Embed Size (px)
Citation preview

J Neurol (2008) 255:311–313DOI 10.1007/s00415-008-0902-y JOURNAL CLUB
JON
2902
Prof. Dr. med. Michael Strupp (�)Dept. of NeurologyLudwig-Maximilians UniversityKlinikum GroßhadernMarchioninistr. 1581377 Munich, GermanyE-Mail: [email protected]
What the eyes tell us
No other motor system has been evaluated as carefully as eye move-ments. Thus, we have exceptionally detailed knowledge of the function of the ocular motor system and its pathologies. This also means that the analysis of eye movements is an excellent tool to evaluate a dysfunc-tion of the brain, in particular, since eye movements can be very pre-cisely measured. The first two arti-cles in this month’s Journal Club will focus on so-called saccadic oscilla-tions and impaired saccades and what we can learn from these eye movements. In the first article, a new familial disorder and syndrome, micro-saccadic oscillations and limb tremor, was described. The careful analysis of these eye move-ments and the tremor extends our knowledge of pathological oscilla-tions, which is also important for other movement disorders. In the second article, the combination of the measurement of voluntary-guided saccades and diffusion ten-sor MR imaging shows in patients with pre-symptomatic Huntington’s disease a selective vulnerability of white matter tracts from the frontal cortex to the caudate body. In the third and final article, a new clinical sign is described which helps to dif-ferentiate non-organic visual loss from an organic disorder: the “sun-glasses sign”.
Micro-saccadic oscillations and limb tremor
The pathophysiology of many tremor disorders, such as essential tremor, is so far not very well under-
stood. The same is true for tremor-like eye movements, so-called sac-cadic oscillations of the eye. These are back-to-back saccades without an intersaccadic interval that impair clear vision. Other examples of sac-cadic oscillations are ocular flutter and opsoclonus.
David Zee from Baltimore and John Leigh from Cleveland and their groups described a new disorder, which is characterised by the com-bination of saccadic oscillation and fine hand tremor, in a mother and daughter. They called this disorder familial micro-saccadic eye oscilla-tions and limb tremor. They care-fully analysed the eye movements and the tremor of the two patients. On the basis of these findings they also developed a model to explain these oscillations.
These two patients had suffered from occasional brief episodes of blurring of vision and hand tremor since early childhood. During oph-thalmoscopy both patients showed nearly continuous small-amplitude high-frequency oscillations of the eye. Eye movement recordings re-vealed nearly continuous small-am-plitude high-frequency saccadic os-cillations with a frequency of about 18 Hz around the horizontal, verti-cal and torsional axis. The frequency of the postural limb tremor was about 12 Hz.
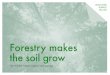
Based on current knowledge of the generation of saccades which in-volves three classes of neurons (ex-citatory burst neurons within the pontine paramedian reticular for-mation, inhibitory burst neurons, and omnidirectional pause neu-rons), the authors simulated a con-ductance-based model for the pre-motor commands of saccades (Figure). It is important to note that due to the physiological phenome-non of post-inhibitory rebound in premotor burst neurons this circuit is inherently unstable, which predis-poses to oscillations unless pre-vented by external inhibition.
To explain the saccadic oscilla-tions in the two subjects the authors carefully analysed the possible func-tion of ion channels of premotor burst neurons. They came up with the hypothesis that an impairment of the glycine receptor can alter membrane properties in a way that impairs inhibition of the inherently unstable neural circuit leading to eye and limb oscillations.
What do we learn from these findings for the pathophysiology of limb tremor? Two mechanisms are likely to be involved in limb tremor: olivo-cerebellar circuits and thal-amo-cortical circuits. After careful re-evaluation of our knowledge, the authors favoured a comparable cir-cuit for limb movements to that for eye movements: the globus pallidus internus has inhibitory GABAergic projections to the motor thalamus, which relays the output to the motor cortex (for references see Shaikh et al. 2007). Thalamic reticular neu-rons likely inhibit each other and the globus pallidus sends inhibitory projection to the thalamo-cortical and thalamic reticular neurons. Rel-evant inhibitory neurotransmitters are GABA and glycine. In conclu-sion, there are analogous neural cir-cuits for eye movements and limb movements.
Conclusions and Comments. The very astute combined clinical, bio-physical and computational ap-proach allows the conclusion that such a rare disorder has consider-able implications for our under-standing of the pathophysiology of different types of oscillations in other motor systems. The next step will be to look for mutations of the glycine and GABA receptor genes. In the long term new pharmacolog-ical tools for the treatment of such oscillations might be developed as a result of this research.
Shaikh AG et al. (2007) A new fa-milial disease of saccadic oscilla-tions and limb tremor provides
311_313_JC_2902_JON_02_08.indd 311311_313_JC_2902_JON_02_08.indd 311 18.02.2008 9:48:26 Uhr18.02.2008 9:48:26 Uhr

312
clues to mechanisms of common tremor disorders. Brain 130:3020–3031 (E-Mail: [email protected])
White matter connections reflect changes in voluntary-guided saccades in pre-symptomatic Huntington’s disease
Huntington’s disease is an autoso-mal dominant disorder caused by expanded CAG trinucleotide repeats in the huntingtin gene, which also allows pre-symptomatic diagnosis. Careful neuropsychological exami-nation and examination of eye movements and saccades reveals that carriers often develop minor symptoms before the real onset of the disease. These carriers are known as pre-symptomatic gene carriers. The minor symptoms and
changes have been attributed to de-generation of the striatum and fron-tal cortex. From a therapeutic point of view pre-symptomatic gene car-riers would be ideal candidates for disease-modifying treatments. Therefore, early identification will be crucial in the future.
Stefan Klöppel and co-workers from London combined two tech-niques to examine pre-symptomatic Huntington’s gene carriers. They used diffusion tensor MR imaging for fibre tracking and eye movement recordings to examine voluntary-guided saccades, in particular, sac-cadic latencies to determine vari-ability of voluntary-guided saccadic latency. They evaluated 25 pre-symptomatic gene carriers and 20 matched controls.
The major findings of this study were as follows: 1) Fibre tracking showed a reduction of frontal cor-
tico-fugal streamlines reaching the body of the caudate. 2) In the left hemispheres the authors found a negative correlation between years to estimated disease onset and streamlines from frontal cortex to the body of the caudate nucleus. Many of these fibres originate from the frontal eye fields, which are par-ticularly important for the control of voluntary saccades. 3) Correla-tion analysis showed that those sub-jects with greater impairment of voluntary-guided saccades had fewer fibres connecting the frontal cortex with the caudate body.
Conclusions and Comments. The authors very elegantly combined fully automated methods to explore white matter changes and particu-lar fibre tracts as well as functional measures such as voluntary sac-cades. At the end of their article, they point out that their method of applying diffusion tensor imaging can be tailored to any specific drugs under study and is therefore of real general importance. They also sug-gest that the next step might be a subject-specific localisation of the frontal eye fields by means of func-tional MRI, which will yield greater sensitivity for the detection of changes in the connecting fibre tracts. Finally, a long-term follow-up study should be carried out to further evaluate the sensitivity of these biomarkers.
Klöppel S et al. (2008) White matter connections reflect changes in vol-untary-guided saccades in presymp-tomatic Huntington’s disease. Brain 131:196–204 (E-Mail: [email protected])
The “sunglasses sign” predicts nonorganic visual loss in neuro-ophthalmologic practice
Nonorganic visual loss is still a di-agnostic challenge and every aid to making this diagnosis is warranted. Based on single observations Bengt-zen and co-workers from Atlanta
Fig. (A) Brain stem circuit for controlling horizontal saccades. The premotor neurons are located in the pons and rostral medulla. The excitatory burst neurons (EBN) project to the ipsilateral abducens nucleus that contains in-terneurons (IN) and motor neurons (AB) that relay excitation to neurons innervating the agonist muscles (green) and also to the region of the ipsilateral IBN. Axons of the IBN cross the midline and project to the contralateral internuclear (IN) and abducens motoneurons (AB) innervating antagonist muscles (red), and to the region of the contralateral excitatory and inhibitory burst neurons (red). When a rightward saccade is called for, the axons from right EBN carry impulses to excite motoneurons (or relay interneurons (IN)) innervating the agonist muscles ro-tating the eyes to the right (green). At the same time, right IBN inhibit the antagonist muscles rotating the eyes to the left (red). The mutual inhibition between the burst neurons across the midline predisposes the neural circuit to instability and can lead to saccadic oscillations (uncalled for back-to-back saccades). (B and C) Demonstration of oscillations in a two-neuron circuit. Neuron-A inhibits neuron-B and vice versa. A small pulse (physiologically evoked, e.g. by a tiny spontaneous saccade) to neuron-A increases its discharge and thus inhibits neuron-B. Once the discharge of the neuron drops (at the end of the pulse) inhibition from neuron-B is removed. This results in a rebound increase in the neuron-B firing rate. Since neuron-B also inhibits neuron-A, the same phenomenon of post-inhibitory rebound repeats for neuron-A (from Shaikh AG et al. (2007))
311_313_JC_2902_JON_02_08.indd 312311_313_JC_2902_JON_02_08.indd 312 18.02.2008 9:48:26 Uhr18.02.2008 9:48:26 Uhr

313
systematically evaluated whether wearing sunglasses (the “sunglasses sign”) helps to predict nonorganic visual loss. Such a sign would be similar to a finding published in 2003 in Neurology on patients with nonepileptic psychogenic events who very often brought a teddy bear with them to the hospital.
Bengtzen and co-workers pro-spectively analysed data on all new patients who came to their Neuro-ophthalmology Unit over 13 months. In particular, they noted whether the patients were wearing sunglasses in the clinic.
The major findings of this study were as follows: 1) Of the 1377 con-secutive new patients 34 wore sun-glasses; 7 of them had organic visual loss. 2) Of the 59 patients who were diagnosed with nonorganic visual
loss 27, i.e. 45.8 %, wore sunglasses. 3) Statistical analysis revealed that the sensitivity of wearing sunglasses for nonorganic visual loss was 0.46. The probability that a patient had nonorganic visual loss was 0.043 but it increased to 0.79 in patients with sunglasses. That means the specific-ity of sunglasses for the diagnosis of nonorganic visual loss was 0.995. 4) Further evaluation revealed that at least one of the following character-istics was found in 26 of the 27 pa-tients with nonorganic visual loss who wore sunglasses: highly posi-tive review of systems, workers’ compensation claim, disability, and lawsuit.
Conclusions and Comments. This very simple approach based on pre-vious clinical experience and care-ful collection of information and
statistical analysis revealed that such a simple observation as whether the patients were wearing sunglasses has a very high specific-ity for the diagnosis of nonorganic visual loss. This should therefore be included in our current clinical knowledge. If the authors had also included the finding that women present almost three times more of-ten with nonorganic visual loss than men, as was also clearly demon-strated in this study, their factual analysis would have been even more helpful.
Bengtzen R et al. (2008) The “sun-glasses sign” predicts nonorganic visual loss in neuro-ophthalmologic practice. Neurology 70:218–221 (E-Mail: [email protected])
311_313_JC_2902_JON_02_08.indd 313311_313_JC_2902_JON_02_08.indd 313 18.02.2008 9:48:26 Uhr18.02.2008 9:48:26 Uhr