Chapter 1 provides a review of the published literature on some important points and current data
regarding Giardia and Cryptosporidium. This chapter describes the biology of the parasites, their impact
on human and animal health (horses, dogs, cats, livestock), their epidemiology and their zoonotic
character, as well as ways of prevention and control of their transmission.
In Chapter 2, we evaluated the presence of Giardia and Cryptosporidium in foals between the age of 1
week and 6 months in Belgium, The Netherlands, Germany and Greece using a quantitative direct
immunofluorescence assay (IFA). Positive samples were genotyped, based on the 18S ribosomal DNA
gene and the heat shock protein (HSP70) gene for Cryptosporidium and on the β-giardin gene and the
triose phosphate isomerase (TPI) gene for Giardia. In total, 134 foals from Belgium, 44 foals from The
Netherlands, 30 foals from Germany and 190 foals from Greece were examined. No Cryptosporidium
oocysts were identified in faecal samples from foals in Germany and The Netherlands. In Belgium and
Greece, 4.5% and 1.1% of the foals examined were Cryptosporidium positive, respectively, all with a low
oocyst excretion ranging from 100 to 2450 oocysts per gram of faeces. For Giardia, 14.2%, 11.4%, 10.0%
and 11.6% of the foals in Belgium, The Netherlands, Germany and Greece, respectively, were found to
excrete cysts, with a range of 50 up to 4,000,000 cysts per gram of faeces. Younger animals secreted
significantly more Giardia cysts than older horses (p<0.05), but no significant correlation between
Giardia infection and diarrhoea was observed. Most Giardia positive samples belonged to assemblage AI
and/or BIV, but also assemblage E was detected in two samples. Together with the identification of
Cryptosporidium horse genotype, this suggests only a low risk for zoonotic transmission.
Chapter 3 focused on the occurrence of intestinal parasites in different dog and cat populations in Crete,
Greece. Also, our objectives were to estimate the zoonotic potential and to identify risk factors
associated with parasite infections. Faecal samples were collected from 879 shelter, household and
161
shepherd dogs as well as 264 shelter and household cats. The samples were analysed using
sedimentation/flotation techniques for helminth eggs and coccidian oocysts, whereas Giardia and
Cryptosporidium were detected by IFA. Besides, PCR and sequencing were performed to evaluate the
zoonotic potential of Giardia and Cryptosporidium positive samples. High levels of parasitism in both
dogs and cats were recorded. Giardia was the most prevalent parasite in all dog and cat populations
except for shepherd dogs. In dogs, the overall prevalence was 25.2% (CI: 22.4-28.1) for Giardia spp; 9.2%
(CI: 7.3-11.1) for Ancylostoma/Uncinaria spp; 7.6% (CI: 5.9-9.4) for Toxocara spp; 5.9% (CI: 4.4-7.5) for
Cryptosporidium spp; 4.6% (CI: 3.2-5.9) for Cystoisospora spp; 2.7% (CI: 1.7-3.8) for Toxascaris leonina;
1.7% (CI: 0.9-2.6) for Capillaria spp; 0.8% (CI: 0.2-1.4) for taeniid eggs; 0.2% (CI: 0-0.5) for Dipylidium
caninum and 0.1% (CI: 0-0.3) for Strongyloides stercoralis. In cats, the prevalence was 20.5% (CI: 15.6-
25.3) for Giardia spp; 9.5% (CI: 5.9-13.0) for Cystoisospora spp; 8.3% (CI: 5.0-11.7) for Toxocara spp;
7.6% (CI: 4.4-10.8) for Ancylostoma/Uncinaria spp; 6.8% (CI: 3.8-9.9) for Cryptosporidium spp.; 4.2% (CI:
1.8-6.6) for Capillaria spp; 0.8% (CI: 0-1.8) for taeniid eggs; and 0.4% (CI: 0-1.1) for
Hammondia/Toxoplasma. Concerning the risk factors evaluated, there was a negative association
between age and Giardia infection and between age and T. leonina infection intensity for dogs.
Sequencing results revealed the presence of mainly animal-specific G. duodenalis assemblages C and D
in dogs and assemblages F, C and BIV-like in cats, with only a limited number of (co-)infections with
assemblage A. However, regarding cats, since the zoonotic assemblage A was identified exclusively at
the conserved 18 SSU-rRNA locus while assemblage F was detected only at other loci even in the same
samples, we cannot exclude the possibility that the isolated assemblage A is in fact assemblage F. As for
Cryptosporidium, the dog-specific C. canis and the pig-specific C. scrofarum were detected in dogs and
the cat-specific C. felis was detected in cats. Genotyping results suggest a limited zoonotic risk of Giardia
and Cryptosporidium infections from dogs and cats in Crete. Taeniid eggs were more prevalent in
shepherd dogs, suggesting access to offal and posing a threat for cystic echinococcosis transmission.
Infection rates of Toxocara spp in both dogs and cats show that companion animals could be a
significant source of roundworm infection to humans.
In Chapter 4, our aim was to study the presence of intestinal human parasitic infections and to identify
the potential source of contamination in two different areas of Greece (Makedonia and Crete). In total,
876 stool samples were collected from 822 adults and 54 children. Ιmmunofluorescence was used for
the detection of Giardia and Cryptosporidium, whereas sedimentation (acid/ether) and
concentration/flotation techniques were performed to detect other intestinal parasites. PCR followed by
sequencing was applied to genotype Giardia and Cryptosporidium positive samples. Thirty-seven (4.5%)

162
of the individuals examined harboured at least one species of intestinal parasite, the majority of which
were protozoa (3.8%). The specific species found were Blastocystis hominis (1.8%), G. duodenalis (1.3%),
Cryptosporidium spp (0.6%), Entamoeba coli (0.2%) and E. histolytica (0.1%). As helminths concerns, 2
people were positive for Enterobius vermicularis, 1 for Taenia spp and 1 for Trichostrongylidae.
Genotyping results revealed the presence of G. duodenalis sub-assemblage AII, whereas sequencing was
not successful for Cryptosporidium positive samples. A novel multi-locus genotype of G. duodenalis was
identified, which has not been described in humans or animals previously. Overall, οccurence of
intestinal parasites in humans was low and similar to previously published data, suggesting that current
socioeconomic changes (increased migration and tourism) had no major impact on parasitism in the
studied area. As regards clinical relevance of all parasitic species detected in this study as well as any
indication of potential sources of infection and risk factors no safe associations to those infections could
be made since the limited number of positive samples did now allow us to draw any statistically
significant conclusion. Based on the parasite species and genotypes detected, there was no indication
that animals were an important source of infection.
In Chapter 5, data presented in this thesis are discussed and compared with similar recently published
studies in the study area and beyond. Overall, prevalence data seem to be consistent with a common
epidemiological scenario in which G. duodenalis and Cryptosporidium spp are abundant in a wide range
of domesticated animals including horses, ruminants, dogs and cats. Prevalence rates of infection in
dogs and cats are high but vary depending on the population, with kennelled animals presenting with
higher infection rates. Humans are also infected but in much lower rates. The potential of a zoonotic
transmission of all animal’s species to humans, especially to what Giardia regards, seems to be weak
since in most of animals and human cases genotype analyses showed infection by the host-specific
isolates. However, since there were cases where animals harboured potentially zoonotic
assemblages/sub-assemblages of Giardia, the above statement (although resonates with and coheres to
current facts) should be further validated in the future by using novel approaches and new generation
molecular tools.
Samenvatting
164
Giardia spp en Cryptosporidium spp zijn twee belangrijke parasitaire protozoa, die een groot aantal
verschillende diersoorten kunnen infecteren, waaronder ook de mens. Wereldwijd worden jaarlijks
ongeveer 280.000 gevallen van humane giardiose en 748.000 gevallen van cryptosporidiose
gerapporteerd. De wijde verspreiding van deze twee parasieten in zowel ontwikkelingslanden als
ontwikkelde landen, hun regelmatige betrokkenheid bij ziekte-uitbraken en hun zoönotisch potentieel
waren de aanleiding om het voorkomen en de transmissie van Giardia en Cryptosporidium te
bestuderen in Griekenland, een land waar weinig data over de transmissie van Giardia en
Cryptosporidium beschikbaar waren. Het eiland Kreta werd uitgekozen als studiegebied, omdatde hoge
bevolkingsdichtheid, de grote mobiliteit (toeristen en migranten) en het grote aantal gezelschapsdieren
en landbouwdieren in een afgebakend gebied, een geschiktesituatie creëert om de transmissie van
Giardia en Cryptosporidium te bestuderen.
Hoofdstuk 1 geeft een overzicht van de wetenschappelijke literatuur in verband met enkele belangrijke
aspecten van Giardia en Cryptosporidium infecties. Achtereenvolgens wordt de biologie van de
parasieten, hun medisch en veterinair belang, de epidemiologie en hun zoönotisch karakter besproken,
gevolgd door de behandeling en mogelijke preventieve maatregelen om de verspreiding ervan tegen te
gaan.
In hoofdstuk 2 werdhet voorkomen van Giardia en Cryptosporidium onderzocht bij veulens van 1 week
tot 6 maanden oud in België, Nederland, Duitsland en Griekenland, met behulp van een kwantitatieve
directe immunofluorescentietest (IFT). Positieve mestmonsters werden gegenotypeerd met PCR, waarbij
het 18S rRNA genen het‘heat shock protein’ (HSP70) gen werden gebruikt voor Cryptosporidium en het
β-giardine genen het triose phosphate isomerase (TPI) gen voor Giardia. In totaal, werden 134 veulens
bemonsterd in België, 44 in Nederland, 30 in Duitsland en 190 in Griekenland, waarvan 45 in Kreta. In
mestmonsters uit Duitsland en Nederland werd geen Cryptosporidium gevonden. In België en
Griekenland waren respectievelijk 4,5% en 1,1% van de veulens positief voor Cryptosporidium, zij het
met een lage oöcysten-uitscheiding, tussen 100 en 2450 oöcysten per gram feces (OPG). Giardia cysten
werden teruggevonden bij 14,2%, 11,4%, 10,0% en 11,6% van de veulens in respectievelijk België,
Nederland, Duitsland en Griekenland, waarbij tussen de 50 en 4.000.000 cysten per gram feces (CPG)
werden geteld. Jongere dieren scheidden significant meer Giardia cysten uit dan oudere veulens
(p<0.05), maar er werd geen correlatie gevonden tussen Giardia infectie en de aanwezigheid van
diarree. De meeste Giardia isolaten behoorden tot assemblage AI en/of BIV, maar ook het assemblage E,
dat specifiek is voor landbouwdieren, werd in twee monsters aangetroffen. Samen met de identificatie
165
van het Cryptosporidium ‘horse genotype’ wijzen deze resultaten op een beperkt risico voor zoönotische
transmissie van paard naar mens.
Hoofdstuk 3 focust op de aanwezigheid van darmparasieten in verschillende honden- en
kattenpopulaties in Kreta. Naast het inschatten van de prevalentie werd ook getracht van het zoönotisch
potentieel van deze infecties in te schatten en van risicofactoren te identificeren die met de infecties
geassocieerd zijn. Stoelgang werd verzameld van 879 honden (asielhonden, huishonden en
herdershonden) en 264 katten (asiel- en huiskatten). De monsters werden onderzocht op aanwezigheid
van wormeieren en oöcysten van coccidia met behulp van sedimentatie-flotatie technieken en met de
IFA voor Giardia en Cryptosporidium. Het zoönotisch potentieel van Giardia-en Cryptosporidium-
positieve monsters werd onderzocht met PCR en sequenering, waarbij dezelfde genen werden gebruikt
als in hoofdstuk 2. Er werd een hoge besmettingsgraad met darmparasieten gevonden bij zowel honden
als katten. Giardia was de meest voorkomende parasiet bij alle honden- en kattenpopulaties, behalve bij
herdershonden. In honden werden de volgende prevalenties gevonden: 25.2% (CI: 22.4-28.1) voor
Giardia spp; 9.2% (CI: 7.3-11.1) voor Ancylostoma/Uncinaria spp; 7.6% (CI: 5.9-9.4) voor Toxocara spp;
5.9% (CI: 4.4-7.5) voor Cryptosporidium spp; 4.6% (CI: 3.2-5.9) voor Cystoisospora spp; 2.7% (CI: 1.7-3.8)
voor Toxascaris leonina; 1.7% (CI: 0.9-2.6) voor Capillaria spp; 0.8% (CI: 0.2-1.4) voor Taenia-type eieren;
0.2% (CI: 0-0.5) voor Dipylidium caninumen 0.1% (CI: 0-0.3) voor Strongyloides stercoralis. In katten was
de prevalentie 20.5% (CI: 15.6-25.3) voor Giardia spp; 9.5% (CI: 5.9-13.0) voor Cystoisospora spp; 8.3%
(CI: 5.0-11.7) voor Toxocara spp; 7.6% (CI: 4.4-10.8) voor Ancylostoma/Uncinaria spp; 6.8% (CI: 3.8-9.9)
voor Cryptosporidium spp; 4.2% (CI: 1.8-6.6) voor Capillaria spp; 0.8% (CI: 0-1.8) voor Taenia-type eieren
en 0.4% (CI: 0-1.1) voor Hammondia/Toxoplasma. Betreffende de risicofactoren, werd een negatieve
associatie gevonden tussen leeftijd en Giardia infectie en tussen leeftijd en T. leonina infectiegraad bij
honden. PCR en sequenering toonde voornamelijk de diersoort-specifieke G. duodenalis assemblages C
en D aan bij honden en assemblages F, C en BIV-like bij katten, met slechts een beperkt aantal
(meng)infecties met het potentieel zoönotische assemblage A. Omdat assemblage A bij de katten enkel
werd gevonden met het geconserveerde 18 SSU-rRNA locus, terwijl in dezelfde mestmonsters alleen
assemblage F werd gevonden m.b.v. de andere loci, kan niet uitgesloten worden dat de assemblage A
isolaten in feite tot assemblage F behoorden. Voor Cryptosporidium werden bij honden enkel de
diersoort-specifieke species C. canis en C. scrofarum geïdentificeerd en bij katten de kat-specifieke C.
felis. Deze resultaten wijzen erop dat Giardia en Cryptosporidium infecties bij honden en katten in Kreta
slechts een heel beperkt zoönotisch risico met zich meebrengen. Taenia-type eieren werden veel
teruggevonden bij herdershonden, hetgeen aangeeft dat het voederen van slachtafval bij deze
166
hondenpopulatie een risico inhoudt voor transmissie van Echinococcus granulosus. De vrij hoge
prevalentie van Toxocara spp. bij honden en katten toont aan dat gezelschapsdieren een belangrijke
besmettingsbron kunnen zijn van spoelworminfecties voor de mens.
Het doel van hoofdstuk 4 was te onderzoeken welke darmparasieten voorkomen bij mensen in twee
verschillende gebieden in Griekenland (Macedonië en Kreta) en mogelijke besmettingsbronnen te
identificeren. In totaal werden 876 stoelgangmonsters verzameld van 822 volwassenen en 54 kinderen.
IFT werd gebruikt voor de detectie van Giardia en Cryptosporidium, terwijl een zuur/ether sedimentatie
techniek en een concentratie-flotatie techniek werden gebruikt om andere darmparasieten aan te
tonen. PCR en sequenering werden gebruikt om Giardia- en Cryptosporidium-positieve monsters te
genotyperen. Zevenendertig individuen (4,5%) waren besmet met minstens één soort darmparasieten,
waarvan de meerderheid (3,8%) protozoa waren: Blastocystis hominis (1.8%), G. duodenalis (1.3%),
Cryptosporidium spp (0.6%), Entamoeba coli (0.2%) en E. histolytica (0.1%). Genotypering van positieve
monsters bevestigde de aanwezigheid van G. duodenalis sub-assemblage AII. Een nieuw multi-locus
genotype van G. duodenalis werdgeïdentificeerd, dat nog niet eerder werd beschreven in mensen of
dieren. Genotypering was niet succesvol voor Cryptosporidium. Wat worminfecties betreft, waren twee
personen besmet met Enterobius vermicularis, 1 met Taenia spp en 1 met Trichostrongylidae. Over het
algemeen was de prevalentie van darmparasieten laag, en lijkt deze niet gestegen te zijn in vergelijking
met eerdere studies, wat erop wijst dat de gewijzigde socio-economische situatie (toegenomen
toerisme en migratie) geen grote impact heeft gehad op het risico voor besmetting met parasieten.
Door het kleine aantal positieve monsters konden geen significante verbanden aangetoond worden
tussen de aanwezigheid van parasieten en klinische symptomen of risicofactoren. Op basis van de
geïdentificeerde parasieten-species en genotypes is er geen indicatie dat dieren een belangrijke
besmettingsbron waren.
In hoofdstuk 5 worden de resultaten van de vorige hoofdstukken besproken in de context van de
recente literatuur. De bekomen prevalentiedata stemmen vrij goed overeen met andere studies die
aangeven dat Giardia en Cryptosporidium wijdverspreid zijn bij verschillende diersoorten. De prevalentie
bij gezelschapsdieren was vrij hoog, vooral bij dieren uit asielen. De lage prevalentie van Giardia en
Cryptosporidium bij mensen en de kleine proportie van zoönotische species/genotypes bij dieren, vooral
voor Giardia, wijzen echter op een beperkt belang van zoönotische transmissie van deze parasieten in
Kreta. Voor een volledige opheldering van de transmissiecycli is verder onderzoek nodig, waarbij gebruik
kan gemaakt worden van een nieuwe generatie moleculaire tools, zoals next generation sequencing, en
167
waarbij de rol van direct contact en voedings- of water-gerelateerde transmissie kan onderzocht
worden.

Acknowledgements
170
All this work would have not been successfully completed without the precious help of a number of
people.
First, I would like to thank from the bottom of my heart, both my promoters Prof. Edwin Claerebout and
Dr. Smaragda Sotiraki. Although thousands of miles far away, Prof. Edwin Claerebout’s presence was
active and constant all over the years. He was always next to me supporting me with patience and
kindness and encouranging me to accomplish my goals. Dr Smaragda Sotiraki, was the reason why I
started this journey and 100% supported me at every difficulty I met. She has been tough on me when
things were easy and more importantly she was going easy on me when things were tough. Edwin and
Smaro, you have been my mentors and you will continue to be for the rest of my professional life. I will
never forget how many times you were there for me.
My sincere gratitude goes also to the members of the examination committee: Dr. Alexandros
Stefanakis, Dr. Thomas Geurden, Prof. Sarah Gabriel and Prof. Pierre Dorny for their valuable and very
beneficial suggestions that helped improving the present dissertation.
I would also like to thank my colleagues from UGENT and especially Stijn Casaert for his constant help
and support.
My thanks also go to all the colleagues from the Veterinary Research Institute for providing me the best
work environment and support with special thanks to our parasitology group: Panagiota Ligda,
Dimitrios Arvanitis, Nikolaos Voutzourakis, Katerina Saratsi and Anastasios Saratsis. Thank you for
being great colleagues but mainly for being adorable friends.
Special thanks to Konstantina Antoniadou, Anastasios Anastasiadis, Dr. Ioannis Ignatiadis and all the
veterinarians and medical doctors for their precious help and collaboration. Also, thanks to Dr.
Theodosios Theodosiou and Dr. Nikolaos Mittas for their statistical support.
Of course, I attribute this thesis to my parents who were the reason why I become the person I am now.
I thank them for all of the sacrifices they have done for me. Also, I thank my sister, my brother, and my
grandparents for their support.





























