Embed Size (px)
Citation preview

What Cons*tutes “Nephrology Clearance”?
Oscar Naidas, MD Frederick Ogbac, MD
What he will say ... • Nephrology Clearance vs Nephrology Risk Stra=fica=on / Assessment and Management
• Composi=on of “Nephrology Clearance” – Pre employment “Nephrology Clearance” – CT-‐Scan with IV contrast – Coronary angiography or PCI – General Surgery – MRI with gadolinium contrast
Define Nephrology Clearance vs Risk Stra*fica*on / Assessment and its Management
• Defini=on of Clearance ( ) “Official authoriza.on for something to proceed or take place”
• Example: “Do not schedule the pa.ent for CT Scan of the abdomen with IV contrast un.l you are given clearance by the nephrologist”
Oxford Advance Learner’s Dic5onaries

Composi*on of a Nephrology Risk Assessment and Management
• Type of poten=al ischemic / nephrotoxic insult • Assessment of risk factors of the pa=ent • An es=mate of the risk (quan=ta=ve or semi-‐quan=ta=ve)
• Management / interven=on to reduce risk • Risk vs Benefit • Communica=on with the referring physician and/or the pa=ent

The seafarer with chronic GN

The seafarer with chronic GN
35 M, asymptoma=c, BP:140/90mmHg, Ht 5’7”, Wt 70 kg, Urine rbc 10-‐15/hpf, prot trace
(UPCR 0.6) Scr 1.4mg/dl (eGFR 68ml/min) US KUB(-‐)
LPD, Losartan (130/80mmHg), UPCR 0.3 Ffup q 6 mos for 3 years, stable

The seafarer with chronic GN
Asymptoma=c, BP 130/80mmHg, Ht 5’7”, Wt 70 kg,no edema, Urine rbc 15-‐20/hpf, protein(-‐) ACR 110 mg/g
Scr 1.5mg/dl (eGFR 62ml/min) US KUB(-‐)

The seafarer with chronic GN
Chronic GN probably IgAN

The seafarer with chronic GN
Chronic GN probably IgAN, CKD G2A2 (moderate risk of progression)

The seafarer with chronic GN
• No indica=on for kidney biopsy, stable for past 3 yrs,
• LPD and Losartan 50mg OD (<BP130/80mmHg ), slows the fall in GFR to 3ml/min/yr


The seafarer with chronic GN
• No indica=on for kidney biopsy, stable for past 3 yr
• LPD and Losartan 50mg OD (<BP130/80mmHg ), slows the fall in GFR to 3ml/min/yr (62ml/min to 59ml/min)
• Low risk of progression of CKD • Low probability of progression of CKD that
will require hospitaliza=on or dialysis within next 9 to 12 months
• Repeat BP, Scr, UPCR ager 9 to 12 months

Pa*ent w/ CKD will undergo CT Scan w/ IV contrast
• 56 F, DM2, HTN, HF symptoms • Insulin 10u SQ OD • Telmisartan 40mg OD, Metoprolol 50mg BID • BP: 130/90 mmHg Wt: 60kg Ht: 5’1” • SCr 1.5 (eGFR 38.5 ml/min) Uprot: +2 • Chronic abdominal pain • US pancrea=c mass? • Will undergo whole abdomen CT-‐Scan with contrast
• Referred for “Nephrology Clearance”


(38.5 ml/min)
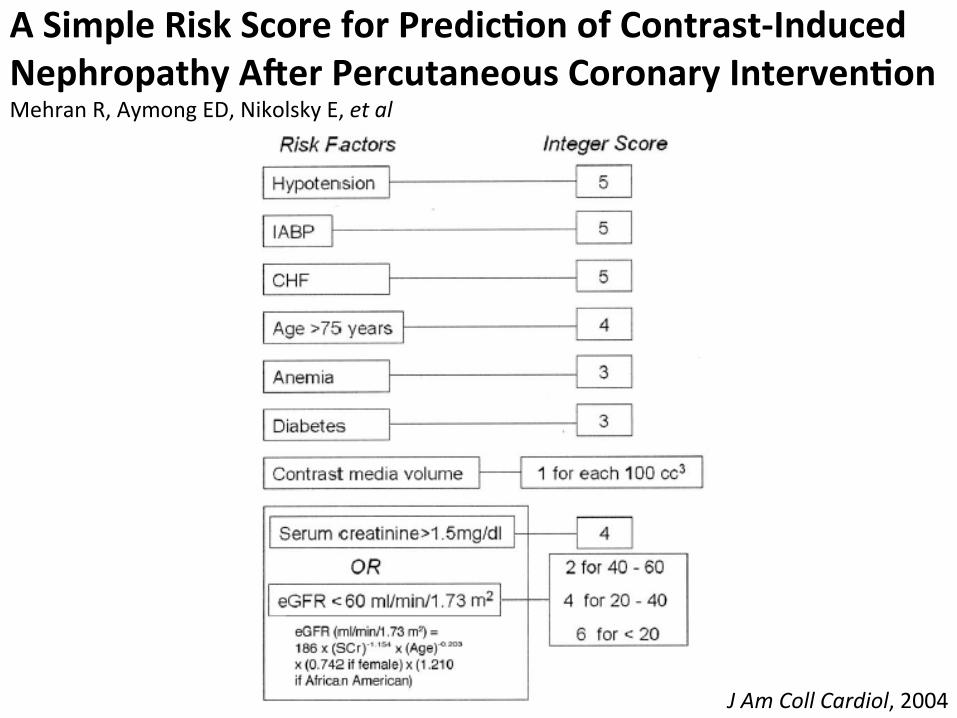
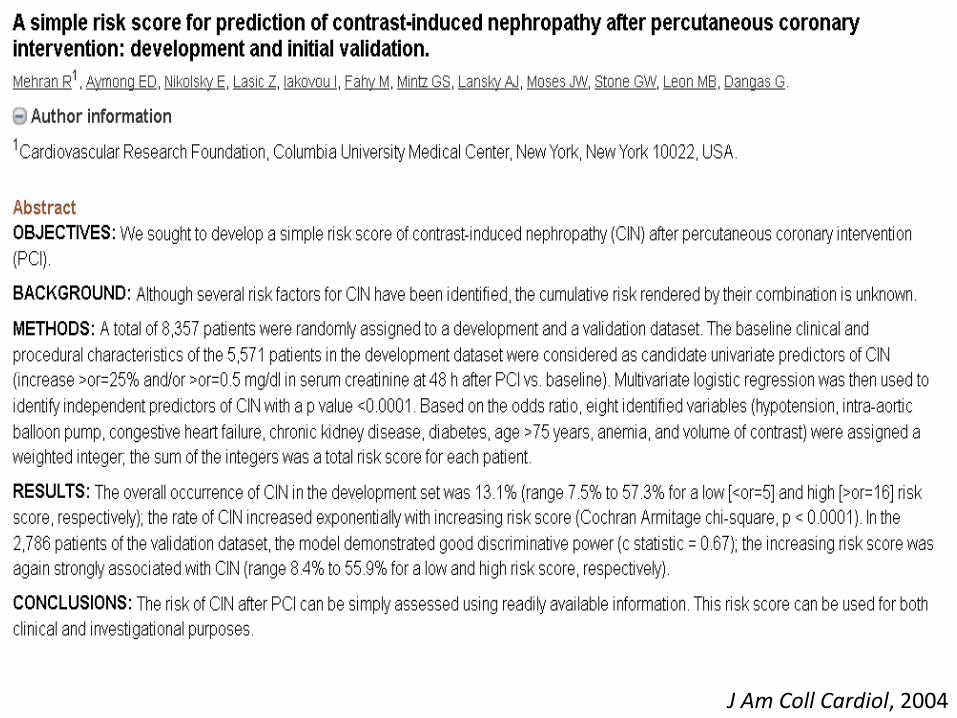
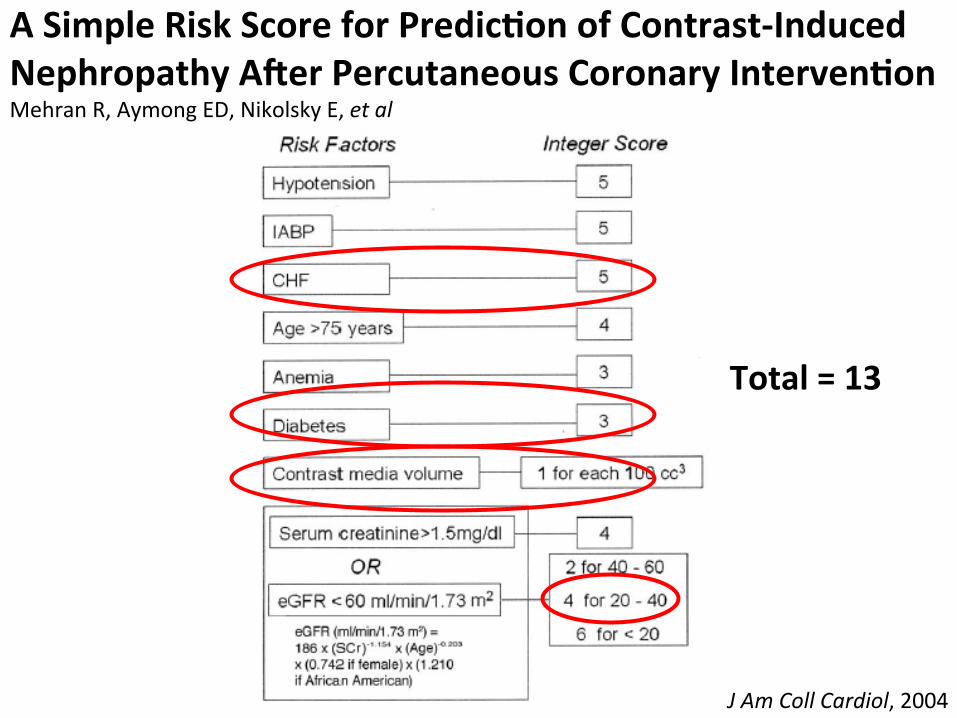
A Simple Risk Score for Predic*on of Contrast-‐Induced Nephropathy ARer Percutaneous Coronary Interven*on Mehran R, Aymong ED, Nikolsky E, et al
J Am Coll Cardiol, 2004

Total = 13
A Simple Risk Score for Predic*on of Contrast-‐Induced Nephropathy ARer Percutaneous Coronary Interven*on Mehran R, Aymong ED, Nikolsky E, et al
J Am Coll Cardiol, 2004

Risk Score Risk of CIN (%) Risk of Dialysis (%) < 5 7.5 0.04
6 to 10 14 0.12 11 to 16 26.1 1.09 > 16 57.3 12.6
Total = 13
A Simple Risk Score for Predic*on of Contrast-‐Induced Nephropathy ARer Percutaneous Coronary Interven*on Mehran R, Aymong ED, Nikolsky E, et al
J Am Coll Cardiol, 2004
Low Mod
Mod
High

Risk Score Risk of CIN (%) Risk of Dialysis (%) < 5 7.5 0.04
6 to 10 14 0.12 11 to 16 26.1 1.09 > 16 57.3 12.6
Total = 13
A Simple Risk Score for Predic*on of Contrast-‐Induced Nephropathy ARer Percutaneous Coronary Interven*on Mehran R, Aymong ED, Nikolsky E, et al
J Am Coll Cardiol, 2004
Low Mod
Mod
High

Am J Cardiol, 2006

Risk Predic*on of Contrast-‐Induced Nephropathy McCullough PA, Adam A, Becker CR, et al
Am J Cardiol, 2006

Risk Predic*on of Contrast-‐Induced Nephropathy McCullough PA, Adam A, Becker CR, Davidson C, Lameire N, Stacul F, Tumlin J, CIN Consensus Working Panel
Am J Cardiol, 2006

Individualizing risk management STEPS HOW TO DO IT
STEP 1 Es=mate your pa=ent’s risk for an event (CI AKI) without treatment (Rc)
56F, stable CKD G3bA3,DM2,HF will undergo abdominal CT w IV contrast with a risk of CI AKI 26% (MODERATE RISK)





Individualizing risk management STEPS HOW TO DO IT
STEP 1 Es=mate your pa=ent’s risk for an event (CI AKI) without treatment (Rc)
56F, stable CKD G3bA3,DM2,HF will undergo abdominal CT w IV contrast with a risk of CI AKI 26% (MODERATE RISK)
STEP 2 Es=mate the RR using the study result


Individualizing risk management STEPS HOW TO DO IT
STEP 1 Es=mate your pa=ent’s risk for an event (CI AKI) without treatment (Rc)
56F, stable CKD G3bA3,DM2,HF will undergo abdominal CT w IV contrast with a risk of CI AKI 26% (MODERATE RISK)
STEP 2 Es=mate the RR using the study result
Saline hydra=on+ NAC, reduces the risk of CI AKI RR = 0.68

Individualizing risk management STEPS HOW TO DO IT
STEP 1 Es=mate your pa=ent’s risk for an event (CI AKI) without treatment (Rc)
56F, stable CKD G3bA3,DM2 will undergo abdominal CT w IV contrast with a risk of CI AKI 26% (MODERATE RISK)
STEP 2 Es=mate the RR using the study result
Saline hydra=on+ NAC, reduces the risk of CI AKI RR = 0.68
STEP 3 Es=mate your individual pa=ent’s risk for an event (CI AKI)with treatment
Rt = Rc x RR = 26% x 0.68 = 18%

Individualizing risk management STEPS HOW TO DO IT
STEP 1 Es=mate your pa=ent’s risk for an event (CI AKI) without treatment (Rc)
56F, stable CKD G3bA3,DM2,HF will undergo abdominal CT w IV contrast with a risk of CI AKI 26% (MODERATE RISK)
STEP 2 Es=mate the RR using the study result
Saline hydra=on+ NAC, reduces the risk of CI AKI RR = 0.68
STEP 3 Es=mate your individual pa=ent’s risk for an event (CI AKI) with treatment
Rt = Rc x RR = 26% x 0.68 = 18%
STEP 4 Es=mate the individualized ARR
ARR = Rc – Rt = 26% -‐ 18% = 8% (LOW RISK)

Composi=on of a Nephrology Risk Assessment and Management
• Type of poten=al ischemic/nephrotoxic insult CT Scan w IV contrast
• Assessment of risk factors of the pa=ent CKD eGFR 38ml/min DM2,HF
• An es=mate of the risk ( quan=ta=ve or semiquan=ta=ve ) CI AKI 26% (MODERATE RISK)
• Management/Interven=on to reduce risk Saline Hydra.on +NAC reduce risk to 8% (LOW RISK)
• Risk vs Benefit Confirma.on +/-‐ of pancrea.c mass with CT Scan w/ IV contrast outweighs LOW RISK of CI AKI
• Communica=on with the referring physician and/or the pa=ent
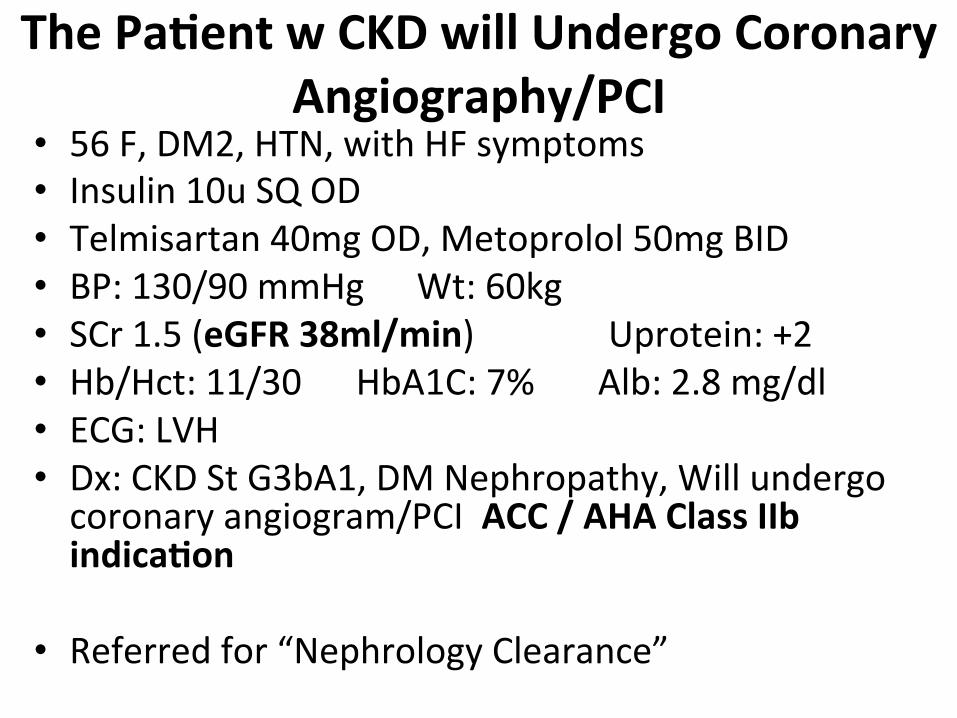
The Pa*ent w CKD will Undergo Coronary Angiography/PCI
• 56 F, DM2, HTN, with HF symptoms • Insulin 10u SQ OD • Telmisartan 40mg OD, Metoprolol 50mg BID • BP: 130/90 mmHg Wt: 60kg • SCr 1.5 (eGFR 38ml/min) Uprotein: +2 • Hb/Hct: 11/30 HbA1C: 7% Alb: 2.8 mg/dl • ECG: LVH • Dx: CKD St G3bA1, DM Nephropathy, Will undergo coronary angiogram/PCI ACC / AHA Class IIb indica*on
• Referred for “Nephrology Clearance”

Renal Risk Stra*fica*ons for CKD pa*ents prior to CA or PCI
• Mehran, et al. A simplified risk score for contrast-‐induced nephropathy ager percutaneous coronary interven=on. JACC, 2004.
• Tziakas, et al. Valida=on of a new risk score to predict contrast-‐induced nephropathy ager percutaneous coronary interven=on. Am J Cardiol, 2014.

Comparison of Renal Risk Stra*fica*ons for CKD pa*ents prior to CA or PCI
Index No. of variables
Score range
Mehran JACC 2004
8 0 – 34
Tziakas Am J Cardiol
2014
5 0 – 8
J Am Coll Cardiol, 2004

A Simple Risk Score for Predic*on of Contrast-‐Induced Nephropathy ARer Percutaneous Coronary Interven*on Mehran R, Aymong ED, Nikolsky E, et al
J Am Coll Cardiol, 2004
Total = 13
A Simple Risk Score for Predic*on of Contrast-‐Induced Nephropathy ARer Percutaneous Coronary Interven*on Mehran R, Aymong ED, Nikolsky E, et al
J Am Coll Cardiol, 2004

Risk Score Risk of CIN (%) Risk of Dialysis (%) < 5 7.5 0.04
6 to 10 14 0.12 11 to 16 26.1 1.09 > 16 57.3 12.6
Total = 13
A Simple Risk Score for Predic*on of Contrast-‐Induced Nephropathy ARer Percutaneous Coronary Interven*on Mehran R, Aymong ED, Nikolsky E, et al
J Am Coll Cardiol, 2004
Low Mod
Mod
High

Risk Score Risk of CIN (%) Risk of Dialysis (%) < 5 7.5 0.04
6 to 10 14 0.12 11 to 16 26.1 1.09 > 16 57.3 12.6
Total = 13
A Simple Risk Score for Predic*on of Contrast-‐Induced Nephropathy ARer Percutaneous Coronary Interven*on Mehran R, Aymong ED, Nikolsky E, et al
J Am Coll Cardiol, 2004
Low Mod
Mod
High

Am J Cardiol, 2014

Valida*on of a New Risk Score to Predict Contrast-‐Induced Nephropathy ARer Percutaneous Coronary Interven*on Tziakas D, Chalikias G, Stakos D, Altun A, Sivri N, Yetkin E, Gur M, Stankovic G, et al
Am J Cardiol, 2014

Valida*on of a New Risk Score to Predict Contrast-‐Induced Nephropathy ARer Percutaneous Coronary Interven*on Tziakas D, Chalikias G, Stakos D, Altun A, Sivri N, Yetkin E, Gur M, Stankovic G, et al
Am J Cardiol, 2014
2
2

Risk Score Risk for CI-‐AKI < 3 7.5% > 3 34%
Valida*on of a New Risk Score to Predict Contrast-‐Induced Nephropathy ARer Percutaneous Coronary Interven*on Tziakas D, Chalikias G, Stakos D, Altun A, Sivri N, Yetkin E, Gur M, Stankovic G, et al
Am J Cardiol, 2014

Risk Score Risk for CI-‐AKI < 3 7.5% > 3 34%
Valida*on of a New Risk Score to Predict Contrast-‐Induced Nephropathy ARer Percutaneous Coronary Interven*on Tziakas D, Chalikias G, Stakos D, Altun A, Sivri N, Yetkin E, Gur M, Stankovic G, et al
Am J Cardiol, 2014
Comparison of Tziakas Risk Score vs Mehran Risk Stra*fica*on in Predic*ng Contrast-‐Induced Acute Kidney Injury among Pa*ents Undergoing Coronary Angiography or Percutaneous Coronary Interven*on at SLMC-‐QC Ogbac FE, Gonzales-‐Prociuncula L, Buaron MJ, Semeniano R, Cheng F, Naidas O • P-‐ Pa=ents undergoing coronary
angiography and/or PCI at St Luke’s QC
• I-‐ Mehran vs Tziakas
• O-‐ occurrence of CI-‐AKI SLMC-‐QC Sec=on of Nephrology, 2014
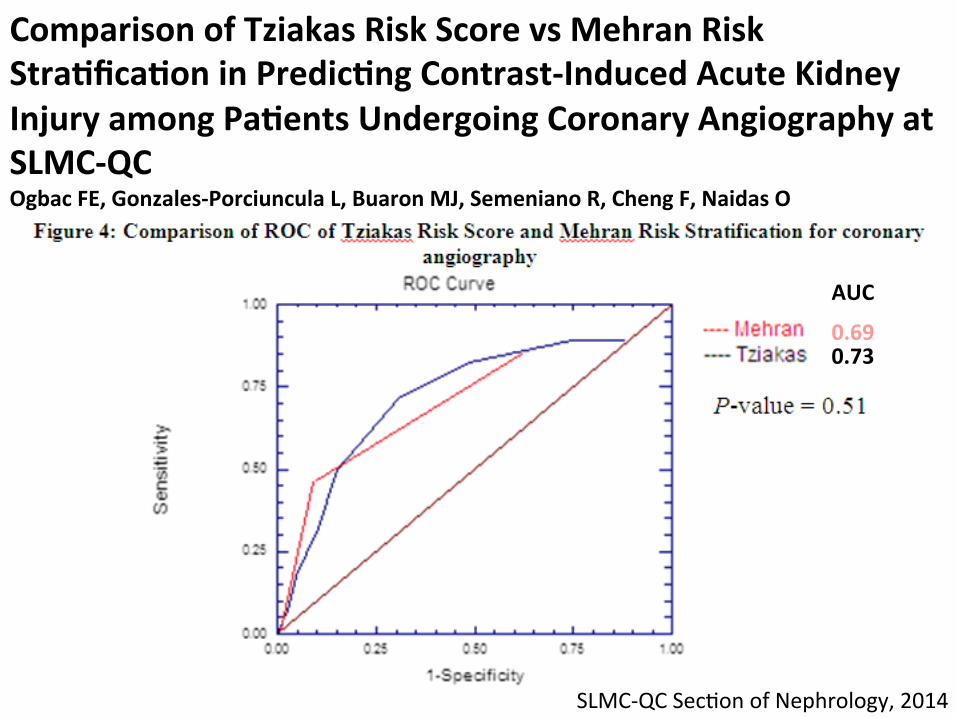
Comparison of Tziakas Risk Score vs Mehran Risk Stra*fica*on in Predic*ng Contrast-‐Induced Acute Kidney Injury among Pa*ents Undergoing Coronary Angiography at SLMC-‐QC Ogbac FE, Gonzales-‐Porciuncula L, Buaron MJ, Semeniano R, Cheng F, Naidas O
SLMC-‐QC Sec=on of Nephrology, 2014
AUC
0.69 0.73

Comparison of Tziakas Risk Score vs Mehran Risk Stra*fica*on in Predic*ng Contrast-‐Induced Acute Kidney Injury among Pa*ents Undergoing Percutaneous Coronary Interven*on at SLMC-‐QC Ogbac FE, Gonzales-‐Porciuncula L, Buaron MJ, Semeniano R, Cheng F, Naidas O
SLMC-‐QC Sec=on of Nephrology, 2014
AUC
071 0.79

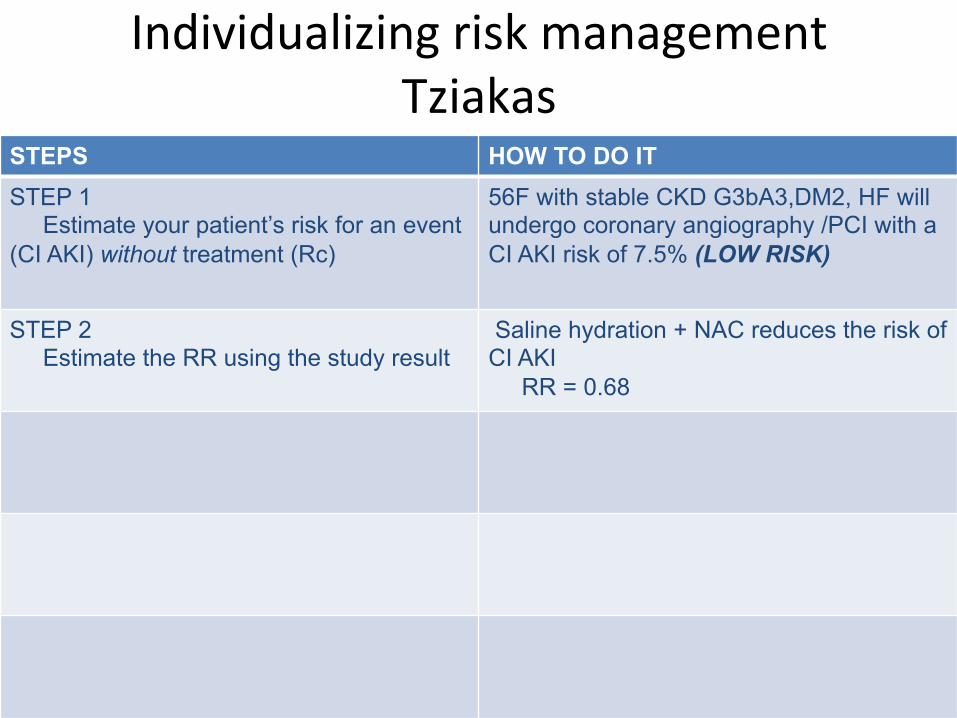
Individualizing risk management Tziakas
STEPS HOW TO DO IT STEP 1 Estimate your patient’s risk for an event (CI AKI) without treatment (Rc)
56F with stable CKD G3bA3,DM2, HF will undergo coronary angiography /PCI with a CI AKI risk of 7.5% (LOW RISK)


Preven*on of CI-‐AKI • Low osmolal or iso-‐osmolal contrast agents • Isotonic saline or isotonic bicarbonate 3 ml/kg 3 hrs prior to procedure and 1 ml/kg/hours for 6 hours ager the procedure
• Leg ventricular end diastolic pressure guided fluid replacement
• Acetylcysteine 1200mg BID • Discon=nua=on of renal vasoconstric=ng agents
Uptodate, 2015
Individualizing risk management Tziakas
STEPS HOW TO DO IT STEP 1 Estimate your patient’s risk for an event (CI AKI) without treatment (Rc)
56F with stable CKD G3bA3,DM2, HF will undergo coronary angiography /PCI with a CI AKI risk of 7.5% (LOW RISK)
STEP 2 Estimate the RR using the study result
Saline hydration + NAC reduces the risk of CI AKI RR = 0.68

Individualizing risk management Tziakas
STEPS HOW TO DO IT STEP 1 Estimate your patient’s risk for an event (CI AKI) without treatment (Rc)
56F with stable CKD G3bA3,DM2, HF will undergo coronary angiography /PCI with a CI AKI risk of 7.5% (LOW RISK)
STEP 2 Estimate the RR using the study result
Saline hydration + NACreduces the risk of CI AKI RR = 0.68
STEP 3 Estimate your individual patient’s risk for an event(CI AKI)with treatment
Rt = Rc x RR = 7.5% x 0.68 = 5%

Individualizing risk management Tziakas
STEPS HOW TO DO IT STEP 1 Estimate your patient’s risk for an event (CI AKI) without treatment (Rc)
56F with stable CKD G3bA3,DM2, HF will undergo coronary angiography /PCI with a CI AKI risk of 7.5% (LOW RISK)
STEP 2 Estimate the RR using the study result
Saline hydration + NAC reduces the risk of CI AKI RR = 0.68
STEP 3 Estimate your individual patient’s risk for an event (CI AKI) with treatment
Rt = Rc x RR = 7.5% x 0.68 = 5%

Individualizing risk management Tziakas
STEPS HOW TO DO IT STEP 1 Estimate your patient’s risk for an event (CI AKI) without treatment (Rc)
56F with stable CKD G3bA3,DM2, HF will undergo coronary angiography /PCI with a CI AKI risk of 7.5% (LOW RISK)
STEP 2 Estimate the RR using the study result
Saline hydration + NAC reduces the risk of CI AKI RR = 0.68
STEP 3 Estimate your individual patient’s risk for an event (CI AKI) with treatment
Rt = Rc x RR = 7.5% x 0.68 = 5%
STEP 4 Estimate the individualized ARR
ARR = Rc – Rt = 7.5% -5% = 2.5% (LOW RISK)

Individualizing the results STEPS HOW TO DO IT STEP 1 Estimate your patient’s risk for an event (CIN) without treatment (Rc)
56F with stable CKD G3bA3,DM2, HF will undergo coronary angiography /PCI with a CI AKI risk of 7.5%
STEP 2 Estimate the RR using the study result
Saline hydration + NACreduces the risk of CI AKI RR = 0..68
STEP 3 Estimate your individual patient’s risk for an event with treatment
Rt = Rc x RR = 7.5% x 0.68 = 5%
STEP 4 Estimate the individualized ARR
ARR = Rc – Rt = 7.5% -5% = 2.5%
STEP 5 Estimate the individualized NNT
NNT = 100/ARR = 100/2.5 = 40

Individualizing risk management Mehran
STEPS HOW TO DO IT STEP 1 Estimate your patient’s risk for an event (CI AKI) without treatment (Rc)
56F with stable CKD G3bA3,DM2, HF will undergo coronary angiography /PCI with a CI AKI risk of 26% (MODERATE RISK)
STEP 2 Estimate the RR using the study result
Saline hydration + NAC reduces the risk of CI AKI RR = 0.68
STEP 3 Estimate your individual patient’s risk for an event (CI AKI) with treatment
Rt = Rc x RR = 26% x 0.68 = 18%
STEP 4 Estimate the individualized ARR
ARR = Rc – Rt = 26% -18% = 8% (LOW RISK)

Composi=on of a Nephrology Risk Assessment and Management
• Type of poten=al ischemic/nephrotoxic insult CA/PCI
• Assessment of risk factors of the pa=ent CKD eGFR 38ml/min, DM2,HF
• An es=mate of the risk ( quan=ta=ve or semiquan=ta=ve ) CI AKI 7.5% to 26% (LOW to MODERATE RISK)
• Management/Interven=on to reduce risk( Saline hydra.on+NAC reduce risk to 2.5% to 8% (LOW RISK)
• Risk vs Benefit Benefit of CA/PCI outweighs LOW RISK of CI AKI
• Communica=on with the referring physician and/or the pa=ent

The Pa*ent withCKD who will undergo abdominal surgery
• 56 F, DM2, HTN • Insulin 10u SQ OD • Telmisartan 40mg OD, Metoprolol 50mg BID • BP: 130/90 mmHg Wt: 60kg • SCr 1.5 Uprotein: +2 eGFR:38.5 mL/min • Hb/Hct: 11/30 HbA1C: 7% Alb: 2.8mg/dL • CT Scan: solid mass at pancrea=c tail, ascites • Coroangio: nega=ve • Pre-‐op CV: stra=fica=on intermediate to high risk of developing periopera=ve CV complica=ons
• Par=al pancreatectomy
• Referred for “Nephrology Clearance”

Anesthesiology, 2009

Development and valida*on of an Acute Kidney Injury Risk Index for Pa*ents Undergoing General Surgery Kheterpal S, Tremper KK, Heung M, et al
Anesthesiology, 2009

Total = 6
Development and valida*on of an Acute Kidney Injury Risk Index for Pa*ents Undergoing General Surgery Kheterpal S, Tremper KK, Heung M, et al
Anesthesiology, 2009

Preopera*ve Risk Class AKI incidence (%) HR (95%, CI) Class I (0-‐2 risk factors) 0.2 Class II (3 risk factors) 0.8 4.0 (2.9 – 5.4) Class III (4risk factors) 1.8 8.8 (6.6 – 11.8) Class IV (5 risk factors) 3.3 16.1 (11.9 – 21.8) Class V (6+ risk factors) 8.9 46.3 (34.2 – 62.6)
Development and Valida*on of an Acute Kidney Injury Risk Index for Pa*ents Undergoing General Surgery Kheterpal S, Tremper KK, Heung M, et al
Anesthesiology, 2009

Preopera*ve Risk Class AKI incidence (%) HR (95%, CI) Class I (0-‐2 risk factors) 0.2 Class II (3 risk factors) 0.8 4.0 (2.9 – 5.4) Class III (4risk factors) 1.8 8.8 (6.6 – 11.8) Class IV (5 risk factors) 3.3 16.1 (11.9 – 21.8) Class V (6+ risk factors) 8.9 46.3 (34.2 – 62.6)
Development and valida*on of an Acute Kidney Injury Risk Index for Pa*ents Undergoing General Surgery Kheterpal S, Tremper KK, Heung M, et al
Anesthesiology, 2009

Pre-‐opera*ve Renal Risk Stra*fica*on of our pa*ent (Class V)
• The incidence of AKI ager exploratory laparotomy is 9%
• She is 46x more likely to develop AKI post exploratory laparotomy vs Class I pa=ents

Individualizing risk management STEPS HOW TO DO IT
STEP 1 Es=mate your pa=ent’s risk for an event (AKI) without treatment (Rc)
56F, stable CKD G3bA3,DM2 will undergo abdominal surgery with a risk of post op AKI 9% (HIGH RISK)


Individualizing risk management STEPS HOW TO DO IT
STEP 1 Es=mate your pa=ent’s risk for an event (AKI) without treatment (Rc)
56F, stable CKD G3bA3,DM2 will undergo abdominal surgery with a risk of post op AKI 9% (HIGH RISK)
STEP 2 Es=mate the RR using the study result
Periopera=ve hemodynamic op=miza=on, reduces the risk of post op AKI RR = 0.64

Individualizing risk management STEPS HOW TO DO IT
STEP 1 Es=mate your pa=ent’s risk for an event (AKI) without treatment (Rc)
56F, stable CKD G3bA3,DM2 will undergo abdominal surgery with a risk of post op AKI 9% (HIGH RISK)
STEP 2 Es=mate the RR using the study result
Periopera=ve hemodynamic op=miza=on, reduces the risk of post op AKI RR = 0.64
STEP 3 Es=mate your individual pa=ent’s risk for an event (AKI) with treatment
Rt = Rc x RR = 9% x 0.64 = 6%

Individualizing risk management STEPS HOW TO DO IT
STEP 1 Es=mate your pa=ent’s risk for an event (AKI) without treatment (Rc)
56F, stable CKD G3bA3,DM2 will undergo abdominal surgery with a risk of post op AKI 9% (HIGH RISK)
STEP 2 Es=mate the RR using the study result
Periopera=ve hemodynamic op=miza=on, reduces the risk of post op AKI RR = 0.64
STEP 3 Es=mate your individual pa=ent’s risk for an event (AKI) with treatment
Rt = Rc x RR = 9% x 0.64 = 6%
STEP 4 Es=mate the individualized ARR
ARR = Rc – Rt = 9% -‐ 6% = 3% (MODERATE RISK)

Composi=on of a Nephrology Risk Assessment and Management
• Type of poten=al ischemic/nephrotoxic insult Par.al pancreatectomy
• Assessment of risk factors of the pa=ent 56F,CKD,DM,2HTN • An es=mate of the risk ( quan=ta=ve or semiquan=ta=ve ) GS AKI
Risk 9% (HIGH RISK)
• Management/Interven=on to reduce risk Periopera.ve hemodynamic op.miza.on reduces risk to 3% (MODERATE RISK)
• Risk vs Benefit Benefit of par.al pancreatectomy outweighs MODERATE RISK of post op AKI
• Communica=on with the referring physician and/or the pa=ent

The pa*ent with CKD will undergo MRI w gadolinium contrast
• 57 F, DM2, and HTN • Insulin 10u SQ OD • Telmisartan 40mg OD, Metoprolol 50mg BID • BP: 120/90 mmHg Wt: 60kg • SCr 1.6 eGFR: 35.4 ml/min/1.73m2 • Hb/Hct: 10/30 HbA1C: 7% Alb: 3.5 mg/dl • Changes in sensorium t/c CVD vs metastasis
• Will undergo MRI with gadolinium contrast


American College of Radiology Manual on Contrast Media (Ver 9, 2013) Nephrogenic Sytemic Fibrosis • A fibrosing disease primarily involving the skin and subcutaneous =ssues seen in pa=ents with renal problem
ACR Manual on Contrast Media, 2013

American College of Radiology Manual on Contrast Media (Ver 9, 2013) Risk Factors for NSF • Gadolinium based contrast agent administra=on • Hemodialysis • Chronic Kidney Disease • Acute Kidney Injury • High dose and mul=ple exposure
ACR Manual on Contrast Media, 2013

American College of Radiology Manual on Contrast Media (Ver 9, 2013)
ACR Manual on Contrast Media, 2013
For Inpa*ents: • eGFR should be obtained within 2 days prior to giving gadolinium

American College of Radiology Manual on Contrast Media (Ver 9, 2013)
ACR Manual on Contrast Media, 2013
For Inpa*ents: • eGFR should be obtained within 2 days prior to giving gadolinium

American College of Radiology Manual on Contrast Media (Ver 9, 2013) For pa*ents with eGFR < 30 ml/min/1.73m2: • Gadolinium agents should be avoided • If gadolinium enhanced MRI is deemed essen=al, use of the
lowest possible dose is recommended For pa*ents with eGFR 30-‐39 ml/min/1.73m2: • NSF is rare, but precau=ons are recommended For pa*ents with eGFR 40-‐59 ml/min/1.73m2: • NSF is rare, with no precau=ons For pa*ents with eGFR > 60 ml/min/1.73m2: • No evidence of increased risk of developing NSF
ACR Manual on Contrast Media, 2013

American College of Radiology Manual on Contrast Media (Ver 9, 2013) For pa*ents with AKI • Gadolinium agents should only be administered if absolutely necessary
ACR Manual on Contrast Media, 2013

American College of Radiology Manual on Contrast Media (Ver 9, 2013) For pa*ents on dialysis: • Gadolinium enhanced MRI be performed as closely as before hemodialysis
ACR Manual on Contrast Media, 2013

Composi=on of a Nephrology Risk Assessment and Management
• Type of poten=al ischemic/nephrotoxic insult MRI w Gadolinium Contrast
• Assessment of risk factors of the pa=ent 56F,CKD,DM2,HTN,eGFR 35ml/min
• • An es=mate of the risk ( quan=ta=ve or semiquan=ta=ve ) NSF is rare
• Management/Interven=on to reduce risk ? Lower dose of gadolinium
• Risk vs Benefit Benefit of MRI w gadolinium contrast outweighs VERY LOW RISK of NSF
• • Communica=on with the referring physician and/or the pa=ent
What he just said ... • Nephrology Clearance vs Nephrology Risk Stra=fica=on / Assessment and Management
• Composi=on of “Nephrology Clearance” – Type of poten=al ischemic/nephrotoxic insult – Assessment of risk factors of the pa=ent – An es=mate of the risk ( quan=ta=ve or semiquan=ta=ve )
– Management/Interven=on to reduce risk – Risk vs Benefit – Communica=on with the referring physician and/or the pa=ent

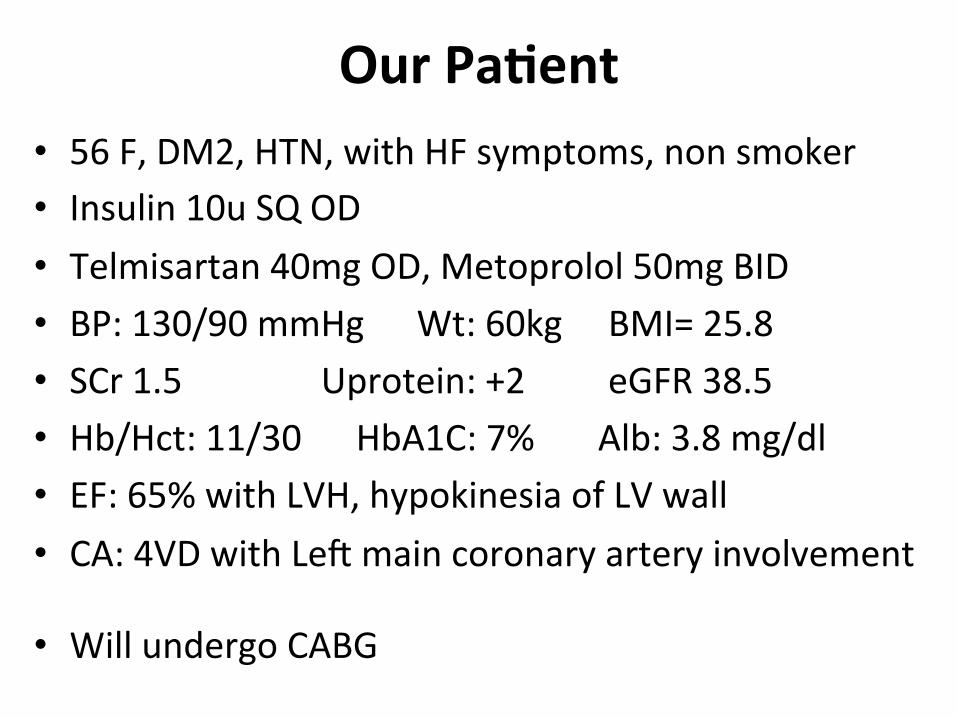
Our Pa*ent • 56 F, DM2, HTN, with HF symptoms, non smoker • Insulin 10u SQ OD • Telmisartan 40mg OD, Metoprolol 50mg BID • BP: 130/90 mmHg Wt: 60kg BMI= 25.8 • SCr 1.5 Uprotein: +2 eGFR 38.5 • Hb/Hct: 11/30 HbA1C: 7% Alb: 3.8 mg/dl • EF: 65% with LVH, hypokinesia of LV wall • CA: 4VD with Leg main coronary artery involvement
• Will undergo CABG
Predic*ve Indices for Es*ma*ng Risk of Post-‐Cardiac Surgery RRT
• SRI – Wijeysundera, et al. Deriva=on and valida=on of a simplified predic=ve index for renal replacement therapy ager cardiac surgery. JAMA, 2005.
• Mehta, et al. Bedside Tool for predic=ng the risk of postopera=ve dialysis in pa=ents undergoing cardiac surgery. Circula=on, 2006
• Thakar, et al. A clinical score to predict acute renal failure ager cardiac surgery. J AM Soc Nephrol, 2005.

Comparison of Predic*ve Indices for Es*ma*ng Risk of Post-‐Cardiac Surgery RRT
Index No. of variables
Score range AUC (Toronto cohort)
SRI 2007 8 0 – 8 0.78 (0.72-‐0.84)
Mehta 2005 10 0 – 83 0.75 (0.66-‐0.83)
Thakar 2005 13 0 – 17 0.81 (0.74-‐0.86)
JAMA, 2007
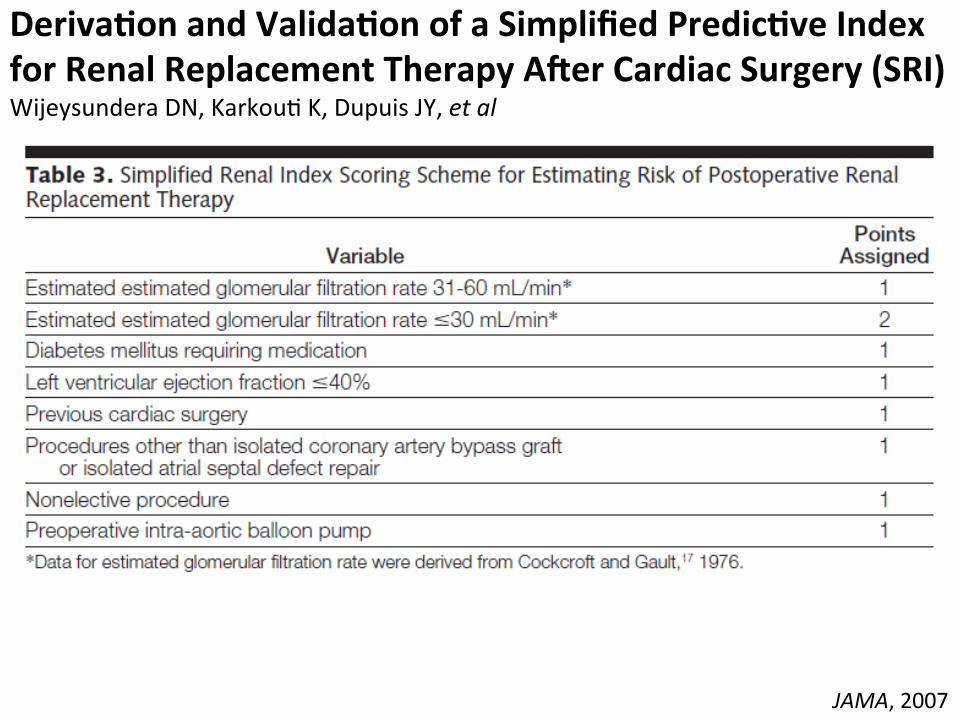
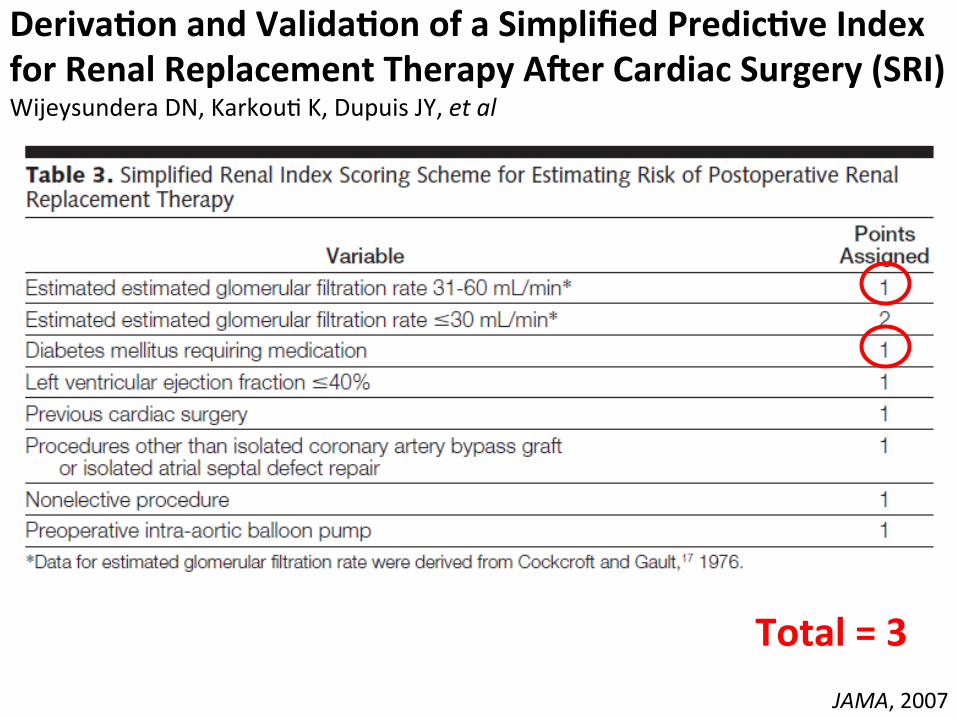
Deriva*on and Valida*on of a Simplified Predic*ve Index for Renal Replacement Therapy ARer Cardiac Surgery (SRI) Wijeysundera DN, Karkou= K, Dupuis JY, et al
JAMA, 2007
JAMA, 2007
Total = 3
Deriva*on and Valida*on of a Simplified Predic*ve Index for Renal Replacement Therapy ARer Cardiac Surgery (SRI) Wijeysundera DN, Karkou= K, Dupuis JY, et al

Risk Categories Risk of RRT (%) Low Risk (0 to 1 point) 0.4 Intermediate Risk (2 to 3 points) 3 High Risk (> 4 points) 10
JAMA, 2007
Deriva*on and Valida*on of a Simplified Predic*ve Index for Renal Replacement Therapy ARer Cardiac Surgery (SRI) Wijeysundera DN, Karkou= K, Dupuis JY, et al

Risk Categories Risk of RRT (%) Low Risk (0 to 1 point) 0.4 Intermediate Risk (2 to 3 points) 3 High Risk (> 4 points) 10
JAMA, 2007
Deriva*on and Valida*on of a Simplified Predic*ve Index for Renal Replacement Therapy ARer Cardiac Surgery Wijeysundera DN, Karkou= K, Dupuis JY, et al

Circula5on, 2006

Bedside Tool for Predic*ng the Risk of Postopera*ve Dialysis in Pa*ents Undergoing Cardiac Surgery Mehta RH, Grab JD, O’Brien SM, et al
Circula5on, 2006

Bedside Tool for Predic*ng the Risk of Postopera*ve Dialysis in Pa*ents Undergoing Cardiac Surgery Mehta RH, Grab JD, O’Brien SM, et al
Circula5on, 2006
12
1
0 5
0
2 0
0
0
20

Bedside Tool for Predic*ng the Risk of Postopera*ve Dialysis in Pa*ents Undergoing Cardiac Surgery Mehta RH, Grab JD, O’Brien SM, et al
Circula5on, 2006

1.1%
Bedside Tool for Predic*ng the Risk of Postopera*ve Dialysis in Pa*ents Undergoing Cardiac Surgery Mehta RH, Grab JD, O’Brien SM, et al
Circula5on, 2006

J Am Soc Nephrol, 2005

A Clinical Score to Predict Acute Renal Failure aRer Cardiac Surgery Thakar CV, Arrigain S, Worley S, Yared JP, Paganini EP
J Am Soc Nephrol, 2005

A Clinical Score to Predict Acute Renal Failure aRer Cardiac Surgery Thakar CV, Arrigain S, Worley S, Yared JP, Paganini EP
J Am Soc Nephrol, 2005
Total = 5

Risk Categories Risk of RRT (%) 0 – 2 0.4 3 – 5 1.8 6 – 8 7.8 9 – 13 21.5
A Clinical Score to Predict Acute Renal Failure aRer Cardiac Surgery Thakar CV, Arrigain S, Worley S, Yared JP, Paganini EP
J Am Soc Nephrol, 2005

Comparison of Predic*ve Indices for Es*ma*ng Risk of Post-‐Cardiac Surgery RRT
Index No. of variables
Score range
Risk Score Risk for RRT post CABG (%)
SRI 2007 8 0 – 8 3 3 Mehta 2005
30 0 – 83 20 1.1
Thakar 2005
13 0 – 17 5 1.8
The risk of AKI requiring RRT post-‐cardiac surgery is between 1.1 to 3%

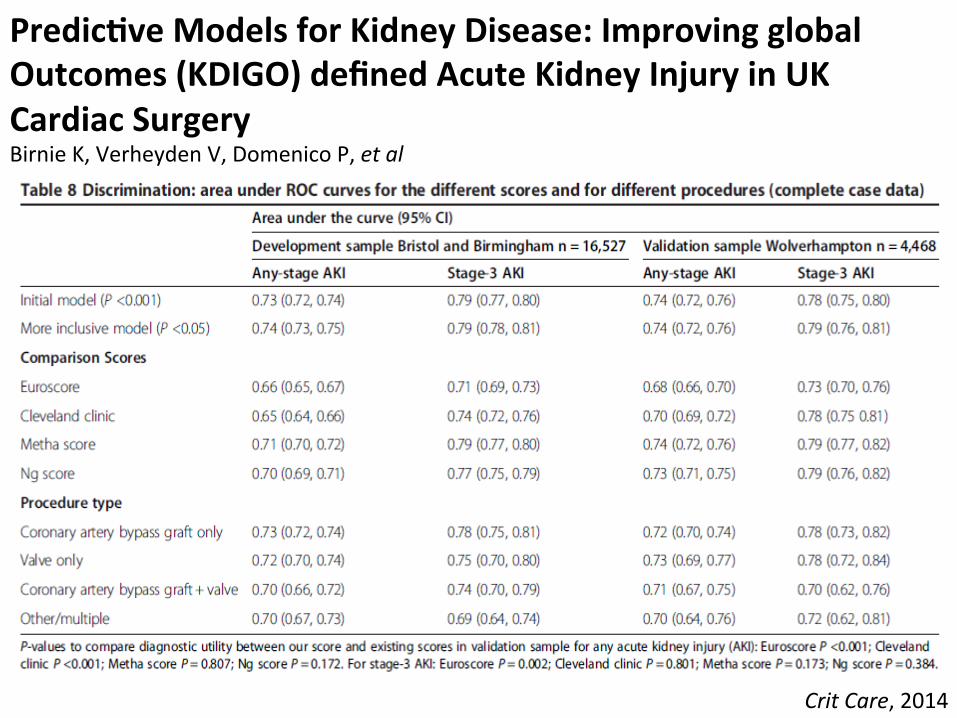
Crit Care, 2014

• P-‐ 20,995 pa=ents underwent cardiac surgery including surgery to thoracic aorta (3 different centers)
• I-‐ retrospec=ve cohort
• O-‐ occurrence of CI-‐AKI and need for RRT
Predic*ve Models for Kidney Disease: Improving global Outcomes (KDIGO) defined Acute Kidney Injury in UK Cardiac Surgery Birnie K, Verheyden V, Domenico P, et al
Crit Care, 2014
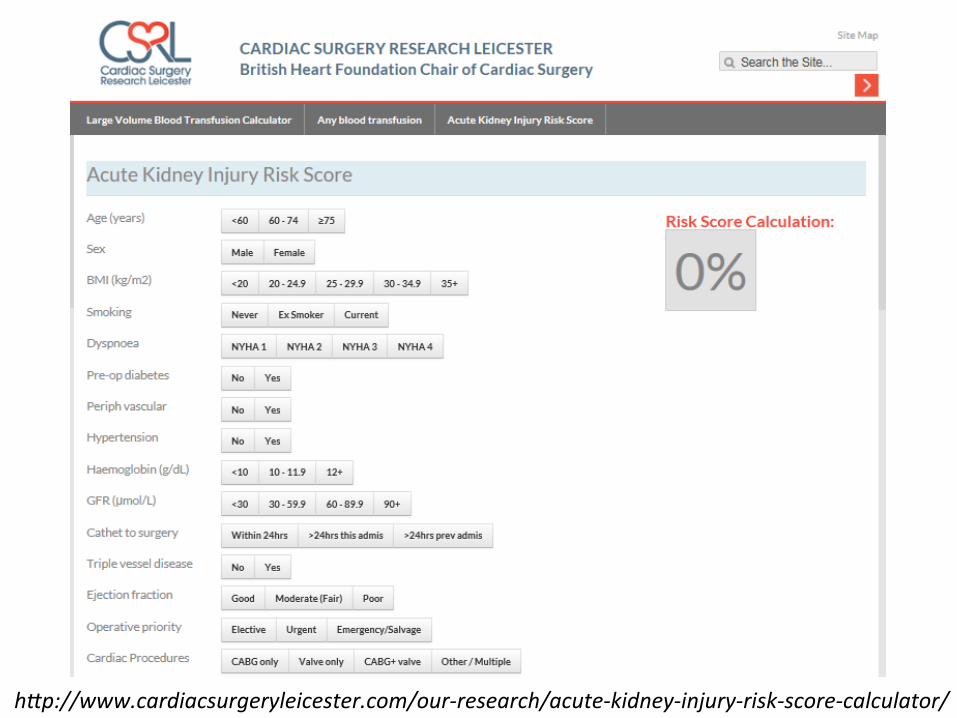
hHp://www.cardiacsurgeryleicester.com/our-‐research/acute-‐kidney-‐injury-‐risk-‐score-‐calculator/
Predic*ve Models for Kidney Disease: Improving global Outcomes (KDIGO) defined Acute Kidney Injury in UK Cardiac Surgery Birnie K, Verheyden V, Domenico P, et al
Crit Care, 2014
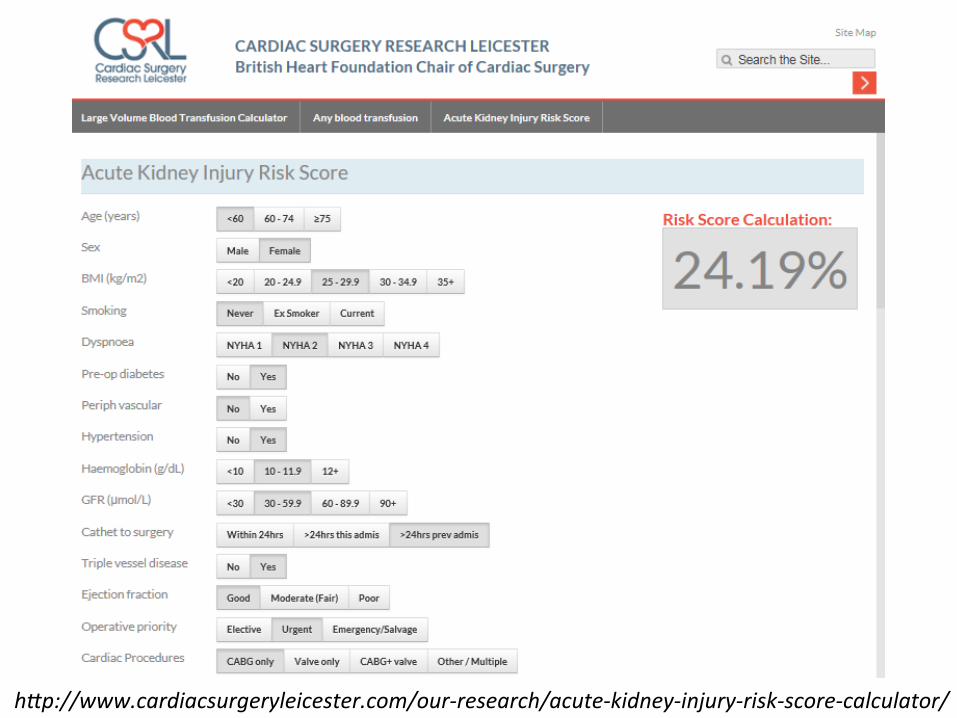
hHp://www.cardiacsurgeryleicester.com/our-‐research/acute-‐kidney-‐injury-‐risk-‐score-‐calculator/

Periopera*ve Acute Kidney Injury Calvet S, Shaw A
Preven*ve measures for cardiac surgery • Fluids and goal directed therapy • Avoidance of nephrotoxic agents • Hemodilu=on and transfusion
Perioper Med, 2012

Our pa*ent post-‐op… • 57 F, DM2, and HTN • Insulin 10u SQ OD • Telmisartan 40mg OD, Metoprolol 50mg BID • BP: 120/90 mmHg Wt: 60kg • SCr 1.6 eGFR: 35.4 ml/min • Hb/Hct: 10/30 HbA1C: 7% Alb: 3.5 mg/dl • Histopath: cervical CA
• Will undergo cispla=n chemotherapy

Risk Factors for Cispla*n Nephrotoxicity • Previous cispla=n chemotherapy • Pre-‐exis=ng kidney damage • Concomitant administra=on of poten=ally nephrotoxic agents
• High peak plasma free pla=num concentra=ons
Uptodate, 2014

Preven*on of Cispla*n Nephrotoxicity • Lower dose of cispla=n • 1L isotonic saline + 20 meqs KCl + 2gms MgSO4 3 hours prior to administering chemotherapy and minimum of 500ml over 2 hours following administra=on
Uptodate, 2015

THANK YOU