Embed Size (px)
Citation preview

1
Why are you here??• Want to know more about waiting times
policy in NHSScotland?• Involved in local/regional/national working
groups?• Leading a team/department/Board (!) and
want to know what’s next?

2
Waiting times policy: 2008 and beyond
Colin LauderScottish Government
Health Delivery Directorate

3
Why bother with targets??
• Earlier diagnosis can lead to improved outcomes
• Reduce unnecessary worry and uncertainty
• Inequality of access between Boards and hospitals
• Reduce waste – managing queues

4
Inpatients Waiting Over 9, 6 months and 18 Weeks
0
5000
10000
15000
20000
25000
Sep-02
Dec-02
Mar-03
Jun-03
Sep-03
Dec-03
Mar-04
Jun-04
Sep-04
Dec-04
Mar-05
Jun-05
Sep-05
Dec-05
Mar-06
Jun-06
Sep-06
Dec-06
Mar-07
Jun-07
Sep-07
Dec-07
Num
ber o
f Pat
ient
s
Over 18 weeks
Over 6 Months
Over 9 Months
5
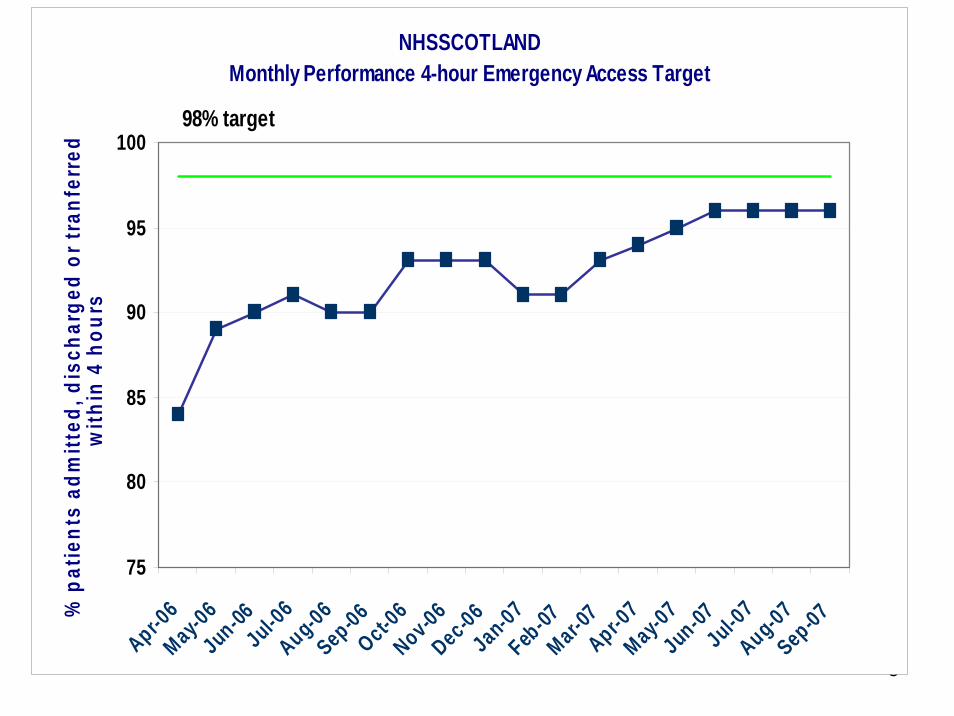
NHSSCOTLAND Monthly Performance 4-hour Emergency Access Target
75
80
85
90
95
100
Apr-06
May-06
Jun-06Jul-0
6Aug-06Sep-06Oct-0
6Nov-06Dec-06Jan-07Feb
-07Mar-0
7Apr-0
7May-0
7Jun-07
Jul-07
Aug-07Sep-07%
pat
ient
s ad
mitt
ed, d
isch
arge
d or
tran
ferr
ed
with
in 4
hou
rs98% target
6
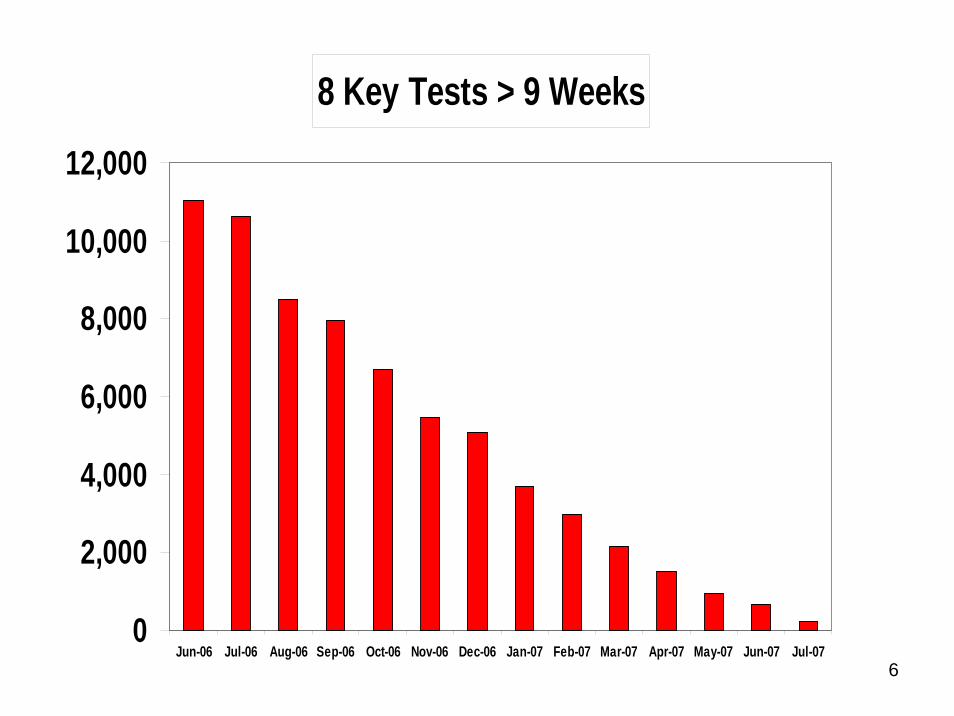
8 Key Tests > 9 Weeks
0
2,000
4,000
6,000
8,000
10,000
12,000
Jun-06 Jul-06 Aug-06 Sep-06 Oct-06 Nov-06 Dec-06 Jan-07 Feb-07 Mar-07 Apr-07 May-07 Jun-07 Jul-07

7
• A&E - 4 hours admit/discharge• Outpatients - 18 weeks from referral to clinic• Diagnostics – 9 weeks for 8 key tests• Inpatients/Daycases - 18 weeks from decision to
treat to treatment • Cardiac conditions – 16 weeks from referral (to
RACP) or from specialist clinic to treatment • Cancer – 62 days from urgent referral to treatment• Cataract Surgery - 18 weeks from referral to
treatment• Hip Fracture - 24 hours from admission to operation

8
“Better Health, Better Care”From December 2011, 18 weeks will become the maximum wait for treatment following referral by a GP for non-urgent patients. Most patients will be seen more quickly than this.Page 68

9
• Redesign StrategyMaking the best use of current capacity, improving flow and bringing best practice to systems and healthcare delivery.• Planning StrategyIntegrated financial, workforce and capacity plans in LDP• Information StrategySetting definitions, developing and using information and eHealth technology to supporting the Programme.• Performance Management StrategyEnsuring clear targets are set, and service improvement momentum is maintained between 2008 and 2011.
10
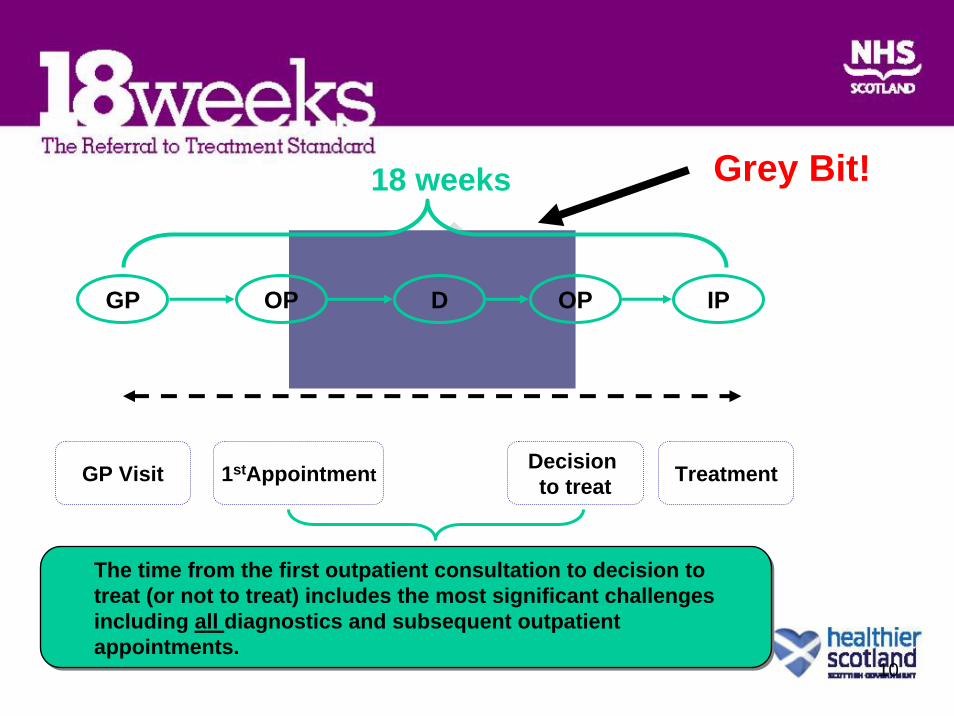
GP IPOP D OP
18 weeks
GP Visit 1stAppointment Decision to treat Treatment
The time from the first outpatient consultation to decision to treat (or not to treat) includes the most significant challengesincluding all diagnostics and subsequent outpatient appointments.
The time from the first outpatient consultation to decision to treat (or not to treat) includes the most significant challengesincluding all diagnostics and subsequent outpatient appointments.
Grey Bit!

11
Workforce planning / development• Whole system view of activity / workforce /
finance• Shift from consultant-delivered services• Continued extended roles for nurses and
AHPs• Competency based approach• Should evolve through current planning
mechanisms……
12
Information Strategy• Delivery Team focus• Three primary tasks
1: defining 2: measuring 3: reporting (HEAT 09/10)
• Only 9 months to PTL and to RTT targets
13
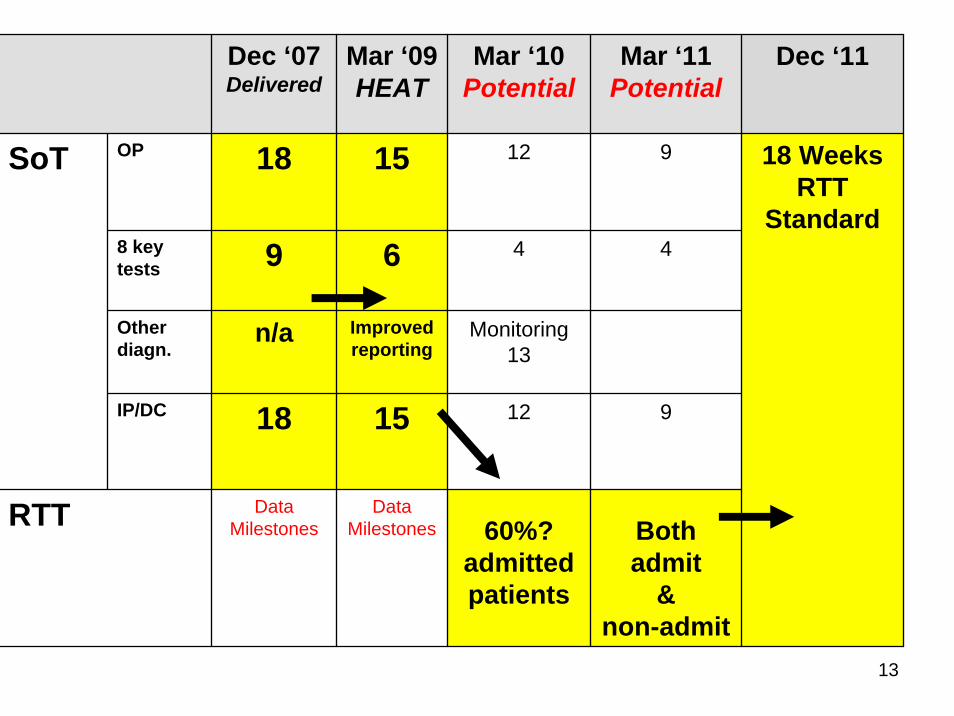
85% non-admitted patients
Dec ‘07Delivered
Mar ‘09HEAT
Mar ‘10Potential
Mar ‘11Potential
Dec ‘11
OP 18 15 12 9
8 key tests 9 6 4 4
Other diagn.
n/a Improved reporting
Monitoring13
IP/DC 18 15 12 9
RTT DataMilestones
DataMilestones 60%?
admitted patients
Both admit
&non-admit
18 Weeks RTT
Standard
SoT

14
Key Features of Programme• Improving on the Delivery Strategy we know • But, not more of the same waiting list initiatives• Continuing the momentum behind redesign
programmes• Using existing capacity & workforce to best
effect• Stage-of-treatment milestones for OP, IP/DC,
diagnostics, moving to RTT measures• Shameless plagiarism….
15
Tracey Gillies
Consultant Surgeon NHS Lothian

16
• Scale and scope• Need to move from stage of
treatment to pathway• Need information about
pathway for improvement and ultimately for measurement of target
What are the challenges for clinical teams in delivering 18RTT?

17
Redesign the patient pathway
Pre-referral Referral Clinical Assessment
Decision to treat
Treatment Discharge from Secondary Care
Review Discharge from pathway
Adapted from NHS Institute Delivering 18 Weeks
18
Redesign
Backlog
Two streams of work going on in parallel
Towards an 18 week total journey by 2011
Between 2008 and 2011
19
Mind the gap!
12 4 or 6 12!!
Many diagnostic cycles result in a further clinic visitDiagnostic cycles may be multipleNot all diagnostics are covered by interim stage of treatment targets
20
Service Redesign and TransformationSustainableApply key principles:Shifting the Balance of Care Merge/ remove steps in the process (add value/
remove waste)
What is the vision ?
21
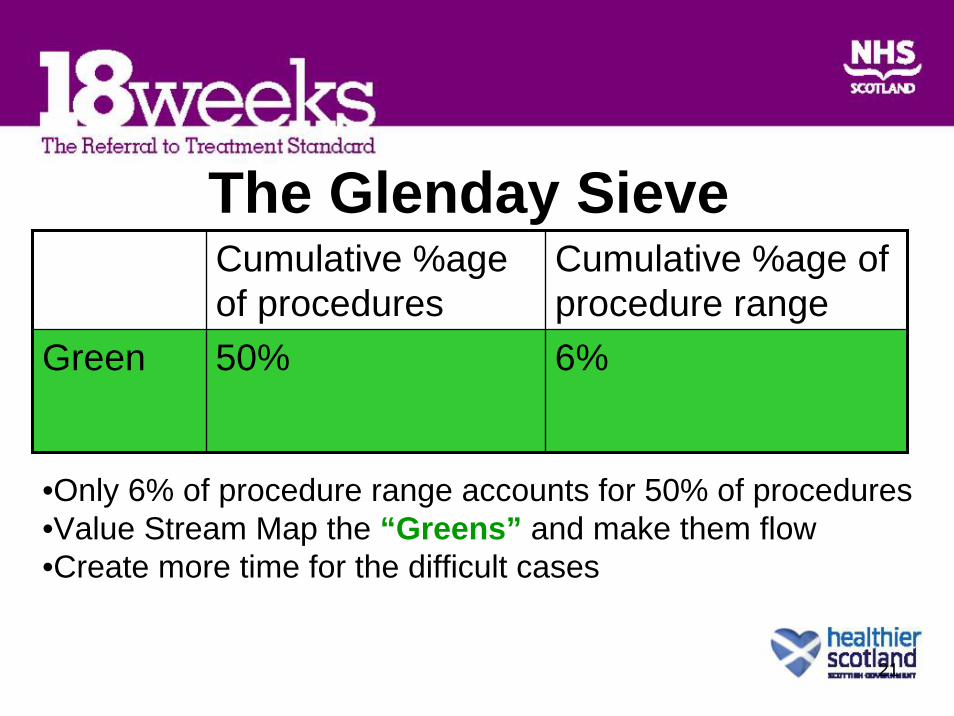
The Glenday SieveCumulative %age of procedures
Cumulative %age of procedure range
Green 50% 6%
•Only 6% of procedure range accounts for 50% of procedures•Value Stream Map the “Greens” and make them flow•Create more time for the difficult cases

22
Develop a vision for service

23
For Patients • Faster treatment and care, earlier relief of symptoms.• Fewer hospital visits• Reduced anxiety• Earlier diagnosis• Greater confidence in the NHS
For Staff• Managing the whole patient pathway-not just stages of
treatment• Easier to plan and manage workload• Better use of professional time• More productive working• Closer working between GPs and hospital clinicians• Knowing where patient are on their pathway
What are the benefits?
18 WEEKS
FROM GP REFERRAL TO TREATMENT
24
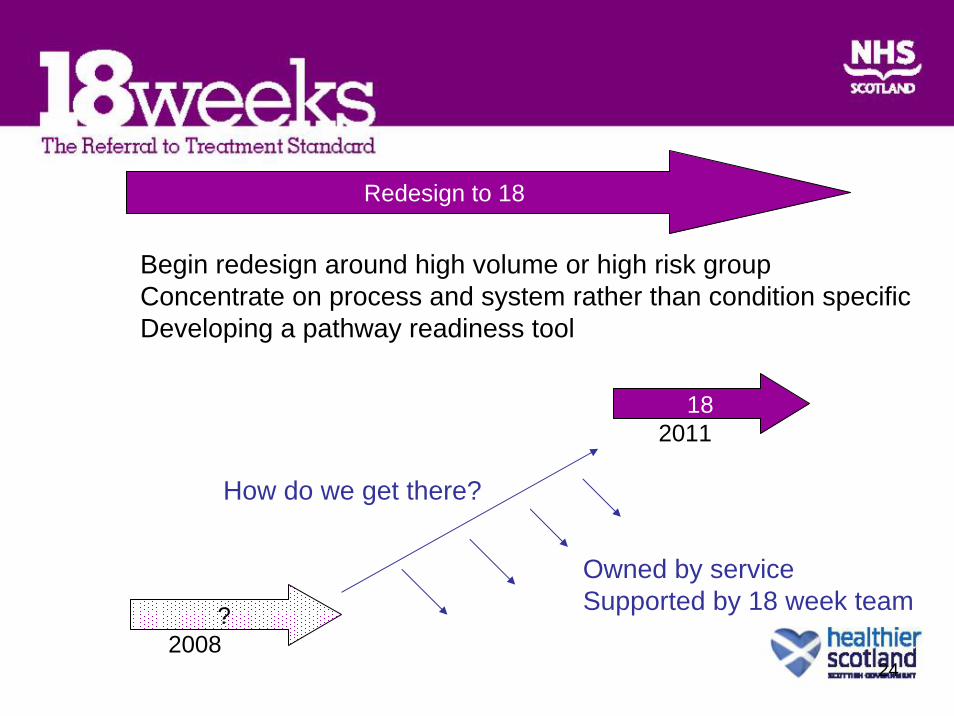
Redesign to 18
Begin redesign around high volume or high risk groupConcentrate on process and system rather than condition specificDeveloping a pathway readiness tool
18
?2008
2011
How do we get there?
Owned by serviceSupported by 18 week team

25
Building on previous experience and best practice
26
27
Information
• Locally owned and understood
• Rapidly available and updated
• Relates to patient pathway
• Allow flexing of capacity to demand

28
Primary Care involvement/Shifting the Balance of Care
• Primary care involvement crucial
• Integrated working with partners across the whole health community
• Clear lines of communication
• Effect on patient if wrong pathway used

29
How might things look in the future?
• One Stop Models & Direct Access• Clear Referral protocols• Improved patient pathway• Reducing non-value added steps• e referrals • Referral Management

30
What we can do now• Gain a clear understanding of Admitted and Non-admitted
• Size of the challenge.
• Clinic Outcomes – why wait?• What happened to the patient?• What is the next stage?
• Non guaranteed Diagnostic Tests
• Communication• Improved links between Primary and Secondary Care

31
“Early involvement of stakeholders and staff with the appropriate operational and clinical knowledge will be necessary to raise awareness of the tasks and challenges. Clinical champions and executive leadership with visible support will be vital in order to implement the plans that will enable RTT measurement.”
18 weeks: The Referral to Treatment Standard

32

33
Tim DavisonChief Executive
NHS Lanarkshire

34
• PAST EXPERIENCE
• FUTURE CHALLENGE
35
• PAST EXPERIENCE– Build on Past Gains– Case Study’s – Changes that Work
• Case StudyStraight to test• One stop Sigmoidoscopy and Barium Enema
service – NHS Lanarkshire

36
ONE-STOP SIGMOIDOSCOPY AND BARIUM ENEMA SERVICE - LANARKSHIRE
• What was the problem• Different ways of working at 3 sites• No clear picture of demand• No cross-site working• Long waiting times for outpatient scans of up to 21
weeks• Patients had to have multiple visits for their barium
and sigmoidoscopy appointments

37
• How was this identified?• Process Mapping• Demand, Capacity, Activity and Queue (DCAQ)
analysis
• What were the implemented improvements?
• One stop sigmoidoscopy and barium enema service so patients only visit hospital once for 2 tests
38
• What is the situation now?• Waiting times are below 4 weeks
• How is this sustainable?• Continual monitoring of DCAQ analysis
• Audit• Backlog reduced from 729 to 124 patients waiting
of which 132 waited over 9 weeks. Now no-one waits longer than 4 weeks.

39
• Waiting Times• This improvement has contributed to a reduction in
waiting times from 12 weeks in May 2006 to 6 weeks in December 2006
• Patient benefits• Patient only has to take bowel preparation once due to
this one-stop service• Reduced waiting times for out-patients
• Staff benefits• Morale has increased as the pressure of work has
reduced

40
– LEADERSHIP CHALLENGE
FUTURE CHALLENGE
•CHIEF EXECUTIVE
•MIDDLE MANAGEMENT
•DEPARTMENT MANAGEMENT
•CLINICAL LEADS

41
SERVICE REDESIGN AND TRANSFORMATION• WHOLE PATIENT PATHWAY
• Shifting from current stages of treatment to whole pathways of care
– Protocols
– ereferrals
– PDSA
– LEAN
– DCAQ
– Methodology
42
BALANCE OF ELECTIVE AND EMERGENCY CARE“To ensure a safe and balanced health care service, elective access targets must not unbalance the system, and equal emphasis should be placed upon access to unscheduled care.”
The Referral to Treatment Standard:18weeks Document
Proactivebed
management system
Length of stay
Effective discharge
Access to support/diagnostic
services
Balance elective vsemergency admissions

43
PATIENTCARERGP
DAY CENTREPHYSIOTHERAPY
AMBULANCE SERVICES
ACUTE SERVICES
OUT-PATIENT CLINICSIN-PATIENT SERVICES
A&E

44
MANAGING THE RED
STUFF

45
• Managing cancer is beginning to manage the red stuff• Protocolised referrals• E-referrals• Single multi-hospital system• Patients seen where can be seen quickest• Straight to test• Common waiting lists• Patient tracking at every stage• Rapid escalation policies to manage problems• Weekly reporting• Etc etc